CADTH Reimbursement Review
Durvalumab (Imfinzi)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Extensive-stage small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
CD80
cluster of differentiation 80
CI
confidence interval
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EP
etoposide-platinum
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ES
extensive-stage
HR
hazard ratio
HRQoL
health-related quality of life
ITT
intention to treat
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
MID
minimal important difference
MMRM
mixed model for repeated measures
NSCLC
non–small cell lung cancer
OR
odds ratio
ORR
objective response rate
OS
overall survival
PCI
prophylactic cranial irradiation
PD
progressive disease
PD-1
programmed cell death protein 1
PD-L1
programmed cell death ligand 1
PFS
progression-free survival
PRO
patient-reported outcome
QLQ-LC13
13-item Lung Cancer Quality of Life Questionnaire
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumors
SAE
serious adverse event
SCLC
small cell lung cancer
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Durvalumab (Imfinzi) concentrate for solution for infusion, 50 mg/mL, IV |
Indication | First-line treatment of adult patients with extensive-stage small cell lung cancer, in combination with etoposide and either carboplatin or cisplatin |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | September 21, 2020 |
Sponsor | AstraZeneca Canada Inc. |
NOC = Notice of Compliance.
Introduction
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in Canada.1 Small cell lung cancer (SCLC) accounts for 12% to 15% of lung cancer cases.2,3 Small cell lung cancer is characterized by a rapid growth rate, early metastasis to regional lymph nodes and/or distant sites, and an initial sensitivity to chemotherapy and radiotherapy.4 In Canada, the 5-year predicted net survival for SCLC is 7%.1 Patients with tumour involvement that is more widespread in the lungs, and who may be diagnosed with malignant pleural or pericardial effusions or hematogenous metastases, are classified as having extensive-stage (ES) SCLC.4 Approximately two-thirds of SCLC patients have ES disease.3 According to the clinical experts consulted by CADTH, patients with ES-SCLC present as severely ill. A diagnosis of SCLC is made using a standard pathologic assessment of a tissue biopsy. Staging to determine whether the patient has ES-SCLC is done with radiology testing (e.g., CT, PET scan, bone scan, or brain MRI). The experts noted that patients who are diagnosed with SCLC are seen urgently by medical oncologists. All patients with ES-SCLC have a poor prognosis.
The clinical experts consulted by CADTH noted that current treatment options for ES-SCLC are limited and have not changed in 30 years. The vast majority of patients receive etoposide with either cisplatin or carboplatin (etoposide-platinum [EP] therapy) for 4 to 6 cycles as a first-line therapy. A small number of patients who are not candidates for platinum therapy or do not want to receive IV systemic therapy may be treated with oral etoposide. Although there is a high initial response rate to first-line treatment with EP therapy, most patients relapse within months. Patients derive limited benefit from second-line chemotherapy, and many patients are not well enough to receive second-line chemotherapy after relapse.
Durvalumab is a humanized immunoglobulin G1 (IgG1) kappa monoclonal antibody that selectively blocks the interaction of programmed cell death ligand 1 (PD-L1) with programmed cell death protein 1 (PD-1) and cluster of differentiation 80 (CD80).5 On September 21, 2020, durvalumab was approved by Health Canada for the first-line treatment of patients with ES-SCLC in combination with etoposide and either carboplatin or cisplatin.5 The reimbursement request for durvalumab by the sponsor is consistent with the Health Canada–approved indication. Durvalumab is available as a single-use vial and is administered as an IV infusion over 60 minutes.5 For the treatment of ES-SCLC in patients with a body weight of more than 30 kg, the recommended dosage is 1,500 mg in combination with etoposide and either carboplatin or cisplatin every 3 weeks for 4 cycles, followed by 1,500 mg every 4 weeks as monotherapy until disease progression or unacceptable toxicity. For patients with a body weight less than or equal to 30 kg, the recommended dosage is 20 mg/kg in combination with etoposide and either carboplatin or cisplatin every 3 weeks for 4 cycles, followed by 20 mg/kg every 4 weeks as monotherapy until disease progression or unacceptable toxicity.
The objective of the report is to perform a systematic review of the beneficial and harmful effects of durvalumab in combination with etoposide and either carboplatin or cisplatin for the first-line treatment of patients with ES-SCLC.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from 2 clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient advocacy groups provide input regarding patients’ experiences, values, and preferences related to SCLC and its treatment: Lung Cancer Canada (LCC) and the Lung Health Foundation (LHF), previously known as the Ontario Lung Association. The LCC group is a registered national charity that focuses exclusively on lung cancer in Canada. The LHF is a registered charity that assists and empowers people living with or caring for others with lung disease, provides programs and services to patients and health care providers, invests in health research, and advocates for better policies on lung health.
According to the patient input received, a diagnosis of lung cancer and the subsequent treatment has a major impact on the life of the patient and their families. Many patients report issues with work, day-to-day chores, and socialization. Caregivers may need to take time off work to provide care, which affects work productivity and finances, and can cause mental stress. The emotional and physical toll during and after treatment may affect caregivers’ ability to fulfill their role in the family and at work and their ability to participate in activities they enjoy.
Key outcomes identified by the patient advocacy groups as important to patients include the following: control the cancer, improve symptoms, delay deterioration, have manageable side effects, be effective on the central nervous system, delay progression, extend survival with a good quality of life, and provide longer-lasting and durable treatment.
The patient groups reported poor numbers in terms of survival for ES-SCLC and a lack of treatment options. According to the patient input received, treatment for SCLC has not changed in the past 30 years, representing a significant unmet need.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Input was provided by 2 clinical specialists with expertise in the diagnosis and management of ES-SCLC. The clinical experts consulted by CADTH indicated that there is a significant unmet need for a systemic therapy that can extend response to first-line treatment, prolong survival, and preserve the symptom and quality-of-life benefits.
The clinical experts indicated that they would administer durvalumab concurrently with first-line EP therapy, then as single-drug maintenance therapy. The clinical experts would offer durvalumab to all patients for whom EP therapy is planned, except for patients who have contraindications to immunotherapy (e.g., autoimmune disease, organ transplant recipient). The clinical experts stated that there are no known patient subgroups that would be more likely to benefit from durvalumab. No biomarkers or patient characteristics have been identified that can predict which patients are more likely to respond to durvalumab.
The clinical experts noted that treatment response in SCLC is assessed by physical examination, history of symptom burden, and serial radiography. The experts agreed that CT scans are usually made at the completion of 4 to 6 cycles of EP and then every 8 weeks to 12 weeks. Chest X-rays may also be taken more frequently between CT scans. The clinical experts agreed that they would discontinue durvalumab if a patient experienced disease progression, intolerable adverse events (AEs) or serious adverse events (SAEs), or the patient wishes to stop treatment.
The clinical experts consulted by CADTH emphasized that current treatment options for ES-SCLC are limited and have not changed in 30 years. The experts indicated that prolonged overall survival (OS) would be a clinically meaningful response to treatment. Delayed disease progression, reduced symptom burden, and improved Eastern Cooperative Oncology Group Performance Status (ECOG PS) are also clinically meaningful.
Clinician Group Input
Clinician group input was provided by Lung Cancer Canada and the Ontario Health Lung and Cancer Drug Advisory Committee. The views of the clinician groups were consistent with those of the clinical experts consulted by CADTH. Similar to the clinical experts consulted by the CADTH, the clinician groups reported that any improvement in the percentage of patients living beyond 18 months to 24 months is considered meaningful.
Drug Program Input
In response to the Drug Plan’s questions about administering durvalumab to patients in Canada, the clinical experts consulted by CADTH generally indicated that they would administer durvalumab according to the pivotal CASPIAN trial design and the product monograph. In response to questions regarding when to stop maintenance therapy with durvalumab, the clinical experts indicated that clinicians prefer to continue durvalumab maintenance therapy until a patient experiences disease progression, intolerable AEs or SAEs, or the patient wishes to stop treatment. The clinical experts indicated that it would be unlikely that patients would have difficulty tolerating 4 cycles of EP therapy when initiating treatment with durvalumab. If durvalumab was temporarily stopped due to an immune-mediated AE, the clinical experts agreed that it would be reasonable to restart durvalumab after the event had resolved. The clinical experts were not aware of evidence to support weight-based dosing of durvalumab in patients with ES-SCLC.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The CASPIAN trial was an international multi-centre, phase III, open-label, randomized controlled trial (RCT) conducted to investigate the efficacy and safety of durvalumab, with or without tremelimumab, in combination with EP compared with EP alone as a first-line treatment regimen in adult patients with ES-SCLC (Figure 2). A total of 805 patients were randomized in a 1:1:1 ratio to 3 treatment arms: durvalumab with tremelimumab in combination with etoposide and either carboplatin or cisplatin (durvalumab + tremelimumab + EP), durvalumab in combination with etoposide and either carboplatin or cisplatin (durvalumab + EP), and etoposide and either carboplatin or cisplatin alone (EP). In the experimental treatment arms, patients received durvalumab, with or without tremelimumab, administered concurrently with first-line EP chemotherapy every 3 weeks for 4 cycles. After chemotherapy was completed, durvalumab was administered every 4 weeks as monotherapy until progressive disease (PD) was recorded. In the control arm, patients received 4 to 6 cycles of EP every 3 weeks and prophylactic cranial irradiation at the investigator's discretion. The type of platinum-based chemotherapy (cisplatin or carboplatin) used was the investigator’s choice. Randomization was stratified by the platinum-based chemotherapy planned for the first treatment cycle. The primary outcome was OS. Secondary outcomes included progression-free survival (PFS), objective response rate (ORR), duration of response (DOR), and change in health-related quality of life (HRQoL) and symptoms as measured by 2 European Organisation for Research and Treatment of Cancer instruments: the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) version 3.0 and the 13-item Lung Cancer Quality of Life Questionnaire (QLQ-LC13).
Data for the durvalumab + tremelimumab + EP arm of the CASPIAN trial will not be presented in the systematic review because tremelimumab is not approved in Canada and the combination is not aligned with the Health Canada product monograph for durvalumab.
The CASPIAN trial enrolled adults with histologically or cytologically confirmed ES-SCLC who were suitable for platinum-based chemotherapy as first-line treatment. Brain metastases at baseline were allowed in the case of asymptomatic or treated and stable patients. Enrolment was limited to patients with an ECOG PS of 0 or 1. Most patients were male (71.6%), White (82.6%) smokers (93.5%) with a small cell carcinoma (combined) histology type (84.1%) and an ECOG PS of 1 (63.0%). The mean age of all patients was 62.6 years. Baseline characteristics were generally well balanced between the durvalumab + EP arm and the EP arm. A total of 7 patients (0.9%) had received previous chemotherapy and 27 (3.4%) had received previous radiotherapy.
A pre-specified interim analysis was planned for after approximately 318 OS events occurred between the durvalumab + EP and EP-alone arms (60% maturity).6 The interim analysis had a data cut-off date of March 11, 2019, at which point the OS data had reached 63% maturity (336 OS events from 537 patients) in the durvalumab + EP and EP-alone arms.6 The primary analysis of OS was planned to be carried out when approximately 425 OS events (80% maturity) were observed across the durvalumab + tremelimumab + EP arm and the EP-alone arm, and the durvalumab + EP arm and the EP-alone arm. The final analysis was conducted with a data cut-off date of January 27, 2020, at which point the OS data had reached 82% maturity (441 events from 537 patients) in the durvalumab + EP arm and the EP-alone arm.7
Efficacy Results
Efficacy results from the CASPIAN trial are summarized in Table 2.
The CASPIAN trial met its primary end point of OS at the pre-specified interim analysis (data cut-off date of March 11, 2019). Median OS was 13.0 months (95% confidence interval [CI], 11.5 to 14.8) in the durvalumab + EP arm compared to 10.3 months (95% CI, 9.3 to 11.2) in the EP arm (hazard ratio [HR] = 0.73; 95% CI, 0.59 to 0.91; P = 0.0047). There was a delay of approximately 6 months in separation of the Kaplan–Meier curves, and the associated log-log plot showed some evidence of non-proportionality of hazards. The post hoc Kaplan–Meier estimate of landmark OS at 12 months was 53.7% (95% CI, 47.4 to 59.5) in the durvalumab + EP arm compared to 39.8% (95% CI, 33.7 to 45.8) in the EP-alone arm. The pre-specified, exploratory subgroup analysis of OS showed that the treatment effect was consistent with the primary analysis across the patient subgroups of smoking status, baseline ECOG PS, and brain metastases at baseline.
As of the final analysis, the median OS was 12.9 months (95% CI, 11.3 to 14.7) in the durvalumab + EP arm compared to 10.5 months (95% CI, 9.3 to 11.2) months in the EP-alone arm (HR = 0.75; 95% CI, 0.625 to 0.910; nominal P = 0.0032). Kaplan–Meier curves are provided in Figure 5. The post hoc Kaplan–Meier estimate of landmark OS at 18 months was 32.0% (95% CI, 26.5 to 37.7) in the durvalumab + EP arm compared to 24.8% (95% CI, 19.7 to 30.1) in the EP-alone arm. The post hoc Kaplan–Meier estimate of landmark OS at 24 months was 22.2% (95% CI, 17.3 to 27.5) in the durvalumab + EP arm versus 14.4% (95% CI, 10.3 to 19.2) in the EP-alone arm.
As of the interim analysis, median PFS was 5.1 months (95% CI, 4.7 to 6.2) in the durvalumab + EP arm and 5.4 months (95% CI, 4.8 to 6.2) in the EP arm (HR = 0.78; 95% CI, 0.645 to 0.936; nominal P = 0.0078). There was a delay of approximately 6 months in separation of the curves, and the associated log-log plot showed some evidence of non-proportionality of hazards. Results from the pre-specified exploratory subgroup analysis of PFS showed that the treatment effect on PFS was consistent with the primary analysis across the patient subgroups of smoking status, baseline ECOG PS, and brain metastases at baseline.
As of the final analysis, median PFS was 5.1 months (95% CI, 4.7 to 6.2) in the durvalumab + EP arm and 5.4 months (95% CI, 4.8 to 6.2) in the EP-alone arm (HR = 0.80; 95% CI, 0.665 to 0.959; nominal P = 0.0157). The post hoc Kaplan–Meier estimate of landmark PFS at 18 months was 13.9% (95% CI, 10.0 to 18.4) in the durvalumab + EP arm compared to 3.4% (95% CI, 1.6 to 6.4) in the EP-alone arm. The landmark PFS at 24 months was 11.0% (95% CI, 7.5 to 15.2) in the durvalumab + EP arm versus 2.9% (95% CI, 1.2 to 5.8) in the EP-alone arm. The unconfirmed ORR was 79.5% and 70.6% in the durvalumab + EP and EP-alone arms, respectively (odds ratio [OR] = 1.61; 95% CI, 1.086 to 2.401; nominal P = 0.0177). The confirmed ORR was 67.9% and 58.0% in the durvalumab + EP and EP-alone arms, respectively (OR = 1.53; 95% CI, 1.078 to 2.185; nominal P = 0.0173). Duration of response was calculated post hoc in the subset of patients who had a confirmed response. At both the interim and final analyses, the Kaplan–Meier estimate of median confirmed DOR was 5.1 months (95% CI, 4.9 to 5.3) in the durvalumab + EP arm and 5.1 months (95% CI, 4.8 to 5.3) in the EP arm. The Kaplan–Meier estimates of the percentage of patients remaining in confirmed response at 24 months were 13.5% (95% CI, not reported) and 3.9% (95% CI, not reported) in the durvalumab + EP and EP-alone arms, respectively.
Health-related quality of life and symptoms assessed by the EORTC QLQ-C30 and QLQ-L13 scales were evaluated at the interim analysis.8 The EORTC QLQ-C30, which evaluates the quality of life of patients with cancer participating in clinical trials, consists of 5 functional scales, 3 symptom scales, and 6 single items. This instrument also includes global health status and overall quality of life. A higher score on a functional scale corresponds to a higher level of function, while a higher score in the symptom scale corresponds to a higher burden of symptoms.9 The QLQ-LC13 is a lung cancer–specific module that consists of lung cancer–related symptoms and treatment side effects.8
Median time to deterioration in global health status/quality of life was 8.4 months (95% CI, 7.3 to 11.5) in the durvalumab + EP arm compared to 7.2 months (95% CI, 6.3 to 9.0) in the EP arm (HR = 0.81; 95% CI, 0.626 to 1.054; nominal P = 0.1166). Time to deterioration analysis suggested that the addition of durvalumab to EP may be beneficial for function scales (physical, role, emotional, cognitive, and social) and the symptoms of dyspnea, insomnia, appetite loss, constipation, diarrhea, hemoptysis, chest pain, arm and/or shoulder pain, and other pain compared to EP alone.
The results from the mixed model for repeated measures (MMRM) analysis of EORTC QLQ-C30 and QLQ-LC13 key symptoms from baseline to PD or 12 months showed a statistically significant difference in appetite loss in favour of durvalumab + EP. The adjusted mean change from baseline in appetite loss score was −12.7 points in the durvalumab + EP arm, which is greater than the minimal important difference (MID), and the estimated difference between treatment arms was −4.5 points (95% CI, −9.04 to −0.04; P = 0.009). No statistically significant differences between treatment arms were observed for the symptoms of fatigue, cough, dyspnea, and chest pain.
Harms Results
Key harms reported in the CASPIAN trial as of the final analysis (data cut-off date January 27, 2020) are summarized in Table 2. A total of 260 patients (98.1%) in the durvalumab + EP arm and 258 patients (97.0%) in the EP arm experienced an AE. The most commonly reported AEs in the durvalumab + EP and EP-alone arms were neutropenia (41.9% and 46.6%, respectively), anemia (38.5% and 47.0%, respectively), nausea (33.6% and 33.5%, respectively), and alopecia (31.7% and 34.2%, respectively). Adverse events led to discontinuation of study treatment in 10.2% of patients in the durvalumab + EP arm and 9.4% of patients in the EP arm. Overall, 34% of patients in the durvalumab + EP and EP-alone arms of the CASPIAN trial experienced an SAE. A greater percentage of patients in the EP arm experienced an SAE compared to the durvalumab + EP arm (36.5% versus 32.1%, respectively). The most commonly reported SAEs in the durvalumab + EP and EP-alone arms were febrile neutropenia (4.5% and 4.5%, respectively), anemia (1.9% and 4.5%, respectively), pneumonia (2.3% and 3.4%, respectively), and thrombocytopenia (0.4% and 3.4%, respectively). As of the final analysis, 78.4% of patients in durvalumab + EP arm and 85.9% of patients in EP arm had died, with most deaths attributable to ES-SCLC.
Immune-related AEs were more frequent in the durvalumab + EP arm compared to the EP arm (53.2% versus 39.1%, respectively). The most commonly reported immune-related AEs in the durvalumab + EP arm were endocrine disorders (n = 75, 28.3%) and dermatitis/rash (n = 51, 19.2%). The most commonly reported immune-related AEs in the EP arm were diarrhea/colitis (n = 31, 11.7%) and dermatitis/rash (n = 25, 9.4%). A small number of patients in both treatment arms (durvalumab + EP and EP alone) experienced infusion-related reactions (1.9% and 1.1%, respectively) and hypersensitivity/anaphylactic reactions (1.1% and 0.8%, respectively). In the durvalumab + EP arm, 35.1% of patients experienced an infection compared to 30.8% of patients in the EP arm.
Table 2: Summary of Key Results From the CASPIAN Trial
Interim analysis (data cut-off: March 11, 2019) | Final analysis (data cut-off: January 27, 2020) | |||
|---|---|---|---|---|
Key results | Durvalumab + EP N = 268 | EP N = 269 | Durvalumab + EP N = 268 | EP N = 269 |
Efficacy outcomes | ||||
OS — ITT population | ||||
Deaths, n (%) | 155 (57.8) | 181 (67.3) | 210 (78.4) | 231 (85.9) |
Median OS (95% CI),a months | 13.0 (11.5 to 14.8) | 10.3 (9.3 to 11.2) | 12.9 (11.3 to 14.7) | 10.5 (9.3 to 11.2) |
HR (95% CI)b,c | 0.73 (0.591 to 0.909) | 0.75 (0.625 to 0.910) | ||
P valued | 0.0047 | 0.0032e | ||
OS at 12 months, % (95% CI)a,f | 53.7 (47.4 to 59.5) | 39.8 (33.7 to 45.8) | 52.8 (46.6 to 58.5) | 39.3 (33.4 to 45.1) |
OS at 18 months, % (95% CI)a,f | 33.9 (26.9 to 41.0) | 24.7 (18.4 to 31.6) | 32.0 (26.5 to 37.7) | 24.8 (19.7 to 30.1) |
OS at 24 months, % (95% CI)a,f | NA | NA | 22.2 (17.3 to 27.5) | 14.4 (10.3 to 19.2) |
PFS by investigator assessment — ITT population | ||||
Events, n (%) | 226 (84.3) | 233 (86.6) | 234 (87.3) | 236 (87.7) |
Median PFS (95% CI),a months | 5.1 (4.7 to 6.2) | 5.4 (4.8 to 6.2) | 5.1 (4.7 to 6.2) | 5.4 (4.8 to 6.2) |
HR (95% CI)b,c | 0.78 (0.645 to 0.936) | 0.80 (0.665 to 0.959) | ||
P valued | 0.0078d | 0.0157e | ||
PFS at 6 months, % (95% CI)a,f | 45.4 (39.3 to 51.3) | 45.6 (39.3 to 51.7) | 45.4 (39.3 to 51.3) | 45.8 (39.5 to 51.9) |
PFS at 12 months, % (95% CI)a,f | 17.5 (13.1 to 22.5) | 4.7 (2.4 to 8.0) | 17.9 (13.5 to 22.8) | 5.3 (2.9 to 8.8) |
PFS at 18 months, % (95% CI)a,f | NA | NA | 13.9 (10.0 to 18.4) | 3.4 (1.6 to 6.4) |
PFS at 24 months, % (95% CI)a,f | NA | NA | 11.0 (7.5 to 15.2) | 2.9 (1.2 to 5.8) |
DORf by investigator assessment — confirmed responders | ||||
Patients with a confirmed response, n (%) | 182 (67.9) | 155 (57.6) | 182 (67.9) | 156 (58.0) |
Median confirmed DOR (95% CI)a | 5.1 (4.9 to 5.3) | 5.1 (4.8 to 5.3) | 5.1 (4.9 to 5.3) | 5.1 (4.8 to 5.3) |
% remaining in response at 12 months (95% CI)a | 22.7 (NR) | 6.3 (NR) | 23.2 (NR) | 7.3 (NR) |
% remaining in response at 24 months (95% CI)a | NA | NA | 13.5 (NR) | 3.9 (NR) |
ORR by investigator assessment — ITT population | ||||
Patients with an unconfirmed response, n (%) | 213 (79.5) | 189 (70.3) | 213 (79.5) | 190 (70.6) |
Complete response | 7 (2.6) | 4 (1.5) | NR | NR |
Partial response | 206 (76.9) | 185 (68.8) | NR | NR |
Stable disease | 20 (7.5) | 42 (15.6) | NR | NR |
Odds ratio (95% CI)g | 1.64 (1.106 to 2.443) | 1.61 (1.086 to 2.401) | ||
P valueh | 0.0137 | 0.0177 | ||
Patients with a confirmed response, n (%) | 182 (67.9) | 155 (57.6) | 182 (67.9) | 156 (58.0) |
Complete response | 6 (2.2) | 2 (0.7) | NR | NR |
Partial response | 176 (65.7) | 153 (56.9) | NR | NR |
Stable disease | 20 (7.5) | 42 (15.6) | NR | NR |
Odds ratio (95% CI)g | 1.56 (1.095 to 2.218) | 1.53 (1.078 to 2.185) | ||
P valueh | 0.0136 | 0.0173 | ||
Symptoms: Adjusted mean change from baseline to PD or 12 monthsj — PRO-evaluable populationk | ||||
Patients contributing to analysis, n | 261 | 260 | NA | NA |
Cough (EORTC QLQ-LC13) | ||||
Adjusted mean change from baseline | −17.1 | −17.1 | NR | NR |
Standard error | 1.71 | 2.10 | NR | NR |
95% CI | −20.43 to −13.71 | −21.21 to −12.96 | NR | NR |
Estimated difference (99% CI)m | 0.0 (−5.25 to 5.29) | NR | ||
P value | 0.992 | NR | ||
Dyspnea (EORTC QLQ-LC13) | ||||
Adjusted mean change from baseline | −8.6 | −8.0 | NR | NR |
Standard error | 1.44 | 1.64 | NR | NR |
95% CI | −11.40 to −5.76 | −11.26 to −4.81 | NR | NR |
Estimated difference (99% CI)m | −0.5 (−4.38 to 3.29) | NR | ||
P value | 0.714 | NR | ||
Chest pain (EORTC QLQ-LC13) | ||||
Adjusted mean change from baseline | −8.1 | −9.4 | NR | NR |
Standard error | 1.59 | 1.85 | NR | NR |
95% CI | −11.27 to −5.01 | −13.04 to −5.75 | NR | NR |
Estimated difference (99% CI)m | 1.3 (−3.20 to 5.71) | NR | ||
P value | 0.465 | NR | ||
Fatigue (EORTC QLQ-C30) | ||||
Adjusted mean change from baseline | −7.4 | −5.6 | NR | NR |
Standard error | 1.64 | 1.87 | NR | NR |
95% CI | −10.67 to −4.22 | −9.24 to −1.88 | NR | NR |
Estimated difference (99% CI)m | −1.9 (−6.28 to 2.51) | NR | ||
P value | 0.268 | NR | ||
Appetite loss (EORTC QLQ-C30) | ||||
Adjusted mean change from baseline | −12.7 | −8.2 | NR | NR |
Standard error | 1.65 | 1.94 | NR | NR |
95% CI | −15.95 to −9.47 | −11.98 to −4.36 | NR | NR |
Estimated difference (99% CI)m | −4.5 (−9.04 to −0.04) | NR | ||
P value | 0.009 | NR | ||
Harms, n (%) — safety population | ||||
N | — | — | 265 | 266 |
AEs | — | — | 260 (98.1) | 258 (97.0) |
Neutropenia | — | — | 111 (41.9) | 124 (46.6) |
Anemia | — | — | 102 (38.5) | 125 (47.0) |
Nausea | — | — | 89 (33.6) | 89 (33.5) |
Alopecia | — | — | 84 (31.7) | 91 (34.2) |
SAEs | — | — | 85 (32.1) | 97 (36.5) |
Febrile neutropenia | — | — | 12 (4.5) | 12 (4.5) |
Anemia | — | — | 5 (1.9) | 12 (4.5) |
Pneumonia | — | — | 6 (2.3) | 9 (3.4) |
Thrombocytopenia | — | — | 1 (0.4) | 9 (3.4) |
Discontinued treatment due to AEs | — | — | 27 (10.2) | 25 (9.4) |
Deaths | — | — | 210 (78.4) | 231 (85.9) |
Notable harms, n (%) | ||||
Immune-related AEs | — | — | 141 (53.2) | 104 (39.1) |
Diarrhea/colitis | — | — | 30 (11.3) | 31 (11.7) |
Endocrine | — | — | 75 (28.3) | 18 (6.8) |
Dermatitis/rash | — | — | 51 (19.2) | 25 (9.4) |
Infusion-related reactions | — | — | 5 (1.9) | 3 (1.1) |
Hypersensitivity/anaphylactic reactions | — | — | 3 (1.1) | 2 (0.8) |
Infection | — | — | 93 (35.1) | 82 (30.8) |
AE = adverse event; CI = confidence interval; DOR = duration of response; EORTC = European Organisation for Research and Treatment of Cancer; EP = etoposide-platinum (carboplatin or cisplatin); HR = hazard ratio; ITT = intention-to-treat; NA = not available; NR = not reported; OS = overall survival; PD = progression disease; PFS = progression-free survival; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire; SAE = serious adverse event.
aCalculated using the Kaplan–Meier technique. CI derived based on the Brookmeyer-Crowley method using a log-log transformation.
bThe HRs and CIs were calculated using a stratified Cox proportional hazards model, adjusting for planned platinum therapy (carboplatin or cisplatin) at cycle 1, and ties were handled by the Efron approach.
cAn HR of less than 1 favours durvalumab + EP.
dStratified log-rank test, adjusted for planned platinum therapy (cisplatin or carboplatin).
eNominal P value (i.e., results are non-inferential).
fCalculated post hoc.
gThe comparisons (vs. EP) were performed using a separate logistic regression model, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), with a 95% CI calculated by profile likelihood. An odds ratio of at least 1 favours durvalumab + EP.
hP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled). P value, derived from a logistic regression model, is based on twice the change in log-likelihood resulting from the addition of a treatment factor to the model.
jThe overall 2-sided 5% alpha is controlled across the 5 key symptoms using the Bonferroni-adjusted procedure (1% significance level for each end point). Change from baseline was analyzed separately for each treatment comparison using a mixed model for repeated measures, based on the restricted maximum likelihood method, with patient, treatment, age at randomization (< 65 years, ≥ 65 years), sex (male, female), smoking status at screening (smoker, non-smoker), visit, and treatment by visit interaction as fixed factors, and the appropriate baseline and baseline by visit interaction as covariates. For all subscales/items, a Toeplitz with a heterogeneity covariance structure was used to model the within-patient error and the Kenward-Roger approximation was used to estimate the degrees of freedom.
kIncludes data up to progressive disease or 12 months (whichever is earlier) and excludes visits with excessive missing data (defined as > 75% missing data).
mAn estimated difference of less than 0 favours durvalumab + EP over EP alone.
Critical Appraisal
The open-label design of the trial makes it prone to biases. The primary outcome of the CASPIAN trial, OS, is an objective outcome, and reporting of deaths is unlikely to be influenced. However, the way in which patients are treated throughout the study could be influenced by knowledge of treatment assignment and affect OS. The direction of this bias is unknown. Outcomes relying on investigator’s assessment (PFS, DOR, and ORR) may have been biased, but the direction of bias is unknown. The open-label design also may have affected AE reporting and patient-reported HRQoL and symptoms, but the direction of bias is unknown.
Subgroup analyses of OS and PFS (ECOG PS, smoking history, and brain metastases at baseline) were specified a priori. However, they were not adjusted for multiplicity and therefore considered exploratory. Treatment exposure was adequate to evaluate the safety and tolerability of durvalumab and EP, although there were high treatment discontinuation rates. There was extremely little loss to follow-up and patients were followed for survival for up to 2 years. Treatment groups were generally well balanced.
The interim analysis of the CASPIAN trial data was planned, and a multiple testing procedure was applied to control the overall type I error rate for OS and PFS at 5%. The CASPIAN trial met its primary end point for OS at the interim analysis. It was not possible to formally test PFS for statistical significance within the multiple testing procedure at either the interim or final analysis.
Four protocol amendments were implemented in the trial, including multiple changes to the primary objective and primary end points of the trial implemented after randomization of study patients was complete. Progression-free survival was originally a co-primary end point but was then changed to the key secondary end point. Blinded central review to determine PD for PFS was removed, and PD was then determined per investigator assessment. The changes in objectives and end points were accompanied by changes to the multiple testing procedure and alpha spending. The direction of the bias introduced by the protocol amendments is unclear.
Overall type I error was controlled for the MMRM analysis for 5 key symptoms assessed by the EORTC QLQ-C30 and QLQ-LC13. There was no adjustment for multiplicity for the other secondary efficacy outcomes (ORR, DOR, and time to deterioration in EORTC QLQ-C30 and QLQ-LC13 scores). Landmark OS, landmark PFS, and DOR were calculated post hoc. Interpretation of the HRQoL and symptom results was limited by the divergence in compliance rates between the treatment arms.
The enrolled study population is generally representative of Canadian patients with ES-SCLC, although there were some differences. Enrolment in the CASPIAN trial was limited to patients with an ECOG PS of 0 or 1, which does not reflect the Canadian ES-SCLC patient population, according to the clinical experts consulted by CADTH. The experts also noted that the study patient population included a greater proportion of non-smokers than is seen in Canadian clinical practice. The CASPIAN trial did not enroll any patients from Canada.
Indirect Comparisons
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Conclusions
One phase III, open-label, active-controlled RCT (CASPIAN) provided direct evidence regarding the efficacy and safety of durvalumab in combination with EP in adult patients with ES-SCLC relative to EP alone. Compared to patients treated with EP, those treated with durvalumab + EP showed benefits in OS. The difference in median OS between treatment arms (2.7 months) was considered statistically significant and clinically relevant by the clinical experts consulted by CADTH. The results suggest that the addition of durvalumab to EP was associated with an improvement in PFS compared to EP alone, but this finding is associated with substantial uncertainty because formal statistical testing was not possible due to the trial’s multiple testing procedure, evidence of non-proportionality of hazards, potential attrition bias, and introduction of bias by removing blinded independent central review after enrolment was complete. The effect of durvalumab on ORR and DOR is also uncertain due to the lack of control for multiplicity and that DOR was calculated post hoc in confirmed responders only when confirmation of response was not required by the study protocol. The results of the time to deterioration in HRQoL and symptoms suggest that durvalumab + EP may have a beneficial effect, but this remains uncertain due to a lack of control for multiplicity and differences between treatment arms in completion rates of the EORTC QLQ-C30 and QLQ-LC13. The results of the symptom analysis suggest that adding durvalumab to EP may have a benefit for appetite loss compared to EP alone. Almost all study participants reported treatment-emergent AEs. Durvalumab + EP was related to more immune-mediated AEs than was EP alone, although the profile and incidence rates of these AEs were expected, according to the clinical experts consulted by CADTH. Infusion-related and hypersensitivity/anaphylactic reactions were uncommon, and the incidence of infections was similar in both treatment arms.
Introduction
Disease Background
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in Canada.1 Survival from lung cancers of all stages and histologies is poor, with an overall 5-year net survival rate of 19%.1 In 2020 alone, an estimated 29,800 new cases of lung cancer will be diagnosed and 21,200 deaths will be associated with lung cancer.1 One in 17 Canadians is expected to die of lung cancer.10 Smoking remains the largest single risk factor for lung cancer, responsible for 90% of lung cancers in men and 80% of lung cancers in women in Canada.4 Lung cancer is classified into SCLC and non–small cell lung cancer (NSCLC). Small cell lung cancer accounts for 12% to 15% of lung cancer cases.2,3 Nevertheless, this represents a significant health burden, with more than 4,000 cases reported annually across Canada.11 Cases of SCLC are distinguished from NSCLC by a rapid growth rate, early metastasis to regional lymph nodes and/or distant sites, and initial sensitivity to chemotherapy and radiotherapy.4 In Canada, the 5-year predicted net survival rate for SCLC is 7%.1 According to the clinical experts consulted by CADTH for this review, SCLC is strongly associated with smoking tobacco.
Small cell lung cancer is most commonly characterized according to 2 stages developed by the Veterans Affairs Lung Cancer Study Group: limited-stage or ES disease.12 Patients with disease confined to 1 hemithorax, regional mediastinal lymph nodes, and ipsilateral supraclavicular lymph nodes are classified as having limited-stage SCLC.4 Patients with tumour involvement that is more widespread in the lungs, and may include malignant pleural or pericardial effusions or hematogenous metastases, are classified as having ES-SCLC.4 Approximately 2-thirds of SCLC patients have ES disease.3 In recent years, there was some movement toward anatomic staging using the tumour-node-metastasis staging system.13 However, according to the clinical experts consulted by CADTH, most clinical trials select patient populations based on the Veterans Affairs Lung Cancer Study Group classification, and most clinicians use this system in clinical practice.
According to the clinical experts consulted by CADTH, patients with ES-SCLC present as very ill. A diagnosis of SCLC is made using a standard pathologic assessment of a tissue biopsy. Staging to determine whether the patient has ES-SCLC is done with radiology testing (e.g., CT, PET scan, bone scan, brain MRI).
Standards of Therapy
In general, surgery does not have a major role in the management of SCLC,14 and most patients with ES-SCLC are treated with chemotherapy alone.15 Thoracic irradiation as primary treatment is not routinely recommended for patients with ES-SCLC.4 However, radiotherapy can be used for symptom control where appropriate.4
The majority of patients with ES-SCLC receive 4 to 6 cycles of a platinum drug (cisplatin or carboplatin) in combination with etoposide for first-line treatment, which has been the standard of care for several decades.4,15-17 Cisplatin + etoposide is generally the preferred regimen in Canadian practice.4 Carboplatin may be used in place of cisplatin in patients who are frail or have significant hearing loss, peripheral neuropathy, decreased heart function, or abnormal renal function.4
Patients with ES-SCLC frequently develop brain metastases and may be offered prophylactic cranial irradiation (PCI).4 According to the clinical experts consulted by CADTH, the gains in OS from these treatments are modest and selection of patients that are most likely to benefit from PCI remains challenging.
Although SCLC is initially chemosensitive, the majority of patients will relapse within months after first-line therapy.4 Further chemotherapy is frequently given at the time of relapse. The preferred option for second-line therapy is EP.4 Topotecan or cyclophosphamide + doxorubicin + vincristine are also options for second-line therapy.4 Modest improvements in OS were observed in a trial of oral topotecan versus best supportive care.18 Additional drugs such as amrubicin have failed to produce any improvement in OS when compared with topotecan.19 There is no established third-line therapy for ES-SCLC.
Little progress has been made recently in the systemic treatment and outcomes for ES-SCLC.20 A variety of strategies have been evaluated over the past 20 years, including the use of non–cross-resistant chemotherapy,21 intense weekly chemotherapy,22,23 maintenance chemotherapy,24 and high-dose chemotherapy with transplantation.25 None of these strategies have resulted in clear improvements in OS for patients with SCLC, according to the clinical experts consulted by CADTH. Multiple trials of drugs targeting a variety of molecular abnormalities have all failed to result in any improvement in treatment outcomes for patients with SCLC.
Drug
Durvalumab is a fully IgG1 kappa monoclonal antibody that selectively blocks the interaction of PD-L1 with PD-1 and CD80.5 Expression of PD-L1 helps tumours evade detection and elimination by the immune system. When PD-L1 interacts with PD-1 and CD80, the PD-L1/PD-1 pathway decreases cytotoxic T-cell activity, proliferation, and cytokine production. By selectively blocking the interaction of PD-L1 with PD-1 and CD80, durvalumab inhibits the immunosuppressive effects of the PD-L1/PD-1 pathway, thereby enhancing antitumour immune responses.
On September 21, 2020, durvalumab was approved by Health Canada for first-line treatment of patients with ES-SCLC in combination with etoposide and either carboplatin or cisplatin.5 The reimbursement request for durvalumab by the sponsor is the Health Canada–approved indication.
Durvalumab is also indicated for the treatment of patients with locally advanced, unresectable, stage III NSCLC.5 Durvalumab has been previously reviewed by CADTH for the treatment of patients with locally advanced, unresectable NSCLC following curative intent, platinum-based chemoradiation therapy, for up to a maximum of 12 months.26 In addition, durvalumab has received marketing authorization with conditions for the treatment of locally advanced or metastatic urothelial carcinoma, pending the results of clinical trials.5
Durvalumab is available as a single-use vial and is administered as an IV infusion for 60 minutes.5 For the treatment of ES-SCLC in patients with a body weight of more than 30 kg, the recommended dosage is 1,500 mg in combination with etoposide and either carboplatin or cisplatin every 3 weeks for 4 cycles, followed by 1,500 mg every 4 weeks as monotherapy until disease progression or unacceptable toxicity. For patients with a body weight less than or equal to 30 kg, the recommended dosage is 20 mg/kg in combination with etoposide and either carboplatin or cisplatin every 3 weeks for 4 cycles, followed by 20 mg/kg every 4 weeks as monotherapy until disease progression or unacceptable toxicity.
Table 3: Key Characteristics of Durvalumab
Characteristic | Durvalumab |
|---|---|
Mechanism of action | Selectively blocks the interaction of PD-L1 with PD-1 and CD80 |
Indicationa | First-line treatment of adult patients with ES-SCLC in combination with etoposide and either carboplatin or cisplatin |
Route of administration | IV |
Recommended dosage | 1,500 mg in combination with etoposide and either carboplatin or cisplatin every 3 weeks (21 days) for 4 cycles, followed by 1,500 mg every 4 weeks as monotherapy until disease progression or unacceptable toxicity |
Serious adverse effects or safety issues | Immune-mediated adverse reactions may occur and require immunosuppression |
CD80 = cluster of differentiation 80; ES-SCLC = extensive-stage small cell lung cancer; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1.
aHealth Canada–approved indication.
Source: Product monograph.5
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
Two patient groups responded to the call from CADTH to provide input about patients’ experience, values, and preferences related to SCLC and its treatment.
Lung Cancer Canada is a registered national charity with an exclusive focus on lung cancer in Canada. The group provided information collected through environmental scans as well as interviews with 7 patients (1 male and 6 females, between 40 and 70 years of age) and their families and/or caregivers who reported their thoughts and experiences with SCLC. The information was accessed from November to December 2020.
The second group that provided information was the LHF, previously known as the Ontario Lung Association. It is a registered charity that assists and empowers people living with or caring for others with lung disease, provides programs and services to patients and health care providers, invests in health research, and advocates for better policies on lung health. This group provided information from online surveys completed by people living with lung cancer and through telephone interviews with 14 patients living in Ontario.
Disease Experience
The patient groups identified lung cancer as the most commonly diagnosed cancer with the highest mortality rate in Canada, accounting for 25% of all cancer deaths. The 5-year survival rate is just 19%, with lower rates for advanced cases. Cases of SCLC represent approximately 15% of lung cancer cases. They are strongly associated with a history of smoking and patients have a median age at diagnosis of 70 years. Small cell lung cancer has a more aggressive presentation, with a median survival of 7 to 11 months with treatment, and is usually diagnosed in the later stages, with a high tumour burden and more symptoms at presentation.
According to the patient input received, a diagnosis of lung cancer and the subsequent treatment has a major impact on the life of the patient and their loved ones. Many caregivers are involved in the care, well-being, and management of their loved ones. More than half of patient respondents from the LHF reported current issues with work, day-to-day chores, and socialization. Lung Cancer Canada reported that with certain treatments, such as chemotherapy and immunotherapy, caregivers need to take their loved ones to the hospital or specialized clinics for their treatments, and care for them afterward for varying periods of time. In some cases, caregivers may need to take time off work to provide this care, affecting work productivity and finances, and causing mental stress. The emotional and physical toll during and after treatment may affect the caregivers’ ability to fulfill their role in the family and at work and affect their ability to participate in activities they enjoy. Direct quotes from patients include:
“My work was demanding, and it would be too stressful to continue with an incurable diagnosis over my head.”
“It takes longer to do everything — getting dressed, doing my personal hygiene, and completing ‘normal’ daily tasks.”
“I have lot of anxiety and sadness now.”
Experiences With Currently Available Treatments
The current therapeutic options for ES-SCLC are chemotherapy and immunotherapy.
According to the patient input received, chemotherapy continues to be a viable form of treatment for this type of cancer. This treatment has been shown to work well in this group of patients, resulting in improved symptoms and increasing patients’ quality of life. However, chemotherapy can lower a patient’s immunity and, in some cases, may result in an inability to return to normal activities, have visitors, or spend quality time with family and loved ones.
Patients reported that immunotherapy is a form of treatment that has allowed many patients to hope for improved outcomes and has been shown to improve quality of life with more manageable side effects. Patients report feeling better within days of their first treatment with immunotherapy. Because lung cancer patients, and SCLC patients in particular, have a high symptom burden, this is an important aspect of this form of treatment. Patients on immunotherapy reported side effects that were mild and easily managed. In a few cases, stronger side effects had to be managed with over-the-counter or prescription drugs. Most patients found that the treatment was tolerable and did not interfere with day-to-day life. Lung Cancer Canada emphasized that no form of immunotherapy has currently been approved for SCLC patients in Canada.
Improved Outcomes
Both groups mentioned outcomes that are considered important for patients. Based on their experience, they include:
control the cancer
improve symptoms and delay deterioration
have manageable side effects
be effective on the central nervous system
delay progression
extend survival with a good quality of life
provide longer-lasting and durable treatment.
All of these align with patients’ values and preferences in the Canadian landscape.
Experience With Drug Under Review
Neither LCC nor the LHF was able to include patients’ experiences with durvalumab because the treatment is not currently accessible to SCLC patients in Canada, and there were no Canadian trial sites for the requested treatment. Lung Cancer Canada was able to look at the outcomes of SCLC patients treated with atezolizumab in combination with chemotherapy to highlight patients’ experiences with an immunotherapy similar to durvalumab. This combination was shown to work well for patients in terms of tolerability.
Additional Information
The groups highlighted the poor survival rates for ES-SCLC, which is reported to have a 2-year survival rate of less than 5%, and a 5-year survival rate of less than 2%. The patient input emphasized that SCLC is a devastating disease, with few treatment options. Treatment for SCLC has not changed in the past 30 years, and this puts these patients at a disadvantage. Patient groups identified an unmet need, unlike the situation for NSCLC patients, for whom a larger range of treatment options is available. Input from LCC emphasized that there is a need for treatment options and that there is no reason to delay SCLC patients’ access to this treatment.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of ES-SCLC.
Unmet Needs
The clinical experts consulted by CADTH noted that current treatment options for ES-SCLC are limited and have not changed in 30 years. Most patients receive either cisplatin or carboplatin with etoposide (EP therapy) for 4 to 6 cycles as first-line therapy. A small number of patients who are not candidates for platinum therapy or do not want to receive IV systemic therapy may be treated with oral etoposide, which is considered an inferior therapy. Although there is a high initial response rate to first-line treatment with EP therapy, most patients relapse within months. Patients derive limited benefit from second-line chemotherapy, which is less effective at extending survival, reducing disease burden, and improving symptoms. In addition, many patients are not well enough to receive second-line chemotherapy after relapse. Patients with ES-SCLC have an OS of approximately 9 months to 1 year.
The experts identified a significant unmet need for a systemic therapy that can extend response to first-line treatment to prolong survival and preserve the symptom and quality of life benefits.
Place in Therapy
The clinical experts consulted by CADTH for this review anticipated that durvalumab would be delivered concurrently with first-line EP therapy, then administered as single-drug maintenance therapy. Durvalumab would address the underlying disease process by potentiating T cells that target the somatic mutations and neoantigens associated with SCLC and are related to tobacco consumption. Durvalumab would be offered to all patients for whom EP therapy is planned, except patients for whom immunotherapy is contraindicated (e.g., those with autoimmune disease).
Patient Population
The clinical experts noted that patients with ES-SCLC who are candidates for EP therapy and for whom immunotherapy is not contraindicated would be suitable for treatment with durvalumab. Contraindications would include severe or active autoimmune disease and organ transplant recipients.
The experts revealed that, to date, no biomarkers or patient characteristics have been identified that can predict which patients are more likely to respond to durvalumab. There are no known patient subgroups that are most likely to respond to durvalumab.
Assessing Response to Treatment
Treatment response is assessed by physical examination, history of symptom burden, and serial radiography (CT) scans at the completion of 4 to 6 cycles of EP and then every 8 weeks to 12 weeks. Chest X-rays may also be done more frequently between CT scans due to the aggressiveness of the disease and its propensity for rapid recurrence. Patients are assessed approximately every 8 weeks during follow-up.
The clinical experts indicated that a clinically meaningful response to treatment would be prolonged OS. Delayed disease progression, reduced symptom burden, and improved ECOG PS are also clinically meaningful.
Discontinuing Treatment
The clinical experts consulted by CADTH agreed that treatment with durvalumab should be discontinued if a patient experiences disease progression, intolerable AEs or SAEs (e.g., anaphylactic allergic reaction, grade 3 colitis, or myocarditis), or the patient wishes to stop treatment.
Prescribing Conditions
A diagnosis of ES-SCLC is made by pathologic assessment of a tissue biopsy by a respirologist/pulmonologist, thoracic surgeon, or interventional radiologist. Treatment should be prescribed and monitored by medical oncologists, general practitioners of oncology, or nurse practitioners who have been trained in oncology and immunotherapy. Treatment with durvalumab could be provided at any outpatient chemotherapy unit at a Canadian cancer centre or hospital.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Input was received from 2 clinician groups:
The Ontario Health (previously Cancer Care Ontario) Lung and Cancer Drug Advisory Committee. The Ontario Health– Cancer Care Ontario drug advisory committees provide timely evidence-based clinical and health-system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
Lung Cancer Canada is a national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. Based in Toronto, Ontario, LCC has a wide reach that includes both regional and pan-Canadian initiatives. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
Unmet Needs
The clinician groups noted that SCLC accounts for approximately 15% of all lung cancers. It is seen mainly in the elderly population, and the median age at diagnosis is approximately 70 years. Patients present at a late stage, and less than 5% of SCLC is diagnosed at a stage that would be amenable to surgical resection. In two-thirds of patients, the cancer is ES and has spread outside the lung and regional lymph nodes. Treatment for ES-SCLC is standard around the globe and has not changed in 30 years. First-line treatment consists of 4 to 6 cycles of systemic chemotherapy with IV etoposide and a platinum compound, either cisplatin or carboplatin.
The clinician groups reported that, despite high response rates to initial therapy, many patients progress rapidly. Less than half the patients live beyond 1 year, with few surviving beyond 2 years. Therefore, there is a high unmet need for more effective therapies that result in longer disease control and better OS.
The clinician groups stated that all patients with ES-SCLC have high unmet needs. They reported that the only factors that predict worse outcome are those associated with a higher tumour burden, making it impossible to identify subgroups of greater need.
Place in Therapy
The clinician groups indicated that durvalumab would be used as initial systemic therapy in patients with ES-SCLC in combination with 4 cycles of platinum and etoposide, followed by maintenance durvalumab until disease progression. The goals of adding durvalumab to EP therapy would be to improve PFS and OS. In particular, the hope is that the addition of durvalumab will increase the proportion of patients living beyond 18 to 24 months.
The clinician groups reported that the current standard of care is platinum and etoposide. This has been the case for the last 3 decades. No other drugs apart from immune checkpoint inhibitors have demonstrated improved OS as first-line therapies for ES-SCLC. According to the clinician group input, it would not be appropriate to recommend the addition of other therapies apart from an immune checkpoint inhibitor such as durvalumab. Importantly, because chemotherapy and durvalumab have non-overlapping toxicity profiles, both components can be administered at full doses without unacceptable toxicity.
The clinician groups anticipated that first-line treatment for ES-SCLC would move from double chemotherapy with EP to a triplet therapy with etoposide-platinum-durvalumab. The clinician groups that provided input for this review stated that it would not be appropriate to recommend that patients try other treatments before initiating treatment with durvalumab in combination with chemotherapy as no more than half of patients are fit enough for second-line treatments if they fail to respond or relapse after first-line therapy.
The clinician groups noted that durvalumab is not currently approved as a second-line treatment for ES-SCLC. They reported that there are no trials demonstrating benefit from an immune checkpoint inhibitor as subsequent therapy. Therefore, the clinician groups did not anticipate that the addition of durvalumab to EP as first-line therapy would have any downstream impact on other treatment options. The groups anticipated that second-line therapy would remain either re-treatment with platinum and etoposide or cyclophosphamide + doxorubicin + vincristine (CAV). The clinician groups noted that topotecan is another option, although it is not funded in all jurisdictions.
Patient Population
The clinician groups reported that all patients with ES-SCLC need improved therapies and that it would not be possible to identify subgroups that are more likely to benefit from the addition of durvalumab as there are no predictive biomarkers of benefit for the addition of durvalumab to chemotherapy. Therefore, this treatment should be considered for any patient with ES-SCLC and an ECOG PS of 2 or greater. ES-SCLC is a common condition that medical oncologists see and treat on a regular basis. These patients would be identified at the time of initial consultation with a medical oncologist. The clinician groups did not identify any specific issues for consideration. All patients with ES-SCLC and an ECOG PS of 2 or greater could be candidates for therapy with EP and durvalumab unless immune checkpoint inhibitors are contraindicated. Patients with symptomatic brain metastases should be treated before commencing systemic therapy. Patients with severe or symptomatic autoimmune disorders should not be treated with durvalumab immunotherapy.
The clinician groups reported that all hospitals in Canada have the ability to undertake the pathologic, hematologic, biochemical, and radiologic tests necessary to diagnose and treat SCLC. The clinician groups thought that advanced molecular profiling is not necessary. Selection of SCLC patients for immunotherapy, including durvalumab, does not require any special testing.
Assessing Response to Treatment
The clinician groups reported that tumour shrinkage on imaging studies would typically be used to determine if a patient is responding to therapy. Improvement in the patient’s symptoms would also be used as a measure of treatment benefit. Any improvement in survival beyond 18 months is considered meaningful.
According to the clinician groups, numerous tumour markers have been evaluated in an attempt to select patients for immunotherapy, including PD-1 and PDL-1 inhibitors. Results have been variable and inconsistent across tumour types and within individual cancers. The most extensively studied markers in lung cancer are PD-L1 status assessed in tumour samples by immunohistochemistry, and tumour mutational burden assessed either in tumour samples or in peripheral blood cell-free DNA.
According to the clinician groups, patients are evaluated in clinical practice for response (and toxicity) before each cycle of therapy by history, physical examination, bloodwork and/or chest radiographs. CT and/or MRI scans are performed every 2 to 3 cycles of chemotherapy and always at the completion of chemotherapy. For patients receiving EP therapy and durvalumab, treatment would continue until disease progression. After 6 months or so, the frequency of imaging may be increased to every 4 cycles of therapy.
Discontinuing Treatment
The clinician groups indicated that EP chemotherapy is never given for more than 6 cycles, and usually only for 4 cycles. In clinical practice, the reasons to discontinue treatment would be unequivocal disease progression, the development of grade 3 immune-related AEs, or patient choice. In this setting of extensive SCLC, immunotherapy similarly continues until disease progression or recurrence, toxicity, or when the patient or physician decides to stop for other reasons.
Prescribing Conditions
The clinician groups anticipated that chemotherapy and durvalumab can be administered as an outpatient treatment. Treatment most often would be given in a specialized cancer hospital with chemotherapy and immunotherapy expertise. Treatment would be administered under the supervision of a medical oncologist, as is standard in most regions of Canada.
Additional Considerations
The clinician groups reported that there have been no significant treatment advances in ES-SCLC in more than 30 years. The addition of durvalumab represents a modest but real improvement in survival for a group of patients with high unmet needs.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect a program’s ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Platinum and etoposide combinations are the standard of care for the initial systemic therapy in patients with ES-SCLC. Second-line regimens include CAV and topotecan. Should a patient not be able to tolerate or receive the platinum and etoposide combination, is it reasonable to extrapolate combining durvalumab with alternate chemotherapy (e.g., CAV, topotecan)? | The clinical experts reported that it would be highly unlikely for patients to receive an alternative chemotherapy such as CAV or topotecan in a first-line setting if patients are able to tolerate IV therapy. Etoposide-platinum has been the standard first-line therapy for more than 30 years, and 4 to 6 cycles can be given to the vast majority of ES-SCLC patients. Patients would only receive alterative chemotherapy in a first-line setting if they were unable to access etoposide-platinum chemotherapy (e.g., drug shortage) or could not tolerate IV therapy. |
What is a clear definition of ES-SCLC that would assist with implementation criteria? | The VALCSG developed the criteria for classifying SCLC as an LS or ES disease. Patients with disease confined to 1 hemithorax, regional mediastinal lymph nodes, and ipsilateral supraclavicular lymph nodes are classified as LS-SCLC. Patients with tumour involvement that is more widespread in the lungs and whose diagnoses may include malignant pleural or pericardial effusions or hematogenous metastases are classified as ES-SCLC. |
If treatment is discontinued before evidence of progressive disease, can durvalumab be administered at time of relapse (i.e., relapse off-therapy)? If so, what would be the appropriate timing of re-treatment? Further, if re-treatment is permitted at relapse, would therapy consist of durvalumab monotherapy or durvalumab + chemotherapy? Which chemotherapy regimens would be appropriate to combine with durvalumab in this scenario? | In the CASPIAN trial, patients were treated with durvalumab until they experienced progressive disease. If durvalumab was discontinued due to an AE (e.g., an immune-mediated AE), the clinical experts indicated that it would be reasonable to restart durvalumab after the AE had resolved as the AEs are often transient in nature and do not reappear upon rechallenge. |
Some patients with ES-SCLC may receive prophylactic cranial radiation. It is noted that patients with asymptomatic or treated/stable CNS metastases were eligible to participate in the CASPIAN study, and only patients enrolled on the chemotherapy arm of the study were permitted to receive prophylactic cranial radiation. Is it safe to administer durvalumab concurrently with cranial radiation? | The clinical experts stated that it would be safe to administer durvalumab concurrently with cranial radiation. Canadian clinicians often do not stop administering other checkpoint inhibitor immunotherapies when administering radiation. |
What is the recommended type and frequency of follow-up recommended for patients receiving durvalumab maintenance for ES-SCLC? | The clinical experts reported that treatment response is assessed by physical examination, history of symptom burden, and serial radiography, which include CT scans at the completion of 4 to 6 cycles of etoposide-platinum and then every 8 to 12 weeks. Chest X-rays may also be taken more frequently between CT scans due to the aggressiveness of the disease and propensity for rapid recurrence. Patients are assessed approximately every 8 weeks during follow-up. |
What definitions or parameters should be used to determine stopping rules for patients on durvalumab maintenance for ES-SCLC? | The clinical experts indicated that treatment with durvalumab should follow the CASPIAN trial design. Durvalumab maintenance therapy should be discontinued if a patient experiences disease progression, intolerable or serious adverse events (e.g., anaphylactic allergic reaction, grade 3 colitis, or myocarditis), or the patient wishes to stop treatment. The experts noted that the CASPIAN trial allowed patients to continue durvalumab maintenance therapy after experiencing radiographic progression if, in the opinion of the investigator, patients were continuing to experience a clinical benefit. If patients are experiencing clinical disease progression, the clinical experts indicated they would stop durvalumab maintenance therapy. |
If there is progression during a drug holiday, can treatment be resumed? Is there a minimum number of cycles of chemo that must be given with durvalumab (e.g., what if the patient has to discontinue the chemo portion after 1 cycle)? | In the CASPIAN trial, patients were treated with durvalumab until they experienced progressive disease. If durvalumab was temporarily stopped due to an AE (e.g., an immune-mediated AE), it would be reasonable to restart durvalumab after the AE had resolved, as the AEs are often transient in nature and do not reappear upon rechallenge. The clinical experts reported that, in their experience, the vast majority of patients are able to tolerate 4 cycles of chemotherapy. As such, most patients eligible for treatment with durvalumab would receive 4 cycles of chemotherapy. |
Is there evidence to suggest stopping durvalumab maintenance therapy after a specified period of time? If yes, is there evidence for re-treatment (and what is the time frame and duration for any re-treatment)? | The clinical experts indicated that treatment with durvalumab should follow the CASPIAN trial design. During the CASPIAN trial, durvalumab maintenance therapy was continued until the patient experienced disease progression, intolerable or serious adverse events (e.g., anaphylactic allergic reaction, grade 3 colitis, myocarditis), or the patient wished to stop treatment. The clinical experts are not aware of any evidence to support stopping durvalumab maintenance therapy after a specified period of time. Based on the currently available evidence from the CASPIAN trial, it is unclear if there is a point in time where maintenance therapy could be stopped without the patient potentially losing the clinical benefit. |
The recommended dose of durvalumab is 1,500 mg IV in combination with chemotherapy (etoposide and either carboplatin or cisplatin) every 3 weeks (21 days) for 4 cycles, followed by 1,500 mg IV every 4 weeks as monotherapy until disease progression or unacceptable toxicity. Patients with a body weight of 30 kg or less should receive weight-based dosing, equivalent to 20 mg/kg IV in combination with chemotherapy every 3 weeks (21 days) for 4 cycles, followed by 20 mg/kg IV every 4 weeks as monotherapy until weight increases to greater than 30 kg. Durvalumab should be administered prior to chemotherapy when given on the same day. In NSCLC, many jurisdictions administer durvalumab as a weight-based dose up to a cap (e.g., 10 mg/kg IV up to a maximum of 750 mg every 2 weeks, or 20 mg/kg IV up to a maximum of 1,500 mg every 4 weeks). Would a weight-based dose up to a cap be reasonable to implement for the SCLC indication, and if so, should the weight-based dose be 15 mg/kg IV (up to 1,125 mg) every 3 weeks during chemotherapy, and 20 mg/kg IV (up to 1,500 mg) every 4 weeks as monotherapy? | The clinical experts are not aware of evidence to support weight-based dosing of durvalumab in ES-SCLC at this time. The clinical experts advised that the sponsor may have pharmacokinetic data that could help determine whether weight-based dosing would be reasonable in the treatment of ES-SCLC. |
The phase III CAPSIAN trial restricted eligibility to patients with an ECOG PS of 0 or 1. Should patients with an ECOG PS > 1 be eligible? | The clinical experts reported that there is an ongoing trial (LUMINANCE) investigating the use of durvalumab in combination with EP in ES-SCLC patients with an ECOG PS > 1. Until data are available, the clinical experts indicated that it could be reasonable to offer durvalumab to patients with an ECOG PS of 2. The clinical experts reported that, based on other lung cancer trials that have expanded ECOG PS eligibility criteria, patients with an ECOG PS of 2 can experience treatment benefit. However, the clinical experts noted that it could also be reasonable to restrict the use of durvalumab to patients with an ECOG PS of 0 or 1 until data are available for patients with an ECOG PS > 1. It was noted that in ES-SCLC, patients often improve after their first cycle of treatment and their ECOG PS score improves. It was also noted that ECOG PS is subjective. |
There is a time-limited need to allow patients currently on platinum-etoposide chemotherapy to add durvalumab who otherwise meet the eligibility criteria. What time frame is appropriate to add durvalumab for patients on chemotherapy alone or who recently completed chemotherapy? Should durvalumab only be reimbursed for patients who are still receiving chemotherapy? Is there a minimum number of cycles of chemotherapy remaining where durvalumab could be added to therapy? Would patients who recently completed chemotherapy be eligible for maintenance durvalumab? | The clinical experts indicated that durvalumab should be administered according to the CASPIAN trial design. The clinical experts would not add durvalumab for patients on chemotherapy alone or those who recently completed chemotherapy. |
Are PD-L1 results needed to confirm eligibility or determine any subsets of patients more likely to derive benefit from durvalumab? | The clinical experts reported that no biomarkers or patient characteristics, including PD-L1, have been identified that can predict which patients are more likely to respond to durvalumab. Currently, there are no known patient subgroups that are most likely to respond to durvalumab. |
If a patient experiences toxicity to chemotherapy, can durvalumab maintenance be administered alone, and is there a minimum number of chemotherapy cycles that must be administered in combination? | The clinical experts report that, in their experience, all patients with an ECOG PS of 0 or 1 can get through at least 2 cycles of chemotherapy, and the vast majority of patients are able to tolerate 4 cycles. The clinical experts noted that the patients who would have difficulty tolerating chemotherapy would be those with an ECOG PS of 3 or 4, and they therefore would be ineligible for durvalumab treatment. |
CAV = cyclophosphamide + doxorubicin + vincristine; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ES = extensive-stage; LS = limited-stage; SCLC = small cell lung cancer; PD-L1 = programmed cell death ligand 1; VALCSG = Veterans Affairs Lung Cancer Study Group.
Clinical Evidence
The clinical evidence included in the review of durvalumab is presented in the Systematic Review section, which includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies selected according to an a priori protocol. No indirect or other evidence was identified.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of durvalumab in combination with etoposide and either carboplatin or cisplatin for the first-line treatment of patients with ES-SCLC.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with ES-SCLC Subgroups
|
Intervention | Durvalumab (1,500 mg, IV infusion) in combination with etoposide and either carboplatin or cisplatin every 3 weeks for 4 cycles followed by durvalumab (1,500 mg) monotherapy every 4 weeks |
Comparators | Etoposide and platinum-based chemotherapy (i.e., cisplatin or carboplatin) Best supportive care |
Outcomes | Efficacy outcomes
Harms outcomes
|
Study designs | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; ECOG = Eastern Cooperative Oncology Group Performance Status; ES-SCLC = extensive-stage small cell lung cancer; HRQoL = quality of life; PD-L1 = programmed cell death ligand 1; SAE = serious adverse event; TMB = tumour mutational burden; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist.27
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Imfinzi (durvalumab) and small cell lung cancer (SCLC). Clinical trials registries searched were the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, the European Union Clinical Trials Register, and Canadian Partnership Against Cancer Corporation’s Canadian Cancer Trials.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on December 22, 2020. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on May 13, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).28 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 5 reports presenting data from a single unique study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
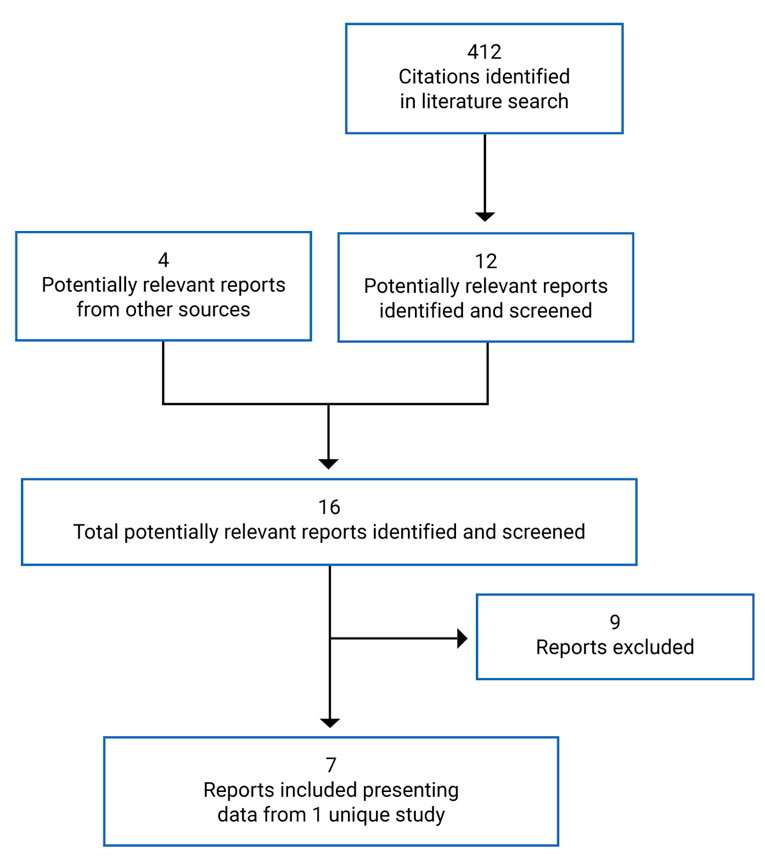
Table 6: Details of Included Study
Detail | CASPIAN Trial |
|---|---|
Designs and populations | |
Study design | Phase III, multi-centre, open-label, active-controlled RCT |
Locations | 209 sites in 23 countries enrolled patients: US (19), Europe (92), Asia (65), Russia (9), Turkey (6), Israel (4), South America (14) |
Patient enrolment dates | April 7, 2017, to May 29, 2018 (global cohort, excluding China extension) |
Randomized (N) | 805
|
Inclusion criteria | ≥ 18 years old at screening (except in Japan, where patients must be ≥ 20 years old) Histologically or cytologically confirmed ES-SCLC Patients with brain metastases were allowed if asymptomatic or treated and stable off steroids and anticonvulsants for ≥ 1 month Suitable to receive platinum-based chemotherapy (cisplatin or carboplatin) as first-line treatment for ES-SCLC Life expectancy ≥ 12 weeks WHO/ECOG PS of 0 or 1 Body weight > 30 kg No prior exposure to immune-mediated therapy Adequate organ and marrow function |
Exclusion criteria | History of radiotherapy to the chest before systemic therapy or planned consolidation chest radiation therapy; radiation therapy outside of chest for palliative care allowed if completed before first dose of study drug Concurrent chemotherapy or other cancer treatment Major surgical procedure within 28 days before first dose of study drug Allogenic organ transplantation Paraneoplastic syndrome of autoimmune nature Autoimmune or inflammatory disorders (except for vitiligo, alopecia, hypothyroidism and stable on hormone replacement, chronic skin condition not requiring systemic therapy, celiac disease controlled by diet alone) Uncontrolled intercurrent illness (e.g., interstitial lung disease, congestive heart failure, cardiac arrhythmia) History of prior malignancy History of leptomeningeal carcinomatosis History of active primary immunodeficiency Active infection including tuberculosis, hepatitis B, hepatitis C, HIV Immunosuppressive medication (current or within 14 days of first dose of study drug) Receipt of live, attenuated vaccine within 30 days before first dose of study drug Pregnant or breastfeeding |
Drugs | |
Intervention | Durvalumab + EP
|
Comparator(s) | Durvalumab + tremelimumab + EP
EP only
|
Duration | |
Phase | |
Screening | 3 weeks |
During chemotherapy | 12 weeks |
Post-chemotherapy | Until progressive disease |
Follow-up | Up to 2 years |
Outcomes | |
Primary end point | Overall survivala |
Secondary and exploratory end points | Secondary
|
• Safety (AEs, physical examination, vital signs, electrocardiograms, laboratory findings) Exploratory
• Correlation of polymorphisms with pharmacoeconomics, pharmacodynamics, safety, or response parameters | |
Notes | |
Publications | Goldman et al. (2020)29 – Final analysis results (data cut-off of January 27, 2020) Goldman et al. (2020a)30 – Patient-reported outcomes (EORTC QLQ-C30 and EORTC QLQ-LC13) as of the interim analysis (data cut-off March 11, 2019 Paz-Ares et al. (2019)31 – Interim analysis results (data cut-off of March 11, 2019) |
ADA = anti-drug antibody; AE = adverse event; DLL3 = delta-like 3; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC = European Organisation for Research and Treatment of Cancer; EP = etoposide-platinum (carboplatin or cisplatin); EQ-5D-5L = EuroQol 5-Dimensions 5-Levels; ES-SCLC = extensive-stage small cell lung cancer; ICU = intensive care unit; ORR = objective response rate; OS = overall survival; OS12 = overall survival at 12 months after randomization; OS18 = overall survival at 18 months after randomization; OS24 = overall survival at 24 months after randomization; PD = progressive disease; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival; PFS2 = progression-free survival after subsequent anticancer therapy; PFS6 = progression-free survival at 6 months from randomization; PFS12 = progression-free survival at 12 months from randomization; PFS18 = progression-free survival at 18 months from randomization; PFS24 = progression-free survival at 24 months from randomization; PGIC = Patient Global Impression of Change; PRO-CTCAE = Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire; q.3.w. = every 3 weeks; q.4.w. = every 4 weeks; RCT = randomized controlled trial.
Note: Four additional reports were included from the submission to CADTH and requests for additional information were made to the sponsor.5-7,32
aAnalysis of OS was event-driven. The interim analysis was planned for after approximately 318 OS events (60% maturity) occurred between the durvalumab + tremelimumab + EP and EP-alone arms and approximately 318 OS events (60% maturity) occurred between the durvalumab + EP and EP-alone arms. The data cut-off date for the primary analysis of OS was planned for when approximately 425 OS events (80% maturity) were observed across the durvalumab + tremelimumab + EP and EP treatment arms, and the durvalumab + EP and EP treatment arms.
Source: Goldman et al. (2020),29 Goldman et al. (2020),30 Paz-Ares et al. (2019),31 and Clinical Study Reports.6,7
Description of Studies
The CASPIAN trial was an international multi-centre, phase III, open-label, RCT conducted to investigate the efficacy and safety of durvalumab, with or without tremelimumab, in combination with etoposide and platinum-based chemotherapy compared to EP alone in adult patients with ES-SCLC.6,7 A total of 805 patients were randomized from April 7, 2017, to May 29, 2018, in a 1:1:1 ratio to 3 treatment arms: durvalumab with tremelimumab in combination with etoposide and either carboplatin or cisplatin (durvalumab + tremelimumab + EP), durvalumab in combination with etoposide and either carboplatin or cisplatin (durvalumab + EP), and EP alone. The CASPIAN trial included a 3-week screening period to complete eligibility assessments. Patients were randomized from 209 sites in 23 countries. No Canadian sites participated in the CASPIAN trial. The type of platinum-based chemotherapy (cisplatin or carboplatin) used was the investigator’s choice. Randomization was stratified by the platinum-based chemotherapy planned for the first treatment cycle. The study design is depicted in Figure 2.
The primary end point of the CASPIAN trial was OS, and the key secondary end point was PFS as assessed by the investigator. Protocol-specified secondary end points included the PFS rate at 6 months after randomization, PFS rate at 12 months after randomization, ORR, and changes in symptoms and HRQoL using the EORTC QLQ-C30 and the QLQ-LC13. Tumour assessments by CT or MRI were performed at screening, week 6, and week 12 after randomization, and every 8 weeks until confirmed disease progression. Tumours were evaluated per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 criteria. A follow-up scan was requested after every radiological PD on study when possible.
Figure 2: Study Schema of the CASPIAN Trial
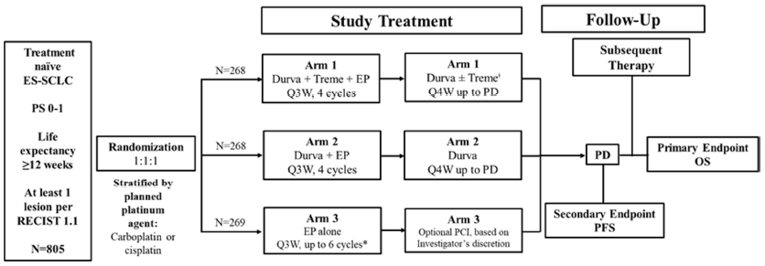
Durva = durvalumab; ES-SCLC = extensive-stage small cell lung cancer; EP = etoposide and platinum-based chemotherapy (consisting of etoposide 80 mg/m2 to 100 mg/m2 with either carboplatin area under the curve 5 mg/mL/min to 6 mg/mL/min or cisplatin 75 mg/m2 to 80 mg/m2); OS = overall survival; PCI = prophylactic cranial irradiation; PD = progressive disease; PFS = progression-free survival; PS = performance status; Q3W = every 3 weeks; Q4W = every 4 weeks; RECIST = Response Evaluation Criteria in Solid Tumours; Treme = tremelimumab.
* Patients in arm 3 were permitted an additional 2 cycles of EP (up to 6 cycles total) per the investigator’s discretion.
‡ Patients received an additional dose of tremelimumab post-EP.
Source: Clinical Study Report.6
Data for the durvalumab + tremelimumab + EP arm of the CASPIAN trial will not be presented in the systematic review because tremelimumab is not approved in Canada and the combination is not aligned with the Health Canada product monograph for durvalumab. However, efficacy and harms data for the durvalumab + tremelimumab + EP arm are available in Appendix 3 for context.
Analyses and Data Cut-Offs
A pre-specified interim analysis was planned to be conducted after approximately 318 OS events occurred between the durvalumab + EP and EP-alone arms (60% maturity).6 The interim analysis had a data cut-off date of March 11, 2019, at which point the OS data had reached 63% maturity (336 OS events from 537 patients) in the durvalumab + EP and EP-alone arms.6 The CASPIAN trial met its primary end point under the statistical analysis plan at the interim analysis, and therefore statistical testing of OS for durvalumab + EP versus EP-alone was considered complete at this analysis.
A primary analysis of OS was planned to be conducted when approximately 425 OS events (80% maturity) were observed across the durvalumab + tremelimumab + EP and EP-alone arms, and the durvalumab + EP and EP-alone arms. The final analysis was conducted with a data cut-off date of January 27, 2020, at which point the OS data had reached 82% maturity (441 events from 537 patients) in the durvalumab + EP and EP-alone arms.7
Protocol Amendments
Four protocol amendments were implemented during the CASPIAN trial, which are summarized in Table 7.7 In the original study protocol, OS and PFS by blinded independent central review were co-primary end points, and the primary objective of the trial was to assess the efficacy of durvalumab + tremelimumab + EP compared with EP alone in terms of OS and PFS. The objective to assess the efficacy of durvalumab + EP efficacy compared with EP alone was originally a secondary objective. Amendments 2 to 4 implemented changes to the primary objective, secondary objectives, determination of PFS, and multiple testing procedure to control alpha spending after randomization of study participants was complete.
Table 7: Summary of Protocol Amendments in the CASPIAN trial
Amendment | Key changes to protocol |
|---|---|
Amendment 1 (January 15, 2018) | Updates to the toxicity management guideline, descriptions of risks, and adverse events of special interest Added option to continue recruitment in China, following achievement of the global recruitment target of 795 randomized patients and an objective to evaluate consistency in efficacy and safety among SCLC patients in China Added an exploratory objective to investigate the relationship between a patient’s tumour mutational burden and efficacy outcomes Updates and clarification of the description of guidelines for evaluation of objective tumour response using RECIST version 1.1 |
Amendment 2 (July 23, 2018) |
|
Amendment 3 (October 29, 2018) |
|
Amendment 4 (November 29, 2018) |
|
BICR = blinded independent central review; EP = etoposide-platinum (carboplatin or cisplatin); OS = overall survival; PFS = progression-free survival.
Source: Clinical Study Report.7
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria are described in Table 6. Briefly, the CASPIAN trial enrolled adults with histologically or cytologically confirmed ES-SCLC who were suitable for platinum-based chemotherapy as first-line treatment.6,7 Brain metastases at baseline were allowed if patients were asymptomatic or treated and stable (off steroids and anticonvulsants for at least 1 month before study treatment). Enrolment was limited to patients with an WHO/ECOG performance status of 0 or 1. Patients were excluded if they had prior exposure to immune-mediated therapy, radiotherapy to the chest, or contraindications to immunotherapy (e.g., history of allogenic organ transplantation, autoimmune or inflammatory disorders).
Baseline Characteristics
Baseline characteristics in the intention-to-treat (ITT) population of the CASPIAN trial are summarized in Table 8. Most patients enrolled in the trial were male (71.6%), White (82.6%), smokers (93.5%) with a small cell carcinoma (combined) histology type (84.1%) and an ECOG PS of 1 (63.0%).7 The mean age of all patients was 62.6 years. Baseline characteristics were generally well balanced between the durvalumab + EP and EP-alone arms. A total of 7 patients (0.9%) had received previous chemotherapy and 27 patients (3.4%) had received previous radiotherapy.
Table 8: Summary of Baseline Characteristics — Intention-to-Treat Population
Characteristic | CASPIAN trial | ||
|---|---|---|---|
Durvalumab + tremelimumab + EP (n = 268) | Durvalumab + EP (n = 268) | EP (n = 269) | |
Age, years, mean (SD) | 62.9 (8.61) | 62.4 (8.12) | 62.4 (8.32) |
Sex, n (%) | — | — | — |
Male | 202 (75.4) | 190 (70.9) | 184 (68.4) |
Female | 66 (24.6) | 78 (29.1) | 85 (31.6) |
Race, n (%) | — | — | — |
White | 215 (80.2) | 229 (85.4) | 221 (82.2) |
Black or African-American | 1 (0.4) | 2 (0.7) | 3 (1.1) |
Asian | 47 (17.5) | 36 (13.4) | 42 (15.6) |
Other | 5 (1.9) | 1 (0.4) | 2 (0.7) |
Missing | 0 | 0 | 1 (0.4) |
Ethnicity, n (%) | — | — | — |
Hispanic or Latino | 7 (2.6) | 10 (3.7) | 6 (2.2) |
Not Hispanic or Latino | 260 (97.0) | 255 (95.1) | 261 (97.0) |
Missing | 1 (0.4) | 3 (1.1) | 2 (0.7) |
Smoking history, n (%) | — | — | — |
Non-smoker | 15 (5.6) | 22 (8.2) | 15 (5.6) |
Smoker | 253 (94.4) | 246 (91.8) | 254 (94.4) |
Former smoker | 141 (52.6) | 126 (47.0) | 128 (47.6) |
Current smoker | 112 (41.8) | 120 (44.8) | 126 (46.8) |
WHO/ECOG PS, n (%) | — | — | — |
0 | 109 (40.7) | 99 (36.9) | 90 (33.5) |
1 | 159 (59.3) | 169 (63.1) | 179 (66.5) |
Histology type | — | — | — |
Small cell carcinoma (neuroendocrine) | 39 (14.6) | 39 (14.6) | 48 (17.8) |
Small cell carcinoma (combined) | 228 (85.1) | 229 (85.4) | 220 (81.8) |
Other | 1 (0.4) | 0 | 1 (0.4) |
Previous chemotherapy | 1 (0.4) | 3 (1.1) | 3 (1.1) |
Previous radiotherapy | 9 (3.4) | 8 (3.0) | 10 (3.7) |
Adjuvant | 0 | 0 | 1 (0.4) |
Palliative | 8 (3.0) | 8 (3.0) | 8 (3.0) |
Definitive | 1 (0.4) | 0 | 1 (0.4) |
ECOG = Eastern Cooperative Oncology Group Performance Status; EP = etoposide-platinum (carboplatin or cisplatin); SD = standard deviation.
Source: Clinical Study Report.7
Interventions
The CASPIAN trial was a randomized, open-label, 3-arm trial.6,7 Patients were randomized in a 1:1:1 ratio to durvalumab + tremelimumab + EP, durvalumab + EP, or EP alone. The durvalumab + tremelimumab + EP arm is not included in the CADTH systematic review because this regimen is not approved by Health Canada.
Durvalumab + Etoposide-Platinum
During the chemotherapy phase, patients received 4 doses of 1,500 mg IV durvalumab co-administered with IV etoposide (80 mg/m2 to 100 mg/m2) with either carboplatin (area under the curve 5 mg/mL per min to 6 mg/mL per min) or cisplatin (75 mg/m2 to 80 mg/m2) every 3 weeks. Durvalumab was administered over 60 minutes and EP was administered over 120 minutes. Treatment with chemotherapy was limited to 4 cycles. After chemotherapy, patients received 1,500 mg IV durvalumab every 4 weeks until PD by RECIST version 1.1 (unconfirmed and confirmed) unless there was unacceptable toxicity or withdrawal of consent, or another discontinuation criterion was met. Other discontinuation criteria included an inability to reduce the corticosteroid dosage to no more than 10 mg of prednisone per day (or equivalent) within 12 weeks after the last dose of the study drug, recurrence of a previously experienced Grade 3 treatment-related AE following resumption of dosing, and severe immune-mediated AEs. If a patient’s weight fell to 30 kg or less, they received weight-based dosing equivalent to 20 mg/kg of durvalumab until the weight had improved to more than 30 kg, at which point the patient started receiving the fixed 1,500 mg dose of durvalumab.
Patients with PD who, in the investigator’s opinion, continued to receive a benefit from durvalumab treatment could continue to receive durvalumab for as long as they were demonstrating a clinical benefit. However, patients with rapid tumour progression or with symptomatic progression requiring urgent medical intervention were not eligible for continuing durvalumab treatment. Following disease progression as assessed by the investigator, standard chemotherapy was offered.
Etoposide-Platinum Alone
Patients received at least 4 doses of etoposide (80 mg/m2 to 100 mg/m2) with either carboplatin (area under the curve 5 mg/mL per min to 6 mg/mL per min) or cisplatin (75 mg/m2 to 80 mg/m2) every 3 weeks over 120 minutes. Patients could receive an additional 2 doses of EP (maximum of 6 cycles total) at the investigator’s discretion, if clinically indicated. Following disease progression as assessed by the investigator, standard chemotherapy was offered. Crossover to durvalumab monotherapy following PD was not permitted.
Concomitant Medications
The following concomitant medications were allowed in the CASPIAN trial6,7: serotonin antagonists, glucocorticoids, colony-stimulating factors, proton pump inhibitors, propulsives, other antiemetics, sulfonamides, electrolyte solutions, anilides, fluoroquinolones, benzodiazepine derivatives, natural opium alkaloids, H2 receptor antagonists, osmotically acting laxatives, selective beta-blocking agents, platelet aggregation inhibitors (excluding heparin), 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, penicillins, ACE inhibitors, and dihydropyridine derivatives.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the following section.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | CASPIAN trial |
|---|---|
Overall survival | Primary |
Progression-free survival | Key secondary |
Duration of response | Secondary |
Objective response rate | Secondary |
HRQoL (EORTC QLQ-C30, EORTC QLQ-LC13) | Secondary |
Symptoms (EORTC QLQ-C30, EORTC QLQ-LC13) | Secondary |
EORTC = European Organisation for Research and Treatment of Cancer; HRQoL = health-related quality of life; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire.
Overall Survival
Overall survival, which was the primary outcome of the CASPIAN trial, was defined as the time from the date of randomization until the date of death due to any cause.
Progression-Free Survival
In the original trial protocol, PFS was a co-primary end point, and disease progression was to be assessed by blinded independent central review per RECIST version 1.1. In the final protocol, PFS was designated the key secondary outcome of the CASPIAN trial, and defined as the time from the date of randomization until the date of disease progression or death by any cause (in the absence of progression). Disease progression for analysis of PFS was determined by the investigator’s RECIST version 1.1 assessments.
Duration of Response and Objective Response Rate
The ORR was defined as the percentage of patients with at least 1 visit response of complete response or partial response. Response was determined by the investigator using RECIST version 1.1 criteria. Confirmation of response was not required per the protocol, and both unconfirmed and confirmed ORRs were reported. Unconfirmed responses corresponded to a complete or partial response observed at 1 or more study visit. Confirmed responses corresponded to a complete or partial response observed at 1 or more study visit and a confirmatory scan at least 4 weeks after the initial response. The DOR was calculated post hoc using confirmed response.
Health-Related Quality of Life
Change in HRQoL using the EORTC QLQ-C30 and QLQ-LC13 was a secondary end point in the CASPIAN trial. A detailed discussion and critical appraisal of the outcome measures are provided in Appendix 4. The EORTC QLQ-C30 is a standardized, patient self-administered questionnaire for evaluating the quality of life of patients with cancer participating in clinical trials.33 This questionnaire complements the lung cancer–specific questionnaire, the QLQ-LC13.8 The EORTC QLQ-C30 consists of 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, nausea/vomiting, and pain), and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). This instrument also includes global health status and overall quality of life. A higher score on a functional scale corresponds to higher level of function, while a higher score in the symptom scale corresponds to higher burden of symptoms.9 The QLQ-LC13 consists of lung cancer–related symptoms (e.g., coughing, hemoptysis, dyspnea, and pain) and treatment side effects (e.g., hair loss, neuropathy, sore mouth, and dysphagia).8
Time to deterioration of EORTC QLQ-C30 and QLQ-LC13 scores was assessed in patients whose baseline scores were at least 10 for functioning and global health status/QoL and no more than 90 for symptoms. The CASPIAN trial defined a clinically meaningful deterioration as an increase of at least 10 points from baseline for symptoms and a decrease of more than 10 points from baseline for function and global health status/quality of life. The MID reported in the literature varies depending on the improvement or deterioration among different items scales. In 1 study, estimates of the MID for the EORTC QLQ-C30 ranged from 9.1 units (cognitive functioning) to 23.5 units (pain), and a meaningful change for deterioration ranging from 7.2 units (physical functioning) to 13.5 units (role functioning).34 In another study, the MID estimates for deterioration based on using WHO performance status and weight loss as anchors were 4 and 6 for physical; 5 and 5 for role; 7 and 9 for social; 4 and 4 for global health status; 6 and 11 for fatigue; and 3 and 7 for pain.35
Time to deterioration was calculated as the time from randomization to the first clinically meaningful deterioration at a subsequent assessment, or death from any cause in the absence of clinically meaningful deterioration.
Symptoms
Change in symptoms using the EORTC QLQ-C30 and QLQ-LC13 was a secondary end point in the CASPIAN trial. The predefined key symptoms were cough, dyspnea, and chest pain (as assessed by the QLQ-LC13), and fatigue and appetite loss (as assessed by EORTC QLQ-C30). The CASPIAN trial defined a clinically meaningful difference as an absolute change in the score from baseline of at least 10 points. The MID reported in the literature varies depending on the improvement or deterioration among different items scales. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Immune-Related Adverse Events
Immune-related AEs included AEs with a potential or likely inflammatory or immune-mediated pathophysiological basis and were recorded as AEs of special interest in the CASPIAN trial. Immune-related AE categories included, but were not limited to, diarrhea/colitis and intestinal perforation, pneumonitis/interstitial lung disease, hepatitis/transaminase increases, endocrinopathies (adrenal insufficiency, hyperthyroidism, hypothyroidism, hypophysitis/ hypopituitarism, and type I diabetes mellitus), nephritis/blood creatinine increases, rash/dermatitis, pancreatitis/serum lipase and amylase increases, myocarditis, myositis/polymyositis, neuropathy/neuromuscular toxicity (e.g., Guillain-Barre and myasthenia gravis), pericarditis, sarcoidosis, uveitis, and infusion-related/hypersensitivity/anaphylactic reactions.
Statistical Analysis
In general, descriptive statistics were reported by treatment arm.6,7 For continuous variables, the mean, standard deviation, median, minimum, and maximum were presented. For categorical variables, counts and percentages were presented. Results of statistical analyses were presented using 95% CIs and 2-sided P values, unless otherwise specified. The planned statistical analysis of the efficacy outcomes of interest in the CADTH systematic review are summarized in Table 10. There were multiple comparisons and a planned interim analysis in this phase III trial.
Multiple Testing Procedure
A multiple testing procedure with a gatekeeping strategy was used to control the overall type I error for OS and PFS at 5% (2-sided).6 Hypotheses were tested in a predefined order with an alpha-exhaustive recycling strategy (Figure 3). The alpha level was controlled at the interim and final analysis time points using a Lan-DeMets spending function that approximates an O’Brien-Fleming approach. The overall 5% type I error was initially split between the analysis of OS for durvalumab + EP versus EP (which was allocated an alpha level of 4%), and the analysis of OS for durvalumab + tremelimumab + EP versus EP (an alpha level of 1%).
Figure 3: Multiple Testing Procedure for Controlling Type I Error of Overall Survival and PFS in the CASPIAN Trial
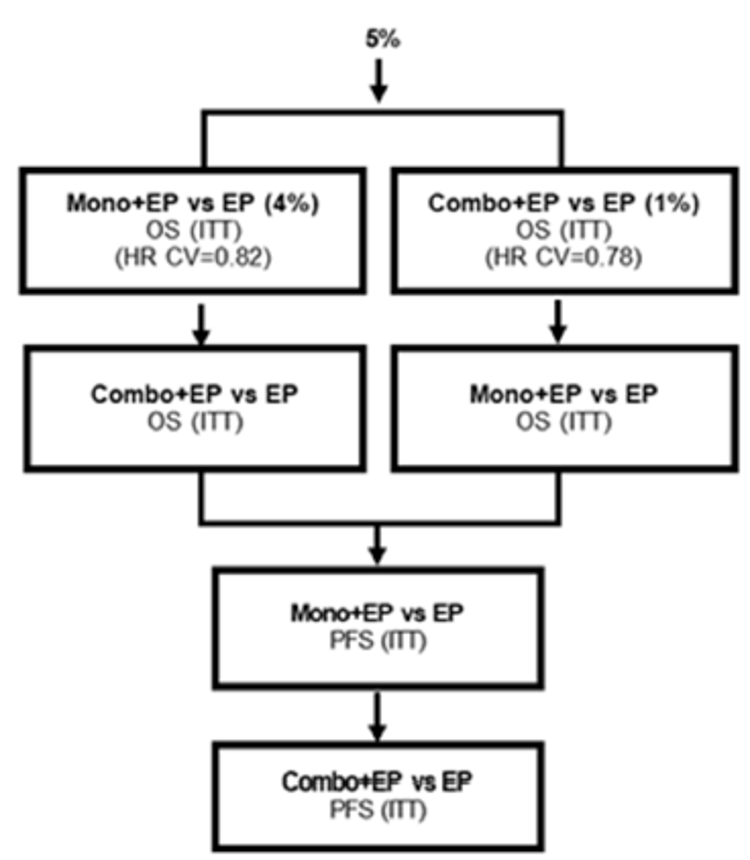
Combo = durvalumab + tremelimumab; CV = critical value; EP = etoposide-platinum; HR = hazard ratio; ITT = intention-to-treat; Mono = durvalumab; OS = overall survival; PFS = progression-free survival.
Note: Alpha recycling between the Mono + EP versus EP and Combo + EP versus EP OS comparisons.
Source: Clinical Study Report.6
Sample Size Determination
The CASPIAN trial planned to randomize 795 eligible patients.6,7 The primary objective of the trial was to assess the efficacy of durvalumab + tremelimumab + EP treatment compared with EP alone and the efficacy of durvalumab + EP treatment compared with EP alone in terms of OS. To control for type I error, a significance level of 1% was used for the analysis of durvalumab + tremelimumab + EP versus EP alone, and a significance level of 4% was used for the analysis of durvalumab + EP versus EP alone. The trial would be considered positive if either of the OS analysis results were statistically significant.
The sample size calculation assumed a 3-month delay in separation of the OS and PFS curves between the immunotherapy arms versus EP alone, and a HR of 0.62 thereafter. The planned data cut-off for the primary analysis of OS was when approximately 425 OS events (80% maturity) were observed across the durvalumab + tremelimumab + EP and EP-alone arms, and the durvalumab + EP and EP treatment arms. If at the time of the primary analysis (425 OS events), the average true OS HR is 0.69, the study would have a 96% power to demonstrate a statistically significant difference at a 2-sided 3.57% significance level (for an overall alpha of 4%) for the comparison of durvalumab + EP versus EP.
Interim Analysis
The interim analysis was planned to be conducted after approximately 318 OS events (60% maturity) occurred between the durvalumab + tremelimumab + EP and EP-alone arms and approximately 318 OS events (60% maturity) occurred between the durvalumab + EP and EP-alone arms.
If the average true OS HR is 0.71 at the interim analysis, the study would have an estimated 48% power to demonstrate a statistically significant difference with a 2-sided 0.23% significance level (for an overall alpha of 1%) for the comparison of durvalumab + tremelimumab + EP versus EP alone, and a 71% power to demonstrate a statistically significant difference at a 2-sided 1.43% significance level (for an overall alpha of 4%) for the comparison of durvalumab + EP versus EP. The smallest treatment difference that would be statistically significant was estimated to be an average HR of 0.71 for durvalumab + tremelimumab + EP versus EP alone and 0.76 for durvalumab + EP versus EP alone.
The alpha level applied at the interim analysis depended upon the observed number of deaths and percent of maturity for OS at the time of interim analysis. At the interim analysis, a total of 336 deaths were observed across the durvalumab + EP and EP arms out of the 425 targeted for the final analysis. The boundary for declaring statistical significance for the analysis of OS for durvalumab + EP versus EP was 0.0178, for a 4% overall alpha.
Primary Outcome
A stratified log-rank test was performed to compare durvalumab + EP to EP alone, adjusting for the type of platinum therapy (carboplatin or cisplatin) planned in cycle 1. The effect of durvalumab + EP versus EP treatment was estimated by the HR together with its CI and P value. The HRs and CIs were estimated from the Cox proportional hazards model. The assumption of proportional hazards was assessed by examining plots of complementary log-log (event times) versus log (time). A Kaplan–Meier plot of OS was presented by treatment arm. A sensitivity analysis was planned to examine censoring patterns to rule out attrition bias, which was done by a Kaplan–Meier plot of time to censoring with the censoring indicator of OS reversed.
Subgroup analyses were planned for type of platinum therapy planned in cycle 1, age, gender, stage (III versus IV), ECOG PS at baseline, smoking status at screening, central nervous system metastasis at baseline, race, and geographical area. For each subgroup, the HR and 95% CI were calculated from an unstratified Cox proportional hazards model with treatment as the only covariate.
Additional exploratory, post hoc analyses were conducted to investigate PD-L1 expression and tumour mutational burden relative to OS. In the exploratory analysis, PD-L1 was analyzed as a continuous variable and expression cut-offs were not predefined.32
Secondary Outcomes
Progression-free survival was the key secondary outcome in the CASPIAN trial, and it was planned to be analyzed in the same method as OS. However, PFS was not formally tested for statistical significance at the interim analysis nor the final analysis due to the multiple testing procedure.6,7 Both the durvalumab + EP and durvalumab + tremelimumab + EP groups were required to achieve statistical significance for OS before stepping down to PFS according to the pre-specified multiple testing procedure, and this was not achieved. As a result, the PFS results and P values should be considered descriptive only.
The ORR was compared between treatment arms using logistic regression models adjusting for the planned type of platinum therapy (cisplatin or carboplatin). Results were presented as an OR together with its associated profile likelihood and 95% CI. An OR of at least 1 favours durvalumab + EP. The analysis of confirmed ORR was post hoc.
Duration of response was calculated post hoc using confirmed responses. Kaplan–Meier estimates with CIs derived using the Brookmeyer-Crowley method and a log-log transformation were presented.
Time to deterioration in EORTC QLQ-C30 and QLQ-LC13 scores was summarized using the same methods as the primary outcome. However, the time to deterioration in EORTC QLQ-C30 and QLQ-LC13 scores was not part of the multiple testing procedure. Kaplan–Meier plots were presented by treatment arm.
Change from baseline in the 5 pre-specified key symptom scores was analyzed using an MMRM analysis of all data from baseline up to PD or 12 months. The overall type I error (2-sided, 5%) was controlled across the 10 hypothesis tests of 2 treatment comparisons in the MMRM analysis for each of the key symptoms using a Bonferroni-adjusted 1% significance level and 99% CIs. The MMRM model included treatment, age, sex, smoking history, visit, and the interaction between treatment and visit interaction as fixed factors and baseline as a covariate, and adjusted for the interaction between baseline and visit. Restricted maximum likelihood estimation was used. An overall adjusted mean estimate was derived to estimate the average treatment effect over visits, giving each visit equal weight. For this overall treatment comparison, adjusted mean estimates per treatment group and corresponding 95% CIs were presented along with an estimate of the treatment difference, 95% CI, and P value.
Table 10: Statistical Analysis of Efficacy End Points
Outcome | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
CASPIAN Trial | |||
OS | Stratified log-rank test. Landmark survival determined using Kaplan–Meier estimates with CI using log-log transformation | Planned platinum therapy during cycle 1 | Kaplan–Meier plot of time to censoring where the censoring indicator of the primary analysis is reversed – attrition bias |
PFS | Stratified log-rank test. Landmark survival determined using Kaplan–Meier estimates with CI using log-log transformation | Planned platinum therapy during cycle 1 | Interval censored analysis – evaluation time bias (log-rank test) Analysis using alternative censoring rules – attrition bias Subsequent anticancer therapy |
ORR | Logistic regression | Planned platinum therapy during cycle 1 | NA |
DOR | Post hoc analysis. Kaplan–Meier estimates with CI derived based on Brookmeyer-Crowley method and using the log-log transformation | NA | NA |
HRQoL (EORTC QLQ-C30 and QLQ-L13) | Time to symptom deterioration using stratified log-rank test | NA | NA |
Symptoms (EORTC QLQ-C30 and QLQ-L13) | Average change from baseline using a MMRM | The MMRM model included treatment, age, sex, smoking history, visit, and the interaction between treatment and visit interaction as fixed factors, baseline as a covariate, further adjusted for the interaction between baseline and visit; restricted maximum likelihood estimation was used | NA |
CI = confidence interval; DOR = duration of response; EORTC = European Organisation for Research and Treatment of Cancer; HRQoL = health-related quality of life; MMRM = mixed model for repeated measures; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire.
Source: Clinical Study Reports6,7 and Statistical Analysis Plan.26
Analysis Populations
The ITT population included all patients randomized. Generally, efficacy analyses used the ITT population, although DOR, HRQoL, and symptoms were analyzed in a subset of patients.
DOR was calculated post hoc in confirmed responders (i.e., patients with a response of complete or partial response at 1 or more study visit and a confirmatory scan no sooner than 4 weeks after the initial complete or partial response per investigator assessment).
Symptoms and HRQoL were assessed in the patient-reported outcome (PRO)-evaluable population,30 which consisted of the ITT population minus patients whose PRO data could not be verified at 1 trial site.30 Time to deterioration of QLQ-C30 and QLQ-LC13 scores was assessed in patients whose baseline scores were 10 or higher for functioning and global health status/quality of life and 90 or lower for symptoms.
The safety analysis set consisted of all patients randomized before the end of global recruitment who received at least 1 dose of study drug.
Results
Patient Disposition
Details of patient disposition in the CASPIAN trial are summarized in Table 11. A total of 972 patients were screened and 805 patients were randomized to receive durvalumab + tremelimumab + EP (N = 268), durvalumab + EP (N = 268), or EP alone (N = 269).7 A total of 156 patients (16.1%) were screen failures, 3 patients (0.3%) died before randomization, and 8 patients (0.8%) withdrew before randomization. A total of 797 patients (99.0%) were treated: 266 (99.3%) received durvalumab + tremelimumab + EP, 265 (98.9%) received durvalumab + EP, and 266 (98.9%) received EP alone. In the durvalumab + EP arm, 223 patients (84.2%) had completed EP and 233 patients (87.9%) had discontinued the durvalumab as of the final analysis. In the EP arm, 190 patients (71.4%) had completed EP treatment as of the final analysis.
As of the final analysis, a total of 662 patients (82.2%) had terminated the study: 212 (79.1%) in the durvalumab + tremelimumab + EP arm, 212 (79.1%) patients in the durvalumab + EP arm, and 238 patients (88.5%) in the EP arm.7 The main reason for study termination was death, and the percentage of patients who died was highest in the EP arm: 76.1% died in the durvalumab + tremelimumab + EP arm, 77.2% in the durvalumab + EP arm, and 83.6% in the EP-alone arm. At the time of the final data cut-off, 11.2% of patients in the durvalumab + tremelimumab + EP arm and 11.9% of patients in the durvalumab + EP arm were ongoing study treatment, whereas 0 patients in the EP arm were ongoing study treatment.
Table 11: Patient Disposition — Final Analysis (Data Cut-Off: January 27, 2020)
Patient disposition | CASPIAN trial | ||
|---|---|---|---|
Durvalumab + tremelimumab + EP | Durvalumab + EP | EP | |
Screened, N | 972 | ||
Randomized, N (%) | 268 | 268 | 269 |
Treated, N (%) | 266 (99.3) | 265 (98.9) | 266 (98.9) |
Discontinued durvalumab, N (%) | 236 (88.7) | 233 (87.9) | NA |
Withdrawal by patient | 11 (4.1) | 7 (2.6) | NA |
Adverse events | 51 (19.2) | 20 (7.5) | NA |
Protocol deviation | 1 (0.4) | 0 | NA |
Disease progression | 160 (60.2) | 186 (70.2) | NA |
Development of withdrawal criteria | 3 (1.1) | 0 | NA |
Lost to follow-up | 0 | 2 (0.8) | NA |
Other | 10 (3.8) | 18 (6.8) | NA |
Discontinued EP, N (%) | 58 (21.8) | 42 (15.8) | 76 (28.6) |
Withdrawal by patient | 5 (1.9) | 4 (1.5) | 19 (7.1) |
Adverse events | 28 (10.5) | 12 (4.5) | 18 (6.8) |
Protocol deviation | 0 | 0 | 0 |
Disease progression | 19 (7.1) | 17 (6.4) | 30 (11.3) |
Development of withdrawal criteria | 0 | 1 (0.4) | 1 (0.4) |
Lost to follow-up | 0 | 0 | 0 |
Other | 6 | 8 (3.0) | 8 (3.0) |
Terminated study, N (%) | 212 (79.1) | 212 (79.1) | 238 (88.5) |
Death | 204 (76.1) | 207 (77.2) | 225 (83.6) |
Lost to follow-up | 2 (0.7) | 1 (0.4) | 1 (0.4) |
Withdrawal | 6 (2.2) | 4 (1.5) | 12 (4.5) |
Ongoing study treatment at final data cut-off, N (%) | 30 (11.2) | 32 (11.9) | 0 |
ITT population, N | 268 | 268 | 269 |
Confirmed responders, N | 156 | 182 | 156 |
PRO-evaluable population,a N | NR | 261 | 260 |
Safety, N | 266 | 265 | 266 |
EP = etoposide-platinum (carboplatin or cisplatin); ITT = intention-to-treat; NA = not applicable; NR = not reported; PRO = patient-reported outcome.
aSymptoms and health-related quality of life was assessed in the PRO-evaluable population evaluated at the interim analysis only.
Source: Clinical Study Report.7
Exposure to Study Treatments
Exposure to durvalumab treatment as of the interim analysis is summarized in Table 12 and exposure to EP treatment is summarized in Table 13. As of the interim analysis, the median duration of exposure to durvalumab in the durvalumab + EP arm was 28 weeks (range = 0.3 to 94.3).6 Exposure to EP was greater in the EP arm compared to the durvalumab + EP arm. In the EP arm, the median numbers of treatment cycles received were 6.0, 6.0, and 4.0 for the etoposide, carboplatin, and cisplatin components, respectively. In the durvalumab + EP arm, the median number of treatment cycles received was 4.0 for all chemotherapy components.
Table 12: Duration of Durvalumab Exposure — Safety Population, Interim Analysis (Data Cut-Off: March 11, 2019)
Durvalumab treatment duration | Durvalumab + EP arm N = 265 |
|---|---|
Number of infusions | |
Mean (SD) | 8.8 (5.19) |
Median (minimum to maximum) | 7.0 (1 to 25) |
Total exposure duration, weeks | |
Mean (SD) | 32.95 (21.059) |
Median (minimum to maximum) | 28.00 (0.3 to 94.3) |
Total treatment years | 167.348 |
Number of cycles received | |
Mean (SD) | 8.8 (5.18) |
Median (minimum to maximum) | 7.0 (1 to 25) |
EP = etoposide-platinum (carboplatin or cisplatin); SD = standard deviation.
Source: Clinical Study Report.6
As of the final analysis (data cut-off on January 27, 2020), mean number of durvalumab infusions was 10.2 (standard deviation = 7.96), and the median (minimum to maximum) number of durvalumab infusions was 7.0 (1 to 37).
Table 13: Duration of Chemotherapy Exposure — Safety Population, Interim Analysis (Data Cut-Off: March 11, 2019)
Chemotherapy treatment duration | Durvalumab + EP arm N = 265 | EP N = 266 | ||||
|---|---|---|---|---|---|---|
Etoposide N = 265 | Carboplatin N = 208 | Cisplatin N = 65 | Etoposide N = 266 | Carboplatin N = 208 | Cisplatin N = 67 | |
Number of infusions | ||||||
Mean (SD) | 11.2 (2.63) | 3.6 (0.88) | 3.7 (1.45) | 14.6 (4.68) | 4.9 (1.52) | 4.3 (1.94) |
Median (minimum to maximum) | 12.0 (2 to 24) | 4.0 (1 to 6) | 4.0 (1 to 12) | 18.0 (1 to 18) | 6.0 (1 to 6) | 4.0 (1 to 7) |
Total exposure duration, weeks | ||||||
Mean (SD) | 11.77 (3.031) | 11.83 (3.238) | 11.13 (3.720) | 16.33 (5.764) | 16.56 (5.698) | 14.35 (7.067) |
Median (minimum to maximum) | 11.86 (0.3 to 20.7) | 12.14 (0.6 to 21.0) | 12.14 (0.3 to 17.9) | 18.71 (0.4 to 26.6) | 19.00 (0.5 to 26.9) | 14.00 (1.7 to 25.9) |
Total treatment years | 59.797 | 47.146 | 13.867 | 83.244 | 66.004 | 18.423 |
Number of cycles received | ||||||
Mean (SD) | 3.7 (0.81) | 3.6 (0.88) | 3.5 (1.00) | 4.9 (1.54) | 4.9 (1.54) | 4.3 (1.93) |
Median (minimum to maximum) | 4.0 (1 to 6) | 4.0 (1 to 6) | 4.0 (1 to 5) | 6.0 (1 to 6) | 6.0 (1 to 6) | 4.0 (1 to 6) |
EP = etoposide-platinum (carboplatin or cisplatin); SD = standard deviation.
Source: Clinical Study Report.6
As of the interim analysis, 3 patients in the durvalumab + EP arm required a durvalumab dose interruption.6 Two patients required an etoposide dose interruption, no patients required a carboplatin dose interruption, and 1 patient required a cisplatin dose interruption. All dose interruptions were due to an AE. A total of 149 (56.2%) patients had durvalumab dose delays, the majority of whom had 1 delay (n = 78, 29.4%). The most common reason for a durvalumab dose delay was AEs (n = 109, 41.1%). A total of 113 patients (42.6%) had dose delays for etoposide, 89 carboplatin-treated patients (42.8%) had dose delays for carboplatin, and 23 cisplatin-treated patients (35.4%) had dose delays for cisplatin. The most common reason for chemotherapy dose delays was an AE.
As of the interim analysis, 9 patients in the EP arm required a dose interruption (7 due to an AE and 2 due to other reasons), 3 patients required a carboplatin dose interruption (all due to AEs), and no patients required a cisplatin dose interruption.6 A total of 144 (54.1%) patients had dose delays for etoposide, 118 carboplatin-treated patients (56.7%) had dose delays for carboplatin, and 29 cisplatin-treated patients (43.3%) had dose delays for cisplatin. The most common reason for dose delays was an AE.
A total of 795 (98.8%) patients received allowed concomitant medications during study treatment.6 Concomitant medications received by patients in the durvalumab + EP and EP-alone arms are summarized in Table 14.
Table 14: Concomitant Medications in the CASPIAN Trial — ITT Population, Final Analysis (Data Cut-Off: January 27, 2020)
Concomitant medications, n (%) | Durvalumab + EP (N = 268) | EP (N = 269) |
|---|---|---|
Number of patients with allowed concomitant medications | 263 (98.1) | 266 (98.9) |
Serotonin (5HT3) antagonists | 223 (83.2) | 243 (90.3) |
Glucocorticoids | 190 (70.9) | 211 (78.4) |
Colony-stimulating factors | 135 (50.4) | 153 (56.9) |
Proton pump Inhibitors | 125 (46.6) | 140 (52.0) |
Propulsives | 92 (34.3) | 111 (41.3) |
Other antiemetics | 79 (29.5) | 87 (32.3) |
Sulfonamides, plain | 71 (26.5) | 91 (33.8) |
Electrolyte solutions | 70 (26.1) | 75 (27.9) |
Anilides | 73 (27.2) | 79 (29.4) |
Fluoroquinolones | 65 (24.3) | 73 (27.1) |
Benzodiazepine derivatives | 57 (21.3) | 78 (29.0) |
Natural opium alkaloids | 56 (20.9) | 70 (26.0) |
H2 receptor antagonists | 64 (23.9) | 64 (23.8) |
Osmotically acting laxatives | 55 (20.5) | 72 (26.8) |
Beta-blockers, selective | 71 (26.5) | 57 (21.2) |
Platelet aggregation inhibitors (excluding heparin) | 60 (22.4) | 57 (21.2) |
Heparin Group | 47 (17.5) | 54 (20.1) |
HMG coenzyme A reductase inhibitors | 63 (23.5) | 57 (21.2) |
Combinations of penicillins (including beta-lactamase inhibitors) | 45 (16.8) | 52 (19.3) |
Ace inhibitors, plain | 54 (20.1) | 52 (19.3) |
Dihydropyridine derivatives | 49 (18.3) | 33 (12.3) |
EP = etoposide-platinum (cisplatin or carboplatin); HMG = 3-hydroxy-3-methylglutaryl; ITT = intention-to-treat.
Note: Includes medications that began before the first dose and were ongoing after the first dose and any medication taken at any time between the date of first dose and up to the date of last dose plus 90 days (both included).
Source: Clinical Study Report.7
Subsequent therapies received by patients in the CASPIAN trial are summarized in Table 15.
Table 15: Subsequent Anticancer Therapy and Radiotherapy — ITT Population, Final Analysis (Data Cut-Off: January 27, 2020)
Subsequent therapy | Durvalumab + EP arm N = 268 | EP N = 269 |
|---|---|---|
Anticancer therapy | ||
Number of patients, n (%) | 123 (45.9) | 125 (46.5) |
Cytotoxic chemotherapy, n (%) | 120 (|) | 118 (|) |
Single regimen | 63 (23.5) | 72 (26.8) |
Platinum doublet | 59 (22.0) | 50 (18.6) |
Other combination | 30 (11.2) | 31 (11.5) |
Immunotherapy | 6 (2.2) | 17 (6.3) |
Other | 4 (1.5) | 5 (1.9) |
Radiotherapy | ||
Number of patients, n (%) | 79 (29.5) | 112 (41.6) |
Brain | 55 (20.5) | 57 (21.2) |
Thoracic region | 20 (7.5) | 47 (17.5) |
Bone | 15 (5.6) | 11 (4.1) |
Prophylactic cranial irradiation | 0 | 22 (8.2) |
Other | 8 (3.0) | 3 (1.1) |
EP = etoposide-platinum (carboplatin or cisplatin); ITT = intention-to-treat.
Source: Clinical Study Report.7
Efficacy
Only those efficacy outcomes and analyses of subgroups for the intervention and comparator arms identified in the review protocol are reported below. See Appendix 3 for detailed efficacy data.
Overall Survival
The OS results of the CASPIAN trial for the durvalumab + EP and EP-alone arms are summarized in Table 16.
As of the interim analysis (data cut-off: March 11, 2019), 336 death events occurred, representing 62.6% maturity for OS overall.6 Median duration of follow-up in all patients was 10.58 months between both treatment groups: 11.30 months in the durvalumab + EP group and 9.86 months in the EP-alone group. Median OS was 13.0 months (95% CI, 11.5 to 14.8) in the durvalumab + EP arm compared to 10.3 months (95% CI, 9.3 to 11.2) the EP arm (HR = 0.73; 95% CI, 0.59 to 0.91; P = 0.0047). Kaplan–Meier curves are depicted in Figure 4. There was a delay of approximately 6 months in separation of the curves, and the associated log-log plot showed some evidence of non-proportionality of hazards. The post hoc Kaplan–Meier estimate of landmark OS at 12 months was 53.7% (95% CI, 47.4 to 59.5) in the durvalumab + EP arm compared to 39.8% (95% CI, 33.7 to 45.8) in the EP arm.
As of the follow-up final analysis (data cut-off: January 27, 2020), 441 deaths had occurred, representing 82.1% maturity for OS overall.7 The median duration of follow-up in censored patients was 25.20 months in the durvalumab + EP group and 23.24 months in the EP-alone group. The median duration of follow-up including patients who died was 12.68 months in the durvalumab + EP group and 10.18 months in the EP-alone group. Median OS was 12.9 months (95% CI, 11.3 to 14.7) in the durvalumab + EP arm compared to 10.5 months (95% CI, 9.3 to 11.2) in the EP arm (HR = 0.75; 95% CI, 0.625 to 0.910; nominal P = 0.0032). Kaplan–Meier curves are depicted in Figure 7 (Appendix 3). The post hoc Kaplan–Meier estimate of landmark OS at 18 months was 32.0% (95% CI, 26.5 to 37.7) in the durvalumab + EP arm compared to 24.8% (95% CI, 19.7, 30.1) in the EP arm. The post hoc Kaplan–Meier estimate of landmark OS at 24 months was 22.2% (95% CI, 17.3, 27.5) in the durvalumab + EP arm versus 14.4% (95% CI, 10.3, 19.2) in the EP arm.
Table 16: Overall Survival in the CASPIAN Trial — ITT Population
Overall survival | Interim analysis (data cut-off: March 11, 2019) | Final analysis (data cut-off: January 27, 2020) | ||
|---|---|---|---|---|
Durvalumab + EP N = 268 | EP N = 269 | Durvalumab + EP N = 268 | EP N = 269 | |
Deaths, n (%) | 155 (57.8) | 181 (67.3) | 210 (78.4) | 231 (85.9) |
Censored patients, n (%) | 113 (42.2) | 88 (32.7) | Not reported | Not reported |
Median OS (95% CI),a months | 13.0 (11.5 to 14.8) | 10.3 (9.3 to 11.2) | 12.9 (11.3 to 14.7) | 10.5 (9.3 to 11.2) |
HR (95% CI)b | 0.73 (0.591 to 0.909) | 0.75 (0.625 to 0.910) | ||
P value | 0.0047 | 0.0032c | ||
OS at 12 months, % (95% CI)d | 53.7 (47.4 to 59.5) | 39.8 (33.7 to 45.8) | 52.8 (46.6 to 58.5) | 39.3 (33.4 to 45.1) |
OS at 18 months, % (95% CI)d | 33.9 (26.9 to 41.0) | 24.7 (18.4 to 31.6) | 32.0 (26.5 to 37.7) | 24.8 (19.7 to 30.1) |
OS at 24 months, % (95% CI)d | NA | NA | 22.2 (17.3 to 27.5) | 14.4 (10.3 to 19.2) |
CI = confidence interval; EP = etoposide-platinum (carboplatin or cisplatin); HR = hazard ratio; ITT = intention-to-treat; NA = not available; OS = overall survival.
aMedian calculated using the Kaplan–Meier technique. CI derived based on the Brookmeyer-Crowley method and using the log-log transformation.
bAn HR less than 1 favours durvalumab + EP. The HRs and CIs were calculated using a stratified Cox proportional hazards model, adjusting for planned platinum therapy (carboplatin or cisplatin) at cycle 1, and ties were handled by the Efron approach.
cNominal P value (i.e., results are non-inferential).
dCalculated post hoc. Median calculated using the Kaplan–Meier technique. CI derived based on the Brookmeyer-Crowley method and using the log-log transformation.
Figure 4: Kaplan–Meier Curves of Overall Survival for the Durvalumab + EP and EP-Alone Arms — ITT Population, Interim Analysis (Data Cut-Off: March 11, 2019)
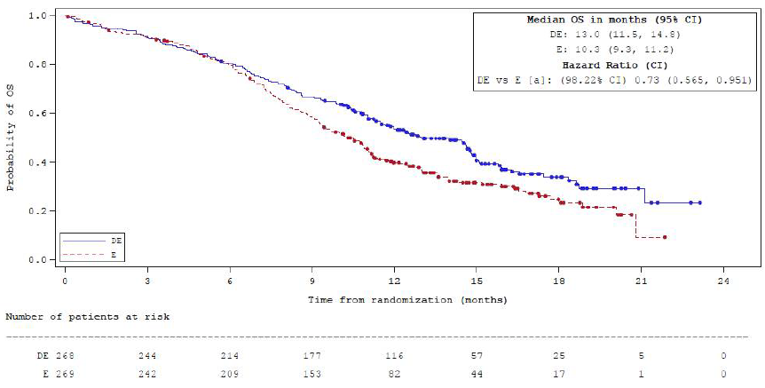
CI = confidence interval; DE = durvalumab in combination with etoposide and either carboplatin or cisplatin; E = etoposide and either carboplatin or cisplatin; OS = overall survival.
Note: A circle indicates a censored observation and 1 month = 30.4375 days.
a Based on a Lan-DeMets alpha spending function with an O’Brien-Fleming boundary with the actual number of events observed; the boundaries for declaring statistical significance are 0.0178 for a 4% overall alpha. Corresponding 95% CIs are shown.
Source: Clinical Study Report.6
In addition, a planned sensitivity analysis was conducted using a Kaplan–Meier plot of time to censoring, with the censoring indicator of OS reversed to assess potential attrition bias. Early censoring (> 10 weeks before data cut-off) was observed for 2 patients (0.7%) in the durvalumab + EP arm compared to 8 patients (3.0%) in the EP arm. This suggests that the potential for attrition bias affecting OS is low.
Results from the pre-specified, exploratory subgroup analysis of OS are summarized in Table 17. The treatment effect on OS was consistent with the primary analysis across the 3 pre-specified patient subgroups of smoking status, baseline ECOG PS, and brain metastases at baseline.
Table 17: Overall Survival Subgroup Analysis — ITT Population, Interim Analysis (Data Cut-Off: March 11, 2019)
Subgroup | Treatment arm | N | Deaths, n (%) | HR (95% CI)a |
|---|---|---|---|---|
Smoking status at screening | ||||
Smoker | Durvalumab + EP | 246 | 141 (57.3) | 0.72 (0.579 to 0.905) |
EP | 254 | 171 (67.3) | ||
Non-smoker | Durvalumab + EP | 22 | 14 (63.6) | 0.90 (0.399 to 2.107) |
EP | 15 | 10 (66.7) | ||
ECOG PS | ||||
0 | Durvalumab + EP | 99 | 51 (51.5) | 0.71 (0.483 to 1.043) |
EP | 90 | 55 (61.1) | ||
1 | Durvalumab + EP | 169 | 104 (61.5) | 0.76 (0.586 to 0.986) |
EP | 179 | 126 (70.4) | ||
Brain metastases at baseline | ||||
Yes | Durvalumab + EP | 28 | 17 (60.7) | 0.69 (0.354 to 1.312) |
EP | 27 | 20 (74.1) | ||
No | Durvalumab + EP | 240 | 138 (57.5) | 0.74 (0.591 to 0.933) |
EP | 242 | 161 (66.5) | ||
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EP = etoposide-platinum (carboplatin or cisplatin); HR = hazard ratio; ITT = intention-to-treat.
aAn HR of less than 1 favours durvalumab + EP and is associated with a longer overall survival compared with EP alone. The HRs and 95% CIs were calculated from an unstratified Cox proportional hazards model with treatment as the only covariate.
Source: Clinical Study Report.6
Exploratory post hoc analyses of OS by PD-L1 expression and tumour mutational burden were conducted for the subset of patients with available and evaluable tissue samples.32 Regarding PD-L1 expression, tumour tissue samples were evaluable for a total of 277 patients (51.6%) in the durvalumab + EP and EP arms. Overall, 94.9% and 77.6% of patients had PD-L1 expression of less than 1% on tumour cells and immune cells, respectively. Due to low PD-L1 expression, a 1% cut-off was used in post hoc analyses. There was no evidence of a statistically significant interaction between PD-L1 expression and OS. Tissue tumour mutational burden was assessed in 283 patients, and results from the exploratory analysis suggested that tumour mutational burden was not predictive of an improvement in OS for durvalumab + EP versus EP alone. Additional data on PD-L1 expression and tumour mutational burden relative to OS are available in Appendix 3 (Figure 8 and Figure 9).
Progression-Free Survival
The investigator-assessed PFS periods in the CASPIAN trial for the durvalumab + EP and EP-alone arms are summarized in Table 18. Median PFS was similar at both the interim and final analysis. As of the interim analysis, median PFS was 5.1 months (95% CI, 4.7 to 6.2) in the durvalumab + EP arm and 5.4 months (95% CI, 4.8 to 6.2) in the EP arm (HR: 0.78; 95% CI, 0.645 to 0.936; nominal P = 0.0078). Kaplan–Meier curves as of the interim analysis are depicted in Figure 6. There was a delay of approximately 6 months in separation of the curves, and the associated log-log plot showed some evidence of non-proportionality of hazards.
As of the final analysis, median PFS was 5.1 months (95% CI, 4.7 to 6.2) in the durvalumab + EP arm and 5.4 months (95% CI, 4.8 to 6.2) in the EP arm (HR = 0.80; 95% CI, 0.665 to 0.959; nominal P = 0.0157). As of the final analysis, the post hoc Kaplan–Meier estimate of landmark PFS at 18 months was 13.9% (95% CI, 10.0 to 18.4) in the durvalumab + EP arm compared to 3.4% (95% CI, 1.6 to 6.4) in the EP arm. The landmark PFS at 24 months was 11.0% (95% CI, 7.5 to 15.2) in the durvalumab + EP arm versus 2.9% (95% CI, 1.2 to 5.8) in the EP arm.
Table 18: Progression-Free Survival by Investigator Assessment — ITT Population
Progression-free survival | Interim analysis (data cut-off: March 11, 2019) | Final analysis (data cut-off: January 27, 2020) | ||
|---|---|---|---|---|
Durvalumab + EP N = 268 | EP N = 269 | Durvalumab + EP N = 268 | EP N = 269 | |
Events, n (%) | 226 (84.3) | 233 (86.6) | 234 (87.3) | 236 (87.7) |
Censored patients, n (%) | 42 (15.7) | 36 (13.4) | Not reported | Not reported |
Median PFS (95% CI), monthsa | 5.1 (4.7 to 6.2) | 5.4 (4.8 to 6.2) | 5.1 (4.7 to 6.2) | 5.4 (4.8 to 6.2) |
HR (95% CI)b | 0.78 (0.645 to 0.936) | 0.80 (0.665 to 0.959) | ||
P valuec | 0.0078 | 0.0157 | ||
PFS at 6 months, % (95% CI)d | 45.4 (39.3 to 51.3) | 45.6 (39.3 to 51.7) | 45.4 (39.3 to 51.3) | 45.8 (39.5 to 51.9) |
PFS at 12 months, % (95% CI)d | 17.5 (13.1 to 22.5) | 4.7 (2.4 to 8.0) | 17.9 (13.5 to 22.8) | 5.3 (2.9 to 8.8) |
PFS at 18 months, % (95% CI)d | NA | NA | 13.9 (10.0 to 18.4) | 3.4 (1.6 to 6.4) |
PFS at 24 months, % (95% CI)d | NA | NA | 11.0 (7.5 to 15.2) | 2.9 (1.2 to 5.8) |
CI = confidence interval; EP = etoposide-platinum (carboplatin or cisplatin); HR = hazard ratio; PFS = progression-free survival.
aMedian calculated using the Kaplan–Meier technique. Derivation of the CI was based on the Brookmeyer-Crowley method and used a log-log transformation.
bAn HR of less than 1 favours durvalumab + EP. The HRs and CIs were calculated using a stratified Cox proportional hazards model, adjusting for planned platinum therapy (carboplatin or cisplatin) at cycle 1, and ties were handled by the Efron approach.
cNominal P value (i.e., results are non-inferential).
dCalculated post hoc using the Kaplan–Meier technique. Derivation of the CI was based on the Brookmeyer-Crowley method and used a log-log transformation.
Figure 5: Kaplan–Meier Curves of PFS for the Durvalumab + EP and EP-Alone Arms in the CASPIAN Trial — ITT Population, Interim Analysis (Data Cut-Off: March 11, 2019)
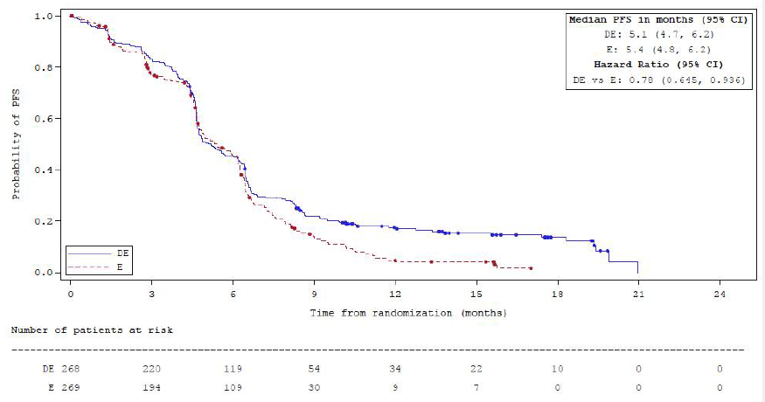
CI = confidence interval; DE = durvalumab in combination with etoposide and either carboplatin or cisplatin; E = etoposide and either carboplatin or cisplatin; PFS = progression-free survival.
Note: A circle indicates a censored observation and 1 month = 30.4375 days.
Source: Clinical Study Report.6
Sensitivity analyses were conducted to assess potential biases, including attrition bias. Fewer patients were censored for PFS in the durvalumab + EP arm (N = 42, 16%) compared to the EP arm (N = 36, 13%).6 The Kaplan–Meier plot of time to censoring showed that patients were censored for PFS earlier in the EP group than were those in the durvalumab + EP group. Eight (3%) patients were early-censored (> 10 weeks before data cut-off) in the durvalumab + EP arm compared to 29 (11%) patients in the EP arm.
Results from the pre-specified, exploratory subgroup analysis of PFS are summarized in Appendix 3 (Table 25). The treatment effect on PFS was consistent with the primary analysis across the 3 pre-specified patient subgroups of smoking status, baseline ECOG PS, and brain metastases at baseline.
Duration of Response
Duration of response was calculated post hoc in the subset of patients that had a confirmed response and results are summarized in Table 19. At both the interim and final analyses, the Kaplan–Meier estimate of median confirmed DOR was 5.1 months (95% CI, 4.9 to 5.3) in the durvalumab + EP arm and 5.1 months (95% CI, 4.8 to 5.3) in the EP arm.6,7 At the final analysis, the Kaplan–Meier estimates of patients remaining in confirmed response at 12 months were 23.2% and 7.3% in the durvalumab + EP and EP-alone arms, respectively. The Kaplan–Meier estimates of patients remaining in confirmed response at 24 months were 13.5% and 3.9% in the durvalumab + EP and EP-alone arms, respectively. Variance was not calculated for the percentage of patients remaining in confirmed response at 12 months and 24 months.
Table 19: Confirmed Duration of Reponses — Confirmed Responders
Duration of response | Interim analysis (data cut-off: March 11, 2019) | Final analysis (data cut-off: January 27, 2020) | ||
|---|---|---|---|---|
Durvalumab + EP N = 268 | EP N = 269 | Durvalumab + EP N = 268 | EP N = 269 | |
Number of confirmed responders who subsequently progressed or died,a n | 146 | 135 | 153 | 138 |
Median DOR (95% CI)a,b | 5.1 (4.9 to 5.3) | 5.1 (4.8 to 5.3) | 5.1 (4.9 to 5.3) | 5.1 (4.8 to 5.3) |
% remaining in response at 12 months (95% CI)a | 22.7 (NR) | 6.3 (NR) | 23.2 (NR) | 7.3 (NR) |
% remaining in response at 24 months (95% CI)a | NA | NA | 13.5 (NR) | 3.9 (NR) |
CI = confidence interval; DOR = duration of response; EP = etoposide-platinum (carboplatin or cisplatin); NA = not applicable; NR = not reported.
bThe CIs for median DOR are derived based on the Brookmeyer-Crowley method using a log-log transformation.
aResponse is determined by the RECIST-based assessment of the investigator.
cCalculated post hoc using the Kaplan–Meier technique.
Objective Response Rate
The investigator-assessed unconfirmed and confirmed ORRs were similar at the interim and final analyses.6,7
As of the interim analysis, the unconfirmed ORRs were 79.5% and 70.3% in the durvalumab + EP and EP arms, respectively (OR = 1.64; 95% CI, 1.106 to 2.443; nominal P = 0.0137). The confirmed ORRs were 67.9% and 57.6% in the durvalumab + EP and EP-alone arms, respectively (OR = 1.56; 95% CI, 1.095 to 2.218; nominal P = 0.0136).
As of the final analysis, the unconfirmed ORRs were 79.5% and 70.6% in the durvalumab + EP and EP-alone arms, respectively (OR = 1.61; 95% CI, 1.086 to 2.401; nominal P = 0.0177). The confirmed ORRs were 67.9% and 58.0% in the durvalumab + EP and EP-alone arms, respectively (OR = 1.53; 95% CI, 1.078 to 2.185; nominal P = 0.0173).
Table 20: Investigator-Assessed ORR per RECIST Version 1.1 — ITT Population
ORR | Interim analysis (data cut-off: March 11, 2019) | Final analysis (data cut-off: January 27, 2020) | ||
|---|---|---|---|---|
Durvalumab + EP N = 268 | EP N = 269 | Durvalumab + EP N = 268 | EP N = 269 | |
Unconfirmed ORR | ||||
Patients with an unconfirmed response, n (%) | 213 (79.5) | 189 (70.3) | 213 (79.5) | 190 (70.6) |
Complete response | 7 (2.6) | 4 (1.5) | NR | NR |
Partial response | 206 (76.9) | 185 (68.8) | NR | NR |
Stable disease | 20 (7.5) | 42 (15.6) | NR | NR |
Odds ratio (95% CI)a,c | 1.64 (1.106 to 2.443) | 1.61 (1.086 to 2.401) | ||
P valued | 0.0137b | 0.0177b | ||
Confirmed ORR | ||||
Patients with a confirmed response, n (%) | 182 (67.9) | 155 (57.6) | 182 (67.9) | 156 (58.0) |
Complete response | 6 (2.2) | 2 (0.7) | NR | NR |
Partial response | 176 (65.7) | 153 (56.9) | NR | NR |
Stable disease | 20 (7.5) | 42 (15.6) | NR | NR |
Odds ratio (95% CI)a,c | 1.56 (1.095 to 2.218) | 1.53 (1.078 to 2.185) | ||
P valued | 0.0136b | 0.0173b | ||
CI = confidence interval; EP = etoposide-platinum (carboplatin or cisplatin); ITT = intention-to-treat; NR = not reported; ORR = objective response rate; RECIST = Response Evaluation Criteria in Solid Tumors.
aAn odds ratio of at least 1 favours durvalumab + EP.
bNominal P value (i.e., results are non-inferential).
cComparisons (vs. EP) were performed using a separate logistic regression model, adjusting for planned platinum therapy (carboplatin or cisplatin) in cycle 1, with a 95% CI calculated by profile likelihood.
dThe P value, derived from a logistic regression model, is based on twice the change in log-likelihood resulting from the addition of a treatment factor to the model.
Health-Related Quality of Life
Results from the EORTC QLQ-C30 and QLQ-L13 were analyzed at the interim analysis.6
Time to deterioration of EORTC QLQ-C30 and QLQ-LC13 scores was assessed in patients whose baseline scores were 10 or higher for functioning and global health status/quality of life and no more than 90 for symptoms. Time to deterioration was calculated as the time from randomization to the first clinically meaningful deterioration at a subsequent assessment, or death from any cause in the absence of clinically meaningful deterioration. The CASPIAN trial defined a clinically meaningful deterioration as an increase of at least 10 points from baseline for symptoms and a decrease of at least 10 points from baseline for function and global health status/quality of life. The MID reported in the literature varied depending on the improvement or deterioration among different items scales. The EORTC QLQ-C30 and QLQ-L13 are described in detail in Appendix 4.
The PRO-evaluable population consisted of 261 patients from the durvalumab + EP arm and 260 patients from the EP-alone arm.6,30 Compliance was defined as the proportion of patients in the PRO-evaluable population for whom data were available at each time point. Compliance rates for EORTC QLQ-C30 and QLQ-L13 were highest at baseline (≥ 94%) and similar between the durvalumab + EP and EP-alone groups for the first 9 weeks (≥ 78%).6 Compliance rates for both groups decreased over time and were generally lower in the EP group. Compliance rates of greater than 60% were observed for up to 84 weeks in the durvalumab + EP group, and for up to 20 weeks in the EP group.
Baseline EORTC QLQ-C30 and QLQ-LC13 scores are summarized in Appendix 3 (Table 26). Baseline scores were comparable between study groups.6
Times to deterioration in EORTC QLQ-C30 and QLQ-L13 scales are summarized in Figure 6 and Appendix 3 (Table 27). Median time to deterioration nominally longer in the durvalumab + EP arm compared to the EP-alone arm were observed for all function scales (physical, role, emotional, cognitive, and social).6 Median time to deterioration was also nominally longer in the durvalumab + EP arm compared to the EP arm for the symptoms of dyspnea, insomnia, appetite loss, constipation, diarrhea, hemoptysis, chest pain, arm/shoulder pain, and other pain.
Figure 6: Forest Plot of Time to Deterioration of EORTC QLQ-C30 and QLQ-L13 Scores — PRO-Evaluable Population, Interim Analysis (Data Cut-Off: March 11, 2019)
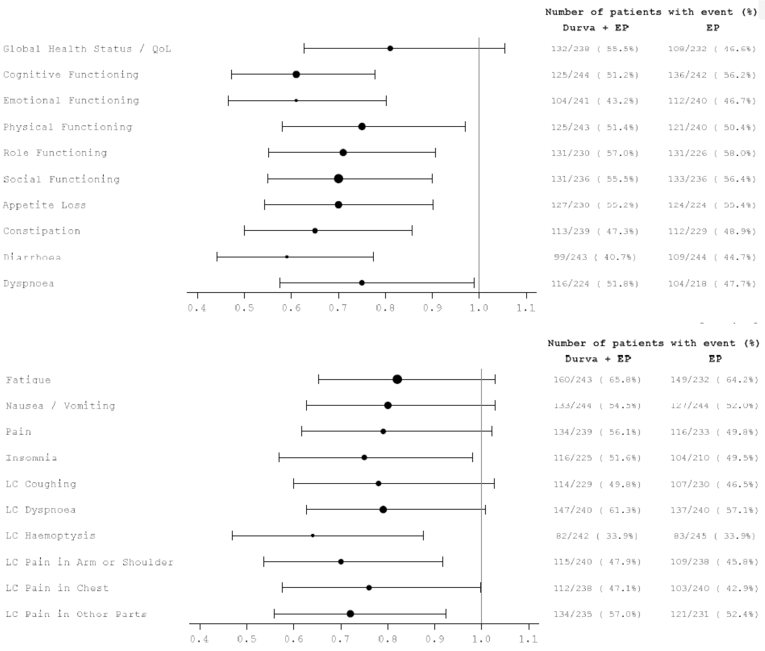
Durva = durvalumab; EP = etoposide-platinum (carboplatin or cisplatin); PRO = patient-reported outcome; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire; QoL = quality of life.
Source: Clinical Study Report.6
Symptoms
Results from the EORTC QLQ-C30 and QLQ-L13 were analyzed at the interim analysis.6
Table 21 presents the results from the MMRM analysis of EORTC QLQ-C30 and QLQ-LC13 key symptoms from baseline to PD or 12 months. The predefined key symptoms were cough, dyspnea, and chest pain (as assessed by EORTC QLQ-LC13), and fatigue and appetite loss (as assessed by EORTC QLQ-C30). The CASPIAN trial defined a clinically meaningful difference as an absolute change in the score from baseline of at least 10 points. The MID reported in the literature varies depending on the improvement or deterioration among different items scales. The EORTC QLQ-C30 and QLQ-L13 are described in detail in Appendix 4.
For appetite loss, the adjusted mean change from baseline in appetite loss score was −12.7 points in the durvalumab + EP arm.6 The estimated difference between treatment arms for appetite loss was −4.5 (95% CI, −9.04 to −0.04; P = 0.009) in favour of durvalumab + EP. No significant differences between treatment arms were observed for the symptoms of fatigue, cough, dyspnea, and chest pain.
Table 21: MMRM Analysis of Adjusted Mean Change From Baseline to PD or 12 Months in Key Symptoms From the EORTC QLQ-C30 and QLQ-LC13 — PRO-Evaluable Population, Interim Analysis (Data Cut-Off: March 11, 2019)
Symptom scale item (instrument) | Durvalumab + EP N = 261 | EP N = 260 |
|---|---|---|
Cough (QLQ-LC13) | ||
Number of patients contributing to the analysis | 231 | 232 |
Adjusted mean change from baselinea | −17.1 | −17.1 |
Standard error | 1.71 | 2.10 |
95% CI | −20.43 to −13.71 | −21.21 to −12.96 |
Estimated difference (99% CI)b | 0.0 (−5.25 to 5.29) | |
P valuec | 0.992 | |
Dyspnea (QLQ-LC13) | ||
Number of patients contributing to the analysis | 231 | 232 |
Adjusted mean change from baselinea | −8.6 | −8.0 |
Standard error | 1.44 | 1.64 |
95% CI | −11.40 to −5.76 | −11.26 to −4.81 |
Estimated difference (99% CI)b | −0.5 (−4.38 to 3.29) | |
P valuec | 0.714 | |
Chest pain (QLQ-LC13) | ||
Number of patients contributing to the analysis | 231 | 232 |
Adjusted mean change from baselinea | −8.1 | −9.4 |
Standard error | 1.59 | 1.85 |
95% CI | −11.27 to −5.01 | −13.04 to −5.75 |
Estimated difference (99% CI)b | 1.3 (−3.20 to 5.71) | |
P valuec | 0.465 | |
Fatigue (EORTC QLQ-C30) | ||
Number of patients contributing to the analysis | 232 | 233 |
Adjusted mean change from baselinea | −7.4 | −5.6 |
Standard error | 1.64 | 1.87 |
95% CI | −10.67 to −4.22 | −9.24 to −1.88 |
Estimated difference (99% CI)b | −1.9 (−6.28 to 2.51) | |
P valuec | 0.268 | |
Appetite loss (EORTC QLQ-C30) | ||
Number of patients contributing to the analysis | 232 | 233 |
Adjusted mean change from baselinea | −12.7 | −8.2 |
Standard error | 1.65 | 1.94 |
95% CI | −15.95 to −9.47 | −11.98 to −4.36 |
Estimated difference (99% CI)b | −4.5 (−9.04 to −0.04) | |
P valuec | 0.009 | |
CI = confidence interval; EORTC = European Organisation for Research and Treatment of Cancer; EP = etoposide-platinum (carboplatin or cisplatin); PRO = patient-reported outcome; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire.
Note: Includes data up to progressive disease or 12 months (whichever is earlier), excluding visits with excessive missing data (defined as more than 75% missing data). Change from baseline was analyzed separately for each treatment comparison using an MMRM model, based on restricted maximum likelihood method, with patient, treatment, age at randomization (< 65 years, ≥ 65 years), sex (male, female), smoking status at screening (smoker, non-smoker), visit and treatment by visit interaction as fixed factors, and the appropriate baseline and baseline by visit interaction as covariates. For all subscales and items, a Toeplitz with heterogeneity covariance structure was used to model the within-patient error and the Kenward-Roger approximation was used to estimate the degrees of freedom.
aAdjusted mean represents the change from baseline.
bAn estimated difference less than 0 favours durvalumab + EP over EP alone.
cThe overall 2-sided 5% alpha is controlled across the 5 key symptoms using the Bonferroni-adjusted procedure (1% significance level for each end point).
Source: Clinical Study Report.6
Harms
Only those harms identified in the review protocol for the durvalumab + EP and EP-alone arms of the CASPIAN trial are reported below. See Table 22 for detailed harms data. Harms data for the durvalumab + tremelimumab + EP arm are available in Appendix 3 (Table 30).
Adverse Events
A total of 260 patients (98.1%) in the durvalumab + EP arm and 258 patients (97.0%) in the EP-alone arm experienced an AE.7 The most commonly reported AEs in the durvalumab + EP and EP-alone arms were neutropenia (41.9% and 46.6%, respectively), anemia (38.5% and 47.0%, respectively), nausea (33.6% and 33.5%, respectively), and alopecia (31.7% and 34.2%, respectively). A greater proportion of patients (≥ 5% difference between groups) in the durvalumab + EP arm compared to the EP-alone arm experienced hyperthyroidism (9.8% versus 0.4%, respectively), hypothyroidism (9.4% versus 1.5%, respectively), cough (12.5% versus 6.8%, respectively), and hyponatremia (9.8% versus 4.5%, respectively). Anemia was reported at a lower proportion in the durvalumab + EP arm compared with the EP-alone arm (38.5% versus 47.0%, respectively).
Serious Adverse Events
Overall, 34% of patients in the durvalumab + EP and EP arms of the CASPIAN trial experienced an SAE.7 A greater number of SAEs were reported in the EP arm (N = 97, 36.5%) compared to the durvalumab + EP arm (N = 84, 32.1%). The most commonly reported SAEs in the durvalumab + EP and EP-alone arms were febrile neutropenia (4.5% and 4.5%, respectively), anemia (1.9% and 4.5%, respectively), pneumonia (2.3% and 3.4%, respectively), and thrombocytopenia (0.4% and 3.4%, respectively).
Withdrawals Due to Adverse Events
Withdrawals specifically due to AEs were not reported.6,7 Withdrawals due to AEs in general in the CASPIAN trial are summarized in Table 11. A total of 4 patients (1.5%) in durvalumab + EP arm and 12 patients (2.5%) in the EP arm left the study due to withdrawal.7 Adverse events led to discontinuation of study treatment in 27 (10.2%) patients in the durvalumab + EP arm and 25 (9.4%) patients in the EP arm.
Mortality
As of the final analysis, 210 patients (78.4%) in durvalumab + EP arm and 231 patients (85.9%) in EP arm had died.7 The majority of deaths were attributed to ES-SCLC in both treatment arms: 189 patients (71.3%) in the durvalumab + EP arm and 200 patients (75.1%) in the EP arm.
Notable Harms
As of the final analysis, 141 patients (53.2%) in the durvalumab + EP arm and 104 patients (39.1%) in the EP arm experienced an immune-related AE. The most frequently reported immune-related AEs in the durvalumab + EP arm were endocrine (n = 75, 28.3%) and dermatitis/rash (n = 51, 19.2%). The most frequently reported immune-related AEs in the EP arm were diarrhea/colitis (n = 31, 11.7%) and dermatitis/rash (n = 25, 9.4%). A greater proportion of patients (≥ 5% difference between groups) in the durvalumab + EP arm compared to the EP arm experienced hepatic (14.0% versus 7.9%, respectively), endocrine (28.3% versus 6.8%, respectively), and dermatitis/rash (19.2% versus 9.4%, respectively) immune-related AEs. Furthermore, a greater proportion of patients (≥ 5% difference between groups) in the durvalumab + EP arm compared to the EP-alone arm received systemic corticosteroids (11.7% versus 2.6%), high-dose steroids (8.3% versus 1.1%), and endocrine therapy (16.6% versus 3.4%).
Five patients in the durvalumab + EP arm and 3 patients in the EP arm experienced an infusion-related reaction. Three patients in durvalumab + EP arm and 2 patients in the EP arm experienced hypersensitivity/anaphylactic reactions.
Ninety-three patients (35.1%) in the durvalumab + EP arm and 82 patients (30.8%) in the EP arm experienced an infection.
Table 22: Summary of Harms in CASPIAN Trial — Safety Population, Final Analysis (Data Cut-Off: January 27, 2020)
Harms | Durvalumab + EP N = 265 | EP N = 266 |
|---|---|---|
Patients with ≥ 1 adverse event | ||
Patients with any AE, n (%) | 260 (98.1) | 258 (97.0) |
Most common events,a n (%) | ||
Neutropenia | 111 (41.9) | 124 (46.6) |
Anemia | 102 (38.5) | 125 (47.0) |
Nausea | 89 (33.6) | 89 (33.5) |
Alopecia | 84 (31.7) | 91 (34.2) |
Constipation | 45 (17.0) | 51 (19.2) |
Decreased appetite | 48 (18.1) | 46 (17.3) |
Thrombocytopenia | 41 (15.5) | 53 (19.9) |
Fatigue | 48 (18.1) | 45 (16.9) |
Vomiting | 39 (14.7) | 44 (16.5) |
Leukopenia | 40 (15.1) | 32 (12.0) |
Asthenia | 42 (15.8) | 40 (15.0) |
Patients with ≥ 1 SAE | ||
n (%) | 85 (32.1) | 97 (36.5) |
Most common events,b n (%) | ||
Febrile neutropenia | 12 (4.5) | 12 (4.5) |
Anemia | 5 (1.9) | 12 (4.5) |
Pneumonia | 6 (2.3) | 9 (3.4) |
Thrombocytopenia | 1 (0.4) | 9 (3.4) |
Neutropenia | 2 (0.8) | 7 (2.6) |
Pancytopenia | 4 (1.5) | 3 (1.1) |
Hyponatremia | 2 (0.8) | 4 (1.5) |
Pneumonitis | 3 (1.1) | 3 (1.1) |
Diarrhea | 1 (0.4) | 4 (1.5) |
Patients who stopped treatment due to adverse events | ||
n (%) | 27 (10.2) | 25 (9.4) |
Deaths | ||
n (%) | 210 (78.4) | 231 (85.9) |
Attributed to ES-SCLC onlyc | 189 (71.3) | 200 (75.1) |
AEs with an outcome of death | 13 (4.9) | 15 (5.6) |
Unknown cause | 9 (3.4) | 12 (4.5) |
Notable harms | ||
Immune-related AEs, n (%) | 141 (53.2) | 104 (39.1) |
Pneumonitis | 9 (3.4) | 5 (1.9) |
Hepatic | 37 (14.0) | 21 (7.9) |
Diarrhea/colitis | 30 (11.3) | 31 (11.7) |
Endocrine | 75 (28.3) | 18 (6.8) |
Hypothyroid | 26 (9.8) | 4 (1.5) |
Hyperthyroid | 27 (10.2) | 1 (0.4) |
Thyroiditis | 4 (1.5) | 0 |
Adrenal insufficiency | 3 (1.1) | 0 |
Type I diabetes mellitus | 15 (5.7) | 13 (4.9) |
Renal | 8 (3.0) | 6 (2.3) |
Dermatitis/rash | 51 (19.2) | 25 (9.4) |
Myocarditis | 0 | 1 (0.4) |
Pancreatic | 17 (6.4) | 9 (3.4) |
Arthritis | 2 (0.8) | 0 |
Received systemic corticosteroids | 31 (11.7) | 7 (2.6) |
Received high-dose steroids | 22 (8.3) | 3 (1.1) |
Received endocrine therapy | 44 (16.6) | 9 (3.4) |
Infusion-related reactions, n (%) | 5 (1.9) | 3 (1.1) |
Infusion-related reaction | 4 (1.5) | 3 (1.1) |
Urticaria | 1 (0.4) | 0 |
Hypersensitivity/anaphylactic reactions, n (%) | 3 (1.1) | 2 (0.8) |
Infection, n (%) | 93 (35.1) | 82 (30.8) |
AE = adverse event; EP = etoposide-platinum; ES-SCLC = extensive-stage small cell lung cancer; SAE = serious adverse event.
aFrequency greater than 15%.
bFrequency of at least 5 patients.
cDeaths were attributed by the investigator to ES-SCLC.
Source: Clinical Study Report.7
Critical Appraisal
Internal Validity
In general, the CASPIAN trial was a well-designed and well-conducted RCT. The sample size was adequate, and a stratified randomization procedure based on the type of platinum-based chemotherapy was used. Most efficacy analyses (including OS and PFS) were conducted according to the ITT principle. Subgroup analyses of OS and PFS (ECOG PS, smoking history, and brain metastases at baseline) were specified a priori. However, they were not adjusted for multiplicity and should therefore be considered exploratory. Treatment exposure was adequate to evaluate the safety and tolerability of durvalumab and EP, although treatment discontinuation rates were high. There was extremely little loss to follow-up and patients were followed for survival for up to 2 years. Treatment groups were generally well balanced. The differences in prognostic baseline characteristics (e.g., brain metastases, ECOG PS) between the 3 treatment arms were considered minor and unlikely to have a significant effect on outcomes, according to the clinical experts consulted by CADTH. There was an imbalance in prior radiotherapy between groups. However, the clinical experts advised that this was unlikely to influence clinical outcomes due to the small numbers of patients relative to the study sample size.
Four protocol amendments were implemented in the trial, including multiple changes to the primary objective and primary end points of the trial after randomization of all study patients was complete. Progression-free survival was originally a co-primary end point but was then changed to the key secondary end point. This may have introduced bias into the trial. In addition, blinded central review to determine PD for PFS was removed, and PD was then determined by investigator assessment. Removal of a blinded review could introduce bias into a trial, particularly as it was done after enrolment. The changes in objectives and end points were accompanied by changes to the multiple testing procedure and alpha spending, which could have introduced further bias. The direction of the bias introduced by the multiple protocol amendments is unclear.
The open-label design of the trial makes it prone to different biases. The primary outcome of the CASPIAN trial, OS, is an objective outcome and reporting of deaths are unlikely to be influenced. However, the way in which patients are treated throughout the study could be influenced by knowledge of treatment assignment and impact OS. The direction of the effect of this potential bias on OS is unknown. In addition, the open-label design could potentially affect study conduct and secondary outcomes, such as investigator assessment of response and disease progression (PFS, DOR, and ORR), patient withdrawals, patient-reported symptoms, and HRQoL. Outcomes that rely on investigator assessments may have been biased, but the direction of bias is unknown. The open-label design also may have affected AE reporting, but the direction of bias is unknown. Despite this, the clinical experts consulted by CADTH noted that maintaining blinding can be challenging in immunotherapy trials because the profile of AEs (e.g., dermatitis/rash and thyroid dysfunction) can reveal which treatment the patient is receiving.
In the CASPIAN trial, a multiple testing procedure was applied to control the overall type I error rate for OS and PFS at 5%. The CASPIAN trial met its primary end point for OS at the interim analysis, which indicated a survival benefit with the addition of durvalumab to EP. The treatment effect of durvalumab on OS was generally observed across patient subgroups as well. Furthermore, the PFS results generally support the observed treatment effect of durvalumab on OS and the results of the subgroup analysis of PFS were also consistent. However, the PFS results are associated with substantial uncertainty. It was not possible to formally test PFS for statistical significance within the multiple testing procedure at either the interim or final analysis. The primary end point of OS was met for the durvalumab + EP versus EP-alone arm, but both this and the durvalumab + tremelimumab + EP versus EP-alone analysis needed to be significant before PFS could be tested. As the latter was not, the results for PFS must be considered with regards to potential type I error. In addition, sensitivity analyses of PFS indicated a potential effect of attrition bias. For the analysis of both OS and PFS, the HRs and CIs were calculated using a stratified Cox proportional hazards model, adjusting for planned platinum therapy (carboplatin or cisplatin) at cycle 1. Kaplan–Meier plots of OS and PFS showed a 6-month delay in separation of the curves, providing some evidence of non-proportionality. This affects the validity of the Cox regression models used to analyze OS and PFS in the trial. Furthermore, because landmark OS and PFS were calculated post hoc, these results should be considered exploratory.
After experiencing disease progression, patients were offered standard chemotherapy per study protocol. Patients may also have received subsequent anticancer treatments after discontinuing the study. The OS data could be confounded by subsequent treatments. Subsequent chemotherapy was balanced between the durvalumab + EP and EP-alone treatment arms. There is a potential confounding effect of PCI, which was permitted only in the EP arm. A greater proportion of patients in the EP arm received subsequent radiotherapy. The radiotherapy imbalance may have biased results in favour of the EP arm. However, the clinical experts consulted by CADTH indicated that the subsequent treatments were unlikely to have a significant effect on OS.
Symptoms and HRQoL were analyzed at the interim analysis only. Overall type I error was controlled using the Bonferroni-adjusted procedure for the MMRM analysis of 5 key symptoms (cough, dyspnea, chest pain, fatigue, and appetite loss) assessed by the EORTC QLQ-C30 and QLQ-LC13. Results showed a statistically significant difference in favour of durvalumab + EP for appetite loss, but not for the other symptoms. Because this analysis was controlled for multiplicity, the results can be regarded with greater confidence.
As the time to deterioration analysis of the EORTC QLQ-C30 and QLQ-LC13 subscales was not controlled for multiplicity, results for HRQoL must be considered with regards to potential type I error, although the time to deterioration analysis results generally suggest that the addition of durvalumab to EP was beneficial to delaying deterioration in HRQoL compared to EP alone. Interpretation of the HRQoL and symptom results is limited by the divergence in compliance rates (i.e., completion of the questionnaires) between the treatment arms. The sample size in the EP arm was markedly lower than that in the durvalumab + EP arm from approximately week 24 onward, although the direction of bias remains unclear.
Because there was no adjustment for multiplicity for ORR and DOR, results must be considered with regards to potential type I error. In addition, confirmation of response was not required by the study protocol, which limits interpretation of the ORR as this may have introduced bias into the results, although the direction of bias is unclear. This also affects DOR, which was calculated post hoc in confirmed responders only. As a result of these factors, substantial uncertainty is associated with the secondary outcome results and interpretation of the data is limited.
External Validity
The assigned treatment in the EP arm of the CASPIAN trial was an appropriate comparator because it is reflective of current Canadian practice. In the durvalumab + EP arm, the dosage and administration schedule of durvalumab + first-line EP aligns with the Health Canada–approved dosing and the anticipated use of durvalumab in clinical practice, according to the clinical experts consulted by CADTH. The platinum component of EP in both treatment arms of interest included either carboplatin or cisplatin, as chosen by the investigator, which also reflects Canadian practice. However, a greater proportion of CASPIAN patients received carboplatin than would be expected in Canadian practice, according to the clinical experts consulted by CADTH.
Duration of follow-up was adequate to evaluate the efficacy and safety of durvalumab and EP. The final analysis provides a median follow-up of greater than 2 years.
The enrolled study population is generally representative of Canadian patients with ES-SCLC. The CASPIAN trial included patients with brain metastases at baseline, which is common in patients with ES-SCLC. However, the clinical experts consulted by CADTH identified some differences between the study population and Canadian ES-SCLC patients. For example, the CASPIAN trial patient population included a greater proportion of non-smokers than is seen in Canadian clinical practice. In addition, enrolment was limited to patients with an ECOG PS of 0 or 1, which does not reflect the Canadian ES-SCLC patient population. The clinical experts advised that Canadian patients with ES-SCLC often have a higher ECOG PS (≥ 2) at baseline. As the CASPIAN study population had a lower ECOG PS at baseline, it is possible that these patients would have better outcomes than patients with higher baseline ECOG PS records. However, the clinical experts noted that classification of ECOG PS is subjective, and a patient’s ECOG PS often improves after the first cycle of chemotherapy. The CASPIAN trial did not enroll any patients from Canada.
Indirect Evidence
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Discussion
Summary of Available Evidence
The systematic review of durvalumab in combination with EP for the first-line treatment of ES-SCLC included a single phase III RCT. The CASPIAN study (N = 805) was an international, multi-centre, phase III, open-label, RCT conducted to investigate the efficacy and safety of durvalumab, with or without tremelimumab, in combination with EP compared to EP alone as a first-line treatment regimen in adult patients with ES-SCLC. Patients were randomized in a 1:1:1 ratio to 3 treatment arms: durvalumab + tremelimumab + EP, durvalumab + EP, and EP alone. Randomization was stratified by the planned platinum drug (i.e., cisplatin or carboplatin). Data for the durvalumab + tremelimumab + EP arm of the CASPIAN trial were not included in the CADTH systematic review because the combination is not aligned with the Health Canada product monograph. The primary outcome of the CASPIAN trial was OS, and the key secondary outcome was PFS. Secondary outcomes included DOR, ORR, and HRQoL/symptoms (assessed by the EORTC QLQ-C30 and QLQ-LC13).
Most patients enrolled in the CASPIAN trial were male, White, smokers with a small cell carcinoma (combined) histology type, and an ECOG PS of 1. The mean age of all patients was 62.6 years. Small proportions of patients had received previous chemotherapy and radiotherapy.
No indirect treatment comparisons or other evidence were included in the sponsor’s submission to CADTH or identified in the literature search.
Interpretation of Results
Efficacy
Overall survival was considered the most important outcome by the clinical experts and clinician groups consulted by CADTH. Prolonging survival is also important to patients. The CASPIAN trial met its primary end point of OS for durvalumab + EP versus EP at the planned interim analysis. Durvalumab + EP demonstrated a statistically significant improvement in OS versus EP. Median OS was 2.7 months longer in the durvalumab + EP arm compared to the EP arm, which was considered clinically meaningful by the clinical experts consulted by CADTH. Kaplan–Meier curves showed a delay of approximately 6 months in separation, providing some evidence of non-proportionality of hazards. This affects the validity of the Cox regression model used in the trial. The subgroup analysis (smoking status, ECOG PS at baseline, and brain metastases at baseline) of OS was consistent with the primary analysis. The final follow-up analysis continued to show a similar improvement in OS with durvalumab + EP compared to EP. The OS benefits were observed against those of a control group that allowed PCI and up to 6 cycles of EP, compared to the 4 cycles allowed in the durvalumab + EP arm, which may have biased results in favour of EP.
The clinical experts consulted by CADTH and the clinician groups reported that the tail end of the Kaplan–Meier survival curves and landmark survival rates were important to the interpretation of study results. Landmark survival was calculated post hoc. The results generally suggest that the addition of durvalumab to EP may be beneficial compared to EP alone. However, the landmark survival analyses in the CASPIAN trial are considered exploratory, and these end points are associated with uncertainty due to the small number of patients alive at these time points. Furthermore, there was no hypothesis testing of these time points. For these reasons, the landmark survival results should be interpreted with caution.
Progression-free survival was the key secondary outcome of the CASPIAN trial. The patient groups that provided input on this review reported that delaying disease progression and prolonging survival is important to patients. The multiple testing procedure required OS to reach statistical significance for the analysis of the durvalumab + EP arm versus the EP arm and for the durvalumab + tremelimumab + EP versus EP-alone arms before stepping down to PFS. Because the latter was not met, PFS was not formally tested for statistical significance and the results for PFS must be considered with regards to potential for type I error. In addition, Kaplan–Meier curves showed a delay of approximately 6 months in separation, suggesting non-proportionality of hazards, and sensitivity analyses indicated potential attrition bias. Therefore, PFS results are associated with substantial uncertainty and must be interpreted with caution. Although the PFS results are uncertain, they were generally congruent with the OS results and the HRs suggested that the addition of durvalumab may be beneficial over EP alone. The landmark PFS rates generally suggested that the addition of durvalumab to EP may be beneficial compared to EP alone, but these analyses are exploratory, associated with a substantial degree of uncertainty due to the small number of patients alive at these time points, and lack hypothesis testing.
Objective response rate and DOR were secondary outcomes in the CASPIAN trial. The patient groups that provided input on this review reported that patients want treatments that provide longer-lasting and durable disease response, which aligns with these outcomes. Median DORs were equal in both treatment arms at both analyses, although the percentage of patients remaining in response at 12 and 24 months suggests that durvalumab + EP may be beneficial compared to EP alone. The ORs calculated for the unconfirmed and confirmed ORRs at both analyses also suggest that the addition of durvalumab may be beneficial over EP alone. However, interpretation of the ORR and DOR is limited as they were not controlled for multiplicity, and analysis of the DOR was post hoc.
Symptoms and HRQoL were evaluated as secondary outcomes in the CASPIAN trial. The patient groups that provided input for this review identified improving symptoms and delaying deterioration in HRQoL as important. Symptoms and HRQoL were analyzed at the interim analysis only, and the MMRM analysis of the 5 key symptoms was controlled for type I error. In the durvalumab + EP arm, the adjusted mean change from baseline in the appetite loss symptom score met the MID, and the difference between treatment arms was statistically significant.
Analysis of the time to deterioration in the function and symptom scales of the EORTC QLQ-C30 and QLQ-LC13 suggests that the addition of durvalumab may be beneficial over EP alone. However, the lack of adjustment for multiplicity means this analysis should be considered exploratory and interpreted with caution. Interpretation of the HRQoL and symptom results is also limited by the divergence in compliance rates between the treatment arms.
Harms
Almost all study participants reported treatment-emergent AEs. The most common AEs in both the durvalumab + EP and EP arms were hematological events (neutropenia and anemia), nausea, and alopecia. The clinical experts consulted by CADTH indicated that these AEs were reflective of the EP component of treatment. A greater proportion of patients died in the EP arm compared to the durvalumab + EP arm. The frequency of SAEs was also greater in the EP arm. The clinical experts consulted by CADTH noted that the greater frequency of SAEs in the EP arm may have been due to the higher number of cycles received (i.e., up to 6 cycles of chemotherapy in the EP arm versus a maximum of 4 cycles in the durvalumab + EP arm).
Notable harms in the review included immune-related AEs, infusion-related reactions, hypersensitivity/anaphylactic reactions, and infections. Immune-related AEs were more frequent in the durvalumab + EP arm compared to the EP arm. The most common immune-related AEs were endocrine-related issues and dermatitis/rash, which is consistent with the safety and tolerability profile of durvalumab, according to the clinical experts. Furthermore, the clinical experts consulted by CADTH reported that the immune-related AE profile was expected and consistent with other immune checkpoint inhibitors. A small number of patients in each treatment arm experienced infusion-related reactions and hypersensitivity/anaphylactic reactions. More patients in the durvalumab + EP arm experienced infection.
Conclusions
One phase III, open-label, active-controlled RCT (CASPIAN) provided direct evidence regarding the efficacy and safety of durvalumab in combination with EP in adult patients with ES-SCLC relative to EP alone. Compared to EP, patients who were treated with durvalumab + EP showed benefits in OS. The difference in median OS between treatment arms (2.7 months) was considered statistically significant and clinically relevant by the clinical experts consulted by CADTH. The results suggest that the addition of durvalumab to EP was associated with an improvement in PFS compared to EP alone, but this finding is associated with substantial uncertainty because of the inability to conduct formal statistical tests within the trial’s multiple testing procedure, evidence of non-proportionality of hazards, potential attrition bias, and introduction of bias by the removal of blinded independent central review after enrolment was complete. The effects of durvalumab on the ORR and DOR are also uncertain due to the lack of control for multiplicity, and the DOR was calculated post hoc in confirmed responders only when confirmation of response was not required by the study protocol. The results of the time to deterioration in HRQoL and symptoms suggest that durvalumab + EP may have a beneficial effect, but this remains uncertain due a lack of control for multiplicity and differences in completion rates of the EORTC QLQ-C30 and QLQ-LC13 between treatment arms. The results of the symptom analysis suggest that adding durvalumab to EP may have a benefit in terms of appetite loss compared to EP alone. Almost all study participants reported treatment-emergent AEs. Durvalumab + EP was related to more immune-mediated AEs compared to EP alone, although the profile and incidence rates of these AEs was expected, according to the clinical experts consulted by CADTH. Infusion-related and hypersensitivity/anaphylactic reactions were uncommon, and the incidence of infections was similar in both treatment arms.
References
1.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics: A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-cancer-statistics-2020_special-report_EN.pdf?la=en&la=en. Accessed 2020 Oct 8.
2.Dawe DE, Pond GR, Ellis PM. Assessment of referral and chemotherapy treatment patterns for elderly patients with non-small-cell lung cancer. Clin Lung Cancer. 2016;17(6):563-572. PubMed
3.Doherty J, Dawe DE, Pond GR, Ellis PM. The effect of age on referral to an oncologist and receipt of chemotherapy among small cell lung cancer patients in Ontario, Canada. J Geriatr Oncol. 2019;10(3):449-458. PubMed
4.Small cell lung cancer: extensive stage. Edmonton (AB): Alberta Health Services; 2012: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lu007-lcsc-extens-stage.pdf Accessed 2021 Feb 25.
5.Imfinzi (durvalumab): concentrate for solution for infusion, 50 mg / mL, intravenous [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2020 Sep 21.
6.Clinical Study Report: D419QC00001. A phase III, randomized, multicenter, open-label, comparative study to determine the efficacy of durvalumab or durvalumab and tremelimumab in combination with platinum-based chemotherapy for the first-line treatment in patients with extensive disease small-cell lung cancer (SCLC) (CASPIAN) (interim analysis) [internal sponsor's report]. Gainthersburg (MD): AstraZeneca; 2019 Sep 5.
7.Clinical Study Report: D419QC00001. A phase III, randomized, multicenter, open-label, comparative study to determine the efficacy of durvalumab or durvalumab and tremelimumab in combination with platinum-based chemotherapy for the first-line treatment in patients with extensive disease small-cell lung cancer (SCLC) (CASPIAN) (updated analysis) [internal sponsor's report]. Gaithersburg (MD): AstraZeneca; 2020 Aug 26.
8.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30A(5):635-642. PubMed
9.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
10.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2019. Toronto (ON): Canadian Cancer Society; 2019: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2019-EN.pdf?la=en&la=en. Accessed 2020 Oct 8.
11.Popat S, Kim HR, Ahn MJ, et al. Intracranial efficacy of brigatinib (BRG) vs crizotinib (CRZ) in the phase III ALTA-1L trial. Ann Oncol. 2018;29(Suppl 8):viii746.
12.Micke P, Faldum A, Metz T, et al. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer--what limits limited disease? Lung Cancer. 2002;37(3):271-276. PubMed
13.Shepherd FA, Crowley J, Van Houtte P, et al. The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. J Thorac Oncol. 2007;2(12):1067-1077. PubMed
14.Barnes H, See K, Barnett S, Manser R. Surgery for limited-stage small-cell lung cancer. Cochrane Database Syst Rev. 2017;4(4):CD011917. PubMed
15.Rudin CM, Ismaila N, Hann CL, et al. Treatment of small-cell lung cancer: American Society of Clinical Oncology endorsement of the American College of Chest Physicians guideline. J Clin Oncol. 2015;33(34):4106-4111. PubMed
16.Fukuoka M, Furuse K, Saijo N, et al. Randomized trial of cyclophosphamide, doxorubicin, and vincristine versus cisplatin and etoposide versus alternation of these regimens in small-cell lung cancer. J Natl Cancer Inst. 1991;83(12):855-861. PubMed
17.Roth BJ, Johnson DH, Einhorn LH, et al. Randomized study of cyclophosphamide, doxorubicin, and vincristine versus etoposide and cisplatin versus alternation of these two regimens in extensive small-cell lung cancer: a phase III trial of the Southeastern Cancer Study Group. J Clin Oncol. 1992;10(2):282-291. PubMed
18.O'Brien ME, Ciuleanu TE, Tsekov H, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol. 2006;24(34):5441-5447. PubMed
19.von Pawel J, Jotte R, Spigel DR, et al. Randomized phase III trial of amrubicin versus topotecan as second-line treatment for patients with small-cell lung cancer. J Clin Oncol. 2014;32(35):4012-4019. PubMed
20.Chute JP, Chen T, Feigal E, Simon R, Johnson BE. Twenty years of phase III trials for patients with extensive-stage small-cell lung cancer: perceptible progress. J Clin Oncol. 1999;17(6):1794-1801. PubMed
21.Feld R, Evans WK, Coy P, et al. Canadian multicenter randomized trial comparing sequential and alternating administration of two non-cross-resistant chemotherapy combinations in patients with limited small-cell carcinoma of the lung. J Clin Oncol. 1987;5(9):1401-1409. PubMed
22.Murray N, Livingston RB, Shepherd FA, et al. Randomized study of CODE versus alternating CAV/EP for extensive-stage small-cell lung cancer: an Intergroup Study of the National Cancer Institute of Canada Clinical Trials Group and the Southwest Oncology Group. J Clin Oncol. 1999;17(8):2300-2308. PubMed
23.Leyvraz S, Pampallona S, Martinelli G, et al. A threefold dose intensity treatment with ifosfamide, carboplatin, and etoposide for patients with small cell lung cancer: a randomized trial. J Natl Cancer Inst. 2008;100(8):533-541. PubMed
24.Niell HB, Herndon JE, 2nd, Miller AA, et al. Randomized phase III intergroup trial of etoposide and cisplatin with or without paclitaxel and granulocyte colony-stimulating factor in patients with extensive-stage small-cell lung cancer: cancer and Leukemia Group B Trial 9732. J Clin Oncol. 2005;23(16):3752-3759. PubMed
25.Humblet Y, Symann M, Bosly A, et al. Late intensification chemotherapy with autologous bone marrow transplantation in selected small-cell carcinoma of the lung: a randomized study. J Clin Oncol. 1987;5(12):1864-1873. PubMed
26.Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab), 50 mg/mL concentrate for solution for intravenous infusion [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc; 2020 Dec 1.
27.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
28.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Dec 16.
29.Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021;22(1):51-65. PubMed
30.Goldman JW, Garassino MC, Chen Y, et al. Patient-reported outcomes with first-line durvalumab plus platinum-etoposide versus platinum-etoposide in extensive-stage small-cell lung cancer (CASPIAN): a randomized, controlled, open-label, phase III study. Lung Cancer. 2020;149:46-52. PubMed
31.Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929-1939. PubMed
32.AstraZeneca Canada Inc response to February 18, 2021 DRR request for additional information regarding Imfinzi (duravalumab) DRR review: biomarker expression (PD-L1, TMB, and DLL3) relative to efficacy outcomes [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2021 Feb 23.
33.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
34.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
35.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
36.Durvalumab lengthens survival in extensive-stage SCLC. Cancer Discov. 2019;9(12). PubMed
37.Arakawa S, Yoshida T, Nakayama Y, Motoi N, Ohe Y. Small cell cancer transformation of lung adenocarcinoma during durvalumab treatment after chemoradiotherapy. J Thorac Oncol. 2020;15(8):e145-e146. PubMed
38.Bang YJ, Golan T, Dahan L, et al. Ramucirumab and durvalumab for previously treated, advanced non-small-cell lung cancer, gastric/gastro-oesophageal junction adenocarcinoma, or hepatocellular carcinoma: an open-label, phase Ia/b study (JVDJ). Eur J Cancer. 2020;137:272-284. PubMed
39.Chen HL, Tu YK, Chang HM, et al. Systematic review and network meta-analysis of immune checkpoint inhibitors in combination with chemotherapy as a first-line therapy for extensive-stage small cell carcinoma. Cancers (Basel). 2020;12(12):3629. PubMed
40.El Kaddissi A, Basse C. New European approvals: durvalumab - In first line metastatic small-cell lung cancer. Bull Cancer. 2020;107(12):1208-1209. PubMed
41.Liu T, Jin B, Chen J, et al. Comparative risk of serious and fatal treatment-related adverse events caused by 19 immune checkpoint inhibitors used in cancer treatment: a network meta-analysis. Ther Adv Med Oncol. 2020;12:1758835920940927. PubMed
42.Wang BC, Xiao BY, Li PC, et al. Efficacy and safety of first-line immunotherapy in combination with chemotherapy for patients with extensive-stage small cell lung cancer: a systematic review and network meta-analysis. J Oncol. 2020;2020:2368164. PubMed
43.Yan Y, Chen X, Wei J, Gong Z, Xu Z. Immunotherapy combinations in patients with small cell lung cancers. J Thorac Oncol. 2019;14(10):e244-e245. PubMed
44.Zhou T, Zhang Z, Luo F, et al. Comparison of first-line treatments for patients with extensive-stage small cell lung cancer: a systematic review and network meta-analysis. JAMA Netw Open. 2020;3(10):e2015748. PubMed
45.Landis JR, and Gary G. Koch. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
46.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
47.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
48.Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A. Modification of the EORTC QLQ-C30 (version 2.0) based on content validity and reliability testing in large samples of patients with cancer. The Study Group on Quality of Life of the EORTC and the Symptom Control and Quality of Life Committees of the NCI of Canada Clinical Trials Group. Qual Life Res. 1997;6(2):103-108. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: December 22, 2020
Alerts: Weekly search updates until project completion
Study types: No filters were applied to limit retrieval by study type
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw .ot .dq | Author keyword (Embase) Original title Candidate term word (Embase) |
.pt .nm | Publication type Name of substance word |
.rn | Registry number |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(durvalumab* or imfinzi* or medi4736 or medi-4736 or 28X28X9OKV or L01XC28).ti,ab,kf,ot,hw,nm,rn.
Small cell lung carcinoma/
(SCLC or SCLCs or ESSCLC or ESSCLCs).ti,ab,kf,ot.
((small or microcellular* or smallcell) adj5 (lung* or bronch* or pulmonar*) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf,ot.
(oat-cell adj3 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf,ot.
(Combined adj5 (small or smallcell) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kf,ot.
or/2–6
1 and 7
8 use medall
*durvalumab/ or (durvalumab* or imfinzi* or medi4736 or medi-4736 or L01XC28).ti,ab,kw,dq.
Small cell lung cancer/
(SCLC or SCLCs or ESSCLC or ESSCLCs).ti,ab,kw,dq.
((small or microcellular* or smallcell) adj5 (lung* or bronch* or pulmonar*) adj5 (cancer* or tumor* or tumor* or carcinoma* or neoplas*)).ti,ab,kw,dq.
(oat-cell adj3 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kw,dq.
(Combined adj5 (small or smallcell) adj5 (cancer* or tumor* or tumour* or carcinoma* or neoplas*)).ti,ab,kw,dq.
or/11–15
10 and 16
17 use oemezd
(conference review or conference abstract).pt.
18 not 19
9 or 20
remove duplicates from 21
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Searched terms: Imfinzi/durvalumab, small-cell lung cancer (SCLC)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Searched terms: Imfinzi/durvalumab, small-cell lung cancer (SCLC)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Searched terms: Imfinzi/durvalumab, small-cell lung cancer (SCLC)]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Searched terms: Imfinzi/durvalumab, small-cell lung cancer (SCLC)]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Searched terms: Imfinzi/durvalumab, small-cell lung cancer (SCLC)]
Grey Literature
Search dates: October 16 to 23, 2020
Keywords: Imfinzi (durvalumab), small-cell lung cancer (SCLC)
Limits:
Updated: Publication years: none
Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Anonymous (2019)36 | Editorial |
Arakawa (2020)37 | Letter to the editor |
Bang (2020)38 | Study design |
Chen (2020)39 | Systematic review |
El Kaddissi (2020)40 | Editorial |
Liu (2020)41 | No relevant comparators |
Wang (2020)42 | Systematic review |
Yan (2019)43 | Letter to the editor |
Zhou (2020)44 | Systematic review |
Appendix 3: Detailed Outcome Data
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Figure 7: Kaplan–Meier Curves of Overall Survival for the Durvalumab + EP and EP Arms — ITT Population, Final Analysis (Data Cut-Off: January 27, 2020)
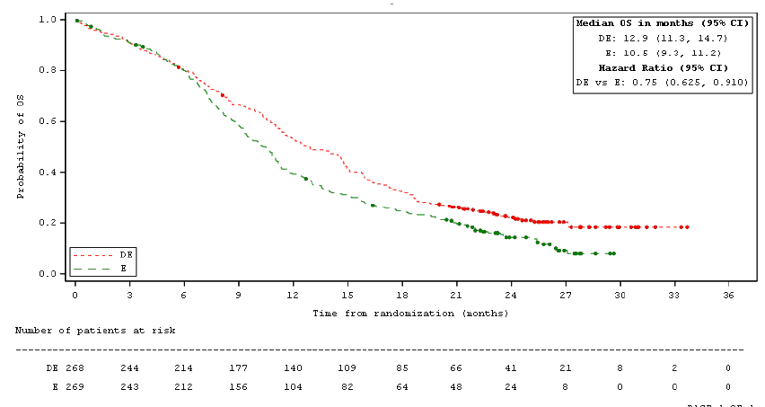
CI = confidence interval; DE = durvalumab in combination with etoposide and either carboplatin or cisplatin; E = etoposide and either carboplatin or cisplatin; OS = overall survival.
Circle indicates a censored observation.
One month = 30.4375 days.
Source: Clinical Study Report7
Table 25: PFS Subgroup Analysis — ITT Population, Interim Analysis (Data Cut-Off March 11, 2019)
Subgroup | Treatment Arm | N | Events, N (%) | HR (95% CI)a |
|---|---|---|---|---|
Smoking status at screening | ||||
Smoker | Durvalumab + EP | 246 | 207 (84.1) | 0.75 (0.544, 1.038) |
EP | 254 | 220 (86.6) | ||
Non-smoker | Durvalumab + EP | 22 | 19 (86.4) | 0.80 (0.636, 1.004) |
EP | 15 | 13 (86.7) | ||
ECOG performance status | ||||
0 | Durvalumab + EP | 99 | 83 (83.8) | 0.76 (0.628, 0.923) |
EP | 90 | 72 (80.0) | ||
1 | Durvalumab + EP | 169 | 143 (84.6) | 0.91 (0.439, 1.910) |
EP | 179 | 161 (89.9) | ||
Brain metastases at baseline | ||||
Yes | Durvalumab + EP | 28 | 25 (89.3) | 0.73 (0.418, 1.286) |
EP | 27 | 26 (96.3) | ||
No | Durvalumab + EP | 240 | 201 (83.8) | 0.638 (0.638, 0.947) |
EP | 242 | 207 (85.5) | ||
CI = confidence interval; EP = etoposide and either carboplatin or cisplatin; HR = hazard ratio; ITT = intention-to-treat.
aHR < 1 favours durvalumab + EP to be associated with a longer PFS than EP. HR and 95% CI were calculated from an unstratified Cox proportional hazards model with treatment as the only covariate.
Source: Clinical Study Report6
Table 26: Baseline EORTC QLQ-C30 and QLQ-LC13 Scores — PRO-Evaluable Population, Interim Analysis (Data Cut-Off March 11, 2019)
Subscale/item | Durvalumab + EP (N = 261) | EP (N = 260) |
|---|---|---|
EORTC QLQ-C30 | ||
Number of patients contributing to the analysis | 245 | 245 |
Global Health Status/QoL, mean (SD) | 56.02 (22.25) | 54.08 (22.41) |
Appetite Loss, mean (SD) | 24.22 (30.23) | 25.58 (32.49) |
Constipation, mean (SD) | 12.24 (23.08) | 18.10 (29.48) |
Diarrhea, mean (SD) | 4.90 (14.89) | 5.58 (15.99) |
Dyspnea, mean (SD) | 36.46 (28.70) | 38.50 (30.64) |
Fatigue, mean (SD) | 35.33 (24.64) | 37.14 (27.21) |
Financial Difficulties, mean (SD) | 17.96 (25.86) | 18.50 (27.37) |
Nausea / Vomiting, mean (SD) | 5.58 (13.77) | 6.94 (16.79) |
Pain, mean (SD) | 28.37 (26.72) | 29.52 (29.52) |
Insomnia, mean (SD) | 29.66 (31.65) | 33.88 (35.58) |
Cognitive Functioning, mean (SD) | 87.01 (19.50) | 86.94 (19.43) |
Emotional Functioning, mean (SD) | 73.78 (21.41) | 71.73 (24.96) |
Physical Functioning, mean (SD) | 72.22 (21.29) | 70.67 (22.42) |
Role Functioning, mean (SD) | 70.14 (29.96) | 69.80 (31.13) |
Social Functioning, mean (SD) | 76.94 (27.49) | 76.26 (27.49) |
EORTC QLQ-LC13 | ||
Number of patients contributing to the analysis | 244 | 245 |
Coughing, mean (SD) | 41.53 (25.95) | 40.54 (26.44) |
Dyspnea, mean (SD) | 30.74 (23.53) | 31.75 (23.91) |
Hemoptysis, mean (SD) | 6.28 (16.47) | 5.31 (14.28) |
Arm/Shoulder Pain, mean (SD) | 16.94 (24.84) | 13.20 (24.76) |
Chest Pain, mean (SD) | 22.81 (25.54) | 21.09 (25.15) |
Other Pain, mean (SD) | 21.45 (27.55) | 22.99 (30.06) |
Dysphagia, mean (SD) | 9.56 (20.72) | 9.39 (22.13) |
Alopecia, mean (SD) | 1.91 (10.30) | 2.99 (12.08) |
Peripheral Neuropathy, mean (SD) | 9.15 (21.45) | 8.57 (19.42) |
Sore Mouth, mean (SD) | 4.78 (14.81) | 4.22 (13.34) |
EORTC = European Organisation for Research and Treatment of Cancer; EP = etoposide + carboplatin or cisplatin; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire; SD = standard deviation.
Source: Clinical Study Report6
Table 27: Time to Deterioration of EORTC QLQ-C30 and QLQ-LC13 — PRO-Evaluable Population, Interim Analysis (Data Cut-Off March 11, 2019)
Symptom scale item | Durvalumab + EP N = 261 | EP N = 260 |
|---|---|---|
EORTC QLQ-C30 | ||
Global Health Status/QoL | ||
Number of patients contributing to the analysis, na | 238 | 232 |
Number of patients with event, n (%) | 132 (55.5) | 108 (46.6) |
Median time to deterioration (95% CI), monthsb | 8.4 (7.3, 11.5) | 7.2 (6.3, 9.0) |
HR (95% CI)c,d | 0.81 (0.626, 1.054) | |
P-valuee | 0.1166 | |
Appetite loss | ||
Number of patients contributing to the analysis, na | 230 | 224 |
Number of patients with event, n (%) | 127 (55.2) | 124 (55.4) |
Median time to deterioration (95% CI), monthsb | 8.3 (6.7, 11.0) | 6.6 (5.5, 7.5) |
HR (95% CI)c,d | 0.70 (0.542, 0.899) | |
P-valuee | 0.0054 | |
Constipation | ||
Number of patients contributing to the analysis, na | 239 | 229 |
Number of patients with event, n (%) | 113 (47.3) | 112 (48.9) |
Median time to deterioration (95% CI), monthsb | 11.1 (8.3, 14.7) | 7.3 (6.2, 9.0) |
HR (95% CI)c,d | 0.65 (0.499, 0.855) | |
P-valuee | 0.0018 | |
Diarrhea | ||
Number of patients contributing to the analysis, na | 243 | 244 |
Number of patients with event, n (%) | 99 (40.7) | 109 (44.7) |
Median time to deterioration (95% CI), monthsb | 14.6 (9.4, 18.7) | 7.7 (7.1, 9.3) |
HR (95% CI)c,d | 0.59 (0.442, 0.774) | |
P-valuee | 0.0002 | |
Dyspnea | ||
Number of patients contributing to the analysis, na | 224 | 218 |
Number of patients with event, n (%) | 116 (51.8) | 104 (47.7) |
Median time to deterioration (95% CI), monthsb | 9.0 (7.6, 11.9) | 7.4 (6.6, 8.8) |
HR (95% CI)c,d | 0.75 (0.574, 0.989) | |
P-valuee | 0.0406 | |
Fatigue | ||
Number of patients contributing to the analysis, na | 243 | 232 |
Number of patients with event, n (%) | 160 (65.8) | 149 (64.2) |
Median time to deterioration (95% CI), monthsb | 5.5 (3.9, 6.6) | 4.3 (3.1, 5.2) |
HR (95% CI)c,d | 0.82 (0.653, 1.027) | |
P-valuee | 0.0835 | |
Nausea / Vomiting | ||
Number of patients contributing to the analysis, na | 244 | 244 |
Number of patients with event, n (%) | 133 (54.5) | 127 (52.0) |
Median time to deterioration (95% CI), monthsb | 8.4 (6.6, 11.5) | 6.6 (5.6, 7.5) |
HR (95% CI)c,d | 0.80 (0.626, 1.027) | |
P-valuee | 0.0809 | |
Pain | ||
Number of patients contributing to the analysis, na | 239 | 233 |
Number of patients with event, n (%) | 134 (56.1) | 116 (49.8) |
Median time to deterioration (95% CI), monthsb | 7.8 (6.7, 9.9) | 6.7 (6.2, 7.8) |
HR (95% CI)c,d | 0.79 (0.615, 1.021) | |
P-valuee | 0.0718 | |
Insomnia | ||
Number of patients contributing to the analysis, na | 225 | 210 |
Number of patients with event, n (%) | 116 (51.6) | 104 (49.5) |
Median time to deterioration (95% CI), monthsb | 8.6 (6.9, 12.2) | 7.3 (6.2, 8.2) |
HR (95% CI)c,d | 0.75 (0.568, 0.980) | |
P-valuee | 0.0349 | |
Cognitive Functioning | ||
Number of patients contributing to the analysis, na | 244 | 242 |
Number of patients with event, n (%) | 125 (51.2) | 136 (56.2) |
Median time to deterioration (95% CI), monthsb | 8.4 (7.3, 11.6) | 6.0 (5.2, 7.1) |
HR (95% CI)c,d | 0.61 (0.472, 0.776) | |
P-valuee | < 0.0001 | |
Emotional Functioning | ||
Number of patients contributing to the analysis, na | 241 | 240 |
Number of patients with event, n (%) | 104 (43.2) | 112 (46.7) |
Median time to deterioration (95% CI), monthsb | 12.9 (9.0, 16.6) | 7.3 (6.7, 9.0) |
HR (95% CI)c,d | 0.61 (0.464, 0.800) | |
P-valuee | 0.0003 | |
Physical Functioning | ||
Number of patients contributing to the analysis, na | 243 | 240 |
Number of patients with event, n (%) | 125 (51.4) | 121 (50.4) |
Median time to deterioration (95% CI), monthsb | 8.5 (7.4, 12.0) | 6.5 (6.0, 8.2) |
HR (95% CI)c,d | 0.75 (0.581, 0.970) | |
P-valuee | 0.0276 | |
Role Functioning | ||
Number of patients contributing to the analysis, na | 230 | 226 |
Number of patients with event, n (%) | 131 (57.0) | 131 (58.0) |
Median time to deterioration (95% CI), monthsb | 7.4 (5.6, 10.2) | 5.9 (4.5, 6.7) |
HR (95% CI)c,d | 0.71 (0.550, 0.904) | |
P-valuee | 0.0059 | |
Social Functioning | ||
Number of patients contributing to the analysis, na | 236 | 236 |
Number of patients with event, n (%) | 131 (55.5) | 133 (56.4) |
Median time to deterioration (95% CI), monthsb | 7.6 (6.5, 9.0) | 6.2 (4.8, 7.3) |
HR (95% CI)c,d | 0.70 (0.549, 0.897) | |
P-valuee | 0.0048 | |
EORTC QLQ-L13 | ||
Coughing | ||
Number of patients contributing to the analysis, na | 229 | 230 |
Number of patients with event, n (%) | 114 (49.8) | 107 (46.5) |
Median time to deterioration (95% CI), monthsb | 9.3 (8.0, 14.1) | 7.7 (6.7, 9.5) |
HR (95% CI)c,d | 0.78 (0.600, 1.026) | |
P-valuee | 0.0747 | |
Dyspnea | ||
Number of patients contributing to the analysis, na | 240 | 240 |
Number of patients with event, n (%) | 147 (61.3) | 137 (57.1) |
Median time to deterioration (95% CI), monthsb | 6.5 (5.2, 7.8) | 5.5 (4.6, 6.7) |
HR (95% CI)c,d | 0.79 (0.625, 1.006) | |
P-valuee | 0.0578 | |
Hemoptysis | ||
Number of patients contributing to the analysis, na | 242 | 245 |
Number of patients with event, n (%) | 82 (33.9) | 83 (33.9) |
Median time to deterioration (95% CI), monthsb | 18.3 (14.5, 21.1) | 10.5 (8.2, 11.9) |
HR (95% CI)c,d | 0.64 (0.469, 0.876) | |
P-valuee | 0.0049 | |
Arm/Shoulder Pain | ||
Number of patients contributing to the analysis, na | 240 | 238 |
Number of patients with event, n (%) | 115 (47.9) | 109 (45.8) |
Median time to deterioration (95% CI), monthsb | 9.9 (8.1, 14.5) | 7.5 (6.5, 9.3) |
HR (95% CI)c,d | 0.70 (0.535, 0.915) | |
P-valuee | 0.0088 | |
Chest Pain | ||
Number of patients contributing to the analysis, na | 238 | 240 |
Number of patients with event, n (%) | 112 (47.1) | 103 (42.9) |
Median time to deterioration (95% CI), monthsb | 10.6 (8.4, 14.6) | 7.8 (7.2, 9.9) |
HR (95% CI)c,d | 0.76 (0.575, 0.996) | |
P-valuee | 0.0464 | |
Other Pain | ||
Number of patients contributing to the analysis, na | 235 | 231 |
Number of patients with event, n (%) | 134 (57.0) | 121 (52.4) |
Median time to deterioration (95% CI), monthsb | 7.8 (6.6, 9.3) | 6.4 (5.0, 7.4) |
HR (95% CI)c,d | 0.72 (0.558, 0.923) | |
P-valuee | 0.0096 | |
CI = confidence interval; EORTC = European Organisation for Research and Treatment of Cancer; EP = etoposide + carboplatin or cisplatin; HR = hazard ratio; PRO = patient-reported outcome; QLQ-C30 = 30-item Core Quality of Life Questionnaire, version 3; QLQ-LC13 = 13-item Lung Cancer Quality of Life Questionnaire; QoL = quality of life; SD = standard deviation.
aAnalysis population is based on patients who have a baseline score ≥ 10 in the EORTC QLQ-C30 function scales and global health status/QoL (respectively ≤ 90 in the EORTC QLQ-C30 and EORTC QLQ-L13 symptom scales/items).
bMedian time to deterioration calculated using the Kaplan–Meier technique. CI is derived based on Brookmeyer-Crowley method and using the log-log transformation.
cThe HR and CIs were calculated using a stratified Cox proportional hazards model, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), and ties handled by Efron approach.
dHR < 1 favours durvalumab + EP to be associated with a longer time to deterioration than EP.
eNominal P value (i.e., results are non-inferential). The analysis was performed using the stratified log-rank test, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), and using the rank tests of association approach.
Source: Clinical Study Report6
Table 28: Duration of Exposure to Study Treatments in the Durvalumab + Tremelimumab + EP Arm of the CASPIAN Trial — Safety Population, Final Analysis (Data Cut-Off January 27, 2020)
Duration of exposure | Durvalumab N = 266 | Tremelimumab N = 266 | Etoposide N = 264 | Carboplatin N = 202 | Cisplatin N = 66 |
|---|---|---|---|---|---|
Number of infusions | |||||
Mean (SD) | 9.1 (8.30) | 4.1 (1.31) | 10.9 (2.85) | 3.6 (0.95) | 3.6 (0.98) |
Median (Min, Max) | 6.0 (1, 35) | 5.0 (1, 6) | 12.0 (1, 21) | 4.0 (1, 6) | 4.0 (1, 6) |
Total exposure duration, weeks | |||||
Mean (SD) | 35.19 (33.881) | 16.91 (6.841) | 11.89 (3.559) | 11.62 (3.694) | 11.79 (3.565) |
Median (Min, Max) | 23.07 (0.1, 143.7) | 20.00 (0.1, 30.9) | 12.29 (0.6, 27.0) | 12.14 (0.9, 27.0) | 12.71 (0.7, 18.0) |
Total treatment years | 179.370 | 86.201 | 60.181 | 44.983 | 14.916 |
Number of cycles received | |||||
Mean (SD) | 9.1 (8.28) | 4.1 (1.31) | 3.6 (0.89) | 3.6 (0.95) | 3.6 (0.93) |
Median (Min, Max) | 6.0 (1, 35) | 5.0 (1, 5) | 4.0 (1, 6) | 4.0 (1, 6) | 4.0 (1, 4) |
EP = etoposide + carboplatin or cisplatin; Max = maximum; Min = minimum; SD = standard deviation.
Source: Clinical Study Report7
Table 29: Summary of Efficacy Outcomes of the Durvalumab + Tremelimumab + EP Arm in the CASPIAN Trial — Final Analysis (Data Cut-Off January 27, 2020)
Outcome | Durvalumab + Tremelimumab + EP N = 268 |
|---|---|
OS – ITT population | |
Deaths, n (%) | 207 (77.2) |
Median OS (95% CI),a months | 10.4 (9.6, 12.0) |
HR (95% CI) for D + T + EP vs D + EPb,c | 1.08 (0.890, 1.309) |
P valued,h | 0.4352 |
HR (95% CI) for D + T + EP vs EPb,c | 0.82 (0.682, 0.995) |
P valued | 0.0451 |
OS12, % (95% CI) a | 43.8 (37.7, 49.7) |
OS18, % (95% CI) a | 30.7 (25.2, 36.4) |
OS24, % (95% CI) a | 23.4 (18.4, 28.8) |
PFSf – ITT population | |
Events, n (%) | 229 (85.4) |
Median PFS (95% CI),a months | 4.9 (4.7, 5.9) |
HR (95% CI) for D + T + EP vs D + EPb,c | 1.03 (0.857, 1.235) |
P valued,h | 0.7540 |
HR (95% CI) for D + T + EP vs EPb,c | 0.84 (0.696, 1.005) |
P valued,h | 0.0568 |
PFS6, % (95% CI)a | 43.2 (37.1, 49.1) |
PFS12, % (95% CI)a | 16.9 (12.6, 21.7) |
PFS18, % (95% CI)a | 12.8 (9.0, 17.2) |
PFS24, % (95% CI)a | 11.5 (7.9, 15.8) |
Confirmed DORe,f – confirmed responders | |
Number of responders who subsequently progressed or died, n | 125 |
Median DOR (95% CI)a | 5.2 (4.9, 5.6) |
% remaining in response at 12 months a | 24.9 |
% remaining in response at 24 months a | 21.5 |
ORRf – ITT population | |
Patients with an unconfirmed response, n (%) | 198 (73.9) |
OR (95% CI) for D + T + EP vs. EPg,j | 1.19 (0.817, 1.746) |
p-valuei | 0.3611 |
Patients with a confirmed response, n (%) | 156 (58.2) |
OR (95% CI) for D + T + EP vs. EPg,j | 1.02 (0.722, 1.436) |
p-valuei | 0.9184 |
CI = confidence interval; D = durvalumab; EP = etoposide + carboplatin or cisplatin; HR = hazard ratio; ORR = objective response rate; OS = overall survival; OS6 = overall survival at 6 months after randomization; OS12 = overall survival at 12 months after randomization; OS18 = overall survival at 18 months after randomization; OS24 = overall survival at 24 months after randomization; PFS = progression-free survival; PFS2 = progression-free survival after subsequent anticancer therapy; PFS6 = proportion of patients alive and progression-free at 6 months from randomization; PFS12 = proportion of patients alive and progression-free at 12 months from randomization; PFS18 = proportion of patients alive and progression-free at 18 months from randomization; PFS24 = proportion of patients alive and progression-free at 24 months from randomization; t = tremelimumab.
aCalculated using the Kaplan–Meier technique; CIs are derived based on the Brookmeyer-Crowley method and using the log-log transformation.
bHR < 1 favours D + T + EP.
cHR and CI were calculated using stratified Cox proportional hazards model, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), and ties handled by Efron approach.
dThe analysis was performed using the stratified log-rank test, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), and using the rank tests of association approach.
eCalculated post hoc.
fDetermined by the RECIST-based assessment per investigator.
gThe comparisons of D + T + EP vs EP were performed using a separate logistic regression model, adjusting for planned platinum therapy in cycle 1 (carboplatin or cisplatin), with 95% CI calculated by profile likelihood.
hNominal P value (i.e., results are non-inferential).
iP-value, derived from logistic regression model, is based on twice the change in log-likelihood resulting from the addition of a treatment factor to the model.
jOR favour D + T + EP.
Source: Clinical Study Report7
Table 30: Summary of Harms of the Durvalumab + Tremelimumab + EP Arm in CASPIAN Trial — Safety Population, Final Analysis (Data Cut-Off January 27, 2020)
Harms | Durvalumab + Tremelimumab + EP N = 266 |
|---|---|
Patients with ≥ 1 adverse event | |
Patients with any AE, n (%) | 264 (99.2) |
Most common eventsa, n (%) | |
Neutropenia | 115 (43.2) |
Anemia | 100 (37.6) |
Nausea | 86 (32.3) |
Alopecia | 79 (29.7) |
Constipation | 54 (20.3) |
Decreased appetite | 57 (21.4) |
Thrombocytopenia | 54 (20.3) |
Fatigue | 53 (19.9) |
Vomiting | 36 (13.5) |
Leukopenia | 33 (12.4) |
Asthenia | 38 (14.3) |
Diarrhea | 44 (16.5) |
Pruritus | 40 (15.0) |
Patients with ≥ 1 SAE | |
n (%) | 121 (45.5) |
Most common eventsb, n (%) | |
Febrile neutropenia | 11 (4.1) |
Anemia | 9 (3.4) |
Pneumonia | 14 (5.3) |
Thrombocytopenia | 6 (2.3) |
Neutropenia | 5 (1.9) |
Hyponatremia | 9 (3.4) |
Pneumonitis | 5 (1.9) |
Diarrhea | 7 (2.6) |
Pulmonary embolism | 7 (2.6) |
Colitis | 5 (1.9) |
Inappropriate antidiuretic hormone secretion | 5 (1.9) |
Patients who stopped treatment due to adverse events | |
n (%) | 57 (21.4) |
Deaths | |
n (%) | 207 (77.2) |
Attributed to ES-SCLC only | 166 (80.2) |
AE with an outcome of death | 27 (10.2) |
Unknown cause | 12 (5.8) |
Notable harms | |
Immune-related AEs, n (%) | 178 (66.9) |
Pneumonitis | 11 (4.1) |
Hepatic | 46 (17.3) |
Diarrhea/colitis | 50 (18.8) |
Endocrine | 85 (32.0) |
Hypothyroid | 30 (11.3) |
Hyperthyroid | 31 (11.7) |
Thyroiditis | 3 (1.1) |
Adrenal Insufficiency | 5 (1.9) |
Hypophysitis | 3 (1.1) |
Type I Diabetes Mellitus | 13 (4.9) |
Renal | 3 (1.1%) |
Dermatitis/rash | 90 (33.8) |
Myocarditis | 1 (0.4) |
Pancreatic | 19 (7.1) |
Myasthenia gravis | 1 (0.4) |
Arthritis | 1 (0.4) |
Arthralgia | 1 (0.4) |
Received systemic corticosteroids | 66 (24.8) |
Received high-dose steroids | 57 (21.4) |
Received endocrine therapy | 49 (18.4) |
Infusion-related reactions, n (%) | 4 (1.5) |
Infusion-related reaction | 3 (1.1) |
Urticaria | 1 (0.4) |
Hypersensitivity/anaphylactic reactions, n (%) | 2 (0.8) |
Infection, n (%) | 102 (38.3) |
AE = adverse event; ES-SCLC = extensive-stage small cell lung cancer; SAE = serious adverse event.
aFrequency > 15% in any treatment arm.
bFrequency ≥ 5 patients.
Source: Clinical Study Report7
Figure 8: Exploratory Post Hoc Analysis of Overall Survival Based on PD-L1 Expression in the Durvalumab + EP Versus EP Arms — ITT Population, Final Analysis (Data Cut-Off: January 27, 2020)
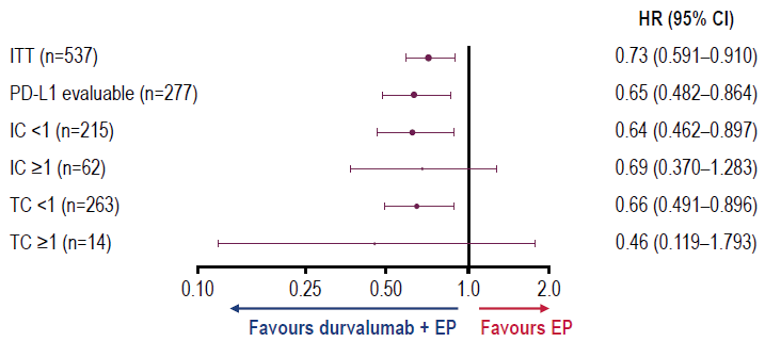
CI = confidence interval; EP = etoposide-platinum; IC = immune cells; ITT = intention-to-treat; HR = hazard ratio; OS = overall survival; PD-L1 = programmed cell death ligand; TC = tumour cells.
Source: Sponsor response to request for information.32
Figure 9: Exploratory Post Hoc Analysis of Overall Survival Based on Tissue Tumour Mutational Burden in the Durvalumab + EP Versus EP Arms — ITT Population, Final Analysis (Data Cut-Off: January 27, 2020)
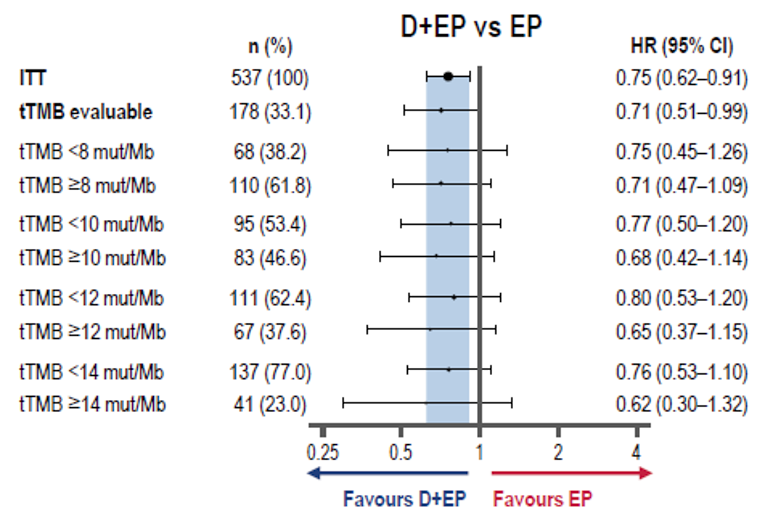
CI = confidence interval; D = durvalumab; EP = etoposide-platinum; ITT = intention-to-treat; HR = hazard ratio; OS = overall survival; tTMB = tissue tumour mutational burden.
Source: Sponsor response to request for information.32
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
HRQoL
Symptoms
Both outcomes are evaluated in the included study and their properties are shown in Table 31.
Findings
The findings about validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 31.
Interpretation of the reliability and validity metrics were based on the following criteria:
Inter-rater reliability, kappa statistics (level of agreement)45:
< 0 = poor agreement
0.00–0.21 = slight agreement
0.21–0.40 = fair agreement
0.41–0.60 = moderate agreement
0.61–0.8 = substantial
0.81–1.00 = almost perfect agreement
Internal consistency (Cronbach alpha) and test-retest reliability: ≥ 0.7 is considered acceptable.46
Validity; i.e., between-scale comparison (correlation coefficient, r)47:
≤ 0.3 = weak
0.3 to ≤ 0.5 = moderate
> 0.5 = strong
Table 31: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
HRQoL & Symptoms | |||
EORTC QLQ-C30 and supplement QLQ LC13 | Standardized, patient self-administered questionnaire for evaluating the quality of life of patients with cancer. Consists of functional scales, 3 symptom scales, and 6 single item scales. The QLQ C30 can be used with a supplement for patients with lung cancer (LC13) with 13 items. | Strong concurrent validity of emotional functioning scales as well as in the pain scales (r = 0.72) and convergent validity (r range = 0.71 to 0.97). Construct, clinical, and criterion validity have also been acceptable. (specifically when assessing the supplementary LC13 questionnaire). Good responsiveness of the functional and symptoms scales Moderate to excellent reliability in both QLQ-C30 AND LC13 (Cronbach alpha values ranging from 0.52 to 0.89) | It varies depending on the improvement or deterioration among different items scales. MID estimates of the EORTC QLQ-30 ranged from a meaningful change for improvement of 9.1 units (cognitive functioning) to 23.5 units (pain), and a meaningful change for deterioration ranging from 7.2 units (physical functioning) to 13.5 units (role functioning). MID for improvement for physical functioning at 9 and 5 (for PS and weight change anchors, respectively), role functioning at 14 and 7; social functioning 5 and 7; global health status at 9 and 4; fatigue 14 and 5; and pain at 16 and 2. The respective MID estimates for deterioration (based on PS, weight loss) were physical 4 and 6; role 5 and 5; social 7 and 9; global health status 4 and 4; fatigue 6 and 11; and pain at 3 and 7. The sponsor defines a clinically meaningful deterioration as a ≥ 10-point increase from baseline for symptoms and a ≥ 10-point decrease from baseline for function and global health status/QoL. |
HRQoL = Health-related quality of Life; EORTC QLQ C30 = European Organization for Research and Treatment of Cancer 30 item Core Quality of Life Questionnaire; LC13 = Lung Cancer Supplement; MID = minimal important difference; PS = WHO performance status.
European Organization for Research and Treatment of Cancer, 30 Item Core Quality of Life Questionnaire (EORTC QLQ C-30) and Lung Cancer Supplement (LC13)
The EORTC QLQ C-30 (version 3) is a standardized, patient self-administered questionnaire for evaluating the quality of life of patients with cancer participating in clinical trials.33 This questionnaire is intended to be complemented by tumour-specific questionnaire modules or supplements, such as the 1 for patients with lung cancer, or QLQ-LC13.8
The EORTC QLQ C-30 consists of 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, nausea/vomiting, and pain), and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). These items are rated on a scale from 1 (not at all) to 4 (very much). This instrument also includes a global health status and overall quality of life section with questions rated on a 1 to 7 scale (very poor to excellent, respectively). Each functional scale, symptom scale, and individual item is converted to a 0 to 100 scale, where a higher score on a functional scale is correlated to higher level of function, while a higher score in the symptom scale means higher burden of symptoms.9
Measurement properties
The validity of the instrument has been assessed in several studies8,9,33,48 providing evidence of good concurrent validity; for example, the emotional functioning scales correlate well to other anxiety and depression scales (e.g., the hospital anxiety and depression scales and global quality of life) as well as in the pain scales (when compared to the brief pain inventory [BPI]; r = 0.72).9 Convergent validity has been evaluated with correlations between domains conceptually related and between items and domains of quality of life with overall good Pearson correlations (from 0.71 to 0.97.).9 Furthermore, good correlations between functioning scales, global QoL, and all symptom scales of the QLQ-C30 have been found with BPI scales. Construct and criterion validity have also been acceptable and consistent throughout the studies. Clinical validity has been assessed demonstrating good ability to discriminate between subgroups of patients with lung cancer (specifically when assessing the supplementary LC13 questionnaire).8 The original studies evaluating the QLQ-C308,33,48 also report good responsiveness of the functional and symptoms scales (only poor in the nausea/vomiting symptoms evaluation).
In terms of reliability, both QLQ-C30 AND LC13 have shown good internal consistency with Cronbach alpha values ranging from 0.52 to 0.89 in functioning and symptom scales,8,9,33 with others reporting even higher reliability scores in quality of life. Smaller values have been observed in the ‘role’ items of the functioning scales but these were improved in subsequent analysis.48
Minimally important difference
In 1 study with patients with advanced cancer (including breast, lung, prostate cancer), MID estimates of the EORTC QLQ-30 using 2 patient-based anchors (overall health and overall quality of life) ranged from a meaningful change for improvement of 9.1 units (cognitive functioning) to 23.5 units (pain), and a meaningful change for deterioration ranging from 7.2 units (physical functioning) to 13.5 units (role functioning). Distribution-based estimates were around 0.5 SD.34
Another study35 using WHO performance status (PS) and weight change as anchors, estimated the MID for improvement for physical functioning at 9 and 5 (for PS and weight change anchors, respectively), role functioning at 14 and 7; social functioning 5 and 7; global health status at 9 and 4; fatigue 14 and 5; and pain at 16 and 2. The respective MID estimates for deterioration (based on PS, weight loss) were physical 4 and 6; role 5 and 5; social 7 and 9; global health status 4 and 4; fatigue 6 and 11; and pain at 3 and 7.
For the sponsor submitted study, a clinically meaningful deterioration was defined as a ≥ 10-point increase from baseline for symptoms and a ≥ 10-point decrease from baseline for function and global health status/QoL.
Limitations
The reliability of social items such as social functioning and the social worker’s ratings of social support and activity still need more study and are yet to be proven. The difference methodology and timing of the studies assessing these values can imply uncertainty in the body of evidence for the properties of the measurement scales.
Not all of the above MIDs mentioned in the evidence found apply to the items included in the submission and an individual approach for each item might be necessary to reach a judgment of meaningful improvement or deterioration.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BSA
body surface area
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EP
etoposide and platinum-based chemotherapy (carboplatin or cisplatin)
ES-SCLC
extensive-stage small cell lung cancer
ICER
incremental cost-effectiveness ratio
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
TTD
time to death
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Durvalumab (Imfinzi), concentrate for solution for infusion |
Submitted price | Durvalumab, 50 mg/mL, IV infusion: $938.67 per 120 mg vial $3,911.11 per 500 mg vial |
Indication | In combination with etoposide and either carboplatin or cisplatin for first-line treatment of adult patients with extensive-stage small cell lung cancer |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | September 21, 2020 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: Yes Indication: for the treatment of patients with locally advanced, unresectable non–small cell lung cancer following curative intent platinum-based chemoradiation therapy for up to a maximum of 12 months Recommendation date: May 3, 2019 Recommendation: Reimburse with clinical criteria and/or conditions |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | First-line treatment of adult patients with extensive-stage small cell lung cancer |
Treatment | Durvalumab in combination with etoposide and either carboplatin or cisplatin |
Comparator | Etoposide with either carboplatin or cisplatin |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (10 years) |
Key data source | CASPIAN RCT |
Submitted results | ICER = $353,824 per QALY ($124,305 incremental costs, 0.35 incremental QALYs) |
Key limitations |
|
CADTH reanalysis results |
|
ECOG PS = Eastern Cooperative Oncology Group Performance Status; EP = etoposide-platinum (carboplatin or cisplatin); ES-SCLC = extensive-stage small cell lung cancer; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; RCT = randomized controlled trial; TTD = time to death.
Conclusions
The CASPIAN trial provided evidence demonstrating the efficacy of durvalumab + etoposide-platinum (EP) therapy in terms of overall survival (OS) as well as the safety of durvalumab + EP in adult patients with extensive-stage small cell lung cancer (ES-SCLC) compared with EP alone. The 2.7-month improvement associated with durvalumab + EP in median OS was considered statistically significant and clinically relevant by the clinical experts consulted by CADTH. Differences in landmark OS observed at 12 months (52.8% versus 39.3% survival for durvalumab + EP and EP alone, respectively), 18 months (32.0% and 24.8%, respectively), and 24 months (22.2% and 14.4%, respectively) were also considered clinically relevant by the clinical experts consulted by CADTH, although the landmark OS data are associated with uncertainty.
The CADTH reanalyses incorporated health state–specific utility values to address the likely overestimation of accrued quality-adjusted life-years (QALYs) in the sponsor’s base case via the sponsor’s time-to-death (TTD) approach to health utilities, and it revised the proportion of patients receiving a subsequent chemotherapy to be consistent with the values reported in the CASPIAN trial. The CADTH base case aligns with the results reported by the sponsor. Durvalumab + EP is not considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY, with an incremental cost-effectiveness ratio (ICER) of $441,635 per QALY gained compared to EP alone. A price reduction of 88% would be required for durvalumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained.
Important identified limitations could not be addressed by CADTH. Uncertainty remains with the generalizability of the results to the patient population most likely to be treated with durvalumab + EP in clinical practice due to the exclusion from the trial of patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) greater than 1. The cost-effectiveness in patients with a higher ECOG PS (worse functioning) is therefore uncertain. There is also uncertainty in the extrapolation of OS and progression-free survival (PFS) curves over the 10-year time horizon from the approximately 2 years of observed data, as more than 65% of incremental QALYs gained in the model accrued during the model’s extrapolated period, for which there are no observed data. A series of scenario analyses were conducted exploring some areas of uncertainty in the submitted model; none of these scenarios was associated with an ICER approaching $50,000 per QALY gained.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process, specifically information that pertains to the economic submission.
Two patient groups provided input for this review: Lung Cancer Canada and the Lung Health Foundation (previously the Ontario Lung Association). Input was gathered through online surveys and interviews with patients and caregivers. The patient groups noted that ES-SCLC is an aggressive disease with very low survival rates. The disease has a major impact on quality of life, and what few treatment options are available have not changed for 30 years. Chemotherapies were associated with improved symptoms and quality of life but with poor impact on patient immunity and, in some cases, they prevent a return to normal activities and time with loved ones. Immunotherapy reportedly provides hope for improved outcomes and quality of life with more manageable side effects and the possibility of feeling better within days. The patient groups reported the following outcomes as important to patients: cancer control, improved symptoms and delayed deterioration, manageable side effects, improved central nervous system function, delayed progression, extended survival with good quality of life, and longer-lasting and durable treatment. The patient groups were unable to include input from patients with durvalumab experience because no trials of the product have been conducted in Canada. However, they noted that Canadians with experience with the immunotherapy, atezolizumab, found treatment to be tolerable.
Input was received from 2 clinician groups: Lung Cancer Canada and Ontario Health’s Lung and Cancer Drug Advisory Committee. The clinician groups noted that small cell lung cancer is seen mainly in the elderly population and that patients typically present at a late stage, beyond when their cancer would be amenable to surgical resection. Treatment was seen as standard around the world and without change for 30 years. Etoposide-platinum chemotherapy was noted to have a high response rate, but many patients progress in a short period of time, with half dying within 1 year and few surviving beyond 2 years. All patients with ES-SCLC were seen as having high unmet needs, and no subgroups for whom drugs such as durvalumab would be most effective have yet been identified. The clinician groups anticipated durvalumab + EP would be used as first-line therapy, and it was not seen as appropriate to have patients try other treatments before initiating durvalumab combination therapy. Tumour shrinkage would typically be used to determine if a patient is responding to therapy, and any improvement in survival beyond 18 months was considered meaningful. The addition of durvalumab was seen as a modest but real improvement in survival for a group of patients with high unmet needs.
The drug plans noted that EP is the current standard of care in Canada and predicted that the uptake of durvalumab over the first year of treatment would be considerably higher than estimated by the sponsor. Drug plan input also raised concerns regarding alternate dosing and the duration of maintenance therapy with durvalumab. However, the clinical experts consulted by CADTH indicated that they would administer durvalumab in a manner consistent with its product monograph and the CASPIAN trial design (the approach considered in the model) and continue therapy until disease progression, the development of intolerable side effects, or a patient wished to stop treatment.
Several of these concerns were addressed in the sponsor’s model:
PFS, OS, and quality of life were incorporated into the model, as were serious adverse events as reported in the CASPIAN trial.
The comparator seen as most relevant to clinicians and drug plans, EP alone, was the comparator within the model.
In addition, CADTH addressed 1 of the concerns as follows:
That a high proportion of eligible patients would receive durvalumab in year 1 of the budget impact analysis, given the high unmet need and the long period of time since the last treatment improvement became available.
CADTH was unable to address the following concern raised from stakeholder input:
The incorporation of TTD utilities more appropriately reflecting patients’ experiences with their condition worsening over a more relevant time scale than provided in the sponsor’s model.
Economic Review
The current review is for durvalumab (Imfinzi) in combination with EP chemotherapy for first-line treatment of patients with ES-SCLC.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis1 assessing durvalumab + etoposide and either carboplatin or cisplatin (EP) compared to EP alone in adult patients with histologically or cytologically documented ES-SCLC due to multiple lung nodules that are too extensive or a tumour or nodal volume that is too large to be encompassed in a tolerable radiation plan. This was consistent with the intention-to-treat population in the CASPIAN clinical trial,2,3 and the sponsor’s modelled population was in line with the Health Canada indication and reimbursement request.4
The recommended dose of durvalumab is 1,500 mg in combination with EP every 3 weeks for 4 cycles, followed by 1,500 mg every 4 weeks as monotherapy until disease progression or unacceptable toxicity. Patients with a body weight of 30 kg or less must receive weight-based dosing of durvalumab at 20 mg/kg in combination with EP on the same schedule.4 At the submitted price of $938.67 per 120 mg and $3,911.11 per 500 mg vial,1 the cost of durvalumab for patients weighing more than 30 kg is $11,733 per 3- or 4-week cycle. A cycle consisted of 80 mg/m2 to 100 mg/m2 of body surface area (BSA) of etoposide on days 1 to 3, and either carboplatin (dosed to a target area under the concentration versus time curve of 5 mg/mL per min or 6 mg/mL per min) or cisplatin (at 75 mg/m2 to 80 mg/m2 of BSA) on day 1 of each cycle. Assuming a patient with a body weight of 70 kg, a BSA of 1.8 m2, and a glomerular filtration rate of 61.7 mL/min, the total drug acquisition cost per patient for the initial 3-week cycle of durvalumab + EP is between $12,588 to $12,783, depending on the choice of cisplatin or carboplatin, respectively. The cost of EP alone is $955 to $1,050 per 3-week cycle per patient, including wastage of excess medications in vials.5
The clinical outcomes were QALYs and life-years. The economic analysis was undertaken over a 10-year time horizon using 1-week cycles from the perspective of a Canadian public health care payer. Discounting (1.5% per annum) was applied to both costs and clinical outcomes, and a half-cycle correction was applied.1
Model Structure
The sponsor submitted a 3-state partitioned survival model, in which the proportions of patients who were progression-free (PFS), had experienced progression (as defined by criteria from the Response Evaluation Criteria in Solid Tumours version 1.1 and assessed by study investigators), or had died were derived from non–mutually exclusive survival curves. All patients entered the model in the progression-free state. In the base case, patients assigned to durvalumab + EP received 4 3-week cycles of durvalumab + EP and continued receiving durvalumab every 4 weeks until progression or death, while patients assigned to EP alone received 4 to 6 cycles of EP until progression or death, whichever was shorter. At the end of each weekly cycle, the proportion of patients in the post-progression or death states was derived from the area under the survival curves, with progressed disease defined as the difference between the OS and PFS curves. Patients who had progressed could receive a second-line chemotherapy, which increased accrued drug costs but did not further affect efficacy.1
Model Inputs
Baseline patient characteristics in the model were aligned with those of the CASPIAN clinical trial population, a phase III, randomized, multi-centre, open-label trial for first-line treatment of patients with ES-SCLC.2,3 Of the patients in the CASPIAN trial, 69.6% were male, with a mean age of 62.4 years, a weight of 73.1 kg, and a BSA of || m2. Parametric survival distributions and odds knot spline models were fitted to CASPIAN trial data to extrapolate observed 2-year follow-up data from the trial to the entirety of the 10-year modelled time horizon. The sponsor fitted survival curves independently for each treatment, as the proportional hazards assumption was violated due to the curves crossing during the first 6 months of the time horizon. The survival extrapolation models selected in the sponsor’s base case were chosen based on the Akaike information criterion, Bayesian information criterion, visual inspection, and clinical plausibility, the latter using real-world data for OS of patients treated with EP. Clinical plausibility was considered most important by the sponsor. Log-logistic models were chosen to extrapolate OS in both treatment arms (Figure 1, Figure 2, and Figure 3), while spline odds 1 knot models were used to extrapolate PFS (Figure 4 and Figure 5). In addition to disease-specific mortality reported in the CASPIAN trial, the model included age- and sex-specific mortality consistent with the general population,6 applied as a weekly probability, to ensure the hazard of death predicted in the extrapolations did not drop below that of the general population.
Utility values were based on EuroQol 5-Dimensions 5-Levels questionnaire data collected during the CASPIAN trial at each treatment cycle until progression, on day 28 post-progression, at 2 months post-progression, and every 8 weeks until second progression or death. These EQ-5D-5L-based utility values were calculated using Canadian-specific utility weights developed by Xie et al. (2016).7 In the base case, the model used a TTD approach for utilities, with time boundaries of 60 or more days before death (mean utility: ||||), 30 to 59 days before death (mean utility of ||||), and less than 30 days before death (mean utility of ||||). A scenario analysis was conducted using health state–specific utilities of |||| pre-progression and |||| post-progression, also based on data from the CASPIAN trial.
Treatment costs consisted of drug acquisition and administration costs, and were weighted by the proportion of patients receiving carboplatin (46.5%) and cisplatin (53.5%), as derived from Alberta Oncology Outcomes study data.8 The drug price of durvalumab was obtained from the sponsor and all other treatments were sourced from IQVIA Delta PA wholesale prices.5 Durvalumab was assumed to have a dose intensity of | %, based on usage in the CASPIAN trial, while EP alone was assigned a dose intensity of 100%. Administration costs consisted of chair time for IV administration and accounted for the cost of regimen preparation, pharmacist time, chemotherapy nurse time, chemotherapy chair time, and overhead costs. The weighted per-cycle cost of durvalumab + EP was $13,279 per cycle for the initial 4 cycles, including wastage, followed by $11,461 per cycle thereafter, while the cost of EP alone was $1,818 per cycle for a maximum of 6 cycles. Of the patients in the EP group, |||| were assumed to undergo prophylactic cranial irradiation, while |||| of durvalumab + EP and |||| of EP-alone patients were assumed to undergo thoracic or other radiotherapy after progression. In both groups, |||| of patients were assumed to receive a subsequent therapy for approximately 3 months after progression, based on Alberta Oncology Outcomes real-world study data.8 Costs for the included regimens ranged from $510 to $1,866 per 3-week cycle, depending on the regimen assigned. All patients accrued disease management costs in the model, including physician visits and monitoring costs, and upon death all patients were assigned a terminal care cost of $43,143, which was assumed to represent the cost of terminal care in the 12 months before death.9
Serious or life-threatening (Grade 3 or 4) adverse events were included in the model for each treatment group in the proportions observed in the CASPIAN trial. These adverse events were associated with a utility decrement and a treatment cost.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (3,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section. Comparator costs are based on publicly available list prices and may not reflect actual costs paid by public drug plans.
Base-Case Results
In the sponsor’s base-case analysis, durvalumab + EP was associated with an expected cost of $184,630 and 1.39 QALYs over the 10-year time horizon. When compared to EP alone, durvalumab + EP had an incremental cost of $124,305 and was associated with 0.35 incremental QALYs, resulting in an ICER of $353,824 (Table 3). The key cost driver in the analysis was the drug acquisition cost of durvalumab, while the key QALY driver was the greater number of QALYs accrued in the 91 or more days until death for patients receiving durvalumab + EP. At a willingness-to-pay threshold of $50,000 per QALY, durvalumab + EP had a 0% probability of being considered cost-effective. When considering life-years, the sponsor’s base case reported that durvalumab + EP was associated with an ICER of $292,843 per life-year gained. At the end of the 10-year time horizon, 2.3% of modelled patients in the durvalumab + EP group and 0.8% in the EP group were still alive.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. EP ($ per QALY) |
|---|---|---|---|---|---|
EP | 60,325 | Reference | 1.04 | Reference | Reference |
Durvalumab + EP | 184,630 | 124,305 | 1.39 | 0.35 | 353,824 |
EP = etoposide-platinum (carboplatin or cisplatin); ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus .
Source: Adapted from sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic base case are presented in Table 11.
Sensitivity and Scenario Analysis Results
The sponsor undertook scenario analyses on its base case assuming alternate OS and PFS extrapolations and a 7-year time horizon. It used health-state utilities for pre- and post-progression rather than TTD utilities, differing resource-use assumptions for disease management, the rates from the CASPIAN trial for second-line therapy, and varying discount rates. All scenario analyses reported ICERs between $310,447 (using the log-normal parametric extrapolation for OS) and $424,798 (using a spline odds 1 knot extrapolation for OS) per QALY. Using health-state utilities derived from CASPIAN for both the pre- and post-progression states resulted in an ICER of $366,860 per QALY, while incorporating a utility value reported by Vedadi et al. (2020)10 for the post-progression state (mean utility of 0.60) resulted in an ICER of $410,613 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Generalizability of the trial results to the population likely to be treated in clinical practice: Data from the CASPIAN trial were used to inform the sponsor’s submitted model. Patients in the CASPIAN trial were limited to those with an ECOG PS of 0 or 1, which is not consistent with the patient population seen in Canadian clinical practice, according to the clinical experts consulted by CADTH. As patients who would receive durvalumab + EP in clinical practice are likely to have a higher ECOG performance status score (worse function) at the start of treatment than those seen in the CASPIAN trial, the extrapolated OS and PFS curves estimated by the sponsor were not aligned with the expected survival of the population most likely to be seen in clinical practice, according to the experts consulted by CADTH, with OS and PFS substantially higher than expected. The clinical experts consulted by CADTH for this review did note that they expected the relative treatment effect of durvalumab + EP in comparison with EP alone to remain similar for patients with a higher ECOG PS. CADTH requested models from the sponsor based on subgroups by ECOG PS (i.e., 0 and 1) in an attempt to predict the direction of effect on the ICER for patients with a higher initial ECOG PS compared to those with a lower initial ECOG PS, given the expected differences in underlying survival. The sponsor provided only a response highlighting the similarity in relative treatment effect associated with durvalumab + EP in patients of ECOG PS of 0 and 1 within the CASPIAN trial with regards to OS, consistent with the prediction made by the experts consulted by CADTH. However, because the sponsor declined to provide the requested models, it is not known whether the difference in patient populations would lead to an overestimated or underestimated ICER for the trial population compared with what would be expected if all patients expected to be treated in practice were included. As the submitted model primarily reflects the trial population and not the population expected to be treated in Canadian practice, interpretation of the cost-effectiveness of durvalumab + EP is subject to substantial uncertainty.
CADTH was unable to address this limitation in its reanalyses.
Long-term efficacy of durvalumab + EP is uncertain: The CASPIAN trial reported approximately 2 years of follow-up data, with a final analysis cut-off date of January 27, 2020. The sponsor fitted several survival curves to extrapolate the data from the observed trial period for both PFS and OS to account for the model’s time horizon (Table 10). Approximately 68% of incremental QALYs within the model were accrued during the extrapolated period, which is associated with a substantially higher degree of uncertainty compared with the incremental costs that accrued primarily during the observation period. While the sponsor’s choice of log-logistic and spline odds 1 knot extrapolations for OS and PFS, respectively, and their base case appears to be appropriate in terms of matching the observed data, the clinical experts consulted by CADTH remained unconvinced that survival rates would be as high as predicted at 5 and 10 years. Input received from clinician groups also indicated that the proportion of patients who survive for more than 2 years under current standards of care are relatively low, which is consistent with the view of the clinical experts consulted by CADTH that long-term survival in the model may be higher than anticipated.
As noted in the limitation above, the available clinical data informing the submitted model is for patients with an ECOG PS of 0 or 1. The clinical experts consulted by CADTH indicated that inclusion of patients with a more severe ECOG PS, such as those that would be seen in clinical practice, would likely decrease long-term survival for both groups compared to the curves used in the model that are based on an extrapolation of the CASPIAN trial data. As a result, the long-term comparative efficacy of durvalumab in the whole population likely to be treated remains uncertain, and the cost-effectiveness of durvalumab + EP in such a scenario remains uncertain as well.
CADTH was unable to address this limitation in its base-case reanalysis as the trial population is different from the population expected in Canadian practice and there are no representative curves. Using feedback from the clinical experts indicating that long-term OS would likely be lower in the full population and therefore may be better represented by the spline odds 1 knot extrapolation, CADTH tested this OS extrapolation curve in a scenario analysis as a plausible alternative. The gamma extrapolation for OS and the generalized gamma extrapolation for PFS were also tested in scenarios, both separately and together, to explore the resulting ICER under substantially more pessimistic PFS and OS assumptions than predicted in the base case.
The approach to modelling health utilities overestimated incremental QALYs: In the sponsor’s base case, health utilities were based on a patient’s TTD, with patients only experiencing a decrease in utility approximately 2 months before death, regardless of disease progression. CADTH had concerns over the validity of this approach, as there is limited evidence on how the time points corresponding to a change in utility within the sponsor’s base case would correspond to key changes in a patient’s quality of life. Due to the sponsor’s selected cut-offs for changes in patient quality of life, lower utility values were applied for only a short amount of time. As a result, even extreme differences in a patient’s assumed quality of life near death had minimal impact on the ICER, decreasing the plausibility that the TTD method as applied in this model appropriately reflects patient experience. Additionally, some of the TTD utility values lack face validity. The average Canadian health utility as reported by Statistics Canada is 0.863,11 which indicates that a health utility of
|||||just 3 months before death due to ES-SCLC appears to be unexpectedly high and is unlikely to be representative of patients’ experiences with progressed ES-SCLC. There are also potential biases in the relative health of patients who could respond to quality-of-life measures within the trial versus those who were no longer well enough or available to respond, particularly as they approached death, which may have led to higher-than-expected utilities being derived from the CASPIAN trial. This may have been exacerbated by the exclusion of patients with an ECOG PS above 1 at baseline. Together, these brief TTD categorizations and the high utility weights likely overestimated the incremental QALYs associated with durvalumab + EP. In the absence of more appropriate TTD utility cut-offs, incorporating pre- and post-progression utility values may be more appropriate.In its base case, CADTH incorporated state-specific utility values derived from Vedadi et al.10 for both the progression-free and progressed health states. Scenarios analyses were also run incorporating progression status–based health-state utilities derived from both the CASPIAN trial2 and Labbe (2017).12 To further explore the uncertainty associated with the implementation and values of utilities used in the model, CADTH ran a series of scenario analyses changing the utility weights of the TTD utilities.
Use of subsequent therapy underestimated: The sponsor’s model included second-line chemotherapy treatment for
||||% of patients in both groups after progression, consistent with its analysis of the Alberta Oncology Outcomes real-world dataset.8 According to the sponsor, the proportion of patients who received second-line chemotherapy in the CASPIAN trial (i.e., > 40%) was too high to represent current Canadian clinical practice. However, the clinical experts consulted by CADTH disagreed with the sponsor’s assumption, estimating that approximately 40% of patients do in fact receive second-line chemotherapy after progression in current Canadian clinical practice.While the sponsor provided a scenario analysis in which |% of modelled durvalumab + EP patients and
||||% of EP-alone patients received second-line chemotherapy, citing CASPIAN trial data, CADTH was unable to locate these inputs in the submitted CASPIAN clinical study reports or publications. CADTH assumed that |% of durvalumab + EP patients and|||% of EP-alone patients would receive second-line chemotherapy, consistent with those reported in the final analysis (data cut-off of January 27, 2020) of the CASPIAN trial.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
A 10-year time horizon is adequate to capture differences in benefits and costs of durvalumab + EP and EP alone. | Acceptable, given the life-expectancy of patients with ES-SCLC in clinical practice. However, as more than 1% of patients were still alive at the end of 10 years in the base case, which may overestimate overall survival, scenarios were run by CADTH to explore the impact of 12- and 15-year time horizons (Table 13). The maximum duration of durvalumab therapy was extended beyond the model’s default 10 years for these scenarios. |
Durvalumab + EP patients receive durvalumab until disease progression, while patients receiving EP alone receive a maximum of 6 cycles. | Acceptable, and consistent with the durvalumab product monograph4 and regimen guidance, such as Cancer Care Ontario’s regimen monographs for EP.13 As the clinical experts consulted by CADTH indicated that patients in clinical practice rarely receive more than 4 cycles of EP, a scenario was run limiting EP treatment to 4 cycles. |
Grade 1 and 2 adverse events from the CASPIAN trial were excluded from the model. | Acceptable, as impacts of minor differences between groups are not expected to result in substantial impacts on patient quality of life or health care resource costs. |
Subsequent therapy costs can be applied as a 1-time cost at the time of discontinuation of first-line therapy. | Inappropriate. Not all patients will survive to receive the average 3 months of subsequent therapy. As durvalumab + EP has an overall survival advantage in the model, this is likely to bias costs in favour of durvalumab + EP. However, CADTH reviewers did not consider this bias would substantively affect results and did not consider it a limitation. |
Subsequent therapy costs include only second-line therapies. | Acceptable. Only a small proportion of ES-SCLC patients receive third-line therapies, and they are relatively inexpensive and unlikely to substantially differ between first-line-therapy groups. |
Dose intensity of durvalumab is | Acceptable. Patients in the CASPIAN trial required dose interruptions and delays leading to a lower overall dose intensity; patients in clinical practice are also expected to sometimes require interruptions or delays. A scenario analysis was run to test the impact of assuming that all patients would receive durvalumab at product monograph recommended intervals (i.e., 100% dose intensity), as shown in Table 13. |
EP = etoposide-platinum (carboplatin or cisplatin); ES-SCLC = extensive-stage small cell lung cancer.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH reanalyses, which addressed several limitations within the economic model, are summarized in Table 5. CADTH was unable to adjust for the absence of patients with a higher ECOG PS in the available clinical data, address uncertainty in the OS and PFS extrapolations, or include TTD utilities over a more relevant time frame. Comparator costs are based on publicly available list prices and may not reflect actual costs paid by public drug plans.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | ||
Changes to derive the CADTH base case | ||
1. Health-state utilities | Source: CASPIAN trial time-to-death utilitiesa < 28 days: 28 to 62 days: ≥ 63 days: | Source: Vedadi (2020) health state utilitiesb Progression-free: 0.72 Progressed: 0.60 |
2. Proportion of patients getting second-line chemotherapy | Source: Alberta O2 Health Databasec Durvalumab + EP: EP: | Source: CASPIANa Durvalumab + EP: EP: |
CADTH base case | 1 + 2 | |
Alberta O2 = Alberta Oncology Outcomes; EP = etoposide-platinum (carboplatin or cisplatin).
bVedadi et al. (2020).10
cAlberta Oncology Outcomes study data.8
CADTH’s base-case results are presented in Table 6. Disaggregated results of the CADTH reanalysis are presented in Table 12. In CADTH’s base case, durvalumab + EP was associated with a cost of $186,802 and 1.11 QALYs over a 10-year time horizon. Approximately 34% of incremental QALYs and 86% of incremental costs accrued during the period for which there was observed data, while the remainder accrued during the extrapolation period. When compared with EP alone, the incremental cost of durvalumab + EP was estimated to be $124,591, while providing 0.28 additional QALYs, resulting in an ICER of $441,635 per QALY gained. Zero percent of iterations would be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | EP | 60,325 | 1.04 | Reference |
Durvalumab + EP | 184,630 | 1.39 | 353,824 | |
CADTH reanalysis 1: Health-state utilities | EP | 60,822 | 0.84 | Reference |
Durvalumab + EP | 184,443 | 1.14 | 426,765 | |
CADTH reanalysis 2: Subsequent treatments | EP | 62,201 | 1.06 | Reference |
Durvalumab + EP | 191,743 | 1.42 | 373,067 | |
CADTH base case | EP | 62,211 | 0.83 | Reference |
Durvalumab + EP | 186,802 | 1.11 | 441,635 |
EP = etoposide-platinum (carboplatin or cisplatin); ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
Scenario analyses were conducted using the CADTH base case to investigate the impact of extending the time horizon, increasing the dose intensity of durvalumab + EP, assuming health-state utilities from different sources, assuming doubling and halving the utility decrements between TTD time points, assuming different OS and PFS extrapolations, and limiting the number of EP cycles to 4. Results for these scenario analyses ranged from $360,705 to $625,719 per QALY, depending on the scenario, with the more pessimistic survival extrapolations having the largest impact on the ICER. Under no scenario did durvalumab + EP approach an ICER considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY at the submitted price (Table 13).
Price-Reduction Analyses
Price-reduction analyses were conducted using both the sponsor’s and CADTH’s base case (Table 7). When considering the CADTH base case, the submitted price of durvalumab would need to be reduced by approximately 88% for durvalumab + EP to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for durvalumab + EP vs. EP ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $353,824 | $441,635 |
20% | $286,793 | $351,326 |
40% | $213,055 | $266,498 |
60% | $140,653 | $177,424 |
80% | $68,961 | $86,126 |
90% | $33,016 | $41,949 |
EP = etoposide-platinum (carboplatin or cisplatin); ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Overall Conclusions
The CASPIAN trial provided evidence demonstrating the efficacy, in terms of OS, as well as the safety of durvalumab + EP OS in adult patients with ES-SCLC compared to EP alone. The improvement associated with durvalumab + EP in median OS was considered statistically significant and clinically relevant by the clinical experts consulted by CADTH, while differences in landmark OS observed at 12 months, 18 months, and 24 months were also considered clinically relevant by the clinical experts consulted by CADTH, although the landmark OS data are associated with uncertainty.
The CADTH review identified several major limitations with the submitted economic evaluation, including uncertainty in the generalizability of the results from the modelled patient population to those most likely to be treated in clinical practice due to the exclusion from the CASPIAN trial of patients with an ECOG performance status greater than 1, uncertainty in the extrapolation of OS and PFS curves from observed data, the probable overestimation of accrued QALYs due to a TTD methodology used to apply patient utilities that did not align with key time points associated with major changes in patient quality of life, and an underestimate of subsequent therapies used by modelled patients.
In its reanalyses, CADTH incorporated utility values associated with being in a progression-free or progressed state and revised the proportion of patients receiving a subsequent chemotherapy to be consistent with that reported in the CASPIAN trial. In the CADTH base case, durvalumab + EP was associated with an ICER of $441,635 per QALY gained compared to EP alone. Under the CADTH base-case assumptions, a price reduction of 88% would be required for durvalumab to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained.
CADTH was unable to address limitations with the generalizability of the clinical evidence to patients with a higher initial ECOG performance status. There is also uncertainty associated with the extrapolation of OS and PFS curves over the 10-year time horizon from the 2 years of observed data, as more than 65% of incremental QALYs gained in the model accrued during the model’s extrapolated period, for which there are no observed data. A series of scenario analyses were conducted exploring other areas of uncertainty in the submitted model. Scenarios with more pessimistic OS and PFS extrapolation estimates led to substantially higher ICERs.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab), 50 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc.; 2020 Dec 1.
2.Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929-1939. PubMed
3.Clinical Study Report: D419QC00001. A phase III, randomized, multicenter, open-label, comparative study to determine the efficacy of durvalumab or durvalumab and tremelimumab in combination with platinum-based chemotherapy for the first-line treatment in patients with extensive disease small-cell lung cancer (SCLC) (CASPIAN) (updated analysis) [internal sponsor's report]. Gaithersburg (MD): AstraZeneca; 2020 Aug 26.
4.Imfinzi (durvalumab): concentrate for solution for infusion, 50 mg / mL, intravenous [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2020 Sep 21.
5.DeltaPA. Ottawa (ON): IQVIA; 2020: https://www.iqvia.com/. Accessed 2021 Jan 28.
6.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2021 Jan 30.
7.Xie F, Pullenayegum E, Gaebel K, et al. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
8.Treatment patterns in Canada: retrospective database analysis to assess treatment patterns, clinical outcomes, cost and health care resource utilization in extensive-stage small cell lung cancer in Alberta [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Imfinzi (durvalumab), 50 mg/mL concentrate for solution for intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc; 2020 Dec 1.
9.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
10.Vedadi A, Shakik S, Brown MC, et al. The impact of symptoms and comorbidity on health utility scores and health-related quality of life in small cell lung cancer using real world data. Qual Life Res. 2021;30(2):445-454. PubMed
11.Guertin JR, Humphries B, Feeny D, Tarride JE. Health Utilities Index Mark 3 scores for major chronic conditions: population norms for Canada based on the 2013 and 2014 Canadian Community Health Survey. Health Rep. 2018;29(11):12-19. PubMed
12.Labbe C, Leung Y, Silva Lemes JG, et al. Real-world EQ5D health utility scores for patients with metastatic lung cancer by molecular alteration and response to therapy. Clin Lung Cancer. 2017;18(4):388-395 e384. PubMed
13.Cancer Care Ontario. Cancer Care Ontario: funded evidence-informed regimens. 2020; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2021 Jan 31.
14.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2018. Toronto (ON): Canadian Cancer Society; 2018: http://www.cancer.ca/Canadian-Cancer-Statistics-2018-EN. Accessed 2021 Feb 05.
15.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics: a 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-cancer-statistics-2020_special-report_EN.pdf. Accessed 2021 Feb 05.
16.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
17.Table: 17-10-0005-01. Population estimates on July 1st, by age and sex. Ottawa (ON): Statistics Canada; 2020: 10.25318/1710000501-eng. Accessed 2021 Feb 05.10.25318/1710000501-eng
18.Indigenous Services Canada. Non-Insured Health Benefits Program: annual report 2018/2019. 2020: https://www.sac-isc.gc.ca/DAM/DAM-ISC-SAC/DAM-HLTH/STAGING/texte-text/nihb-Annual_Report_2018-19_1589921777815_eng.pdf. Accessed 2021 Feb 03.
Appendix 1: Cost Comparison Table
Note that this appendix has been formatted for accessibility but has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison for Extensive-Stage Small Cell Lung Cancer
Treatment | Strength/ concentration | Form (vial size if single-use) | Price | Recommended dosage | Daily cost | Per 21-day cycle cost |
|---|---|---|---|---|---|---|
Durvalumab + etoposide + platinum-based chemotherapy | ||||||
Durvalumab (Imfinzi) | 50 mg/mL | Concentrate solution for infusion 2.4 mL 10 mL | . . 938.6700a 3,911.1100a | 1,500 mg in combo with chemotherapy every 3 weeks for 4 cycles, then 1,500 mg every 4 weeks as monotherapyb | $558.71 Monotherapy thereafter: $419.04 | $11,733 Per 28 days monotherapy thereafter: $11,733 |
Etoposide (generics) | 20 mg/mL | Injection 5 mL 10 mL 25 mL 50 mL | . 75.0000 150.0000 375.0000 750.0000 | 100 mg/m2 on days 1 to 3 every 3 weeks for 4 cyclesc | $21.43 | $450 |
Carboplatin (generics) | 10 mg/mL | Solution for injection 5 mL 15 mL 45 mL 60 mL | . . 70.0000 210.0000 600.0000 775.0000 | AUC 5 on day 1 every 3 weeks for 4 cyclesc | $28.57 | $600 |
Cisplatin (generics) | 1 mg/mL | Injection 50 mL 100 mL | . 135.0000 270.0000 | 75 mg/m2 on day 1 every 3 weeks for 4 cyclesc | $19.29 | $405 |
Durvalumab + etoposide + either carboplatin or cisplatin | $599.42 to $608.71 Monotherapy thereafter: $419.04 | $12,588 to $12,783 Per 28 days monotherapy thereafter: $11,733 | ||||
Etoposide + platinum-based chemotherapy | ||||||
Etoposide (generics) | 20 mg/mL | Injection 5 mL 10 mL 25 mL 50 mL | . 75.0000 150.0000 375.0000 750.0000 | 100 mg/m2 on days 1 to 3 every 3 weeks for 4 to 6 cyclesc | $21.43 | $450.00 |
Carboplatin (generics) | 10 mg/mL | Solution for injection 5 mL 15 mL 45 mL 60 mL | . . 70.0000 210.0000 600.0000 775.0000 | AUC 5 on day 1 every 3 weeks for 4 to 6 cyclesc | $28.57 | $600.00 |
Cisplatin (generics) | 1 mg/mL | Injection 50 mL 100 mL | . 135.0000 270.0000 | 75 mg/m2 on day 1 every 3 weeks for 4 to 6 cyclesc | $19.29 | $405.00 |
Etoposide + either carboplatin or cisplatin | $40.71 to $50.00 | $855 to $1,050 | ||||
AUC = target area under the concentration vs. time curve.
Note: All prices are IQVIA Delta PA database wholesale list prices (accessed January 2021), unless otherwise indicated, and do not include dispensing fees or administration. Assumes a 70 kg patient with a body surface area of 1.8 m2 and a glomerular filtration rate of 61.7 mL/min. Wastage of excess medication in vials is also assumed.
aSponsor’s submitted price.
bPatients with a body weight less than 30 kg must receive weight-based dosing at 20 mg/kg on the same schedule, until their weight increases to more than 30 kg.
c4 to 6 cycles unless disease progression or unacceptable toxicity occurs.
Appendix 2: Submission Quality
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | See issues with generalizability of the trial data to the indicated population in the key limitations section |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Figure 1: Kaplan-Meier Plot and Extrapolated OS for Durvalumab + EP
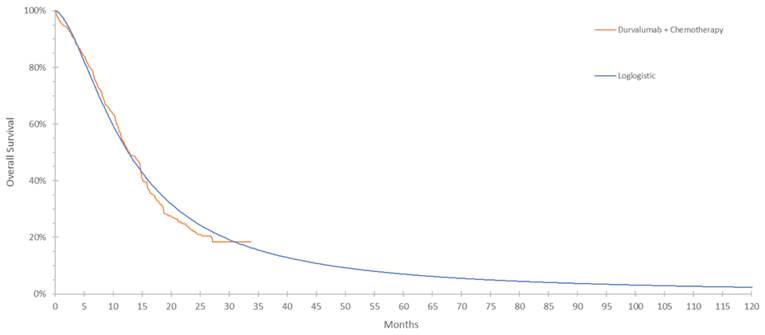
CI = confidence interval; EP = etoposide and either carboplatin or cisplatin; OS = overall survival.
Source: Adapted from Figure 5.5 in sponsor’s pharmacoeconomic submission.1
Figure 2: Kaplan-Meier Plot and Extrapolated OS for EP Alone
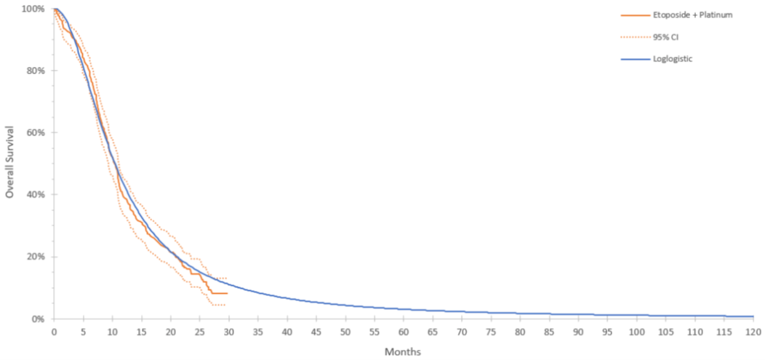
CI = confidence interval; EP = etoposide and either carboplatin or cisplatin; OS = overall survival.
Source: Figure 5.6 in sponsor’s pharmacoeconomic submission.1
Figure 3: Kaplan-Meier Curves, Sponsor’s Chosen Extrapolations, and RWE for OS
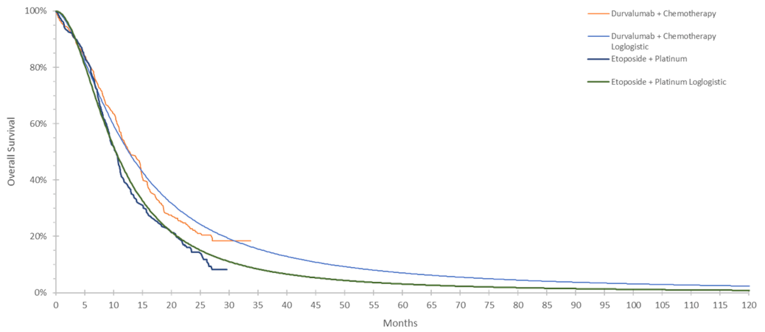
ECOG = Eastern Cooperative Oncology Group; OS = overall survival; PS = performance status; RWE = real-world evidence.
Source: Adapted from Figure 5.7 in sponsor’s pharmacoeconomic submission.1
Figure 4: Kaplan-Meier Plot and Extrapolated PFS for Durvalumab + EP
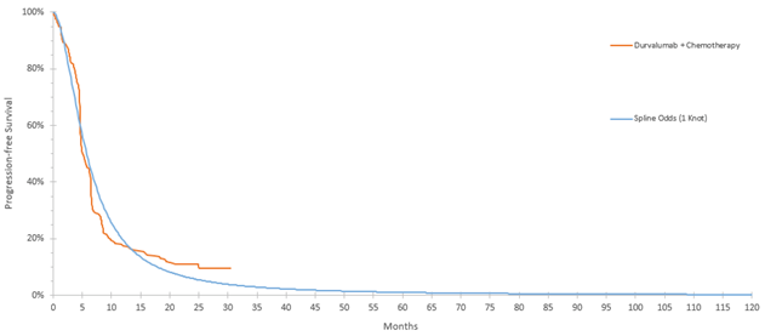
CI = confidence interval; EP = etoposide and either carboplatin or cisplatin; PFS = progression-free survival.
Source: Adapted from Figure 5.9 in the sponsor’s pharmacoeconomic submission.1
Figure 5: Kaplan-Meier Plot and Extrapolated PFS for EP Alone
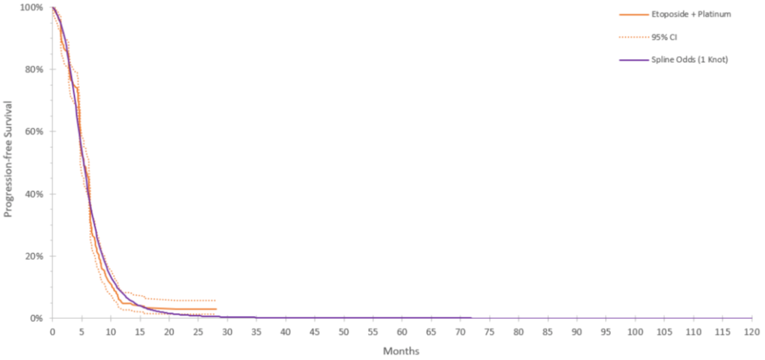
CI = confidence interval; EP = etoposide and either carboplatin or cisplatin; PFS = progression-free survival.
Source: Figure 5.10 in sponsor’s pharmacoeconomic submission.1
Table 10: Parametric Extrapolations in Sponsor’s Base Case and CADTH Scenario Analyses
Distribution | Durvalumab + EP | EP alone | ||||||
|---|---|---|---|---|---|---|---|---|
1 year | 2 years | 5 years | 10 years | 1 year | 2 years | 5 years | 10 years | |
Overall survival | ||||||||
CASPIAN data | 52.4% | 22.2% | NA | NA | 39.3% | 14.4% | NA | NA |
Log-logistic (base case) | 52.1% | 25.6% | 7.0% | 2.3% | 43.0% | 16.2% | 3.1% | 0.8% |
Spline odds 1-knot (sponsor and CADTH scenario) | 53.6% | 22.6% | 4.3% | 1.1% | 43.6% | 13.2% | 1.7% | 0.3% |
Gamma (CADTH scenario) | 53.3% | 23.6% | 1.6% | 0.0% | 44.8% | 13.6% | 0.2% | 0.0% |
Progression-free survival | ||||||||
CASPIAN data | 17.9% | 11.0% | NA | NA | 5.3% | 2.9% | NA | NA |
Spline odds 1-knot (base case) | 19.5% | 5.9% | 1.0% | 0.3% | 7.9% | 0.9% | 0.0% | 0.0% |
Generalized gamma (CADTH scenario) | 23.3% | 7.0% | 0.6% | 0.0% | 10.5% | 0.6% | 0.0% | 0.0% |
EP = etoposide and either carboplatin or cisplatin; NA = not applicable.
Source: Sponsor’s pharmacoeconomic submission; adapted from economic model.1
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Drug | Durvalumab + EP | EP | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 1.71 | 1.28 | 0.42 |
By health state | |||
Pre-progression | 0.75 | 0.52 | 0.23 |
Post-progression | 0.96 | 0.76 | 0.20 |
Discounted QALYs | |||
Total | 1.39 | 1.04 | 0.35 |
By health state | |||
≥ 91 days to death | 1.22 | 0.86 | 0.36 |
63 – 90 days to death | 0.06 | 0.06 | (0.002) |
28-62 days to death | 0.07 | 0.07 | (0.002) |
< 28 days to death | 0.05 | 0.05 | (0.001) |
AE decrement | −0.001 | −0.001 | 0.00 |
Discounted Costs ($) | |||
Total | $184,630 | $60,325 | $124,305 |
Drug acquisition – first line | $129,050 | $5,289 | $123,760 |
Administration – first line | $5,175 | $4,262 | $913 |
Subsequent treatment – second line | $1,442 | $1,326 | $116 |
PCI and other radiotherapy | $858 | $1,300 | ($442) |
Scans and monitoring – on treatment | $2,187 | $939 | $1,249 |
Scans and monitoring – off treatment | $1,311 | $1,354 | ($44) |
Terminal care | $41,451 | $42,314 | ($863) |
Adverse events | $3,157 | $3,540 | ($384) |
ICER ($/LY) | $282,209 | ||
ICER ($/QALY) | $341,078 | ||
AE = adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; PCI = prophylactic cranial irradiation; QALY = quality-adjusted life-year.
Source: Adapted from sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Drug | Durvalumab + EP | EP | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 1.71 | 1.28 | 0.42 |
By health state | |||
Pre-progression | 0.75 | 0.52 | 0.23 |
Post-progression | 0.96 | 0.76 | 0.20 |
Discounted QALYs | |||
Total | 1.11 | 0.83 | 0.28 |
By health state | |||
Pre-progression | 0.54 | 0.37 | 0.16 |
Post-progression | 0.58 | 0.46 | 0.12 |
AE decrement | −0.001 | −0.001 | 0.000 |
Discounted costs ($) | |||
Total | $186,802 | $62,211 | $124,591 |
Drug acquisition – first line | $129,169 | $5,292 | $123,877 |
Administration – first line | $5,153 | $4,250 | $903 |
Subsequent treatment – second line | $3,454 | $3,139 | $315 |
PCI and other radiotherapy | $850 | $1,297 | ($447) |
Scans and monitoring – on treatment | $2,383 | $1,114 | $1,269 |
Scans and monitoring – off treatment | $1,211 | $1,264 | ($53) |
Terminal care | $41,451 | $42,313 | ($862) |
Adverse events | $3,129 | $3,541 | ($412) |
ICER ($/LY) | $293,348 | ||
ICER ($/QALY) | $441,635 | ||
AE = adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; PCI = prophylactic cranial irradiation; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: CADTH Scenario Analyses
Scenario | CADTH base case | CADTH scenario | ICER ($ per QALY) | ||
|---|---|---|---|---|---|
Sponsor base case | 353,824 | ||||
CADTH base case | 441,635 | ||||
Scenario analyses | |||||
Scenario A: 12-year time horizon | Time horizon: 10 years | Time horizon: 12 years | 425,308 | ||
Scenario B: 15-year time horizon | Time horizon: 10 years | Time horizon: 15 years | 410,470 | ||
Scenario C: Dose intensity | Durvalumab intensity: | Durvalumab intensity: 100% | 461,468 | ||
Scenario D: EP duration limited | Max EP duration: 6 cycles | Max EP duration: 4 cycles | 455,671 | ||
Scenario E: CASPIAN health-state utilities | PFS: 0.72 Progressed: 0.60 | PFS: Progressed: | 368,352 | ||
Scenario F: Labbe (2017) health-state utilities | PFS: 0.72 Progressed: 0.52 | 471,328 | |||
Scenario G: Time-to-death utility farthest from death unchanged, increments doubled | Sponsor’s TTD utilitiesa ≥ 63 days: 28 to 62 days: < 28 days: | ≥ 63 days: 28 to 62 days: < 28 days: | 362,017 | ||
Scenario H: Time-to-death utility farthest from death unchanged, increments halved | ≥ 63 days: 28 to 62 days: < 28 days: | 360,705 | |||
Scenario I: Time-to-death utility nearest to death lowered, increments unchanged | ≥ 63 days: 28 to 62 days: < 28 days: | 447,605 | |||
Scenario J: Spline odds 1 knot extrapolation for overall survival | Log-logistic | Spline odds 1 knot | 521,360 | ||
Scenario K: Overall survival pessimistic extrapolation | Log-logistic | Gamma | 612,691 | ||
Scenario L: progression-free survival pessimistic extrapolation | Spline Odds Knot 1 | Generalized Gamma | 453,022 | ||
Scenario M: Overall and progression-free pessimistic extrapolation | K + L | K + L | 625,719 | ||
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TTD = time-to-death.
aThe CADTH base case uses health-state utilities based on progression, therefore the TTD utilities from the sponsor’s base case are presented here for comparison. CADTH’s reanalysis 2 (Table 5 and Table 6) can be directly compared to these reanalyses (ICER = $373,067 per QALY).
Appendix 5: Submitted Business Impact Analysis and CADTH Appraisal
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 14: CADTH Summary Findings from the Sponsor’s Business Impact Analysis
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an incidence-based budget impact analysis (BIA), assessing the expected budgetary impact from the introduction of durvalumab plus EP (Formulary with durvalumab scenario) for patients with ES-SCLC receiving first-line treatment, over a 3-year time horizon (2022 to 2024), from the perspective of Canadian public drug payers. The population in the model was consistent with the indicated population, and the comparator was treatment with EP alone (Formulary without durvalumab scenario).
Data for the model were obtained from various sources including: the CASPIAN clinical trial,2,3 Canadian Cancer Society data,14-16 an analysis conducted by the sponsor on Alberta Oncology Outcomes study data,8 Statistics Canada,17 and the NIHB annual report.18 The sponsor included drug acquisition costs, including wastage, as well as administration costs in the base case; dispensing fees and mark-ups were not included.
Key inputs to the BIA are documented in Table 15. Assumptions made by the sponsor included:
The average patient in Canadian clinical practice is similar to the average patient in the CASPIAN trial
All patients eligible for durvalumab + EP would otherwise receive EP alone
IQVIA Delta PA list prices can be used as a proxy for the drug acquisition costs paid by jurisdictional plans.
Table 15: Summary of Sponsor’s Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) |
|---|---|
Target population | |
Canadian adult population (2022 to 2024, excluding Quebec)a National lung cancer incidence (per 100,000) Proportion SCLC Proportion ES-SCLC Proportion ES-SCLC receiving first-line therapy Proportion patients eligible for public funding | 24,174,960 / 24,524,995 / 24,880,423 97b 12.1%c 67.4%d 54.8%e 100%f |
Number of patients eligible for drug under review | 951 / 964 / 978 |
Market uptake (3 years) | |
Uptake (reference scenario; without durvalumab) | |
EP | 100% / 100% / 100% |
Uptake (new drug scenario; with durvalumab) | |
Durvalumab + EP EP |
|
Cost of treatment (per patient) | |
Cost of treatment per 2-week period, assuming wastageg | |
Durvalumab + EP EP | $8,188 for first 4 cycles, $5,632 thereafter until progression $1,357 for 4 to 6 cycles |
Cost of administration | |
Durvalumab + EP EP | $656 for first 4 cycles, $98 thereafter until progression $525 for 4 to 6 cycles |
EP = etoposide and either carboplatin (46%) or cisplatin (54%)8; ES-SCLC = extensive-stage small cell lung cancer; SCLC = small cell lung cancer.
aCalculated from jurisdictional populations by CADTH. Source: Statistics Canada17
bWeighted average jurisdictional incidence. Source: Brenner et al. (2020).16
cWeighted average by gender. Source: Canadian Cancer Society (2020).15
dPercentage of SCLC patients in Stage IV. Source: Canadian Cancer Society (2018).14
ePercentage of de novo ES-SCLC patients who initiated first-line chemotherapy from the Alberta Oncology Outcomes database analysis.8
fAssumption, based on all comparators being publicly funded hospital drugs.
gDuration of therapy was based on the CASPIAN trial,2,3 and consistent with the durvalumab product monograph4 and the Cancer Care Ontario regimen monograph for EP.13 Drug costs for comparators are based on wholesale prices as listed in IQVIA Delta PA.5
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s base case suggest that the incremental budget impact, including wastage and administration, associated with the reimbursement of durvalumab + EP for the first-line treatment of ES-SCLC would be $22,666,017 in year 1, $65,653,953 in year 2, and $87,837,528 in year 3, for a cumulative 3-year budget impact of $176,157,498.
The sponsor ran a number of sensitivity analyses testing alternate inputs or assumptions, varying: the BSA or creatine clearance of patients, the proportion of patients with ES-SCLC who receive first-line therapy or are eligible for public funding, the market share capture of durvalumab + EP in each year, and the proportion of patients on durvalumab + EP or EP alone who receive carboplatin as part of first-line therapy. Of these, the proportion of patients receiving first-line treatment had the largest impact on results. Scenario analyses were also run by the sponsor, including an analysis where administration costs were excluded that led to a 3-year budget impact of $174,270,171, and 1 which included the cost of second-line chemotherapy, where the estimated 3-year budget impact was $176,137,318.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Proportion of patients receiving first-line therapy is underestimated: The proportion of ES-SCLC patients receiving first-line therapy (54.8%) was considered to be underestimated by the clinical experts consulted by CADTH. Their estimation was that close to 80% of patients with ES-SCLC would begin a first-line treatment. The sponsor’s assumption underestimated the potential market size and resulting budget impact with durvalumab + EP.
CADTH assumed 80% of ES-SCLC patients would receive a first-line chemotherapy. In a scenario analysis, CADTH lowered this assumption to 70%.
Uptake of durvalumab in the first year is underestimated: The sponsor assumed a
|% uptake of durvalumab in the first year. Given that the standard of care for first-line treatment of ES-SCLC has not changed in 30 years, and both patient and clinician group input indicated a high degree of need for a new therapy, the anticipated uptake of durvalumab is likely to be larger. The clinical experts consulted by CADTH estimated that 60% to 70% of patients who would otherwise be treated with EP alone would instead receive durvalumab + EP in its first year of reimbursement. This is also consistent with drug plan input predicting a substantially higher uptake of durvalumab than predicted by the sponsor. The sponsor’s assumption is likely to underestimate the anticipated budget impact of durvalumab.CADTH assumed that 60% of eligible patients would receive durvalumab + EP in the first year of its reimbursement in the base case, while 70% was assumed in a scenario analysis.
Administration costs are not appropriate from a drug payer perspective: As the base case BIA is intended to be presented from the perspective of a public drug plan, administration costs should only be included in scenario analyses.
CADTH excluded administration costs from its base-case analysis, reintroducing them instead in a scenario analysis.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by increasing the proportion of patients who receive first-line therapy to 80%, increasing the proportion of eligible patients who would receive durvalumab + EP in the first year of its availability to 60%, and excluding administration costs. Table 16 outlines the parameters used by the sponsor in comparison to those used by CADTH.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Proportion of patients who receive a first-line therapy | 54.8% | 80% |
2. Proportion of eligible patients receiving durvalumab in first year of availability |
| 60% |
3. Exclusion of administration costs from a drug plan perspective | Administration costs included | Administration costs excluded |
CADTH base case | — | 1 + 2 + 3 |
Applying these changes increased the total 3-year budget impact associated with the introduction of durvalumab + EP for the treatment of adults with ES-SCLC to $283,353,601. The results of the CADTH step-wise reanalyses are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $176,157,498 |
CADTH reanalysis 1: Increased proportion receiving first-line treatment to 80% | $257,106,585 |
CADTH reanalysis 2: Increased uptake in year 1 | $196,258,846 |
CADTH reanalysis 3: Exclusion of administration costs | $174,270,171 |
CADTH base case | $283,353,601 |
CADTH also conducted scenario analyses considering:
The 88% price reduction at which durvalumab would be considered cost-effective at a $50,000 per QALY threshold in the CADTH base-case economic evaluation.
The inclusion of administration costs.
A reduced proportion of patients receiving a first-line therapy (70%).
A reduced proportion of patients receiving a first-line therapy, as assumed by the sponsor (54.8%).
An increased uptake of durvalumab + EP of 70% of eligible patients in the first year of its reimbursement.
Of the scenarios incorporating the submitted price of durvalumab, lowering the proportion of ES-ECLC patients assumed to receive a first-line therapy down to 70% rather than 80% had the largest effect on results, (Table 18), while assuming the 88% price reduction for durvalumab at which durvalumab + EP would be considered cost-effective in the CADTH economic evaluation led to a much smaller estimated budget impact.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $6,544,924 | $7,557,422 | $7,662,944 | $7,770,067 | $22,990,434 |
New drug | $6,544,924 | $30,223,440 | $73,316,897 | $95,607,595 | $199,147,932 | |
Budget impact | $0 | $22,666,017 | $65,653,953 | $87,837,528 | $176,157,498 | |
CADTH base case | Reference | $5,385,254 | $6,218,352 | $6,305,177 | $6,393,319 | $18,916,848 |
New drug | $5,385,254 | $55,354,834 | $111,175,575 | $135,740,040 | $302,270,449 | |
Budget impact | $0 | $49,136,482 | $104,870,398 | $129,346,721 | $283,353,601 | |
CADTH scenario analysis: 88% price reduction | Reference | $5,385,254 | $6,218,352 | $6,305,177 | $6,393,319 | $18,916,848 |
New drug | $5,385,254 | $11,681,098 | $18,070,361 | $21,003,228 | $50,754,686 | |
Budget impact | $0 | $5,462,745 | $11,765,183 | $14,609,909 | $31,837,838 | |
CADTH scenario analysis: Admin costs included | Reference | $9,552,491 | $11,030,260 | $11,184,273 | $11,340,621 | $33,555,153 |
New drug | $9,552,491 | $60,652,749 | $117,183,236 | $142,164,209 | $320,000,194 | |
Budget impact | $0 | $49,622,489 | $105,998,963 | $130,823,589 | $286,445,041 | |
CADTH scenario analysis: 70% receive first-line therapy | Reference | $6,544,924 | $7,557,422 | $7,662,944 | $7,770,067 | $22,990,434 |
New drug | $6,544,924 | $41,556,448 | $80,288,514 | $97,404,317 | $219,249,280 | |
Budget impact | $0 | $33,999,026 | $72,625,570 | $89,634,251 | $196,258,846 | |
CADTH scenario analysis: 54.8% receive first-line therapy | Reference | $3,688,899 | $4,259,571 | $4,319,046 | $4,379,423 | $12,958,041 |
New drug | $3,688,899 | $37,918,061 | $76,155,269 | $92,981,927 | $207,055,258 | |
Budget impact | $0 | $33,658,490 | $71,836,223 | $88,602,504 | $194,097,217 | |
CADTH scenario analysis: 70% uptake Year 1 | Reference | 5,385,254 | 6,218,352 | 6,305,177 | 6,393,319 | 18,916,848 |
New drug | 5,385,254 | 63,544,248 | 116,198,310 | 137,028,702 | 316,771,259 | |
Budget impact | $0 | $57,325,896 | $109,893,133 | $130,635,383 | $297,854,411 |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.