Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Iptacopan (Fabhalta)
Indication: For the treatment of adult patients with C3 glomerulopathy to reduce proteinuria
Sponsor: Novartis Pharmaceuticals Canada Inc.
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Fabhalta?
Canada’s Drug Agency (CDA-AMC) recommends that Fabhalta be reimbursed by public drug plans for adult patients with C3 glomerulopathy (C3G) to reduce proteinuria, if certain conditions are met.
Why Did CDA-AMC Recommend Reimbursement?
The Canadian Drug Expert Committee (CDEC) determined that it is uncertain whether Fabhalta demonstrates acceptable clinical value versus placebo in adult patients with C3G. Evidence from 1 clinical trial showed that Fabhalta reduced protein in the urine after 6 months of treatment, compared to placebo. The clinical impact of this reduction on patient health is uncertain. Fabhalta may decrease glomerular C3 deposit, which is associated with the pathologic mechanism of the disease. However, the evidence for Fabhalta is uncertain because the study was small and did not show whether the treatment improves kidney function or improves important long-term outcomes like kidney failure, heart problems, need for dialysis or kidney transplant, and survival.
Due to the uncertainty in the evidence regarding Fabhalta, CDEC was unable to base its recommendation solely on clinical value. Therefore, the committee also considered whether Fabhalta addresses a significant unmet clinical need. C3G is a rare, serious kidney disease that leads to kidney failure in half of patients. Currently available therapies do not address the underlying disease and are mostly ineffective at stopping disease progression, and they often cause substantial side effects. Patients and caregivers report major impacts on daily functioning, emotional well-being, and financial stability. CDEC concluded that Fabhalta, a treatment option for adults with C3G that targets the underlying complement dysregulation, may address this unmet need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value, considering the rarity and severity of the disease despite available treatments.
There are significant unmet nonclinical needs and equity considerations due to the rarity of C3G. Patients face multiple types of treatment burdens, and this is especially the case for those who live far from specialized centres. Caregiver burdens include time away from work, income loss, and stress. Fabhalta is the first treatment for C3G that can be taken orally. CDEC concluded that this may reduce the burden of treatment and make it easier for patients, as it avoids the challenges that come with injections.
Based on all of the preceding considerations, CDEC recommended that Fabhalta be reimbursed.
Which Patients Are Eligible for Coverage?
Fabhalta should only be covered for patients aged 18 years or older with a confirmed diagnosis of C3G based on kidney biopsy, who have an estimated glomerular filtration rate (eGFR) of at least 30 mL/min/1.73 m2 and a proteinuria level of at least 1 g/g. Fabhalta should not be used in patients with previous transplant other than kidney, nor in patients who have a rapidly progressive disease or severe chronic kidney injury (e.g., when most of the kidney tissue is scarred or damaged, based on a kidney biopsy); in these patients, it is unknown whether Fabhalta would show a similar level of benefit.
What Are the Conditions for Reimbursement?
Fabhalta should only be reimbursed if prescribed by a kidney specialist experienced in managing C3G, and if the cost of Fabhalta is reduced. Fabhalta should be initially covered for 6 months and may be continued if the patient shows a meaningful response (such as reduced protein in the urine with stable kidney function, or clear removal of C3 build-up in the kidneys, as seen on a follow-up kidney biopsy). Reassessment should be conducted at least every year.
Important budget impact considerations must be addressed for health systems to be able to adopt Fabhalta.
Review Background
Disease background: Complement 3 glomerulopathy (C3G) is a rare, progressive kidney disease caused by complement system dysregulation. This leads to progressive glomerular damage and impairs kidney function. Half of patients will experience kidney failure within 10 years, a condition that requires dialysis or kidney transplant. Disease onset typically occurs in childhood or young adulthood. Approximately 542 adults have a diagnosis of C3G in Canada, excluding Quebec.
Indication and reimbursement request: Iptacopan (Fabhalta) has been approved by Health Canada for the treatment of adult patients with C3G to reduce proteinuria. The sponsor is seeking reimbursement for this patient population. The application was submitted by the sponsor before receiving a Notice of Compliance from Health Canada, and the review by Canada’s Drug Agency (CDA-AMC) reflects the anticipated indication for iptacopan at the time this review was conducted, which was for the treatment of adult patients with C3G.
Drug under review: Iptacopan is a complement inhibitor that binds to complement factor B and inhibits the alternative complement pathway. It is available as a 200 mg capsule and the recommended dosage is 200 mg taken orally twice daily.
Treatment costs: At the submitted price of $719.94 per 200 mg oral capsule, the annual cost of iptacopan is expected to be $525,916 per patient, based on the Health Canada–recommended dosage.
