Drugs, Health Technologies, Health Systems
Reimbursement Recommendation
Fidaxomicin
Reimbursement request: For the treatment of Clostridioides difficile infection for adult patients who have initial episode or first recurrence
Requester: Public drug programs
Final recommendation: Reimburse with conditions
Summary
What Is the Reimbursement Recommendation for Fidaxomicin?
The Formulary Management Expert Committee (FMEC) recommends that fidaxomicin be reimbursed for the treatment of Clostridioides difficile infection (CDI) in adult patients who have an initial episode or first recurrence of CDI and are at high risk for recurrence or are allergic to vancomycin, provided certain conditions are met.
What Are the Conditions for Reimbursement?
Fidaxomicin should be covered for the treatment of CDI for adult patients who have an initial episode or first recurrence of CDI and are at high risk for recurrence or are allergic to vancomycin.
Based on the Canada’s Drug Agency (CDA-AMC) assessment of the health economic evidence, fidaxomicin may not represent good value to the health care system at the public list price. A price reduction may therefore be required.
Why Did CDA-AMC Make This Recommendation?
FMEC reviewed the CDA-AMC report, which included a review of the clinical evidence, specifically 1 randomized controlled trial comparing extended-pulsed fidaxomicin to a standard regimen of vancomycin, 2 randomized controlled trials comparing a standard regimen of fidaxomicin to a standard regimen of vancomycin, a cost comparison of fidaxomicin versus other treatments used in Canada, and an appraisal of an economic evaluation.
While the authors of 1 trial reported that extended-pulsed fidaxomicin improved sustained clinical cure and reduced recurrence compared with a standard regimen of vancomycin, evidence from 2 studies suggests that a standard regimen of fidaxomicin was similar to a standard regimen of vancomycin in clinical cure, global cure, and recurrence rates among patients with CDI.
FMEC also considered input received from drug plans and heard from a person with lived experience. FMEC concluded that fidaxomicin demonstrates acceptable clinical value in that it is at least comparable to vancomycin, an appropriate comparator in the setting in Canada, and that fidaxomicin potentially addresses an unmet clinical need for patients who are at high risk for recurrence or are allergic to vancomycin, despite the lack of clinical evidence available in these subpopulations.
Therapeutic Landscape
What Is Clostridioides Difficile Infection?
Clostridioides difficile infection (CDI) is 1 of the most common health care-associated infections that causes substantial patient burden, prolonged hospital stays, and increased health care costs. The CDI incidence rate in Canada was estimated to be 5.02 infections per 10,000 patient days in 2022. The clinical presentation of CDI can vary from the asymptomatic carrier state to symptomatic CDI (diarrhea, abdominal pain, fever) and fulminant CDI (previously severe complicated infection).
What Are the Current Treatment Options?
In Canada, the current clinical practice is to use a standard course (10 to 14 days) of vancomycin as first-line treatment for the initial CDI episode and first recurrence. While metronidazole is still listed as a treatment option, clinical experts confirmed that metronidazole is no longer used for CDI in practice due to reduced effectiveness and tolerability. Access to fidaxomicin is limited across Canada. Fecal microbiota transplant can be considered for prevention in those with multiple CDI recurrences.
What Is the Treatment Under Review?
Fidaxomicin is a narrow-spectrum macrocyclic antibacterial that inhibits bacterial ribonucleic acid synthesis.
Fidaxomicin is approved by Health Canada for the treatment of CDI in adults.
Why Did We Conduct This Review?
In 2012, the Canadian Drug Expert Committee reviewed fidaxomicin and, at that time, issued a recommendation that it not be listed at the submitted price. The data protection status of fidaxomicin ended in June 2020, making it eligible for a nonsponsored reimbursement review. At the request of the participating public drug programs, we reviewed fidaxomicin as a nonsponsored reimbursement review to inform a recommendation on whether it should be reimbursed for adult patients with an initial episode or first recurrence of CDI.
Input From Interested Parties
We did not receive input from clinician groups, patient groups, or industry.
