Drugs, Health Technologies, Health Systems
Reimbursement Review
Evolocumab
Requester: Public drug programs
Therapeutic area: Dyslipidemia and lipid disorders
Summary
What Is Homozygous Familial Hypercholesterolemia?
Homozygous familial hypercholesterolemia (HoFH) is a rare and life-threatening genetic disorder characterized by defects in the low-density lipoprotein (LDL) receptor–mediated clearance of low-density lipoprotein cholesterol (LDL-C). HoFH manifests as extreme elevations in LDL-C with untreated levels typically exceeding 10 mmol/L, which predisposes patients to accelerated atherosclerotic cardiovascular disease and premature mortality, often as early as childhood or young adulthood. Other clinical manifestations of HoFH may include tendon or cutaneous xanthomas and premature atherosclerosis.
HoFH is generally estimated to occur in approximately 1 in 300,000 to 1 in 400,000 individuals worldwide from 2014 to 2024. In Canada, 38 to 100 cases are estimated based on the overall population of 38,000,000 in 2018 to 2019. Quebec was reported to have a higher prevalence of HoFH due to founder effects.
Genetic testing for HoFH comprises assessing for mutations in the LDLR, APOB, PCSK9, and LDLRAP1 genes. In Canada, genetic confirmation of HoFH can complement clinical diagnosis; however, availability is variable across the country. Due to the rarity of the disease and the likelihood that many existing patients may already have undergone genetic testing, minimal health system impacts are anticipated from a testing perspective to establish eligibility for treatment with evolocumab.
What Are the Treatment Goals and Current Treatment Options for HoFH?
Treatment goals for HoFH include reducing LDL-C as much and as early as possible to delay or prevent premature cardiovascular events and improve long-term survival.
Standard therapy includes high-intensity statins and ezetimibe, but these are often insufficient for most patients with HoFH. Lipoprotein apheresis is effective but burdensome, requiring frequent procedures, specialized centres, and vascular access.
Additional lipid-lowering therapies may be used. Alirocumab can be effective in patients with HoFH and residual LDL receptor activity. Evinacumab, lomitapide, and mipomersen are potent lipid-lowering therapies specifically indicated for the treatment of HoFH, but their use may be limited by variable efficacy (i.e., depending on specific gene mutation), safety concerns, high cost, and restricted availability.
What Is Evolocumab and Why Did Canada’s Drug Agency Conduct This Review?
Evolocumab is a proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor that is administered by subcutaneous injection. Health Canada has approved evolocumab as an adjunct to diet and other LDL-C–lowering therapies (e.g., statins, ezetimibe) in patients aged 10 years and older with HoFH who require additional lowering of LDL-C.
At the request of the participating public drug programs, Canada’s Drug Agency (CDA-AMC) reviewed evolocumab to inform a recommendation on whether it should be reimbursed for HoFH.
How Did CDA-AMC Evaluate Evolocumab?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects of evolocumab and compared the costs of evolocumab versus other treatments used in Canada for HoFH. Background therapy (e.g., statins or ezetimibe) alone or with placebo as well as background therapy combined with evinacumab, alirocumab, or lomitapide were considered relevant treatments to compare with evolocumab when added to background therapy.
The clinical evidence was identified through systematic searches for available studies.
CDA-AMC identified equity and ethical considerations relevant to evolocumab and HoFH.
The review was also informed by 1 clinician group submission and 1 industry submission in response to our call for input, and by input from the participating public drug programs regarding issues that may impact their ability to implement a recommendation.
One endocrinologist and 2 cardiologists (1 adult and 1 pediatric cardiologist) were consulted as part of the review process.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
one randomized controlled phase III trial (the TESLA Part B trial) comparing evolocumab with placebo in 50 patients aged 13 to 57 years with HoFH
three reports addressing evidence gaps in the included trial.
The TESLA Part B trial demonstrated that evolocumab significantly reduced LDL-C levels by 30.9% more than placebo at 12 weeks in patients with HoFH on stable background therapy (moderate certainty). This reduction was clinically meaningful.
LDL-C reductions were greatest in patients with at least 1 LDL receptor allele exhibiting defective function. Patients with 2 null alleles in the LDLR gene, resulting in little to not functional LDL receptor activity, showed minimal or no response. However, the observed subgroup effects were considered as having low or very low credibility.
Evolocumab reduces apolipoprotein B levels compared with placebo in patients with HoFH (moderate certainty).
This trial did not report cardiovascular outcomes or health-related quality of life.
Evolocumab can be described as well tolerated in the TESLA Part B trial, with no serious treatment-related adverse events, but the certainty of the evidence is very low due to the small sample size and the short duration of the study.
In the open-label, single-arm TAUSSIG study, evolocumab demonstrated an acceptable safety profile over a median of 4.1 years, with a cardiovascular event rate of 2.7% per patient-year in the overall study population, which included adult patients with HoFH (35% of participants) and severe heterozygous hypercholesterolemia.
The pooled analysis of 3 open-label studies in adolescents (aged 10 to 17 years) showed evolocumab was well tolerated, with no new safety signals. Residual LDL receptor activity did not reliably predict response.
One report on 2 case reports in children younger than 10 years reported LDL-C reductions of approximately 30% with good tolerability. However, this is insufficient evidence to support routine use in patients younger than 10 years. No comparative or long-term evidence exists for this population.
No studies were identified that compared the efficacy and safety of evolocumab with other relevant comparators (e.g., evinacumab, alirocumab, lomitapide) in this patient population.
Economic Evidence
Reimbursing evolocumab for HoFH can reduce costs to the public drug programs with an unknown impact on clinical outcomes.
Abbreviations
AE
adverse event
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HoFH
homozygous familial hypercholesterolemia
HRQoL
health-related quality of life
LDL
low-density lipoprotein
LDL-C
low-density lipoprotein cholesterol
MACE
major adverse cardiovascular event
PCSK9
proprotein convertase subtilisin/kexin type 9
RCT
randomized controlled trial
SAE
serious adverse event
TEAE
treatment-emergent adverse event
Background
Introduction
The objective of the Clinical Review is to review and critically appraise the evidence on the beneficial and harmful effects of evolocumab as an adjunctive therapy to lifestyle intervention and other low-density lipoprotein (LDL)–lowering therapies (background therapy) in patients aged 10 years and older with homozygous familial hypercholesterolemia (HoFH) who require additional lowering of low-density lipoprotein cholesterol (LDL-C). The review focuses on comparing evolocumab to relevant comparators in clinical practice in Canada and identifying gaps in the current evidence. The Economic Review consists of a cost comparison for evolocumab compared with relevant comparators for the same population. The comparators considered relevant to the reviews were background therapy only and background therapy with adjunctive therapy.
Table 1: Information on the Drug Under Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the drug under review | |
Drug | Evolocumab, 140 mg in 1.0 mL (140 mg/mL), 420 mg in 3.5 mL (120 mg/mL), solution for injection, subcutaneous injection |
Relevant Health Canada indication | Evolocumab is indicated as an adjunct to diet and other LDL-C–lowering therapies (e.g., statins, ezetimibe, LDL apheresis) in adult and pediatric patients aged 10 years and older with HoFH who require additional lowering of LDL-C. |
Mechanism of action | Evolocumab is a fully human monoclonal immunoglobulin G2 that binds selectively and with high affinity to PCSK9 and inhibits circulating PCSK9 from binding to LDL receptors on the surface of liver cells, thus preventing PCSK9-mediated LDL receptor degradation. This increases the number of LDL receptors available to clear LDL, thereby lowering serum LDL-C levels. |
Recommended dosage | The initial recommended dosage is 420 mg once monthly. After 12 weeks of treatment, dose frequency can be uptitrated to 420 mg once every 2 weeks if a clinically meaningful response is not achieved. Patients undergoing apheresis may initiate treatment with 420 mg every 2 weeks to correspond with their apheresis schedule. |
Data protection status | March 10, 2024 |
Status of generic drugs or biosimilars | There are currently no biosimilars under review or approved by Health Canada. |
Information on the CDA-AMC review | |
Requester | Formulary Working Group |
Indication under consideration for reimbursement | Adult and pediatric patients aged 10 years and older with HoFH who require additional lowering of LDL-C (i.e., in addition to diet and other LDL-lowering therapies, such as statins, ezetimibe, or LDL apheresis) |
CDA-AMC = Canada’s Drug Agency; HoFH = homozygous familial hypercholesterolemia LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; LDLR = low-density lipoprotein receptor; PCSK9 = proprotein convertase subtilisin/kexin type 9.
Source: Repatha product monograph.1
Context for the Review
A review of the evidence for evolocumab in patients with HoFH was requested by the Formulary Working Group. Evolocumab is indicated by Health Canada as an adjunct to diet and other LDL-lowering therapies (e.g., statins, ezetimibe, LDL apheresis) in adult and pediatric patients aged 10 years and older with HoFH who require additional lowering of LDL-C. The indication aligns with the request for the Reimbursement Review of evolocumab in adult and pediatric patients aged 10 years and older with HoFH who require additional lowering of LDL-C (i.e., in addition to diet and other LDL-lowering therapies such as statins, ezetimibe, or LDL apheresis).
Submission History for the Drug Under Review
CDA-AMC previously reviewed evolocumab for the treatment of:
primary hyperlipidemia and mixed dyslipidemia in adult patients (final recommendation: reimburse with clinical criteria and/or conditions in adult patients with confirmed heterozygous familial hypercholesterolemia [HeFH], issued on February 19, 2016)
primary hyperlipidemia and mixed dyslipidemia (final recommendation: reimburse with clinical criteria and/or conditions in adult patients for clinical atherosclerotic cardiovascular disease, issued on November 22, 2017)
elevated LDL-C in adult patients with primary hyperlipidemia (final recommendation: reimburse with clinical criteria and/or conditions in adult patients with primary hyperlipidemia, including HeFH and atherosclerotic cardiovascular disease, issued on August 8, 2024).
Sources of Information
The contents of the Clinical Review are informed by studies identified through systematic literature searches, input received from interested parties (a clinician group, drug programs, and industry), and input from 3 clinical experts consulted for this review.
Calls for patient group, clinician group, and industry input are issued for each Non-Sponsored Reimbursement Review. The following submissions were received: 1 clinician group submission from the Canadian Cardiovascular Society and 1 submission from industry (Amgen Canada Inc.). The Canadian Cardiovascular Society gathered input by circulating a draft submission to experts in diverse areas of cardiovascular care and incorporating their evidence-informed feedback through a consensus-based approach. There were no submissions from patient groups. The full submissions received are available on the project landing page) in the consolidated input document.
Input from the clinician group and clinical experts is considered throughout the review, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical evidence. Relevant clinician group input and industry input are summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
The drug programs provide input on each drug being reviewed through the Reimbursement Review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions from the public drug programs and corresponding responses from the clinical experts consulted for this review are summarized in the Summary of Drug Program Input and Clinical Expert Responses table in Appendix 1 of the Supplemental Material document available on the project landing page.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. One endocrinologist and 2 cardiologists (1 adult and 1 pediatric cardiologist) with expertise in the diagnosis and management of HoFH participated as part of the review team, with representation from Ontario and the Prairies.
Disease Background
HoFH is a rare and life-threatening genetic disorder characterized by defects in the catabolism of LDL-C.2,3 These defects are driven by mutations in genes essential to the LDL receptor pathway, leading to a critical reduction in LDL receptor function. Clinically, the disease manifests as extreme elevations in LDL-C, with untreated levels typically exceeding 10 mmol/L, which predisposes patients to accelerated atherosclerotic cardiovascular disease, often as early as childhood or young adulthood, and premature mortality.2,3 Other clinical manifestations of HoFH may include tendon or cutaneous xanthomas.2,3 Although precise epidemiologic data are limited, HoFH is generally estimated to occur in approximately 1 in 300,000 to 1 in 400,000 individuals worldwide from 2014 to 2024.2 In Canada, 38 to 100 cases are estimated based on the overall population of 38,000,000 in 2018 to 2019.4 Quebec was reported to have a higher prevalence of HoFH in 2023 due to founder effects.4 Among 48 patients enrolled in a HoFH registry in Canada, the median age at diagnosis was 12 years (interquartile range, 5 to 24 years), and the median untreated LDL-C level was 15.0 mmol/L (interquartile range, 10.5 mmol/L to 18.6 mmol/L).4
The genetic etiology of HoFH is predominantly linked to mutations in the LDLR gene, which accounts for more than 90% to 95% of cases. This is followed by mutations in the APOB gene (less than 4%), and the PCSK9 gene (less than 0.5%).2,3 HoFH can be categorized by mutational status into true homozygotes or compound heterozygotes; however, patients in these groups are generally managed using similarly intensive lipid-lowering protocols.5 The degree of residual LDL receptor function serves as a critical prognostic indicator. Accordingly, HoFH is commonly classified as LDL receptor negative (< 2% residual activity) or LDL receptor defective (2% to 25% residual activity), with receptor status correlating with the severity of hypercholesterolemia and cardiovascular disease risk.5 Patients with HoFH are considered to be at very high risk of atherosclerotic cardiovascular disease.6
Current Management
Treatment Goals
According to the Canadian Cardiovascular Society, the current treatments for HoFH do not correct the underlying genetic defect but reduce poor outcomes by lowering circulating LDL-C and preventing cardiovascular events. The primary goal of treating HoFH is to achieve long-term reduction in cardiovascular morbidity and mortality. In routine clinical practice, clinically meaningful reductions in LDL-C as early as possible are considered an appropriate surrogate for treatment efficacy to slow the disease progression and reduce the need for LDL apheresis and, in rare cases, liver transplantation. The clinician group indicated that the best treatment would lower LDL-C levels significantly and reduce atherosclerotic cardiovascular disease risk, with benefits that can be sustained for a long time, regardless of LDL receptor status. Reducing treatment-related side effects and improving patients’ health-related quality of life (HRQoL) are also important. The clinician group indicated that patients and caregivers often value meaningful benefits from fewer invasive procedures, avoidance of significant side effects, reduced psychological burden, better daily functioning and quality of life, and fewer disruptions to school, work, and family life.
Current Treatment Options
According to the Canadian Cardiovascular Society, the standard of care in Canada is to refer patients with HoFH to specialized lipid centres for comprehensive evaluation and management. The current treatments combine nonpharmacological and pharmacological interventions, with a strong emphasis on early diagnosis and aggressive lipid-lowering.
Nonpharmacological managements include lifestyle interventions, LDL apheresis, and liver transplantation. Lifestyle interventions, such as a heart-healthy diet, physical activity, weight optimization, stress reduction, and smoking cessation, are recommended for all patients with HoFH, including children and adolescents, but their impact on LDL-C is limited. LDL apheresis or plasmapheresis is an invasive and frequent (every 1 to 2 weeks) intervention and is considered when LDL-C remains uncontrolled on drug therapy. In Canada, LDL apheresis, or plasmapheresis, is limited to a few centres. It also imposes a substantial physical, psychological, and economic burden on patients with HoFH and their families and on health systems. Most patients with HoFH in Canada do not have access to LDL apheresis or plasmapheresis. For extremely severe cases of HoFH, liver transplantation may be considered.
Due to the disease severity, most patients received multiple agents in parallel, and the pharmacological interventions typically involve combination therapy. According to the clinician group, statins, ezetimibe, and PCSK9 monoclonal antibodies (e.g., evolocumab and alirocumab) are considered standard lipid-lowering therapy for patients with HoFH and are widely used in Canada. Evolocumab is administered by subcutaneous injection and is indicated as an adjunct to diet and other LDL-C–lowering therapies in patients aged 10 years and older with HoFH who require additional LDL-C lowering. Evinacumab or lomitapide may be offered as the advanced lipid-lowering therapy when LDL-C is not adequately controlled with standard lipid-lowering therapy, with or without LDL apheresis or plasmapheresis. Other lipid-lowering agent options may include bempedoic acid, apolipoprotein B antisense strategies, and fibrates.
Unmet Needs and Existing Challenges
Despite meaningful progress in the management of HoFH, the Canadian Cardiovascular Society emphasizes that substantial unmet needs persist regarding effectiveness, safety, and accessibility. The clinician group noted that the available treatments do not address the fundamental gene mutation in HoFH, and most treatments rely on LDL receptor activity. Many patients have LDL receptor function that is markedly impaired or absent; and most have LDL-C levels that remain higher than guideline-recommended targets (e.g., 1.8 mmol/L) even when treated with maximally tolerated statins, ezetimibe, or PCSK9 monoclonal antibodies, highlighting a persistent gap in treatment effectiveness and long-term cardiovascular risk reduction. For patients with reluctance to use statins or with concomitant elevations of lipoprotein(a), evolocumab may be more important to fill unmet needs.
The clinician group further indicated that patients continue to experience severe atherosclerotic cardiovascular disease, often in childhood or early adulthood, underscoring that therapies lower LDL-C but do not fully address long-term outcomes and the need for effective therapies that can be initiated early and sustained long term. This aligns with the industry input, which also stressed the heterogeneity of responses to LDL receptor–dependent therapies, with particularly limited benefit in patients with minimal or no residual LDL receptor activity.
Safety and tolerability limitations also contribute to unmet needs. Lomitapide is an LDL receptor-independent lipid-lowering agent, but it is difficult for many patients to maintain due to gastrointestinal adverse effects and liver enzyme elevations, limiting its real-world implementation. Significant challenges also arise from inequitable access to specialized services. LDL apheresis, although sometimes clinically necessary, is available only in a small number of highly specialized centres in Canada. Therefore, most families cannot consistently access it. For patients who can access it, they often must travel long distances every 1 to 2 weeks for an invasive and time-intensive procedure, resulting in substantial physical, psychological, financial, and logistical burden. This disproportionately affects patients in rural or remote regions, in regions without specialized lipid clinics, or those who lack the resources to travel regularly.
The clinical experts consulted for this review pointed out that there remains an unmet need for affordable, well tolerated, and effective therapies that provide consistent LDL-C reduction and demonstrate cardiovascular benefit in the HoFH population. The management of HoFH remains challenging due to substantial variability in LDL-C lowering among available therapies and a strong dependence on residual LDL receptor activity. Maximally tolerated statins and ezetimibe provide only modest LDL-C reductions, and the efficacy of PCSK9 inhibitors is limited to patients with residual LDL receptor function. Some lipid-lowering agents, such as PCSK9 inhibitors, lomitapide, and evinacumab, offer greater LDL-C lowering, but their use is limited by treatment burden, safety considerations, or high cost. There is a lack of robust evidence on cardiovascular outcomes, affecting the certainty about their long-term clinical benefit.
Considerations for Using the Drug Under Review
Place in Therapy
The Canadian Cardiovascular Society indicated that evolocumab is already established as an adjunctive lipid-lowering treatment for patients with HoFH in Canada and it is generally considered a key component of early combination therapy. The input indicated that evolocumab is often initiated after inadequate LDL-C reduction with statins and ezetimibe. The clinician group also emphasized that evolocumab is commonly used as part of combination therapy rather than as monotherapy and plays a key role in helping patients achieve LDL-C targets. Even with the addition of evolocumab to other lipid-lowering therapies, some patients with HoFH still cannot achieve the LDL-C targets outlined in clinical practice guidelines.
The clinical experts aligned with the clinician group and noted that evolocumab currently fits within a stepwise treatment approach for HoFH in clinical practice in Canada. The clinical experts indicated that evolocumab is usually added early on as part of the combination therapy, especially in people with partial LDL receptor function. Evolocumab is typically given with the maximally tolerated statin and ezetimibe. In some cases, it is also given with LDL apheresis or plasmapheresis to lower LDL-C levels in patients with HoFH.
Patient Population
The clinician group indicated that the patients with HoFH who will get the most benefit from evolocumab are those who still have some LDL receptor activity. This is because evolocumab works by increasing the number of LDL receptors on the cell surface. In routine clinical practice, it is typically not possible to estimate the level of residual LDL receptor activation.
The clinical experts aligned with the clinician group regarding the relevant patient population and noted that the most suitable candidates for treatment with evolocumab are patients with residual LDL receptor function who require aggressive LDL-C reduction despite maximally tolerated lipid-lowering therapy (e.g., statins with or without ezetimibe) or who are unable to tolerate adequate statin therapy. Identification of eligible patients is based on combined clinician judgment and laboratory assessment, particularly persistently elevated LDL-C levels, with diagnosis informed by clinical features and established criteria rather than mandatory genetic testing. Evolocumab is not expected to be effective in HoFH patients with null LDL receptor function. Patients who achieve LDL-C targets with statins and ezetimibe alone, those unwilling to use subcutaneous injections, or individuals with contraindications to monoclonal antibody therapy are not appropriate candidates for evolocumab.
Testing Procedure Considerations
HoFH is an umbrella term for a variety of genotypes.7 The most commonly encountered mutations are 2 identical or 2 different variants in the LDLR gene.4,7-9 Less frequently, HoFH can be caused by single-gene variants in the APOB or PCSK9 genes, variants in the 2 separate genes, or by a recessive mutation in the LDLRAP1 gene.4,7-9 Genetic confirmation of HoFH is typically done by next-generation sequencing using targeted panels for a minimum of the LDLR, APOB, PCSK9, and LDLRAP1 genes.10-16 Other genes may be included on the panel (e.g., ABCG5, ABCG8, LIPA) to rule out other rare, but clinically similar, hereditary dyslipidemias.10,15
Guidelines from Canada recommend genetic testing as a complement to clinical diagnosis in familial hypercholesterolemia patients.8 International guidelines recommend genetic confirmation in the HoFH population, but also state that treatment should be based on phenotype (e.g., LDL-C levels).7,9 According to the clinical experts consulted for this review, HoFH can be diagnosed before the age of 10 years based on clinical presentation and family history alone, so genetic confirmation is not necessary. According to the clinical experts, the value of genetic testing lies in validating the clinical diagnosis and prompting cascade testing in family members. They mentioned that genetic testing could also be helpful to predict response to PCSK9 inhibitors (e.g., through the detection of 1 or more LDLR null mutations), although treatment efficacy would be apparent through the standard-of-care monitoring of LDL-C levels. However, relying on a genetic confirmation of diagnosis before initiating treatment could potentially delay the onset of the optimal course of treatment. In addition, some individuals may be unwilling or unable to access genetic testing. These patients, who could otherwise be diagnosed with HoFH based on clinical symptoms, risk being ineligible for optimal treatment, including access to later lines of therapy or future, more potent cholesterol-lowering drugs if PCSK9-inhibitor therapy was limited to only those with genetic confirmation.
The availability and funding of genetic testing for HoFH is variable across Canada.8,17 In some jurisdictions, testing is available through research avenues only, whereas in other jurisdictions, testing is routinely offered through specialty lipid clinics and is publicly funded.10-17 The clinical experts commented that many existing patients with HoFH already have genetic results available.
The potential impacts of genetic testing were considered to ascertain eligibility for evolocumab for HoFH, including those to health systems, patients (including families and caregivers), and costs. Because genetic testing is not necessary to confirm the diagnosis of HoFH, minimal health system impacts are anticipated from a testing perspective if evolocumab were to be reimbursed in this population. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team when possible and are summarized in the Supplemental Material document (available on the project landing page) in Appendix 2.
Assessing the Response to Treatment
The Canadian Cardiovascular Society indicated that the magnitude of LDL-C reduction was generally used to assess the response to evolocumab treatment, typically calculated as the percentage change from baseline after approximately 12 weeks of treatment. Clinically meaningful response in this population is often considered to be an LDL-C reduction of 15% or greater. A reduction of less than 15% is typically classified as a nonresponse and patients may be considered for treatment discontinuation. Both clinical trials and routine practice rely on LDL-C reduction as the principal outcome measure, although additional factors are also considered, such as tolerability, safety, and the potential to reduce the frequency of LDL apheresis. In some cases, clinicians may assess achievement of guideline-recommended LDL-C targets (e.g., < 1.8 mmol/L), noting that these targets may not be attainable for many patients. Improvements in cardiovascular outcomes or symptom stabilization are clinically meaningful but represent long-term end points and are not routinely used for early response assessment.
The clinical experts agreed with the clinician group input and noted that the primary goal of treatment is long-term reduction in atherosclerotic cardiovascular disease events and mortality; however, clinically meaningful reductions in LDL-C are considered an appropriate surrogate for treatment efficacy in routine clinical practice. Achievement of guideline-recommended LDL-C targets (e.g., < 1.8 mmol/L), or reductions in apolipoprotein B (ApoB), are used to assess response and are associated, based on broader lipid-lowering evidence, with reduced rates of angina, nonfatal myocardial infarction, need for revascularization, and stroke. According to the clinical experts, treatment response should be assessed initially within 4 to 12 weeks of therapy initiation, reassessed at approximately 3 months, and monitored annually thereafter. Safety and tolerability should also be assessed, such as injection-site reactions and hypersensitivity events.
Discontinuing Treatment
The Canadian Cardiovascular Society indicates that discontinuation of evolocumab in patients with HoFH should be considered when clinical efficacy is lacking, adverse events (AEs) occur, or the treatment burden is high. The most common reason for discontinuation is inadequate LDL-C reduction; patients whose LDL-C does not achieve a clinically meaningful reduction of at least 15% from baseline after 4 to 12 weeks of therapy should be re-evaluated, and continuation of evolocumab should be reconsidered in the context of alternative or additional lipid-lowering therapies. Although evolocumab is generally well tolerated, discontinuation may also be considered in cases of severe or persistent AEs, such as injection-site reactions or hypersensitivity. Patient preference and treatment burden may also contribute to discontinuation decisions. The clinical experts agreed with these points and indicated that discontinuation of evolocumab should be considered in patients who are pregnant or breastfeeding a child.
Prescribing Considerations
Guidance from the Canadian Cardiovascular Society and expert consensus indicate that the diagnosis and initial management of HoFH typically require specialist expertise (e.g., lipid specialist or cardiologist) due to the complexity of the disease. In specialized settings, multidisciplinary teams can oversee complex lipid management; coordinate additional interventions, such as LDL apheresis; and collaborate with other physicians (e.g., primary care providers) over the longer term. Evolocumab is typically initiated in specialized clinics with involvement from lipid specialists or cardiologists for patients with HoFH. Follow-up may occur in primary care settings with continued monitoring by the specialty clinic.
The clinical experts aligned with the clinician group and noted that treatment initiation and guidance are often provided by specialists, and ongoing monitoring does not necessarily require specialist involvement. Follow-up and routine monitoring can be undertaken in primary care settings, provided that family physicians receive appropriate instructions from the treating specialist. Evolocumab is administered by subcutaneous injection either biweekly or monthly; no specific clinical setting is required. Evolocumab may be administered in specialty lipid clinics, primary care, or specialist clinics, or self-administered by patients at home following appropriate counselling and training, typically provided by a nurse or pharmacist, depending on patient preference and local practice.
Clinical Review
Methods
The review team conducted a systematic review to identify evidence for evolocumab for the treatment of patients with HoFH. Studies were selected according to the eligibility criteria in Table 2. Long-term extension studies of included RCTs, indirect treatment comparisons that adhered to the eligibility criteria (except for the study design criteria), and studies addressing gaps that did not meet the eligibility criteria but were considered to address important gaps in the systematic review evidence were included. Because direct evidence was lacking versus background therapy with active comparators, a search for indirect treatment comparisons was also conducted.
Relevant comparators included treatments used in clinical practice in Canada in the patient population under review. Clinical expert input and patient and clinician group input were considered when selecting outcomes (and follow-up times) for review. Selected outcomes are those considered relevant to expert committee deliberations. Detailed methods for the literature searches, study selection, data extraction, risk of bias appraisal, and assessment of certainty are in the Supplemental Material document (available on the project landing page) in Appendix 3.
Table 2: Systematic Review Eligibility Criteria
Criteria | Description |
|---|---|
Population | Adult and pediatric patients with HoFH who require additional lowering of LDL-C (i.e., in addition to lifestyle intervention and other LDL-lowering therapies)a Subgroups: LDLR defective vs. LDLR negative |
Intervention |
|
Comparator |
|
Outcomes | Efficacy:
Safety:
|
Study design | Phase II, III, and IV RCTs |
AE = adverse event; HoFH = homozygous familial hypercholesterolemia; HRQoL = health-related quality of life; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; RCT = randomized controlled trial; SAE = serious adverse event.
aOther LDL-lowering therapies and background therapy may include statins, ezetimibe, or LDL apheresis.
The review team selected important outcomes to assess the certainty of evidence in this review based on the clinical expert and clinician group input. Included outcomes are those considered relevant to expert committee deliberations, and they were selected in consultation with committee members. Evidence from the systematic review for the most important outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Based on the treatment goals for HoFH, all outcomes of interest were selected for GRADE assessment.
Methods for data extraction, risk of bias appraisal, and certainty of evidence assessment are in the Supplemental Material document in Appendix 3.
Clinical Evidence
An information specialist conducted a literature search of key bibliographic databases, trial registries, and grey literature sources, using a peer-reviewed search strategy. The initial search was completed on December 16, 2025, with alerts maintained until the Formulary Management Expert Committee (FMEC) meeting on June 5, 2026. Refer to Appendix 3 in the Supplemental Material document for detailed search strategies. From the search for primary studies, the review team identified 921 unique records via the searches of databases and registers, of which 864 were excluded by title and abstract. The review team screened 57 records by full text and included 1 report of 1 study (TESLA Part B).18
From the search for indirect treatment comparisons, the review team identified 52 unique records via the searches of databases, of which 47 were excluded by title and abstract. The review team screened 5 records by full text and excluded all the reports due to the wrong patient population. Three studies addressing potential gaps in the included trial evidence were identified.19-21
A list of excluded studies, including reasons for exclusion, is in the Supplemental Material document in Appendix 3.
Systematic Review
Description of Studies
Study Characteristics
Details regarding the study design, inclusion criteria, intervention and comparator, and relevant outcome measures of the included trial are presented in Table 3.
The primary objective of the TESLA Part B trial was to evaluate the efficacy and safety of evolocumab compared with placebo in reducing LDL cholesterol in patients with HoFH.18 The primary efficacy end point was the percentage change from baseline in ultracentrifugation-measured LDL-C at week 12. The relevant secondary end points were absolute change in LDL-C at week 12 and at the mean of weeks 6 and 12, percentage change in LDL-C at the mean of weeks 6 and 12, and absolute and percentage changes from baseline in LDL-C in apolipoprotein B at week 12 and at the mean of weeks 6 and 12. The exploratory end points (e.g., inflammatory markers, treatment response) were not relevant to this review. Safety outcomes were also reported and are relevant to this review.
Table 3: Characteristics of the Included Randomized Controlled Trial
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparator | Relevant end points |
|---|---|---|---|---|
TESLA Part B18 Study design: multicentre, phase III, double-blind, placebo-controlled RCT Total N = 50 |
|
| Intervention: Evolocumab 420 mg, administered subcutaneously every 4 weeks (at weeks 0, 4, and 8), in addition to stable background lipid-lowering therapy. Comparator: Matching placebo administered subcutaneously every 4 weeks for 12 weeks, plus the same background lipid-lowering therapy. | Efficacy:
Safety:
|
AE = adverse event; HoFH = homozygous familial hypercholesterolemia; LDL-C = low-density lipoprotein cholesterol; RCT = randomized controlled trial; SAE = serious adverse event, TEAE = treatment-emergent adverse event.
Source: Raal et al. (2015).18
Statistical Testing and Analysis Populations
The planned sample size of 51 patients (with a 2:1 randomization favouring evolocumab) provided 81% power to detect an approximately 18% difference in LDL cholesterol reduction between evolocumab and placebo, assuming a common standard deviation of 20.9% and a 2-sided significance level of 0.05.18 The primary and secondary efficacy analyses were conducted using a repeated-measures linear mixed-effects model, which included fixed effects for treatment group, the stratification factor (screening LDL-C < 11 mmol/L vs. ≥ 11 mmol/L), scheduled visit, and the interaction between treatment and scheduled visit. No imputation was conducted for missing data in these models.
Statistical testing followed a hierarchical approach. If the primary end point was statistically significant at the 0.05 level, statistical testing of secondary and selected exploratory end points proceeded using the Hochberg procedure to maintain the overall family-wise type I error rate at 0.05. Safety outcomes were analyzed descriptively, with no formal hypothesis testing.
The efficacy analysis set included almost all randomized patients who received at least 1 dose of study drug, consistent with a modified intention-to-treat approach for the primary and secondary efficacy end points. One patient who was randomized and withdrew consent before receiving the study drug was excluded from both the efficacy and safety analyses. Patients who discontinued treatment early but had postbaseline data were included in the efficacy analyses. The safety analysis set included all patients who received at least 1 dose of the study drug and was used to summarize treatment-emergent adverse events (TEAEs) and serious adverse events (SAEs).
In addition, prespecified subgroup analyses were conducted according to LDLR mutation status (e.g., LDL receptor defective vs. receptor negative or unclassified mutations). These analyses used the same repeated-measures modelling framework as the primary analysis and were intended to explore the relationship between underlying genetic defects and treatment response; results from these subgroup analyses were considered exploratory analyses.
Baseline Characteristics
Patient dispositions and baseline characteristics of the included trial are presented in Appendix 4 in the Supplemental Material document.
The demographic and clinical characteristics were generally well-balanced between the evolocumab and placebo groups. Patient age ranged from 13 to 57 years, with a mean age of 31 years; 49% of patients were female. Most patients were white (90%), while 4% were Asian. Patients had severe hypercholesterolemia despite intensive background lipid-lowering therapy, with a mean baseline ultracentrifugation LDL-C concentration of 9.0 mmol/L. Clinically evident cardiovascular disease was common: 43% of patients had documented coronary artery disease, 25% had a history of coronary artery bypass surgery, and 14% had undergone aortic valve replacement.
Genotyping confirmed HoFH in nearly all participants. LDLR mutations were present in 92% of patients, including 45% with true homozygous variants and 47% with compound heterozygous variants. LDL receptor functional status varied, with patient groups classified as receptor defective, receptor negative, or unclassified based on available genetic and functional data. One patient who met clinical diagnostic criteria was later found to genetically have the heterozygous variant but was retained in the intention-to-treat analyses.
Treatment exposure and concomitant medications of the included trial are summarized in Appendix 4 in the Supplemental Material document.
Critical Appraisal
Internal Validity
A summary of the internal validity of the included RCT is presented in Table 4. Detailed results of the internal validity appraisal are available in Appendix 4 in the Supplemental Material document.
Table 4: Critical Appraisal — Internal Validity of the Included Randomized Controlled Trial
Domain | Outcomes | Risk of bias | Reasons |
|---|---|---|---|
Randomization process | All | Low | Patients were randomized in a 2:1 ratio to receive evolocumab or placebo using a computer-generated randomization sequence, with stratification by screening LDL cholesterol level (< 11 mmol/L vs. ≥ 11 mmol/L). Randomization was centrally implemented via an interactive voice-response system, and treatment allocation was concealed. |
Deviation from the intended intervention | All | Low | The patients, study staff, and the sponsor were blinded to treatment assignment. Analysis was performed for all patients who received at least 1 dose. The 2 patients who discontinued the drug early were still included in the final analysis (consistent with ITT principles). The background lipid-lowering therapies remained stable during the trial, and no meaningful differences in concomitant treatment were reported. |
Missing outcome data | All | Low | One patient withdrew consent before receiving the drug and their data were excluded; it is unlikely that this exclusion biased the results. Of the 49 patients who received the study drug, all 49 (100%) completed the 12-week follow-up. Due to the high study completion rate and apparently low frequency of missing data for LDL-C, the potential risk of bias is likely low. Information on data missingness was not reported for other end points; therefore, the impact of missing data for these outcomes remains unknown. |
Measurement of the outcome | All | Low | All lipid results were masked by the central laboratory after the baseline visit. AEs were assessed under double-blind conditions and classified according to the Medical Dictionary for Regulatory Activities version 16.1. |
Selection of the reported result | All | Low | The trial was registered (NCT01588496). The reported primary end point (12-week LDL-C change) matches the prespecified protocol on the registered web page. No evidence of selective reporting. |
Other concerns: subgroup analyses | All efficacy outcomes | High (low or very low credibility) | The subgroup analyses based on LDLR mutation status were prespecified and biologically plausible but involved a very small number of patients in some categories (e.g., only 1 patient in the mutation-negative LDLR group). |
AE = adverse event; HoFH = homozygous familial hypercholesterolemia; ITT = intention to treat; LDL-C = low-density lipoprotein cholesterol.
Source: Raal et al. (2015).18
External Validity
A summary of the strengths and weaknesses of the external validity of the included RCT is presented in Table 5. Detailed findings from an external validity appraisal are provided in Appendix 4 in the Supplemental Material document.
Table 5: Critical Appraisal — External Validity of the Included Randomized Controlled Trial
Domain | Strengths | Limitations |
|---|---|---|
Population | The TESLA Part B trial was conducted at 17 sites across 10 countries, including North America (with 2 patients from Canada), Europe, the Middle East, and South Africa. This geographic diversity indicates that the findings can be applied to lipid clinics in Canada. | The applicability of the study's findings to patients younger than 12 years remains uncertain. In the TESLA Part B trial, the majority of participants were white (90%) and 4% were Asian, which may limit the generalizability of the results to patients of other ethnicities. The enrolled population reflects a highly selected population with HoFH: patients were aged ≥ 12 years (range, 13 to 57 years); clinically stable; had received maximally tolerated statins and, in most cases, ezetimibe; and had stable background therapy before randomization. The findings may not be applicable to individuals with HoFH who are receiving apheresis or these lipid-lowering agents. |
Intervention | Evolocumab was administered at a dosage of 420 mg every 4 weeks, along with other lipid-lowering treatments and regular laboratory tests, in accordance with clinical guidelines for the treatment of HoFH. | None identified. |
Comparator | The use of placebo as a comparator in the TESLA Part B trial was appropriate for patients without access to other lipid-lowering therapies after statins and ezetimibe. | In Canada, patients with HoFH may have access to other lipid-lowering therapies after treatment with statins and ezetimibe. The evidence did not compare efficacy and safety outcomes with any other active lipid-lowering therapies. |
Outcome | The primary outcome of this trial was change in LDL-C level, which is both clinically relevant in assessing the disease response and routinely assessed in the context of HoFH treatment. | The trial did not examine the impact of evolocumab on mortality or cardiovascular events directly. |
Time frame | This study provided direct evidence regarding the efficacy and safety of evolocumab at 12 weeks of follow-up. | The short-term duration of the study (12 weeks) prevents evaluation of long-term effectiveness and safety outcomes beyond 12 weeks. |
HoFH = homozygous familial hypercholesterolemia; LDL-C = low-density lipoprotein cholesterol.
Source: Raal et al. (2015).18
Results
Efficacy
Table 6 present the results for outcomes important to this review. Figure 1 presents the mean percentage change in ultracentrifugation LDL-C concentration from baseline to week 12.
The key efficacy results are the following:
LDL-C levels
Evolocumab reduced LDL-C by 30.9% and 2.4 mmol/L compared with placebo at 12 weeks.
LDL-C reductions were observed by week 4 and were maintained through week 12, with similar results when outcomes were assessed by calculated LDL-C levels or by the mean of weeks 6 and 12.
Apolipoprotein B
Evolocumab reduced apolipoprotein B by 23.1% compared with placebo at week 12.
Similar results were observed when apolipoprotein B was assessed using the mean of weeks 6 and 12.
There were no differences in LDL-C or apolipoprotein B between patients with different types of LDLR mutations. Details regarding subgroup effects are summarized in Appendix 4 in the Supplemental Material document.
Major adverse cardiovascular events (MACE) and HRQoL were not evaluated in the TESLA Part B trial.
Table 6: Summary of Key Efficacy Results of the Included Randomized Controlled Trial
Variable | Placebo n = 16 | Evolocumab n = 33 |
|---|---|---|
LDL cholesterol, ultracentrifugation | ||
Number of patients contributing to the analysis, n | 16 | 33 |
Baseline (mmol/L), mean (SD) | 8.7 (3.8) | 9.2 (3.5) |
At week 12 | ||
% change from baseline | ||
Change from baseline, least squares mean (95% CI) | 7.9% (–2.7% to 18.5%) | –23.1% (–30.7% to –15.4%) |
Treatment group difference vs. placebo (95% CI) | –30.9% (–43.9% to –18.0%) | |
P value | < 0.0001a | |
Absolute values (mmol/L) | ||
Change from baseline, least squares mean (95% CI) | 0.5 (–0.5 to 1.6) | –1.9 (–2.6 to –1.1) |
Treatment group difference vs. placebo (95% CI) | –2.4 (–3.7 to –1.1) | |
P value | 0.0004 | |
Mean of weeks 6 and 12 | ||
% change from baseline | ||
Change from baseline, least squares mean (95% CI) | 4.2% (–5.0% to 13.4%) | –25.6% (–32.2% to –19.0%) |
Treatment group difference vs. placebo (95% CI) | –29.8% (–40.9% to –18.6%) | |
P value | < 0.0001a | |
Absolute values (mmol/L) | ||
Change from baseline, least squares mean (95% CI) | 0.2 (–0.7 to 1.1) | –2.1 (–2.7 to –1.5) |
Treatment group difference vs. placebo (95% CI) | –2.3 (–3.3 to –1.2) | |
P value | < 0.0001 | |
Apolipoprotein B | ||
Number of patients contributing to the analysis, n | 16 | 33 |
Baseline (g/L), mean (SD) | 2.1 (0.8) | 2.1 (0.7) |
% change from baseline at week 12 | ||
Change from baseline, least squares mean (95% CI) | 4.0% (–5.6% to 13.5%) | –19.2% (–26.1% to –12.2%) |
Treatment group difference vs. placebo (95% CI) | –23.1% (–34.8% to –11.5%) | |
P value | 0.0007a | |
% change from baseline at the mean of weeks 6 and 12 | ||
Change from baseline, least squares mean (95% CI) | 2.7% (–6.3% to 11.6%) | –20.2% (–26.6% to –13.8%) |
Treatment group difference vs. placebo (95% CI) | –22.9% (–33.7% to –12.1%) | |
P value | 0.0004a | |
CI = confidence interval; HoFH = homozygous familial hypercholesterolemia; LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation; vs. = versus.
aMultiplicity adjustments following the Hochberg procedure were used to control for overall significance at the 0·05 level of significance for the primary and secondary end points.
Source: Raal et al. (2015).18
Figure 1: LDL-C Levels Results From the Included Randomized Controlled Trial
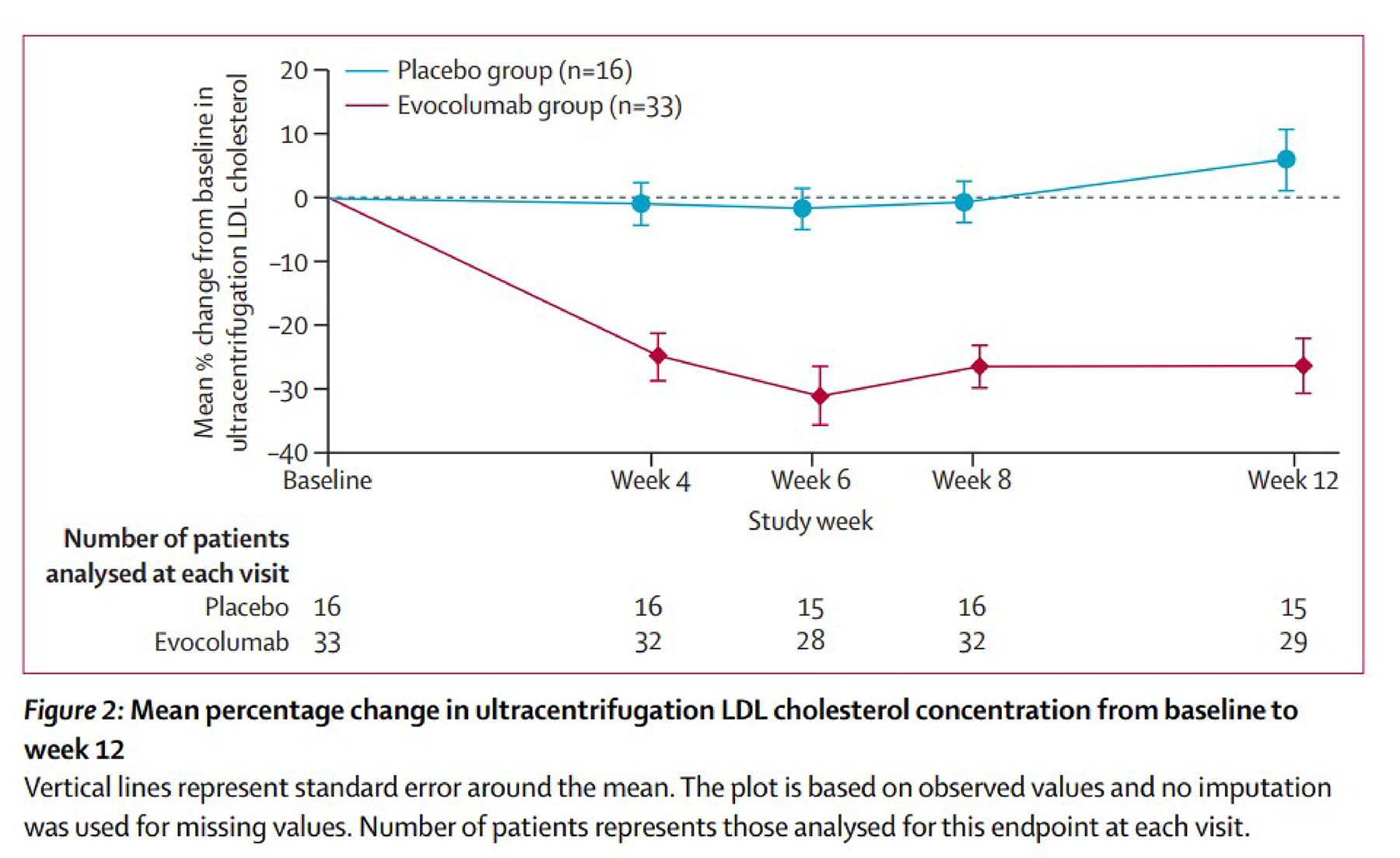
LDL = low-density lipoprotein; LDL-C = low-density lipoprotein cholesterol.
Source: Raal et al. (2015).18 Reprinted from The Lancet, Vol 385, Issue 9965, Raal FJ, Honarpour N, Blom DJ et al., Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA Part B): a randomized, double-blind, placebo-controlled trial, p. 345, with permission from Elsevier.
Harms
The analyses for safety outcomes were descriptive in the included trial. The key results are:
TEAEs occurred in 36% of patients in the evolocumab group and 63% of patients in the placebo group. All events were mild to moderate in severity.
No SAEs, deaths, or AEs leading to discontinuation of the study drug were reported in either treatment group.
The most frequently reported AEs in the evolocumab group were upper respiratory tract infection and influenza (each n = 3; 9%). In the placebo group, nausea was the most common adverse event (n = 2; 13%).
Summary of Findings and Certainty of the Evidence
The summary of findings from the GRADE assessment are presented in Appendix 4 in the Supplemental Material document. Based on thresholds suggested by the clinical experts, a reduction of at least 10% from baseline was considered a clinically meaningful change in LDL-C levels. In the absence of estimates of clinically meaningful change in apolipoprotein B outcomes, the certainty in the presence of a non-null effect was used.
The key narrative findings are:
Evolocumab likely reduces LDL-C levels in patients with HoFH compared with placebo.
Evolocumab likely reduces apolipoprotein B levels in patients with HoFH compared with placebo.
The effect of evolocumab on TEAEs in patients with HoFH is uncertain. Events were numerically less frequent in the evolocumab group, but this may be due to chance.
No new serious safety signals related to evolocumab were identified in the HoFH population, but the evidence is very uncertain.
Studies Addressing Gaps in the Systematic Review Evidence
Evidence gaps in the included study (the TESLA Part B trial) and 3 reports that provided evidence to address these gaps, are presented in Table 7.
Description of Studies
Characteristics of the 3 studies are summarized in Table 8.
Table 7: Summary of Gaps in the Included Randomized Controlled Trial
Evidence gap in the TESLA Part B trial | First author (year) | Article title |
|---|---|---|
Safety and effectiveness of evolocumab in pediatric patients ≥ 10 years | Raal et al. (2024)19 | Evolocumab Treatment in Pediatric Patients With Homozygous Familial Hypercholesterolemia: Pooled Data From Three Open-Label Studies |
Longer-term (> 12 weeks) safety and effectiveness of evolocumab in patients with HoFH | Santos et al. (2020)20 | Long-Term Evolocumab in Patients With Familial Hypercholesterolemia |
Safety and effectiveness of evolocumab in pediatric patients aged < 10 years | Buonuomo et al. (2021)21 | Evolocumab in the Management of Children < 10 Years of Age Affected by Homozygous Familial Hypercholesterolemia |
HoFH = homozygous familial hypercholesterolemia.
Table 8: Characteristics of Studies Addressing Gaps in Systematic Review Evidence
Study name, study design, and sample size | Patient population | Intervention and comparator | Relevant end points and follow-up |
|---|---|---|---|
Raal et al. (2024)19 Pooled post hoc analysis of 3 open-label, single-arm, multicentre studies (TAUSSIG, RAMAN, HAUSER-OLE) Total N = 39 |
|
|
Follow-up: 12 weeks |
Santos et al. (2020)20 Open-label, single-arm, multicentre study (TAUSSIG) Total N = 300 (106 patients with HoFH) |
|
|
Follow-up: median = 4.1 years (range, 0.2 to 5.0 years) |
Buonuomo et al. (2021)21 Case reports Total N = 2 |
|
|
Follow-up: 24 months |
AE = adverse event; HoFH = homozygous familial hypercholesterolemia; IQR = interquartile range; LDL-C = low-density lipoprotein cholesterol; NR = not reported; SAE = severe adverse event; SD = standard deviation; TEAE = treatment-emergent adverse event.
Sources: Raal et al. (2024);19 Santos et al. (2020);20 Buonuomo et al. (2021).21
Critical Appraisal
Raal et al. (2024) Study 19
The post hoc pooled analysis of 3 single-arm, open-label studies — NCT01624142 (TAUSSIG), NCT03403374 (RAMAN), NCT02624869 (HAUSER-OLE) — does not allow causal conclusions about the efficacy and safety of evolocumab. The absence of a comparator arm limits attribution of LDL-C changes to evolocumab.
Patient selection may introduce bias due to the small, pooled sample size (N = 39) and heterogeneity in background therapy, including the use of lipoprotein apheresis in a minority of patients (n = 4). Although the primary lipid outcomes were objective laboratory measurements, the open-label design may increase the risk of bias in the reporting of subjective outcomes, such as TEAEs. Several patients discontinued treatment due to administrative reasons or patient or investigator decision, which may have increased the risk of attrition bias and complicates interpretation of longer-term safety.
The analyses of the study were descriptive, without hypothesis testing, adjustment for multiplicity, or imputation of missing data. Heterogeneity across studies in concomitant statin intensity, ezetimibe use, and dosing schedules further increases risk of bias and complicates the interpretation of efficacy and safety findings.
External validity is limited by the small cohort and demographic concentration, with most patients enrolled from the Asia-Pacific region (27 of 39) and Europe (10 of 39); only a few were from North America (2 of 39). Because no country-level breakdown is provided, it is unclear if the study included pediatric patients from Canada.
Santos et al. (2020) Study 20
The TAUSSIG study was an open-label, single-arm study to assess the long-term effectiveness and safety of evolocumab in patients with HoFH. Without a comparator arm, it is not possible to determine how the observed changes are attributable to evolocumab, background therapy, or other lipid-lowering options.
Eligibility criteria for HoFH were clearly described. However, the study population may not represent all patients with HoFH in Canada, particularly those with more severe forms of the disease or those without easy access to specialized lipid clinics. A total of 54 patients with HoFH entered the TAUSSIG trial after completing TESLA Part A or B, which may introduce selection bias because patients continuing from prior trials may differ systematically from those enrolled directly. The cohort also included 14 adolescents, but the small sample size limits conclusions regarding this subgroup.
Treatment exposure in the HoFH cohort was heterogeneous due to individualized dosing based on apheresis status and lipid or PCSK9 response. In addition, withdrawal of patients with an LDL-C reduction of less than 5% may bias longer-term results toward patients who responded. Early study termination by the sponsor led to small sample sizes beyond 4 years, reducing confidence in long-term estimates. All analyses were descriptive, with no formal hypothesis testing, which limits interpretation of differential responses by LDLR genotype.
Safety findings may be influenced by the open-label design, and cardiovascular outcomes cannot be attributed solely to evolocumab without a comparator and standardized background therapy. Geographic representativeness was not reported, restricting assessment of applicability to clinical practice in Canada.
Buonuomo et al. (2021) Study 21
This letter-to-the-editor publication reported 2 individual cases of HoFH in children younger than 10 years. The letter provided very low–certainty evidence and did not allow causal conclusions regarding the efficacy or safety of evolocumab.
The absence of a comparator group, the extremely small and highly selected population, and concomitant weekly or biweekly lipoprotein apheresis limit the interpretability of the observed 30% or greater LDL-C reductions. Outcome reporting was descriptive, with limited detail on measurement, variability, or factors related to the sequencing of apheresis and evolocumab. Safety findings were reported only in general terms, without detailed AE documentation.
The 2 cases were treated in a specialized single centre with strong multidisciplinary support; the results have limited generalizability without access to such resources or support. Overall, the observed LDL-C reductions and the safety profile of evolocumab in this population should be considered preliminary.
Results
Results for efficacy and harm outcomes important to this review from the 3 studies that fill evidence gaps of the systematic review are presented in Table 9.
Table 9: Summary of Results of Studies Addressing Gaps in Systematic Review Evidence
First author (year), study design, and sample size | Efficacy outcomes | Harms outcomes |
|---|---|---|
Raal et al. (2024)19 Post hoc pooled analysis of 3 open-label, single-arm, multicentre studies (TAUSSIG, RAMAN, HAUSER-OLE). Total N = 39 | LDL-C (change from baseline to 12 weeks) Nonapheresis group (n = 35)
Apheresis group (n = 4)
Residual LDL receptor activity did not reliably predict LDL-C response to evolocumab Apolipoprotein B (change from baseline to 12 weeks)
| Any TEAE
Most common TEAEs
SAEs
Injection-site reactions (nonserious):
Treatment discontinuation due to AE:
Deaths: 0 |
Santos et al. (2020)20 Open-label, single-arm, multicentre study (TAUSSIG) Total N = 300 Relevant n = 106 | LDL-C (change from baseline)
LDL-C reduction ≥ 15% achieved by 56.7% to 72.2% of patients with HoFH from week 12 to week 216. Apolipoprotein B (change from baseline)
Cardiovascular events (rates per year):
| Safety, n (%)
Most common TEAEs, n (%)
Injection-site reactions, n (%):
|
Buonuomo et al. (2021)21 Case reports Total N = 2 | LDL-C (mean time-averaged values at 24 months): Patient #1:
Patient #2:
| TEAEs: 0 SAEs: 0 |
AE = adverse events; LDL-C = low-density lipoprotein cholesterol; MI = myocardial infarction; Q1 = quartile 1; Q3 = quartile 3; SAE = serious adverse event; SD = standard deviation; TEAE = treatment-emergent adverse event; URTI = upper respiratory tract infection.
Sources: Raal et al. (2024);19 Santos et al. (2020);20 Buonuomo et al. (2021).21
Discussion
Efficacy
TESLA Part B was a randomized, double-blind, placebo-controlled trial evaluating the efficacy of evolocumab in patients with HoFH receiving stable background lipid-lowering therapy.18 The trial demonstrated a statistically significant reduction in LDL-C with evolocumab compared with placebo. At week 12, evolocumab likely reduced ultracentrifugation LDL-C by 30.9% (95% CI, –43.9% to –18.0%; moderate certainty due to cumulative concerns regarding indirectness and imprecision), corresponding to an absolute reduction of 2.4 mmol/L, and reduced apolipoprotein B (moderate certainty due to cumulative concerns regarding indirectness and imprecision) compared with placebo. Clinical experts generally consider a 15% LDL-C reduction to be clinically meaningful in HoFH, given the limited responsiveness of this population to conventional therapies. The trial did not report cardiovascular outcomes or HRQoL. LDL-C reduction is a recognized surrogate end point in HoFH, and high LDL-C (> 130 mg/dL) is associated with a higher risk of cardiovascular events. Given its effects on LDL-C, evolocumab may indirectly reduce the risk of MACE in patients with HoFH compared with placebo.
The prespecified and exploratory subgroup analyses evaluated LDL-C and apolipoprotein B responses according to LDLR mutation status. Patients with at least 1 LDL receptor allele classified as defective experienced the greatest benefit, with a mean 40.8% reduction versus placebo; patients with both negative LDLR mutations showed minimal or no response. However, there were no statistically significant interactions between different LDLR mutation subgroups. The observed subgroup effects were considered as low or very low credibility.
Due to the small sample size (N = 50), short duration (12 weeks), and exclusion of patients receiving lipoprotein apheresis, the generalizability of the findings from the TESLA Part B trial to settings in Canada is limited. The trial population was highly selected, with most patients having access to specialized lipid clinics. The findings may not fully reflect real-world heterogeneity in treatment access for patients with HoFH in Canada.
The open-label TAUSSIG study provides supportive evidence on the use of evolocumab in patients with HoFH.20 In the TAUSSIG study, patients with HoFH treated with evolocumab for a median of 4.1 years experienced sustained LDL-C reductions of approximately 20% to 30%, with greater reductions observed after dosage escalation to 420 mg every 2 weeks. Due to the single-arm design, the observed changes cannot be attributed solely to evolocumab. Additional evidence from pediatric studies, including pooled analyses of 3 single-arm studies19 and from 2 patients younger than 10 years,21 indicated that evolocumab produces similar LDL-C reductions in children with HoFH.
The relationship between LDL-C reduction and long-term cardiovascular outcomes in HoFH remains unclear. The TESLA Part B trial did not report cardiovascular events or HRQoL measures.18 The TAUSSIG study reported low event rates but lacked a comparator arm.20 The absence of head-to-head comparisons with other advanced therapies (e.g., lomitapide, mipomersen, evinacumab) further limits the ability to draw comparative effectiveness conclusions.
Harms
In the TESLA Part B trial, evolocumab was generally well tolerated, with no SAEs reported during the 12-week treatment period.18 TEAEs occurred in 36% of patients treated with evolocumab versus 63% of those treated with placebo. The most common events in the evolocumab group were mild upper respiratory tract infections and influenza. No SAEs, treatment discontinuations due to AEs, or death due to AEs were reported. Due to the small sample size (N = 50) and the short duration (12 weeks) of the TESLA Part B trial, the evidence on the safety outcome was very low.
Over a median exposure of 4.1 years in the long-term single-arm study (TAUSSIG), 89% of patients experienced at least 1 AE, most of which were mild infections or headaches.20 SAEs were reported at a rate of 2.7% per year in this study.20 Data on pediatric patients from the pooled analysis and 2 case reports reported no unexpected safety concerns, even in children as young as 4 years old.19,21 No studies reported safety outcomes based on different LDL receptor genotypes were identified. The limited data in children younger than 10 years also restrict broader generalizability.
Ethics and Equity Considerations
Although HoFH is rare overall, some populations experience a higher prevalence due to founder effects and genetics, predominately in individuals with French Canadian ancestry living in the Saguenay–Lac-Saint-Jean region.22-24 Other populations in which founder effects have been described include individuals with Ashkenazi Jewish, Christian Lebanese, and South African Afrikaner ancestry.24
According to the clinical experts, children and adolescents may experience disproportionate impacts of HoFH due to manifestation in early life, which leads to rapid progression of atherosclerosis and premature cardiovascular events. In addition, due to the age restriction for Health Canada approval (10 years and older), evolocumab can only be used off label in children younger than 10 years. Some population subgroups (e.g., groups that are marginalized, persons with geographic- and/or resource-related disparities) may have limited access to treatment for HoFH. For example, patients living in rural, remote, or less affluent regions may have limited access to experts, diagnostic testing, and treatment centres (e.g., specialty lipid clinics, apheresis centres). This could potentially lead to late identification or underidentification, limited treatment options, worse cardiovascular outcomes, and mortality. Advanced therapies, such as evolocumab, are expensive and coverage varies across Canada. Out-of-pocket costs may be prohibitive for some patients and their families.
The clinical experts informed us that some population subgroups may experience disproportionate burden of harms and benefits to treatment for HoFH. Specifically, patients with extremely severe forms of HoFH (i.e., very severe phenotypes with minimal residual LDL receptor activity) or with 2 null gene variants may have poor or no response to evolocumab. Individuals with statin intolerance or those with reduced or absent LDL receptor function have a limited response to statins; therefore, these patients would be reliant on expensive alternatives (e.g., ezetimibe, lomitapide, evinacumab, lipoprotein apheresis). For pediatric populations, there is limited safety evidence and, as previously described, there are access disparities due to geographic location and socioeconomic status.
To support equitable access to evolocumab, the medication must also be available for patients in remote or rural locations. If ready access to the medication is available and all pharmacies can receive it, it is not anticipated that further changes to the health system are required according to the clinical experts.
Conclusion
The results from the TESLA Part B trial suggested that evolocumab likely provides clinically meaningful reductions in LDL-C and apolipoprotein B in patients with HoFH.18 The overall certainty of the evidence is moderate for both LDL-C and apolipoprotein B outcomes. The short duration, small sample size, and lack of direct evaluation of effect on MACE limits the ability to draw firm conclusions about target cardiovascular outcomes. The LDL receptor genotypes and variable responsiveness to PCSK9 inhibitors introduce uncertainty in predicting individual treatment benefit. Comparative evidence against other advanced therapies is lacking, and data remain limited in very young children, patients with LDLR-negative genotypes, and those receiving apheresis or combination therapy. No SAEs were identified in either treatment arm during the 12-week trial. Longer-term observational data from the TAUSSIG study and emerging pediatric evidence suggest a consistent safety profile as described in the product monograph for evolocumab.19-21 However, the overall certainty of evidence on safety outcomes was low or very low given the relatively small sample sizes across all studies and evidence from noncomparative study designs.
Economic Review
CDA-AMC Assessment of Costs
The Economic Review consisted of a cost comparison for evolocumab compared with alirocumab, lomitapide, and evinacumab for HoFH.
Based on public list prices, evolocumab is expected to have a per-patient cost of $7,609 per year (refer to Supplemental Material document, Appendix 5). Alirocumab, lomitapide, and evinacumab are expected to have per-patient costs of $6,987, $379,860, and $461,154 per year, respectively (Figure 2).
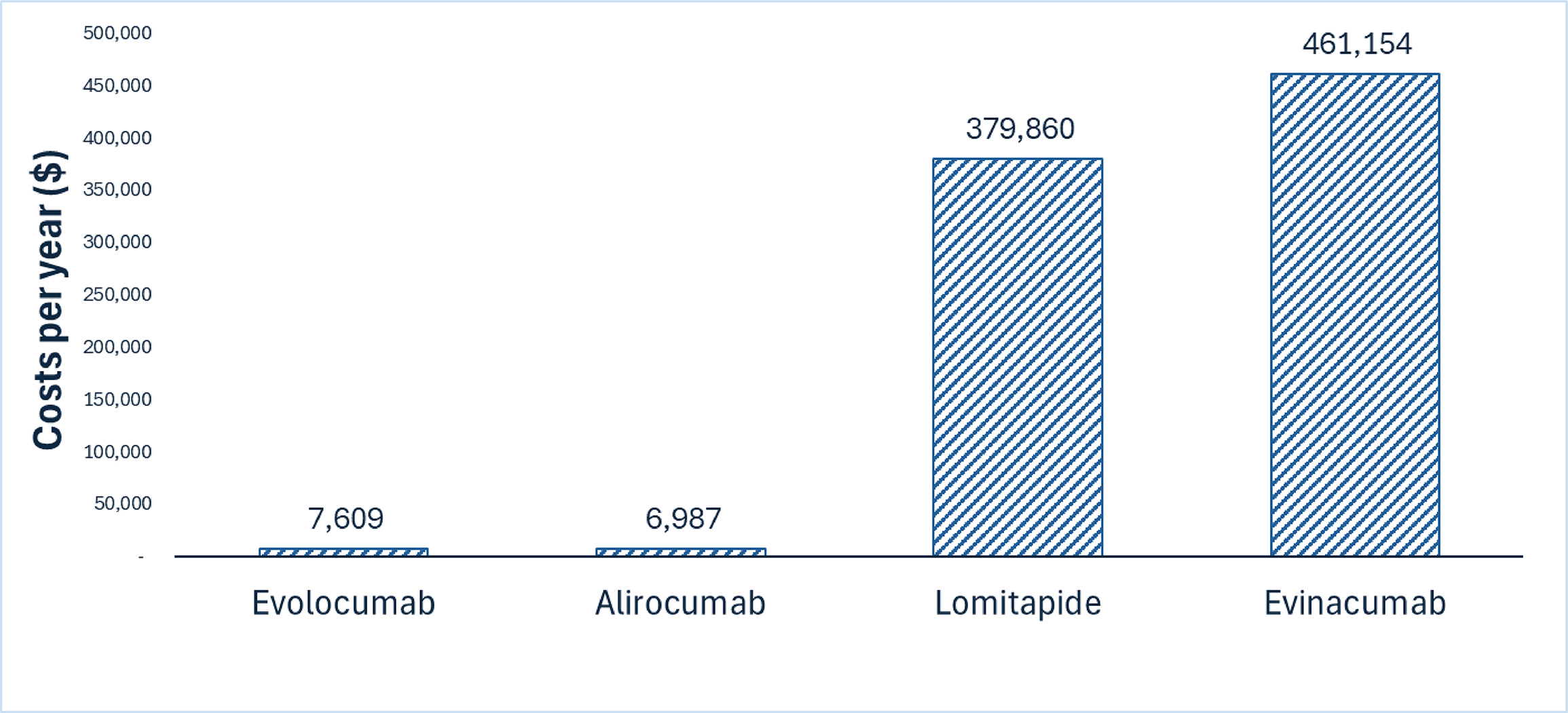
The difference per year in the cost of evolocumab varies between $453,545 in cost savings compared to evinacumab, and $622 in increased costs when compared with alirocumab. As such, the impact of the reimbursement of evolocumab for HoFH is contingent on which treatments are displaced. Additional items for consideration include the following:
Evidence from the studies included in the Clinical Review suggests that evolocumab improved LDL-C levels compared to placebo and has an acceptable safety profile. No evidence was identified regarding the comparative efficacy and safety of evolocumab versus other active comparators.
Evolocumab is only available as a brand name product in Canada (Repatha). There are no biosimilars currently under review at Health Canada.
Clinical experts consulted for this review provided the following considerations on possible impacts of the reimbursement of evolocumab on the use of health care resources:
Because treatment administration of evolocumab is subcutaneous, its treatment administration costs are lower compared to evinacumab (IV), similar to alirocumab (subcutaneous), and higher than lomitapide (oral).
Compared to lomitapide, evolocumab is expected to have lower monitoring and other health care costs related to management of AEs because lomitapide has a worse safety profile.
Evolocumab is expected to have similar health care costs related to monitoring and management of AEs compared to evinacumab and alirocumab.
Evolocumab, lomitapide, and evinacumab are approved for the treatment of HoFH in Canada. Lomitapide is approved for the adult population only, whereas evolocumab is approved for patients at least 10 years old and evinacumab is approved for patients at least 6 months old. Alirocumab is only approved for the treatment of HeFH in Canada.
Evolocumab was previously reviewed by CADTH in 2016,25 2017,26 and 202427 for other lipid disorders, with positive recommendations for reimbursement. CADTH previously reviewed lomitapide (2015)28 and evinacumab (2024)29 for HoFH, with positive recommendations for reimbursement.
Based on feedback from participating drug plans, lomitapide may not be reimbursed or may have very limited coverage by any public drug plan in Canada. Alirocumab has very limited coverage, and evinacumab is the comparator with greatest coverage for patients with HoFH. For jurisdictions that do not reimburse either alirocumab or lomitapide, evinacumab is currently the only comparator reimbursed for HoFH. If evolocumab were to be introduced in these jurisdictions, it would most likely be done as an earlier line of therapy (i.e., before lomitapide or evinacumab).
There were no cost-effectiveness studies conducted in Canada that included evolocumab for HoFH identified in a literature search conducted on December 17, 2025, with alerts maintained until the FMEC meeting on June 5, 2026.
Conclusion
The reimbursement of evolocumab for the treatment of HoFH is expected to decrease overall drug acquisition costs in settings where alirocumab is not reimbursed. In settings where alirocumab is reimbursed for HoFH, reimbursement of evolocumab is expected to increase overall drug acquisition costs. Based on the findings from the Clinical Review, there were no direct or indirect comparisons of evolocumab with active regimens for HoFH; as such, the comparative efficacy of evolocumab versus identified comparators is unknown and its cost-effectiveness cannot be determined. Given that evolocumab has lower drug acquisition costs compared to most of its comparators, it can reduce costs to the public health system with unknown impact on clinical outcomes.
References
1.Amgen Canada Inc. Repatha (evolocumab): Solution for Subcutaneous Injection, 140 mg in 1.0 mL (140 mg/mL), 420 mg in 3.5 mL (120 mg/mL) [product monograph]. September 10, 2015 Updated May 16, 2025. Accessed June 3, 2026. 00080599.PDF.
2.Sarah D de Ferranti ML. Familial hypercholesterolemia in children. In: Fulton DR, ed. 2025.
3.Robert S Rosenson RAH, Cert Endo. Familial hypercholesterolemia in adults: Overview. 2025.
4.Brown L, Ruel I, Baass A, et al. Homozygous Familial Hypercholesterolemia in Canada: An Observational Study. JACC Adv. 2023;2(3):100309. doi:10.1016/j.jacadv.2023.100309 PubMed
5.Cuchel M, Bruckert E, Ginsberg HN, et al. Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur Heart J. 2014;35(32):2146-2157. doi:10.1093/eurheartj/ehu274 PubMed
6.Mach F, Koskinas KC, Roeters van Lennep JE, et al. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Developed by the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. 2025;46(42):4359-4378. doi:10.1093/eurheartj/ehaf190 PubMed
7.Cuchel M, Raal FJ, Hegele RA, et al. 2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: new treatments and clinical guidance. Eur Heart J. 2023;44(25):2277-2291. doi:10.1093/eurheartj/ehad197 PubMed
8.Brunham LR, Ruel I, Aljenedil S, et al. Canadian Cardiovascular Society Position Statement on Familial Hypercholesterolemia: Update 2018. Can J Cardiol. 2018;34(12):1553-1563. doi:10.1016/j.cjca.2018.09.005 PubMed
9.Cuchel M, Bruckert E, Ginsberg HN, et al. Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur Heart J. 2014;35(32):2146-57. doi:10.1093/eurheartj/ehu274 PubMed
10.Alberta Precision Laboratories. Familial or Inherited Hypercholesterolemia Panel. 2025. Accessed January 01, 2026. https://www.albertahealthservices.ca/webapps/labservices/indexAPL.asp?id=9275&tests=&zoneid=1&details=true
11.Alberta Precision Laboratories. Familial Hypercholesterolemia: Information for Ordering Providers. 2025. Accessed January 01, 2026. https://www.albertahealthservices.ca/assets/wf/lab/if-lab-hc-gls-familial-hypercholesterolemia-information-for-ordering-providers.pdf
12.Saskatchewan Health Authority. Inherited Cardiovascular Diseases Testing Requisition version 1.2 - Genomics Laboratory. 2023. Accessed January 01, 2026. https://www.saskhealthauthority.ca/system/files/2024-01/Form-LabMed-InheritedCardiovascularDiseasesTestingReq.pdf
13.IWK Health. IWK CGL Test Menu - with restrictions and gene content. 2025. Accessed January 01, 2026. https://iwkhealth.ca/sites/default/files/2025-12/IWK%20CGL%20Restrictions%20List%20External.pdf
14.London Health Sciences Centre. FAMILIAL HYPERCHOLESTEROLEMIA FOCUSED PANEL. 2023. Accessed January 01, 2026. https://www.lhsc.on.ca/media/13181/download?attachment=
15.Ontario Health. Genetic Testing for Familial Hypercholesterolemia: Implementation Recommendations. 2022. Accessed January 01, 2026. https://ontariohealth.ca/content/dam/ontariohealth/documents/familial-hypercholesterolemia-implementation-recommendations.pdf
16.Hamilton Regional Laboratory Medicine Program. Familial Hypercholesterolemia. 2024. Accessed January 01, 2026. https://ltig.hrlmp.ca/ViewTestHRLMP.aspx?testID=2291
17.Kramer AI, Christian S, Bartels K, Vaizman N, Hegele RA, Brunham LR. Genetic Testing for Familial Hypercholesterolemia: The Current State of Its Implementation in Canada. CJC Open. 2024;6(11):1395-1402. doi:10.1016/j.cjco.2024.08.005 PubMed
18.Raal FJ, Honarpour N, Blom DJ, et al. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA Part B): a randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9965):341-50. doi:10.1016/S0140-6736(14)61374-X PubMed
19.Raal FJ, Hegele RA, Ruzza A, et al. Evolocumab Treatment in Pediatric Patients With Homozygous Familial Hypercholesterolemia: Pooled Data From Three Open-Label Studies. Arterioscler Thromb Vasc Biol. 2024;44(5):1156-1164. doi:10.1161/ATVBAHA.123.320268 PubMed
20.Santos RD, Stein EA, Hovingh GK, et al. Long-Term Evolocumab in Patients With Familial Hypercholesterolemia. J Am Coll Cardiol. 2020;75(6):565-574. doi:10.1016/j.jacc.2019.12.020 PubMed
21.Buonuomo PS, Mastrogiorgio G, Leone G, et al. Evolocumab in the management of children <10 years of age affected by homozygous familial hypercholesterolemia. Atherosclerosis. 2021;324:148-150. doi:10.1016/j.atherosclerosis.2021.03.026 PubMed
22.Bchetnia M, Bouchard L, Mathieu J, et al. Genetic burden linked to founder effects in Saguenay–Lac-Saint-Jean illustrates the importance of genetic screening test availability. J Med Genet. 2021;58(10):653-665. PubMed
23.Paquette M, Genest J, Baass A. Familial hypercholesterolemia: experience from the French-Canadian population. Curr Opin Lipidol. 2018;29(2):59-64. doi:10.1097/mol.0000000000000487 PubMed
24.Mszar R, Buscher S, Taylor HL, Rice-DeFosse MT, McCann D. Familial hypercholesterolemia and the founder effect among Franco-Americans: a brief history and call to action. CJC Open. 2020;2(3):161-167. PubMed
25.CADTH. Drug Reimbursement Review: Evolocumab (Repatha) for primary hyperlipidemia and mixed dyslipidemia. 2016. Accessed March 30, 2026. https://www.cda-amc.ca/evolocumab
26.CADTH. Drug Reimbursement Review: Evolocumab (Repatha) for primary hyperlipidemia and mixed dyslipidemia. 2017. Accessed March 30, 2026. https://www.cda-amc.ca/evolocumab-0
27.CADTH. Drug Reimbursement Review: Evolocumab (Repatha) for primary hyperlipidemia. 2024. Accessed March 30, 2026. https://www.cda-amc.ca/evolocumab-1
28.CADTH. Drug Reimbursement Review: Lomitapide (Juxtapid) for homozygous familial hypercholesterolemia. 2015. Accessed March 30, 2026. https://www.cda-amc.ca/lomitapide
29.CADTH. Drug Reimbursement Review: Evinacumab (Evkeeza) for homozygous familial hypercholesterolemia. 2024. Accessed March 30, 2026. https://www.cda-amc.ca/evinacumab
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.