CADTH Reimbursement Review
Lorlatinib (Lorbrena)
Sponsor: Pfizer Canada
Therapeutic area: ALK-positive locally advanced or metastatic non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ALK
anaplastic lymphoma kinase
ALT
alanine transaminase
AST
aspartate transaminase
BICR
blinded independent central review
CI
confidence interval
CNS
central nervous system
CR
complete response
CrI
credible interval
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13
EQ-5D-5L
EQ-5D 5-Levels
EQ VAS
EQ-5D Visual Analogue Scale
FAS
full analysis set
HR
hazard ratio
HRQoL
health-related quality of life
IC
intracranial
IHC
immunohistochemistry
ITC
indirect treatment comparison
LCC
Lung Cancer Canada
MID
minimal important difference
NE
not estimable
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OR
odds ratio
ORR
objective response rate
OS
overall survival
pERC
CADTH pan-Canadian Oncology Drug Review Expert Review Committee
PR
partial response
PRO
patient-reported outcome
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumors Version 1.1
RPSFT
rank-preserving structural failure time
RR
relative risk
SAE
serious adverse event
SD
standard deviation
SE
standard error
TKI
tyrosine kinase inhibitor
TTD
time to deterioration
TTP
time to progression
TTR
time to response
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Lorlatinib (Lorbrena), 25 mg and 100 mg tablets, orally |
Indication | As monotherapy for the first-line treatment of adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Other: Expedited pathway — Project Orbis |
NOC date | June 7, 2021 |
Sponsor | Pfizer Canada |
ALK = anaplastic lymphoma kinase; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Source: Lorbrena product monograph.1
Introduction
Lung cancer is the most commonly diagnosed cancer in Canada and the leading cause of cancer-related deaths.2 The majority of lung cancers are classified as non–small cell lung cancer (NSCLC). The 5-year survival for patients with NSCLC is 25%, and this estimate is even lower for patients with metastatic NSCLC.3 Approximately 5% of NSCLC tumours harbour the anaplastic lymphoma kinase (ALK) tumour mutation, which is a rare mutation that is responsive to small-molecule tyrosine kinase inhibitors (TKIs).4,5 Patients with the ALK-positive NSCLC are highly susceptible to developing intracranial metastases and typically have a life expectancy of between 5 years and 10 years. Approximately 25% of patients develop intracranial metastases during the first year of their disease, and those who do not will develop intracranial metastases within 5 years.6 Treatment with TKIs may help increase the chance of patient survival.7
New-generation TKIs, such as alectinib and brigatinib, have become the new standards of care over crizotinib (a first-generation TKI) because of their improved efficacy and superior penetration of the blood-brain barrier for treating brain metastases. Alectinib is typically the first-line treatment choice for patients; however, the CADTH pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recently issued a positive reimbursement recommendation for brigatinib for the same indication. Brigatinib is currently under consideration for price negotiations with the pan-Canadian Pharmaceutical Alliance. The clinical experts consulted by CADTH indicated there is an unmet need for treatments after patients progress on first-line therapies, and that lorlatinib should be made available for use in multiple lines of therapy. The clinical experts stated that their preference would be to reserve use of lorlatinib for a later line of therapy unless the patient presented with active central nervous system (CNS) metastases, in which case the preference would be to use it as first-line treatment.
Lorlatinib is a selective, brain-penetrating, small molecule that competes with adenosine triphosphate for binding of ALK and ROS1 tyrosine kinases. This mechanism of action addresses resistance mechanisms following previous treatment with ALK inhibitor therapy.1 Lorlatinib was approved by Health Canada as monotherapy for the treatment of patients with ALK-positive locally advanced or metastatic NSCLC. The recommended dosage of lorlatinib is 100 mg orally once daily continuously. Treatment with lorlatinib should continue until disease progression or the advent of unacceptable toxicity.1 Previous CADTH reviews for advanced or metastatic ALK-positive NSCLC include brigatinib,8,9 lorlatinib,10 alectinib,11-13 ceritinib,14,15 and crizotinib.16 The previous CADTH review for lorlatinib was for the treatment of adult patients with ALK-positive metastatic NSCLC who had progressed on crizotinib and at least 1 other ALK inhibitor, or patients who had progressed on ceritinib or alectinib. The pERC review of lorlatinib for this indication in 2020–2021 resulted in a negative recommendation for reimbursement due to uncertain clinical benefits in this treatment setting stemming from limitations of the evidence, including a non-randomized clinical trial with no specific hypothesis testing.
The objective of this CADTH review is to perform a systematic review of the efficacy and safety of lorlatinib as monotherapy for the first-line treatment of patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
Input was received from 2 patient groups: CanCertainty Coalition and Lung Cancer Canada (LCC). Patients did not contribute to the submission from the CanCertainty Coalition. The received input highlighted the financial burdens associated with oral lung cancer treatments, which are not funded in the same manner as IV therapies, and coverage varies by province. In Ontario and the Atlantic provinces, only individuals over the age of 65 are automatically covered for oral oncology medications. According to CanCertainty, for patients without private insurance, access to medication requires navigating a complicated process of funding applications that are associated with approval delays, and most often result in patients incurring out-of-pocket costs. The group also indicated that the high cost of oral therapies may result in medication nonadherence, particularly among younger and lower-income patients.
The submission from LCC was based on data retrieved through interviews, questionnaires, and environmental scanning of records of patients and caregivers of patients with ALK-positive NSCLC. Data were received from 17 patients, including 9 females and 8 males, most of whom were 35 years of age or older. Twelve of the respondents were patients and 5 were caregivers. The LCC respondents were from Spain, the US, Canada, the UK, Switzerland, Philippines, and online.
Respondents in the LCC submission emphasized the unmet need for treatments that provide a cure for their lung cancer. Currently, all treatment options are considered palliative. Unmet need was also highlighted for patients with brain metastases, as there are few effective treatment options to treat brain involvement. Respondents described their experiences receiving crizotinib, ceritinib, alectinib, and chemotherapy. Crizotinib, while an effective treatment option, was described as not as effective against brain metastases, resulting in the need for radiation therapy. Patients also reported difficult side effects with crizotinib and ceritinib. Alectinib was described by LCC as the current standard of care for patients with ALK-positive NSCLC due to its efficacy and reduced toxicity compared to crizotinib, and as an effective treatment for patients with brain metastases. Chemotherapy was described to be associated with toxic side effects and limited benefit. The LCC submission also described the burden of disease on caregivers who are often at the centre of their loved one’s care and who often require taking time off work, resulting in further financial burden.
The LCC highlighted the following goals for treatments: improvement in disease symptoms, preservation of patient quality of life, manageable toxicity profiles for treatments, delayed progression, and maintenance of patient’s functionality and independence. The LCC gathered the experiences of 17 patients who had experience with lorlatinib; however, only 1 of these patients (from Spain) had received lorlatinib as first-line treatment. The respondents reported positive experiences with lorlatinib treatment, noting that it showed efficacy against their disease, including metastases, and therefore provided a sense of hope. Patients also commented that lorlatinib had a tolerable toxicity profile, improved their disease symptoms, and preserved independence and quality of life, with patients reporting being able to return to work, engaging in social activities, and having more energy.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The 2 clinical experts consulted by CADTH stated that, in Canada, alectinib is the first-line treatment used for most patients with ALK-positive NSCLC, although brigatinib is also an option. Lorlatinib would serve as another first-line option for patients; however, the clinicians highlighted that the use of lorlatinib would also be beneficial in later lines of therapy. According to the clinical experts, the goals of therapy are to prolong life, improve disease symptoms, maintain quality of life, delay progression, reduce the severity and frequency of symptoms, and reduce loss of cognition. Both clinical experts highlighted the need for curative therapies that are better tolerated and preserve patient quality of life. They also noted that improved biomarker-targeted therapies are needed to allow for multiple lines of therapy that provide patients with additional treatment options upon disease progression. Patients with brain metastases were highlighted as a group of patients with unmet needs, as currently there are few therapies that also have efficacy in the brain. Patients eligible for treatment are identified through imaging and ALK testing. Assessment varies by line of therapy, but typically patients are assessed every 3 months, with brain imaging conducted every 6 months. The clinical experts indicated that lorlatinib could be administered in inpatient and outpatient settings, and discontinuation of the drug would occur once patients experience clinical deterioration and cognitive dysfunction that affects quality of life.
