Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Caplacizumab (Cablivi)
Indication: For the treatment of adults with acquired thrombotic thrombocytopenic purpura in combination with plasma exchange and immunosuppressive therapy
Sponsor: Sanofi-Aventis Canada Inc.
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Cablivi?
Canada’s Drug Agency (CDA-AMC) recommends that Cablivi be reimbursed by public drug plans for the treatment of adults with acquired thrombotic thrombocytopenic purpura (aTTP) in combination with plasma exchange (PE) and immunosuppressive therapy (IST), if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
CDA-AMC previously reviewed Cablivi in 2020 and 2023, for the treatment of adults with aTTP in combination with PE and IST, and issued a recommendation not to reimburse in both reviews. This is a resubmission based on new information submitted by the sponsor to address the gaps identified in the previous recommendations.
The Canadian Drug Expert Committee (CDEC) determined that it is uncertain whether Cablivi with PE and IST demonstrates acceptable clinical value versus PE and IST alone in patients with aTTP. Given that Cablivi is expected to be an additive treatment to PE and IST, acceptable clinical value refers to added value versus PE and IST alone.
Previous CDEC recommendations for Cablivi in 2020 and 2023 concluded that treatment with Cablivi with PE and IST reduced the time for platelet counts to return to normal based on evidence from 1 clinical trial (the HERCULES study; N = 145) and other supportive studies. However, CDEC could not draw conclusions on important outcomes, such as survival, organ damage, preventing new aTTP episodes over long periods of time, use of health care resources, or quality of life. Evidence from a retrospective observational study reviewed for the resubmission (the Capla 1000+ project; N = 1,525) suggested that Cablivi with PE and IST improved survival at 3 months versus PE and IST alone in patients with aTTP. The treatment effect for other important outcomes was consistent across the study in this review and past reviews; however, there was uncertainty because of study limitations. There was also a lack of information for outcomes that are important to patients, such as long-term survival, reduced organ damage, and improved quality of life.
CDEC determined that there was significant unmet clinical need because aTTP is a severe disease despite treatments being available, and because there is difficulty with conducting clinical studies in aTTP. CDEC determined that Cablivi with PE and IST may address a significant unmet clinical need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value.
Based on all of the preceding considerations, CDEC recommended that Cablivi be reimbursed.
Which Patients Are Eligible for Coverage?
Cablivi should only be reimbursed for adults aged 18 years and older experiencing an episode of aTTP, and when used in combination with PE and IST, in line with the Health Canada indication.
What Are the Conditions for Reimbursement?
Cablivi should only be reimbursed if the maximum time that Cablivi is used for each aTTP episode is no more than 58 days after the last day that PE is used, and if the cost of Cablivi is reduced. Cablivi should only be prescribed and used by health care specialists who have expertise in managing aTTP and in a clinical setting where PE is provided.
Review Background
Disease background: aTTP is a rare and serious blood condition. It is caused by an immune reaction that stops the ADAMTS13 enzyme, which is involved in regulating the blood-clotting process, from functioning properly. Small blood clots form throughout the body ― causing symptoms of tiredness, bleeding, nausea, headache, and stroke ― and can lead to organ damage and death. If aTTP is left untreated, the risk of death is greater than 90%. No prevalence data for aTTP were available for Canada; however, thrombotic thrombocytopenic purpura is estimated to occur in 4.3 individuals per million based on data from 2012 to 2019 in Quebec.
Indication and reimbursement request: Caplacizumab (Cablivi) has been approved by Health Canada for the treatment of adults with aTTP, in combination with plasma exchange (PE) and immunosuppressive therapy (IST). The sponsor is seeking reimbursement for this patient population.
Drug under review: Caplacizumab is an antithrombotic drug. It is available as an 11 mg powder for solution that is administered by IV infusion or subcutaneous (SC) injection. The dosage recommended in the product monograph is an 11 mg bolus IV injection at least 15 minutes before PE, followed by an 11 mg SC injection after completion of PE on the first day. A once-daily 11 mg SC injection is administered after daily PE, and for 30 days after PE stops. If signs of persistent underlying disease remain present after the initial treatment course, treatment may be extended for a maximum of a further 28 days.