Highlights of Input From Interested Parties
The patient group (the Kidney Foundation of Canada) noted the following regarding impacts of the disease, unmet needs, and important outcomes:
Patients emphasized experiencing difficult-to-manage symptoms including fatigue and lethargy, as well as a range of physical symptoms that disrupt daily routines, social activities, emotional well-being, and overall quality of life. Patients with C3G often progress to kidney failure, at which point dialysis or kidney transplant would be required.
The disease and its treatment impose a substantial burden on both patients and caregivers, including the emotional toll of stress, time off work associated with managing daily treatments and symptoms, and financial burden stemming from out-of-pocket medical expenses and loss of employment, which can affect financial stability and access to care.
There is a need for treatments that preserve kidney function, are well tolerated, and improve quality of life by reducing the physical symptoms as well as the emotional and mental burden. Patients valued support for emotional and mental well-being to help them maintain stability and remain engaged in meaningful daily activities. Patients also emphasized the importance of therapies that are accessible and affordable, and can minimize out-of-pocket expenses.
The clinician group (the Canadian C3G and IC-MPGN Physician Network) and the clinical experts consulted by CDA-AMC noted the following regarding unmet needs arising from the disease and the place in therapy for the drug under review:
There is a significant need for effective therapies with meaningful benefits in preserving kidney function in the long term and overall patient well-being. Currently, there are no disease-specific therapies that target complement dysregulation and have a meaningful impact on preventing progression to end-stage kidney disease or recurrence after transplant.
Supportive therapies that are currently used are associated with substantial and burdensome toxicities. The harms profiles pose significant challenges, including broad immunosuppression, and were reported to have a substantial negative impact on patients’ quality of life. Access to advanced therapies is restricted, and specialized care is limited by geographic and systemic barriers, currently resulting in inequities in treatment availability and outcomes. This limited equitable access to health care resources that are needed for C3G stems from the rarity of the disease.
Iptacopan may cause a paradigm shift as a first-line therapy and potentially a new standard of care (SOC), offering targeted complement inhibition.
The participating public drug programs raised potential implementation issues related to considerations for initiation, renewal, discontinuation, and prescribing of therapy; generalizability of trial populations to broader populations; and system and economic issues.
Note: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through with this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as 1 element contributing to a broader understanding of the condition and treatment under review.
Recommendation
With a vote of 13 in favour and 0 against, the Canadian Drug Expert Committee (CDEC) recommends that iptacopan be reimbursed for the treatment of adult patients with C3G to reduce proteinuria, only if the conditions listed in Table 1 are met.
Table 1: Reimbursement Conditions and Reasons
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Iptacopan may be initiated for the treatment of C3G if all of the following conditions are met: 1.1. aged 18 years or older 1.2. confirmed diagnosis of C3G based on kidney biopsy 1.3. eGFR ≥ 30 mL/min/1.73 m2 1.4. UPCR of ≥ 1 g/g or ≥ 100 mg/mmola in at least 2 FMU samples. | In the APPEAR-C3G trial, iptacopan demonstrated clinically meaningful benefits in adult patients with C3G. These clinically important benefits included a reduction in proteinuria, an increase in the proportion of patients achieving the composite renal end point, and a decrease in glomerular C3 deposit at week 26 compared with placebo. The effect of iptacopan on improvement in eGFR or fatigue was uncertain. Eligible patients in the APPEAR-C3G trial had a UPCR of ≥ 1 g/g in at least 2 FMU samples collected during screening. Patients also needed to have an eGFR ≥ 30 mL/min/1.73 m2 for inclusion. | CDEC noted that in the APPEAR-C3G trial, diagnosis of C3G was confirmed by kidney biopsy showing 2+ C3 staining. Patients in the APPEAR-C3G trial were on a maximally recommended or tolerated dose of an ACE inhibitor or ARB for at least 90 days. The doses of other antiproteinuric medications — including MPA, corticosteroids, SGLT2 inhibitors and MRAs — should have been stable for at least 90 days before randomization. CDEC agreed with the clinical experts that prior or current use of supportive care medications should not determine eligibility for iptacopan. Public drug plans may consider measuring proteinuria using any appropriate urine collection method, including spot urine, FMU, or 24-hour urine collection.a Public drug plans may also consider quantifying proteinuria using a measure other than UPCR, including the use of UACR ≥ 60 mg/mmol. |