Clinician Group Input
Two clinician group inputs were received, 1 from the Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee and 1 from LCC. In total, input was received from 26 clinicians. Identification of the patients who would be eligible for treatment was stated to occur up front, as ALK testing occurs at initial diagnosis. Both inputs identified alectinib and brigatinib, which is currently accessed through special access programs, as the available first-line treatments for patients with ALK-positive NSCLC. Both inputs noted that treatment goals include prolonging life; delaying disease and CNS progression; maintaining or improving quality of life; reducing severity of symptoms; minimizing adverse events (AEs); reducing the loss of cognition, memory and other sequalae of CNS metastases and its local treatments; and maintaining patient independence. The input from Cancer Care Ontario stated that many of these needs are addressed through alectinib; however, new treatments that provide longer control of symptomatic disease, improved progression-free survival (PFS) and overall survival (OS) are desired. Input from LCC indicated an unmet need for more effective therapies in the first line, alternative therapies to allow for individualization of therapy, convenient dosing of treatments, and more effective therapies that treat brain metastases. Both LCC and Cancer Care Ontario emphasized the need for more effective treatments in later lines of therapy, as patients eventually become refractory to currently available treatment options. While both groups acknowledged that lorlatinib would be a first-line option for patients, they also stated that lorlatinib could address treatment gaps in later lines of therapy. After patients progress on lorlatinib in the first line, TKIs are not typically available to patients in later lines of therapies and both clinician groups stated that use of ALK TKIs after first-line therapy would be preferential.
According to the clinician groups, assessment of a patient’s response to treatment is based on improvement of symptoms and assessment of radiographic response, as well as through PFS, OS, and intra- and extracranial PFS. The clinician groups agreed that testing for response should occur every 2 to 3 months, with imaging conducted every 2 to 6 months, or as needed. Patients would be discontinued from treatment due to disease progression or unmanageable toxicities. Lorlatinib would be administered in an outpatient setting, although community or inpatient settings were considered acceptable at times under the supervision of the prescribing oncologist.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. For the CADTH review of lorlatinib, the drug programs provided input and/or had questions pertaining to the initiation of therapy, the prescribing of therapy, generalizability, funding algorithms, care provision, and system and economic issues. The clinical experts consulted by CADTH weighed evidence from the CROWN trial and other clinical considerations to provide responses to questions, which can be found in the Drug Program Input section.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One multinational, multi-centre, randomized, active-controlled, open-label superiority trial met the criteria for the CADTH systematic review. The CROWN trial evaluated the efficacy and safety of lorlatinib compared to crizotinib as first-line treatment in adult patients with locally advanced or metastatic ALK-positive NSCLC who had not received previous systemic treatment for metastatic disease. Patients who were diagnosed with and treated for an earlier stage of disease were eligible for enrolment if their treatment was completed more than 12 months before randomization. Eligible patients were required to have their ALK status confirmed through an immunohistochemistry (IHC) test approved by the FDA or Pharmaceutical and Medical Devices Agency or marked by Conformité Européene performed on Ventana ULTRA or XT platforms and a good performance status defined as an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 2. Patients with brain metastases were eligible for enrolment.17
The trial recruited patients from 104 sites in 23 countries (in Asia, the European Union, and North America), including Canada. A total of 296 patients were randomized in a 1:1 ratio using an interactive web-based response technology system; 149 patients were randomized to the lorlatinib group and 147 patients were randomized to the crizotinib group. Randomization was stratified according to presence of brain metastases (yes versus no) and ethnic origin (Asian versus non-Asian). Patients randomized to the lorlatinib group received 100 mg daily, and patients randomized to the crizotinib group received 250 mg daily. Both lorlatinib and crizotinib were administered orally.17
The primary objective of the study was to determine whether lorlatinib was superior to crizotinib in prolonging PFS based on Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1) criteria according to a blinded independent central review (BICR). The trial was designed as a group sequential trial using a Lan-DeMets (O’Brien-Fleming) alpha spending function to determine efficacy boundaries. The overall significance level was preserved at 0.025 with a 1-sided stratified log-rank test. The trial results were based on an interim analysis (with a data cut-off date of March 20, 2020), after approximately 133 PFS events (75%) had occurred per BICR. A final analysis of PFS was specified only if the boundary for efficacy was not crossed at the interim analysis.
OS was planned as a secondary end point that was hierarchically tested if statistical significance was obtained for PFS. Other pre-planned exploratory end points of the trial included PFS according to investigator assessment, objective response rate (ORR), duration of response (DOR), time to response (TTR), and intracranial efficacy end points (intracranial objective response rate [IC-ORR], intracranial duration of response [IC-DOR], intracranial time to progression [IC-TTP], and intracranial time to response [TTR]); these end points were not part of the statistical testing hierarchy. Health-related quality of life (HRQoL) was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), its corresponding survey for lung cancer (EORTC QLQ-LC13), and the EQ-5D 5-Levels questionnaire (EQ-5D-5L).
Patient characteristics at baseline were mostly balanced between the treatment groups. Patients’ mean ages were 59 years (standard deviation [SD] = 13) in the lorlatinib group and 56 years (SD = 14) in the crizotinib group. A higher proportion of patients in the lorlatinib group were 65 years or older compared to patients in the crizotinib group (39.6% versus 29.9%, respectively). There were more females in both the lorlatinib (56.4%) and crizotinib (61.9%) groups. Most patients were White (48.2% versus 49.0%, respectively) or Asian (43.6% versus 44.2%, respectively).17 Almost all patients had measurable disease at baseline (96.6% versus 97.3%, respectively), with approximately one-quarter of patients presenting with brain metastasis (25.5% versus 27.2%, respectively). Most patients had an ECOG PS of 0 (45.0% versus 38.8%, respectively) or 1 (53.0% versus 55.1%, respectively), with the adenocarcinoma type of NSCLC (94.0% versus 95.2%, respectively), which is stage IV metastatic disease (90.6% versus 94.6%, respectively). Most patients were classified as either never smokers (54.4% versus 63.9%, respectively) or former smokers (36.9% versus 29.3%, respectively).17
Efficacy Results
Key efficacy results from the CROWN trial are reported in Table 2. Two analyses for PFS were planned, an interim and a final analysis. At the data cut-off date (March 20, 2020), results for PFS crossed the pre-specified stopping boundary for statistical significance, which favoured the lorlatinib group (stratified hazard ratio [HR] = 0.28; 95% confidence interval [CI], 0.191 to 0.413; stratified log-rank 1-sided P < 0.0001). The results for PFS at the data cut-off date were considered final. At the data cut-off date, OS was also tested in accordance with the statistical testing hierarchy, with the results showing that the majority of patients remained alive; there were 23 deaths (15.4%) in the lorlatinib group and 28 deaths (19.0%) in the crizotinib group and the between-group difference was not statistically significant (HR = 0.72; 95% CI, 0.414 to 1.249). The intracranial efficacy end points, including IC-ORR, IC-DOR, IC-TTP, and IC-TTR, were also assessed, with the results demonstrating a consistently improved response among patients with brain metastases who were treated with lorlatinib compared to those treated with crizotinib. However, the CROWN trial was not powered to assess these end points, and the analyses of intracranial efficacy end points are therefore considered exploratory.17
Health-related quality of life was assessed as a pre-specified exploratory end point in the CROWN trial. No clinically meaningful differences between treatment groups, based on a difference of at least 10 points, were observed in any of the EORTC QLQ-C30 functioning domains. In general, the mean change in scores from baseline to the end of study period were similar for the EORTC QLQ-C30 and QLQ-LC13 in both treatment groups in the Global Health Scale and subscales. Also, the mean scores in the EQ-5D-5L index and Visual Analogue Scale (EQ VAS) were similar in both treatment groups. The time to deterioration (TTD) analysis conducted for symptom scales in the EORTC QLQ-C30 also showed no differences between the lorlatinib and crizotinib groups.17
Harms Results