Treatment costs: At the submitted price of $6,200.00 per 11 mg vial, the course cost of caplacizumab is expected to be $223,200 per patient, based on the Health Canada–recommended dosage and the median duration of treatment (35 days).
Submission history: Caplacizumab was previously reviewed by CDA-AMC on 2 occasions for the treatment of adults with aTTP in combination with PE and IST, and received a recommendation not to reimburse from CDEC both times (August 26, 2020 [initial review], and April 5, 2023 [resubmission]). The initial reimbursement review of caplacizumab considered the HERCULES trial (a phase III, double-blind, randomized, placebo-controlled trial) and the TITAN trial (a phase II, single-blind, randomized, placebo-controlled trial). The first resubmission reviewed the post-HERCULES study (a phase III, prospective, follow-up study), an integrated post hoc analysis of the HERCULES and TITAN studies, and 3 studies of 2 real-world evidence (RWE) cohorts. Key reasons for the committee’s recommendations were insufficient evidence of clinically meaningful outcomes (lack of evidence on long-term survival, reduced organ damage, reduced long-term disease recurrence, reduced health care resource use, and improved health-related quality of life [HRQoL]), lack of an identifiable subpopulation most likely to benefit from the drug, and uncertainty around the generalizability to clinical practice in Canada.
Basis of resubmission: This resubmission is based on the availability of new evidence (the Capla 1000+ project), which provides new information that may support generalizability of caplacizumab use to clinical practice in Canada and support the findings of the pivotal evidence.
Highlights of Input From Interested Parties
The patient group (Answering TTP Canada, with support from the Network of Rare Blood Disorder Organizations) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
aTTP episodes are sudden and occur without warning. Patients can die without immediate treatment, and serious complications (such as stroke, heart attack, kidney injury, and organ damage) can occur despite treatment. An episode can lead to admission to the intensive care unit (ICU) and an extended hospital stay that may be far from the patient’s home, resulting in added psychological, emotional, and financial burden.
There is a need for treatment that is safe and immediately effective, and reduces total treatment time.
The clinician group (the Canadian Apheresis Group, with letters of support from 6 clinicians) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs arising from the disease and place in therapy for the drug under review:
There is a need for treatment that rapidly normalizes platelet counts and avoids the long-term complications associated with the disease (e.g., organ damage and death) and with current standard of care (SOC) treatments (i.e., PE and IST).
Caplacizumab should only be used once thrombotic microangiopathy caused by ADAMTS13 deficiency is confirmed (i.e., low ADAMTS13 activity with or without the presence of ADAMTS13 autoantibody). Once aTTP is confirmed, caplacizumab would be used as a first-line treatment with SOC treatments.
The participating public drug programs raised potential implementation issues related to considerations for initiation, discontinuation, and prescribing of therapy; generalizability of trial populations to broader populations; and system and economic issues.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through with this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input, and should be considered as 1 element contributing to a broader understanding of the condition and treatment under review.
Recommendation
With a vote of 10 in favour to 5 against, CDEC recommends that caplacizumab be reimbursed for adults with aTTP in combination with PE and IST, only if the conditions listed in Table 1 are met.