2. Treatment with iptacopan should not be used in patients with any of the following: 2.1. any cell or solid, nonkidney organ transplant 2.2. RPGN (i.e., 50% decline in eGFR within 3 months with kidney biopsy findings of glomerular crescent formation in ≥ 50% of glomeruli) 2.3. kidney biopsy showing interstitial fibrosis/tubular atrophy of > 50% 2.4. confirmed MGUS. | The APPEAR-C3G trial excluded such patients, and there is no evidence regarding the efficacy and safety of treatment with iptacopan in patients with these characteristics. | — |
3. The duration of initial authorization is 6 months. | The APPEAR-C3G trial assessed the primary and secondary end points at 6 months during the randomized controlled phase. | CDEC agreed with the clinical experts that although follow-up occurs every 3 to 6 months in clinical practice, meaningful change for response assessment requires at least 6 to 12 months. |
Renewal | ||
4. For renewal after initial authorization, the physician must provide proof of maintained clinical response to iptacopan, defined as either of the following: 4.1. any reduction in proteinuria, and no more than 15% decline in eGFR 4.2. clearance of C3 deposits on repeat biopsy, if available. | In the APPEAR-C3G trial, proteinuria reduction was the primary efficacy end point. A 25% (ideally 50%) reduction in proteinuria of was considered clinically meaningful improvement in the treatment of C3G. | Assessment of treatment response should be based on clinical expert practice. CDEC relied on clinician input to define clinical response to therapy. |
5. For subsequent renewal, the clinical response achieved after the initial authorization must be maintained, as assessed by the treating nephrologist. | This is meant to ensure that the clinical response achieved after the initial authorization is sustained over time. | Given the chronic and progressive nature of C3G, clinical expert input suggested that an increase in proteinuria alone should not be interpreted as evidence of treatment inefficacy, provided the treating nephrologist judges the overall disease trajectory to be stable on treatment; however, treatment should be discontinued if the eGFR declines to below 15 mL/min/1.73 m2. |
6. Assessment of treatment response for subsequent renewal may be conducted every 12 months. | The APPEAR-C3G trial assessed the primary and secondary end points at 6 months during the randomized controlled phase and at 12 months during the open-label phase of the study. | — |
Prescribing | ||
7. Iptacopan should be prescribed by a glomerulonephritis specialist, a nephrologist with experience in managing C3G, or a nephrologist in consultation with a glomerulonephritis specialist. | This is meant to ensure that iptacopan is prescribed for appropriate patients. | CDEC noted that in rural or remote areas with limited access to specialists, iptacopan may be prescribed by an internal medicine physician with experience in C3G, ideally within a shared-care model. |
Pricing | ||
8. A reduction in price. | Using the CDA-AMC base-case analysis, the ICER for iptacopan in combination with standard of care was $2,762,300 per QALY gained when compared with standard of care in the indicated population. A band 4 price reductionb would be required to achieve cost-effectiveness at a $50,000 per QALY threshold. A band 4 price reductionb would be required to achieve cost-effectiveness at a $100,000 per QALY threshold. Exact price reductions at any given willingness-to-pay threshold can be found in the CDA-AMC main report and Supplemental Material document. | The CDA-AMC analysis is based on public list prices for all treatments. Further price reductions may be required if there are price arrangements (discounts) currently in place for any treatment included in the economic analysis. |
Feasibility of adoption | ||
9. The economic feasibility of adoption of iptacopan in combination with standard of care must be addressed. | At the submitted price, the incremental budget impact of iptacopan in combination with standard of care is expected to be greater than $40 million in years 1, 2, and 3. The magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption, given the difference between the sponsor’s estimate and the CDA-AMC estimate. | — |
2+ = at least 2 orders of magnitude greater intensity; ACE = angiotensin-converting enzyme, ARB = angiotensin II receptor blocker; C3 = complement 3; C3G = complement 3 glomerulopathy; CDA-AMC = Canada’s Drug Agency; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; FMU = first-morning urine; MGUS = monoclonal gammopathy of undetermined significance; MMF = mycophenolate mofetil; MPA = mycophenolic acid; MRA = mineralocorticoid receptor antagonist; QALY = quality-adjusted life-year; RPGN = rapidly progressive glomerulonephritis; UACR = urine albumin-to-creatinine ratio; UPCR = urine protein-to-creatinine ratio.
aIn Canada, proteinuria measurement by UPCR may be expressed in different units, where UPCR 1 g/g = 100 mg/mmol on a spot urine test, or 1 g/day on a 24-hour urine collection.
bFor the statement regarding the size of the price reduction required, band 1 = 1% to 24%, band 2 = 25% to 49%, band 3 = 50% to 74%, and band 4 = 75% or greater.
Rationale for the Recommendation
Due to uncertainty in the evidence regarding iptacopan, CDEC was unable to base its recommendation solely on clinical value. Therefore, the committee also considered whether iptacopan addresses a significant unmet clinical need. CDEC concluded that iptacopan may address this unmet need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value, considering the rarity and severity of the disease despite available treatments.