Public drug plans inquired about the evidence for fidaxomicin to inform a recommendation on whether it should be reimbursed for the treatment of CDI for adult patients who have an initial episode or first recurrence of CDI. The public drug plans outlined implementation questions related to treatment eligibility.
Disclaimer: The perspectives shared by people with lived experience who present to the committee reflect their individual experiences and are not necessarily representative of all people with the same condition or course of treatment. Their insights provide valuable context about what a patient, support person, or caregiver might go through when facing this condition or treatment, helping to inform the committee’s deliberations. These narratives complement other forms of evidence and input and should be considered as part of a broader understanding of the condition and treatment under review.
Summary of Deliberation
The Formulary Management Expert Committee (FMEC) deliberated on all domains of value of the deliberative framework before developing their recommendation: clinical value, unmet clinical need, distinct social and ethical considerations, economic considerations, and impacts on health systems. For further information on the domains of value, please refer to the Expert Committee Deliberation at Canada’s Drug Agency document.
FMEC considered the following key discussion points, organized by the 5 domains of value.
Clinical Value
FMEC concluded that fidaxomicin demonstrates acceptable clinical value in that it is at least comparable to vancomycin, an appropriate comparator in the setting in Canada.
Through reflection on the insights shared by the person with lived experience and the patient member perspective, FMEC members noted the burden of illness on the patient and family, the difficulties of dealing with symptoms (e.g., diarrhea, cramps, fatigue, weight loss), the impact on mental health, and the ability to resume activities of daily living (e.g., resume work and social life). FMEC also noted the importance of a cure and preventing recurrence for patients.
FMEC members highlighted the following discussion points:
FMEC noted that the current clinical practice is to use vancomycin (10 to 14 days) as first-line treatment for an initial CDI episode and first recurrence. Fidaxomicin was compared to vancomycin in 3 studies. The primary outcome was related to clinical cure, which is important to patients. The secondary outcome was related to recurrence rates, which are also important to patients. Evidence from the Mikamo et al. and Rao et al. studies suggest that a standard regiment of fidaxomicin was similar to a standard regimen of vancomycin in clinical cure, global cure (sustained clinical cure), and recurrence rates among patients with CDI, while the EXTEND trial reported that extended-pulsed fidaxomicin improved sustained clinical cure and reduced recurrence compared with a standard regimen of vancomycin. FMEC noted that the comparison of the EXTEND trial used different dosing regimens between the 2 drugs (extended-pulsed fidaxomicin versus a standard regimen of vancomycin). FMEC also noted that the extended fidaxomicin dosing has the same number of total tablets as the standard dosing and that standard dosing is an on-label regimen, while the EXTEND regimen is an off-label regimen.
FMEC noted that the majority of patients in the EXTEND and Mikamo et al. trials had an initial episode or first recurrence of CDI.
FMEC discussed the microbiome activity of vancomycin and fidaxomicin and heard from the clinical experts about the biological plausibility that fidaxomicin may be more effective than vancomycin in older adults due to the differing effects on their gut microbiome. FMEC did not review any clinical evidence with respect to this issue, and therefore, the microbiome activity of vancomycin and fidaxomicin as it relates to patient outcomes in clinical practice remains unknown.
Unmet Clinical Need
FMEC concluded that it is uncertain whether there is a significant clinical need arising from CDI despite available treatments because vancomycin is effective and safe. However, fidaxomicin potentially addresses an unmet clinical need for patients who are at high risk for recurrence or are allergic to vancomycin, despite the lack of clinical evidence available in these subpopulations.
Through reflection on the insights shared by the person with lived experience and the patient member perspective, FMEC members noted the burden of illness on the patient and family, the difficulties of dealing with symptoms (e.g., diarrhea, cramps, fatigue, weight loss), and the importance of preventing recurrence and being cured and having treatment options.
FMEC members highlighted the following discussion points:
The rate of recurrence varies between 15% and 25% after an initial episode. According to the clinical experts, there is a population at higher risk for recurrence, including those who are older than 65 years, immunocompromised, frequently hospitalized, or have a number of comorbidities, including gastrointestinal conditions such as inflammatory bowel disease.
FMEC heard from guest specialists (clinical experts) that, despite vancomycin, the current standard of care in Canada, being a well- tolerated and effective treatment for controlling active CDI, a key disadvantage is that vancomycin causes disruption of the gut microbiome, lasting for weeks or months, which leads to an increased risk of recurrence of CDI. According to the clinical experts, fidaxomicin should not replace vancomycin as first-line therapy for individuals without risk factors for recurrence.
FMEC agreed that there remains an unmet clinical need for patients who are at high risk for recurrence or are allergic to vancomycin, and fidaxomicin could potentially address this unmet need despite the lack of evidence in these subpopulations.
FMEC noted that there was no difference in recurrence rates found in the 2 studies in which the same standard dosing was used. However, the authors of the EXTEND trial reported that extended-pulsed fidaxomicin improved sustained clinical cure and reduced recurrence compared with a standard regimen of vancomycin. FMEC discussed the potential that the dosing used in the EXTEND trial had an influence on the result that was independent of the drug being used. As a result, for many FMEC members, this limited their ability to understand whether fidaxomicin meets the unmet clinical need as compared to vancomycin. FMEC acknowledged that an extended therapy regimen supports improved benefit in terms of recurrence. However, whether or not vancomycin extended therapy regimen would have the same benefit remains unknown.
Distinct Social and Ethical Considerations
FMEC did not identify any important measures that should be implemented to ensure that fidaxomicin addresses relevant social and ethical implications.
Through reflection on the insights shared by the person with lived experience and the patient member perspective, FMEC members noted the burden of illness on the patient and family, the impact on mental health and daily life in terms of the ability to work or socialize, and the out-of-pocket expense of vancomycin.
FMEC members highlighted the following discussion points:
As vancomycin and fidaxomicin are both oral treatments, there is no expectation of a difference between them in terms of care setting; geographic setting; treatment burden on patients, family, or caregivers; or mode of administration, and for this reason, there are no apparent nonclinical needs arising from the condition despite available treatments.
Economic Considerations
FMEC concluded that there are economic considerations that are important to address when implementing fidaxomicin.
FMEC members highlighted the following discussion points:
The reimbursement of fidaxomicin for the treatment of the initial episode or first recurrence of CDI in adult patients is expected to increase overall drug acquisition costs compared with vancomycin-based regimens, based on publicly available list prices.
FMEC concluded that, based on the available evidence, the clinical benefit of fidaxomicin may be comparable to vancomycin.
FMEC noted that, because there was no evidence provided in the review to support a benefit for fidaxomicin versus vancomycin in higher-risk individuals, the clinical and cost-effectiveness of fidaxomicin in this subgroup is unknown.
Given that fidaxomicin is associated with higher drug acquisition costs and comparable clinical benefit compared with vancomycin-based regimens, FMEC noted that price reductions may be required to ensure cost-effectiveness.
A cost-effectiveness study from Canada was identified for those with recurrent CDI, which compared fidaxomicin with vancomycin standard dosing. Based on the included cost-effectiveness study, fidaxomicin may represent a cost-effective alternative to a standard regimen of vancomycin for the treatment of recurrent CDI, but some generalizability concerns exist.
The cost-effectiveness of fidaxomicin relative to a vancomycin tapered-pulsed regimen for first recurrence, and the cost-effectiveness of fidaxomicin relative to a vancomycin standard regimen for initial CDI, is unknown in the absence of clinical evidence.
Impacts on Health Systems
FMEC did not identify any impacts on health systems that are important to address when implementing fidaxomicin.
FMEC members highlighted the following discussion points:
There are no specific impacts of using fidaxomicin compared to vancomycin from a health system perspective.
FMEC noted that if the rate of recurrence could be reduced, it would have a positive benefit for both patients and the health care system.
FMEC acknowledged that cost, including opportunity cost, becomes a factor in considering health system sustainability.
Figure 1: Recommendation Pathway
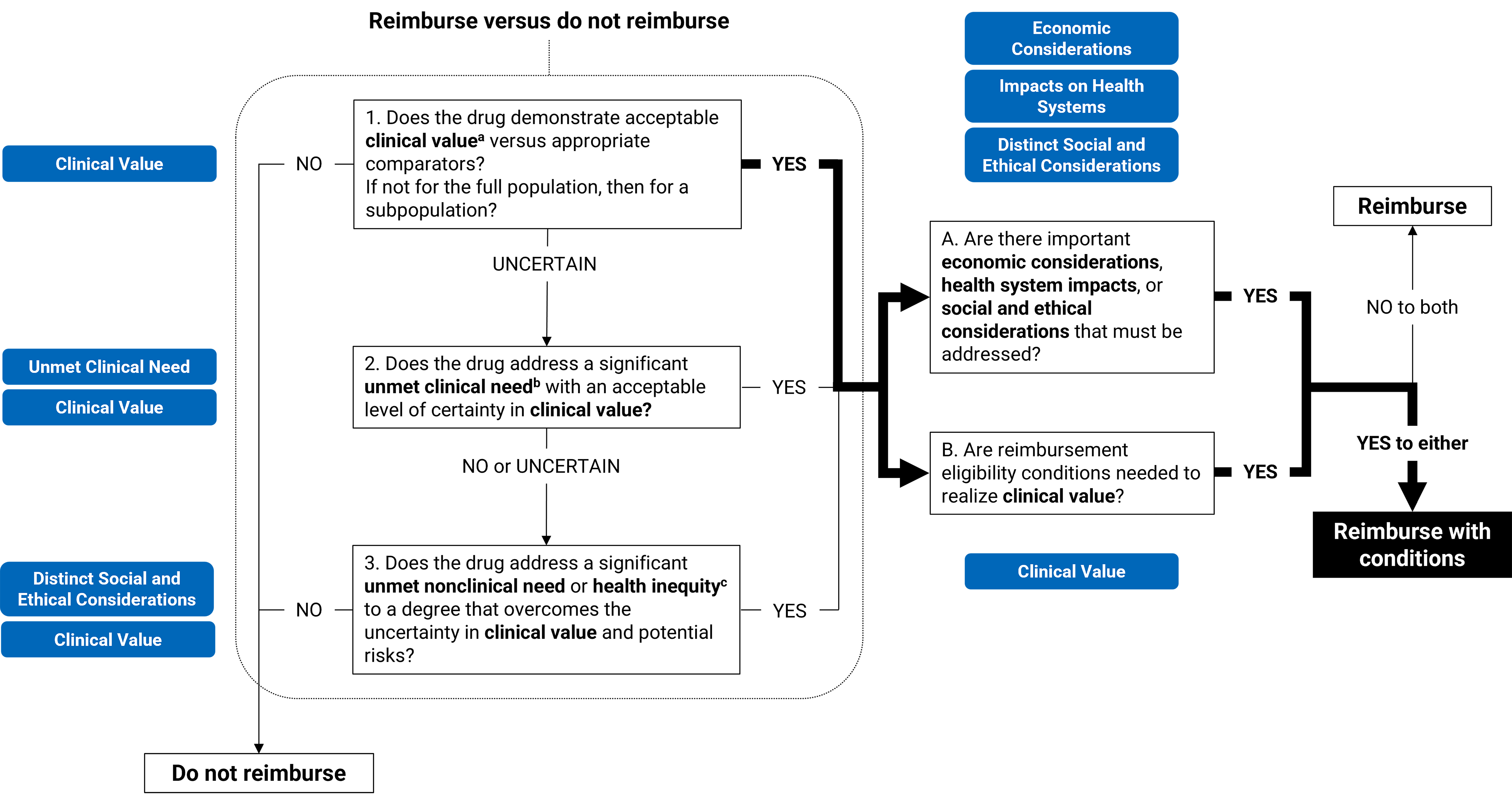
a Acceptable clinical value refers to at least comparable clinical value (if expected to be substitutive treatment) or added clinical value (if expected to be additive treatment) versus appropriate comparators.
b Significant unmet clinical need depends on all the following: severity of the condition, availability of effective treatments, and challenges in evidence generation due to rarity of the condition or ethical issues.
c Unmet nonclinical need and health inequity are key components within the Distinct Social and Ethical Considerations domain of value.
Full Recommendation
With a vote of 8 to 0, FMEC recommends that fidaxomicin for the treatment of CDI for adult patients who have an initial episode or first recurrence of CDI be reimbursed if the conditions presented in Table 1 are met.
Table 1: Conditions, Reasons, and Guidance
Reimbursement condition | Reason | Implementation guidance |
|---|---|---|
Initiation | ||
1. Fidaxomicin may be initiated for the treatment of CDI in adult patients who have an initial episode or first recurrence of CDI and are at high risk for recurrence or are allergic to vancomycin. | There remains an unmet clinical need for patients who are at high risk for recurrence or are allergic to vancomycin, and fidaxomicin could potentially address this unmet need. Evidence from the Mikamo et al. and Rao et al. studies suggests that fidaxomicin was similar to vancomycin in terms of clinical cure, global cure (sustained clinical cure), and recurrence rates among patients with CDI. The evidence from the EXTEND trial identifies a benefit in terms of recurrence for individuals on an extended regimen of fidaxomicin (off-label) vs. a standard regimen of vancomycin. While there is no evidence provided in the review to support a benefit in higher-risk individuals vs. lower-risk individuals, FMEC agreed with clinical experts that there may theoretically be a population at greater risk of recurrence who might derive greater benefit from fidaxomicin. | Based on clinical expert opinion, patients at a high risk for recurrence include those older than 65 years, who are immunocompromised, frequently hospitalized, or who have significant comorbidities. |
Pricing | ||
2. A price reduction may be required. | The reimbursement of fidaxomicin for the treatment of the initial episode or first recurrence of CDI in adult patients is expected to increase overall drug acquisition costs compared with vancomycin-based regimens. Given that fidaxomicin was associated with higher drug acquisition costs and comparable clinical benefit vs. vancomycin, a price reduction may be required. | — |
CDI = Clostridioides difficile infection; FMEC = Formulary Management Expert Committee; vs. = versus.
Feedback on Draft Recommendation
The public drug programs have shared that further implementation guidance is needed to define the high-risk population that may benefit from fidaxomicin. Given that this information is not directly informed by the evidence, an implementation advice panel comprising clinicians with expertise in the management of CDI will be set up to support this request. The public drug programs have provided suggestions for editorial revisions, which have been incorporated where feasible. We have not received any additional feedback from external partners on the draft recommendation.
FMEC Information
Members of the committee: Dr. Emily Reynen (Chair), Dr. Zaina Albalawi, Dr. Hardit Khuman, Ms. Valerie McDonald, Dr. Bill Semchuk, Dr. Jim Silvius, Dr. Marianne Taylor, Dr. Maureen Trudeau, Dr. Dominika Wranik. Two guest specialists from Ontario and British Columbia participated in this review.
Meeting date: May 15, 2025
Conflicts of interest: None
Special thanks: Canada’s Drug Agency (CDA-AMC) extends our special thanks to the individuals who presented directly to FMEC and to patient organizations representing the community of those living with or having experienced CDI, including the Canadian Digestive Health Foundation, Tara Petch, and LH.
Note: CDA-AMC makes every attempt to engage with people with lived experience as closely to the indication and treatments under review as possible; however, at times, CDA-AMC is unable to do so and instead engages with individuals with similar treatment journeys or experience with comparators under review to ensure lived experience perspectives are included and considered in Reimbursement Reviews. CDA-AMC is fortunate to be able to engage with individuals who are willing to share their treatment journey with FMEC.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.