This recommendation supersedes the CDEC recommendation for this drug and indication dated April 2023.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Treatment with a course of caplacizumab should be reimbursed when initiated in combination with PE and IST for adults (aged ≥ 18 years) experiencing an episode of aTTP. | Based on the totality of the evidence reviewed, treatment of adults with aTTP with caplacizumab plus SOC was associated with improvements in time to platelet response, the rate of refractory disease, the rate of disease exacerbation, and PE duration when compared to PE and IST alone. | In the HERCULES trial, eligible patients were required to have a clinical diagnosis of aTTP, defined as thrombocytopenia and microscopic evidence of red blood cell fragmentation. CDEC agreed with the clinical experts that patients with a clinical suspicion of aTTP should have a diagnosis confirmed based on laboratory testing, including ADAMTS13 activity with or without enzyme inhibitor level (i.e., ADAMTS13 activity less than 10% and evidence of anti-ADAMTS13 antibodies), lactate dehydrogenase, complete blood count, peripheral blood film review, or diagnostic imaging. The clinical experts stated that hospitals may lack onsite ADAMTS13 testing, which can delay diagnosis and treatment. Where enzyme activity testing is not readily accessible, SOC without caplacizumab is generally initiated. However, CDEC noted that in select cases of strong clinical suspicion of aTTP, caplacizumab may be considered before confirmation of ADAMTS13 activity, based on clinical judgment. |
2. The maximum duration of initial authorization for each episode of aTTP is 58 days beyond the last daily PE. | Per the Health Canada product monograph, if after the initial treatment course of caplacizumab (i.e., 30 days after the last daily PE), signs of persistent underlying disease such as suppressed ADAMTS13 activity levels remain present, treatment with caplacizumab may be extended for a maximum of 28 days beyond the initial 30 days after the last daily PE. | CDEC noted that the dosing and duration of treatment with caplacizumab should follow the product monograph. Per the Health Canada product monograph, treatment with caplacizumab should be discontinued if the patient experiences more than 2 recurrences of aTTP while on caplacizumab. In the HERCULES trial, recurrence (exacerbation or relapse) was defined as recurrent thrombocytopenia after initial recovery of platelet count (platelet count ≥ 150 × 109/L, and daily PE must have been stopped for at least 1 day), requiring reinitiation of daily PE, occurring during the first 30 days following the daily PE period (exacerbation); or recurrent thrombocytopenia after initial recovery of platelet count requiring reinitiation of daily PE, occurring after the 30-day period following daily PE (relapse). CDEC also agreed with the clinical experts that the treatment duration of caplacizumab could be guided by ADAMTS13 response, clinical judgment, and Health Canada–recommended dose and dosage adjustment. This was based on evidence that suggested fewer relapses and exacerbations occur when caplacizumab is continued until ADAMTS13 activity exceeds 10% to 20%. |
Renewal | ||
3. In the case of new episodes of aTTP, the physician must provide evidence demonstrating that the criteria outlined in condition 1 continue to be met. | This is meant to ensure patients are still in need of treatment with caplacizumab. | — |
Prescribing | ||
4. Prescribing and treatment with caplacizumab should be limited to clinicians (e.g., specialists such as hematologists or general internists) and health care teams with expertise in managing aTTP in a clinical setting where PE is available. | This is meant to ensure that caplacizumab is prescribed for appropriate patients and that adverse effects are managed in an optimized and timely manner. | CDEC acknowledged that specialist care and resources are not always accessible to all patients across jurisdictions. CDEC and the clinical experts agreed that once the disease enters remission and a patient is released from the hospital, caplacizumab can be administered in a community or specialty clinic, or by the patient at home after adequate education and supervision. |
Pricing | ||
5. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for caplacizumab in combination with SOC was $269,158 per QALY gained when compared with SOC alone in the indicated population. A band 4 price reductiona would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. A band 3 price reductiona would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. Price reductions for any given willingness-to-pay threshold are available in the main report by CDA-AMC and its accompanying Supplemental Material document. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. |
aTTP = acquired thrombotic thrombocytopenic purpura; CDA-AMC = Canada’s Drug Agency; CDEC = Canadian Drug Expert Committee; ICER = incremental cost-effectiveness ratio; IST = immunosuppressive therapy; PE = plasma exchange; QALY = quality-adjusted life-year; SOC = standard of care.
aFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Clinical Value
Based on the totality of the clinical evidence reviewed, CDEC concluded that it is uncertain whether caplacizumab in combination with PE and IST demonstrates acceptable clinical value compared with PE and IST alone in adult patients with aTTP. Given that caplacizumab is expected to be an additive treatment to PE and IST, acceptable clinical value refers to added value versus PE and IST.
Previous CDEC recommendations for caplacizumab in 2020 and 2023 concluded that treatment with caplacizumab resulted in a statistically significantly reduction in the time to normalization of platelet count based on evidence from 1 phase III, double-blind, randomized controlled trial (RCT) (the HERCULES study; N = 145) and other supportive studies. Patients previously described the significant impact that aTTP had on their quality of life and stated a need for effective treatments that improve survival and quality of life, prevent disease complications, reduce recurrence rates, reduce the need for PE, and have fewer side effects. As outlined in both prior recommendations, CDEC could not draw conclusions on clinically important outcomes, including survival, organ damage, long-term disease recurrence, health care use, or HRQoL, due to study limitations. The HERCULES study was not designed to assess the effects of caplacizumab on these outcomes, and there was notable uncertainty in the clinical relevance of the primary end point (i.e., time to platelet count response) between treatment groups and how well time to normalization of platelet count correlates with the aforementioned clinical outcomes.
