CADTH Health Technology Review
The Use of Cone Beam CT in Dental, Oral, and Maxillofacial Surgery, and Otolaryngology Settings
Environmental Scan
Authors: Sarah Ndegwa, Yan Li, Melissa Severn, Caitlyn Ford
Abbreviations
2-D
two-dimensional
3-D
three-dimensional
CBCT
cone beam CT
ENT
ear, nose, and throat
FOV
field of view
MSCT
multislice CT
TMJ
temporomandibular joint
µSV
microsievert
Key Messages
The objective of this Environmental Scan was to determine how cone beam CT (CBCT) is being used in Canada, to identify the types of professionals conducting CBCT exams, and to identify the training requirements for CBCT operators.
This scan was informed by a literature search and survey of a sample representation from various clinical settings across Canada. Survey responses were received from Ontario, British Columbia, Manitoba, Prince Edward Island, and Alberta. More than a third of responses were received from dentists in Ontario.
Ionizing radiation has been shown to be a risk factor for the development of malignancy. Since CBCT delivers a higher dose of radiation compared to conventional 2-D imaging, it is important to ensure that the level of exposure to radiation is as low as possible.
Based on responses from the survey, CBCT scans appear to be most commonly being used for dental implantology planning in adults. CBCT also appears to be commonly used for detection of impacted teeth, detection of oral and facial cysts, tumours, and endodontic imaging in adults.
Survey feedback suggests that CBCT is rarely used in children, who are the most sensitive to the effects of ionizing radiation. With the exception of 1 respondent, survey feedback suggested that CBCT is not typically being used for infants and children younger than the age of 5. Respondents rarely used CBCT for children aged 5 to 9 years. The most common procedures used in children 5 years to 17 years of age appear to be for the detection of impacted teeth and the detection of oral and facial cysts, and tumours.
Across all age groups, respondents rarely used CBCT for caries (tooth decay) detection, gum disease detection, nasal septum imaging, and cleft palate imaging. No respondents reported using CBCT for plastic surgery, inner ear imaging, or skull and cranial imaging; however, this may be because of the responses being primarily from dentists.
A wide range of radiation dose levels associated with CBCT use were reported in the survey, depending on the age group, specific procedure, and the radiation dose metric used.
Educational provisions in place for CBCT operators to ensure safety and technical competence differs between the provinces, with some taking more structured approaches than others. The health professionals allowed to operate CBCT scanners also vary between provinces. Based on the survey results, dentists made up the bulk of health professionals currently conducting CBCT scans; however, dentists were also the most well-represented among survey respondents, which may have influenced this result.
Several CBCT scanner models are currently being used in Canada. Most respondents indicated that CBCT scanners have imaging pre-sets that they use for the procedures they perform. Approximately half of respondents indicated that they have also defined their own imaging parameters for some procedures. Most of the CBCT systems being used include exposure tables, which the majority of respondents found easy to understand.
Abstract
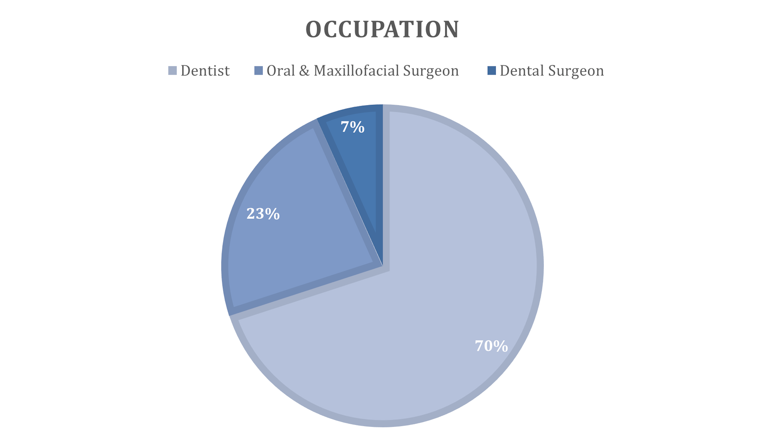
This Environmental Scan presents an overview of the current context of the use of cone beam CT (CBCT) in Canada based on a literature search and a survey of a small number of people working in the field. Thirty survey responses were received from Ontario (60%), Manitoba (16.7%), British Columbia (13.3%), Prince Edward Island (6.7%), and Alberta (3.3%). The majority (70.0%) of responses were received from dentists, with a smaller number of responses received from oral and maxillofacial surgeons (23.3%) and dental surgeons (6.3%). CBCT use and training requirements vary across Canadian jurisdictions; however, 1 consistency seemed to be the limited use in infants and children younger than 5 years who are the most vulnerable to potential negative effects of ionizing radiation. Based on responses from the survey, CBCT scans appear to be most commonly being used for dental implantology planning in adults. CBCT also appears to be commonly used for the detection of impacted teeth, oral and facial cysts, tumours, and for endodontic imaging in adults. The most common procedures reported by survey respondents of CBCT use in children 5 years to 17 years of age appear to be for the detection of impacted teeth and the detection of oral and facial cysts and tumours. Educational provisions in place for CBCT operators to ensure safety and technical competence differ between the provinces, with some taking more structured approaches than others. The health professionals allowed to operate CBCT scanners also vary between provinces. Based on the survey results, dentists made up the bulk of health professionals currently conducting CBCT scans; however, dentists were also the most well-represented among survey respondents, which may have influenced this result. A wide range of radiation dose levels associated with CBCT use were reported in the survey, depending on the age group, specific procedure, and the radiation dose metric used. Most respondents used the CBCT unit’s manufacturer-provided pre-sets.
Context
Cone beam CT (CBCT) is used by health care professionals in dental and other settings to rotate around the patient to capture 3-dimensional (3-D) images of anatomic regions such as the oral and maxillofacial region; and otolaryngology (or ears, nose, and throat — ENT) area.1 Compared to traditional multislice CT (MSCT), CBCT uses cone-shaped X-ray beams to allow for the imaging of larger volumes at lower radiation doses in a single scan.1,2 CBCT scanners can easily be installed in outpatient clinics because of their compact size.3 Due to a small footprint that does not require additional infrastructure, the ability to generate images of diagnostic quality, and a specialized design for imaging the oral and maxillofacial region, CBCT is used in the evaluation, diagnosis, and treatment planning of various conditions and procedures such as dental implants, cleft palates, root canals, and dental traumas.1,3
Nonetheless, there are tradeoffs that clinicians need to consider when assessing the risk versus the benefit of using CBCT in routine practice. CBCT imaging has inferior soft tissue differentiation compared to MSCT2 and is more susceptible to image artifacts caused by metal implants.4 Furthermore, CBCT delivers a higher dose of radiation compared to conventional 2-dimensional (2-D) imaging.4 The radiation exposure of a single CBCT scan is equivalent to at least 10 panoramic radiographs.5 Ionizing radiation has been shown to be a risk factor for the development of malignancy.6 As the effects are cumulative and there is no safe threshold for radiation exposure, imaging professionals need to observe the “as low as reasonably achievable” radiation safety principle.5 Specifically, CT scanner operators should use sufficient doses to obtain acceptable image quality and avoid unnecessary exposure of ionization radiation.7 This principle is especially important for children, who are more sensitive to ionizing radiation exposure, as they have a longer lifespan for cumulative effects to develop.1,7 Compared to adults, whose risk is estimated to be between 1 out of 100,000 and 1 out of 350,000, children may have double the risk of fatal malignancy associated with the ionizing radiation from CBCT.8 Hence, educational provisions for CBCT operators and imaging guidelines have been developed to help ensure technical competence and prevent unnecessary image retakes.5
A previous CADTH Reference List report published in 2009 identified studies that reviewed the clinical effectiveness, safety, and guidelines for the use of CBCT for patients with dental and/or maxillofacial abnormalities.9 To assess current training requirements for CBCT operators and how CBCT is being used in routine clinical practice in Canada, this Environmental Scan was informed by a literature search and survey of a sample representation from various clinical practices across Canada.
Objectives
The key objective of this Environmental Scan are as follows:
Determine procedures for which CBCT is commonly used.
Identify the professionals conducting CBCT exams for dental, maxillofacial, and ENT procedures.
Outline specific education and training provisions provided at the provincial level.
Verify the number of CBCT units across Canada.
Identify CBCT models being used across Canada and how settings are being used.
Ascertain the ranges of radiation dose per procedure type and age group (infant, child, adolescent, adult).
Methods
This Environmental Scan is based on results from a literature search and responses from a survey that was distributed to relevant stakeholders from Canadian dental and other practice settings. Table 1 outlines the criteria for information gathering and selection.
Table 1: Components of the Environmental Scan
Criteria | Description |
Population | People of any age requiring imaging in the dental, maxillofacial and oral surgery, or ENT settings |
Interventions | Cone beam CT |
Dento-maxillofacial imaging:
• detection of oral/facial cysts, tumours | |
ENT imaging:
| |
Other:
| |
Outcomes |
|
Information gathering approach | Survey Literature search: bibliographic databases and grey literature |
CBCT = cone beam CT; ENT = ear, nose, and throat.
Literature Search and Selection
A literature search helped identify information to address the key objectives pertaining to: common procedures in which CBCT is used, professionals conducting CBCT scans in dental and other settings, education and training requirements, and radiation dose ranges across procedures and age groups. A literature search of key bibliographic databases and grey literature (based on the Grey Matters checklist) was conducted on April 28, 2010, by an information specialist (and subsequently updated September 1, 2020), based on a peer-reviewed search strategy developed with input from the project team.
One author screened the literature search results to select articles pertaining to procedures for which CBCT is used, educational and training requirements, radiation doses, and the type of professionals performing CBCT scans for full-text review, using the selection criteria shown in Table 1. Additionally, handsearching of provincial and territorial professional association and college websites was also conducted to identify any other references not found in the literature search.
Survey
A survey was conducted from to February 26 to March 26, 2021 to address the key objectives pertaining to common procedures in which CBCT is used, the range of professionals conducting CBCT scans in dental and other settings, the number of CBCT units across Canada, and radiation dose ranges across procedures and age groups. In addition, questions addressed the key demographics of respondents (i.e., discipline and jurisdiction), information about CBCT scanners used in their facilities (e.g., brand, whether pre-sets are used, whether facility-defined parameters are used), and whether respondents were willing to participate in a follow up consultation, if required. The survey was distributed electronically using Survey Monkey. A draft of the survey was reviewed internally and externally, and pilot-tested before being finalized. A final version of the questionnaire used in the survey is available on request to CADTH.
A sample representation of stakeholders from dental, maxillofacial, and ENT settings from each province and territory (including rural locations) were identified through CADTH’s Liaison Officers and other available networks. National and provincial associations and regulatory authorities responsible for dental, maxillofacial, and ENT procedures were engaged to distribute the survey. Furthermore, the provincial colleges of physicians and surgeons were also surveyed to help inform educational and training requirements for CBCT operators and to distribute the survey to their contacts. A query was also sent to provincial radiation protection agencies to help inform this scan about the number of CBCT units in their jurisdiction.
Participants received email invitations and were given 20 business days to complete the survey. Survey respondents were given the opportunity to electronically consent to the reporting of the information they provided. Following an initial analysis of the survey data, it was noted that there were no or few responses from respondents in some jurisdictions and some professional areas. The survey was then re-opened for an additional 5 business days, with a reminder sent to previous potential informants and the survey further distributed to additional potential participants, targeting provinces and professional areas for which responses were not received from the initial survey period.
Feedback from respondents who gave consent to use their survey feedback was included in this report. A response was deemed partially complete if 1 or more questions were left blank by the respondent. Partially complete responses that did not include any CBCT-specific information were excluded from the data analysis.
Synthesis Approach
Disaggregated jurisdictional data were used to identify any notable similarities or differences regarding CBCT use in different settings. Because of the limited data that was received from Alberta (one respondent), feedback from this province was only included in the pan-Canadian analysis of the professionals conducing CBCT exams and the procedures for which CBCT is commonly used. Feedback from open-ended questions was also incorporated into the text. Respondents self-selected their professional designations and responses were reported as such. Findings from the literature search and survey are summarized narratively and grouped by objective.
Stakeholder Feedback
A draft version of this report was posted on the CADTH website and sent to survey participants to elicit stakeholder feedback. Relevant stakeholder feedback was incorporated into the final version of this report based on the input received.
Findings
This Environmental Scan is based on findings from a literature search and responses from a survey of health care professionals currently using CBCT in their settings. Because of the nature of how the survey was distributed, it is not exactly known how many individuals received the survey. A total of 53 responses were received. Of these, 23 (43.4%) were duplicates or incomplete and were excluded. A total of 30 responses from the survey were included in the report. Details of the jurisdictions and occupations represented by the survey respondents are presented in Figures 1 and 2, as well as in Appendix 1. More than a third (36.7%) of responses were received from dentists in Ontario. There were also responses from oral and maxillofacial surgeons (23.3%), and dental surgeons (6.7%). There was lower representation from other provinces including Manitoba (16.7%), British Columbia (13.3%), Prince Edward Island (6.7%), and Alberta (3.3%). In response to the request for stakeholder feedback, 2 personal communications from an ENT physician and a radiologist describing CBCT use in Alberta were included in the report, in addition to a personal communication from a dentist in Ontario identifying the number of CBCT units in Ontario.
Figure 1: Survey Respondent Information by Province
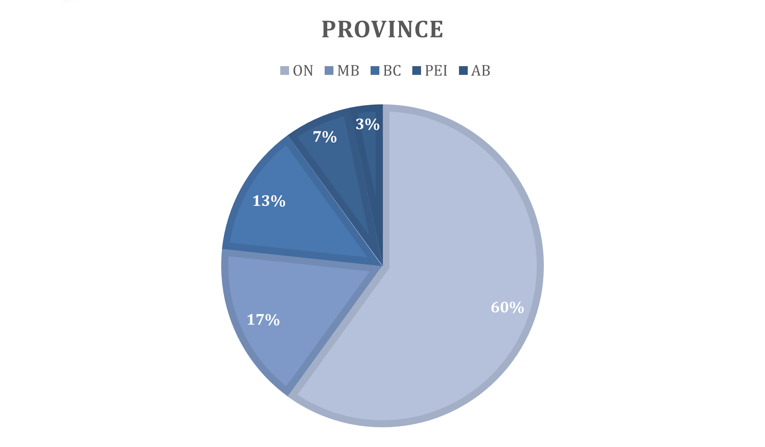
AB = Alberta; BC = British Columbia; MB = Manitoba; ON = Ontario; PE = Prince Edward Island.
Objective 1: Common Procedures in Which CBCT is Used
Relevant articles from a literature search provided contextual information on the use of CBCT in dental practices. Feedback from the survey was used to identify the exams and procedures, and age groups, currently using CBCT in different settings in Canada (Appendix 2).
Compared to conventional 2-D radiography X-ray, CBCT is reported to have advantages in identifying the location and severity of dental pathologies, the quantity and quality of bone, and spatial relationship of surrounding anatomies.8 Hence, it may help dental professionals in their decision-making for procedures or the treatment of conditions such as implant placement, oral cancer, root fracture, orthodontic traction of an impacted canine, or extraction of an impacted molar.8 In children, CBCT may be indicated for procedures such as severe dental trauma (e.g., multiple fractures, mobile fragments), developmental disorders (e.g., osteogenesis imperfecta, cleft palate), or tumours.10 Nonetheless, according to the Alberta Dental Association and College Guide for Radiation Health and Safety Program, CBCT should not be used routinely as a screening tool or as a replacement for conventional radiography.11 According to the American Dental Association, CBCT should be used as a supplement to conventional imaging techniques.12 CBCT may be used as a substitute if the dental professional determines that conventional imaging may not adequately capture the anatomic structure of interest.12
Overall, combined feedback from all survey respondents suggests that the vast majority of CBCT scans are being used for dental implantology planning in adults (Appendix 2, Table 5). CBCT is also being commonly used for the detection of impacted teeth, the detection of oral and facial cysts, tumours, and endodontic imaging in adults. With the exception of 1 respondent, survey feedback suggests that CBCT is not typically being used in infants and children younger than the age of 5. A single respondent from Manitoba reported using CBCT in infants for sinus imaging. Furthermore, respondents rarely used CBCT for children aged 5 to 9 years. The most common procedures for which CBCT is used for children 5 years to 17 years of age appear to be for the detection of impacted teeth and the detection of oral and facial cysts and tumours. Across all age groups, respondents rarely used CBCT for the detection of caries (tooth decay), gum disease detection, nasal septum imaging, and cleft palate imaging. No respondents reported using CBCT for plastic surgery, inner ear imaging, or skull and cranial imaging.
These findings are largely consistent across responses with few exceptions (Appendix 2, Tables 6 to 8). Fewer respondents in dental settings reported CBCT use in ENT or “Other” procedures. One exception is respondents in British Columbia who reported common use of CBCT in adults for mandible and jaw imaging, and temporomandibular joint (TMJ) imaging. Furthermore, CBCT was used in relatively more respondents in British Columbia compared to the other provinces for the detection of oral and facial fractures in children (5 to 17 years) and adults. Respondents in Manitoba appear to be using CBCT more commonly in adults for exploratory imaging compared with the other provinces.
In general, respondents in oral and maxillofacial surgery settings in Ontario and Prince Edward Island (Appendix 2, Tables 9 and 10) reported more common CBCT use in “Other” procedures for adults including maxillofacial surgery planning, maxillofacial surgery guidance, mandible and jaw imaging, and TMJ imaging, as compared to other provinces represented in the survey.
Respondents in dental surgery from Ontario (Appendix 2, Table 11) also reported more common use of CBCT as compared to other provinces in “Other” procedures for adults including maxillofacial surgery planning, maxillofacial surgery guidance, mandible and jaw imaging, and TMJ imaging. They also reported the common use of CBCT for exploratory imaging, dental surgery planning, and detection of oral/facial fractures in adults.
Objective 2: Professionals Conducting CBCT Scans in Dental, Oral and Maxillofacial Surgery, and ENT Settings
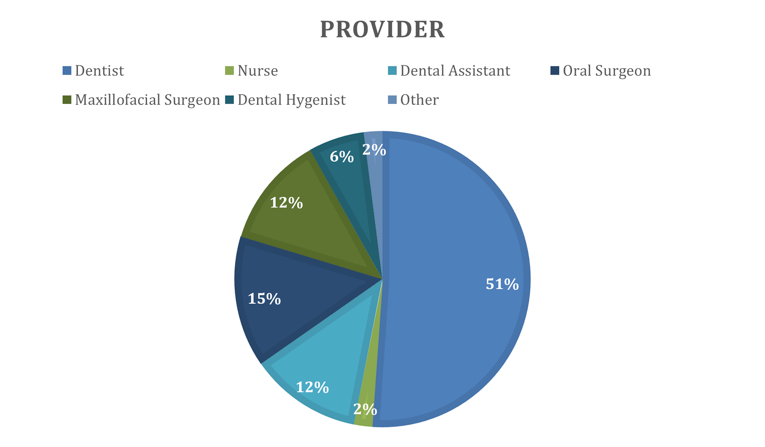
Literature on qualified professionals permitted to take CBCT scans was identified and publicly available from 4 provincial sources: Ontario, Quebec, Alberta, and British Columbia. For other provincial and territorial jurisdictions across Canada, literature was not identified or not publicly available at the time of the search. Feedback from survey respondents in Ontario, British Columbia, Manitoba, and Prince Edward Island was used to provide additional information for professionals conducting CBCT scans in dental, oral, and maxillofacial surgery and dental surgery settings (Appendix 3). Overall, results from the survey showed that dentists made up the bulk of health professionals currently conducting CBCT scans, noting that dentists represented 70% of the final survey sample. (Figure 3).
In Ontario, authorized dentists meeting educational requirements and registered medical radiation technologists under the supervision of a qualified dentist can take dental CT scans;13 dental assistants and hygienists are not allowed to operate CBCT scanners.13 This information was confirmed by survey respondents from Ontario in different practice settings. In addition, oral surgeons and maxillofacial surgeons are permitted to take CBCT scans in dental and oral and maxillofacial surgery settings.
The Ordre des dentistes du Québec published a guideline for dental professionals, which states that qualified dentists, general practitioners, and specialists can use CBCT to help in the diagnosis and evaluate the extent of disorders in dentoalveolar or craniofacial regions.14
In Alberta, registered and qualified dentists can order, acquire, and interpret CBCT scans in dental settings.11 While qualified dental assistants and hygienists can operate ionizing radiation equipment, it is unclear from this guideline if they are permitted to operate CBCT scanners.11
In British Columbia, qualified dentists can acquire and evaluate CBCT scans.15 Survey respondents also indicated that dental assistants and hygienists are permitted to take CBCT scans in dental settings. One dental clinic reported outsourcing their scanning to another location with a dedicated CBCT machine.
Dental clinics in Manitoba permit dental hygienists and dental assistants to perform CBCT scans in addition to dentists.
Information received from respondents in oral and maxillofacial surgery settings in Prince Edward Island indicate that dental assistants, oral surgeons, maxillofacial surgeons, and nurses can conduct CBCT imaging.
Based on a personal communication from a radiologist in Alberta:
CBCT imaging is increasing in Alberta. To my knowledge, CBCT is most commonly used by specialist dental groups as it is quickly becoming standard of care in orthodontic and periodontic practices. It is also being used in general dentistry. Orthopedic surgeons have also been using CBCT for intraoperative imaging. Radiologists provide ‘safety reports’ on request, assessing the CBCT images for pathology the specialist (dentist or surgeon) might miss when focused on the main pertinent clinical question. This is not mandatory in Alberta but is preferred by many groups as a way to transfer liability. (Dr. Jacob Jaremenko, Radiologist, University of Alberta Associate Professor, Edmonton, AB: personal communication, May 6, 2021).
Objective 3: Provincial and Territorial Education and Training Provisions
Literature on education and training provisions was identified and publicly available from 4 provincial sources: Ontario, Quebec, Alberta, and British Columbia. For other jurisdictions across Canada, literature was not identified or was password-protected for dental college members. In addition, survey respondents from Ontario, British Columbia, Manitoba, and Prince Edward Island provided further information regarding CBCT training requirements for their jurisdictions. Of note, as dentists represented 70% of the final survey sample, this information may not be representative of other disciplines.
The Royal College of Dental Surgeons of Ontario created a standards of practice document, which lists the education requirements for dental CT scanner operators.16 The qualification requirements differ between dentoalveolar CT scans (i.e., small field of view [FOV] scans of 8 cm or less of the teeth, supporting structures, mandible, and maxilla) and craniofacial CT scans (i.e., large FOV scans of more than 8 cm of intracranial structures, base of the skull, temporomandibular joint, paranasal sinuses, cervical spine, neck, and airway spaces).16 For dentoalveolar scans, registered dentists must complete a minimum 2-day training program with theoretical and practical components, examination, and certificate.16 For craniofacial scans, registered dentists must complete post-graduate specialist training in oral and maxillofacial radiology.16 The training program must be taught by dentists specializing in oral and maxillofacial radiology and the program must be affiliated with an accredited university.16 Furthermore, qualified dentists must complete onsite training on safe operating procedures and ensure they participate in relevant continuing education.16 Based on survey and stakeholder feedback, oral and maxillofacial surgeons may take CBCT scans after successful completion of a craniofacial CBCT course sanctioned by the Royal College of Dental Surgeons of Ontario. In addition, oral and maxillofacial surgeons must complete a mentoring program with a certified oral and maxillofacial radiologist involving the interpreting and reporting of at least 50 craniofacial CT scans.16
In Quebec, qualified dentists, general practitioners, and specialists using CBCT must have the proper theoretical and practical training, with different training durations, according to the scanning FOV.14 Specifically, qualified professionals must obtain 15 or 30 hours of training to take dentoalveolar (i.e., small FOV of 8 cm or less) or craniofacial (i.e., large FOV more than 8 cm) scans, respectively.14 The training program should cover topics such as radiation physics, operating procedures, and patient safety.14 While the Ordre des dentistes du Québec states the required aspects and duration of training programs, the qualifications of instructors and eligible training organizations were not specified.14 Similar to Ontario, CBCT users must also complete onsite training on safe operating procedures and the scanner’s reconstruction software.14 It is the permit holder’s responsibility to ensure that the clinic’s CBCT operators are qualified and trained.14
In Alberta, there are 3 tiers of training that dentists must achieve depending on their practice needs.11 The first tier of training permits dentists to take, interpret, and report on small and medium FOV CBCT scans (i.e., 10 cm or less) of dentoalveolar structures.11 The next 2 tiers of training, classified as Levels 1 and 2, pertain to large FOV CBCT scans (i.e., more than 10 cm) of craniofacial structures.11 Dentists with Level 1 training can acquire large FOV scans, while those with Level 2 training can also interpret and report on these scans.11 The Alberta Dental Association and College recommends that these training programs should be at least 1 day in duration and include theoretical and practical components.11 The training program must be appropriate and approved (e.g., University of Alberta, University of Toronto) by the Alberta Dental Association and College.11 Furthermore, similar to Ontario and Quebec, CBCT operators must also receive manufacturer-provided onsite training and engage in CBCT-related continuing education.11
In British Columbia, all staff involved with CBCT must obtain theoretical and practical training in radiological practices validated by the British Columbia Dental Association17 and maintain continuing education, especially when CBCT scanners are installed or new techniques are adopted.15 Dentists, certified dental assistants, and registered dental hygienists can all receive certification in dental radiology. For dentoalveolar CBCT scans (i.e., small FOV of 8 cm or less), clinical evaluation should be made by a specially trained dental and maxillofacial radiologist or qualified general dental practitioner.15 For non-dentoalveolar small FOV and craniofacial large FOV CBCT scans, clinical evaluations should be made by a dental and maxillofacial radiologist or medical radiologist.15 The College of Dental Surgeons of British Columbia states that training programs should be designed and taught by dental and maxillofacial radiologists.15
In Manitoba, there does not appear to be any structured training requirements in addition to professional licensure. Some of the respondents described continuing education courses and CBCT manufacturer training.
In Prince Edward Island, there does not appear to be any formal training requirements. One respondent mentioned that staff were initially trained by the CBCT manufacturer. Those staff (who have been using CBCT for more than 10 years) now train any new staff.
Objective 4: Number of CBCT Units Across Canada
No information was received from the initial query sent to provincial radiation protection agencies to help inform the number of CBCT units in their jurisdictions. However, 1 response from Ontario was received in reply to the call for stakeholder feedback on a draft version of this report. “The number of CBCT units actively used in Ontario presently are 353.” (Dr. Sangeeta Patodia, Dental Anesthesiologist, Toronto, ON: personal communication, Jun 17, 2021).
Objective 5: CBCT Models in Use in Canada
Survey respondents provided information regarding which CBCT scanner models are currently being used in their facilities. The survey also provided information as to the way in which scanner settings are being used and interpreted.
The following CBCT models were identified (24 respondents):
Carestream CS 9000 3D (2 respondents)
Carestream CS 9300 (1 respondent)
Carestream CS 8100SC 3D (1 respondent)
Carestream CS 8100 3D (2 respondents)
Dentsply Sirona Orthophos XG 3D (4 respondents)
Dentsply Sirona Orthophos XG 5 (1 respondent)
Dentsply Sirona Galileos (1 respondent)
Vatech Pax-Reve 3D Plus (1 respondent)
Vatech PaX-i3D (1 respondent)
Vatech Green CT (1 respondent)
Morita Veraviewepocs 3D R100 (1 respondent)
Morita (no model provided) (3 respondents)
i-CAT FLX (1 respondent)
i-CAT Next Generation (1 respondent)
i-CAT (no model provided) (2 respondents)
Kodak (no model provided) (1 respondent).
Most respondents (83%) indicated that CBCT scanners have imaging pre-sets that they use for the procedures they perform (Appendix 4). Less than half of respondents (43%) indicated that they have also defined their own imaging parameters for some procedures. Most of the CBCT systems being used include exposure tables (73%), which the majority of respondents (70%) found easy to understand.
Objective 6: Radiation Dose Ranges Across Procedures and Age Groups
Relevant articles from a literature search provided contextual information on radiation doses from CBCT. The survey was used to identify the radiation dose ranges being used for various procedures and patient age groups in Canada.
The amount of radiation dose a patient receives from a CBCT scan is dependent on variables such as the imaging device used and exposure parameters (e.g., FOV).12,18 The authors of the SEDENTEXCT project conducted a systematic review that identified 13 studies that used adult and pediatric anthropomorphic phantom devices to calculate dental CBCT effective dose ranges (Table 2) according to the FOV used.18 The included studies were categorized into small and medium FOV scans (i.e., dentoalveolar region that is less than 10 cm in height) versus large FOV scans (i.e., craniofacial region that is more than 10 cm in height).18 For comparison, radiation exposure from dental CBCT scans is typically higher than conventional 2-D radiography, which ranges in effective dose from less than 1.5 microsievert (µSv) for intraoral imaging to 24.3 µSv for panoramic imaging.18 However, radiation exposure from CBCT is lower than MSCT scans of the dental area, with an effective dose ranging between 280 µSv and 1,410 µSv.18
Table 2: Dental CBCT Effective Doses Calculated From Anthropomorphic Phantom Devices
Phantom device | Effective dose (µSv) from dentoalveolar scans (median dose [dose range]) | Effective dose (µSv) from craniofacial scans (median dose [dose range]) |
Adult phantom | 61 (11 to 674) | 87 (30 to 1,073) |
10 year-old phantom | 43 (16 to 214) | 186 (114 to 282) |
Adolescent phantom (age unspecified) | 32 (18 to 70) | 135 (81 to 216) |
CBCT = cone beam CT; µSv = microsievert.
Survey feedback from 11 respondents indicates that different radiation dose metrics are being used. These include dose-area product — milligray square centimetre (6 respondents); and CT dose index — milligray (3 respondents). Two respondents reported using a unit of µSv for radiation dose but were not able to provide any further information regarding how these measurements were taken. Six respondents provided the radiation dose ranges for various procedures and patient age groups. Ranges were variable depending on the procedure and patient age group, as well as the radiation dose metric used.
Table 3: CBCT Radiation Dose Provided by Survey Respondentsa,b
Exam/procedure | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||
Exploratory imaging | NR | 40 to 87 µSv | 40 to 87 µSv |
Detection of impacted teeth | 2.0263 to 5.5992 mGy.cm2c | 2.0263 to 5.5992 mGy.cm2c 40 to 87 µSv 20 to 50 µSv | 3.4905 to 3.6882 mGy.cm2c 174 to 245 mGy.cm2 40 to 87 µSv 50 to 70 µSv |
Dental treatment planning | NR | 20 to 50 µSv | 50 to 70 µSv |
Orthodontic planning | NR | 92 to 154 mGy.cm2 | — |
Endodontic imaging | NR | NR | 217 to 431 mGy.cm2 174 to 245 mGy.cm2 40 to 120 mGyc 50 to 70 µSv |
Dental implantology planning | 2.0263 to 5.5992 mGy.cm2c | 2.0263 to 5.5992 mGy.cm2c | 3.4905 to 3.6882 mGy.cm2c 92 to 627 mGy.cm2 249 to 352 mGy.cm2 20 to 60 mGyc 40 to 87 µSv 50 to 70 µSv |
Dental surgery planning | 2.0263 to 5.5992 mGy.cm2c | 2.0263 to 5.5992 mGy.cm2c 40 to 87 µSv 20 to 50 µSv | 3.4905 to 3.6882 mGy.cm2c 92 to 280 mGy.cm2 40 to 87 µSv 50 to 70 µSv |
Detection of oral/facial fractures | NR | 87 µSv | 87 µSv |
Detection of oral/facial cysts, tumours | 2.0263 to 5.5992 mGy.cm2c 5 to 30 µSv | 2.0263 to 5.5992 mGy.cm2c 87 µSv 20 to 50 µSv | 3.4905 to 3.6882 mGy.cm2c 87 µSv 50 to 70 µSv |
Ear, Nose, Throat | |||
Sinus imaging | NR | 40 to 87 µSv | 40 to 87 µSv |
Cleft palate imaging | 2.0263 to 5.5992 mGy.cm2c | 2.0263 to 5.5992 mGy.cm2c | 3.4905 to 3.6882 mGy.cm2c |
Other | |||
Mandible and jaw imaging | NR | 40 to 87 µSv 20 to 50 µSv | 40 to 87 µSv 50 to 70 µSv |
Temporomandibular joint imaging | NR | 40 to 87 µSv | 249 to 352 mGy.cm2 40 to 87 µSv 50 to 70 µSv |
Maxillofacial surgery planning | 2.0263 to 5.5992 mGy.cm2c | 2.0263 to 5.5992 mGy.cm2c 40 to 87 µSv | 40 to 87 µSv |
CBCT = cone beam CT; µSv = microsievert; mGy.cm2 = milligray square centimetre; NR = not reported.
aThe same line is used for the same respondent.
bNo respondent provided radiation dosage information for infants and children younger than 5 years of age.
cRaw data are reported as they were received. Respondents could not be reached to verify accuracy.
Limitations
The findings of this Environmental Scan present an overview of the current context of the use of CBCT in Canada based on a literature search and the perspectives of a small number of people working in the field. A systematic literature search was not conducted and the report is not intended as a comprehensive review of the topic. Furthermore, the clinical and cost-effectiveness of CBCT was not evaluated. The focus was to describe the use of CBCT in various settings. Hence, conclusions or recommendations about treatment effectiveness, cost-effectiveness, or place in therapy are outside the scope of this report. Work on this Environmental Scan began in the spring of 2020, with the literature review being conducted and completed in July of 2020. Due to the COVID-19 pandemic, survey distribution was delayed until February 2021. However, the literature review was not updated at that time.
Overall, the information gathered from the survey was limited. A potential contributing factor to the low number of survey responses was the COVID-19 pandemic, which could have restricted the time and resources required for survey response. The highest proportion of responses were received from dentists in Ontario. Although this information was invaluable, the generalizability of the findings to other disciplines (including ENT, interventional radiology, orthopedics, plastic surgery, oral and maxillofacial surgery, and dental surgery) and other provinces and territories is limited. Furthermore, the survey was only available in English, limiting the inclusion of primarily French-speaking respondents. Findings do not represent the current landscape of the CBCT use in areas of Canada where limited or no survey feedback was received. This includes Alberta, Saskatchewan, Prince Edward Island, New Brunswick, Newfoundland and Labrador, Nova Scotia, Quebec, and the 3 territories. Very little feedback was obtained regarding radiation dose ranges or the number of CBCT units in Canada.
Conclusions
This Environmental Scan was informed by a review of the literature and responses received from a survey. The majority (70.0%) of responses were received from dentists, with a smaller number of responses received from oral and maxillofacial surgeons (23.3%) and dental surgeons (6.3%). Based on the survey, dentists made up the bulk of health professionals currently conducting CBCT scans. No survey responses were received from certain disciplines including plastic surgery, orthopedics, and ENT specialists. Therefore, the extent to which CBCT is being used by these specialties in Canada is not known. According to 1 ENT physician in Alberta:
The advantages of CBCT in otolaryngology are well known. The primary advantage is ease of access. CBCT devices can easily be installed in outpatient ENT clinics and in non-hospital surgical facilities. A patient presenting with sinus issues can have a diagnostic scan at the same appointment. This scan can then be used to help with diagnosis and, particularly in ENT clinics, be used as a navigation scan for a future operation. However, there is currently no significant use of CBCT in outpatient ENT clinics in Alberta. The primary barriers are remuneration and insurance coverage. Even though an otolaryngologist can readily interpret such scans, a radiologist is currently required to review all scans in order to receive government remuneration. Furthermore, the scan is typically inexpensive when facilitated by insurance. However, very few patients have private insurance coverage for such tests. Therefore, for a private ENT clinic to operate such an instrument, it is likely that a radiology group would have to facilitate its use and integration into our existing healthcare system. However, with rising waitlists for traditional CT scans and increasing collaboration with radiology groups (i.e., MIC, Canadian Diagnostic Centres), it is possible there may be increased uptake of CBCT in outpatient ENT clinics with time. (Dr. R. Chowdhury, Otolaryngologist, University of Alberta Assistant Professor, Edmonton, AB: personal communication, Apr 14, 2021).
As CBCT delivers a higher dose of radiation compared to conventional 2-D imaging, it is important to ensure that the level of exposure to radiation is as low as possible, particularly in children who are the most sensitive to the effects of ionizing radiation. Findings from the literature in the adult population suggest that CBCT may guide dental professionals for procedures or the treatment of conditions such as implant placement, oral cancer, root fracture, orthodontic planning, or the detection of impacted teeth. Results from the survey mostly mirror this finding, with respondents reporting the majority of CBCT scans being used in adults for dental implantology planning, as well as for the detection of impacted teeth, detection of oral and facial cysts, tumours, and endodontic imaging. In children, the literature indicates that CBCT may be used for procedures such as severe dental trauma, developmental disorders (such as cleft palate), or tumours. Survey feedback suggests that CBCT is rarely used in children. With the exception of 1 respondent, CBCT is not typically being used in infants and children younger than the age of 5. Respondents rarely used CBCT in children aged 5 to 9 years. The most common procedures reported by survey respondents of CBCT being used in children 5 years to 17 years of age appear to be for the detection of impacted teeth and the detection of oral and facial cysts and tumours. Across all age groups, respondents rarely used CBCT for caries (tooth decay) detection, gum disease detection, nasal septum imaging, and cleft palate imaging. No respondents reported using CBCT for plastic surgery, inner ear imaging, or skull and cranial imaging.
A wide range of radiation dose levels associated with CBCT use were reported in the survey depending on the age group, specific procedure, and the radiation dose metric used. Educational provisions in place for CBCT operators to ensure safety and technical competence differ between the provinces, with some taking more structured approaches than others. The health professionals allowed to operate CBCT scanners also vary between provinces.
Several CBCT scanner models are currently being used in Canada. Most respondents indicated that CBCT scanners have imaging pre-sets that they use for the procedures they perform. Approximately half of respondents indicated that they have also defined their own imaging parameters for some procedures. Most of the CBCT systems being used include exposure tables, which the majority of respondents found easy to understand.
The findings of this Environmental Scan present an overview of the current context of the use of CBCT in Canada based on a literature search and the perspectives of a small number of people working in the field. CBCT use and training requirements vary in Canadian jurisdictions. However, 1 consistency seemed to be the limited use in infants and children younger than 5 years of age, who are the most vulnerable to potential negative effects of ionizing radiation. It is important for regulators to know that most respondents used the manufacturer-provided pre-sets.
References
1.U.S. Food and Drug Administration. Dental cone-beam computed tomography. 2020; https://www.fda.gov/radiation-emitting-products/medical-x-ray-imaging/dental-cone-beam-computed-tomography. Accessed 2021 Jun 2.
2.Lechuga L, Weidlich GA. Cone beam CT vs. fan beam CT: a comparison of image quality and dose delivered between two differing CT imaging modalities. Cureus. 2016;8(9):e778-e778. PubMed
3.Venkatesh E, Elluru SV. Cone beam computed tomography: basics and applications in dentistry. J Istanb Univ Fac Dent. 2017;51(3 Suppl 1):S102-S121. PubMed
4.Kamburoğlu K. Use of dentomaxillofacial cone beam computed tomography in dentistry. World J Radiol. 2015;7(6):128-130. PubMed
5.MacDonald D. Cone beam computed tomography: how can CBCT enhance patient care? CDA Essentials. 2014;1(6):31-40. https://www.cda-adc.ca/en/services/essentials/2014/issue6/index.html#31/z. Accessed 2021 Jun 2.
6.Puckett Y, Nappe TM. Ionizing Radiation. Treasure Island (FL): StatPearls Publishing; 2021 Apr 13: https://www.ncbi.nlm.nih.gov/books/NBK534237/. Accessed 2021 Jul 19.
7.The College of Physicians & Surgeons of Ontario (CPSO). Clinical practice parameters and facility standards: magnetic resonance imaging & computed tomography. 2015.
8.Adibi S, Zhang W, Servos T, O'Neill PN. Cone beam computed tomography in dentistry: what dental educators and learners should know. J Dent Educ. 2012;76(11):1437-1442. PubMed
9.Ndegwa S. Cone beam volumetric tomography for patients with dental or maxillofacial abnormalities: clinical effectiveness and guidelines Ottawa: CADTH; 2009: https://www.cadth.ca/sites/default/files/pdf/htis/J0181%20Cone%20Beam%20Volumetric%20Tomography%20final%20updated.pdf. Accessed 2020 Jun 16.
10.Kuhnisch J, Anttonen V, Duggal MS, et al. Best clinical practice guidance for prescribing dental radiographs in children and adolescents: an EAPD policy document. Eur Arch Paediatr Dent. 2020;21(4):375-386. PubMed
11.Alberta Dental Association & College. Guide for radiation health and safety program Edmonton: Alberta Dental Association and College; 2015: https://www.dentalhealthalberta.ca/wp-content/uploads/2019/09/Guide-for-the-Radiation-Health-and-Safety-Program.pdf. Accessed 2020 Jun 18.
12.The use of cone-beam computed tomography in dentistry: an advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2012;143(8):899-902. PubMed
13.Royal College of Dental Surgeons of Ontario (RCDSO). Frequently asked questions - dental radiographs. 2020; https://www.rcdso.org/en-ca/rcdso-members/practice-advisory-service/information-on-dental-radiographs. Accessed 2020 Jun 17.
14.Ordre des dentistes du Québec. Use of cone beam computed tomography in 3D mode (3D CBCT) in dental offices. Montréal: Ordre des dentistes du Québec; 2015: http://www.odq.qc.ca/Portals/5/fichiers_publication/politiques/ODQ_Tomography_Avril2015_A.pdf. Accessed 18 June 2020.
15.College of Dental Surgeons of British Columbia. Standards & guidelines: dental radiography. Vancouver: College of Dental Surgeons of British Columbia; 2015: https://www.cdsbc.org/CDSBCPublicLibrary/Dental-Radiography-Standards-and-Guidelines.pdf. Accessed 2020 Jun 18.
16.Royal College of Dental Surgeons of Ontario (RCDSO). Standard of practice: dental CT scanners. Toronto: Royal College of Dental Surgeons of Ontario; 2011: https://az184419.vo.msecnd.net/rcdso/pdf/standards-of-practice/RCDSO_Standard_of_Practice__Dental_CT_Scanners.pdf. Accessed 2020 Jun 16.
17.BC Centre for Disease Control. Guidelines on radiation protection & quality assurance applicable to dental cone beam computed tomography (CBCT). Vancouver: BC Centre for Disease Control; 2014.
18.Cone beam CT for dental and maxillofacial radiology: evidence-based guidelines. Brussels: European Commission; 2012: https://www.sedentexct.eu/files/radiation_protection_172.pdf. Accessed 2020 Jun 18.
Appendix 1: Disciplines Represented by Survey Respondents, by Province
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 4: Disciplines by Province as Per Survey Respondents (N = 30)
Province | Dentist | Oral and maxillofacial surgery | Dental surgery |
British Columbia (n = 4) | 4 | 0 | 0 |
Manitoba (n = 5) | 5 | 0 | 0 |
Ontario (n = 18) | 11 | 5 | 2 |
Prince Edward Island (n = 2) | 0 | 2 | 0 |
Alberta (n = 1) | 1 | 0 | 0 |
TOTAL (%) | 21 (70.0) | 7 (23.3) | 2 (6.7%) |
Appendix 2: Use of Cone Beam CT Exams
Note that this appendix has not been copy-edited.
Table 5: Overall Use of Cone Beam CT Exams in Canada (N = 30)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 1 (3.3%) | 2 (6.7%) |
Exploratory imaging | 0 | 0 | 2 (6.7%) | 8 (26.7%) | 13 (43.3%) |
Gum disease detection | 0 | 0 | 1 (3.3%) | 0 | 3 (10.0%) |
Detection of impacted teeth | 0 | 0 | 4 (13.3%) | 18 (60.0%) | 23 (76.7%) |
Dental treatment planning | 0 | 0 | 0 | 3 (10.0%) | 13 (43.3%) |
Orthodontic planning | 0 | 0 | 0 | 6 (20.0%) | 4 (13.3%) |
Endodontic imaging | 0 | 0 | 1 (3.3%) | 1 (3.3%) | 20 (66.7%) |
Dental implantology planning | 0 | 0 | 1 (3.3%) | 1 (3.3%) | 28 (93.3%) |
Dental surgery planning | 0 | 0 | 1 (3.3%) | 7 (23.3%) | 16 (53.3%) |
Detection of oral/facial fractures | 0 | 0 | 3 (10.0%) | 8 (26.7%) | 16 (53.3%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 6 (20.0%) | 14 (46.7%) | 20 (66.7%) |
Ear, Nose, Throat | |||||
Sinus imaging | 1 (3.3%) | 0 | 0 | 3 (10.0%) | 6 (20.0%) |
Nasal septum imaging | 0 | 0 | 0 | 1 (3.3%) | 1 (3.3%) |
Cleft palate imaging | 0 | 0 | 1 (3.3%) | 1 (3.3%) | 1 (3.3%) |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 4 (13.3%) | 9 (30.0%) |
Temporomandibular joint imaging | 0 | 0 | 1 (3.3%) | 3 (10.0%) | 12 (40.0%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 1 (3.3%) | 4 (13.3%) | 5 (16.7%) |
Maxillofacial surgery guidance | 0 | 0 | 1 (3.3%) | 1 (3.3%) | 3 (10.0%) |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 6: Use of Cone Beam CT Exams by Dentists in Ontario (n = 11)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 0 | 0 |
Exploratory imaging | 0 | 0 | 0 | 3 (27.3%) | 4 (36.4%) |
Gum disease detection | 0 | 0 | 1 (9.1%) | 1 (9.1%) | 1 (9.1%) |
Detection of impacted teeth | 0 | 0 | 1 (9.1%) | 6 (54.5%) | 7 (63.6%) |
Dental treatment planning | 0 | 0 | 0 | 2 (18.2%) | 6 (54.5%) |
Orthodontic planning | 0 | 0 | 0 | 2 (18.2%) | 1 (9.1%) |
Endodontic imaging | 0 | 0 | 1 (9.1%) | 1 (9.1%) | 10 (90.9%) |
Dental implantology planning | 0 | 0 | 0 | 0 | 10 (90.9%) |
Dental surgery planning | 0 | 0 | 0 | 2 (18.2%) | 6 (54.5%) |
Detection of oral/facial fractures | 0 | 0 | 1 (9.1%) | 3 (27.3%) | 6 (54.5%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 1 (9.1%) | 4 (36.4%) | 7 (63.6%) |
Ear, Nose, Throat | |||||
Sinus imaging | 0 | 0 | 0 | 1 (9.1%) | 3 (27.3%) |
Nasal septum imaging | 0 | 0 | 0 | 0 | 0 |
Cleft palate imaging | 0 | 0 | 0 | 0 | 0 |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 0 | 2 (18.2%) |
Temporomandibular joint imaging | 0 | 0 | 0 | 1 (9.1%) | 3 (27.3%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery guidance | 0 | 0 | 0 | 0 | 0 |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 7: Use of Cone Beam CT Exams by Dentists in Manitoba (n = 5)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 1 (20%) | 2 (40%) |
Exploratory imaging | 0 | 0 | 0 | 1 (20%) | 4 (80%) |
Gum disease detection | 0 | 0 | 0 | 2 (40%) | |
Detection of impacted teeth | 0 | 0 | 0 | 1 (20%) | 4 (80%) |
Dental treatment planning | 0 | 0 | 0 | 0 | 3 (60%) |
Orthodontic planning | 0 | 0 | 0 | 0 | |
Endodontic imaging | 0 | 0 | 0 | 0 | 4 (80%) |
Dental implantology planning | 0 | 0 | 0 | 0 | 5 (100%) |
Dental surgery planning | 0 | 0 | 0 | 1 (20%) | 3 (60%) |
Detection of oral/facial fractures | 0 | 0 | 0 | 0 | 2 (40%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 0 | 2 (40%) | 1 (20%) |
Ear, Nose, Throat | |||||
Sinus imaging | 1 (20%) | 0 | 0 | 0 | 0 |
Nasal septum imaging | 0 | 0 | 0 | 0 | 0 |
Cleft palate imaging | 0 | 0 | 0 | 0 | 0 |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 0 | 0 |
Temporomandibular joint imaging | 0 | 0 | 0 | 0 | 1 (20%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery guidance | 0 | 0 | 0 | 0 | 0 |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 8: Use of Cone Beam CT Exams by Dentists in British Columbia (n = 4)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 0 | 0 |
Exploratory imaging | 0 | 0 | 0 | 0 | 0 |
Gum disease detection | 0 | 0 | 0 | 0 | 0 |
Detection of impacted teeth | 0 | 0 | 0 | 3 (75%) | 3 (75%) |
Dental treatment planning | 0 | 0 | 0 | 0 | 1 (25%) |
Orthodontic planning | 0 | 0 | 0 | 2 (50%) | 1 (25%) |
Endodontic imaging | 0 | 0 | 0 | 3 (75%) | |
Dental implantology planning | 0 | 0 | 0 | 0 | 3 (75%) |
Dental surgery planning | 0 | 0 | 0 | 0 | 3 (75%) |
Detection of oral/facial fractures | 1 (25%) | 2 (50%) | 3 (75%) | ||
Detection of oral/facial cysts, tumours | 0 | 0 | 0 | 2 (50%) | 2 (50%) |
Ear, Nose, Throat | |||||
Sinus imaging | 0 | 0 | 0 | 1 (25%) | 1 (25%) |
Nasal septum imaging | 0 | 0 | 0 | 1 (25%) | 1 (25%) |
Cleft palate imaging | 0 | 0 | 0 | 0 | 0 |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 1 (25%) | 2 (50%) |
Temporomandibular joint imaging | 0 | 0 | 1 (25%) | 1 (25%) | 3 (75%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery guidance | 0 | 0 | 0 | 0 | 0 |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 9: Use of Cone Beam CT Exams in by Oral and Maxillofacial Surgeons in Ontario (n = 5)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 0 | 0 |
Exploratory imaging | 0 | 0 | 2 (40%) | 2 (40%) | 2 (40%) |
Gum disease detection | 0 | 0 | 0 | 0 | 0 |
Detection of impacted teeth | 0 | 0 | 2 (40%) | 5 (100%) | 5 (100%) |
Dental treatment planning | 0 | 0 | 0 | 1 (20%) | 2 (40%) |
Orthodontic planning | 0 | 0 | 0 | 1 (20%) | 1 (20%) |
Endodontic imaging | 0 | 0 | 0 | 1 (20%) | |
Dental implantology planning | 0 | 0 | 1 (20%) | 1 (20%) | 5 (100%) |
Dental surgery planning | 0 | 0 | 1 (20%) | 2 (40%) | 2 (40%) |
Detection of oral/facial fractures | 0 | 0 | 1 (20%) | 1 (20%) | 1 (20%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 4 (80%) | 4 (80%) | 5 (100%) |
Ear, Nose, Throat | |||||
Sinus imaging | 0 | 0 | 0 | 0 | 0 |
Nasal septum imaging | 0 | 0 | 0 | 0 | 0 |
Cleft palate imaging | 0 | 0 | 1 (20%) | 1 (20%) | 1 (20%) |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 1 (20%) | 2 (40%) |
Temporomandibular joint imaging | 0 | 0 | 0 | 0 | 2 (40%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 1 (20%) | 2 (40%) | 3 (60%) |
Maxillofacial surgery guidance | 0 | 0 | 1 (20%) | 1 (20%) | 3 (60%) |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 10: Use of Cone Beam CT Exams by Oral and Maxillofacial Surgeons in Prince Edward Island (n = 2)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 0 | 0 |
Exploratory imaging | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Gum disease detection | 0 | 0 | 0 | ||
Detection of impacted teeth | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Dental treatment planning | 0 | 0 | 0 | 0 | 0 |
Orthodontic planning | 0 | 0 | 0 | 0 | 0 |
Endodontic imaging | 0 | 0 | 0 | 0 | 0 |
Dental implantology planning | 0 | 0 | 0 | 0 | 2 (100%) |
Dental surgery planning | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Detection of oral/facial fractures | 0 | 0 | 0 | 2 (100%) | 2 (100%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 1 (50%) | 2 (100%) | 2 (100%) |
Ear, Nose, Throat | |||||
Sinus imaging | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Nasal septum imaging | 0 | 0 | 0 | 0 | 0 |
Cleft palate imaging | 0 | 0 | 0 | 0 | 0 |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 1 (50%) | 2 (100%) |
Temporomandibular joint imaging | 0 | 0 | 0 | 1 (50%) | 2 (100%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Maxillofacial surgery guidance | 0 | 0 | 0 | 0 | 0 |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Table 11: Use of Cone Beam CT Exams by Dental Surgeons in Ontario (n = 2)a,b
Exam/Procedure | Infants (0 months to 11 months) | Children (12 months to 4 years) | Children (5 years to 9 years) | Children (10 years to 17 years) | Adults (18 years and older) |
Dental | |||||
Caries/tooth decay detection | 0 | 0 | 0 | 0 | 0 |
Exploratory imaging | 0 | 0 | 0 | 1 (50%) | 2 (100%) |
Gum disease detection | 0 | 0 | 0 | 1 (50%) | |
Detection of impacted teeth | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Dental treatment planning | 0 | 0 | 0 | 0 | 1 (50%) |
Orthodontic planning | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Endodontic imaging | 0 | 0 | 0 | 1 (50%) | |
Dental implantology planning | 0 | 0 | 0 | 0 | 2 (100%) |
Dental surgery planning | 0 | 0 | 0 | 1 (50%) | 2 (100%) |
Detection of oral/facial fractures | 0 | 0 | 0 | 0 | 2 (100%) |
Detection of oral/facial cysts, tumours | 0 | 0 | 0 | 0 | 2 (100%) |
Ear, Nose, Throat | |||||
Sinus imaging | 0 | 0 | 0 | 0 | 1 (50%) |
Nasal septum imaging | 0 | 0 | 0 | 0 | 0 |
Cleft palate imaging | 0 | 0 | 0 | 0 | 0 |
Inner ear imaging | 0 | 0 | 0 | 0 | 0 |
Other | |||||
Mandible and jaw imaging | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Temporomandibular joint imaging | 0 | 0 | 0 | 0 | 1 (50%) |
Skull/cranial imaging | 0 | 0 | 0 | 0 | 0 |
Maxillofacial surgery planning | 0 | 0 | 0 | 1 (50%) | 1 (50%) |
Maxillofacial surgery guidance | 0 | 0 | 0 | 0 | 1 (50%) |
Plastic surgery | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey questions:
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following dental exams or procedures.”
“In your setting, please indicate the age groups (if any) for which you used CBCT in the following ear, nose, and throat (ENT) exams or “Other” exams or procedures.”
bResults are presented as the number (percentage) of respondents indicating which procedures use CBCT in different age groups.
Appendix 3: Cone Beam Computed Tomography Providers
Note that this appendix has not been copy-edited.
Table 12: Cone Beam CT Providers in Dental Settingsa,b
Province | Dentist | Dental Hygienist | Dental Assistant | Oral Surgeon | Maxillofacial Surgeon | Nurse | Other |
Ontario (n = 11) | 11 (100%) | 0 | 0 | 1 (9.1%) | 1 (9.1%) | 0 | 0 |
British Columbia (n = 4) | 4 (100%) | 2 (50%) | 2 (50%) | 0 | 0 | 0 | 1 (25%) |
Manitoba (n = 5) | 5 (100%) | 1 (20%) | 2 (40%) | 0 | 0 | 0 | 0 |
aIn response to the survey question: “In your setting, which staff members can conduct a CBCT exam? (Select all that apply).”
bResults are presented as the number (percentage) of respondents indicating which professionals conduct CBCT exams in their setting.
Table 13: Cone Beam CT Providers in Oral and Maxillofacial Surgery Settingsa,b
Province | Dentist | Dental Hygienist | Dental Assistant | Oral Surgeon | Maxillofacial Surgeon | Nurse | Other |
Ontario (n = 5) | 2 (40%) | 0 | 0 | 5 (100%) | 3 (60%) | 0 | 0 |
Prince Edward Island (n = 2) | 0 | 0 | 2 (100%) | 1 (50%) | 2 (100%) | 1 (50%) | 0 |
aIn response to the survey question: “In your setting, which staff members can conduct a CBCT exam? (Select all that apply).”
bResults are presented as the number (percentage) of respondents indicating which professionals conduct CBCT exams in their setting.
Table 14: Cone Beam CT Providers in Dental Surgery Settingsa,b
Province | Dentist | Dental Hygienist | Dental Assistant | Oral Surgeon | Maxillofacial Surgeon | Nurse | Other |
Ontario (n = 2) | 2 (100%) | 0 | 0 | 0 | 0 | 0 | 0 |
aIn response to the survey question: “In your setting, which staff members can conduct a CBCT exam? (Select all that apply).”
bResults are presented as the number (percentage) of respondents indicating which professionals conduct CBCT exams in their setting.
Appendix 4: Use of Cone Beam Computed Tomography Scanner Settings
Note that this appendix has not been copy-edited.
Table 15: Cone Beam Computed Tomography Scanner Details
System-Specific Questions | Yes | No | No Answer |
Does your CBCT system have imaging pre-sets for the procedures you perform? | 25 | 2 | 3 |
If yes, do you use the imaging pre-sets? | 25 | 1 | 4 |
Have you defined your own imaging parameters? | 13 | 14 | 3 |
Does the system labelling or manual include exposure tables? | 22 | 5 | 3 |
If yes, are the exposure tables easily understood? | 21 | 4 | 5 |
Acknowledgements: Andra Morrison, Jeff Mason, Michelle Clark
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.