CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck
Therapeutic area: Metastatic microsatellite instability-high/mismatch repair-deficient colorectal cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
CCC
Colorectal Cancer Canada
CCRAN
Colorectal Cancer Resource and Action Network
CGOEN
Canadian Gastrointestinal Oncology Evidence Network
CI
confidence interval
CrI
credible interval
DAE
discontinuation due to adverse events
DIC
deviance information criterion
dMMR
mismatch repair deficient
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC
European Organisation for Research and Treatment of Cancer
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels questionnaire
EQ VAS
EuroQol Visual Analogue Scale
FP
fractional polynomial
GI DAC
Gastrointestinal Cancer Drug Advisory Committee
HR
hazard ratio
HRQoL
health-related quality of life
ITC
indirect treatment comparison
ITT
intention to treat
mCRC
metastatic colorectal cancer
MID
minimal important difference
MSI-H
microsatellite instability-high
NMA
network meta-analysis
OR
odds ratio
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
PHA
proportional hazards assumption
PICOS
population, intervention, comparator, outcome, and study
QLQ-C30
Quality of Life Questionnaire Core 30
QLQ-CR29
Quality of Life Questionnaire Colorectal Cancer Module
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumors
RMST
restricted mean survival time
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
SOC
standard of care
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Drug Product Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda) 200 mg administered intravenously |
Indication | As monotherapy, for the first-line treatment of adults with metastatic microsatellite instability-high (MSI-H)/mismatch repair deficient (dMMR) colorectal cancer |
Reimbursement request | As per the indication |
Health Canada approval status | Complete |
Health Canada review pathway | Standard |
NOC date | March 3, 2021 |
Sponsor | Merck |
NOC = Notice of Compliance.
Introduction
Colorectal cancer begins in the colon or rectum and is characterized by cancerous cells that grow into and destroy nearby tissue. In metastatic disease, the tumour spreads to and damages other parts of the body.1 About 70% to 90% of colorectal cancers are diagnosed after symptom onset, although population-based screening is increasing the number of asymptomatic cases identified.2
The Canadian Cancer Society expects colorectal cancer to be the third most commonly diagnosed cancer in Canada in 2020 and the second and third leading cause of death from cancer in men and women, respectively.3 Approximately 20% to 25% of newly diagnosed colorectal cancers are metastatic at the time of diagnosis, where untreated patients with metastatic disease survive only 6 to 10 months.4-6 Despite advances in treatment, less than 20% of patients are alive at 5 years, and unfavourable prognostic factors (e.g., mutations in BRAF, proximal primary tumour location) are associated with survival under 18 months.7
For most patients with metastatic disease, therapy is often palliative and focuses on systemic chemotherapy. The recommended chemotherapeutic regimen varies by jurisdiction and is individualized based on the patient’s health, patient’s ability to tolerate chemotherapy, mutation status, presence of mismatch repair-deficient (dMMR) proteins or microsatellite high instability, location of primary tumour, aggressiveness of disease, and goals of therapy. Monoclonal antibodies are often used in addition to combination chemotherapy to target specific genetic subtypes of colorectal cancer. The microsatellite instability-high (MSI-H)/dMMR subtype may be present in 15%8 of colorectal cancer patients and in about 3.5% to 6.5% of stage IV patients. There is some evidence of favourable prognosis in early-stage disease and a hypothesis that such tumours may have lower metastatic potential.9 However, these patients may benefit less from adjuvant chemotherapy than other patients.9-12
Pembrolizumab is an IV-administered monoclonal antibody that binds PD1 receptors on T cells, reversing T-cell suppression and inducing antitumour responses.
This report’s objective is to summarize a systematic review of the beneficial and harmful effects of pembrolizumab 200 mg administered every 3 weeks intravenously for the first-line treatment of adults with MSI-H/dMMR metastatic colorectal cancer (mCRC).
Stakeholder Perspectives
The information in this section is a summary of input from patient and clinician groups who responded to CADTH’s call for input, from clinical experts consulted by CADTH, and from drug programs that provided input to CADTH for the purpose of this review.
Patient Input
With the assistance of Colorectal Cancer Canada (CCC) and Colorectal Cancer Resource and Action Network (CCRAN), CADTH received feedback from 81 patients, 19 caregivers, and 5 individuals who were both patients and caregivers. Feedback was collected through online surveys, focus groups, and phone interviews. Patients noted the most common symptoms were bloody stools, diarrhea, fatigue, and pain. Most felt that their symptoms affected their daily lives, work, ability to exercise, and quality of life and had a psychological impact leading to various mental health issues. In general, patients hoped therapies could improve physical health and quality of life. Patients were willing to tolerate increasingly significant side effects for improved survival. In addition to improved health and quality of life, treatment funding, symptom improvement, simple administration, and limitation of side effects were important.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Among patients with unresectable or mCRC, the experts identified an unmet need among MSI-H/dMMR patients who would benefit from pembrolizumab. In these patients, the experts felt pembrolizumab could be used as any line of therapy, consequently shifting the current treatment paradigm for these patients. Given the severity and type of disease, a patient with tolerable or manageable adverse events (AEs), preservation of quality of life, tumour response, survival, and stable disease would be considered a responder, while the opposite would be considered treatment failure and likely result in treatment discontinuation.
Clinician Group Input
Three registered clinician groups (the Ontario Health Gastrointestinal Cancer Drug Advisory Committee, the Canadian Gastrointestinal Oncology Evidence Network [CGOEN], and the Medical Advisory Board of the CCC), consisting of 16 clinicians, provided input for this review.
Drug Program Input
Input was obtained from all 9 provinces (ministries of health and/or cancer agencies) participating in CADTH reimbursement reviews. The Provincial Advisory Group identified the following as clinical factors that could impact the implementation:
numerous clinical eligibility criteria
barriers to diagnosing MSI-H/dMMR colorectal cancer and monitoring treatment effects.
The clinical experts consulted by CADTH provided responses that can be found in the Drug Program Input section.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
One open-label randomized controlled trial (RCT) (KEYNOTE-177) was included in this review; the trial compared pembrolizumab 200 mg, intravenously, every 3 weeks to standard of care (SOC) to assess the efficacy and safety in adult patients with unresectable or metastatic MSI-H/dMMR colorectal cancer. The study randomized 307 patients across 120 sites from 23 countries. Notably, patients in the SOC arm were permitted to cross over to the pembrolizumab arm. Further, all patients were permitted to receive subsequent anticancer medications.
Efficacy Results
Median progression-free survival (PFS) was higher in the pembrolizumab group (16.5 months; 95% confidence interval [CI], 5.4 to 32.4) than in the SOC group (8.2 months; 95% CI, 6.1 to 10.2), resulting in a statistically significant hazard ratio (HR) of 0.60 (95% CI, 0.45 to 0.80). However, because the HR may be biased due to a violated proportional hazards assumption (PHA), the restricted mean survival time (RMST) was calculated. The RMST after 24 months of follow-up suggested pembrolizumab survival (13.7 months; 95% CI, 12.0 to 15.4) was higher than SOC survival (10.8 months; 95% CI, 9.4 to 12.2), indicating that patients receiving pembrolizumab for 24 months would survive for an average of 13.7 months, compared to 10.8 months for patients receiving SOC, a difference of 2.9 months (95% CI, 0.7 to 5.1). Because crossovers or use of subsequent anticancer therapies could bias these results, 2 sensitivity analyses were conducted. These analyses yielded similar HRs (HR = 0.61; 95% CI, 0.48 to 0.79, in the first analysis, and HR = 0.63; 95% CI, 0.45 to 0.88, in the second), suggesting the benefit observed in the primary analysis is generally robust. However, the first sensitivity analysis suggested only a small difference in median survival (7.0 months; 95% CI, 4.2 to 12.4, for pembrolizumab, versus 6.3 months; 95% CI, 4.6 to 8.2, for SOC).
Median overall survival (OS) was not reached; however, a statistically non-significant difference in OS was reported (HR = 0.77; 95% CI, 0.54 to 1.09). Three methods leading to 3 sensitivity analyses were conducted to adjust for any bias introduced by crossovers or subsequent use of anti-PD1/PDL1 treatment (but not subsequent use of other anticancer medications). The inverse probability of censoring weighting method (HR = 0.59; 95% CI, 0.32 to 1.24), the rank preserving structural failure time method (HR = 0.72; 95% CI, 0.47 to 1.11) and 2-stage analysis (HR = 0.89; 95% CI, 0.76 to 1.04) led to a wide range of point estimates, suggesting some bias and uncertainty in the primary analysis. While each point estimate suggests pembrolizumab may improve OS, due to variable point estimates, wide CIs, and the lack of statistical significance testing, the exact magnitude of any benefit is uncertain.
The overall response rate (ORR) was higher in the pembrolizumab arm (43.8%; 95% CI, 35.8 to 52.0) than in the SOC arm (33.1%; 95% CI, 25.8% to 41.4%). The between-group difference (10.7%; 95% CI, –0.2% to 21.3%) was statistically insignificant. The exploratory outcome of median time to response was similar in the pembrolizumab and SOC arms (2.2 and 2.1 months, respectively). Another exploratory outcome, median duration of response, could not be compared as there was no reported value in the pembrolizumab arm, but the percentage of patients with an extended response duration was higher in the pembrolizumab arm at 6, 9, 12, 18, and 24 months. Another exploratory analysis, quality of life, was measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) at baseline and at 18 weeks. Scores in the pembrolizumab arm improved from baseline by 3.33 points (95% CI, –0.05 to 6.72), while scores decreased by 5.63 points (95% CI, –9.32 to –1.94) in the SOC arm. This difference (8.96; 95% CI, 4.24 to 13.69) exceeds the minimal important difference (MID) of 5 for colorectal cancer patients. The final exploratory analysis of quality of life was also measured by the EuroQol Visual Analogue Scale (EQ VAS) and EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) utility score at baseline and 18 weeks. Visual analogue scale scores in the pembrolizumab arm increased from baseline by 4.50 points (95% CI, 1.16 to 7.83) and decreased by 2.88 points (95% CI, –6.46 to 0.69) in the SOC arm for a difference of 7.38 (95% CI, 2.82 to 11.93) in favour of pembrolizumab, exceeding the MID of 6 for cancer patients. Finally, EQ-5D-3L utility scores in the pembrolizumab arm increased from baseline by 0.04 points (95% CI, 0.00 to 0.08) and decreased by 0.01 points (95% CI, –0.05 to 0.02) in the SOC arm for a difference of 0.05 (95% CI, 0.00 to 0.10) in favour of pembrolizumab, meeting the MID of 0.05 for cancer patients.
Harms Results
The proportion of individuals experiencing an AE was slightly lower in the pembrolizumab arm (97.4%) than in the SOC arm (99.3%). The most common AEs in both groups were gastrointestinal events and fatigue. The percentage of patients who reported serious AEs (SAEs) was lower in the pembrolizumab arm (40.5%) than in the SOC arm (52.4%). The frequency of AEs resulting in treatment discontinuation, death, or death due to an AE were similar between both groups. The frequency of immune-mediated AEs (which were identified as harms of interest for the review) were higher in the pembrolizumab arm (30.7%) than in the SOC arm (12.6%). The most common immune-mediated AEs were hypothyroidism, colitis, hyperthyroidism, pneumonitis, adrenal insufficiency, hepatitis, and infusion reactions. However, the frequency of infusion-related reactions was higher in the SOC arm.
Table 2: Summary of Key Results From KEYNOTE-177
Outcome | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Progression-free survival | ||
Number of events, n (%) Progression, n (%) Death, n (%) Censored, n (%) | 82 (53.6) 65 (42.5) 17 (11.1) 71 (46.4) | 113 (73.4) 86 (55.8) 27 (17.5) 41 (26.6) |
Median PFS, months (95% CI) | 16.5 (5.4 to 32.4) | 8.2 (6.1 to 10.2) |
Hazard ratio (95% CI; P value) | 0.60 (0.45 to 0.80; 0.0002)a | |
Restricted mean survival time, months (95% CI) | 13.7 (12.0 to 15.4) | 10.8 (9.4 to 12.2) |
Difference in restricted mean survival time, months (95% CI) | 2.9 (0.7 to 5.1) | |
Overall survival | ||
Number of events, n (%) | 56 (36.6) | 69 (44.8) |
Hazard ratio (95% CI; P value) | 0.77 (0.54 to 1.09; 0.0694)b | |
Median survival, months (95% CI) | Not reached | 34.8 (26.3 to not reached) |
Overall response rate | ||
Number of responses, n (%) Complete response, n (%) Partial response, n (%) Stable disease, n (%) Progressive disease, n (%) Could not be evaluated or no assessment, n (%) | 67 (43.8) 17 (11.1) 50 (32.7) 32 (20.9) 45 (29.4) 9 (5.9) | 51 (33.1) 6 (3.9) 45 (29.2) 65 (42.2) 19 (12.3) 19 (12.3) |
Overall response rate, % (95% CI) | 43.8 (35.8 to 52.0) | 33.1 (25.8 to 41.1) |
Difference in overall response rate between pembrolizumab and SOC (95% CI; P value) | 10.7% (–0.2 to 21.3; 0.0275)b | |
Duration of response | ||
Median, months (range) | NR (2.3 to 41.4) | 10.6 (2.8 to 37.5) |
Patients with extended response duration, n (%) | ||
≥ 6 months | 61 (96.9) | 43 (87.9) |
≥ 9 months | 55 (91.9) | 27 (59.9) |
≥ 12 months | 50 (85.1) | 19 (43.8) |
≥ 18 months | 45 (85.1) | 11 (35.3) |
≥ 24 months | 29 (82.6) | 9 (35.5) |
Health-related quality of lifec | ||
Global health/quality of life score, change from baseline to 18 weeks, mean (95% CI) | 3.33 (–0.05 to 6.72) | –5.63 (–9.32 to –1.94) |
Least squares mean difference in global health/quality of life score, mean (95% CI) | 8.96 (4.24 to 13.69) | |
EQ VAS, change from baseline to 18 weeks, mean (95% CI) | 4.50 (1.16 to 7.83) | –2.88 (–6.46 to 0.69) |
Least squares mean difference in EQ VAS score (95% CI) | 7.38 (2.82 to 11.93) | |
EQ-5D-3L utility score, change from baseline to 18 weeks, least squares mean (95% CI) | 0.04 (0.00 to 0.08) | –0.01 (–0.05 to 0.02) |
Least squares mean difference in EQ-5D-3L utility score (95% CI) | 0.05 (0.00 to 0.10) | |
Harms | ||
Patients with > 1 AE, n (%) | 149 (97.4) | 142 (99.3) |
Patients with > 1 SAE, n (%) | 62 (40.5) | 75 (52.4) |
Patients with AE resulting in treatment discontinuation, n (%) | 21 (13.7) | 17 (11.9) |
Patients with AE resulting in death, n (%) | 6 (3.9) | 7 (4.9) |
Death due to AE, n (%) | 0 (0) | 1 (0.7) |
AE = adverse event; CI = confidence interval; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; PFS = progression-free survival; SAE = serious adverse event; SOC = standard of care.
aStatistically significant after adjusting for multiple testing.
bStatistically insignificant after adjusting for multiple testing.
cIn the EORTC HRQoL analysis there were 141 and 131 patients in the pembrolizumab and SOC arms, respectively. In the EQ-5D-3L analysis, there were 142 and 133 patients in the pembrolizumab and SOC arms, respectively.
Source: Clinical Study Report P177V01MK3475.13
Critical Appraisal
The major limitations on the internal and external validity of KEYNOTE-177 stem from the open-label nature of the study and the ability for patients in the SOC arm to cross over to the pembrolizumab arm and patients in either arm to receive subsequent anticancer medications, including other anti-PD1/PDL1 medications. While no patients crossed over from the pembrolizumab arm to the SOC arm, 56 patients (36.4%) in the SOC arm crossed over to the pembrolizumab arm. Further, 44 patients (28.6%) and 44 patients (28.8%) in the SOC and pembrolizumab arms, respectively, received subsequent anticancer therapy. The differential crossover and subsequent use of anticancer medications could have introduced bias. Consequently, 2 sensitivity analyses were conducted to assess the impact of crossovers and the use of subsequent anticancer medications on PFS. These sensitivity analyses did not alter the HR from the primary analysis substantially and indicated that the primary analysis is robust. Notably, 1 analysis suggested there may be similar median PFS in the pembrolizumab arm (7.0 months; 95% CI, 4.2 to 12.4) and SOC arm (6.3 months; 95% CI, 4.6 to 8.2); however, this is likely an overly conservative estimate of the treatment effect. Three sensitivity analyses were conducted to adjust for the impact of crossovers but not the subsequent use of other anticancer medications. Each analysis differed from the primary analysis, which suggested some bias in the primary analysis. However, despite this bias, all estimates also suggest some benefit from pembrolizumab. Unfortunately, due to variations in the point estimates, lack of significance testing, and wide CIs, the exact magnitude of any benefit is uncertain. While crossovers and use of subsequent anticancer therapies in such a trial is clinically and morally reasonable, real-world application of these data should acknowledge their contributing role in the results achieved in the study. Moreover, the trial did not enrol patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score greater or equal to 2. Finally, the PHA was violated in the PFS analysis; thus, the RMST is likely a more accurate estimate of any PFS benefit from pembrolizumab.
Indirect Comparisons
Description of Studies
The sponsor-submitted indirect treatment comparison (ITC) evaluated the comparative efficacy and safety of pembrolizumab versus competing interventions for the treatment of patients with MSI-H/dMMR mCRC. Pembrolizumab was compared with CAPOX, panitumumab plus FOLFOX, and SOC (which consisted of FOLFOX or FOLFIRI with or without cetuximab, as administered in KEYNOTE-177) for OS, PFS, ORR, and safety outcomes. Bayesian network meta-analysis (NMA) methods were used for the comparisons. The base-case NMA for OS and PFS consisted of all included studies and used a subgroup of patients from the KEYNOTE-177 trial who did not receive treatment with bevacizumab (termed “ITT-Bev”).14
Efficacy Results
Five studies (mostly phase II or III, open-label RCTs) were included in the NMA, including the pembrolizumab pivotal study, KEYNOTE-177. The base-case analysis of OS showed no difference between pembrolizumab and SOC or other interventions. Results from other analyses (e.g., time-varying analysis, adjustment for different crossover methods) generally showed similar results.
The base-case analysis for PFS indicated that pembrolizumab was favoured over all other treatments. Pembrolizumab was favoured for ORR compared to CAPOX for ORR.
Harms Results
Pembrolizumab was favoured over comparator treatments with lower odds of AEs of grade 3 or higher, treatment-related AEs of grade3 or higher, and treatment-related SAEs. No treatments were favoured over the others for discontinuations due to AEs (DAEs).
Critical Appraisal
Few inferences can be made from the results of the NMA because of important limitations with the included studies and the methods and assumptions made in the NMA.
There were several clinical assumptions made in the NMA and several notable differences in the characteristics of patients across studies, which impact the interpretation of the NMA results. In addition, the small size (5 studies) and structure of the network prevented the use of random-effects models in most outcomes of interest and the ability to model between-study heterogeneity and to assess consistency between direct and indirect comparisons as there were no closed loops.
The systematic review did not sufficiently follow accepted guidelines for reporting and conduct: Information was not provided on the search criteria or the search methodology, the methods used for study selection and data extraction were omitted, and no critical appraisal assessment of the included studies was reported.
Bevacizumab was excluded from the list of comparators, and so studies that included it as a treatment were excluded, including a subset of patients who received bevacizumab in the SOC group of KEYNOTE-177. Bevacizumab was identified as a relevant comparator for this review, and its exclusion limits the generalizability of the results. Furthermore, base-case networks were constructed using subgroups of patients from KEYNOTE-177, which would potentially bias the results in favour of pembrolizumab because this would break randomization of the trial(s) and because a comprehensive set of relevant comparators that were evaluated as part of the SOC group in the trial would not be included. As well, this approach led to imprecision in the results of these comparisons due to the smaller sample size for the subgroup of patients who did not receive bevacizumab, as evidenced by the wider credible intervals (CrIs).
The clinical characteristics of the populations of patients were heterogeneous. For example, 1 study enrolled patients with MSI-H/dMMR mCRC, 1 looked at patients with KRAS mutations, and 3 evaluated the general mCRC population. It was assumed that there would be no difference in treatment effect estimates between patients with MSI-H/dMMR, KRAS wild type (other than panitumumab), or general mCRC. However, these variations in population are expected to impact the relative treatment effects, as these are potentially important treatment effect modifiers, as evidenced by accumulated literature, like many other genetic biomarkers in oncology therapies. In addition, baseline ECOG PS and durations on treatment or on trial also varied considerably across trials.
Study design was another key source of heterogeneity. KEYNOTE-177 allowed patients to cross over from SOC to pembrolizumab following progression during the study. Statistical methods were used to account for crossover from SOC to pembrolizumab. Given the immature results on OS in the KEYNOTE-177 trial, the sponsor-submitted NMA was compromised on this outcome.
The authors noted that the networks were constructed based on availability of outcome data. Besides the comparison between SOC and CAPOX for OS, comparisons for almost all competing interventions were based on single trials. The available trials formed networks with no closed loops; therefore, it was not possible to validate the transitivity assumption of the NMA and check for consistency of results between direct and indirect comparisons. Random-effects models were attempted and determined not to be feasible due to the small number of studies for all outcomes except for OS. Consequently, as connections were only described by a single trial for PFS, ORR, and safety, results for these outcomes are based on fixed-effects model, as random-effects analyses were not meaningful.
The variable length in follow-up across trials means there is potential for bias related to underestimating the frequency of AEs, as some may occur rarely or may only become apparent long after the beginning of treatment.
Conclusions
Pembrolizumab improved PFS versus SOC in a single RCT of patients with MSI-H/dMMR mCRC. The difference between treatment groups was considered clinically meaningful based on input from the clinical experts consulted by CADTH. Although fewer patients died in the pembrolizumab group than in the SOC group, no statistically significant benefit in OS was found. The study was not adequately designed to evaluate treatment effects on OS, and estimates are uncertain due to crossovers and use of subsequent anticancer medications. Overall response rate, duration of response, and health-related quality of life (HRQoL) were also numerically improved relative to SOC. Although benefits aside from PFS could not be supported by statistical significance in all outcomes, the efficacy results in totality suggest pembrolizumab improves outcomes over SOC in a difficult-to-treat patient population whose cancer is often unresponsive to SOC. Pembrolizumab does not appear to be associated with more AEs than the SOC regimens evaluated. Known AEs of interest, such as immune-mediated AEs, occurred more frequently in the pembrolizumab group and remain a concern.
Introduction
Disease Background
Colorectal cancer is a potentially fatal disease that begins in the colon or rectum and is characterized by a group of cancerous cells (a tumour) that grow into and destroy nearby tissue. In metastatic disease, the tumour spreads to and damages other parts of the body.1 About 70% to 90% of colorectal cancers are diagnosed after symptom onset, although population-based screening is increasing the number of asymptomatic cases identified.2 Common early symptoms include a change in bowel habits, rectal bleeding, a rectal or abdominal mass, iron deficiency anemia, and abdominal pain. In metastatic disease, right upper-quadrant pain, abdominal distention, early satiety, supraclavicular adenopathy, and periumbilical nodules can be observed. Colorectal cancers are often diagnosed by histologic examination of a biopsy. Colonoscopies are accurate and versatile diagnostic tests, while flexible sigmoidoscopy and CT colonography are appropriate diagnostic techniques in specific circumstances. The Canadian Cancer Society expects colorectal cancer to be the third most commonly diagnosed cancer in Canada in 2020 and the second and third leading cause of death from cancer in men and women, respectively.3 Colorectal cancer is also expected to account for 12% of new cancer cases and 12% of new cancer deaths, leading to an additional 26,900 Canadians being diagnosed with colorectal cancer and 9,700 additional deaths due to the disease.3
Approximately 20% to 25% of newly diagnosed colorectal cancers are metastatic at time of diagnosis, and untreated patients with metastatic disease survive only 6 to 10 months.4-6 With the development of 5-fluorouracil therapy, survival is extended to 11 to 12 months and up to 3 years with additional therapeutic innovations.15 Yet despite these innovations, less than 20% of patients are alive at 5 years, and unfavourable prognostic factors (e.g., mutations in BRAF genes, proximal primary tumour location) are associated with survival under 18 months.7
Standards of Therapy in mCRC
For most patients with metastatic disease, therapy is palliative and focuses on systemic chemotherapy. Several therapeutic options are available, with the backbone of therapy consisting of a combination of 5-fluorouracil and leucovorin (or capecitabine) plus either irinotecan or oxaliplatin. The most recommended combinations are FOLFOX (fluorouracil-leucovorin-oxaliplatin), FOLFIRI (fluorouracil-leucovorin-irinotecan), FOLFOXIRI (fluorouracil-leucovorin-irinotecan-oxaliplatin) or CAPOX (capecitabine-oxaliplatin). The recommended combination of therapy varies by jurisdiction and is individualized based on the patient's health, the patient’s ability to tolerate chemotherapy, the goals of therapy, plus the tumour’s molecular profile (e.g., mutation status in RAS and BRAF genes, presence of dMMR or MSI-H) and the location of the primary tumour. Monoclonal antibodies such as bevacizumab, cetuximab, and panitumumab are often used in addition to combination chemotherapy. Cetuximab and panitumumab target the epidermal growth factor receptor and are used in patients with tumours with wild-type RAS and BRAF genes. Bevacizumab, which targets vascular endothelial growth factor, is also often considered for use in the first-line setting. Although the treatment of patients with mCRC continues to evolve, it is now best thought of as a continuum of care, where the evidence-based treatment options are administered with consideration of biomarkers and primary tumour location, in combination and in sequence with the intent to carefully balance a patient’s quality of life with the treatment’s life-prolonging effects. In patients with incurable distribution of metastatic disease, the primary goals of therapy may be to delay tumour progression to ensure quality of life and prolong survival.16
Ultimately, the diversity of therapeutic approaches is a function of the heterogenous pathophysiology of mCRC. The MSI-H/dMMR subtype may be present in 15%8 of colorectal cancer patients and in about 3.5% to 6.5% of stage IV patients.15 There is some evidence of favourable prognosis in early disease and a hypothesis that such tumours may have lower metastatic potential.9 However, these patients may benefit less from adjuvant therapy with 5-fluorouracil or capecitabine.9-12 In brief, dMMR patients accumulate errors throughout their genome, specifically the accumulation of repeating sequences of nucleotide bases called microsatellites. Accumulation of microsatellites in critical growth regulatory genes may lead to abnormalities in cell growth control.
Drug
Pembrolizumab falls under the class of checkpoint inhibitors or anti-PD1 medications. It is a monoclonal antibody that binds PD1 receptors on T cells, reversing T-cell suppression and inducing antitumour responses. It is administered intravenously and is indicated in Canada for classical Hodgkin lymphoma, mediastinal B-cell lymphoma, adult urothelial carcinoma, endometrial cancer, melanoma, non–small cell lung carcinoma, renal cell carcinoma, and head-neck squamous cell carcinoma. Pembrolizumab is also indicated for but not universally funded for dMMR/MSI-H colorectal cancer whose tumours have progressed following treatment with fluoropyrimidine, oxaliplatin, and irinotecan.17
Pembrolizumab received a Health Canada Notice of Compliance in March 2021 as first-line therapy in adult patients with unresectable or metastatic dMMR/MSI-H colorectal cancer. The sponsor has requested CADTH to review pembrolizumab in line with the indication. Pembrolizumab has been approved for this indication by the FDA18 and the European Medicines Agency.19
Table 3: Key Characteristics of Pembrolizumab and Other Comparators
Drug or drug regimen | Mechanism of action | Route of administration | Recommended dose | Serious adverse events |
|---|---|---|---|---|
Pembrolizumab | Activates antitumour immune response | IV | 200 mg every 3 weeks | Hepatic impairment, immune-mediated pneumonitis, colitis, hepatitis, nephritis or endocrinopathy, adrenal insufficiency, hypophysitis, type 1 diabetes, and thyroid disorders |
mFOLFOX Oxaliplatin 85 mg/m2 + leucovorin 400 mg/m2 + fluorouracil 400 mg/m2 on day 1 then 2,400 mg/m2 over 46 hours | Interferes with DNA synthesis and cellular replication | IV | Regimen repeated every 2 weeks | Neuropathy, myelosuppression, nausea, vomiting, diarrhea, fatigue, mucositis, pharyngolaryngeal dysesthesia, increased liver function tests |
FOLFIRI Irinotecan 180 mg/m2 + leucovorin 400 mg/m2 + fluorouracil 400 mg/m2 on day 1 then 2,400 mg/m2 over 46 hours | Interferes with DNA synthesis and cellular replication | IV | Regimen repeated every 2 weeks | Diarrhea, myelosuppression, nausea, vomiting, fatigue, alopecia, abdominal pain, anorexia, weight loss, increased liver function tests, mucositis, cholinergic symptoms |
FOLFOXIRI Irinotecan 165 mg/m2 + oxaliplatin 85 mg/m2 + leucovorin 400 mg/m2 + fluorouracil 3,200 mg/m2 over 46 hours | Interferes with DNA synthesis and cellular replication | IV | Regimen repeated every 2 weeks | Diarrhea, myelosuppression, nausea, vomiting, fatigue, increased liver function tests, mucositis, cholinergic symptoms, neuropathy, pharyngolaryngeal dysesthesia |
Bevacizumab | Inhibits microvascular growth and retards tissue growth | IV | If used with FOLFOX, FOLFIRI, or FOLFOXIRI: 5 mg/kg every 2 weeks If used with CAPOX: 7.5 mg/kg every 3 weeks | Hypertension, thromboembolism, gastrointestinal perforations and fistulas, tracheoesophageal fistula, proteinuria, central nervous system or pulmonary hemorrhage |
Panitumumab | Inhibits cell growth, survival, and proliferation | IV | 6 mg/kg every 2 weeks | Dermatologic toxicity, hypomagnesemia, infusion reactions, interstitial lung disease, ocular toxicity |
CAPOX oxaliplatin 130 mg/m2 + capecitabine 1,000 mg/m2 twice daily for 14 days | Interferes with DNA synthesis and replication | Oral/IV | Regimen repeated every 3 weeks | Neuropathy, myelosuppression, nausea, vomiting, hand-foot syndrome, increased liver function tests, diarrhea, fatigue, mucositis, pharyngolaryngeal dysesthesia, palmar-plantar erythrodysesthesia |
Capecitabine | Interferes with DNA synthesis and replication | Oral | 1,250 mg/m2 twice daily for 14 days, repeat every 3 weeks | Cardiotoxicity, alopecia, rash, palmar-plantar erythrodysesthesia, anorexia, diarrhea, dehydration, dyspepsia, mucositis, fatigue, nausea, vomiting, dizziness, dysgeusia, conjunctivitis |
Leucovorin + fluorouracil leucovorin 400 mg/m2 + fluorouracil 400 mg/m2 on day 1 then 2,400 mg/m2 over 46 hours | Interferes with DNA synthesis and cellular replication | IV | Regimen repeated every 2 weeks | Leucovorin: seizures, syncope Fluorouracil: arrythmia, cardiotoxicity, electrocardiogram changes, anorexia, diarrhea, mucositis, nausea, vomiting, myelosuppression, infection, increased bilirubin, conjunctivitis |
Irinotecan | Interferes with DNA synthesis and cellular replication | IV | 350 mg/m2 every 3 weeks | Diarrhea, flushing, alopecia, anorexia, dyspepsia, mucositis, nausea, vomiting, fatigue, myelosuppression, infection, rhinitis, increased liver function tests |
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
CADTH received 2 patient input submissions from CCC and CCRAN for this review. Both groups are national, not-for-profit patient advocacy groups. CCC posted a survey on its social media platforms as well as on those of international colorectal cancer organizations between October 30, 2020, and January 1, 2021. Information from 8 patients and 2 caregivers from Canada (n = 6), the US (n = 3), and Malaysia (n = 1) made up the responses. All responses were from or on behalf of patients receiving pembrolizumab, 50% of whom were females and 70% of whom had stage IV cancer at the time of survey. At the time of diagnosis, 2 patients were younger than 40 years old, 3 were between 40 and 49, 2 were between 50 and 59, and 3 were between 60 and 69. CCRAN collected information through 3 separate processes for its submission and advertised with the help of its support group members and members of its Medical Advisory Board. The first was a national online survey run from December 6 to 30, 2020, during which time the organization received input from 63 colorectal cancer patients, 17 caregivers, and 5 patients who were also caregivers, all of whom were living in Canada. Almost 59% of respondents were female, and patient age varied from 31 to 90 years old, although most were between 41 and 70 years old. Later stages of cancer were more heavily represented, with most respondents in either stage III or IV. The second process was a focus group discussion conducted over Zoom (teleconference platform) on November 15, 2020, to gain insight into the experiences and symptoms of 7 patients who had mCRC. The third process was phone interviews made between December 8 and 21, 2020, with 3 patients who had specifically received pembrolizumab treatment.
Disease Experience
Patients from both CCC and CCRAN surveys noted that some of their common cancer symptoms included bloody stools, diarrhea, fatigue, and pain. Most felt that their symptoms affected their daily lives, work, and ability to exercise; interfered with their quality of life; and had a psychological impact leading to various mental health issues. Respondents from the CCRAN survey reported that they were unable to work (51%) and unable to fulfill family obligations (42%). Patients also felt that their treatments made them forgetful and fatigued and made it difficult to plan for the future. One respondent stated, “Currently afraid to make future plans as historically, I have done so many times and had to stop and restart my life over and over again. Anxiety is high and not inappropriate for someone in my position. The less I talk or have to think about cancer and the more I engage with people and life pursuits outside of a cancer focus, the healthier I get, so it is a self-care balance.” The CCRAN focus group identified pain in various locations, breathing issues, debilitating fatigue, and diminished appetite as key burdens resulting from the spread of the disease to other organs. Moreover, respondents noted that, from their experience, there were often no warning signs before the cancer had advanced and was more difficult to treat. “I felt fine. You would never know that I have stage four disease. I guess that’s why they call it the silent killer.”
Caregivers also shared feelings of helplessness, challenges with frequent travel over long distances for treatments, difficulties of managing side effects, loss of lifestyle, and loss of work and income. From the CCRAN survey, caregivers expressed feeling the psychological impacts that come with supporting someone with cancer, and some had sought out help from support groups (n = 20), from psychologists (n = 16), and through online resources (n = 9).
Experiences With Currently Available Treatments
Most patients from the CCC survey had accessed previous therapies, such as chemotherapy (7), radiation therapy (3), and surgery (4), to treat their cancer. Two respondents had not received pembrolizumab but were on other immunotherapies (nivolumab and ipilimumab) at the time of the survey. Six patients who had previous treatments felt that symptoms were either not controlled or only partially controlled. Respondents identified diarrhea, nausea, hair loss, vomiting, fatigue, and pain as the most difficult symptoms to tolerate. On a scale from 1 to 10, all respondents ranked at least an 8 the importance of having a choice in treatment based on known side effects.
When asked about accessing cancer treatments, 4 out of 10 patients expressed difficulties, while 4 individuals reported that the therapies they had been recommended were based on what was funded in their region of residence. For the 2 who were receiving immunotherapies, 1 had to pay out of pocket for the drug and 1 had to go to the US to gain access. Three patients had received financial assistance that covered from 20% to 100% of their treatment cost. In addition to treatment costs, patients and caregivers reported financial stress related to travel expenses, medical visits and tests, and lost time from work. Most patients (70%) felt that paying out of pocket for access to new therapeutics would depend on the cost.
Six patients from the CCC survey who received treatment in Canada felt that access to treatment was appropriate or fair in their region. One patient shared their concerns with accessing drugs in Canada:
I don’t think colorectal patients should have to pay for treatments with proven efficacy. There are studies that now recommend immunotherapy treatment for MSI- High/mismatch repair deficient colorectal cancers. In other countries these treatments are now first-line treatments. Canadians should have access to these treatments and they should be covered. If new treatments arise that haven’t had proven efficacy through peer reviewed studies, but look promising, I would consider paying out of pocket if the cost wasn’t exorbitant and some financial help was available on a compassionate basis.
Patients from the CCRAN survey listed a variety of therapies they had received, including FOLFOX (72%), FOLFIRI (34%), capecitabine (40%), bevacizumab/MVASI (21%), panitumumab (15%), cetuximab (6%), pembrolizumab (6%), trifluridine-tipiracil (4%), regorafenib (2%), and encorafenib (2%). Most respondents noted that diarrhea, hand and foot syndrome, and neuropathy were common with their current medication, but that fatigue and nausea were the 2 side effects most difficult to tolerate. Aside from the previous list of drugs, respondents had also had surgery, radiation therapy, and other forms of chemotherapy.
When asked about access to treatments, CCRAN responses (all respondents were from Canada) were variable from very limited or restrictive (4% of responses) to very appropriate and/or fair (24%). When asked if the treatments they were offered were based solely on what was publicly funded in their province, 14 patients responded yes, 12 responded no, and many were unsure (26). Twelve individuals reported receiving financial assistance for their treatments, while another 41 had not received any. For those who had assistance, the amounts received ranged from 10% to 100% of their treatment costs. Furthermore, 19 patients noted that in addition to the cost of the drugs, they had expenses for travel, accommodations, medical tests, supplies, and procedures. Forty respondents stated that they would be willing to pay out of pocket to access new therapies through a private clinic, while another 10 responded they would not. Reasons for the latter were often due to high costs or to avoid creating a financial burden on their family.
Improved Outcomes
Respondents from both CCC and CCRAN surveys felt it was very important that new therapies would improve both physical condition and quality of life. Furthermore, nearly all patients and caregivers expressed interest in a treatment that was proven to provide a better quality of life even if it did not extend OS, since this would allow them to engage in social activities and return to daily life without worrying about side effects. When asked about the severity of side effects patients would be willing to tolerate for extended survival, both survey results were variable from no side effects to significant ones, though the general trend was a tolerance toward more significant side effects in exchange for improved survival. Patients from the CCRAN survey chose the top 3 outcomes they would like to see with cancer treatments: provides a cure, if possible (94%); prolongs life by a substantial amount of time (86%); and promotes good quality of life (82%). Other key outcomes included limited side effects, treatment funding, improvement in symptoms, and simple administration.
Experience With Drug Under Review
Five patients from the CCC survey confirmed receiving pembrolizumab, 2 as first-line treatment and 1 each as second, third, and fourth line. Patients were able to access pembrolizumab via clinical trials, special access programs, and private insurance. At the time of the survey, most patients had been treated for 18 months to 24 months.
With regard to trialling different treatments before finding 1 that worked, 1 individual stated the following, “a lot of time was wasted on other treatments,” and she felt she “could have avoided brutal, ineffective chemo [had she] started with Keytruda instead of other treatments.” While receiving pembrolizumab, patients experienced hair loss, fatigue, constipation, fever, and muscle, bone, and joint pain but felt these side effects were somewhat tolerable and relatively minor. However, 2 respondents stated that diarrhea, bloody stools, and constipation were managed less effectively compared to other therapies they had received. In general, on a scale from 1 to 10, the side effects had a low (1 to 3) impact on their lives and their overall experience was much better (10) than with other treatments. When asked specifically about immunotherapies, patients felt that the psychological impacts like feelings of isolation, emotional drain, anxiety, and fatigue from long medical appointments were the most difficult to deal with. When asked about treatment response, most patients stated that their cancer was completely gone, shrunken, or controlled.
Patients and caregivers hope pembrolizumab will increase OS, maintain or improve quality of life, delay onset of symptoms, delay need for chemotherapy, be easy to use, and reduce the side effects from other medications. Importantly, nearly all patients felt that their quality of life was high or normal and that they had been able to return to all their daily activities. One patient emphasized, “Without Keytruda, I probably wouldn’t be here. I’ve endured this battle for four years now. I’ve been able to switch to the 6-week treatment making it even easier to enjoy a ‘normal’ life.” Another recalled her experience, “Tumour Board deemed me ‘inoperable.’ I underwent 25 radiation, 25 oral chemo. Nothing. I was told to get my affairs in order. Two months later Keytruda became an option. Here I am 45 treatments later and still kicking...working full-time, working part-time, two teenage sons, a single mom taking care of the household. Without Keytruda, I would be dead.”
CCC respondents noted additional travel costs related to accessing treatment, with 1 respondent citing the lack of provincial coverage as a barrier; all agreed that pembrolizumab should be funded in their regions. CCRAN interviewed patients who had experience with pembrolizumab, 1 of whom had received the immunotherapy as a first-line treatment during a clinical trial (in combination with cyclophosphamide and Survivac vaccine). The other 2 patients used pembrolizumab as second-line therapy, 1 through a clinical trial (in combination with cyclophosphamide and Survivac vaccine) and 1 as monotherapy through private insurance at a private infusion clinic. None travelled or paid out of pocket for testing. They also did not wait long for their test results, though 1 patient experienced some anxiety while waiting, knowing it would determine if they could receive pembrolizumab.
When asked about their lives since beginning treatment with pembrolizumab, 1 reported no side effects, a second stated they only had elevated lipase enzyme levels, and a third was uncertain since their experience was a combination therapy. All 3 were enthusiastic about the improvements in quality of life compared to side effects related to either chemotherapy or cancer symptoms. One patient stated, “My life did a total turn around. I have more energy and feeling more like myself today than ever, cancer notwithstanding.” The patients all reported their tumours had shrunken, some to the point that they were unidentifiable. The individual who reported having elevated lipase levels had to stop pembrolizumab treatment in May 2020 after 9 cycles and had not resumed treatment at the time of the interview, though they noted that their cancer was still controlled despite stopping immunotherapy. A second patient reported having 42 cycles and only had to stop for a month while receiving radiation treatment in March 2018, while the last individual had received 9 cycles and did not have to stop at any time. Patients indicated that not only were infusion times shorter than for traditional chemotherapy, but they were also able to receive pembrolizumab every 3 weeks — rather than every 2 weeks — with minimal side effects. When asked if accessing pembrolizumab was worth it, 1 patient responded, “Oh, yes, yes, yes, it was very worth it. It saved my life! It brought me back to the woman I used to be who used to play and love life. I felt like nothing was going to happen for me and my cancer and then, bang, Keytruda came along and pulled off a miracle for me. It gave me a second chance at life. So, it was very worth it for me to have accessed it.” Furthermore, patients have been able to return to their normal lives, work again, and spend time with family.
Companion Diagnostic Test
Patients listed the various methods that were used to diagnose their colorectal cancer, such as reporting symptoms, colonoscopy, CT scan, incidental finding or physical examination, biopsy, and blood work. Most patients from the CCC survey received positive biomarker testing after diagnosis, and all were tested before being prescribed pembrolizumab. For individuals who received biomarker testing, 2 received chemotherapy as their first treatments, another received immunotherapy right away, and a fourth could choose between the 2 options but had to pay out of pocket for immunotherapy. CCRAN asked patients if there were additional costs for testing such as tumour genomic profiling and, if so, what the costs were. Nine responses confirmed the supplementary costs, and while not all patients followed through with the tests, for those who did, expenses were more than $2,500.
Additional Information
Both patient groups emphasized the need for new and effective treatments for patients with MSI-H/dMMR cancer. They highlighted that patients should have equitable access without financial restrictions to a medication like pembrolizumab that has led to improvements in quality of life and survival outcomes, has few side effects, and can be easily administered.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 3 clinical specialists with expertise in the diagnosis and management of colorectal cancer.
Unmet Needs
The clinical experts highlighted the lack of a current therapy that exploits the distinct profile observed in MSI-H/dMMR patients. This mutational profile can be unresponsive to the largely chemotherapy-based conventional treatments — treatments that are associated with important adverse effects. Thus, a treatment that better targets these tumours with improved outcomes and fewer adverse effects is needed.
Place in Therapy
The clinical experts stated that pembrolizumab would be used alone for any line of therapy, including first line, in patients with MSI-H/dMMR colorectal cancer.
Patient Population
The clinical experts suggest that only patients with MSI-H/dMMR confirmed mCRC would benefit from pembrolizumab. Any eligibility criteria for first-line use should adhere to the enrolment criteria of the KEYNOTE-177 study. In short, this would include patients with an incurable distribution of mCRC, an MSI-H/dMMR profile, an ECOG PS of 0 or 1, willingness to adopt an adequate method of contraception, and adequate organ function. Patients should be free of active autoimmune disease (requiring disease-modifying agents, corticosteroids, or immunosuppressive therapies); uncontrolled metastases to the central nervous system; prior therapy with an immune checkpoint inhibitor (i.e., another anti-PD1/PDL1 or anti-CTLA-4 agent); unsuppressed HIV, hepatitis B, or hepatitis C; interstitial lung disease or active non-infectious pneumonitis; active infection requiring systemic therapy; pregnancy; or breastfeeding. It is considered SOC to assess tumours for MSI-H/dMMR status through immunohistochemistry and polymerase chain reaction–based analysis; thus, potentially eligible patients would be identified by the patient’s oncologist through standard care.
Assessing Response to Treatment
The experts suggested that assessing treatment response carefully balances survival, HRQoL, and AEs. Benefits related to survival and HRQoL (including a delay in deterioration in quality of life), while minimizing SAEs, would be considered a response to treatment. In some circumstances, disease stability or surrogate end points, such as PFS as determined by radiologic imaging, will be assessed. Typically, a 2- to 3-month trial of therapy is offered before reassessment of therapy.
Discontinuing Treatment
Disease progression (as determined by radiologic imaging or unequivocal clinical findings), intolerable or unmanageable toxicities, and a change in the patient status taking them outside of standard eligibility criteria would preclude ongoing treatment.
Prescribing Conditions
Treatment should be provided in a multidisciplinary centre with expertise in the use of such medications. This includes patient selection and management by an experienced medical oncologist, drug preparation in an accredited oncology-specific pharmacy, and administration by trained nurses in an environment where infusion-related and other emergencies can be promptly addressed. A gastroenterologist, surgeon, and/or interventional radiologist would need to obtain a biopsy or surgical specimen. A pathologist would be required to confirm the histologic diagnosis and to interpret the necessary molecular studies. Ultimately, a medical oncologist would ensure that the relevant criteria are met and that the patient is involved in the decision-making process.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Three registered clinician groups provided input for this review. One submission was by the Ontario Health (Cancer Care Ontario) (OH-CCO) Gastrointestinal Cancer Drug Advisory Committee (GI DAC), which included 4 physicians. OH-CCO GI DAC provides evidence-based clinical and health system guidance for the Provincial Drug Reimbursement Programs and Systemic Treatment Program. CGOEN, the Medical Advisory Board of the CCC, and other gastrointestinal cancer-treating clinicians provided a separate submission. The group consisted of 12 medical oncologists and gastroenterologists who practice in Alberta, British Columbia, Nova Scotia, Ontario, Quebec, and Saskatchewan. CGOEN consists of Canadian gastrointestinal oncology clinicians who work to advance the knowledge and treatments of gastrointestinal cancers, while the Medical Advisory Board of the CCC acts as a link between patient groups and the medical community, helping to ensure that activities and health information are relevant and communicated between the 2. More information about the latter group can be found at https://www.colorectalcancercanada.com/about/staff-board-medical-advisory.
Unmet Needs
Both GI DAC and CGOEN noted a lack of targeted treatment available for the MSI-H/dMMR colorectal cancer population, as well as for patients who have more aggressive disease, are unresponsive to standard chemotherapy, or have chemotherapy-related toxicities. Of these groups, patients diagnosed with MSI-H/dMMR colorectal cancer — who make up approximately 5% of the unresectable or mCRC population — were identified as having the greatest unmet needs.
Place in Therapy
GI DAC anticipated that if patients are treated with pembrolizumab as a single agent for first-line use, therapies that are current SOC will continue to be funded and shifted downstream. It was also suggested that patients who experience disease progression after being treated with chemotherapy could receive pembrolizumab next.
Patient Population
Patients with MSI-H/dMMR advanced or mCRC who also have good performance status and who align with the criteria outlined in the KEYNOTE-177 clinical trial would be most suitable and have the greatest need for treatment with pembrolizumab. The patients who are best suited for pembrolizumab would be identified through companion diagnostics, although GI DAC acknowledged that reflex testing is not universally available. The group also emphasized that testing should be available to all patients with colorectal cancer and performed in a timely manner to prevent treatment delays. Likewise, CGOEN highlighted that MSI-H/dMMR cancers are readily identifiable with locally available assays such as immunohistochemistry and/or polymerase chain reaction testing and suggested that next-generation sequencing could also be an option for detecting multiple genetic aberrations such as MSI. Conversely, patients who are not MSI-H/dMMR, patients who have contraindications to immunotherapy or poor performance status, or patients who meet the exclusion criteria used in KEYNOTE-177 would not be candidates to receive pembrolizumab.
Assessing Response to Treatment
To assess treatment response, GI DAC listed the following outcomes that would be used in clinical practice: carcinoembryonic antigen testing, biochemistry results, standard imaging, and clinical improvement. CGOEN stated that patients will normally have a CT scan performed every 2 to 3 months to assess response and that this will continue until disease progression or treatment-limiting toxicities occur or until the patient decides to stop. Furthermore, the group confirmed that the outcomes used in clinical trials are consistent with those used in clinical practice. Overall survival and quality of life outcomes were identified as the most important outcome measures when considering a clinically meaningful response. Both groups noted that other measures of meaningful response include improvement or stabilization of symptoms; reduction in the frequency or severity of symptoms such as abdominal pain, rectal bleeding, anemia, and constipation; and ability to perform daily activities. These outcomes would be assessed per current SOC or every 3 to 4 cycles.
Discontinuing Treatment
When deciding to discontinue treatment, both groups stated that evidence of disease progression, such as deterioration in clinical status or objective progression on imaging, would be important. GI DAC would also consider the occurrence of specific AEs and the need for additional treatment as major factors, while CGOEN identified immune-mediated adverse reactions and grade 3 or 4 toxicities as reasons for stopping treatment.
Prescribing Conditions
Pembrolizumab should be administered in an approved oncology infusion clinic in an outpatient hospital setting. GI DAC felt that it would be ideal if reflex testing were in place at the time of reimbursement and if all current downstream chemotherapy continued to be funded.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program question | Clinical expert response |
|---|---|
What is pembrolizumab’s place in therapy relative to comparators not studied in KEYNOTE-177? | Pembrolizumab’s place in therapy is likely ahead of all current standards of care, including those not studied in KEYNOTE-177. |
Is MSI-H/dMMR testing required for all metastatic colorectal cancer patients at time of diagnosis of metastatic or recurrent disease? (Regardless of any other related factors: patient age; hereditary risk factors; left-sided and right-sided primary tumour; de novo and recurrent cancer; BRAF mutant and BRAF wild type?) | Yes, testing is required. |
What is the status of access to and funding for MSI-H/dMMR testing across jurisdictions in Canada? | Testing is likely funded across Canada, but age restrictions in some jurisdictions may apply. |
What is the preferred methodology for determining MSI-H/dMMR status? | Immunohistochemistry and polymerase chain reaction tests are the preferred methods. |
How should MSI-H/dMMR status be determined for patients with relapsed or unresectable colorectal cancer who underwent prior surgery from earlier stage disease? (Is new tissue required at recurrence to establish MSI-H/dMMR status? Can MSI-H/dMMR status be established using frozen tissue from prior surgeries?) | Assuming that a diagnosis of adenocarcinoma has previously been confirmed, a biopsy of the recurrence or metastasis is not typically required, provided the imaging or other evidence is compelling. |
What is the turnaround time for testing? | Two days to 2 weeks, depending on the jurisdiction. |
Which test(s)/laboratories are validated or approved to evaluate MSI-H/dMMR testing? | The review team was unable to answer this question. |
What is the optimal approach for tissue sampling? (Is biopsy of accessible tissue sufficient?) | Any biopsy is appropriate. |
Can MSI-H/dMMR status change over the course of illness? | MSI-H/dMMR status is not known to change. |
Should the enrolment criteria regarding prior treatment used in KEYNOTE-177 be used in a reimbursement scenario? | Those who relapsed on a previous therapy or prior treatment with chemotherapy should also be eligible for pembrolizumab. |
Should patients with potentially resectable, confirmed MSI-H/dMMR metastatic colorectal cancer be eligible for pembrolizumab? | No, this population should not be treated with pembrolizumab. |
Should patients with confirmed MSI-H/dMMR colorectal cancer who experience disease relapse within 6 months of completion of adjuvant chemotherapy be eligible for pembrolizumab first line? | Yes, these patients should be eligible for pembrolizumab. |
Should re-initiation of treatment be permitted for patients who elected for a treatment break from pembrolizumab but did not experience disease progression or unacceptable toxicity while receiving pembrolizumab? What duration of treatment is recommended after a treatment break? | Re-initiation may be reasonable if the break in therapy is not due to progression or toxicity. While there is no evidence supporting this approach or specific duration, the experts felt that following a break, patients should complete the remaining doses in the 35-dose treatment regimen. |
Should patients who complete 2 years of pembrolizumab and experience disease progression or recurrence off treatment be eligible for re-treatment? What duration of time is appropriate to have elapsed between completion of pembrolizumab and recurrence or progression of disease? What duration of re-treatment is recommended? | There is no evidence to provide guidance on these issues, but eligibility likely depends on the break between treatments. The appropriate duration is also unknown but is likely guided by a discussion between the patient and the multidisciplinary cancer care team. |
Noting the proportion of patients with early progression in the pembrolizumab arm of KEYNOTE-177, how frequently should patients on pembrolizumab for MSI-H/dMMR colorectal cancer be monitored for disease progression, and with which tests? | Patients should be assessed clinically every 3 weeks and radiologically every 3 months. |
What is the most appropriate definition of progressive disease for patients receiving pembrolizumab? | KEYNOTE-177 followed the RECIST 1.1 guidelines to define disease progression. |
Is pseudoprogression possible during pembrolizumab treatment for metastatic colorectal cancer? If so, how should treatment response or disease progression be confirmed? | The RECIST 1.1 guidelines categorize lesions into those with a complete response, partial response, progressive disease, or stable disease. |
Is there evidence to inform if there are any patient groups that could discontinue pembrolizumab earlier than 2 years, such as any who experience a complete response? | Discontinuation may be possible in those with a complete response sustained for 6 months, but it is a patient-clinician decision. |
Should a weight-based pembrolizumab dose (i.e., 2 mg/kg up to a maximum of 200 mg every 3 weeks) be used for colorectal cancer? Should alternative dosing (i.e., 400 mg or 4 mg/kg up to a maximum of 400 mg every 6 weeks) of pembrolizumab be used as an option for MSI-H/dMMR colorectal cancer? | There is no evidence to support either dosing regimen. |
Should patients with an ECOG performance status of 2 or greater be eligible? | No, these patients would not be considered eligible. |
Do patients with known hereditary syndromes (e.g., Lynch syndrome) require confirmation of MSI-H/dMMR status to be eligible for pembrolizumab? | No, these patients would not require confirmation (as it would already be established). |
Are there any subgroups of patients with MSI-H/dMMR colorectal cancer for whom alternative systemic therapy may be preferred over pembrolizumab? | V600E patients, patients with contraindications to pembrolizumab, patients with prior organ transplant, patients with an immune illness, or patients who meet the KEYNOTE-177 exclusion criteria may benefit from current standard of care over pembrolizumab. |
Should patients with confirmed MSI-H/dMMR colorectal cancer currently receiving first-line therapy with alternative systemic therapy regimens, and with no evidence of disease progression, be eligible to change over to pembrolizumab? | The decision should be permitted, but it should only be implemented after a careful discussion between the patient and their multidisciplinary cancer care team. |
Should patients with confirmed MSI-H/dMMR colorectal cancer who received other systemic therapies for first-line colorectal cancer who experienced disease progression be eligible to receive pembrolizumab in later lines of therapy? | Yes, these patients should be eligible. |
Could increased testing lead to a different than anticipated number or proportion of patients identified to have MSI-H/dMMR status (who may not have otherwise been identified)? This would have direct impact on the estimated number of patients eligible to receive pembrolizumab. | Testing is becoming universal but likely has not been fully optimized across Canada; thus, fully optimized universal testing will likely improve the system’s ability to identify MSI-H/dMMR patients. |
dMMR = mismatch repair deficient; ECOG = Eastern Cooperative Oncology Group; MSI-H = microsatellite instability-high; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors version 1.1.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab 200 mg administered every 3 weeks intravenously for the treatment of unresectable or metastatic MSI-H/dMMR colorectal cancer in adults.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5.
Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | As first-line therapy in adults with unresectable or metastatic microsatellite instability-high/mismatch repair-deficient colorectal cancer |
Intervention | Pembrolizumab 200 mg intravenously every 3 weeks |
Comparators | FOLFIRI ± bevacizumab FOLFIRI ± cetuximab FOLFIRI ± panitumumab FOLFOX ± bevacizumab FOLFOX ± cetuximab FOLFOX ± panitumumab FOLFOXIRI ± bevacizumab CAPOX ± bevacizumab Capecitabine ± bevacizumab Fluorouracil + leucovorin ± bevacizumab Irinotecan |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
HRQoL = health-related quality of life; RCT = randomized controlled trial.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS (Peer Review of Electronic Search Strategies) checklist available on the CADTH website.20
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Keytruda/pembrolizumab and colorectal cancer. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform search portal, the Canadian Cancer Trials Database, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies. The initial search was completed on January 5, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on May 13, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist available on the CADTH website.21 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6. A list of excluded studies is presented in Appendix 2.
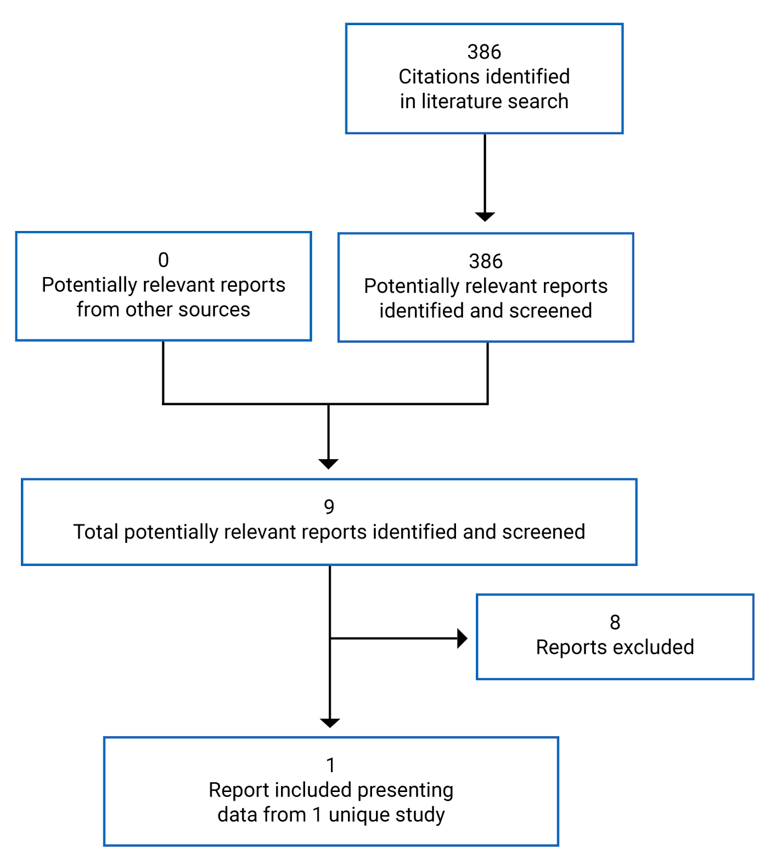
Table 6: Details of Included Study
Detail | KEYNOTE-177 |
|---|---|
Designs and populations | |
Study design | Multi-centre, open-label, active-controlled randomized controlled trial |
Locations | 120 centres in 23 countries (e.g., Australia, Brazil, Canada, Europe, Japan, South Korea, South Africa, Taiwan, and the US) |
Patient enrolment dates | November 30, 2015 (first patient, first visit) to February 19, 2020 (last patient, last visit) |
Randomized (N) | 307
|
Inclusion criteria | Male or female 18 years or older Locally confirmed MSI-H or dMMR stage IV colorectal carcinoma ECOG PS of 0 or 1, 10 days before treatment initiation Life expectancy of 3 months or greater Measurable disease at baseline based on RECIST 1.1 For women of childbearing potential, a negative serum pregnancy test within 72 hours of initiating first dose of medication For females and males of childbearing potential, agreement to use adequate method of contraception Adequate organ function Prior systemic therapy for stage IV colorectal cancer acceptable if completed at least 6 months before randomization |
Exclusion criteria | History or current evidence of any condition, therapy, or lab abnormality that might confound study results, interfere with full participation, or make it not in the patient’s best interest to participate, in the opinion of the investigator. Participation in another trial or use of an investigational medication within 4 weeks of randomization. Active autoimmune disease that required treatment in the past 2 years. However, replacement therapies (e.g., thyroxine, insulin) were not considered systemic treatments. Diagnosis of immunodeficiency or use of systemic steroids or any other immunosuppressive therapy within 7 days of randomization. Radiation therapy within 4 weeks of randomization without recovery from adverse effects to baseline from radiation. Active central nervous system metastases and/or carcinomatous meningitis. Those with stable brain metastases could participate if there was no steroid use for brain metastases within 28 days of study initiation. Major surgical procedure, open biopsy, or significant traumatic injury within 28 days of randomization. Prior therapy with immune checkpoint inhibitor. |
Progression of another malignancy or need for active treatment. Receipt of live vaccine within 30 days of medication initiation. Known history of or active interstitial lung disease or tuberculosis, HIV, active chronic or acute hepatitis B or C, tuberculosis, or psychiatric or substance abuse disorder that would interfere with trial participation. Active non-infectious pneumonitis or infection requiring systemic therapy. Pregnancy, breastfeeding, or expecting to conceive a child within projected duration of study. | |
Drugs | |
Intervention | Pembrolizumab 200 mg every 3 weeks administered intravenously |
Comparators | FOLFOX FOLFOX + bevacizumab FOLFOX + cetuximab FOLFIRI FOLFIRI + bevacizumab FOLFIRI + cetuximab |
Duration | |
Phase | |
Screening | 42 days |
Treatment | Treatment provided every 3 weeks until discontinuation |
Follow-up | Estimated total trial duration was 57 months from first patient signing informed consent form. Patients were followed up every 9 weeks following treatment discontinuation. |
Outcomes | |
Primary end points | Progression-free survival per RECIST 1.1 (assessed by an independent central imaging vendor) and overall survival |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Andre et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. New England Journal of Medicine. 2020:383 (23):2207-2218. |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors version 1.1.
Source: Clinical study protocol and Clinical Study Report P177V01MK3475.13
Description of Studies
KEYNOTE-177 is an ongoing, open-label randomized trial comparing pembrolizumab 200 mg every 3 weeks with SOC, as defined in Table 6, in adults with unresectable or metastatic MSI-H/dMMR colorectal cancer. The submitted information constitutes the final analysis of 1 co-primary end point (PFS) and the second interim analysis of another co-primary end point (OS). The study recruited patients from 120 sites across 23 countries, including Canada (4 sites), the US, Asia, Europe, and Australia. It randomized 307 adult patients in total. The first patient visit was on November 30, 2015; the last visit was on February 19, 2020, and the database was locked on March 16, 2020.
Populations
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria for KEYNOTE-177 are described in Table 6. KEYNOTE-177 recruited adults with locally confirmed MSI-H/dMMR stage IV colorectal cancer. Patients needed to be 18 years or older, have an ECOG PS of 0 or 1 established 10 days before initiation of therapy, and have a life expectancy greater than 3 months.
Baseline Characteristics
Baseline characteristics for the intention-to-treat (ITT) analysis are summarized in Table 7. Between the pembrolizumab and SOC arms, there are small differences in the proportion of female participants (53.6% versus 46.8%), the number of patients recruited from outside Asia, North America, and Western Europe (14.4% versus 9.7%), the proportion of patients with an ECOG PS of 0 (49.0% versus 54.5%), the proportion of patients with an ECOG PS of 1 (51.0% versus 45.5%), the proportion of patients with hepatic or pulmonary metastases (56.2% versus 47.4%), and the proportion of patients with other metastases (43.8% versus 52.6%) or other mutation status (34.0% versus 24.7%).
Table 7: Summary of Baseline Characteristics in KEYNOTE-177
Characteristic | Pembrolizumab (N = 153) | SOC (N = 154) |
|---|---|---|
Female, n (%) | 82 (53.6) | 72 (46.8) |
Male, n (%) | 71 (46.4) | 82 (53.2) |
Mean age, years (SD) | 61.9 (14.9) | 60.6 (14.8) |
Median age, years (range) | 63.0 (24 to 93) | 62.5 (26 to 90) |
≥ 65 years of age, n (%) | 73 (47.7) | 71 (46.1) |
Race, n (%) | ||
Asian | 24 (15.7) | 26 (16.9) |
Black | 9 (5.9) | 5 (3.2) |
White | 113 (73.9) | 116 (75.3) |
Missing | 7 (4.6) | 7 (4.5) |
Ethnicity, n (%) | ||
Hispanic or Latino | 11 (7.2) | 10 (6.5) |
Not Hispanic or Latino | 128 (83.7) | 131 (85.1) |
Not reported/unknown | 12 (7.8) | 12 (7.8) |
Missing | 2 (1.3) | 1 (0.6) |
Geographic area, n (%) | ||
Asia | 22 (14.4) | 26 (16.9) |
Western Europe or North America | 109 (71.2) | 113 (73.4) |
Rest of world | 22 (14.4) | 15 (9.7) |
Eastern Cooperative Oncology Group Performance Status, n (%) | ||
0 | 75 (49.0) | 84 (54.5) |
1 | 78 (51.0) | 70 (45.5) |
Site of primary tumour, n (%) | ||
Right | 102 (66.7) | 107 (69.5) |
Left | 46 (30.1) | 42 (27.3) |
Other | 4 (2.6) | 5 (3.2) |
Missing | 1 (0.7) | 0 (0) |
Metastases location, n (%) | ||
Hepatic or pulmonary | 86 (56.2) | 73 (47.4) |
Othera | 67 (43.8) | 81 (52.6) |
Diagnosed state, n (%) | ||
Recurrent | 80 (52.3) | 74 (48.1) |
Newly diagnosed | 73 (47.7) | 80 (51.9) |
Prior systemic therapy, n (%) | ||
Adjuvant only | 33 (21.6) | 37 (24.0) |
Neoadjuvant only | 2 (1.3) | 3 (1.9) |
Neoadjuvant and adjuvant | 3 (2.0) | 5 (3.2) |
None | 115 (75.2) | 109 (70.8) |
Mutation status, n (%) | ||
BRAF/KRAS/NRAS all wild type | 34 (22.2) | 35 (22.7) |
KRAS/NRAS mutant and BRAF V600E not mutant | 33 (21.6) | 38 (24.7) |
BRAF V600E mutant and KRAS/NRAS not mutant | 34 (22.2) | 40 (26.0) |
BRAF V600E and KRAS/NRAS mutant | 0 (0) | 3 (1.9) |
Other | 52 (34.0) | 38 (24.7) |
MSI-H status, n (%) | ||
Positive | 153 (100) | 153 (99.4) |
Negative | 0 (0) | 1 (0.6) |
Received oncologic surgery with curative intent, n (%) | ||
Yes | 14 (9.2) | 13 (8.4) |
No | 139 (90.8) | 141 (91.6) |
MSI-H = microsatellite instability-high; SD = standard deviation; SOC = standard of care.
aNo additional information is provided regarding the location of “other” metastases.
Source: Clinical Study Report P177V01MK3475.13
Interventions
Patients in KEYNOTE-177 were centrally randomized in a 1:1 ratio to pembrolizumab 200 mg administered intravenously every 3 weeks or to SOC every 2 weeks. SOC was determined by the treating clinician and could consist of any of the following:
mFOLFOX (oxaliplatin, 85 mg/m2 of body surface area on day 1; leucovorin, 400 mg/m2 of body surface area on day 1; and 5-fluropyrimidine, 400 mg/m2 of body surface area on day 1, then 2,400 mg over 46 to 48 hours)
FOLFOX (as above) plus bevacizumab (5 mg/kg on day 1)
FOLFOX (as above) plus cetuximab (400 mg/m2 of body surface area on day 1 then 250 mg/m2 weekly)
FOLFIRI (irinotecan, 180 mg/m2 of body surface area on day 1; leucovorin, 400 mg/m2 of body surface area on day 1; and 5-fluropyrimidine, 400 mg/m2 of body surface area on day 1, then 2,400 mg over 46 to 48 hours)
FOLFIRI (as above) plus bevacizumab (as above)
FOLFIRI (as above) plus cetuximab (as above).
Pembrolizumab and SOC regimens were provided for a maximum of 35 treatments, until disease progression, development of unacceptable AEs, or decision by the physician or patient to withdraw. Those in the SOC arm were permitted to cross over to the pembrolizumab arm, and those in either arm could receive subsequent anticancer therapy. Crossovers were allowed if several criteria were met, notably including the following: progressive disease per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1), not having received other anticancer therapy since the last study dose, adverse effects from study medications at grade 1 or better, and having maintained an ECOG PS of 0 or 1. There is no information regarding the criteria used to initiate subsequent anticancer therapy, when it was initiated, or why it was initiated.
Outcomes
A list of efficacy outcomes identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. A detailed discussion and critical appraisal of outcome measures is provided in Appendix 4.
Progression-Free Survival
Progression-free survival was a co-primary outcome and defined as the time from randomization to the first of either disease progression per RECIST 1.1 based on a blinded central imaging vendor or death due to any cause. Patients were censored at the last disease assessment if there was no progression, death, or use of subsequent anticancer treatment. If a new anticancer treatment was initiated, patients were censored at the last disease assessment before treatment initiation. A sensitivity analysis was conducted that treated the crossovers or the addition of anticancer medications as death or progression events. Additionally, a second sensitivity analysis defined PFS as the time from randomization to progression on next line of therapy or death from any cause and thus provided no consideration for the crossovers or addition of anticancer medications. The clinical experts consulted suggest any survival beyond 8 to 10 months is clinically significant.
Overall Survival
Overall survival was a co-primary outcome and defined as the time from randomization to death from any cause. Patients with no known death were censored at the point of last contact. The clinical experts consulted suggested any incremental survival above the SOC arm would be considered clinically significant.
Overall Response Rate
Overall response rate was a secondary outcome and was defined as the proportion of patients who had a partial or complete response per RECIST 1.1 based on a blinded central imaging vendor. No MID was identified.
Duration of Response
Duration of response was an exploratory outcome and defined as the time from first response to disease progression or death for any patient with a demonstrated partial or complete response, per RECIST 1.1, based on a blinded central imaging vendor. No MID was identified.
Time to Response
Time to response was not defined in the documentation provided.
Health-Related Quality of Life
HRQoL was measured by the EORTC QLQ-C30, the EORTC Quality of Life Questionnaire Colorectal Cancer Module (QLQ-CR29), and the EQ-5D-3L. The EORTC QLQ-30 is a widely used cancer-specific HRQoL instrument consisting of 30 items measuring 5 functional dimensions (physical, role, cognitive, emotional, and social), 3 symptoms dimensions (fatigue, nausea/vomiting, and pain), 6 additional items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact), and a global HRQoL measure. The EORTC QLQ-CR29 includes scales to assess functional issues and symptoms such as urinary frequency, fecal seepage, stool consistency, body image, and other common problems associated with treatment of colorectal cancer. EQ-5D-3L is another standard instrument to measure health outcomes and is particularly useful in developing economic models. EQ-5D-3L measures mobility, self-care, usual activities, pain/discomfort, and anxiety/depression using a 3-point ordinal scale. These measurements can be pooled into a single utility score. Further, the EQ-5D-3L contains a Visual Analogue Scale (EQ VAS) ranging from 0 to 100 so that participants may rate their general health state.
Each of the HRQoL questionnaires was conducted at baseline and at 18 weeks so that the change could be calculated and compared between groups. The MID for colorectal cancers on the EORTC QLQ-C30 is 5,22 the MID for cancer patients on the EQ VAS is 6 to 10, and the MID for US patients with cancer on the EQ-5D utility scale is 0.05 to 0.08.23 No MID on the EQ-5D-3L scale was identified for colorectal cancer patients.
Harms
AEs were defined as any unfavourable or unintended sign, symptom, disease, or worsening of a pre-existing condition temporally associated with a study treatment. Serious AEs were those that resulted in death; were life-threatening; resulted in persistent or significant disability or incapacity; resulted in or prolonged existing inpatient hospitalization; were a congenital anomaly or birth defect, an important medical event, or a new cancer; or were associated with an overdose. Immune-mediated AEs were defined as SAEs characterized by inflammation and included infusion-related reactions.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome category | KEYNOTE-177 |
|---|---|
Primary | Progression-free survival |
Primary | Overall survival |
Secondary | Overall response rate |
Exploratory | Duration of response |
Exploratory | Time to response |
Exploratory | Health-related quality of life |
Statistical Analysis
The study was a group sequential trial with PFS and OS as co-primary end points and ORR as a secondary end point. All analyses were conducted on an ITT basis. PFS and OS were analyzed using log-rank tests for Kaplan–Meier plots and simple Cox proportional hazards models using the Efron method of tie handling to assess the magnitude of treatment differences between the treatment arms.
In the PFS analysis, the PHA was violated; hence, the RMST was calculated instead. Like an HR, RMST measures long-term survival profiles relative to median survival, better accounts for long-term survivors, and is a more stable measure. The RMST is typically calculated over a specific follow-up period; thus, an RMST of 20 months over a 24-month follow-up period would suggest that if an individual is followed for 24 months, they would survive an average of 20 months. The sponsor also calculated piecewise HRs and weighted HRs. In the former, HRs were calculated before and after 3 months, and in the latter, Fleming-Harrington weights as described by León et al. were derived and applied to the Cox model.24 In this analysis, 3 additional HRs were calculated with heavier weights on the early, late, or middle time points. Again, patients were censored at the last disease assessment if there was no progression, death, or use of other anticancer treatment. If any new anticancer treatment was initiated, patients were censored at the last disease assessment before treatment initiation. A sensitivity analysis was conducted to assess the impact of this phenomenon on PFS, and crossovers or the addition of any anticancer medications were treated as death or progression events. Additionally, a second sensitivity analysis defined PFS as the time from randomization to progression on the next line of therapy or death from any cause, thus providing no consideration for crossovers or subsequent use of any anticancer medications.
To adjust for patients crossing over or receiving subsequent anti-PD1/PDL1 (but not other anticancer) therapies in the OS analysis, the inverse probability of censoring weighting, rank preserving structural failure time, and 2-stage analysis methods were used. In brief, the inverse probability of censoring weighting method adjusts for crossovers by differentially weighting all patients in the control arm. Those who cross over receive a lower weight, while those who do not cross over but have characteristics that suggest they are likely to cross over receive a higher weight. However, these weightings rely on a comprehensive collection and analysis of all variables correlated with crossing over. The rank preserving structural failure time method assumes all patients would receive equal benefit from identical interventions. This method compares time on and off treatment to estimate survival times without treatment and a treatment effect adjusted for crossovers. Finally, 2-stage adjustment assumes crossovers only occur following disease progression and uses this point to establish a “secondary” baseline. Within the control group, the treatment effect is estimated between those who do and do not cross over and adjusts for “secondary” baseline characteristics. The incremental treatment effect between these groups is then used to discount the treatment effect observed in those who cross over; these effects are then compared with those of the experimental group to estimate the treatment effect adjusted for crossovers. Additional information on these methods can be found in Latimer et al.25
Overall response rate was analyzed using the Miettinen and Nurminen method, and duration of response and time to response were analyzed using the Kaplan–Meier method. A partial or complete response or progression was defined according to the RECIST 1.1 guidelines. Health-related quality of life measures were analyzed using mixed-effects models with an assumption that missing data were random. No statistical testing or models were used to analyze harms data.
Power calculations in the PFS Cox model required 209 events within 24 months for 98% power to detect a 0.55 HR and assumed a 30-month enrolment period and 13 months of follow-up. In the OS analysis, 190 events were required for 85% power to detect an HR of 0.62 and assumed a 30-month enrolment period and 33.5 months of follow-up. The ORR analysis assumed a 50% response rate in the SOC arm would result in 92% power to detect an effect size of 19%.
The study had originally planned for 2 interim analyses and a final analysis of PFS and OS. The first interim analysis was performed after approximately 162 PFS events had occurred and 6 months after the last patient was randomized. The statistical plan stipulated that the second interim analysis should be performed after approximately 209 PFS events had occurred or 24 months after the last patient was randomized, whichever occurred first. This report constitutes the final analysis for PFS, but the second interim analysis for OS. At the interim analysis, the O’Brien (Lan-DeMets) alpha-spending function was used to construct group sequential boundaries to control the type I error rate across both primary end points and interim analyses at a 1-sided alpha level of 2.5%. By using the graphical approach of Maurer and Bretz, if 1 primary hypothesis is rejected, the alpha will be shifted to the other hypotheses. Initially, 1.25% was allocated each to the PFS and OS analysis and 0% to the ORR analysis. The statistical analysis plan stipulated that should the PFS analysis null hypothesis fail to be rejected, the ORR analysis would then be tested at 0.0125% and the OS analysis at 0.249%. An identical method was used should the OS analysis fail to reject the null hypothesis.
Table 9: Statistical Analysis of Efficacy End Points in KEYNOTE-177
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Progression-free survival | Log-rank test and Cox proportional hazards | Unadjusted | Additional analyses to address censoring definitions |
Overall survival | Log-rank test and Cox proportional hazards | Unadjusted | Additional analyses to adjust for crossovers and subsequent use of anti-PD1/PDL1 therapies |
Overall response rate | Miettinen and Nurminen | Unadjusted | Missing data were treated as nonresponders |
Duration and time to response | Kaplan-Meier | Unadjusted | None |
Health-related quality of life | Mixed-effects model | Unadjusted | None |
Harms | None | None | None |
Analysis Populations
Efficacy data were analyzed using an ITT approach, while only those who received at least 1 dose of pembrolizumab or SOC were included in the safety analysis.
Results
Patient Disposition
KEYNOTE-177 screened 852 patients, of whom 307 met the pre-specified eligibility criteria. These 307 were randomized in a 1:1 ratio (153 and 154 patients to the pembrolizumab and SOC arms, respectively) and were analyzed in the efficacy analyses. All patients in the pembrolizumab arm received at least 1 dose of treatment and were analyzed in the safety analyses, while 143 patients (92.8%) in the SOC arm received at least 1 dose of treatment and were analyzed in the safety analyses. Fifty-eight pembrolizumab patients (37.9%) and 75 SOC patients (48.7%) discontinued the trial. An additional 44 patients (28.8%) and 44 patients (28.6%) in the pembrolizumab and SOC arms, respectively, received other anticancer therapy. No patients from the pembrolizumab arm crossed over to the SOC arm, but 56 SOC patients (36.4%) crossed over to the pembrolizumab arm. All efficacy end points were analyzed with an ITT approach, while only those receiving the medication were assessed for safety outcomes.
Table 10: Patient Disposition in KEYNOTE-177
Patient disposition | Pembrolizumab | SOC |
|---|---|---|
Screened, n | 852 | |
Randomized, n | 153 | 154 |
Treated with at least 1 dose, n (%) | 153 (100) | 143 (92.8) |
Discontinued treatment, n (%) | 94 (61.4) | 137 (95.8) |
Disease progression | 50 (32.7) | 86 (60.1) |
Adverse events | 22 (14.4) | 17 (11.9) |
Clinical progression | 9 (5.9) | 6 (4.2) |
Complete response | 9 (5.9) | 4 (2.8) |
Physician decision | 3 (2.0) | 12 (8.4) |
Patient withdrawal | 1 (0.7) | 11 (7.7) |
Protocol violation or other | 0 (0) | 1 (0.7) |
Discontinued trial, n (%) | 58 (37.9) | 75 (48.7) |
Crossed over to opposite arm, n (%) | 0 (0) | 56 (36.4) |
Received subsequent anticancer therapy, n (%) | 44 (28.8) | 44 (28.6) |
Anti-PD1/PDL therapy | 9 (5.9) | 35 (22.7) |
Antimuscarinic/non–disease-related medication | 2 (1.3) | 0 (0) |
CD40 inhibitor | 0 (0) | 1 (0.6) |
CTLA-4 inhibitor | 0 (0) | 4 (2.6) |
Chemotherapy | 35 (22.9) | 18 (11.7) |
EGFR inhibitor | 8 (5.2) | 4 (2.6) |
Estrogen derivative/non-disease-related medication | 1 (0.7) | 0 (0.0) |
Folic acid derivative | 24 (15.7) | 12 (7.8) |
ICOS inhibitor | 1 (0.7) | 1 (0.6) |
Nucleoside analogue/thymidine phosphorylase inhibitor | 1 (0.7) | 2 (1.3) |
TIM3 inhibitor | 1 (0.7) | 1 (0.6) |
VEGF inhibitor | 22 (14.4) | 11 (7.1) |
Median exposure to treatment, months (range) | 11.1 (0.0 to 30.6) | 5.7 (0.1 to 39.6) |
Median follow-up, months (range) | 28.4 (0.2 to 48.3) | 27.2 (0.8 to 46.6) |
ITT, n | 153 | 154 |
Safety, n | 153 | 143 |
EGFR = epidermal growth factor receptor; ICOS = inducible co-stimulator; ITT = intention to treat; SOC = standard of care; VEGF = vascular endothelial growth factor.
Source: Clinical Study Report P177V01MK3475.13
Exposure to Study Treatments
Median exposure to treatment was higher in the pembrolizumab arm (11.1 months) than in the SOC arm (5.7 months). Median follow-up was similar between the pembrolizumab arm (28.4 months) and SOC arm (27.2 months). No patient in the pembrolizumab arm crossed over to the SOC arm, but 56 patients (36.3%) in the SOC arm crossed over to receive pembrolizumab. Similarly, about 28% in each arm received subsequent anticancer therapies. The class of medication used subsequently differed in each arm, with use of anti-PD1/PDL1 higher in the SOC arm and use of chemotherapy, epidermal growth factor receptor inhibitors, folic acid derivatives, and vascular endothelial growth factor inhibitors higher in the pembrolizumab arm.
Efficacy
Only those efficacy outcomes identified in the review protocol are reported below. See Appendix 3 for detailed efficacy data.
Progression-Free Survival
In the pembrolizumab and SOC arms, 82 patients (53.6%) and 113 patients (73.4%) experienced an event, respectively. Median survival was higher in the pembrolizumab arm (16.5 months; 95% CI, 5.4 to 32.4) than in the SOC arm (8.2 months; 95% CI, 6.1 to 10.2), yielding a statistically significant HR of 0.60 (95% CI, 0.45 to 0.80). However, because the PHA was violated, complicating the interpretation of the HR, the RMST after 24 months of follow-up was reported. Pembrolizumab survival (13.7 months; 95% CI, 12.0 to 15.4) was higher than SOC survival (10.8 months; 95% CI, 9.4 to 12.2), indicating that patients who received pembrolizumab for 24 months would survive an average of 13.7 months compared to 10.8 months for patients receiving SOC. The RMST results are consistent with those of the median survival and HR in favour of pembrolizumab. The mean difference in RMST was 2.9 months (95% CI, 0.7 to 5.1). Progression-free survival at specific time points is also displayed in Table 11. To further investigate this issue, piecewise and weighted HRs are presented in Appendix 3. Appendix 3 also outlines 2 sensitivity analyses to examine of the effect of crossovers and the use of subsequent anticancer medications on PFS.
Table 11: Progression-Free Survival in KEYNOTE-177
Progression-free survival | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Number of events, n (%) | 82 (53.6) | 113 (73.4) |
Progression, n (%) | 65 (42.5) | 86 (55.8) |
Death, n (%) | 17 (11.1) | 27 (17.5) |
Censored, n (%) | 71 (46.4) | 41 (26.6) |
Median progression-free survival, months (95% CI) | 16.5 (5.4 to 32.4) | 8.2 (6.1 to 10.2) |
Hazard ratio (95% CI; P value) | 0.60 (0.45 to 0.80; 0.0002)a,b | |
Restricted mean survival time based on 24 months of follow-up, months (95% CI) | 13.7 (12.0 to 15.4) | 10.8 (9.4 to 12.2) |
Difference in restricted mean survival time, months (95% CI) | 2.9 (0.7 to 5.1) | |
Progression-free survival rate at time point, % (95% CI) | ||
6 months | 57.6 (49.3 to 65.0) | 59.7 (51.1 to 67.3) |
9 months | 56.8 (48.5 to 64.3) | 45.5 (36.9 to 53.7) |
12 months | 55.3 (47.0 to 62.9) | 37.3 (29.0 to 45.5) |
18 months | 49.1 (40.7 to 57.0) | 26.7 (19.2 to 34.7) |
24 months | 48.3 (39.9 to 56.2) | 18.6 (12.1 to 26.3) |
CI = confidence interval; SOC = standard of care.
aStatistically significant after adjusting for multiple testing.
bProportional hazards assumption was violated.
Source: Clinical Study Report P177V01MK3475.13
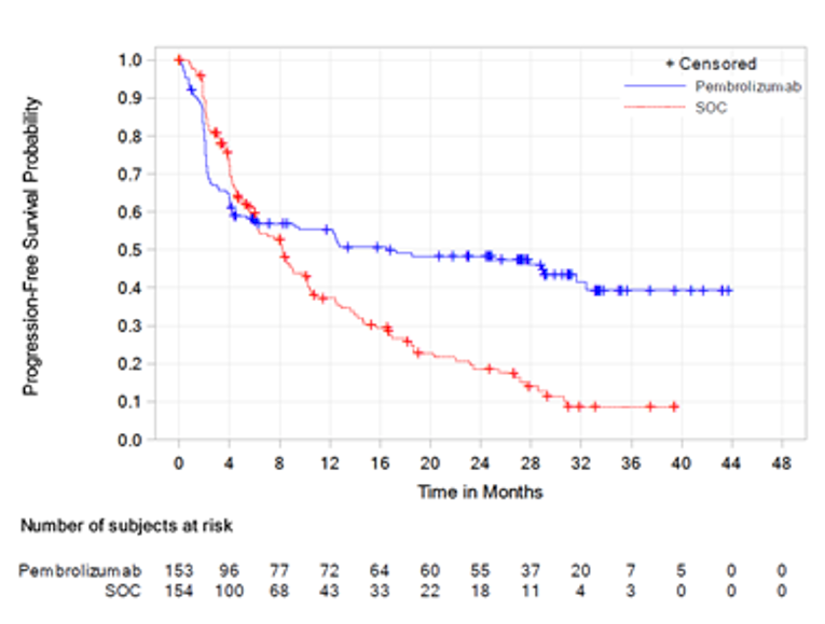
Overall Survival
Fewer deaths occurred in the pembrolizumab arm (36.6%) than in the SOC arm (44.8%). No median survival was reported for the pembrolizumab arm, but median survival was 34.8 months (95% CI, 26.3 to not reached) in the SOC arm. The HR was 0.77 (95% CI, 0.54 to 1.09; P = 0.0694). Survival rates at specific time points are displayed in Table 12. To adjust for the impact of crossovers and the use of subsequent anti-PD1/PDL1 therapies, the sponsor also conducted 3 sensitivity analyses, which are available in Appendix 3.
Table 12: Overall Survival in KEYNOTE-177
Overall survival | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Number of events, n (%) | 56 (36.6) | 69 (44.8) |
Median survival, months (95% CI) | NR | 34.8 (26.3 to NR) |
Hazard ratio (95% CI; P value) | 0.77 (0.54 to 1.09; 0.0694)a | |
Overall survival rate at time point, % (95% CI) | ||
6 months | 83.0 (76.1 to 88.1) | 86.0 (79.4 to 90.7) |
9 months | 79.7 (72.5 to 85.3) | 78.7 (71.3 to 84.4) |
12 months | 77.8 (70.3 to 83.6) | 74.0 (66.2 to 80.3) |
18 months | 71.2 (63.4 to 77.7) | 65.9 (57.7 to 72.9) |
24 months | 68.0 (59.9 to 74.7) | 59.8 (51.5 to 67.2) |
CI = confidence interval; NR = not reached; SOC = standard of care.
aStatistically insignificant after adjusting for multiple testing.
Source: Clinical Study Report P177V01MK3475.13
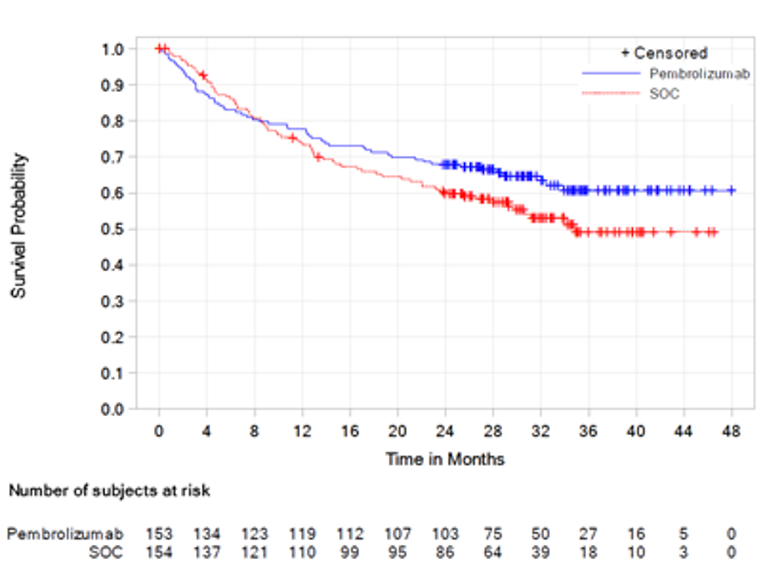
Overall Response Rate
The ORR was higher in the pembrolizumab arm (43.8%; 95% CI, 35.8% to 52.0%) than the SOC arm (33.1%; 95% CI, 25.8% to 41.1%). After adjustment for multiplicity, the between-group difference of 10.7% (95% CI, –0.2% to 21.3%) was not statistically significant. Full results are displayed in Table 13.
Table 13: Overall Response Rate in KEYNOTE-177
Overall response rate | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Number of responses, n (%) Complete response, n (%) Partial response, n (%) Stable disease, n (%) Progressive disease, n (%) Could not be evaluated or no assessment, n (%) | 67 (43.8) 17 (11.1) 50 (32.7) 32 (20.9) 45 (29.4) 9 (5.9) | 51 (33.1) 6 (3.9) 45 (29.2) 65 (42.2) 19 (12.3) 19 (12.3) |
Overall response rate, % (95% CI) | 43.8 (35.8 to 52.0) | 33.1 (25.8 to 41.1) |
Difference in overall response rate between pembrolizumab and SOC, % (95% CI; P value) | 10.7 (–0.2 to 21.3; 0.0275)a | |
CI = confidence interval; SOC = standard of care.
aStatistically insignificant after adjusting for multiple testing.
Source: Clinical Study Report P177V01MK3475.13
Duration of Response
Duration of response was evaluated in KEYNOTE-177 as an exploratory outcome without adjustment for multiplicity, but no median duration of response could be calculated for the pembrolizumab arm. The median duration of response in the SOC arm was 10.6 months. The proportion of patients with an extended duration of response at discrete time points is displayed in Table 14.
Table 14: Duration of Response in KEYNOTE-177
Duration of response | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Median, months (range) | NR (2.3 to 41.4) | 10.6 (2.8 to 37.5) |
Patients with extended response duration, n (%) | ||
≥ 6 months | 61 (96.9) | 43 (87.9) |
≥ 9 months | 55 (91.9) | 27 (59.9) |
≥ 12 months | 50 (85.1) | 19 (43.8) |
≥ 18 months | 45 (85.1) | 11 (35.3) |
≥ 24 months | 29 (82.6) | 9 (35.5) |
SOC = standard of care.
Source: Clinical Study Report P177V01MK3475.13
Time to Response
The exploratory outcome mean time to response was similar between the pembrolizumab arm (4.0 months; standard deviation [SD] = 3.7) and SOC arm (3.6 months; SD = 4.1). Similarly, the median times to response were similar between the pembrolizumab arm (2.2 months; range, 1.8 to 18.8) and SOC arm (2.1 months; range, 1.7 to 24.9). Full results are presented in Appendix 3.
Health-Related Quality of Life
Health-related quality of life was evaluated in KEYNOTE-177 as an exploratory outcome without adjustment for multiplicity. Based on the EORTC QLQ-C30, HRQoL improved between 18 weeks and baseline in the pembrolizumab arm (3.33; 95% CI, –0.05 to 6.72) and decreased in the SOC arm (–5.63; 95% CI, –9.32 to –1.94). The least squares mean difference between these scores was 8.96 (95% CI, 4.24 to 13.69). Results for the EORTC QLQ-CR29 symptom scale were only provided as figures. Of note, those in the SOC arm saw more improvements in buttock pain, hair loss, and taste relative to those in the pembrolizumab arm, while bloating improved more in the pembrolizumab arm. Health-related quality of life as measured by the EQ VAS determined that HRQoL also improved in the pembrolizumab arm between 18 weeks and baseline (4.50; 95% CI, 1.16 to 7.83) and decreased in the SOC arm (–2.88; 95% CI, –6.46 to 0.69). The least squares mean difference between these scores was 7.38 (95% CI, 2.82 to 11.93). The EQ-5D-3L utility score increased in the pembrolizumab arm (0.04; 95% CI, 0.00 to 0.08) and decreased in the SOC arm (–0.01; 95% CI, –0.05 to 0.02), with a least squares mean difference of 0.05 (95% CI, 0.00 to 0.10).
Table 15: Health-Related Quality of Life in KEYNOTE-177
Quality of life using EORTC QLQ-C30 and QLQ-CR29 | Pembrolizumab N = 141 | SOC N = 131 |
|---|---|---|
Global health/quality of life score, change from baseline to 18 weeks, least squares mean (95% CI) | 3.33 (–0.05 to 6.72) | –5.63 (–9.32 to –1.94) |
Least squares mean difference in global health/quality of life score (95% CI) | 8.96 (4.24 to 13.69) | |
Time to deterioration in global health status/quality of life, HR (95% CI) | 0.61 (0.38 to 0.98) | |
Time to deterioration in EORTC QLQ-C30 physical functioning, HR (95% CI) | 0.50 (0.32 to 0.81) | |
Time to deterioration in EORTC QLQ-C30 social functioning, HR (95% CI) | 0.53 (0.32 to 0.87) | |
Time to deterioration in EORTC QLQ-C30 fatigue, HR (95% CI) | 0.48 (0.33 to 0.69) | |
Time to deterioration in EORTC QLQ-CR29 urinary incontinence, HR (95% CI) | 0.43 (0.14 to 1.31)a | |
Quality of life using EQ-5D-3L | Pembrolizumab N = 142 | SOC N = 133 |
EQ VAS, change from baseline to 18 weeks, least squares mean (95% CI) | 4.50 (1.16 to 7.83) | –2.88 (–6.46 to 0.69) |
Least squares mean difference in EQ VAS score (95% CI) | 7.38 (2.82 to 11.93) | |
EQ-5D-3L utility score, change from baseline to 18 weeks, least squares mean (95% CI) | 0.04 (0.00 to 0.08) | –0.01 (–0.05 to 0.02) |
Least squares mean difference in EQ-5D-3L utility score (95% CI) | 0.05 (0.00 to 0.10) | |
CI = confidence interval; EORTC = European Organisation for Research and Treatment of Cancer; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; HR = hazard ratio; QLQ-C30 = Quality of Life Questionnaire Core 30; QLQ-CR29 = Quality of Life Questionnaire Colorectal Cancer Module; SOC = standard of care.
aIn this analysis, there were 139 and 132 individuals in the pembrolizumab and SOC arms, respectively.
Source: Clinical Study Report P177V01MK3475.13
Figure 4: Least Squares Mean Change in EORTC QLQ-CR29 Symptom Scale From Baseline to Week 18
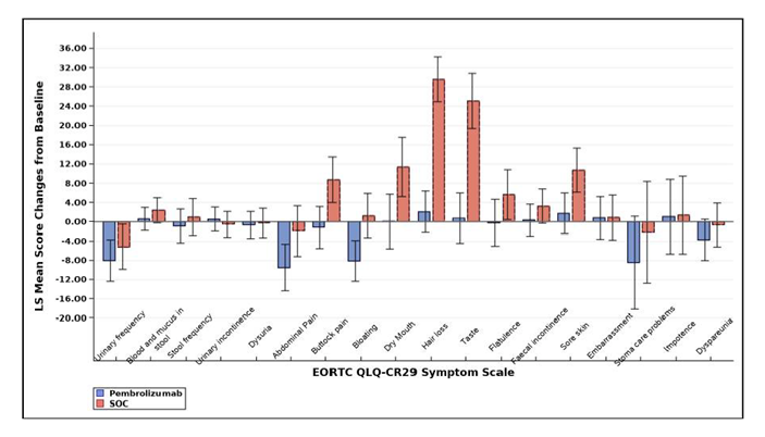
EORTC = European Organisation for Research and Treatment of Cancer; LS = least squares; QLQ-CR29 = Quality of Life Questionnaire Colorectal Cancer Module; SOC = standard of care.
Figure 5: Least Squares Mean Change in EORTC QLQ-CR29 Functional Scale From Baseline to Week 18
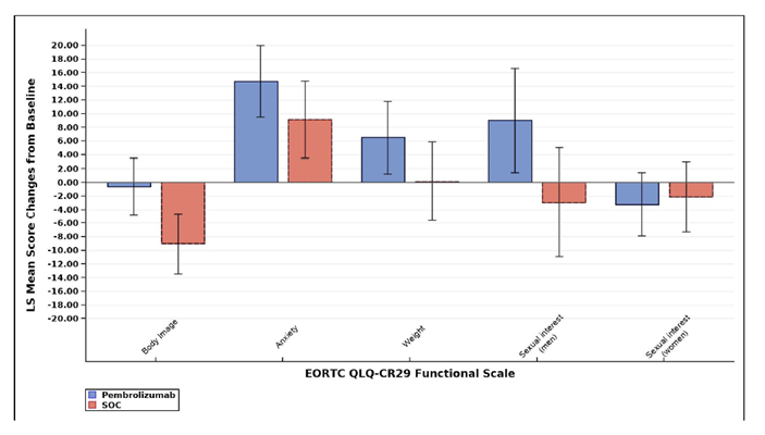
EORTC = European Organisation for Research and Treatment of Cancer; LS = least squares; QLQ-CR29 = Quality of Life Questionnaire Colorectal Cancer Module; SOC = standard of care.
Harms
Only those harms identified in the review protocol are reported below. See Table 16, Table 17, and Table 18 for detailed harms data.
Adverse Events
The frequency of any AE was similar in both arms of KEYNOTE-177. The most common AEs in the pembrolizumab arm were diarrhea, fatigue, nausea, abdominal pain, decreased appetite, and vomiting. The most common AEs in the SOC arm were diarrhea, fatigue, nausea, decreased appetite, vomiting, constipation, stomatitis, abdominal pain, anemia, decreased neutrophil count, peripheral sensory neuropathy, asthenia, neutropenia, and alopecia.
Table 16: Summary of Adverse Events in KEYNOTE-177
Adverse event | Pembrolizumab N = 153 | SOC N = 143 |
|---|---|---|
Patients with > 1 AE, n (%) | 149 (97.4) | 142 (99.3) |
Patients with > 1 SAE, n (%) | 62 (40.5) | 75 (52.4) |
Patients with AE resulting in treatment discontinuation, n (%) | 21 (13.7) | 17 (11.9) |
Patients with AE resulting in death, n (%) | 6 (3.9) | 7 (4.9) |
Death due to AE, n (%) | 0 (0) | 1 (0.7) |
Most common events,a n (%) | ||
Diarrhea | 68 (44.4) | 89 (62.2) |
Fatigue | 58 (37.9) | 72 (50.3) |
Nausea | 47 (30.7) | 85 (59.4) |
Abdominal pain | 37 (24.2) | 42 (29.4) |
Decreased appetite | 36 (23.5) | 58 (40.6) |
Vomiting | 33 (21.6) | 53 (37.1) |
Arthralgia | 28 (18.3) | 7 (4.9) |
Pyrexia | 28 (18.3) | 20 (14.0) |
Anemia | 27 (17.6) | 32 (22.4) |
Constipation | 26 (17.0) | 45 (31.5) |
Cough | 26 (17.0) | 23 (16.1) |
Back pain | 26 (17.0) | 24 (16.8) |
Pruritus | 25 (16.3) | 12 (8.4) |
Aspartate aminotransferase increase | 24 (15.7) | 12 (8.4) |
Dizziness | 24 (15.7) | 27 (18.9) |
Alanine aminotransferase increase | 22 (14.4) | 16 (11.2) |
Blood alkaline phosphatase increase | 22 (14.4) | 6 (4.2) |
Dyspnea | 21 (13.7) | 15 (10.5) |
Headache | 21 (13.7) | 22 (15.4) |
Abdominal pain, upper | 20 (13.1) | 11 (7.7) |
Nasopharyngitis | 20 (13.1) | 10 (7.0) |
Rash | 20 (13.1) | 16 (11.2) |
Asthenia | 19 (12.4) | 31 (21.7) |
Dry skin | 19 (12.4) | 13 (9.1) |
Hypertension | 19 (12.4) | 16 (11.2) |
Hypothyroidism | 19 (12.4) | 3 (2.1) |
Pain in extremity | 18 (11.8) | 11 (7.7) |
Edema, peripheral | 18 (11.8) | 12 (8.4) |
Dry mouth | 17 (11.1) | 9 (6.3) |
Upper respiratory tract infection | 16 (10.5) | 8 (5.6) |
Urinary tract infection | 14 (9.2) | 16 (11.2) |
Hypokalemia | 13 (8.5) | 24 (16.8) |
Alopecia | 11 (7.2) | 29 (20.3) |
Stomatitis | 10 (6.5) | 43 (30.1) |
Dyspepsia | 9 (5.9) | 16 (11.2) |
Mucosal inflammation | 7 (4.6) | 27 (18.9) |
Weight decrease | 7 (4.6) | 17 (11.9) |
Neutropenia | 3 (2.0) | 30 (21.0) |
Neuropathy, peripheral sensory | 3 (2.0) | 31 (21.7) |
Epistaxis | 2 (1.3) | 23 (16.1) |
Neutrophil count decrease | 2 (1.3) | 33 (23.1) |
Neuropathy, peripheral | 1 (0.7) | 27 (18.9) |
Palmar-plantar erythrodysesthesia syndrome | 1 (0.7) | 25 (17.5) |
White blood cell count decrease | 1 (0.7) | 17 (11.9) |
AE = adverse event; SAE = serious adverse event; SOC = standard of care.
aFrequency greater than 10% in either treatment group.
Source: Clinical Study Report P177V01MK3475.13
Serious Adverse Events
The rate of SAEs was lower in the pembrolizumab arm (40.5%) than in the SOC arm (52.4%). The most common SAEs in the pembrolizumab arm were abdominal pain, diarrhea, pyrexia, acute kidney injury, colitis, and pneumonia. The most common SAEs in the SOC arm were diarrhea, febrile neutropenia, small intestinal obstruction, and pulmonary embolism.
Table 17: Summary of Serious Adverse Events in KEYNOTE-177
Serious adverse event, n (%) | Pembrolizumab N = 153 | SOC N = 143 |
|---|---|---|
Abdominal pain | 7 (4.6) | 2 (1.4) |
Diarrhea | 4 (2.6) | 9 (6.3) |
Pyrexia | 4 (2.6) | 0 (0) |
Acute kidney injury | 3 (2.0) | 2 (1.4) |
Colitis | 3 (2.0) | 0 (0) |
Pneumonia | 3 (2.0) | 2 (1.4) |
Adrenal insufficiency | 2 (1.3) | 0 (0) |
Autoimmune colitis | 2 (1.3) | 0 (0) |
Hepatitis | 2 (1.3) | 0 (0) |
Infection | 2 (1.3) | 0 (0) |
Intestinal obstruction | 2 (1.3) | 2 (1.4) |
Small intestinal obstruction | 2 (1.3) | 5 (3.5) |
Squamous cell carcinoma | 2 (1.3) | 0 (0) |
Subileus | 2 (1.3) | 0 (0) |
Anemia | 1 (0.7) | 2 (1.4) |
Dyspnea | 1 (0.7) | 0 (0) |
Febrile neutropenia | 1 (0.7) | 6 (4.2) |
Ileus | 1 (0.7) | 3 (2.1) |
Influenza | 1 (0.7) | 2 (1.4) |
Large intestinal obstruction | 1 (0.7) | 2 (1.4) |
Pneumonitis | 1 (0.7) | 0 (0) |
Pulmonary embolism | 1 (0.7) | 4 (2.8) |
Vomiting | 1 (0.7) | 4 (2.8) |
Cholangitis | 0 (0) | 2 (1.4) |
Decreased appetite | 0 (0) | 3 (2.1) |
Dehydration | 0 (0) | 4 (2.8) |
Device-related infection | 0 (0) | 2 (1.4) |
Fatigue | 0 (0) | 3 (2.1) |
Hypokalemia | 0 (0) | 2 (1.4) |
Intestinal perforation | 0 (0) | 2 (1.4) |
Neutropenia | 0 (0) | 3 (2.1) |
Pleural effusion | 0 (0) | 0 (0) |
Tumour-associated fever | 0 (0) | 2 (1.4) |
Urinary tract infection | 0 (0) | 1 (0.7) |
Urosepsis | 0 (0) | 2 (1.4) |
SOC = standard of care.
Source: Clinical Study Report P177V01MK3475.13
Withdrawals Due to Adverse Events
Withdrawals due to AEs were similar between the pembrolizumab (13.7%) and SOC (11.9%) arms.
Mortality
The proportion of individuals with an AE resulting in death was lower in the pembrolizumab arm (3.9%) than in the SOC arm (4.9%). Deaths attributed to an AE were similar between the arms (0% versus 0.7%).
Immune-Mediated Adverse Events
The frequency of immune-mediated AEs is summarized in Table 18. Such AEs were higher in the pembrolizumab arm (30.7%) than in the SOC arm (12.6%). The most common immune-mediated AEs in the pembrolizumab arm were hypothyroidism, colitis, hyperthyroidism, and pneumonitis. However, the rate of infusion reactions was higher in the SOC arm.
Table 18: Immune-Mediated Adverse Events in KEYNOTE-177
Immune-mediated adverse event | Pembrolizumab N = 153 | SOC N = 143 |
|---|---|---|
Patients with 1 or more immune-mediated adverse events, n (%) | 47 (30.7) | 18 (12.6) |
Patients with 1 or more grade 3 to 5 immune-mediated adverse events, n (%) | 14 (9.2) | 3 (2.1) |
Hypothyroidism, n (%) | 19 (12.4) | 3 (2.1) |
Colitis, n (%) | 10 (6.5) | 0 (0) |
Hyperthyroidism, n (%) | 6 (3.9) | 0 (0) |
Pneumonitis, n (%) | 6 (3.9) | 1 (0.7) |
Adrenal insufficiency, n (%) | 4 (2.6) | 0 (0) |
Hepatitis, n (%) | 4 (2.6) | 0 (0) |
Infusion reactions, n (%) | 3 (2.0) | 11 (7.7) |
Hypophysitis, n (%) | 2 (1.3) | 0 (0) |
Severe skin reactions, n (%) | 2 (1.3) | 2 (1.4) |
Thyroiditis, n (%) | 2 (1.3) | 0 (0) |
Myositis, n (%) | 1 (0.7) | 0 (0) |
Nephritis, n (%) | 1 (0.7) | 0 (0) |
Pancreatitis, n (%) | 1 (0.7) | 0 (0) |
Type 1 diabetes, n (%) | 1 (0.7) | 0 (0) |
Myocarditis, n (%) | 0 (0) | 1 (0.7) |
SOC = standard of care.
Source: Clinical Study Report P177V01MK3475.13
Critical Appraisal
Internal Validity
Patients in KEYNOTE-177 were randomized 1:1 centrally using an interactive voice response system and integrated web response system. The baseline patient characteristics were generally balanced. A steeper drop in survival among pembrolizumab patients was observed early in the trial. The clinical experts suggested that pembrolizumab’s onset of action may be slower than SOC, leading to this phenomenon; however, the time to response was equal in each arm. The experts suggested, alternatively, that there may be a subgroup of patients, yet to be identified, who may not benefit from pembrolizumab. While the trial was open-label, clinical outcomes such as PFS, ORR, and duration of response were assessed by blinded central independent reviewers per RECIST 1.1 and are unlikely subject to bias.
Patients in the SOC arm were permitted to cross over to the pembrolizumab arm, and patients in either arm were eligible to receive subsequent anticancer medication, which confounds the study’s ability to ascertain the size of the effect between pembrolizumab and SOC. Fifty-six patients (36.4%) originally randomized to SOC crossed over to the pembrolizumab arm. No patients randomized to the pembrolizumab arm crossed over to the SOC arm. An additional 44 patients (28.8%) and 44 patients (28.6%) in the pembrolizumab and SOC arms, respectively, subsequently received other anticancer therapy. Notably, use of anti-PD1/PDL1 therapies was higher among patients in the SOC arm, and use of chemotherapy, epidermal growth factor inhibitors, folic acid derivatives, and vascular endothelial growth factor inhibitors was higher among patients in the pembrolizumab arm. No additional information is provided regarding the criteria that triggered the use of subsequent anticancer medications. Also, discontinuation from the trial and treatment were higher in the SOC arm.
Crossing over or receiving subsequent anticancer therapy was considered a censoring event in the primary PFS analysis; however, crossing over or receiving subsequent anticancer medications may not be independent of pembrolizumab or SOC use, an assumption of this analysis. Thus, to supplement the ITT method in the primary analysis, PFS sensitivity analysis 1, presented in Appendix 3, was conducted; this analysis considered subsequent use of another anticancer medication or a crossover as a death or progression event instead of a censoring event. This analysis yielded an HR of 0.61 (95% CI, 0.48 to 0.79) and similar median PFS between the pembrolizumab arm (7.0 months; 95% CI, 4.2 to 12.4) and SOC arm (6.3 months; 95% CI, 4.6 to 8.2), but these are likely conservative estimates of the true median survival. As a corollary, PFS sensitivity analysis 2 was conducted. This analysis treated death or disease progression on the subsequent line of therapy as an event and, thus, did not account for crossovers or subsequent use of new anticancer medications. This analysis did not report a median survival for pembrolizumab patients but reported a similar treatment effect (HR = 0.63; 95% CI, 0.45 to 0.88) as the primary PFS analysis (HR = 0.60; 95% CI, 0.45 to 0.80). Thus, the similar HRs in each analysis suggest that the benefit observed in the primary PFS analysis is robust to crossovers and subsequent use of other anticancer medications.
In the primary OS analysis, crossing over to pembrolizumab or subsequent use of another anticancer therapy was not treated as a censoring event. A sensitivity analysis adjusting for those who were randomized to SOC and later crossed over to receive pembrolizumab or subsequently received another anti-PD1/PDL treatment (but not other treatments) yielded statistically non-significant results whether using the inverse probability of censoring weighting method (HR = 0.54; 95% CI, 0.27 to 1.39), the rank preserving structural failure time method (HR = 0.72; 95% CI, 0.47 to 1.11), or 2-stage analysis (HR = 0.89; 95% CI, 0.76 to 1.04). These point estimates vary from the primary analysis (HR = 0.77; 95% CI, 0.54 to 1.09), suggesting that crossover and subsequent use of another anti-PD1/PDL treatment introduced some degree of bias. Moreover, each sensitivity analysis possesses wide CIs, suggesting further uncertainty regarding the true effect size and significance testing was not applied. However, in each analysis, the point estimates favour pembrolizumab, and while the exact effect size and statistical significance is uncertain, the direction of the benefit is likely in favour of pembrolizumab.
The primary and secondary outcomes were analyzed using an ITT analysis. Appropriate statistical tests were used; however, the PHA was not met in the PFS analysis. To address the issue, the sponsor performed the RMST analysis at 24 months, which suggests a benefit in the use of pembrolizumab over SOC (13.7 months; 95% CI, 12.0 to 15.4 versus 10.8 months; 95% CI, 9.4 to 12.2); this difference (2.9 months; 95% CI, 0.7 to 5.1) was deemed clinically significant by the clinical experts. Further sensitivity analyses to address this issue using differing methods to create weighted HRs yielded HRs ranging from 0.32 (95% CI, 0.19 to 0.54) to 0.81 (95% CI, 0.57 to 1.16). Piecemeal HRs were also reported, with an estimate of 1.88 before 3 months and 0.22 beyond 3 months; unfortunately, 95% CIs were not reported in this analysis. These analyses are available in Appendix 3 and, in general, suggest a benefit in the use of pembrolizumab on PFS. Finally, it is unclear if the PHA was met in the OS analysis.
The data presented constitute a final analysis of PFS but only an interim analysis for OS. The trial for the final analysis of OS was intended to be conducted when 190 deaths occurred; however, only 125 deaths are presented, further complicating the interpretation of OS. The independent data-monitoring committee reviewed the issue and recommended the final analysis still be conducted at 190 events, or 12 months from this second interim analysis, which should be reached in February or March 2021.
External Validity
The chosen SOC regimens generally align with the recommended guidelines in Canada and contain the most commonly used regimens, but some regimens were not studied in KEYNOTE-177, such as FOLFOX with panitumumab, FOLFIRI with panitumumab, FOLFOXIRI with or without bevacizumab, CAPOX with or without bevacizumab, capecitabine with or without bevacizumab, 5-fluorouracil and leucovorin with or without bevacizumab, and single-agent irinotecan. Cetuximab is not funded in Canada in the first-line setting, and panitumumab is a reasonable substitution for those with RAS wild-type disease and distal primary tumours, which compose about 40% of this patient population. Regardless, the clinical experts consulted suggest the KEYNOTE-177 results are sufficiently compelling to conclude that pembrolizumab is likely beneficial over alternative comparators not studied. No unreasonable co-interventions were identified. Study participants were representative of the population in question, and the inclusion and exclusion criteria likely did not intentionally exclude any populations of interest, except for those with an ECOG PS of 2 or higher who may have a more severe disease. The outcomes analyzed were of interest to patients and clinicians and were studied for an appropriate duration. As discussed previously, some patients crossed over to the opposite arm or received subsequent anticancer medications. Sensitivity analyses were provided to investigate the confounding effect, but clinicians should be aware that residual confounding may remain that could limit generalizability to patients who are not subject to similar crossover conditions or are unlikely to receive similar anticancer medications, if any. The clinical experts consulted also suggest that a longer follow-up and more information regarding the number of patients who required re-treatment would be helpful. Table 19 summarizes the generalizability of the evidence.
Table 19: Assessment of Generalizability of Evidence for Pembrolizumab
Domain | Factor | Evidence | CADTH assessment of generalizability |
|---|---|---|---|
Population | Adults with MSI-H/dMMR stage IV colorectal cancer | Trial inclusion and exclusion criteria | The inclusion and exclusion criteria seemed to recruit the appropriate patient population but excluded those with an ECOG PS of 2 or greater. |
Intervention | Pembrolizumab | Trial protocol | The medication is available in Canada for other indications. |
Comparator | FOLFOX or FOLFIRI alone or with either cetuximab or bevacizumab | Trial protocol | Most of the regimens are recommended and/or reimbursed, although some SOC regimens that are used in practice were missing (capecitabine, CAPEOX, FOLFOXIRI, fluorouracil-leucovorin, and irinotecan) and some may not be relevant based on lack of reimbursement (e.g., cetuximab). |
Outcomes | PFS, OS, ORR | Trial protocol | These are relevant to patients and clinicians. |
Setting | Outpatient cancer care | Trial sites | The listed trial sites are similar to the Canadian sites that would typically treat this disease. |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; SOC = standard of care.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
A focused literature search for NMAs dealing with colorectal cancer was run in MEDLINE All (1946–) on January 8, 2021. No limits were applied to the search. Forty-eight citations were identified, but no indirect evidence met the inclusion criteria of the CADTH review protocol, as none included pembrolizumab as a treatment of interest.
The objective of this section is to summarize and critically appraise the methods and findings of the sponsor-submitted review of the literature and NMA comparing pembrolizumab with comparators relevant for the treatment of MSI-H/dMMR mCRC.14
Description of Indirect Comparisons
The sponsor-submitted ITC first conducted a systematic literature review (SLR) to evaluate the comparative efficacy and safety of pembrolizumab versus competing interventions for the treatment of patients with MSI-H/dMMR mCRC, following which it was of interest to conduct an NMA. The feasibility of performing an NMA regarding OS, PFS, ORR, and safety outcomes for pembrolizumab, CAPOX, panitumumab plus FOLFOX, and SOC (which consisted of FOLFOX or FOLFIRI with or without cetuximab, as administered in KEYNOTE-177) was assessed, and results were synthesized by means of Bayesian NMA.14
Table 20 summarizes the study selection criteria and method for the SLR in the sponsor-submitted ITC and NMA. From the 13 studies identified, studies were subselected for inclusion in the feasibility assessment based on network geometry constraints and availability of outcome data. The selection criteria specific to the ITC and NMA were not provided.
Table 20: Study Selection Criteria and Method for Systematic Literature Review
Criteria | Sponsor-submitted NMA |
|---|---|
Population | Previously untreated adult patients with unresectable or metastatic colorectal cancer, MSI-H or dMMR colorectal cancer |
Intervention | Pembrolizumab 200 mg q.3.w. |
Comparator | (m)FOLFOX or FOLFIRI ± cetuximab, mFOLFOX + panitumumab, capecitabine + oxaliplatin, SOCa |
Outcome | OS, PFS, safety |
Study design | RCTs |
Publication characteristics | Publication in English |
Exclusion criteria | mFOLFOX/FOLFIRI to mFOLFOX/FOLFIRI + cetuximab treatments with no other UK-relevant comparator Patients who were assigned to bevacizumab combinations, where these data were available Single-arm clinical trials |
Databases searched | Embase, MEDLINE, CENTRAL |
Selection process | NR |
Data extraction process | NR |
Quality assessment | NR |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; NMA = network meta-analysis; NR = not reported; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; RCT = randomized controlled trial; SOC = standard of care.
aThe 6 comparator regimens of KEYNOTE-177 consist of FOLFOX or FOLFIRI with or without cetuximab and FOLFOX or FOLFIRI with bevacizumab, and these were combined into a single SOC arm. For the purposes of the UK NMA, the primary analysis excluded patients assigned to bevacizumab combinations before randomization, as bevacizumab is not a relevant comparator in the UK context.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Methods of Sponsor-Submitted NMA
Objectives
The objective of the sponsor-submitted report was to conduct a feasibility assessment via an SLR and, if possible, conduct an NMA evaluating the relative efficacy and safety of pembrolizumab versus competing interventions relevant to the UK perspective for the treatment of MSI-H/dMMR mCRC patients.14
Study Selection Methods
An SLR was conducted to identify relevant clinical evidence on pembrolizumab and competing interventions. Study selection was conducted in accordance with the predefined inclusion and exclusion criteria and summarized in the population, intervention, comparator, outcome, and study (PICOS) framework in Table 21. Eligible studies included randomized and nonrandomized clinical trials in previously untreated adult patients with unresectable or metastatic MSI-H or dMMR CRC, as well as the general mCRC population. Treatments of interest included FOLFOX or mFOLFOX6 (plus cetuximab or panitumumab), FOLFIRI (plus cetuximab or panitumumab), and capecitabine plus oxaliplatin. For the SLR and NMA, patients taking bevacizumab combinations before randomization were excluded, as bevacizumab is not a relevant comparator in the UK. Key outcomes of interest for the SLR included efficacy (OS, PFS, duration of response, time to second objective disease progression, ORR, and surgical conversion rate), safety (AEs, DAEs, SAEs), and HRQoL (patient-reported outcomes, such EQ-5D-3L, EORTC QLQ-C30, or EORTC QLQ-CR29). Outcomes assessed in the NMA included OS, PFS, ORR, and safety (DAEs, SAEs, and grade ≥ 3 and serious treatment-related AEs).14
Citations were identified through searches of Embase, MEDLINE, and CENTRAL databases. From the studies that met the inclusion criteria in the SLR, studies were reselected for inclusion in the NMA based on network geometry constraints and availability of outcome data.14 Information regarding key steps of study selection for screening and data extraction and for quality assessment, including how many reviewers were involved and how differences of opinion were settled, was not provided for the SLR or the NMA. No list of studies excluded at the full-text stage was provided, and therefore it was not possible to assess whether potentially eligible studies may have been excluded.
Table 21: PICOS Criteria of the Sponsor-Submitted NMA to Identify Trials for the SLR
Criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population | Previously untreated adult patients with unresectable or metastatic MSI-H or dMMR CRC Previously untreated adult patients with unresectable or metastatic CRCa | Patients who received prior systemic therapy for stage IV CRC; patients may have received prior adjuvant chemotherapy for CRC if completed at least 6 months before randomization Patients under 18 years old |
Interventions | UK intervention subset:
| — |
Comparators | Placebo or BSC Any intervention of interest Any treatment that facilitates an indirect comparison | — |
Outcomes | OS PFS DOR Surgical conversion rate PFS2 ORR Drug-related AE ≥ 10% Grade 3 to 5 AE (all, drug related) DAE SAE PRO (e.g., EQ-5D, EORTC QLQ-C30, EORTC QLQ-CR29) | — |
Time | No time restriction | — |
Study design | RCTs Controlled clinical trials Nonrandomized clinical trials, including single-arm prospective interventional trials | Prospective and retrospective cohort studies Case-control studies Cross-sectional studies Case reports and case series |
Other | Only studies published in English | — |
AE = adverse event; BSC = best supportive care; CRC = colorectal cancer; DAE = discontinuation due to adverse events; dMMR = mismatch repair deficient; DOR = duration of response; EORTC = European Organisation for Research and Treatment of Cancer; EQ-5D = EuroQol 5-Dimensions questionnaire; MSI-H = microsatellite instability-high; NMA = network meta-analysis; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PFS2 = time to second objective disease progression; PICOS = population, intervention, comparator, outcome, and study; PRO = patient-reported outcome; QLQ-C30 = Quality of Life Questionnaire Core 30; QLQ-CR29 = Quality of Life Questionnaire Colorectal Cancer Module; RCT = randomized controlled trial; SAE = serious adverse event; SLR = systematic literature review.
aOnly RCTs of interest for the metastatic CRC population that is unselected for MSI-H/dMMR.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Feasibility Assessment
An assessment was conducted to determine the feasibility and appropriateness of performing an ITC and NMA with the eligible trials, which included (1) determination of whether the RCT evidence for the interventions of interest form 1 evidence network for each population and outcome of interest and (2) assessment of the distribution of treatment, outcomes, studies, and patient characteristics that may affect treatment effects across direct comparisons of the evidence networks.14
ITC Analysis Methods
The NMA methods are briefly summarized in Table 22. The analyses were conducted within a Bayesian framework. The outcomes included in the NMA included OS, PFS, ORR, and safety. Both fixed-effects and random-effects models were considered for the analysis of the OS, PFS, ORR, and safety outcomes. Random-effects models were fitted within the OS outcome for all networks, as connections were described by more than 1 trial; however, this was not the case for all other outcomes. For the remaining outcomes, because almost all connections in the network were only described by a single trial, stable estimates of between-study heterogeneity could not be obtained, and results of random-effects analyses were not meaningful. Therefore, only the results of fixed-effects analyses are shown for PFS, ORR, and safety outcomes. For all outcomes analyzed, no closed loops were present in the evidence base, which prevented the evaluation of consistency.14
For binary outcomes, ORR, DAEs, AEs of grade 3 or higher, treatment-related AEs of grade 3 or higher and serious treatment-related AEs, the NMA was performed (based on the proportion of patients experiencing the event of interest) using a regression model with a binomial likelihood and logit link. The NMA of reported HRs in terms of OS and PFS, assuming proportional hazards between treatments, was performed using a regression model with a contrast-based normal likelihood for the log HR of each trial in the network. Additionally, a time-varying HR NMA in terms of OS and PFS was carried out where feasible. Normal non-informative prior distributions for the parameters were used with a mean of 0 and a variance of 10,000. Relative treatment effects were expressed as odds ratios (ORs). No sensitivity or subgroup analyses were conducted to assess the impact of the priors.14
The model introduced by Jansen et al., was used for the NMA of OS and PFS.26,27 Multiple survival distributions for OS and PFS were considered and included the following: Weibull, Gompertz, and second-order fractional polynomials (FPs), including p1 = 0 or 1 and p2 = –0 or 1. For the relative treatment effects in the second-order FP framework, we assessed models that assumed (1) treatment only has an impact on 2 of the 3 parameters describing the hazard function over time (i.e., 1 scale and 1 shape parameter), and (2) treatment has an impact on all 3 parameters describing the hazard function over time (i.e., 1 scale and 2 shape parameters). A test of proportionality suggested there were violations of the PHA for several trials (TREE-1, KEYNOTE-177).14
The deviance information criterion (DIC) was used to compare the goodness-of-fit of competing survival models and to inform model selection. A difference in DIC between models of approximately 5 points was considered clinically meaningful. The plausibility of the obtained HR was also considered. The parameters of the different models were estimated using a Markov chain Monte Carlo method implemented in the OpenBUGS software package. A first series of iterations from the OpenBUGS sampler were discarded as “burn-in,” and the inferences were based on additional iterations using 2 chains.14
The results of the NMA were presented with estimates for treatment effects of each intervention relative to the reference treatment. The posterior distributions of estimated relative treatment effects are summarized by the median and 95% CrIs, which were constructed from the 2.5th and 97.5th percentiles of the posterior distributions. The results of the NMA are presented in terms of cross-tables with relative treatment effect estimates between all interventions of interest, along with 95% CrIs for all outcomes, except for time-to-event outcomes based on Kaplan–Meier outcomes. For time-to-event outcomes based on reported HRs (PFS and OS), the results are also presented as HRs. The HR with the shortest follow-up was used as reported in primary publications, where possible. For time-to-event outcomes based on Kaplan-Meier curves, results are presented in terms of HRs up to 40 months. In cases where no HR was reported but the trial reported Kaplan-Meier curves, HRs were derived using the Guyot algorithm.28
Table 22: ITC Analysis Methods
Method | Sponsor-submitted NMA |
|---|---|
ITC methods | Bayesian NMA and ITC |
Priors | Normal non-informative prior distributions were used for all parameters (mean = 0; variance = 10,000) |
Assessment of model fit | DIC was used to compare the goodness-of-fit of competing survival models |
Assessment of consistency | No closed loops preventing the assessment of consistency |
Assessment of convergence | NR |
Outcomes | OS, PFS, ORR, AEs |
Follow-up time points | Time-varying NMA: 4 to 40 months |
Construction of nodes | As breakdown of SOC regimens was available for the KEYNOTE-177 trial, networks considered the regimen of mFOLFOX or FOLFIRI ± cetuximab to be a single SOC node |
Sensitivity analyses | The ITT population of each study was used as sensitivity analysis, which included bevacizumab as a comparator |
Subgroup analysis | NR |
Methods for pairwise meta-analysis | NR |
AE = adverse event; DIC = deviance information criterion; ITC = indirect treatment comparison; ITT = intention to treat; NMA = network meta-analysis; NR = not reported; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; SOC = standard of care.
Source: Sponsor-submitted ITC and NMA.14
Assumptions
Comparisons of study design, inclusion and exclusion criteria, and patient characteristics were used to assess transitivity, homogeneity, and consistency; however, no information on this process was provided. The authors noted the following assumptions to construct the network14:
Networks constructed with mFOLFOX or FOLFIRI with or without cetuximab regimens being considered a single SOC node. The authors noted that 6 trials comparing mFOLFOX or FOLFIRI to mFOLFOX or FOLFIRI with or without cetuximab — treatments with no other UK-relevant comparator — were excluded from the analysis as they did not contribute any indirect evidence to the desired comparisons.29-34 As these regimens were considered a single SOC node, the studies were considered single-arm studies in the context of the network. One additional trial was excluded as it was single arm,35 and 1 was excluded as it only included 4 MSI-H/dMMR patients in a single trial arm.36
Applicability of treatment effect estimates in mCRC patients to MSI-H/dMMR patients. To construct a network and make requested comparisons to SOC, the authors assumed that relative treatment effects do not differ between MSI-H/dMMR patients and mCRC patients.
Equivalence of FOLFOX to FOLFIRI and equivalence of different FOLFOX regimens. The authors noted that several studies have shown the similarity between FOLFOX and FOLFIRI as well as different FOLFOX regimens.
Lack of effect of adding cetuximab to FOLFOX or FOLFIRI. Due to data availability, the authors noted that results for KEYNOTE-177 were not available for patients just receiving FOLFOX or FOLFIRI; these results were combined with the patients receiving FOLFOX or FOLFIRI with or without cetuximab to form the SOC arm. In 1 study, there was evidence of advantage in PFS in unselected and KRAS wild-type patients receiving cetuximab.30 In the other study, there was no difference in response rate or PFS between patients receiving cetuximab plus FOLFOX4 versus FOLFOX4 alone, but an advantage in KRAS wild-type patients.32 Therefore, caution should be taken in interpreting results that include cetuximab in the SOC arm, particularly for KRAS wild-type patients. Results for OS may be less biased than those involving response or PFS.
Lack of effect modification in KRAS patients for interventions other than panitumumab. Authors noted that a systematic review found that while KRAS was an effect modifier for patients receiving anti–epidermal growth factor receptor treatment, there was no evidence of effect modification on chemotherapy regimens. Within KEYNOTE-177, KRAS wild-type patients on pembrolizumab had significantly improved PFS versus SOC (HR = 0.44; 95% CI, 0.29 to 0.67), while KRAS mutant patients on pembrolizumab showed evidence of worse PFS than those on SOC (HR = 1.19; 95% CI, 0.68 to 2.07). This indicates that conclusions concerning KRAS patients should be regarded with caution.
Results of Sponsor-Submitted NMA
Summary of Included Studies
Thirty-one publications from 13 unique studies were identified from the SLR and evaluated in a feasibility assessment to determine the possibility of conducting an NMA in the study population. No list of studies excluded at the full-text stage was provided, and therefore it was not possible to assess whether potentially eligible studies may have been excluded. Five studies were subselected for inclusion in the NMA based on network geometry and availability of outcome data: KEYNOTE-177, PRIME, NO16966, Porschen 2007, and TREE-1.8,37-40 Key study characteristics and inclusion criteria for these studies are summarized in Table 23.
All studies were phase II or III, open-label RCTs, except for the NO16966 study, which was double blind; masking was not reported for the Porschen 2007 study. Three studies were multinational, while the Porschen 2007 study was conducted in Germany and Austria, and the TREE-1 study was conducted in the US. All trials enrolled adult patients (≥ 18 years). Porschen 2007 and PRIME allowed patients with an ECOG PS of 0 to 2; the remaining trials allowed only patients with an ECOG PS of 0 or 1. No trials allowed prior chemotherapy. The median duration of follow-up differed across trials, ranging from 15 months in TREE-1 to 28.4 months in KEYNOTE-177; it was not reported in the NO16966 study. Additionally, KEYNOTE-177 only enrolled patients who had MSI-H or dMMR mCRC, while PRIME only enrolled patients with KRAS wild-type mCRC. The 3 remaining studies enrolled mCRC patients without selecting for any specified biomarkers, and so the assumption of homogeneity may not hold, given that the treatment effect may vary across different mCRC patients, particularly between subgroups of patients with MSI-H or dMMR versus those with general mCRC. Moreover, the included studies spanned more than 18 years during which the treatment paradigms evolved rapidly in the management of cancer patients.
Some key differences between the KEYNOTE-177 trial and other included studies had the potential to bias the results. The KEYNOTE-177 study was the only included study that allowed crossover from the SOC arm to receive pembrolizumab after confirmed disease progression. The authors noted that this may introduce bias to the NMA and therefore incorporated 3 statistical methods to adjust for crossover in KEYNOTE-177. In the first, a 2-stage parametric survival model that accounted for important covariates was developed to estimate the effect of switching in the control arm. The adjusted survival times were analyzed with a proportional hazards model in the second stage. The second method was the inverse probability of censoring weighting model, which addressed treatment switching by introducing artificial censoring at the time of switch for each patient and by weighting the observations before switching. Observations after switching treatment were ignored (weight = 0), while the times during which a patient is not at risk of switching were unweighted (weight = 1). The third statistical method was the rank preserving structural failure time method, which estimates the survival time gained or lost by receiving active treatment. The model assumes that active therapy is acting on longevity by multiplying survival by a given factor once a patient starts receiving the treatment. In the case of KEYNOTE-177, since only patients in the SOC arm crossed over to active treatment, the model would assume that the crossover patients would present a similar effect on OS had they continued in the SOC arm, by comparing to those patients who remained on the SOC with similar baseline and disease characteristics. Other studies either did not allow crossover or did not report it.
All included trials had an SOC arm. However, there was substantial heterogeneity in the regimens of SOC across trials, as chemotherapy regimens were made up of different combinations and doses of FOLFOX or FOLFIRI, with or without cetuximab. FOLFOX was administered in all included trials. Administration of FOLFOX varied across the trials with respect to dose, cycle, and treatment duration. KEYNOTE-177 was the only trial to include FOLFIRI regimens, and the authors noted that while the inclusion of FOLFIRI is unlikely to introduce substantial bias to the analysis, the addition of cetuximab in the SOC arm would likely reduce the estimated treatment effect of pembrolizumab compared to FOLFOX or FOLFIRI alone. Doses of oxaliplatin varied from 50 mg/m2 to 85 mg/m2; leucovorin doses varied from 20 mg/m2 to 500 mg/m2, and 5-fluorouracil doses varied from 400 mg/m2 to 2,000 mg/m2. The KEYNOTE-177 trial was the only included study that administered the FOLFIRI and pembrolizumab regimens. Pembrolizumab monotherapy was administered at a dose of 200 mg on day 1 of each 21-day cycle for up to 35 cycles. The CAPOX regimen was administered in 3 trials (NO16966, Porschen 2007, and TREE-1), and panitumumab was only administered in the PRIME trial at a dose of 6 mg/kg until disease progression.
Both the KEYNOTE-177 trial and the NO16966 study evaluated bevacizumab in the SOC arms at a dose of 5 mg/kg and 8 mg/kg, respectively. These treatment arms, inclusive of bevacizumab, were included for completeness but were not of interest to the base case of the UK NMA. The authors noted that the use of subgroup data causes smaller sample sizes than the use of the ITT population, which may reduce precision, and that the use of the sample sizes that do not include bevacizumab from KEYNOTE-177 would result in more uncertainty and wider CrIs for comparisons involving pembrolizumab, which limits the ability to draw statistically meaningful conclusions. Bevacizumab is included in an alternate analysis that includes the full ITT population of KEYNOTE-177.
Table 23: Study Characteristics and Inclusion Criteria of Included MSI-H/dMMR and mCRC Trials
Trial | Study design | Phase | Region | Study population | Treatment | Study start date | Study completion date | Masking | ECOG PS | Median duration of follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
KEYNOTE-177 | RCT | III | Multinational | Adult (≥ 18 years) with dMMR or MSI-H stage IV CRC | Pembrolizumab mFOLFOX6 or FOLFIRI, or mFOLFOX6 + bevacizumab, or mFOLFOX6 + cetuximab, or FOLFIRI + bevacizumab, or FOLFIRI + cetuximab | November 2015 | December 2021 | Open label | 0 to 1 | 28.4 months (pembrolizumab) 27.2 months (SOC) |
NO16966 | RCT | III | Multinational | Adult (≥ 18 years) with mCRC | CAPOX FOLFOX4 CAPOX + placebo CAPOX + bevacizumab FOLFOX4 + placebo FOLFOX4 + bevacizumab | July 2003 | April 2009 | Double (participant and investigator) | 0 to 1 | NR |
Porschen 2007 | RCT | III | Germany and Austria | Adult (≥ 18 years) with mCRC | CAPOX FOLFOX | — | — | — | 0 to 2 | 17.3 months |
PRIME | RCT | III | Multinational | Adult (≥ 18 years) mCRC with KRAS wt | Panitumumab + FOLFOX4 FOLFOX4 | August 2006 | March 2013 | Open label | 0 to 2 | 89 weeks |
TREE-1 | RCT | III | US | Adult (≥ 18 years) with mCRC | mFOLFOX6 bFOLFOX CAPOX | November 2002 | — | Open label | 0 to 1 | 15 months |
CRC = colorectal cancer; dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; NR = not reported; RCT = randomized controlled trial; SOC = standard of care; wt = wild type.
Source: Sponsor-submitted ITC and NMA.14
Table 24 summarizes the reported primary outcomes and definitions for the included studies. KEYNOTE-177 reported progression measured by RECIST 1.1, while NO16966 and PRIME reported RECIST. KEYNOTE-177 used version 4.0 of Common Terminology Criteria for Adverse Events to measure AEs, while NO16966 and PRIME used version 3.0. Porschen 2007 and TREE-1 did not report a measure of disease progression or a measure for reporting of AEs.
Table 24: Outcome Definitions for Studies Included in the Feasibility Assessment
Trial | Primary outcome | Response definitions | Safety outcome measure | |||
|---|---|---|---|---|---|---|
Outcome | Measure | OS | PFS | ORR | ||
KEYNOTE-177 | PFS and OS | RECIST 1.1 | Date of randomization to date of death | Time from randomization to disease progression or death due to any cause | — | NCI CTCAE version 4.0 |
NO16966 | PFS | RECIST | Date of randomization to date of death | Time from randomization to disease progression or death due to any cause | Best response recorded from start of treatment until disease progression or recurrence | NCI CTCAE version 3.0 |
Porschen 2007 | PFS | NR | — | Time from randomization to disease progression or death due to any cause | — | — |
PRIME | PFS | RECIST | Date of randomization to date of death | Time from randomization to disease progression measured with RECIST or death due to any cause | Defined as the incidence of either a confirmed CR or PR while on the first-line treatment, as determined by a BICR and confirmed no less than 4 weeks after the criteria for response are first met | NCI CTCAE version 3.0 |
TREE-1 | Overall incidence of grade 3 or 4 AEs | NR | — | — | — | — |
AE = adverse event; BICR = blinded independent review committee; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; NCI = National Cancer Institute; NR = not reported; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Baseline characteristics of the included studies are summarized in Table 25. The KEYNOTE-177 study only enrolled MSI-H/dMMR mCRC patients, while the PRIME study enrolled mCRC patients with wild-type KRAS mutations. All other studies included mCRC patients, with no specific biomarkers. Overall, baseline characteristics were well balanced, as the median age of patients in studies included in the NMA and ITC ranged from 60 years to 66 years and the proportion of males ranged from 46% to 67%. Patients with an ECOG PS of 0 ranged from 49% (KEYNOTE-177) to 61% (TREE-1) and patients with an ECOG PS of 1 ranged from 39% (TREE-1) to 51% (KEYNOTE-177). Only Porschen 2007 enrolled patients with an ECOG PS of 2 (9%).
No information on the quality assessment of the studies included in the SLR was reported.
Table 25: Baseline Characteristics of Randomized Controlled Trials Included in the Feasibility Assessment
Trial | Treatment | N | Age, median (range) | Male, n (%) | ECOG PS = 0, n (%) | ECOG PS = 1, n (%) | ECOG PS = 2, n (%) | Rectum site, n (%) | Colon site, n (%) | Liver metastasis, n (%) | Lung metastasis, n (%) | Other metastasis, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
KEYNOTE-177 | Pembro | 153 | 63 (24 to 93) | 71 (46.4) | 75 (49) | 78 (51) | — | — | — | — | — | 67 (43.8) |
SOC | 154 | 62.5 (26 to 90) | 82 (53.2) | 84 (54.5) | 70 (45.5) | — | — | — | — | — | 81 (52.6) | |
NO16966 | CAPOX | 317 | 61 (24 to 84) | 194 (61.2) | 160 (50.5) | 157 (49.5) | 0 (0) | 83 (26) | 204 (64) | — | — | — |
FOLFOX4 | 317 | 62 (24 to 83) | 204 (64.4) | 163 (51.4) | 154 (48.6) | 0 (0) | 100 (32) | 200 (63) | — | — | — | |
CAPOX + placebo | 350 | 61 (18 to 83) | 205 (58.6) | 207 (59.1) | 143 (40.9) | 0 (0) | 87 (25) | 233 (67) | — | — | — | |
FOLFOX4 + placebo | 351 | 60 (26 to 83) | 189 (53.8) | 211 (60.1) | 138 (39.3) | 0 (0) | 94 (27) | 232 (66) | — | — | — | |
Porschen 2007 | FOLFOX | 233 | 64 (34 to 86) | 146 (62.7) | — | — | 17 (7.3) | — | — | — | — | — |
CAPOX | 241 | 66 (32 to 81) | 150 (62.2) | — | — | 22 (9.1) | — | — | — | — | — | |
PRIME | Pan + FOLFOX4 | 325 | 62 (27 to 85) | 217 (66.8) | — | — | — | 111 (34) | 214 (66) | 60 (18.5) | — | 40 (12.3) |
FOLFOX4 | 331 | 61 (24 to 82) | 204 (61.6) | — | — | — | 115 (35) | 216 (65) | 56 (16.9) | — | 47 (14.2) | |
TREE-1 | mFOLFOX6 | 49 | 62 (35 to 79) | 28 (57) | 30 (61) | 19 (39) | — | — | — | 38 (76) | 23 (47) | 27 (55) |
bFOLFOX | 50 | 62 (31 to 84) | 31 (62) | 29 (58) | 21 (42) | — | — | — | 38 (76) | 25 (50) | 34 (68) | |
CAPOX | 48 | 62.5 (32 to 84) | 31 (65) | 25 (52) | 23 (48) | — | — | — | 31 (65) | 24 (50) | 31 (65) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Table 26: Assessment of Homogeneity for Sponsor-Submitted ITC and NMA
Item | Description and handling of potential effect modifiers |
|---|---|
Disease severity | The sponsor-submitted ITC and NMA analyzed the mCRC population as a whole and did not conduct analyses separately, given that 3 trials enrolled mCRC patients, 1 enrolled MSI-H/dMMR mCRC patients, and 1 enrolled mCRC patients with wild-type KRAS mutation. |
Treatment history | No trials allowed for prior chemotherapy. No analyses were conducted based on prior treatments received. |
Clinical trial eligibility criteria | Aside from the minor differences in the populations based on biomarkers, the eligibility criteria of the trials were similar. |
Dosing of comparators | Doses varied across the studies, and analyses by dose were not incorporated into networks. |
Definitions of end points | Definitions and reporting of end points were consistent among trials, particularly for OS, PFS, and safety outcomes. |
Timing of end point evaluation or trial duration | The median duration of follow-up for key outcomes differed across trials, ranging from 15 months in TREE-1 to 28.4 months in KEYNOTE-177, and was not reported in the NO16966 study. |
Withdrawal frequency | Not reported. |
Clinical trial setting | Most trials were multi-centre and multinational. |
Study design | Similar study design across included studies (open-label RCTs). |
dMMR = mismatch repair deficient; ITC = indirect treatment comparison; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial.
Source: Sponsor-submitted ITC and NMA.14
Results
The overall network for the 5 trials that were included in the ITC and NMA — based on the assumptions outlined in Table 26 — is shown in Figure 6, irrespective of outcomes or dose. In KEYNOTE-177, the 6 comparator regimens were combined into a single SOC arm to connect the network. In the primary analysis of the NMA, patients assigned to the bevacizumab combinations before randomization in KEYNOTE-177 were excluded, as bevacizumab was not a relevant comparator in the UK context. No breakdown of SOC regimens was available for KEYNOTE-177, and networks were constructed with mFOLFOX or FOLFIRI with or without cetuximab considered a single SOC node. Three trials compared CAPOX to SOC of (m)FOLFOX or FOLFIRI with or without cetuximab (NO16966, Porschen 2007, and TREE-1),38-40 and 1 trial compared (m)FOLFOX with panitumumab to SOC of (m)FOLFOX or FOLFIRI with or without cetuximab (PRIME).37
The base-case NMA consisted of all included studies and used a subgroup of patients from the KEYNOTE-177 trial who did not receive treatment with bevacizumab (termed “ITT-Bev”). The base-case ITT-Bev population was only used for NMAs of OS and PFS. The scenario analyses of the NMA included all ITT populations from each trial and were conducted for all outcomes (OS, PFS, ORR, safety). Additional scenario analyses using crossover-adjusted results were conducted for OS using both populations.
As previously mentioned, no closed loops were shown in any network, and random-effects models were only conducted within the OS outcome, as situations where network connections were described by more than 1 trial existed.
Figure 6: Network of Evidence for All Included Randomized Controlled Trials in Feasibility Assessment: All Outcomes
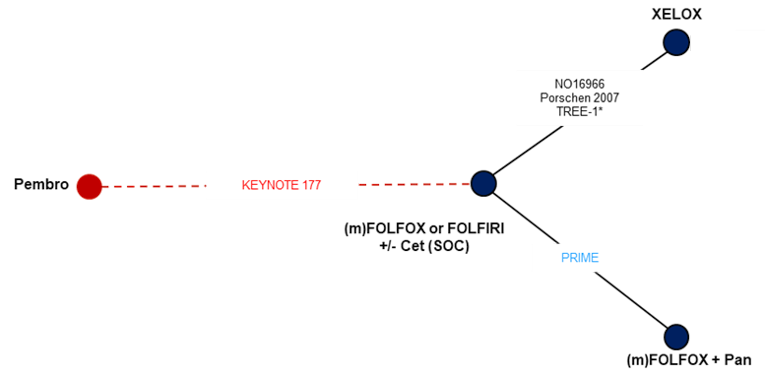
Cet = cetuximab; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Overall Survival
The network for OS is the same as that presented for all included trials in the NMA, shown in Figure 6. All 5 RCTs were included in the base-case OS analysis, and 4 interventions (pembrolizumab, CAPOX, mFOLFOX plus panitumumab, and SOC) were evaluated. Network meta-analyses for the base-case analyses were deemed feasible for OS since KEYNOTE-177 reported subgroup data (ITT-Bev). Constant and time-varying HR analyses were both performed because some of the Kaplan-Meier curves crossed, which indicates that the PHA may have been violated.14
The pairwise results of the fixed-effects NMA are shown for each trial in Table 27 for both the base-case and scenario analysis. The results showed that pembrolizumab was no different from SOC or any other intervention of interest with regard to OS in the ITT-Bev or ITT populations. Of the included interventions, only panitumumab plus FOLFOX was favoured over SOC (HR = 0.83; 95% CrI, 0.70 to 0.98, for both ITT-Bev and ITT populations). This combination also showed statistical benefit over CAPOX (HR = 0.80; 95% CrI, 0.66 to 0.98, for both ITT-Bev and ITT populations).14 In the random-effects model, no treatment was favoured over another (Table 28).
Table 27: Overall Survival Estimated From Fixed-Effects NMA — Base-Case (ITT-Bev) and ITT Populations
Intervention 2 | Intervention 1, HR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
ITT-Bev population | ||||
SOC | — | 0.97 (0.87 to 1.08) | 1.20 (1.02 to 1.42) | 1.35 (0.77 to 2.37) |
CAPOX | 1.04 (0.93 to 1.16) | — | 1.25 (1.02 to 1.53) | 1.40 (0.79 to 2.46) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.12 (0.63 to 2.02) |
Pembrolizumab | 0.74 (0.42 to 1.29) | 0.71 (0.41 to 1.26) | 0.89 (0.50 to 1.60) | — |
ITT population | ||||
SOC | — | 0.96 (0.87 to 1.08) | 1.21 (1.02 to 1.43) | 1.30 (0.91 to 1.83) |
CAPOX | 1.04 (0.93 to 1.15) | — | 1.25 (1.02 to 1.53) | 1.35 (0.93 to 1.93) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.08 (0.73 to 1.58) |
Pembrolizumab | 0.77 (0.55 to 1.10) | 0.74 (0.52 to 1.08) | 0.93 (0.63 to 1.37) | — |
Bev = bevacizumab; CrI = credible interval; HR = hazard ratio; ITT = intention to treat; NMA = network meta-analysis; OS = overall survival; Pan = panitumumab; SOC = standard of care.
Note: Deviance information criterion = 7.45; deviance = 4.46.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Table 28: Overall Survival Estimated From Random-Effects NMA — Base-Case (ITT-Bev) and ITT Populations
Intervention 2 | Intervention 1, HR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
ITT-Bev population | ||||
SOC | — | 0.98 (0.39 to 2.64) | 1.21 (0.23 to 6.32) | 1.36 (0.26 to 7.20) |
CAPOX | 1.02 (0.38 to 2.58) | — | 1.23 (0.18 to 7.71) | 1.38 (0.20 to 8.76) |
Pan + FOLFOX | 0.83 (0.16 to 4.30) | 0.81 (0.13 to 5.51) | — | 1.12 (0.11 to 11.10) |
Pembrolizumab | 0.73 (0.14 to 3.79) | 0.73 (0.11 to 4.91) | 0.89 (0.09 to 9.16) | — |
ITT population | ||||
SOC | — | 0.98 (0.45 to 2.32) | 1.20 (0.29 to 5.06) | 1.31 (0.30 to 5.22) |
CAPOX | 1.02 (0.43 to 2.22) | — | 1.23 (0.24 to 5.94) | 1.33 (0.23 to 6.18) |
Pan + FOLFOX | 0.83 (0.20 to 3.44) | 0.81 (0.17 to 4.21) | — | 1.09 (0.14 to 7.47) |
Pembrolizumab | 0.77 (0.19 to 3.32) | 0.75 (0.16 to 4.27) | 0.92 (0.13 to 7.31) | — |
Bev = bevacizumab; CrI = credible interval; HR = hazard ratio; ITT = intention to treat; NMA = network meta-analysis; OS = overall survival; Pan = panitumumab; SOC = standard of care.
Note: ITT-Bev: deviance information criterion = 8.81; deviance = 4.34; standard deviation = 0.47. ITT: deviance information criterion = 8.81; deviance = 4.34; standard deviation = 0.42.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Results of the time-varying analysis are summarized in Table 29, where HRs at selected time points are presented. In both the fixed- and random-effects analyses, the best-fitting model was the second-order FP model, with p1 = 0, p2 = 1 (fixed effects: ITT-Bev DIC = 1,861.18 and ITT DIC = 1,938.24; random effects: ITT-Bev DIC = 1,862.36 and ITT DIC = 1,939.14). Point estimates generally decreased over time for all interventions.
In the fixed-effects NMA of the ITT-Bev population, pembrolizumab alone and panitumumab plus FOLFOX showed no benefit compared to SOC at any time point. CAPOX was favoured over SOC at 4 months and all time points at 28 months and beyond.
In the ITT population, results for CAPOX versus SOC were the same as in the ITT-Bev group, with CAPOX being favoured at the 4-month and the 28-month and beyond time points. Pembrolizumab was favoured over SOC at 12 months and onward until 40 months. Panitumumab plus FOLFOX was no different than SOC at any time point.
No treatments were favoured over SOC in the random-effects analysis for the ITT-Bev or ITT groups.
Table 29: Time-Varying Overall Survival From Fixed- and Random-Effects NMA
Month | Intervention vs. SOC, HR (95% CrI)a | |||||
|---|---|---|---|---|---|---|
ITT-Bev | ITT | |||||
CAPOX | Pan + FOLFOX | Pembro | CAPOX | Pan + FOLFOX | Pembro | |
Fixed effects | ||||||
4 | 1.28 (1.05 to 1.55) | 0.85 (0.59 to 1.22) | 0.86 (0.45 to 1.67) | 1.28 (1.04 to 1.56) | 0.85 (0.59 to 1.23) | 1.01 (0.64 to 1.59) |
8 | 1.12 (0.98 to 1.27) | 0.86 (0.68 to 1.08) | 0.71 (0.40 to 1.26) | 1.12 (0.98 to 1.27) | 0.86 (0.68 to 1.08) | 0.78 (0.54 to 1.11) |
12 | 1.03 (0.93 to 1.14) | 0.86 (0.72 to 1.03) | 0.64 (0.34 to 1.20) | 1.03 (0.93 to 1.15) | 0.86 (0.71 to 1.03) | 0.67 (0.45 to 0.97) |
16 | 0.98 (0.89 to 1.07) | 0.86 (0.72 to 1.03) | 0.59 (0.28 to 1.20) | 0.98 (0.89 to 1.08) | 0.86 (0.72 to 1.03) | 0.60 (0.38 to 0.92) |
20 | 0.94 (0.85 to 1.03) | 0.86 (0.71 to 1.05) | 0.55 (0.24 to 1.22) | 0.94 (0.85 to 1.04) | 0.86 (0.71 to 1.04) | 0.55 (0.34 to 0.89) |
24 | 0.90 (0.81 to 1.01) | 0.87 (0.70 to 1.07) | 0.53 (0.22 to 1.25) | 0.90 (0.81 to 1.01) | 0.86 (0.70 to 1.07) | 0.52 (0.30 to 0.87) |
28 | 0.88 (0.78 to 0.99) | 0.87 (0.68 to 1.10) | 0.51 (0.19 to 1.28) | 0.88 (0.78 to 0.99) | 0.87 (0.68 to 1.09) | 0.49 (0.27 to 0.86) |
32 | 0.86 (0.75 to 0.97) | 0.87 (0.67 to 1.13) | 0.49 (0.17 to 1.31) | 0.86 (0.75 to 0.98) | 0.87 (0.67 to 1.12) | 0.46 (0.25 to 0.85) |
36 | 0.84 (0.73 to 0.96) | 0.87 (0.66 to 1.15) | 0.47 (0.16 to 1.34) | 0.84 (0.73 to 0.96) | 0.87 (0.65 to 1.15) | 0.44 (0.23 to 0.85) |
40 | 0.82 (0.70 to 0.95) | 0.87 (0.64 to 1.18) | 0.46 (0.15 to 1.36) | 0.82 (0.70 to 0.95) | 0.87 (0.64 to 1.17) | 0.43 (0.21 to 0.84) |
Random effects | ||||||
4 | 1.28 (0.70 to 2.26) | 0.86 (0.34 to 2.43) | 0.87 (0.28 to 2.61) | 1.27 (0.67 to 2.49) | 0.86 (0.30 to 2.92) | 1.00 (0.35 to 2.98) |
8 | 1.11 (0.62 to 1.95) | 0.86 (0.35 to 2.36) | 0.71 (0.24 to 2.05) | 1.11 (0.59 to 2.16) | 0.86 (0.31 to 2.86) | 0.78 (0.28 to 2.26) |
12 | 1.03 (0.57 to 1.81) | 0.86 (0.36 to 2.32) | 0.64 (0.21 to 1.91) | 1.03 (0.54 to 1.98) | 0.86 (0.31 to 2.86) | 0.67 (0.24 to 1.98) |
16 | 0.97 (0.54 to 1.71) | 0.86 (0.36 to 2.32) | 0.59 (0.18 to 1.86) | 0.97 (0.51 to 1.87) | 0.86 (0.31 to 2.85) | 0.60 (0.22 to 1.81) |
20 | 0.93 (0.52 to 1.64) | 0.87 (0.36 to 2.31) | 0.55 (0.16 to 1.82) | 0.93 (0.49 to 1.80) | 0.87 (0.31 to 2.85) | 0.55 (0.20 to 1.71) |
24 | 0.90 (0.50 to 1.59) | 0.87 (0.36 to 2.33) | 0.52 (0.14 to 1.83) | 0.90 (0.47 to 1.74) | 0.87 (0.31 to 2.86) | 0.52 (0.18 to 1.63) |
28 | 0.87 (0.48 to 1.55) | 0.87 (0.36 to 2.34) | 0.50 (0.13 to 1.84) | 0.87 (0.45 to 1.69) | 0.87 (0.31 to 2.84) | 0.49 (0.17 to 1.56) |
32 | 0.85 (0.47 to 1.51) | 0.87 (0.36 to 2.34) | 0.48 (0.12 to 1.85) | 0.85 (0.44 to 1.65) | 0.87 (0.31 to 2.85) | 0.46 (0.16 to 1.51) |
36 | 0.83 (0.46 to 1.49) | 0.87 (0.36 to 2.34) | 0.46 (0.11 to 1.88) | 0.83 (0.43 to 1.62) | 0.87 (0.31 to 2.85) | 0.44 (0.15 to 1.46) |
40 | 0.81 (0.45 to 1.46) | 0.87 (0.36 to 2.36) | 0.45 (0.11 to 1.88) | 0.81 (0.42 to 1.59) | 0.87 (0.31 to 2.85) | 0.43 (0.14 to 1.42) |
CrI = credible interval; FP = fractional polynomial; HR = hazard ratio; ITT = intention to treat; NMA = network meta-analysis; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care.
aTime-varying HRs at select follow-up times for competing interventions vs. SOC based on fixed- and random-effects NMA (second-order model [p1 = 0, p2 = 1]) —base-case (ITT-Bev) and ITT populations.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Results of the different crossover adjustment methods are summarized in Table 30; the methods generally yielded similar results. For constant HR analysis, the point estimate favoured pembrolizumab compared to all other interventions; however, results were also not statistically meaningful. In all crossover-adjusted analyses, panitumumab plus FOLFOX was the only regimen favoured over SOC, as well as over CAPOX, but was no different to pembrolizumab.
For time-varying Kaplan-Meier analysis, pembrolizumab showed a much more significant result compared to the base-case scenario, which had the lowest point HR versus SOC compared to other interventions from 4 months throughout the follow-up and was favoured over SOC starting from 8 months (Table 31 and Table 32).
Table 30: Overall Survival Estimated From Fixed-Effects NMA of OS for All Models — Crossover Adjusted
Intervention 2 | Intervention 1, HR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
Two-stage model (ITT) | ||||
SOC | — | 0.97 (0.87 to 1.07) | 1.20 (1.02 to 1.42) | 1.70 (0.86 to 3.43) |
CAPOX | 1.04 (0.93 to 1.16) | — | 1.25 (1.02 to 1.52) | 1.76 (0.89 to 3.59) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.41 (0.70 to 2.92) |
Pembrolizumab | 0.59 (0.29 to 1.16) | 0.57 (0.28 to 1.13) | 0.71 (0.34 to 1.43) | — |
IPCW model (ITT) | ||||
SOC | — | 0.96 (0.86 to 1.08) | 1.21 (1.02 to 1.42) | 1.70 (0.86 to 3.32) |
CAPOX | 1.04 (0.93 to 1.16) | — | 1.25 (1.02 to 1.52) | 1.76 (0.89 to 3.46) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.41 (0.71 to 2.80) |
Pembrolizumab | 0.59 (0.30 to 1.16) | 0.57 (0.29 to 1.12) | 0.71 (0.36 to 1.41) | — |
RPSFT model (ITT) | ||||
SOC | — | 0.96 (0.87 to 1.08) | 1.20 (1.02 to 1.42) | 1.47 (0.88 to 2.50) |
CAPOX | 1.04 (0.93 to 1.16) | — | 1.25 (1.02 to 1.52) | 1.53 (0.90 to 2.62) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.22 (0.71 to 2.15) |
Pembrolizumab | 0.68 (0.40 to 1.14) | 0.66 (0.38 to 1.11) | 0.82 (0.47 to 1.41) | — |
RPSFT model (ITT-Bev) | ||||
SOC | — | 0.97 (0.87 to 1.07) | 1.20 (1.02 to 1.42) | 1.59 (0.67 to 3.71) |
CAPOX | 1.04 (0.93 to 1.15) | — | 1.25 (1.02 to 1.52) | 1.65 (0.69 to 3.85) |
Pan + FOLFOX | 0.83 (0.70 to 0.98) | 0.80 (0.66 to 0.98) | — | 1.32 (0.55 to 3.13) |
Pembrolizumab | 0.63 (0.27 to 1.49) | 0.61 (0.26 to 1.44) | 0.76 (0.32 to 1.81) | — |
Bev = bevacizumab; CrI = credible interval; HR = hazard ratio; IPCW = inverse probability of censoring weighting; ITT = intention to treat; NMA = network meta-analysis; OS = overall survival; Pan = panitumumab; RPSFT = rank preserving structural failure time; SOC = standard of care.
Note: Two-stage, IPCW model: deviance information criterion (DIC) = 7.43; deviance = 4.44. RPSFT model: DIC = 7.44; deviance = 4.45. RPSFT model (ITT-Bev): DIC = 7.43; deviance = 4.42.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Table 31: Time-Varying Overall Survival — ITT Population
Month | Intervention vs. SOC, HR (95% CrI)a | ||
|---|---|---|---|
CAPOX | Pan + FOLFOX | Pembro | |
2-stage model | |||
4 | 1.27 (1.04 to 1.56) | 0.85 (0.59 to 1.23) | 0.87 (0.56 to 1.35) |
8 | 1.12 (0.98 to 1.27) | 0.86 (0.68 to 1.08) | 0.59 (0.41 to 0.84) |
12 | 1.03 (0.93 to 1.15) | 0.86 (0.72 to 1.03) | 0.47 (0.31 to 0.70) |
16 | 0.98 (0.89 to 1.08) | 0.86 (0.72 to 1.03) | 0.40 (0.25 to 0.63) |
20 | 0.94 (0.85 to 1.03) | 0.86 (0.71 to 1.05) | 0.35 (0.21 to 0.59) |
24 | 0.90 (0.81 to 1.01) | 0.86 (0.70 to 1.07) | 0.32 (0.18 to 0.56) |
28 | 0.88 (0.78 to 0.99) | 0.86 (0.69 to 1.10) | 0.29 (0.16 to 0.54) |
32 | 0.86 (0.75 to 0.97) | 0.87 (0.67 to 1.12) | 0.27 (0.14 to 0.52) |
36 | 0.84 (0.72 to 0.96) | 0.87 (0.66 to 1.15) | 0.25 (0.13 to 0.50) |
40 | 0.82 (0.70 to 0.95) | 0.87 (0.65 to 1.17) | 0.24 (0.12 to 0.49) |
IPCW model | |||
4 | 1.28 (1.04 to 1.57) | 0.86 (0.60 to 1.25) | 0.83 (0.54 to 1.31) |
8 | 1.12 (0.98 to 1.28) | 0.86 (0.68 to 1.09) | 0.54 (0.38 to 0.78) |
12 | 1.04 (0.93 to 1.15) | 0.86 (0.72 to 1.04) | 0.42 (0.28 to 0.62) |
16 | 0.98 (0.89 to 1.08) | 0.86 (0.72 to 1.03) | 0.35 (0.22 to 0.55) |
20 | 0.94 (0.85 to 1.04) | 0.86 (0.71 to 1.04) | 0.31 (0.18 to 0.51) |
24 | 0.91 (0.81 to 1.01) | 0.86 (0.70 to 1.06) | 0.27 (0.15 to 0.48) |
28 | 0.88 (0.78 to 0.99) | 0.86 (0.68 to 1.09) | 0.25 (0.13 to 0.45) |
32 | 0.86 (0.75 to 0.97) | 0.86 (0.66 to 1.12) | 0.23 (0.12 to 0.44) |
36 | 0.84 (0.73 to 0.96) | 0.86 (0.65 to 1.14) | 0.21 (0.10 to 0.42) |
40 | 0.82 (0.70 to 0.95) | 0.86 (0.64 to 1.16) | 0.20 (0.09 to 0.41) |
RPSFT method | |||
4 | 1.28 (1.05 to 1.56) | 0.86 (0.59 to 1.23) | 0.96 (0.62 to 1.50) |
8 | 1.12 (0.98 to 1.27) | 0.86 (0.68 to 1.08) | 0.69 (0.48 to 0.98) |
12 | 1.03 (0.93 to 1.14) | 0.86 (0.72 to 1.03) | 0.56 (0.38 to 0.83) |
16 | 0.98 (0.89 to 1.08) | 0.86 (0.72 to 1.03) | 0.49 (0.31 to 0.76) |
20 | 0.94 (0.85 to 1.03) | 0.86 (0.72 to 1.04) | 0.44 (0.26 to 0.72) |
24 | 0.90 (0.81 to 1.01) | 0.87 (0.70 to 1.07) | 0.40 (0.23 to 0.69) |
28 | 0.88 (0.78 to 0.99) | 0.87 (0.69 to 1.09) | 0.37 (0.20 to 0.67) |
32 | 0.86 (0.75 to 0.97) | 0.87 (0.67 to 1.12) | 0.35 (0.18 to 0.66) |
36 | 0.84 (0.73 to 0.96) | 0.87 (0.66 to 1.14) | 0.33 (0.17 to 0.64) |
40 | 0.82 (0.70 to 0.95) | 0.87 (0.64 to 1.17) | 0.32 (0.15 to 0.63) |
CrI = credible interval; FP = fractional polynomial; HR = hazard ratio; IPCW = inverse probability of censoring weighting; ITT = intention to treat; Pan = panitumumab; Pembro = pembrolizumab; RPSFT = rank preserving structural failure time; SOC = standard of care.
aTime-varying HRs at select follow-up times for competing interventions vs. SOC (second-order model [p1 = 0, p2 = 1]) — ITT Population.
Note: Two-stage model deviance information criterion (DIC) = 1,929.21; IPCW DIC = 1,988.18; RPSFT DIC = 1,933.3.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Table 32: Time-Varying Overall Survival — ITT-Bev Population
Month | Intervention vs. SOC, HR (95% CrI)a | ||
|---|---|---|---|
CAPOX | Pan + FOLFOX | Pembro | |
4 | 1.29 (1.05 to 1.58) | 0.85 (0.59 to 1.24) | 0.72 (0.37 to 1.39) |
8 | 1.12 (0.99 to 1.28) | 0.86 (0.68 to 1.09) | 0.46 (0.24 to 0.91) |
12 | 1.04 (0.93 to 1.15) | 0.86 (0.71 to 1.04) | 0.35 (0.16 to 0.82) |
16 | 0.98 (0.89 to 1.08) | 0.86 (0.72 to 1.03) | 0.29 (0.11 to 0.79) |
20 | 0.94 (0.85 to 1.04) | 0.86 (0.71 to 1.04) | 0.25 (0.09 to 0.77) |
24 | 0.90 (0.81 to 1.01) | 0.86 (0.70 to 1.07) | 0.22 (0.07 to 0.76) |
28 | 0.88 (0.78 to 0.99) | 0.86 (0.68 to 1.09) | 0.20 (0.06 to 0.76) |
32 | 0.85 (0.75 to 0.98) | 0.87 (0.67 to 1.12) | 0.19 (0.05 to 0.76) |
36 | 0.84 (0.72 to 0.96) | 0.87 (0.65 to 1.15) | 0.17 (0.04 to 0.75) |
40 | 0.82 (0.70 to 0.95) | 0.87 (0.64 to 1.17) | 0.16 (0.04 to 0.75) |
Bev = bevacizumab; CrI = credible interval; FP = fractional polynomial; HR = hazard ratio; ITT = intention to treat; Pan = panitumumab; Pembro = pembrolizumab; RPSFT = rank preserving structural failure time; SOC = standard of care; vs. = versus .
aTime-varying HRs at select follow-up times for competing interventions vs. SOC (second-order model [p1 = 0, p2 = 1]) — ITT-Bev Population.
Note: RPSFT deviance information criterion = 1,842.09.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Progression-Free Survival
For PFS, a connected network included 3 trials (KEYNOTE-177, Porschen 2007, and PRIME; see Figure 7) evaluating 4 interventions (pembrolizumab, CAPOX, mFOLFOX plus panitumumab, and SOC). Network meta-analyses for the base-case analyses were deemed feasible for PFS since KEYNOTE-177 reported subgroup data (ITT-Bev). Visual assessment (curves are non-parallel) of Schoenfeld residuals and P values (P < 0.05) of the Grambsch and Therneau test for proportional hazards in KEYNOTE-177 indicated these interventions violated the PHA. Network connections were only described by a single trial; therefore, between-study heterogeneity could not be estimated, and the results of random-effects analyses were not meaningful. As a result, only the fixed-effects analyses are shown.
Figure 7: Network of Evidence for Progression-Free Survival — Base Case
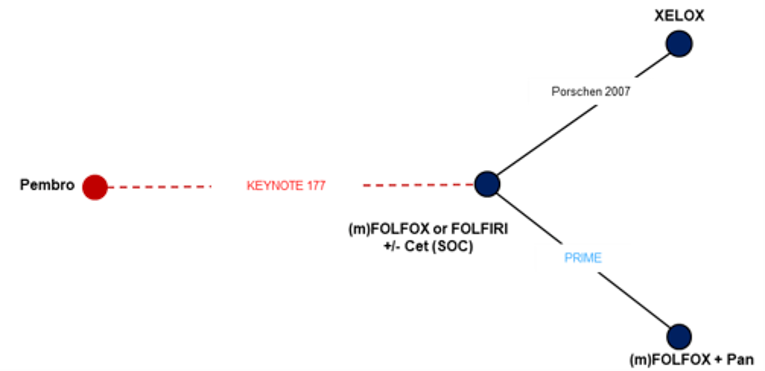
CET = cetuximab; Pembro = pembrolizumab; Pan = panitumumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Note: Trials in red evaluate patients in the microsatellite instability-high/mismatch repair-deficient population. Trials in blue were conducted in RAS wild-type patients.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
Pairwise results of the fixed-effects NMA are summarized in Table 33. In the ITT-Bev analysis, pembrolizumab was favoured over all other treatments. Panitumumab plus FOLFOX was also favoured over SOC and CAPOX. For the ITT population, both pembrolizumab alone and panitumumab plus FOLFOX were favoured over SOC and CAPOX.
Table 33: Progression-Free Survival Estimated From Fixed-Effects NMA — Base-Case (ITT-Bev) and ITT Populations
Intervention 2 | Intervention 1, HR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
ITT-Bev population | ||||
SOC | — | 0.85 (0.70 to 1.04) | 1.25 (1.05 to 1.49) | 2.49 (1.49 to 4.21) |
CAPOX | 1.17 (0.96 to 1.43) | — | 1.46 (1.13 to 1.90) | 2.92 (1.67 to 5.12) |
Pan + FOLFOX | 0.80 (0.67 to 0.95) | 0.68 (0.53 to 0.89) | — | 2.00 (1.16 to 3.45) |
Pembrolizumab | 0.40 (0.24 to 0.67) | 0.34 (0.20 to 0.60) | 0.50 (0.29 to 0.86) | — |
ITT Population | ||||
SOC | — | 0.85 (0.70 to 1.04) | 1.25 (1.05 to 1.49) | 1.66 (1.25 to 2.23) |
CAPOX | 1.17 (0.96 to 1.43) | — | 1.46 (1.13 to 1.91) | 1.95 (1.37 to 2.77) |
Pan + FOLFOX | 0.80 (0.67 to 0.95) | 0.68 (0.52 to 0.89) | — | 1.34 (0.95 to 1.86) |
Pembrolizumab | 0.60 (0.45 to 0.80) | 0.51 (0.36 to 0.73) | 0.75 (0.54 to 1.06) | — |
Bev = bevacizumab; CrI = credible interval; HR = hazard ratio; ITT = intention to treat; NMA = network meta-analysis; Pan = panitumumab; PFS = progression-free survival; SOC = standard of care.
Note: ITT-Bev: deviance information criterion = 5.36; deviance = 2.36. ITT: deviance information criterion = 5.38; deviance = 2.38.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Results of the time-varying analysis are summarized in Table 34. In the ITT-Bev population, the best-fitting model was the second-order FP model with p1 = 0, p2 = 1 (DIC = 869.35), while in the ITT group, the best-fitting model was the second-order FP model with p1 = 0, p2 = 0 (DIC = 996.24). In the ITT-Bev and ITT populations, pembrolizumab was favoured over SOC starting, respectively, at 4 months and 8 months and — for both populations — throughout the entire follow-up period. Panitumumab plus FOLFOX showed benefit over SOC from 4 months to 16 months, and from 4 months to 12 months in the ITT-Bev and ITT groups, respectively. The regimen of CAPOX was no different from SOC at any time point beyond 4 months in either group.
Table 34: Time-Varying Progression-Free Survival — Base-Case (ITT-Bev) and ITT Populations
Month | Intervention vs. SOC, HR (95% CrI)a | |||||
|---|---|---|---|---|---|---|
Second-order FP with p1 = 0, p2 = 1 (ITT-Bev) | Second-order FP with p1 = 0, p2 = 0 (ITT) | |||||
CAPOX | Pan + FOLFOX | Pembro | CAPOX | Pan + FOLFOX | Pembro | |
4 | 1.33 (1.01 to 1.75) | 0.79 (0.63 to 0.99) | 0.41 (0.24 to 0.66) | 1.34 (1.02 to 1.78) | 0.79 (0.63 to 0.99) | 0.76 (0.56 to 1.04) |
8 | 1.13 (0.93 to 1.36) | 0.80 (0.68 to 0.94) | 0.22 (0.12 to 0.40) | 1.12 (0.93 to 1.35) | 0.81 (0.69 to 0.94) | 0.38 (0.27 to 0.53) |
12 | 1.02 (0.81 to 1.28) | 0.81 (0.68 to 0.96) | 0.16 (0.08 to 0.32) | 1.00 (0.80 to 1.26) | 0.81 (0.69 to 0.96) | 0.25 (0.17 to 0.38) |
16 | 0.96 (0.72 to 1.26) | 0.82 (0.67 to 1.00) | 0.12 (0.05 to 0.28) | 0.93 (0.70 to 1.23) | 0.82 (0.67 to 1.00) | 0.19 (0.12 to 0.31) |
20 | 0.91 (0.65 to 1.26) | 0.82 (0.65 to 1.03) | 0.10 (0.04 to 0.25) | 0.88 (0.63 to 1.22) | 0.82 (0.65 to 1.04) | 0.15 (0.09 to 0.26) |
24 | 0.87 (0.59 to 1.27) | 0.82 (0.64 to 1.07) | 0.09 (0.03 to 0.23) | 0.84 (0.57 to 1.22) | 0.83 (0.64 to 1.07) | 0.13 (0.07 to 0.23) |
28 | 0.84 (0.55 to 1.28) | 0.82 (0.62 to 1.10) | 0.08 (0.03 to 0.22) | 0.80 (0.53 to 1.22) | 0.83 (0.62 to 1.10) | 0.11 (0.06 to 0.20) |
32 | 0.81 (0.51 to 1.28) | 0.83 (0.61 to 1.13) | 0.07 (0.02 to 0.21) | 0.78 (0.49 to 1.22) | 0.83 (0.61 to 1.13) | 0.10 (0.05 to 0.19) |
36 | 0.79 (0.48 to 1.29) | 0.83 (0.60 to 1.15) | 0.06 (0.02 to 0.19) | 0.75 (0.46 to 1.22) | 0.84 (0.60 to 1.16) | 0.09 (0.04 to 0.17) |
40 | 0.77 (0.45 to 1.30) | 0.83 (0.59 to 1.18) | 0.06 (0.02 to 0.19) | 0.73 (0.44 to 1.22) | 0.84 (0.59 to 1.19) | 0.08 (0.04 to 0.16) |
Bev = bevacizumab; CrI = credible interval; FP = fractional polynomial; HR = hazard ratio; ITT = intention to treat; NMA = network meta-analysis; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care.
aTime-varying HRs at select follow-up times for competing interventions vs. SOC from fixed-effects models, base-case (ITT-Bev) and ITT Populations.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Overall Response Rate
For ORR, a connected network was available for ITT analysis, which included 4 studies (Figure 8). The population of KEYNOTE-177 for the ORR NMA was the ITT population, which included bevacizumab patients. Stable estimates of between-study heterogeneity could not be obtained, and results of random-effects analyses were not meaningful; therefore, only results of fixed-effects analyses are shown.
Figure 8: Network of Evidence for Overall Response Rate: ITT Population
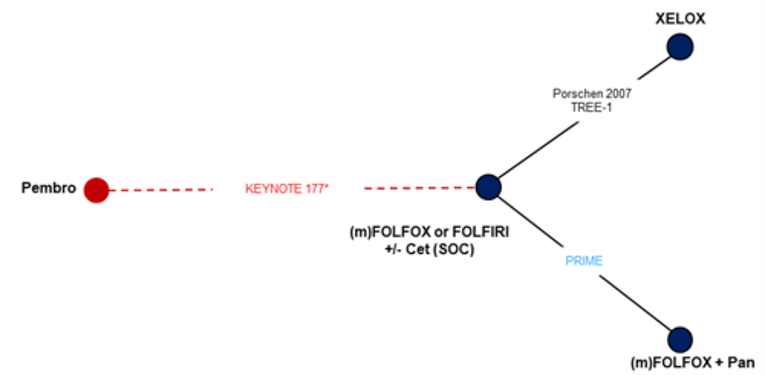
Cet = cetuximab; ITT = intention to treat; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Note: Trials in red evaluate patients in the microsatellite instability-high or mismatch repair-deficient population. Trials in blue were conducted in RAS wild-type patients.
* The ITT population of KEYNOTE-177 was used.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
The results of the fixed-effects NMA are summarized in Table 35. Pembrolizumab was favoured for ORR compared to CAPOX (OR = 1.98; 95% CrI, 1.12 to 3.47), and panitumumab plus FOLFOX was favoured over SOC (OR = 1.47; 95% CrI, 1.08 to 2.00) and CAPOX (OR = 1.84; 95% CrI, 1.18 to 2.90).
Table 35: Overall Response Rate Estimated From Fixed-Effects NMA — ITT Population
Intervention 2 | Intervention 1, OR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
SOC | — | 1.26 (0.90 to 1.73) | 0.68 (0.50 to 0.93) | 0.64 (0.40 to 1.01) |
CAPOX | 0.80 (0.58 to 1.11) | — | 0.54 (0.34 to 0.85) | 0.51 (0.29 to 0.89) |
Pan + FOLFOX | 1.47 (1.08 to 2.00) | 1.84 (1.18 to 2.90) | — | 0.93 (0.54 to 1.63) |
Pembrolizumab | 1.57 (0.99 to 2.51) | 1.98 (1.12 to 3.47) | 1.07 (0.61 to 1.86) | — |
CrI = credible interval; ITT = intention to treat; NMA = network meta-analysis; OR = odds ratio; ORR = overall response rate; Pan = panitumumab; SOC = standard of care.
Note: Deviance information criterion = 13.37; deviance = 6.37.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Safety
The results of safety NMAs were based on the KEYNOTE-177 ITT population. The authors noted that this could bias results in favour of trials that did not include bevacizumab as it has a worse safety profile than cetuximab. Figure 9 to Figure 12 show the networks of evidence for DAEs, AEs grade of 3 or higher, treatment-related AEs of grade 3 or higher, and treatment-related SAEs, respectively.
Discontinuations Due to Adverse Events: For DAEs, a connected network including 2 trials (KEYNOTE-177 and Porschen 2007) and evaluating 3 interventions (pembrolizumab, CAPOX, and SOC) is shown in Figure 9.
Figure 9: Network of Evidence for Discontinuations Due to AEs
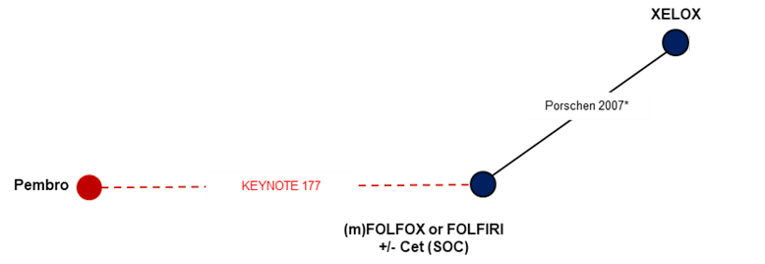
AE = adverse event; CET = cetuximab; Pembro = pembrolizumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Note: Trials in red evaluate patients in the microsatellite instability-high or mismatch repair-deficient population. ITT population of KEYNOTE-177 was used.
* Discontinuation due to serious AEs were used.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Discontinuations due to AEs were reported in the 2 included trials. The results of the fixed-effects NMA are summarized in Table 36. No treatments were favoured over any other with respect to discontinuations due to AEs.
Table 36: Discontinuations Due to Adverse Events Estimated From Fixed-Effects NMA
Intervention 2 | Intervention 1, OR (95% CrI) | ||
|---|---|---|---|
SOC | CAPOX | Pembrolizumab | |
SOC | — | 1.18 (0.77 to 1.82) | 0.73 (0.37 to 1.45) |
CAPOX | 0.85 (0.55 to 1.30) | — | 0.62 (0.27 to 1.38) |
Pembrolizumab | 1.36 (0.69 to 2.72) | 1.61 (0.72 to 3.65) | — |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; SOC = standard of care.
Note: Deviance information criterion = 7.4; deviance = 3.39.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Adverse Events of Grade 3 or Higher: For AEs grade 3 or higher, a connected network including 4 trials (KEYNOTE-177, PRIME, NO16966, and TREE-1) evaluating 4 interventions (SOC, pembrolizumab, CAPOX, panitumumab plus FOLFOX) is shown in Figure 10.
Figure 10: Network of Evidence for AEs of Grade 3 or Higher
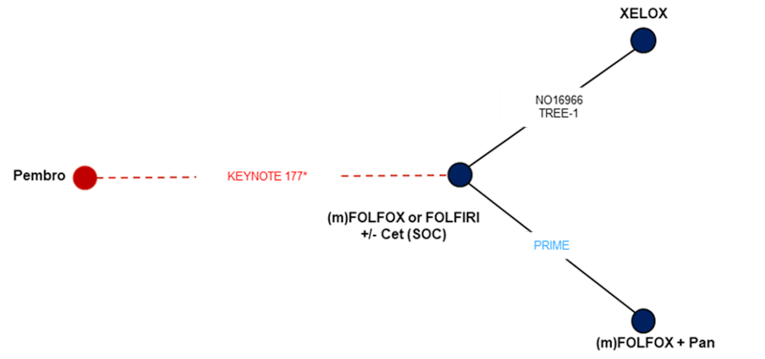
AE = adverse event; Cet = cetuximab; ITT = intention to treat; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Note: Trials in red evaluate patients in the microsatellite instability-high or mismatch repair-deficient population. Trials in blue were conducted in RAS wild-type patients.KEYNOTE-177 reported grade 3 to 5 AEs; the other trials reported grade 3 to 4 AEs.
* The ITT population of KEYNOTE-177 was used.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
The KEYNOTE-177 study reported AEs of grade 3 or higher (grade 3 to 5), whereas NO16966, TREE-1, and PRIME reported grade 3 to 4 AEs. The authors noted that although grade 5 AEs are unlikely to occur in patients who did not also experience a grade 3 to 4 AE, the inclusion of grade 3 to 4 and grade 3 or higher AEs in this analysis may bias results against KEYNOTE-177. The results of the fixed-effects NMA are shown in Table 37. Pembrolizumab was favoured over all other treatments with lower odds of AEs of grade 3 or higher (SOC: OR = 0.37; 95% CrI, 0.22 to 0.61; CAPOX: OR = 0.47; 95% CrI, 0.26 to 0.83; and panitumumab plus FOLFOX: OR = 0.16; 95% CrI, 0.08 to 0.30). Additionally, CAPOX was associated with lower odds of AEs grade 3 or higher compared to SOC. Panitumumab plus FOLFOX was associated with increased odds of grade 3 or higher AEs compared to all other treatments.
Table 37: Adverse Events of Grade 3 or Higher Estimated From Fixed-Effects NMA
Intervention 2 | Intervention 1, OR (95% CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
SOC | — | 1.29 (1.02 to 1.62) | 0.44 (0.30 to 0.63) | 2.73 (1.63 to 4.58) |
CAPOX | 0.78 (0.62 to 0.98) | — | 0.34 (0.22 to 0.53) | 2.12 (1.20 to 3.79) |
Pan + FOLFOX | 2.29 (1.59 to 3.36) | 2.95 (1.90 to 4.63) | — | 6.26 (3.32 to 11.84) |
Pembrolizumab | 0.37 (0.22 to 0.61) | 0.47 (0.26 to 0.83) | 0.16 (0.08 to 0.30) | — |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; Pan = panitumumab; SOC = standard of care.
Note: Deviance information criterion = 19.19; deviance = 12.2.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Treatment-Related Adverse Events of Grade 3 or Higher: For treatment-related AEs of grade 3 or higher, a connected network including 3 trials (KEYNOTE-177, PRIME, and TREE-1) evaluating 4 interventions (SOC, pembrolizumab, CAPOX, and panitumumab plus FOLFOX) is shown in Figure 11.
Figure 11: Network of Evidence for Treatment-Related AEs of Grade 3 or Higher
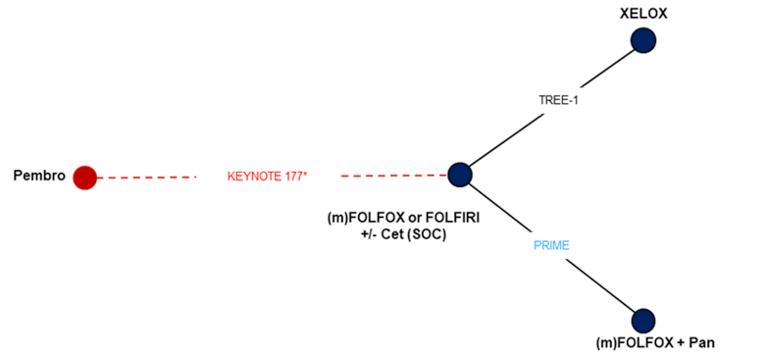
AE = adverse event; Cet = cetuximab; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care; XELOX = CAPOX (capecitabine and oxaliplatin).
Note: Trials in red evaluate patients in the microsatellite instability-high or mismatch repair-deficient population. Trials in blue were conducted in RAS wild-type patients.KEYNOTE-177 reported grade 3 to 5 AEs; the other trials reported grade 3 to 4 AEs.
* ITT population of KEYNOTE-177 was used.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
The results of the fixed-effects NMA are shown in Table 38. Pembrolizumab was favoured over all other treatments (OR = 0.14; [95% CrI, 0.08 to 0.24], OR = 0.06 [95% CrI, 0.03 to 0.15], and OR = 0.05 [95% CrI, 0.03 to 0.10] versus SOC, CAPOX, and panitumumab plus FOLFOX, respectively), showing reduced odds of treatment-related AEs of grade 3 or higher. Conversely, both panitumumab plus FOLFOX and CAPOX were also associated with increased odds of treatment-related AEs of grade 3 or higher over SOC (OR = 2.68 [95% CrI, 1.87 to 3.92] and OR = 2.22 [95% CrI, 1.09 to 4.73], respectively).
Table 38: Treatment-Related Adverse Events of Grade 3 or Higher Estimated From Fixed-Effects NMA
Intervention 2 | Intervention 1, OR (CrI) | |||
|---|---|---|---|---|
SOC | CAPOX | Pan + FOLFOX | Pembrolizumab | |
SOC | — | 0.45 (0.21 to 0.92) | 0.37 (0.26 to 0.54) | 7.10 (4.23 to 11.89) |
CAPOX | 2.22 (1.09 to 4.73) | — | 0.83 (0.37 to 1.89) | 15.82 (6.54 to 39.52) |
Pan + FOLFOX | 2.68 (1.87 to 3.92) | 1.20 (0.53 to 2.69) | — | 19.04 (10.10 to 36.17) |
Pembrolizumab | 0.14 (0.08 to 0.24) | 0.06 (0.03 to 0.15) | 0.05 (0.03 to 0.10) | — |
CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; Pan = panitumumab; SOC = standard of care.
Note: Deviance information criterion = 7.42; deviance = 3.38.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Treatment-Related Serious Adverse Events: For treatment-related SAEs of grade 3 or higher, a connected network including 2 trials (KEYNOTE-177 and PRIME) evaluating 3 interventions (SOC, pembrolizumab, and panitumumab plus FOLFOX) is shown in Figure 12.
Figure 12: Network of Evidence for Treatment-Related SAEs
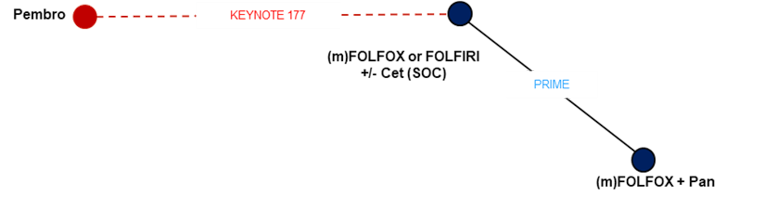
Cet = cetuximab; ITT = intention to treat; Pan = panitumumab; Pembro = pembrolizumab; SOC = standard of care; TRAE = treatment-related adverse event.
Note: Trials in red evaluate patients in the microsatellite instability-high or mismatch repair-deficient population. Trials in blue were conducted in RAS wild-type patients.
Source: Sponsor-submitted indirect treatment comparison and network meta-analysis.14
The results of the fixed-effects NMA for serious treatment-related SAEs are summarized in Table 39. Pembrolizumab was favoured over panitumumab plus FOLFOX (OR = 0.41; 95% CrI, 0.21 to 0.77), as well as SOC (OR = 0.48; 95% CrI, 0.27 to 0.83), with reduced odds of serious TRAEs.
Table 39: Treatment-Related Serious Adverse Events Estimated From Fixed-Effects NMA
Intervention 2 | Intervention 1, OR (95% CrI) | ||
|---|---|---|---|
SOC | Pan + FOLFOX | Pembrolizumab | |
SOC | — | 0.85 (0.61 to 1.16) | 2.06 (1.20 to 3.72) |
Pan + FOLFOX | 1.18 (0.86 to 1.63) | — | 2.44 (1.30 to 4.78) |
Pembrolizumab | 0.48 (0.27 to 0.83) | 0.41 (0.21 to 0.77) | — |
CrI = credible interval; ITT = intention to treat; NMA = network meta-analysis; OR = odds ratio; Pan = panitumumab; SAE = serious adverse event; SOC = standard of care.
Note: Deviance information criterion = 7.42; deviance = 3.38.
Source: Sponsor-submitted indirect treatment comparison and NMA.14
Critical Appraisal of Sponsor-Submitted NMA
The key limitations of the ITC and NMA include several major clinical assumptions made and several notable differences in the characteristics of patients across studies, which impact the interpretation of the NMA results, as well as the small size and structure of the network, which prevented the use of random-effects models in most outcomes of interest and the ability to model between-study heterogeneity and to assess consistency between direct and indirect comparisons as there were no closed loops.
The ITC and NMA was based on an SLR that identified studies according to pre-specified inclusion criteria. Insufficient information was provided on the search criteria and search methodology, and therefore it is unclear if all relevant published or unpublished studies were included. The methods of study selection and data extraction were omitted, so it is unclear whether appropriate methods were followed. Moreover, no risk of bias assessment was included in the report. The key limitation of the SLR, and therefore the ITC and NMA, was that it was conducted for the UK context and only assessed interventions relevant to the UK. As such, key PICOS criteria related to Canadian practice, such as bevacizumab as a treatment option, were not included in the pre-specified PICOS framework, and publications related to these criteria were likely missed. Therefore, the relevance of the SLR and NMA to the Canadian context is unclear. A full list of excluded publications and reasons for exclusion was not provided, and therefore it was not possible to assess whether potentially relevant studies may have been excluded. The SLR search aimed at identifying UK-relevant interventions in the broader mCRC population, as opposed to that of the funding request in Canada. The populations of patients from the included publications for the SLR and NMA varied, with 1 study looking at MSI-H/dMMR mCRC, 1 evaluating KRAS mutants, and 3 evaluating the general mCRC population. Other key differences in study characteristics include the study design of the KEYNOTE-177 trial, where patients could cross over from SOC during the study. The sponsor noted that this may bias the results, and therefore statistical methods were implemented to account for crossover from SOC to pembrolizumab. Results from the crossover analyses for OS for 3 models used yielded identical results (HR = 0.83; 95% CrI, 0.7 to 0.98), indicating that the crossover adjustments, as compared to the primary unadjusted analyses, did not show significant impact on the results of OS and that both of these sets of results were statistically non-significant. However, it is unclear whether the applied adjustment models would have effectively accounted for the crossover from SOC to pembrolizumab, which highly likely biased the effect toward null, provided that patients who shifted to receive pembrolizumab would have had responded to the treatment in the subsequent short observation period. Nevertheless, given the immature results on OS in the KEYNOTE-177 trial, the sponsor-submitted NMA was significantly compromised on this outcome.
Overall, the outcomes assessed were appropriate; however, other important outcomes, such as HRQoL, were not considered, despite HRQoL being an outcome of interest in the pre-specified PICOS framework for the SLR. It is unclear whether the authors chose not to assess HRQoL or whether no information was provided in the included studies. Based on the NMA report, the outcomes assessed in the included trials appeared similar with respect to the definitions used. Assessment methods (blinded independent review or investigator assessed) were not reported for any of the studies. The authors also did not report the criteria of the trials used to determine response. Any differences in outcome assessment and the criteria used for response across included studies may be a source of heterogeneity between studies and have the potential to influence relative treatment effect estimates.
Several differences in study characteristics across the trials are noted as potential sources of heterogeneity: namely, characteristics of the populations in the studies. As previously mentioned, the populations of included studies varied from the general mCRC population to populations with specific biomarkers. One of the main clinical assumptions in the NMA was that there was no difference in effect estimates between patients with MSI-H/dMMR, KRAS wild-type (other than panitumumab), or general mCRC; however, these variations in population are expected to impact the relative treatment effects as they are potentially important treatment effect modifiers, as evidenced by accumulated literature, like many other genetic biomarkers in oncology therapies. Therefore, any results of the NMA should be interpreted with caution with respect to population. In addition to the differences in the baseline characteristics of the patients (particularly the site and stage of metastasis), ECOG PS and durations on treatments or on trial had considerable variations. The ECOG important characteristics of age and gender were relatively similar across trials and study arms; however, there appeared to be a lower proportion of males in the KEYNOTE-177 trial than in the other studies. The primary tumour site proportions varied somewhat among trials, although NO16966 and Porschen 2007 trials did not report this distribution. The Porschen 2007 study was also the only study that enrolled patients with an ECOG PS of 2, likely underestimating the effectiveness of CAPOX. Lastly, although follow-up time was reported, there were considerable differences in median follow-up of patients in the included trials, ranging from 15 months to 28.4 months, which may impact time-to-response outcomes and safety outcomes.
The authors made some clinical assumptions around equivalence of treatments, as well as assumptions around the addition and removal of treatments in the SOC regimens, which may impact the results and generalizability of the NMA. As previously mentioned, the comparator of bevacizumab was not of interest in the NMA as it is not a relevant comparator in the UK. Therefore, the authors constructed networks for the base case that consisted of mFOLFOX or FOLFIRI, with or without cetuximab, and did not include patients from KEYNOTE-177 who received bevacizumab in the SOC arm (ITT-Bev), which may bias the results in favour of pembrolizumab because a comprehensive set of relevant comparators was not evaluated. Moreover, there is uncertainty and imprecision in the results of these comparisons due to the smaller sample size for the subgroup of patients who did not receive bevacizumab, as evidenced by the wider CrIs. Although not drastically different from the overall ITT population, results of the NMA for OS and PFS using the ITT-Bev analysis should be interpreted with caution. It was assumed that there was equivalence of different FOLFOX regimens since various FOLFOX regimens were used by different trials, as well as equivalence of FOLFOX to FOLFIRI, although these assumptions are not expected to drastically affect the results of the NMA. Additionally, the authors assumed a lack of effect of adding cetuximab to SOC of FOLFOX or FOLFIRI regimens, given the lack of available data from KEYNOTE-177 on patients who did not receive cetuximab. The authors noted that conclusions based on the analysis of the ITT-Bev population assumed similarity between FOLFOX or FOLFIRI plus bevacizumab and FOLFOX or FOLFIRI plus cetuximab regimens. It was also noted that this may impact the results of the NMA, particularly in those with KRAS wild-type mCRC, as the authors noted there was evidence of advantage in terms of PFS in such patients who were receiving cetuximab. Moreover, cetuximab is not a routinely funded treatment in all Canadian provinces and, therefore, may not be considered a relevant comparator.
The authors noted that the networks were constructed based on availability of outcome data. Besides the comparison between SOC and CAPOX for OS, comparisons for almost all competing interventions were based on single trials. The available trials formed networks with no closed loops; therefore, it was not possible to validate the transitivity assumption of NMA and check for consistency of results between direct and indirect comparisons. Random-effects models were attempted and determined not to be feasible due to the small number of studies for all outcomes except OS. Consequently, as connections were only described by a single trial for PFS, ORR, and safety, results for these outcomes are based on a fixed-effects model, as random-effects analyses were not meaningful.
The authors noted that the PHA in the KEYNOTE-177 trial was violated for OS and PFS, as shown in Kaplan-Meier curves, and therefore both constant and time-varying analyses were conducted. In this case, results from the time-varying analyses are preferred; however, the authors noted that uncertainty in time-varying estimates of HRs often leads to wider CrIs, which can make it more difficult to draw statistically meaningful conclusions. In general, point estimates and CrIs of OS and PFS for interventions compared to SOC in the ITT population were not significantly different to the NMAs using constant HRs. Results tended to favour pembrolizumab in the time-varying analyses, with pembrolizumab exhibiting statistically different results on PFS compared to SOC after the first few months, while other treatments were only favoured over SOC at the beginnings of treatment, but not long-term. Interestingly, in the constant HR analysis, panitumumab plus FOLFOX was the preferred treatment compared to SOC but was not favoured over SOC in the time-varying analysis of OS and PFS. It was noted by the authors that constant HR analyses are considered to be appropriate compared to time-varying HR analyses due to the overlap of CrIs and uncertainty as a result of short follow-up times and low numbers of events; however, violations to the PHA need to be acknowledged, and therefore results for the time-varying analyses are preferred.
Safety results show that pembrolizumab was favoured over all competing interventions for AEs of grade3 or higher and treatment-related AEs of grade 3 or higher, and over panitumumab plus FOLFOX for treatment-related SAEs in the ITT population. The results of the ITC and NMA, focusing on overall AEs reported in the trials, should be interpreted with caution given the differences in study design, definitions, and reporting of AEs. Given the variable length in follow-up across trials, there is potential for biased results in the frequency of AEs, as some may occur rarely or may only become apparent long after the beginning of treatment. Therefore, results of the NMAs focusing on DAEs, AEs of grade 3 or higher, treatment-related AEs of grade 3 or higher, and treatment-related SAEs of grade3 or higher should be interpreted with caution. For a more meaningful interpretation of AEs, the authors should have focused on special AEs of interest.
Overall, the results of the ITC and NMA may not be generalizable to the Canadian context. The exclusion of bevacizumab as a comparator in the SLR and NMA may have biased the results, as relevant studies may not have been identified. Moreover, the results of the NMA include a heterogeneous patient population made up of MSI-H/dMMR mCRC, KRAS wild type mCRC, and general mCRC patients, who were not assessed as subgroups, and therefore it is uncertain how the different subgroups of patients would respond to treatment with pembrolizumab.
Summary
The sponsor-submitted NMA did not clearly demonstrate that pembrolizumab was favoured, not favoured, or similar to the comparators included in the analyses. Regardless, the significant limitations associated with the NMA would have precluded drawing definitive conclusions on the comparative efficacy and safety of pembrolizumab. Key limitations of the NMA were the exclusion of bevacizumab as a comparator, the small and sparsely populated networks, and the considerable clinical and methodological heterogeneity, which was not adequately addressed.
Discussion
Summary of Available Evidence
The systematic review protocol identified 1 study of interest, KEYNOTE-177. This study was a phase III, open-label trial consisting of 307 adults with unresectable or metastatic MSI-H/dMMR colorectal cancer randomized to receive pembrolizumab 200 mg every 3 weeks or SOC, which was defined as 1 of FOLFOX, FOLFOX plus bevacizumab, FOLFOX plus cetuximab, FOLFIRI, FOLFIRI plus bevacizumab, or FOLFIRI plus cetuximab. The trial’s co-primary outcomes were PFS and OS, and it contained a secondary outcome of ORR. In KEYNOTE-177, 50.2% of patients were female; average patient age was 61.2 years; 74.6% of patients were White, 16.3% Asian, 4.6% Black, and 6.8% Hispanic or Latino; and 51.8% had an ECOG PS of 0 and 48.2% had an ECOG PS of 1.
Interpretation of Results
Efficacy
The primary analysis of PFS indicates that pembrolizumab increases median PFS by approximately 8 months, a clinically significant amount as determined by CADTH’s clinical experts. The HR was statistically significant, but because of the violated PHA, the estimate may be biased. Instead, RMST, a commonly used alternate metric of long-term survival for such situations, suggests a 2.9-month improvement in PFS, which was also considered clinically significant by the clinical experts. Additionally, PFS was higher in the pembrolizumab arm at 9, 12, 18, and 24 months. Two sensitivity analyses investigating the impact of crossovers and the use of subsequent anticancer medications on the results were conducted. In both analyses, the HRs only changed slightly, suggesting that pembrolizumab’s benefit as observed in the primary analysis is robust. However, 1 sensitivity analysis suggests the median survival in the pembrolizumab arm (7.0 months; 95% CI, 4.2 to 12.4) and SOC arm (6.3 months; 95% CI, 4.6 to 8.2) may not differ substantially. However, in this analysis, the survival rate at 12 months was higher in the pembrolizumab arm (44.1%; 95% CI, 36.0% to 51.8%) than in the SOC arm (30.2%; 95% CI, 23.0% to 37.6%). Survival rates at other time points were not provided. Ultimately, the totality of evidence suggests pembrolizumab improves PFS to a clinically meaningful degree.
Pembrolizumab’s impact on OS is less certain. Median survival could not be reported in the pembrolizumab arm, and the HR was statistically insignificant (HR = 0.77; 95% CI, 0.54 to 1.09). However, the OS at 9, 12, 18, and 24 months was higher in the pembrolizumab arm than in the SOC arm. As crossovers and subsequent use of anti-PD1/PDL1 therapy could bias the primary OS analysis, 3 sensitivity analyses were conducted. The results from each sensitivity analysis differ from the primary analysis, suggesting some bias in the latter. However, the point estimates from the primary and sensitivity analyses indicate some benefit from pembrolizumab in OS, but due to the variation in point estimates, wide CIs and lack of significance testing, the exact magnitude of any benefit from pembrolizumab on OS is uncertain. Although PFS is a surrogate outcome, there is evidence that it is correlated with OS in mCRC. Correlation between PFS HRs and OS HRs has been estimated to be moderate to very strong (r ≥ 0.4) and may be strongest in the setting of first-line phase III trials of targeted drugs.41 Nonetheless, the lack of robust and final OS results from KEYNOTE-177 preclude drawing concrete conclusions regarding the effects of pembrolizumab on OS as a first-line treatment in adults with unresectable or metastatic MSI-H/dMMR colorectal cancer.
In the PFS and OS analyses, pembrolizumab patients experienced worse outcomes for the first 6 months to 8 months. In some circumstances, this may indicate an imbalance in prognostic factors at baseline, but the table of baseline characteristics did not identify such imbalances. Instead, the clinical experts suggest that pembrolizumab’s onset of action may be slower than that of SOC, leading to poor outcomes in the early stages of the study. Alternatively, there may be a subgroup, yet to be identified, which may not benefit from pembrolizumab.
The ORR was higher in the pembrolizumab arm and, while it was not statistically significant, it was considered clinically significant by the clinical experts. A median duration of response could not be calculated for the pembrolizumab arm, but more pembrolizumab patients experienced a response extending beyond 6, 9, 12, 18, and 24 months. Mean and median time to response was similar between both arms. Finally, while statistical significance testing adjusted for multiplicity was not applied, HRQoL was higher to a clinically significant degree in the pembrolizumab arm when measured by the EORTC global health–quality of life score or EQ-5D visual analogue or utility scores. Although the HRQoL results are only considered supportive because they were analyzed as exploratory outcomes in KEYNOTE-177, the different directions of the within-group changes from baseline in the 2 treatment groups are notable.
The totality of the evidence from KEYNOTE-177, improved PFS and HRQoL, suggests that patients with unresectable or metastatic MSI-H/dMMR colorectal cancer will have better outcomes with pembrolizumab than with the SOC regimens used in the trial.
The sponsor provided an NMA that compared pembrolizumab versus other treatments for unresectable or metastatic MSI-H/dMMR colorectal cancer. However, the geometry of the sparsely populated networks and considerable clinical and methodological heterogeneity that could not be fully accounted for made the results of the NMA difficult to interpret. It could not be concluded whether pembrolizumab was favoured, not favoured, or similar to the comparators included in the analysis of comparative efficacy.
Harms
The frequency of overall AEs was similar in both treatment groups, but patients in the pembrolizumab group reported fewer SAEs. Treatment discontinuation and deaths following an AE were similar in each arm. Compared to the sponsor’s cumulative running safety dataset, these rates did not differ. No new AEs were identified in KEYNOTE-177 beyond the ones typically observed with pembrolizumab. Unsurprisingly, immune-mediated AEs, which were pre-specified in the review protocol as events of interest, were more frequent in the pembrolizumab arm. Relative to the sponsor’s cumulative running safety dataset for pembrolizumab, the number of such AEs were higher in KEYNOTE-177.
The sponsor-provided NMA reported that pembrolizumab was favoured over comparators with regard to grade 3 and higher AEs and grade 3 and higher treatment-related AEs. Pembrolizumab was also favoured over panitumumab plus FOLFOX for treatment-related SAEs. However, as described for the efficacy outcome analyses, the results of comparative harms may not be valid because of the significant limitations of the NMA.
Patient groups in their input to CADTH for the review of pembrolizumab identified safety as an important consideration. It was suggested that patients were willing to tolerate more SAEs for additional survival time, delayed progression, and improved quality of life. Likewise, clinicians noted that treatment maybe limited with SOC regimens because of associated serious adverse effects. Although the comparative safety data are not robust, there is a suggestion that patients may experience fewer SAEs with pembrolizumab than with SOC regimens.
Implementation Considerations
In 2016, CADTH published an Optimal Use Report titled DNA Mismatch Repair Deficiency Tumour Testing for Patients With Colorectal Cancer: Recommendation.42 The gold standard for detecting MSI-H/dMMR patients is through germline genetic testing; however, polymerase chain reaction to test for MSI-H status or immunohistochemistry to assess dMMR status may be considered before genetic testing. Both tests have high sensitivity and moderate-to-high specificity, though the latter provides additional information regarding the nature of the mutation, which can guide further diagnostics, is cheaper, and may be preferred by clinicians. The report recommended universal dMMR tumour testing for patients with colorectal cancer followed by reflex tumour testing for MLH1 promoter hypermethylation, which would be cost-effective if the willingness to pay ranges from $28,902 to $387,330.
Conclusions
Pembrolizumab improved PFS versus SOC in a single RCT of patients with unresectable or metastatic MSI-H/dMMR colorectal cancer. The difference between treatment groups was considered clinically meaningful based on input from the clinical experts consulted by CADTH. Although fewer patients died in the pembrolizumab group than in the SOC group, no statistically significant benefit in OS was found. The study was not adequately designed to evaluate treatment effects on OS, and estimates are uncertain due to crossovers and use of subsequent anticancer medications. The ORR, duration of response, and HRQoL were also numerically improved relative to SOC. Although benefits aside from PFS could not be supported by statistical significance in all outcomes, the efficacy results in totality suggest pembrolizumab improves outcomes over SOC in a difficult-to-treat patient population whose cancer is often unresponsive to SOC. Pembrolizumab does not appear to be associated with more AEs than the SOC regimens evaluated. Known AEs of interest such as immune-mediated AEs occurred more frequently in the pembrolizumab group and remain a concern.
References
1.Canadian Cancer Society. Colorectal cancer. What is colorectal cancer? 2021; https://www.cancer.ca/en/cancer-information/cancer-type/colorectal/colorectal-cancer/?region=on. Accessed 2021 Mar 8.
2.Macrae FA, Bendell J. Clinical presentation, diagnosis, and staging of colorectal cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Mar 8.
3.Canadian Cancer Society. Colorectal cancer. Colorectal cancer statistics. 2021; https://www.cancer.ca/en/cancer-information/cancer-type/colorectal/statistics/?region=on. Accessed 2021 Mar 8.
4.Pestana C, Reitemeier RJ, Moertel CG, Judd ES, Dockerty MB. The natural history of carcinoma of the colon and rectum. Am J Surg. 1964;108:826-829. PubMed
5.Bengmark S, Hafström L. The natural history of primary and secondary malignant tumors of the liver. I. The prognosis for patients with hepatic metastases from colonic and rectal carcinoma by laparotomy. Cancer. 1969;23(1):198-202. PubMed
6.Rodriguez-Bigas MA, Grothey A. Overview of the management of primary colon cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com.
7.Heinemann V, von Weikersthal LF, Decker T, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(10):1065-1075. PubMed
8.André T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207-2218. PubMed
9.Venderbosch S, Nagtegaal ID, Maughan TS, et al. Mismatch repair status and BRAF mutation status in metastatic colorectal cancer patients: a pooled analysis of the CAIRO, CAIRO2, COIN, and FOCUS studies. Clin Cancer Res. 2014;20(20):5322-5330. PubMed
10.Boland CR, Goel A. Microsatellite instability in colorectal cancer. Gastroenterology. 2010;138(6):2073-2087. PubMed
11.Innocenti F, Ou FS, Qu X, et al. Mutational analysis of patients With colorectal cancer in CALGB/SWOG 80405 identifies new roles of microsatellite instability and tumor mutational burden for patient outcome. J Clin Oncol. 2019;37(14):1217-1227. PubMed
12.Tougeron D, Sueur B, Zaanan A, et al. Prognosis and chemosensitivity of deficient MMR phenotype in patients with metastatic colorectal cancer: an AGEO retrospective multicenter study. Int J Cancer. 2020;147(1):285-296. PubMed
13.Clinical study report: P177V01MK3475. A phase III study of pembrolizumab (MK-3475) vs. chemotherapy in microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) stage IV colorectal carcinoma (KEYNOTE-177) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme; 2020 May 13.
14.Systematic literature review and network meta-analysis for treatments of untreated, unresectable or metastatic, microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) for colorectal cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor's submission: Keytruda (pembrolizumab) powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada; 2020.
15.Clark JW, Grothey A. Systemic therapy for nonoperable metastatic colorectal cancer: selecting the initial therapeutic approach. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Feb 13.
16.Clark JW, Grothey A. Systemic chemotherapy for metastatic colorectal cancer: general principles. In: Post.T.W., ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Feb 13.
17.PrKeytruda® (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada; 2020 Jul 20.
18.FDA approves pembrolizumab for first-line treatment of MSI-H/dMMR colorectal cancer. Silver Spring (MD): US Food and Drug Administration; 2020: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-first-line-treatment-msi-hdmmr-colorectal-cancer. Accessed 2021 Mar 8.
19.European Public Assessment Report (EPAR): Keytruda (pembrolizumab). Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/medicines/human/EPAR/keytruda. Accessed 2021 Mar 8.
20.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
21.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2020 Dec 18.
22.Musoro JZ, Sodergren SC, Coens C, et al. Minimally important differences for interpreting the EORTC QLQ-C30 in patients with advanced colorectal cancer treated with chemotherapy. Colorectal Dis. 2020;07:07.
23.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2020 Oct 13.
24.León LF, Lin R, Anderson KM. On weighted log-rank combination tests and companion Cox model estimators. Stat Biosci. 2020;12:225-245.
25.Latimer NR, Henshall C, Siebert U, Bell H. Treatment switching: statistical and decision-making challenges and approaches. Int J Technol Assess Health Care. 2016;32(3):160-166. PubMed
26.Jansen JP, Cope S. Meta-regression models to address heterogeneity and inconsistency in network meta-analysis of survival outcomes. BMC Med Res Methodol. 2012;12(1):152. PubMed
27.Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol. 2011;11(1):61. PubMed
28.Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
29.Ye LC, Liu TS, Ren L, et al. Randomized controlled trial of cetuximab plus chemotherapy for patients with KRAS wild-type unresectable colorectal liver-limited metastases. J Clin Oncol. 2013;31(16):1931-1938. PubMed
30.Van Cutsem E, Köhne C-H, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408-1417. PubMed
31.Tveit KM, Guren T, Glimelius B, et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol. 2012;30(15):1755-1762. PubMed
32.Bokemeyer C, Bondarenko I, Makhson A, et al. Fluorouracil, leucovorin, and oxaliplatin with and without cetuximab in the first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2009;27(5):663-671. PubMed
33.Personeni N, Rimassa L, Verusio C, et al. Prognostic factors in KRAS wild-type (wt) metastatic colorectal cancer (mCRC) patients (pts) treated with biweekly cetuximab (C) plus irinotecan, fluorouracil, and leucovorin (FOLFIRI): a phase II study [abstract]. J Clin Oncol. 2013;31(15 Suppl):e14611.
34.Qin S, Li J, Wang L, et al. Efficacy and tolerability of first-line cetuximab plus leucovorin, fluorouracil, and oxaliplatin (FOLFOX-4) versus FOLFOX-4 in patients with RAS wild-type metastatic colorectal cancer: the open-label, randomized, phase III TAILOR trial. J Clin Oncol. 2018;36(30):3031-3039. PubMed
35.des Guetz G, Mariani P, Cucherousset J, et al. Microsatellite instability and sensitivitiy to FOLFOX treatment in metastatic colorectal cancer. Anticancer Res. 2007;27(4c):2715-2719. PubMed
36.Müller CI, Schulmann K, Reinacher-Schick A, et al. Predictive and prognostic value of microsatellite instability in patients with advanced colorectal cancer treated with a fluoropyrimidine and oxaliplatin containing first-line chemotherapy. A report of the AIO Colorectal Study Group. Int J Colorectal Dis. 2008;23(11):1033-1039. PubMed
37.Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol. 2010;28(31):4697-4705. PubMed
38.Cassidy J, Clarke S, Díaz-Rubio E, et al. XELOX vs FOLFOX-4 as first-line therapy for metastatic colorectal cancer: NO16966 updated results. Br J Cancer. 2011;105(1):58-64. PubMed
39.Porschen R, Arkenau HT, Kubicka S, et al. Phase III study of capecitabine plus oxaliplatin compared with fluorouracil and leucovorin plus oxaliplatin in metastatic colorectal cancer: a final report of the AIO Colorectal Study Group. J Clin Oncol. 2007;25(27):4217-4223. PubMed
40.Hochster HS, Hart LL, Ramanathan RK, et al. Safety and efficacy of oxaliplatin and fluoropyrimidine regimens with or without bevacizumab as first-line treatment of metastatic colorectal cancer: results of the TREE Study. J Clin Oncol. 2008;26(21):3523-3529. PubMed
41.Sidhu R, Rong A, Dahlberg S. Evaluation of progression-free survival as a surrogate endpoint for survival in chemotherapy and targeted agent metastatic colorectal cancer trials. Clin Cancer Res. 2013;19(5):969-976. PubMed
42.DNA mismatch repair deficiency tumour testing for patients with colorectal cancer: recommendations. (CADTH optimal use report vol.5, no.3d). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/OP0522_dMMR_Report_Recommendations.pdf. Accessed 2021 Mar 8.
43.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
44.EORTC Quality of life: FAQs. Brussels (BE): EORTC: https://qol.eortc.org/faq/. Accessed 2021 Mar 8.
45.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
46.EORTC QLC-C30 scoring manual. Brussels (BE): EORTC; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2021 Mar 8.
47.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
48.Luo N, Fones CS, Lim SE, Xie F, Thumboo J, Li SC. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-c30): validation of English version in Singapore. Qual Life Res. 2005;14(4):1181-1186. PubMed
49.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
50.Snyder CF, Blackford AL, Sussman J, et al. Identifying changes in scores on the EORTC-QLQ-C30 representing a change in patients' supportive care needs. Qual Life Res. 2015;24(5):1207-1216. PubMed
51.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
52.Wong CK, Chen J, Yu CL, Sham M, Lam CL. Systematic review recommends the European Organization for Research and Treatment of Cancer colorectal cancer-specific module for measuring quality of life in colorectal cancer patients. J Clin Epidemiol. 2015;68(3):266-278. PubMed
53.Ganesh V, Agarwal A, Popovic M, et al. Comparison of the FACT-C, EORTC QLQ-CR38, and QLQ-CR29 quality of life questionnaires for patients with colorectal cancer: a literature review. Support Care Cancer. 2016;24(8):3661-3668. PubMed
54.Gujral S, Conroy T, Fleissner C, et al. Assessing quality of life in patients with colorectal cancer: an update of the EORTC quality of life questionnaire. Eur J Cancer. 2007;43(10):1564-1573. PubMed
55.van der Hout A, Neijenhuijs KI, Jansen F, et al. Measuring health-related quality of life in colorectal cancer patients: systematic review of measurement properties of the EORTC QLQ-CR29. Support Care Cancer. 2019;27(7):2395-2412. PubMed
56.Whistance RN, Conroy T, Chie W, et al. Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer. 2009;45(17):3017-3026. PubMed
57.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
58.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
59.Teckle P, Peacock S, McTaggart-Cowan H, et al. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health Qual Life Outcomes. 2011;9:106. PubMed
60.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: January 5, 2021
Alerts: Bi-weekly search updates until project completion
Study types: All study types
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
? | Truncation symbol for one or no characters only |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ab | Abstract |
.dq. | Candidate term word |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.nm. | Name of substance word |
.ot. | Original title |
.pt | Publication type |
.rn | Registry number |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Database(s):
Embase 1974 to 2021 January 04
Ovid MEDLINE(R) ALL 1946 to January 04, 2021
Search strategy:
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,ot,kf,hw,rn,nm.
exp Colorectal neoplasms/
((colorectal or colonic or colitis-associated or sigmoid* or colon or rectal or rectum or anus or anal or perianal or peri-anal or circumanal or circum-anal or recti or pararectal or para-rectal or retrorectal or retro-rectal or mesocolon or meso-colon) adj4 (neoplas* or tumo?r* or cancer* or carcinoma* or adenoma*)).ti,ab,kf.
((adenomatous adj4 polypos*) and (colus or coli or colon or familial or intestinal)).ti,ab,kf.
(familial adj4 ademonatous adj4 (syndrome* or coli or colon or polypos* or intestinal)).ti,ab,kf.
(familial adj4 polypos* adj4 (coli or colus or colon or syndrome*)).ti,ab,kf.
(familial multiple polypos* or familial intestinal polypos* or myh-associated polypos* or polypos* col*).ti,ab,kf.
(hereditary polypos* adj4 (coli or colus or colon)).ti,ab,kf.
((Gardner* or Lynch) adj4 syndrome*).ti,ab,kf.
or/2-9
1 and 10
11 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kw,dq.
13 or 14
exp Colon Tumor/ or exp Rectum Tumor/
((colorectal or colonic or colitis-associated or sigmoid* or colon or rectal or rectum or anus or anal or perianal or peri-anal or circumanal or circum-anal or recti or pararectal or para-rectal or retrorectal or retro-rectal or mesocolon or meso-colon) adj4 (neoplas* or tumo?r* or cancer* or carcinoma* or adenoma*)).ti,ab,kw,dq.
((adenomatous adj4 polypos*) and (colus or coli or colon or familial or intestinal)).ti,ab,kw,dq.
(familial adj4 ademonatous adj4 (syndrome* or Coli or colon or polypos* or intestinal)).ti,ab,kw,dq.
(familial adj4 polypos* adj4 (coli or colus or colon or syndrome*)).ti,ab,kw,dq.
(familial multiple polypos* or familial intestinal polypos* or myh-associated polypos* or polypos* col*).ti,ab,kw,dq.
(hereditary polypos* adj4 (coli or colus or colon)).ti,ab,kw,dq.
((Gardner* or Lynch) adj4 syndrome*).ti,ab,kw,dq.
or/16-23
15 and 24
25 use oemezd
26 not (conference abstract or conference review).pt.
12 or 27
remove duplicates from 28
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | pembrolizumab AND colorectal cancer]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab AND colorectal cancer]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab AND colorectal cancer]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab AND colorectal cancer]
Canadian Cancer Trials
Produced by the Canadian Partnership Against Cancer Corporation. Targeted search used to capture registered clinical trials.
[Search terms -- pembrolizumab AND colorectal cancer]
Grey Literature
Search dates: December 14 to 23, 2020
Keywords: Keytruda, pembrolizumab, colorectal cancer
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Hirano H, Takashima A, Hamaguchi T, Shida D, Kanemitsu Y, Colorectal Cancer Study Group of the Japan Clinical Oncology G. Current status and perspectives of immune checkpoint inhibitors for colorectal cancer. Jpn J Clin Oncol. 2021 Jan 01;51(1):10-19. | Review study |
Jacobi EM, Landon G, Broaddus RR, Roy-Chowdhuri S. Evaluating mismatch repair/microsatellite instability status using cytology effusion specimens to determine eligibility for immunotherapy. Arch Pathol Lab Med. 2021 Jan 01;145(1):46-54. | Study design |
Li F, Li J, Yin K, et al. CS1003, a novel human and mouse cross-reactive PD-1 monoclonal antibody for cancer therapy. Acta Pharmacol Sin. 2021 Jan;42(1):142-148. | Study design |
Almquist DR, Ahn DH, Bekaii-Saab TS. The role of immune checkpoint inhibitors in colorectal adenocarcinoma. Biodrugs. 2020 Jun;34(3):349-362. | Review study |
Andre T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020 12 03;383(23):2207-2218. | Included |
PD-1 inhibitor bests chemo for colorectal cancer. Cancer Discov. 2020 Jul;10(7):OF2. | Review study |
Ashitomi Y, Yano M, Kono M, et al. Undifferentiated carcinoma of the transverse colon with rhabdoid features that developed during treatment of non-small cell lung carcinoma with pembrolizumab: a case report. Surg Case Rep. 2020 Aug 03;6(1):196. | Study design |
Bekki T, Takakura Y, Kochi M, et al. A case of isolated adrenocorticotropic hormone deficiency caused by pembrolizumab. Case Rep. 2020 Jan-Apr;13(1):200-206. | Study design |
Carvalho JP, Del Giglio A, Achatz MI, Carvalho FM. Complete clinical response in stage IVB endometrioid endometrial carcinoma after first-line pembrolizumab therapy: report of a case with isolated loss of PMS2 protein. Case rep. 2020 Sep-Dec;13(3):1067-1074. | Incorrect patient population |
Chan JK, Lakomy DS, McDonald Y, Kapp DS. Long-term durable responses after pembrolizumab immunotherapy for recurrent, resistant endometrial cancer. Gynecologic Oncol Rep. 2020 August;33(100581). | Incorrect patient population |
Chan KH, Lakkasani S, Ramahi A, Shaaban HS. Hyperprogressive disease in an advanced stage colon cancer patient on pembrolizumab: a case report. Cureus. 2020 Apr 21;12(4):e7764. | Study design |
Chen S, Zhang X, Shen L, et al. Transcatheter arterial infusion of anti-programmed cell death 1 antibody pembrolizumab combined with temozolomide or nab-paclitaxel in patient with primary anorectal malignant melanoma: four case reports. J Cancer Res Ther. 2020;16(2):387-392. | Incorrect patient population |
Cooksley T, Gupta A, Al-Sayed T, Lorigan P. Emergency presentations in patients treated with immune checkpoint inhibitors. Eur J Cancer. 2020 May;130:193-197. | Incorrect patient population |
Coupez D, Hulo P, Touchefeu Y, Bossard C, Bennouna J. Pembrolizumab for the treatment of colorectal cancer. Expert Opin Biol Ther. 2020 03;20(3):219-226. | Review study |
da Silva CM, Shimba D, Oishi D, Cagnacci A, de Gouvea A, Ades F. VUS-type alteration in POLD1 and microsatellite instability in a metastatic luminal B breast cancer patient. Ecancermedicalscience. 2020;14:1002. | Incorrect patient population |
da Silva CM, Shimba D, Oishi D, Cagnacci A, de Gouvea ACRC, Ades F. VUS-type alteration in POLD1 and microsatellite instability in a metastatic luminal B breast cancer patient. Ecancermedicalscience. 2020 21 Jan;14(1002). | Incorrect patient population |
Das S, Allen A, Berlin J. Immunotherapy after immunotherapy: response rescue in a patient with microsatellite instability-high colorectal cancer post-pembrolizumab. Clin Colorectal Cancer. 2020 06;19(2):137-140. | Study design |
De Souza A. Finding the hot spot: identifying immune sensitive gastrointestinal tumours. Transl. 2020;5:48. | Review study |
Demisse R, Damle N, Kim E, et al. Neoadjuvant immunotherapy-based systemic treatment in MMR-deficient or MSI-high rectal cancer: case series. J Natl Compr Canc Netw. 2020 Jul;18(7):798-804. | Study design |
Demisse R, Damle N, Kim E, et al. Neoadjuvant immunotherapy-based systemic treatment in MMR-deficient or MSI-high rectal cancer: case series. JNCCN. 2020 July;18(7):798-804. | Study design |
Elia G, Ferrari SM, Galdiero MR, et al. New insight in endocrine-related adverse events associated to immune checkpoint blockade. Best Pract Res Clin Endocrinol Metab. 2020 01;34(1):101370. | Review study |
Eso Y, Seno H. Current status of treatment with immune checkpoint inhibitors for gastrointestinal, hepatobiliary, and pancreatic cancers. Therap Adv Gastroenterol. 2020;13:1756284820948773. | Review study |
Fischer LE, Heinemann V. Systemic treatment of metastatic anal canal carcinoma. [German]. Onkologe. 2020 01 Apr;26(4):356-361. | Review study |
Florou V, Nevala-Plagemann C, Barber KE, Mastroianni JN, Cavalieri CC, Garrido-Laguna I. Treatment rechallenge with checkpoint inhibition in patients with mismatch repair-deficient pancreatic cancer after planned treatment interruption. JCO Precis Oncol. 2020;4:780-784. | Incorrect patient population |
Galluzzi L. Targeting mutant KRAS for immunogenic cell death induction. Trends Pharmacol Sci. 2020 01;41(1):1-3. | Incorrect intervention |
Gao F, Yang C. Anti-VEGF/VEGFR2 monoclonal antibodies and their combinations with PD-1/PD-l1 inhibitors in clinic. Curr Cancer Drug Targets. 2020;20(1):3-18. | Incorrect intervention |
Geva R, Voskoboynik M, Dobrenkov K, et al. First-in-human phase 1 study of MK-1248, an anti-glucocorticoid-induced tumour necrosis factor receptor agonist monoclonal antibody, as monotherapy or with pembrolizumab in patients with advanced solid tumours. Cancer. 2020 Nov 15;126(22):4926-4935. | Incorrect intervention |
Giglio D, Berntsson H, Fred A, Ny L. Immune checkpoint inhibitor-induced polymyositis and myasthenia gravis with fatal outcome. Case Rep. 2020 Sep-Dec;13(3):1252-1257. | Study design |
Giraud N, Popinat G, Regaieg H, Tonnelet D, Vera P. Positron-emission tomography-guided radiation therapy: ongoing projects and future hopes. Cancer Radiother. 2020 Aug;24(5):437-443. | Incorrect intervention |
Golshani G, Zhang Y. Advances in immunotherapy for colorectal cancer: a review. Therap Adv Gastroenterol. 2020;13:1756284820917527. | Review study |
Graham LS, Montgomery B, Cheng HH, et al. Mismatch repair deficiency in metastatic prostate cancer: Response to PD-1 blockade and standard therapies. PLoS ONE [Electronic Resource]. 2020;15(5):e0233260. | Incorrect patient population |
Grothey A. Pembrolizumab in MSI-H-dMMR advanced colorectal cancer - a new standard of care. N Engl J Med. 2020 12 03;383(23):2283-2285. | Review study |
Haanen JB, Blank CU. Prognostic and predictive role of the tumour immune landscape. Q J Nucl Med Mol Imaging. 2020 June;64(2):143-151. | Incorrect outcome |
Hiraki T, Hatanaka M, Arimura A, et al. Granulomatous/sarcoid-like reactions in the setting of programmed cell death-1 inhibition: a potential mimic of disease recurrence. J Cutan Pathol. 2020 Feb;47(2):154-160. | Study design |
Hirsch D, Gaiser T, Merx K, et al. Clinical responses to PD-1 inhibition and their molecular characterization in six patients with mismatch repair-deficient metastatic cancer of the digestive system. J Cancer Res Clin Oncol. 2020 Aug 09. | Study design |
Hurley PJ, Bose N, Jha G, et al. Immunoglobulin restores immune responses to BTH1677 in patients with low levels of antibodies to beta-glucan. Anticancer Res. 2020 Mar;40(3):1467-1473. | Incorrect intervention |
Huynh JC, Schwab E, Ji J, et al. Recent advances in targeted therapies for advanced gastrointestinal malignancies. Cancers (Basel). 2020 May 06;12(5):06. | Review study |
Imbert C, Montfort A, Fraisse M, et al. Resistance of melanoma to immune checkpoint inhibitors is overcome by targeting the sphingosine kinase-1. Nature Commun. 2020 01 23;11(1):437. | Incorrect patient population |
Johncilla M, Grover S, Zhang X, Jain D, Srivastava A. Morphological spectrum of immune check-point inhibitor therapy-associated gastritis. Histopathology. 2020 01 Mar;76(4):531-539. | Study design |
Ju JY, Dibbern ME, Mahadevan MS, Fan J, Kunk PR, Stelow EB. Mismatch repair protein deficiency/microsatellite instability is rare in cholangiocarcinomas and associated with distinctive morphologies. Am J Clin Pathol. 2020 04 15;153(5):598-604. | Study design |
Jung G, Benitez-Ribas D, Sanchez A, Balaguer F. Current treatments of metastatic colorectal cancer with immune checkpoint inhibitors-2020 update. J Clin Med. 2020 Oct 31;9(11):31. | Review study |
Karki S, Umar S, Kasi A. Treating colorectal cancer with immunotherapy: implications for single versus combination therapy. Curr Colorectal Cancer Rep. 2020 Oct;16(5):107-117. | Review study |
Kasi PM. Circulating tumour DNA and plasma microsatellite instability during PD-1 blockade. J Gastrointest Oncol. 2020 01 Aug;11(4):826-828. | Study design |
Kawazoe A, Kuboki Y, Shinozaki E, et al. Multicenter phase I/II trial of napabucasin and pembrolizumab in patients with metastatic colorectal cancer (EPOC1503/SCOOP Trial). Clin Cancer Res. 2020 Nov 15;26(22):5887-5894. | Incorrect intervention |
Khaddour K, Fields RC, Ansstas M, Rosman IS, Ansstas G. Metachronous cutaneous squamous cell carcinoma in a young patient as the only presenting symptom to uncover Lynch syndrome with MLH1 Germline mutation. Hered Cancer Clin Pract. 2020 Nov 16;18(1):23. | Incorrect intervention |
Kichloo A, Albosta MS, McMahon S, et al. Pembrolizumab-induced diabetes mellitus presenting as diabetic ketoacidosis in a patient with metastatic colonic adenocarcinoma. J Investig Med High Impact Case Rep. 2020;8. | Study design |
Kim H, Liew D, Goodall S. Cost-effectiveness and financial risks associated with immune checkpoint inhibitor therapy. Br J Clin Pharmacol. 2020 01 Sep;86(9):1703-1710. | Review study |
Kishore C, Bhadra P. Current advancements and future perspectives of immunotherapy in colorectal cancer research. Eur J Pharmacol. 2020 Dec 29;893:173819. | Review study |
Kooshkaki O, Derakhshani A, Safarpour H, et al. The latest findings of PD-1/PD-L1 inhibitor application in gynecologic cancers. Int J Mol Sci. 2020 Jul 16;21(14):16. | Incorrect patient population |
Korpics MC, Polley MY, Bhave SR, et al. A validated T cell radiomics score is associated with clinical outcomes following multisite SBRT and pembrolizumab. Int J Radiat Oncol Biol Phys. 2020 1 Sep;108(1):189-195. | Incorrect intervention |
Kreidieh M, Mukherji D, Temraz S, Shamseddine A. Expanding the scope of immunotherapy in colorectal cancer: current clinical approaches and future directions. Biomed Res Int. 2020:9037217. | Review study |
Krishnan T, Tomita Y, Roberts-Thomson R. A retrospective analysis of eosinophilia as a predictive marker of response and toxicity to cancer immunotherapy. Future Sci OA. 2020 December;6 (10)(FSO608). | Study design |
Lapman S, Whittier WL, Parikh R, et al. Immune checkpoint inhibitor-associated renal amyloid A amyloidosis: a case series and review of the literature. J Onco-Nephrol 2020 01 Feb;4(1-2):52-58. | Study design |
Le DT, Kim TW, Van Cutsem E, et al. Phase II open-label study of pembrolizumab in treatment-refractory, microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: KEYNOTE-164. J Clin Oncol. 2020 01 01;38(1):11-19. | Incorrect patient population |
Lin AC, Shriver EM. The role of pembrolizumab in the treatment of sebaceous carcinoma. Int Ophthalmol Clin. 2020 01 Mar;60(2):39-46. | Incorrect patient population |
Mancuso JG, Foulkes WD, Pollak MN. Cancer immunoprevention: a case report raising the possibility of "immuno-interception." Cancer Prev Res (Phila Pa). 2020 04;13(4):351-356. | Study design |
Marabelle A, Fakih M, Lopez J, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020 10;21(10):1353-1365. | Incorrect patient population |
Marabelle A, Le DT, Ascierto PA, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair-deficient cancer: Results from the phase II KEYNOTE-158 study. J Clin Oncol. 2020;38(1):1-10. | Incorrect patient population |
Marin JJG, Macias RIR, Monte MJ, et al. Cellular mechanisms accounting for the refractoriness of colorectal carcinoma to pharmacological treatment. Cancers (Basel). 2020 Sep 11;12(9):11. | Study design |
Marquez-Rodas I, Longo F, Rodriguez-Ruiz ME, et al. Intratumoural nanoplexed poly I:C BO-112 in combination with systemic anti-PD-1 for patients with anti-PD-1-refractory tumours. Sci Transl Med. 2020 14 Oct;12 (565)(eabb0391). | Incorrect patient population |
Marsh RL, Kolodney JA, Iyengar S, et al. Formation of eruptive cutaneous squamous cell carcinomas after programmed cell death protein-1 blockade. JAAD Case Reports. 2020 May;6(5):390-393. | Incorrect patient population |
Mendes D, Rigueiro G, Silva RS, et al. Intensive safety monitoring program of antineoplastic medicines: a pilot study in a Portuguese oncology hospital. J Oncol Pharm Pract. 2020 01 Jan;26(1):133-140. | Incorrect patient population |
Mizuno N, Doi T, Grande E, et al. Efficacy and safety of pembrolizumab in previously treated advanced neuroendocrine tumours: results from the phase II KEYNOTE-158 study. Clin Cancer Res. 2020 01 May;26(9):2124-2130. | Incorrect patient population |
Morse MA, Hochster H, Benson A. Perspectives on treatment of metastatic colorectal cancer with immune checkpoint inhibitor therapy. Oncologist. 2020 01;25(1):33-45. | Review study |
Mosele F, Remon J, Mateo J, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol. 2020 11;31(11):1491-1505. | Study design |
Mutlu L, Khadraoui W, Khader T, Menderes G. Robotic Tumour debulking off external iliac vessels for the management of recurrent ovarian cancer. J Minim Invasive Gynecol. 2020 Jul - Aug;27(5):1021-1022. | Incorrect patient population |
Nguyen M, Tipping Smith S, Lam M, et al. An update on the use of immunotherapy in patients with colorectal cancer. Expert Rev Gastroenterol Hepatol. 2020 Nov 09:1-14. | Review study |
Ntanasis-Stathopoulos I, Kyriazoglou A, Dimopoulos MA, Gavriatopoulou M. Clinical biomarkers directing the management of patients with colon and lung cancer (beyond on-cogene-addicted NSCLC). Forum Clin Oncol. 2020 01 Mar;11(1):3-6. | Study design |
Palaskas N, Lopez-Mattei J, Durand JB, Iliescu C, Deswal A. Immune checkpoint inhibitor myocarditis: pathophysiological characteristics, diagnosis, and treatment. J Am Heart Assoc. 2020 21 Jan;9 (2)(e013757). | Incorrect patient population |
Park D, Airi R, Sherman M. Microsatellite instability driven metastatic parathyroid carcinoma managed with the anti-PD1 immunotherapy, pembrolizumab. BMJ Case Rep. 2020 Sep 23;13(9):23. | Incorrect patient population |
Patil NR, Khan GN. Exceptional response to a single cycle of immunotherapy in a Lynch Syndrome patient with metastatic pancreatic adenocarcinoma. Am J Case Rep. 2020 Jul 13;21:e923803. | Incorrect patient population |
Payandeh Z, Khalili S, Somi MH, et al. PD-1/PD-L1-dependent immune response in colorectal cancer. J Cell Physiol. 2020 Jul;235(7-8):5461-5475. | Review study |
Peer CJ, Goldstein DA, Goodell JC, Nguyen R, Figg WD, Ratain MJ. Opportunities for using in silico-based extended dosing regimens for monoclonal antibody immune checkpoint inhibitors. Br J Clin Pharmacol. 2020 01 Sep;86(9):1769-1777. | Study design |
Pestana RC, Sen S, Hobbs BP, Hong DS. Histology-agnostic drug development - considering issues beyond the tissue. Nature Reviews Clinical Oncology. 2020 01 Sep;17(9):555-568. | Study design |
Phuong L, Rajdev L. Immunotherapy in anal cancer. Curr Oncol Rep. 2020 Jul 11;22(9):94. | Review study |
Picard E, Verschoor CP, Ma GW, Pawelec G. Relationships between immune landscapes, genetic subtypes and responses to immunotherapy in colorectal cancer. Front Immunol. 2020;11:369. | Review study |
Raghavan AM, Giffen ZC, Irwin PM, Mostafa HI, Buck BJ. PD-L1 pathway as a novel target in carcinosarcoma of the kidney and renal pelvis. Urol Case Rep. 2020 Nov;33:101261. | Incorrect patient population |
Razak AR, Cleary JM, Moreno V, et al. Safety and efficacy of AMG 820, an anti-colony-stimulating factor 1 receptor antibody, in combination with pembrolizumab in adults with advanced solid tumours. J Immunother Cancer. 2020 Oct;8(2). | Incorrect intervention |
Reddy TP, Khan U, Burns EA, Abdelrahim M. Chemotherapy rechallenge in metastatic colon cancer: a case report and literature review. World J Clin Oncol. 2020 Nov 24;11(11):959-967. | Review study |
Roth MT, Das S. Pembrolizumab in unresectable or metastatic MSI-high colorectal cancer: safety and efficacy. Expert Rev Anticancer Ther. 2020 Dec 04:1-10. | Review study |
Sahin IH. Fine-tuning immunotherapy in MMR-D/MSI-H colorectal cancer. Colorectal Cancer. 2020;8 (4)(CRC12). | Review study |
Sahin IH. Immune checkpoint inhibitor response in mismatch repair-deficient colorectal cancer and other solid tumours: Is it truly disease-agnostic? Colorectal Cancer. 2020 December;9 (4)(0020). | Review study |
Sahin IH, Kane SR, Brutcher E, et al. Safety and efficacy of immune checkpoint inhibitors in patients with cancer living with HIV: a perspective on recent progress and future needs. JCO Oncol Pract. 2020 Jun;16(6):319-325. | Review study |
Shazib MA, Woo SB, Sroussi H, et al. Oral immune-related adverse events associated with PD-1 inhibitor therapy: a case series. Oral Dis. 2020 01 Mar;26(2):325-333. | Study design |
Shetty I, Fuller S, Raygada M, et al. Adrenocortical carcinoma masquerading as pheochromocytoma: a histopathologic dilemma. Endocrinol Diabetes Metab Case Rep. 2020 Jan 08. | Incorrect patient population |
Subbiah V, Solit DB, Chan TA, Kurzrock R. The FDA approval of pembrolizumab for adult and pediatric patients with tumour mutational burden (TMB) >=10: a decision centered on empowering patients and their physicians. Ann Oncol. 2020 Sep;31(9):1115-1118. | Study design |
Sun BL. Current microsatellite instability testing in management of colorectal cancer. Clin Colorectal Cancer. 2020 Aug 10. | Study design |
Sun J, Zheng Y, Mamun M, Li X, Chen X, Gao Y. Research progress of PD-1/PD-L1 immunotherapy in gastrointestinal tumours. Biomed Pharmacother. 2020 Sep;129:110504. | Review study |
Tapia Rico G, Chan MM, Loo KF. The safety and efficacy of immune checkpoint inhibitors in patients with advanced cancers and pre-existing chronic viral infections (Hepatitis B/C, HIV): a review of the available evidence. Cancer Treat Rev. 2020 June;86(102011). | Review study |
Terashima T. Microsatellite instability-high in Japanese patients with hepatocellular carcinoma. Hepatol Res. 2020 01 Jul;50(7):773-774. | Incorrect patient population |
Thomas J, Leal A, Overman MJ. Clinical development of immunotherapy for deficient mismatch repair colorectal cancer. Clin Colorectal Cancer. 2020 06;19(2):73-81. | Study design |
Tolba MF. Revolutionizing the landscape of colorectal cancer treatment: the potential role of immune checkpoint inhibitors. Int J Cancer. 2020 Dec 01;147(11):2996-3006. | Review study |
Tuo Z, Zheng X, Zong Y, et al. HK3 is correlated with immune infiltrates and predicts response to immunotherapy in non-small cell lung cancer. Clin Transl Med. 2020 Jan;10(1):319-330. | Incorrect patient population |
Wang C, Chevalier D, Saluja J, Sandhu J, Lau C, Fakih M. Regorafenib and nivolumab or pembrolizumab combination and circulating tumour DNA response assessment in refractory microsatellite stable colorectal cancer. Oncologist. 2020 Aug;25(8):e1188-e1194. | Incorrect intervention |
Wang Z, Wu X. Study and analysis of antitumour resistance mechanism of PD1/PD-L1 immune checkpoint blocker. Cancer Medicine. 2020 01 Nov;9(21):8086-8121. | Study design |
Wu Q, Chu Q, Zhang H, et al. Clinical outcomes of coronavirus disease 2019 (COVID-19) in cancer patients with prior exposure to immune checkpoint inhibitors. Cancer Commun. 2020 01 Aug;40(8):374-379. | Incorrect patient population and intervention |
Yarchoan M, Huang CY, Zhu Q, et al. A phase 2 study of GVAX colon vaccine with cyclophosphamide and pembrolizumab in patients with mismatch repair proficient advanced colorectal cancer. Cancer Medicine. 2020 02;9(4):1485-1494. | Incorrect intervention |
Yoshino T, Pentheroudakis G, Mishima S, et al. JSCO-ESMO-ASCO-JSMO-TOS: international expert consensus recommendations for tumour-agnostic treatments in patients with solid tumours with microsatellite instability or NTRK fusions. Ann Oncol. 2020 July;31(7):861-872. | Study design |
Zen Y, Chen YY, Jeng YM, Tsai HW, Yeh MM. Immune-related adverse reactions in the hepatobiliary system: second-generation check-point inhibitors highlight diverse histological changes. Histopathology. 2020 01 Feb;76(3):470-480. | Study design |
Zhang CH, Li M, Lin YP, Gao Q. Systemic therapy for hepatocellular carcinoma: advances and hopes. Curr Gene Ther. 2020;20(2):84-99. | Incorrect patient population |
Zhao B, Zhao H, Zhao J. Efficacy of PD-1/PD-L1 blockade monotherapy in clinical trials. Ther Adv Med Oncol. 2020;12. | Review study |
Abida W, Cheng ML, Armenia J, et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 2019 Apr 01;5(4):471-478. | Incorrect patient population |
Aguilar PB, Peixoto R, Lim F, Wan BA, Silva MF. Management of anal cancer in Latin America. J Pain Manag. 2019;12(4):333-343. | Review study |
Arora S, Velichinskii R, Lesh RW, et al. Existing and emerging biomarkers for immune checkpoint immunotherapy in solid tumours. Adv Ther. 2019 10;36(10):2638-2678. | Review study |
Ayers M, Nebozhyn M, Cristescu R, et al. Molecular profiling of cohorts of tumour samples to guide clinical development of pembrolizumab as monotherapy. Clin Cancer Res. 2019 01 Mar;25(5):1564-1573. | Study design |
Badran YR, Cohen JV, Brastianos PK, Parikh AR, Hong TS, Dougan M. Concurrent therapy with immune checkpoint inhibitors and TNFalpha blockade in patients with gastrointestinal immune-related adverse events. Journal for ImmunoTherapy of Cancer. 2019 22 Aug;7 (1)(226). | Incorrect intervention |
Banerjee N, Hossain F, Wirtschafter E, Fathizadeh P. Pembrolizumab in the treatment of microsatellite instability-high sebaceous carcinoma: a case report with review of the literature. JCO Precis Oncol. 2019;3:61-65. | Incorrect patient population |
Barbacid M. On the right TRK: from oncogene discovery to cancer therapeutics. Ann Oncol. 2019 November;30(Suppl 8):viii3-viii4. | Study design |
Calapre L, Warburton L, Millward M, Gray ES. Circulating tumour DNA (ctDNA) as a biomarker in metachronous melanoma and colorectal cancer- a case report. BMC Cancer. 2019 Nov 14;19(1):1109. | Study design |
Chakrabarti S, Huebner LJ, Finnes HD, et al. Intratumoural CD3+ and CD8+ T-cell densities in patients with DNA mismatch repair-deficient metastatic colorectal cancer receiving programmed cell death-1 blockade. JCO Precision Oncology. 2019;3. | Study design |
Cohen R, Pellat A, Boussion H, et al. Immunotherapy and metastatic colorectal cancers with microsatellite instability or mismatch repair deficiency. Bull Cancer. 2019 Feb;106(2):137-142. | Review study |
Courand PY, Bouali A, Harbaoui B, Cautela J, Thuny F, Lantelme P. [Myocarditis: uncommon but severe toxicity of immune checkpoint inhibitors]. Bull Cancer. 2019 Nov;106(11):1050-1056. | Review study |
D'Alterio C, Buoncervello M, Ierano C, et al. Targeting CXCR4 potentiates anti-PD-1 efficacy modifying the tumour microenvironment and inhibiting neoplastic PD-1. J Exp Clin Cancer Res. 2019 Oct 28;38(1):432. | Study design |
Damotte D, Warren S, Arrondeau J, et al. The tumour inflammation signature (TIS) is associated with anti-PD-1 treatment benefit in the CERTIM pan-cancer cohort. J Transl Med. 2019 04 Nov;17 (1)(357). | Study design |
Damsky W, Jilaveanu L, Turner N, et al. B cell depletion or absence does not impede anti-tumour activity of PD-1 inhibitors. J Immunother Cancer. 2019 06 14;7(1):153. | Incorrect patient population |
Doyle LA, Nowak JA, Nathenson MJ, et al. Characteristics of mismatch repair deficiency in sarcomas. Mod Pathol. 2019 07;32(7):977-987. | Study design |
Du Rusquec P, De Calbiac O, Robert M, Campone M, Frenel JS. Clinical utility of pembrolizumab in the management of advanced solid tumours: An evidence-based review on the emerging new data. Cancer Manag Res. 2019;11:4297-4312. | Review study |
Eckstein M, Gupta S. New insights in predictive determinants of the tumour immune microenvironment for immune checkpoint inhibition: a never ending story? Ann Translat Med. 2019;7 (Suppl 3)(S135). | Review study |
Evert K, Stiegler C, Schafer C, et al. [Successful pembrolizumab therapy in metastasized adenosquamous carcinoma of the colon]. Pathologe. 2019 Sep;40(5):540-545. | Study design |
Fan L, Li Y, Chen JY, Zheng YF, Xu XM. Immune checkpoint modulators in cancer immunotherapy: Recent advances and combination rationales. Cancer Lett. 2019 1 Aug;456:23-28. | Review study |
Farmer JR. Testing immune-related adverse events in cancer immunotherapy. Clin Lab Med. 2019 Dec;39(4):669-683. | Study design |
Feng Y, Cao Y, Yuan M, Chen R, Ji X, Hu X. Different responses to anti-programmed cell death protein 1 (PD-1) immunotherapy in a patient with Lynch syndrome and metachronous urothelial and colon cancer: a case report. Oncol Lett. 2019 Nov;18(5):5085-5090. | Study design |
Fojo AT. Immunotherapy for adrenocortical cancer. Semin Oncol. 2019 Feb;46(1):1-2. | Incorrect patient population |
Fong W, To KKW. Drug repurposing to overcome resistance to various therapies for colorectal cancer. Cell Mol Life Sci. 2019 Sep;76(17):3383-3406. | Review study |
Franke AJ, Skelton WP, Starr JS, et al. Immunotherapy for colorectal cancer: a review of current and novel therapeutic approaches. J Natl Cancer Inst. 2019 11 01;111(11):1131-1141. | Review Study |
Gallan AJ, Alexander E, Reid P, Kutuby F, Chang A, Henriksen KJ. Renal vasculitis and pauci-immune glomerulonephritis associated with immune checkpointiInhibitors. Am J Kidney Dis. 2019 12;74(6):853-856. | Study design |
Ganesh K, Stadler ZK, Cercek A, et al. Immunotherapy in colorectal cancer: rationale, challenges and potential. Nat Rev Gastroenterol Hepatol. 2019 06;16(6):361-375. | Review study |
Garcia CR, Jayswal R, Adams V, Anthony LB, Villano JL. Multiple sclerosis outcomes after cancer immunotherapy. Clin Transl Oncol. 2019 Oct;21(10):1336-1342. | Incorrect patient population |
Gong J, Robertson MD, Kim E, et al. Efficacy of PD-1 Blockade in refractory microsatellite-stable colorectal cancer with high tumour mutation burden. Clin Colorectal Cancer. 2019 12;18(4):307-309. | Incorrect patient population |
Goodman AM, Sokol ES, Frampton GM, Lippman SM, Kurzrock R. Microsatellite-stable tumours with high mutational burden benefit from immunotherapy. Cancer Immunol Res. 2019 10;7(10):1570-1573. | Incorrect patient population |
Gurjao C, Liu D, Hofree M, et al. Intrinsic resistance to immune checkpoint blockade in a mismatch repair-deficient colorectal cancer. Cancer Immunol Res. 2019 08;7(8):1230-1236. | Study design |
Hamilton B, Xu K, Honeyball F, Balakrishnar B, Zielinski R. Patterns of immunotherapy use and management of toxicities in regional and tertiary settings. Intern Med J. 2019;49(8):1010-1015. | Review study |
Haslam A, Prasad V. Estimation of the percentage of us patients with cancer who are eligible for and respond to checkpoint inhibitor immunotherapy drugs. JAMA Network Open. 2019 May;2 (5)(e192535). | Study design |
Hatakeyama K, Nagashima T, Ohshima K, et al. Mutational burden and signatures in 4000 Japanese cancers provide insights into tumourigenesis and response to therapy. Cancer Sci. 2019;110(8):2620-2628. | Incorrect intervention |
Hendifar AE, Larson BK, Rojansky R, et al. Pancreatic cancer 'mismatch' in Lynch syndrome. BMJ Open Gastroenterol. 2019;6(1):e000274. | Incorrect patient population |
Henick BS, Ingham M, Shirazi M, et al. Assay complementarity to overcome false-negative testing for microsatellite instability/mismatch repair deficiency: a pembrolizumab-sensitive intimal sarcoma. JCO Precis Oncol. 2019;3:570-574. | Study design |
Hwang SJE, Park JJW, Wakade D, Chou S, Byth K, Fernandez-Penas P. Cutaneous adverse events of anti-programmed death 1 antibodies combined with anti-cytotoxic T-lymphocyte-Associated protein 4 therapy use in patients with metastatic melanoma. Melanoma Res. 2019 01 Apr;29(2):172-177. | Incorrect patient population |
Jiang K, Martens B, Meyer L, Truong K, Lauwers GY. A mismatch repair-deficient and HPV-negative anorectal squamous cell carcinoma. Virchows Arch. 2019 01 Jun;474(6):769-773. | Study design |
Jun J, Lee SR, Lee JY, et al. Pneumonitis and concomitant bacterial pneumonia in patients receiving pembrolizumab treatment: three case reports and literature review. Medicine. 2019 Jun;98(25):e16158. | Study design |
Kamatham S, Shahjehan F, Kasi PM. Immune checkpoint inhibitors in metastatic colorectal cancer: current status, recent advances, and future directions. Curr Colorectal Cancer Rep. 2019 15 Aug;15(4):112-121. | Review study |
Kato S, Hayashi T, Suehara Y, et al. Multicenter experience with large panel next-generation sequencing in patients with advanced solid cancers in Japan. Jpn J Clin Oncol. 2019 Feb 01;49(2):174-182. | Study design |
Katoh M. Genomic testing, tumour microenvironment and targeted therapy of Hedgehog-related human cancers. Clin Sci. 2019 04 30;133(8):953-970. | Study design |
Keating M, Giscombe L, Tannous T, Hartshorn K. Prolonged treatment response to pembrolizumab in a patient with pretreated metastatic colon cancer and Lynch Syndrome. Case Rep Oncol Med. 2019:3847672. | Study design |
Kim H, Lee JE, Hong SH, Lee MA, Kang JH, Kim IH. The effect of antibiotics on the clinical outcomes of patients with solid cancers undergoing immune checkpoint inhibitor treatment: a retrospective study. BMC Cancer. 2019 12 Nov;19 (1)(1100). | Incorrect patient population |
Kok M, Chalabi M, Haanen J. How I treat MSI cancers with advanced disease. ESMO Open. 2019;4(Suppl 2):e000511. | Study design |
Lasinska I, Mackiewicz J. Integrins as a new target for cancer treatment. Curr Med Chem Anti-Cancer Agents. 2019;19(5):580-586. | Incorrect intervention |
Lei M, Michael A, Patel S, Wang D. Evaluation of the impact of thyroiditis development in patients receiving immunotherapy with programmed cell death-1 inhibitors. J Oncol Pharm Pract. 2019 01 Sep;25(6):1402-1411. | Study design |
Llosa NJ, Luber B, Siegel N, et al. Immunopathologic stratification of colorectal cancer for checkpoint blockade immunotherapy. Cancer Immunol Res. 2019 10;7(10):1574-1579. | Study design |
Mahipal A, Tella SH, Kommalapati A, Lim A, Kim R. Immunotherapy in hepatocellular carcinoma: Is there a light at the end of the tunnel? Cancers (Basel). 2019 Aug;11 (8)(1078). | Incorrect patient population |
Marcus L, Lemery SJ, Keegan P, Pazdur R. FDA Approval Summary: pembrolizumab for the treatment of microsatellite instability-high solid tumours. Clin Cancer Res. 2019 07 01;25(13):3753-3758. | Review study |
Martin SZ, Wagner DC, Horner N, et al. Ex vivo tissue slice culture system to measure drug-response rates of hepatic metastatic colorectal cancer. BMC Cancer. 2019 01 Nov;19 (1)(1030). | Review study |
Michalarea V, Fontana E, Garces AI, et al. Pseudoprogression on treatment with immune-checkpoint inhibitors in patients with gastrointestinal malignancies: case series and short literature review. Curr Probl Cancer. 2019 10;43(5):487-494. | Study design |
Michel L, Rassaf T, Totzeck M. Cardiotoxicity from immune checkpoint inhibitors. IJC Heart Vasc. 2019 Dec;25(100420). | Review study |
Minoves M, Pepin JL, Godin-Ribuot D. Targeting intermittent hypoxia downstream pathways for biomarker discovery and new treatment perspectives in cutaneous melanoma. Eur Respir J. 2019 01 Feb;53 (2)(1802444). | Incorrect patient population |
Modest DP, Pant S, Sartore-Bianchi A. Treatment sequencing in metastatic colorectal cancer. Eur J Cancer. 2019 03;109:70-83. | Review study |
Moujaess E, Haddad FG, Eid R, Kourie HR. The emerging use of immune checkpoint blockade in the adjuvant setting for solid tumours: a review. Immunotherapy. 2019 11;11(16):1409-1422. | Review study |
Moya-Plana A, Herrera Gomez RG, Rossoni C, et al. Evaluation of the efficacy of immunotherapy for non-resectable mucosal melanoma. Cancer Immunol Immunother. 2019 Jul;68(7):1171-1178. | Incorrect patient population |
Musher B, Rahal A. Single-agent immunotherapy for two types of cancer in one patient. Ann Intern Med. 2019 02 05;170(3):210-211. | Study design |
Nishino M, Hatabu H, Hodi FS. Imaging of cancer immunotherapy: current approaches and future directions. Radiology. 2019 Jan;290(1):9-22. | Study design |
Otter S, Whitaker S, Chatterjee J, Stewart A. The human papillomavirus as a common pathogen in oropharyngeal, anal and cervical cancers. Clin Oncol. 2019 February;31(2):81-90. | Incorrect patient population |
Overman MJ. Immunotherapy in colorectal cancer with mismatch repair deficiency. Clin Adv Hematol Oncol. 2019 May;17(5):265-267. | Review study |
Parker NA, McBride C, Forge J, Lalich D. Bowel obstruction caused by colonic metastasis of lung adenocarcinoma: a case report and literature review. World J Surg Oncol. 2019 Apr 08;17(1):63. | Incorrect patient population |
Qiao G, Wang X, Zhou X, et al. Immune correlates of clinical benefit in a phase I study of hyperthermia with adoptive T cell immunotherapy in patients with solid tumours. Int J Hyperthermia. 2019 11;36(Suppl 1):74-82. | Incorrect patient population |
Ramos-Casals M, Maria A, Suarez-Almazor ME, et al. Sicca/Sjogren's syndrome triggered by PD-1/PD-L1 checkpoint inhibitors. data from the International Immunocancer Registry (ICIR). Clin Exp Rheumatol. 2019;37(Suppl 3):S114-S122. | Incorrect patient population |
Rawla P, Barsouk A, Hadjinicolaou AV, Barsouk A. Immunotherapies and targeted therapies in the treatment of metastatic colorectal cancer. Med Sci (Basel). 2019 Jul 30;7(8):30. | Review study |
Ree AH, Nygaard V, Russnes HG, et al. Responsiveness to PD-1 blockade in end-stage colon cancer with gene locus 9p24.1 copy-number gain. Cancer Immunol Res. 2019 05;7(5):701-706. | Study design |
Reichert ZR, Urrutia J, Alumkal JJ. Microsatellite instability as an emerging biomarker for checkpoint inhibitor response in advanced prostate cancer. JAMA Oncol. 2019 Apr;5(4):478-479. | Incorrect patient population |
Ruiz-Banobre J, Goel A. DNA Mismatch repair deficiency and immune checkpoint inhibitors in gastrointestinal cancers. Gastroenterology. 2019 Mar;156(4):890-903. | Review study |
Sato S, Senmaru N, Ishido K, et al. Perforation of small intestinal metastasis of lung adenocarcinoma treated with pembrolizumab: a case report. Surg Case Rep. 2019 Oct 30;5(1):166. | Study design |
Sawai Y, Katsuya Y, Shinozaki-Ushiku A, et al. Rapid temporal improvement of pembrolizumab-induced pneumonitis using the anti-TNF-alpha antibody infliximab. Drug Discov Therap. 2019;13(3):164-167. | Study design |
Schaer DA, Geeganage S, Amaladas N, et al. The folate pathway inhibitor pemetrexed pleiotropically enhances effects of cancer immunotherapy. Clin Cancer Res. 2019 12 01;25(23):7175-7188. | Incorrect patient population |
Schrock AB, Ouyang C, Sandhu J, et al. Tumour mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann Oncol. 2019 07 01;30(7):1096-1103. | Study design |
Shindo Y, Hazama S, Tsunedomi R, Suzuki N, Nagano H. Novel biomarkers for personalized cancer immunotherapy. Cancers (Basel). 2019 Sep;11 (9)(1223). | Study design |
Silberman R, Steiner DF, Lo AA, et al. Complete and prolonged response to immune checkpoint blockade in pole-mutated colorectal cancer. JCO Precis Oncol. 2019;3. | Incorrect patient population |
Singh R, Patel P, Thakker M, Sharma P, Barnes M, Montana S. Naloxone and maintenance naltrexone as novel and effective therapies for immunotherapy-induced pruritus: a case report and brief literature review. J Oncol Pract. 2019 06;15(6):347-348. | Incorrect intervention |
Smith KN, Llosa NJ, Cottrell TR, et al. Persistent mutant oncogene specific T cells in two patients benefitting from anti-PD-1. J ImmunoThe Cancer. 2019 11 Feb;7 (1)(40). | Study design |
Smyth EC, Moehler M. Late-line treatment in metastatic gastric cancer: today and tomorrow. Ther Adv Med Oncol. 2019;11. | Review study |
Stueger A, Winder T, Tinguely M, Petrausch U, Helbling D. Metastatic mixed adenoneuroendocrine carcinoma of the colon with response to immunotherapy with pembrolizumab: a case report. J Immunother. 2019 09;42(7):274-277. | Study design |
Thomopoulou K, Tzardi M, Mavroudis D, Souglakos I. A case presentation of a patient with microsatellite instability and BRAF mutant metastatic colon cancer and bibliography update. Case Rep Oncol Med. 2019:4767019. | Study design |
Trabjerg ND, Rask C, Jensen LH, Hansen TF. Pseudoprogression during treatment with pembrolizumab followed by rechallenge with chemotherapy in metastatic colorectal cancer: a case report. Clin Case Rep. 2019 Jul;7(7):1445-1449. | Study design |
van Vugt MJH, Stone JA, De Greef R, et al. Immunogenicity of pembrolizumab in patients with advanced tumours. J Immunother Cancer. 2019 08 08;7(1):212. | Review study |
Wang C, Sandhu J, Fakih M. Complete response to pembrolizumab in a patient with metastatic colon cancer with microsatellite instability and a history of Guillain-Barre syndrome. J Gastrointest Oncol. 2019 Feb;10(1):161-165. | Study design |
Wang GZ, Zhang L, Zhao XC, et al. The Aryl hydrocarbon receptor mediates tobacco-induced PD-L1 expression and is associated with response to immunotherapy. Nature Comm. 2019 01 Dec;10 (1)(1125). | Study design |
Whitman J, Kardosh A, Diaz L, et al. Complete response and immune-mediated adverse effects with checkpoint blockade: Treatment of mismatch repair-deficient colorectal neuroendocrine carcinoma. JCO Precis Oncol. 2019;3. | Incorrect patient population |
Williams KJ, Grauer DW, Henry DW, Rockey ML. Corticosteroids for the management of immune-related adverse events in patients receiving checkpoint inhibitors. J Oncol Pharm Pract. 2019 01 Apr;25(3):544-550. | Incorrect intervention |
Wilson K, Narasimhan V, Pham T, Das A, Ramsay R, Heriot A. Precision medicine in colorectal surgery: coming to a hospital near you. ANZ J Surg. 2019 09;89(9):995-996. | Incorrect patient population |
Winer A, Ghatalia P, Bubes N, et al. Dual checkpoint inhibition with ipilimumab plus nivolumab after progression on sequential PD-1/PDL-1 inhibitors pembrolizumab and atezolizumab in a patient with Lynch Syndrome, metastatic colon, and localized urothelial cancer. Oncologist. 2019 11;24(11):1416-1419. | Incorrect intervention |
Wu X, Snir O, Rottmann D, Wong S, Buza N, Hui P. Minimal microsatellite shift in microsatellite instability high endometrial cancer: a significant pitfall in diagnostic interpretation. Mod Pathol. 2019 05;32(5):650-658. | Incorrect patient population |
Yamamoto H, Imai K. An updated review of microsatellite instability in the era of next-generation sequencing and precision medicine. Semin Oncol. 2019 06;46(3):261-270. | Incorrect patient population |
Zhao P, Li L, Jiang X, Li Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J Hematol Oncol. 2019 05 31;12(1):54. | Review study |
Zhou C, Zhang J. Immunotherapy-based combination strategies for treatment of gastrointestinal cancers: current status and future prospects. Front. 2019 Feb;13(1):12-23. | Review study |
Pembrolizumab (Keytruda) for cancers with biomarkers. Med Lett Drugs Ther. 2018 01 Jan;60(1537):e8-e9. | Review study |
Armstrong S, Al-Ghawi H, Helft P, et al. Two months of therapy: a case of pathologic complete response to chemoimmunotherapy in a patient with metastatic colorectal cancer. Clin Colorectal Cancer. 2018 06;17(2):e229-e232. | Study design |
Azharuddin M, Sharayah A, Abbas SH, Belitsis K. Malignant melanoma metastasizes to colonic polyp. Cureus. 2018 Jun 18;10(6):e2822. | Incorrect patient population |
Baimas-George M, Baker E, Kamionek M, et al. A complete pathological response to pembrolizumab following ex vivo liver resection in a patient with colorectal liver metastases. Chemotherapy. 2018 Apr 05;63(2):90-94. | Study design |
Bangalore Kumar A, Maus R, Markovic SN. Pharmacologic modulation of human immunity in the era of immuno-oncology: something old, something new. Mayo Clin Proc. 2018 Jul;93(7):917-936. | Study design |
Boyiadzis MM, Kirkwood JM, Marshall JL, Pritchard CC, Azad NS, Gulley JL. Significance and implications of FDA approval of pembrolizumab for biomarker-defined disease. J ImmunoTher Cancer. 2018 14 May;6 (1)(35). | Review study |
Burgess BT, Kolesar JM. Defective DNA repair in hereditary ovarian cancers: implications for therapy. Am J Health Syst Pharm. 2018 Nov 01;75(21):1697-1707. | Incorrect patient population |
Casadei Gardini A, Passardi A, Fornaro L, et al. Treatment of squamous cell carcinoma of the anal canal: a new strategies with anti-EGFR therapy and immunotherapy. Crit Rev Oncol Hematol. 2018 Mar;123:52-56. | Incorrect intervention |
Casey RT, Giger O, Seetho I, et al. Rapid disease progression in a patient with mismatch repair-deficient and cortisol secreting adrenocortical carcinoma treated with pembrolizumab. Semin Oncol. 2018 06;45(3):151-155. | Study design |
Chang L, Chang M, Chang HM, Chang F. Microsatellite instability: a predictive biomarker for cancer immunotherapy. Appl Immunohistochem Mol Morphol. 2018 Feb;26(2):e15-e21 | Study design |
Chen CL, Pan QZ, Weng DS, et al. Safety and activity of PD-1 blockade-activated DC-CIK cells in patients with advanced solid tumours. Oncoimmunology. 2018 03 Apr;7 (4)(e1417721). | Incorrect intervention |
Chu E. How I treat chemorefractory metastatic colorectal cancer. Clin Adv Hematol Oncol. 2018 May;16(5):340-345. | Review study |
Ciombor KK, Goldberg RM. Hypermutated tumours and immune checkpoint inhibition. Drugs. 2018 Feb;78(2):155-162. | Review study |
Clark DP. Biomarkers for immune checkpoint inhibitors: the importance of tumour topography and the challenges to cytopathology. Cancer Cytopathol. 2018 Jan;126(1):11-19. | Study design |
Das S, Ciombor KK, Haraldsdottir S, Goldberg RM. Promising new agents for colorectal cancer. Curr Treat Options Oncol. 2018 05 11;19(6):29. | Review study |
Faure M, Rochigneux P, Olive D, Taix S, Brenot-Rossi I, Gilabert M. Hyperprogressive disease in anorectal melanoma treated by PD-1 inhibitors. Front Immunol. 2018;9:797. | Incorrect patient population |
Fuca G, De Braud F, Di Nicola M. Immunotherapy-based combinations: an update. Curr Opin Oncol. 2018 01 Sep;30(5):345-351. | Review study |
George A. Inherited gynaecological cancers. Curr Opin Oncol. 2018 09;30(5):317-322. | Incorrect patient population |
Gleeson FC, Levy MJ, Roden AC, et al. EUS fine-needle pancreatic core biopsy can determine eligibility for tumour-agnostic immunotherapy. Endosc Int Open. 2018;6(10):E1278-E1282 | Study design |
Grothey A, Venook AP. Optimizing adjuvant therapy for localized colon cancer and treatment selection in advanced colorectal cancer. J Natl Compr Canc Netw. 2018 05;16(5S):611-615. | Incorrect intervention |
Hara H, Yoshino T, Taniguchi H, et al. Phase II KEYNOTE-164 study of pembrolizumab (pembro) monotherapy for patients (pts) with previously treated, mismatch repair-Deficient (dMMR) advanced colorectal cancer (CRC): primary and Japan subgroup analyses. Ann Oncol. 2018 Nov;29(Suppl 9):ix32 | Duplicate |
Iyer PC, Cabanillas ME, Waguespack SG, et al. Immune-related thyroiditis with immune checkpoint inhibitors. Thyroid. 2018 10;28(10):1243-1251. | Review study |
Jindal V. Immune checkpoint inhibitors in gastrointestinal malignancies. J Gastrointest Oncol. 2018 01 Apr;9(2):390-403. | Review study |
Kalyan A, Kircher S, Shah H, Mulcahy M, Benson A. Updates on immunotherapy for colorectal cancer. J Gastrointest Oncol. 2018 Feb;9(1):160-169. | Review study |
Kawahara T, Nishiyama H. [Diagnosis and treatment of MSI-H cancer in the urological malignancy]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2018 Nov;45(11):1573-1576. | Incorrect patient population |
Klevansky M, Karapetis CS. Checkpoint inhibitor therapy for breast cancer, colon cancer, merkel cell carcinoma and sarcoma. Cancer Forum. 2018;42(1). | Review study |
Koustas E, Papavassiliou AG, Karamouzis MV. The role of autophagy in the treatment of BRAF mutant colorectal carcinomas differs based on microsatellite instability status. PLoS ONE. 2018;13(11):e0207227 | Review study |
Kuo JC, Lilly LB, Hogg D. Immune checkpoint inhibitor therapy in a liver transplant recipient with a rare subtype of melanoma: a case report and literature review. Melanoma Res. 2018;28(1):61-64. | Incorrect patient population |
Le D, Kavan P, Kim T, et al. Safety and antitumour activity of pembrolizumab in patients with advanced microsatellite instability-high (MSI-H) colorectal cancer: KEYNOTE-164. Ann Oncol. 2018 Jun;29(Suppl 5):v107 | Duplicate study |
Marginean EC, Melosky B. Is there a role for programmed death ligand-1 testing and immunotherapy in colorectal cancer with microsatellite instability? Part II-the challenge of programmed death ligand-1 testing and its role in microsatellite instability-high colorectal cancer. Arch Pathol Lab Med. 2018 Jan;142(1):26-34. | Review study |
Marginean EC, Melosky B. Is there a role for programmed death ligand-1 testing and immunotherapy in colorectal cancer with microsatellite instability? Part I-colorectal cancer: microsatellite instability, testing, and clinical implications. Arch Pathol Lab Med. 2018 Jan;142(1):17-25. | Review study |
Micheel A, Aigner F, Henke O. Histologic remission following neoadjuvant immunotherapy in a patient with Lynch-syndrome and primarily unresectable relapse of rectum carcinoma. [German]. Tumour Diagnostik und Therapie. 2018 01 Feb;39(1):42-46. | Incorrect intervention |
Min Lee CK, Li S, Tran DC, et al. Characterization of dermatitis after PD-1/PD-L1 inhibitor therapy and association with multiple oncologic outcomes: a retrospective case-control study. J Am Acad Dermatol. 2018 Dec;79(6):1047-1052. | Review study |
Nozawa Y, Oka Y, Oosugi J, Takemura S. Immunotherapy for pulmonary squamous cell carcinoma and colon carcinoma with pembrolizumab: a case report. Medicine. 2018 May;97(19):e0718 | Study design |
Ogino S, Nowak JA, Hamada T, et al. Integrative analysis of exogenous, endogenous, tumour and immune factors for precision medicine. Gut. 2018 06;67(6):1168-1180. | Incorrect patient population |
Overman MJ, Ernstoff MS, Morse MA. Where we stand with immunotherapy in colorectal cancer: deficient mismatch repair, proficient mismatch repair, and toxicity management. Am Soc Clin Oncol Educ Book. 2018 May 23;38:239-247. | Review study |
Palmieri DJ, Carlino MS. Immune checkpoint inhibitor toxicity. Curr Oncol Rep. 2018 01 Sep;20 (9)(72) | Review study |
Patel SA, Longacre TA, Ladabaum U, Lebensohn A, Lin AY, Haraldsdottir S. Tumour molecular testing guides anti-PD-1 therapy and provides evidence for pathogenicity of mismatch repair variants. Oncologist. 2018 12;23(12):1395-1400. | Study design |
Prasad V, Kaestner V, Mailankody S. Cancer drugs approved based on biomarkers and not tumour type-FDA approval of pembrolizumab for mismatch repair-deficient solid cancers. JAMA Oncology. 2018 Feb 01;4(2):157-158. | Review study |
Prasad V, Kaestner V, Mailankody S. In reply. JAMA Oncol. 2018 Sep;4(9):1300-1301. | Study design |
Puccini A, Lenz HJ. Colorectal cancer in 2017: Practice-changing updates in the adjuvant and metastatic setting. Nat Rev Clin Oncol. 2018 02;15(2):77-78. | Review study |
Qiu H, Zhou Z. [Updates and interpretation on NCCN clinical practice guidelines for gastric cancer 2017 version 5]. Zhonghua Weichang Waike Zazhi. 2018 Feb 25;21(2):160-164. | Review study |
Ratner D, Lennerz JK. Implementing Keytruda/pembrolizumab testing in clinical practice. Oncologist. 2018 Jun;23(6):647-649. | Study design |
Riley JM, Cross AW, Paulos CM, Rubinstein MP, Wrangle J, Camp ER. The clinical implications of immunogenomics in colorectal cancer: a path for precision medicine. Cancer. 2018 04 15;124(8):1650-1659. | Study design |
Roskoski R Jr. Targeting oncogenic Raf protein-serine/threonine kinases in human cancers. Pharmacol Res. 2018 09;135:239-258. | Incorrect intervention |
Sacdalan DB, Lucero JA, Sacdalan DL. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: a review and meta-analysis. Onco Targets Ther. 2018 23 Feb;11:955-965. | Study design |
Salman P, Panay S, Fernandez R, Mahave M, Soza-Ried C. Evidence of response to pembrolizumab in a patient with Lynch syndrome-related metastatic colon cancer. Onco Targets Ther. 2018;11:7295-7300. | Incorrect patient population |
Sclafani F, Rao S. Systemic therapies for advanced squamous cell anal cancer. Curr Oncol Rep. 2018 05 04;20(7):53. | Review study |
Shinozaki T, Iwami E, Ikemura S, et al. A case of pulmonary adenocarcinoma showing rapid progression of peritoneal dissemination after immune checkpoint inhibitor therapy. BMC Cancer. 2018 31 May;18 (1)(620) | Incorrect patient population |
Solomon BL, Garrido-Laguna I. Upper gastrointestinal malignancies in 2017: current perspectives and future approaches. Fut Oncol. 2018 Apr;14(10):947-962. | Review study |
Sorscher S. The importance of distinguishing sporadic cancers from those related to cancer predisposing germline mutations. Oncologist. 2018 11;23(11):1266-1268. | Incorrect patient population |
Sorscher S. Clarification of the FDA accelerated agnostic approval of pembrolizumab and the opportunities arising from the required confirmatory studies. JAMA Oncol. 2018 Sep;4(9):1299-1300. | Study design |
Stein A, Moehler M, Trojan J, Goekkurt E, Vogel A. Immuno-oncology in GI tumours: clinical evidence and emerging trials of PD-1/PD-L1 antagonists. Crit Rev Oncol Hematol. 2018 Oct;130:13-26. | Review study |
Suh DH, Kim M, Lee KH, et al. Major clinical research advances in gynecologic cancer in 2017. J Gynecol Oncol. 2018 03;29(2):e31 | Review study |
Ta RM, Hecht JL, Lin DI. Discordant loss of mismatch repair proteins in advanced endometrial endometrioid carcinoma compared to paired primary uterine tumours. Gynecol Oncol. 2018 12;151(3):401-406. | Incorrect patient population |
Voutsadakis IA. Immune blockade inhibitors and the radiation abscopal effect in gastrointestinal cancers. World J Gastrointest Oncol. 2018 01 Sep;10(9):221-227. | Review study |
Yan L, Zhang W. Precision medicine becomes reality-tumour type-agnostic therapy. Cancer Commun. 2018 03 31;38(1):6. | Study design |
Yee NS. Update in Systemic and targeted therapies in gastrointestinal oncology. Biomedicines. 2018 Mar 16;6(1):16. | Review study |
Yu Y. Molecular classification and precision therapy of cancer: immune checkpoint inhibitors. Front. 2018 Apr;12(2):229-235. | Review study |
Abdel-Rahman O. Nonconventional patterns of benefit of solid tumours treated with PD-(L)1 inhibitors: a systematic review. Immunotherapy. 2017 Sep;9(12):995-1004. | Review study |
Al-Hajeili M, Shields AF, Hwang JJ, Wadlow RC, Marshall JL. Molecular testing to optimize and personalize decision making in the management of colorectal cancer. Oncology (Williston Park). 2017 04 15;31(4):301-312. | Study design |
US Food and Drug Administration approves first cancer treatment for any solid tumours with specific biomarker. Cancer. 2017 01 Oct;123(19):3652-3653. | Study design |
Pembrolizumab for dMMR/MSI-H tumours marks first tumour agnostic FDA approval. J Community Support Oncol. 2017 December;15(6):e294-e296 | Study design |
Ashizawa M, Okayama H, Aung Kyi Thar M, et al. [Regulation of PD-L1 by microRNA in mismatch repair deficient-colorectal cancer]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2017 Oct;44(10):889-891. | Study design |
Atrash S, Makhoul I, Mizell JS, Hutchins L, Mahmoud F. Response of metastatic mucosal melanoma to immunotherapy: it can get worse before it gets better. J Oncol Pharm Pract. 2017 01 Apr;23(3):215-219. | Incorrect patient population |
Atwal D, Joshi KP, Ravilla R, Mahmoud F. Pembrolizumab-induced pancytopenia: a case report. Perm J. 2017;21:17-004. | Study design |
Backlund M, Freedman J. Microwave ablation and immune activation in the treatment of recurrent colorectal lung metastases: a case report. Case Rep. 2017 Jan-Apr;10(1):383-387. | Incorrect patient population |
Basile D, Garattini SK, Bonotto M, et al. Immunotherapy for colorectal cancer: where are we heading? Expert Opin Biol Ther. 2017 06;17(6):709-721. | Review study |
Bellmunt J, Powles T, Vogelzang NJ. A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: the future is now. Cancer Treat Rev. 2017 01 Mar;54:58-67. | Incorrect patient population |
Bilgin B, Sendur MA, Bulent Akinci M, Sener Dede D, Yalcin B. Targeting the PD-1 pathway: a new hope for gastrointestinal cancers. Curr Med Res Opin. 2017 04;33(4):749-759. | Review study |
Bottlaender L, Breton AL, de Laforcade L, Dijoud F, Thomas L, Dalle S. Acute interstitial nephritis after sequential ipilumumab - nivolumab therapy of metastatic melanoma. J Immunother Cancer. 2017 07 18;5(1):57. | Incorrect patient population |
Cabel L, Riva F, Servois V, et al. Circulating tumour DNA changes for early monitoring of anti-PD1 immunotherapy: a proof-of-concept study. Ann Oncol. 2017 Aug 01;28(8):1996-2001. | Study design |
Casadei Gardini A, Valgiusti M, Passardi A, Frassineti GL. Treatment of squamous cell carcinoma of the anal canal (SCCA): a new era? Ann Oncol. 2017;28(10):2620-2620. | Review study |
Chen G. [Interpretation of the updates of NCCN 2017 version 1.0 guideline for colorectal cancer]. Zhonghua Weichang Waike Zazhi. 2017 Jan 25;20(1):28-33. | Review study |
Cohen R, Svrcek M, Duval A, Parc Y, Osterlund PP, Andre T. Immune checkpoint inhibitors for patients with colorectal cancer: mismatch repair deficiency and perspectives. Colorectal Cancer. 2017 Nov;6(1):23-31. | Review study |
Diehl A, Yarchoan M, Hopkins A, Jaffee E, Grossman SA. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumours treated with PD-1 checkpoint inhibitors. Oncotarget. 2017;8(69):114268-114280. | Irrelevant study topic |
Esfahani K, Miller WH, Jr. Reversal of autoimmune toxicity and loss of tumour response by interleukin-17 blockade. N Engl J Med. 2017 05 18;376(20):1989-1991. | Incorrect intervention |
Finocchiaro G, Langella T, Corbetta C, Pellegatta S. Hypermutations in gliomas: a potential immunotherapy target. Discov Med. 2017 02;23(125):113-120. | Irrelevant study topic |
Firwana B, Ravilla R, Raval M, Hutchins L, Mahmoud F. Sarcoidosis-like syndrome and lymphadenopathy due to checkpoint inhibitors. J Oncol Pharm Pract. 2017 01 Dec;23(8):620-624. | Incorrect patient population |
Freshwater T, Kondic A, Ahamadi M, et al. Evaluation of dosing strategy for pembrolizumab for oncology indications. J Immunother Cancer. 2017;5:43. | Study design |
Fujiyoshi K, Yamamoto G, Takenoya T, et al. Metastatic pattern of stage IV colorectal cancer with high-frequency microsatellite instability as a prognostic factor. Anticancer Res. 2017 01;37(1):239-247. | Incorrect intervention |
Geanta M, Cioroboiu C. The FDA changed everything. Biomed. 2017 Nov-Dec;2(Suppl 1):52-54. | Review study |
Ghatalia P, Nagarathinam R, Cooper H, Geynisman DM, El-Deiry WS. Mismatch repair deficient metastatic colon cancer and urothelial cancer: a case report of sequential immune checkpoint therapy. Cancer Biol Ther. 2017 Sep 02;18(9):651-654. | Study design |
Gokare P, Lulla AR, El-Deiry WS. MMR-deficiency and BRCA2/EGFR/NTRK mutations. Aging. 2017 Aug 03;9(8):1849-1850. | Incorrect intervention |
Gong J, Wang C, Lee PP, Chu P, Fakih M. Response to PD-1 blockade in microsatellite stable metastatic colorectal cancer harboring a POLE mutation. J Natl Compr Canc Netw. 2017 02;15(2):142-147. | Study design |
Grimaldi AM, Simeone E, Festino L, Vanella V, Strudel M, Ascierto PA. MEK Inhibitors in the treatment of metastatic melanoma and solid tumours. Am J Clin Dermatol. 2017 01 Dec;18(6):745-754. | Incorrect intervention |
Iafolla MAJ, Juergens RA. Update on programmed death-1 and programmed death-ligand 1 inhibition in the treatment of advanced or metastatic non-small cell lung cancer. Front Oncol. 2017 06 Apr;7(67). | Incorrect intervention |
Johnson B, Eng C. The promise of immunotherapy in anal squamous cell carcinoma: a novel approach for an orphan disease. Clin Adv Hematol Oncol. 2017 Dec;15(12):968-976. | Review study |
Katoh M. Canonical and non-canonical WNT signaling in cancer stem cells and their niches: Cellular heterogeneity, omics reprogramming, targeted therapy and tumour plasticity (Review). Int J Oncol. 2017 Nov;51(5):1357-1369. | Review study |
Khoja L, Day D, Wei-Wu Chen T, Siu LL, Hansen AR. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377-2385. | Review study |
Killock D. Immunotherapy: PD-1 blockade exploiting MMR deficiency. Nat Rev Clin Oncol. 2017 01 Aug;14(8):459. | Review study |
Kroeze SGC, Fritz C, Hoyer M, et al. Toxicity of concurrent stereotactic radiotherapy and targeted therapy or immunotherapy: a systematic review. Cancer Treat Rev. 2017 01 Feb;53:25-37. | Incorrect intervenetion |
Le DT, Durham JN, Smith KN, et al. Mismatch repair deficiency predicts response of solid tumours to PD-1 blockade. Science. 2017 07 28;357(6349):409-413. | Study design |
Lemery S, Keegan P, Pazdur R. First FDA approval agnostic of cancer site - when a biomarker defines the indication. N Engl J Med. 2017 Oct 12;377(15):1409-1412. | Review study |
Liao X, Zhao L, Wu S, et al. Microsatellite stability and mismatch repair proficiency in nasopharyngeal carcinoma may not predict programmed death-1 blockade resistance. Oncotarget. 2017 Dec 22;8(68):113287-113293. | Incorrect patient population |
Lindauer A, Valiathan C, Mehta K, et al. Translational pharmacokinetic/pharmacodynamic modeling of tumour growth inhibition supports dose-range selection of the anti-PD-1 antibody pembrolizumab. CPT: Pharmacometrics Systems Pharmacol. 2017 01 Jan;6(1):11-20. | Study design |
Liu B, Song Y, Liu D. Recent development in clinical applications of PD-1 and PD-L1 antibodies for cancer immunotherapy. J Hematol Oncol. 2017 01 Dec;10 (1)(174) | Review study |
Machida T, Hiraoka K, Matsubara N. [A case of duodenum dissemination after surgery for transverse colon carcinoma which was unresponsive to chemotherapy, but immunotherapy was significantly effective]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2017 Nov;44(12):1170-1172. | Study design |
Micheel A, Aigner F, Henke O. [Histologic remission following neoadjuvant immunotherapy in a patient with Lynch-syndrome and primarily unresectable relapse of rectum carcinoma]. Dtsch Med Wochenschr. 2017 Jun;142(11):842-846. | Study design |
Murphy AG, Kelly RJ. The evolving role of checkpoint inhibitors in the management of gastroesophageal cancer. Hematol Oncol Clin North Am. 2017 Jun;31(3):485-498. | Incorrect patient population |
Nebot-Bral L, Brandao D, Verlingue L, et al. Hypermutated tumours in the era of immunotherapy: The paradigm of personalised medicine. Eur J Cancer. 2017 10;84:290-303. | Incorrect patient population |
O'Neil BH, Wallmark JM, Lorente D, et al. Safety and antitumour activity of the anti-PD-1 antibody pembrolizumab in patients with advanced colorectal carcinoma. PLoS ONE. 2017;12(12):e0189848 | Incorrect intervention |
Oracion K. The remarkable complete response and improvement of performance status to pembrolizumab of a recurrent microsatellite instability high, metastatic colon cancer, previously treated with Cetuximab, FOLFOX and Irinotecan. Ann Oncol. 2017 01 Oct;28(Suppl 7):vii19 | Incorrect intervention |
Ott PA, Piha-Paul SA, Munster P, et al. Safety and antitumour activity of the anti-PD-1 antibody pembrolizumab in patients with recurrent carcinoma of the anal canal. Ann Oncol. 2017 05 01;28(5):1036-1041. | Incorrect intervention |
Queirolo P, Spagnolo F. Atypical responses in patients with advanced melanoma, lung cancer, renal-cell carcinoma and other solid tumours treated with anti-PD-1 drugs: a systematic review. Cancer Treat Rev. 2017 September;59:71-78. | Review study |
Rickman DS, Beltran H, Demichelis F, Rubin MA. Biology and evolution of poorly differentiated neuroendocrine tumours. Nat Med. 2017 Jun 06;23(6):1-10. | Review study |
Sclafani F. PD-1 inhibition in metastatic dMMR/MSI-H colorectal cancer. Lancet Oncol. 2017 Sep;18(9):1141-1142. | Review study |
Shin DS, Zaretsky JM, Escuin-Ordinas H, et al. Primary resistance to PD-1 blockade mediated by JAK1/2 mutations. Cancer Discov. 2017 02;7(2):188-201. | Study design |
Shin SH, Dong Z. Pairing cancer biomarkers to biomedicine. EBioMedicine. 2017 11;25:1-2. | Study design |
Sorscher S, Resnick J, Goodman M. First case report of a dramatic radiographic response to a checkpoint inhibitor in a patient with proficient mismatch repair gene expressing metastatic colorectal cancer. JCO Precis Oncol. 2017;2017(1):1-4. | Study design |
Tomasek J, Kiss I. [Immunotherapy of colorectal and anal carcinoma]. Klin. 2017 2017;30(Suppl 3):62-65. | Review study |
Valecha GK, Vennepureddy A, Ibrahim U, Safa F, Samra B, Atallah JP. Anti-PD-1/PD-L1 antibodies in non-small cell lung cancer: the era of immunotherapy. Expert Rev Anticancer Ther. 2017 02 Jan;17(1):47-59. | Incorrect patient population |
Wagner LM, Adams VR. Targeting the PD-1 pathway in pediatric solid tumours and brain tumours. Onco Targets Ther. 2017 12 Apr;10:2097-2106. | Incorrect patient population |
Wang PF, Chen Y, Song SY, et al. Immune-related adverse events associated with anti-PD-1/PD-L1 treatment for malignancies: a meta-analysis. Front Pharmacol. 2017;8:730. | Review study |
Wu TH, Hsiue EHC, Yuan CT, Tseng LH, Lin CC, Yeh KH. Durable response to programmed death-1 (PD-1) blockade in a metastatic gastric cancer patient with mismatch repair deficiency and microsatellite instability. J Cancer Res Pract. 2017 Jun;4(2):72-75. | Study design |
Yoshida Y, Noura S, Matsumura T, et al. [Anorectal malignant melanoma is a very rare disease and has a poor prognosis]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2017 Nov;44(12):1817-1819. | Incorrect patient population |
Blocking PD-1 in tumours with faulty DNA repair. Cancer Discov. 2016 08;6(8):OF6. | Study design |
Chen KH, Yuan CT, Tseng LH, Shun CT, Yeh KH. Case report: mismatch repair proficiency and microsatellite stability in gastric cancer may not predict programmed death-1 blockade resistance. J Hematol Oncol. 2016 Mar 24;9:29. | Study design |
Economopoulou P, Psyrri A. Overview and management of toxicities of immune checkpoint-blocking drugs. Forum Clin Oncol. 2016;7(1):28-37. | Review study |
Festino L, Botti G, Lorigan P, et al. Cancer treatment with anti-PD-1/PD-L1 agents: is PD-L1 expression a biomarker for patient selection? Drugs. 2016 Jun;76(9):925-945. | Review study |
Galanternik F, Valsecchi ME, Greco M, Recondo G, de la Vega M, Canton ED. What is the current role of immunotherapy for colon cancer? Rev Recent Clin Trials. 2016 01 Jun;11(2):93-98. | Review study |
Gentzler R, Hall R, Kunk PR, et al. Beyond melanoma: inhibiting the PD-1/PD-L1 pathway in solid tumours. Immunotherapy. 2016 May;8(5):583-600. | Incorrect patient population |
Hecht M, Buttner-Herold M, Erlenbach-Wunsch K, et al. PD-L1 is upregulated by radiochemotherapy in rectal adenocarcinoma patients and associated with a favourable prognosis. Eur J Cancer. 2016 09;65:52-60. | Study design |
Heinzerling L, Kirchberger MC, Walter L, Schuler G. Predicting the response to anti-PD1 therapy in metastatic melanoma. Transl Cancer Res. 2016;5(Suppl 3):S576-S579. | Incorrect patient population |
Iyevleva AG, Imyanitov EN. Cytotoxic and targeted therapy for hereditary cancers. Hered Cancer Clin Pract. 2016;14(1):17. | Review study |
Johanns TM, Miller CA, Dorward IG, et al. Immunogenomics of hypermutated glioblastoma: a patient with germline POLE deficiency treated with checkpoint blockade immunotherapy. Cancer Discov. 2016 Nov;6(11):1230-1236. | Incorrect patient population |
Kieler M, Scheithauer W, Zielinski CC, Chott A, Al-Mukhtar A, Prager GW. Case report: impressive response to pembrolizumab in a patient with mismatch-repair deficient metastasized colorectal cancer and bulky disease. ESMO Open. 2016;1(6):e000084. | Study design |
Medina PJ, Adams VR. PD-1 Pathway inhibitors: immuno-oncology agents for restoring antitumour immune responses. Pharmacotherapy. 2016 01 Mar;36(3):317-334. | Review study |
Morse MA. The outlook for immune checkpoint targeting strategies in colorectal cancer. Curr Colorectal Cancer Rep. 2016 01 Feb;12(1):51-56. | Review study |
Pohl M, Schmiegel W. Therapeutic strategies in diseases of the digestive tract - 2015 and beyond targeted therapies in colon cancer today and tomorrow. Dig Dis. 2016;34(5):574-579. | Review study |
Postel-Vinay S, Aspeslagh S, Lanoy E, Robert C, Soria JC, Marabelle A. Challenges of phase 1 clinical trials evaluating immune checkpoint-targeted antibodies. Ann Oncol. 2016 01 Feb;27(2):214-224. | Study design |
Ronnekleiv-Kelly SM, Burkhart RA, Pawlik TM. Molecular markers of prognosis and therapeutic targets in metastatic colorectal cancer. Surg Oncol. 2016 Sep;25(3):190-199. | Study design |
Sehdev A, Cramer HM, Ibrahim AA, Younger AE, O'Neil BH. Pathological complete response with anti-PD-1 therapy in a patient with microsatellite instable high, BRAF mutant metastatic colon cancer: a case report and review of literature. Discov Med. 2016 05;21(117):341-347. | Study design |
Toh JWT, de Souza P, Lim SH, et al. The potential value of immunotherapy in colorectal cancers: review of the evidence for programmed death-1 inhibitor therapy. Clin Colorectal Cancer. 2016 12;15(4):285-291. | Review study |
Wurz GT, Kao CJ, Degregorio MW. Novel cancer antigens for personalized immunotherapies: latest evidence and clinical potential. Ther Adv Med Oncol. 2016 01 Jan;8(1):4-31. | Review study |
Aguiar PN, Jr., Tadokoro H, Forones NM, de Mello RA. MMR deficiency may lead to a high immunogenicity and then an improvement in anti-PD-1 efficacy for metastatic colorectal cancer. Immunotherapy. 2015;7(11):1133-1134. | Review study |
Aprile G, Leone F, Giampieri R, et al. Tracking the 2015 Gastrointestinal Cancers Symposium: bridging cancer biology to clinical gastrointestinal oncology. Onco Targets Ther. 2015;8:1149-1156. | Review study |
Buque A, Bloy N, Aranda F, et al. Trial Watch: Immunomodulatory monoclonal antibodies for oncological indications. Oncoimmunology. 2015 Apr;4(4):e1008814. | Review study |
de Guillebon E, Roussille P, Frouin E, Tougeron D. Anti program death-1/anti program death-ligand 1 in digestive cancers. World J Gastrointest Oncol. 2015 Aug 15;7(8):95-101. | Review study |
Eisterer W. ASCO 2015: highlights in colorectal cancer. Memo - Magazine of European Medical Oncology. 2015 01 Dec;8(4):218-221. | Review study |
Faghfuri E, Faramarzi MA, Nikfar S, Abdollahi M. Nivolumab and pembrolizumab as immune-modulating monoclonal antibodies targeting the PD-1 receptor to treat melanoma. Expert Rev Anticancer Ther. 2015 02 Sep;15(9):981-993. | Incorrect patient population |
Gangadhar TC, Salama AK. Clinical applications of PD-1-based therapy: a focus on pembrolizumab (MK-3475) in the management of melanoma and other tumour types. Onco Targets Ther. 2015;8:929-937. | Review study |
Goel G, Sun W. Advances in the management of gastrointestinal cancers - an upcoming role of immune checkpoint blockade. J Hematol Oncol. 2015 16 Jul;8 (1)(86). | Review study |
Gonzalez-Cao M, Karachaliou N, Viteri S, et al. Targeting PD-I/PD-LI in lung cancer: current perspectives. Lung Cancer. 2015 31 Jul;6:55-70. | Incorrect patient population |
Kim KB. Nivolumab in the treatment of advanced melanoma. Expert Opin Orphan Drugs. 2015 01 Aug;3(8):945-956. | Incorrect patient population |
Kroemer G, Galluzzi L, Zitvogel L, Fridman WH. Colorectal cancer: the first neoplasia found to be under immunosurveillance and the last one to respond to immunotherapy? Oncoimmunology. 2015 Jul;4(7):e1058597. | Review study |
Lau E. Mismatch repair deficiency predicts benefit of anti-PD-1 therapy. Lancet Oncol. 2015 Jul;16(7):e319. | Study design |
Le DT, Uram JN, Wang H, et al. PD-1 Blockade in tumours with mismatch-repair deficiency. N Engl J Med. 2015 Jun 25;372(26):2509-2520. | Study design |
Lin AY, Lin E. Programmed death 1 blockade, an Achilles heel for MMR-deficient tumours? J Hematol Oncol. 2015 Nov 05;8:124. | Review study |
Lin EI, Tseng LH, Gocke CD, et al. Mutational profiling of colorectal cancers with microsatellite instability. Oncotarget. 2015 Dec 08;6(39):42334-42344. | Review study |
Lote H, Cafferkey C, Chau I. PD-1 and PD-L1 blockade in gastrointestinal malignancies. Cancer Treat Rev. 2015 Dec;41(10):893-903. | Review study |
McDermott J, Jimeno A. Pembrolizumab: PD-1 inhibition as a therapeutic strategy in cancer. Drugs Today. 2015 01 Jan;51(1):7-20. | Review study |
Preusser M, Lim M, Hafler DA, Reardon DA, Sampson JH. Prospects of immune checkpoint modulators in the treatment of glioblastoma. Nature Rev Neurol. 2015 07 Sep;11(9):504-514. | Review study |
Reichert JM. Antibodies to watch in 2015. MAbs. 2015 01 Jan;7(1):1-8. | Review study |
Schalper KA, Venur VA, Velcheti V. Programmed death-1/programmed death-1 ligand axis as a therapeutic target in oncology: current insights. J Receptor, Ligand Channel Res. 2015;8:1-7. | Review study |
Shrimali RK, Janik JE, Abu-Eid R, Mkrtichyan M, Khleif SN. Programmed death-1 & its ligands: promising targets for cancer immunotherapy. Immunotherapy. 2015 01 Jul;7(7):777-792. | Review study |
Singh PP, Sharma PK, Krishnan G, Lockhart AC. Immune checkpoints and immunotherapy for colorectal cancer. Gastroenterol Rep. 2015 Nov;3(4):289-297. | Review study |
Sunshine J, Taube JM. PD-1/PD-L1 inhibitors. Curr Opin Pharmacol. 2015 03 Jun;23:32-38. | Review study |
Kyi C, Postow MA. Checkpoint blocking antibodies in cancer immunotherapy. FEBS Lett. 2014 21 Jan;588(2):368-376. | Review study |
Marabelle A, Kohrt H, Caux C, Levy R. Intratumoural immunization: a new paradigm for cancer therapy. Clin Cancer Res. 2014 01 Apr;20(7):1747-1756. | Review study |
Merelli B, Massi D, Cattaneo L, Mandala M. Targeting the PD1/PD-L1 axis in melanoma: biological rationale, clinical challenges and opportunities. Crit Rev Oncol Hematol. 2014 Jan;89(1):140-165. | Incorrect patient population |
Momtaz P, Postow MA. Immunologic checkpoints in cancer therapy: focus on the programmed death-1 (PD-1) receptor pathway. Pharmgenomics Pers Med. 2014 15 Nov;7:357-365. | Review study |
Perez-Gracia JL, Labiano S, Rodriguez-Ruiz ME, Sanmamed MF, Melero I. Orchestrating immune check-point blockade for cancer immunotherapy in combinations. Curr Opin Immunol. 2014 April;27(1):89-97. | Review study |
Callahan MK, Wolchok JD. At the bedside: CTLA-4- and PD-1-blocking antibodies in cancer immunotherapy. J Leukoc Biol. 2013 July;94(1):41-53. | Review study |
Gogas H, Polyzos A, Kirkwood J. Immunotherapy for advanced melanoma: fulfilling the promise. Cancer Treat Rev. 2013 Dec;39(8):879-885. | Incorrect patient population |
Hamid O, Carvajal RD. Anti-programmed death-1 and anti-programmed death-ligand 1 antibodies in cancer therapy. Expert Opin Biol Ther. 2013 Jun;13(6):847-861. | Review study |
Hausner PF. Image-guided thermal ablation of tumour increases the plasma level of interleukin-6 and interleukin-10: is plasma level of interleukin-6 a surrogate for immunogenic cell death? J Vasc Interv Radiol. 2013 Aug;24(8):1112-1113. | Incorrect intervention |
Liu Q, Gong W, Cheng Z, Jiang H, Cao F, Li X. Counteracting immunosuppressive cofactor B7-H1 may enhance the effects of chemotherapy in cancer patients. Immunotherapy. 2013 Jun;5(6):557-559. | Incorrect intervention |
Melero I, Grimaldi AM, Perez-Gracia JL, Ascierto PA. Clinical development of immunostimulatory monoclonal antibodies and opportunities for combination. Clin Cancer Res. 2013 01 Mar;19(5):997-1008. | Incorrect intervention |
Mullard A. New checkpoint inhibitors ride the immunotherapy tsunami. Nat Rev Drug Discov. 2013 July;12(7):489-492. | Review study |
Patel SP, Osada T, Osada K, Hurwitz H, Lyerly HK, Morse MA. Modulation of immune system inhibitory checkpoints in colorectal cancer. Curr Colorectal Cancer Rep. 2013 Dec;9(4):391-397. | Review study |
Salama AKS. Evolving pharmacotherapies for the treatment of metastatic melanoma. Clin Med Insights Oncol. 2013;7:137-149. | Incorrect patient population |
Tang PA, Heng DYC. Programmed death 1 pathway inhibition in metastatic renal cell cancer and prostate cancer. Curr Oncol Rep. 2013 Apr;15(2):98-104. | Incorrect patient population |
Franks HA, Wang Q, Patel PM. New anticancer immunotherapies. Anticancer Res. 2012 July;32(7):2439-2454. | Review study |
Sapoznik S, Hammer O, Ortenberg R, et al. Novel anti-melanoma immunotherapies: disarming tumour escape mechanisms. Clin Develop Immunol. 2012;(818214). | Review study |
Zitvogel L, Kroemer G. Targeting PD-1/PD-L1 interactions for cancer immunotherapy. Oncoimmunology. 2012;1(8):1223-1225. | Review study |
Xie T, Feng Q, Li Z, et al. Heterogeneous constitutional mismatch repair deficiency with MSH6 missense mutation clinically benefits from pembrolizumab and regorafenib combination therapy: a case report and literature review. Hered Cancer Clin Pract. 2021 Jan 09;19(1):7. | Study design |
Ishiguro T, Ishikawa H, Muta Y, et al. [A case of advanced recurrent colorectal cancer with complete response to pembrolizumab chemotherapy]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2020 Dec;47(13):2299-2301. | Study design |
Moriuchi T, Shimizu Y, Shimizu W, et al. [MSI-H Small bowel cancer with peritoneal dissemination successfully treated with pembrolizumab-a case report]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2020 Dec;47(13):2009-2011. | Study design |
Wiggins CJ, Chon SY. Dermatomyositis, pembrolizumab, and squamous cell carcinoma of the lung. Baylor Univ Med Cent Proc. 2020 Aug 27;34(1):120-121. | Incorrect patient population |
Yoshino T, Kim TW, Yong WP, et al. Pembrolizumab vs chemotherapy in patients with microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer: Asia subgroup results of the phase III KEYNOTE-177 study [abstract]. Ann Oncol. 2020;31:S1284-S1285. | Duplicate study |
Xie T, Feng Q, Li Z, et al. Heterogeneous constitutional mismatch repair deficiency with MSH6 missense mutation clinically benefits from pembrolizumab and regorafenib combination therapy: a case report and literature review. Hered Cancer Clin Pract. 2021 Jan 09;19(1):7. | Review study |
Ishiguro T, Ishikawa H, Muta Y, et al. [A case of advanced recurrent colorectal cancer with complete response to pembrolizumab chemotherapy]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2020 Dec;47(13):2299-2301. | Study design |
Moriuchi T, Shimizu Y, Shimizu W, et al. [MSI-H Small bowel cancer with peritoneal dissemination successfully treated with pembrolizumab-a case report]. Gan to Kagaku Ryoho [Jpn J Cancer Chemother]. 2020 Dec;47(13):2009-2011. | Study design |
Wiggins CJ, Chon SY. Dermatomyositis, pembrolizumab, and squamous cell carcinoma of the lung. Baylor Univ Med Cent Proc. 2020 Aug 27;34(1):120-121. | Incorrect patient population |
Yoshino T, Kim TW, Yong WP, et al. Pembrolizumab vs chemotherapy in patients with microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer: Asia subgroup results of the phase III KEYNOTE-177 study [abstract]. Ann Oncol. 2020;31:S1284-S1285. | Duplicate study |
Arteaga Perez I. Game-changing? When biomarker discovery and novel forms of patient work meet. Med Anthropol. 2021 14 Jan:1-13. | Review study |
Cho YA, Han JM, Kang SY, et al. Analysis of risk factors for hepatotoxicity induced by immune checkpoint inhibitors. J Immunother. 2021 January;44(1):16-21. | Review study |
Hirano H, Takashima A, Hamaguchi T, Shida D, Kanemitsu Y. Current status and perspectives of immune checkpoint inhibitors for colorectal cancer. Jpn J Clin Oncol. 2021 01 Jan;51(1):10-19. | Review study |
Khetan V, Blake EA, Ciccone MA, Matsuo K. Rhabdomyolysis following single administration of pembrolizumab: Is severe immune-reaction a marker for durable treatment response? Gynecol Oncol Rep. 2021 Feb;35 (no pagination)(100700). | Study design |
Roberts A, Bentley L, Tang T, et al. Ex vivo modelling of PD-1/PD-L1 immune checkpoint blockade under acute, chronic, and exhaustion-like conditions of T-cell stimulation. Sci Rep. 2021 Feb 17;11(1):4030. | Incorrect patient population |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Additional clinically relevant information obtained from KEYNOTE-177 is presented below; however, these observations were strictly exploratory and were not controlled for multiplicity.
Table 42: Additional Outcome Data From KEYNOTE-177
Outcome | Pembrolizumab N = 153 | SOC N = 154 |
|---|---|---|
Progression-Free Survival | ||
Hazard Ratio (95% CI) | 0.60 (0.45 to 0.80) | |
Piecewise Hazard Ratioa | ||
<3 Months | 1.88 | |
≥ 3 Months | 0.22 | |
Weighted Hazard Ratio (95% CI) | ||
Early Weighting | 0.81 (0.57 to 1.16) | |
Late Weighting | 0.32 (0.19 to 0.54) | |
Middle Weighting | 0.42 (0.21 to 0.84) | |
Progression-Free Survival Sensitivity Analysis 1b | ||
Number of Events, n (%) | 106 (69.3) | 145 (94.2) |
Median, Months (95% CI) | 7.0 (4.2 to 12.4) | 6.3 (4.6 to 8.2) |
Hazard Ratio (95% CI) | 0.61 (0.48 to 0.79) | |
Survival Rate at Time Point, % (95% CI) 12 Months | 44.1 (36.0 to 51.8) | 30.2 (23.0 to 27.6) |
Progression-Free Survival Sensitivity Analysis 2c | ||
Number of Events, n (%) | 59 (38.6) | 84 (54.5) |
Median, Months (95% CI) | NR | 23.5 (16.6 to 32.6) |
Hazard Ratio (95% CI) | 0.63 (0.45 to 0.88) | |
Survival Rate at Time Point, % (95% CI) | ||
6 Months | 81.0 (73.9 to 86.4) | 82.0 (74.9 to 87.3) |
9 Months | 77.8 (70.3 to 83.6) | 75.4 (67.7 to 81.5) |
12 Months | 75.8 (68.2 to 81.8) | 67.4 (59.2 to 74.2) |
18 Months | 68.0 (59.9 to 74.7) | 55.1 (46.7 to 62.7) |
24 Months | 64.7 (56.6 to 71.7) | 49.6 (41.3 to 57.3) |
Overall Survival Adjusting for Subsequent Anti-PD1/PDL1 Treatment Using Inverse Probability of Censoring Weighting | ||
Number of Events, n (%) | 56 (36.6) | 39 (25.3) |
Median, Months (95% CI) | NR | 15.2 (15.2 to 15.2) |
Hazard Ratio (95% CI) | 0.54 (0.27 to 1.39) | |
Overall Survival Adjusting for Subsequent Anti-PD1/PDL1 Treatment Using Rank Preserving Structural Failure Time | ||
Number of Events, n (%) | 56 (36.6) | 57 (37.0) |
Median, Months (95% CI) | NR | NR (20.2 to NR) |
Hazard Ratio (95% CI) | 0.72 (0.47 to 1.11) | |
Overall Survival Adjusting for Subsequent Anti-PD1/PDL1 Treatment Using Two-Stage Analysis | ||
Number of Events, n (%) | 56 (36.6) | 31 (20.1) |
Median, Months (95% CI) | NR | NR |
Hazard Ratio (95% CI) | 0.89 (0.76 to 1.04) | |
Time to Response | ||
Number of Patients with Response, n (%) | 67 (43.8) | 51 (33.1) |
Mean, Months (SD) | 4.0 (3.7) | 3.6 (4.1) |
Median, Months (Range) | 2.2 (1.8 to 18.8) | 2.1 (1.7 to 24.9) |
95% CI = 95% confidence interval; NR = not reached; SOC = standard of care
aNo CIs were provided by the sponsor.
bEvents were defined as the first of death, disease progression, crossover to opposite arm or subsequent use of another anticancer medication
cEvents were defined as the first death or disease progression on next line of therapy
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – core 30 items (EORTC QLQ-C30)
European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – colorectal cancer module 29 items (EORTC QLQ-CR29)
European Quality of Life Scale – 5 Dimensions – 3 Levels (EQ-5D-3L)
Findings
Table 43: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | 30-item, patient-reported, cancer-specific, quality of life questionnaire using 4- and 7-point Likert scales. | Validity, reliability, and responsiveness: Evidence of validity and reliability in populations with cancer. No literature was identified that assessed responsiveness in populations with cancer. Limited evidence supporting adequate validity, reliability, and responsiveness in patients with CRC. | Patients with cancer:
Patients with CRC:
|
EORTC QLQ-CR29 | 29-item, patient-reported, CRC-specific, quality of life questionnaire using a 4-point Likert scale to be administered with EORTC QLQ-C30. | Validity: Evidence of validity was of indeterminate quality in patients with CRC. Reliability: Insufficient evidence of reliability in patients with CRC. Responsiveness: Evidence of responsiveness was of indeterminate quality in patients with CRC | No MID identified in patients with CRC. |
EQ-5D-3L | Patient-reported, generic quality of life instrument using a 3-point ordinal scale to assess health in 5 dimensions. | Validity: Moderate to poor ability to distinguish between cancer severity by 3 scales (self-reported health status, ECOG PS, stage of cancer). Reliability: Evidence of acceptable reliability for 5 functioning scales and global health status in patients with CRC. Responsiveness: No literature was identified that assessed responsiveness in patients with CRC. | MID 0.033 to 0.074 estimated for the general population. MID 0.07 to 0.11 for UK-index scores and 0.05 to 0.08 for US-index scores for patients with cancer. VAS MID 6-10 for patients with cancer. No MID identified in patients with CRC. |
CRC = colorectal cancer; ECOG PS = Eastern Cooperative Oncology Group-Performance Status; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – core 30 items; EORTC QLQ-CR29 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – colorectal cancer module 29 items; EQ-5D-3L = European Quality of Life Scale – 5 Dimensions – 3 Levels; MID = minimal important difference.
aFor select scales, see Table 27 for details.
EORTC QLQ-C30
Description
The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-Core 30, or EORTC QLQ-C30, is one of the most commonly used patient-reported outcome measures in oncology clinical trials.43 It is a multi-dimensional, cancer-specific, evaluative measure of health-related quality of life (HRQoL). It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials in response to treatment.44 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item quality of life (QoL) scale, as outlined in Table 44. The first 2 versions of the questionnaire have been previously validated in patients with cancer.45 Version 3.0 of the questionnaire is the most current version and has been in use since December of 1997.46 It is available in 90 languages and is intended for use in adult populations only. The global QoL scale is also known as the Global Health Status.47
Table 44: EORTC QLQ-C30 Scales
Functional Scales (15 Questions) | Symptom Scales (7 Questions) | Single-Item Symptom Scales (6 Questions) | Global Quality of Life (2 Questions) |
|---|---|---|---|
Physical function (5) Role function (2) Cognitive function (2) Emotional function (4) Social function (2) | Fatigue (3) Pain (2) Nausea and vomiting (2) | Dyspnea (1) Insomnia (1) Appetite loss (1) Constipation (1) Diarrhea (1) Financial impact (1) | Global Quality of Life (2) |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period to assess function and symptoms.46 Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from one to 4. For the 2 items that form the global QoL scale, the response format is a 7-point Likert-type scale with anchors at 1 = “very poor” and 7 = “excellent.”
Raw scores for each scale are computed as the average of the items that contribute to a particular scale.46 This scaling approach is based on the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of one unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scale would reflect an improvement. According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.
Psychometric properties
Validity
One cross-sectional study aimed to validate the EORTC QLQ-C30 in a convenience sample of cancer patients in Singapore.48 Most patients had breast and colorectal cancers, but leukemia, lung cancer, lymphoma, germ cell tumour, and other cancers were also reported. Construct validity was assessed by cross-sectional correlational evidence and discriminative evidence. First, convergent validity was assessed using Spearman’s correlations between QLQ-C30 and Short Form-36 (SF-36) scales, hypothesizing moderate to strong correlation (defined as correlation coefficient of 0.35 to 0.5, and > 0.5, respectively) between scales of these 2 instruments measuring similar dimensions of HRQoL. Results showed moderate to strong correlations between QLQ-C30 and SF-36 scales, ranging from 0.35 to 0.67 across the assessed scales. Next, known-groups approach was used to compare 6 QLQ-C30 scale scores between patients reporting mild and severe symptoms, as well as by stage of disease and presence of comorbid conditions. With the exception of emotional functioning, the remaining 5 scales showed better scores in patients with mild symptoms than those with severe symptoms (P < 0.05 for all other comparisons). Patients in early stages of cancer (or with no comorbid conditions) generally had better QLQ-C30 scores than those in advanced disease stages (or with comorbid conditions); however, none of these differences were statistically significant.
A recent cross-sectional study in Kenya was conducted to evaluate the psychometric properties of the EORTC QLQ-C30, using the English or Kiswahili version in 100 patients with cancer.47 Most patients had breast cancer, followed by prostate, Kaposi sarcoma, lung, and other cancers. Construct validity was assessed by examining the inter-scale correlations among the subscales of EORTC QLQ-C30. The inter-scale correlations were weak to strong with an absolute magnitude ranging from 0.07 to 0.73. Notably, with the exception of cognitive functioning, emotional functioning, nausea and vomiting, dyspnea, appetite loss, constipation, and diarrhea, the Global Health Status correlated moderately with the remaining subscales (r ≥ 0.30). Cross-cultural validity was evaluated but not reported here.
Reliability
The Singaporean cross-sectional study above also assessed internal consistency reliability by calculating Cronbach α for all QLQ-C30 scales.48 Cronbach α was ≥ 0.70 for 6 of the 9 assessed QLQ-C30 scales; cognitive functioning, physical functioning, and nausea and vomiting had a Cronbach α ranging from 0.19 to 0.68.
The Kenyan study described above assessed the internal consistency of each scale of the questionnaire using Cronbach α-coefficients.47 With the exception of the cognitive function scale, all of the scales had a Cronbach α ≥ 0.70.
No studies evaluating the responsiveness of the instrument were not found.
MID
For use in clinical trials, scores on the EORTC QLQ-C30 can be compared between different groups of patients or within a group of patients over time. One study from 1998 conducted in patients with breast cancer and small cell lung cancer estimated a clinically relevant change in score on any scale of the EORTC QLQ-C30 to be 10 points.49 The estimate was based on a study that used an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Participants who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported being “very much” changed had corresponding changes of more than 20 points.
More recently in 2015, a Canadian study estimated the MIDs of EORTC QLQ-C30 scales using data from 193 patients newly diagnosed with breast and colorectal cancers.50 The Supportive Care Needs Survey-Short Form-34 (SCNS-SF34) was used as an anchor; mean changes in EORTC QLQ-C30 scales associated with improvement, worsening, and no-change in supportive care based on the SCNS-SF34 was then calculated. MIDs were assessed for the following scales: physical function, role function, emotional function, global health/QoL (i.e., the Global Health Status), pain, and fatigue. For improvement, MIDs associated with a statistically significant improvement in supportive care needs ranged from 10 to 32 points. For worsening, MIDs associated with a statistically significant worsening of supportive care needs ranged from 9 to 21 points. The range for unchanged supportive care needs was from 1-point worsening to 16-point improvement in EORTC QLQ-C30 score. Based on this, the authors suggested a 10-point change in EORTC QLQ-C30 score represented changes in supportive care needs, and therefore, should be considered for clinical use.
In 2014, another Canadian study estimated the MID for EORTC QLQ-C30 in 369 patients with advanced cancer who completed the questionnaire at baseline and 1-month post-radiation.51 The most common cancer type was breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other cancers. MID was estimated using both anchor- and distribution-based methods for improvement and deterioration. Two anchors of overall health and overall QoL were used, both taken directly from the EORTC QLQ-C30 (questions 29 and 30) where patients rated their overall health and QoL themselves. Improvement and deterioration were categorized as an increase or decrease by 2 units to account for the natural fluctuation of patient scoring. With these 2 anchors, the estimated MIDs across all EORTC QLQ-C30 scales ranged from 9.1 units to 23.5 units for improvement, and from 7.2 units to 13.5 units for deterioration. Distribution-based estimates were closest to 0.5 SD.
EORTC QLQ-C30 for patients with CRC
Wong et al. conducted a systematic review of HRQoL instruments used to assess patients with CRC which examined the psychometric properties of the instruments.52 The level of evidence supporting the measurements was ranked on a 4-point Likert scale of “poor,” “fair,” “good,” or “excellent” and each instrument was given an overall rating of “unknown,” “limited,” “moderate,” or “strong.” Table 26 summarizes the findings. In general, very few instruments demonstrated moderate or excellent evidence supporting the psychometric properties that were investigated though there was evidence identified for internal consistency, reliability, structural validity, a priori hypothesis testing, and responsiveness for the EORTC QLQ-C30.52
Table 45: Summary of Methodological Quality and Level of Evidence for Select HRQoL Instruments in Patients with CRC
Instrument | Internal consistency | Reliability | Content validity | Structural validity | Hypothesis testing | Cross-cultural validity | Criterion validity | Responsiveness |
|---|---|---|---|---|---|---|---|---|
EORTC QLQ-C30 (Version 1) | ||||||||
Methodological quality | Poor | — | — | Poor | Good/excellent | — | — | — |
Overall strength of evidence | Uncertain | — | — | Uncertain | Excellent | — | — | — |
EORTC QLQ-C30 (Version 3) | ||||||||
Methodological quality | Poor/good/excellent | Fair | — | Poor/good/excellent | Poor/good/excellent | Poor | Poor | Poor/fair/good |
Overall strength of evidence | Excellent | Limited | — | Uncertain | Excellent | Uncertain | Uncertain | Unknown |
EQ-5D | ||||||||
Methodological quality | — | Fair | — | — | Excellent | — | — | — |
Overall strength of evidence | — | Limited | — | — | Excellent | — | — | — |
FACT-C | ||||||||
Methodological quality | Poor | Fair | Excellent | Poor/excellent | Good/poor/excellent | Poor/fair | — | Fair/good |
Overall strength of evidence | Uncertain | Limited | Excellent | Uncertain | Excellent | Uncertain | — | Moderate |
CRC = colorectal cancer; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – core 30 items; EQ-5D = European Quality of Life Scale – 5 Dimensions; FACT-C = Functional Assessment of Cancer Therapy – Colon Cancer; HRQoL = health-related quality of life.
Source: Wong 201452
Musoro et al. compared EORTC QLQ-C30 data from 3 clinical trials (N = 1,491) to estimate MIDs of patients with advanced colorectal cancer (CRC) treated with chemotherapy.22 For their analyses, the financial impact scale was omitted. Clinical anchors were used and those with a correlation ≥ |0.3| were given priority in their analyses. To estimate the MID for within-group changes, an effect size was calculated from the mean score divided by the SD of the change scores for all time points. For between-group changes, linear regression was used. An effect size between 0.2 and 0.8 was deemed acceptable since a value < 0.2 was considered clinically unimportant while a value > 0.8 was more than minimally important. Table 27 summarizes MID estimates for within- and between-group changes of some scales. In general, the MIDs ranged from around 7 to 18 points and 4 to 10 points for improvement and deterioration within-group changes, respectively.22 MIDs for between-group changes were estimated to be from 5 to 14 points and 4 to 9 points for improvement and deterioration, respectively. Scales that are missing from the table (pain, cognitive function, social function, dyspnea, and insomnia) either did not have an anchor or had an effect size outside of the 0.2 to 0.8 range.
Table 46: EORTC QLQ-C30 With Anchor-Based MIDs for Within- and Between-Group Changes in Patients With CRC
Scale | Within-group change | Between-group change | ||
|---|---|---|---|---|
Improvement | Deterioration | Improvement | Deterioration | |
Physical functioning | 7.31 to 8.52 | –8.43 to –6.09 | 6.05 to 10.04 | –7.23 to –4.16 |
Role functioning | 10.43 to 18.06 | –10.66 | 7.95 to 14.17 | –9.96 |
Social functioning | 8.11 to 10.26 | –6.18 | 6.73 to 7.79 | –6.03 |
Global quality of life | 7.14 to 10.34 | –7.97 to –4.83 | 5.53 to 6.36 | –9.12 to –6.81 |
Fatiguea | 7.65 to 13.82 | –7.73 to –7.05 | 5.43 to 12.01 | –6. 98 to –6.76 |
Nausea and/or vomitinga | 7.75 | –7.95 to 5.30 | 7.34 | –7.33 to –5.17 |
Appetite lossa | 12.28 | –9.78 | 10.0 | –7.11 |
Diarrheaa | 6.35 | –7.96 | 8.25 | –5.46 |
Constipationa | 12.75 | No MIDb | 14.56 | No MIDb |
CRC = colorectal cancer; MID = minimal important difference.
aSymptom score directions were reversed to align with functioning scores (0 represents the worst possible scores and 100 represents the best)
bNo MID indicated either no suitable anchor was available or the effect size was outside of the 0.2 to 0.8 range.
Source: Musoro 202022
EORTC QLQ-CR29
In 2007, the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire – colorectal cancer module 29 items (EORTC QLQ-CR29) was developed as a revised version of its 38-item predecessor, EORTC QLQ-CR38, also specific to colorectal cancer.53 The 29-item version was updated based on evidence from the literature (n = 20), interviews with patients who had confirmed a confirmed CRC diagnosis (n = 199), and consultations with health care professionals (n = 11).54 It was designed to reflect newer treatments and different side effects of such treatments.53,54 While the EORTC QLQ-C30 is a generic QoL questionnaire for patients with any form of cancer, the EORTC QLQ-CR29 is a colorectal cancer-specific module, thus, the latter is a supplement to and is intended to be assessed alongside the generic QLQ-C30.53,54 The EORTC QLQ-CR29 uses a 4-point Likert scale to assess the following items: urinary frequency, blood/mucus in stools, stool frequency, body image, urinary incontinence, dysuria, abdominal pain, buttock pain, bloating, dry mouth, hair loss, taste, anxiety, weight, flatulence, fecal incontinence, sore skin, embarrassment, stoma care problems, sexual interest for men, sexual interest for women, impotence, and dyspareunia.53 The questionnaire has a recall period of one week. Raw scores are linearly transformed to a score from 0 to 100 where higher functioning scores and lower symptom scores indicate better QoL.
van der Hout et al. conducted a SLR to assess the psychometric properties of the EORTC QLQ-CR29.55 The review included 11 studies, though not all studies evaluated every property. In summary, structural and construct validity were both deemed indeterminate for methodological reasons and responsiveness was found to be indeterminate since there were inconsistencies with sensitivity to detect score changes. Evidence of subscale and single-item test-retest reliability was considered insufficient due to unacceptable ICCs (< 0.7) as well as missing values. Based on the 6 studies that were evaluated, urinary frequency and urinary incontinence had the lowest ICCs ranging from 0.33 to 0.68 and 0.11 to 1.0, respectively. There were no subscales or items that had ICCs > 0.7 for all 6 studies, though stool frequency, body image, buttock pain, and hair loss had ICCs > 0.7 for 4 of 6 studies. Internal consistency was rated sufficient though the quality of evidence was low. The authors concluded that further investigation of the properties of the EORTC QLQ-CR29 is needed.
Table 27 summarizes the findings of the Wong et al. systematic review of HRQoL instruments used to assess patients with CRC.52 In general, the investigators concluded that their literature search found evidence of moderate strength supporting reliability though the evidence supporting validity and responsiveness was of uncertain strength for the EORTC QLQ-CR29.
Whistance et al. conducted an international study of 351 patients with CRC in which patients completed both the EORTC QLQ-CR29 and QLQ-C30.56 Treatments included surgery, chemotherapy, radiotherapy, and palliative chemotherapy and patients were spread across the different tumour stages. The questionnaire scales had ICCs > 0.68 while individual items had ICCs > 0.55. The group calculated a correlation < 0.40 between the EORTC QLQ-CR29 and QLQ-C30 indicating the 2 questionnaires do not have overlapping topics.
No MID information was identified in patients with CRC.
EQ-5D-3L
The European Quality of Life Scale (EQ-5D) is a generic HRQoL instrument that may be applied to a wide range of health conditions and treatments.57,58 The first of 2 parts of the EQ-5D is a descriptive system that classifies respondents (aged ≥12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-3L has 3 possible levels (1, 2, or 3) for each domain representing ‘no problems,’ ‘some problems,’ and ‘extreme problems,’ respectively. Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions, corresponding with 243 different health states. A scoring function can be used to assign a value (EQ-5D-3L index score) to self-reported health states from a set of population-based preference weights.57,58 The second part is a 20 cm visual analogue scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of ‘worst imaginable health state’ and ‘best imaginable health state.’ Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ VAS which best represents their health on that day. Hence, the EQ-5D produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121, 33211
A population preference-weighted health index score based on the descriptive system,
A self-reported assessment of health status based on the EQ VAS.
The EQ-5D index score is generated by applying a multi-attribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). The lowest possible overall score for the 3L version (corresponding to severe problems on all 5 attributes) varies depending on the utility function that is applied to the descriptive system (e.g., −0.59 for the UK algorithm and −0.109 for the US algorithm). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states ‘dead’ and ‘perfect health,’ respectively. Reported MIDs for the 3L version of the scale have ranged from 0.033 to 0.074.23
Teckle et al. conducted a study of patients (N = 184) who had either breast (36%), colorectal (31%), or lung (33%) cancer at the Vancouver Cancer Clinic to investigate if disease severity could be distinguished by cancer-specific and generic preference-based instruments.59 Internal consistency was calculated using Cronbach α and all 5 functioning scales along with global health status showed acceptable consistency (α > 0.7) with values ranging from 0.77 to 0.82. Validity was assessed using Pearson’s correlation coefficient (r) where r between 0 and 0.3 demonstrated weak correlation, between 0.3 and 0.49 was moderate, and greater than 0.5 was considered strong. Teckle et al. found the following, between the EORTC QLQ-C30 and EQ-5D, r = 0.43; comparing the EORTC QLQ-C30 and EQ VAS, r = 0.73; and between EQ-5D and EQ VAS, r = 0.43. External validity was estimated between cancer severity (self-reported health status, ECOG Performance Status [ECOG PS], and cancer stage). An effect size (ES) between 0.2 and 0.5 was considered small, between 0.5 and 0.8 was medium, and greater than 0.8 was large. The EQ-5D was able to discriminate populations based on self-reported health status (excellent/good versus fair/very poor; ES = 0.90), and somewhat based on ECOG PS (0 versus 1 to 3; ES = 0.31), but not for stage of cancer (stages 1 and 2 versus stages 3 and 4; ES = 0.06). The EORTC QLQ-C30 performed better in all 3 areas: self-reported health status (ES = 1.39), ECOG PS (ES = 0.65), and stage of cancer (ES = 0.49). It is worth noting that the EQ-5D was based on a non-Canadian population and the comparison with EORTC QLQ-C30 was based solely on the 2 questions asking about overall health and QoL rather than the questionnaire as a whole. This study was a mixed population of 3 types of cancer and the results may not exactly reflect what would be observed in only patients with CRC. Furthermore, there was no information on what type of treatment the patients were receiving when completing the questionnaires.
Pickard et al. conducted a retrospective analysis of 534 patients with 11 types of cancer (including colon/rectal cancer) to estimate the MID using distribution-based (SEM, 1/2 SD, and 1/3 SD) and anchor-based (ECOG) methods.60 After stratifying by ECOG status, the mean weighted index score MID for all cancer patients was estimated to be between 0.07 and 0.11 for UK-index scores and between 0.05 and 0.08 for US-index scores. The VAS MID was estimated to range from 6 to 11 points for all patients.
No MID information was identified in patients with CRC.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
dMMR
mismatch repair deficient
FU
fluorouracil
ICER
incremental cost-effectiveness ratio
MSI-H
microsatellite instability-high
NMA
network meta-analysis
OS
overall survival
PAN
panitumumab
PFS
progression-free survival
QALY
quality-adjusted life-year
SOC
standard of care
WTP
willingness to pay
Executive Summary
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda),200 mg administered intravenously |
Submitted price | Pembrolizumab, 100 mg, solution: $4,400.00 per 100 mg/4 mL vial for IV infusion |
Indication | First-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair-deficient (dMMR) colorectal cancer |
Health Canada approval status | Complete |
Health Canada review pathway | Standard |
NOC date | March 3, 2021 |
Reimbursement request | As per indication |
Sponsor | Merck |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for multiple indications at CADTH. The following indications were reviewed in 2020: Indication: Metastatic squamous non–small cell lung cancer Recommendation date: January 3, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level Indication: Advanced renal cell carcinoma Recommendation date: April 2, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level Indication: Metastatic or unresectable recurrent head and neck squamous cell carcinoma Recommendation date: December 22, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | First-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer |
Treatment | Pembrolizumab |
Comparators | SOC, consisting of mFOLFOX6 (oxaliplatin + leucovorin + 5-FU); FOLFIRI (irinotecan + leucovorin + 5-FU); mFOLFOX6 + cetuximab; FOLFIRI + cetuximab; mFOLFOX6 + bevacizumab; FOLFIRI + bevacizumab mFOLFOX6 (oxaliplatin + leucovorin + 5-FU) + panitumumab FOLFIRI (irinotecan + leucovorin + 5-FU) + panitumumab |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (15 years) |
Key data sources | KEYNOTE-177 trial, indirect treatment comparison (KEYNOTE-177 trial, NO16966 trial, Porschen 2007 trial, PRIME trial, TREE-1 trial) |
Submitted results | Based on the sequential analyses, the 2 optimal treatments (i.e., on the frontier) are SOC and pembrolizumab. ICER for pembrolizumab was $48,980 per QALY compared to SOC (incremental costs = $122,907; incremental QALYs = 2.51). Pembrolizumab was associated with more QALYs and lower total costs than mFOLFOX6 + panitumumab (i.e., pembrolizumab is dominant), and FOLFIRI + panitumumab is ruled out as an optimal option by extended dominance through SOC and pembrolizumab. |
Key limitations | The sponsor incorporated treatment-specific utilities, which does not reflect CADTH guidelines. Furthermore, the EQ-5D values applied to the “pre-progression” and “progressed disease” health states lacked face validity as they closely approximated population norms among people without metastatic disease. According to feedback from the clinical experts consulted by CADTH for this review, assumptions about whether patients received brand name bevacizumab (i.e., Avastin) (86%) vs. the biosimilar equivalent (14%), and the degree of drug wastage associated with the administration of bevacizumab and panitumumab, did not reflect clinical practice. The sponsor’s approach for defining the comparator treatments limited their comparability to Canadian clinical practice. Comparators included cetuximab-based regimens, which are not funded in Canada for this indication; included regimens that are relevant exclusively to a narrow subset of all patients with MSI-H/dMMR metastatic or unresectable colorectal cancer; and excluded several relevant comparators that represent current SOC in Canada. The sponsor incorporated an estimate of the cost of administering IV drugs that does not align with Canadian clinical practice based on feedback from the clinical experts consulted by CADTH for this review. The modelled time horizon of 15 years is not long enough to reflect all relevant costs and outcomes for the decision. |
CADTH reanalysis results | CADTH reanalyses included the revision of utility weights for each health state; a combination of vial sharing and drug wastage for bevacizumab and panitumumab; an assumption that all recipients of bevacizumab received the biosimilar equivalent; a revised cost estimate for the administration of IV drugs; and a longer time horizon. CADTH was unable to address uncertainty associated with the omission of relevant treatment comparators.
|
dMMR = mismatch repair deficient; EQ-5D = EuroQol 5-Dimensions questionnaire; FU = fluorouracil; ICER = incremental cost-effectiveness ratio; incr. = incremental; LY = life-year; MSI-H = microsatellite instability-high; QALY = quality-adjusted life-year; SOC = standard of care; WTP = willingness to pay.
Conclusions
CADTH undertook reanalyses to address limitations with the sponsor’s submission, including revised utility weights for the progression-free survival (PFS) and progressed disease health states; revised assumptions about how bevacizumab and panitumumab are administrated in clinical practice (i.e., use of bevacizumab biosimilar price, magnitude of drug wastage); revised assumption that 0% in the standard of care (SOC) comparator are treated with cetuximab-based regimens; revised resource use cost estimate for the administration of IV drugs; and extended model time horizon. In the CADTH base case, pembrolizumab and SOC were considered optimal treatments (i.e., on the efficiency frontier), while mFOLFOX6 plus panitumumab (PAN) and FOLFIRI + PAN were not. Pembrolizumab was more costly (incremental cost = $173,843) and more effective (incremental quality-adjusted life-years [QALYs] = 2.80) than SOC, generating an incremental cost-effectiveness ratio (ICER) of $62,090 per QALY for pembrolizumab compared with SOC. Pembrolizumab had a 1% chance of being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY. A price reduction of at least 21% is needed for pembrolizumab to be cost-effective at a WTP threshold of $50,000 per QALY when compared with SOC. The estimated QALY benefit associated with pembrolizumab was based on the assumed relationship between PFS and overall survival (OS). CADTH’s Clinical Review found that there was insufficient evidence within the trial data of an OS benefit. The cost-effectiveness analysis was sensitive to this assumption and the time horizon of the analysis.
Due to the lack of comparative data, CADTH was unable to address the omission of relevant comparators within the economic model. As such, the cost-effectiveness of pembrolizumab compared with commonly used first-line treatments in Canada remains unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups (Colorectal Cancer Canada and the Colorectal Cancer Resource and Action Network) participated in a national online survey, focus group, and phone interviews to contribute to CADTH’s appraisal of the pharmacoeconomic analysis of pembrolizumab for the first-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair-deficient (dMMR) colorectal cancer. The participants included adult patients and caregivers from Canada (n = 6), the US (n = 3), and Malaysia (n = 1). Several important symptoms that affect quality of life were reported: bloody stools, diarrhea, fatigue, pain, and memory loss. Chemotherapy, radiation therapy, and surgery are often the SOC for patients with advanced MSI-H/dMMR colorectal cancer. Patients expressed a desire for new treatments that reduce or eliminate treatment symptoms, provide a cure, prolong life, improve quality of life, and involve simpler administration. Two participants had experience taking pembrolizumab and reported that diarrhea, bloody stools, and constipation were managed less effectively while taking pembrolizumab than with other therapies.
One registered clinician and 1 clinician input group reported that the SOC in the first-line treatment setting for unresectable or metastatic MSI-H/dMMR colorectal cancer includes 5-fluorouracil (FU) backbone regimens (FOLFIRI, mFOLFOX6, FOLFOXIRI, FOLFIRINOX) with or without biologics (i.e., bevacizumab) or anti–epidermal growth factor receptor therapy. The expectation for pembrolizumab was that it would improve OS, delay disease progression, and improve health-related quality of life.
The drug plans highlighted considerations for the implementation of pembrolizumab as relevant to the economic analysis. One issue was that infrastructure to facilitate MSI-H/dMMR testing needs to be in place to identify patients who would be eligible for treatment with pembrolizumab. The input from the plans also suggested that more patients would be tested for MSI-H/dMMR mutations than was reflected in the sponsor’s budget impact model. Another issue was the potential reduction in drug wastage with the fixed dosing regimen, though this approach would be higher in cost than weight-based dosing for patients weighing less than 100 kg.
Several of these concerns were addressed in the sponsor’s model:
PFS and OS were modelled for the overall population.
The sponsor incorporated quality of life impacts of treatment-related symptoms (i.e., use of treatment-specific utility), though the appropriateness of the methodology and the extent to which such estimates characterized health-related quality of life in the indicated population is uncertain. The cost impacts of treatment-related symptoms were also incorporated. Adverse events (AEs) included in the sponsor’s model were grade 3 or higher. However, the impacts of experiencing bloody stools and constipation associated with pembrolizumab use, which the patient inputs explicitly reported, were not accounted for.
The cost impacts of MSI-H/dMMR testing were included.
In addition, CADTH addressed some of these concerns as follows:
CADTH incorporated feedback from the drug plans in a sensitivity analysis to address the possibility that a greater proportion of patients will be tested for MSI-H/dMMR mutations than the sponsor modelled.
CADTH was unable to address the following concerns raised from stakeholder input:
Within the economic model, the dosing regimens that the sponsor included for pembrolizumab were limited to the fixed-dose approaches (i.e., 200 mg every 3 weeks or 400 mg every 6 weeks) per the KEYNOTE-177 trial.1 The sponsor did not include an option to assess the effects of weight-based dosing for pembrolizumab, and as such, CADTH was unable to explore such options further. Nonetheless, the clinical experts consulted by CADTH for this review reported that the fixed dose of 200 mg every 3 weeks is preferred.
Economic Review
The current review is for pembrolizumab (Keytruda) for the first-line treatment of adult patients with unresectable or metastatic MSI-H/dMMR colorectal cancer.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of pembrolizumab compared with 3 comparators: SOC, mFOLFOX6 (oxaliplatin plus leucovorin plus 5-FU) plus PAN (mFOLFOX6 + PAN), and FOLFIRI (irinotecan plus leucovorin plus 5-FU) plus PAN (FOLFIRI + PAN).2 The model population comprised adult patients with unresectable or metastatic MSI-H/dMMR colorectal cancer. This population was consistent with the Health Canada indication and the reimbursement request.
The recommended dosing regimen for pembrolizumab is 200 mg every 3 weeks, which should be administered as an IV infusion until disease progression or unacceptable toxicity, or for a maximum of 35 treatment cycles in patients without disease progression per the KEYNOTE-177 trial.1 At the sponsor’s submitted price of $4,400.00 per 100 mg/4mL vial of pembrolizumab, the total drug acquisition cost of each 21-day treatment cycle within the model was $8,800.00.2 Except for bevacizumab and PAN, the sponsor did not incorporate the effects of drug wastage for pembrolizumab or other drugs in the model comparators. The sponsor assumed SOC included 6 regimens: mFOLFOX6, FOLFIRI, mFOLFOX6 plus cetuximab, FOLFIRI plus cetuximab, mFOLFOX6 plus bevacizumab, and FOLFIRI plus bevacizumab. The percentage of patients assumed to be treated with each of these SOC regimens was based on the KEYNOTE-177 trial. The modelled treatment costs of all comparators are summarized in Appendix 3, Table 10. The cost per treatment cycle for SOC was $2,554.27 to $2,646.17, for mFOLFOX6 + PAN was $4,681.57, and for FOLFIRI + PAN was $3,275.20.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime horizon (15 years) from the perspective of a publicly funded health care payer. Discounting (1.5% per annum) was applied to both costs and outcomes.
Model Structure
A partitioned survival model was developed in Microsoft Excel. The model comprised 3 health states characterized as PFS (time to the first documented tumour progressed as per the Response Evaluation Criteria in Solid Tumors version 1.1, to unacceptable toxicity, or to death from any cause), progressed disease, and death. The modelled time cycle was 1 week. The proportion of patients who were progression-free, who experienced progressed disease, or who were dead at any time over the model horizon was derived from non-mutually exclusive extrapolations of PFS and OS.
All patients entered the model in the PFS health state. Over time, the proportion of patients transitioning to progressed disease in each cycle was estimated as the difference between the proportion of living patients (estimated from the OS curve) and the proportion of patients who did not progress (estimated from the PFS curve). Patients who progressed were assumed to stop first-line treatment.
Model Inputs
The model’s population characteristics and clinical parameters were obtained from multiple studies of treatments for adults with metastatic or recurrent colorectal cancer. The mean measures modelled for patient age (61.2 years), weight (71.14 kg), and body surface area (1.81 m2) aligned with the KEYNOTE-177 trial’s all-comers population.1 The data used to characterize PFS, OS, duration on treatment, and the risk of AEs within the pembrolizumab and SOC comparators were obtained from the KEYNOTE-177 trial. For both comparators, the sponsor modelled the PFS curves using a piecewise approach by applying observed PFS data for the first 20 weeks, and thereafter an exponential distribution that was fit to PFS data from each treatment group, which was collected in the KEYNOTE-177 trial at 21 weeks and onwards (Appendix 3, Figure 2). The sponsor chose this approach using goodness-of-fit statistics (Akaike information criterion and Bayesian information criterion), feedback from clinical experts, and assessments of visual fit. Projections of OS were approximated for the pembrolizumab and SOC comparators using the same approach as for PFS. However, for SOC, the exponential function was fit to the sponsor’s 2-stage crossover-adjusted OS data (Appendix 3, Figure 3) since 56 of 154 patients (36%) in the SOC treatment arm of the KEYNOTE-177 trial switched to the pembrolizumab arm and an additional 35 of 154 patients (22.7%) in the SOC treatment arm received subsequent anti-PD1/PDL1 therapy. To model duration on treatment in this model, the sponsor applied observed KEYNOTE-177 trial data for the pembrolizumab comparator and an exponential extrapolation of these data for the SOC comparator. For these comparators, the sponsor included severe treatment-related AEs (grade 3 or higher) experienced by at least 5% of patients in either treatment arm of the KEYNOTE-177 trial. To model PFS, OS, duration on treatment, and the probability of AEs for the indirect comparators (i.e., FOLFIRI + PAN and mFOLFOX6 + PAN), the sponsor conducted a network meta-analysis (NMA) to estimate the comparative efficacy of mFOLFOX6 + PAN versus SOC. Given the maturity of SOC data from the KEYNOTE-177 study, the sponsor chose SOC to be the reference group within the NMA rather than pembrolizumab. The NMA was based on data from the KEYNOTE-177 trial, the NO16966 trial, the Porschen 2007 trial, the PRIME trial, and the TREE-1 trial. The sponsor assumed that the NMA outcomes for mFOLFOX6 + PAN could be used to approximate the comparative efficacy and safety outcomes between FOLFIRI + PAN and SOC as well. As such, for each of the indirect comparators in the model, PFS and OS were determined by applying hazard ratios from the NMA to PFS and OS extrapolations for SOC. The duration on treatment was assumed to be equal to the respective comparator’s PFS curve. To estimate the probability of AE for the additional comparators, the sponsor applied an NMA-derived odds ratios to the odds of AEs in the SOC comparator.
Health state utility values were collected in the KEYNOTE-177 trial’s all-comers population using EQ-5D values with tariffs based on the US population. In the pembrolizumab treatment arm, the assessments occurred at treatment cycles 1, 2, 3, 4, 5, and 7; at treatment completion; and 30 days after treatment discontinuation. In the SOC arm, EQ-5D data were collected at treatment cycles 1, 2, 4, and 7; between cycles 5 and 6; at treatment completion; and 30 days after treatment discontinuation. The sponsor incorporated utility values in the base case that differed by health state. For the PFS health state, however, the value applied for SOC, mFOLFOX6 + PAN, and FOLFIRI + PAN (0.845) was lower than for pembrolizumab (0.881). For the progressed disease health state, the same utility weight (0.796) was used for all comparators. To model the utility impacts of experiencing severe treatment-related AEs (grade 3 or higher), the sponsor applied 1-off, treatment-specific QALY losses for pembrolizumab (0.021), SOC (0.024), mFOLFOX6 + PAN (0.050), and FOLFIRI + PAN (0.050).
The model included costs related to drug acquisition and administration, MSI-H/dMMR testing, AEs, subsequent therapy, surgery costs, resource use for each health state, and terminal care. Drug acquisition costs for the comparator treatments were sourced from 2 previous CADTH Economic Guidance Reports and a report by the Institut national d’excellence en santé et en services sociaux (INESSS).3-6 The cost of administering IV drugs was obtained from a published study.7 Subsequent therapy costs for mFOLFOX6, FOLFIRI, mFOLFOX6 plus bevacizumab, and FOLFIRI plus bevacizumab were modelled based on alternative distributions of drug use across all comparators and assumptions about the time on each drug. To inform the frequency of MSI-H/dMMR testing, health state resource use, surgery for each comparator, and AEs (grade 3 or higher), the sponsor incorporated data from the KEYNOTE-177 trial, the sponsor-conducted NMA, and other published sources.8-11 The costs for these resource items and terminal care were based on the Ontario Case Costing Initiative and literature.12-17
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented below.
Base-Case Results
In the sponsor’s base-case analysis, costs within the pembrolizumab comparator were estimated at an average of $345,886 and 4.85 QALYs over a 15-year time horizon. Costs and QALYs in the pembrolizumab comparator were higher than the SOC and FOLFIRI + PAN comparators. Costs were lower in the pembrolizumab comparator than in the mFOLFOX6 + PAN comparator, but QALYs were higher (Table 3). Based on a full sequential analysis, SOC is the preferred treatment option if a decision-maker’s WTP is below $48,980 per QALY, while pembrolizumab is the preferred treatment if the WTP threshold is greater than $48,980 per QALY. The mFOLFOX6 + PAN regimen was dominated by pembrolizumab, whereas FOLFIRI + PAN was extendedly dominated through SOC and pembrolizumab, indicating this treatment has a higher ICER when compared to SOC and the next most effective treatment (i.e., pembrolizumab). At a WTP of $50,000 per QALY, the probability of being considered the most likely cost-effective intervention was 61% for pembrolizumab, 39% for SOC, 0% for FOLFIRI + PAN, and 0% for mFOLFOX6 + PAN.
The majority of QALYs were accrued in the PFS state for pembrolizumab and in the progressed disease state for SOC, FOLFIRI + PAN, and mFOLFOX6 + PAN. The majority of total QALYs estimated for pembrolizumab (68%), FOLFIRI + PAN (60%), and mFOLFOX6 + PAN (60%) were accrued during the extrapolation period. At the end of the 15-year time horizon, the percentage of patients estimated to remain alive was 1% for SOC, 15% for pembrolizumab, 2% for FOLFIRI + PAN, and 2% for mFOLFOX6 + PAN. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs, $ | Total QALYs | Sequential ICER |
|---|---|---|---|
SOC | 222,979 | 2.34 | Reference |
FOLFIRI + PAN | 328,257 | 2.70 | Extendedly dominated through SOC and pembrolizumab |
Pembrolizumab | 345,886 | 4.85 | $48,980/QALY vs. SOC |
mFOLFOX6 + PAN | 376,881 | 2.68 | Dominated by pembrolizumab |
ICER = incremental cost-effectiveness ratio; PAN = panitumumab; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus .
Note: “Dominated” refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment. “Extendedly dominated” refers to a treatment having a higher ICER when compared to the next most cost-effective treatment. The submitted analysis is based on publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters in probabilistic scenario analyses, as reported in Appendix 3, Table 12. A scenario in which a Weibull function was used to estimate OS for the pembrolizumab and SOC arms produced an ICER that was 10% higher than in the base case.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Utility estimates were derived using uncertain methodology and lacked face validity: As per current CADTH guidelines for the conduct of economic evaluations, utilities should reflect the health states within the model and should not be specific to treatment.18 No justification was provided to support the use of the treatment-specific utility values within the PFS health state. The use of treatment-specific utilities within the model overestimated the incremental QALYs associated with pembrolizumab versus the comparators. Furthermore, the utility weights assigned to the PFS (pembrolizumab = 0.881; SOC, FOLFIRI + PAN, mFOLFOX6 + PAN = 0.845) and progressed disease (0.791) health states appeared to be clinically implausible as these values were either considerably higher than or similar to the EQ-5D population norms among 45- to 64-year-olds (mean = 0.83; standard deviation = 0.16) and 65- to 74-year-olds (mean = 0.82; standard deviation = 0.15) in Canada.19 As such, CADTH was concerned that the modelled utility weights appear to underestimate the severity of metastatic colorectal disease at baseline and the utility impacts associated with developing progressed disease following first-line treatment. Applying these utility weights led to an overestimation of total expected QALYs for all comparators, but particularly for pembrolizumab.
In the absence of Canadian utility estimates for unresectable or metastatic MSI-H/dMMR colorectal cancer, CADTH revised the input for the PFS health state to the lowest value submitted by the sponsor (range for PFS: 0.781 to 0.881), which was derived using European tariffs. For consistency in the type of tariffs used for estimating EQ-5D outcomes, CADTH applied the corresponding results for the progressed disease health state.
Sponsor’s characterization of bevacizumab and PAN’s administration does not reflect clinical practice in Canada: The sponsor incorporated inaccurate assumptions regarding the type of bevacizumab prescribed and the degree of drug wastage associated with bevacizumab and PAN’s administration. The sponsor assumed that 84% of patients receiving bevacizumab were prescribed the branded equivalent (i.e., Avastin). According to the clinical experts consulted by CADTH for this review, all new starts of chemotherapy would receive the biosimilar for bevacizumab rather than the branded drug. This assumption increased the total expected cost of the SOC comparator for the first-line treatment setting, biasing incremental costs in favour of bevacizumab. Additionally, the sponsor assumed that all unused drug contents were wasted during the administration of bevacizumab and PAN in clinical practice. Feedback from participating drug plans, however, indicated that a combination of vial sharing and drug wastage of about 12% is more likely to be observed. The clinical experts consulted by CADTH also confirmed these assumptions. The sponsor’s approach led to an inflation of the total expected costs of SOC, mFOLFOX6 + PAN, and FOLFIRI + PAN.
CADTH revised the base case to reflect 100% use of non-branded bevacizumab and revised the assumption of no vial sharing to 1 that incorporated a combination of vial sharing and 12% drug wastage.
The modelled comparators had limited generalizability to Canadian practice: CADTH identified multiple issues that limited the generalizability of modelled comparators to the indicated population. First, the sponsor submitted a comparison of pembrolizumab versus a pooled SOC strategy consisting of 6 chemotherapy regimens. As pooled efficacy and safety data from the KEYNOTE-177 trial’s SOC treatment arm were used to parameterize the SOC comparator, the sponsor assumed 10.4% of patients in the SOC comparator were treated with cetuximab. Clinical experts consulted by CADTH reported that cetuximab is not funded in Canada in the indicated patient population. Second, the clinical experts stated that the PAN-based comparators (mFOLFOX6 + PAN, FOLFIRI + PAN) were exclusively relevant to patients with distal tumours that are RAS wild type and metastatic — a clinical subgroup that composes less than 40% of the indicated population. The experts further noted that in some cases (e.g., in Ontario), funding for first-line treatment with PAN is permitted if the patient has a contraindication to bevacizumab (e.g., high risk of bleeding, cardiovascular disease). As such, the cost-effectiveness of pembrolizumab relative to the PAN-based regimens does not apply to the full indicated population. Third, according to the clinical experts’ feedback, the sponsor omitted several relevant comparators used in the first-line treatment setting in Canada: capecitabin, capecitabin plus bevacizumab, FU, FU plus bevacizumab, FOLFIRI, single-agent CAPOX, and single-agent irinotecan. The cost-effectiveness of pembrolizumab compared with such treatments that are missing from the model remains unknown.
CADTH revised the assumed percentage of patients who received cetuximab within the SOC comparator to 0% and redistributed an equal proportion of the percentage (2.6%) to each of the remaining chemotherapy regimens included in the SOC comparator.
Drug administration resource use was inappropriately calculated: To model the cost of administering IV drugs in the first-line treatment setting, the sponsor incorporated an estimate of $198 per hour of drug administration, as obtained from a published study.7 The sponsor did not report which health care resources were considered to derive this estimate, which likely inflated the total expected cost of the model comparators alone, and not the drug under review. The participating drug plans and the clinical experts consulted by CADTH reported that estimates of the cost of drug administration should primarily be based on a nurse’s time for administering the drug and monitoring adverse reactions.
CADTH revised the cost estimate for drug administration according to an hourly wage for an experienced nurse.20
The model’s time horizon was not long enough to reflect all relevant costs and outcomes: According to the current CADTH guidelines for the economic evaluation of health technologies, each model’s time horizon should be long enough to capture all potential differences in costs and outcomes associated with the interventions being compared.18 At the end of the modelled time horizon of 15 years within the sponsor’s economic model, 15% of the population within the pembrolizumab comparator was alive (7.5% in the PFS and progressed disease health states), whereas there was less than 2% survival in the remaining comparators. Capping the time horizon prematurely resulted in an underestimation of the total expected costs and QALYs for pembrolizumab during the extrapolation period, systematically improving the cost-effectiveness of the drug under review relative to the indirect comparators.
CADTH revised the time horizon to 30 years.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (see Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted As Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The parametric extrapolations of overall survival generated a large survival benefit for pembrolizumab vs. SOC | The survival benefit modelled for pembrolizumab vs. SOC remains uncertain. However, model results were robust to the use of alternate parametric functions for overall survival. |
Sponsor-conducted NMA that estimated the comparative efficacy of mFOLFOX + PAN vs. SOC was used to parameterize clinical outcomes for the mFOLFOX + PAN and FOLFIRI + PAN comparators | According to the CADTH Clinical Review Report, the results of the ITC-NMA should be interpreted with caution due to a variety of methodological concerns. However, the use of these results in the economic model was considered to be reasonable given the lack of any alternative data. |
Inclusion of a blended comparator of 6 different chemotherapy regimens | Where multiple comparators are relevant to the funding decision, treatments should be considered on their own, and all comparators should be assessed in a sequential analysis. Several alternative chemotherapy regimens are cheaper than the 21-day cycle cost of pembrolizumab based on its submitted price (e.g., $8,800 vs. $319 for FOLFIRI; see Appendix 1). However, the submitted model lacked the functionality to compare pembrolizumab with each of the 6 individual chemotherapy regimens such that differences in treatment costs and regimen-specific comparative efficacy and safety parameters for individual regimens were accounted for. As such, the interpretation of the economic value of pembrolizumab was restricted to a comparison with the pooled comparator, and the cost-effectiveness of pembrolizumab relative to individual SOC treatments is unknown. |
Arbitrary standard error of 10% applied within probabilistic analysis | The sponsor varied model parameters in the probabilistic analysis but applied an arbitrary standard error estimate of 10% to numerous parameters, including 20 estimates of the frequency of adverse events in the SOC, FOLFIRI + PAN, and mFOLFOX6 + PAN comparators. |
ITC = indirect treatment comparison; NMA = network meta-analysis; PAN = panitumumab; SOC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
To address limitations identified within the economic model, the CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (Table 5).
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | ||
Changes to derive the CADTH base case | ||
1. Utility estimates were derived using uncertain methodology and lacked face validity | Pre-progression health state:
Progressed disease health state: 0.791 | Pre-progression health state: 0.781 Progressed disease health state: 0.703 |
2. Inaccurate characterization of bevacizumab and PAN’s administration in clinical practice | Of those who take bevacizumab:
No vial sharing for bevacizumab or PAN | Of those who take bevacizumab
A combination of vial sharing and 12% drug wastage for bevacizumab or PAN |
3. Limited generalizability of model comparators | Percentage of treatment use within the SOC comparator:
| Percentage of treatment use within the SOC comparator:
|
4. Uncertainty in resource use cost estimates | $198.39 per hour of drug administration | $40 per hour of drug administration |
5. Inappropriate time horizon applied | 15 years | 30 years |
CADTH base case | Combined revisions 1 + 2 + 3 + 4 + 5 | |
PAN = panitumumab; SOC = standard of care.
CADTH undertook a stepped analysis, incorporating each change proposed in Table 5 to the sponsor’s base case to highlight the impact of each change (Table 6).
In CADTH’s base case, pembrolizumab was the most costly comparator ($372,511) and generated 4.93 QALYs over a 30-year time horizon. According to the sequential analysis, SOC is preferred if the WTP threshold is below $62,090 per QALY, while pembrolizumab is most cost-effective if the threshold is $62,090 per QALY or greater. The mFOLFOX6 + PAN regimen was dominated by FOLFIRI + PAN (i.e., was more costly and equally effective). FOLFIRI + PAN was extendedly dominated (had a higher sequential ICER than the next most effective treatment) through SOC and pembrolizumab, indicating this treatment has a higher ICER when compared to SOC as well as the next most effective treatment (i.e., pembrolizumab). The probability that pembrolizumab represented the most cost-effective strategy was 1% if the WTP threshold was $50,000 per QALY. The disaggregated results are reported in Appendix4, Table 14.
Seventy-one percent of pembrolizumab’s total expected QALYs were generated beyond the period for which observed data were available. Furthermore, 91% of pembrolizumab’s incremental QALYs compared with SOC (2.81 QALYs) were accrued during the extrapolated period. At the end of the 30-year time horizon, the percentage of patients estimated to remain alive was 2.5% for pembrolizumab and 0% for SOC, FOLFIRI + PAN, and mFOLFOX6 + PAN.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs, $ | Total QALYs | ICER vs. SOC, $/QALY | Sequential ICER |
|---|---|---|---|---|
SOC | 198,668 | 2.13 | Reference | Reference |
FOLFIRI + PAN | 304,174 | 2.48 | 296,745 | Extendedly dominated through SOC and pembrolizumab |
mFOLFOX6 + PAN | 348,630 | 2.48 | 421,780 | Dominated by FOLFIRI + PAN |
Pembrolizumab | 372,511 | 4.93 | 62,090 | $62,090/QALY vs. SOC |
ICER = incremental cost-effectiveness ratio; PAN = panitumumab; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Note: “Dominated” refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment. “Extendedly dominated” refers to a treatment having a higher ICER when compared to the next most cost-effective treatment. Reanalyses are based on publicly available prices of the comparator treatments.
Scenario Analysis Results
Price reduction analyses were conducted using both the sponsor and CADTH base cases (Table 7). Within the CADTH base case, a price reduction of at least 21% is needed for pembrolizumab to be considered cost-effective at a WTP threshold of $50,000 per QALY.
Table 7: CADTH Price Reduction Analyses
Price reduction | ICERs for pembrolizumab vs. SOC,a $/QALY | |
|---|---|---|
Sponsor base case | CADTH reanalysis | |
No price reduction | 48,980 | 62,090 |
10% | 42,489 | 56,276 |
20% | 35,964 | 50,397 |
30% | 29,502 | 44,731 |
40% | 22,985 | 38,841 |
50% | 16,422 | 32,908 |
60% | 10,211 | 27,107 |
70% | 3,331 | 21,410 |
80% | Pembrolizumab dominant | 15,608 |
90% | Pembrolizumab dominant | 9,688 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus .
Note: Only non-dominated strategies are presented. Reanalyses are based on publicly available prices of the comparator treatments.
aSince mFOLFOX plus panitumumab and FOLFIRI plus panitumumab remain off the efficiency frontier, the sequential analysis is focused on the comparison between pembrolizumab and SOC.
CADTH also performed analyses on alternate scenarios (Table 15). The scenarios included an assumption of perfect vial sharing (i.e., 100% wasted bevacizumab and PAN were administered to additional patients); an increased percentage of patients who were tested for MSI-H/dMMR mutations; hazard ratios of PFS and OS for mFOLFOX6 + PAN versus SOC and for FOLFIRI + PAN versus SOC being set to 1.0; the risk of AEs for mFOLFOX + PAN versus SOC and for FOLFIRI + PAN versus SOC being revised to 1.0; and an assumption that pembrolizumab and SOC had equal PFS beyond the extrapolated period.
Based on the sequential analysis across all but 1 of these scenarios, the ICER for pembrolizumab versus SOC did not change notably from the base case, and the PAN-based comparators remained dominated or extendedly dominated. In the scenario where pembrolizumab was assumed to have the same PFS as SOC beyond the trial period, the ICER for pembrolizumab versus SOC was $113,674 per QALY.
Taken together, the findings within the CADTH base-case reanalysis and scenario analyses suggest that in the absence of long-term data, the predicted incremental QALYs remain uncertain. The CADTH base-case and scenario results suggest that the magnitude of incremental QALYs appears to be driven by 2 principal factors: the large difference in PFS observed within the trial data, and assumptions about the length of the OS benefit. The sponsor’s use of a partitioned survival model, while appropriate for the decision question, introduces structural assumptions about the relationship between PFS and OS (i.e., non-mutually exclusive curves) that could not be adjusted for in reanalysis. These assumptions introduce a post-progression survival bias that favours pembrolizumab; however, the majority (92.81%) of incremental QALYs between pembrolizumab and SOC, as estimated within the CADTH reanalysis base case, were observed within the PFS state (Appendix 4, Table 14), suggesting that this structural bias has minimal impact on the cost-effectiveness results. The model findings were robust to changes in parametric extrapolation assumptions about OS.
Issues for Consideration
The submitted economic model did not include an option to assess a weight-based dosing regimen for pembrolizumab but, rather, 2 fixed-dose regimens (i.e., 200 mg every 3 weeks and 400 mg every 6 weeks) based on the anticipated Health Canada indication and the KEYNOTE-177 trial’s study protocol. Accordingly, the clinical experts consulted by CADTH for this review reported preference for the 200 mg dose administered every 3 weeks per the clinical trial. The experts noted that this regimen would be used in practice far more frequently than the 400 mg regimen every 6 weeks since the latter regimen required too few assessments while managing patients with metastatic colorectal cancer. Nonetheless, the drug plans suggested, given the variable practice recommendations in past CADTH pan-Canadian Oncology Drug Review Expert Review Committee recommendations for immune checkpoint inhibitors, that a weight-based dose up to a cap of the flat dose (i.e., 200 mg) may be applied in some parts of Canada. The cost-effectiveness of pembrolizumab’s weight-based dosing regimen, however, is unknown.
Overall Conclusions
Based on the CADTH Clinical Review of the KEYNOTE-177 study results, treatment with pembrolizumab increased PFS compared with SOC among patients with unresectable or metastatic MSI-H/dMMR colorectal cancer over the trial’s follow-up (3.6 years). The comparative effects of pembrolizumab relative to PAN-based regimens are unclear and to other commonly used treatments are unknown, as are the long-term effects of pembrolizumab in the indicated population. The extrapolated difference in PFS between pembrolizumab and SOC was a key driver in the economic analysis. The Clinical Review also found that the magnitude of the OS benefit is uncertain.
CADTH undertook reanalyses to address limitations with the sponsor’s submission, including revised utility weights for the PFS and progressed disease health states, revised assumptions about bevacizumab and PAN’s administration in clinical practice (i.e., use of bevacizumab biosimilar price, magnitude of drug wastage), a revised assumption that 0% in the SOC comparator are treated with cetuximab-based regimens, a revised resource use cost estimate for the administration of IV drugs, and an extended model time horizon. In the CADTH reanalysis, mFOLFOX6 + PAN was dominated (i.e., more costly and less effective) by FOLFIRI + PAN. FOLFIRI + PAN was extendedly dominated through SOC and pembrolizumab, indicating this treatment has a higher ICER when compared to SOC as well as the next most effective treatment (i.e., pembrolizumab). Pembrolizumab was more costly (incremental cost = $173,843) and more effective (incremental QALY = 2.80) than SOC, generating an ICER of $62,090 per QALY for pembrolizumab versus SOC at the listed price ($4,400.00 per 100 mg/4 mL vial). Pembrolizumab had a 1% chance of being cost-effective at a WTP threshold of $50,000 per QALY. A price reduction of at least 21% is needed for pembrolizumab to be cost-effective compared to SOC at a WTP threshold of $50,000.
The CADTH base-case results are associated with substantial uncertainty for multiple reasons. First, CADTH was unable to address the omission of relevant treatment comparators (capecitabin, capecitabin plus bevacizumab, FU, FU plus bevacizumab, FOLFIRI, single-agent CAPOX, and single-agent irinotecan); the cost-effectiveness of pembrolizumab compared with these comparators is unknown. Second, 91% of the incremental QALYs estimated for pembrolizumab versus SOC occurred during the extrapolated period. In a scenario analysis where no survival benefit for pembrolizumab was assumed beyond the trial period compared with SOC, the ICER for pembrolizumab versus SOC increased to $113,674 per QALY gained. Taken together, these findings suggest that the cost-effectiveness results were driven primarily by assumptions about the relationship between PFS and OS, which was uncertain within the trial data.
References
1.Andre T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207-2218. PubMed
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada; 2020.
3.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2020; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Feb 19.
4.MvasiMC - cancer colorectal métastatique. Avis transmis à la ministre en janvier 2019. Québec (QC): Institut national d’excellence en santé et en services sociaux; 2019: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Fevrier_2019/Mvasi_2019_01.pdf. Accessed 2021 Feb 19.
5.pan-Canadian Oncology Drug Review (pCODR) final economic guidance report: panitumumab (Vectibix) for left-sided metastatic colorectal cancer. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr_panitumumab_vectibix_ls_mcrc_fn_egr%20.pdf. Accessed 2021 Feb 19.
6.pan-Canadian Oncology Drug Review (pCODR) final economic guidance report: cetuximab (Erbitux) for metastatic colorectal cancer. Ottawa (ON): CADTH; 2014: https://www.cadth.ca/sites/default/files/pcodr/pcodr-erbitux-mcrc-fn-egr.pdf. Accessed 2021 Feb 19.
7.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
8.Riesco-Martinez MC, Berry SR, Ko YJ, et al. Cost-effectiveness analysis of different sequences of the use of epidermal growth factor receptor inhibitors for wild-type KRAS unresectable metastatic colorectal cancer. J Oncol Pract. 2016;12(6):e710-723. PubMed
9.Porgo TV, Moore L, Truchon C, et al. Patient-level resource use for injury admissions in Canada: a multicentre retrospective cohort study. Injury. 2019;50(6):1192-1201. PubMed
10.Cetuximab and panitumumab for previously untreated metastatic colorectal cancer. (NICE technology appraisal guidance TA439). London (UK): National Institute for Health and Care Excellence (NICE); 2017: https://www.nice.org.uk/guidance/ta439/resources/cetuximab-and-panitumumab-for-previously-untreated-metastatic-colorectal-cancer-pdf-82604732556229. Accessed 2021 Feb 19.
11.McKay A, Kutnikoff T, Taylor M. A cost-utility analysis of treatments for malignant liver tumours: a pilot project. HPB (Oxford). 2007;9(1):42-51. PubMed
12.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2021 Feb 8.
13.Lathia N, Mittmann N, DeAngelis C, et al. Evaluation of direct medical costs of hospitalization for febrile neutropenia. Cancer. 2010;116(3):742-748. PubMed
14.Dranitsaris G, Maroun J, Shah A. Severe chemotherapy-induced diarrhea in patients with colorectal cancer: a cost of illness analysis. Support Care Cancer. 2005;13(5):318-324. PubMed
15.Peterse EFP, Naber SK, Daly C, et al. Cost-effectiveness of active identification and subsequent colonoscopy surveillance of Lynch syndrome cases. Clin Gastroenterol Hepatol. 2020;18(12):2760-2767 e2712. PubMed
16.DNA mismatch repair deficiency tumour testing for patients with colorectal cancer: a health technology assessment. (CADTH optimal use report; vol.5, no.3b). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/OP0522_dMMR_Science_Report.pdf. Accessed 2021 Feb 19.
17.Fujiyoshi K, Yamamoto G, Takenoya T, et al. Metastatic pattern of stage IV colorectal cancer with high-frequency microsatellite instability as a prognostic factor. Anticancer Res. 2017;37(1):239-247. PubMed
18.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 Mar 2.
19.Alberta population norms for EQ-5D-5L. Edmonton (AB): University of Alberta; 2018: https://apersu.ca/wp-content/uploads/2021/02/Alberta-Norms-Report_APERSU.pdf. Accessed 2021 Feb 19.
20.Highlights of collective agreement changes as a result of the Kaplan award and items in agreement between ONA and participating hospitals. Toronto (ON): Ontario Nurses' Association; 2020: https://www.ona.org/wp-content/uploads/ona_hospitalcahighlightdoc_20180731f.pdf. Accessed 2021 Feb 19.
21.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2019. Toronto (ON): Canadian Cancer Society; 2019: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2019-EN.pdf?la=en. Accessed 2021 Mar 3.
22.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics - a 2018 special report on cancer incidence by stage. Toronto (ON): Canadian Cancer Society; 2018: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2018-EN.pdf?la=en. Accessed 2021 Mar 3.
23.Battaglin F, Naseem M, Lenz H-J, Salem ME. Microsatellite instability in colorectal cancer: overview of its clinical significance and novel perspectives. Clin Adv Hematol Oncol. 2018;16(11):735-745. PubMed
24.Halpern N, Goldberg Y, Kadouri L, et al. Clinical course and outcome of patients with high-level microsatellite instability cancers in a real-life setting: a retrospective analysis. Onco Targets Ther. 2017;10:1889-1896. PubMed
25.Annual demographic estimates: Canada, provinces and territories, 2019. Ottawa (ON): Statistics Canada; 2019: https://www150.statcan.gc.ca/n1/pub/91-215-x/91-215-x2019001-eng.htm. Accessed 2021 Mar 3.
26.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada; 2020.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Unresectable or Metastatic Microsatellite Instability-High or Mismatch Repair-Deficient Colorectal Cancer
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Pembrolizumab | 100 mg/4mL | Vial | 4,400.0000 | 200 mg Q3W | 419.05 | 11,733 |
Combination regimens | ||||||
mFOLFOX6 | 107.22 | 3,002 | ||||
Oxaliplatin | 50 mg/10mL | Vial | 36.2700 | 85 mg/m2 Q2W | 10.36 | 290 |
100 mg/20mL | Vial | 72.5400 | 10.36 | 290 | ||
5 mg/40mL | Vial | 145.0800 | 10.36 | 290 | ||
Leucovorin a | 50 mg/mL | Vial | 13.7886 | 400 mg/m2 Q2W | 73.87 | 2,068 |
500 mg/mL | Vial | 13.7886 | 98.49 | 2,758 | ||
Fluorouracil bolus | 5,000 mg/mL | Vial | 160.9000 | 400 mg/m2 Q2W | 11.49 | 322 |
Fluorouracil infusion | 5,000 mg/mL | Vial | 160.9000 | 2,400 mg/m2 Q2W | 11.49 | 322 |
FOLFIRI | 230.79 | 6,462 | ||||
Irinotecan | 20 mg/2mL | Vial | 208.3400 | 180 mg/m2 Q2W | 133.93 | 3,750 |
20 mg/5mL | Vial | 520.8500 | 148.81 | 4,167 | ||
20 mg/25mL | Vial | 2,604.2500 | 186.02 | 5,209 | ||
Leucovorin a | 50 mg/mL | Vial | 13.7886 | 400 mg/m2 Q2W | 73.87 | 2,068 |
500 mg/mL | Vial | 13.7886 | 98.49 | 2,758 | ||
Fluorouracil bolus | 5,000 mg/mL | Vial | 160.9000 | 400 mg/m2 Q2W | 11.49 | 322 |
Fluorouracil infusion | 5,000 mg/mL | Vial | 160.9000 | 2,400 mg/m2 Q2W | 11.49 | 322 |
mFOLFOX6 + panitumumab | 153.06 | 4,286 | ||||
mFOLFOX6 | - | - | - | - | 107.22 | 3,002 |
panitumumab | 100 mg/5mL | Vial | 641.8200 | 6mg/kg Q2W | 45.84 | 1,284 |
400 mg/8mL | Vial | 2,567.2800 | 183.38 | 5,135 | ||
FOLFIRI + panitumumab | 277.63 | 7,746 | ||||
FOLFIRI | - | - | - | - | 230.79 | 6,462 |
panitumumab | 100 mg/5mL | Vial | 641.8200 | 6mg/kg Q2W | 45.84 | 1,284 |
400 mg/8mL | Vial | 2,567.2800 | 183.38 | 5,135 | ||
mFOLFOX6 + bevacizumab | 217.49 to 255.56 | 6,090 to 7,156 | ||||
mFOLFOX6 | - | - | - | - | 107.22 | 3,002 |
Bevacizumab (brand) | 4mL | Vial | 519.2000 | 5 mg/kg Q2W | 148.34 | 4,154 |
16mL | Vial | 2,076.800 | 148.34 | 4,154 | ||
Mvasi (bevacizumab biosimilar) | 4mL | Vial | 385.9600 | 110.27 | 3,088 | |
16mL | Vial | 1,543.7700 | 110.27 | 3,088 | ||
FOLFIRI + bevacizumab | 341.06 to 379.13 | 9,550 to 10,616 | ||||
FOLFIRI | - | - | - | - | 230.79 | 6,462 |
Bevacizumab (brand) | 4mL | Vial | 519.2000 | 5 mg/kg Q2W | 148.34 | 4,154 |
16mL | Vial | 2,076.800 | 148.34 | 4,154 | ||
Mvasi (bevacizumab biosimilar) | 4mL | Vial | 385.9600 | 110.27 | 3,088 | |
16mL | Vial | 1,543.7700 | 110.27 | 3,088 | ||
Capecitabine + bevacizumab | 117.59 to 155.66 | 3,293 to 4,359 | ||||
Capecitabine b | 150 mg 500 mg | Tab Tab | 0.4575 1.5250 | 2,000 mg/m2 daily on days 1-14 Q3W | 7.32 8.13 | 205 228 |
Bevacizumab (brand) | 4mL | Vial | 519.2000 | 5 mg/kg Q2W | 148.34 | 4,154 |
16mL | Vial | 2,076.800 | 148.34 | 4,154 | ||
Mvasi (bevacizumab biosimilar) | 4mL | Vial | 385.9600 | 110.27 | 3,088 | |
16mL | Vial | 1,543.7700 | 110.27 | 3,088 | ||
Fluorouracil + bevacizumab | 121.77 to 159.84 | 3,409 to 4,475 | ||||
Fluorouracil infusion | 5,000 mg/mL | Vial | 160.9000 | 2,400 mg/m2 Q2W | 11.49 | 322 |
Bevacizumab (brand) | 4mL | Vial | 519.2000 | 5 mg/kg Q2W | 148.34 | 4,154 |
16mL | Vial | 2,076.800 | 148.34 | 4,154 | ||
Mvasi (bevacizumab biosimilar) | 4mL | Vial | 385.9600 | 110.27 | 3,088 | |
16mL | Vial | 1,543.7700 | 110.27 | 3,088 | ||
CAPOX | 20.27 | 568 | ||||
Capecitabine b | 150 mg 500 mg | Tab Tab | 0.4575 1.5250 | 2,000 mg/m2 daily on days 1-14 Q3W | 7.32 8.13 | 205 228 |
Oxaliplatin | 50 mg/10mL | Vial | 518.1600 | 130 mg/m2 Q2W | 12.95 | 363 |
100 mg/20mL | Vial | 1,036.3200 | 12.95 | 363 | ||
5 mg/40mL | Vial | 2,072.6400 | 12.95 | 363 | ||
Single-agent regimens | ||||||
Capecitabine b | 150 mg 500 mg | Tab Tab | 0.4575 1.5250 | 2,500 mg/m2 per day for 14 days | 7.32 | 205 |
Irinotecan | 20 mg/2mL | Vial | 208.3400 | 180 mg/m2 Q2W | 133.93 | 3,750 |
20 mg/5mL | Vial | 520.8500 | ||||
20 mg/25mL | Vial | 2,604.2500 | ||||
Fluorouracil | 5,000 mg/mL | Vial | 160.9000 | 2,400 mg/m2 Q2W | 11.49 | 322 |
QW3 = every 3 weeks; Q2W = every 2 weeks
Note: All prices are from the Delta IQVIA database (accessed February 2021), unless otherwise indicated, and do not include dispensing fees. Dosing is based on Health Canada product monographs. For dosing that depends on weight or body surface area, CADTH assumed 71 kg or 1.8 m2. Total cost estimates per regimen are based on the cheapest combination of the component drugs.
aAlberta drug formulary
bOntario drug formulary
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Despite the inclusion of some relevant comparators, the SOC comparator was a pooled strategy of 6 chemotherapy regimens and several other treatments used in the first-line treatment setting were missing from the model. The cost-effectiveness of PEM compared with each of the individual chemotherapies, modelled within the SOC comparator, and omitted comparators remains unknown. |
Model has been adequately programmed and has sufficient face validity | Yes | The model was adequately programmed but had limited face validity with respect to the method used for estimating the duration on treatment for the indirect comparators, i.e., FOLFIRI + PAN and mFOLFOX6 + PAN. For each comparator, the duration on therapy was assumed to be equal to the respective comparator’s progression-free survival curve. In the absence of observed time on treatment data to address this limitation further, CADTH was unable to address this issue. |
Model structure is adequate for decision problem | No | While the model structure was adequate for the decision problem, the chosen approach for modelling the derivation of survival outcomes for the indirect treatment comparators (i.e., the application of hazard ratios) limited CADTH’s ability to perform scenario analyses or test the sensitivity of the model. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | The sponsor varied model parameters in the probabilistic analysis but applied an arbitrary standard error estimate of 10% to numerous parameters including 20 estimates of the frequency of adverse events in the SOC, FOLFIRI + PAN, mFOLFOX6 + PAN comparators. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | Parameter uncertainty and structural uncertainty in the survival outcomes for the direct comparators were adequately incorporated within the model. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | The report was generally well organized. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Table 10: Summary of Treatment Comparators in the Sponsor’s Economic Evaluation
Drug regimen | Cost per treatment dose | Cost per treatment cycle |
|---|---|---|
Drug under review | ||
Pembrolizumab | $8,800.00 | $8,800.00 every 21 days |
Modelled comparators | ||
Standard of care | $2,554.27 to $2,646.17 every 14 days a | |
mFOLFOX6 | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Oxaliplatin | $2.17 $13.03 $36.20 $1,569.27 | |
FOLFIRI | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Irinotecan | $2.17 $13.03 $36.20 $162.90 | |
mFOLFOX6 + cetuximab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Oxaliplatin Cetuximab – first dose Cetuximab – subsequent dose | $2.17 $13.03 $36.20 $1,569.27 $2,662.51 $1,664.07 | |
FOLFIRI + cetuximab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Irinotecan Cetuximab – first dose Cetuximab – subsequent dose | $2.17 $13.03 $36.20 $162.90 $2,662.51 $1,664.07 | |
mFOLFOX6 + bevacizumab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Oxaliplatin Bevacizumab | $2.17 $13.03 $36.20 $1,569.27 $2,648.43 | |
FOLFIRI + bevacizumab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Irinotecan Bevacizumab | $2.17 $13.03 $36.20 $1,569.27 $2,648.43 | |
mFOLFOX6 plus panitumumab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Oxaliplatin Panitumumab | $2.17 $13.03 $36.20 $1,569.27 $2,739.97 | $4,681.57 every 14 days |
FOLFIRI plus panitumumab | ||
Fluorouracil bolus Fluorouracil infusion Leucovorin Irinotecan Panitumumab | $2.17 $13.03 $36.20 $162.90 $2,739.97 | $3,275.20 every 14 days |
aDenotes the weighted sum of the standard of care comparator based on the assumed use of treatment regimens (mFOLFOX6, 9.1%; FOLFIRI, 11.0%; mFOLFOX6 plus cetuximab, 3.2%; FOLFIRI plus cetuximab, 7.1%; mFOLFOX6 plus bevacizumab, 43.5%; and FOLFIRI plus bevacizumab, 26%)
Figure 1: Percentage of Patients in Each Health State Within the Model
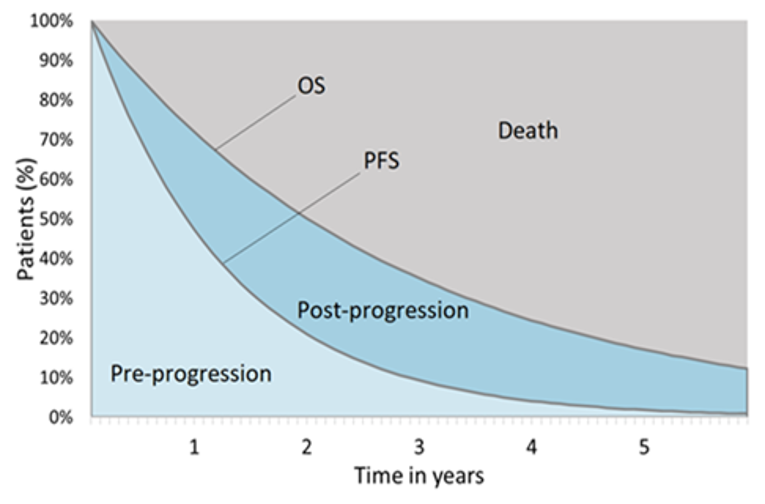
Source: Sponsor’s pharmacoeconomic submission.2
Figure 2: KM Plots and Exponential Extrapolations of Progression-Free Survival for Pembrolizumab and SOC
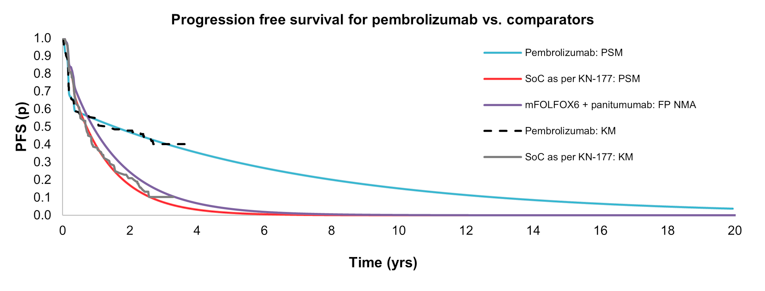
SOC = standard of care; KN-177 = KEYNOTE-177 trial; KM = Kaplan–Meier; FP NMA = fractional polynomials network meta-analysis; PSM = parametric survival model
Source: Sponsor’s pharmacoeconomic submission2
Figure 3: KM Plots and Exponential Extrapolations of Overall Survival for PEM and SOC
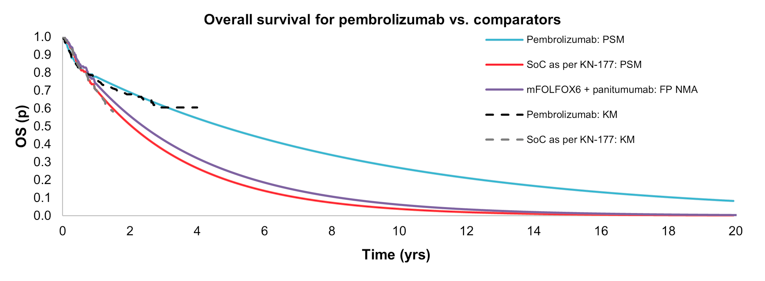
SOC = standard of care; KN-177 = KEYNOTE-177 trial; KM = Kaplan–Meier; FP NMA = fractional polynomials network meta-analysis; PSM = parametric survival model
Source: Sponsor’s pharmacoeconomic submission2
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. SOC) | |
|---|---|---|---|---|
Discounted LYs | ||||
SOC | PFS | 1.12 | - | |
PD | 1.78 | - | ||
Total | 2.90 | - | ||
FOLFIRI + PAN | PFS | 1.42 | 0.30 | |
PD | 1.93 | 0.15 | ||
Total | 3.35 | 0.45 | ||
PEM | PFS | 3.69 | 2.57 | |
PD | 2.04 | 0.26 | ||
Total | 5.73 | 2.83 | ||
mFOLFOX6 + PAN | PFS | 1.42 | 0.30 | |
PD | 1.93 | 0.15 | ||
Total | 3.35 | 0.45 | ||
Discounted QALYs | ||||
SOC | PFS | 0.95 | - | |
PD | 1.42 | - | ||
QALY loss due to AEs | −0.02 | - | ||
Total | 2.34 | - | ||
FOLFIRI + PAN | PFS | 1.20 | 0.26 | |
PD | 1.55 | 0.13 | ||
QALY loss due to AEs | −0.05 | −0.03 | ||
Total | 2.70 | 0.35 | ||
PEM | PFS | 3.25 | 2.31 | |
PD | 1.62 | 0.20 | ||
QALY loss due to AEs | −0.02 | 0.00 | ||
Total | 4.85 | 2.51 | ||
mFOLFOX6 + PAN | PFS | 1.20 | 0.26 | |
PD | 1.55 | 0.13 | ||
QALY loss due to AEs | −0.05 | −0.03 | ||
Total | 2.70 | 0.35 | ||
Discounted costs ($) | ||||
SOC | Testing | - | - | |
Drug acquisition | 52,211 | - | ||
Administration | 6,731 | - | ||
AEs | 6,808 | - | ||
Surgery | 384 | - | ||
Disease management | 118,363 | - | ||
Subsequent treatments | 15,975 | - | ||
End of life | 22,505 | - | ||
Total costs | 222,979 | - | ||
FOLFIRI + PAN | Testing | - | - | |
Drug acquisition | 121,568 | 69,357 | ||
Administration | 18,410 | 11,678 | ||
AEs | 15,947 | 9,139 | ||
Surgery | 384 | - | ||
Disease management | 129,867 | 11,503 | ||
Subsequent treatments | 19,970 | 3,995 | ||
End of life | 22,110 | −395 | ||
Total costs | 328,257 | 105,278 | ||
PEM | Testing | 501 | 501 | |
Drug acquisition | 162,987 | 110,776 | ||
Administration | 1,837 | −4,894 | ||
AEs | 2,393 | −4,415 | ||
Surgery | 387 | 3 | ||
Disease management | 148,333 | 29,970 | ||
Subsequent treatments | 10,618 | −5,358 | ||
End of life | 18,829 | −3,676 | ||
Total costs | 345,886 | 122,907 | ||
mFOLFOX6 + PAN | Testing | - | - | |
Drug acquisition | 173,770 | 121,559 | ||
Administration | 22,091 | 15,360 | ||
AEs | 15,947 | 9,139 | ||
Surgery | 384 | - | ||
Disease management | 129,867 | 11,503 | ||
Subsequent treatments | 12,711 | −3,265 | ||
End of life | 22,110 | −395 | ||
Total costs | 376,881 | 153,902 | ||
Sequential ICER ($) | ICER vs. SOC ($) | |||
SOC | ref | ref | ||
FOLFIRI + PAN | Extendedly dominated through SOC and PEM | $297,411 | ||
PEM | 48,980 | $48,980 | ||
mFOLFOX6 + PAN | Dominated by PEM | $434,773 | ||
AE = adverse events; PEM = pembrolizumab; mFOLFOX6 + PAN = mFOLFOX6 plus panitumumab; FOLFIRI + PAN = FOLFIRI plus panitumumab; SOC = standard of care; vs. = versus ; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year
Note: The submitted analysis is based on publicly available prices of the comparator treatments. Dominated refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment. Extendedly dominated refers to a treatment having a higher ICER when compared to the next most cost-effective treatment.
Source: Sponsor’s pharmacoeconomic submission.2
Table 12: Probabilistic Results of Sponsor’s Scenario Analyses
Scenario | ICER for PEM vs. SOC ($/QALY) | ICER for PEM vs. FOLFIRI + PAN ($/QALY) | ICER for PEM vs. mFOLFOX6 + PAN ($/QALY) | |
|---|---|---|---|---|
Base case | 48,980 | 8,992 | PEM dominates | |
1 | Time horizon: 10 years | 53,023 | PEM dominates | PEM dominates |
2 | Time horizon: 30 years | 48,470 | 15,867 | PEM dominates |
3 | Discount rate for costs, QALYs and LYs: 0% | 47,045 | 9,077 | PEM dominates |
4 | Discount rate for costs, QALYs and LYs: 3% | 51,431 | 7,383 | PEM dominates |
5 | Crossover method: RPSFTM | 40,301 | PEM dominates | PEM dominates |
6 | Crossover method: IPCW | 50,498 | 12,676 | PEM dominates |
7 | Exclude adjustment for wastage | 51,395 | 14,279 | PEM dominates |
8 | Subsequent treatment: KEYNOTE-177 trial | 46,569 | 8,727 | PEM dominates |
9 | PFS: PSM: Weibull | 51,402 | 7,295 | PEM dominates |
10 | OS: PSM: Weibull | 53,980 | 23,739 | 3,230 |
11 | ToT: PSM (SOC only): Weibull | 47,228 | 8,618 | PEM dominates |
12 | Utility: US algorithm, not pooled for progressed | 47,586 | 7,789 | PEM dominates |
13 | Utility: UK algorithm, pooled for progressed | 50,225 | 7,706 | PEM dominates |
14 | Utility: UK algorithm, not pooled for progressed | 48,171 | 6,718 | PEM dominates |
15 | Utility: EU algorithm, pooled for progressed | 51,434 | 8,822 | PEM dominates |
16 | Utility: EU algorithm, not pooled for progressed | 49,363 | 7,829 | PEM dominates |
17 | Treatment waning: Apply between 10 and 15 years | 48,240 | 5,526 | PEM dominates |
18 | AE disutilities: Do not apply, use HSUVs incl. AE disutilities | 49,557 | 8,827 | PEM dominates |
AE = adverse events; EU = European Union; m FOLFOX6 + PAN = mFOLFOX6 plus panitumumab; FOLFIRI + PAN = FOLFIRI plus panitumumab; IPCW = inverse proportion of censoring weighting; HSUV = health state utility values; SOC = standard of care; vs. = versus ; ICER = incremental cost-effectiveness ratio; LY = life-year; PEM = pembrolizumab; PFS = progression-free survival; PSM = parametric survival model; OS = overall survival; QALY = quality-adjusted life-year; RPSFTM = rank-preserving structural failure time model
aBased on sponsor’s deterministic analysis of the base case
Note: Dominated refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment.
Note: The submitted analysis is based on publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission2
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Druga | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 222,979 | 2.34 | ref |
FOLFIRI + PAN | 328,257 | 2.68 | Extendedly dominated through SOC and PEM | |
PEM | 345,886 | 4.85 | 48,980 vs. SOC | |
mFOLFOX6 + PAN | 376,881 | 2.68 | Dominated by PEM | |
CADTH reanalysis 1 – Utility weights | SOC | 223,404 | 2.11 | ref |
FOLFIRI + PAN | 328,605 | 2.43 | Extendedly dominated through SOC and PEM | |
PEM | 346,183 | 4.35 | $54,768 vs. SOC | |
mFOLFOX6 + PAN | 377,282 | 2.43 | Dominated by PEM | |
CADTH reanalysis 2 – Inputs for bevacizumab and panitumumab | SOC | 208,516 | 2.34 | ref |
FOLFIRI + PAN | 315,537 | 2.70 | Extendedly dominated through SOC and PEM | |
PEM | 344,065 | 4.85 | $53,993 vs. SOC | |
mFOLFOX6 + PAN | 362,984 | 2.70 | Dominated by PEM | |
CADTH reanalysis 3 – Percentage of treatment use within SOC comparator | SOC | 218,811 | 2.35 | ref |
FOLFIRI + PAN | 328,336 | 2.70 | Extendedly dominated through SOC and PEM | |
PEM | 346,053 | 4.85 | $50,730 vs. SOC | |
mFOLFOX6 + PAN | 377,047 | 2.70 | Dominated by PEM | |
CADTH reanalysis 4 – Resource use cost | SOC | 215,696 | 2.34 | ref |
FOLFIRI + PAN | 311,360 | 2.69 | Extendedly dominated through SOC and PEM | |
PEM | 343,215 | 4.86 | 50,760 vs. SOC | |
mFOLFOX6 + PAN | 356,776 | 2.69 | Dominated by PEM | |
CADTH reanalysis 5 – Time horizon | SOC | 224,166 | 2.36 | ref |
FOLFIRI + PAN | 331,584 | 2.74 | Extendedly dominated through SOC and PEM | |
PEM | 377,388 | 5.50 | 48,703 vs. SOC | |
mFOLFOX6 + PAN | 380,227 | 2.74 | Dominated by PEM | |
CADTH base case 1 + 2 + 3 + 4 + 5 | SOC | 198,668 | 2.13 | ref |
FOLFIRI + PAN | 304,174 | 2.48 | Extendedly dominated through SOC and PEM | |
mFOLFOX6 + PAN | 348,630 | 2.48 | Dominated by FOLFIRI + PAN | |
PEM | 372,511 | 4.93 | 62,090 vs. SOC |
AE = adverse events; PEM = pembrolizumab; mFOLFOX6 + PAN = mFOLFOX6 plus panitumumab; FOLFIRI + PAN = FOLFIRI plus panitumumab; SOC = standard of care; vs. = versus ; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year
aReference product is least costly alternative.
Note: Dominated refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment. Extendedly dominated refers to a treatment having a higher ICER when compared to the next most cost-effective treatment.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. SOC) |
|---|---|---|---|
Discounted LYs | |||
SOC | Total | 2.93 | - |
FOLFIRI + PAN | Total | 3.44 | 0.51 |
mFOLFOX6 + PAN | Total | 3.44 | 0.51 |
PEM | Total | 6.51 | 3.58 |
Discounted QALYs | |||
SOC | PFS | 0.88 | - |
PD | 1.27 | - | |
QALY loss due to AEs | −0.02 | - | |
Total | 2.13 | ||
FOLFIRI + PAN | PFS | 1.11 | 0.24 |
PD | 1.42 | 0.14 | |
QALY loss due to AEs | −0.05 | −0.03 | |
Total | 2.48 | 0.36 | |
mFOLFOX6 + PAN | PFS | 1.11 | 0.24 |
PD | 1.42 | 0.14 | |
QALY loss due to AEs | −0.05 | −0.03 | |
Total | 2.48 | 0.36 | |
PEM | PFS | 3.16 | 2.28 |
PD | 1.73 | 0.46 | |
QALY loss due to AEs | 0.03 | 0.06 | |
Total | 4.93 | 2.80 | |
Discounted costs ($) | |||
SOC | Testing | - | - |
Drug acquisition | 36,457 | - | |
Administration | 1,301 | - | |
AEs | 6,794 | - | |
Surgery | 386 | - | |
Disease management | 119,811 | - | |
Subsequent treatments | 11,217 | - | |
End of life | 22,703 | - | |
Total costs | 198,668 | - | |
FOLFIRI + PAN | Testing | - | - |
Drug acquisition | 111,295 | 74,838 | |
Administration | 3,719 | 2,418 | |
AEs | 15,879 | 9,086 | |
Surgery | 386 | - | |
Disease management | 134,303 | 14,492 | |
Subsequent treatments | 16,091 | 4,874 | |
End of life | 22,502 | −202 | |
Total costs | 304,174 | 105,506 | |
mFOLFOX6 + PAN | Testing | - | - |
Drug acquisition | 163,594 | 127,138 | |
Administration | 4,463 | 3,161 | |
AEs | 15,879 | 9,086 | |
Surgery | 386 | - | |
Disease management | 134,303 | 14,492 | |
Subsequent treatments | 7,503 | −3,714 | |
End of life | 22,502 | −202 | |
Total costs | 348,630 | 149,961 | |
PEM | Testing | 519 | 519 |
Drug acquisition | 162,992 | 126,535 | |
Administration | 370 | −931 | |
AEs | 2,389 | −4,405 | |
Surgery | 387 | 1 | |
Disease management | 177,001 | 57,190 | |
Subsequent treatments | 7,808 | −3,409 | |
End of life | 21,045 | −1,658 | |
Total costs | 372,511 | 173,843 | |
Sequential ICER ($/QALYs) | ICER vs. SOC ($) | ||
SOC | ref | ref | |
FOLFIRI + PAN | Extendedly dominated through SOC and PEM | 296,745 | |
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | 421,780 | |
PEM | 62,090 | 62,090 | |
AE = adverse events; PEM = pembrolizumab; mFOLFOX6 + PAN = mFOLFOX6 plus panitumumab; FOLFIRI + PAN = FOLFIRI plus panitumumab; SOC = standard of care; vs. = versus ; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year
aReference product is least costly alternative.
Note: Dominated refers to a treatment having a higher total cost and lower total QALYs when compared to the previous less costly treatment. Extendedly dominated refers to a treatment having a higher ICER when compared to the next most cost-effective treatment.
Scenario Analyses
Table 15: Summary of the CADTH Scenario Analysis
Scenario | Drug | Sequential ICER ($/QALY) | |
|---|---|---|---|
1 | Perfect vial sharing for bevacizumab and panitumumab (i.e., no drug wastage) | SOC | ref |
FOLFIRI + PAN | Extendedly dominated through SOC and pembrolizumab | ||
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | ||
pembrolizumab | 62,633 vs. SOC | ||
2 | Percentage who receive MSI-H/dMMR testing set to 85% per feedback from participating drug plans | SOC | ref |
FOLFIRI + PAN | Extendedly dominated through SOC and pembrolizumab | ||
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | ||
pembrolizumab | 61,979 vs. SOC | ||
3 | HRs used to derive PFS and OS for indirect treatment comparators, relative to SOC, were all set to 1.0 | SOC | ref |
FOLFIRI + PAN | Extendedly dominated through SOC and pembrolizumab | ||
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | ||
pembrolizumab | 62,098 vs. SOC | ||
4 | Odds ratio used to derive proportion who develop a serious adverse event for indirect treatment comparators, relative to SOC, set to 1.0 | SOC | ref |
FOLFIRI + PAN | Extendedly dominated through SOC and pembrolizumab | ||
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | ||
pembrolizumab | 62,034 vs. SOC | ||
5 | Assumption that pembrolizumab and SOC have equal progression-free survival beyond the trial period | SOC | ref |
FOLFIRI + PAN | Extendedly dominated through SOC and pembrolizumab | ||
mFOLFOX6 + PAN | Dominated by FOLFIRI + PAN | ||
pembrolizumab | 113,674 vs. SOC | ||
FOLFIRI + PAN = FOLFIRI plus panitumumab; ICER = incremental cost-effectiveness ratio; mFOLFOX6 + PAN = mFOLFOX6 plus panitumumab; MSI-H/dMMR = metastatic microsatellite/mismatch repair deficient QALY = quality-adjusted life-year; SOC = standard of care
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
The sponsor estimated the budget impact of pembrolizumab over 3 years. Several key limitations were identified including the assumed delay in PEM’s market share uptake, the percentage who received branded bevacizumab’s rather than generic, the cost estimate for drug administration, the proportion of patients tested for MSI-H/dMMR mutations, and vial sharing. CADTH reanalysis included revisions to the time to pembrolizumab’s market share uptake, percentage who received bevacizumab’s biosimilar equivalent, and the cost estimate for drug administration. While the sponsor’s results suggested the introduction of with pembrolizumab would lead to a budget impact of $45,395,210 over a 3-year time horizon, the CADTH reanalyses estimated a budget impact of $67,056,712 ($9,659,592 in year 1; $24,519,576 in year 2; $32,877,544 in year 3). CADTH noted these results were associated with substantial uncertainty, particularly with regards to assumptions made about the percentage who are tested for mutations. |
Summary of Sponsor’s BIA
The sponsor’s submitted budget impact analysis investigated the adoption of pembrolizumab as a first-line treatment option for patients with microsatellite instability-high (MSI-H) or mismatch repair deficiency (dMMR) unresectable or metastatic colorectal cancer. In the sponsor’s reference scenario, the current treatment comparators were mFOLFOX6 plus PAN, FOLFIRI plus pintumomab, mFOLFOX6 plus bevacizumab, FOLFIRI plus bevacizumab, FOLFIRI, mFOLFOX6, FOLFIRI plus cetuximab, FOLFOXIRI, FOLFOXIRI plus bevacizumab, fluorouracil plus leucovorin, fluorouracil, capecitabine, and capecitabin plus bevacizumab. The BIA was undertaken from the public payer perspective for the Canadian setting using a population-based approach over a 3-year projected time horizon (2022 to 2024). The BIA investigates the Canadian population, excluding Quebec. Key inputs to the BIA are documented in Table 15, and the following key assumptions were made:
The duration between pembrolizumab’s list date and the start of fiscal period was assumed to be zero months (i.e., no related budget impacts were accounted for during this time).
To derive the number of patients who would be eligible for first-line treatment, the sponsor first estimated: 1) the number of patients with stage IV disease; and, 2) the numbers of patients in stages I, II, or III as some of these individuals would later progress to stage IV (Figure 4).21,22 Next, 67% of individuals within each disease stage group were assumed to receive MSI-h/dMMR testing. Twenty percent of those tested in the stage I and II disease groups, 12% in the stage III disease group, and 4% in the stage IV disease group were expected to be diagnosed with MSI-H/dMMR colorectal cancer.23 In the stage I, II and III disease groups, 0%, 6%, and 55%, respectively, who had MSI-H/dMMR colorectal cancer were anticipated to progress to recurrent metastatic disease a year following the diagnosis.24 Finally, based on the sponsor’s internal data, 80% of patients with stage IV disease who were diagnosed with MSI-H/dMMR colorectal (n = 78/98) and 80% of those who progressed to stage IV a year after being diagnosed while in an earlier stage of disease (n = 212/265) were assumed to receive first-line treatment, resulting in an eligible population of 290 individuals in year 1.
BIA outcomes were estimated according to the number of patients expected to be treated each week, which was modelled to increase over time. The baseline number of patients initiating treatment at week 1 of the analysis was calculated by dividing the total treated in year 1 (n = 290) by the sum of 1 plus a 0.03% growth rate exponentiated to week i over 52 weeks.25 Each subsequent week in the analysis, the total treated per week increased by another 0.03%.
The number of patients initiating treatment is the same in the current and new drug scenarios, but the number of patients tested differed across scenarios. In each year of the reference scenario, the percentage tested for MSI-h/dMMR was 67% whereas in the new drug scenario, the percentage increased from 67% to 77% during year 1 based on a linear model and was 77% during years 2 and 3. These proportions were weighted by the assumed distribution who received an MSI test (0%), an MMR test (90%), or tests for both (10%).
In the new drug scenario, the market shares modelled for pembrolizumab increased from 0% to 80% over a 52-week period based on a linear model.
The duration of treatment for pembrolizumab were based on Kaplan–Meier data from the KEYNOTE-177 trial. For the comparators, the duration on treatment was based on the sponsor’s extrapolations of PFS in the submitted pharmacoeconomic model.
No vial sharing is assumed. As such, all unused drug contents were assumed to be wasted.
Second-line treatments included mFOLFOX6, mFOLFOX6 plus bevacizumab, FOLFIRI, FOLFIRI plus bevacizumab, XELOX. Only 29% of patients taking pembrolizumab were assumed to incur subsequent treatment costs, whereas 65% to 70% of those taking the alternate treatments received second-line treatment. The uptake of second-line treatments differed across model comparators, but each lasted 20.16 weeks.
Non-compliance is accounted for through relative dose intensity estimates lower than 100%, which are assumed to represent missed or delayed doses instead of lower doses than planned/recommended for all treatments.
Figure 4: Sponsor’s Estimation of the Size of the Eligible Population
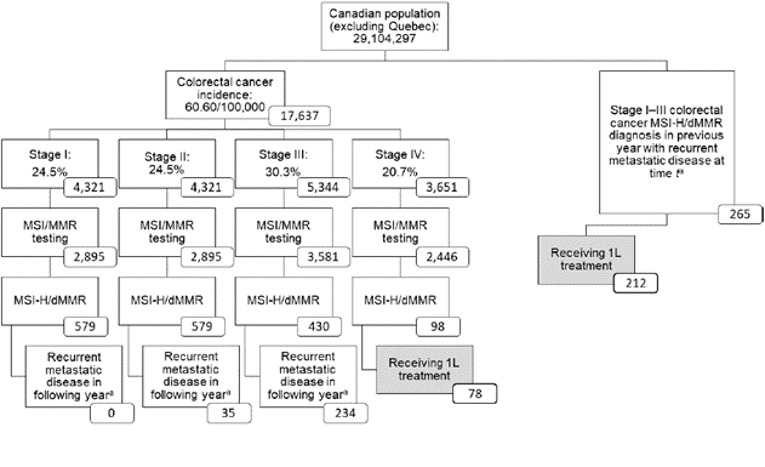
1L = first-line; dMMR = mismatch repair deficient = MMR, mismatch repair = MSI, microsatellite instability = MSI-H, microsatellite instability-high.
Note: Boxes shaded in grey refer to the target population in time t.
a Based on patients diagnosed with stage III colorectal cancer who then presented with recurrent metastatic disease and whose mean time for the diagnosis of recurrent metastatic disease was 17.5 months (range: 7 to 48 months).21
Source: Sponsor’s Budget Impact Analysis26
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate |
|---|---|
Target Population | Previously untreated patients with MSI-H/dMMR unresectable or metastatic colorectal cancer |
State how the sponsor derived the eligible population (stepwise), if not captured in a figure | See Figure 4
|
Number of incident patients eligible for drug under review, Year 1 / Year 2 / Year 3 | 312 / 332 / 337 |
Market Uptake (3 years) | |
Uptake each year (reference scenario and new drug scenarios) | See Table 18 |
Cost of treatment course (per patient) | |
Pembrolizumab mFOLFOX6 + panitumumab FOLFIRI + panitumumab mFOLFOX6 + bevacizumab FOLFIRI + bevacizumab FOLFIRI mFOLFOX6 FOLFIRI + cetuximab FOLFOXIRI FOLFOXIRI + bevacizumab Fluorouracil + leucovorin Fluorouracil Capecitabine Capecitabine + bevacizumab | $177,970 $189,211 $141,749 $71,601 $51,837 $27,473 $48,845 $98,343 $62,341 $89,711 $21,855 $15,262 $18,978 $40,618 |
MSI-H = microsatellite instability high; dMMR = mismatch repair deficiency
Table 18: Sponsor’s Estimation of Market Uptake in the New Drug Scenario
Comparator | Reference Scenario | New Drug Scenario at the end of Year 1 | New Drug Scenario Year 2 | New Drug Scenario Year 3 |
|---|---|---|---|---|
Pembrolizumab | 0.0% | 80.0% | 80.0% | 80.0% |
mFOLFOX6 + panitumumab | 4.1% | 0.8% | 0.8% | 0.8% |
FOLFIRI + panitumumab | 10.2% | 2.0% | 2.0% | 2.0% |
mFOLFOX6 + bevacizumab | 8.2% | 1.6% | 1.6% | 1.6% |
FOLFIRI + bevacizumab | 40.8% | 8.2% | 8.2% | 8.2% |
FOLFIRI | 8.2% | 1.6% | 1.6% | 1.6% |
mFOLFOX6 | 5.1% | 1.0% | 1.0% | 1.0% |
FOLFIRI + cetuximab | 1.0% | 0.2% | 0.2% | 0.2% |
FOLFOXIRI | 2.0% | 0.4% | 0.4% | 0.4% |
FOLFOXIRI + bevacizumab | 2.0% | 0.4% | 0.4% | 0.4% |
Fluorouracil + leucovorin | 2.0% | 0.4% | 0.4% | 0.4% |
Fluorouracil | 2.0% | 0.4% | 0.4% | 0.4% |
Capecitabine | 10.2% | 2.0% | 2.0% | 2.0% |
Capecitabine + bevacizumab | 4.1% | 0.8% | 0.8% | 0.8% |
Source: Sponsor’s Budget Impact Analysis26
Summary of the Sponsor’s BIA Results
The 3-year budget impact of pembrolizumab is $45,395,210. The annual budget impact was $2,993,245 in 2022, $15,276,624 in 2023, and $27,125,341 in 2024 (Table 3). Incremental drug acquisition costs ($51,551,425) contributed to the majority of the total budget impact over 3 years (114%; Table 4) but were partially offset due to given additional second-line drug acquisition costs and drug administration costs.
Stepped analysis | Annual Cost Year 1 | Annual Cost Year 2 | Annual Cost Year 3 | Three-year total |
|---|---|---|---|---|
Reference scenario | $9,389,309 | $18,516,767 | $21,928,254 | $49,834,331 |
New drug scenario | $12,382,554 | $33,793,392 | $49,053,595 | $95,229,540 |
Incremental costs | $2,993,245 | $15,276,624 | $27,125,341 | $45,395,210 |
Source: Sponsor’s Budget Impact Analysis
Table 20: Three-Year Cost Breakdown
Stepped analysis | Reference scenario | New drug scenario | Incremental costs |
|---|---|---|---|
First-line drug acquisition | $33,649,018 | $85,200,443 | $51,551,425 |
Second-line drug acquisition | $7,897,672 | $4,893,871 | -$3,003,801 |
First-line drug administration | $5,535,850 | $2,912,971 | -$2,622,879 |
Second-line drug administration | $1,620,620 | $950,289 | -$670,331 |
MSI/MMR testing | $1,131,170 | $1,271,966 | $140,796 |
Total | $49,834,331 | $95,229,540 | $45,395,210 |
Source: Sponsor’s Budget Impact Analysis26
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Unlikely delay applied to pembrolizumab’s market share uptake: The sponsor assumed that it would take 52 weeks for PEM’s total expected market share uptake to be achieved. According to drug plan feedback, the uptake of PEM versus existing systemic therapies is likely to be immediate. The modelled assumption considerably underestimated the total budget impact.
CADTH revised the time to PEM’s uptake to be 0 weeks.
Inappropriate assumptions characterizing bevacizumab’s biosimilar: Within the submitted BIA, first-line treatment comparators included bevacizumab-related regimens in which 100% of patients were assumed to receive the brand drug product, Avastin, rather than the biosimilar equivalent. In the submitted economic model, 84% were assumed to take Avastin. The clinical experts consulted by CADTH indicated that cetuximab is not funded in Canada for the current indication and that in practice, all new starts on chemotherapy would receive bevacizumab’s biosimilar. As such, the sponsor’s characterization of these comparators resulted in an underestimation of PEM’s budget impact.
CADTH revised the proportions who received cetuximab to 0%, Avastin to 0%, and bevacizumab’s biosimilar to 100%.
Uncertainty in resource use cost estimate: The sponsor assumed the cost of drug administration per hour was $198 and did not state which health care resources were included in this estimate. Participating drug plans and the clinical experts consulted by CADTH reported that the cost of drug administration should primarily be estimated based on a nurse’s time for administering the drug and monitoring adverse reactions. The sponsor’s cost estimate underestimated PEM’s budget impact.
CADTH revised the cost estimate for drug administration according to an hourly wage for an experienced nurse.
Underestimation of the percentage tested for MSI-H/dMMR mutations: According to the sponsor, 67% of patients with the indicated condition would undergo MSI-H/dMMR testing at baseline and that after 52 weeks, this proportion would increase to 77%. Input from participating drug plans suggested that a larger proportion of the patient population (approximately 85%) would need to be tested to identify all potential eligible patients. Accordingly, the sponsor’s approach likely underestimated the budget impact of PEM.
In a scenario analysis, CADTH tested a larger proportion of testing (85%) by 4 weeks.
No vial sharing: The sponsor assumed that all unused drug contents were wasted. Input from participating drug plans and the clinical experts suggested that a combination of vial sharing and drug wastage is likely to occur. The sponsor’s assumption of no vial sharing overestimated the total expected costs of the comparators and thereby underestimated PEM’s budget impact.
Whereas the sponsor’s economic model included the functionality to assess the combined impacts of vial sharing and drug wastage, the submitted BIA was not programmed to reflect drug wastage. As such, CADTH was only able to explore the impact of vial sharing in a scenario analysis.
CADTH Reanalyses of the BIA
Table 21: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | ||
Changes to derive the CADTH base case | ||
1. Unlikely delay applied to pembrolizumab’s market share uptake | 52 weeks | 0 weeks |
2. Limited comparability of the model comparators | 1% received cetuximab + FOLFIRI 100% received Avastin 0% received bevacizumab’s biosimilar | 1% received cetuximab + FOLFIRI 100% received Avastin 0% received bevacizumab’s biosimilar |
3. Uncertainty in resource use cost estimate | $198.39 per hour of drug administration | $40 per hour of drug administration |
CADTH base case | 1 + 2 + 3 | |
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 22 and a more detailed breakdown is presented in Table 23.
Table 22: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $45,395,210 |
CADTH reanalysis 1 | $58,946,326 |
CADTH reanalysis 2 | $49,414,297 |
CADTH reanalysis 3 | $47,906,419 |
CADTH base case | $67,056,712 |
BIA = budget impact analysis
Note: Reanalyses are based on publicly available prices of the comparator treatments.
In the CADTH reanalyses, the estimated a budget impact for PEM is $9,659,592 in year 1, $24,519,576 in year 2, $32,877,544 in year 3. After 3 years since entering the market, the total anticipated budget impact of PEM is $67,056,712. CADTH noted these resulted were associated with substantial uncertainty, particularly with regards to assumptions made about the percentage who are tested for mutations. If a price reduction of 21% is applied to PEM, the 3-year budget impact is $47,435,345.
Table 23: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|
Submitted base case | Reference | $9,389,309 | $18,516,767 | $21,928,254 | $49,834,331 |
New drug | $12,382,554 | $33,793,392 | $49,053,595 | $95,229,540 | |
Budget impact | $2,993,245 | $15,276,624 | $27,125,341 | $45,395,210 | |
CADTH base case | Reference | $7,060,153 | $13,936,475 | $16,591,535 | $37,588,163 |
New drug | $16,719,745 | $38,456,051 | $49,469,078 | $104,644,875 | |
Budget impact | $9,659,592 | $24,519,576 | $32,877,544 | $67,056,712 | |
CADTH scenario analysis: 21% price reduction | Reference | $7,060,153 | $13,936,475 | $16,591,535 | $37,588,163 |
New drug | $13,669,587 | $31,214,105 | $40,139,815 | $85,023,508 | |
Budget impact | $6,609,434 | $17,277,630 | $23,548,280 | $47,435,345 | |
85% tested for MSI-h/dMMR after 4 weeks | Reference | $8,284,798 | $15,693,646 | $18,397,028 | $42,375,473 |
New drug | $19,774,580 | $43,691,470 | $55,091,629 | $118,557,678 | |
Budget impact | $11,489,781 | $27,997,824 | $36,694,600 | $76,182,205 | |
Vial sharing assumed | Reference | $6,336,864 | $12,470,839 | $14,841,882 | $33,649,585 |
New drug | $16,528,003 | $38,079,149 | $48,977,679 | $103,584,832 | |
Budget impact | $10,191,140 | $25,608,310 | $34,135,797 | $69,935,247 |
BIA = budget impact analysis; dMMR = mismatch repair deficiency; MSI-H = microsatellite instability high
Note: Reanalyses are based on publicly available prices of the comparator treatments.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.