CADTH Health Technology Review
Using Health Care Resources Wisely After the COVID-19 Pandemic: Recommendations to Reduce Low-Value Care
Report
Authors
Sinwan Basharat, MSc, Program Development Officer (CADTH)
Karen Born, MSc, PhD, Knowledge Translation Lead (Choosing Wisely Canada)
Contributors
The authors are grateful to CADTH staff Heather Logan; Tasha A. Narain, MSc; Deirdre DeJean, PhD; Nicole Mittman, MSc, PhD; and Choosing Wisely Canada members Wendy Levinson, MD; Tai Huynh, MDes MBA; and Stephanie Callan, BA, for their involvement in this expert panel, including providing feedback on the content of this report.
Panellists
These individuals were panellist participants and kindly provided comments on this report:
Adina Weinerman MD, FRCPC, MHSc
Medical Director, Quality and Patient Safety
Sunnybrook Health Sciences Centre
Toronto, Ontario
Alexander Singer, BSc, MB BAO BCh, CCFP
Director, Office of Research and Quality Improvement
University of Manitoba, Winnipeg, Manitoba
Christy Simpson, PhD
Department Head and Associate Professor
Department of Bioethics, Dalhousie University
Halifax, Nova Scotia
Cindy Dumba
Patient Partner
Saskatchewan Health Authority and Partner Choosing Wisely
Regina, Saskatchewan
Johanna Trimble
Patient Champion
Patients for Patient Safety Canada
Roberts Creek, British Columbia
Maggie Keresteci, MA, CHE
Executive Director
Canadian Association for Health Services and Policy Research
Toronto, Ontario
Patrick Quail, MB
Medical Leader Supportive Living
Alberta Health Services Calgary Zone
Calgary, Alberta
Sophia Ikura, BScN, MPA
Executive Director
Health Commons Solutions Lab
Toronto, Ontario
Susan Shaw, MD
Chief Medical Officer
Saskatchewan Health Authority
Saskatoon, Saskatchewan
Wm. Kenneth Milne, MD
Adjunct Professor
Schulich School of Medicine and Dentistry, Western University
London, Ontario
Conflicts of Interest
Three expert panellists declared conflicts of interest as listed below, whereas all other participants had no conflicts of interest to declare that were relevant to this report. One panellist received payments from Canadian Blood Services as an advisor, one panellist received research funding from IBM for Natural language processing, and one panellist has a family member who is a former employee of Health Quality Ontario
Key Messages
Low-value tests, treatments, and procedures are an important health care quality problem in Canada and across the world because they provide little clinical benefit, may be harmful for patients, and waste limited resources.
Due to the COVID-19 pandemic, health care systems face increased challenges of limited resources, reduced capacity, and a growing backlog of surgeries and other procedures. The pandemic has compelled health care professionals to make challenging decisions to prioritize health care services while coping with increased demand.
As Canada emerges from the pandemic and health care systems rebuild and begin to address the backlog of delayed or cancelled services, there is an imperative to introduce lasting changes to reduce low-value care and ensure high-quality care is available to everyone.
To help inform efforts for using health care resources wisely and to support decision-making, CADTH and Choosing Wisely Canada convened a 10-member multi-disciplinary panel of clinicians, patient representatives, and health policy experts to review areas of low-value care that can be reduced or limited. This panel reviewed, deliberated, and prioritized 19 recommendations of the more than 400 Choosing Wisely Canada recommendations, the implementation of which can help ensure high-value care after the pandemic.
Examples of the 19 recommendations include:
Avoiding unnecessary transfers for patients in long-term care to hospitals unless there is an urgent medical need.
Limiting blood tests and imaging unless required to answer a specific clinical question or guide treatment.
Not transfusing red blood cells for hemodynamically stable patients in the intensive care unit.
Not delaying palliative care for patients with serious illness because they are pursuing disease-directed treatment.
Moreover, the panel’s discussion highlighted how the selected recommendations can advance key priorities, including improving health equity and access to care, appropriately using limited resources, emphasizing patient-focused care, and addressing challenges the pandemic has presented for long-term care.
Background
Choosing Wisely campaigns in Canada and around the world have raised awareness about the problem of overuse or low-value interventions in health care. These are tests, treatments, and procedures that may provide little to no clinical benefit, waste limited resources, and may even be harmful to patients.1,2 Choosing Wisely Canada (CWC) was established in 2014 as a clinician-led effort to raise awareness about overuse in health care.3 CWC is the national voice on overuse, and has built an evidence base and several initiatives to support and enable change across the health care landscape.4,5 The campaign has extensive reach and engagement across clinician groups, including physicians, nurses, dentists, pharmacists, and other allied health care professionals in Canada.6
One of the key efforts of CWC has been to bring together national clinician societies to develop evidence-based recommendations of low-value tests, treatments, and procedures to question. To date, more than 400 recommendations have been developed by engaging with societies, patients, and the public, along with clinical evidence reviews, working group deliberations, and practitioner surveys. Recommendations are reviewed annually to incorporate emerging evidence and knowledge.7
The aim of the recommendations is to improve health care quality and patient safety by reducing low-value tests, treatments, and procedures.8 In some cases, low-value care may lead to adverse events or further testing, which may increase anxiety for patients and caregivers and increase the likelihood of false-positives or other preventable harms.8,9
Need for Further Progress in Reducing Low-Value Care
However, there is a gap between evidence and practice. In 2017, the Canadian Institute for Health Information (CIHI) analyzed health system data associated with 8 key campaign recommendations related to different tests, treatment, and procedures across several clinical settings. Their report found that up to 30% of the tests, treatments, and procedures in Canada related to the 8 selected recommendations may be low value and offer no clinical benefit to patients.9
An illustrative example of the gaps between evidence and practice is a CWC recommendation against ordering diagnostic imaging for people with uncomplicated lower back pain who do not exhibit other red flags (e.g., including but not limited to people with cancer, a recent infection, or a fracture).7,10 Evidence from a systematic review reaffirms that routine imaging does not lead to any better pain or well-being outcomes, but rather exposes people to unnecessary radiation, may increase the number of downstream tests, and can increase anxiety and worry.11 However, despite this evidence-based recommendation, it was found that 30% of patients with uncomplicated lower back pain received potentially unnecessary diagnostic imaging in 1 Canadian jurisdiction.12
Clinicians report that CWC recommendations help identify specific tests, treatments, and procedures that are overused and offer no clinical value, yet implementing these recommendations across health care systems is a challenge.13 Developing and disseminating evidence-based lists of recommendations is a first step that can drive sustained changes to practice.14 Research from Canada and the US also highlights that awareness campaigns for clinicians to change their practices that are tied to policies to support these changes are more likely to drive sustainable reductions in low-value care.15,16
Addressing the problem of low-value care also requires understanding barriers that clinicians and health systems can face when implementing change. Practice habits, perceptions of patient demands, and clinical environments can create barriers to reducing low-value care.13,17,18 As such, CWC’s framework for reducing low-value care identifies and considers potential barriers and facilitators for implementing recommendations.14
Impetus for Change in Post-Pandemic Health Care
The COVID-19 pandemic has claimed thousands of lives, drawn attention to persistent inequities in access to care and outcomes, and has emphasized an imperative to improve health care systems.19,20 As Canada emerges from the pandemic and health systems rebuild, there are opportunities to learn from the rapid changes put in place to address urgent short-term pandemic needs which may improve health care in the long term. For example, the pandemic rapidly brought on changes to virtual care that are likely to continue to improve access.21,22 Similarly, the temporary pause and delay of many potentially unnecessary procedures may facilitate health care professionals to re-assess and evaluate different health care services that may be low value yet common practice before the pandemic.23 This evaluation is particularly important as health care systems face resource constraints while having to support the increased health needs of the population.24,25
Since March 2020, hospitals in different parts of the country have had to make difficult decisions about deferring or limiting different procedures. These measures were taken to ensure there was enough capacity to provide care for patients with COVID-19, support public health directives, and reduce the likelihood of exposing patients and health care professionals to the virus.26 In April 2020, coronary artery bypass graft surgeries were reduced by more than 40% compared with the start of the year, and cataract and knee replacement procedures were nearly halted altogether.27 Overall, surgeries between March and June 2020 were reduced by 47% compared with the previous year.28
It is estimated that clearing the backlog of procedures in various jurisdictions will require considerable time and resources. In Ontario, estimates show it may take between 0.9 years to 2.8 years to clear the backlog of surgical procedures alone.29 In British Columbia, it may take approximately 2 years to clear the backlog of surgeries.30 The total cost for clearing the backlog by August 2021 for 6 of the most affected procedures and imaging tests across Canada is estimated to be more than $1.3 billion dollars.27
In spring 2021, more than a year after the pandemic began, many Canadian jurisdictions are in the midst of a third wave with sharply rising COVID-19 cases and unprecedented challenges to health care system capacity. This third wave has further added to the backlog of other health procedures.31 The pause and re-prioritization of many procedures during the pandemic has spurred a careful assessment of all health care services to ensure resources are deployed to those who need it most.23 Although many low-value services have been reduced for the time being, enabling sustainable change for limiting low-value care requires a concerted effort assessing the value of health care services.25 As health care systems emerge from the pandemic, prioritizing high-value care services can help to manage the demands on limited health care resources and also help efficiently address the backlog. CWC released a policy document in the fall of 2020 highlighting 5 policy ideas to reduce low-value care in the midst of and after the pandemic.25 Rebuilding from the pandemic can also be informed by campaign recommendations and a broader conversation with and consensus from health care professionals, patients, and decision-makers for whom these recommendations may be the most relevant and impactful in the post-pandemic era.
Objective
CADTH and CWC convened an independent panel of clinicians, patient representatives, and health policy experts to assess and prioritize low-value health care recommendations in the context of post-pandemic health systems. The panel voted and deliberated on these recommendations and highlighted the ones that, based on their assessment, could have the most impact in reducing low-value care in health care systems across Canada after the pandemic.
Approach
Developing a Short List of Recommendations
In February 2021, 2 members of CWC’s leadership team reviewed the 400 recommendations developed by national clinician societies.7 CWC members used their expertise to narrow down the 400 recommendations to a short list of 45 that are likely to have the greatest impact as Canada emerges and health care systems rebuild from the COVID-19 pandemic.
Four criteria were considered in selecting recommendations for the short list. These recommendations addressed tests, treatments, and procedures that:
are common in clinical practice, may cause harm, and/or are resource intensive
are associated with an area of need delayed by the pandemic or where there is an existing backlog
can lead to potential strains on health care human resources and system capacity
are aligned with categories of overuse identified and measured by CWC and CIHI: hospital care, primary care, long-term care, oncology care, end-of-life care, specialist or outpatient care, and the use of blood products.9
Panel Selection
CADTH and CWC brought together a multi-disciplinary expert panel to prioritize and assess the short list of 45 recommendations. Panel members were chosen with both geographic and gender considerations in mind. As well, clinicians from diverse areas of practice, including emergency medicine, internal medicine, family medicine, geriatric care, and intensive care, were represented. Policy expert members were selected based on their experience with either developing or advising on health policy, with at least 1 person with expertise in health ethics. Patient representatives were chosen to reflect a diversity of experiences across health care systems.
The 10-member panel consisted of 5 clinicians, 3 health policy experts, and 2 patient representatives from 6 provinces (Table 1). All panel members were aware of CWC’s campaign and focus on low-value care. All panel members were also required to comply with existing CADTH policy regarding disclosure and management of conflicts of interest.
Role | Name | Background |
Clinicians | Milne, Wm. Ken | Emergency physician and Adjunct Professor of Medicine, Schulich School of Medicine and Dentistry, Ontario |
Quail, Patrick | Family physician and Medical Leader, Supportive Living, Alberta Health Services, Alberta | |
Shaw, Susan | Anesthesiologist and Chief Medical Officer, Saskatchewan Health Authority, Saskatchewan | |
Singer, Alexander | Family physician and Director of Research and Quality Improvement, University of Manitoba, Manitoba | |
Weinerman, Adina | Internist and Medical Director, Quality and Patient Safety, Sunnybrook Health Sciences Centre, Ontario | |
Health policy experts | Ikura, Sophia | Executive Director, Health Commons Solution Lab, Ontario |
Keresteci, Maggie | Executive Director, Canadian Association for Health Services and Policy Research (CAHSPR); caregiver; Ontario | |
Simpson, Christy | Head and Associate Professor, Department of Bioethics, Dalhousie University, Nova Scotia | |
Patient representatives | Dumba, Cindy | Patient partner, Choosing Wisely Canada, Saskatchewan |
Trimble, Johanna | Patient champion, Patients for Patient Safety Canada, British Columbia |
Step 1: Online Survey Process
Prior to the panel meeting, panel members were given 5 work days to complete an online survey. The purpose of the survey was to indicate whether, in their opinion, each of the 45 short-listed recommendations should or should not be included in the final list of recommendations for reducing low-value care post-pandemic. Panel members also had the option to select “maybe/unsure” and to provide any open-ended comments. Panellists were asked to consider the same criteria used by CWC as the basis of their decisions.
Step 2: Panel Deliberation
The survey results showing the detailed breakdown of each recommendation and the level of consensus were shared with the panellists. After this, a virtual panel meeting was held on April 15, 2021, to review the recommendations with the highest level of consensus. This meeting was co-facilitated by CADTH and CWC.
During the meeting, the panel was asked to discuss recommendations that had consensus from at least 8 out of 10 members (i.e., high consensus) and additional recommendations that had less consensus (i.e., fewer than 8 out of 10 members) but were flagged by individual members as warranting further discussion. Two panel members also examined the full list of 400 recommendations and suggested 12 recommendations not on the shortlist that could also be considered, but only 1 recommendation was flagged for review.
Live voting was held during the panel meeting to re-assess the level of consensus for recommendations that had detailed discussions. Live voting was not used for recommendations with high agreement that did not have any detailed discussion; the survey results were considered sufficient to represent the level of consensus.
The final list consists of those recommendations which had consensus from at least 8 out of 10 members (80%). Conventional content analysis32 was used to develop qualitative themes to structure the findings from the panel discussion and to provide further context, rationale behind the panel’s decisions, and considerations for implementation.
Findings
Step 1: Online Survey Results
All panellists responded to the survey and the results indicated a high level of consensus (i.e., at least 8 out of 10 members or 80%) for 14 out of 45 recommendations. Of these, 3 recommendations had consensus from 9 members (90%), but there were no recommendations with unanimous support. Additionally, 18 recommendations had consensus from 7 out of 10 members (70%). Figure 1 shows the total number of recommendations by clinical area and the level of panel consensus in the survey.
Figure 1: Number of Recommendations in Each Clinical Area Based on Level of Panel Consensus (N = 45 Recommendations)
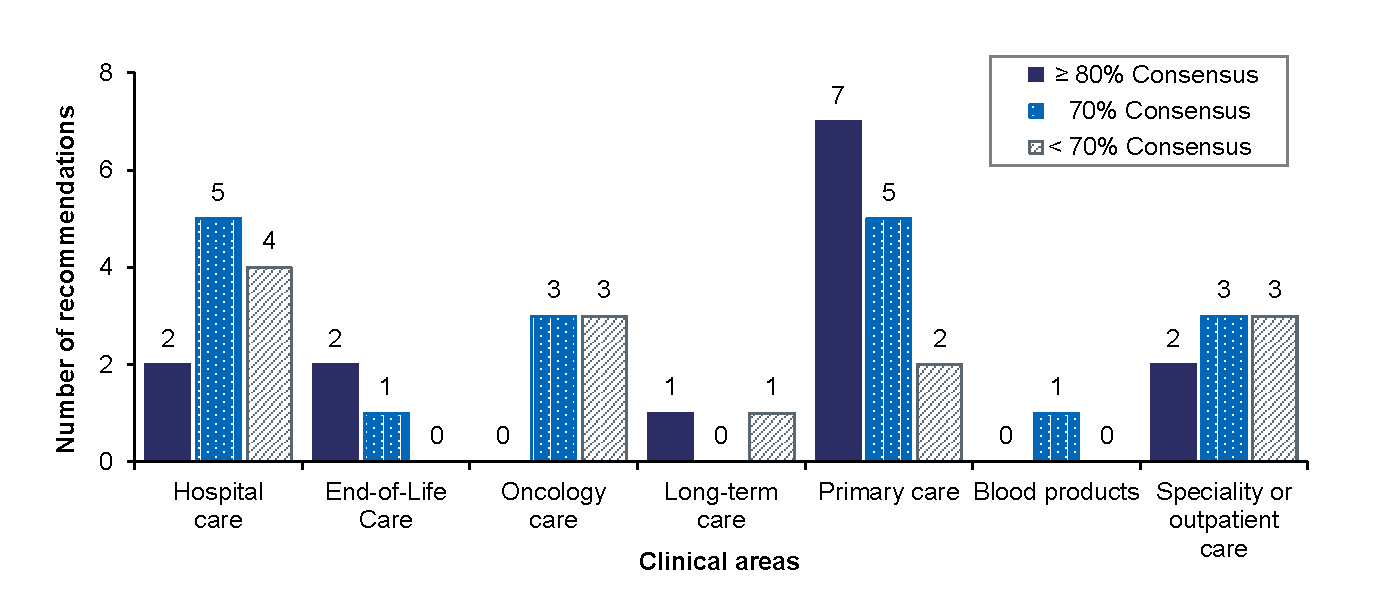
Note: Voted “should be included” in the survey.
Half of the primary care recommendations (7 out of 14) and most of the end-of-life care recommendations (2 out of 3) had a high level of consensus in the survey. Hospital and specialty or outpatient care also had 2 recommendations each with high consensus. For some recommendations with less consensus (less than 80% consensus), panel members indicated in the open comments that they were unsure about the recommendation or felt it should not be included because the recommendation seemed too specific and may have limited impact in reducing low-value care across health care systems. Likewise, they indicated that other recommendations seemed too general for this current prioritization and, although important, they may not be a pressing priority for improving care post-pandemic.
Step 2: Panel Deliberation
Because of the high degree of consensus in the online survey results, the panel meeting was structured to provide discussion of 22 of the 45 short-listed recommendations. These 22 recommendations had 80% or higher consensus (n = 14), had lower consensus but were flagged by 1 or more panel members (n = 7), or were not part of the original short list but were still flagged (n = 1) to be included in the deliberation.
Final Recommendations After Panel Deliberation
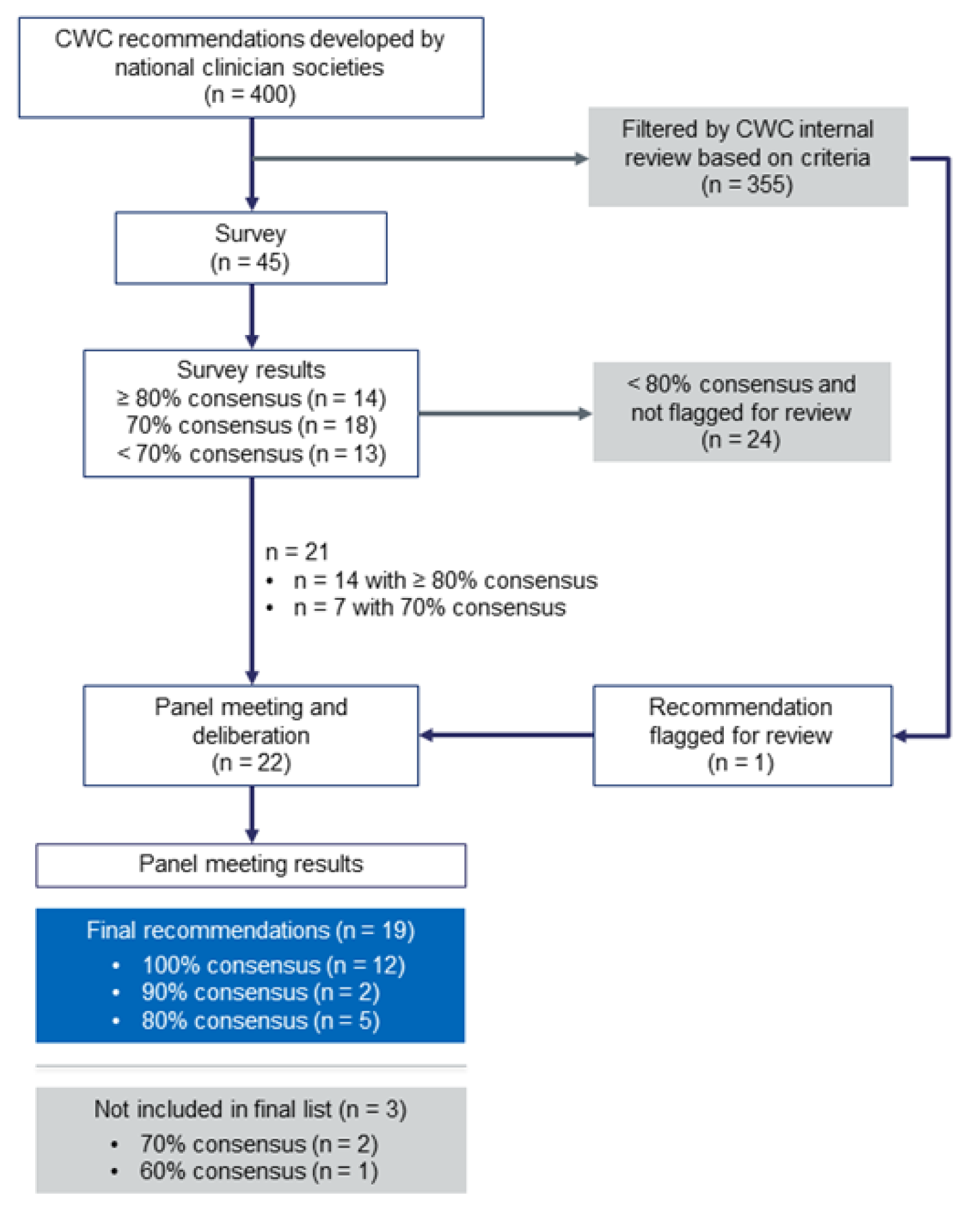
Figure 2 provides the overview of the selection process starting from the list of 400 recommendations to the survey results, deliberation, and the final list following the panel meeting.
Of the 22 recommendations reviewed during the panel meeting, the panellists did not discuss 5 of them. These recommendations already had consensus from at least 8 out of 10 panel members based on the survey and the panellists had no reservations against them being included in the final list. The panel discussed each of the remaining 17 recommendations and held a live vote during the virtual meeting following the discussions.
Based on the live vote and the survey results of the 5 recommendations that did not require extensive discussion, 12 recommendations had unanimous consensus to be included in the final list, 2 had 90% consensus, and 5 had 80% consensus. In total, the panel had high consensus for 19 final recommendations for reducing low-value care in post-pandemic health care. Table 2 shows the final list of recommendations.
Three recommendations were not included in the final list because they only had consensus from 6 or 7 members (i.e., less than 80%) after the live vote. Table 3 and Table 4 in Appendix 1 show the complete voting results of the panel.
Table 2: Top 19 Choosing Wisely Canada Recommendations to Reduce Low-Value Care After the Pandemic
Clinical area | Category | Recommendation |
Hospital care | Routine investigations | Don't order routine investigations, including chest radiographs or blood tests, in critically ill patients except to answer a specific clinical question. |
Preoperative testing | Don’t order baseline laboratory studies (complete blood count, coagulation testing, or serum biochemistry) for asymptomatic patients undergoing low-risk non-cardiac surgery. | |
End-of-life care | Advance care planning conversations | Don’t start or continue life-supporting interventions unless they are consistent with the patient’s values and realistic goals of care. |
Don’t delay advance care planning conversations. | ||
Palliative care | Don’t delay palliative care for a patient with serious illness who has physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment. | |
Specialty or outpatient care | Nephrology | Don’t initiate chronic dialysis without ensuring a shared decision-making process between patients, their families, and their nephrology health care team. |
Gastroenterology | Avoid performing a colonoscopy for constipation in those under the age of 50 years without a family history of colon cancer or alarm features. | |
Cardiology | Don’t perform stress cardiac imaging or advanced non-invasive imaging in the initial evaluation of patients without cardiac symptoms unless high-risk markers are present. | |
Orthopedics | Don’t order a knee MRI when weight-bearing X-rays demonstrate osteoarthritis and symptoms are suggestive of osteoarthritis as the MRI rarely adds useful information to guide diagnosis or treatment. | |
Long-term care | Transfer | Don’t send the frail resident of a nursing home to the hospital unless their urgent comfort and medical needs cannot be met in their care home.a |
Blood products | Red blood cells transfusion | Don’t routinely transfuse red blood cells in hemodynamically stable ICU patients with a hemoglobin concentration greater than 70 g/L (a threshold of 80 g/L may be considered for patients undergoing cardiac or orthopedic surgery and those with active cardiovascular disease). |
Oncology | Palliative | Don’t delay or avoid palliative care for a patient with metastatic cancer because they are pursuing disease-directed treatment. |
Primary care | Rural transfer | Don’t send a patient for a specialist visit that requires several hours of transport if the visit can be done virtually or by a local physician. |
Annual examinations | Don’t do annual physical exams on asymptomatic adults with no significant risk factors.b | |
Unnecessary screening tests | Don’t perform population-based screening for 25-OH-vitamin D deficiency. | |
Unnecessary imaging | Don’t order screening chest X-rays and ECGs for asymptomatic or low-risk outpatients. | |
Don’t do imaging for lower back pain unless red flagsb are present. | ||
Don’t do imaging for uncomplicated headache unless red flagsb are present. | ||
Don’t order a CT scan for uncomplicated acute rhinosinusitis. |
CT = computed tomography; ECG = electrocardiogram; ICU = intensive care unit; MRI = magnetic resonance imaging.
aThis recommendation was not included in the short list of 45 recommendations; however, it was added after it was flagged for consideration.
bSpecific risk factors or red flags may vary based on clinical assessment. See Choosing Wisely Canada’s detailed guide on Family Medicine.33
Qualitative Review of Recommendations
During the virtual panel meeting, members discussed their decision-making process for selecting or not selecting certain recommendations. They also shared their knowledge and insights related to the different recommendations and implementation considerations, which informed the panel, their deliberation, and live voting. The major themes discussed by the panel included a focus on the relative impact of recommendations, health equity, patient-focused care, and challenges facing long-term care homes.
Focus on the Relative Impact of Recommendations
Several panel members expressed that many, if not all, of the recommendations that they reviewed in the short list were important and could help contribute to reducing low-value care overall. However, to develop the final list, they focused on the potential impact of recommendations to support decision-making in the context of providing care during and following the pandemic. As such, they prioritized recommendations that ensure limited health care resources are appropriately used and can be directed to areas of most need effectively and efficiently. Panellists also appreciated that there will be significant regional variation driven by local context on the extent of pandemic-related backlogs and what is possible or needed to shift patterns of care.
Similar to the criteria set out by CWC for developing the short list, panel members primarily considered how commonly specific tests or procedures were being performed and the number of people it would likely affect. They stated that the health care services that are performed more commonly are likely to affect a larger number of people and these were given a higher rating. Alternatively, services that are performed less frequently but still place high-demand resources under constraint could also have wider system-level impact. For example, although unnecessary blood transfusions show evidence of decreasing in Canada, blood products are a highly scarce resource, particularly during the pandemic, and waste still occurs.9,34 Similarly, unnecessary imaging puts increased demand on limited resources — resources that are and will be needed to address backlogs.9 Therefore, adopting recommendations that reduce the unnecessary use of high-frequency services or high-demand resources were given priority because they may have a greater impact on the overall health system and access to care for patients.
One panel member also said that they chose to make their prioritization decisions for health care services that often require multiple contact points or contribute to a cascade of additional tests because that would help to reduce not only low-value care but also the potential exposure to the SARS-CoV-2 virus. Recommendations related to primary care, which often serves as a gateway to the health care system and downstream tests, received high consensus from the panel. More than a third (7 out of 19) of the recommendations in the final list are associated with primary care. Panel members acknowledged that the relative impact on reducing low-value care would vary among these 7 recommendations in primary care. For example, recommendations against imaging for lower back pain and CT scans for uncomplicated acute rhinosinusitis were both included in the final list. However, because the former is a much more prevalent than the latter, it would likely have a greater impact on the overall system.
Several other recommendations on the final list were part of clinical areas that tend to have a greater emphasis on procedures. For example, unnecessary dialysis in nephrology and unnecessary colonoscopy in gastroenterology had unanimous consensus from the panel. Reducing low-value procedures could help address the backlog of deferred procedures and may have a large impact in freeing up high-demand resources.
Reducing Low-Value Care Is Important for Health Equity
Throughout the discussion, panel members acknowledged that reducing low-value care has important implications for health equity. These concerns were reflected in the comments by a panel member who stated, “Many of our equity-seeking populations may look at this list and have a concern that ‘Does it mean I am going to receive less care? Are decisions being made about what I will and will not get?’”
In Canada, there are underserved populations and groups who need more access to care, rather than less, so communicating the rationale for the final recommendations is critical. The panel stated that as practitioners adopt these recommendations, there is a corresponding need for health care decision-makers to emphasize that reducing low-value care is positioned to help improve health equity by reducing waste and freeing up capacity. The recommendations ensure that health care resources are distributed appropriately and remain accessible to the people who need them the most. This includes addressing disparities in access to care people in rural and remote areas and other underserved groups. During and after the pandemic, promoting the appropriate use of tests, treatments, and procedures helps ensure these services are accessible to everyone when needed.
The panel also unanimously supported the recommendation related to unnecessarily transferring patients from rural communities to urban centres for specialist visits if a visit could be done virtually or by a local physician. Panel members who live or work in rural settings discussed how many patients are required to travel for specialist visits against their preference of receiving care in their communities and who often incur out-of-pocket expenses.35 In terms of health equity, panellists also shared examples from case studies which highlighted that virtual services, when appropriate and suitable, may even improve access to specialist care.36,37 Therefore, reducing unnecessary transfers may contribute to improving equity and reducing waste.
Need for Emphasis on Patient-Focused Care
Panel members discussed that those recommendations that encourage shared decision-making conversations between clinicians, patients, and caregivers can play an important role in reducing low-value care. These conversations are especially important for avoiding overuse at the end of life and ensuring high-quality care for those with serious illness. Recommendations that suggest “not delaying” specific interventions, and having those conversations early, may help limit a cascade of low-value care later. The panel also noted that advance care planning conversations can take place with many health care professionals, and not just physicians. All 3 advance care planning recommendations had high consensus from the panel as being important in post-pandemic health care and were included in the final list.
Although the panel showed strong consensus for palliative care recommendations, they also described some challenges and opportunities that may need to be considered based on local context. Palliative care can be limited in many settings, particularly in rural and remote regions. Capacity may be also stretched due to the pandemic.38 However, 1 panel member remarked that if more resources are provided for palliative care, it could improve system-level efficiencies on the whole and be better for patients and caregivers. They stated,
While we know palliative care resources are limited, I also think that if there is a way to stop doing some other things, that may help provide more resources for palliative care. Or, if some patients can receive palliative care sooner, it opens up space for those advanced care planning discussions and better symptoms control. Patients are then also not coming back to the hospital through emergency care.
Challenges Facing Long-Term Care
Recommendations related to long-term care spurred significant discussion among the panel. As the COVID-19 pandemic has disproportionally affected residents of long-term care, it has also disrupted the way residents, families, and clinicians in long-term care use health care system resources.39 Based on initial survey results, a recommendation related to abstaining from placing feeding tubes in people with advanced staged dementia in long-term care homes had high consensus (80%) to be included on the final list. However, after further discussion during the panel meeting, this recommendation received less consensus because only 6 out of 10 members agreed it should be on the final list.
Panel members who wanted to discuss this recommendation stated that they did not have reservations inherently against the recommendation. It is supported by clinical guidelines and evidence reviews which show that feeding tubes for patients with dementia, do not provide clinical benefits and may in some circumstances be harmful.40 Panellists were also cognizant that, during the pandemic, staff resources at long-term care homes have been constrained and, in most places, family and caregiver restrictions have been in place. In these circumstances, additional supports may be needed to support residents with oral feeding rather than encouraging feeding tubes.
However, 1 panel member with clinical expertise in long-term care stated that inserting feeding tubes was not a common practice across the country. This panellist also shared a data report from CIHI showing that the prevalence of residents on feeding tubes in long-term care homes was low (between 2% and 7%) across the country, except in 2 jurisdictions.41 In the panellist’s specific practice experience, they noted that feeding tubes are often placed in the hospital setting before a resident is admitted to a long-term care home, and primarily for those people affected by a stroke. As such, the panellists who were against including the recommendation in the final list suggested that placing feeding tubes specifically within long-term care homes may not be a pressing priority across the whole country, although it could still be important to focus on in certain areas.
One panel member, who acknowledged they had less experience with long-term care, noted that they originally voted in the survey based on the inherent rationale of the recommendation. However, after hearing that it may not be a common practice everywhere, they had concerns it may be misinterpreted as being a priority area or aspect that needs to be specifically reinforced for post-pandemic care.
Although this did not make the final list, another panel member emphasized they had concerns and worry about how staff constraints at long-term care homes could affect the usage of feeding tubes in the future. They said,
[Inserting feeding tubes] is not a very common practice, then when you see the chart with regional variation, it is definitely happening in parts of the country where it should not be happening. And then the question is, how do you best prevent that from occurring, particularly in a post-pandemic era when there may be a lot fewer staff within long-term care?
The panel emphasized that despite not making the final list, the practice of feeding tubes for residents with dementia should not be promoted. Moreover, the panel noted that decisions around placing feeding tubes should be part of advance care planning.
One recommendation related to long-term care was included in the final list. This recommendation was added to the panel discussion after being flagged for consideration. Despite not being on the original short list and the survey, the recommendation was unanimously supported by the panel after the discussion. The recommendation was against sending residents from a nursing home unnecessarily to the hospital. Panellists who flagged the recommendation shared insights that when residents in long-term care are transferred to hospitals, they may receive low-value care and medications, be exposed to infections, and may have worse overall outcomes within the hospital setting.42-44 As such, adopting this recommendation could help improve outcomes for long-term care residents and reduce demand of critical resources within hospitals.
Discussion
Low-value tests, treatments, and procedures are common across Canadian health care systems, with consequences for patient outcomes and resource use.9 As Canada emerges and rebuilds from the COVID-19 pandemic, addressing overuse is imperative for ensuring resources are used wisely.25,26 To respond to the pandemic, heath care systems have postponed or cancelled various tests, treatments, and procedures. As they are reintroduced, reducing low-value care can help free up vital capacity that can address a growing backlog and the increasing health care needs of the population.25 In the period of rebuilding health care systems after the pandemic, implementing sustainable and long-lasting changes that address low-value care is possible.
To highlight key recommendations that can make a sustainable impact on post-pandemic health care systems, CADTH and CWC convened an independent and multi-disciplinary expert panel of clinicians, patient representatives, and health policy experts. Following refinement of a short list developed by CWC internal reviewers, the panel responded to a survey, deliberated, and came to a high consensus for 19 key recommendations. These recommendations cover a range of clinical areas and settings, including hospitals, primary care, and long-term care homes. The panel selected these recommendations based on their assessment that adopting these priority recommendations may have the most impact in reducing low-value care and the strain on health systems across Canada due to the pandemic. The panel’s discussion provided further context about how these recommendations may have important considerations for health equity and access to care, health resources, patient-focused care, and the challenges the pandemic has disproportionally presented for long-term care homes.
Limitations
The overall process was designed exclusively to prioritize the more than 400 CWC recommendations. There are potentially many more types of low-value care that could be reduced after the pandemic that were not considered.
Findings from the independent panel were not based on a quantitative analysis comparing the relative value of the CWC recommendations. Rather, they were assessed based on the panel’s expertise related to clinical care, patient experience, and health policy. Although panellists had diverse sets of knowledge and experience, deliberations did not include detailed information or data about specific usage rates of different health care services and cost-benefit implications. Direct measurement of low-value care and its impact on health systems, irrespective of the pandemic, is a complex assessment and was beyond the scope of this panel.45
Panel members also acknowledged it was difficult for them to forecast what would be the critical areas of improvement following the pandemic. However, similar consensus-building approaches among experts have been used previously to prioritize areas of low-value care to support decision-making.46
Implications for Implementation
These 19 recommendations provide a focus for areas where low-value care can be reduced or eliminated in post-pandemic health care systems. Health care professionals across the country can use this list to support decision-making and ensure high-value care is provided to patients. Regional variation and local context are important factors that may influence the relevance of these selected recommendations. In some jurisdictions, substantial efforts may have already occurred for reducing specific low-value tests, treatments, or procedures included in the final list. Therefore, the final list of recommendations serves as a guide for developing priorities, which will be based on local circumstances. The full list of more than 400 recommendations developed by national clinician societies can be consulted to identify additional ways to use health care resources wisely.
References
1.MacLeod S, Musich S, Hawkins K, Schwebke K. Highlighting a common quality of care delivery problem: Overuse of low-value healthcare services. J Healthc Qual. 2018;40(4):201-208. PubMed
2.OECD. Tackling wasteful spending on health. Paris: OECD; 2017: https://www.oecd.org/health/tackling-wasteful-spending-on-health-9789264266414-en.htm. Accessed 2021 May 6.
3.Choosing Wisely Canada. About Choosing Wisely Canada. 2020; https://choosingwiselycanada.org/about/. Accessed 2021 Mar 29.
4.Hurley R. Can doctors reduce harmful medical overuse worldwide? BMJ. 2014;349:g4289. PubMed
5.Born KB, Levinson W. Choosing Wisely campaigns globally: a shared approach to tackling the problem of overuse in healthcare. J Gen Fam Med. 2019;20(1):9-12. PubMed
6.Stern SJ, Holbrook A, Patel M, Hillis C, Patel A. Assessing physician awareness of the Choosing Wisely Canada recommendations. Canadian Journal of General Internal Medicine. 2017;12(3).
7.Choosing Wisely Canada. Recommendations and resources, by specialty. 2020; https://choosingwiselycanada.org/recommendations/. Accessed 2021 Mar 29.
8.Brownlee SM, Korenstein D. Better understanding the downsides of low value healthcare could reduce harm. BMJ. 2021;372:n117. PubMed
9.Canadian Institute for Health Information. Unnecessary care in Canada. Ottawa (ON): CIHI; 2017: https://www.cihi.ca/sites/default/files/document/choosing-wisely-baseline-report-en-web.pdf. Accessed 2021 May 7.
10.Hall AM, Aubrey-Bassler K, Thorne B, Maher CG. Do not routinely offer imaging for uncomplicated low back pain. BMJ. 2021;372:n291. PubMed
11.Chou R, Qaseem A, Owens DK, Shekelle P, Clinical Guidelines Committee of the American College of Physicians. Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Ann Intern Med. 2011;154(3):181-189. PubMed
12.Bouck Z, Pendrith C, Chen XK, et al. Measuring the frequency and variation of unnecessary care across Canada. BMC Health Serv Res. 2019;19(1):446. PubMed
13.Embrett M, Randall GE. Physician perspectives on Choosing Wisely Canada as an approach to reduce unnecessary medical care: a qualitative study. Health Res Policy Syst. 2018;16(1):95. PubMed
14.Grimshaw JM, Patey AM, Kirkham KR, et al. De-implementing wisely: developing the evidence base to reduce low-value care. BMJ Qual Saf. 2020;29(5):409-417. PubMed
15.Rosenberg A, Agiro A, Gottlieb M, et al. Early trends among seven recommendations from the Choosing Wisely Campaign. JAMA Internal Medicine. 2015;175(12):1913-1920. PubMed
16.Henderson J, Bouck Z, Holleman R, et al. Comparison of payment changes and Choosing Wisely recommendations for use of low-value laboratory tests in the United States and Canada. JAMA Intern Med. 2020;180(4):524-531. PubMed
17.Lam JH, Pickles K, Stanaway FF, Bell KJL. Why clinicians overtest: development of a thematic framework. BMC Health Serv Res. 2020;20(1):1011. PubMed
18.Hall AM, Scurrey SR, Pike AE, et al. Physician-reported barriers to using evidence-based recommendations for low back pain in clinical practice: a systematic review and synthesis of qualitative studies using the Theoretical Domains Framework. Implement Sci. 2019;14(1):49. PubMed
19.Guttmann A, Gandhi S, Wanigaratne S, et al. COVID-19 in immigrants, refugees and other newcomers in Ontario: characteristics of those tested and those confirmed positive, as of June 13, 2020. Toronto (ON): ICES; 2020: https://www.ices.on.ca/Publications/Atlases-and-Reports/2020/COVID-19-in-Immigrants-Refugees-and-Other-Newcomers-in-Ontario. Accessed 2021 May 6.
20.Choi KH, Denice P, Haan M, Zajacova A. Studying the social determinants of COVID‐19 in a data vacuum. Can Rev Sociol. 2021. PubMed
21.Glazier RH, Green ME, Wu FC, Frymire E, Kopp A, Kiran T. Shifts in office and virtual primary care during the early COVID-19 pandemic in Ontario, Canada. CMAJ. 2021;193(6):E200-E210. PubMed
22.Enablers for virtual visits. (CADTH policy insights). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/covid-19/cy0006-enablers-for-virtual-visits.pdf. Accessed 2021 May 4.
23.Oakes AH, Segal JB. The COVID-19 pandemic can help us understand low-value health care. Health Affairs Blog. 2020. https://www.healthaffairs.org/do/10.1377/hblog20201023.522078/full/. Accessed 2021 Apr 20.
24.The Conference Board of Canada. Health care cost drivers in Canada: pre-and post-COVID-19. Ottawa (ON): Conference Board of Canada; 2020: https://www.conferenceboard.ca/e-library/abstract.aspx?did=10816. Accessed 2021 Apr 21.
25.Choosing Wisely Canada. Not necessary: policy ideas for limiting low-value care in Canada. Toronto (ON): Choosing Wisely Canada; 2020: https://choosingwiselycanada.org/perspective/not-necessary/. Accessed 2021 May 6.
26.Resumption of elective health services amid COVID-19. (COVID-19 CADTH briefing note). Ottawa (ON): CADTH; 2020: https://covid.cadth.ca/treatment/resumption-of-elective-health-services-amid-covid-19/. Accessed 2021 May 7.
27.Canadian Medical Association, Deloitte LLP. Clearing the backlog: the cost to return wait time to pre-pandemic levels. Ottawa (ON): CMA; 2020: https://www.cma.ca/sites/default/files/pdf/Media-Releases/Deloitte-Clearing-the-Backlog.pdf. Accessed 2021 May 7.
28.Canadian Institute for Health Information. COVID-19’s effect on hospital care services. 2020; https://www.cihi.ca/en/covid-19-resources/impact-of-covid-19-on-canadas-health-care-systems/covid-19s-effect-on-hospital. Accessed 2021 Apr 12.
29.Wang J, Vahid S, Eberg M, et al. Clearing the surgical backlog caused by COVID-19 in Ontario: a time series modelling study. CMAJ. 2020;192(44):E1347-E1356. PubMed
30.BC Ministry of Health. A Commitment to Surgical Renewal in B.C. Victoria (BC): BC Ministry of Health; 2020: https://www2.gov.bc.ca/assets/gov/health/conducting-health-research/surgical-renewal-plan.pdf. Accessed 2021 Apr 21.
31.Canadian Medical Association. CMA calls for extraordinary measures as pandemic surpasses critical point. 2021; https://www.cma.ca/news-releases-and-statements/cma-calls-extraordinary-measures-pandemic-surpasses-critical-point. Accessed 2021 April 20.
32.Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qualitative Health Research. 2005;15(9):1277-1288. PubMed
33.Choosing Wisely Canada, College of Family Physicians of Canada. Family medicine. 2020; https://choosingwiselycanada.org/family-medicine/. Accessed 2021 May 7.
34.Stanworth SJ, New HV, Apelseth TO, et al. Effects of the COVID-19 pandemic on supply and use of blood for transfusion. The Lancet Haematology. 2020;7(10):e756-e764. PubMed
35.Centre for Rural Health Research. Out of pocket costs for rural residents when travelling for health care. Vancouver (BC): University of British Columbia (UBC); 2020: https://crhr.med.ubc.ca/out-of-pocket-costs-survey/. Accessed 2021 Apr 28.
36.Pooja C, Suraiya N. Choosing Wisely in the Northwest Territories: a case for thinking beyond the test in rural and remote northern communities. HealthcarePapers. 2019;18(1):19-24.
37.Liddy C, McKellips F, Armstrong CD, Afkham A, Fraser-Roberts L, Keely E. Improving access to specialists in remote communities: a cross-sectional study and cost analysis of the use of eConsult in Nunavut. Int J Circumpolar Health. 2017;76(1):1323493. PubMed
38.Arya A, Buchman S, Gagnon B, Downar J. Pandemic palliative care: beyond ventilators and saving lives. CMAJ. 2020;192(15):E400-E404. PubMed
39.Canadian Institute for Health Information. The impact of COVID-19 on long-term care in Canada: focus on the first 6 months. Ottawa (ON): CIHI; 2021: https://www.cihi.ca/sites/default/files/document/impact-covid-19-long-term-care-canada-first-6-months-report-en.pdf. Accessed 2021 May 6.
40.Sorrell JM. Use of feeding tubes in patients with advanced dementia: are we doing harm? J Psychosoc Nurs Ment Health Serv. 2010;48(5):15-18. PubMed
41.Canadian Institute for Health Information. Continuing Care Reporting System (CCRS) metadata. 2021; https://www.cihi.ca/en/continuing-care-metadata. Accessed 2021 May 6. - An extraction of this metadata was presented during the Panel meeting.
42.Walker JD, Teare GF, Hogan DB, Lewis S, Maxwell CJ. Identifying potentially avoidable hospital admissions from canadian long-term care facilities. Med Care. 2009;47(2):250-254. PubMed
43.Kadu M, Heckman GA, Stolee P, Perlman C. Risk of hospitalization in long-term care residents living with heart failure: a retrospective cohort study. Can Geriatr J. 2019;22(4):171-181. PubMed
44.Brown KA, Daneman N, Buchan SA, Chan AK, Stall NM. Variation in care of community and nursing home residents who died of COVID-19 in Ontario, Canada. J Am Med Dir Assoc. 2021.
45.Brownlee S, Chalkidou K, Doust J, et al. Evidence for overuse of medical services around the world. The Lancet. 2017;390(10090):156-168. PubMed
46.Soril LJJ, Seixas BV, Mitton C, Bryan S, Clement FM. Moving low value care lists into action: prioritizing candidate health technologies for reassessment using administrative data. BMC Health Serv Res. 2018;18(1):640. PubMed
Appendix 1: Voting Results of the Panel
Table 3: Final Recommendations of the Expert Panel That Had a High Level of Consensus
Clinical area | Category | Recommendation | Live vote | Consensus |
Hospital care | Routine investigations | Don’t order routine investigations, including chest radiographs or blood tests, in critically ill patients, except to answer a specific clinical question. | No | 80% |
Preoperative testing | Don’t order baseline laboratory studies (complete blood count, coagulation testing, or serum biochemistry) for asymptomatic patients undergoing low-risk non-cardiac surgery. | No | 80% | |
End-of-life care | Advance care planning conversations | Don’t start or continue life-supporting interventions unless they are consistent with the patient’s values and realistic goals of care. | No | 90% |
Don’t delay advance care planning conversations. | Yes | 90% | ||
Palliative care | Don’t delay palliative care for a patient with serious illness who has physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment. | Yes | 100% | |
Specialty or outpatient care | Nephrology | Don’t initiate chronic dialysis without ensuring a shared decision-making process between patients, their families, and their nephrology health care team. | Yes | 100% |
Gastroenterology | Avoid performing a colonoscopy for constipation in those under the age of 50 years without family history of colon cancer or alarm features. | Yes | 100% | |
Cardiology | Don’t perform stress cardiac imaging or advanced non-invasive imaging in the initial evaluation of patients without cardiac symptoms unless high-risk markers are present. | Yes | 100% | |
Orthopedics | Don’t order a knee MRI when weight-bearing X-rays demonstrate osteoarthritis and symptoms are suggestive of osteoarthritis as the MRI rarely adds useful information to guide diagnosis or treatment. | Yes | 80% | |
Long-term care | Transfer | Don’t send the frail resident of a nursing home to the hospital unless their urgent comfort and medical needs cannot be met in their care home. | Yesa | 100% |
Blood products | Red blood cells transfusion | Don’t routinely transfuse red blood cells in hemodynamically stable ICU patients with a hemoglobin concentration greater than 70 g/L (a threshold of 80 g/L may be considered for patients undergoing cardiac or orthopedic surgery and those with active cardiovascular disease). | Yes | 100% |
Oncology | Palliative | Don’t delay or avoid palliative care for a patient with metastatic cancer because they are pursuing disease-directed treatment. | Yes | 100% |
Primary care | Transfers | Don’t send a patient for a specialist visit that requires several hours of transport if the visit can be done virtually or by a local physician. | Yes | 100% |
Annual examination | Don’t do annual physical exams on asymptomatic adults with no significant risk factors.b | No | 80% | |
Unnecessary screening tests | Don’t perform population-based screening for 25-OH-vitamin D deficiency. | Yes | 100% | |
Unnecessary imaging | Don’t order screening chest X-rays and ECGs for asymptomatic or low-risk outpatients. | No | 80% | |
Don’t do imaging for lower back pain unless red flagsb are present. | Yes | 100% | ||
Don’t do imaging for uncomplicated headache unless red flagsb are present. | Yes | 100% | ||
Don’t order a CT scan for uncomplicated acute rhinosinusitis. | Yes | 100% |
CT = computed tomography; ECG = electrocardiogram; ICU = intensive care unit; MRI = magnetic resonance imaging.
Note: Where re-voting did not occur (since no extensive discussion was required), percentages show the level consensus according to the survey results.
aThis recommendation was not including in the original short list; however, it was added after it was flagged for consideration.
bSpecific risk factors or red flags may vary based on clinical assessment. See Choosing Wisely Canada’s detailed guide on Family Medicine.
Table 4: Recommendations Discussed by the Panel That Did Not Receive Consensus From at Least 8 Members
Clinical area | Category | Recommendation | Live vote | Consensus |
Long-term care | Feeding tube | Don’t insert a feeding tube in individuals with advanced dementia. Instead, assist the resident to eat. | Yes | 60% |
Oncology | Routine cancer screening | Don’t order tests to detect recurrent cancer in asymptomatic patients if there is not a realistic expectation that early detection of recurrence can improve survival or quality of life. | Yes | 70% |
Specialty or outpatient care | Cardiology | Don’t perform annual stress cardiac imaging or advanced non-invasive imaging as part of routine follow-up in asymptomatic patients. | Yes | 70% |
Table 5: Choosing Wisely Canada’s Short List of 45 Recommendations and the Level of Consensus in the Survey
Clinical area | Category | Recommendation | Reviewed in panel meeting | Survey consensus |
Hospital care | Routine investigations | In the inpatient setting, don’t order repeated CBC and chemistry testing in the face of clinical and lab stability. | No | 70% |
Don’t order routine investigations, including chest radiographs or blood tests, in critically ill patients, except to answer a specific clinical question. | Yes | 80% | ||
CT head | Don’t order CT head scans in adults and children who have suffered minor head injuries (unless positive for a head injury clinical decision rule). | No | 60% | |
Don’t order CT head scans in adult patients with simple syncope in the absence of high-risk predictors. | No | 40% | ||
Don’t routinely obtain head CT scans in hospitalized patients with delirium in the absence of risk factors. | No | 60% | ||
CT pulmonary angiogram for PE | Don’t order CT pulmonary angiograms or VQ scans in patients with suspected pulmonary embolism until risk stratification with decision rule has been applied and, when indicated, D-dimer biomarker results are obtained. | No | 60% | |
Screening blood or laboratory tests | Don’t routinely order qualitative toxicology testing (urine drug screen) on all psychiatric patients presenting to the emergency room. | No | 70% | |
Preoperative testing | Don’t order baseline laboratory studies (complete blood count, coagulation testing, or serum biochemistry) for asymptomatic patients undergoing low-risk non-cardiac surgery. | Yes | 80% | |
Don’t order a baseline electrocardiogram for asymptomatic patients undergoing low-risk non-cardiac surgery. | No | 70% | ||
Don’t perform stress cardiac imaging or advanced non-invasive imaging as a preoperative assessment in patients scheduled to undergo low-risk non-cardiac surgery. | No | 70% | ||
Don’t perform resting echocardiography as part of preoperative assessment for asymptomatic patients undergoing low to intermediate-risk non-cardiac surgery. | No | 70% | ||
End-of-life care | Advanced care planning conversations | Don’t start or continue life-supporting interventions unless they are consistent with the patient’s values and realistic goals of care. | Yes | 90% |
Don’t delay advance care planning conversations. | Yes | 90% | ||
Palliative care | Don’t delay palliative care for a patient with serious illness who has physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment. | Yes | 70% | |
Oncology | Routine cancer screening | Don’t order tests to detect recurrent cancer in asymptomatic patients if there is not a realistic expectation that early detection of recurrence can improve survival or quality of life. | Yes | 70% |
Don’t perform routine cancer screening, or surveillance for a new primary cancer, in the majority of patients with metastatic disease. | No | 40% | ||
Don’t screen for ovarian cancer in asymptomatic women at average risk. | No | 60% | ||
Radiation therapy | Don’t recommend more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis. | No | 40% | |
Palliative care | Avoid chemotherapy and instead focus on symptom relief and palliative care in patients with advanced cancer unlikely to benefit from chemotherapy (e.g., performance status 3 or 4). | No | 70% | |
Don’t delay or avoid palliative care for a patient with metastatic cancer because they are pursuing disease-directed treatment. | Yes | 70% | ||
Long-term care | Feeding tubes | Don’t insert a feeding tube in individuals with advanced dementia. Instead, assist the resident to eat. | Yes | 80% |
Routine chronic disease testing or screening | Don’t order screening or routine chronic disease testing just because a blood draw is being done. | No | 60% | |
Primary care | Annual exam | Don’t do annual physical exams on asymptomatic adults with no significant risk factors. | Yes | 80% |
Don’t do annual screening blood tests unless directly indicated by the risk profile of the patient. | No | 70% | ||
Don’t order screening chest X-rays and ECGs for asymptomatic or low-risk outpatients. | Yes | 80% | ||
Unnecessary imaging | Don’t do imaging for lower back pain unless red flags are present. | Yes | 80% | |
Don’t do imaging for uncomplicated headache unless red flags are present. | Yes | 80% | ||
Don’t repeat dual-energy X-ray absorptiometry (DEXA) scans more often than every 2 years. | No | 70% | ||
Don’t order a CT scan for uncomplicated acute rhinosinusitis. | Yes | 80% | ||
Unnecessary screening tests in low-risk patients | Don’t order an erythrocyte sedimentation rate (ESR) to screen asymptomatic patients or as a general test to look for inflammation in patients with undiagnosed conditions. | No | 60% | |
Don’t perform routine urinalysis (protein, glucose) at every antenatal visit (in low-risk normotensive women). | No | 70% | ||
Don’t perform population-based screening for 25-OH vitamin D deficiency. | Yes | 80% | ||
Don’t screen women with Pap smears if under 21 years of age or over 69 years of age. | No | 70% | ||
Don’t order thyroid function tests as screening for asymptomatic, low-risk patients. | No | 70% | ||
Transfers in rural medicine | Don’t send a patient for a specialist visit that requires several hours of transport if the visit can be done virtually or by a local physician. | Yes | 90% | |
Don’t transfer a patient by ambulance with skilled personnel if the patient is unlikely to require medical intervention en route. | No | 60% | ||
Blood products | Red blood cells transfusion | Don’t routinely transfuse red blood cells in hemodynamically stable ICU patients with a hemoglobin concentration greater than 70 g/L (a threshold of 80 g/L may be considered for patients undergoing cardiac or orthopedic surgery and those with active cardiovascular disease). | Yes | 70% |
Specialty or outpatient | Orthopedics | Don’t order a knee MRI when weight-bearing X-rays demonstrate osteoarthritis and symptoms are suggestive of osteoarthritis as the MRI rarely adds useful information to guide diagnosis or treatment. | Yes | 70% |
Don’t order a hip MRI when X-rays demonstrate osteoarthritis and symptoms are suggestive of osteoarthritis as the MRI rarely adds useful information to guide diagnosis or treatment. | No | 60% | ||
Don’t use arthroscopic debridement as a primary treatment in the management of osteoarthritis of the knee. | No | 60% | ||
Nephrology | Don’t initiate chronic dialysis without ensuring a shared decision-making process between patients, their families, and their nephrology health care team. | Yes | 80% | |
Gastroenterology | Avoid performing an endoscopy for dyspepsia without alarm symptoms for patients under the age of 65 years. | No | 50% | |
Avoid performing a colonoscopy for constipation in those under the age of 50 years without family history of colon cancer or alarm features. | Yes | 80% | ||
Cardiology | Don’t perform stress cardiac imaging or advanced non-invasive imaging in the initial evaluation of patients without cardiac symptoms unless high-risk markers are present. | Yes | 70% | |
Don’t perform annual stress cardiac imaging or advanced non-invasive imaging as part of routine follow-up in asymptomatic patients. | Yes | 70% |
CT = computed tomography; ECG = electrocardiogram; ICU = intensive care unit; MRI = magnetic resonance imaging.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.