Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Naloxegol
Reimbursement request: For the treatment of opioid induced constipation in adult patients with inadequate response to laxative(s), irrespective of the cause of pain (i.e., for noncancer or cancer pain)
Requester: Public drug programs
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Naloxegol?
The Formulary Management Expert Committee (FMEC) recommends that naloxegol be reimbursed for the treatment of opioid-induced constipation (OIC) in adult patients with either cancer pain or noncancer pain, who have inadequate response to laxative(s) provided certain conditions are met.
What Are the Conditions for Reimbursement?
Naloxegol should only be covered to treat patients who are receiving chronic, stable opioid therapy and report fewer than 3 spontaneous bowel movements per week despite the use of combination laxative therapy, including a stimulant laxative and an osmotic laxative, and do not have infiltrative gastrointestinal tract malignancies or peritoneal metastases.
Based on the Canada’s Drug Agency (CDA-AMC) assessment of the health economic evidence, it is unknown whether naloxegol represents good value to the health care system at the public list price. A price reduction may therefore be required.
Why Did CDA-AMC Make This Recommendation?
FMEC reviewed the CDA-AMC report, which included a review of the clinical evidence, specifically 2 randomized, controlled, phase III trials and 1 long-term extension study comparing naloxegol with placebo for OIC in adults with noncancer pain; 3 single-arm observational studies on naloxegol for OIC in adults with cancer pain and an inadequate response to laxative(s); and a cost comparison of naloxegol versus other treatments used in Canada.
FMEC concluded that there is a significant clinical need arising from OIC despite available treatments and that naloxegol addresses this unmet clinical need. For noncancer pain, both pivotal trials reported statistically significant improvements in the primary outcome (response rate) with 25 mg dosing. For cancer pain, the open-labelled studies have signalled its efficacy as well. FMEC heard from the clinical experts that the effect of naloxegol in cancer-related pain is not expected to be different in noncancer pain. FMEC also considered input received from a person with lived experience and drug plans.
Therapeutic Landscape
What Is Opioid-Induced Constipation?
Opioid-induced constipation (OIC) is constipation that is triggered or aggravated by opioid therapy taken for pain control. The binding of opioid agonists to mu-opioid receptors in the enteric nervous system leads to increased nonpropulsive contractions and inhibited water and electrolyte excretion. This results in decreased ability to evacuate the bowels, changes in stool consistency, sense of incomplete rectal evacuation, bloating, abdominal distention and discomfort, and difficulty with digestion. Constipation is the most common adverse event experienced by patients taking opioids, ranging from 40% to 90%. OIC has traditionally been treated pharmacologically with osmotic and stimulant laxatives. However, these laxatives fail to effectively treat OIC in more than 50% of patients.
What Are the Current Treatment Options?
Current treatment options for patients with OIC include nonpharmacological and pharmacological interventions. Nonpharmacological interventions include increased fluid intake, increased physical activity, reduction of offending medications (e.g., 5-HT3 antagonists, antidepressants), and increased consumption of foods that improve stool output. Pharmacological interventions include traditional (osmotic and stimulant) laxatives (e.g., polyethylene glycol, lactulose, magnesium citrate, magnesium hydroxide) for first-line treatment and peripherally acting mu-opioid receptor antagonists (e.g., naloxegol, methylnaltrexone) for second-line treatment.
For those in the noncancer pain population, there have been many more agents available on the market for OIC in the past 10 years. However, the treatment offered to a patient in clinical practice is often dependent on cost. Some patients combine prescribed treatment with over-the-counter medication.
What Is the Treatment Under Review?
Naloxegol is a peripherally acting mu-opioid receptor antagonist drug that is available as an oral tablet. It is a PEGylated derivative of the mu-opioid receptor antagonist naloxone which antagonizes opioid binding at the peripheral mu-opioid receptors. It acts primarily on the gut mu-opioid receptors and counteracts OIC with limited impact on opioid-mediated analgesic effects on the central nervous system at the intended therapeutic doses.
Why Did We Conduct This Review?
Palliative care prescriber groups requested provincial funding of naloxegol for patients experiencing OIC who have had an inadequate response to standard stimulant and osmotic laxatives (or are unable to tolerate them), irrespective of the cause of pain for which patients are taking opioids (i.e., cancer pain or noncancer pain). At the request of participating public drug programs, we reviewed naloxegol to inform a recommendation on whether it should be reimbursed for adult patients with noncancer or cancer pain who have had an inadequate response to laxative(s). Data protection ended on June 2, 2023. There is report of 1 generic submission under Health Canada review in August 2021; however, the name of the generic manufacturer or review status is not available.
Input From Interested Parties
We did not receive input from patient groups, clinician groups, or industry.
Public drug plans inquired about the evidence for naloxegol to inform a recommendation on whether it should be reimbursed for the treatment of OIC in adult patients with either cancer or noncancer pain who have inadequate response to laxative(s). The public drug plans outlined implementation questions related to treatment eligibility and discontinuation of therapy.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through when facing this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as part of a broader understanding of the condition and treatment under review.
Summary of Deliberation
The Formulary Management Expert Committee (FMEC) deliberated on all domains of value of the deliberative framework before developing their recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, please refer to the Expert Committee Deliberation at Canada’s Drug Agency document.
FMEC considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
FMEC concluded that it is uncertain whether naloxegol demonstrates acceptable clinical value versus appropriate comparators in the Canadian setting.
Through reflection on the insights shared by a person with lived experience and patient member perspective, FMEC members noted the following important patient values or perspectives: the need for better-tolerated, easy-to-administer treatments that improve bowel function, reduce OIC symptoms, and improve health-related quality of life (HRQoL) with fewer harms.
FMEC members highlighted the following discussion points:
The committee members agreed that the trials did include first-line agents that are used in Canada; however, the committee discussed that a large proportion of patients may have been on agents that are known to be ineffective for the management of OIC (i.e., docusate and bulking agents) and the number of agents that each patient was on may not be fully reflective of current Canadian practice. FMEC noted that the trials were performed 5 years before the most recent American Gastroenterological Association guidelines were published in 2019. The committee members discussed the true effect of naloxegol given the limitations highlighted with variable baseline laxative usage by patients in the trials. The committee members also heard from the guest specialists (clinical experts) that the multimodal baseline treatment used by patients highlights the need for better effective therapy for patients with OIC.
FMEC noted that at least 50% of patients were classified as having a laxative-inadequate response in the KODIAC-04 and KODIAC-05 trials; these patients had medication from 1 or more laxative classes for at least 4 days within the 2 weeks before screening and had ratings of moderate, severe, or very severe on 1 or more stool symptom domains. FMEC acknowledged that the results from the laxative-inadequate response subgroup, not the full trial population, are relevant to the population requested for reimbursement.
For noncancer pain, both pivotal trials reported statistically significant improvements in the primary outcome (response rate) with 25 mg dosing; however, there was no meaningful difference in patient-reported symptoms or HRQoL scores. For cancer pain, no randomized controlled trial evidence was available, and available evidence was limited to open-label noncomparative studies. The committee heard from the guest specialists (clinical experts) that the findings in the noncancer population would be expected to be generalizable to patients with cancer.
The committee members agreed that the frequency of weekly bowel movements was a relevant outcome. Other outcomes assessing the quality of bowel movements were appropriate, and 1 trial reported HRQoL using a suitable scale.
The committee members agreed the trials reported no significant harms compared to laxative therapy and there was sufficient long-term follow-up data reported.
There is no comparison with methylnaltrexone, an appropriate comparator in the Canadian setting. Therefore, it is uncertain whether naloxegol demonstrates acceptable clinical value versus methylnaltrexone.
Unmet Clinical Need
FMEC concluded that there is significant clinical need arising from OIC despite available treatments and naloxegol addresses this unmet clinical need.
Through reflection on the insights shared by a person with lived experience and the patient member perspective, FMEC members noted the following important patient values or perspectives: they value treatments that improve bowel function, reduce OIC symptoms, and improve HRQoL. In addition, they also appreciate treatments that are better tolerated, easier to administer, and have fewer harms.
FMEC members highlighted the following discussion points:
Opioids are prescribed for noncancer and cancer pain, and constipation is the most common side effect.
There is substantial morbidity associated with OIC. In addition to serious complications of chronic constipation, patients can experience bloating, discomfort, decreased digestion, and reduced quality of life.
FMEC discussed that OIC has traditionally been treated pharmacologically with osmotic and stimulant laxatives. Although there are many classes of traditional first-line laxatives available in Canada, more than 50% of patients do not respond to them. If patients do not respond to first-line treatment, methylnaltrexone is an option, which is available as subcutaneous injection. However, public coverage for methylnaltrexone is very limited. FMEC noted that suppositories and enemas are also second-line options (first-line agents would be oral).
Distinct Social and Ethical Considerations
FMEC concluded that naloxegol would potentially address a significant nonclinical need arising from OIC despite available treatments.
FMEC did not identify any important measures that should be implemented to ensure that the use of naloxegol addresses relevant social and ethical implications.
Through reflection on the insights shared by a person with lived experience and an FMEC patient member, FMEC members noted the following important patient perspective: The financial burden of out-of-pocket treatment and stress of pursuit of treatment exists, especially in an equity-deserving population. Patients also prefer treatments that are easier to administer.
FMEC members highlighted the following discussion points:
The committee agreed that some patients cannot tolerate first-line agents that are currently used due to intolerances and OIC would be an on-going concern for both patients and providers because patients who are chronically on opioid therapy will likely remain on them long-term.
Naloxegol provides an oral option for therapy compared with subcutaneous methylnaltrexone and a variety of laxative suppositories and enemas.
The committee reiterated that although some patients with private drug coverage may be able to access therapy (e.g., methylnaltrexone), public coverage for methylnaltrexone is very limited.
The committee agreed that oral naloxegol is not hazardous and its production and disposal would likely have a lower environmental impact compared to subcutaneous methylnaltrexone.
Economic Considerations
FMEC concluded that there are economic considerations that are important to address when implementing naloxegol.
FMEC members highlighted the following discussion points:
The reimbursement of naloxegol for the treatment of patients with OIC who have had an inadequate response to laxatives is generally expected to increase overall drug acquisition costs.
FMEC concluded that, based on the available clinical evidence, naloxegol may result in a clinical benefit compared with placebo. No evidence was identified regarding the cost-effectiveness of naloxegol relative to placebo or active comparators for the treatment of patients with OIC who have had an inadequate response to laxatives. Therefore, estimates of cost-effectiveness were not available to the committee. Because naloxegol is associated with increased drug acquisition costs and potential clinical benefit compared with placebo, FMEC recommended that price reductions may be required to ensure cost-effectiveness.
No clinical evidence was identified regarding the comparative efficacy and safety of naloxegol versus active comparators. The cost-effectiveness of naloxegol versus active comparators is unknown.
Impacts on Health Systems
FMEC did not identify any impacts on health systems that are important to address when implementing naloxegol.
FMEC members highlighted the following discussion points:
The committee highlighted that naloxegol is an oral therapy, with no specific monitoring or imaging parameters.
The committee members agreed that there is potential for fewer emergency department or primary care visits for management of severe OIC and its related complications with naloxegol use.
The committee agreed there are no major factors that need to be addressed to support the equitable implementation.
Figure 1: Recommendation Pathway
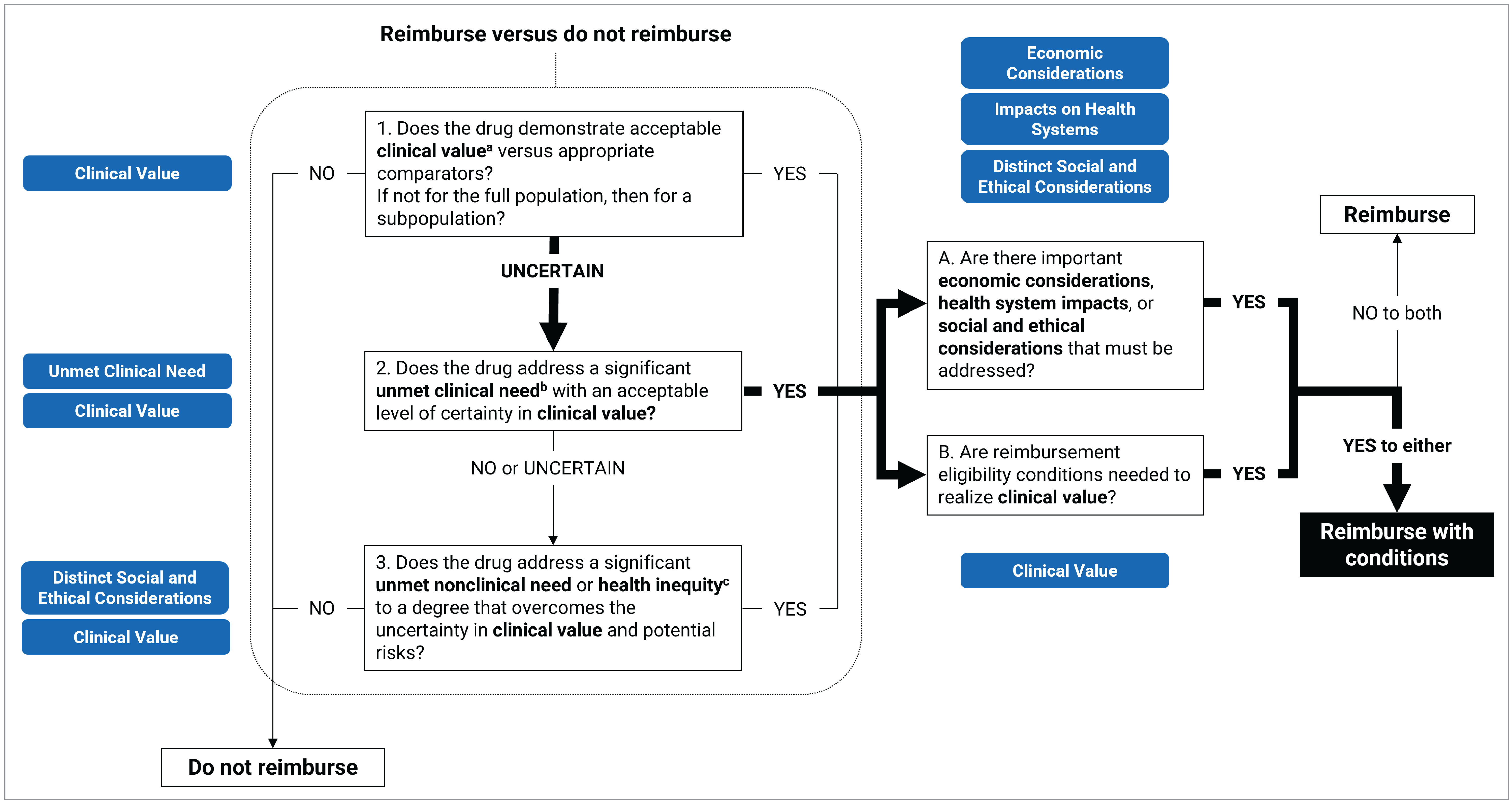
aAcceptable clinical value refers to at least comparable clinical value (if expected to be substitutive treatment) or added clinical value (if expected to be additive treatment) versus appropriate comparators.
bSignificant unmet clinical need depends on all the following: severity of the condition, availability of effective treatments, and challenges in evidence generation due to rarity of the condition or ethical issues.
cUnmet nonclinical need and health inequity are key components within the Distinct Social and Ethical Considerations domain of value.
Full Recommendation
With a vote of 7 to 0, FMEC recommends that naloxegol for the treatment of OIC in adult patients with either cancer pain or noncancer pain who have an inadequate response to laxative(s) be reimbursed if the conditions presented in Table 1 are met.
Table 1: Conditions, Reasons, and Guidance
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Naloxegol may be initiated for the treatment of OIC in adult patients with either cancer pain or noncancer pain, who have an inadequate response to laxatives if all of the following criteria are met: 1.1. receiving chronic, stable opioid therapy and report fewer than 3 spontaneous bowel movements per week despite the use of combination laxative therapy, including a stimulant laxative and an osmotic laxative 1.2. without infiltrative gastrointestinal tract malignancies or peritoneal metastases | The primary goal of therapy is bowel frequency. For noncancer pain, both pivotal trials reported statistically significant improvements in response rate with 25 mg dosing. For cancer pain, the open-labelled studies have signalled its efficacy as well. The use of combination laxative therapy is consistent with 2019 AGA OIC guidelines; a combination of at least 2 types of laxatives before escalating therapy is recommended. | In adult patients with cancer or noncancer pain, who are intolerant of or have a contraindication to standard laxatives (stimulant and osmotic) and have failed either stimulant or osmotic laxatives, naloxegol may be initiated. An adequate trial of standard laxatives (stimulant and osmotic) should be at least 7 days. In KODIAC-04 and KODIAC-05, patients were enrolled if they had been taking an oral opioid at a stable total daily dose of 30 mg to 1,000 mg of morphine (or equivalent) for 4 weeks or longer. |
Renewal or discontinuation | ||
2. Naloxegol should be discontinued if either: 2.1. opioid therapy is discontinued 2.2. there are new infiltrative gastrointestinal tract malignancies or peritoneal metastases or evidence of bowel obstruction. | Consistent with the initiation criteria, clinical practice, and/or KODIAC-04 and KODIAC-05 trials. | Naloxegol therapy may be renewed at 6 months for initial assessment of treatment response. Thereafter, naloxegol therapy may be renewed annually for patients who are stable. If there is a lack of response after a 14-day trial, naloxegol therapy should be discontinued. |
Pricing | ||
3. A price reduction may be required. | The reimbursement of naloxegol for the treatment of patients with OIC who have had an inadequate response to laxatives is generally expected to increase overall drug acquisition costs. No evidence was identified regarding the cost-effectiveness of naloxegol. Therefore, estimates of cost-effectiveness were not available to the committee. A cost-effectiveness analysis would be needed to determine whether naloxegol is cost-effective. Given that naloxegol is associated with increased drug acquisition costs and potential clinical benefit (compared with placebo) or unknown clinical benefit (compared with active comparators), price reductions may be required. | — |
AGA = American Gastroenterological Association; OIC = opioid-induced constipation.
Feedback on Draft Recommendation
The public drug programs have reviewed the draft recommendation and provided suggestions for editorial revisions, which have been incorporated. We have received no additional feedback from external partners.
FMEC Information
Members of the committee: Dr. Emily Reynen (Chair), Dr. Zaina Albalawi, Dr. Hardit Khuman, Ms. Valerie McDonald, Dr. Bill Semchuk, Dr. Jim Silvius, Dr. Marianne Taylor, Dr. Maureen Trudeau, Dr. Dominika Wranik. Two guest specialists from the Prairies participated in this review.
One member did not attend.
Meeting date: May 15, 2025
Conflicts of interest: None
Special thanks: CDA-AMC extends our special thanks to the individuals who presented directly to FMEC and to patient organizations representing the community of those living with OIC, including the Canadian Digestive Health Foundation, Tara Petch, and Christabel.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication and treatments under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys or experience with comparators under review to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journey with FMEC.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.