Evidence informing this resubmission presented new clinical information to support the efficacy and safety of caplacizumab for the treatment of an acute aTTP episode and to address gaps identified in the previous resubmission, which included insufficient evidence of clinically meaningful outcomes, lack of an identifiable subpopulation most likely to benefit, and generalizability to Canadian clinical practice. This included 1 retrospective observational study (the Capla 1000+ project [N = 1,525]), which evaluated caplacizumab with PE and IST versus PE and IST alone. Results from this study suggested that caplacizumab plus PE and IST was associated with an improved 3-month survival rate (98.5% versus 94%), and the direction of effect for secondary outcomes of time to platelet count normalization, number of PE sessions, refractoriness, and exacerbations was consistent with the studies evaluated in the previous reviews, although there were some differences in magnitude. However, CDEC noted that the evidence was very uncertain due to risk of bias from the selection of participants in the study, confounding, and time-related bias. The committee emphasized that although the Capla 1000+ project supported the findings of the pivotal evidence previously reviewed, as well as generalizability to clinical practice in Canada, the study did not address the evidence gaps previously identified in clinically important outcomes ― such as long-term survival, reduced organ damage, and improved HRQoL ― as these were not evaluated in the body of evidence.
Further information on the committee’s discussion around clinical value is provided in the Summary of Deliberation section.
Considering Significant Unmet Clinical Need
CDEC established that there was significant unmet clinical need due to the rarity and severity of aTTP. Previously, patients identified a need for effective treatments that improve survival, prevent disease complications, reduce recurrence rates and the need for PE, and have fewer side effects, improving overall quality of life. Within this resubmission, patient groups further emphasized the burden of PE and IST, citing a need for treatment that is safe and immediately effective, reduces treatment time, and can treat disease that is refractory to SOC. The totality of evidence reviewed suggests that caplacizumab may result in improved time to platelet count normalization, potential reduction in PE requirements (i.e., duration and volume), and fewer patients with refractory disease or aTTP exacerbations; however, the magnitude of benefit is uncertain. As such, CDEC concluded that, when added to PE and IST, caplacizumab may address a significant unmet clinical need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value.
Further information on the committee’s discussion around unmet clinical need is provided in the Summary of Deliberation section.
Developing the Recommendation
Due to the uncertainty in clinical value, CDEC could not recommend whether to reimburse caplacizumab or not based on clinical value alone. Therefore, they also considered whether caplacizumab addresses a significant unmet clinical need. CDEC concluded that caplacizumab addresses a significant unmet clinical need with an acceptable level of certainty. Based on the preceding considerations, CDEC recommended that caplacizumab be reimbursed. As part of the deliberation on whether to recommend reimbursement or not, the committee also considered unmet nonclinical need and health inequity. Information on this discussion is provided in the Distinct Social and Ethical Considerations domain in the Summary of Deliberation section.
Because CDEC recommended that caplacizumab be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
CDEC considered all domains of value of the deliberative framework (clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems) before developing its recommendation. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: CDEC noted that caplacizumab is expected to be used first-line as an add-on treatment to SOC; thus, the committee considered SOC alone, consisting of PE and IST, to be the most appropriate comparator. CDEC noted variability in the ISTs that may be used in Canada (e.g., rituximab, cyclosporin, cyclophosphamide, vincristine, and bortezomib).
Efficacy versus SOC (PE and IST): In the initial review of caplacizumab, CDEC discussed 1 phase III, double-blind RCT (the HERCULES study; N = 145) in adults with aTTP receiving PE and IST, which demonstrated that treatment with caplacizumab statistically significantly reduced the time to normalization of platelet count versus placebo (2.69 days in the caplacizumab treatment group and 2.88 days in the placebo group); however, the difference between treatment groups was of unknown clinical relevance. Additional evidence from the phase II TITAN study was consistent with the HERCULES study. Evidence considered in the first resubmission of caplacizumab included a 3-year follow-up study of patients who completed the HERCULES study (the post-HERCULES study; N = 104) evaluating long-term aTTP relapse in patients who did not experience an aTTP recurrence during the HERCULES study or before the beginning of the post-HERCULES study; a post hoc integrated analysis of data from the HERCULES and TITAN studies (N = 220) evaluating survival, health care use, organ damage, and refractory aTTP; and several RWE studies providing supportive evidence on survival, health care use, and refractory aTTP. Within this resubmission, 1 retrospective observational study (the Capla 1000+ project; N = 1,525) demonstrated that treatment with caplacizumab may result in similar clinical benefit for patients with aTTP compared with SOC alone in 3-month survival (98.5% in the caplacizumab group and 94.0% in the control group). Additionally, treatment with caplacizumab may reduce the rate of refractory disease (1% in the caplacizumab group and 10.1% in the control group) and disease exacerbations (4% in the caplacizumab group and 32% in the control group) compared to SOC alone. However, because the evidence was very uncertain, CDEC could not determine if there was a meaningful improvement in reducing the time or number of PE sessions to achieve platelet normalization, and time to increase ADAMTS13 enzyme activity to at least 20% with caplacizumab over SOC alone. Only caplacizumab-related harms were reported in the Capla 1000+ project. CDEC noted that there is an increased risk of bleeding with caplacizumab, although the committee agreed with the clinical experts that the reported harms are expected to be manageable.
Certainty of the evidence and clinical importance of treatment effects: The uncertainty in the clinical evidence considered as part of the initial review and first resubmission has previously been described. With regard to this resubmission, CDEC noted that although the evidence from the Capla 1000+ project showed a consistent direction of effect suggesting benefits in survival rate, disease refractoriness and exacerbations, and disease response, the magnitude of benefit was very uncertain due to risk of bias from the selection of participants in the study, time-related bias, potential confounding, and concern whether the difference in treatment effects was clinically meaningful to patients. Further, consistent with the previous reviews, CDEC and the clinical experts noted that it was unclear if the numerical differences between the caplacizumab and SOC groups for the time or number of PE sessions to clinical response (sustained platelet count of at least 150 × 109/L) or the time to biological response (sustained ADAMTS13 activity recovery of at least 10% to 20%) were clinically meaningful. CDEC also discussed how the mortality rate in the trials was lower than what would be expected in routine clinical practice but reasoned that it could reflect the recruitment of patients by clinical teams who are familiar with managing aTTP into the studies. For the Capla 1000+ project, the committee considered the 3-month follow-up adequate to inform the short-term survival during the acute phase of an aTTP episode, but insufficient to evaluate the impact of caplacizumab on aTTP relapse, exacerbation, safety, or survival associated with subsequent aTTP episodes.
Discussion on gaps in the evidence from previous recommendations: CDEC discussed whether the evidence provided for this resubmission addressed the gaps identified during the previous reviews:
Clinically relevant outcomes: As outlined in the previous recommendations for caplacizumab, CDEC could not draw conclusions on clinically important outcomes including survival, reduction in organ damage, health care use, quality of life, or long-term recurrence of aTTP. The committee discussed how the outcomes of the Capla 1000+ project may address some patient-important outcomes, given the observed results for short-term survival and disease refractoriness or exacerbations. Results for other secondary outcomes were supportive of the results observed in the evidence that was previously reviewed by CDEC. However, CDEC maintained that there was no evidence to support the impact of caplacizumab on long-term survival, organ damage, health care resource use, or HRQoL; therefore, the gaps that were previously identified in prior reviews of caplacizumab remain, although the committee noted that it is unlikely that high-quality evidence will be generated for these outcomes.
Subpopulation: As outlined in the previous recommendations for caplacizumab, CDEC was unable to identify a subpopulation of patients most likely to benefit from the drug. During the current resubmission, CDEC discussed that treatment with caplacizumab resulted in lower rates of refractory disease compared to SOC alone across the evidence available for the initial review and both resubmissions and that patients with refractory disease could be a subpopulation that would benefit from treatment with caplacizumab. However, the committee agreed with the clinical experts, acknowledging that there is no rapid way to determine which patients would benefit more from caplacizumab, and due to the seriousness and need for immediate treatment, all patients with aTTP are treated the same.
Generalizability: Previous CDA-AMC reviews and CDEC recommendations highlighted that the proportion of patients who received rituximab in the HERCULES study and the RWE cohort studies was higher than would be expected in Canada. Given that 40% of patients in the overall HERCULES trial period received caplacizumab in addition to rituximab (and PE plus corticosteroids), it was unclear if the observed effects of caplacizumab in the trial would be observed in Canadian practice at the time. The committee noted that there was insufficient evidence to determine the effect of concomitant use of rituximab on the overall study outcomes. Furthermore, the generalizability of the study results to a patient population with aTTP in Canada is limited because of the lack of study sites in Canada, not all patients received corticosteroids, and the limited ethnic diversity of patients in the study. CDEC noted that, in the Capla 1000+ project, 90.5% of patients in the caplacizumab group received rituximab compared to 71% in the control group. CDEC and the clinical experts consulted for this review noted that rituximab is typically provided to patients with more severe, refractory, or exacerbating disease, and the clinical experts noted that this was generally aligned with clinical practice. CDEC also noted that caplacizumab is not indicated for patients younger than 18 years of age but agreed with the clinical experts that if caplacizumab were to be used in pediatric patients, it would be important to rule out congenital TTP first.
Clinical value: Based on all of the preceding considerations, the committee was uncertain whether there was added clinical value when adding caplacizumab to SOC treatments.
Unmet Clinical Need
Input on unmet clinical need: Patients identified a need for a safe treatment that prevents organ damage and death. Clinicians stated that there is also a need for treatment that rapidly normalizes platelet counts and avoids the long-term complications of the disease and current SOC. CDEC acknowledged the seriousness of the disease and unpredictability of another aTTP episode, as described in the patient group input. Further, the committee noted that despite treatment, each aTTP episode puts patients at risk of serious complications, such as stroke, heart attack, kidney injury, permanent cognitive impairment, and organ damage. CDEC also discussed the need for a treatment that is less burdensome to patients compared to the current SOC. The clinical experts noted that while current treatments reduce mortality to 10% to 20% (mortality remains greater than 30% for refractory disease), patients can still develop depression and posttraumatic stress disorder once an aTTP episode resolves. CDEC discussed how caplacizumab is an add-on to SOC and does not directly address the need for treatment that is less burdensome, nor does it impact the underlying cause of aTTP. The committee acknowledged that while caplacizumab may reduce the time and number of PE sessions to clinical response, it was uncertain if this reduction was clinically meaningful to patients.
Severity of aTTP: CDEC noted that aTTP is a serious, incapacitating, and life-threatening condition, and if left untreated, the risk of death is greater than 90% in the first 30 days.
Availability of treatment options: CDEC discussed the current treatment options that include PE and ISTs. While PE and IST are effective treatment options, there are still patients who experience persistent or recurrent thrombotic microangiopathy, which can lead to thrombotic complications. The clinical experts and clinician group stated that reimbursement of rituximab tends to be approved only for patients whose disease is relapsing or refractory and not as a first-line treatment for the first aTTP episode. The patient group and clinicians noted that PE is invasive, uncomfortable, slow to work, associated with complications due to the use of a central venous catheter, and exposes patients to donor blood products. Additionally, the clinical experts reported that mortality remains as high as 20% despite treatment with PE. ISTs (e.g., rituximab and corticosteroids) do not address the microvascular thrombosis that causes end-organ damage, are also slow to work, can have adverse effects, and may have limited effect due to toxicity. CDEC acknowledged that access to PE and ISTs varies across jurisdictions and IST may only be funded for relapsing disease. In situations in which patients cannot access these drugs through public or private insurance or exceptional access programs, they are at an increased risk of relapse and poor clinical outcomes. CDEC recognized that caplacizumab was previously approved for use in Canada and received a Notice of Compliance (NOC) on February 28, 2020. At the time of this review, caplacizumab did not have a Drug Identification Number (DIN) (cancelled in January 2025), and the sponsor has participated with an expectation to reactivate their marketing authorization. CDEC and the clinical experts noted that the current availability of caplacizumab through Health Canada’s Special Access Program is limited, given that aTTP is a medical emergency and hospitals would be required to keep the product in stock for use.
Significant unmet clinical need: Due to challenges with evidence generation associated with the rarity of aTTP and the severity of the disease despite available treatment options, CDEC considered there to be significant unmet need as described in the recommendation framework in the Procedures for Reimbursement Reviews.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: The patient group identified a need for treatment that is immediately effective and reduces total treatment time. CDEC acknowledged that patients living in rural and remote communities are often required to travel to receive treatment due to the limited access to apheresis clinics outside major cities, which puts additional financial and psychological burden on both patients and their families while they are separated. The clinical experts indicated that rural and underserved communities often consist of a higher proportion of systematically marginalized groups who, as a result, may experience a disproportionate burden of harms.
Equity considerations: CDEC discussed how aTTP may disproportionately affect individuals who are female and of reproductive age, have African ancestry, have a high body mass index, or have other rheumatological or immunological conditions. CDEC noted that some ethnic groups were underrepresented in the evidence (e.g., those who are Asian, Hispanic, or Latino) compared to the ethnic diversity of patients with aTTP in Canada. However, according to the clinical experts consulted for this review, treatment effects are not expected to vary by ethnicity. Because there is no rapid way to determine which patients would benefit more from caplacizumab, and given the need for immediate treatment, the clinical experts stated that all patients are treated the same. CDEC considered the health inequities among patients with aTTP and determined that caplacizumab is unlikely to address these.
Significant unmet nonclinical need or health inequity: CDEC determined that there is an unmet nonclinical need or health inequity for patients with aTTP (e.g., travel to apheresis clinics, disproportionate burden on those living in underserviced communities). However, the committee concluded that it is unlikely that caplacizumab can address these needs.
Economic Considerations
Health impacts of caplacizumab in combination with SOC versus SOC alone: Caplacizumab in combination with SOC is predicted to be associated with a gain of 1.03 life-years when compared to SOC alone and may result in a gain of 0.65 quality-adjusted life-years (QALYs) compared to SOC over a lifetime time horizon.
Cost of caplacizumab in combination with SOC versus SOC alone: Caplacizumab in combination with SOC is predicted to be associated with higher costs to the health care system than SOC alone (incremental costs = $278,078) over a lifetime time horizon, primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio (ICER) for caplacizumab in combination with SOC in aTTP was $269,158 per QALY gained when compared with SOC (Figure 1).
Figure 1: Estimate of the ICER Used by CDEC to Inform the Price Condition
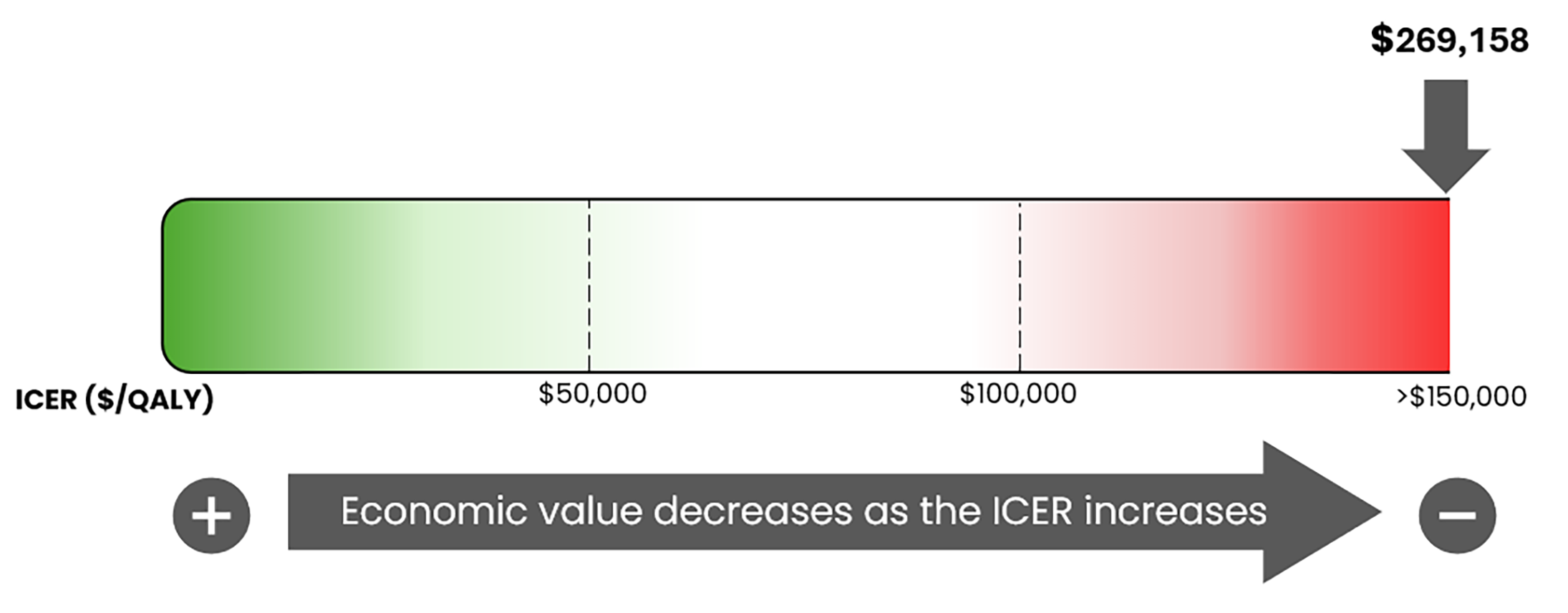
CDEC = Canadian Drug Expert Committee; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Certainty of the evidence: There remains considerable uncertainty in the long-term outcomes predicted by the economic model based on the relative risk of long-term sequelae. Scenario analyses were conducted to explore the uncertainty associated with long-term sequelae. Additional price reductions may be required to achieve cost-effectiveness at a given willingness-to-pay threshold.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimates that by year 3 of reimbursement, 79 patients would be eligible for caplacizumab; of these, 55 patients are expected to receive caplacizumab. CDA-AMC also estimates that the budget impact of reimbursing caplacizumab in combination with SOC for the treatment of adult patients with aTTP will be approximately $24.9 million over the first 3 years of reimbursement compared to the amount currently spent on SOC, with an estimated expenditure of $24.9 million on caplacizumab over this period. The actual budget impact of reimbursing caplacizumab will depend on the number of eligible patients.
Health system implications: CDEC acknowledged the input from the clinician group and clinical experts who described how extended hospital admissions and prolonged PE put additional strain on inpatient units and health care system that are already overburdened. The clinician group and clinical experts also stated that reducing PE duration and ICU exposure results in improved patient outcomes and more efficient use of scarce health system resources. CDEC noted that aTTP is a rare disease and, consequently, the impacts on the health system are likely to be small. The committee also discussed how patients living outside of major cities, where apheresis clinics are located, must travel to receive treatment; however, caplacizumab is not expected to have an impact on whether or not patients receive PE or reduce the need for travel.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to caplacizumab (refer to the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, Answering TTP Canada, with support from the Network of Rare Blood Disorder Organizations (refer to the Patient and Clinician Group Input document)
input from a person with lived experience who delivered a brief presentation and answered questions from the committee (refer to the Person with Lived Experience section earlier in this document)
input from 1 clinician group, the Canadian Apheresis Group, with letters of support from 6 clinicians (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 3 clinical experts with expertise in the management of aTTP consulted by CDA-AMC.
Special thanks: CDA-AMC extends its special thanks to the individual who presented directly to CDEC, and to the patient organizations supporting the community of those living with aTTP, including Mina Rajan and Answering TTP Canada.
General note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journeys with CDEC.
CDEC Information
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. Kerry Mansell (Vice-Chair), Sally Bean, Daryl Bell, Dan Dunsky, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Dr. Dennis Ko, Dr. Christine Leong, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Nicholas Myers, Dr. Krishnan Ramanathan, Dr. Marco Solmi, Carla Velastegui, Dr. Edward Xie, and Dr. Peter Zed
Meeting date: March 26, 2026
Regrets: One expert committee member did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca