Drugs, Health Technologies, Health Systems
Reimbursement Review
Fidaxomicin
Requester: Public drug programs
Therapeutic area: Clostridioides difficile infection
Summary
What Is Clostridioides difficile Infection?
Clostridioides difficile infection (CDI) is 1 of the most common health care-associated infections and is associated with substantial patient burden, prolonged length of hospital stays, and increased health care costs.
The CDI incidence rate in Canada was estimated as 5.02 infections per 10,000 patient days in 2022.
A clinical picture of CDI can vary from the asymptomatic carrier state or symptomatic CDI (e.g., diarrhea) to life-threatening fulminant colitis with a high mortality rate.
What Are the Treatment Goals and Current Treatment Options for CDI?
The goals of treatment for CDI are to promptly resolve clinical symptoms (mainly watery diarrhea), achieve sustained clinical response, reduce recurrence, and improve quality of life.
In Canada, vancomycin is the first-line treatment for the first CDI episode and first recurrence due to cost. Fidaxomicin is considered as an alternative option. Guidelines recommend metronidazole for initial, nonsevere CDI episodes only if fidaxomicin and vancomycin are unavailable. Fecal microbiota transplant can be considered to prevent CDI recurrences.
What Is Fidaxomicin and Why Did We Conduct This Review?
Fidaxomicin is a drug that is available as an oral tablet. Health Canada has approved fidaxomicin for the treatment of CDI in adults.
We previously reviewed fidaxomicin as a sponsored review in 2012 and issued a do not reimburse recommendation due to higher cost than existing treatment (i.e., vancomycin) and uncertainty in the cost-effectiveness. Since then, more recent evidence has become available.
At the request of the participating public drug programs, we reviewed fidaxomicin to inform a recommendation on whether it should be reimbursed for adult patients with initial episode or first-recurrence CDI.
How Did We Evaluate Fidaxomicin?
We reviewed the clinical evidence on the beneficial and harmful effects and compared the costs of fidaxomicin versus other treatments used in Canada for CDI. Vancomycin was considered a relevant treatment to compare with fidaxomicin.
The clinical evidence was identified through systematic searches for available studies. The review was also informed by input from the participating public drug programs around issues that may impact their ability to implement a recommendation. We consulted 2 clinical experts in infectious diseases as part of the review process.
What Did We Find?
Clinical Evidence
We reviewed the following clinical evidence:
One randomized controlled trial (RCT) (EXTEND in Guery et al.) comparing extended-pulsed fidaxomicin (EPFX) to vancomycin standard regimen.
Two RCTs (Mikamo et al. and Rao et al.) comparing fidaxomicin to vancomycin.
The EXTEND trial reported that fidaxomicin improved sustained clinical cure and reduced recurrence compared with vancomycin.
Evidence from the Mikamo et al. and Rao et al. studies suggests fidaxomicin was similar to vancomycin in clinical cure, global cure (sustained clinical cure), and recurrence rates among patients with CDI.
Based on safety data from the EXTEND and Mikamo et al. studies, more patients treated with fidaxomicin discontinued treatment due to adverse events (AEs) than patients treated with vancomycin. Frequencies of serious AEs (SAEs), deaths due to AEs, and any AEs were similar between treatment groups.
There was no reported data to assess the effect of fidaxomicin on quality of life in the included studies.
Economic Evidence
Reimbursing fidaxomicin for adult patients for the initial episode or first recurrence of CDI is expected to increase costs to the public drug programs.
Abbreviations
AE
adverse event
AMMI Canada
Association of Medical Microbiology and Infectious Disease Canada
CD
Clostridioides difficile
CDA-AMC
Canada’s Drug Agency
CDI
Clostridioides difficile infection
CI
confidence interval
EOT
end of treatment
EPFX
extended-pulsed fidaxomicin
HRQoL
health-related quality of life
IBD
inflammatory bowel disease
IDSA
Infectious Diseases Society of America
INESSS
l’Institut national d'excellence en santé et services sociaux
RCT
randomized controlled trial
SAE
serious adverse event
SHEA
Society for Healthcare Epidemiology of America
Background
Introduction
The objective of the clinical review is to review and critically appraise the evidence on the beneficial and harmful effects of fidaxomicin in the treatment of CDΙ in adults with initial or first-recurrent episode of CDI. The focus will be placed on comparing fidaxomicin to relevant comparators and identifying gaps in the current evidence. The economic review consists of a cost comparison for fidaxomicin compared with relevant comparators for the same population. The comparator considered relevant to the review was vancomycin.
CADTH (now Canada’s Drug Agency [CDA-AMC]) reviewed fidaxomicin in 2012 and issued a do not reimburse recommendation due to higher costs than existing treatment (i.e., vancomycin) and uncertainty in the cost-effectiveness. In 2022, l’Institut national d'excellence en santé et services sociaux (INESSS) re-evaluated and issued a positive recommendation with conditions for fidaxomicin for the treatment of CDI.1
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug (product) | Fidaxomicin (Dificid), 200 mg tablet for oral administration |
Relevant Health Canada indication | Treatment of C. difficile infection |
Mechanism of action | Narrow spectrum macrocyclic antibacterial that inhibits bacterial RNA synthesis |
Recommended dosage | 200 mg twice daily for 10 days |
Data protection status | Ended June 2020 |
Status of generic drugs or biosimilars | No generic drug on the market or under review |
Information on the CDA-AMC review | |
Requester | Formulary Working Group |
Indication under consideration for reimbursement | C. difficile infection for adult patients who have initial episode or first recurrence |
CDA-AMC = Canada’s Drug Agency; C. difficile = Clostridioides difficile; RNA = ribonucleic acid.
Sources of Information
The contents of the clinical review report are informed by studies identified through systematic literature searches and input received from interested parties.
Calls for patient group, clinician group, and industry input are issued for each Nonsponsored Reimbursement Review. We did not receive submissions from any of these groups for this review. The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized and provided to the expert committee in a separate document.
Each review team includes at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two infection disease specialists with expertise in the diagnosis and management of CDI participated as part of the review team, with representation from British Columbia and Ontario. Relevant input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Disease Background
CDI is widely recognized as 1 of the most common health care-associated infections and is associated with substantial patient burden, prolonged length of hospital stays, and increased health care costs.2 While the majority of CDIs are diagnosed in hospitals, evidence suggests community-associated CDI among healthy individuals who have not been recently hospitalized or have used antibiotics is significant, accounting for 25% to 36% of CDI cases.3,4 In Canada, Clostridioides difficile (CD) incidence was estimated at 38,000 infections per year.4 Attributable costs are estimated to be $280 million per year (plausible range, $254 to $309 million).4 In 2022, the CDI incidence rate in Canada was estimated at 5.02 infections per 10,000 patient days.5
The clinical presentation of CDI can vary from the asymptomatic carrier state to symptomatic CDI (diarrhea, abdominal pain, or fever) and fulminant colitis (previously severe complicated infection).6 Fulminant CD ϲοlitis is not common, occurring in 2% to 4% of patients with CDІ but accounts for most of the serious life-threatening complications such as sepsis, toxic megacolon, bowel perforation, and death.6
A major risk factor for CDI is the use of antibiotics, which disrupt the gut microbiota and enable the overgrowth of CD and subsequent infection.7 CDI is more common in patients aged 65 years and older, in people with severe underlying medical disorders, in people with immunocompromised status, and in patients who are hospitalized.6,7 Gastrointestinal surgery, obesity, cancer, hematopoietic stem cell transplant, and inflammatory bowel disease (IBD) all contribute to a higher risk of CDI.6,7
Recurrence of CDI is a major challenge to patients and the health care system and is associated with prolonged hospitalization and higher health care costs.6,7 About 15% to 25% of individuals experience recurrent CDI after an initial episode and up to 65% of individuals after first-recurrent episode.6,7
Current Management
Treatment Goals
The clinical experts consulted for this review emphasized that the primary goal of treating CDI is to achieve sustained clinical response, defined as the resolution of clinical symptoms (e.g., diarrhea) by the end of treatment (EOT) without subsequent recurrence. Guidelines define recurrence as the reappearance of symptoms 4 to 8 weeks after EOT.8,9 Reducing the recurrence of CDI and improving quality of life for patients are equally important outcomes of clinical success.
Current Treatment Options
The Association of Medical Microbiology and Infectious Disease Canada (AMMI Canada)8 and Infectious Diseases Society of America (IDSA)-Society for Healthcare Epidemiology of America (SHEA) treatment guidelines,9 differ on the first-line therapy for adult patients with initial episode or first recurrence of CDI. The 2021 IDSA update recommends fidaxomicin. In Canada, vancomycin is used as first-line treatment because fidaxomicin is more expensive and not accessible to most patients, which is consistent with the recommendation in the AMMI Canada guidelines. Similarly, INESSS’s 2025 Optimal Use Guide recommends either vancomycin or fidaxomicin for an initial episode, with fidaxomicin identified as a preferred option in patients with risk factors for recurrence. INESSS also recommends fidaxomicin as a first-line treatment for a first recurrence.10 The clinical experts confirmed metronidazole is no longer used for CDI in practice due to reduced effectiveness, reduced tolerability, and increasing treatment failure. However, the AMMI Canada and IDSA-SHEA guidelines support its use in specific situations. For example, patients with nonsevere infection and mild diarrhea can be treated with metronidazole when the cost of vancomycin or fidaxomicin is prohibitive or if fidaxomicin and vancomycin are unavailable.
Vancomycin in a tapered and pulsed dosing is recommended for second or subsequent recurrence CDIs. On March 6, 2025, Health Canada recently approved fecal microbiota transplant (Rebyota) for prevention of recurrent CDI following antibiotic treatment for recurrent CDI.
Key characteristics of fidaxomicin are summarized with other treatments available for CDI in the key characteristics table in Appendix 1 in the Supplemental Material.
Unmet Needs and Existing Challenges
Recurrent CDI is a major challenge, particularly as the risk of another recurrence increases with each subsequent CDI episode. Currently, fidaxomicin is only reimbursed for second or greater recurrence of CDI in Canada. The clinical experts noted that while vancomycin is well tolerated and effective for controlling active CDI, a key disadvantage is that it causes more disruption of the gut microbiome and recurrence of CDI is more common after completing treatment. There is a potential treatment gap, as patients who may benefit from fidaxomicin treating a first episode or first recurrence of CDI are currently excluded according to the current reimbursement approach with vancomycin as a first-line treatment option. Fecal microbiota transplant and/or other microbiome-based therapies are not accessible to many eligible patients and is only approved for patients with recurrent CDI, typically reserved for 2 or more recurrences of CDI. Therefore, there are limited options for patients with CD, and they are not receiving optimal care in Canada.
Considerations for Using the Drug Under Review
Contents within this section have been informed by input from the clinical experts consulted for the purpose of this review. The following has been summarized by the review team.
Place in Therapy
The clinical experts consulted indicated that fidaxomicin would be best used as first-line therapy for the initial episode or first-recurrent CDI for patients at high risk for recurrence — these would include individuals aged 65 years and older, those who are immunocompromised, frequently hospitalized, or present with other risk factors. The experts asserted that it would not be appropriate to recommend that patients first try other treatments (e.g., vancomycin) before initiating fidaxomicin. The clinical experts further noted that fidaxomicin should not replace existing first-line therapeutic options for individuals without risk factors for further recurrence. Fidaxomicin would not be routinely considered for treatment of multiply recurrent CDI.
Patient Population
According to the clinical experts, patients with risk factors for recurrent CDI should be eligible for treatment with fidaxomicin as they are likely to benefit the most from a reduced risk of recurrence. Risk factors for recurrent disease include age; immunocompromised status; significant comorbidities such as renal failure, end stage liver disease, IBD, and other predisposing gastrointestinal disease; repeated hospitalization; and frequent antibiotic exposures. The diagnosis of CDI does not pose a challenge as it is based on the presence of symptoms of diarrhea, nausea, and abdominal pain combined with detection of CDI toxins or toxin genes in a stool test, which is widely available in clinical practice. No companion testing is required for diagnosis.
Assessing the Response to Treatment
A clinically meaningful response to treatment with fidaxomicin would be considered as sustained improvement in the frequency and consistency of bowel movements without recurrence of symptoms. The clinical experts stated that resolution or significant improvement in symptoms is used to determine treatment response, and it is reasonable to evaluate a patient’s response from a functional and quality of life perspective as many patients may not always return to their baseline state. Thus, while the return to pre-CDI infection state may be ideal, it is not always reflective of treatment response in clinical practice as some individuals may not return to their pre-CDI state even after the infection has resolved.
Discontinuing Treatment
Persistence of symptoms of diarrhea, nausea, and abdominal pain with or without fever at the EOT would be considered as reasons to discontinue treatment with fidaxomicin. The clinical experts indicated that the presence of ongoing symptoms may be indicative that patients may need a longer duration of treatment, may not be benefiting from treatment, or may have another diagnosis. For example, patients with concomitant IBD may take longer to respond to therapy than those without IBD.
Prescribing Considerations
Fidaxomicin can be prescribed and administered in the community or in hospital (both outpatient and inpatient) settings. No restriction to a particular setting or physician specialist is required for diagnosis and prescribing. Specialist involvement could be considered on an individual basis if it is deemed essential to ensure the risk factors are appropriately considered.
Clinical Review
Methods
We conducted a systematic review to identify evidence of fidaxomicin for the treatment of adult patients for initial episode or first recurrence of CDI. Studies were selected according to the eligibility criteria in Table 2.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. We selected outcomes (and follow-up times) for review considering clinical expert input. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for literature searches, study selection, data extraction, and risk of bias appraisal are in Appendix 2 in the Supplemental Material.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adult patients for the initial episode or first recurrence of CDI Subgroups:
|
Intervention | Initial CDI: Fidaxomicin standard regimen First CDI recurrence: Fidaxomicin standard regimen or fidaxomicin extended-pulsed regimen |
Comparator | Initial CDI: Vancomycin standard dosing First CDI recurrence: Vancomycin standard or vancomycin tapered-pulsed regimen |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published Comparative phase III and IV RCTs |
AE = adverse event; CDI = Clostridioides difficile infection; EOT = end of treatment; HRQoL = health-related quality of life; RCT = randomized clinical trial; SAE = serious adverse event.
Clinical Evidence
An information specialist conducted a peer reviewed literature search of key bibliographic databases, trial registries, and grey literature sources. The initial search was completed on December 19, 2024, with alerts maintained until the Formulary Management Expert Committee (FMEC) meeting on May 15, 2025. Refer to the Supplemental Material for detailed search strategies.
From the search of databases and registers for primary studies, we identified 319 unique records. After screening titles and abstracts, 301 records were excluded. We screened 18 records by full text and included 3 reports of 3 studies in the systematic review. No additional relevant records were identified via other sources. A list of excluded studies, including reasons for exclusion, are in the Supplemental Material.
Systematic Review
Description of Studies
Study Characteristics
Characteristics of the included studies are summarized in Table 3.
Table 3: Characteristics of Studies Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
Guery et al.11 EXTEND study Phase IIIb-IV superiority, vancomycin-controlled, open-label RCT N = 364 |
|
| Intervention: Extended-pulsed fidaxomicin 200 mg twice daily on day 1 to day 5, and then only once daily on alternate days from day 7 to day 25. Comparator: Vancomycin 125 mg orally 4 times daily for 10 days. | Primary end point:
Secondary end points:
Exploratory end points:
|
Mikamo et al.12 Phase III, noninferiority vancomycin-controlled, double-blind RCT N = 215 |
|
| Intervention:
Comparator:
| Primary end point:
Secondary end points:
|
Rao et al.13 Phase IV vancomycin-controlled, open-label RCT N = 144 |
|
| Intervention: Fidaxomicin 200 mg orally twice daily for 10 days. Comparator: Vancomycin 125 mg orally 4 times daily for 10 days. | Primary end point:
Secondary end points:
|
CD = Clostridioides difficile; CDI = Clostridioides difficile infection; EOT = end of treatment; FAS = full analysis set; mFAS = modified full analysis set; RCT = randomized controlled trial; rCDI = recurrent CDI; UBM = unformed bowel movement.
Sources: Guery et al.,11 Mikamo et al.,12 Rao et al.13
The EXTEND,11 Mikamo et al.,12 and Rao et al.13 studies were all phase III or IV RCTs. While the EXTEND11 and Rao et al.13 studies were open-label, Mikamo et al.12 was a double-blind study. All studies included adult patients with confirmed symptomatic CDI. In addition, all patients enrolled for the Rao et al.13 trial were receiving concomitant antibiotics. Patients with IBD were excluded in the EXTEND trial while the other 2 trials excluded patients with life-threatening fulminant CDI (severe complicated disease). The dosing of fidaxomicin varied between trials. The EPFX dosing regimen was used in the EXTEND trial, contrasted with standard dosing of fidaxomicin in the other 2 trials. All 3 trials used standard dosing of vancomycin as the active comparator. Primary end points differed slightly between the studies — sustained clinical cure at 30 days after EOT for the EXTEND trial, global (sustained) cure of CDI at EOT with no recurrence during 28-day follow-up for the Mikamo et al.12 trial, and clinical cure at EOT for the Rao et al.13 trial.
Statistical Testing and Analysis Populations
EXTEND study (Guery et al.11): A required sample size of 346 patients (173 per treatment group) was identified to provide at least 90% power to reject a 2-sided null hypothesis of no difference in sustained clinical cure 30 days after treatment at an alpha significance level of 0.05. Historical sustained cure rates of 85% for EPFX and 70% for vancomycin were used in sample size calculation. Sustained clinical cure for the study was calculated using the Cochran-Mantel-Haenszel test adjusted for baseline stratification factors. Secondary end points included sustained clinical cure at days 40, 55, and 90; clinical response; and recurrence rates. Multivariate logistic regression was performed for end points of sustained clinical cure at days 40, 55, and 90; clinical response at day 12; and rate of relapse on day 90. Time-to-event analyses used Kaplan-Meier methods and the stratified Wilcoxon-Gehan test to compare survival time distributions. Efficacy outcomes were analyzed using the modified full analysis set (primary analysis) and per-protocol set. The safety analysis set included all patients who received at least 1 dose of study medication. Difference in time to resolution of diarrhea was analyzed using the Cox proportional hazards model, adjusting for treatment arm, and baseline stratification factors. Adjusted P values were obtained using the Hochberg procedure for certain end points if the primary end point showed significant differences between treatment arms.
Mikamo et al.12 trial: A total of 210 patients (105 per treatment group) were required to achieve 90% power to reject a 1-sided noninferiority hypothesis of no difference at an alpha level of 0.025. This sample size calculation was based on the assumptions of a 1:1 allocation ratio, 10% noninferiority margin, allowing for withdrawal of 10% of patients, historical global cure rates of 75.5% with fidaxomicin and 63.8% with vancomycin. Treatment difference between fidaxomicin and vancomycin groups and the 95% confidence intervals (CIs) were calculated using the Mantel-Haenszel test based on whether patients had a prior episode of CDI. The primary population for clinical efficacy (cure, global cure, and resolution of diarrhea) was the full analysis set. Patients with missing data for clinical cure and CDI recurrence were considered to have negative outcomes — no clinical cure and CDI recurrence. Global cure (sustained cure) of CDI was derived from the cure and recurrence of CDI imputed for missing values. Global cure, clinical cure, recurrence, and microbiological efficacy and 95% CIs were calculated. Kaplan-Meier estimates were calculated for time to CDI recurrence and resolution of diarrhea, and comparisons made between treatment groups using the log rank test. Noninferiority of fidaxomicin versus vancomycin would be demonstrated in the primary analysis if the lower limit of the 95% CIs for a difference in global cure rate were higher than −10%.
Rao et al.13 study: Power calculations were based on an expected 90% cure rate with fidaxomicin and 75% with vancomycin. It was estimated that 200 patients (100 per treatment group) were required to achieve 80% power to reject a null hypothesis of no difference in clinical cure rates at an alpha level of 0.05 using the Fisher exact test. Other analyses relevant to clinical cure was performed using the chi-square test, Student t test, and Wilcoxon rank sum test. Difference in the time to resolution of diarrhea was analyzed using the Cox proportional hazards model.
Patient Disposition
Patient disposition for each included study is summarized in Guery et al.,11 Mikamo et al.,12 and Rao et al.13
In the EXTEND trial in Guery et al.,11 364 adult patients were enrolled and randomly assigned to receive EPFX (183 patients) or vancomycin (181 patients). Two patients randomized to the fidaxomicin arm were withdrawn from the study before receiving treatment as they did not have clinically confirmed CDI, resulting in 181 patients in each treatment group for safety analysis. Six patients who did not have confirmed CD toxin were further excluded — 4 patients in the EPFX group and 2 patients in the vancomycin group. In total, 356 patients with confirmed CD were included in the modified full analysis set for efficacy analysis, 177 in the EPFX group and 179 in the vancomycin group. Of the patients assigned to treatment, 38 of 181 in the EPFX group and 15 of 181 in the vancomycin group discontinued treatment. Reasons for treatment discontinuation in the EPFX arm were death (13 patients), AEs (8 patients), patient decision to withdraw (6 patients), lack of efficacy (4 patients), loss to follow-up (4 patients), physician decision (2 patients), and noncompliance with the study drug. Vancomycin discontinuation was due to death (4 patients), AEs (2 patients), patient decision to withdraw (4 patients), lack of efficacy (4 patients), or another unspecified reason (1 patient). After excluding patients who discontinued the study after treatment completion during the 40, 55, or 90-day follow-up time points, 132 patients treated with EPFX, and 125 patients treated with vancomycin completed the study.
The Mikamo et al.12 study enrolled 215 eligible patients who were randomized: 106 to fidaxomicin and 109 to vancomycin. Two patients in the fidaxomicin group and 1 in the vancomycin group withdrew before receiving treatment. All remaining patients tested positive for CD toxins A and B and were included in the full analysis set and safety analysis set. In the fidaxomicin arm, a total of 12 patients discontinued treatment. Of these 12 patients, 6 discontinued due to AEs, 1 requested to withdraw, 3 had protocol deviations, and 2 discontinued study treatment for other reasons. In the vancomycin arm, 8 patients discontinued treatment. Of these 8 patients, 1 discontinued due to AEs, 4 had protocol deviations, and 3 discontinued study treatment for other reasons. A total of 68 patients treated with fidaxomicin and 70 patients treated with vancomycin completed the study.
Of the 144 patients enrolled in the Rao et al.13 study, there were 74 patients randomized to fidaxomicin and 70 patients randomized to vancomycin. In the fidaxomicin arm, a total of 10 patients discontinued treatment. Of these 10 patients, 3 died, 3 patients had their CDI therapy changed by their physician, 3 withdrew to receive comfort care, 3 withdrew after 12 weeks of CDI or concomitant antibiotics, and 2 discontinued study treatment for other reasons. In the vancomycin arm, 16 patients discontinued treatment. Of these 16 patients, 7 died, 4 patients had their CDI therapy changed by their physician, 1 withdrew to receive comfort care, 3 withdrew after 12 weeks of CDI or concomitant antibiotics, and 1 was withdrawn by physician. During the 30-day follow-up after completing assigned treatment, 4 patients died in the fidaxomicin group, and 4 patients died in the vancomycin group.
Baseline Characteristics
The key patients’ baseline characteristics from each included study are outlined in Table 4. Detailed baseline characteristics can be found in Guery et al.11 Table 1, Mikamo et al.12 Table 2, and Rao et al.13 Table 1.
Treatment Exposure and Concomitant Medications
Patients in the EXTEND study received either fidaxomicin or vancomycin. Fidaxomicin was administered as 200 mg twice daily on day 1 to day 5, and then only once daily on alternate days from day 7 to day 25. Vancomycin was 125 mg orally 4 times daily for 10 days. Concomitant therapies were not reported in the EXTEND trial.11
In the Mikamo et al.12 study, 1 treatment arm received fidaxomicin 200 mg orally twice daily for 10 days and placebo 4 times daily for 10 days. The other treatment arm received vancomycin 125 mg orally 4 times daily for 10 days and placebo twice daily for 10 days. The use of concomitant medications was reported in 8 patients in the fidaxomicin group and 11 patients in the vancomycin group, although the specific type of medications were not described.
Concomitant antibiotics were administered to all patients in the Rao et al.13 study. Patients were treated with either fidaxomicin 200 mg twice daily or vancomycin 125 mg 4 times daily for 10 days or until the end of duration of concomitant antibiotics. The duration of fidaxomicin treatment was 15 days (± 12.2) and vancomycin treatment was 17.2 days (± 17). The maximum duration of treatment with fidaxomicin or vancomycin during concomitant antibiotics was up to 12 weeks.
Adherence to study treatments was not reported in the 3 trials.
Table 4: Baseline Characteristics From Studies Included in the Systematic Review
Characteristic | EXTEND study in Guery et al.11 | Mikamo et al.12 | Rao et al.13 | |||
|---|---|---|---|---|---|---|
EPFX fidaxomicin (N = 177) | Vancomycin (N = 179) | Fidaxomicin (N = 104) | Vancomycin (N = 108) | Fidaxomicin (n = 74) | Vancomycin (n = 70) | |
Age (years) | ||||||
mean (SD) | NR | NR | 74.0 (13.5) | 75.0 (12.5) | NR | NR |
median (range) | 75 (IQR, 69 to 83) | 75 (IQR, 67 to 82) | 76.5 (26 to 93) | 78.0 (21 to 92) | NR | NR |
Age category (years), n (%) | ||||||
< 65 | NR | NR | 17 (16.3) | 18 (16.7) | 51 (68.9) | 40 (57.1) |
≥ 65 to 74 | NR | NR | 26 (25.0) | 16 (14.8) | 15 (20.3) | 20 (28.6) |
≥ 75 | NR | NR | 61 (58.7) | 74 (68.5) | 8 (10.8) | 10 (14.3) |
Sex, n (%) | ||||||
Female | 107 (60) | 100 (56) | 56 (53.8) | 54 (50.0) | 40 (54.1) | 35 (50.0) |
Male | 70 (40) | 79 (44) | — | — | 34 (45.9) | 35 (50.0) |
Racea | ||||||
Asian | NR | NR | NR | NR | 2 | 3 |
Black | NR | NR | NR | NR | 10 | 5 |
White | 149 (84) | 153 (85) | NR | NR | 61 | 61 |
Missing | 28 (16) | 26 (15) | NR | NR | 1 | 1 |
Number of UBM per day | ||||||
Mean (SD) | 6.8 (4.7) | 6.4 (3.4) | 5.8 (6.3) | 5.6 (3.9) | NR | NR |
Median (range) | 5 (IQR, 4 to 7) | 5 (IQR, 4 to 7) | 4.0 (0 to 60) | 5.0 (0 to 29) | NR | NR |
Severity of CDI, n (%)b | ||||||
Nonsevere (mild or moderate) | 114 (64) | 112 (63) | 79 (76.0) | 86 (79.6) | NR | NR |
Severe | 63 (36) | 67 (37) | 25 (24.0) | 22 (20.4) | NR | NR |
Prior CDI, n (%) | ||||||
Yes | NR | NR | 14 (13.5) | 16 (14.8) | 16 (21.6) | 8 (11.4) |
No | NR | NR | 90 (86.5) | 92 (85.2) | NR | NR |
Prior CDI ≤ 3 months, n (%) | ||||||
0 | 141 (80) | 140 (78) | 92 (88.5) | 96 (88.9) | NR | NR |
1 | 26 (15) | 29 (16) | 12 (11.5) | 12 (11.1) | NR | NR |
2 | 10 (6) | 10 (6) | NR | NR | ||
Use of antibiotics for condition other than CDI, n (%) | ||||||
Yes | 128 (72) | 129 (72) | NR | NR | 74 (100) | 70 (100) |
No | 49 (28) | 50 (28) | NR | NR | 0 | 0 |
Use of antibiotics for CDI before screening, n (%) | ||||||
Metronidazolec | NR | NR | 5 (4.8) | 3 (2.8) | NR | NR |
No | NR | NR | 99 (95.2) | 105 (97.2) | NR | NR |
Duration of CAs, days | NR | NR | NR | NR | 16.5 (13.1) | 20.6 (19.7) |
Duration of CDI therapy, days | NR | NR | NR | NR | 15 ± 12.2 | 17.2 ± 17 |
Cancer status, n (%) | ||||||
Yes | 38 (21) | 37 (21) | NR | NR | 34 (45.9) | 38 (54.3) |
No | 139 (79) | 142 (79) | NR | NR | NR | NR |
History of stem cell transplant, n (%) | NR | NR | NR | NR | 4 (5.4) | 10 (14.3) |
History of IBD, n (%) | NR | NR | NR | NR | 3 (4.1) | 2 (2.9) |
ICU admission, n (%) | NR | NR | NR | NR | 12 (16.2) | 11 (15.7) |
Proton pump inhibitors, n (%) | NR | NR | NR | NR | 29 (39.2) | 30 (42.9) |
Residential setting before study enrolment, n (%) | ||||||
Own residence | 102 (58) | 103 (58) | NR | NR | NR | NR |
Family residence | 66 (37) | 59 (33) | NR | NR | NR | NR |
Nursing home | 4 (2) | 6 (3) | NR | NR | NR | NR |
Long-term care facility | 1 (1) | 4 (2) | NR | NR | NR | NR |
Other | 2 (1) | 7 (4) | NR | NR | NR | NR |
Missing | 2 (1%) | 0 | NR | NR | NR | NR |
CA = concomitant antibiotics; CDI = Clostridioides difficile infection; EPFX = extended-pulsed fidaxomicin; IBD = inflammatory bowel disease; ICU = intensive care unit; IQR = interquartile range; NR = not reported; SD = standard deviation; UBM = unformed bowel movement.
aFor the Guery et al.11 study, not all study sites were permitted to report the race of patients, and in these cases this information was reported as missing.
bSevere CDI defined as creatinine > 1.5 mg/dL, white blood cell count > 15,000/mL, or body temperature > 38.5°C at baseline.
cTreatment for ≥ 3 days but failed to achieve clinical improvement.
Sources: Guery et al.,11 Mikamo et al.,12 and Rao et al.13
Critical Appraisal
Internal Validity
In the EXTEND RCT, randomization was achieved using an interactive web response system that helped conceal allocation. Patients were stratified by baseline CDI severity (severe versus nonsevere), presence or absence of cancer (defined as diagnosis of cancer within 6 months of the study or ongoing therapy for cancer treatment), age (younger than 75 years versus 75 years and older), or number of previous CDI episodes (0, 1, or 2) in the 3 months before study entry. The baseline characteristics of patients appear balanced between treatment groups. In the Mikamo et al.12 RCT, randomization was performed using dynamic allocation with a biased-coin minimization approach, with study centre and prior occurrence of CDI as allocation factors. The treatment arms were balanced across demographic and comorbidities. Patients were stratified for randomization based on 2 criteria: intensive care unit admission at study enrolment and the CDI episode (first episode or first recurrence vs. second or more recurrence). Randomization was done using a randomization binder stored electronically by the trial coordinating centre. Differences between treatment groups were reported for some baseline characteristics (prior history of CDI, history of stem cell transplant, or duration of concomitant antibiotics). The imbalances introduce uncertainty in the magnitude and precision of the reported effects of treatment.
The Mikamo et al.12 trial was double-blind, in which caregivers were also unaware of treatment assignments. Both the EXTEND11 and Rao et al.13 trials were open-label trials that lacked blinding meaning patients and investigators were aware of assigned treatments. Because investigators were aware of treatment in both studies, there was potential for observer bias in the efficacy of treatment on subjective outcome assessments. In addition, patients who were discharged from the hospital during the follow-up provided the information by telephone. Self-reported outcomes can introduce the possibility of recall or preference bias.
Imputations were used for missing data in the EXTEND trial for clinical cure, sustained clinical cure, and recurrence. No imputation was used to account for other missing data. Patients who discontinued treatment early and had missing tests of cure assessment were regarded as not achieving clinical cure. Similarly, patients with missing assessments for sustained clinical cure after EOT were included in the analysis as not achieving sustained clinical cure. Patients with clinical response who discontinued before day 40 and had missing assessments for CDI recurrence before early discontinuation on days 40, 55, or 90 were included in the analysis as not having recurrence. Patients with missing data for clinical cure and CDI recurrence in the Mikamo et al.12 trial were considered to have negative outcomes — no clinical cure and CDI recurrence. Global cure (sustained cure) of CDI was derived from the cure and recurrence of CDI imputed for missing values. For the Rao et al.13 study, patients with missing data due to the loss to follow-up and with missing assessment for CDI recurrence, readmission, and cure, were considered indeterminate and treated in 2 analyses. One analysis was restricted to the clinically evaluable population, excluding patients lost to follow-up while the intention-to-treat analysis included patients lost to follow-up as negative efficacy outcomes.
External Validity
All 3 trials included patients with clinically confirmed CDI, defined as having diarrhea (more than 3 unformed bowel movements in a day) and a positive stool test for CD, which is important in making treatment decisions that are consistent with what would be expected in clinical practice. The EXTEND trial was designed to include only older adults. Although the Mikamo et al.12 trial allowed the inclusion of young adults, defined as 20 years and older, older adults were predominantly enrolled in the study. The median ages in the EXTEND11 and Mikamo et al.12 studies were aged 75 to 78 years. These 2 trials had an older patient population compared with the Rao et al.13, in which the population was younger than 65 years. There is a possibility that the results of the EXTEND11 and Mikamo et al.12 studies are more applicable to the demographic of patients seen in clinical practice in Canada considering that age groups aligned with the higher risk for patients with CD treated by the consulted clinical experts.
Findings from the 3 trials did not distinguish between results for an initial episode or first recurrence of CDI. Notably, the trial population consisted of a large proportion of patients with an initial episode or first recurrence of CDI, amounting to about 95% in the EXTEND trial and 88% in the Mikamo et al.12 trial. The number of patients with second recurrence is low (6% of each treatment arm). The results are reported for the combined population, which makes interpretation of the efficacy results based on the number of previous CDI occurrence difficult. None of the trials evaluated HRQoL, resulting in the effect of fidaxomicin on HRQoL being unknown. AEs appeared to be consistent with the documented events expected for the treatments used in the trials; however, the open-label design in 2 studies makes it challenging to determine whether knowledge of treatment assignment influenced AE reporting.
The EXTEND,11 Mikamo et al.,12 and Rao et al.13 trials only enrolled patients who were hospitalized and those with multiple comorbidities which may be associated with lower response rates. For example, some patients had cancer, received a stem cell transplant, had IBD, had used proton pump inhibitors, or had concomitant use of antibiotics (all patients in Rao et al.13 trial), which may be associated with lower response rates. The clinical experts noted that the rate of clinical cure for fidaxomicin they observed in practice is higher than those reported in the studies, sometimes up to 90% cure rates. The response rate is higher for individuals without comorbidities and uncomplicated initial or first-recurrent CDI in contrast to the participants in these trials who were either hospitalized and/or had multiple comorbidities. The Rao et al.13 study may have enrolled participants with multiple recurrences of CDI as this data were not reported.
There were a substantial number of patients with severe CDI (but not fulminant CDI) reported in both treatment arms of the EXTEND and Mikamo et al.12 studies. Across both studies reporting on CDI severity, the percentage of patients with severe disease ranged from 20% to 37% of the study population. While severity of CDI has no strictly defined or standard definition, the clinical experts mentioned that the assessment of severity in the trials aligned with the parameters commonly used in practice. For example, severe CDI in the EXTEND trial was defined as leucocyte count of more than 15 x 109 cells/L or increase in serum creatinine of more than 50% higher than a patient's normal level or albumin of less than 30 g/L. Severe CDI in the Mikamo et al.12 trial was defined as creatinine of more than 1.5 mg/dL, white blood cell count of more than 15,000 per mL or body temperature of more than 38.5°C at baseline.
The dosages and administration of fidaxomicin used in the Mikamo et al.12 and Rao et al.13 trials were aligned with the standard 10-day dosing approved by Health Canada and can be generalizable to the clinical setting in Canada. The EXTEND11 trial used an EPFX regimen as the intervention, which has the same total dose of fidaxomicin as a standard regimen but administered over a longer period (25 days). No comparison between the standard 10-day regimen to the extended-pulse regimen was planned for this study. Adherence to study treatments and use of concomitant therapy were not reported in the EXTEND11 trial, so whether these were aligned with clinical practice in Canada is unknown. In the Mikamo et al.12 study, concomitant medications were reported for 8 patients in the fidaxomicin group and 11 patients in the vancomycin group, though the treatments were not specified. This may introduce potential for bias in the estimates of efficacy due to deviations from intended interventions, however the use of concomitant medications is expected in practice. Concomitant antibiotics for non-CDIs were taken by all patients in the Rao et al.13 study.
Three trials compared fidaxomicin with vancomycin which was the relevant comparator for this review, which are treatments that are currently reimbursed by at least 1 public drug plan in Canada. Clinical experts consulted in this review indicated that vancomycin in a standard dosing regimen is a relevant comparator for both an initial episode and a first recurrence of CDI, although a tapered-pulsed vancomycin regimen may also be used for a first recurrence. However, the 3 trials included in this review only evaluated vancomycin using a standard dosing regimen and did not distinguish between patients with an initial episode versus a first recurrence.
The efficacy outcomes used in the trials (clinical cure, sustained clinical cure, recurrence rates) are standard in trials of antibiotics. The clinical experts highlighted that time to resolution of diarrhea is an outcome measurement routinely used in clinical trials. In the clinical setting, it is used in the initial follow-up period but not in monitoring long-term efficacy.
Results
Efficacy
Results for important outcomes for this review are presented in Tables 5, 6, and 7 and Figures 1 and 2.
Key results in the EXTEND study in Guery et al.11 include:
Evidence failed to demonstrate a significant difference in clinical cure rates between the EPFX and vancomycin groups at day 12 and 2 days after EOT.
Sustained clinical cure of CDI at 30 days after EOT was higher in the EPFX group than in the vancomycin group.
Recurrence rates were lower in the EPFX group compared with the vancomycin group at all 3 time points in the follow-up visits after treatment (day 40, 55, and 90).
No significant difference in the median time to resolution of diarrhea between both CDI treatments.
Key results in the Mikamo et al.12 study include:
Global cure rates and recurrence rates for CDI for patients treated with fidaxomicin were comparable with patients treated with vancomycin.
Higher cure rates were observed in post hoc analysis for global cure and clinical cure, though these are not presented in the table in this report.
Median time to resolution of diarrhea was similar between the treatment groups.
Key results in the Rao et al.13 study include:
Evidence failed to show difference in clinical cure rate, sustained clinical cure, and recurrence rate between fidaxomicin and vancomycin treatment groups.
Figure 1: Efficacy Outcomes in the EXTEND Study in Guery et al.
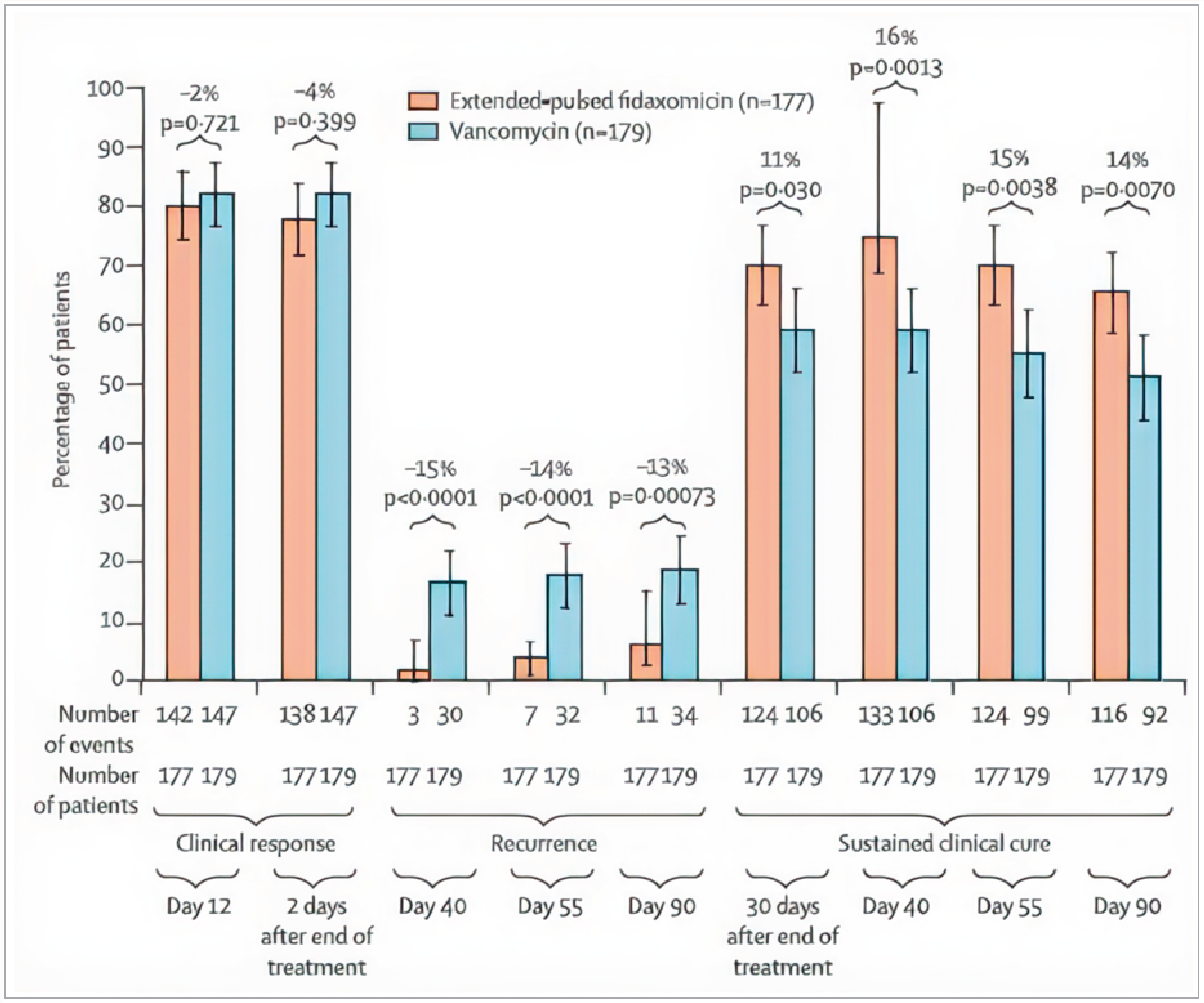
Source: Guery et al.11 Reprinted from: Guery B, Menichetti F, Anttila VJ, et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomized, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis. 2018;18(3):296-307. Copyright (2025) with permission from Elsevier.
Figure 2: Efficacy Outcomes in the Mikamo et al. Study
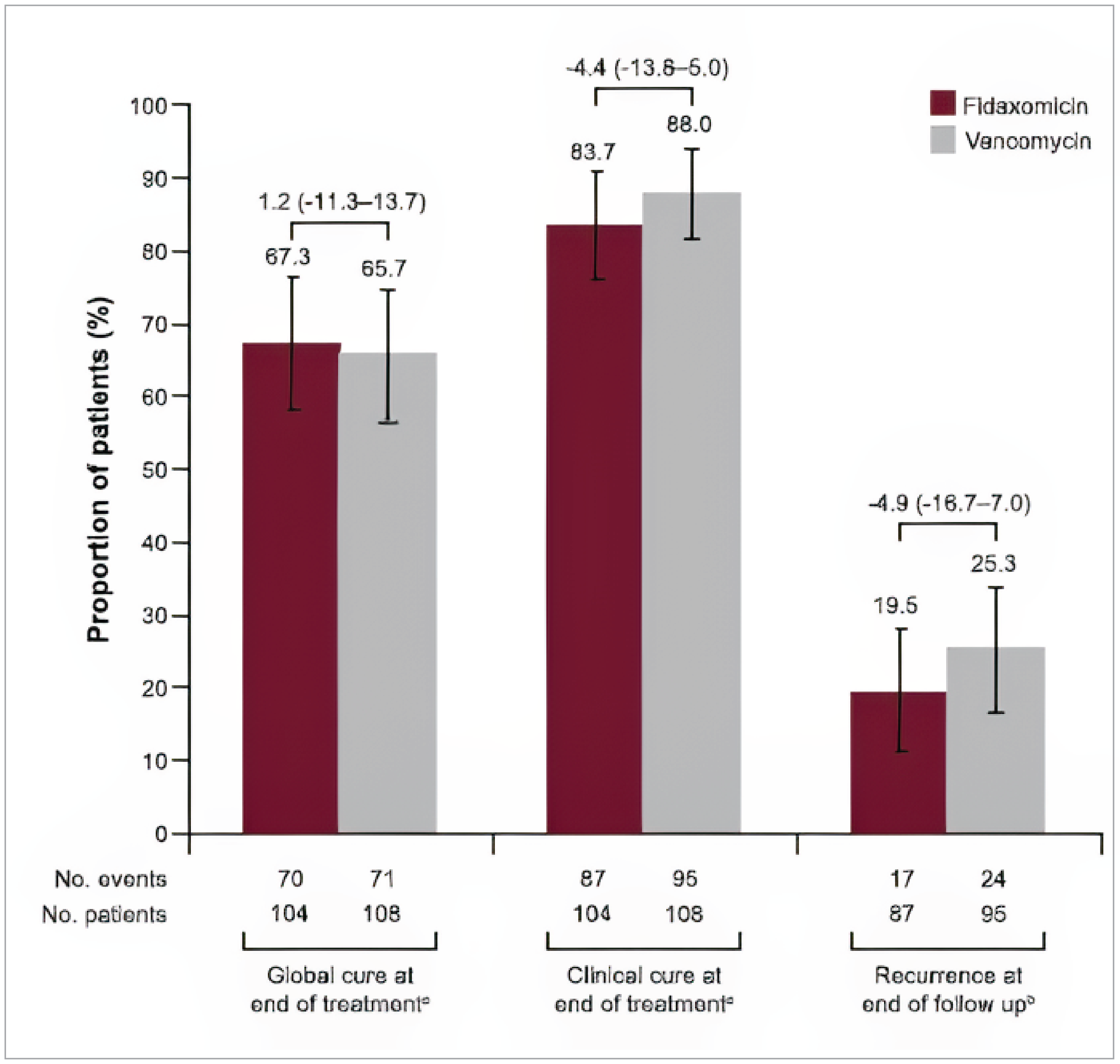
FAS = full analysis set; FAS-R = full analysis set for recurrence.
aFAS.
bFAS-R.
Source: Mikamo H, Tateda K, Yanagihara K, et al.12 Efficacy and safety of fidaxomicin for the treatment of Clostridioides (Clostridium) difficile infection in a randomized, double-blind, comparative Phase III study in Japan. J Infect Chemother. 2018;24(9):744-752. Copyright 2018 by the authors. Available from: https://www.sciencedirect.com/science/article/pii/S1341321X18301570. Reprinted in accordance with Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0): https://creativecommons.org/licenses/by-nc-nd/4.0/.
Table 5: Key Efficacy Results of EXTEND Study
Variable | Modified FAS | |
|---|---|---|
EPFX fidaxomicin (N = 177) | Vancomycin (N = 179) | |
Clinical cure rate at day 12 | ||
Clinical cure rate, n (%) | 142 (80%) | 147(82%) |
Treatment difference in clinical cure rates, % (95% CI) | −1.9% (−10.0% to 6.2%) | |
Odds ratio (95% CI) | 0.91 (0.54 to 1.54) | |
P value | 0.721 | |
Clinical cure rate 2 days after EOT | ||
Clinical cure rate, n (%) | 138 (78%) | 147 (82%) |
Treatment difference in clinical cure rates, % (95% CI) | −4.2% (−12.5% to 4.1%) | |
Odds ratio (95% CI) | 0.81 (0.48 to 1.35) | |
P value | 0.399 | |
Sustained clinical cure of CDI at 30 days after EOT | ||
Sustained clinical cure, n (%) | 124 (70%) | 106 (59%) |
Treatment difference in sustained clinical cure, % (95% CI) | 11% (1.0% to 20.7%) | |
Odds ratio (95% CI) | 1.62 (1.04 to 2.54) | |
P value | 0.030 | |
Sustained clinical cure | ||
At day 40, sustained clinical cure, n (%) | 133 (75%) | 106 (59%) |
Odds ratio (95% CI) | 2.10 (1.32 to 3.34) | |
P value | 0.0013 | |
At day 55, sustained clinical cure, n (%) | 124 (70%) | 99 (55%) |
Odds ratio (95% CI) | 1.91 (1.23 to 2.98) | |
P value | 0.0038 | |
At day 90, sustained clinical cure, n (%) | 116 (66%) | 92 (51%) |
Odds ratio (95% CI) | 1.80 (1.17 to 2.77) | |
P value | 0.0070 | |
Recurrence rate of CDI | ||
At day 40, rate of recurrence, n (%) | 3 (2%) | 30 (17%) |
Odds ratio (95% CI) | 0.09 (0.03 to 0.29) | |
P value | < 0.0001 | |
At day 55, rate of recurrence, n (%) | 7 (4%) | 32 (18%) |
Odds ratio (95% CI) | 0.20 (0.08 to 0.46) | |
P value | < 0.0001 | |
At day 90, rate of recurrence, n (%) | 11 (6%) | 34 (19%) |
Odds ratio (95% CI) | 0.29 (0.14 to 0.60) | |
P value | 0.00073 | |
Time to resolution of diarrhea | ||
Median time to resolution, hours (95% Cl) | 34.0 (25.0 to 49.0) | 22.0 (10.0 to 30·0) |
P value | 0.068 | |
CDI = Clostridioides difficile infection; CI = confidence interval; EOT = end of treatment; EPFX = extended-pulsed fidaxomicin; FAS = full analysis set.
Notes: Odds ratios were calculated using Cochran-Mantel-Haenszel test, adjusted for baseline stratification factors. Adjusted P values were obtained using the Hochberg procedure.
Source: Guery et al.11
Table 6: Key Efficacy Results of Mikamo et al. Study
Variable | Full analysis set | |
|---|---|---|
Fidaxomicin (n = 104) | Vancomycin (n = 108) | |
Clinical cure rate of CDI at EOT | ||
Clinical cure rate, n (%) | 87 (83.7) | 95 (88.0) |
Treatment difference in clinical cure, % (95% CI) | −4.4% (−13.8% to 5.0%) | |
Global cure rate of CDI at EOTa | ||
Global cure rate, n (%) | 70 (67.3) | 71 (65.7) |
Global cure rate, 95% CI | 58.3 to 76.3 | 56.8 to 74.7 |
Treatment difference in global cure rate, % (95% CI) | 1.2% (−11.3% to 13.7%) | |
Recurrence rate during 28-day follow-upb | ||
Number of patients contributing to the analysis, n | 87 | 95 |
Rate of recurrence, n (%) | 17 (19.5) | 24 (25.3) |
Treatment difference in recurrence rate, % (95% CI) | −4.9% (−16.7% to 7.0%) | |
Time to resolution of diarrhea, days | 4 days | 3 days |
P value | 0.342 | |
CDI = Clostridioides difficile infection; CI = confidence interval; EOT = end of treatment.
aGlobal cure rate is the proportion of all treated patients who were cured at EOT and had no recurrence during follow-up.
bRecurrence rate is the proportion of patients who were cured at EOT and had recurrence during the follow-up period.
Notes: 95% CIs were obtained using the Mantel-Haenszel test.
Source: Mikamo et al.12
Table 7: Key Efficacy Results of Rao et al. Study
Variable | Fidaxomicin (n = 74) | Vancomycin (n = 70) |
|---|---|---|
Clinical cure rate of CDI at EOT (per ITT) | ||
Clinical cure rate, n (%) | 54 (73.0%) | 44 (62.9%) |
P valuea | 0.195 | |
Clinical cure rate of CDI at EOT (per protocol) | ||
Clinical cure rate, n (%) | 54 (84.4%) | 44 (81.5%) |
P valuea | 0.864 | |
Sustained clinical cure (per protocol)b | 52 (86.7%) | 42 (84%) |
P valuea | 0.693 | |
Excluded from per-protocol analysis | 14 | 20 |
Recurrence during follow-up (per protocol) | 2 (3.3%) | 2 (4%) |
P valuea | > 0.99 | |
CDI = Clostridioides difficile infection; EOT = end of treatment; ITT = intention to treat.
aP value calculated with chi-square tests for categorical data.
bSustained clinical cure is clinical cure without recurrence during follow-up.
Source: Rao et al.13
Harms
Detailed results for harms for each included study are in Guery et al.11 and Mikamo et al.12
Harms are presented in Table 8. Key results include:
In the EXTEND11 study, AEs were slightly more frequent for vancomycin compared with fidaxomicin. For the Mikamo et al.12 study, AEs occurred at similar rates in patients receiving fidaxomicin or vancomycin (70%).
Safety was not reported in the Rao et al.13 study.
SAEs were higher in patients treated with vancomycin than in those treated with fidaxomicin.
Grade 3 or higher AEs were similar for both treatment groups in the Mikamo et al.12 study.
A higher percentage of patients withdrew from treatment due to AEs in the fidaxomicin group than in the vancomycin group in both trials, with a difference of about 5% between the treatment groups in each trial.
In the fidaxomicin group in Mikamo et al.,12 AEs leading to treatment discontinuation were ventricular fibrillation (grade 4), duodenal ulcer hemorrhage (grade 3), vomiting (grade 1), general physical health deterioration (grade 3), liver carcinoma rupture (grade 4), delusion (grade 2), and peripheral artery aneurysm (grade 4). In the vancomycin group, AEs leading to treatment discontinuation were pancreatic leak (grade 3).
Fewer deaths related to AEs were reported (range, 1.9% to 2.9%). The rates of death were similar between the treatment groups across both trials.
AE | Guery et al.11 | Mikamo et al.12 | ||
|---|---|---|---|---|
EPFX Fidaxomicin n = 181 | Vancomycin n = 181 | Fidaxomicin n = 104 | Vancomycin n = 108 | |
AEs, n (%) | 121 (67) | 128 (71) | 73 (70.2) | 76 (70.4) |
SAEs, n (%)a | 68 (38) | 78 (43) | 16 (15.4) | 14 (13.0) |
Grade ≥ 3 AEs, n (%) | NR | NR | 24 (23.1)b | 27 (25.1)b |
Discontinuation due to AEs, n (%) | 14 (8) | 5 (3) | 6 (5.8) | 1 (0.9) |
Deaths related to AEs, n (%) | 3 (2) | 3 (2) | 3 (2.9) | 2 (1.9) |
AE by preferred term, n (%)c,d | ||||
Clostridium difficile infection | 7 (4) | 24 (13) | 13 (12.5) | 21 (19.4) |
Urinary tract infection | 6 (3) | 12 (7) | 3 (2.9) | 11 (10.2) |
Constipation | 10 (6) | 5 (3) | 6 (5.8) | 7 (6.5) |
Diarrhea | 10 (6) | 12 (7) | 2 (1.9) | 3 (2.8) |
Pyrexia | 7 (4) | 12 (7) | 5 (4.8) | 6 (5.6) |
Pneumonia | 5 (3) | 10 (6) | NR | NR |
Sepsis | 1 (1) | 9 (5) | NR | NR |
Anemia | 5 (3) | 10 (6) | NR | NR |
Cardiac failure | 4 (2) | 10 (6) | NR | NR |
Delirium | NR | NR | 3 (2.9) | 2 (1.9) |
Hemorrhoids | NR | NR | 3 (2.9) | 2 (1.9) |
Febrile neutropenia | NR | NR | 1 (1.0) | 3 (2.8) |
Hepatic function abnormal | NR | NR | 1 (1.0) | 3 (2.8) |
Liver function test abnormal | NR | NR | 0 | 3 (2.8) |
Skin exfoliation | NR | NR | 3 (2.9) | 1 (0.9) |
Pruritus | NR | NR | 3 (2.9) | 2 (1.9) |
Dermatitis contact | NR | NR | 4 (3.8) | 3 (2.8) |
AE = adverse event; EPFX = extended-pulsed fidaxomicin; NR = not reported; SAE = serious adverse event.
aDefined as AEs resulting in death, or considered to be life-threatening, requiring hospitalization, or resulting in persistent or substantial disability or incapacity, congenital anomaly, or other medically important events.
bData from the total number of grade 3, 4, and 5 AEs reported in Mikamo et al.12 If a patient had multiple AEs, but with differing grades, the patient was counted only once with the highest grade.
cFor the Guery et al.11 study, AEs reported in ≥ 5% of patients in any treatment group.
dFor the Mikamo et al.12 study, AEs reported in ≥ 2% of patients in any treatment group and regardless of relationship to the study drug.
Sources: Guery et al.,11 Mikamo et al.12
Discussion
Efficacy
This review included 3 comparative trials: a phase IIIb-IV open-label RCT (EXTEND in Guery et al.11), a phase III, double-blind RCT (Mikamo et al.12), and a phase IV, open-label RCT (Rao et al.13).
The EXTEND trial demonstrated an improvement in sustained clinical cure of CDI 30 days after EOT among patients that received EPFX compared with those that received vancomycin. The probability of sustained clinical cure of CDI 30 days after EOT was 11% higher in favour of fidaxomicin. The clinical experts indicated that the results for the sustained clinical cure are clinically meaningful. Fidaxomicin resulted in comparable clinical cure of CDI and failed to show superiority compared with vancomycin for this outcome. The results for sustained clinical cure were supported by reduced rate of recurrent CDI assessed at different time points over 90 days. Significantly lower recurrence rates at day 40 (15%), day 55 (14%), and day 90 (13%) were observed for the fidaxomicin treatment group compared to the vancomycin group. Clinical experts expressed that the follow-up time of 90 days was sufficient to measure the sustained clinical cure of CDI.
Evidence from the Mikamo et al.12 study suggests fidaxomicin resulted in comparable global cure (sustained clinical cure) and recurrence rates for CDI. There was insufficient evidence to demonstrate a difference in clinical cure rate, sustained clinical cure, and recurrence rate between fidaxomicin and vancomycin treatment groups in the Rao et al.13 study. The reported efficacy in the Mikamo et al.12 and Rao et al.13 studies were different from those reported in the EXTEND trial. These differences may be related to the patient population. For example, the Rao et al.13 study had a high proportion of individuals with concomitant antibiotic use, comorbidities, cancer, and those who have received a stem cell transplant. These have been found to increase the risk or recurrence.
Harms
In the EXTEND and Mikamo et al.12 trials, the number of patients with any AEs was similar between groups. SAEs and AEs with grades of 3 or more occurred at similar rates in the fidaxomicin and vancomycin groups, where reported. Notably, discontinuation due to AEs was higher among patients treated with fidaxomicin than patients treated with vancomycin. However, the overall frequencies of discontinuation due to AEs were low, 8% in the EXTEND11 study and 5.8% in the Mikamo et al.12 study. Deaths due to AEs occurred at a low rate in the studies, estimated at about 2% to 3%. Treatment groups had a similar proportion of patients dying due to AEs. The clinical experts expressed that the AEs were not surprising and there were no new safety signals from the trials. Overall, the proportion of patients experiencing adverse effects was similar across treatment groups.
Conclusion
The evidence from the EXTEND11 trial show that fidaxomicin may improve sustained clinical cure and reduce recurrence compared with vancomycin in treating adult patients for initial episode or first recurrence of CDI. Evidence from the Mikamo et al.12 and Rao et al.13 studies suggest fidaxomicin resulted in comparable global cure (sustained clinical cure) and recurrence rates for CDI. The safety profile in terms of any AEs, SAEs, and deaths due to AEs was comparable between fidaxomicin and vancomycin treatment groups in the EXTEND11 and Mikamo et al.12 studies. However, harms results suggest higher frequencies of discontinuation due to AEs within the fidaxomicin compared with vancomycin groups. There was no evidence about HRQoL reported in the studies.
Economic Review
The economic review consisted of a cost comparison of fidaxomicin compared with vancomycin for the treatment of adult patients for the initial episode or first recurrence of CDI.
Based on public list prices, fidaxomicin is expected to have a per patient cost of $1,892 per course cost (10 days) for initial episode (Appendix 3, Table 4 in the Supplemental Material) and a per patient cost of $1,892 per course cost (10 or 25 days, depending on dosing regimen) for first recurrence of CDI (Appendix 3, Table 5 in the Supplemental Material). The incremental cost of fidaxomicin compared with vancomycin ranges from $1,602 to $1,685 per patient per course for initial CDI and from $1,348 to $1,685 per patient per course for first CDI recurrence. As such, the reimbursement of fidaxomicin for the treatment of adult patients for the initial episode or first recurrence of CDI is expected to increase overall drug acquisition costs. Additional items for consideration include:
According to the clinical review, fidaxomicin may improve sustained clinical cure and reduce recurrence compared with vancomycin standard dosing, with comparable safety profiles. However, harms results suggest higher frequencies of discontinuation due to AEs with fidaxomicin compared with vancomycin groups. There was no evidence about HRQoL reported in the studies. The results are reported for the combined population, which makes interpretation of the efficacy results based on the number of previous CDI occurrences difficult. No evidence was identified for fidaxomicin versus vancomycin taper pulse for first recurrence in the literature.
As of April 8, 2025, fidaxomicin is only available as a brand name product in Canada. No generics are currently under review at Health Canada (Table 1).
No health care resource use outcomes were reported in the clinical trial.14
Fidaxomicin was reviewed by CADTH in 2012, and received a Do Not List recommendation.15
Fidaxomicin was re-evaluated by INESSS in 2022 and received positive recommendation.1
Fidaxomicin underwent negotiations with pan-Canadian Pharmaceutical Alliance that concluded on September 14, 2023, and with a letter of intent.16
No cost-effectiveness studies set in Canada were identified for the initial CDI episode. A cost-effectiveness study set in Canada was identified that included the comparison of fidaxomicin and vancomycin for patients diagnosed with recurrent CDI based on a literature search conducted on April 7, 2025. The identified literature compared fidaxomicin with standard vancomycin for the treatment of first CDI recurrence. This comparison was consistent with the evidence summarized in the clinical review (i.e., fidaxomicin versus vancomycin standard for the treatment of first recurrence of CDI). Additional information regarding this literature has been summarized in the Other Economic Evidence section of Appendix 3 in the Supplemental Material.
Conclusion
The reimbursement of fidaxomicin for the treatment of the initial episode or first recurrence of CDI in adult patients is expected to increase overall drug acquisition costs compared with vancomycin-based regimens. Based on the clinical review conclusions, fidaxomicin may improve sustained clinical cure and reduce recurrence compared with vancomycin. The clinical review highlighted that the safety profile in terms of AEs, SAEs, and deaths due to AEs was comparable with vancomycin.
Given that fidaxomicin is associated with increased drug acquisition costs and incremental benefit in terms of sustained clinical cure and reducing recurrence, a cost-effectiveness analysis would be required to determine the cost-effectiveness of fidaxomicin relative to vancomycin. A cost-effectiveness study from Canada was identified for those with recurrent CDI,17 which compared fidaxomicin with vancomycin standard dosing. Based on the included cost-effectiveness study, fidaxomicin may represent a cost-effective alternative to the vancomycin standard regimen for the treatment of recurrent CDI, but some generalizability concerns exist. The cost-effectiveness of fidaxomicin relative to vancomycin pulse-taper regimen for first recurrence, and the cost-effectiveness of fidaxomicin relative to vancomycin standard regimen for initial CDI, is unknown in the absence of evidence.
References
1.Institut national d'excellence en santé et services sociaux (INESSS). Dificid (infection à Clostridium difficile). 2022. Accessed April 11, 2025. https://www.inesss.qc.ca/en/themes/medicaments/drug-products-undergoing-evaluation-and-evaluated/extract-notice-to-the-minister/dificid-infection-a-clostridium-difficile-6361.html
2.Balsells E, Shi T, Leese C, et al. Global burden of Clostridium difficile infections: a systematic review and meta-analysis. J Glob Health. 2019;9(1):010407. doi:10.7189/jogh.09.010407 PubMed
3.Du T, Choi KB, Silva A, et al. Characterization of Healthcare-Associated and Community-Associated Clostridioides difficile Infections among Adults, Canada, 2015-2019. Emerg Infect Dis. 2022;28(6):1128-1136. doi:10.3201/eid2806.212262 PubMed
4.Levy AR, Szabo SM, Lozano-Ortega G, et al. Incidence and Costs of Clostridium difficile Infections in Canada. Open Forum Infect Dis. 2015;2(3):ofv076. doi:10.1093/ofid/ofv076 PubMed
5.Healthcare-associated infections and antimicrobial resistance in Canadian acute care hospitals, 2018-2022. Can Commun Dis Rep. 2024;50(6):179-196. doi:10.14745/ccdr.v50i06a02 PubMed
6.Lamont JT, Kelly CP, Bakken JS. Clostridioides difficile infection in adults: Clinical manifestations and diagnosis. UpToDate; 2024. Accessed December 10, 2024. www.uptodate.com
7.Lamont JT, Kelly CP, Bakken JS. Clostridioides difficile infection in adults: Epidemiology, microbiology, and pathophysiology. UpToDate; 2024. Accessed December 10, 2024. www.uptodate.com
8.Loo V, Davis I, Embil J, et al. Association of Medical Microbiology and Infectious Disease Canada treatment practice guidelines for Clostridium difficile infection. JAMMI. 2018;3:71-92. doi:10.3138/jammi.2018.02.13
9.Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin Infect Dis. 2021;73(5):e1029-e1044. doi:10.1093/cid/ciab549 PubMed
10.Poisson C. Guide d'usage optimal pour le traitement de la diarrhée ou de la colite associée à Clostridium difficile. Institut national d'excellence en santé et services sociaux (INESSS). 2025. Accessed April 11, 2025. https://www.inesss.qc.ca/publications/repertoire-des-publications/publication/guide-dusage-optimal-pour-le-traitement-de-la-diarrhee-ou-de-la-colite-associee-a-clostridium-difficile.html
11.Guery B, Menichetti F, Anttila VJ, et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis. 2018;18(3):296-307. doi:10.1016/S1473-3099(17)30751-X PubMed
12.Mikamo H, Tateda K, Yanagihara K, et al. Efficacy and safety of fidaxomicin for the treatment of Clostridioides (Clostridium) difficile infection in a randomized, double-blind, comparative Phase III study in Japan. J Infect Chemother. 2018;24(9):744-752. doi:10.1016/j.jiac.2018.05.010 PubMed
13.Rao K, Zhao Q, Bell J, et al. An Open-Label, Randomized Trial Comparing Fidaxomicin With Oral Vancomycin for the Treatment of Clostridioides difficile Infection in Hospitalized Patients Receiving Concomitant Antibiotics for Concurrent Infections. Clin Infect Dis. 2024;78(2):277-282. doi:10.1093/cid/ciad606 PubMed
14.Gerding DN, Hecht DW, Louie T, et al. Susceptibility of Clostridium difficile isolates from a Phase 2 clinical trial of cadazolid and vancomycin in C. difficile infection. J Antimicrob Chemother. 2016;71(1):213-9. doi:10.1093/jac/dkv300 PubMed
15.CADTH. CADTH Canadian Drug Expert Committee (CDEC) final recommendation: fidaxomicin (Dificid – Optimer Pharmaceuticals Canada Inc.). December 19, 2012. Accessed April 7, 2025. https://www.cda-amc.ca/fidaxomicin
16.pan-Canadian Pharmaceutical Alliance. Dificid (fidaxomicin) file number 22141. 2023. Accessed April 11, 2025. https://www.pcpacanada.ca/negotiation/22141
17.Lapointe-Shaw L, Tran KL, Coyte PC, et al. Cost-Effectiveness Analysis of Six Strategies to Treat Recurrent Clostridium difficile Infection. PLoS One. 2016;11(2):e0149521. doi:10.1371/journal.pone.0149521 PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.