Clinical Value
Based on the totality of the clinical evidence, CDEC concluded that it is uncertain whether iptacopan demonstrates acceptable clinical value compared with an appropriate comparator (placebo plus supportive therapies) in adult patients with C3G.
Evidence from 1 phase III, double-blind, placebo-controlled trial (the APPEAR-C3G trial; N = 74) showed that 6 months of treatment with iptacopan in combination with supportive therapies resulted in a reduction in proteinuria in adult patients with C3G compared with placebo plus supportive therapies. However, the clinical meaningfulness of this reduction is uncertain. In the APPEAR-C3G trial, iptacopan likely increased the proportion of patients who met the composite renal end point compared with placebo. In addition, iptacopan may have decreased glomerular C3 deposit on kidney biopsy at 6 months compared with placebo, demonstrating a tissue-level improvement in adults with available biopsy samples that is typically not observed in the natural disease trajectory. Iptacopan may result in little to no clinically important difference in estimated glomerular filtration rate (eGFR); 6 months is likely insufficient to observe a meaningful change, and eGFR may not accurately reflect short-term response to treatment. Uncertainty surrounds the findings; due to the small sample size of the APPEAR-C3G trial, effect estimates are likely to be unstable. In addition, the evidence for iptacopan relies on surrogate end points, without information about its effect on long-term clinical outcomes such as progression to end-stage kidney disease (ESKD), initiation of dialysis, kidney transplant, cardiovascular events, and mortality. Surrogate measures are commonly used in rare kidney diseases and reflect feasibility constraints in generating evidence; however, reliance on surrogate outcomes remains an evidence gap. Iptacopan may have little to no clinically meaningful impact on relief of patients’ symptoms (such as fatigue). Results from the open-label treatment period of the APPEAR-C3G trial and from the long-term extension B12001B study suggest potential for sustained efficacy beyond 6 months; however, causal interpretations could not be made due to the single-arm study design and substantial reductions in sample size over time. The X2202 study provided limited evidence regarding the potential efficacy of iptacopan in patients with posttransplant recurrence of C3G.
With respect to safety, the evidence is very uncertain regarding the effect of iptacopan on serious adverse events or infection by encapsulated bacteria at 6 months. Overall, no new safety signals were identified in the APPEAR-C3G trial, and the observed safety profile of iptacopan was consistent with the product monograph and clinical expert input.
Further information on the committee’s discussion regarding clinical value is provided in the Summary of Deliberation section.
Considering Significant Unmet Clinical Need
C3G is a rare, progressive kidney disease that begins early in life and leads to kidney failure in approximately half of patients, despite available supportive care. Current treatments — including ACE inhibitors, angiotensin II receptor blockers (ARBs), SGLT2 inhibitors, immunosuppressive therapies, and other off-label rescue options — do not target the complement dysregulation that drives disease progression, have limited and inconsistent effectiveness on kidney function and overall patient well-being, and are associated with substantial toxicities and challenges with access. Kidney transplant does not correct the underlying disease mechanism and recurrence rates remain high, leading to kidney allograft loss. Input from patients and caregivers highlighted major impacts on daily functioning, emotional well-being, and financial stability, emphasizing the need for treatments that preserve kidney function while being safe and accessible.
CDEC concluded that iptacopan may address a significant unmet clinical need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value.
Further information on the committee’s discussion regarding unmet clinical need is provided in the Summary of Deliberation section.
Developing the Recommendation
Based on the preceding considerations, CDEC recommended that iptacopan be reimbursed. As part of the deliberation on whether to recommend reimbursement or not, the committee also considered unmet nonclinical need and health inequity. Information on this discussion is provided in the Distinct Social and Ethical Considerations domain in the Summary of Deliberation section.
Because CDEC recommended that iptacopan be reimbursed, the committee also deliberated on whether reimbursement conditions should be added to address important economic considerations, health system impacts, or social and ethical considerations, or to ensure clinical value is realized. The resulting reimbursement conditions, with accompanying reasons and implementation guidance, are stated in Table 1.
Summary of Deliberation
CDEC considered all domains of value of the deliberative framework (clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems) before developing its recommendation. For further information on the domains of value, refer to Expert Committee Deliberation at Canada’s Drug Agency.
The committee considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
Appropriate comparators: The committee considered placebo added to stable supportive therapy (e.g., ACE inhibitors, ARBs, and SGLT2 inhibitors) to be an appropriate comparator for the drug under review. In the absence of disease-targeted therapies, ACE inhibitors, ARBs, and SGLT2 inhibitors remain the SOC for C3G. Immunosuppressive agents and other rescue therapies were not viewed as relevant comparators due to limited evidence, inconsistent access, and tolerability issues.
Efficacy versus placebo: One phase III, double-blind, placebo-controlled trial (the APPEAR-C3G trial, N = 74) suggested that, in adult patients with C3G, iptacopan results in a reduction in proteinuria at 6 months compared with placebo. The relative reduction was 35.1% (95% confidence interval [CI], 13.8% to 51.1%; P = 0.0014) with iptacopan compared to placebo. However, the clinical meaningfulness of this reduction is uncertain. Additionally, compared with placebo, iptacopan likely increased the proportion of patients who met the composite renal end point (between-group difference = ██████ ███ ███ ████ ██ █████) and may result in a decrease in the glomerular C3 deposit on kidney biopsy at 6 months (between-group difference = 1.875; 95% CI, −3.298 to −0.452). Iptacopan may result in little to no clinically meaningful difference in eGFR after 6 months of treatment compared with placebo (between-group difference = 2.156; 95% CI, −2.749 to 7.061 mL/min/1.73m2). Iptacopan may also have little to no clinically meaningful impact on patients’ fatigue compared to placebo (between-group difference = −2.598; 95% CI, −6.032 to 0.835). Results from the open-label treatment period of the APPEAR-C3G trial and from the long-term extension B12001B study suggest potential for sustained efficacy beyond 6 months, but causal interpretations could not be made due to the single-arm study design and substantial reductions in sample size over time. The X2202 study provided limited evidence regarding the potential efficacy of iptacopan in patients with posttransplant recurrence of C3G. The effect of iptacopan on harms outcomes (incidence of serious adverse events and infection by encapsulated bacteria) was very uncertain. The clinical experts indicated that there were no unusual safety signals identified in the APPEAR-C3G trial.
Clinical importance of treatment effects: Patient input emphasized the need for treatments that preserve kidney function, are well tolerated, and improve quality of life by reducing the physical symptoms, as well as the emotional and mental burden of progressive kidney disease. In the APPEAR-C3G trial, outcomes related to proteinuria and kidney function (i.e., composite renal end point), and C3c staining addressed several of these priorities. Observational evidence from the literature suggests that reductions in proteinuria and stabilization of eGFR may each be associated with longer term patient-important clinical outcomes such as delayed progression to ESKD and reduced mortality. However, the absence of evidence on important long-term outcomes, such as the need for future dialysis and long-term morbidity and mortality, remains an evidence gap. In the absence of literature-based minimal important difference (MID) estimates, thresholds for between-group differences were informed by expert opinion to support interpretation of the evidence. Reduction in proteinuria was assessed against a threshold of 50%, which is associated with a dramatic reduction in long-term kidney failure risk, as well as against a threshold of 25%, which may also reduce long-term kidney complications and may be considered clinically meaningful by some physicians according to the input received. An MID threshold of 20% was applied for the composite renal end point, and 5-point change for the Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-Fatigue) total score. For change in eGFR, glomerular C3 deposit score, and harms, treatment effect was evaluated in the presence of a nonnull effect. Using these MIDs, iptacopan showed potential but uncertain clinically meaningful benefits compared with placebo in reducing proteinuria, achieving the composite renal end point, and decreasing glomeruli C3 deposit; however, its effect on stabilizing eGFR was uncertain. Overall, CDEC concluded that the availability of a treatment option providing such benefits was important to patients with C3G; however, CDEC noted substantial uncertainty surrounding the findings, especially for the important outcome of change in eGFR, and noted that effect estimates are likely to be unstable.
Certainty of the evidence: The certainty of the evidence for the assessment of proteinuria (i.e., urine protein-to-creatinine ratio [UPCR]) was rated as moderate (compared to placebo) using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The certainty of the evidence for the assessment of eGFR, glomeruli C3 deposit score, and symptom of fatigue was rated as low due to serious imprecision and serious risk of bias. The certainty of the evidence for the assessment of the composite renal end point was rated as moderate due to serious imprecision. The certainty of the evidence for the assessment of incidence of serious adverse events and infection by encapsulated bacteria was rated as very low due to extremely serious imprecision.
Use of surrogate end points: CDEC noted that the APPEAR-C3G trial relied on surrogate end points, such as UPCR and eGFR. Although these measures are commonly used in rare kidney disease trials and are considered prognostic of long-term clinical outcomes based on observational evidence, their use represents an evidence gap because it remains uncertain how changes in these surrogates translate into true clinical benefit. However, CDEC acknowledged that reliance on surrogate markers reflects feasibility constraints, as evaluating outcomes like progression to ESKD would require long-term follow-up and a much larger sample size, which are difficult to achieve given the rarity of the condition.
Studies addressing gaps: The X2202 study provided very limited supportive evidence of potential efficacy of iptacopan in patients with posttransplant recurrence of C3G. Interpretation of the findings was limited by the study design, lack of a comparator, and small sample size.
Clinical value: Based on all of the preceding considerations, the committee determined that it is uncertain whether iptacopan plus supportive therapies demonstrates acceptable clinical value compared with the appropriate comparator (placebo plus supportive therapies).
Unmet Clinical Need
Input on unmet clinical need: Based on patient and clinician input, CDEC noted several unmet needs in the management of C3G. Patients reported substantial impacts on quality of life due to fatigue, low energy, and a range of additional physical symptoms, along with disruptions to daily routines, social activities, emotional well-being, and financial stability. Caregivers also described significant stress and difficulties in maintaining a work-life balance. Patients identified a need for treatments that preserve kidney function, are accessible, are convenient to administer, and reduce both physical and emotional burden. Clinical experts highlighted that many patients’ disease is refractory to available therapies, which offer limited benefit and are associated with numerous and considerable toxicities — including the risk of serious infection, hyperglycemia, hypertension, metabolic complications, and osteoporosis — all of which have a substantial negative impact on patients’ quality of life. Experts also noted high rates of posttransplant recurrence. CDEC noted that these challenges underscore the need for safer, more effective, and more tolerable treatments for C3G.
Severity of the disease: CDEC acknowledged that C3G is a rare, progressive, and serious chronic kidney disease due to ongoing complement dysregulation that drives glomerular inflammation, proteinuria, hematuria, and steady loss of kidney function. Approximately half of patients progress to kidney failure within 10 years of initial diagnosis, a condition that requires dialysis or kidney transplant. Even with transplant, high rates of disease recurrence limit long-term outcomes. Patient and clinician input highlighted the substantial symptom burden, early onset, and significant impact on daily functioning and well-being, underscoring the severity of these conditions and the need for more effective treatment options.
Availability of treatment options: CDEC noted that currently there are no approved targeted therapies for C3G, and that many patients ultimately progress to kidney failure. Treatments currently used are considered supportive therapies (e.g., ACE inhibitors, ARBs, and SGLT2 inhibitors), as they may reduce proteinuria but do not target the complement dysregulation that drives disease progression. They have limited and inconsistent effectiveness to improve kidney function and are associated with toxicities. Based on patient and clinical expert input, immunosuppressive therapies such as glucocorticoids and mycophenolate mofetil (MMF) are used in severe cases but have inconsistent benefit and significant toxicities, while other drugs used off-label (e.g., rituximab, cyclophosphamide, calcineurin inhibitors, eculizumab, and avacopan) offer limited evidence of effectiveness and inconsistent access. Patients and clinicians emphasized the lack of effective, well-tolerated, disease-specific therapies that target complement dysregulation, prevent progression to ESKD, and reduce posttransplant recurrence.
Recurrence of C3G after kidney transplant: Kidney transplant does not correct the underlying disease mechanism and, as such, patients frequently experience kidney allograft loss, limiting the possibility of repeated transplant, especially for younger patients. CDEC acknowledged the significant unmet need in patients with kidney transplant but noted that there is very limited supportive evidence for the potential efficacy of iptacopan in this population. Despite the uncertainty, the committee concluded that reimbursement of iptacopan may be considered in patients with posttransplant recurrence of C3G, considering the severity of the condition and lack of alternative treatment options.
Significant unmet clinical need: Due to challenges with evidence generation associated with the rarity of C3G and the severity of the disease despite available treatment options, CDEC established that there was significant unmet clinical need, and concluded that iptacopan, as a treatment option for patients with C3G that targets the underlying complement dysregulation, may address some of the unmet clinical need to a degree that justifies a positive recommendation despite the uncertainty in the clinical value.
Distinct Social and Ethical Considerations
Input on unmet nonclinical need: CDEC noted several unmet nonclinical needs from the input received, including treatment burden due to the rarity of the disease. CDEC acknowledged that patients with C3G and their family and caregivers face multiple types of treatment burden, and their health-related quality of life may be significantly compromised. Patients who live far from specialized centres face significant travel and time burdens and may not consistently have the opportunity to access adequate health care, such as visiting a specialist and receiving treatments for C3G. Caregiver burden related to time away from work, income loss, and stress was also highlighted, along with reduced patient autonomy caused by persistent symptoms and frequent medical visits. Overall, there is a need for more accessible treatment options.
Significant unmet nonclinical need or health inequity: The most important ethical issues and equity considerations stem from the rarity of C3G. CDEC also noted several unmet nonclinical needs, including diagnostic inequities due to limited access to kidney biopsy in rural or remote regions and inconsistent availability of C3-specific staining across Canada. CDEC also noted that the oral administration of iptacopan may be meaningful for patients with C3G, particularly as some currently available treatments require IV or subcutaneous administration. The committee noted that, as the first oral therapy for this rare condition, iptacopan may have the potential to reduce treatment burden and may help address practical access challenges associated with injectable therapies, including the need for health care visits or infusion services.
Economic Considerations
Health impacts of iptacopan in combination with SOC versus relevant comparators: Iptacopan in combination with SOC is predicted to be associated with a gain of 3.49 life-years (LYs) compared to SOC and may result in a gain of 5.73 quality-adjusted life-years (QALYs) compared to SOC.
Cost of iptacopan in combination with SOC versus relevant comparators: Iptacopan in combination with SOC is predicted to be associated with higher costs to the health care system than SOC alone (incremental costs = $15,833,147), primarily driven by increased costs associated with drug acquisition.
Key findings of the economic evaluation: Based on the submitted evidence using the sponsor’s cost-utility analysis, the CDA-AMC base-case analysis estimated that the incremental cost-effectiveness ratio (ICER) for iptacopan in combination with SOC for C3G was $2,762,300 per QALY gained when compared with SOC (Figure 1).
Figure 1: Estimate of the ICER Used by CDEC to Inform the Price Condition
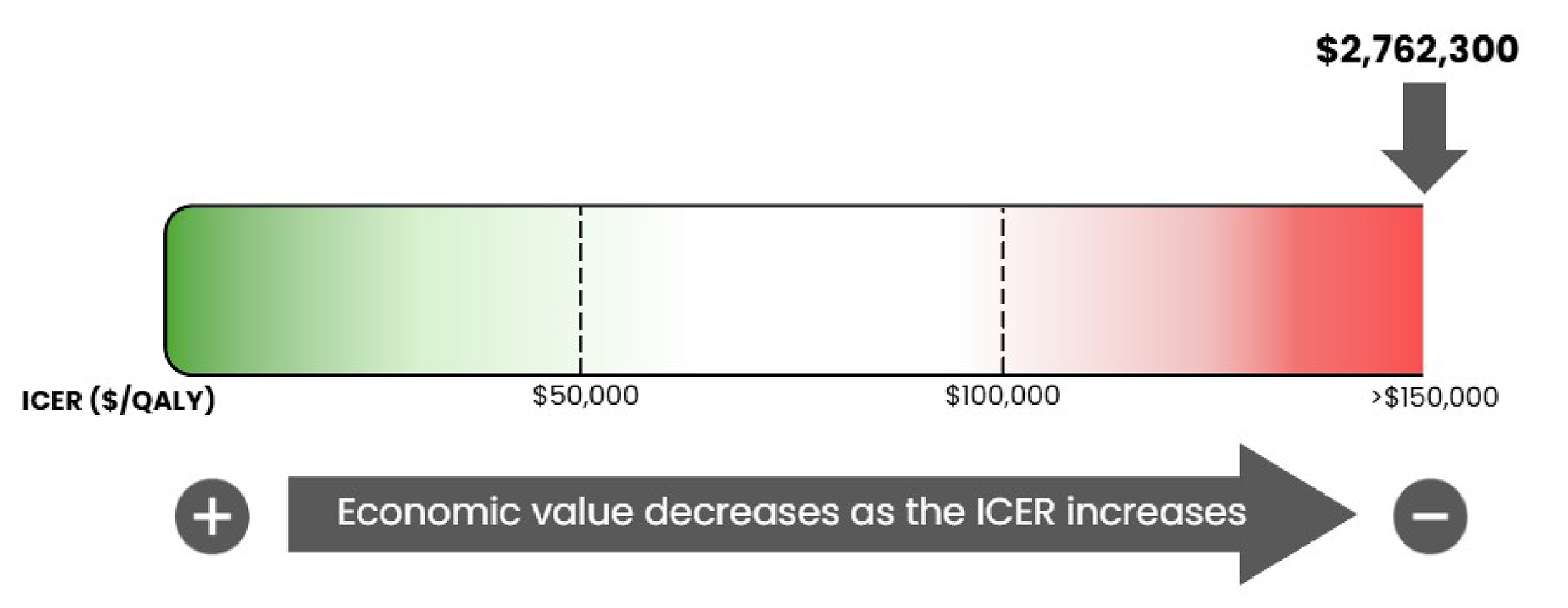
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Certainty of the evidence: CDEC noted that the certainty of the evidence supporting the reimbursement of iptacopan is limited because the cost-effectiveness results are reliant on the decline of eGFR, which is not well supported by available data. Based on the post hoc analysis of the APPEAR-C3G trial, eGFR decline in patients treated with iptacopan in combination with SOC was −0.03 mL/min/1.73m2/year, indicating a near halting of eGFR decline and an annualized rate that is slower than the general population without C3G. This decline in eGFR translates to improvements in renal outcomes; however, it is highly uncertain if the benefits predicted by an extrapolated eGFR decline will persist over the modelled time horizon (100 years). At the submitted price, iptacopan in combination with SOC was associated with a very high incremental cost of $15,833,147, accompanied with incremental benefits of 3.49 LYs and 5.73 QALYs, compared to SOC, yielding an ICER of $2.7 million per QALY gained. These results are associated with uncertainty, as the economic analysis translates the 6-month improvements of eGFR into lifetime reductions in ESKD, dialysis, transplant, and mortality. When considering both the clinical evidence and the predicted long-term benefits, the cost-effectiveness of iptacopan in combination with SOC compared to SOC alone is uncertain due to uncertainty in the treatment effect of iptacopan and uncertainty in the effect of iptacopan on long-term renal outcomes. Due to the uncertainty of the evidence and extrapolation of long-term outcomes, further price reductions may be warranted.
Posttransplant population: CDEC noted that despite the uncertainty in the evidence, patients with C3G who received a kidney transplant should not be excluded from iptacopan treatment. As there is no comparative clinical efficacy evidence of iptacopan treatment against any comparator in this patient population, the cost-effectiveness of iptacopan in combination with SOC when compared to SOC alone is unknown.
Other considerations: The sponsor submitted an additional cost-effectiveness analysis adopting a societal perspective. In this analysis, the sponsor’s approach to estimating productivity and out-of-pocket expenses was uncertain due to a lack of robust evidence. As a result of the lack of robust evidence related to the impact of iptacopan treatment for patients with C3G and caregivers on these outcomes, CDA-AMC was unable to present an analysis from the societal perspective.
Impacts on Health Systems
Anticipated budget impact: CDA-AMC estimated that by year 3 of reimbursement, 215 patients would be eligible for iptacopan in combination with SOC; of these, 183 patients are expected to receive iptacopan. The estimated incremental budget impact of reimbursing iptacopan is predicted to be approximately $250.5 million over the first 3 years, with an expected expenditure of $250.7 million on iptacopan. There is uncertainty in the anticipated budget impact because the base-case population in the budget impact analysis by CDA-AMC included those with a UPCR less than 1.0 g/day. Therefore, the anticipated budget impact of reimbursing iptacopan in the recommended population may be lower than estimated in the CDA-AMC base case.
Sources of Information Used by the Committee
To make its recommendation, the committee considered the following information (links to the full documents for the review can be found on the project webpage):
the CDA-AMC review of the clinical and pharmacoeconomic evidence submitted by the sponsor, as well as relevant ethical issues related to iptacopan (refer the Main Report and Supplemental Material document)
the sponsor’s comments on the draft report and the CDA-AMC responses
patients' perspectives gathered by 1 patient group, the Kidney Foundation of Canada (refer to the Patient and Clinician Group Input document)
input from a person with lived experience who delivered a brief presentation and answered questions from the committee (refer to the Person With Lived Experience section earlier in this document)
input from 1 clinician group, The Canadian C3G and IC-MPGN Physician Network (refer to the Patient and Clinician Group Input document)
input from public drug programs that participate in the reimbursement review process (refer to the Supplemental Material document)
input from 2 clinical experts consulted by CDA-AMC with expertise in the management of C3G.
Special thanks: CDA-AMC extends our special thanks to the individual who presented directly to CDEC, and to the patient organizations representing and supporting the community of those living with C3G, including T. Campbell.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journeys with CDEC.
CDEC Information
Members of the Committee
Dr. Peter Jamieson (Chair), Dr. Kerry Mansell (Vice-Chair), Sally Bean, Daryl Bell, Dan Dunsky, Dr. Ran Goldman, Dr. Trudy Huyghebaert, Dr. Dennis Ko, Dr. Christine Leong, Dr. Alicia McCallum, Dr. Srinivas Murthy, Dr. Nicholas Myers, Dr. Krishnan Ramanathan, Dr. Marco Solmi, Carla Velastegui, Dr. Edward Xie, and Dr. Peter Zed
Meeting date: April 22, 2026
Regrets: Three expert committee members did not attend.
Conflicts of interest: None
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca