CADTH Reimbursement Review
Nivolumab (Opdivo) in combination with Ipilimumab (Yervoy)
Sponsor: Bristol Myers Squibb Canada
Therapeutic area: Malignant pleural mesothelioma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ASBI
Average Symptom Burden Index
BICR
blinded independent central review
CCO
Cancer Care Ontario
CI
confidence interval
CrI
credible interval
CTLA-4
cytotoxic T-lymphocyte-associated protein 4
DCR
disease control rate
DIC
deviance information criteria
ECOG
Eastern Cooperative Oncology Group
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels
HR
hazard ratio
HRQoL
health-related quality of life
IMAE
immune-mediated adverse event
ITC
indirect treatment comparison
ITT
intention-to-treat
IV
intravenous
LCC
Lung Cancer Canada
LCSS-Meso
Lung Cancer Symptom Score–mesothelioma
MID
minimally important difference
MPM
malignant pleural mesothelioma
m-RECIST
modified Response Evaluation Criteria in Solid Tumors
NMA
network meta-analysis
NPH
non-proportional hazards
ORR
objective response rate
OS
overall survival
PD-1
programmed cell-death protein 1
PD-L1
programmed cell-death ligand 1
PFS
progression-free survival
PH
proportional hazards
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumors Version 1.1
SAE
serious adverse event
VAS
visual analogue scale
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo) 10 mg/mL for injection; administered by IV infusion Ipilimumab (Yervoy) 5 mg/mL for injection; administered by IV infusion |
Indication | Nivolumab (Opdivo) in combination with ipilimumab (Yervoy) is indicated for the treatment of adult patients with unresectable MPM who have not received prior systemic therapy for MPM |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Other expedited pathway (Project Orbis) |
NOC date | May 28, 2021 |
Sponsor | Bristol Myers Squibb Canada |
IV = IV; MPM = malignant pleural mesothelioma; NOC = Notice of Compliance.
Source: Sponsor’s submission1 (Application Overview), nivolumab (Opdivo) product monograph,2 and ipilimumab (Yervoy) product monograph.3
Malignant mesothelioma is a rare neoplasm arising from the mesothelial cells lining the pleura, pericardium, peritoneum, or tunica vaginalis. Malignant pleural mesothelioma (MPM) is the most common form of the disease and accounts for 70% to 80% of reported mesotheliomas, with asbestos exposure implicated in approximately 80% of cases.4 Due to the long latency period between exposure and development of MPM, the incidence is expected to peak in the next few decades.4,5 Symptoms of MPM include unilateral or bilateral chest-wall pain, coughing, pleurisy, and progressive dyspnea due to pleural effusion.5,6 In Canada, there were 445 cases of mesothelioma in 2016, with approximately 84% of diagnosis (375 patients) occurring in men; in 2017, there were 490 deaths due to mesothelioma, also with the majority (401 deaths) occurring in men.7 The median overall survival (OS) of patients with unresectable MPM is approximately 1 year, with a 5-year OS of approximately 10%.8,9 Malignant pleural mesothelioma is considered an aggressive cancer; by the time symptoms develop, patients often have advanced disease and are therefore not candidates for surgical resection.5 For those who are not candidates for surgical approaches, systemic chemotherapy is the primary treatment modality.8 The recommended first-line regimen in Canada is pemetrexed plus a platinum compound (cisplatin or carboplatin).9
Nivolumab and ipilimumab are monoclonal antibodies that improve antitumour response. Nivolumab targets the programmed cell-death (PD-1) receptor and ipilimumab inhibits cytotoxic T-lymphocyte-associated protein 4 (CTLA-4). In combination, they are thought to have a synergistic effect in enhancing T cell function.2 This dual-drug therapy underwent an expedited review at Health Canada for the indication of treatment of adult patients with unresectable MPM who have not received prior systemic therapy.1 The recommended dosage of nivolumab is either 3 mg/kg every 2 weeks or 360 mg every 3 weeks, administered as an IV (IV) infusion over 30 minutes. The recommended dosage of ipilimumab is 1 mg/kg every 6 weeks, administered as an IV infusion over 30 minutes. Treatment is continued at the same dosage until disease progression or unacceptable toxicity, or for up to 2 years in patients without disease progression.2
The objective of this CADTH drug reimbursement review is to perform a systematic review of the beneficial and harmful effects of nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable MPM.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, Lung Cancer Canada (LCC) and the Canadian Mesothelioma Foundation, submitted joint patient input for this review. Information incorporated into their input was collected by conducting surveys, interviews, and an environmental scan. Interviews included 4 patients and 1 caregiver, and the environmental scan included 1 patient and 1 caregiver. Of the 7 patients who provided input, 3 were located in Canada and 2 were in the US. Surveys of mesothelioma patients and their caregivers were completed by 10 patients and 23 caregivers.
Just over half of the patients who completed the survey were working full-time outside of the home at diagnosis; the remainder were either retired or had left the workforce before their diagnosis. Due to their illness, patients who were working full-time had to quit their job or reduce the number of hours they worked. More than half of the respondents reported that their experience with mesothelioma has worsened their financial situation and nearly all reported that their experience with mesothelioma has been stressful. All patients reported that their mesothelioma is affecting their quality of life, including functionality, activity level, and independence. Caregivers of patients with mesothelioma also spoke to the impact of mesothelioma on their quality of life and described difficulties managing the treatment of loved ones.
The patient input stated that treatments that allow patients to live longer with a good quality of life are needed, as the aggressiveness of the disease and late stage of diagnosis mean many patients do not have the time to wait. With few available treatment options for this group of patients, there is an unmet need to provide treatments that alleviate symptoms, delay disease progression, provide a better quality of life, prolong survival, and have manageable side effects.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinicians consulted by CADTH for this review indicated that there is a significant unmet need for treatment that prolongs survival in patients diagnosed with MPM. Current treatment for unresectable MPM is chemotherapy, which is associated with limited benefits and significant toxicity. The clinical experts consulted for this review anticipated that if nivolumab plus ipilimumab becomes available for the requested target population, it will be the preferred first-line systemic treatment for unresectable MPM in patients who are candidates for systemic therapy. As overall prognosis is poor, nivolumab plus ipilimumab is considered an improvement in available treatment options for the full population of patients in the reimbursement request.
Clinician Group Input
Two registered joint clinician inputs were provided for this review: a joint input was on behalf of 4 clinicians and 1 pharmacist from Ontario Health’s Cancer Care Ontario (CCO) Lung Cancer Drug Advisory Committee, and another from LCC on behalf of 13 clinicians from across the country. The inputs from the clinician groups align with those of the clinical experts and emphasize the high unmet need for more efficacious and less-toxic systemic therapy in patients with unresectable MPM. Both clinician groups had experience using the treatment under review, and both anticipated that nivolumab plus ipilimumab will replace pemetrexed plus platinum as first-line therapy in newly diagnosed patients who have no contraindications.
Drug Program Input
Input was obtained from all 9 provincial ministries of health and/or cancer agencies participating in CADTH reimbursement reviews. The Provincial Advisory Group identified 2 clinical factors that could affect implementation: numerous clinical eligibility criteria and scenarios for a time-limited need and indication creep.
The clinical experts consulted by CADTH weighed evidence from the CheckMate 743 trial along with other clinical considerations to provide responses.
Clinical Evidence
The CADTH systematic review identified 1 relevant randomized controlled trial (RCT), CheckMate 743.10 In addition, an indirect treatment comparison (ITC) submitted by the sponsor has been included in this review.1
Pivotal Studies and Protocol-Selected Studies
Description of Studies
CheckMate 743 is an international, multi-centre, open-label, phase III trial that compares nivolumab in combination with ipilimumab to standard of care chemotherapy (pemetrexed plus cisplatin or carboplatin) in adult patients with unresectable MPM. Enrolled patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, and must not have received prior MPM treatment (i.e., adjuvant or neoadjuvant chemotherapy, radical pleuropneumonectomy, or non-palliative radiotherapy). Eligible patients were randomized in a 1:1 ratio to receive IV nivolumab (3 mg/kg every 2 weeks) plus IV ipilimumab (1 mg/kg every 6 weeks) or standard of care chemotherapy. Standard of care was the combination of pemetrexed (500 mg/m2 IV) plus either cisplatin (75 mg/m2 IV) or carboplatin (area under the curve 5 IV) given every 3 weeks. Although cisplatin was preferred, carboplatin could be given at the investigator’s discretion. Treatment was continued until disease progression, unacceptable toxicity, or completion of a maximum of 2 years for nivolumab plus ipilimumab and 6 cycles for chemotherapy. Treatment with nivolumab plus ipilimumab was permitted to continue beyond initial confirmed disease progression if the investigator deemed that the patient met certain criteria demonstrating clinical benefit and tolerance of the study drugs.10
The study enrolled 605 patients, with 303 randomized to nivolumab plus ipilimumab and 302 randomized to the chemotherapy group. Randomization was stratified by histology (epithelioid versus non-epithelioid) and gender. Tumour response was assessed by investigators and a blinded independent central review (BICR) using an adapted version of the modified Response Evaluation Criteria in Solid Tumors (m-RECIST) for pleural mesothelioma and/or the Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1).
The primary efficacy end point was OS. Secondary end points included BICR-measured progression-free survival (PFS), objective response rate (ORR), and disease control rate (DCR), but these end points were not formally tested statistically. The study also explored whether programmed cell-death ligand 1 (PD-L1) expression is a predictive biomarker for response for OS, PFS, or ORR as a secondary outcome. Health-related quality of life (HRQoL), an exploratory end point, was measured using the EuroQol 5-Dimensions 3-Levels (EQ-5D-3L) and Lung Cancer Symptom Score–mesothelioma (LCSS-Meso) questionnaires.10
Patient enrolment occurred over approximately 17 months (November 28, 2016, to April 18, 2018).11 The median duration of follow-up (i.e., time from randomization to the date the patient was last known to be alive) was 17.35 months for the nivolumab plus ipilimumab group and 13.27 months in the chemotherapy group, reflecting a minimum follow-up of 19.8 months.10 The minimum length of OS follow-up (i.e., time from randomization to the clinical cut-off date) was 22.1 months, with a median of 29.7 months for the interim OS analysis. Twenty-one patients did not receive treatment, resulting in a safety population of 584 patients, of whom 300 received nivolumab plus ipilimumab, and 284 received chemotherapy. Of those who received treatment, 295 patients (98.3%) in the nivolumab plus ipilimumab group and all patients in the chemotherapy group had discontinued randomized treatment by the time of database lock (April 3, 2020). Only 5 patients, all in the nivolumab plus ipilimumab group, remained on treatment. The main reason for treatment discontinuation in the nivolumab plus ipilimumab group was disease progression (60.7%) or study-drug toxicity (19.7%). The majority of patients in the chemotherapy group discontinued treatment as they had completed the maximum length of treatment (62.0%) or experienced disease progression (15.5%). The median duration of treatment was 5.55 months in the nivolumab plus ipilimumab group and 3.48 months in the chemotherapy group. At the time of database lock, 459 patients (75.9%) had discontinued from the study (n = 218 in the nivolumab plus ipilimumab group and n = 241 in the chemotherapy group), mainly due to death.10,12
Overall, the median age of enrolled patients was 69 years (range = 25 to 89 years; interquartile range = 64 to 75 years), the majority (77.2%) were male, and 85.3% were White. Notably, most enrolled patients had an ECOG performance status of 1 (59.8%), advanced disease at baseline (51.1% were stage IV and 34.5% were stage III), and epithelioid tumour histology (75.4%). Of patients who had a non-epithelioid tumour histology, 11.7% had sarcomatoid, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Most patients (58.2%) were enrolled in the trial from sites in Europe and 9.8% were enrolled from North America. Baseline demographics and characteristics were generally well balanced between the 2 treatment groups. Patients randomized to nivolumab plus ipilimumab were slightly older (≥ 65 years of age; 76.6% nivolumab plus ipilimumab versus 68.2% chemotherapy) and more had an ECOG performance status of 1 (62.4% versus 57.3%) compared to patients randomized to chemotherapy.10
Efficacy Results
Key efficacy results for the CheckMate 743 study are summarized in Table 2. Final analysis for OS data was scheduled to take place after 473 deaths had occurred. Efficacy results were reported based on a pre-specified interim analysis (approximately 85% of total events or 403 deaths, with a minimum survival follow-up of 22.1 months). At the survival data cut-off date, 419 patients had died, including 200 patients (66.0%) in the nivolumab plus ipilimumab group and 219 patients (72.5%) in the chemotherapy group. The median OS was 18.07 months (95% confidence interval [CI], 16.82 to 21.45) in the nivolumab plus ipilimumab group and 14.09 months (95% CI, 12.45 to 16.23) in the chemotherapy group. The interim OS analysis found the difference between the 2 treatment groups was statistically significant in favour of nivolumab plus ipilimumab (hazard ratio [HR] = 0.74; 95% CI, 0.61 to 0.89; P = 0.0020).10
Sensitivity analyses also showed consistent results with the primary analysis. Subgroup analyses for the primary end point of OS were also generally consistent with the intention-to treat (ITT) population, with most HRs favouring treatment with nivolumab plus ipilimumab, although these results should be considered exploratory as the analyses did not account for multiplicity. Confidence intervals included the null value (1.0) for some subgroups, notably including patients with an ECOG performance status of 0 (n = 242; HR = 0.87; 95% CI, 0.64 to 1.19) or epithelioid tumours (n = 456; HR = 0.86; 95% CI, 0.69 to 1.08), or those who were former smokers (n = 318; HR = 0.84; 95% CI, 0.65 to 1.09), indicating uncertainty in the true benefit of the immunotherapy combination over chemotherapy. Also, the HRs favoured chemotherapy in patients who were 75 years or older (n = 157), had stage I (n = 32) or II (n = 45) disease, or had prior radiotherapy (n = 57); however, the CIs all also crossed the null value and the small sample sizes contributed to the uncertainty and difficulty in drawing definitive conclusions from these subgroups. The benefit of nivolumab plus ipilimumab on OS was consistent in patients with PD-L1–positive tumours (≥ 1% expression; HR = 0.69; 95% CI, 0.55 to 0.87), whereas the benefit in patients with PD-L1–negative tumours (< 1%) was less pronounced (HR = 0.94; 95% CI, 0.62 to 1.40). However, the relatively small sample size of the PD-L1 negative subgroup (n = 135) should be considered when interpreting these results. Secondary end points such as PFS, ORR, and DCR did not favour treatment with nivolumab plus ipilimumab.10
Measures of quality of life showed a numerical improvement in patients in the nivolumab plus ipilimumab group, and no clear change or decline in scores in patients in the chemotherapy group. The disease-related symptom deterioration rate at week 12 was numerically higher in the nivolumab plus ipilimumab group (48.0%; 95% CI, 41.7% to 54.4%) compared to the chemotherapy group (40.6%; 95% CI, 34.2% to 47.3%).10 As both of these outcomes were exploratory, no firm conclusions can be made based on these results.
Harms Results
A similar proportion of patients in each treatment group experienced an adverse event (AE) due to any cause (Table 2). When adjusted for the different lengths of treatment exposure, the incidence per 100 person-years was higher in the chemotherapy group (e.g., AEs due to any cause: 1,485.0 versus 2,306.4 with chemotherapy). A higher proportion of patients treated with nivolumab plus ipilimumab experienced all-cause grade 3 to 4 AEs (53.0% versus 42.6%) and all-cause serious adverse events (SAEs; 54.7% versus 25.4%) compared with patients treated with chemotherapy. Reported AEs were generally consistent with the known safety profile of the study treatments. According to the Clinical Study Report, the overall frequency of drug-related hypersensitivity and/or infusion reactions in the nivolumab plus ipilimumab group (12.0% versus 2.5% chemotherapy) was higher than previously reported for other cancers; however, most reactions were grade 1 or 2 in severity and resolved within a day.10
Predefined immune-mediated adverse events (IMAEs) that occurred within 100 days of the last study treatment dose were reported, and analysis was limited to patients who received an immunomodulator for treatment (except for endocrine events, which were included regardless of treatment). In total, 128 patients in the nivolumab plus ipilimumab group experienced an IMAE, of which |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.12 In patients treated with nivolumab plus ipilimumab, the most frequently reported IMAEs of any grade were rashes (13.0%), hypothyroidism or thyroiditis (11.7%), diarrhea or colitis (8.7%), and pneumonitis (6.7%). In patients treated with chemotherapy, 1.1% experienced an immune-mediated rash. Most IMAEs were grade 1 or 2 in severity.10
A greater proportion of patients who received the immunotherapy combination discontinued study treatment due to an AE from any cause (29.3% versus 20.4% for chemotherapy group). In patients treated with nivolumab plus ipilimumab, the most common AEs leading to treatment discontinuation were colitis (2.3%), diarrhea (2.3%), infusion-related reactions (1.7%), and pneumonitis (1.7%). In patients treated with chemotherapy, the most common AEs leading to treatment discontinuation were anemia (3.9%), asthenia (2.1%), nausea (1.8%), fatigue (1.8%), neutropenia (1.8%), and thrombocytopenia (1.8%).10
Overall, 410 deaths occurred during the study, most due to disease progression. Toxicity from the study drug led to 3 deaths (1.0%) in the immunotherapy group and 1 death (0.4%) in the chemotherapy group. In patients treated with nivolumab plus ipilimumab, the causes of treatment-related deaths were pneumonitis, acute heart failure, and neurologic complications (encephalitis), each of which occurred in 1 patient. The cause of the treatment-related death in the 1 patient treated with chemotherapy was myelosuppression and salmonella sepsis.10
Table 2: Summary of Key Results from Pivotal and Protocol-Selected Studies
Key result | CheckMate 743 | |
|---|---|---|
Nivolumab plus ipilimumab | Chemotherapya | |
Efficacy outcomes – ITT population | N = 303 | N = 302 |
Primary outcome – overall survivalb | ||
Median, months (95% CI) | 18.07 (16.82 to 21.45) | 14.09 (12.45 to 16.23) |
Events, n (%) | 200 (66.0) | 219 (72.5) |
Stratified hazard ratio (95% CI)c | 0.74 (0.61 to 0.89) | |
P value | 0.0020 | |
Harms outcomes, n (%) – safety population | N = 300 | N = 284 |
All-cause adverse events | 299 (99.7) | 277 (97.5) |
Serious adverse events | 164 (54.7) | 72 (25.4) |
Withdrawals due to adverse events | 88 (29.3) | 58 (20.4) |
Deaths | 198 (66.0) | 212 (74.6) |
Deaths due to disease progression | 183 (61.0) | 199 (70.1) |
Deaths due to study drug toxicity | 3 (1.0) | 1 (0.4) |
CI = confidence interval; ITT = intention-to-treat.
aStandard of care chemotherapy regimen consisted of pemetrexed in combination with cisplatin or carboplatin. Cisplatin was preferred for the combination, but carboplatin could be used at the investigator’s discretion. At cycle 1, cisplatin was initiated in 104 patients and carboplatin was initiated in 180 patients. Switching between cisplatin and carboplatin was permitted; during the trial 29 patients switched from cisplatin to carboplatin, and a total of 209 patients were exposed to carboplatin.
bOverall survival results represent data from the interim analysis. Based on 419 deaths of 473 anticipated for final analysis, the multiplicity-adjusted 2-sided significance level was 0.0345.
cThe hazard ratio and corresponding 2-sided CI were estimated using a stratified Cox proportional hazards model. A hazard ratio of less than 1 favours nivolumab plus ipilimumab; stratification factors include tumour histology and gender.
Source: Clinical Study Report.10
Critical Appraisal
A few major limitations and sources of bias are provided below. Further details for each point, as well as a complete list of limitations and sources of bias are available in the Clinical Evidence – Results; Critical Appraisal section of this report.
Open-label studies are susceptible to reporting, performance, detection, and selection biases as patients and investigators are not blinded to study treatment allocation. In CheckMate 743, the risk for bias remains a concern for subjective outcomes assessed in the trial, including HRQoL and safety.
To account for the interim analysis, the nominal significance level for the primary end point was adjusted for overall type I error. Many pre-specified subgroup analyses were preformed, but no statistical considerations were employed to account for multiplicity. Secondary objectives were not controlled for type I error, nor was formal testing performed. As the trial was not powered to test specific hypotheses in subgroups or secondary end points, the results of these analyses should be considered exploratory in nature.
Longer-term survival is influenced by all treatment received. Subsequent treatment would confound the assessment of OS if patients experienced additional clinical benefits. This may prolong survival beyond what would have occurred with front-line treatment alone and overestimate the survival benefit. Overall, a similar proportion of patients in both treatment groups received subsequent systemic therapy after discontinuing study treatment, although the types of treatment differed. In an unblinded trial setting, the choice of subsequent therapy may be influenced by the treatment received. The impact of this bias in CheckMate 743 is unknown.
The graphical representation of PFS clearly showed crossing of the Kaplan–Meier curves, violating the proportional hazards (PH) assumption and indicating that the HR does not provide a long-term stable estimate of treatment effect on this outcome.
A published and validated minimally important difference (MID) has not been established for the LCSS-Meso questionnaire in patients with MPM. Consequently, it is unclear if the threshold used in the trial (i.e., an MID of 10 points) is appropriate and reflective of a clinically meaningful change in outcomes in patients with MPM.
Although pre-specified, CheckMate 743 measured patient-reported outcomes (PROs) as part of exploratory end points and did not adjust for multiplicity. Also, the few patients left in the trial and included in the analyses of PROs at later assessment time points — who therefore have a better HRQoL — are likely not representative of all patients randomized in each treatment group, and the results are not generalizable to the broader patient population. Finally, due to the open-label study design and exploratory nature of the end point, it is difficult to fully describe the effect of treatment on HRQoL, and results should be interpreted with consideration of these important limitations.
Indirect Comparisons
Description of Studies
Five studies were included in the sponsor’s ITC analysis: CheckMate 743,10 Habib and Fahmy (2013),13 Zalcman et al. (2016)14 (MAPS), Vogelzang et al. (2003)15 (EMPHACIS), and van Meerbeeck et al. (2005)16 (EORTC 08983). The ITC compared the efficacy of nivolumab plus ipilimumab to treatment with pemetrexed plus cisplatin or carboplatin; cisplatin; bevacizumab plus pemetrexed plus cisplatin; raltitrexed plus cisplatin; and gemcitabine plus cisplatin.
Efficacy Results
The results of the network meta-analysis (NMA) of OS relative to nivolumab plus ipilimumab reported HRs of 0.74 for pemetrexed plus cisplatin or carboplatin (95% credible interval [CrI], 0.61 to 0.89), 0.96 for bevacizumab plus pemetrexed plus cisplatin (95% CrI, 0.72 to 1.28), 0.57 for cisplatin (95% CrI, 0.42 to 0.77), 0.47 for gemcitabine (95% CrI, 0.20 to 1.09), and 0.77 for raltitrexed plus cisplatin (95% CrI, 0.51 to 1.16). Based on the reported 95% CrIs, nivolumab plus ipilimumab was favoured as it showed an increase in OS relative to pemetrexed plus cisplatin or carboplatin, and to cisplatin. No treatment was favoured for all other comparisons of OS.
The results of the NMA of PFS relative to nivolumab plus ipilimumab reported HRs of 1.00 for pemetrexed plus cisplatin/carboplatin (95% CrI, 0.82 to 1.22), 1.64 for bevacizumab plus cisplatin plus pemetrexed (95% CrI, 1.24 to 2.17), 0.70 for cisplatin (95% CrI, 0.53 to 0.93), and 0.91 for raltitrexed plus cisplatin (95% CrI, 0.63 to 1.34). Nivolumab plus ipilimumab was favoured relative to cisplatin based on the reported 95% CrI, which showed an increase in PFS. Based on the reported 95% CrI, bevacizumab plus pemetrexed plus cisplatin was favoured, showing increased PFS relative to nivolumab plus ipilimumab. There were no favoured comparators for PFS between either nivolumab plus ipilimumab and pemetrexed plus cisplatin or carboplatin or between nivolumab plus ipilimumab and raltitrexed plus cisplatin.
The results of the NMA of ORRs relative to nivolumab plus ipilimumab reported risk ratios of 0.94 for pemetrexed plus cisplatin or carboplatin (95% CrI, 0.80 to 1.09), 1.23 for raltitrexed plus cisplatin (95% CrI, 0.80 to 2.16), 2.38 for gemcitabine plus cisplatin (95% CrI, 0.96 to 7.81), and 1.97 for cisplatin (95% CrI, 1.40 to 2.91). Based on the reported 95% CrIs, nivolumab plus ipilimumab was favoured in showing improved ORR compared to cisplatin. No other treatment was clearly favoured in terms of ORR for other comparisons.
Harms Results
No comparisons for harms or safety were incorporated in the sponsor’s ITC.
Critical Appraisal
The sponsor’s ITC included analyses of only efficacy (i.e., OS, PFS, and ORR) between nivolumab plus ipilimumab and other comparators. The sponsor’s ITC therefore cannot be used to inform conclusions regarding the relative safety or HRQoL between treatment regimens. The main limitations of efficacy comparisons pertained to trial differences in baseline and clinical characteristics, use of subsequent therapies that may bias results toward comparator groups, and trial length. As the published trials used in the ITC were conducted between 5 and 18 years ago, data from these trials may not accurately reflect current clinical practices for treatment of MPM. Clinical experts also confirmed that the sponsor’s ITC included a treatment regimen (raltitrexed plus cisplatin) that is no longer relevant to current clinical practice; the most relevant comparator was pemetrexed plus cisplatin or carboplatin.
Conclusions
Malignant pleural mesothelioma is an aggressive cancer with poor prognosis and few treatment options. The combination of nivolumab plus ipilimumab resulted in longer OS compared with pemetrexed plus platinum-based standard of care for the treatment of patients with unresectable MPM in a single phase III RCT. According to the clinical experts consulted for this review, the results of this study indicate that nivolumab plus ipilimumab would be used as a first-line therapy for patients with unresectable MPM. However, at this time, limitations associated with the subgroup analyses of histology preclude drawing concrete conclusions regarding the effects of nivolumab plus ipilimumab.
Secondary outcomes of PFS, ORR, and DCR did not show numerically favourable results for nivolumab plus ipilimumab, and differences between groups for these outcomes were not formally tested statistically.
Measurement of HRQoL using EQ-5D-3L and LCSS-Meso were included as exploratory results only, and firm conclusions cannot be drawn for these end points. Although a high percentage of patients experienced AEs with treatment with nivolumab plus ipilimumab, the events were in line with those expected from these drugs and were considered manageable by the clinical experts consulted by CADTH.
Introduction
Disease Background
Malignant mesothelioma is a rare neoplasm arising from the mesothelial cells lining the pleura, pericardium, peritoneum, or tunica vaginalis. Malignant pleural mesothelioma develops in the pleural cavity, which is the most common site of disease, and accounts for 70% to 80% of reported mesotheliomas; approximately 20% occurs in the peritoneum.4 Malignant mesothelioma is broadly classified as epithelioid, sarcomatoid, or biphasic. The epithelioid subtype is the most common (60% to 70%), and is generally associated with better prognosis compared with sarcomatoid or mixed histologies.5,8
Occupational, environmental, or domestic asbestos exposure is implicated in approximately 80% of MPM cases, although other etiologic factors, including genetic susceptibility, have been suggested.4,5 As inhalational exposure to asbestos has been widely recognized as a risk factor, Canada banned asbestos and asbestos-containing products in 2018. However, the latency period between exposure and development of MPM has been estimated to range between 20 and 40 years, depending on the severity and duration of exposure.5,17 Asbestos-related MPM is therefore expected to peak in the next few decades. The risk of developing this cancer increases with age, and most patients are older than 50 years at the time of presentation.4,5
Symptoms of MPM include unilateral or bilateral chest-wall pain, coughing, pleuritic pain, and progressive dyspnea due to pleural effusion. Such symptoms can affect daily functioning and quality of life.5,6 Malignant pleural mesothelioma is considered an aggressive cancer, and patients often have advanced disease by the time symptoms develop.5
The incidence rates vary considerably between countries.5 In Canada, there were 445 cases of mesothelioma in 2016, with approximately 84% of the diagnoses (375 patients) made in men. Death due to mesothelioma was recorded in 490 Canadians in 2017, with 401 deaths occurring in men.7 The median OS of patients with unresectable MPM is approximately 1 year, with a 5-year OS of approximately 10%.8,9
Standards of Therapy
The treatment options for patients newly diagnosed with MPM include surgery, radiation therapy, and/or chemotherapy.8 Patients generally present with advanced disease, and only a minority are candidates for surgical resection. For eligible candidates with early disease and an epithelioid subtype, surgery is sometimes performed as a part of multimodal therapy that involves chemotherapy with or without radiotherapy. Patients who undergo multimodal therapy have demonstrated a median OS of 13 to 23.9 months.9
The goal of surgery in appropriate candidates is maximum cytoreduction or a macroscopic complete resection, although which technique best achieves this goal is still under debate.9 The 2 techniques used for surgical resection are pleurectomy or decortication and extrapleural pneumonectomy, although data from RCTs are lacking to inform practice.8 Radiation is used only as part of multimodal regimens or palliative therapy, and radiation alone is not recommended for the treatment of MPM.8
For patients who are not candidates for surgical approaches and have an ECOG performance status of 0 to 2, systemic chemotherapy is the primary treatment modality. Best supportive care is generally recommended for patients with an ECOG performance status of 3 to 4.8 The recommended first-line chemotherapy regimen is pemetrexed plus a platinum compound.9 Based on randomized trial data, this combination is considered standard of care according to Canadian clinicians and the American Society of Clinical Oncology.15 The combination of pemetrexed plus cisplatin is approved by Health Canada for the first-line treatment of unresectable MPM.18 Carboplatin is often substituted for cisplatin, particularly if there are concerns with tolerability.9 Other combinations such as bevacizumab plus pemetrexed-based regimens may also be prescribed in certain patients.9,14,19 The MAPS trial, which investigated the addition of bevacizumab to standard of care (pemetrexed plus cisplatin), found triplet therapy was associated with a statistically significant improvement in OS (median = 16.1 months versus 18.8 months; HR = 0.77; 95% CI, 0.62 to 0.85).14 However, the frequency of use of bevacizumab in Canada is low because the cost of treatment is not covered by provincial jurisdictions.
According to the clinicians consulted by CADTH for this review, 2 main considerations guide treatment for patients diagnosed with MPM: Is the disease operable and can the patient receive chemotherapy? In patients with unresectable disease, the current standard of care is pemetrexed plus cisplatin or carboplatin. Some patients in specific jurisdictions may receive bevacizumab in addition to this combination, but funding is through different mechanisms and is not covered by public drug plans. The main goals of treatment in patients diagnosed with MPM are prolonging life and improving HRQoL.
Drug
Nivolumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and programmed cell-death ligand 2. This binding releases the PD-1 pathway–mediated inhibition of immune response, which includes the antitumour immune response. Combining nivolumab (anti–PD-1) with ipilimumab, a monoclonal antibody that targets and inhibits CTLA-4, results in enhanced T cell function and an improved antitumour response, according to the product monograph.2
The recommended dosage of nivolumab is either 3 mg/kg every 2 weeks or 360 mg every 3 weeks, administered as an IV infusion over 30 minutes. The recommended dosage of ipilimumab is 1 mg/kg every 6 weeks, administered as an IV infusion over 30 minutes. Treatment is continued at the same dosage until disease progression or unacceptable toxicity, or for up to 2 years in patients without disease progression. Treatment may also be continued in clinically stable patients with initial evidence of disease progression until disease progression is confirmed. According to the Health Canada product monograph, atypical responses (i.e., an initial transient increase in tumour size or small new lesions within the first few months of treatment followed by tumour shrinkage) have been observed.2
Nivolumab plus ipilimumab for the first-line treatment of MPM underwent an expedited review (Project Orbis) at Health Canada. The requested reimbursement criteria aligns with the Health Canada indication. Bristol Myers Squibb Canada, the sponsor, is requesting reimbursement of nivolumab in combination with ipilimumab for the first-line treatment of adult patients with unresectable MPM.1 The FDA approved nivolumab plus ipilimumab for this indication in October 2020.20
The combination of nivolumab plus ipilimumab has been previously reviewed by CADTH for the following indications:
First-line treatment of patients with metastatic or recurrent non–small cell lung cancer with no epidermal growth factor receptor or anaplastic lymphoma kinase genomic tumour aberrations
Treatment of intermediate- and poor-risk patients with previously untreated, advanced, or metastatic renal cell carcinoma
Treatment-naive adult patients with advanced (unresectable or metastatic) melanoma, regardless of BRAF status.
Table 3: Key Characteristics of Key Treatments for First-line Systemic Treatment of MPM
Characteristic | Nivolumab | Ipilimumab | Pemetrexed | Cisplatin | Carboplatin |
|---|---|---|---|---|---|
Mechanism of action | PD-1 inhibitor | CTLA-4 inhibitor | Antifolate antimetabolite | Platinum-based alkylating agent | Platinum-based alkylating agent |
Indicationa | Nivolumab in combination with ipilimumab is indicated for the treatment of adult patients with unresectable MPM who have not received prior systemic therapy for MPM | In combination with cisplatin for the first-line treatment of patients with MPM whose disease is unresectable or who are otherwise not candidates for curative surgery | None | None | |
Route of administration | IV infusion | IV infusion | IV infusion | IV infusion | IV infusion |
Recommended dosage | 3 mg/kg every 2 weeks or 360 mg every 3 weeks | 1 mg/kg every 6 weeks | 500 mg/m2 every 3 weeks | 75 mg/m2 every 3 weeks | AUC 5 every 3 weeks |
Serious adverse events or safety issues | IMAEs | IMAEs | Cutaneous reactions GI-related toxicity Hepatotoxicity Interstitial pneumonitis Myelosuppression | Cardiovascular toxicity Hypersensitivity Myelosuppression Nephrotoxicity Neurotoxicity Ototoxicity | Hypersensitivity Myelosuppression Nephrotoxicity Neurotoxicity |
Treatment duration | 2 years maximum | 2 years maximum | 6 cycles | 6 cycles | 6 cycles |
CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4; GI = gastrointestinal; IV = IV; IMAE = immune-mediated adverse event; MPM = malignant pleural mesothelioma; PD-1 = programmed cell-death protein 1.
aHealth Canada–approved indication for condition under review, according to product monographs.
Source: Sponsor’s submission,1 Opdivo (nivolumab) product monograph,2 Yervoy (ipilimumab) product monograph,3 Alimta (pemetrexed disodium) product monograph,18 Cisplatin Injection product monograph,21 Carboplatin Injection product monograph,22 and National Comprehensive Cancer Guidelines.8
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. Quotes are reproduced as they appeared in the survey, with no modifications made for spelling, punctuation, or grammar. The statistical data that are reported have also been reproduced as is, according to the submission and without modification.
About the Patient Groups and Information Gathered
Lung Cancer Canada and the Canadian Mesothelioma Foundation submitted joint patient input for this review. A registered national charity, LCC is the only organization in Canada focused exclusively on lung cancer. The Canadian Mesothelioma Foundation is a registered charity dedicated to raising awareness and understanding about mesothelioma in Canada.
Information incorporated into their input was collected by conducting surveys, interviews, and an environmental scan. Interviews included 4 patients and 1 caregiver, and the environmental scan included 1 patient and 1 caregiver. Of the 7 patients who provided input, 3 were located in Canada and 2 in the US. Four were male and 3 were female. Most were 70 years of age or older (n = 4).
Surveys of mesothelioma patients and their caregivers were also undertaken, and the data were accessed between October and November 2020. Ten patient respondents completed the survey. Ninety percent of respondents had been diagnosed with MPM and 10% with peritoneal mesothelioma. Approximately half of patient respondents were 65 years of age or older, 36% were 55 to 64 years of age; and 18% were 45 to 54 years of age. Forty-five percent of patient respondents were from British Columbia, 18% were from Ontario, and the remaining 37% were split evenly among Alberta, Saskatchewan, New Brunswick, and Newfoundland and Labrador. Thirty percent reported having metastatic or advanced disease, 40% reported that their disease was not metastatic or advanced, and 30% were not sure. Nearly 2-thirds were currently living with mesothelioma and 1-third had been diagnosed with mesothelioma in the past and were currently cancer-free. Twenty-three caregiver respondents answered the survey. Forty-eight percent were currently caring for someone living with mesothelioma and 52% had previously cared for someone living with mesothelioma. Of 19 caregiver respondents, 53% have or had spent less than a year providing care, 26% have or had spent 1 to 2 years providing care, 16% have or had spent 3 to 5 years providing care, and 5% have or had spent more than 5 years providing care.
Disease Experience
The Canadian Mesothelioma Foundation and LCC stated that a diagnosis of mesothelioma can be devastating. Not only is this an aggressive disease, but it also has a poor prognosis with no known cure, and there are few treatment options. Many of the patients diagnosed were exposed to asbestos while performing their duties as asbestos miners; electricians; plumbers; builders in various sectors such as shipyards, factories, and construction workers; or, in some cases, washing the clothes of a loved 1 working in these industries. With few treatment options for this group of patients, there is an unmet need for treatments that work, prolong survival, and delay progression while allowing patients to have a good quality of life.
Just over half the patients who completed the survey were working full-time outside of the home at diagnosis; the remainder were either retired or had left the workforce before their diagnosis. Of the 5 patients who were working full-time, 3 reported they had often had to reduce the number of hours they worked because of their illness, while 2 reported they had quit their job. More than half of the respondents reported that their mesothelioma has negatively affected their financial situation and nearly all reported that their experience with mesothelioma has been stressful (20% reported it was moderately stressful, 70% reported it was extremely stressful). All patients reported that their mesothelioma affected their quality of life, including functionality, activity levels, and independence.
Due to the aggressiveness of the disease and late stage of diagnosis, new treatment options for MPM that can allow patients to live longer with a good quality of life are needed, as many of these patients do not have the time to wait.
Of the 11 caregivers who were working at the time of diagnosis, 7 reported they sometimes had to reduce the number of hours they worked because of their loved 1’s illness, while 4 reported they had quit their job entirely. One caregiver stated, “the whole course of our lives changed from both of us being self-employed at home and gradually heading into retirement to suddenly stopping.”
When caregivers were asked about the primary aspects of mesothelioma treatment that were the most difficult to manage, the most frequent response was “managing the symptoms of mesothelioma,” followed by “managing side effects of treatments.” One caregiver reported, “initially my husband was able to manage most of the risks, side effects, and travel requirements on his own. But as the tumour growth has increased, I have had to step in and assist him. The emotional toll his disease has taken on myself and our children is immeasurable.” Another caregiver who lost their father to mesothelioma shared this experience: “It was horrible for all, but especially my dad who suffered greatly. Watching that was the absolute worst part of it.”
Experience With Treatment
Ninety percent of patients responding to the survey reported that they had received some form of treatment. Radiation alone or in combination with other treatments was most frequently mentioned (n = 7), with nearly half of these (n = 3) reporting that they had received a combination of radiation, chemotherapy, and immunotherapy. The use of chemotherapy is standard of care, but patients have progressed on this form of treatment. One patient who was diagnosed with MPM in 2017 had 13 sessions of chemotherapy but progressed after the 12th session and was then switched to immunotherapy. Chemotherapy is also known for toxic side effects, including extreme fatigue, nausea, vomiting, diarrhea, and a low blood count. The top 3 most difficult aspects of treatment reported by patients were the side effects of treatment (100% of respondents), fear of the unknown (90% of respondents), and having to travel or commute to the hospital (44% of respondents). The most difficult side effects of treatment reported were fatigue or a lack of energy (67% of respondents), followed by pain (44% of respondents), breathing issues caused or worsened by treatment (44% of respondents), and nausea and vomiting (44% of respondents).
Multiple patient respondents described their experiences with nivolumab and ipilimumab. Many patients reported that, after taking the combination treatment of nivolumab plus ipilimumab, their tumours shrunk considerably and they have a much better quality of life. One patient respondent spoke to how, after progressing on chemotherapy, they were switched to nivolumab plus ipilimumab, and after 2 months of treatment, the respondent’s tumours shrunk by 50%. Patients who have received treatment with nivolumab plus ipilimumab reported improved symptoms and greater functionality and independence. One patient described how the treatment changed his life completely, stating, “I see and feel improvements.” Since starting nivolumab plus ipilimumab, the patient says he feels as if nothing is wrong.
One patient respondent spoke to how they were required to stop the treatment with nivolumab plus ipilimumab temporarily due to elevated liver enzymes. Another patient indicated that their adrenal gland stopped working, and they now take steroids for treatment. However, other patient respondents reported manageable side effects overall.
Improved Outcomes
Patients reported a preference for durable treatments that alleviate symptoms, delay disease progression, provide better quality of life, prolong survival, and have manageable side effects.
Patients with mesothelioma, in particular those who are not entitled to benefits under the workers’ compensation system because they were not workers at the time of their exposure, are also looking for equitable access to treatments.
Clinician Input
Input from Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 3 clinical specialists with expertise in the diagnosis and management of MPM.
Unmet Needs
Malignant pleural mesothelioma is an aggressive cancer with poor prognosis. There is consensus among the clinical experts that there is a significant unmet need in this patient population. Patients most often present with advanced disease, and treatment options are currently limited. Chemotherapy, the standard treatment, prolongs survival, particularly in patients with the epithelioid subtype, although it is not ideal and is associated with significant toxicity. Treatment that prolongs survival further is needed in patients diagnosed with MPM.
Place in Therapy
The clinical experts consulted for this review anticipated that if nivolumab plus ipilimumab becomes available for the requested target population, it will be the preferred first-line systemic treatment of unresectable MPM in patients who have eligible ECOG performance status and no contraindications. Chemotherapy remains an important alternative first-line therapy.
Patient Population
The reimbursement request aligns with the patient population with unmet needs. Patients diagnosed with the sarcomatoid or non-epithelioid subtype typically have the greatest unmet need as chemotherapy is not rarely effective and the subtype is more challenging to treat than the epithelioid subtype. Therefore, a treatment that demonstrates improvement in OS in the subgroup of patients with the non-epithelioid subtype would be useful. Further evidence is required to better understand the potential difference in treatment effect on the different subtypes of MPM. Currently there is no difference in treatment approaches based on histological subtype. As prognosis is overall poor, nivolumab plus ipilimumab is considered an improvement in available treatment options for the full population of patients in the reimbursement request.
Assessing Response to Treatment
Overall survival is considered the most important and clinically meaningful end point in this patient population.
CheckMate 743 explored several secondary end points, including PFS, that did not show favourable results for immunotherapy. However, the clinical experts noted that the benefit of immunotherapy must be evaluated within the context of how patients respond to different treatments. Values such as median PFS do not necessarily provide a meaningful measure of comparative effects of immunotherapy and chemotherapy, nor do they fully define the benefit of either treatment over the other. The PFS Kaplan–Meier curves crossed in this trial, suggesting that patients with unresectable MPM who derive a benefit from immunotherapy can experience long-term gains. Treatment with immunotherapy may have a substantial effect on some patients, which leads to a long-term benefit that contributes to significant survival and quality-of-life gains.
Discontinuing Treatment
The decision to continue or discontinue treatment is based on the patient’s tolerability of the drug(s) and evidence of disease control. With the currently available treatment, patients who are experiencing benefits (e.g., symptomatically) may be continued on treatment even without a clear radiographic response. Immunotherapy may also be continued if the patient is deriving a clinical benefit from treatment. Treatment will be discontinued if there is a compelling reason in the form of, for example, clear progression (radiological or clinical) of disease or intolerable adverse reactions. With certain immune-related AEs that lead to discontinuation of treatment (e.g., ≥ grade 3 pneumonitis or colitis), restarting immunotherapy is generally not recommended even after resolution of the AE.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Two registered joint clinician inputs were provided for the review of nivolumab in combination with ipilimumab for the first-line treatment of adult patients with unresectable MPM. One joint input was on behalf of 4 clinicians and 1 pharmacist from Ontario Health’s CCO Lung Cancer Drug Advisory Committee, and another was from LCC on behalf of 13 clinicians from across the country.
Unmet Needs
Both clinician groups stated that there is a considerable unmet need in the population within the funding request for more efficacious and less-toxic systemic therapy. These patients are often older than 70 years of age and have significant cardiac, pulmonary, and other comorbidities, including other asbestos-related pulmonary diseases. These patients are rarely surgical candidates. The LCC clinicians noted that only select mesothelioma patients who are young, healthy, at clinical stage I, II, or selected stage IIIA, and of the epithelioid subtype can be considered for aggressive extrapleural pneumonectomy or extensive pleurectomy, hemithoracic radiation, and/or chemotherapy. More than 85% of patients will be deemed unresectable and have a median survival of 12 months. For those who can undergo aggressive resection, the median survival is up to 29 months. Cho et al. reported a 3-year OS rate of 58% in a highly selective group of mesothelioma patients with clinical stage T1 to 3N0M0 (T1 to 3 primary tumour size/extent, no regional lymph node metastases, and no distant metastases) and good performance in lung and cardiac function who underwent preoperative radiation and extrapleural pneumonectomy.23 Those with non-epithelioid histology had a 3-year OS rate of 18% as compared to 58% among those who had epithelioid subtype. At the time of recurrence in these surgically resected patients, palliative systemic therapy will be offered.
Place in Therapy
Both clinician groups identified that the current standard of care for this patient population is pemetrexed plus platinum.
Clinicians at LCC stated that any person with newly diagnosed pleural and peritoneal mesothelioma who has no contraindications should be offered nivolumab and ipilimumab as first-line therapy. Patients who have a recurrence of mesothelioma after initial curative surgery with or without (neo)adjuvant chemotherapy should also be allowed to use this combination. The benefit may be particularly clinically significant in those with non-epithelioid subtypes. Patients who have active autoimmune disease requiring more than 10 mg daily of a steroid (prednisone or equivalent) or other immunosuppressants may not be considered for this combination.
Clinicians from LCC stated that patients who have received prior palliative chemotherapy and now have disease progression would also be considered for treatment with nivolumab plus ipilimumab as second-line therapy.
Both clinician groups had experience with nivolumab plus ipilimumab. Clinicians at CCO anticipate that nivolumab plus ipilimumab will replace pemetrexed plus platinum as first-line therapy and be the preferred therapy for most patients (70% to 80%). Additionally, as a subsequent systemic therapy after immunotherapy failure, patients who do not benefit from nivolumab plus ipilimumab will be treated with pemetrexed plus platinum (chemotherapy), although no clinical data are available to date. However, because not all patients will be candidates for first-line nivolumab plus ipilimumab then pemetrexed plus platinum (or vice versa) because of contraindications, it is important to have treatment options for these patients. As CheckMate 743 was unpublished at the time of the clinician input, and based on use of nivolumab plus ipilimumab in other contexts, it is predicted by CCO clinicians that this combination will have toxicities that exceed those of pemetrexed plus platinum in many cases.
Patient Population
CCO clinicians indicated that the reimbursement request aligns with the unmet need in this therapeutic space. Based on the information available at the time of input (i.e., trial abstract and presentation at World Conference on Lung Cancer), the CheckMate 743 trial criteria are appropriate for practice. This reimbursement request is appropriate for all MPM patients. There are no patient subgroups within the study population to which the new treatment should be limited, regardless of histology.
Patients who are treatment-naive with unresectable mesothelioma and an ECOG performance status of 0 to 1, which represents the majority of the incurable mesothelioma patients who are seen in the Canadian cancer centres, are the target population.24 Like other immunotherapy trials in various disease sites, patients with an ECOG performance status of 2 were excluded. Although there was no study of this combination in mesothelioma patients with an ECOG performance status of 2, the CheckMate 817 study reported treatment-naive, metastatic non–small cell lung cancer patients with an ECOG performance status of 2 treated with nivolumab and ipilimumab had an inferior median OS (9.9 months versus 17 months) and median PFS compared with those who had an ECOG performance status of 0 to 1 but experienced similar toxicity.25,26 It is unclear if treatment-naive, incurable mesothelioma patients with an ECOG performance status of 2 will benefit from the nivolumab and ipilimumab combination due to a lack of relevant data. However, this patient population may experience significant toxicity or be reluctant to undergo treatment with pemetrexed plus platinum. The combination of nivolumab plus ipilimumab would therefore be considered an option for this subpopulation of mesothelioma patients in practice, particularly those with non-epithelioid mesothelioma, given the significant benefit reported in CheckMate 743.24
Discontinuing Treatment
Clinicians from LCC stated that AEs are an important consideration for discontinuing therapy. Thoracic oncologists are familiar with management of toxicity from immunotherapy (e.g., anti–PD-1 and/or anti–CTLA-4 antibodies) from their clinical practice.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Eligible patient population | |
In view of the characteristics of the included patient population and exclusion criteria in the CheckMate 743 trial, PAG is seeking clarity on whether the following patients would be eligible for treatment with nivolumab in combination with ipilimumab:
| CheckMate 743 was limited to patients with an ECOG PS of 0 or 1. The clinical experts indicated it would be reasonable to offer nivolumab plus ipilimumab to patients with a good performance status. Clinicians selectively offer targeted therapies to patients with an ECOG PS of 2 or greater as ECOG PS may be related to the underlying disease/tumour symptoms. The clinical experts noted that CNS metastases are rare in MPM and it is reasonable to make patients with controlled brain metastases eligible for nivolumab plus ipilimumab. There is currently no evidence supporting treatment with nivolumab plus ipilimumab based on PD-L1 expression (≥ 50%, < 50%, others), therefore PD-L1 expression should not be used to determine whether patients should be eligible for nivolumab plus ipilimumab. There is currently insufficient evidence supporting treatment with nivolumab plus ipilimumab in patients with unresectable malignant peritoneal mesothelioma. |
Implementation factors | |
The recommended dosage is nivolumab 3 mg/kg every 2 weeks plus ipilimumab 1 mg/kg every 6 weeks, up to 24 months, toxicity, or progression or nivolumab 360 mg every 3 weeks plus ipilimumab 1 mg/kg every 6 weeks, for up to 24 months or until unacceptable toxicity or progression. PAG is seeking a clear definition of “disease progression.” Because the dosing schedule for nivolumab is 3 mg/kg every 2 weeks or 360 mg every 3 weeks, PAG is seeking confirmation whether there is potential to use the weight-based dosing up to a cap (e.g., 4.5 mg/kg to dose cap of 360 mg every 3 weeks). | The trial evaluated a weight-based dosing schedule of nivolumab plus ipilimumab (i.e., without a cap). The clinical experts felt it was reasonable for provinces, based on approved dosing schedules in other settings (e.g., non–small cell lung cancer) and financial considerations, to provide nivolumab plus ipilimumab in weight-based dosing up to a cap (e.g., 4.5 mg/kg to dose cap of 360 mg every 3 weeks). |
Sequencing and priority of treatments | |
The PAG is seeking to confirm the place in therapy and sequencing with nivolumab in combination with ipilimumab in the scenarios below:
| Most patients in the CheckMate 743 trial stopped treatment due to progression. For other scenarios, the clinical experts noted it would be appropriate for patients to be re-treated with nivolumab plus ipilimumab after relapse or in instances where they have discontinued treatment due to toxicity (e.g., after at least 6 months disease-free/stable from last treatment/discontinuation of treatment). There is currently insufficient evidence supporting nivolumab-ipilimumab in patients who have received prior systemic treatment for MPM. After failure of nivolumab plus ipilimumab, standard chemotherapies (e.g., platinum/pemetrexed then gemcitabine or vinorelbine) should remain available. The clinical experts indicated it was reasonable to continue with single-drug nivolumab if patients have difficulty tolerating the nivolumab plus ipilimumab combination; this would align with current treatment practices. In CheckMate 743, patients were permitted to continue nivolumab treatment alone when ipilimumab was discontinued due to toxicity. During the trial, 18 patients (6.0%) discontinued ipilimumab prematurely due to an adverse event. |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group performance status; MPM = malignant pleural mesothelioma; PAG = Provincial Advisory Group; PD-L1 = programmed cell-death ligand 1.
Clinical Evidence
The clinical evidence included in the review of nivolumab plus ipilimumab is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and selected from the literature that met the selection criteria specified in the review. No additional relevant studies were identified that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objective
The objective is to perform a systematic review of the beneficial and harmful effects of nivolumab plus ipilimumab for first-line treatment of adult patients with unresectable MPM.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered important by patients, clinicians, and drug plans.
The systematic review protocol presented in Table 5 was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adults (≥ 18 years of age) with treatment-naive, unresectable MPM Subgroups:
|
Intervention | Nivolumab 3 mg/kg IV every 2 weeks plus ipilimumab 1 mg/kg IV every 6 weeks or Nivolumab 360 mg IV every 3 weeks plus ipilimumab 1 mg/kg IV every 6 weeks Administered until intolerable toxicity or disease progression occurs, up to 24 months |
Comparators | Pemetrexed plus cisplatin Pemetrexed plus carboplatin Administered until intolerable toxicity or disease progression occurs, usually up to 6 cycles |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; ECOG PS = Eastern Cooperative Oncology Group performance status; HRQoL = health-related quality of life; MPM = malignant pleural mesothelioma; PD-L1 = programmed cell-death ligand 1; SAE = serious adverse event; TNM = tumour, node, metastases; WDAE = withdrawal due to adverse event.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).27
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Opdivo (nivolumab), Yervoy (ipilimumab), and mesothelioma. Clinical trials registries searched were the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on November 26, 2020. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on April 15, 2020.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).28 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
These searches were supplemented through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings from the Literature
One study was identified for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6: A list of excluded studies is presented in Appendix 2.
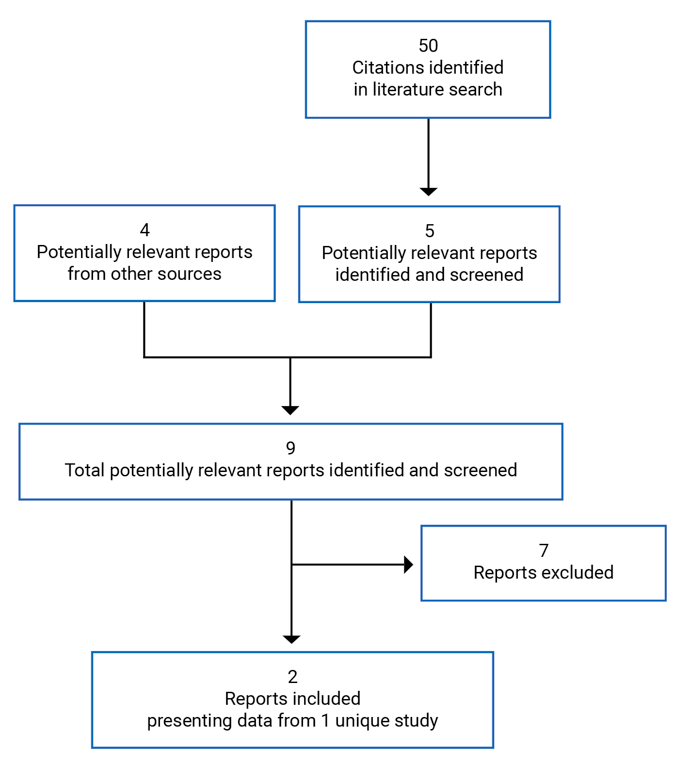
Table 6: Details of Included Studies
CheckMate 743 | |
|---|---|
Designs & Populations | |
Study design | Phase III, multi-centre, open-label, active-controlled RCT |
Locations | 103 sites in 21 countries: Australia, Belgium, Brazil, Chile, China, Colombia, France, Germany, Greece, Italy, Japan, Mexico, Netherlands, Poland, Romania, Russia, South Africa, Switzerland, Turkey, UK, and US |
Patient enrolment dates | November 28, 2016, to April 18, 2018 |
Data cut-off | Overall survival analysis: March 25, 2020 (Database lock: April 3, 2020) |
Randomized (N) | 605 patients:
|
Inclusion criteria | Male and female adults (≥ 18 years) Histologically proven diagnosis of MPM, with measurable diseasea Advanced disease not amenable to curative therapy (i.e., surgery ± chemotherapy) ECOG PS 0 to 1 Adequate hematological, renal, hepatic function Available pathological sample for centralized PD-L1 immunohistochemistry testing |
Exclusion criteria | Primitive peritoneal, pericardial and tunica vaginalis testis mesotheliomas Brain metastasisb Prior MPM treatment with adjuvant or neoadjuvant chemotherapy, radical pleuropneumonectomy (± intensity modulated RT), or non-palliative RTc Prior treatment with an antibody or drug specifically targeting T cell co-stimulation or checkpoint pathways (e.g., anti–PD-1, anti–PD-L1, anti–PD-L2, anti–CTLA-4 antibody) Prior intraoperative or intracavitary chemotherapy for pleural mesothelioma History of chronic inflammatory or autoimmune diseased Prior or concurrent malignancy that requires or is anticipated to require concurrent intervention Interstitial lung disease that is symptomatic, or has potential to interfere with the detection or management of suspected drug-related pulmonary toxicity |
Drugs | |
Intervention | Nivolumab plus ipilimumab:
Administered as infusions until disease progression or unacceptable toxicity (maximum 2 years). |
Comparator(s) | Chemotherapy (pemetrexed plus cisplatin or carboplatin):
Administered as infusions on day 1 of each 21-day cycle until disease progression, unacceptable toxicity, or completion of 6 cycles. |
Outcomes | |
Primary end point | Overall survival |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publicationsf | Bass et al. (2020)29 Clinicaltrials.gov (NCT02899299)30 |
AUC = area under the plasma drug concentration-time curve; CTLA-4 = cytotoxic T-lymphocyte-associated protein 4; ECOG PS = Eastern Cooperative Oncology Group performance status; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels; HRQoL = health-related quality of life; IV = IV; LCSS-Meso = Lung Cancer Symptom Score–mesothelioma; MPM = malignant pleural mesothelioma; m-RECIST = modified Response Evaluation Criteria in Solid Tumors; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PD-1 = programmed cell-death protein 1; PD-L1 = programmed cell-death ligand 1; PD-L2 = programmed cell-death ligand 2; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; RCT = randomized controlled trial; RT = radiotherapy.
aDetermination of epithelioid vs. non-epithelioid histology was required. Measurable disease was defined as at least 1 lesion, measured in up to 2 positions at 3 separate levels on transvers cuts (at least 10 mm apart) of the CT scan, that can be repeatedly assessed using an adapted m-RECIST for pleural mesothelioma. Non-pleural metastatic target lesions were measured unidimensionally using the RECIST 1.1 criteria. Patients without measurable pleural lesions but with target metastatic lesions (as per RECIST 1.1 criteria) may have been included in the trial upon consultation with the medical monitor.
bPatients with brain metastases were excluded except if they were treated with stereotaxic radiotherapy or surgical resection, with no evolution within 3 months before inclusion in the study, and were asymptomatic. Additionally, patients must have discontinued corticosteroid treatment, or be on a stable or decreasing dosage of no more than 10 mg daily of prednisone (or equivalent) for a minimum of 2 weeks before randomization.
cPrior palliative radiotherapy was acceptable, as long as 14 days or more had passed since the administration of radiotherapy, and there were no ongoing signs of toxicity.
dExceptions include type 1 diabetes mellitus, hypothyroidism that requires only hormone replacement, skin disorders (e.g., alopecia, psoriasis, vitiligo) that do not require systemic treatment, or conditions that are not expected to recur in the absence of an external trigger.
eMeasured using adapted m-RECIST and/or RECIST 1.1 criteria, as assessed by the blinded independent central review.
fTwo additional reports/sources of information were included: Sponsor’s submission package1 and Clinical Study Report.10
Source: Sponsor’s submission (pre-submission form),1 Clinical Study Report,10 and sponsor’s response to additional information.11
Description of Studies
CheckMate 743 is an international, open-label, phase III, active-controlled trial that investigated nivolumab in combination with ipilimumab in patients with unresectable MPM. The primary objective was to compare the OS of patients treated with nivolumab plus ipilimumab to patients who received standard of care chemotherapy (pemetrexed plus either cisplatin or carboplatin) in the first-line treatment of unresectable MPM. This international study was conducted at 103 sites in 21 countries, which are listed in Table 6.10 No study sites were located in Canada.1
Radiographic imaging for baseline assessment of disease sites were reviewed centrally, using m-RECIST for mesothelioma criteria and/or RECIST 1.1 criteria.
Eligible patients were assigned in a 1:1 ratio to receive open-label treatment with nivolumab plus ipilimumab or standard of care chemotherapy. Randomization, performed through an interactive web response system, was stratified by tumour histology (epithelioid versus non-epithelioid [sarcomatoid or mixed histology subtype]) and gender (male versus female). The study design is briefly summarized in Figure 2. After discontinuation of treatment, patients entered the post-treatment follow-up phase. Patients who discontinued treatment due to reasons other than disease progression continued to undergo tumour assessments until progression was confirmed by the BICR. All patients were followed for survival every 3 months until death, consent withdrawal, loss to follow-up, or study conclusion.10
Figure 2: Overview of CheckMate 743 Study Design
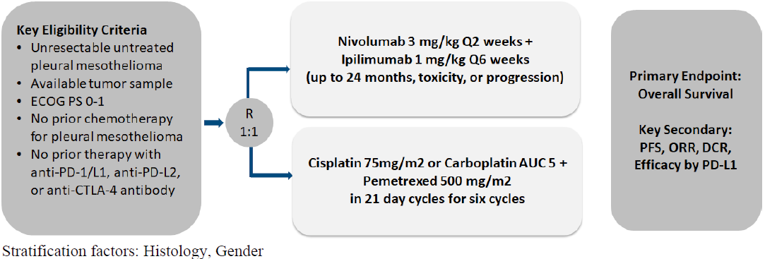
AUC = area under the plasma drug concentration-time curve; CTLA-4 = cytotoxic T-lymphocyte-associated protein 4; DCR = disease control rate; ECOG PS = Eastern Cooperative Oncology Group performance status; ORR = objective response rate; PD-1 = programmed cell-death protein 1; PD-L1 = programmed cell-death ligand 1; PD-L2 = programmed cell-death ligand 2; PFS = progression-free survival; Q2 = every 2 weeks; Q6 = every 6 weeks.
Source: Clinical Study Report.10
The clinical data cut-off date for the interim analysis of OS was March 25, 2020 (minimum of 22.1 months of follow-up), and the clinical cut-off date for all other data was January 15, 2020, based on last patient last visit. Date of interim analysis database lock was April 3, 2020. CheckMate 743 was sponsored by Bristol Myers Squibb.10
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria are outlined in Table 6. Briefly, patients were adults who had histologically proven, advanced, unresectable MPM whose disease was not amenable to curative therapy (i.e., surgery with or without chemotherapy). Enrolled patients had an ECOG performance status of 0 to 1, and they must not have received prior MPM treatment (i.e., adjuvant or neoadjuvant chemotherapy, radical pleuropneumonectomy, non-palliative radiotherapy). Prior treatment with anti–PD-1, anti–PD-L1, anti–programmed cell-death ligand 2, or anti–CTLA-4 were also not permitted. Patients could have received prior palliative radiotherapy, as long as 14 days or more had passed since its administration and there were no ongoing signs of toxicity. Patients with primitive peritoneal, pericardial, and tunica vaginalis testis mesotheliomas were excluded. Individuals with untreated brain metastases were also excluded from this trial.10
Baseline Characteristics
Key baseline and demographic characteristics of the CheckMate 743 study are summarized in Table 7. Of the total number of patients enrolled, the median age was 69 years (range = 25 to 89 years; interquartile range = 64 to 75 years), and the majority were male (77.2%) and White (85.3%). Notably, most enrolled patients had an ECOG performance status of 1 (59.8%), advanced disease at baseline (51.1% had stage IV and 34.5% had stage III), and epithelioid tumour histology (75.4%). Of patients who had non-epithelioid tumour histology, 11.7% had sarcomatoid, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Most patients (58.2%) were enrolled from sites in Europe and 9.8% were enrolled from North America. Baseline demographics and characteristics were generally well balanced between the 2 treatment groups.10
Most patients (96.9%) had tumour samples with quantifiable PD-L1 expression, and PD-L1–positive tumours (i.e., ≥ 1% PD-L1 expression) were identified in 77.0% of patients. A greater number of patients in the nivolumab plus ipilimumab group had baseline PD-L1–positive status (80.3% versus 73.7% chemotherapy). Also, higher PD-L1 expression was seen in patients with non-epithelioid MPM.10
Table 7: Summary of Baseline Characteristics, ITT Population
Characteristic | CheckMate 743 | |
|---|---|---|
Nivolumab plus ipilimumab N = 303 | Chemotherapy N = 302 | |
Age, years | . | |
Mean (standard deviation) | 68.7 (8.5) | 67.8 (9.7) |
Median (range) | 69.0 (32.0 to 85.0) | 69.0 (25.0 to 89.0) |
Gender, n (%) | . | |
Male | 234 (77.2) | 233 (77.2) |
Female | 69 (22.8) | 69 (22.8) |
Race, n (%) | . | . |
White | 266 (87.8) | 250 (82.8) |
Asian | 26 (8.6) | 39 (12.9) |
American Indian or Alaskan native | 2 (0.7) | 4 (1.3) |
Other | 9 (3.0) | 9 (3.0) |
Geographic region, n (%) | . | . |
North America | 32 (10.6) | 27 (8.9) |
Europe | 177 (58.4) | 175 (57.9) |
Asia | 26 (8.6) | 39 (12.9) |
Rest of world | 68 (22.4) | 61 (20.2) |
Disease stage at study entry, n (%) | . | . |
Stage I | 12 (4.0) | 20 (6.6) |
Stage II | 23 (7.6) | 22 (7.3) |
Stage III | 103 (34.0) | 106 (35.1) |
Stage IV | 160 (52.8) | 149 (49.3) |
Not reported | 5 (1.7) | 5 (1.7) |
ECOG PS, n (%) | . | |
0 | 114 (37.6) | 128 (42.4) |
1 | 189 (62.4) | 173 (57.3) |
2 | 0 | 1 (0.3) |
Tumour histology, n (%) | ||
Epithelioid | 229 (75.6) | 227 (75.2) |
Non-epithelioid | 74 (24.4) | 75 (24.8) |
Prior cancer treatment | ||
Systemic therapy | 0 | 0 |
Radiotherapy | 29 (9.6) | 28 (9.3) |
Surgerya | 156 (51.5) | 163 (54.0) |
ECOG PS = Eastern Cooperative Oncology Group performance status.
aMost of the prior surgeries were diagnostic procedures and/or biopsies of the tumour as per protocol, or palliative surgery.
Source: Clinical Study Report.10
Interventions
Study Treatments
Patients were randomized in a 1:1 ratio to 1 of 2 treatment arms, as outlined in Table 8. Treatment was started within 3 days of randomization.
Table 8: Details of Treatment in the CheckMate 743 Safety Population
Detail | Nivolumab plus ipilimumab | Chemotherapy |
|---|---|---|
Treated, N | 300 | 284 |
Cycle length | 6 weeks (42 days) | 3 weeks (21 days) |
Dosage | Nivolumab 3 mg/kg IV infusiona
Ipilimumab 1 mg/kg IV infusiona
Treatment was continued until disease progression, unacceptable toxicity, withdrawal of consent, maximum of 2 years, or study closure, whichever occurred first; patients who initially met the criteria for radiographic disease progression (investigator-assessed and BICR-confirmed) were permitted to continue study treatment, if the patient was still experiencing clinical benefit (according to investigator assessment) and tolerating treatmentb | Pemetrexed 500 mg/m2 IV infusionc
Cisplatin 75 mg/m2 IV infusionc or carboplatin AUC 5 IV infusionc
Cisplatin was preferred for the combination, but carboplatin could have been used at the investigator’s discretion. Treatment was continued until completion of 6 cycles, or until disease progression, unacceptable toxicity, or withdrawal of consent, whichever occurred first |
Premedication | None | The following were administered to reduce hematologic and gastrointestinal toxicityd:
|
Dosing modification key points | Nivolumab plus ipilimumab:
Chemotherapy
| |
Concomitant treatment | Use of immunosuppressive agents and immunosuppressive doses of systemic corticosteroids were not permitted, unless used to treat a drug-related AE. A brief course (< 3 weeks) of corticosteroids for prophylaxis or treatment of non-autoimmune conditions was permitted Patients receiving standard of care chemotherapy and experiencing hematologic toxicity were permitted use of growth factors (e.g., G-CSF and erythropoietin) at the investigator’s discretion. | |
5HT3-RA = 5-HT3 receptor antagonist; AE = adverse event; AUC = area under plasma drug concentration-time curve; BICR = blinded independent central review; G-CSF = granulocyte colony stimulating factor; IM = intramuscular; IV = IV.
aNivolumab plus ipilimumab was infused over 30 minutes each, with ipilimumab following nivolumab administration.
bPatients were permitted to continue nivolumab plus ipilimumab if they: a) were experiencing investigator-assessed clinical benefit; b) were tolerating study drug; c) had stable performance status; d) did not have serious complications of disease progression (e.g., central nervous system metastases) requiring imminent intervention that could be delayed with continuing study treatment; and e) provided written informed consent before receiving further treatment. To determine whether there was a reduction in tumour size or continued disease progression, a follow-up scan was performed within 6 weeks (± 7 days) of the original progressive disease. Treatment was then discontinued in patients who experienced further progression, defined as an additional 10% increase in tumour burden, with at least a 5 mm absolute increase from time of initial progressive disease. This definition also included an increase in the sum of the diameters of all target lesions and/or the diameters of new measurable lesions since initial progressive disease.
cPemetrexed was infused over 10 minutes; cisplatin and carboplatin were administered as per label and/or local policy.
dPremedication administration notes:
• Anti-emetics were administered according to local standards before study drug infusions.
• Dexamethasone (or equivalent corticosteroid) could have been administered as per local policy or be given as IV infusion on the day of treatment.
• Folic acid was started 1 week before the first dose of pemetrexed, continued throughout treatment, and for 21 days after last dose.
• Vitamin B12 injection was given approximately 1 week before first dose of pemetrexed and repeated according to local policy.
Source: Clinical Study Report.10
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further described in the following section. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | CheckMate 743 | Definition and censoring rules |
|---|---|---|
OS | Primary | Time from randomization to the date of death due to any cause. Patients who were alive at the time of data cut-off were censored at the date they were last known to be alive (i.e., date of last contact); patients who were randomized but had no follow-up were censored at the date of randomization. |
PFS | Secondary | Two definitions were used in the analysis of PFS: 1. Primary definition: time from date of randomization to the date that the first of the following occurred: a) first documented tumour progression according to BICR assessment using adapted m-RECIST and/or RECIST 1.1 criteria, or b) death due to any cause. This definition also accounted for subsequent therapy, such that patients who received subsequent anti-cancer treatment were censored (truncated) at the date of last evaluable tumour assessment conducted on or before starting subsequent therapy. This was applicable to patients who received subsequent treatment before documented progression as well as those who did not experience documented progression. Patients who did not experience disease progression or death (and did not receive subsequent therapy) were censored on the date of the last evaluable tumour assessment. Patients who did not experience death and did not have any on-study tumour assessments were censored on the date of randomization. Patients who died without reported disease progression were considered to have progressed on the date of death. 2. Secondary definition: similar to the primary definition, but patients who initiated subsequent anti-cancer treatment were not censored, and as such the ITT population was used in the analysis. For the purpose of determining PFS, clinical deterioration in the absence of unequivocal evidence of disease progression, as per adapted m-RECIST and/or RECIST 1.1 criteria, was not considered as progression. |
ORR | Secondary | The number of patients who achieved a best response of complete or partial response as measured by the BICR using adapted m-RECIST and/or RECIST 1.1 criteria, divided by the number of all patients randomized into the trial. The BOR was defined as the best response between date of randomization and date of objectively documented disease progression or the date of subsequent therapy (including tumour-directed surgery and radiotherapy), whichever occurred sooner. Patients without documented disease progression or subsequent treatment will have a BOR determined according to all available response designations. After initial response, confirmation was required at least 4 weeks later. As part of ORR analysis, TTR and DOR were also evaluated. |
DCR | Secondary | The proportion of patients who achieved a best overall response of completed or partial response or stable disease as measured by the BICR using adapted m-RECIST and/or RECIST 1.1 criteria. |
PD-L1 expressiona | Secondary | Whether PD-L1 expression is a predictive biomarker for response was evaluated for OS, PFS, ORR results. The definition of quantifiable PD-L1 expression was the percent of tumour cells membrane staining in a minimum of 100 evaluable tumour cells according to the validated Dako PD-L1 immunohistochemistry assay. PD-L1 staining that could not be quantified were categorized as either indeterminate (due to biology of the tissue sample) or not evaluable (due to improper sample collection, preparation, or handling). All PD-L1 tested subjects (i.e., randomized patients who had a tumour biopsy specimen assessed) were used in this analysis. |
EQ-5D-3L | Exploratory | Assessment of overall health status and health utility used the EQ-5D-3L Visual Analogue Scale and utility index. |
LCSS-Meso | Exploratory | Assessment was according to cancer-related symptoms and quality of life. |
BICR = blinded independent central review; BOR = best overall response; DOR = duration of response; EQ-5D-3L = EuroQol 5-Dimensions 3-Level; ITT = intention-to-treat; LCSS-Meso = Lung Cancer Symptom Score–mesothelioma; m-RECIST = modified Response Evaluation Criteria in Solid Tumors; ORR = objective response rate; OS = overall survival; PD-L1 = programmed cell-death ligand 1; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; TTR = time to response.
aPD-L1 expression status was identified as a subgroup of interest in the CADTH review protocol. In the CheckMate 743 trial, PD-L1 expression was included in the subgroup analyses as was a secondary end point, and therefore was included in this table.
Source: Clinical Study Report.10
EuroQol 5-Dimensions 3-Levels Questionnaire
Measures of general health status using the EQ-5D-3L was an exploratory end point of the CheckMate 743 trial. Currently, the validity and reliability of this questionnaire has not been evaluated specifically in patients with MPM, nor has an MID been established (see Appendix 4 for details). The EQ-5D-3L consists of 2 parts:
A descriptive section comprised of 5 dimensions. Each of the 5 dimensions (i.e., anxiety/depression, pain/discomfort, mobility, self-care, usual activities) has 3 response levels reflecting health and well-being (i.e., no problems, moderate problems, and extreme problems). The health utility index values were calculated according to a scoring algorithm based on time-trade-off values based on the UK population. In CheckMate 743, an MID for clinically meaningful change was deemed a change from baseline of 0.08 in the utility index score.
A visual analogue scale (VAS) that provides a quantitative measure by recording a respondent’s self-rated health on a 101-point scale between the best health to the worst health the patient can imagine. Global scores can be measured, with higher scores indicating better HRQoL An MID was considered a change from baseline of 7.10
Questionnaires were completed at baseline according to a specific schedule outlining designated time windows corresponding to different time points during the study. Briefly, assessments in the nivolumab plus ipilimumab group were performed before each nivolumab dose through 12 weeks after the initial dose (i.e., cycle 3, day 1), every 6 weeks thereafter for the first 12 months, and then every 12 weeks until study discontinuation. Assessments in the standard of care chemotherapy group were performed before each treatment through 12 weeks after the initial dose (i.e., cycle 5, day 1), every 6 weeks thereafter for the first 12 months, and then every 12 weeks until study progression. After discontinuation of treatment, assessments were performed during follow-up visits 1 (30 ± 7 days from last dose) and 2 (90 ± 7 days from follow-up visit 1), every 3 months during the first year of the survival follow-up phase, then every 6 months thereafter. Analysis of data was performed in all randomized patients who had a valid assessment before administration of treatment on cycle 1, day 1, and at least 1 subsequent assessment while receiving treatment. A questionnaire completion rate (i.e., proportion of questionnaires actually received out of the number of questionnaires expected) was calculated at each assessment.10
Lung Cancer Symptom Score
Disease-related symptoms were measured using the LCSS-Meso. Disease-related symptom deterioration rate by week 12 was also an exploratory end point, defined as the proportion of randomized patients who experienced an increase of 10 points or greater from baseline in the Average Symptom Burden Index (ASBI) score, from randomization to week 12.10
The original LCSS scale reports 6 symptom-specific questions (coughing, dyspnea, fatigue, pain, hemoptysis, and anorexia) and 3 summary scores (symptom distress, interference with activity level, and global HRQoL). To adapt the scale to mesothelioma, the hemoptysis item was removed, leaving 5 disease-related symptoms. The responses were captured using a VAS, with scores for individual items ranging from 0 (no symptoms; highest quality of life) to 100 (worst symptoms or quality of life). The ASBI score was derived by averaging the symptom-related item scores, and a change in ASBI score of 10 points was deemed clinically meaningful. Although no validated MID was identified in patients with MPM, the LCSS-Meso questionnaire has been assessed for validity, reliability, and feasibility in this population (Appendix 4). All LCSS-Meso questionnaires were completed according to the same schedule as the EQ-5D-3L. However, after study discontinuation, LCSS-Meso was only collected during follow-up visits 1 and 2. Data from the LCSS-Meso and compliance were analyzed in the same population and manner as the EQ-5D-3L data.10
Safety Outcomes
The CheckMate 743 trial included assessment of the following safety parameters: AEs, SAEs, AEs leading to discontinuation, AEs leading to dose modification, and death. Adverse events were defined per standard definitions.10
Investigators also analyzed IMAEs that met specific criteria, regardless of causality (i.e., occurring within 100 days of last dose, treated with immune-modulating medications [except for endocrine IMAEs], with no clear alternate etiology or an immune-mediated component).10
Statistical Analysis
Sample Size
Sample size was determined based on a comparison of the primary end point of OS between the 2 treatment groups, with approximately 600 patients planned for randomization. To detect an average HR of 0.72, approximately 473 events (i.e., deaths) were required to achieve 90% overall power, with the difference detected using a log-rank test at a 2-sided significance level of 0.05. For the chemotherapy group, an assumption of an exponential distribution was made, with a median OS of 16 months and an HR of 0.04. Assumptions for the nivolumab plus ipilimumab group were derived from a piecewise exponential model to capture features of immunotherapy survival curves.10
One formal interim OS analysis was planned for superiority testing at approximately 85% of total events (403 deaths). The numbers of events required for the interim and final OS analyses were estimated to occur at approximately 39 months and 56 months, respectively, assuming an accrual rate of 34 patients per month. A group sequential design was used to test the OS end point to account for conducting only a single interim analysis. An alpha spending using the Lan-DeMets method to approximate the O’Brien-Fleming boundaries was applied to control for the overall type I error rate at a 2-sided significance level of 0.05. The projected stopping boundaries were based on the exact number of deaths, with an estimated 2-sided significance level of 0.03 at the interim analysis, and 0.041 at final analysis.10
At the time of the database lock (April 3, 2020), 605 patients had been randomized, and 419 deaths were recorded. Based on this observation, the adjusted 2-sided alpha level was 0.0345 for the first interim analysis of OS. With a P value of 0.0020, the boundary for statistical significance was crossed. As such, the trial was stopped early at the interim analysis for superiority of OS, and the P value from the stratified log-rank test was considered the final primary analysis result.10
Primary Outcome
Overall survival between the 2 treatment groups was compared using a log-rank test stratified for tumour histology and gender. The HR and corresponding 2-sided CI were estimated using a stratified Cox PH model, using the randomized arm as a single covariate. The OS curves was estimated for each treatment group using the Kaplan–Meier product-limit method. The log-log transformation method was applied to the Brookmeyer and Crowley method to calculate the 2-sided 95% CI for median OS in each treatment group. OS rates at specific time points (i.e., 6, 12, 18, 24, 36, 48 months and 5 years) were also estimated using the Kaplan–Meier approach, with corresponding CIs derived from the Greenwood formula for variance deviation and application of log-log transformation to the survivor function. Patients who were alive at the time of data cut-off were censored at the date they were last known to be alive (i.e., date of last contact); patients who were randomized but had no follow-up were censored at the date of randomization.10
Several sensitivity analyses for OS were performed in all randomized patients as follows:
The delayed effect of immunotherapy, which may cause a late separation in the Kaplan–Meier curves and non-proportional hazards (NPH) was studied. A comparison of OS between treatment groups was performed using a 2-sided stratified weighted log-rank test.
Treatment effects were estimated after adjustments for possible imbalance in known or potential prognostic factors by including 2 covariates in addition to the stratification factors used during randomization. Specifically, ECOG performance status (0, ≥ 1) and PD-L1 status (positive, negative, not reported) were added in a multivariate Cox regression model.
Overall survival was examined using an unstratified log-rank test.
The assumptions of PH in the Cox regression model were examined. A time-dependent variable (i.e., treatment by time interaction) was added into the model in addition to treatment. A w-sided Wald chi-square P value of less than 0.1 may indicate a nonconstant treatment effect.10
Exploratory subgroup analyses of the primary end point were performed, including for the following pre-specified variables that are relevant to this review per the protocol (Table 5): ECOG performance status, baseline histology, disease stage at study entry, and PD-L1 status. The influence of these characteristics on the treatment effect were analyzed if the subgroup included more than 10 patients. Median OS was estimated using the Kaplan–Meier product-limit method, with 2-sided 95% CIs. The HRs were calculated from an unstratified Cox PH model.10
Secondary Outcomes
Secondary end points were descriptive, and no formal statistical testing was performed. Statistical methods for estimating PFS in each treatment group, the HR and corresponding 95% CI, rates of PFS at fixed time points, and the PFS curves were similar to those employed in the primary OS analysis. A sensitivity analysis of PFS, as determined by the investigator, was conducted. ORR and DCR estimates, along with the corresponding 2-sided 95% CIs for each treatment group, were calculated using the Clopper-Pearson method. The duration of response was estimated using the Kaplan–Meier product-limit method, with median values and corresponding 95% CIs also calculated using a log-log transformation.10
Exploratory Outcomes
The EQ-5D-3L utility index scores, VAS scores, and post-baseline changes in scores were summarized at each assessment time point using descriptive statistics (i.e., N, mean with standard deviation and 95% CI, median, first and third quartiles, minimum, and maximum). A 95% exact CI for each proportion was calculated using the Clopper-Pearson method. Subjects with missing data were excluded from the analysis.
The LCSS-Meso scores and post-baseline changes in scores for the following components were summarized at each assessment time point using descriptive statistics: 5 items measuring disease-related symptoms; 3 items measuring overall symptom burden, disease-related functional limitations, and quality of life; ASBI; and a 3-item index. The proportion (N) of patients with disease-related symptom deterioration (defined as a clinically meaningful increase in LCSS-Meso ASBI score) was summarized at 12 weeks, and a 95% exact CI for the proportion was calculated using the Clopper-Pearson method.
Analysis Populations
Efficacy analyses were performed in the ITT population, which included all patients randomized to treatment and analyzed according to the treatment group to which they were assigned. Measures of HRQoL were restricted to randomized patients who had a baseline assessment and at least 1 post-baseline assessment. Safety analyses were performed in all treated subjects who received at least 1 dose of any study treatment according to the actual treatment received through the entire treatment period.10
Results
Patient Disposition
Patient disposition for the CheckMate 743 study is summarized in Table 10. A total of 713 patients were screened for inclusion, and 108 patients were excluded, mostly due to failure to meet study criteria (n = 84). A total of 605 patients were randomized to either nivolumab plus ipilimumab (n = 303) or standard of care chemotherapy (n = 302). Three patients in the nivolumab plus ipilimumab group and 18 patients in the chemotherapy group did not receive treatment, resulting in a safety population of 584 patients, of whom 300 received nivolumab plus ipilimumab and 284 received chemotherapy. The main reason for patients not receiving randomized treatment included no longer meeting study criteria (n = 2) in the nivolumab plus ipilimumab group, and withdrawal of consent (n = 11) in the chemotherapy group. Of those who received treatment, 295 patients (98.3%) in the nivolumab plus ipilimumab group and all patients in the chemotherapy group had discontinued randomized treatment by the time of database lock. Only 5 patients remained on treatment, all in the nivolumab plus ipilimumab group. The main reason for treatment discontinuation in the nivolumab plus ipilimumab group was disease progression (60.7%) or study drug toxicity (19.7%). The majority of patients in the chemotherapy group discontinued treatment because they had completed the maximum length of treatment (6 cycles; 62.0%) or experienced disease progression (15.5%).10 Of patients who discontinued treatment, the majority entered the follow-up phase and continued in the study (87% nivolumab plus ipilimumab, 93.3% chemotherapy).11 At the time of database lock, 459 patients (75.9%) had discontinued from the study (218 in the nivolumab plus ipilimumab group and 241 in the chemotherapy group), mainly due to death.10,12
Patient information | CheckMate 743 | |
|---|---|---|
Nivolumab plus ipilimumab | Chemotherapy | |
Screened, N | 713 | |
Randomized (ITT population), N | 303 | 302 |
Treated (safety population), N | 300 | 284 |
Status of randomized patients | N = 303 | N = 302 |
Continuing in study, N (%) | 85 (28.1) | 61 (20.2) |
On treatment | 5 (1.7) | 0 |
In follow-up | 80 (26.4) | 61 (20.2) |
Discontinued completely from study, N (%) | 218 (71.9) | 241 (79.8) |
Death | 200 (66) | 219 (72.5) |
Status of treated patients | N = 300 | N = 284 |
Continuing study treatment, N (%) | 5 (1.7) | 0 |
Discontinued treatment, N (%) | 295 (98.3) | 284 (100) |
Reason for treatment discontinuation, N (%) | ||
Disease progression | 182 (60.7) | 44 (15.5) |
Study drug toxicity | 59 (19.7) | 24 (8.5) |
Adverse event unrelated to study drug | 12 (4.0) | 9 (3.2) |
Subject request to discontinue study drug | 4 (1.3) | 10 (3.5) |
Consent withdrawal | 6 (2.0) | 3 (1.1) |
Lost to follow-up | 0 | 1 (0.4) |
Maximum clinical benefit | 10 (3.3) | 2 (0.7) |
Poor/non-compliance | 1 (0.3) | 0 |
Patient no longer met study criteria | 4 (1.3) | 0 |
Administrative reason (according to sponsor) | 2 (0.7) | 0 |
Other | 11 (3.7) | 2 (0.7) |
Not reporteda | 4 (1.3) | 189 (66.5) |
ITT = intention-to-treat.
aIncludes patients who achieved the maximum duration of therapy according to the protocol (i.e., 2 years of nivolumab plus ipilimumab or 6 cycles of chemotherapy). Three patients in the nivolumab plus ipilimumab group and 176 patients in the chemotherapy group reached maximum duration of therapy.
Source: Clinical Study Report,10 and sponsor’s response to additional information request.12
Exposure to Study Treatments
Details on-study treatment exposure and concomitant therapies are summarized in Table 11.
Table 11: Treatment Exposure and Concomitant Therapies in CheckMate 743
Treatment | Nivolumab plus ipilimumab | Standard of care chemotherapy |
|---|---|---|
Treated, N | 300 | 284 |
Treatment exposure | Duration of treatment:
Treatment beyond initial progression:
Relative dose intensities:
| Duration of treatment:
Platinum agent initiated at cycle 1:
Relative dose intensities:
|
Premature treatment discontinuation | 28 patients (9.3%) discontinued ipilimumab:
Median duration of nivolumab monotherapy after ipilimumab discontinuation: 112.5 days (range 13 to 750 days) | 3 patients (1.1%) discontinued cisplatin or carboplatin 4 patients (1.4%) discontinued pemetrexed All premature discontinuations were due to AEs |
Dosing modification | Nivolumab plus ipilimumab:
| |
Chemotherapy:
| ||
Concomitant treatment | Almost all patients (99.5%) received concomitant medication(s). Examples included (nivolumab plus ipilimumab vs. chemotherapy):
| |
Tumour response assessment | Tumour response was evaluated by CT scan at 6 weeks (± 7 days) from the first dose, then every 6 weeks (± 7 days) for the first 12 months, until week 48. Thereafter, evaluations were performed every 12 weeks (± 7 days) until BICR-confirmed documented disease progression. Tumour response and disease progression was determined by investigator and confirmed by independent central review, using the adapted m-RECIST for mesothelioma and/or RECIST 1.1 criteria. Prior to treatment discontinuation, confirmation of disease progression was required by BICR. If radiographic disease progression was not confirmed by the independent review, study treatment was continued. However, the principal investigator was permitted to make the initial assessment of progression and treatment continuation decision based on safety and evaluation of benefit-risk. Overall, 48 patients (n = 34 nivolumab plus ipilimumab, n = 14 chemotherapy) had treatment discontinued due to investigator-assessed disease progression, without BICR-confirmed disease progression. | |
AE = adverse event; BICR = blinded independent central review; CI = confidence interval; G-CSF = granulocyte colony stimulating factor; IQR = interquartile range; m-RECIST = modified Response Evaluation Criteria in Solid Tumors criteria for pleural mesothelioma; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: Clinical Study Report10 and sponsor’s response to additional information request.31
Subsequent Treatments
Subsequent anti-cancer therapies administered after discontinuation of study drug are summarized in Table 12.
Table 12: Subsequent Anti-Cancer Treatment, ITT population, CheckMate 743
Subsequent treatment | Nivolumab plus ipilimumab N = 303 | Chemotherapy N = 302 |
|---|---|---|
Any subsequent systemic therapy, n (%) | 134 (44.2) | 123 (40.7) |
Chemotherapy, n (%) | 131 (43.2) | 95 (31.5) |
Immunotherapy, n (%) | 10 (3.3) | 61 (20.2) |
Experimental treatment, n (%) | 2 (0.7) | 12 (4.0) |
Select subsequent treatments | ||
Chemotherapy, n (%) Carboplatin Cisplatin Gemcitabine Pemetrexed Vinorelbine | . 89 (29.4) 40 (13.2) 25 (8.3) 121 (39.9) 15 (5.0) | . 39 (12.9) 8 (2.6) 45 (14.9) 48 (15.9) 25 (8.3) |
Immunotherapy, n (%) Anti–PD-1 Nivolumab Pembrolizumab Anti–PD-L1 Atezolizumab Avelumab Anti–CTLA-4 Ipilimumab | . . 7 (2.3) 2 (0.7) . 0 0 . 2 (0.7) | . . 41 (13.6) 17 (5.6) . 1 (0.3) 1 (0.3) . 3 (1.0) |
CTLA-4 = cytotoxic T-lymphocyte–associated antigen 4; PD-1 = programmed cell-death protein 1; PD-L1 = programmed cell-death ligand 1
Source: Clinical Study Report.10
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported. See Appendix 3 for detailed efficacy data.
The median overall follow-up times (i.e., between randomization and date last known to be alive) in CheckMate 743 were 17.35 months for the nivolumab plus ipilimumab group and 13.27 months in the chemotherapy group.10
Overall Survival (Primary End Point)
At the OS data cut-off date of March 25, 2020, the median follow-up survival time was 29.7 months (minimum of 22.1 months for time from randomization to clinical cut-off date) and there was a total of 419 deaths; 200 patients (66.0%) in the nivolumab plus ipilimumab group and 219 (72.5%) randomized to the chemotherapy group had died. The median OS difference between patients randomized to nivolumab plus ipilimumab and chemotherapy was 3.98 months, with a stratified HR for death of 0.74 (95% CI, 0.61 to 0.89; P = 0.0020) in favour of nivolumab plus ipilimumab.10 The Kaplan–Meier curve for OS is shown in Figure 3. The percentage of patients surviving to 6, 12, and 24 months was higher in the nivolumab plus ipilimumab group than in the chemotherapy group.
Table 13: Summary of Primary and Secondary End Points, CheckMate 743
Summary of end points | CheckMate 743 | |
|---|---|---|
Nivolumab plus ipilimumab | Chemotherapya | |
Efficacy outcomes – ITT population | N = 303 | N = 302 |
Primary outcome – OSb | ||
Median, months (95% CI) | 18.07 (16.82 to 21.45) | 14.09 (12.45 to 16.23) |
Events, n (%) | 200 (66.0) | 219 (72.5) |
Stratified HR (95% CI)c | 0.74 (0.61 to 0.89) | |
P value | 0.0020 | |
Secondary outcome – PFSd | ||
Median, months (95% CI) | 6.77 (5.59 to 7.36) | 7.20 (6.93 to 8.05) |
Events, n (%) | 218 (71.9) | 209 (69.2) |
Stratified HR (95% CI)c | 1.00 (0.82 to 1.21) | |
PFS rate | ||
6 months, % (95% CI) | 52.1 (46.0 to 57.8) | 61.9 (55.6 to 67.7) |
12 months, % (95% CI) | 30.2 (24.6 to 35.9) | 23.8 (18.4 to 29.7) |
24 months, % (95% CI) | 16.3 (11.7 to 21.5) | 7.2 (4.0 to 11.7) |
Secondary outcome – ORRe | ||
Responders, n | 120 | 129 |
Responders, % (95% CI) | 39.6 (34.1 to 45.4) | 42.7 (37.1 to 48.5) |
Time to response, months | 2.69 | 2.53 |
Duration of response, months, (95% CI) | 11.01 (8.11 to 16.49) | 6.67 (5.32 to 7.10) |
Secondary outcome – DCRf | ||
Responders, n | 232 | 257 |
Responders, % (95% CI) | 76.6 (71.4 to 81.2) | 85.1 (80.6 to 88.9) |
CI = confidence interval; DCR = disease control rate; HR = hazard ratio; ITT = intention-to-treat; m-RECIST = modified Response Evaluation Criteria in Solid Tumors; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
aStandard of care chemotherapy regimen consisted of pemetrexed in combination with cisplatin or carboplatin. Cisplatin was preferred for the combination, but carboplatin could have been used at the investigator’s discretion. At cycle 1, cisplatin was initiated in 104 patients and carboplatin was initiated in 180 patients. Switching between cisplatin and carboplatin was permitted; during the trial 29 patients switched from cisplatin to carboplatin; in total, 209 patients were exposed to carboplatin.
bOverall survival results represent data from the interim analysis. Based on 419 deaths of 473 anticipated for final analysis, the multiplicity-adjusted 2-sided significance level was 0.0345.
cThe HR and corresponding 2-sided CI were estimated using a stratified Cox proportional hazards model. An HR of less than 1 favours nivolumab plus ipilimumab; stratification factors included tumour histology and gender.
dTwo definitions were used in the analysis of PFS. Results reflect analysis using the primary definition, which accounted for subsequent anti-cancer therapy by censoring patients who received subsequent anti-cancer treatment at the date of last evaluable tumour assessment conducted on or before starting subsequent therapy. Results of PFS analysis according to the secondary definition of PFS, which did not censor patients who initiated subsequent anti-cancer treatment (ITT population), were similar to the analysis based on the primary definition. PFS events occurred in 246 patients (81.2%) in the nivolumab plus ipilimumab group and 251 patients (83.1%) in the chemotherapy group. The estimated median PFS according to a blinded independent central review was 6.93 months (95% CI, 5.59 to 8.21) in the nivolumab plus ipilimumab group and 7.16 months (95% CI, 6.93 to 7.69) in the chemotherapy group, with a corresponding stratified HR of 0.93 (95% CI, 0.78 to 1.12).
eDefined as number of patients who achieved complete response or partial response as best overall response, according to the adapted m-RECIST and/or RECIST 1.1 response criteria.
fDefined as the number of patients who achieved complete response, partial response, or stable disease as best overall response, according to the adapted m-RECIST and/or RECIST 1.1 response criteria.
Source: Clinical Study Report.10
Figure 3: Kaplan–Meier Analysis for Overall Survival, ITT population, CheckMate 743
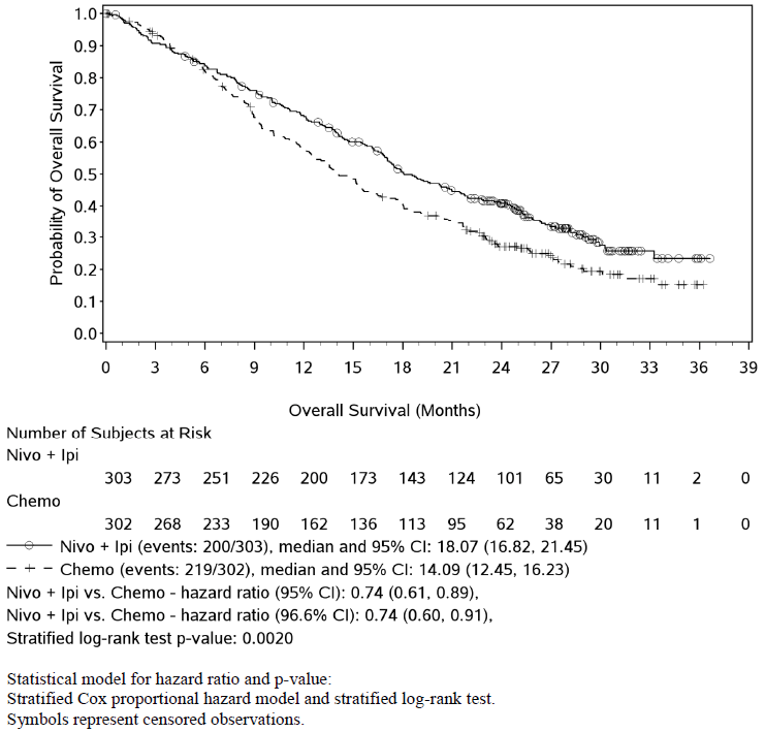
Chemo = chemotherapy; CI = confidence interval; Ipi = ipilimumab; ITT = intention-to-treat; Nivo = nivolumab.
Source: Clinical Study Report.10
Sensitivity and Subgroup Analyses
Results of pre-specified sensitivity analyses for OS were generally consistent with the primary analysis (Table 28, Appendix 3).
Pre-specified subgroup analyses of the primary end point generally showed a similar treatment effect favouring nivolumab plus ipilimumab regardless of the subgroup analyzed (Figure 4). However, the sample sizes were small in certain subgroups, such as disease stage at study entry and PD-L1 negative status, with CIs crossing 1.0. Also, the CIs for the unstratified HRs of larger subgroups of patients with an ECOG performance status of 0 (n = 242) or epithelioid tumours (n = 456) also included unity (1.0), indicating uncertainty in the true benefit of nivolumab plus ipilimumab over chemotherapy in these subgroups.10
Of the identified subgroups of interest in the review protocol (i.e., ECOG performance status, histological subtype, disease stage, and PD-L1 expression status), analyses showed that differences in treatment outcomes were notable for performance status and histological subtype. There was greater uncertainty in treatment effect for patients with a performance status of 0 (HR = 0.87; 95% CI, 0.64 to 1.19) compared to a status of 1 or greater (HR = 0.66; 95% CI, 0.52 to 0.85). Similarly, results suggest that the benefit of nivolumab plus ipilimumab may not be as pronounced in epithelioid tumours (HR = 0.86; 95% CI, 0.69 to 1.08) compared to non-epithelioid tumours (HR = 0.46; 95% CI, 0.31 to 0.68). Subgroup analysis was also pre-specified for PD-L1 status, with an expression of 1% or greater categorized as PD-L1 positive. The benefit of nivolumab plus ipilimumab on OS was consistent in patients with PD-L1 positive tumours (HR = 0.69; 95% CI, 0.55 to 0.87), whereas the benefit in patients with PD-L1 negative tumours was less pronounced (HR = 0.94; 95% CI, 0.62 to 1.40).10
Figure 4: Subgroup Analysis for Overall Survival, ITT Population, CheckMate 743
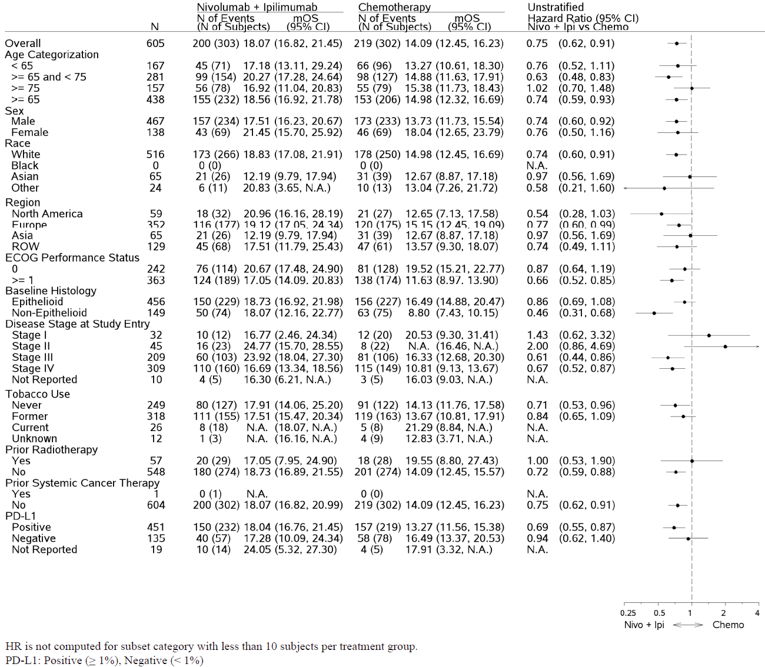
Chemo = chemotherapy; ECOG = Eastern Cooperative Oncology Group; Ipi = ipilimumab; ITT = intention-to-treat; mOS = modified overall survival; N.A. = not available; Nivo = nivolumab; PD-L1 = programmed cell-death ligand 1; vs. = versus .
Source: Clinical Study Report.10
Secondary Outcomes
Progression-Free Survival
At the time of database lock, according to the primary definition of PFS and as measured by BICR, a total of 427 patients had experienced disease progression or death: 218 patients (71.9%) in the nivolumab plus ipilimumab group and 209 patients (69.2%) in the chemotherapy group had experienced a PFS event. Disease progression was the main contributor to PFS events, occurring in 63.4% (n = 192) of patients in the nivolumab plus ipilimumab group and 59.3% (n = 179) in the chemotherapy group. Death was the earliest contributing event in 8.6% (n = 26) and 9.9% (n = 30) in the nivolumab plus ipilimumab and chemotherapy groups, respectively.10
Progression-free survival was also longer in the chemotherapy group at 6 months, although the curves crossed at approximately 8 months and subsequently showed longer PFS in the nivolumab plus ipilimumab group. The Kaplan–Meier curve for PFS is shown in Figure 5.10
Figure 5: Kaplan–Meier Analysis for Progression-Free Survival – Primary Definition, ITT Population, CheckMate 743
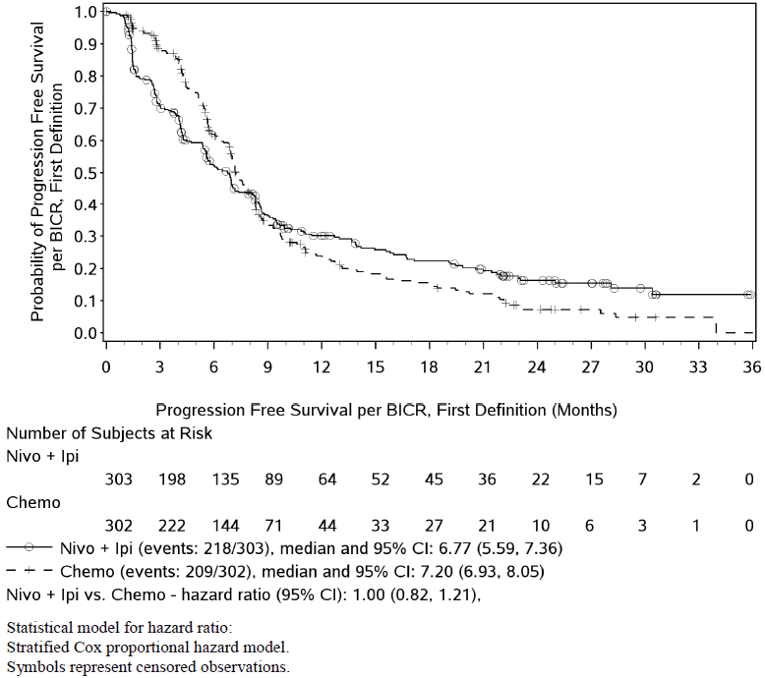
BICR = blinded independent central review; Chemo = chemotherapy; CI = confidence interval; Ipi = ipilimumab; ITT = intention-to-treat; Nivo = nivolumab; vs. = versus .
Source: Clinical Study Report10
Results of PFS analysis, according to the secondary definition of PFS and as measured by BICR, were similar to the analysis based on the primary definition (Table 30, Appendix 3).
Objective Response Rate
A best overall response of complete or partial response was achieved by 120 patients in the nivolumab plus ipilimumab group and 129 in the chemotherapy group. The ORR according to BICR was numerically lower in the nivolumab plus ipilimumab group. Most patients achieved partial response as the best overall response. A complete response was achieved by 5 patients (1.7%) in the nivolumab plus ipilimumab group compared to none in the chemotherapy group. As part of ORR analysis, time to response and duration of response were also evaluated; both were numerically superior with nivolumab plus ipilimumab than with chemotherapy.10
Disease Control Rate
A best overall response of complete or partial response or stable disease (or non–complete response/non–progressive disease) was achieved by 232 patients in the nivolumab plus ipilimumab group and 257 patients in the chemotherapy group. The disease control rate according to BICR was numerically lower in the nivolumab plus ipilimumab group. The best overall response achieved by the greatest number of patients in both groups was partial response (n = 115; 38.0% nivolumab plus ipilimumab versus n = 129; 42.7% chemotherapy), followed by stable disease (n = 112; 37.0% versus n = 125; 41.5%).10
Progressive disease was the best overall response in more patients in the nivolumab plus ipilimumab group compared to patients in the chemotherapy group (n = 55; 18.2% versus n = 14; 4.6%), while a greater proportion of patients in the chemotherapy group achieved partial response or stable disease. A summary of confirmed best overall response can be found in Appendix 3, Table 29.10
EuroQol 5-Dimensions 3-Levels Questionnaire
More than 74% of patients randomized to nivolumab plus ipilimumab and at least 82% in patients randomized to chemotherapy completed the EQ-5D-3L questionnaire during treatment. At least 10 patients were eligible to respond up to week 96 in the nivolumab plus ipilimumab group and week 42 in the chemotherapy group.10
Mean baseline scores for the utility index were similar between treatment groups (0.6959 for nivolumab plus ipilimumab, 0.7119 for chemotherapy). In the nivolumab plus ipilimumab group, utility scores improved gradually, with a numerical improvement from baseline seen at week 72 and reaching a peak score (0.8529) at week 84. In the chemotherapy group, scores during treatment appeared to improve more slowly and reached a peak score (0.7910) at week 24 then worsened to below baseline at week 30.10
Mean baseline VAS scores were also numerically similar between treatment groups (69.9 for nivolumab plus ipilimumab, 69.6 for chemotherapy). In the nivolumab plus ipilimumab group, scores improved numerically during treatment and reached a peak score (82.7) at week 72. In the chemotherapy group, scores also improved from baseline during treatment and reached a peak score (75.4) at week 30.10
Lung Cancer Symptom Scale to Mesothelioma
More than 76% of patients randomized to the nivolumab plus ipilimumab group and at least 82% of patients randomized to chemotherapy completed the LCSS-Meso questionnaire during treatment. A minimum of 10 patients were eligible to respond up to week 96 in the nivolumab plus ipilimumab group and week 30 in the chemotherapy group.10
Mean baseline scores were numerically similar between treatment groups (31.42 for nivolumab plus ipilimumab and 31.25 for chemotherapy). In the nivolumab plus ipilimumab group, the mean LCSS-Meso scores appeared stable during treatment, with a numerical trend for improvement (reduction in scores) over time. In the chemotherapy group, the mean LCSS-Meso scores appeared to fluctuate over the course of treatment.10
At week 12, the LCSS-Meso disease-related symptom deterioration rate was numerically higher for the nivolumab plus ipilimumab group (48.0%; 95% CI, 41.7 to 54.4) compared to the chemotherapy group (40.6%; 95% CI, 34.2% to 47.3%) but no formal comparison was made for these outcomes.10
Harms
Only those harms identified in the review protocol are reported. Aggregate AE outcomes are summarized in Table 14.
Table 14: Summary of Adverse Events, Safety Population, CheckMate 743
Events, n (%) | Nivolumab plus ipilimumab N = 300 | Chemotherapy N = 284 |
|---|---|---|
All-cause AEs | 299 (99.7) | 277 (97.5) |
All-cause grade 3 to 4 AEs | 159 (53.0) | 121 (42.6) |
All-cause SAEs | 164 (54.7) | 72 (25.4) |
WDAEs | 88 (29.3) | 58 (20.4) |
Deaths | 198 (66.0) | 212 (74.6) |
Deaths due to disease progression | 183 (61.0) | 199 (70.1) |
Deaths due to AEs | 3 (1.0) | 1 (0.4) |
AE = adverse event; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Source: Clinical Study Report.10
As duration of treatment was different between the groups, the study reported incidence rates adjusted for the different lengths of exposure. The exposure-adjusted incidences per 100 person-years are presented in Table 15.
Table 15: Summary of Exposure-Adjusted Incidence of Adverse Events, Safety Population, CheckMate 743
Events per 100 person-years | Nivolumab plus ipilimumab N = 300 | Chemotherapy N = 284 |
|---|---|---|
All-cause AEs | 1,485.0 | 2,306.4 |
All-cause grade 3 to 4 AEs | 164.3 | 332.2 |
AEs leading to treatment discontinuation | 47.7% | 76.2% |
AE = adverse event.
Source: Clinical Study Report10 and sponsor’s response to additional information request.31
Adverse Events
Table 14 and Table 16 provide a summary of all-cause AEs that were reported in at least 10% of patients within either treatment group in the CheckMate 743 trial. Adverse events of any grade occurred at a similar incidence in both treatment groups. More patients treated with nivolumab plus ipilimumab experienced grade 3 to 4 AEs of any cause.10
Table 16: Adverse Events of Any Cause Reported in ≥ 10% of Patients, Safety Population, CheckMate 743
Events, n (%) | Nivolumab plus ipilimumab N = 300 | Chemotherapy N = 284 | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 3 to 4 | Grade 5 | Any grade | Grade 3 to 4 | Grade 5 | |
Diarrhea | 94 (31.3) | 12 (4.0) | 0 | 32 (11.3) | 2 (0.7) | 0 |
Fatigue | 86 (28.7) | 9 (3.0) | 0 | 77 (27.1) | 5 (1.8) | 0 |
Dyspnea | 78 (26.0) | 7 (2.3) | 0 | 41 (14.4) | 9 (3.2) | 0 |
Nausea | 73 (24.3) | 2 (0.7) | 0 | 123 (43.3) | 7 (2.5) | 0 |
Decreased appetite | 71 (23.7) | 3 (1.0) | 0 | 72 (25.4) | 4 (1.4) | 0 |
Cough | 65 (21.7) | 2 (0.7) | 0 | 22 (7.7) | 0 | 0 |
Pruritus | 62 (20.7) | 3 (1.0) | 0 | 4 (1.4) | 0 | 0 |
Rash | 60 (20.0) | 3 (1.0) | 0 | 21 (7.4) | 0 | 0 |
Constipation | 56 (18.7) | 1 (0.3) | 0 | 84 (29.6) | 2 (0.7) | 0 |
Pyrexia | 55 (18.3) | 4 (1.3) | 0 | 13 (4.6) | 2 (0.7) | 0 |
Asthenia | 49 (16.3) | 4 (1.3) | 0 | 57 (20.1) | 12 (4.2) | 0 |
Peripheral edema | 45 (15.0) | 0 | 0 | 18 (6.3) | 0 | 0 |
Vomiting | 43 (14.3) | 0 | 0 | 52 (18.3) | 6 (2.1) | 0 |
Anemia | 43 (14.3) | 8 (2.7) | 0 | 119 (41.9) | 39 (13.7) | 0 |
Non-cardiac chest pain | 40 (13.3) | 5 (1.7) | 0 | 14 (4.9) | 1 (0.4) | 0 |
Arthralgia | 40 (13.3) | 3 (1.0) | 0 | 3 (1.1) | 0 | 0 |
Hypothyroidism | 38 (12.7) | 0 | 0 | 3 (1.1) | 0 | 0 |
Malignant neoplasm progression | 32 (10.7) | 9 (3.0) | 19 (6.3) | 14 (4.9) | 5 (1.8) | 8 (2.8) |
Abdominal pain | 31 (10.3) | 2 (0.7) | 0 | 12 (4.2) | 2 (0.7) | 0 |
Neutropenia | 5 (1.7) | 3 (1.0) | 0 | 79 (27.8) | 45 (15.8) | 0 |
Thrombocytopenia | 3 (1.0) | 2 (0.7) | 0 | 31 (10.9) | 11 (3.9) | 0 |
Note: Table sorted by decreasing frequency of events (any grade) in the nivolumab plus ipilimumab treatment group.
Source: Adapted from Clinical Study Report.10
Serious Adverse Events
Serious adverse events were reported more frequently in patients treated with nivolumab plus ipilimumab. Details of the most commonly reported (≥ 2%) all-cause SAEs are outlined in Table 17.
Table 17: Serious Adverse Events Reported in ≥ 2% of Patients, Safety Population, CheckMate 743
Events, n (%) | Nivolumab plus ipilimumab N = 300 | Chemotherapy N = 284 | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 3 to 4 | Grade 5 | Any grade | Grade 3 to 4 | Grade 5 | |
Malignant neoplasm progression | 32 (10.7) | 9 (3.0) | 19 (6.3) | 13 (4.6) | 5 (1.8) | 8 (2.8) |
Pleural effusion | 9 (3.0) | 2 (0.7) | 1 (0.3) | 2 (0.7) | 2 (0.7) | 0 |
Colitis | 9 (3.0) | 7 (2.3) | 0 | 0 | 0 | 0 |
Pneumonitis | 7 (2.3) | 2 (0.7) | 0 | 0 | 0 | 0 |
Infusion-related reaction | 7 (2.3) | 4 (1.3) | 0 | 0 | 0 | 0 |
Acute kidney injury | 7 (2.3) | 5 (1.7) | 0 | 1 (0.4) | 0 | 0 |
Diarrhea | 6 (2.0) | 4 (1.3) | 0 | 1 (0.4) | 0 | 0 |
Dyspnea | 5 (1.7) | 3 (1.0) | 0 | 6 (2.1) | 5 (1.8) | 0 |
Anemia | 5 (1.7) | 3 (1.0) | 0 | 8 (2.8) | 5 (1.8) | 0 |
Pyrexia | 13 (4.3) | 3 (1.0) | 0 | 2 (0.7) | 2 (0.7) | 0 |
Pneumonia | 11 (3.7) | 8 (2.7) | 0 | 5 (1.8) | 5 (1.8) | 0 |
Note: Table sorted by decreasing frequency of events (any grade) in the nivolumab plus ipilimumab treatment group.
Source: Adapted from Clinical Study Report.10
Withdrawals Due to Adverse Events
More patients in the nivolumab plus ipilimumab group discontinued study treatment due to an AE. All-cause AEs leading to discontinuation of study therapy represented 29.3% (n = 88) of the nivolumab plus ipilimumab group, compared to 20.4% (n = 58) of the chemotherapy group. In patients treated with nivolumab plus ipilimumab, the most common AEs leading to treatment discontinuation were colitis (2.3%), diarrhea (2.3%), infusion-related reactions (1.7%), and pneumonitis (1.7%). In patients treated with chemotherapy, the most common AEs leading to treatment discontinuation were anemia (3.9%), asthenia (2.1%), nausea (1.8%), fatigue (1.8%), neutropenia (1.8%), and thrombocytopenia (1.8%).10
Deaths
At the database lock date of April 3, 2020, a total of 410 patients had died, including 198 patients (66.0%) treated with nivolumab plus ipilimumab and 212 patients (74.6%) treated with chemotherapy. Disease progression accounted for the majority of deaths. The primary reason for death was disease progression, which accounted for 183 deaths (61.0%) and 199 deaths (70.1%) in the nivolumab plus ipilimumab and chemotherapy groups, respectively. Study-drug toxicity led to 3 deaths (1.0%) in the immunotherapy group and 1 death (0.4%) in the chemotherapy group. In patients treated with nivolumab plus ipilimumab, the causes of treatment-related deaths were pneumonitis, acute heart failure, and neurologic complications (encephalitis), each of which occurred in 1 patient. The cause of treatment-related death in the 1 patient treated with chemotherapy was myelosuppression and salmonella sepsis.10
Adverse Events of Special Interest
Immune-Mediated Adverse Events
Predefined IMAEs that occurred within 100 days of the last study treatment dose were reported, and analysis was limited to patients who received an immunomodulator for treatment (except for endocrine events, which were included regardless of treatment).10 In total, 128 patients in the nivolumab plus ipilimumab group and 6 patients in the chemotherapy group experienced at least 1 predefined IMAE.12
In patients treated with nivolumab plus ipilimumab, the most frequently reported IMAEs of any grade were rash (13.0%), hypothyroidism or thyroiditis (11.7%), diarrhea or colitis (8.7%), and pneumonitis (6.7%). In patients treated with chemotherapy, 1.1% developed an immune-mediated rash. Most IMAEs were grade 1 or 2 in severity and resolved with administration of corticosteroids. The exception was hepatitis and nephritis or renal dysfunction, in which a greater number of grades 3 and 4 reactions were noted, but they were manageable using established algorithms. The median time to resolution ranged from 0.14 to 17.14 weeks, although some endocrine IMAEs were considered unresolved due to an ongoing requirement for hormone-replacement therapy.10 Table 18 summarizes the details of onset, management, and resolution of IMAEs.10
Of the patients who experienced at least 1 predefined IMAE, 107 (83.6%) in the nivolumab plus ipilimumab group and 4 patients (66.7%) in the chemotherapy group received an immunomodulator for treatment.12 The clinical experts consulted on this review expressed interest in identifying the administration of high-dose corticosteroids for the treatment of IMAEs. In the CheckMate 743 trial, a high-dose corticosteroid was defined as a dose of a least 40 mg of prednisone equivalent. Based on this threshold, |||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.12
Table 18: Onset, Management, Resolution of All-cause IMAEs, Nivolumab Plus Ipilimumab Treated Population, CheckMate 743
IMAE Category | % Subj. with Any Grade/Grade 3-4 IMAEs | Median Time to IMAE Onset (range), wks | % Subj. with IMAE leading to DC / Dose Delay | % Subj. with IMAEs Receiving IMM / High-dose Corticosteroidsa | Median Duration IMM (range), wks | % Subj. with Resolution of IMAEd,e | Medianb Time to Resolution (range), wksc,d,e | % Subj. with Recurrence after Reinitiation |
|---|---|---|---|---|---|---|---|---|
Pneumonitis | 6.7/2.0 | 10.14 (1.9-90.3) | 3.0/3.3 | 100/80.0 | 12.86 (1.1 - 82.4) | 65.0 | 17.14 (1.3 - 113.1 + ) | 11.1 (1/9) |
Diarrhea / Colitis | 8.7/4.0 | 26.71 (1.3-99.6) | 3.7/4.3 | 100/84.6 | 6.21 (0.4 - 50.7) | 92.3 | 3.71 (0.4 - 63.3 + ) | 6.7 (1/15) |
Hepatitis | 6.0/4.7 | 8.79 (2.0 - 72.0) | 4.3/2.7 | 100/88.9 | 10.50 (0.1 - 61.0) | 88.9 | 4.71 (1.0 - 35.1) | 0 (0/8) |
Nephritis / Renal Dysfunction | 2.7/1.7 | 18.50 (3.3-46.1) | 1.0/2.3 | 100/62.5 | 9.07 (2.3 - 40.4) | 50.0 | N.A. (0.9 - 126.4 + ) | 0 (0/8) |
Rash | 13.0/2.7 | 11.00 (0.4 - 82.3) | 0/2.7 | 100/23.1 | 10.71 (0.4 - 122.0) | 61.5 | 17.00 (1.3 - 131.9 + ) | 2.9 (1/35) |
Hypersensitivity | 1.7/0.3 | 2.14 (2.1 - 8.0) | 0.3/0 | 100/60.0 | 0.14 (0.1 - 4.7) | 100 | 0.14 (0.1 - 8.1) | 0 (0/4) |
Adrenal Insufficiency | 2.3/0.7 | 26.00 (17.6 - 53.7) | 0.7/1.0 | 85.7/28.6 | 47.14 (0.9 - 70.7) | 42.9 | N.A. (1.1 - 108.7 + ) | 0 (0/ 6) |
Hypophysitis | 4.0/1.0 | 22.79 (2.1 - 47.6) | 0/2.7 | 100/33.3 | 57.93 | 25.0 | N.A. (0.7 - 144.1 + ) | 0 (0/12) |
Hypothyroidism/Thyroiditis | 11.7/0 | 14.00 (4.3 - 90.3) | 0/1.3 | 5.7/0 | 37.29 (19.1 - 55.4) | 25.7 | N.A. (2.1 - 129.9 + ) | 0 (0/34) |
Hyperthyroidism | 3.7/0 | 6.14 (2.0 - 24.0) | 0/0.7 | 9.1/0 | 6.00 (6.0 - 6.0) | 90.9 | 5.43 (0.3 - 130.4 + ) | 0 (0/9) |
Diabetes Mellitus | 0.3/0.3 | 56.86 (56.9 - 56.9) | 0/0 | 0/0 | N.A. | 100 | 0.71 (0.7 - 0.7) | 0 (0/1) |
DC = discontinuation; IMAE = immune-mediate adverse event; IMM = immune-modulating medication; N.A. = not available.
aDenominator is based on the number of subjects who experienced the event.
bFrom Kaplan–Meier estimation.
cSymbol + indicates a censored value.
dDenominator is based on the number of subjects who were re-challenged.
eEvents without a stop date or with a stop date equal to the death as well as grade 5 events are considered unresolved.
Source: Clinical Study Report.10
Infusion-Related Reactions
Infusion-related reactions were reported in 8.3% of patients treated with nivolumab plus ipilimumab compared to 0.7% of patients treated with chemotherapy. Grade 3 or 4 reactions were reported in 1.3% of patients treated with nivolumab plus ipilimumab. Similarly, a low proportion of patients (2.3%) in the immunotherapy group reported a serious infusion-related reaction. Study treatment was discontinued due an infusion reaction in 1.7% of patients treated with nivolumab plus ipilimumab. None of the patients treated with chemotherapy reported a grade 3 to 4 or serious infusion-related reaction, or discontinued treatment due to an infusion-related reaction.10
More broadly speaking, all-cause hypersensitivity/infusion-related reactions were reported in 12.3% of patients treated with nivolumab plus ipilimumab compared to 2.5% of patients treated with chemotherapy. Grade 3 or 4 hypersensitivity/infusion-related reactions were reported in 1.3% and 0% of patients treated with nivolumab plus ipilimumab and chemotherapy, respectively. According to the Clinical Study Report, the frequency of drug-related hypersensitivity or infusion reactions in the nivolumab plus ipilimumab group (12.0%) was relatively high compared to previous experiences with the treatment of non–small cell lung cancer, melanoma, or renal cell carcinoma. However, most of the events were grade 1 or 2 in severity, and resolved within a day.
Chemotherapy-Related AEs
Chemotherapy-related AEs identified as important to patients and relevant to this review have been included in the summary of AEs discussed in the previous section.
Critical Appraisal
Internal Validity
Trial Design and Statistical Analysis
The open-label study design was susceptible to reporting, performance, detection, and selection biases as patients and investigators were not blinded to study treatment allocation. Lack of blinding can influence trial results in favour of the investigational therapy (i.e., nivolumab plus ipilimumab). However, OS was the primary end point of the trial and is an objective measure that is unlikely to be biased by the open-label study design. The secondary efficacy end points (PFS, ORR, and DCR) were measured by a BICR committee to mitigate the potential for bias. The open-label design remains a concern for subjective outcomes assessed in the trial, including HRQoL and safety, as patient or investigator knowledge of treatment assignment could have influenced the assessment and reporting of these outcomes.
The study protocol of CheckMate 743 was amended twice. Some amendments affected statistical analyses, interim analysis, and end points of the trial, which raise concerns about the integrity of the results. For example, the original protocol had designated the primary outcome as a co-primary end point of OS and PFS. With Revised Protocol 02, PFS was changed from the co-primary to a secondary end point, and hierarchical testing of secondary end points was removed. Overall survival was then deemed the only primary end point for the study, and the alpha level as well as the required number of events for OS analyses (interim and final) were adjusted. By the time Revised Protocol 02 was implemented, all patients had been randomized into the study. However, the changes made to the end points and statistical assumptions were informed by external trial data. According to the sponsors, the considerations included the challenges and risk of imprecise measurements for tumours lacking demarcated margins (e.g., in mesothelioma), and data from studies showing that PFS with immunotherapy may not be a reliable end point to evaluate clinical benefits, when compared with chemotherapy. The sponsors stated that the decision was not influenced by knowledge of the trial data; efficacy results had not been reviewed by the sponsors at the time of this amendment.11 The changes made to the protocol were therefore unlikely to be influenced by the trial sponsor staff’s access to preliminary unaggregated data.
The study provided 2 definitions of PFS based on different censoring rules. In the analysis of PFS using the primary definition, patients who received subsequent anti-cancer therapy were censored in the analysis. This may lead to biased results through informative censoring. The study also conducted an analysis of PFS using a secondary definition that did not consider the receipt of subsequent therapy (i.e., ITT population). The results of the analysis of PFS based on this secondary definition (HR = 0.93; 95% CI, 0.78 to 1.12) were similar and supported the results of the primary definition (HR = 1.00; 95% CI, 0.82 to 1.21).
Final analysis of OS was scheduled to be conducted after 473 deaths, which has yet to occur (419 deaths occurred by database lock). Current data reflects the pre-planned interim analysis, but as the end point was met, the trial was stopped for superiority and results were considered final. According to the sponsors, further updates of data may be provided for characterization of longer-term effects; however, statistical testing is no longer required.10 Although the benefit over time will need to be confirmed with a longer follow-up, the current OS data (89% of events targeted for final OS analysis, median survival follow-up of 29.8 months) are likely reflective of the benefit of immunotherapy in this patient population and considered clinically meaningful. There is a risk of overestimating the true treatment effect when trials are stopped early based on an interim analysis. However, the likelihood decreases if analyses are performed close to the planned completion of the trial, and the risk of an overestimate of the treatment effect in the CheckMate 743 trial is likely small. Secondary outcomes, including PFS, ORR, and DCR, are also clinically relevant, although they were not part of the statistical hierarchy and therefore no adjustments were made for multiple comparisons of these outcomes. These results may be considered supplemental to the primary end point but should be interpreted with caution.
To account for the single interim analysis, the nominal significance level for the primary end point was adjusted for overall type I error. Many pre-specified subgroup analyses were performed, but no statistical considerations were employed to account for multiplicity. Although there were differences in OS within some pre-specified subgroups, such as tumour histology, these results should be interpreted with caution. Secondary objectives were not controlled for type I error, nor was formal testing performed. Because the trial was not powered to test specific hypotheses in subgroups or secondary end points, the results of these analyses should be considered exploratory in nature.
The analysis of OS, PFS, and corresponding treatment-effect estimates were based on a stratified Cox PH model in which the HR between treatments is assumed to be unchanged over the duration of the comparison. At the interim analysis, the results for OS demonstrated the statistically significant superiority of nivolumab plus ipilimumab over pemetrexed plus cisplatin or carboplatin. The Kaplan–Meier survival curves initially lay close to each other, then diverged at approximately 6 months and showed a sustained effect. A sensitivity analysis tested for the PH assumption for OS confirmed the assumption was met and supported the conclusion of improved efficacy of nivolumab plus ipilimumab over chemotherapy. However, a graphical representation of PFS clearly showed crossing of the Kaplan–Meier curves, suggesting a violation of the PH assumption. The HRs for PFS inverted at approximately 8 months, favouring first chemotherapy then immunotherapy, indicating that the magnitude of effect changes over time, with different effects seen from each treatment. The HR from the Cox PH model therefore does not provide a stable, long-term estimate, and is not an appropriate measure of the treatment effect for PFS.
Longer-term survival is influenced by all treatment received. Overall, a similar proportion of patients in both treatment groups received subsequent systemic therapy after discontinuing study treatment (44.2% in the nivolumab plus ipilimumab group versus 40.7% in the chemotherapy group). Chemotherapy was administered in both treatment groups (43.2% for nivolumab plus ipilimumab versus 31.5% chemotherapy). Immunotherapy was administered to more patients in the chemotherapy group (20.2%) compared to the nivolumab plus ipilimumab group (3.3%). Subsequent treatment would confound the assessment of OS if patients experienced additional clinical benefit. This may prolong survival beyond what would have occurred with front-line treatment alone and overestimate the survival benefit. In an unblinded trial setting, the choice of subsequent therapy may be influenced by the treatment received in the study. The impact of this bias in CheckMate 743 is unknown.
Study Treatment
The chemotherapy regimen was administered for a shorter fixed duration (up to 6 cycles) compared to the immunotherapy combination (a maximum of 24 months). The median duration of treatment was 5.55 months (interquartile range = 2.04 to 11.35) for the nivolumab plus ipilimumab group and 3.48 months (interquartile range = 2.66 to 3.70) for the chemotherapy group. Most patients randomized to chemotherapy (n = 176; 58.2%) completed the maximum number of cycles by the data cut-off date, whereas 3 patients (1%) received the maximum duration of nivolumab plus ipilimumab treatment. The potential impact on outcomes introduced by the differences in the length of treatment between the 2 groups should be considered, particularly when interpreting AE or HRQoL data that may be related to duration of exposure.
Patients were permitted to continue treatment with the immunotherapy combination beyond radiographic disease progression (as measured by m-RECIST and/or RECIST 1.1), if there was evidence of clinical benefit. During the study, 39% of patients (117 of 300) treated with nivolumab plus ipilimumab continued treatment beyond radiographic progression.11 In an open-label trial setting, investigator bias may have contributed to the decision to continue or discontinue treatment. The differential treatment between groups may contribute to differential assessment and potentially affect OS, although the magnitude of this impact is unknown. See the last bullet of the trial design and statistical analysis section regarding the impact that subsequent treatment may also have on OS.
Study End Points
An MID has not been established for the LCSS-Meso questionnaire in patients with MPM. The sponsor provided supporting literature that described measuring HRQoL and symptoms in patients with non–small cell lung cancer with this instrument.11,32 However, currently, there is no established MID to guide the analysis and interpretation of PRO data using the LCSS-Meso ASBI in patients with unresectable MPM. Consequently, it is unclear if the threshold used in the trial (i.e., an MID of 10 points) is appropriate and reflective of a clinically meaningful threshold for responder analysis for this scale in patients with MPM.
Patients identified HRQoL as an outcome of particular interest. Although pre-specified, CheckMate 743 measured PROs as part of exploratory end points, but as the PROs were not adjusted for multiplicity, they should only be considered descriptive. Completion rates, defined as the proportion of questionnaires actually received out of the number of questionnaires expected, of the EQ-5D-3L and LCSS-Meso during treatment were 75% or greater in both treatment groups. The study noted that a minimum of 10 patients were eligible to respond up to week 96 for both questionnaires in the nivolumab plus ipilimumab group, and week 42 for EQ-5D-3L and week 30 for LCSS-Meso questionnaires for patients in the chemotherapy group. The small number of patients left in the trial and included in the analyses of PROs at later assessment time points is likely not representative of all patients randomized in each treatment group, (i.e., in terms of their HRQoL). Finally, due to the open-label study design and exploratory nature of the end point, it is difficult to fully appreciate the adverse effect of treatment on HRQoL and results should be interpreted with caution.
External Validity
Checkmate 743 was an international, multi-centre design that spanned 21 countries. Although there were no Canadian sites in the study, the clinical experts consulted on this review stated that the population enrolled in the trial is consistent with the population expected to be treated for MPM in Canada. They noted that study eligibility criteria of this trial limited enrolment to patients with an ECOG performance status of 0 to 1, although in practice, some patients with a performance status of 2 may be considered for treatment.
Standard of care chemotherapy, specifically pemetrexed in combination with cisplatin or carboplatin administered in the CheckMate 743 trial, is an appropriate comparator and is used most often in Canadian practice for first-line systemic treatment of MPM.
Overall, CheckMate 743 measured clinically important outcomes that are relevant to patients with MPM.
In CheckMate 743, for the purpose of determining PFS, clinical deterioration in the absence of unequivocal evidence of disease progression, as per m-RECIST and/or RECIST 1.1 criteria, was not considered as progression. Although it is important to take into consideration clinical status, this can be affected by several factors, including adverse effects of treatment, in addition to disease progression. To ensure an objective measure is used to determine disease progression, this differentiation was considered appropriate for the purposes of this study by the clinical experts.
As mentioned, an MID has not been established for the LCSS-Meso questionnaire in patients with MPM, making it difficult to interpret the clinical relevance of changes from baseline on the scale. Similarly, for the EQ-5D-3L instrument, an MID has not been established, nor has it been assessed for validity and reliability specifically in patients with MPM. However, as it is a widely used, standardized, and generic measure of health status and an important part of economic analyses, the application of EQ-5D-3L is considered reasonable in this trial.
Indirect Evidence
A focused literature search for NMAs dealing with mesothelioma was run in MEDLINE All (1946–) on November 25, 2020. No limits were applied.
Objectives and Methods for the Summary of Indirect Evidence
The CheckMate 743 trial compared nivolumab plus ipilimumab to pemetrexed plus cisplatin or carboplatin for first-line treatment of patients with unresectable MPM. However, other first-line treatments for unresectable MPM patients are available. In the absence of direct evidence from a comparison of clinical efficacy and safety end points, indirect evidence may be used to provide comparative information. The objective of this section is to summarize and critically appraise available indirect evidence comparing nivolumab plus ipilimumab to relevant first-line treatments for MPM (as specified in the CADTH review protocol).
Description of Indirect Comparison
The sponsor-submitted ITC was summarized and appraised. A supplemental search of the medical literature for publicly available ITCs was conducted by CADTH staff; no ITCs were identified that evaluated the comparative efficacy and safety of nivolumab plus ipilimumab as first-line treatment of adults with MPM.
Table 19: Study Selection Criteria and Methods for the Indirect Treatment Comparison
Criteria | Sponsor’s indirect treatment comparison | |
|---|---|---|
Population | Patients with MPM, with no limitations placed based on sex, race, or ethnicity | |
Intervention | The following interventions were incorporated into the sponsors literature search; treatments were chosen based on those approved for treatment of MPM as well as those in development, each could be a monotherapy or use in combination:
|
|
Comparator | Any of the included interventions, placebo, best supportive care, active symptom control | |
Outcome | OS PFS DCR (complete response + partial response + stable disease) ORR (complete response + partial response) Safety (any grade and grade 3 or 4 AEs) | |
Study design | RCTs | |
Publication characteristics | Published in English Published from database inception to May 9, 2018 | |
Exclusion criteria | None | |
Databases searched | Embase via embase.com MEDLINE via embase.com MEDLINE in-process via PubMed CENTRAL via Cochrane Library CDSR via Cochrane Library ASCO ESMO AACR ISPOR WCLC ELCC IMIG | |
Selection process | (e.g., articles screened independently by 2 researchers) | |
Data extraction process | Data were extracted into a table with predefined criteria by 1 reviewer, followed by a quality check by a secondary reviewer. | |
Quality assessment | Critical appraisal of RCTs was conducted using the NICE checklist | |
AACR = American Association for Cancer Research; AE = adverse effect; ASCO = American Society of Clinical Oncology; DCR = disease control rate; ELCC = European Lung Cancer Congress; EMSO = European Society for Medical Oncology; IMIG = International Mesothelioma Interest Group; ISPOR = Professional Society for Health Economics and Outcomes Research; MPM = malignant pleural mesothelioma; NICE = National Institute for Health and Care Excellence; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized control trial; WCLC = World Conference on Lung Cancer.
Source: Sponsor’s network meta-analysis.33
Methods of the Indirect Treatment Comparison
Objectives
The aim of the submitted ITC was to compare the efficacy of first-line treatments for adult patients with clinically diagnosed MPM based on outcomes of OS, PFS, and ORR, via an NMA.
Study Selection Methods
A literature search was conducted based on the details in Table 19. Studies were screened by abstract and then full text, resulting in inclusion of 267 studies. Twenty-three of the studies were RCTs compared to 178 non-randomized studies (Figure 6). The sponsor considered only RCTs.
Figure 6: PRISMA Flow Diagram for Systematic Literature review for NMA
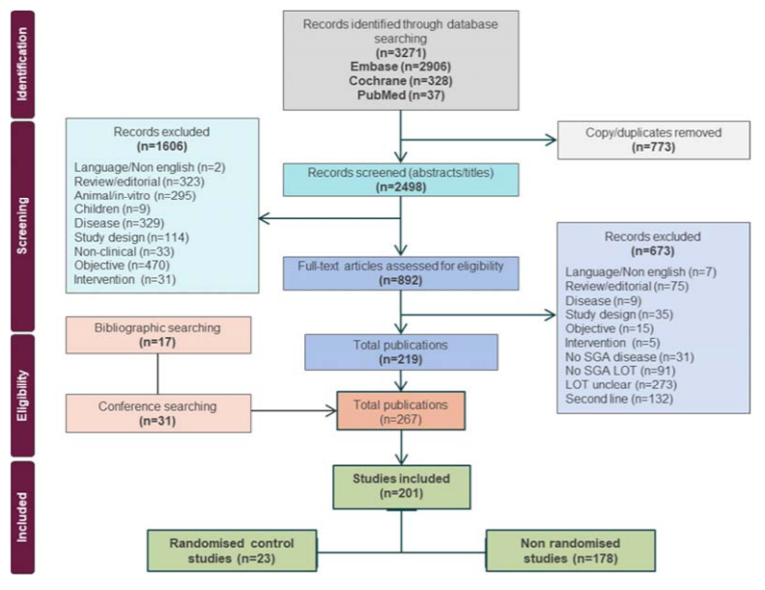
NMA = network meta-analysis; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Source: Sponsor’s network meta-analysis.33
Assessment of Feasibility for Indirect Treatment Comparison Network
The sponsor conducted a feasibility assessment of studies for inclusion in the NMA. The feasibility assessment aimed to narrow the list of 23 trials to studies that could be used to create connected networks. Thirteen of the 23 RCTs, including the CheckMate 743 trial,10 contributed evidence, with pemetrexed plus cisplatin or carboplatin as a reference comparator.
Selection of Most Appropriate Comparators for the NMA
Two retrospective observational studies were referenced to provide context for first-line treatment of adult patients with MPM and a list of appropriate comparators for the NMA. The 2 studies were conducted in a US oncology network community practice setting (n = 474 patients) and an observational study evaluating real-world treatment patterns among 5 European countries (n = 1,388 patients). After reviewing the results of the 2 studies, only 5 were considered for inclusion in the sponsor’s NMA: CheckMate 743 trial,10 Habib and Fahmy (2013),13 Zalcman et al. (2016)14 (MAPS), Vogelzang et al., (2003)15 (EMPHACIS), and van Meerbeeck et al. (2005)16 (EORTC 08983).
Indirect Treatment Comparison Analysis Methods
Outcomes of interest for all NMA analyses were OS, PFS and ORR, and were performed in the ITT population. Statistical analyses of the sponsor’s NMA were conducted using:
Aggregate data (PH NMA) for OS and PFS:
A PH NMA was conducted using the summary results reported in publications of the included trials, including syntheses of HRs for end points of OS, PFS, and ORR. A Bayesian NMA analysis was conducted using fixed-effect linear models with a normal likelihood distribution for time to event outcomes (e.g., log HR and SE), and a binomial likelihood with a log link for dichotomous outcomes (e.g., ORR). In addition to the fixed-effect model, a random-effect model for OS and PFS was analyzed. An assessment of violation of the PH assumption was conducted using appropriate methods by regenerating individual patient data from published Kaplan–Meier curves as per Guyot et al.34 All PH assumptions were tested through visual inspections non-proportionality of −log(−log(S(t))) versus log(t) curves derived from the empirical survival functions for each study contributing to the OS and PFS network. Statistical testing was also performed using Harrell and Grambsch and Therneau’s tests. As the goodness of fit was not considered to be substantially improved using the random-effect model, and based on residual deviance and deviance information criteria (DIC) statistics, the fixed-effect model was chosen for parsimony and interpretability. Analyses were performed in WinBUGS version 1.4.3 (MRC Biostatistics Unit, Cambridge, UK) using coding by Dias et al.35 Results of the NMA were based on 80,000 iterations on a minimum of 3 chains, with the first 20,000 iterations discarded as burn-in. Convergence was assessed by visual inspection of trace plots. The Monte Carlo error was used to assess the accuracy of posterior estimates for each parameter (a Monte Carlo error less than 1% of the posterior standard deviation or an error divided by posterior standard deviations should be less than 0.05). Point estimates (median of posterior) were reported for comparative treatment effects with associated 95% CrIs.
An NPH NMA using patient-level data from the CheckMate 743 trial and pseudo-patient-level data from comparator trials:
The NPH NMA was conducted using a shape-and-scale adjustment technique originally outlined in Ouwens et al.36; this approach can be applied easily to economic models and avoid the use of a new class of function. The fixed-effects model approach was chosen based on the limited amount of evidence as only 1 study was available per comparator.
The NPH NMA involved a simulated analysis of mean OS and PFS over a time horizon of 20 years based on parametric survival analysis. The NPH NMA also involved simulated landmark survival probabilities and an associated survival curve extrapolated over a 20-year time horizon. Five parametric models were considered for the NPH NMA for both OS and PFS: exponential, Weibull, Gompertz, log-normal and log-logistic. Pemetrexed plus cisplatin or carboplatin treatment based on the CheckMate 743 trial was used as the reference group. Convergence was assessed using the Gelman-Rubin diagnostic measure of convergence for a list of Markov chain Monte Carlo sequences. Based on the DIC goodness-of-fit statistics, the log-logistic model was chosen as the best-fitting model for extrapolation of OS and PFS data. Predicted mean (up to study follow-up and over a lifetime) OS and PFS were generated and compared with the study results, where available. Simulated results for OS and PFS over a 20-year time horizon were derived using the baseline survival function of pemetrexed plus cisplatin or carboplatin in the CheckMate 743 trial,10 and adjusted were for the effect of comparators on the shape and scale of the survival distribution. The parametric NMA was performed using the “survivalnma” package in R.
Results of the Indirect Treatment Comparison
Summary of Included Studies
Assessment of Heterogeneity in Trial Design and Study Characteristics
A visual comparison of study characteristics was conducted to determine the similarities and differences in the study and patient characteristics that could modify the relative treatment effect (Table 20). Four of the studies were published in peer-reviewed journals, while information from the CheckMate 743 trial was available as data on file. Treatment crossover was not permitted in 2 of the studies.14,15
Table 20: Summary of Key Characteristics from Included RCTs (n = 5)
Author name (trial name) | N | Interventions | Population | Country | Phase | Blinding | Primary end point |
|---|---|---|---|---|---|---|---|
NR (CheckMate 743) | 303 | Nivolumab + ipilimumab | Unresectable | Multiple | III | Open-label | OS |
302 | Pemetrexed + cisplatin or carboplatin | ||||||
Habib (2013) (NR) | 19 | Pemetrexed + carboplatin | Unresectable | Egypt | II | Single-blind | NR |
21 | Gemcitabine + cisplatin | ||||||
Vogelzang (2003) (EMPHACIS) | 226 | Pemetrexed + cisplatin | Unresectable | Multiple | III | Single-blind | OS |
222 | Cisplatin | ||||||
Zalcman (2016) (MAPS) | 223 | Bevacizumab + pemetrexed + cisplatin | Unresectable | France | III | Open-label | OS |
225 | Pemetrexed + cisplatin | ||||||
Van Meerbeeck (2005) (EORTC 08983) | 126 | Raltitrexed + cisplatin | Unresectable | Multiple | III | NR | OS |
124 | Cisplatin |
NR = not reported; OS = overall survival; RCT = randomized controlled trial.
Source: Sponsor’s network meta-analysis.33
The EMPHACIS trial reported in Vogelzang et al. (2003),15 did not control for the use of second-line treatments in the analysis of OS; it is therefore possible that results for the control arm were biased to overestimate treatment effect, as a greater proportion of patients in the control group than the intervention group received second-line chemotherapy (47.3% versus 37.6%). Despite the difference in use of second-line therapy between treatment groups, the observed improvement in the intervention group (pemetrexed plus cisplatin) over the control group (cisplatin monotherapy) was statistically significant.
In the MAPS trial reported in Zalcman et al. (2016),14 second-line treatments were used at the discretion of the investigators; however, in the control group, the use of bevacizumab was not permitted, as the trial did not permit treatment crossover. A greater proportion of patients in the control group received second-line treatment compared with the intervention group (72.4% versus 62.0%, respectively). A statistically significant treatment effect was observed indicating benefit in the treatment group (HR = 0.77; 95% CI, 0.62 to 0.95; P = 0.0167); however, the median OS rates between treatment groups, while longer in the treatment group, were not statistically significantly different (18.8 months; 95% CI, 15.9 to 22.6, in the intervention group versus 16.1 months; 95% CI, 14.0 to 17.9, in the comparator group).14 The effect of second-line treatments may have resulted in improved OS in the control group, potentially underestimating the effect of bevacizumab plus pemetrexed plus cisplatin in this trial.
In trial EORTC 08983 by van Meerbeeck et al. (2005),16 32% of patients reported receiving second-line chemotherapy, with similar proportions of patients reporting second-line treatment in both treatment groups. The authors reported that it was unlikely for imbalances in second-line treatments to be responsible for the lack of statistically significant results in OS between treatment groups (HR = 0.79; 95% CI, 0.58 to 1.00), as pemetrexed was not available as a treatment in Europe at the time of the study, and other cytostatic drugs were of unproven value for second-line treatment of patients with mesothelioma; although results did favour treatment with the intervention group (raltitrexed plus cisplatin).
Quality Assessment of Included Studies
A risk-of-bias assessment using the National Institute for Health and Care Excellence checklist was conducted by the sponsor for the 4 published studies (Table 21). The risk-of-bias assessment for the CheckMate 743 trial10 was stated to take place upon data availability. The risk of bias related to randomization and allocation concealment was stated to be unclear for 2 studies. All 4 studies were reported by the sponsor to have a low risk of bias related to baseline characteristics. Three of the studies were reported to have a high risk of bias related to blinding due to the open-label study designs. Only 1 trial reported information pertaining to withdrawal of participants, and it was determined by the sponsor that there were no systematic differences between treatment groups in patients lost and participants observed; the remaining studies did not report details related to patient withdrawals. The sponsor concluded that the risk of bias related to outcome selection and reporting for 2 studies was low; the risk of bias was unclear in the trials by van Meerbeeck et al. (2005)16 and Habib and Fahmy (2013).13 Statistical analyses in all trials was concluded to have a low risk of bias as efficacy and safety analyses were conducted in the ITT or modified ITT populations.
Table 21: Risk-of-Bias Assessment Using NICE Checklist (n = 4 RCTs)
Study name (trial name) | Jaded score | Randomization and allocation concealment | Baseline characteristics | Blinding | Withdrawals | Outcome selection and reporting | Statistical analysis |
|---|---|---|---|---|---|---|---|
Habib (2013) (NR) | 1 | Unclear | Low risk | High risk | Unclear | Unclear | Low risk |
Vogelzang (2003) (EMPHACIS) | 1 | Unclear | Low risk | High risk | Unclear | Low risk | Low risk |
Zalcman (2016) (MAPS) | 3 | Low risk | Low risk | High risk | Low risk | Low risk | Low risk |
Van Meerbeeck (2005) (EORTC 08983) | 2 | Low risk | Low risk | Unclear | Unclear | Unclear | Low risk |
NICE = National Institute for Health and Care Excellence; RCT = randomized controlled trial.
Source: Sponsor’s network meta-analysis.33
Assessment of Clinical Heterogeneity
A summary of baseline characteristics of the included trials is reported in Table 22. The baseline characteristics were mostly similar across the trials. The median age of patients was between 57 and 69 years, and most patients (between 73% and 81%) in all trials were male. Most patients had epithelioid histology (between 68% and 81%), with good performance status (between 83% and 100%). There was some variation in baseline characteristics regarding clinical stage of disease; a greater proportion of patients presented with stage IV disease at baseline in 2 of the studies.10,14 The sponsor reported that the stage of disease at baseline was not reported by Vogelzang et al. (2003); however, upon review by the CADTH reviewers, it was determined that 31% of patients were stage III at baseline, compared to 47% of patients who were stage IV. The stage of disease of patients at baseline did not differentiate between stage III or IV for 1 study.16 Due to the few number of included studies (< 10), the sponsor did not perform a meta-regression to account for differences in baseline characteristics.
Table 22: Summary of Baseline Characteristics of Studies Contributing to Feasibility Assessment (n = 5 RCTs)
Study name | Age (years), median | Predominant histology | % male | Performance status | Stage at baseline | Smokersa | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Epithelioid | Sarcomatoid/ mixed | Scale | 0 | 1 | 2 | III | IV | ||||
Habib (2013) | 57.0 | 70% | 30% | 72.5 | ECOG | 15% | 67.5% | 17.5% | 85% | 15% | 70% |
Zalcman (2016) (MAPS) | 60.5 | 68.3% | 25.95% | 81.4 | KPSb | 84.8% | 15.2% | 31.7% | 46.7% | NR | |
Vogelzang (2003) (EMPHACIS) | 65.7 | 81% | 19% | 75% | ECOG | 97% | 3% | NR | NR | 57% | |
NR (CheckMate 743) | 68.5 | 75.4% | 24.65% | 77.2 | ECOG | 40% | 59.8% | 0% | 34.5% | 51.1% | 56.8% |
Van Meerbeeck (2005) (EORTC 08983) | 58.0 | 68% | 24.5% | 80.0 | ECOG | 24.5% | 62% | 13.5% | 82% | NR | |
ECOG = Eastern Cooperative Oncology Group; KPS = Karnofsky Performance Status; NR = not reported; RCT = randomized controlled trial.
aIncludes both current and/or former smokers.
bKPS scale scores were converted to ECOG scores.
Source: Sponsor’s network meta-analysis.33
Assessment of Similarities of Outcome Definitions Across Trials
All 5 included trials reported results for OS, PFS, and ORR, with the exception of Habib and Fahmy (2013), which did not report PFS, and Zalcman et al. (2016) (the MAPS trial), which did not report results for ORR. Table 23 provides the definitions for study end points in the included trials. Definitions of OS and PFS were generally consistent across all trials. Reporting of definitions for ORR varied across trials; 1 study15 defined patients’ response using RECIST 1.0 criteria versus 2 trials that used RECIST 1.1 and m-RECIST criteria. Two trials13,16 did not specify the version of RECIST used for measurement of patient response. Due to the limited evidence available, the sponsor reported it was unable to assess the impact of response criteria within the NMA.
Table 23: Outcome-Specific Definitions (Author-Reported) Across Included RCTs (n = 5)
Author name (trial name) | OS | PFS | ORR |
|---|---|---|---|
NR (CheckMate 743) | OS was defined as the time from randomization to the date of death | PFS was defined as the time from randomization to the date of the first documented tumour progression as assessed by BICR or death due to any cause (per adapted m-RECIST and/or RECIST 1.1) | ORR was defined as the proportion of all randomized subjects whose BOR from baseline was either a CR or PR per adapted m-RECIST and/or RECIST 1.1 criteria as assessed by BICR |
Vogelzang (2003) (EMPHACIS) | OS was defined as the time from randomization to the time of death from any cause | Time to progressive disease was defined as the time from randomization until documented progression or death from any cause | Tumour response rate was defined as the proportion of patients who experienced either a CR or PR times 100 (RECIST 1.0) |
Zalcman (2016) (MAPS) | OS was defined as the time from randomization to death from any cause | PFS was defined as the time from randomization to documented disease progression or death, whichever occurred first | NR |
Habib (2013) (NR) | OS was calculated from the time of study entry until death from any cause | Outcome not evaluated | The response rate was assessed by a net combination of radiologic data and the percentage of deterioration or improvement of the clinical symptoms of the patient (RECIST) |
Van Meerbeeck (2005) (EORTC 08983) | OS was computed from randomization to the time of death from any cause | PFS was defined as the time elapsed from randomization to progression or death from any cause | Objective response was evaluated and calculated only in patients presenting with measurable disease, using RECIST |
BICR = blinded independent central review; BOR = best overall response; CR = complete response; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: Sponsor’s network meta-analysis.33
Assessment of Heterogeneity Between Reference Groups (Pemetrexed plus Cisplatin/Carboplatin)
Considering differences observed across definitions for ORR, further assessment of heterogeneity between the reference groups across the included trials was conducted to validate study findings. Based on the network feasible, the most common comparators as a reference treatment were pemetrexed plus cisplatin and pemetrexed plus carboplatin. Statistical heterogeneity was presented using the I2 statistic, with a threshold of greater than 75% indicating high levels of heterogeneity between reference groups across trials. The sponsor concluded that there was high heterogeneity for the outcome of ORR based on I2 and relative efficacy analysis. However, the I2 value should be interpreted with caution due to the limited number of studies (n = 3), which may overestimate the amount of heterogeneity.
Based on the I2 value, the assessments for heterogeneity for OS and PFS were low (0%). Additional assessment of heterogeneity in reference groups was conducted for OS and PFS by plotting the reference groups in all studies used for comparisons. Visual representation of these Kaplan–Meier curves indicated high similarity in relative efficacy of pemetrexed plus cisplatin or carboplatin across the 3 trials for PFS. The relative efficacy of OS for pemetrexed plus cisplatin or carboplatin were similar across trials, except for results observed in Habib and Fahmy (2013), which indicated a slightly higher OS compared to the other 3 trials.10,14,15
Testing of Proportional Hazards Assumption
For all studies reporting OS, the evaluation did not suggest a violation of the PH assumption except for Habib and Fahmy (2013). For studies reporting PFS, the evaluation did not suggest a violation of the PH assumption for 2 studies, but Vogelzang et al. (2003)15 and CheckMate 74310 did show a violation.
Table 24: Proportional Hazards Assumption Testing for Studies Reporting OS (n = 5) and PFS (n = 4) Curves
Trial | End point | Global test chi-square, P value | PH assumption true (Yes/No) by log-log plot | Log-log plot |
|---|---|---|---|---|
Habib (2013) | OS | 4.11, P = 0.0427 | No | Study 1 |
PFS | NA | NA | NA | |
Zalcman (2016) | OS | 0.08, P = 0.7745 | Yes | Study 2 |
PFS | 0.10, P = 0.7555 | Yes | Study 2 | |
Vogelzang (2003) | OS | 0.06, P = 0.8076 | Yes | Study 3 |
PFS | 9.45, P = 0.0021 | No | Study 3 | |
Van Meerbeeck (2005) | OS | 0.03, P = 0.8664 | Yes | Study 5 |
PFS | 0.03, P = 0.8536 | Yes | Study 5 | |
CheckMate 743 | OS | 0.01, P = 0.9241 | Yes | Study 4 |
PFS | 23.65, P = 0.0000 | No | Study 4 |
NA = not applicable; OS = overall survival; PFS = progression-free disease.
Source: Sponsor’s network meta-analysis.33
Findings of Feasibility Assessment
An NMAs of OS and PFS were considered feasible due to the availability of evidence to form connected networks. As the PH assumption was not held across all trials, parametric models were fitted to the pseudo-independent patient data. Based on the availability of HRs and Kaplan–Meier curves, CheckMate 743,10 Zalcman et al. (2016),14 van Meerbeeck et al. (2005),16 Vogelzang et al. (2003),15 and Habib and Fahmy (2013)13 contributed to the NMA of OS, and CheckMate 743,10 Zalcman et al. (2016),14 Vogelzang et al. (2003),15 and van Meerbeeck et al. (2005)16 contributed to the NMA of PFS. The sponsor reported that meta-regression analyses of results based on baseline characteristics (i.e., histology and PD-L1 status) could not be conducted due to the limited number of studies included in the NMA.
Checkmate 743,10 Vogelzang et al. (2003),15 van Meerbeeck et al. (2005),16 and Habib and Fahmy (2013)13 were included in the NMA of ORR based on the availability of response data across trials. A high amount of heterogeneity was observed across the reference treatments across trials. The sponsor reported that it was not possible to conduct a sensitivity analysis to account for the potential heterogeneity across trials due to the limited number of studies.
Results
A summary of the PH NMA and NPH NMA results are reported in Table 25 and Table 26, respectively.
Table 25: Summary of Proportional Hazards Network Meta-Analysis Results
End point | Nivolumab plus ipilimumab vs. | ||||
|---|---|---|---|---|---|
Pemetrexed plus cisplatin/carboplatin | Raltitrexed plus cisplatin | Bevacizumab plus pemetrexed plus cisplatin | Cisplatin | Gemcitabine plus cisplatin | |
OS, HR (95% CrI) | 0.74 (0.61 to 0.89) | 0.77 (0.51 to 1.16) | 0.96 (0.72 to 1.28) | 0.57 (0.42 to 0.77) | 0.47 (0.20 to 1.09) |
PFS, HR (95% CrI) | 1.0 (0.82 to 1.22) | 0.91 (0.63 to 1.34) | 1.64 (1.24 to 2.17) | 0.70 (0.53 to 0.93) | NA |
ORR, RR (95% CrI) | 0.94 (0.80 to 1.09) | 1.23 (0.80 to 1.09) | NA | 1.97 (1.40 to 2.91) | 2.38 (0.98 to 7.81) |
Crl = credible interval; HR = hazard ratio; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RR = risk ratio.
Source: Sponsor’s network meta-analysis.33
Table 26: Summary of Non-Proportional Hazards Network Meta-Analysis Results
End point | Nivolumab plus ipilimumab | Pemetrexed plus cisplatin/carboplatin | Raltitrexed plus cisplatin | Bevacizumab plus pemetrexed plus cisplatin | Cisplatin | Gemcitabine plus cisplatin |
|---|---|---|---|---|---|---|
OSa | ||||||
Overall mean survival timeb | 34.81 | 24.04 | 21.40 | 29.42 | 17.53 | NR |
PFSa | ||||||
Mean PFS timec | 15.48 | 10.62 | 10.21 | 16.54 | 8.24 | NA |
Crl = credible interval; NA = not applicable; NR = not reported; OS = overall survival; PFS = progression-free survival.
aFive parametric models (exponential, Weibull, Gompertz, log-normal, and log-logistic) were considered. Based on the deviance information criteria goodness-of-fit statistics, the log-logistic model ranked as the best-fitting model.
bBased on a simulated analysis of mean OS over a 20-year time horizon based on parametric analysis.
cBased on a simulated analysis of mean PFS over a 20-year time horizon based on parametric analysis.
Source: Sponsor’s network meta-analysis.33
Overall Survival
A diagram illustrating the network of the 5 studies used for analysis of OS is presented as Figure 7.
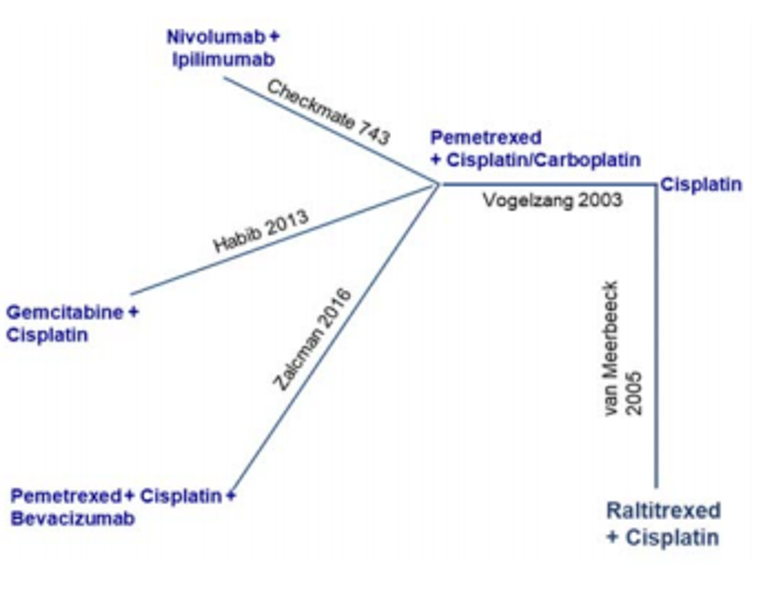
Proportional Hazards Network Meta-Analysis
The results of the NMA reported HRs for OS relative to nivolumab plus ipilimumab of 0.74 for pemetrexed plus cisplatin or carboplatin (95% CrI, 0.61 to 0.89), 0.96 for bevacizumab plus pemetrexed plus cisplatin (95% CrI, 0.72 to 1.28), 0.57 for cisplatin (95% CrI, 0.42 to 0.77), 0.47 for gemcitabine (95% CrI, 0.20 to 1.09), and 0.77 for raltitrexed plus cisplatin (95% CrI, 0.51, to 1.16). Based on the reported 95% CrI, nivolumab plus ipilimumab was favoured in showing an increase in OS relative to pemetrexed plus cisplatin or carboplatin, and cisplatin. For all other comparisons, no comparator was clearly favoured for OS. A summary of OS results based on the fixed-effects models is reported in Figure 8.
Figure 8: Summary Plot of Overall Survival (Fixed-Effects Model)
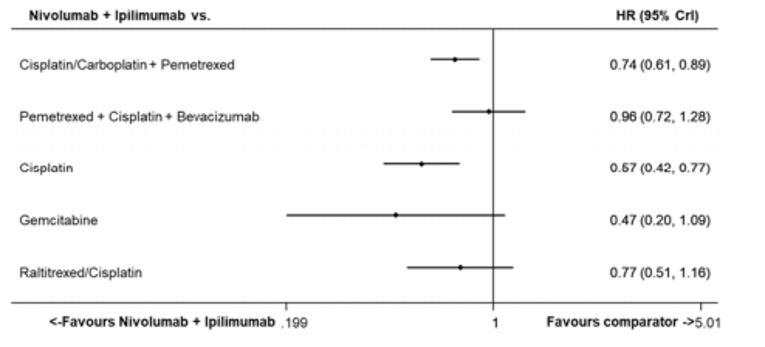
CrI = credible interval; HR = hazard ratio; vs. = versus .
Note: Analyses were conducted via Bayesian linear modelling using a normal likelihood distribution.
Source: Sponsor’s NMA.33
Non-Proportional Hazards Network Meta-Analysis
Based on log-logistic parametric modelling, the NPH NMA predicted survival of 34.81 months with nivolumab plus ipilimumab, 24.04 months with pemetrexed plus cisplatin or carboplatin, 17.53 months with cisplatin, 29.42 months with bevacizumab plus pemetrexed plus cisplatin, and 21.40 months with raltitrexed plus cisplatin. Based on these predictions, treatment with nivolumab plus ipilimumab was estimated to yield the following additional years of survival: 10.8 months compared to pemetrexed plus cisplatin or carboplatin, 17.3 months compared to cisplatin, 5.4 months compared to bevacizumab plus pemetrexed plus cisplatin, and 13.5 months compared to raltitrexed plus cisplatin.
Progression-Free Survival
A diagram illustrating the network of the 4 studies used for analysis of PFS is presented as Figure 9.
Figure 9: Network Diagram of Progression-Free Survival
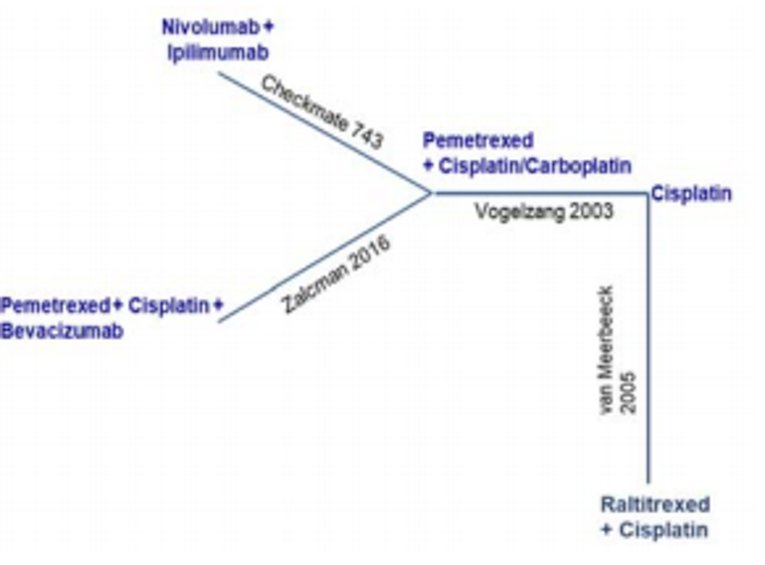
Note: Analyses were conducted via Bayesian linear modelling using a normal likelihood distribution.
Source: Sponsor’s network meta-analysis.33
Proportional Hazards Network Meta-Analysis
The results of the NMA reported HRs for PFS relative to nivolumab plus ipilimumab of 1.00 for pemetrexed plus cisplatin or carboplatin (95% CrI, 0.82 to 1.22), 1.64 for bevacizumab plus cisplatin plus pemetrexed (95% CrI, 1.24 to 2.17), 0.70 for cisplatin (95% CrI, 0.53 to 0.93), and 0.91 for raltitrexed plus cisplatin (95% CrI, 0.63 to 1.34). Nivolumab plus ipilimumab was favoured relative to cisplatin based on the reported 95% CrI, which showed an increase in PFS. Based on the reported 95% CrI, bevacizumab plus pemetrexed plus cisplatin was favoured, showing an increased PFS relative to nivolumab plus ipilimumab. There were no favoured comparators for PFS between nivolumab plus ipilimumab and pemetrexed plus cisplatin or carboplatin or raltitrexed plus cisplatin (Figure 10).
Figure 10: Summary Plot of Progression-Free Survival (Fixed-Effects Model)
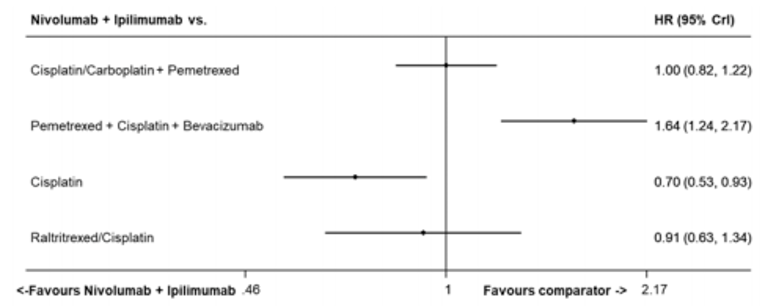
CrI = credible interval; HR = hazard ratio; vs. = versus .
Note: Analyses were conducted via Bayesian linear modelling using a binomial likelihood distribution with a log link.
Source: Sponsor’s NMA.33
Non-Proportional Hazards Network Meta-Analysis
Based on log-logistic parametric modelling, the NPH NMA predicted a PFS of 15.48 months with nivolumab plus ipilimumab, 10.62 months with pemetrexed plus cisplatin or carboplatin, 8.24 months with cisplatin, 16.54 months with bevacizumab plus pemetrexed plus cisplatin, and 10.21 months with raltitrexed plus cisplatin. Based on these predictions, treatment with nivolumab plus ipilimumab was estimated to yield the following additional years of PFS: 4.9 months compared to pemetrexed plus cisplatin or carboplatin, 5.3 months compared to cisplatin, and 7.2 months compared to raltitrexed plus cisplatin. However, when compared to bevacizumab plus pemetrexed plus cisplatin, nivolumab plus ipilimumab was estimated to yield 1 month less of PFS.
Objective Response Rate
A diagram illustrating the network of the 4 studies used for analysis of ORR is presented as Figure 11.
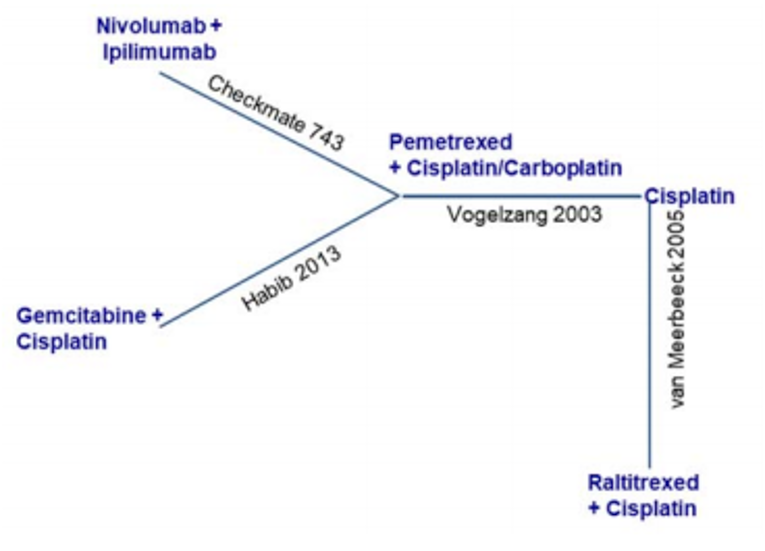
The results of the NMA reported relative risks for ORR relative to nivolumab plus ipilimumab of 0.94 for pemetrexed plus cisplatin or carboplatin (95% CrI, 0.80 to 1.09), 1.23 for raltitrexed plus cisplatin (95% CrI, 0.80 to 2.16), 2.38 for gemcitabine plus cisplatin (95% CrI, 0.96 to 7.81), and 1.97 for cisplatin (95% CrI, 1.40 to 2.91) (Figure 12). Based on the reported 95% CrIs, nivolumab plus ipilimumab was favoured, showing improved ORR compared to cisplatin. No other comparator was clearly favoured for ORR in other comparisons.
Figure 12: Summary Plot of Objective Response Rate (Fixed-Effects Model)
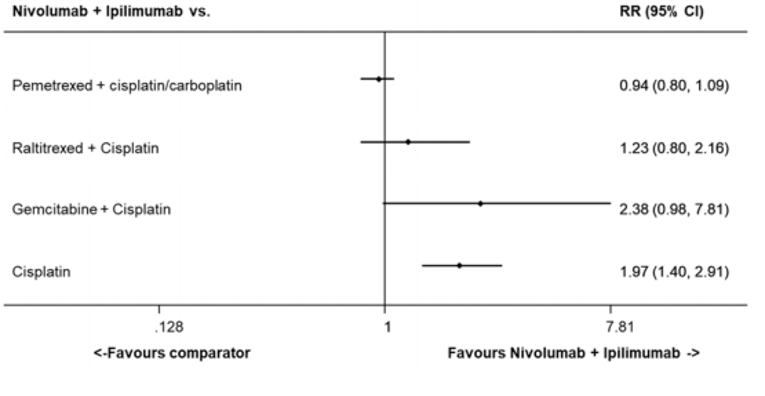
CrI = credible interval; RR = relative risk; vs. = versus .
Source: Sponsor’s network meta-analysis.33
Critical Appraisal of the ITC
The sponsor-conducted NMA was appropriate to the current review for MPM; a systematic review of published literature was conducted to identify all relevant literature for the ITC. In addition, a feasibility assessment was conducted to determine studies of most relevance for incorporation into the NMA; in total 5 studies were incorporated into the NMA to compare the efficacy of nivolumab plus ipilimumab to other first-line treatments for adult patients with MPM. The included studies allowed for pairwise comparisons in treatment effect between nivolumab plus ipilimumab and other comparators (i.e., pemetrexed plus cisplatin or carboplatin, bevacizumab plus pemetrexed plus cisplatin, gemcitabine plus cisplatin, raltitrexed plus cisplatin, and cisplatin monotherapy). The systematic literature review was based on published results up to May 9, 2018, while this CADTH report is current as of 2021. However, the clinical experts consulted for this review suggested that there was likely no new information that would have been missed which would limit the conclusions of the ITC.
The sponsor conducted a risk-of-bias assessment based on the National Institute for Health and Care Excellence checklist for RCTs. In general, there was low risk of bias pertaining to baseline characteristics and statistical analyses of the included trials; however, many of the included studies were unclear in their reporting of randomization and allocation concealment, patient withdrawals, and outcome selection and reporting. Most included trials were open-label and resulted in a high risk of bias related to blinding; the lack of blinding is unlikely to have affected analyses of OS in the sponsor’s ITC as OS is an objective measure that is unlikely to be affected by bias related to lack of blinding compared with analyses of PFS, and ORR may be at greater risk for bias. The sponsor also assessed the PH assumption for analyses of OS and PFS in the included trials. In most instances, the PH assumption was maintained, except in the analysis of OS in the trial by Habib and Fahmy (2013),13 PFS in the trial by Vogelzang et al. (2003),15 and PFS in the CheckMate 743 trial.10 A violation of the PH assumption may be expected in oncology trials in which comparisons are made between treatments with different mechanisms of action that may affect disease progression. The sponsor conducted an NPH NMA, which provided results aligning with the PH NMA. Therefore, while a potential for violation of the PH assumption exists, there is no evidence that this limitation significantly affected the results of the sponsor’s ITC.
Of the included trials, baseline characteristics were generally balanced across trials. Variation was observed in the proportion of patients presenting with stage III or IV disease; although it was not expected to greatly affect results of treatment comparisons. Further, the median ages of patients in the trials by Habib and Fahmy (2013)13 (57 years) and van Meerbeeck et al. (2005)16 (58 years) were lower than in the other 3 trials, including CheckMate 743,10 which reported a median age of 68.5 years. The performance status of patients in CheckMate 743 may be slightly superior, as no patents had an ECOG performance status greater than 1 versus Habib and Fahmy (2013),13 Zalcman et al. (2016),14 and van Meerbeeck et al. (2005),16 in which 17.5%, 15.2%, and 13.5%, respectively, of patients had a performance status of 2. No additional analyses were performed to determine the effect of differences in baseline characteristics across trials on comparisons of efficacy. It is therefore unclear how these imbalances across the included trials may have affected comparisons of efficacy in the NMA. Also, no subgroup analyses were specified or conducted within the NMA. Clinical outcomes for patients with MPM may vary based on performance status of histology. Comparisons of efficacy across subgroups of histology may have been useful in determining the benefit of nivolumab plus ipilimumab relative to other comparators.
The sponsor generated fixed-effect models for the PH NMA of OS and PFS. Fixed-effects models were chosen due to the limited number of trials included used for treatment comparisons. The sponsor also assembled random-effect models and determined, based on residual deviance and DIC statistics, that there was no additional improvement in model fit. To retain parsimony and allow for easy interpretation of NMA results, the fixed-effect models were chosen. Due to the small number of trials used in the treatment comparisons and based on the similar goodness-of-fit analyses of the random-effect models, the use of fixed-effect models was considered acceptable by the CADTH reviewers.
Based on the protocol developed for the CADTH systematic review (as described in the Clinical Evidence section) and input from clinical experts, pemetrexed plus cisplatin or carboplatin were the most relevant comparators in current practice. The additional comparators incorporated into the sponsor’s NMA are not currently approved for use in Canadian clinical practice or may not be relevant as the current standard of care has evolved to be pemetrexed plus cisplatin or carboplatin. Results of the NMA favoured an improvement in OS for treatment with nivolumab plus ipilimumab compared to pemetrexed plus cisplatin or carboplatin (HR = 0.74; 95% CrI, 0.61 to 0.89).33 Estimates for a longer-term OS based on extrapolated data from the NPH NMA were generally consistent with the results from the PH NMA, although the treatments were not formally compared in this approach. Neither treatment was favoured in PFS between nivolumab plus ipilimumab and pemetrexed plus cisplatin or carboplatin. Long-term extrapolations in PFS from the NPH NMA numerically favoured treatment with nivolumab plus ipilimumab, but no formal comparison was made with pemetrexed plus cisplatin or carboplatin for this analysis. The results for PFS should be interpreted with caution as there was evidence of violation of the PH assumption across the included trials. Comparisons of OS between nivolumab plus ipilimumab and bevacizumab plus pemetrexed plus cisplatin did not favour either treatment. While comparisons between these treatments for PFS favoured treatment with bevacizumab plus pemetrexed plus cisplatin, treatment of patients with MPM with bevacizumab plus pemetrexed plus cisplatin is not commonplace in clinical practice and is not considered part of standard of care.
Results for ORR indicated no treatment was favoured between nivolumab plus ipilimumab and pemetrexed plus cisplatin or carboplatin or raltitrexed plus cisplatin, but they did favour an improved ORR with nivolumab plus ipilimumab compared to cisplatin alone. However, a high degree of heterogeneity was observed in the control groups of the included trials for comparison. The variation of results reported for ORR across the trials raises concerns regarding the overall validity of the NMA results, and drawing firm conclusions based on the results of ORR is not recommended.
The sponsor conducted an NPH NMA that involved long-term (20-year) extrapolation of OS and PFS data. Results of follow-up for the included trials, and methods for handling the differences in trial follow-up in the NMA were not reported by the sponsor. The data obtained from such long-term extrapolations may be subject to bias as trials may not report data for such a long follow-up period. Results of the NPH NMA showed numerical improvements in long-term OS and PFS with nivolumab plus ipilimumab relative to other comparators; however, no formal comparisons were made from this analysis, which prevents drawing firm conclusions. Furthermore, estimates of long-term efficacy may be over- or underestimated due to differences in trial length, follow-up and censoring for outcomes, as well as general concerns that accompany extrapolating estimated treatment effects beyond the duration of the included studies.
In addition, the use of second-line therapies was reported to have affected results for 2 of the trials14,15; the analyses of OS in the intervention groups of these trials may have been underestimated due to the higher proportion of patients in the control groups reporting second-line therapies, leading to continued clinical benefit. Data for indirect comparisons from these trials may therefore underestimate the effects of pemetrexed plus cisplatin or carboplatin or the effects of bevacizumab plus pemetrexed plus cisplatin compared to nivolumab plus ipilimumab.
While the sponsor conducted an efficacy analyses (i.e., OS, PFS, ORR) of nivolumab plus ipilimumab relative to other comparators for first-line treatment of patients with MPM, comparisons were not conducted regarding safety or HRQoL. The relative toxicities of nivolumab plus ipilimumab to other comparators included in the NMA are unclear. Because the published trials included indirect comparisons conducted between 5 and 18 years ago, the data from earlier published trials, including Vogelzang et al. (2003)15 and van Meerbeeck et al. (2005)16 may not reflect current clinical practices and may include outdated information; treatments in these trials included pemetrexed plus cisplatin, raltitrexed plus cisplatin, and cisplatin monotherapy. Based on input from the clinical experts consulted for this review, raltitrexed plus cisplatin and cisplatin monotherapy are no longer relevant to the current treatment space for MPM.
Summary
One ITC, submitted and conducted by the sponsor, was summarized and critically appraised. The results of the PH NMA favoured superior OS with nivolumab plus ipilimumab compared to pemetrexed plus cisplatin or carboplatin, and to cisplatin. No treatment was favoured in OS when comparing nivolumab plus ipilimumab to bevacizumab plus pemetrexed plus cisplatin and raltitrexed plus cisplatin. The PH NMA did not favour any treatment in PFS between nivolumab plus ipilimumab and pemetrexed plus cisplatin or carboplatin or raltitrexed plus cisplatin. However, PFS was improved for patients treated with bevacizumab plus pemetrexed plus cisplatin compared to nivolumab plus ipilimumab. Results for OS and PFS from the PH NMA should be interpreted with caution due to potential violations of the PH assumption, particularly for PFS; although results from the NPH NMA were generally consistent with results from the PH NMA. Due to concerns about heterogeneity in the definition of ORR across studies, drawing firm conclusions from the results comparing ORR across treatments is not recommended. Although the sponsor-conducted NMA included many comparators, the CADTH reviewers, with input from clinical experts, determined that the most relevant comparators for the Canadian context were pemetrexed plus cisplatin or pemetrexed plus carboplatin. The sponsor-provided ITC made no comparisons of safety or HRQoL, making the relative toxicity profile of treatments and impact of treatments on PROs uncertain.
Discussion
Summary of Available Evidence
One international, open-label, RCT met the inclusion criteria for this review. CheckMate 743 randomized 605 patients with MPM to either nivolumab plus ipilimumab or standard of care chemotherapy. Enrolled patients were required to have disease that was not amenable to curative therapy (i.e., surgery with or without chemotherapy) and an ECOG performance status of 0 to 1. The combination of nivolumab plus ipilimumab was administered until progressive disease or unacceptable toxicity, or for a maximum of 2 years. Standard of care chemotherapy consisted of pemetrexed plus cisplatin or carboplatin, administered until progressive disease, unacceptable toxicity, or completion of 6 cycles. The primary outcome of this trial was OS, and secondary outcomes included PFS, ORR, and DCR. Health-related quality of life was measured as part of exploratory outcomes. The clinical experts involved in the review noted that the baseline demographic and disease characteristics of patients enrolled in the study were reflective of patients seen in Canadian practice, who would be eligible for front-line systemic treatment for MPM.
A sponsor-submitted ITC compared the efficacy of first-line treatments in adult patients with MPM. The sponsor-conducted NMA included many comparators; however, the most relevant comparators for the Canadian context were pemetrexed plus cisplatin or pemetrexed plus carboplatin. Other comparators included in the NMA may not be relevant as they are not approved for use in Canadian clinical practice (i.e., bevacizumab), or are no longer considered standard of care (i.e., raltitrexed plus cisplatin).
Interpretation of Results
Efficacy
The CheckMate 743 trial showed statistically significant improvement with nivolumab plus ipilimumab over chemotherapy in the primary end point of OS in patients with unresectable MPM (3.98 months longer median survival; HR = 0.74; 95% CI, 0.61 to 0.89). The primary outcome assessed, OS, is a clinically relevant end point in the treatment of MPM and was also an outcome of importance to patients. Although the data reflect results from an interim analysis, this improvement in survival with the combination of nivolumab plus ipilimumab compared to pemetrexed plus cisplatin or carboplatin is considered clinically meaningful. The trial enrolled previously untreated patients with an ECOG performance status of 0 or 1 and disease that is not amenable to curative surgery; the population enrolled in the trial is generally reflective of Canadian patients who would be eligible for systemic treatment. Also, the standard of care chemotherapy used in CheckMate 743 is appropriate; according to the clinical experts consulted for this review, allowing investigators to choose between cisplatin and carboplatin is reflective of usual practice and can be considered a strength of the trial. The clinical experts agreed that the overall results are generalizable to the Canadian setting.
Subgroup analyses of OS were pre-specified and generally consistent with the overall results. Subgroups that showed discordant results were generally due to small sample sizes and wide CIs, leading to imprecise estimates. No firm conclusions can be drawn from these subgroup analyses due to various limitations, including the absence of stratification based on ECOG performance status or PD-L1 expression status, and the study was not powered to detect differences in subgroups. Notable differences in effect were seen in a few subgroups. For example, the unstratified HR for larger subgroups of patients who were former smokers (n = 318) or who had epithelioid tumours (n = 456) included the line of no effect (1.0), indicating uncertainty in the true benefit of nivolumab plus ipilimumab over chemotherapy. Patients with the epithelioid subtype appeared to benefit less (HR = 0.86; 95% CI, 0.69 to 1.08) compared to patients with the non-epithelioid subtype (HR = 0.46; 95% CI, 0.31 to 0.68). As chemotherapy is generally not as effective in patients with non-epithelioid MPM, a greater relative improvement with immunotherapy may be observed, according to the clinical experts. Although this subgroup analysis shows positive results for the group of MPM patients with the greatest unmet need, confirmatory studies are required. As subgroup analyses were not adjusted for multiple comparisons and are exploratory in nature, the treatment effect of nivolumab plus ipilimumab should be interpreted using the overall ITT results.
The patient input identified delayed disease progression as an outcome of importance. The secondary outcomes of PFS, ORR, and DCR were analyzed in CheckMate 743, but the results did not demonstrate that nivolumab plus ipilimumab was superior to chemotherapy. The median PFS was similar in both treatment groups at the time of database lock (6.77 versus 7.20 months; HR = 1.00). The Kaplan–Meier curves for PFS crossed at approximately 8 months, initially showing favourable benefit with chemotherapy, then with immunotherapy, which demonstrates that the magnitude of effect changes over time. The clinical experts consulted by CADTH suggested that this may be an indication that there are 2 patient subpopulations: 1 in which patients do not derive benefit from immunotherapy and another group that derives benefit and experiences longer-term survival from immunotherapy. Importantly, the clinical experts noted that the median PFS alone has not been established as a valid surrogate outcome for OS in patients with MPM. Results for ORR and DCR were similar between the 2 treatment groups, although they were numerically slightly higher for patients treated with chemotherapy. Similar to PFS, both ORR and DCR are unlikely to provide an accurate reflection of benefit in patients with MPM treated with immunotherapy.
Health-related quality life, which was identified by patients as an outcome of particular importance, was measured using appropriate scales. However, these outcomes were exploratory in nature and an MID for LCSS-Meso has not been validated in this patient population. The clinical experts noted that HRQoL in patients with MPM is difficult to measure, as many factors have an impact on-study results. The small number of patients left in the trial and included in the analyses of PROs at later assessment time points (who therefore have better HRQoL) are likely not representative of all patients randomized in each treatment group. In this scenario, data are not missing at random as patients who have left the trial are likely sicker or have died, and therefore, the HRQoL results at later time points are likely biased and not generalizable to the broader patient population. Furthermore, based on the study design, only descriptive results were provided in the Clinical Study Report. The true impact of the study treatments on HRQoL is therefore unknown, and no firm conclusions can be made.
The doses of nivolumab and ipilimumab were similar to what are typically seen for other approved indications. CheckMate 743 used a weight-based dosing regimen for both agents, although the recommended dosage also includes a flat dosage of nivolumab (360 mg every 3 weeks).1 The flat-dose regimen has not been clinically studied in patients with MPM, and it is unknown whether the results of CheckMate 743 can be directly applied to the flat-dose regimen. Also, because the maximum duration of treatment for nivolumab plus ipilimumab in this study is 2 years, the effects of treatment in this patient population beyond 2 years is unknown. However, according to the sponsors, this duration of therapy is in line with other tumour types, and is based on results of a risk-benefit assessment suggesting treatment beyond 2 years with PD-1 checkpoint inhibitors is unlikely to confer additional benefit, but has potential for increased toxicity with continued exposure.11
Several sources of uncertainty in CheckMate 743 were identified. Key limitations include early stopping of the trial based on interim-analysis data; including patients who received subsequent cancer treatment as part of the OS analysis; and enrolling only patients with an ECOG performance status of 0 or 1. These points likely lead to an overestimate of effects, although, based on the Kaplan–Meier curves and primary outcome of OS, the results and conclusion showing improved survival with nivolumab plus ipilimumab appear reasonable.
The sponsor provided an ITC comparing the efficacy of nivolumab plus ipilimumab to pemetrexed plus cisplatin or carboplatin, raltitrexed plus cisplatin, bevacizumab plus pemetrexed and cisplatin, gemcitabine plus cisplatin, or cisplatin monotherapy. The ITC provided little additional evidence to inform the assessment of the clinical benefits associated with nivolumab plus ipilimumab. The results were consistent with those from CheckMate 743 indicating favourable OS with nivolumab plus ipilimumab compared to pemetrexed plus cisplatin or carboplatin, as well as cisplatin monotherapy; however, no treatment was favoured in OS between nivolumab plus ipilimumab and bevacizumab plus pemetrexed plus cisplatin, gemcitabine plus cisplatin, or raltitrexed plus cisplatin. Likewise, the results for PFS and ORR did not clearly favour 1 regimen over the others. Analyses for the various outcomes were limited by notable heterogeneity (particularly in the definition of ORR across trials) and potential violation of the PH assumption for the outcome of PFS. In addition, the published trials used for the ITC were conducted between 5 and 18 years ago, and the clinical practices they studied may not be reflective of current standard of care (i.e., diagnostic staging, treatment patterns). Baseline characteristics of included trials were not consistently similar with CheckMate 743, including worse ECOG performance status, younger median age, and other demographic or clinical variations that may have influenced the results of the ITC. Further, the use of subsequent therapies in the trials was handled differently; trials that did not control for subsequent therapies may have been biased toward the comparator group of the trial, ultimately biasing the ITC. In addition, the sponsor’s ITC did not consider outcomes related to HRQoL, which were key outcomes to patients. Finally, the comparator for the CADTH review was pemetrexed plus cisplatin or carboplatin. The ITC included other comparators that are not relevant for the treatment of MPM in current Canadian clinical practice.
Harms
Overall, AEs reported in CheckMate 743 were consistent with the known AE profile of each drug included in the study. Serious AEs and withdrawals due to AEs were experienced by a greater proportion of patients treated with nivolumab plus ipilimumab compared with chemotherapy. Malignant neoplasm progression, pleural effusion, colitis, pneumonitis, infusion-related reactions, pyrexia, and pneumonia accounted for most of the differences in reported serious AEs. In their input for this reimbursement review, patients identified fatigue or a lack of energy, pain, breathing issues caused by or worsened by treatment, nausea, and vomiting as the most difficult AEs associated with treatment; such AEs were experienced by patients in both treatment groups of CheckMate 743. Of note, according to the Clinical Study Report, the frequency of drug-related hypersensitivity/infusion reaction in the nivolumab plus ipilimumab group (12.0%) was relatively high compared to previous experiences in the treatment of non–small cell lung cancer, melanoma, or renal cell carcinoma. However, most of the events were grade 1 or 2 in severity and resolved within a day. Overall, AEs experienced in this trial were manageable using the established AE management algorithms. As duration of treatment was different between the groups, the study reported incidence rates adjusted for the different lengths of exposure. The exposure-adjusted incidence per 100 person-years was consistently higher in the chemotherapy group for all-cause AEs, grade 3 and 4 AEs, and SAEs. Death due to study-drug toxicity occurred in few patients in both treatment groups (1.0% in nivolumab plus ipilimumab group and 0.4% in the chemotherapy group).
Administration of folic acid and vitamin B12 before administration of pemetrexed plus cisplatin have been shown to reduce the risk of serious toxicity.15 Consistent with usual practice, patients randomized to the chemotherapy group in the CheckMate 743 trial received appropriate routine pre-medications. Based on the mechanism of action, a notable harm monitored with immunotherapy is IMAEs. The Canadian product monographs for both nivolumab and ipilimumab include warnings about the risk of severe and fatal IMAEs such as encephalitis, myocarditis, pneumonitis, hepatitis, enterocolitis, dermatitis (e.g., toxic epidermal necrolysis), neuropathies, endocrinopathies, and toxicities in other organ systems.2,3 In CheckMate 743, pre-specified IMAEs were analyzed in patients who received an immunomodulatory for treatment, except for endocrine events, which were included regardless of treatment. Overall, 128 patients in the nivolumab plus ipilimumab group and 6 patients in the chemotherapy group experienced at least 1 predefined IMAE. Most IMAEs were manageable with the administration of an immune-modulating agent, mostly corticosteroids. Of patients who experienced at least 1 predefined IMAE, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. This translates to approximately 23% of all patients treated with nivolumab plus ipilimumab. However, this may not fully capture all patients who required a high-dose corticosteroid due to any immune-related AE, as the study collected data only on predefined events (i.e., diarrhea and colitis, hepatitis, pneumonitis, nephritis and renal dysfunction, rashes, hypersensitivity or infusion reactions, and endocrine events), and other immune-related AEs discussed in the product monograph may not have been captured in this trial. The proportion of patients who required a high-dose corticosteroid may be indicative of the severity of IMAEs; however, the IMAEs in the trial were manageable using established algorithms.
A limitation of this trial is the open-label study design, in which patient or investigator knowledge of treatment assignment could have influenced the assessment and reporting of AEs. However, there is no clear evidence that the design of the study influenced AE reporting. The clinical experts consulted by CADTH felt that, overall, AEs were similar to what is seen with use of nivolumab and ipilimumab in other cancers, and that the AEs are generally manageable.
A main limitation of the ITC submitted by the sponsor was the lack of comparisons regarding safety. No conclusions regarding the relative safety of nivolumab plus ipilimumab to comparators included in the sponsor’s ITC can be made.
Other Considerations
For this submission, the sponsor proposed 2 dosing regimens for nivolumab: a weight-based dosage of 3 mg/kg given every 2 weeks and a flat dosage of 360 mg given every 3 weeks. Both were subsequently approved by Health Canada for the indication under review. As part of its regulatory submission to Health Canada, the sponsor provided details on both proposed dosing regimens. The sponsor proposed a flat dose of nivolumab for the treatment of patients with MPM, based on the combination of nivolumab 360 mg every 3 weeks with ipilimumab 1 mg/kg every 6 weeks plus 2 cycles of platinum-based chemotherapy shown to be efficacious and safe in patients with previously untreated non–small cell lung cancer. Furthermore, the recommended flat dose and dosing schedule for first-line therapy in patients with MPM were based on evidence from pharmacometric analyses including both population pharmacokinetics simulations and exposure response, as well as clinical subgroup analyses (Appendix 5).1 The CheckMate 743 trial investigated only efficacy and safety of the weight-based dosage of 3 mg/kg every 2 weeks.10 No phase III comparative RCTs that the flat-dose regimen and no direct comparisons of the 2 doses are currently in clinical trials.
Conclusions
Malignant pleural mesothelioma is an aggressive cancer with poor prognosis and few treatment options. The combination of nivolumab plus ipilimumab resulted in longer OS compared with pemetrexed plus platinum-based standard of care for the treatment of patients with unresectable MPM in a single phase III RCT. According to the clinical experts, the results of this study indicate that nivolumab plus ipilimumab would be used as a first-line therapy for patients with unresectable MPM. Limitations with the subgroup analyses preclude drawing concrete conclusions regarding the effects of nivolumab plus ipilimumab based on histology at this time.
Secondary outcomes of PFF, ORR, and DCR did not show numerically favourable results for nivolumab plus ipilimumab, and differences between groups for these outcomes were not formally tested statistically.
The HRQoL as measured using the EQ-5D-3L and LCSS-Meso questionnaires were included as exploratory tools, and firm conclusions cannot be drawn for these end points. Although a high percentage of patients experienced AEs with nivolumab plus ipilimumab, the events were in line with those expected from these drugs and were considered manageable by the clinical experts consulted by CADTH.
References
1.Drug Reimbursement Review sponsor submission: Opdivo+ Yervoy (nivolumab + ipilimumab), 10 mg/mL + 5 mg/mL and administration. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020 Nov 13.
2.Opdivo (nivolumab): 10mg/mL, 40 mg and 100 mg single-use vials, for injection [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada Co; 2021 May 28: https://www.bms.com/assets/bms/ca/documents/productmonograph/OPDIVO_EN_PM.pdf. Accessed 2021 May 31.
3.Yervoy (ipilimumab): for injection. 5 mg/mL, 10 mL and 40 mL vials, for injection [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada Co; 2021 Mar 05: https://www.bms.com/assets/bms/ca/documents/productmonograph/YERVOY_EN_PM.pdf. Accessed 2021 Mar 23.
4.Hiriart E, Deepe R, Wessels A. Mesothelium and Malignant Mesothelioma. J Dev Biol. 2019;7(2):7. PubMed
5.Fels Elliott DR, Jones KD. Diagnosis of Mesothelioma. Surg Pathol Clin. 2020;13(1):73-89. PubMed
6.Nowak AK, Stockler MR, Byrne MJ. Assessing quality of life during chemotherapy for pleural mesothelioma: feasibility, validity, and results of using the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire and Lung Cancer Module. J Clin Oncol. 2004;22(15):3172-3180. PubMed
7.Canadian Cancer Society. Mesothelioma statistics. 2021; https://www.cancer.ca/en/cancer-information/cancer-type/mesothelioma/statistics/?region=on. Accessed 2021 Jan 12.
8.NCCN Guidelines. Malignant Pleural Mesothelioma. Version 2.2020. Plymouth Meeting (PA): National Comprehensive Cancer Network (NCCN); 2020 Oct 15: https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed 2020 Nov 16.
9.Kindler HL, Ismaila N, Armato SG, 3rd, et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36(13):1343-1373. PubMed
10.Clinical Study Report: CA209743. A phase III, randomized, open label trial of nivolumab in combination with ipilimumab versus pemetrexed with cisplatin or carboplatin as first line therapy in unresectable pleural mesothelioma. CheckMate 743: CHECKpoint pathway and nivoluMAb clinical Trial Evaluation 743 [CONFIDENTIAL sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2020 Aug 03.
11.Bristol Myers Squibb Canada response to January 08, 2021 DRR request for additional information regarding Opdivo + Yervoy DRR review: questions related to clinical review [CONFIDENTIAL additional sponsor's information]. Montreal (QC): Bristol Myers Squibb Canada; 2021 Jan 15.
12.Bristol Myers Squibb Canada response to January 22, 2021 DRR request for additional information regarding Opdivo + Yervoy DRR review: patient disposition [CONFIDENTIAL additional sponsor's information]. Montreal (QC): Bristol Myers Squibb Canada; 2021 Jan 27.
13.Habib EE, Fahmy ES. Chemotherapy management of malignant pleural mesothelioma: a phase II study comparing two popular chemotherapy regimens. Clin Transl Oncol. 2013;15(11):965-968. PubMed
14.Zalcman G, Mazieres J, Margery J, et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): a randomised, controlled, open-label, phase 3 trial. Lancet. 2016;387(10026):1405-1414. PubMed
15.Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21(14):2636-2644. PubMed
16.van Meerbeeck JP, Gaafar R, Manegold C, et al. Randomized phase III study of cisplatin with or without raltitrexed in patients with malignant pleural mesothelioma: an intergroup study of the European Organisation for Research and Treatment of Cancer Lung Cancer Group and the National Cancer Institute of Canada. J Clin Oncol. 2005;23(28):6881-6889. PubMed
17.News release: The Government of Canada takes measures to ban asbestos and asbestos-containing products. Ottawa (ON): Environment and Climate Change Canada; 2018: https://www.canada.ca/en/environment-climate-change/news/2018/10/the-government-of-canada-takes-measures-to-ban-asbestos-and-asbestoscontaining-products.html. Accessed 2021 Jan 12.
18.Alimta (pemetrexed disodium): 100 mg or 500 mg per vial, for injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2013 May 10: https://pdf.hres.ca/dpd_pm/00020514.PDF. Accessed 2021 Mar 23.
19.de Perrot M, Vella ET, Bradbury P, et al. Endorsement of the 2018 American Society of Clinical Oncology Treatment of Malignant Pleural Mesothelioma Guideline. Guideline Endorsement 7-14 Version 3. Toronto (ON): Cancer Care Ontario (CCO); 2018: https://www.cancercareontario.ca/en/file/41121/download?token=CZptaqfC. Accessed 2021 Mar 23.
20.U.S. Food and Drug Administration (FDA). FDA News Release: FDA Approves Drug Combination for Treating Mesothelioma. 2020; https://www.fda.gov/news-events/press-announcements/fda-approves-drug-combination-treating-mesothelioma. Accessed 2021 Jan 13.
21.Cisplatin: 1 mg/mL, 50 mg and 100 mg vial, sterile solution for injection BP [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2020 April 03: https://pdf.hres.ca/dpd_pm/00055682.PDF. Accessed 2021 Mar 23.
22.Carboplatin: 10 mg/mL, 50 mg, 150 mg, 450 mg, and 600 mg per vial, sterile solution for injection BP [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2019 Dec 16: https://pdf.hres.ca/dpd_pm/00054389.PDF. Accessed 2021 Mar 23.
23.Cho BC, Feld R, Leighl N, et al. A feasibility study evaluating Surgery for Mesothelioma After Radiation Therapy: the “SMART” approach for resectable malignant pleural mesothelioma. J Thorac Oncol. 2014;9(3):397-402. PubMed
24.International Association for the Study of Lung Cancer (IASLC). 2020 World Conference on Lung Cancer. Presidential Symposium. First-Line Nivolumab + Ipilimumab vs Chemotherapy in Unresectable Malignant Pleural Mesothelioma: CheckMate 743 2020; https://vps2020.iaslc.org/. Accessed 2021 Mar 23.
25.Barlesi F, Audigier-Valette C, Felip E, et al. 92O - Nivolumab plus low-dose ipilimumab as first-line treatment of advanced NSCLC: Overall survival analysis of checkmate 817. ESMO Immuno-Oncology Congress 2019. Ann Oncol. 2019;30(suppl_11). https://oncologypro.esmo.org/meeting-resources/esmo-immuno-oncology-congress-2019/nivolumab-plus-low-dose-ipilimumab-as-first-line-treatment-of-advanced-nsclc-overall-survival-analysis-of-checkmate-817. Accessed 2021 Mar 23.
26.Barlesi F, Audigier-Valette C, Felip E, et al. Abstract OA04.02. Checkmate 817: First-Line Nivolumab + Ipilimumab in Patients with ECOG PS2 and Other Special Populations with Advanced NSCLC. 2019 World Conference on Lung Cancer. Barcelona (ES): International Association for the Study of Lung Cancer (IASLC); 2019: https://wclc2019.iaslc.org/wp-content/uploads/2019/08/WCLC2019-Abstract-Book_web-friendly.pdf. Accessed 2021 Mar 23.
27.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
28.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Nov 16.
29.Baas P, Scherpereel A, Nowak AK, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2021;397(10272):375-386. PubMed
30.Bristol-Myers Squibb. NCT02899299: Study of Nivolumab Combined With Ipilimumab Versus Pemetrexed and Cisplatin or Carboplatin as First Line Therapy in Unresectable Pleural Mesothelioma Patients (CheckMate743). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT02899299. Accessed 2020 Dec 10.
31.Bristol Myers Squibb Canada response to January 08, 2021 DRR request for additional information regarding Opdivo + Yervoy DRR review: questions related to clinical review [CONFIDENTIAL additional sponsor's information]. Montreal (QC): Bristol Myers Squibb Canada; 2021 Jan 20.
32.Bristol-Myers Squibb. NCT02477826: An Investigational Immuno-therapy Trial of Nivolumab, or Nivolumab Plus Ipilimumab, or Nivolumab Plus Platinum-doublet Chemotherapy, Compared to Platinum Doublet Chemotherapy in Patients With Stage IV Non-Small Cell Lung Cancer (NSCLC) (CheckMate 227). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT02477826. Accessed 2021 Mar 23.
33.A network meta-analysis of first-line treatments in patients with malignant pleural mesothelioma. Technical report version 1.0 [CONFIDENTIAL sponsor's report]. In: Drug Reimbursement Review sponsor's submission: Opdivo+ Yervoy (nivolumab + ipilimumab), 10 mg/mL + 5 mg/mL and administration. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020.
34.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12:9. PubMed
35.Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. 2013;33(5):607-617. PubMed
36.Ouwens MJ, Philips Z, Jansen JP. Network meta-analysis of parametric survival curves. Res Synth Methods. 2010;1(3-4):258-271. PubMed
37.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
38.Nunnally JC, Bernstein IH. Psychometric theory. 3rd ed. New York (NY): McGraw‐Hill; 1994.
39.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
40.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
41.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
42.Kontodimopoulos N, Pappa E, Niakas D, Yfantopoulos J, Dimitrakaki C, Tountas Y. Validity of the EuroQoL (EQ-5D) instrument in a Greek general population. Value Health. 2008;11(7):1162-1169. PubMed
43.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
44.Hollen PJ, Gralla RJ, Liepa AM, Symanowski JT, Rusthoven JJ. Measuring quality of life in patients with pleural mesothelioma using a modified version of the Lung Cancer Symptom Scale (LCSS): psychometric properties of the LCSS-Meso. Support Care Cancer. 2006;14(1):11-21. PubMed
45.Hollen PJ, Gralla RJ, Liepa AM, Symanowski JT, Rusthoven JJ. Adapting the Lung Cancer Symptom Scale (LCSS) to mesothelioma: using the LCSS-Meso conceptual model for validation. Cancer. 2004;101(3):587-595. PubMed
46.Gelhorn HL, Skalicky AM, Balantac Z, et al. Content validity and electronic PRO (ePRO) usability of the Lung Cancer Symptom Scale-Mesothelioma (LCSS-Meso) in mesothelioma patients. Support Care Cancer. 2018;26(7):2229-2238. PubMed
47.Sarna L, Swann S, Langer C, et al. Clinically meaningful differences in patient-reported outcomes with amifostine in combination with chemoradiation for locally advanced non-small-cell lung cancer: an analysis of RTOG 9801. Int J Radiat Oncol Biol Phys. 2008;72(5):1378-1384. PubMed
48.Bristol-Myers Squibb. NCT02869789: An Investigational Immuno-therapy Study for Safety of Nivolumab in Combination With Ipilimumab to Treat Advanced Cancers. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT02869789. Accessed 2021 Mar 23.
49.Bristol-Myers Squibb. NCT03215706: A Study of Nivolumab and Ipilimumab Combined With Chemotherapy Compared to Chemotherapy Alone in First Line NSCLC (CheckMate 9LA). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03215706. Accessed 2021 Mar 23.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: November 26, 2020
Alerts: Biweekly search updates until project completion
Study Types: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search Strategy:
Nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335 or 31YO63LBSN).ti,ab,kf,ot,rn,nm.
or/1-2
Ipilimumab/
(yervoy* or ipilimumab* or IPI or strentarga or anti ctla 4* or anti ctla4* or antictla4* or mdx ctla 4 or mdx ctla4 or mdxctla 4 or mdxctla4 or "mdx 010" or mdx010 or mdx 101 or mdx101 or bms 734016 or bms734016 or moab ctla 4 or moabctla 4 or moab ctla4 or moabctla4 or 6T8C155666).ti,ab,kf,ot,rn,nm.
or/4-5
Mesothelioma/ or pleural neoplasms/ or pleural effusion, malignant/
(mesotheli* or celotheli* or submesothali* or MPM).ti,ab,kf.
(pleura* and (neoplas* or cancer* or carcinoma* or tumor* or tumour* or mass or effusion*)).ti,ab,kf.
or/7-9
3 and 6 and 10
11 use medall
*nivolumab/
(opdivo* or nivolumab* or nivo or bms 936558 or bms936558 or cmab 819 or cmab819 or mdx 1106 or mdx1106 or ono 4538 or ono4538 or HSDB 8256 or HSDB8256 or GTPL 7335 or GTPL7335).ti,ab,kw,dq.
or/13-14
*ipilimumab/
(yervoy* or ipilimumab* or IPI or strentarga or anti ctla 4* or anti ctla4* or antictla4* or mdx ctla 4 or mdx ctla4 or mdxctla 4 or mdxctla4 or "mdx 010" or mdx010 or mdx 101 or mdx101 or bms 734016 or bms734016 or moab ctla 4 or moabctla 4 or moab ctla4 or moabctla4 or 6T8C155666).ti,ab,kw,dq.
or/16-17
mesothelioma/ or pleura mesothelioma/ or pleura tumor/ or pleura cancer/ or malignant pleura effusion/
(mesotheli* or celotheli* or submesothali* or MPM).ti,ab,kw,dq.
(pleura* and (neoplas* or cancer* or carcinoma* or tumor* or tumour* or mass or effusion*)).ti,ab,kw,dq.
or/19-21
15 and 18 and 22
23 use oemezd
24 not conference abstract.pt.
12 or 25
remove duplicates from 26
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search] Studies with results | Opdivo/nivolumab, Yervoy/ipilimumab, and mesothelioma
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms] Opdivo/nivolumab, Yervoy/ipilimumab, and mesothelioma
Health Canada’sClinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms] Opdivo/nivolumab, Yervoy/ipilimumab, and mesothelioma
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms] Opdivo/nivolumab, Yervoy/ipilimumab, and mesothelioma
Grey Literature
Search dates: November 16, 2020 – November 26, 2020
Keywords: Search terms – Opdivo/nivolumab, Yervoy/ipilimumab, and mesothelioma
Limits: Publication years: all
Updated: Search updated prior to the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC)
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Table 28: Excluded Studies and Reports
Reference | Reason for exclusion |
|---|---|
CHOW, K. L., et al. Neurology Asia 2020 25(1):87-88 MALLER, B., et al. Journal of Immunotherapy 2018 41(9):411-412 WRIGHT, K. Oncology (Williston Park, N.Y.) 2020 34(11):502-503 | Study design |
HOTTA, K., et al. Expert Opinion on Biological Therapy 2020 20(2):109-114 HOTTA, K., et al. Journal for Immunotherapy of Cancer 2020 8(1) | Review article |
EudraCT Number: 2016-001859-43 | Duplicate trial registry |
Note that this appendix has not been copy-edited.
Appendix 3: Detailed Outcome Data
Table 29: Pre-Specified Sensitivity Analyses for Overall Survival, CheckMate 743
Sensitivity analysis | |
|---|---|
Unstratified log-rank test, HR (97% CI) | 0.75 (0.60 to 0.93) P =0.0030 |
Two-sided stratified weighted log-rank test using G (rho=0, gamma=1) weightsa, HR (97% CI) | 0.74 (0.59 to 0.91) P =0.0027 |
OS multivariate analysisb, HR (96.6% CI) | 0.72 (0.58 to 0.89) P =0.0010 |
Wald P value (for coefficient of time-dependent covariate)c | 0.9646 |
CI = confidence interval; HR = hazard ratio; OS = overall survival.
aTo investigate the delayed effect of immunotherapy, comparing OS between treatment groups.
bTo estimate treatment effect after adjustments made for possible imbalance in known or potential prognostic factors (adjusted for baseline European Cooperative Oncology Group performance status and programmed cell-death ligand 1 status).
cTests for assumptions in the primary Cox proportional hazards model for OS. A 2-sided Wald chi-square P value of less than 0.1 may have suggested a nonconstant treatment effect.
Note that this appendix has not been copy-edited.
Source: Clinical Study Report.10
Table 30: Confirmed Best Objective Response Rate, ITT Population, CheckMate 743
Best overall responsea | Nivolumab plus ipilimumab N = 303 | Chemotherapy |
|---|---|---|
Complete response | 5 (1.7) | 0 |
Partial response | 115 (38.0) | 129 (42.7) |
Stable disease | 112 (37.0) | 125 (41.4) |
Progressive Disease | 55 (18.2) | 14 (4.6) |
Non-CR/Non-PD | 0 | 3 (1.0) |
Unable to Determine | 4 (1.3) | 5 (1.7) |
Not Reported | 12 (4.0) | 26 (8.6) |
CR = complete response; ITT = intention-to-treat; PD = progressive disease.
aMeasured using adapted modified Response Evaluation Criteria in Solid Tumors for pleural mesothelioma and/or Response Evaluation Criteria in Solid Tumors Version 1.1 response criteria and confirmed by blinded independent central review.
Source: Clinical Study Report.10
Table 31: Progression-Free Survival According to Secondary Definition, CheckMate 743
Outcome | CheckMate 743 | |
|---|---|---|
Nivolumab plus ipilimumab | Chemotherapya | |
Efficacy outcomes – ITT population | N = 303 | N = 302 |
Secondary outcome – PFSb | ||
Median, months (95% CI) | 6.93 (5.59 to 8.21) | 7.16 (6.93 to 7.69) |
Events, n (%) | 246 (81.2) | 251 (83.1) |
Stratified HR (95% CI)c | 0.93 (0.78 to 1.12) | |
CI = confidence interval; HR = hazard ratio; ITT = intention-to-treat; PFS = progression-free survival.
aStandard of care chemotherapy regimen consisted of pemetrexed in combination with cisplatin or carboplatin. Cisplatin was preferred for the combination, but carboplatin could have been used at the investigator’s discretion. At cycle 1, cisplatin was initiated in 104 patients, carboplatin was initiated in 180 patients. Switching between cisplatin and carboplatin was permitted; during the trial 29 patients switched from cisplatin to carboplatin; in total, 209 patients were exposed to carboplatin.
bTwo definitions were used in the analysis of PFS. Results reflect analysis using the secondary definition, which did not censor patients who initiated subsequent anti-cancer treatment (ITT population).
cThe HR and corresponding two-sided CI were estimated using a stratified Cox proportional hazards model. An HR of less 1 favours nivolumab plus ipilimumab; stratification factors include tumour histology and gender.
Source: Clinical Study Report.10
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EuroQol 5-Dimensions 3-Level questionnaire (EQ-5D-3L)
Lung Cancer Symptom Score with the mesothelioma adaptation (LCSS-Meso)
Findings
A focused literature search was conducted to identify the psychometric properties and MID of each of the stated outcome measures. Table 31 summarizes the findings.
Interpretation of the reliability and validity metrics were based on the following criteria:
Inter/intra-rater reliability/agreement (kappa statistics or intraclass coefficient); less than 0 to 0.2 = poor, 0.21 to 0.4 = fair, 0.41 to 0.6 = moderate, 0.61 to 0.8 = substantial, 0.81 to1.00 = almost perfect agreement37
Internal consistency (Cronbach alpha) and test-retest reliability (≥ 0.7 is considered acceptable)38
Validity, i.e., between-scale comparison (correlation coefficient, r; ≤ 0.3 = weak, 0.3 to ≤ 0.5 = moderate, > 0.5 = strong).39
Table 32: Summary of Outcome Measures and their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EQ-5D-3L | Generic preference-based HRQoL instrument, consisting of a VAS and a composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression | Validity and reliability not assessed in MPM patients | Not found in MPM patients |
LCSS-Meso | Disease-specific measure designed to measure HRQoL, consisting of 6 symptom-specific questions that address cough, dyspnea, fatigue, pain, hemoptysis, and anorexia, plus 3 summary items on symptom distress, interference with activity level, and global HRQoL10 | Validity, reliability, and feasibility assessed in MPM patients | Not found in MPM patients |
EQ-5D-3L = EuroQol 5-Dimensions 3-Level questionnaire; HRQoL = health-related quality of life; LCSS = Lung Cancer Symptom Score; Meso = Mesothelioma; MID = minimal important difference; MPM = malignant pleural mesothelioma; VAS = visual analogue scale
EuroQol 5-Dimensions Questionnaire
The EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments including mesothelioma. The first of 2 parts of the EQ-5D-3L is a descriptive system that classifies respondents (aged ≥ 12 years) into one of 243 distinct health states. The descriptive system consists of the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 possible levels (1, 2, or 3) representing “no problems,” “some problems,” and “extreme problems,” respectively. Respondents are asked to choose 1 level that reflects their own health state for each of the 5 dimensions. A scoring function can be used to assign a value (EQ-5D-3L index score) to self-reported health states from a set of population-based preference weights. The second part is a vertical, calibrated 20 cm VAS that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state,” respectively. Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the VAS that best represents their own health on that day. Hence, the EQ-5D-3L produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121, or 33211
A population preference-weighted health index score based on the descriptive system
A self-reported current health status based on the EQ-VAS that is used to assess the overall health of the respondent rather than selected dimensions of individuals’ health.
The EQ-5D-3L index score is generated by applying a multi-attribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). For this study, EQ-5D-3L utility index values were computed using a scoring algorithm based on the United Kingdom Time-Trade-Off value set.10 The lowest possible overall score (corresponding to severe problems on all 5 attributes) varies depending on the utility function that is applied to the descriptive system (e.g., −0.59 for the UK algorithm). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.40,41
Internal consistency reliability of the EQ-5D-3L was good with Cronbach alpha of 0.743, exceeding the recommended 0.70 standard for group-level comparisons. The EQ-5D-3L has been extensively validated across countries around the world and in various conditions. However, the EQ-5D-3L has not been validated in patient with mesothelioma specifically, therefore its validity, reliability, and responsiveness to change have not been evaluated in the patient population of interest. There were no studies found to date that assessed the validity and reliability of the EQ-5D-3L in mesothelioma patients. When validated in the general population, internal consistency reliability of the EQ-5D-3L was good with a Cronbach alpha of 0.743, exceeding the recommended 0.70 standard for group-level comparisons. The EQ-5D dimensions, the VAS, and the UK-based utility index were capable of distinguishing between groups of respondents in the general population, in the expected manner, on the basis of sex, age, education, socioeconomic status, self-reported health problems, and health services utilization, thus providing evidence of construct validity. Internal consistency reliability and sensitivity were also satisfactorily demonstrated.42
MID
No reported MID was found for mesothelioma patients. The sponsors submitted evidence reported that an MID for clinically meaningful change was deemed as a change from baseline of 0.08 in the utility index score, for VAS, a MID was considered as change from baseline of 7. For UK-utility scores, MID estimates based on PS ranged from 0.10 to 0.12 both for all cancers and for lung cancer subgroup. For US-utility scores, MIDs ranged from 0.07 to 0.09 grouped by PS for all cancers and for lung cancer. MIDs for VAS scores were similar for lung and all cancers, ranging from 8 to 12 (PS).43
Lung Cancer Symptom Score with the Mesothelioma Adaptation
The LCSS-Meso is a slightly modified version of the LCSS developed for use in subjects with pleural mesothelioma. It includes 5 items measuring disease-related symptoms, including loss of appetite, fatigue, coughing, shortness of breath, and pain. Three additional items measure overall symptom burden, disease-related functional limitations, and HRQoL. The questionnaire uses a 24-hour recall period, and responses for each item are captured using a 100-mm VAS. Scores for individual items ranging from 0 (no symptomatology or highest quality of life) to 100 (worst symptomatology or QoL) are derived by dividing the length of the line drawn from the lowest possible response to the subject’s response by the length of the VAS and multiplying the resulting quotient by 100. An ASBI score can be derived as the mean of scores for the 5 symptom-related items. Higher scores indicate worse symptom severity. A 3-item index of symptom distress, activity level, and QoL can also be derived as the sum of scores for the corresponding items with higher scores being better. The LCSS-Meso has been translated for use in more than 40 languages.10
Hollen et al. examined the LCSS-Meso quantitatively among a cohort of 512 mesothelioma patients drawn from 19 different countries and 5 continents, including evaluations of feasibility, reliability, support of content, construct, and criterion-related validity. Feasibility was demonstrated with a high completion rate of 90% by 512 patients.44
Using the Cronbach alpha coefficient, internal consistency for the eight-item measure was 0.86 for the sample of 495 patients with pleural mesothelioma. The alpha coefficient for the 5-item ASBI was 0.72 for this same sample size. The baseline alpha coefficient for the 5-item observer measure was 0.66. Stability was demonstrated using test-retest with 2 baseline assessments completed 1-16 days apart prior to the start of therapy, there was a high Pearson correlation coefficient for the modified (without the hemoptysis item) eight-item LCSS-Meso (r = 0.87) for a subgroup of 474 patients. Using the guideline by Nunnally and Bernstein that a reliability coefficient ≥ 0.70 is acceptable for new measures, the modified LCSS was judged to be reliable for this group of patients with mesothelioma.38
Nearly all the 495 patients with mesothelioma validated that the symptoms included in the scale captured their disease experience. The only exception was the hemoptysis item, which subsequently was removed from the instrument. Content validity was supported by a literature review aimed specifically at patients with MPM and patient self-report of presenting symptoms (92% of patients had 3 or more symptoms). Using the contrasted group approach, construct validity was well supported by the relationship of median total LCSS-Meso scores with 4 known groups based on performance status. Better scores were found in the higher Karnofsky performance status (KPS) groups, and greater symptom improvement was seen in patients with tumour response. There was good concordance with the LCSS conceptual model and good explanation of variance for summation items. In addition, using the convergence approach to determine the degree to which the 2 forms (eight-item patient and 5-item observer instruments) of the modified LCSS-Meso measure converged, the forms correlated highly (r = 0.57 for 429 patients) despite a median interval of 6 days between measures.44,45
Criterion-related validity was supported by predicting survival time, time to progression, and tumour response rate; all 3 summary items and the total LCSS-Meso score were statistically significant predictors (P < 0.005).44
One study by Gelhorn et al., obtained qualitative data to evaluate the content validity of the LCSS-Meso and the usability of electronic PROs. Twenty-one participants were recruited from 4 clinical sites in the in the USA and were interviewed in person or by telephone. Patients were 18 years of age or older with a clinical diagnosis of mesothelioma with previous or current chemotherapy treatment, and an ECOG status of 0 or 1. Semi-structured interviews were conducted consisting of concept elicitation, cognitive interviewing, and evaluation of electronic patient-reported outcome usability. Results of the LCSS-Meso cognitive interviews provide support for the content validity of the instrument for use in patients with pleural mesothelioma. Most pleural participants were able to understand the LCSS-Meso items, instructions, and response options and thought that the instrument comprehensively assessed symptoms of pleural mesothelioma. Support was found for the clarity and ease of interpretation of each of the LCSS-Meso symptom items comprising the ASBI summary score.46
MID
A clinically meaningful change in LCSS-Meso ASBI score was defined as 10 points by the sponsor. This MID has been extrapolated from literature, specifically, one study where QoL and symptoms were assessed in non–small-cell lung cancer patients treated with amifostine. This study used the European Organization for Research and Treatment of Cancer Global Quality of Life and Pain subscales and the Lung Cancer-13 symptom tool. Clinically meaningful differences in quality of life were characterized by 10-point differences in individual scores pre/post treatment.47
No reported MID was found for mesothelioma patients via literature search.
Appendix 5: Rationale for Proposed Dosing Regimens
Note that this appendix has not been copy-edited.
In the regulatory submission to Health Canada, the sponsors provided details on the 2 proposed dosing regimens of nivolumab. The recommended flat dose and dosing schedule for first-line therapy in patients with MPM of nivolumab 360 mg every 3 weeks plus ipilimumab 1 mg/kg every 6 weeks has been based on evidence from pharmacometrics analyses including both population pharmacokinetics simulation and exposure response, and clinical subgroup analyses.10 To stay consistent with the nivolumab global development program objective of transitioning to a fixed dosing regimen across tumour types, the sponsor conducted an assessment of the key safety and efficacy end points across patient body weights. Additionally, nivolumab exposure quartiles were conducted to support the transition of 3 mg/kg every 2-weeks weight-based dosing to the proposed 360 mg Q3W flat-dosing regimen. The assessment included the efficacy end point OS observed in study CA20974330 and safety end points of grade 2 or more IMAEs, grade 3 or 4 AEs and SAEs observed in studies CA209227,32 CA209817,48 and CA209743.30
The flat-dosing regimen of nivolumab 360 mg every 3 weeks plus ipilimumab 1 mg/kg Q6W plus 2 cycles of platinum-based chemotherapy has been shown in previously untreated first-line NSCLC subjects to be efficacious and safe (Study CA2099LA).49 Thus, the sponsors proposed a flat dose of nivolumab 360 mg Q2W in combination with ipilimumab 1 mg/kg every 6 weeks for the treatment of patients with MPM. The simulated nivolumab exposures are either similar or higher with the flat-dose (360 mg every 3 weeks) regimen compared to the weight-based (3 mg/kg every 2 weeks) dosing. Thus, the efficacy of the flat-dosing regimen is not expected to be compromised. The sponsors submitted an efficacy-response analysis which demonstrated that there is no evidence of improved efficacy with higher exposures of either nivolumab or ipilimumab within the weight-based dosing regimens. Additionally, the exposure-efficacy model predicted similar mean OS probabilities when nivolumab was administered as a weight-based dose or a flat dose in combination with ipilimumab for the first-line treatment of MPM.10
Simulated nivolumab Cmax is higher with the flat-dosing compared to the weight-based regimen, however the concentration is 82% lower than that seen with a dose of 10 mg/kg every 2 weeks. This 10 mg/kg dose was well tolerated with no dose-limiting toxicity observed in the CA209003 study.49 In first-line treatment of MPM, the predicted probability of patients experiencing grade 2 or higher IMAEs is similar when nivolumab dosing regimens of 3 mg/kg every 2 weeks, 240 mg every 2 weeks and 360 mg every 3 weeks are administered. The sponsors submitted clinical safety subgroup analysis which suggested that, overall, no association was observed between body weight subgroups and frequencies of IMAEs, grade 3 and 4 AEs, and SAEs in study CA209743. Examination of safety of MPM patients by exposure quartiles did not indicate a relationship between higher exposures and AEs.30
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
ICER
incremental cost-effectiveness ratio
ECOG
Eastern Cooperative Oncology Group
MPM
malignant pleural mesothelioma
NMA
network meta-analysis
PFS
progression-free survival
OS
overall survival
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo; single-use vial for injection), to be used in combination with ipilimumab (Yervoy; single-use vial for injection) |
Submitted price | Nivolumab, 40 mg (10 mg/mL), IV injection: $782.22 Nivolumab, 100 mg (10 mg/mL), IV injection: $1,955.56 Ipilimumab, 50 mg (5 mg/mL), IV injection: $5,800.00 |
Indication | Nivolumab (Opdivo), in combination with ipilimumab (Yervoy), is indicated for the treatment of adult patients with unresectable MPM who have not received prior systemic therapy for MPM |
Health Canada approval status | NOC |
Health Canada review pathway | Other expedited pathway (Project Orbis) |
NOC date | May 28, 2021 |
Reimbursement request | As per indication |
Sponsor | Bristol Myers Squibb Canada |
Submission history | Previously reviewed: Yes (nivolumab plus ipilimumab and 2 cycles of platinum doublet chemotherapy) Indication: First-line treatment of adult patients with metastatic or recurrent non–small cell lung cancer with no known epidermal growth factor receptor or anaplastic lymphoma kinase genomic tumour aberrations Recommendation date: March 4, 2021 Recommendation: Recommended with a price reduction to improve the cost-effectiveness of nivolumab to an acceptable level Previously reviewed: Yes (nivolumab plus ipilimumab) Indication: Patients with intermediate or poor-risk advanced renal-cell carcinoma based on the International Metastatic Renal Cell Carcinoma Database Consortium Recommendation date: November 1, 2018 Recommendation: Recommended with a price reduction to improve the cost-effectiveness of nivolumab to an acceptable level Previously reviewed: Yes (nivolumab plus ipilimumab) Indication: Patients with unresectable or metastatic melanoma regardless of BRAF status who are treatment-naive, with Eastern Cooperative Oncology Group performance status of 0 or 1 and stable brain metastases, if present Recommendation date: November 30, 2017 Recommendation: Recommended with a price reduction to improve the cost-effectiveness of nivolumab and ipilimumab to an acceptable level |
MPM = malignant pleural mesothelioma; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients with previously untreated unresectable malignant pleural mesothelioma |
Treatment | Nivolumab plus ipilimumab |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (20 years) |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Conclusions
The clinical effectiveness of nivolumab plus ipilimumab is based on a single randomized controlled trial, CheckMate 743, which demonstrated that nivolumab plus ipilimumab is associated with a clinically and statistically significant benefit in overall survival (OS) compared to pemetrexed plus cisplatin or carboplatin after the trial’s median follow-up of 29.7 months. The CADTH clinical review noted limitations related to the receipt of subsequent cancer treatment and the enrolment of only patients with a baseline European Cooperative Oncology Group (ECOG) performance status of 0 or 1. These limitations indicate the magnitude of OS benefits observed in the trial is uncertain. Additionally, no conclusions could be drawn on the long-term comparative effectiveness of nivolumab plus ipilimumab.
CADTH undertook reanalyses to address the limitations in the sponsor’s economic submission, including the exclusion of raltitrexed as a comparator; an assumption of no vial sharing for nivolumab or ipilimumab; and a revision of the prices for comparator chemotherapy treatments. CADTH’s findings remained aligned with the sponsor’s: nivolumab plus ipilimumab is not a cost-effective treatment option for patients with previously untreated unresectable malignant pleural mesothelioma (MPM) at a willingness-to-pay threshold of $50,000 per quality-adjusted life-year (QALY). In the CADTH base-case reanalysis, nivolumab plus ipilimumab was more costly (by $126,305) and more effective (by 0.42 QALYs), for an incremental cost-effectiveness ratio (ICER) of $300,921 per QALY compared to pemetrexed with carboplatin or cisplatin. To achieve an ICER of $50,000 per QALY, the price of nivolumab and ipilimumab would need to be reduced by at least 72%. CADTH was unable to address limitations related to the uncertainty in the long term comparative effectiveness of nivolumab plus ipilimumab in comparison with pemetrexed with platinum-based chemotherapy.
Stakeholder Input Relevant to the Economic Review
This section is a summary of feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Lung Cancer Canada and the Canadian Mesothelioma Foundation submitted joint patient input for this review. Information was collected from environmental scans and surveys and interviews with patients and their caregivers. The top 3 most difficult aspects of treatment reported by those who had received treatment were side effects of treatment (100% of respondents), fear of the unknown (90% of respondents), and having to travel or commute to the hospital (44% of respondents). The most difficult side effects of treatment were fatigue or a lack of energy (67% of respondents), followed by pain (44% of respondents), breathing issues caused or worsened by treatment (44% of respondents), and nausea and vomiting (44% of respondents). One patient respondent spoke to how they were required to temporarily stop treatment with nivolumab plus ipilimumab due to elevated liver enzymes. Another patient reported that their adrenal gland stopped working, and they now take steroids for treatment.
Registered clinician input was provided by representatives of Ontario Health’s Cancer Care Ontario and Lung Cancer Canada. They reported a significant unmet need for more efficacious and less-toxic systemic therapy for patients with MPM, as these patients are often older than 70 years of age and have significant cardiac, pulmonary, and other comorbidities. Clinicians estimate that nivolumab plus ipilimumab will replace pemetrexed plus platinum-based chemotherapy as first-line therapy and will be the preferred therapy for most patients, with about 70% to 80% of patients being treated with nivolumab plus ipilimumab.
Drug plans raised a concern about wastage of ipilimumab, as only 50 mg and 200 mg vials are available in smaller centres. Drug plans pointed out that the dosing schedule described for nivolumab plus ipilimumab is different than those of the other combinations currently funded for nivolumab plus ipilimumab. The drug plans did not acknowledge any relevant comparators other than pemetrexed plus platinum-based chemotherapy.
Several of these concerns were addressed in the sponsor’s model:
Disutility from adverse events (grade 3 and higher), including nausea, vomiting, and fatigue, were applied.
Treatment efficacy, OS, and progression-free survival (PFS) were considered in the economic model using the results of the CheckMate 743 trial.
In addition, CADTH addressed some of these concerns:
CADTH reanalyses assumed no vial sharing for nivolumab and ipilimumab.
CADTH reanalyses did not include raltitrexed as a comparator.
CADTH conducted a scenario analysis with a flat dosing schedule for nivolumab of 360 mg every 3 weeks.
CADTH was unable to address the following concerns raised from stakeholder input
CADTH was unable to conduct a scenario analysis from a societal perspective to account for patients’ needs to commute to hospitals, and other indirect costs. Such a scenario was also not reported in the sponsor’s submission.
CADTH was unable to account for the impact of long-term side effects from treatment, including potential liver or adrenal gland damage.
Economic Review
The current review is for nivolumab (Opdivo) plus ipilimumab (Yervoy) for adult patients with unresectable MPM.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing nivolumab plus ipilimumab to pemetrexed plus cisplatin or carboplatin, and raltitrexed plus cisplatin or carboplatin, for first-line treatment of adult patients with unresectable MPM. The modelled population reflected those recruited in the CheckMate 743 trial and aligns with the Health Canada indication and the reimbursement request.
The sponsor assumed a dosage of 3 mg/kg every 3 weeks for nivolumab and 1 mg/kg every 6 weeks for ipilimumab until loss of clinical benefit or unacceptable toxicity, for up to 2 years, which is aligned with 1 of the dosing regimens in the Health Canada draft product monograph and CheckMate 743.1 At the sponsor’s submitted price of $782.22 per 40 mg vial or $1,955.56 per 100 mg vial for nivolumab, and $5,800.00 per 50 mg vial for ipilimumab, the average drug acquisition cost per 21-day treatment cycle is $12,253, assuming a patient weight of 70 kg and typical drug wastage. The average annual cost of treatment with nivolumab and ipilimumab would be $107,413 per patient.
According to values from the IQVIA drug database, the average drug acquisition cost per 21-day treatment cycle of pemetrexed with platinum-based chemotherapy is $4,266 to $4,491 and the average drug acquisition cost per 21-day treatment cycle of raltitrexed with platinum-based chemotherapy is $1,428 to $1,653.2 The per-cycle price of both drugs is dependent on the type of companion platinum-based chemotherapy, and both can be used for a maximum of 6 cycles.
In the sponsor’s base case, near-perfect vial sharing was assumed for nivolumab and ipilimumab (5% wasted per vial) while no vial sharing was assumed for pemetrexed, raltitrexed, cisplatin, carboplatin, or any subsequent therapies.
The sponsor modelled QALYs and life-years as the primary clinical outcomes. The sponsor’s model took the perspective of the Canadian health care payer and had a lifetime (20-year) time horizon. Costs and QALYs were discounted at an annual rate of 1.5%.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: PFS (according to the modified Response Evaluation Criteria in Solid Tumours criteria3,4), post-progression survival, and death (Figure 1). The model used extrapolated PFS and OS curves to calculate the proportion of patients in each health state over time.4 Patients incurred costs and had health state utilities applied over time depending on the health state they occupied. All patients entered the model in the PFS state and the proportion of patients with progressed disease was estimated as the difference between the proportion of patients living (from the OS curve) and the proportion of patients with progression-free disease (from the PFS curve). Time on treatment was modelled independently from PFS. Subsequent lines of treatment were not explicitly modelled, and only subsequent treatment costs were captured.5,6
Model Inputs
The population characteristics for the sponsor’s model was derived from the CheckMate 743 patient population. As a result, the model included adult patients with unresectable MPM who had not yet received first-line therapy. The average starting age of patients was 68.2, females accounted for 23% of patients, and the average patient weight was 72.75 kg.6
Overall survival, PFS, and time on treatment for nivolumab plus ipilimumab and pemetrexed with platinum-based chemotherapy were sourced from CheckMate 743. Standard parametric survival methods were applied to extrapolate the trial data over the entire model time horizon. The curves were selected for the base case based on statistical fit, visual inspection, and clinical plausibility. Values for PFS and OS for pemetrexed in combination with platinum-based chemotherapy were further validated against the MAPS trial and SEER data.7,8 Dependent and independent parametric survival models were considered based on guidance from the National Institute for Health and Care Excellence.9,10 The sponsor found evidence to suggest that the proportional hazards assumption did not hold for the PFS curves for nivolumab plus ipilimumab compared to pemetrexed with platinum-based chemotherapy, whereas the assumption did hold for OS. Consequently, the sponsor fitted independent survival curves to the PFS data, and a dependent survival model was selected for OS. For PFS curves, the sponsor selected a generalized gamma curve for nivolumab plus ipilimumab and a log-logistic curve for pemetrexed with platinum-based chemotherapy. A dependent log-logistic distribution was selected to extrapolate the OS of both treatments. The sponsor ensured PFS rates in the model were lower or equivalent to OS to avoid a clinically implausible scenario. For duration of treatment, the sponsor found that the trial design and the Kaplan–Meier curves did not lend themselves to dependent analyses and the proportional hazard assumption was violated. The sponsor therefore used the treatment-duration Kaplan–Meier curves from CheckMate 743 to populate treatment duration in the model.6 Nivolumab plus ipilimumab has a stopping rule of 2 years, which was adhered to in CheckMate 743 and was therefore adhered to in the model, with the exception of a small number of trial patients who exceeded it by less than 3 months.5 Risks of adverse events associated with nivolumab plus ipilimumab and pemetrexed with platinum-based chemotherapy were sourced from CheckMate 743.5,6
The sponsor commissioned a network meta-analysis (NMA) to inform the efficacy of nivolumab plus ipilimumab compared with raltitrexed with platinum-based chemotherapy.11 The proportional hazards assumption did not hold for the NMA, as the survival distributions overlapped (i.e., crossed each other). To accommodate this, the sponsor conducted a non-proportional hazards NMA using parametric survival methods. This approach uses a shape-and-scale adjustment technique to account for relative treatment effects. The sponsor identified the log-logistic curve as the best fit for both PFS and OS as it had the lowest deviance information criterion. The risk of adverse events with raltitrexed in combination with platinum-based chemotherapy was sourced from van Meerbeeck et al. (2005).12
Health-state utilities were sourced from a EuroQol 5-Dimensions 3-Levels patient survey conducted as part of CheckMate 743.5,6 Disutility was also applied for adverse events occurring in the model, with disutility values sourced from the literature and adverse event rates sourced from CheckMate 743 and van Meerbeeck et al. (2005).6,12-14
The model included costs related to drug acquisition and administration, adverse events, and health-state resource use. Costs for nivolumab and ipilimumab were based on the sponsor’s submitted price.4 The prices of comparator and subsequent treatments were sourced from previous CADTH reports and the IQVIA drug price database.15,16 The proportion of patients on each type of platinum-based chemotherapy in combination with pemetrexed or raltitrexed were 33% for cisplatin and 67% for carboplatin, based on the patient population in CheckMate 743.5 The sponsor’s model included subsequent therapies (i.e., gemcitabine, vinorelbine, pemetrexed, cisplatin, and carboplatin). A unique proportion of patients in each treatment arm received subsequent therapies, and the distribution among available options was based on CheckMate 743 and clinical expert opinion (Appendix 3).5,6 Treatment administration costs were sourced from the Ontario Schedule of Benefits, while costs of adverse events were sourced from the literature, expert opinion, and the Ontario Case Costing Initiative.17-19 Resource utilization rates for disease management were based on a National Institute for Health Care and Excellence submission for non–small cell lung cancer.20 Costs incurred from the resource use associated with each health state were sourced from the Ontario Schedule of Benefits and the literature.21-23 All costs reported in the model were in 2020 dollars.
Summary of Sponsor’s Economic Evaluation Results
The sponsor’s model reported the mean of its probabilistic results over 1,000 model iterations. The probabilistic results are all based on publicly available prices for the comparator treatments.
The sponsor also submitted deterministic results from its model. The deterministic results did not align with the probabilistic results as raltitrexed plus platinum-based chemotherapy was dominated by nivolumab plus ipilimumab in the deterministic results (i.e., raltitrexed plus platinum-based chemotherapy is more costly and less effective than nivolumab plus ipilimumab). However, when accounting for parameter uncertainty around the estimate of clinical effectiveness of raltitrexed plus platinum-based chemotherapy in the probabilistic analysis, raltitrexed plus platinum-based chemotherapy was on the frontier of cost-effectiveness.
Base-Case Results
The sponsor’s base case results are presented in Table 3. All 3 interventions were on the cost-effectiveness frontier, with pemetrexed in combination with platinum-based chemotherapy resulting in the lowest total costs, and nivolumab in combination with ipilimumab resulting in the highest total costs. Based on the sequential analysis and a willingness-to-pay threshold below $175,691 per QALY, pemetrexed with platinum-based chemotherapy was the preferred treatment option. Raltitrexed with platinum chemotherapy was the preferred treatment option at a willingness-to-pay threshold between $175,691 per QALY, while nivolumab plus ipilimumab was the preferred option at $350,503 per QALY. Nivolumab plus ipilimumab had a 0% chance of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. Additional results from the sponsor’s submitted economic evaluation base case, including cost-effectiveness acceptability curves, are presented in Appendix 3.
The ICER was driven primarily by drug acquisition costs, particularly the higher cost of nivolumab plus ipilimumab. Additionally, 47% of the incremental benefit observed with nivolumab plus ipilimumab in comparison with pemetrexed plus platinum-based chemotherapy was from the period for which observed data were available. The rest of the incremental benefit was observed over the extrapolation period.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Pemetrexed + cisplatin or carboplatin | 51,593 | 1.477 | Reference |
Raltitrexed + cisplatin or carboplatin | 67,990 | 1.571 | 175,691 |
Nivolumab + ipilimumab | 187,005 | 1.910 | 350,503 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.21
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses to measure the impact of alternative assumptions in its base case, as reported in Table 12. These analyses included a 0% and 3% discount rate, a flat dose for nivolumab (360 mg every 3 weeks), full drug wastage for all drugs (i.e., no vial sharing allowed), near-perfect vial sharing for all drugs (minimal drug wastage), treatment-specific utilities, PFS used as a proxy for duration of treatment, and alternative OS curve distributions (independent log-logistic curves for both nivolumab plus ipilimumab and pemetrexed plus platinum-based chemotherapy).
Adjusting the distributions used for the OS curve or PFS extrapolation reduced the ICER of nivolumab plus ipilimumab versus raltitrexed with chemotherapy by approximately 30% from the sponsor’s base case to $217,020 per QALY. Using PFS as a proxy for treatment duration increased the ICER of nivolumab plus ipilimumab versus raltitrexed with chemotherapy by 22% from the sponsor’s base case to $413,453 per QALY. No other scenario produced meaningful changes to the ICER.
The sponsor also conducted subgroup analyses assessing the cost-effectiveness of nivolumab and ipilimumab by histology (i.e., epithelioid and non-epithelioid patients). As subgroup data were not available for raltitrexed with chemotherapy, this comparator was excluded from subgroup analyses. In analysis of the non-epithelioid patient subgroup, the ICER of nivolumab plus ipilimumab versus pemetrexed with chemotherapy was reduced to $167,328 per QALY. Focusing the analysis on the subgroup of epithelioid patients, the ICER of nivolumab plus ipilimumab versus pemetrexed with chemotherapy increased to $693,398 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations with the sponsor’s analysis that have notable implications on the economic analysis:
The long-term comparative efficacy of nivolumab plus ipilimumab to pemetrexed with platinum-based chemotherapy remains uncertain. To inform the clinical efficacy for the entirety of the 20-year model time horizon, the sponsor used parametric survival analysis to extrapolate PFS and OS data from the CheckMate 743 trial. While both OS and PFS were considered mature (i.e., median survival was reached), the sponsor’s parametric survival analyses extrapolated a maximum of 3 years of follow-up data from the trials over 20 years. Approximately 47% of the QALY benefit observed with nivolumab plus ipilimumab in the sponsor’s base case was from the initial 3-year period for which observed data were available, with the remaining 53% of the QALY gain compared with pemetrexed plus platinum-based chemotherapy obtained from the extrapolation period. The CADTH clinical review was unable to reach a definitive conclusion on the long-term PFS and OS benefit of nivolumab plus ipilimumab, noting that, due to limitations related to the receipt of subsequent cancer treatment and the enrolment of only patients with a baseline ECOG performance status of 0 or 1, the OS benefit observed in the trial with nivolumab plus ipilimumab may be overestimated. As a result, there is uncertainty with the data informing extrapolations of PFS and OS, and the long-term efficacy of nivolumab plus ipilimumab compared to pemetrexed plus platinum-based chemotherapy remains uncertain.
The CADTH clinical review concluded that the combination of nivolumab plus ipilimumab resulted in longer OS compared with pemetrexed plus platinum-based chemotherapy. Additionally, the clinical experts consulted by CADTH for this review noted that the curves selected by the sponsor for its base case were plausible in the absence of supporting evidence.
CADTH conducted a scenario analysis testing an OS distribution that was less-optimistic than the distribution selected by the sponsor in its base case.
Raltitrexed has limited relevance to Canadian clinical practice and its comparative effectiveness relative to nivolumab plus ipilimumab and to pemetrexed with carboplatin or cisplatin is uncertain. The sponsor included raltitrexed with platinum-based chemotherapy as a comparator in its base case, with comparative clinical effectiveness informed by the sponsor’s NMA. The clinical experts and drug plan representatives consulted by CADTH for this review stated that raltitrexed with platinum-based chemotherapy is not currently used for the treatment of MPM in Canada. Additionally, differences between CheckMate 743 and the van Meerbeeck et al. (2005) trial (EORTC-08983) informing the sponsor’s NMA reduce the comparability of the clinical effectiveness between treatments. Baseline characteristics of patients in EORTC-08983, including worse ECOG performance status, younger median age, and other demographic or clinical variations, were not aligned with those of CheckMate 743 and may have influenced the results of the trial.11 The EORTC-08983 trial was conducted almost 16 years before CheckMate 743 and does not reflect changes in standard of care or available treatment options that have occurred during that time. The ITC results are highly uncertain.
Raltitrexed was excluded as a comparator in the CADTH base case and was only considered a comparator in a scenario analysis
The extent of drug wastage modelled for nivolumab and ipilimumab is uncertain. In its base case, the sponsor assumed that vials of the comparator treatments (pemetrexed, raltitrexed, carboplatin, and cisplatin) would not be shared and that drug wastage would occur. However, near-perfect vial sharing (no drug wastage) was assumed for nivolumab and ipilimumab. According to their draft product monographs, nivolumab and ipilimumab are single-use vials.1,24 Although larger cancer-treatment centres may be able to accommodate some vial sharing due to large volumes of patients, vial sharing may not be near-perfect and would be less likely in smaller cancer-treatment centres according to clinical experts consulted by CADTH. The assumed near-perfect vial sharing underestimated the drug acquisition costs associated with the combination of nivolumab and ipilimumab, biasing results in its favour.
Vial sharing was not considered in the CADTH base case to align with the draft product monographs. Near-perfect vial sharing was considered for ipilimumab plus nivolumab and pemetrexed plus platinum-based chemotherapies in a scenario analysis.
Prices for comparator chemotherapy were inaccurate. The prices of certain chemotherapy drugs used in the sponsor’s submitted model were sourced from previous CADTH reports and did not align with costs reported in the IQVIA Delta PA database. The costs of pemetrexed, cisplatin, carboplatin, and subsequent chemotherapies were all underestimated in the sponsor’s model. The sponsor’s model priced a 100 mL vial (1 mg/mL) of cisplatin at $19.00, a 15 mL vial (10 mg/mL) of carboplatin at $18.80, a 50 mg vial of pemetrexed at $38.00, a 20 mL vial of gemcitabine at $44.00, and a 1 mL vial (10 mg/mL) of vinorelbine at $6.80. The IQVIA drug price database priced a 100 mL vial (1 mg/mL) vial of cisplatin at $135.00, a 60 mL vial (10 mg/mL) vial of carboplatin at $56.00, a 100 mg vial of pemetrexed at $429.00, a 1 g vial of gemcitabine at $270.00, and a 1 mL vial (10 mg/mL) of vinorelbine at $80.00. The inaccurate costs of chemotherapy led to underestimates of the cost of pemetrexed-based therapy, and overestimates of the incremental costs associated with nivolumab plus ipilimumab, biasing the results against nivolumab plus ipilimumab.
The CADTH base case was informed by prices in the IQVIA drug price database.11
The cost-per-dose formulas for several comparators were incorrect. The sponsor made several calculation errors with regards to the cost per dose of various first- and second-line drugs included in the model. This led to over- and underestimates of the cost per dose of several included comparators (Table 5). Additionally, there were inconsistencies in the sponsor’s base case with regards to the cost of equivalently dosed first- and second-line drugs. This had minimal impact on the sponsor’s base case results and had a greater impact on scenarios in which alternative vial-sharing assumptions were tested.
CADTH corrected the cost-per-dose formulas in the sponsor’s model to accurately reflect the dose and number of vials needed in situations without vial sharing for nivolumab, ipilimumab, carboplatin, cisplatin, and pemetrexed. CADTH also ensured alignment between costs per dose in the first-line and second-line regimens, in which doses were supposed to be equivalent.
Key assumptions made by the sponsor and appraised by CADTH are presented in Table 4.
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Weight-based dosing for nivolumab as opposed to flat dosing | Appropriate. The clinical experts consulted by CADTH for this review indicated weight-based dosing would be preferred in Canadian clinical practice. The flat dose was considered in a CADTH scenario analysis. |
Distribution of the use of carboplatin and cisplatin as companion therapies to pemetrexed and raltitrexed (33% cisplatin, 67% carboplatin) | Appropriate. Even though these values do not perfectly align with the CheckMate 743 trial data, the clinical experts consulted by CADTH for this review stated that this distribution is likely representative of clinical practice. |
Treatment discontinuation based on trial data | Appropriate. The clinical experts consulted by CADTH stated that the treatment discontinuation seen in the trial likely reflects real-world practice. |
Dosing of carboplatin of 550 mg once every 3 weeks | Appropriate. This dose falls within the range provided by clinical experts consulted by CADTH. |
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH undertook a stepped analysis, incorporating each change detailed in Table 5 into the sponsor’s corrected base case to highlight the impact of each change. The summary results of the sponsor’s corrected base case and the CADTH reanalyses are presented in Table 6.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption | |
|---|---|---|---|
Correctionsa to sponsor’s base case | |||
Cost per dose: the formulas used by the sponsor to calculate vials required per administration (assuming wastage) resulted in erroneous values; inconsistencies between costing of first-line and second-line drug regimen costs were fixed as well | Values provided in the model: First-line therapies Nivolumab: $4,492.62 Ipilimumab: $8,883.162 Cisplatin: $9.47 Carboplatin: $75.87 Second-line therapies Pemetrexed: $684.00 | Values calculated using patient weight, drug strength, drug vial size, administration frequency, and the sponsor’s vial sharing assumptions: First-line therapies Nivolumab: $4,481.39 Ipilimumab: $8,860.95 Cisplatin: $28.50 Carboplatin: $75.20 Second-line therapies Pemetrexed: $722.00 | |
Changes to derive the CADTH base case | |||
1. Choice of comparators | Pemetrexed with platinum-based chemotherapy and raltitrexed with platinum-based chemotherapy | Pemetrexed with platinum-based chemotherapy only | |
2. Vial sharing | Near-perfect vial sharing for nivolumab and ipilimumab but no vial sharing for pemetrexed, cisplatin, carboplatin, or subsequent treatments | No vial sharing for any drugs | |
3. Price of chemotherapy | Cisplatin: 100 mL vial (1 mg/mL): $19.00 Carboplatin: 15 mL vial (10 mg/mL): $18.80 Pemetrexed: 50 mg vial: $38.00 Gemcitabine: 20 mL vial: $44.00 Vinorelbine: 1 mL (10 mg/mL) vial: $6.80 | Cisplatin: 50 mL vial (1 mg/mL): $135.00 Carboplatin: 60 mL vial (10 mg/mL): $56.00 Pemetrexed: 100 mg vial: $429.00 Gemcitabine: 1g vial: $270.00 Vinorelbine: 1 mL (10 mg/mL) vial: $80 | |
CADTH base case | 1 + 2 + 3 | ||
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses) that are not identified as limitations.
In the CADTH base case, nivolumab plus ipilimumab was associated with additional costs of $126,305 and 0.42 additional QALYs, for an ICER of $300,921 per QALY gained compared to pemetrexed with platinum-based chemotherapy. Using a willingness-to-pay threshold of $50,000 per QALY, there is a 0% probability that nivolumab plus ipilimumab would be cost-effective under the CADTH base case. This is primarily due to the higher treatment acquisition costs of nivolumab and ipilimumab. Additionally, only 47% of the incremental benefit observed with nivolumab plus ipilimumab in comparison with pemetrexed with platinum-based chemotherapy was from the period for which observed data were available.
Detailed results of the CADTH base case are presented in Table 13 of Appendix 4.
The reanalysis is based on publicly available prices of the comparator treatments. A run-to-run variation in the total QALYs was observed for all comparators. This contributed to raltitrexed being on the cost-effectiveness frontier in some results and being extendedly dominated in others.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Pemetrexed plus cisplatin or carboplatina | 51,593 | 1.477 | Reference |
Raltitrexed plus cisplatin or carboplatin | 67,990 | 1.571 | 175,691 | |
Nivolumab plus ipilimumab | 187,005 | 1.910 | 350,503 | |
Sponsor’s corrected base case | Pemetrexed plus cisplatin or carboplatina | 52,132 | 1.480 | Ref |
Nivolumab plus ipilimumab | 186,856 | 1.897 | 323,079 | |
Raltitrexed plus cisplatin or carboplatin | 67,056 | 1.509 | Extendedly dominated | |
CADTH reanalysis 1 (raltitrexed removed as comparator) | Pemetrexed plus cisplatin or carboplatina | 52,092 | 1.478 | Reference |
Nivolumab plus ipilimumab | 186,968 | 1.907 | 314,396 | |
CADTH reanalysis 2 (no vial sharing) | Pemetrexed plus cisplatin or carboplatina | 51,809 | 1.479 | Reference |
Raltitrexed plus cisplatin or carboplatin | 67,372 | 1.531 | 299,288 | |
Nivolumab plus ipilimumab | 200,689 | 1.910 | 351,760 | |
CADTH reanalysis 3 (updated chemotherapy prices) | Pemetrexed plus cisplatin or carboplatina | 75,870 | 1.478 | Reference |
Nivolumab plus ipilimumab | 188,292 | 1.899 | 267,036 | |
Raltitrexed plus cisplatin or carboplatin | 81,073 | 1.489 | Extendedly dominated | |
CADTH base case (1 + 2 + 3) | Pemetrexed plus cisplatin or carboplatina | 76,090 | 1.481 | Reference |
Nivolumab plus ipilimumab | 202,176 | 1.900 | 300,921 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aReference product is the least-costly alternative.
Scenario Analysis Results
Several scenario and sensitivity analyses were conducted on the CADTH base case (Table 14, Appendix 4).
These scenario analyses explored vial-sharing assumptions, choice of OS curve for both treatment arms, dosing of nivolumab, and the prices of comparator and subsequent chemotherapies (Table 15). The model interpretations remained robust as no scenario or subgroup brought the ICER of nivolumab plus ipilimumab near the threshold of $50,000 per QALY. CADTH explored the long-term comparative efficacy of nivolumab and ipilimumab versus pemetrexed with platinum-based chemotherapy in a scenario analysis by implementing a less-optimistic OS curve for nivolumab plus ipilimumab. Switching the distribution of the OS curves of both treatment arms to the more pessimistic but statistically superior gamma distribution resulted in an ICER of $360,203 per QALY.
Price-reduction analyses were conducted using both the sponsor and CADTH base cases and assuming proportional price reductions for both nivolumab and ipilimumab (Table 7). A 72% price reduction is required for nivolumab plus ipilimumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
The comparator raltitrexed was excluded from the sponsor’s corrected base-case column in Table 7 due to its limited clinical relevance and to align the results of the sponsor’s corrected base case with the CADTH reanalysis.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for nivolumab plus ipilimumab vs. pemetrexed with platinum-based chemotherapy and raltitrexed with platinum-based chemotherapy | |
|---|---|---|
Price reduction | Sponsor-corrected base case | CADTH reanalysis |
No price reduction | $323,264 | $300,921 |
10% | $272,418 | $266,291 |
20% | $244,023 | $226,440 |
30% | $213,868 | $194,572 |
40% | $185,342 | $157,461 |
50% | $153,577 | $123,035 |
60% | $124,707 | $88,122 |
70% | $91,665 | $53,762 |
80% | $62,367 | $18,607 |
90% | $31,909 | Dominant |
ICER = incremental cost-effectiveness ratio.
CADTH also conducted an exploratory subgroup analysis by histology (epithelioid and non-epithelioid patients) (Appendix 4, Table 16). The ICER for nivolumab and ipilimumab compared with pemetrexed plus platinum-based chemotherapy was $538,804 per QALY for epithelioid patients and $159,303 per QALY for non-epithelioid patients. However, the data informing these subgroups were based on exploratory analyses from the CheckMate 743 trial, and the duration on treatment data, which is a key driver of drug acquisition costs, was not specific to each subgroup.
Issues for Consideration
Dosing for nivolumab for this indication is different than the dosing for nivolumab for other indications. The sponsor’s model uses a weight-based dose (3 mg/kg every 2 weeks), which aligns with the draft product monograph. The sponsor presented the option of using a flat dose of nivolumab (360 mg every 3 weeks), which is the other dosing option in the draft product monograph.1 CADTH explored this dose in a scenario analysis. Clinical experts noted that the weight-based approach used in the CADTH base case is the dosing schedule most likely to be used in clinical practice.
Gemcitabine (with or without platinum-based chemotherapy) and vinorelbine monotherapy may be considered under certain circumstances, such as for patients who cannot tolerate pemetrexed. These options were not included as comparators in the sponsor’s submission but have limited relevance to the majority of patients with unresectable MPM. The cost-effectiveness of nivolumab plus ipilimumab in comparison to gemcitabine with platinum-based chemotherapy and vinorelbine monotherapy remains unknown.
Nivolumab plus ipilimumab is an IV injection. Nivolumab is administered as an infusion over 30 minutes, followed by ipilimumab administered as an infusion over 30 minutes on the same day. Pemetrexed is administered as an IV infusion over 10 minutes followed by platinum-based chemotherapy for 2 hours. The difference in time spent receiving infusion is minimal; however, pemetrexed is delivered for a maximum of 18 weeks while nivolumab plus ipilimumab is delivered for a maximum of 2 years.
Overall Conclusions
Based on the CADTH clinical review of the sponsor-submitted trial (CheckMate 743), nivolumab plus ipilimumab was associated with a statistically and clinically significant increase in OS when compared with pemetrexed in combination with platinum-based chemotherapy for patients with unresectable MPM. The CADTH clinical review noted limitations related to the receipt of subsequent cancer treatment and the enrolment of only patients with a baseline ECOG performance status of 0 or 1. These limitations make the magnitude of the OS benefit observed in the trial uncertain. Additionally, no conclusions could be drawn on the long-term comparative effectiveness of nivolumab plus ipilimumab with pemetrexed with platinum-based chemotherapy.
CADTH undertook reanalyses to address limitations with the sponsor’s submission, including removing raltitrexed as a comparator; considering vial wastage for nivolumab and ipilimumab; and updating the price of comparator chemotherapies. The CADTH base case found nivolumab plus ipilimumab is associated with a higher incremental cost of $126,305 and more QALYs (0.42), for an ICER of $300,921 per QALY gained compared to pemetrexed with platinum-based chemotherapy. These findings are aligned with the sponsor’s results: nivolumab plus ipilimumab has a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. A price reduction of at least 72% is necessary for a combination of nivolumab and ipilimumab to be cost-effective at a threshold of $50,000 per QALY.
The model requires extrapolation of data from the CheckMate 743 trial, which had a maximum follow-up of 3 years, to a time horizon of 20 years. This introduces some uncertainty to the results, as the true long-term efficacy of nivolumab plus ipilimumab remains uncertain, although clinical experts considered the estimates used in the CADTH base case plausible. When an alternative distribution with less-optimistic estimates of OS, but a better statistical fit, were used, the ICER for nivolumab plus ipilimumab rose to $360,203. Additionally, the model is sensitive to drug acquisition costs. While clinical experts consulted by CADTH stated that the use of the alternative dosing schedule described in the draft product monograph for nivolumab (360 mg every 3 weeks) is unlikely to be used in clinical practice, CADTH found it had minimal impact on the ICER ($314,394 per QALY versus pemetrexed).
The sponsor also submitted subgroup analyses by patient histology. While there is evidence that the clinical efficacy and resulting ICERs for nivolumab plus ipilimumab differ between patients with non-epithelioid and epithelioid histologies, the data informing the model for these subgroups were based on exploratory analyses, and the data for duration on treatment, which is a key driver of drug acquisition costs, was not specific to each subgroup. As a result, the cost-effectiveness of nivolumab plus ipilimumab by histology is highly uncertain.
References
1.B.C. Government. BC PharmaCare formulary search. 2020; https://pharmacareformularysearch.gov.bc.ca. Accessed 2021 Feb 17.
2.PharmaStat. Ottawa (ON): IQVIA; 2020: https://www.iqvia.com/. Accessed 2021 Feb 17.
3.Tovoli F, Renzulli M, Granito A, Golfieri R, Bolondi L. Radiologic criteria of response to systemic treatments for hepatocellular carcinoma. Hepat Oncol. 2017;4(4):129-137. PubMed
4.Drug Reimbursement Review sponsor submission: Opdivo+ Yervoy (nivolumab + ipilimumab), 10 mg/mL + 5 mg/mL and administration. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020 Nov 13.
5.Bank of Canada. Inflation calculator. 2020; https://www.bankofcanada.ca/rates/related/inflation-calculator/. Accessed 2021 Feb 17.
6.Baas P, Scherpereel A, Nowak AK, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2021;397(10272):375-386. PubMed
7.Clinical Study Report: IFCT-1501 MAPS2. A randomized phase II study evaluating efficacy and safety of 2nd or 3rd line treatment by nivolumab monotherapy or nivolumab plus ipilimumab, for unresectable malignant pleural mesothelioma (MPM) patients. MAPS2: Mesothelioma anti-PD-1/ anti-CTLA-4 Study 2 [CONFIDENTIAL sponsor's report]. Paris (FR): Intergroupe Francophone de Cancérologie Thoracique (IFCT); 2020 Jun 12.
8.National Cancer Institute. Surveillance, Epidemiology, and End Results Program. 2020; https://seer.cancer.gov/index.html. Accessed 2021 Feb 17.
9.Government of Alberta. Interactive drug benefit list. 2020; https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2021 Feb 17.
10.Latimer N. NICE DSU Technical Support Document 14: Undertaking survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2011: http://nicedsu.org.uk/wp-content/uploads/2016/03/NICE-DSU-TSD-Survival-analysis.updated-March-2013.v2.pdf. Accessed 2021 Feb 17.
11.A network meta-analysis of first-line treatments in patients with malignant pleural mesothelioma. Technical report version 1.0 [CONFIDENTIAL sponsor's report]. In: Drug Reimbursement Review sponsor's submission: Opdivo+ Yervoy (nivolumab + ipilimumab), 10 mg/mL + 5 mg/mL and administration. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020.
12.van Meerbeeck JP, Gaafar R, Manegold C, et al. Randomized phase III study of cisplatin with or without raltitrexed in patients with malignant pleural mesothelioma: an intergroup study of the European Organisation for Research and Treatment of Cancer Lung Cancer Group and the National Cancer Institute of Canada. J Clin Oncol. 2005;23(28):6881-6889. PubMed
13.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
14.Lloyd A, van Hanswijck de Jonge P, Doyle S, Cornes P. Health state utility scores for cancer-related anemia through societal and patient valuations. Value Health. 2008;11(7):1178-1185. PubMed
15.DeltaPA. Ottawa (ON): IQVIA; 2020: https://www.iqvia.com/. Accessed 2021 Feb 17.
16.CADTH pan-Canadian Oncology Drug Review: Keytruda for non-squamous non-small cell lung cancer. (CADTH pCODR final economic guidance report). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10153PembroNSQ-NSCLC_fnEGR_NOREDACT-ABBREV_Post_31May2019_final.pdf. Accessed 2021 Feb 17.
17.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2021 Feb 17.
18.Bremner KE, Krahn MD, Warren JL, et al. An international comparison of costs of end-of-life care for advanced lung cancer patients using health administrative data. Palliat Med. 2015;29(10):918-928. PubMed
19.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2020; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Feb 17.
20.National Institute for Health Care and Excellence. NICE Home page. 2020; https://www.nice.org.uk/. Accessed 2020 Dec 01.
21.Pharmacoeconomic evaluation. In: Drug Reimbursement Review sponsor submission: Opdivo+ Yervoy (nivolumab + ipilimumab), 10 mg/mL + 5 mg/mL and administration. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020 Nov 13.
22.National Institute for Health Care and Excellence. Nintedanib for previously treated locally advanced, metastatic, or locally recurrent non-small-cell lung cancer. (Technology appraisal guidance TA347) 2015; https://www.nice.org.uk/guidance/ta347/chapter/1-Guidance. Accessed 2021 Feb 17.
23.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2021 Feb 17.
24.Yervoy (ipilimumab): 5 mg/mL intravenous infusion, 10 mL and 40 mL vials [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada Co; 2020 Nov 27: https://www.bms.com/assets/bms/ca/documents/productmonograph/YERVOY_EN_PM.pdf. Accessed 2021 Feb 17.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison for Unresectable Malignant Pleural Mesothelioma – First- Line Therapies
Treatment | Strength/ concentration | Form (vial size if single use) | Price ($) | Recommended dosage | Daily cost | 21-day course ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|---|
Nivolumab and ipilimumab | |||||||
Nivolumaba | 10 mg/mL | IV infusion 4 mL 10 mL | 782.2200 1,955.5600 | 3 mg/kg once every 2 weeks or 360 mg every 3 weeks | 307.30 335.24 | 6,453 7,040 | 8,604 9,387 |
Ipilimumaba | 5 mg/mL | Vial for IV infusion 10 mL | 5,800.0000 | 1 mg/kg once every 6 weeks | 276.19 | 5,800 | 7,733 |
Nivolumab + Ipilimumab | 583.49 to 611.43 | 12,253 to 12,840 | 16,337 to 17,120 | ||||
Pemetrexed and platinum-based chemotherapy | |||||||
Pemetrexed | 100 mg 1,000 mg | IV infusion | 429.0000 4,290.0000 | 500 mg/m2 every 3 weeks | 183.86 | 3,861 | 5,148 |
Cisplatin | 1 mg/mL | IV infusion 50 mL 100 mL | 135.0000 646.0000 | 75 mg/m2 every 3 weeks | 19.29 | 405 | 540 |
Carboplatin | 10 mg/mL | IV infusion 5 mL 45 mL 60 mL | 56.0000 600.0000 775.2000 | 400 mg/m2 every 4 weeks 550 mg every 3 weeks | 30.00 29.33 | 630 616 | 840 821 |
Pemetrexed + cisplatin or carboplatin | 203.15 to 213.86 | 4,266 to 4,491 | 5,688 to 5,988 | ||||
IV = IV.
Note: All prices are from IQVIA drug price database (accessed November 2020), unless otherwise indicated, and do not include dispensing fees. Dosing is based on Health Canada product monographs, unless otherwise indicated. For treatments using weight-based dosing, CADTH assumed 70 kg or 1.8 m2. No vial sharing is assumed.
aSponsor’s submitted price.
Table 9: CADTH Cost Comparison for Unresectable Malignant Pleural Mesothelioma – Alternatives to First-Line Therapies
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost | 21-day course ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|---|
Raltitrexed and platinum-based chemotherapy | |||||||
Raltitrexed | 2 mg | Powder for solution for IV infusion | 340.8500 | 3 mg/m2 every 3 weeks | 48.69 | 1,023 | 1,363 |
Cisplatin | 1 mg/mL | IV infusion 50 mL 100 mL | 135.0000 646.0000 | 75 mg/m2 every 3 weeks | 19.29 | 405 | 540 |
Carboplatin | 10 mg/mL | IV infusion 5 mL 45 mL 60 mL | 56.0000 600.0000 775.2000 | 400 mg/m2 every 4 weeks 550 mg every 3 weeks | 30.00 29.33 | 630 616 | 840 821 |
Raltitrexed + cisplatin/carboplatin | 67.98 to 78.69 | 1,428 to 1,653 | 1,903 to 2,203 | ||||
Other therapies | |||||||
Gemcitabinea | 1 g 2 g | Powder for IV solution | 270.0000 540.0000 | 1,000 to 1,250 mg/m2 day 1 and day 8 of every 3-week cycle | 46.29 to 57.86 | 972 to 1,215 | 1,296 to 1,620 |
Vinorelbinea | 10 mg/mL | IV infusion 1 mL | 80.0000 | 25 to 30 mg/m2 day 1 and day 8 of every 3-week cycle | 38.09 to 45.71 | 800 to 960 | 1,067 to 1,280 |
IV = IV.
Note: All prices are from IQVIA drug price database (accessed November 2020), unless otherwise indicated, and do not include dispensing fees. Dosing is based on Health Canada product monographs, unless otherwise indicated. For treatments using weight-based dosing, CADTH assumed 70 kg or 1.8 m2. No vial sharing is assumed.
aDosing provided by feedback from clinical experts.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Sponsor’s formulas for calculating vial sharing result in erroneous number of vials required per treatment |
Model structure is adequate for decision problem | Yes | |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Sponsor’s prices for chemotherapy did not align with publicly available sources in Canada (see key limitations) |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Figure 1: Sponsor's Model Structure
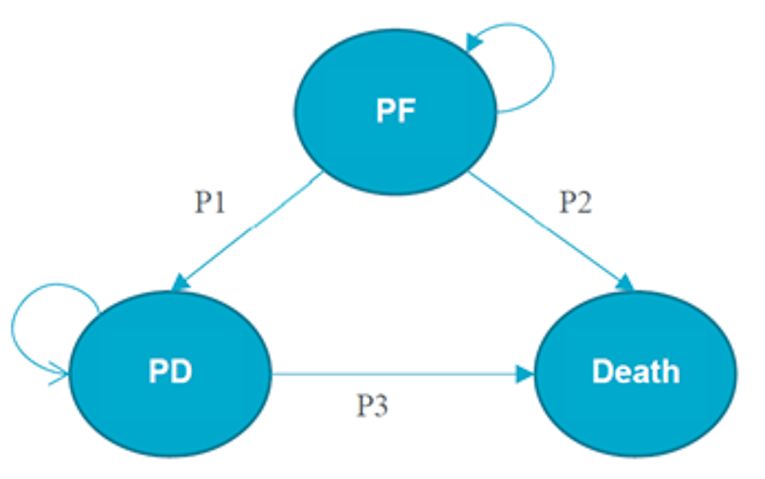
P1 = transition probability 1; P2 = transition probability 2; P3 = transition probability 3; PD = progressed disease; PF = progression-free.
Source: Sponsor’s pharmacoeconomic submission.21
Table 11: Distribution of Subsequent Therapies for Each First-Line Therapy
To | From | |||
|---|---|---|---|---|
Nivolumab plus ipilimumab | Pemetrexed with platinum-based chemotherapy | Raltitrexed with platinum-based chemotherapy | Average time on subsequent treatment (months) | |
Gemcitabine | 8.6% | 27.3% | 27.3% | 1.7 |
Vinorelbine | 5.2% | 15.2% | 15.2% | 1.7 |
Pemetrexed | 41.7% | 29.1% | 29.1% | 1.7 |
Cisplatin | 13.8% | 4.8% | 4.8% | 1.7 |
Carboplatin | 30.7% | 23.6% | 23.6% | 1.7 |
Source: Sponsor’s pharmacoeconomic submission.11
Table 12: Sponsor’s Scenario Results
Scenario | Sponsor’s value | Scenario value | Nivolumab plus ipilimumab sequential ICER ($ per QALY) |
|---|---|---|---|
Lower discount rate | 1.5% | 0% | $306,327 vs. pemetrexed with platinum-based chemotherapy (raltitrexed was extendedly dominated) |
Higher discount rate | 1.5% | 3% | $351,130 vs. raltitrexed with platinum-based chemotherapy |
Flat dose of nivolumab | 3 mg/kg every 2 weeks | 360 mg once every 3 weeks | $333,465 vs. raltitrexed with platinum-based chemotherapy |
Alternative OS curves | Dependent log-logistic for all treatment arms | Independent log-logistic for all treatment arms | $229,971 vs. raltitrexed with platinum-based chemotherapy |
Treatment-specific utilities | Utility defined by health state, equal across treatments (progression-free: 0.79, progressed disease: 0.70) | Treatment-specific utilities; for progression-free and progressed disease respectively, nivolumab plus ipilimumab: 0.79, 0.72, pemetrexed with platinum-based chemotherapy and raltitrexed with platinum-based chemotherapy: 0.78, 0.67) | $303,553 vs. raltitrexed with platinum-based chemotherapy |
ICER = Incremental cost-effectiveness ratio; QALY = quality-adjusted life-year
Source: Sponsor’s pharmacoeconomic submission.11
Figure 2: Sponsor’s Cost-Effectiveness Acceptability Curve
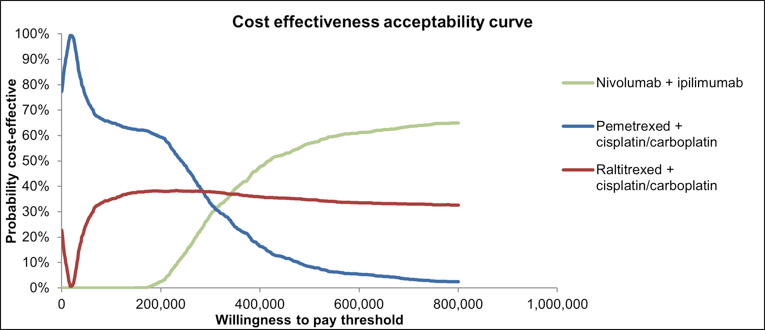
Source: Sponsor’s submitted economic model.21
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Nivolumab plus ipilimumab | Pemetrexed with platinum-based chemotherapy | Incremental |
|---|---|---|---|
Discounted life-years | |||
Total life-years | 2.54 | 2.07 | 0.47 |
Progression-free disease | 1.46 | 0.87 | 0.59 |
Progressed disease | 1.07 | 1.20 | −0.13 |
Discounted QALYs | |||
Total QALYs | 1.90 | 1.48 | 0.42 |
Progression-free disease | 1.15 | 0.68 | 0.47 |
Progressed disease | 0.75 | 0.84 | −0.09 |
Discounted costs | |||
Total costs ($) | 202,176 | 76,090 | 126,086 |
Progression-free disease costs ($) | 17,417 | 10,296 | 7,121 |
Progressed-disease costs ($) | 15,856 | 17,789 | −1,933 |
Drug acquisition costs ($) | 148,156 | 27,097 | 121,059 |
Drug administration ($) | 2,511 | 383 | 2,128 |
Monitoring costs ($) | 45 | 18 | 27 |
Adverse event management costs ($) | 336 | 2,871 | −2,535 |
Subsequent treatment costs ($) | 2,443 | 2,061 | 382 |
End-of-life costs ($) | 15,412 | 15,576 | −164 |
ICER ($ per QALY) | 300,921 | ||
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analyses
Table 14: CADTH Sensitivity and Scenario Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption | Sensitivity/scenario value |
|---|---|---|---|
1. Distribution informing nivolumab plus ipilimumab and pemetrexed with chemotherapy OS curves | Log-logistic distribution | Log-logistic distribution | Gamma distribution |
2. Sponsor’s chemotherapy prices | Cisplatin: 100 mL vial (1 mg/mL): $19.00 Carboplatin: 15 mL vial (10 mg/mL): $18.80 | Cisplatin: 50 mL vial (1 mg/mL): $135.00 Carboplatin: 5mL vial (10 mg/mL): $56.00 | Cisplatin: 100 mL vial (1 mg/mL): $19.00 Carboplatin: 15 mL vial (10 mg/mL): $18.80 |
3. Flat dose of nivolumab | Weight-based dosing (3 mg/kg every 2 weeks) | Weight-based dosing (3 mg/kg every 2 weeks) | Flat dose of nivolumab (360 mg every 3 weeks) |
4. Non-epithelioid patient subgroup | All-comers population | All-comers population | Non-epithelioid patient subgroup |
5. Epithelioid patient subgroup | All-comers population | All-comers population | Epithelioid patient subgroup |
6. Near-perfect vial sharing for nivolumab, ipilimumab, and all chemotherapies | 95% vial sharing for nivolumab and ipilimumab, no vial sharing for chemotherapies | No vial sharing for all drugs | Vial sharing for nivolumab, ipilimumab, and all chemotherapies |
Table 15: CADTH Sensitivity and Scenario Analysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
CADTH base case | Pemetrexed plus cisplatin or carboplatin | 76,090 | 1.481 | Reference |
Nivolumab plus ipilimumab | 202,176 | 1.900 | 300,921 | |
1. Distribution informing OS curves | Pemetrexed plus cisplatin or carboplatin | 69,014 | 1.127 | Reference |
Nivolumab plus ipilimumab | 195,085 | 1.477 | 360,203 | |
2. Sponsor’s chemotherapy prices | Pemetrexed plus cisplatin or carboplatin | 87,967 | 1.478 | Reference |
Nivolumab plus ipilimumab | 219,145 | 1.896 | 313,823 | |
3. Flat dose of nivolumab | Pemetrexed plus cisplatin or carboplatin | 76,025 | 1.480 | Reference |
Nivolumab plus ipilimumab | 209,543 | 1.904 | 314,901 | |
4. Vial sharing for nivolumab, ipilimumab, and all chemotherapies | Pemetrexed plus cisplatin or carboplatin | 73,819 | 1.478 | Reference |
Nivolumab plus ipilimumab | 182,087 | 1.904 | 253,794 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exploratory Analyses
Table 16: CADTH Exploratory Analysis Results – Subgroup by Histology
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
CADTH base case | Pemetrexed plus cisplatin or carboplatin | 76,090 | 1.481 | Reference |
Nivolumab plus ipilimumab | 202,176 | 1.900 | 300,921 | |
Epithelioid subgroup | Pemetrexed plus cisplatin or carboplatin | 79,084 | 1.648 | Reference |
Nivolumab plus ipilimumab | 203,009 | 1.878 | 538,804 | |
Non-epithelioid subgroup | Pemetrexed plus cisplatin or carboplatin | 66,860 | 0.974 | Reference |
Nivolumab plus ipilimumab | 199,719 | 1.808 | 159,303 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Business Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the Business Impact Analysis |
|---|
|
Summary of Sponsor’s Business Impact Analysis
The sponsor’s submitted budget impact analysis (BIA) investigated the adoption of nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable MPM. The sponsor included pemetrexed with platinum-based chemotherapy and raltitrexed with platinum-based chemotherapy as comparators; however, raltitrexed was assumed to have a 0% market share. The BIA was undertaken from the public payer perspective for the Canadian setting using a population-based approach over a 3-year projected time horizon (2021 to 2023) as well as a baseline year (2020). The BIA investigates the Canadian population, excluding Quebec. Key inputs to the BIA are documented in Table 17, and the following key assumptions were made:
||||of eligible patients will enter clinical trials in both the reference and new drug scenario as opposed to receiving standard first-line treatment.The costs of subsequent treatments were included in the sponsor’s base case.
The monitoring costs and costs of administration relating to adverse events were not included in the sponsor’s base case.
The sponsor assumed near-perfect vial sharing for nivolumab and ipilimumab (only 5% of each vial wasted), while none of the comparators or subsequent treatments experienced vial sharing.
Nivolumab dosage is based on a weight-based approach.
Subsequent therapy options and the proportion of patients from each treatment arm that would receive each subsequent treatment option was sourced from the CheckMate 743 trial and expert opinion.6 A breakdown of subsequent therapies is presented in Appendix 3, Table 11.
The BIA was found to be sensitive to patients’ body weight, treatment duration, and vial sharing. The BIA does not include a subgroup analysis by histology.
Figure 3: Sponsor's Estimation of the Size of the Eligible Population in Year 1
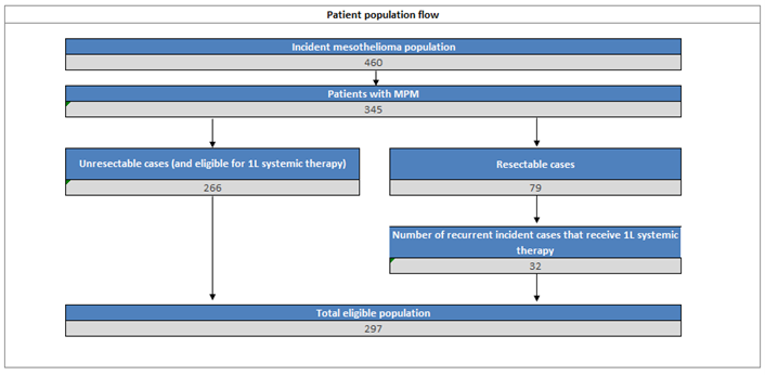
MPM: malignant pleural mesothelioma; 1L: first-line therapy
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) |
|---|---|
Target population | |
Incident mesothelioma population | 460/465/470 |
Proportion of mesothelioma patients with MPM | 75% |
Proportion of MPM patients with unresectable disease | 77% |
Proportion of unresectable MPM patients eligible for first-line treatment | 100% |
Number of patients eligible for drug under review Year 1/year 2/year 3 | 297/301/304 (*Assuming 1.1% annual growth in case numbers) |
Market uptake (3 years) | |
Uptake (reference scenario) Pemetrexed with cisplatin or carboplatin Clinical trials |
|
Uptake (new drug scenario) Nivolumab plus ipilimumab Pemetrexed with cisplatin or carboplatin Clinical trials |
|
Cost of treatmenta (per patient) | |
Annual cost of treatments per patient Nivolumab plus ipilimumabb Pemetrexed with cisplatin/carboplatin Clinical Trials Cost of subsequent therapies Nivolumab plus ipilimumab subsequent treatment Pemetrexed with cisplatin or carboplatin subsequent treatment | $111,203 $3,339 $0 $503 $584 |
Proportion of patients on each subsequent therapy option | See Table 19 |
MPM = malignant pleural mesothelioma.
aTreatment duration was sourced from the mean treatment duration of the CheckMate 743 trial.5
bAssumes vial sharing with 5% wastage.
In the new drug scenario, the sponsor assumes that nivolumab plus ipilimumab enters the market with a 60% market share that steadily increases by |||||| in years 2 and 3. This market share comes solely from pemetrexed with cisplatin/carboplatin.
Summary of the Sponsor’s BIA Results
The 3-year budget impact of nivolumab plus ipilimumab for MPM is $63,982,324. The annual budget impact was $19,166,286 in year 1, $21,960,730 in year 2, and $22,855,307 in year 3. Nivolumab plus ipilimumab had a considerably higher price per cycle and a longer mean duration on treatment than pemetrexed with platinum-based chemotherapy.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Clinical trial participation is not a relevant comparator: The sponsor considered participation in a clinical trial as a relevant comparator in the BIA and assumed
||||||of patients would enter clinical trials as opposed to receiving nivolumab and ipilimumab or pemetrexed with platinum-based chemotherapy. The inclusion of investigational therapy (i.e., participation in clinical trials) may be problematic as patients entering trials are not receiving approved therapies for the same indication as nivolumab plus ipilimumab. Additionally, the inclusion of clinical trials as a comparator does not align with the comparators included in the pharmacoeconomic evaluation submitted by the sponsor. This underestimates the potential market size and uptake, underestimating the potential budget impact associated with nivolumab plus ipilimumab.The clinical trial market share was distributed evenly between nivolumab plus ipilimumab and pemetrexed and platinum-based chemotherapy in the CADTH reanalyses.
The proportion of patients with resectable MPM identified by the sponsor is not reflective of clinical expert expectations: The sponsor sourced the proportion of patients with resectable versus unresectable disease from SEER data (23% resectable).8 These values strongly differ from expectations of the clinical experts consulted by CADTH for this review. The clinical experts consulted by CADTH indicated that 5% would be a more accurate estimate of the proportion of MPM cases that are resectable in Canada. The proportions chosen by the sponsor likely underestimate the eligible population size and thus nivolumab plus ipilimumab’s budgetary impact.
The proportion of patients with resectable disease was updated to 5% in the CADTH reanalysis to align with expectations of Canadian clinical experts. CADTH conducted a scenario analysis using the sponsor’s proportion of resectable cases.
Uncertainty in the extent of drug wastage modelled for nivolumab and ipilimumab: In their base case, the sponsor assumed that comparator treatments (pemetrexed, carboplatin, cisplatin) would not be shared. However, near-perfect vial sharing was assumed for nivolumab and ipilimumab. According to their respective draft product monographs, nivolumab and ipilimumab are single-use vials that expire after use. Though larger cancer-treatment centres maybe be able to accommodate some vial sharing due to their volume of patients, vial sharing may not be near-perfect and would also be less likely in lower in smaller cancer-treatment centres. The assumed near-perfect vial sharing underestimated the drug acquisition costs associated with nivolumab and ipilimumab, biasing results in its favour.
Vial sharing was not considered in the CADTH base case to align with the draft product monographs. Perfect vial sharing was considered in scenario analyses.
Inaccurate pricing for comparator chemotherapy: The prices of certain chemotherapy drugs used in the sponsor’s submitted model were sourced from previous CADTH reports and did not align with costs reported in the IQVIA Delta PA database. The costs of pemetrexed, cisplatin, carboplatin, and subsequent chemotherapies were all underestimated in the sponsor’s model. The sponsor’s model priced a 10 mL vial (1mg/mL) of cisplatin at $9.50, a 60mL vial (10 mg/mL) of carboplatin at $12.92, a 50mg vial of pemetrexed at $41.50, a 1 g vial of gemcitabine at $220.00, and a 1 mL vial (10 mg/mL) of vinorelbine at $6.80. The IQVIA drug price database priced a 50 mL vial (1 mg/mL) vial of cisplatin at $135.00, a 5mL vial (10 mg/mL) vial of carboplatin at $56.00, a 100 mg vial of pemetrexed at $429.00, a 1 g vial of gemcitabine at $270.00, and a 1 mL vial (10 mg/mL) of vinorelbine at $80.00. The inaccurate costs of chemotherapy led to the cost of pemetrexed-based therapy being underestimated, overestimating the incremental costs associated with nivolumab plus ipilimumab and biasing results against nivolumab plus ipilimumab.
The CADTH base case was informed by the prices identified from the IQVIA drug price database.11
CADTH Reanalyses of the BIA
The revisions made by CADTH to the sponsor’s submitted budget impact analysis are presented in Table 19. The results of the stepwise reanalyses are presented in Table 20 and a more detailed breakdown is presented in Table 21. The submitted analysis is based on the publicly available prices of the comparator treatments.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case (if not applicable, state “none”)b | ||
None | None | None |
Changes to derive the CADTH base case | ||
1. Market share of clinical | The sponsor assumed | CADTH distributed clinical trial patients evenly across treatments; no patients were assumed to enter clinical trials |
2. Proportion of patients who have resectable disease | 23% of MPM cases are resectable | 5% of MPM cases are resectable |
3. Vial sharing | The sponsor assumed near-perfect vial sharing for nivolumab and ipilimumab but no vial sharing for pemetrexed, cisplatin, carboplatin, or subsequent treatments | CADTH assumed no vial sharing for all drugs |
4. Price of chemotherapy | Cisplatin: 100 mL vial (1 mg/mL): $19.00 Carboplatin: 15 mL vial (10 mg/mL): $18.80 Pemetrexed: 50 mg vial: $41.50 Gemcitabine: 20 mL (10 mg/mL) vial: $44.00 Vinorelbine: 1 mL (10 mg/mL) vial: $6.80 | Cisplatin: 50 mL vial (1 mg/mL): $135.00 Carboplatin: 60 mL vial (10 mg/mL): $56.00 Pemetrexed: 100 mg vial: $429.00 Gemcitabine: 1 g vial: $270.00 Vinorelbine: 1 mL (10 mg/mL) vial: $80.00 |
CADTH base case | 1 + 2 + 3 + 4 | |
MPM = malignant pleural mesothelioma.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses) that are not identified as limitations.
Table 20: Summary of the CADTH Reanalyses of the Business Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 63,982,324 |
CADTH reanalysis 1 – Market Share | 68,826,796 |
CADTH reanalysis 2 – Proportion of patients with resectable disease | 71,998,670 |
CADTH reanalysis 3 – Vial sharing | 70,228,940 |
CADTH reanalysis 4 – Price of comparator chemotherapy | 53,916,189 |
CADTH base case | 72,959,111 |
CADTH also conducted additional scenario analyses to address uncertainty surrounding the proportion of patients with resectable disease, the cost of comparator chemotherapies, the proportion of patients with unresectable MPM eligible for systemic therapy, and the market share of nivolumab plus ipilimumab, summarized in Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Table 21: Detailed Breakdown of the CADTH Reanalyses of the Business Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 1,136,825 | 1,149,330 | 1,161,972 | 1,174,754 | 4,622,880 |
New drug | 1,136,825 | 20,315,616 | 23,122,703 | 24,030,061 | 68,605,204 | |
Budget impact | 0 | 19,166,286 | 21,960,730 | 22,855,307 | 63,982,324 | |
CADTH base case | Reference | 7,614,834 | 7,698,598 | 7,783,282 | 7,868,898 | 30,965,612 |
New drug | 7,614,834 | 29,708,699 | 32,774,229 | 33,826,960 | 103,924,723 | |
Budget impact | 0 | 22,010,102 | 24,990,947 | 25,958,062 | 72,959,111 | |
CADTH scenario analysis: nivolumab plus ipilimumab experiences a 10% increase in market share | Reference | 7,612,660 | 7,696,399 | 7,781,060 | 7,866,651 | 30,956,770 |
New drug | 7,612,660 | 33,089,226 | 36,191,570 | 37,281,799 | 114,175,256 | |
Budget impact | 0 | 25,392,827 | 28,410,511 | 29,415,147 | 83,218,485 | |
CADTH scenario analysis: nivolumab plus ipilimumab experiences a 10% decrease in market share | Reference | 7,614,834 | 7,698,598 | 7,783,282 | 7,868,898 | 30,965,612 |
New drug | 7,614,834 | 26,322,530 | 29,350,811 | 30,365,885 | 93,654,061 | |
Budget impact | 0 | 18,623,932 | 21,567,529 | 22,496,987 | 62,688,449 | |
CADTH scenario analysis: Sponsor’s proportion of patients who have resectable disease | Reference | 6,766,997 | 6,841,434 | 6,916,690 | 6,992,773 | 27,517,894 |
New drug | 6,766,997 | 26,400,927 | 29,125,139 | 30,060,660 | 92,353,723 | |
Budget impact | 0 | 19,559,492 | 22,208,450 | 23,067,886 | 64,835,828 | |
CADTH scenario analysis: vial sharing for nivolumab, ipilimumab, and all first-line chemotherapies | Reference | 7,040,419 | 7,117,863 | 7,196,160 | 7,275,318 | 28,629,760 |
New drug | 7,040,419 | 25,974,867 | 28,606,982 | 29,514,710 | 91,136,978 | |
Budget impact | 0 | 18,857,004 | 21,410,822 | 22,239,392 | 62,507,218 | |
CADTH scenario analysis: using sponsor’s chemotherapy prices | Reference | 1,421,587 | 1,437,224 | 1,453,034 | 1,469,017 | 5,780,861 |
New drug | 1,421,587 | 27,123,132 | 30,617,603 | 31,762,215 | 90,924,537 | |
Budget impact | 0 | 25,972,256 | 29,489,699 | 30,630,910 | 86,092,866 | |
CADTH scenario analysis: 50% of patients eligible to receive systemic therapy | Reference | 3,885,921 | 3,928,666 | 3,971,881 | 4,015,572 | 15,802,039 |
New drug | 3,885,921 | 15,160,625 | 16,724,993 | 17,262,212 | 53,033,750 | |
Budget impact | 0 | 11,231,959 | 12,753,112 | 13,246,640 | 37,231,711 | |
CADTH scenario analysis: 72% price reduction of nivolumab and ipilimumab a | Reference | 7,614,834 | 7,698,598 | 7,783,282 | 7,868,898 | 30,965,612 |
New drug | 7,614,834 | 10,621,056 | 11,101,532 | 11,315,559 | 40,652,981 | |
Budget impact | 0 | 2,922,459 | 3,318,249 | 3,446,661 | 9,687,369 |
aThe reduction in price necessary in the cost-effectiveness model for nivolumab plus ipilimumab to be considered cost-effective at a threshold of $50,000 per QALY.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.