In general, AEs were more commonly reported in patients treated in the lorlatinib group than in the crizotinib group. The most common AEs in the lorlatinib group were hypercholesterolemia (70.5% versus 3.5% in the lorlatinib group), hypertriglyceridemia (63.8% versus 5.6%, respectively), edema (55.0% versus 39.4%, respectively), increased weight (38.3% versus 12.7%, respectively), peripheral neuropathy (33.6% versus 14.8%, respectively), cognitive effects (21.5% versus 5.6%, respectively), diarrhea (21.5% versus 52.1%, respectively), and dyspnea (20.1% versus 16.2%, respectively). More AEs related to CNS effects were reported in the lorlatinib group than in the crizotinib group (cognitive effects: 21.5% versus 5.6%, respectively; mood effects: 16.1% versus 4.9%; speech effects: 4.7% versus 0; psychotic effects: 3.4% versus 0). Serious adverse events (SAEs) of any grade (34.2% versus 27.5%) and grade 3 or 4 AEs (22.8% versus 17.6%) were higher in the lorlatinib group than in the crizotinib group, respectively.17 More AEs related to CNS effects were reported in the lorlatinib group than in the crizotinib group (cognitive effects: 21.5% versus 5.6%, respectively; mood effects: 16.1% versus 4.9%; speech effects: 4.7% versus 0; psychotic effects: 3.4% versus 0), and SAEs of any grade (34.2% versus 27.5%) and grade 3 or 4 (22.8% versus 17.6%) were higher in the lorlatinib group than in the crizotinib group, respectively.17
AEs that resulted in dose reductions were generally infrequent, occurring in 31 patients (20.8%) in the lorlatinib group and 22 patients (15.5%) in the crizotinib group. Grade 3 AEs resulting in dose reductions occurred in 9 patients (6.0%) in the lorlatinib group and 7 patients (4.9%) in the crizotinib group; no grade 4 AEs resulted in dose reductions in either treatment group. Dose interruptions due to AEs occurred in similar proportions of patients in both the lorlatinib (49.0%) and crizotinib (44.4%) treatment groups, with 32.9% and 36.6% of interruptions due to grade 3 or 4 AEs.17
Deaths occurred in 23 patients (15.4%) in the lorlatinib group and 18 patients (19.7%) in the crizotinib group, with most deaths considered to be due to disease progression (11.4% versus 16.2%, respectively).17
Notable harms identified by the sponsor included hypercholesterolemia, hypertriglyceridemia, edema, peripheral neuropathy, CNS effects, vision disorder, pneumonitis, weight gain, liver function test increase, QT prolongation, atrioventricular block, and pancreatitis, and these aligned with the CADTH protocol. Notable AEs were more common in the lorlatinib group, except for vision disorder and liver function test increase, which were more common in the crizotinib group than in the lorlatinib group (39.4% versus 18.1% and 37.3% versus 20.8%, respectively). The most common AEs of special interest were hypercholesterolemia (70.5% in the lorlatinib group versus 3.5% in the crizotinib group), hypertriglyceridemia (63.8% versus 5.6%, respectively), edema (55.0% versus 39.4%, respectively), weight gain (38.3% versus 12.7%, respectively), peripheral neuropathy (33.6% versus 14.8%, respectively), cognitive effects (21.5% versus 5.6%, respectively), liver function test increase (20.8% versus 37.3%, respectively), and mood effects (16.1% versus 4.9%, respectively).17
Table 2: Summary of Key Outcome Results From the CROWN Trial
Key outcomes | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Primary outcome: PFS per BICR | ||
Events, n (%) | 41 (27.5) | 86 (58.5) |
Median, months (95% CI) a | NE (NE to NE) | 9.3 (7.6 to 11.1) |
Stratified HR (95% CI)b,c | 0.28 (0.191 to 0.413) | 0.28 (0.191 to 0.413) |
Stratified log-rank 1-sided P valued | < 0.0001e | |
Secondary outcome: OS | ||
Events, n (%) | 23 (15.4) | 28 (19.0) |
Median, months (95% CI)a | NE (NE to NE) | NE (NE to NE) |
Stratified HR (95% CI)c | 0.72 (0.414 to 1.249) | |
Exploratory outcome: IC-TTP per BICR (modified RECIST 1.1) | ||
Events, n (%) | 5 (3.4) | 45 (30.6) |
Median, months (95% CI) | NE (NE to NE) | 16.6 (11.1 to NE) |
Stratified HR (95% CI)b,c | 0.07 (0.026 to 0.170) | |
Stratified log-rank 1-sided P valuee | < 0.0001f | |
Harms (safety analysis set), n (%) | ||
Patients with AEs | 149 (100.0) | 140 (98.6) |
Patients with maximum grade 3 or 4 AEs | 108 (72.5) | 79 (55.6) |
Patients with SAEs | 51 (34.2) | 39 (27.5) |
Patients with maximum grade 3 or 4 SAEs | 22.8 | 17.6 |
Patients discontinued study treatment due to AEs | 10 (6.7) | 13 (9.2) |
Patients with dose reduced or temporary discontinuation due to AEs | 79 (53.0) | 71 (50.0) |
Notable harms, n (%) | ||
Hypercholesterolemia | 105 (70.5) | 5 (3.5) |
Hypertriglyceridemia | 95 (63.8) | 8 (5.6) |
Edema | 82 (55.0) | 56 (39.4) |
Peripheral neuropathy | 50 (33.6) | 21 (14.8) |
CNS effects | ||
Cognitive effects | 32 (21.5) | 8 (5.6) |
Mood effects | 24 (16.1) | 7 (4.9) |
Speech effects | 7 (4.7) | 0 |
Psychotic effects | 5 (3.4) | 0 |
Vision disorder | 27 (18.1) | 56 (39.4) |
Pneumonitis | 2 (1.3) | 4 (2.8) |
Weight gain | 57 (38.3) | 18 (12.7) |
Liver function test increase | 31 (20.8) | 53 (37.3) |
QT prolongation | 5 (3.4) | 8 (5.6) |
Atrioventricular block | 4 (2.7) | 0 |
Pancreatitis | 23 (15.4) | 26 (18.3) |
AE = adverse event; BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; CI = confidence interval; HR = hazard ratio; IC-TTP = intracranial time to progression; IRT = interactive response technology; NE = not evaluable; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; SAE = serious adverse event.
aBased on the Brookmeyer and Crowley method.
bStratified by presence of brain metastases (yes or no) and ethnic origin (Asian or non-Asian) at randomization from IRT stratification values.
cHR based on Cox proportional hazards model under proportional hazards, HR < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to crizotinib.
dClopper-Pearson method used.
eP value was based on stratified log-rank test.
fP value was not adjusted for multiplicity.
Source: CROWN Clinical Study Report.17
Critical Appraisal
The CROWN trial was a multinational, multi-centre, open-label, phase III trial that employed a group sequential design. A BICR was implemented to assess end points that involved judgments of patients’ clinical progression (i.e., PFS, ORR, and DOR). However, it is possible that the open-label design posed a greater risk of bias for end points involving subjective reporting, such as HRQoL and safety (e.g., CNS effects).
The primary and secondary end points of the CROWN trial were PFS and OS. Both end points were considered in power calculations, and OS was tested hierarchically at the time of the data cut-off if PFS was deemed to be statistically significant. Other secondary and exploratory end points were not included in the statistical hierarchy. The statistically significant findings on subgroup analyses were likely subject to multiplicity and an inflated type I error rate. At the time of the data cut-off, the interim analysis of PFS had crossed the pre-specified efficacy boundary and showed a statistically significant difference in favour of lorlatinib, and the analysis was therefore considered final by the sponsor. However, OS data were deemed immature, as only 26% of the 198 OS events required for the final analysis of OS had occurred.17 An improvement in PFS may not always correlate with a difference in OS in assessments of oncology treatment benefit. In fact, mainly due to disease progression, a higher proportion of patients in the crizotinib group compared to the lorlatinib group (17.4% versus 58.5%, respectively) withdrew from the study. This would largely bias the estimate of OS in the final analysis. Therefore, further evidence is required to confirm the superiority of lorlatinib over crizotinib in treatment efficacy in terms of OS.
The majority of patients included in the CROWN trial had an ECOG PS score 0 or 1. The generalizability of the results in terms of a PFS benefit to patients with a poor ECOG PS remains unknown. Moreover, the study excluded patients with potential vascular or cardiac diseases, or those with unfavourable laboratory testing of renal, liver, pancreatic, or bone marrow function. In reality, the safety profile of lorlatinib for patients with those comorbidities or abnormal testing may be even worse considering that lorlatinib increased the risk of hypercholesterolemia and hypertriglyceridemia. The CROWN trial allowed for enrolment of patients with brain metastases, who accounted for 25.5% of the lorlatinib group and 27.2% of the crizotinib group.17 Inclusion of patients with brain metastases is highly relevant as many patients with ALK-positive metastatic NSCLC develop brain metastases. The results for the assessed intracranial-specific efficacy end points consistently showed numerically improved outcomes in the lorlatinib group compared with the crizotinib group. Despite the limitations associated with exploratory end points, the clinical experts consulted by CADTH recognized the results of patients with brain metastases as noteworthy.
Indirect Comparisons
Description of Studies
Four indirect treatment comparisons (ITCs) were summarized and critically appraised, including 1 from the sponsor18 and 3 published ITCs by Chuang et al. (2021),19 Wang et al. (2021),20 and Ando et al. (2021).21
The ITCs compared the safety and efficacy of lorlatinib to alectinib (600 mg and 300 mg), brigatinib, crizotinib, ceritinib, chemotherapy, and ensartinib among patients with ALK-positive metastatic NSCLC who had not received prior systemic treatment in the first line. While not all ITCs included comparisons to each of these treatments, all ITCs compared lorlatinib to alectinib, brigatinib, and crizotinib.
The sponsor’s ITC compared lorlatinib to alectinib (600 mg and 300mg), brigatinib, ceritinib (450 mg, 600 mg, 750 mg), crizotinib, chemotherapy, and ensartinib.18 Ando et al. (2021),21 compared lorlatinib to alectinib, brigatinib, ceritinib, crizotinib, and chemotherapy. Wang et al. (2021)20 compared lorlatinib to alectinib and brigatinib. Chuang et al. (2021)19 compared lorlatinib to alectinib (600 mg and 300 mg), brigatinib, crizotinib, and ensartinib.
Efficacy Results
Efficacy results reported here focus on PFS as this was the primary end point of all trials included in the ITCs.
Results of the sponsor’s ITC18 favoured lorlatinib over all comparators, including alectinib at 600 mg (HR = 0.61; 95% credible interval [CrI], 0.38 to 0.99), brigatinib (HR = 0.57; 95% CrI, 0.34 to 0.95), ceritinib at 750 mg (HR = 0.22; 95% CrI, 0.13 to 0.37), ceritinib at 450 mg (HR = 0.31; 95% CrI, 0.15 to 0.66), ceritinib at 600 mg (HR = 0.25; 95% CrI, 0.12 to 0.54), crizotinib (HR = 0.0.28; 95% CrI, 0.19 to 0.41), ensartinib (HR = 0.55; 95% CrI, 0.32 to 0.93), and chemotherapy (HR = 0.12; CrI, 0.08 to 0.19) except for alectinib at 300 mg (HR = 0.83; 95% CrI, 0.36 to 1.85).
The results in the ITC by Ando et al. (2021)21 favoured lorlatinib over all comparators, including brigatinib (HR = 0.572; 95% CrI, 0.326 to 0.997), ceritinib (HR = 0.220; 95% CrI, 0.131 to 0.367), crizotinib (HR = 0.280; 95% CrI, 0.191 to 0.411), and chemotherapy (HR = 0.121; 95% CrI, 0.078 to 0.187), except for alectinib (HR = 0.742; 95% CrI, 0.4666 to 1.180).21
The ITC by Wang et al. (2021)20 conducted comparisons among patients who were ALK inhibitor– and chemotherapy-naive, and patients who were ALK inhibitor–naive. Results favoured lorlatinib compared to alectinib (ALK inhibitor– or chemotherapy-naive patients: HR = 0.59; 95% CrI, 0.37 to 0.94; ALK inhibitor–naive: HR = 0.65; 95% CrI, 0.42 to 1.01) and brigatinib (ALK inhibitor– or chemotherapy-naive patients: HR = 0.54; 95% CrI, 0.31 to 0.94; ALK inhibitor–naive: HR = 0.57; 95% CrI, 0.34 to 0.95) in both groups of patients.
In the ITC by Chuang et al. (2021),19 lorlatinib was favoured over crizotinib (HR = 0.28; 95% CrI, 0.19 to 0.41), ensartinib (HR = 0.54; 95% CrI, 0.32 to 0.92), and brigatinib (HR = 0.57; 95% CrI, 0.32 to 0.95), but not over alectinib at 600 mg (HR = 0.68; 95% CrI, 0.42 to 1.08) or 300 mg (HR = 0.76; 95% CrI, 0.34 to 1.28).
Harms Results
The sponsor’s ITC18 conducted a safety analysis for grade 3 and 4 AEs. Grade 3 and 4 AEs were |||||||||||||||| reported in the lorlatinib group compared to alectinib at 300 mg (odds ratio [OR] = ||; 95%CrI, ||||||||||||||) or 600 mg (OR = ||; 95% CrI, ||||||||||||) and crizotinib (OR = ||; 95% CrI, ||||||||||||). |||||||||||||||| were observed between lorlatinib and brigatinib (OR = ||; 95% CrI, ||||||||), ceritinib (750 mg) (OR = ||; 95% CrI, ||||||||||||), ensartinib (OR = ||; 95% CrI, ||||||||||||), and chemotherapy (OR = ||; 95% CrI, ||||||||||||).
Ando et al. (2021)21 conducted safety analyses for any grade of AEs, SAEs, grade 3 or higher SAEs, and specific AEs including nausea, diarrhea, increased alanine transaminase (ALT), increased aspartate transaminase (AST), and pneumonitis. Because a different number of trials was included in the analysis of each safety end point, the comparators were different for each safety end point. In general, lorlatinib was not favoured over comparators. For any grade of AEs, no treatments were favoured between lorlatinib and alectinib (relative risk [RR] = 1.018; 95% CrI, 0.985 to 1.051), lorlatinib and brigatinib (RR = 1.041; 95% CrI, 1.001 to 1.083), or lorlatinib and crizotinib (RR = 1.010; 95% CrI, 0.985 to 1.035). Regarding SAEs, no treatments were favoured between lorlatinib and alectinib (RR = 1.614; 95% CrI, 1.041 to 2.503) or lorlatinib and crizotinib (RR = 1.249; 95% CrI, 0.881 to 1.768). Regarding grade 3 or higher AEs, no treatments were favoured between lorlatinib and alectinib (RR = 1.255; 95% CrI, 0.737 to 2.146) or lorlatinib and crizotinib (RR = 1.219; 95% CrI, 0.816 to 1.818). Regarding specific AEs (nausea, diarrhea, increased ALT and/or AST, and pneumonitis), lorlatinib was generally favoured over chemotherapy, crizotinib, or ceritinib, but not over alectinib or brigatinib.
Wang et al. (2021)20 conducted safety analyses involving assessments of AEs, AEs leading to treatment discontinuation, and AEs leading to dose reduction. None of the treatments (lorlatinib, alectinib, and brigatinib) were favoured over another.
Chuang et al. (2021)19 conducted a safety analysis for AEs of grade 3 or higher. Lorlatinib had a higher risk of grade 3 or higher AEs compared to crizotinib (RR = 1.27; CrI 1.07 to 1.52), and alectinib at 600 mg (RR = 1.62; 95% CrI, 1.24 to 2.12) and 300 mg (RR = 2.09; 95% CrI, 1.48 to 2.95), but not brigatinib (RR = 1.07; 95% CrI, 0.84 to 1.37).
Critical Appraisal
All ITCs involve issues related to heterogeneity. Specifically, differences in baseline characteristics may limit the comparability of patients across trials. For example, there were differences in the proportions of patients with brain metastases, the enrolment of patients from Asian and non-Asian countries, and the inclusion of patients who may have received prior treatment with an ALK inhibitor and/or chemotherapy. These characteristics may serve as treatment-effect modifiers of the comparisons of efficacy and safety in the ITCs. In some cases, the ITCs conducted subgroup or sensitivity analyses that accounted for differences in some but not all of these characteristics. The sponsor’s ITC included the ASCEND-8 trial, which was a phase I, dose-ranging, active-controlled trial. The inclusion of this trial is likely to have introduced bias to the comparisons with ceritinib, although it is possible that the evidence base of the ITC was broadened by inclusion of this trial. In addition, some studies included in the ITCs assessed treatment at different doses; specifically, alectinib was assessed at 300 mg and 600 mg. While some ITCs considered the 2 doses to be different nodes in the overall networks of comparisons, 2 of the ITCs combined data from trials that assessed alectinib at different doses and included only 1 node for alectinib. The different doses of alectinib may not be equivalent in efficacy or safety, and comparisons against alectinib that include data from both doses (600 mg and 300 mg) may have introduced uncertainty. The efficacy end points of PFS, OS, and ORR were assessed in the ITCs. Only PFS was powered for all trials included in the ITCs, and interpretation of evidence should therefore be limited to this end point. Overall, due to limitations of the ITCs, it is not possible to determine the true magnitude and direction of comparative treatment effects between lorlatinib, alectinib, and brigatinib.
Conclusions
One ongoing, phase III, open-label, randomized superiority trial (CROWN) provided evidence regarding the efficacy and safety of lorlatinib as first-line treatment in adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC. Compared to crizotinib, patients treated with lorlatinib showed a statistically significant improvement in PFS that was considered clinically meaningful by the clinical experts consulted by CADTH. A consistent improvement in PFS was observed in all patient subgroups assessed, most notably those with brain metastasis. The intracranial efficacy outcomes assessed in the trial (IC-ORR, IC-TTP, IC-DOR, IC-TTR), although exploratory, also showed a consistent treatment benefit for lorlatinib. These results suggest that, compared to crizotinib, lorlatinib may be capable of improved penetration of the blood-brain barrier and may be an option for patients with brain metastasis. Due to immaturity of the trial data, no evidence was available on OS. The trial is ongoing, and longer-term data are needed to determine whether the observed PFS benefit will translate to an improvement in OS. Lorlatinib may have a poorer safety profile compared to crizotinib, as the incidence of grade 3 and 4 AEs was higher (by approximately 17%) in patients treated with lorlatinib, although this did not appear to result in a higher rate of dose modification, interruption, or treatment discontinuation. In particular, patients and clinicians considering initiating treatment with lorlatinib should be aware that lorlatinib was associated with a higher incidence of neurologic AEs (i.e., cognitive and mood effects). The HRQoL analyses did not reveal any clinically meaningful differences between the treatment groups. In general, the results of the CROWN trial support the use of lorlatinib as another first-line treatment option for patients with ALK-positive locally advanced or metastatic NSCLC.
Comparison of efficacy and safety between lorlatinib and other TKIs, specifically alectinib and brigatinib, were considered more relevant in the Canadian first-line treatment setting for advanced or metastatic ALK-positive NSCLC. The ITCs included in this review showed that, similar to lorlatinib, both alectinib and brigatinib are associated with improved PFS compared to crizotinib, and therefore are more likely to be choices for first-line therapy than crizotinib. However, given the limitations related primarily to clinical and methodological heterogeneity across trials included in the ITCs, the magnitude and direction of comparative estimates of efficacy and safety between lorlatinib, alectinib, and brigatinib are uncertain.
Introduction
Disease Background
Lung cancers are the most commonly diagnosed cancers in both males and females in Canada. In 2020, they were expected to account for 29,800 cases. Lung cancer is also the leading cause of cancer-related death; approximately 25% of cancer deaths were expected to be due to lung cancer.2 Lung cancers may be classified as either small cell lung cancer or NSCLC. The latter accounts for approximately 88% of lung cancer cases in Canada (excluding Quebec) and is classified into histological subtypes, including adenocarcinoma, squamous cell carcinoma, and large cell carcinoma; of these, adenocarcinomas are the most commonly diagnosed histological subtype. Patients with adenocarcinoma typically do not have any smoking history and may grow more slowly than other types of lung cancers.22 The 5-year survival of NSCLC varies depending on the stage, but on average, the estimated 5-year survival for NSCLC is 25%.3
Some lung cancers can harbour chromosomal rearrangements, including ALK rearrangement, which is responsive to small-molecule TKIs and occurs in approximately 5% of NSCLC tumours.4,5 Testing for the ALK rearrangement occurs at initial diagnosis using an IHC test or ribonucleic acid panels that show the fusion mutation of ALK. Patients with the ALK-positive disease typically have a life expectancy of between 5 and 10 years. This patient group is highly susceptible to developing intracranial metastases. Approximately 25% of patients will typically develop intracranial metastases within the first year of their disease, and 70% to 80% will develop intracranial metastases approximately 5 years after their disease onset.6 Treatment with TKIs may help increase the chance of patient survival.7
Standards of Therapy
Current National Comprehensive Cancer Network guidelines suggest the following treatments as first-line options for patients with ALK-positive NSCLC: alectinib, brigatinib, ceritinib, crizotinib, or lorlatinib.23
In addition to these treatments, the clinical experts consulted by CADTH indicated that ensartinib may also be used. These first-line treatments have been studied in clinical trials against crizotinib. However, the clinical experts noted that crizotinib is no longer commonly used as a first-line treatment for ALK-positive metastatic NSCLC due to its poor penetration of the blood-brain barrier.
The clinical experts consulted by CADTH indicated that, based on data from the ALEX trial, the first-line treatment for ALK-positive patients is typically alectinib. However, it was also noted that first-line treatment with brigatinib has shown similar efficacy to alectinib. The clinical experts agreed that lorlatinib could serve as another first-line option, given the improved efficacy observed in the CROWN trial. While no head-to-head studies comparing lorlatinib to available first-line treatments other than crizotinib have been conducted, lorlatinib is associated with the lowest HR against crizotinib.
The clinical experts consulted by CADTH indicated that no ALK inhibitors are currently publicly reimbursed for use as second-line treatment for patients with ALK-positive metastatic NSCLC. Consequently, second-line therapies typically include any treatment available through a special access program, or chemotherapy. Lorlatinib has received Health Canada approval for use as second- or third-line treatment for patients who have progressed on crizotinib and at least 1 other ALK inhibitor or patients who have progressed on ceritinib or alectinib. However, as previously mentioned, the CADTH review for this indication resulted in a negative recommendation for reimbursement from pERC. In the opinion of the clinical experts consulted by CADTH, lorlatinib should be made available for use in multiple lines of therapy, and their preference would be to reserve its use for later-line therapy unless the patient presents with active CNS metastases, in which case the preference would be to use it as first-line treatment. Lorlatinib is typically not used in combination with other therapies and should only be used as a monotherapy; although some patients may require concurrent radiotherapy for a variety of reasons, including symptomatic brain or bone metastases and oligoprogression.
The clinicians consulted by CADTH consider lorlatinib to be best suited for patients with brain metastases due to its ability to penetrate the blood-brain barrier. These patients would typically be identified using radiographic imaging or MRI. However, it was noted that MRI can be associated with challenges such as long wait times and high costs of travel to regional sites. Patients with asymptomatic brain metastases were considered to be candidates for treatment with lorlatinib, as evidence suggests that lorlatinib both delays the occurrence of brain metastases and treats it. One of the clinical experts stated that it may be possible for patients to be misdiagnosed with metastases; imaging for patients typically occurs around every 6 months, but many patients may not be diagnosed until symptoms appear.
The clinical experts consulted by CADTH indicated that a patient’s response to treatment is assessed through imaging, including CT, MRI, carcinoembryonic antigen scans, and chest X-rays, and assessment of clinical progression. Patients may be assessed for response to treatment every 3 months, with imaging occurring approximately every 6 months. Although assessments may vary depending on the line of therapy, the clinical experts indicated that a clinically meaningful response to treatment would be improved survival, reduced symptom severity, improvement in symptoms, and maintenance quality of life, and ability to complete tasks of daily living. Treatments would typically be discontinued if patients experience clinical deterioration, and when cognitive dysfunction affects their quality of life.
Overall, the goals of treatment for patients with ALK-positive metastatic NSCLC include improving survival; improving or maintaining quality of life, employment, and independence; decreasing disease progression, and reducing severity of symptoms.
No treatments for ALK-positive metastatic NSCLC patients were considered curative and all currently available treatments are palliative, although treatments do provide benefits of disease response, decreased disease progression, and improved survival. In terms of treatment gaps. In addition, treatments with improved toxicity profiles that allow patients to preserve their quality of life are needed. Both clinicians emphasized the need for treatments that target specific biomarkers to help direct treatment. Current targeted treatment options are limited to first-line therapies, and further lines of therapy are needed to provide options for patients whose disease will ultimately progress.
Drug
Lorlatinib is approved by Health Canada and indicated for use as monotherapy for first-line treatment of adult patients with ALK-positive locally advanced (not amendable to curative therapy) or metastatic NSCLC.1 Lorlatinib is a selective adenosine triphosphate–competitive small molecule that can penetrate the blood-brain barrier and inhibit ALK and ROS1 tyrosine kinases.1 The Health Canada–recommended dose of lorlatinib is 100 mg taken orally once daily. The sponsor has requested the reimbursement of lorlatinib according to the Health Canada indication.
Key characteristics commonly used in treatments of ALK-positive metastatic NSCLC are presented in Table 3.
Table 3: Key Characteristics of Lorlatinib, Crizotinib, Alectinib, and Brigatinib
Characteristic | Lorlatinib | Crizotinib | Alectinib | Brigatinib |
|---|---|---|---|---|
Mechanism of action | A small, selective, ATP-competitive, brain-penetrating molecule that inhibits the ALK and ROS1 tyrosine kinases | A small, selective molecule that inhibits the ALK RTK and its oncogenic variants; inhibits HGFR RTK, ROS, and RON RTKs | A highly selective ALK and RET TKI | A TKI that targets ALK |
Indicationa | Monotherapy for first-line treatment of adult patients with ALK-positive locally advanced or metastatic NSCLC | Monotherapy for use in patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC | For first-line treatment of patients with ALK-positive, locally advanced (not amenable to curative therapy) or metastatic NSCLC | Monotherapy for first-line treatment of adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC |
Route of administration | Oral | Oral | Oral | Oral |
Recommended dosage | 100 mg once daily | 250 mg twice daily | 600 mg twice daily | 180 mg once daily |
Serious adverse effects or safety issues | High lipid blood levels (cholesterols or triglycerides) Lung problems Liver problems | QT interval prolongation and bradycardia Hepatotoxicity, including fatal outcomes Interstitial lung disease (pneumonitis), including fatal cases Vision loss | GI perforation Interstitial lung disease Hepatotoxicity Bradycardia | Pulmonary AEs Hypertension Elevation of pancreatic enzymes Hyperglycemia Creatine phosphokinase |
Other | Neurologic AEs of the CNS have been noted with lorlatinib, including seizures, psychotic effects and changes in cognitive function, mood (including suicidal ideation), speech, mental status, and sleep | Caution was suggested among patients with requiring peritoneal dialysis or hemodialysis as crizotinib has not been studied in patients with severe renal impairment | Cation was suggested among patients with severe renal impairment | None |
AE = adverse event; ALK = anaplastic lymphoma kinase; ATP = adenosine triphosphate; CNS = central nervous system; GI = gastrointestinal; HGFR = hepatocyte growth factor receptor; NSCLC = non–small cell lung cancer; RET = rearranged during transfection; RON = recepteur d’origine Nantais; RTK = receptor tyrosine kinase.
aHealth Canada–approved indication.
Source: Lorbrena product monograph,1 Xalkori product monograph,24 Alecensaro product monograph,25 and Alunbrig product monograph.26
Stakeholder Perspectives
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Comparators are crizotinib (a first-generation ALK TKI) and alectinib or brigatinib (second-generation ALK TKIs). Alectinib and brigatinib have demonstrated superiority over crizotinib. Alectinib and crizotinib are funded by most jurisdictions. Brigatinib has a conditional positive recommendation from the CADTH pCODR and is at pCPA for negotiation. Lorlatinib is a third-generation ALK TKI designed to have efficacy in patients with CNS metastases and ALK resistance mutations. The CROWN trial compared lorlatinib against crizotinib, which is no longer the standard first-line ALK inhibitor. The sponsor submitted a network meta-analysis, as well as the NCCN 2021 guidelines to support lorlatinib as the preferred first-line option. | For consideration by pERC. |
Considerations for initiation of therapy | |
The sponsor noted improved CNS response rates with lorlatinib compared to other ALK inhibitors. What is the preferred ALK inhibitor for patients with ALK-positive NSCLC with active CNS disease? | The clinical experts agreed that lorlatinib would be the preferred ALK inhibitor in patients with ALK-positive NSCLC with active CNS disease, due to the improved response among patients with brain metastases observed in the CROWN trial. |
For consistency with initiation criteria associated with other drugs reviewed by CADTH for this indication, consider alignment with the initiation criteria for alectinib and brigatinib. | For consideration by pERC. |
Considerations for prescribing of therapy | |
Dosing, schedule/frequency, and dose intensity:
| For consideration by pERC. |
Generalizability | |
The CROWN clinical trial included patients with an ECOG PS of 0 to 2. Should patients with an ECOG PS > 2 be eligible? | The clinical experts agreed that patients who have an ECOG PS > 2 should be eligible for treatment with lorlatinib. The decision to offer lorlatinib to these patients should be left to the judgment of the treating physician. |
Could patients being treated with crizotinib, alectinib, or brigatinib be switched to lorlatinib? | The clinical experts indicated that if a patient is responding to a treatment they are currently receiving (i.e., crizotinib, alectinib, or brigatinib), then they should remain on that treatment while they are responding to and tolerating that therapy. Patients receiving other treatments (i.e., crizotinib, alectinib, or brigatinib) who experience toxicities typically will undergo dose reduction or dose interruption or receive supportive medications. In patients whose toxicities cannot be managed in these ways, the clinical experts indicated switching to another agent would be a useful option. |
Funding algorithm | |
Lorlatinib may change the place in therapy of drugs reimbursed in subsequent lines and may be used preferentially over alectinib or brigatinib. Is there any information on sequential use of TKIs after treatment with lorlatinib? | Based on the CROWN trial, patients received subsequent second-line treatment with TKIs (65.4% in the lorlatinib group vs. 91.9% in the crizotinib group), chemotherapy with or without anti-angiogenic therapy (30.8% vs. 3.8%, respectively), immunotherapy (3.8% vs. 0%, respectively) and other (0% vs. 4.7%, respectively). Information regarding third- and fourth-line therapies were also reported. However, the relative efficacy of subsequent treatments is unknown. Treating physicians should use their judgment and recommended treatment guidance when administering subsequent therapies. |
Care provision issues | |
Management of adverse effects:a
| For consideration by pERC. |
Companion diagnostics:
| For consideration by pERC. |
System and economic issues | |
Concerns regarding the anticipated budget impact and sustainability:
| For consideration by pERC. |
Additional costs to be considered (other than related to care provision):
| For consideration by pERC. |
Involvement of additional payers:
| For consideration by pERC. |
Presence of confidential negotiated prices for comparators:
| For consideration by pERC. |
ALK = anaplastic lymphoma kinase; CNS = central nervous system; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NCCN = National Comprehensive Cancer Network; NSCLC = non–small cell lung cancer; pCPA = pan-Canadian Pharmaceutical Alliance; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; TKI = tyrosine kinase inhibitor; vs. = versus.
aThe drug plan included the following statement about the management of adverse effects in input that was provided before the product monograph change (effective 24 November 2021): “Drug-drug interaction with CYP3A inducers – discontinue use. If concomitant use of moderate CYP3A inducers is required, monitor AST, ALT, and bilirubin 48 hours after initiation and at least 3 times during the first week.” As the wording for the concomitant use of moderate CYP3A inducers and lorlatinib has changed and the required monitoring for aspartate transaminase, alanine transaminase, and bilirubin 48 hours after lorlatinib initiation was removed from the updated product monograph, consideration of this item is no longer required.
Clinical Evidence
The clinical evidence included in the review of lorlatinib is presented in 2 sections. The first section, Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review.
Systematic Review of Pivotal and Protocol-Selected Studies
Objectives
To perform a systematic review of the beneficial and harmful effects of lorlatinib at 100 mg orally once daily for the first-line treatment of adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect those considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC who have not received previous systemic treatment for metastatic disease Subgroups:
|
Intervention | Lorlatinib monotherapy 100 mg orally once daily |
Comparator | Alectinib Brigatinib Crizotinib |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; ALK = anaplastic lymphoma kinase; CNS = central nervous system; NSCLC = non–small cell lung cancer; SAE = serious adverse event; TEAE = treatment-emergent adverse event; vs. = versus; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.27
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was lorlatinib. Clinical trials registries searched the US National Institutes of Health’s clinicaltrials.gov, the WHO International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on July 21, 2021. Regular alerts updated the search until the meeting of pERC on November 10, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.28 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
Findings From the Literature
A total of 345 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 1.
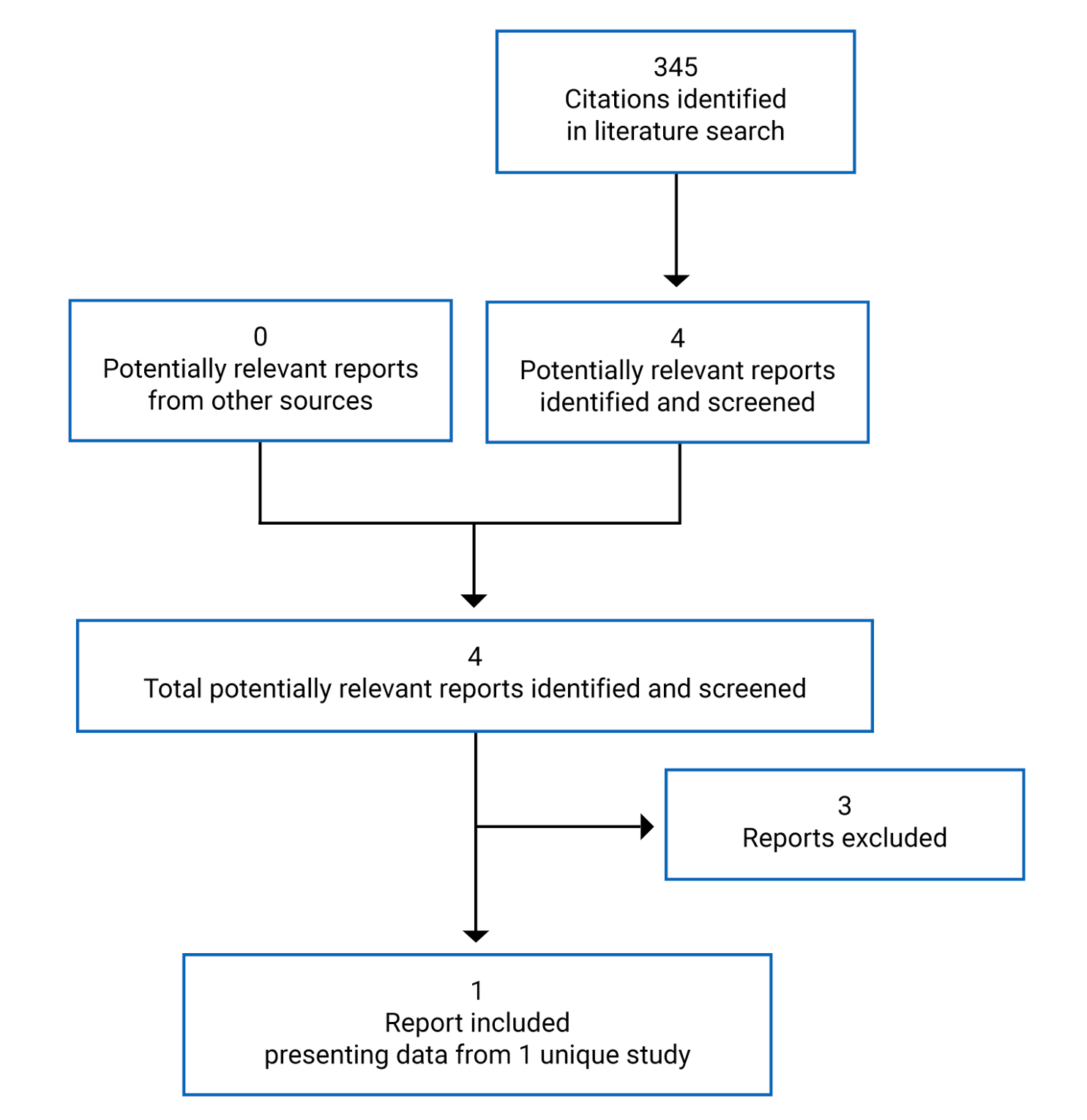
Table 6: Details of the CROWN Study
Detail | Description |
|---|---|
Designs and populations | |
Study design | Phase III multinational, multi-centre, open-label randomized controlled trial |
Locations | 104 sites in 23 countries, including Japan, Italy, Russia, France, South Korea, Spain, China, Mexico, Poland. Taiwan, Singapore, Hong Kong, India, the UK, Argentina, Netherlands, Czech Republic, Germany, the US, Canada, Turkey, Australia, and Belgium |
Patient enrolment dates | Not reported |
Data cut-off | March 20, 2020 |
Randomized (N) | 296 |
Inclusion criteria | Adults (≥ 18 years, or ≥ 20 years as required by local regulation) with histologically or cytologically confirmed locally advanced (stage IIIB not amenable for multimodality treatment) or metastatic (stage IV) NSCLC (as determined by AJCC version 7.0) ALK-positive status determined by the FDA-approved (for use in the US), CE-marked (for EU and other countries that accept CE marking), and PMDA-approved (for use in Japan) Ventana ALK (D5F3) Companion Diagnostic (CDx) IHC test performed on Ventana ULTRA or XT platforms ≥ 1 extracranial measurable target lesion per RECIST 1.1 criteria that has not been previously irradiated. CNS metastases were allowed if a patient was asymptomatic and 1 of the following:
All patients must have had an archival formalin-fixed, paraffin-embedded tissue specimen available and collected before randomization; if archived tissue was unavailable, a de novo biopsy was mandatory No prior systemic treatment for advanced or metastatic NSCLC, including molecularly targeted agents (e.g., ALK TKIs), angiogenesis inhibitors, immunotherapy, or chemotherapy; prior treatment for earlier stages of NSCLC were permitted if they were completed > 12 months before randomization Eastern Cooperative Oncology Group Performance Status of 0, 1, or 2 Adequate bone marrow function (absolute neutrophil count ≥ 1,500/mm3 or ≥ 1.5 × 109/L; platelets ≥ 100,000/mm3 or ≥ 100 × 109/L; hemoglobin ≥ 9 g/dL), adequate pancreatic function (serum total amylase ≤ 1.5 × upper limit of normal (ULN); serum lipase ≤ 1.5 × ULN), adequate renal function (serum creatinine ≤ 1.5 × ULN or estimated creatinine clearance ≥ 60 mL/min as calculated using the method standard for the institution), adequate liver function (total serum bilirubin ≤ 1.5 × ULN; aspartate transaminase and alanine transaminase ≤ 2.5 × ULN or, in case of liver metastases, ≤ 5.0 × ULN) Acute effects of prior radiotherapy resolved to baseline severity or to Common Terminology Criteria for Adverse Events grade ≤ 1 except for AEs that in the investigator’s judgment do not constitute a safety risk for the patient |
Exclusion criteria | Radiation therapy within 2 weeks before randomization, including stereotactic or partial brain irradiation. Patients who had completed whole-brain irradiation within 4 weeks before randomization or palliative radiotherapy outside of the CNS within 48 hours before randomization were also excluded from the study. Known prior or suspected severe hypersensitivity to study drugs or any component in their formulations Spinal cord compression unless the patient had good pain control attained through therapy, and there was stabilization or recovery of neurologic function for the 4 weeks before randomization Major surgery within 4 weeks before randomization; minor surgical procedures (e.g., port insertion) were not excluded, but sufficient time should have passed for adequate wound healing Gastrointestinal abnormalities, requirement for IV alimentation, prior surgical procedures affecting absorption including total gastric resection or lap band, active inflammatory gastrointestinal disease, chronic diarrhea, symptomatic diverticular disease, treatment for active peptic ulcer disease in the past 6 months, or malabsorption syndromes Active and clinically significant bacterial, fungal, or viral infection, including hepatitis B or C, HIV, or AIDS-related illness Clinically significant vascular (both arterial and venous) and nonvascular cardiac conditions, active or within 3 months before enrolment Evidence of active malignancy (other than NSCLC, non-melanoma skin cancer, or localized prostate cancer or any in situ cancer that does not currently require treatment) within the past 3 years before randomization Other severe acute or chronic medical or psychiatric condition, including recent (within the past year) or active suicidal ideation or behaviour, or laboratory abnormality that may increase the risk associated with study participation or investigational product administration or that may interfere with the interpretation of study results and, in the judgment of the investigator, would make the patient inappropriate for entry into this study |
Drugs | |
Intervention | Lorlatinib 100 mg, orally, daily |
Comparator | Crizotinib 250 mg, orally, twice daily |
Duration | |
Phase | |
Screening phase | ≤ 28 days before randomization |
Treatment phase | Each cycle of treatment was 4 weeks (28 days); patients were treated until disease progression (assessed by BICR), patient withdrawal, lost to follow-up, unacceptable toxicity, death, or termination of the study by the sponsor, whichever occurred first |
Follow-up phase | Post-treatment follow-up: every 4 weeks until disease progression Survival follow-up: every 4 months for up to 3 years, and then every 6 months thereafter |
Outcomes | |
Primary end point | PFS per BICR |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Shaw et al. (2020)29 |
AE = adverse event; AJCC = American Joint Committee on Cancer; ALK = anaplastic lymphoma kinase; BICR = blinded independent central review; CE = Conformité Européene; CNS = central nervous system; DOR = duration of response; IC-DOR = intracranial duration of response; IC-ORR = intracranial objective response rate; IC-TTP = intracranial time to progression; IC-TTR = intracranial time to response; IHC = immunohistochemistry; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PDMA = Pharmaceuticals and Medical Devices Agency; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; TKI = tyrosine kinase inhibitor; TTR = time to response; ULN = upper limit of normal.
Source: CROWN Clinical Study Report17 and CADTH submission.18
Description of Studies
The CROWN trial was a phase III, multinational, multi-centre, open-label randomized controlled trial (RCT) comparing the efficacy and safety of lorlatinib to crizotinib among patients with locally advanced (stage IIIB, not amenable for multimodality treatment) or metastatic (stage IV) ALK-positive NSCLC who had not received previous systemic treatment for metastatic disease. Patients (N = 296) from 104 centres in 23 countries, including 2 patients from Canada (1 in each treatment group), were randomized in a 1:1 ratio using an interactive web-based response technology system to receive either lorlatinib or crizotinib. Patients had to receive study treatments no later than 7 days after they were randomized. Patents were stratified by the presence of brain metastases (yes versus no) and ethnic origin (Asian versus non-Asian).17 Patients were classified as having brain metastases if they had brain lesions that were present and observed at study entry or which were known from a patient’s medical history to have been present in the past even if the brain lesions were no longer visible (e.g., irradiated or surgically removed). Brain lesions were permitted to be either measurable or nonmeasurable and were classified as target or nontarget lesions. The ethnic origin of patients referred to the patient’s actual race and not where they were living or where they were being treated. Stratified randomization was centrally allocated across all participating study centres through the interactive response technology system. Crossover was not permitted between treatment groups.17
Patients were required to undergo molecular testing for the presence of ALK tumour aberrations. Patients who screened as ALK-negative were considered screen failures.17 All patients were required to undergo CNS imaging using MRI (unless contraindicated) at baseline. A BICR was used for assessment of imaging to determine patient’s overall tumour response according to RECIST 1.1 criteria. The BICR of patient intracranial tumour response used a modified version of RECIST 1.1 criteria.
The CROWN trial included 3 phases: screening, treatment, and follow-up. Assessments were conducted at screening and then repeated every 8 weeks (± 1 week) starting from randomization while on treatment until disease progression. Patients were eligible to be treated beyond progression. If patients continued treatment beyond disease progression, they continued receiving tumour assessments every 8 weeks (± 1 week). Assessments for bone progression were conducted every 16 weeks (± 1 week) only if evidence of bone metastases was observed at baseline.17 Patients who discontinued treatment for reasons other than disease progression were followed for disease progression regardless of receipt of new anticancer therapy. Tumour assessments were repeated after at least 4 weeks to confirm patient response (complete response [CR] or partial responses [PR]).18
The primary end point of the CROWN trial was PFS with 2 pre-specified analyses, including interim and final analyses. The interim analysis was pre-specified to occur when approximately 133 events occurred (75% of the 177 events planned at the end of the study). By the data cut-off date (March 20, 2020), 127 PFS events had occurred (72% of the 177 events planned for the final analysis of PFS). The pre-specified superiority boundary for PFS was crossed at the interim analysis and was considered final, although the trial is currently ongoing. The secondary end point of the trial was OS, which was hierarchically tested depending on statistical significance of PFS. By the data cut-off date, OS data were immature as the majority of patients remained alive. Two additional pre-specified analyses are planned for OS, with the next analysis planned to occur in early 2025. The CROWN trial was funded and conducted by Pfizer.
A representation of the CROWN trial study design is depicted in Figure 2.
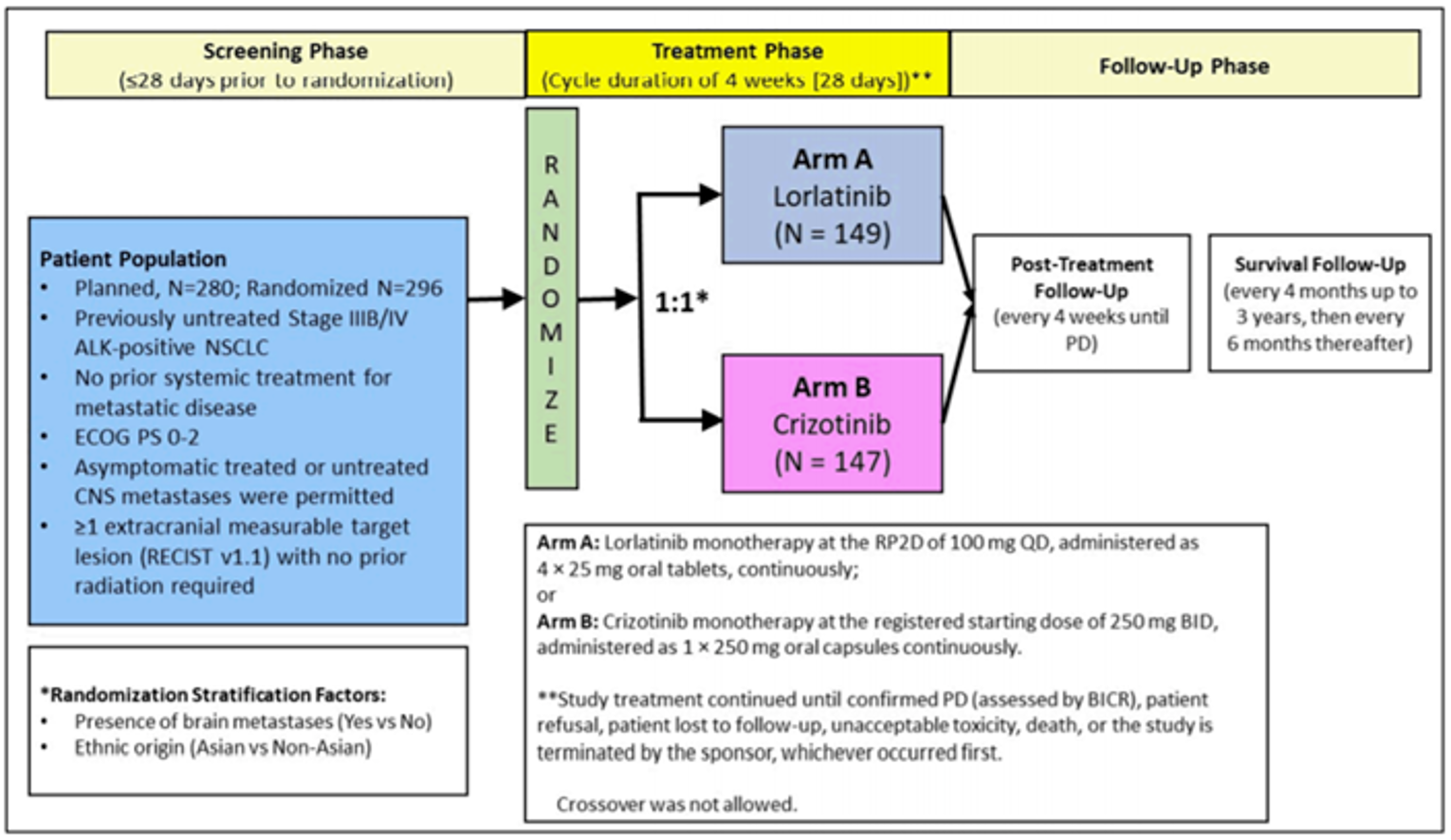
ALK = anaplastic lymphoma kinase; BICR = blinded independent central review; BID = twice a day; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NSCLC = non–small cell lung cancer; PD = progressive disease; QD = every day; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1. RP2D = recommended phase II dose.
Source: CROWN Clinical Study Report.17
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria used in the CROWN trial are summarized in Table 6. Briefly, the trial enrolled adult patients with histologically or cytologically confirmed diagnosis of locally advanced or metastatic ALK-positive NSCLC. ALK-positive status was required to have been determined by a Ventana ALK (D5F3) CDx IHC test performed on the Ventana ULTRA or XT platform. Patients were also required to have at least 1 extracranial measurable target lesion (per RECIST 1.1 criteria) that had not been previously irradiated. Patients could have treated or untreated CNS metastases, as long as they were asymptomatic and aligned with other criteria specified in Table 6. Patients were required to have an ECOG PS of 0, 1, or 2.17
Key exclusion criteria included the presence of chronic or uncontrolled conditions, such as vascular or nonvascular conditions, predisposing characteristics for acute pancreatitis, lung disease, or psychiatric conditions. Patients must not have received prior systemic treatment for advanced or metastatic NSCLC; although prior treatment for earlier stages of NSCLC was permitted if it was completed more than 12 months before randomization. Patients must also not have received major surgery within 4 weeks of randomization or have spinal cord compression unless the patient had good pain control attained through therapy and had stabilized or recovered neurological function within 4 weeks of randomization. Radiation therapy, including stereotactic or partial brain irradiation, was also not permitted within 2 weeks before randomization. Patients who completed brain irradiation within 4 weeks before randomization or who received palliative radiotherapy outside of the CNS within 48 hours before randomization were also not permitted in the trial.17
Baseline Characteristics
A summary of the baseline characteristics of patients in the CROWN trial is presented in Table 7. Demographic characteristics were generally balanced across the treatment groups. The mean age of patients was 59 years (SD = 13) in the lorlatinib group and 56 years (SD = 14) in the crizotinib group, with most patients being 45 years of age or older (83% versus 76.2%, respectively). A larger proportion of patients in the lorlatinib group were aged 65 years or older than patients in the crizotinib group (39.6% versus 29.9%, respectively), and a slightly smaller proportion of patients in the lorlatinib group were between 18 and 45 years of age compared with the crizotinib group (17.4% versus 23.8%, respectively). Most patients were female, (56.4% and 61.9%, respectively), White (48.2% and 49.0%, respectively) or Asian (43.6% versus 44.2%, respectively). Of the Asian patients, most were Japanese (38.5% versus 35.4%, respectively) or Chinese (40.0% versus 35.4%, respectively), followed by Korean (12.3% versus 20.0%, respectively) and other (9.2% in both groups).17
Baseline disease characteristics were balanced across the treatment groups. Almost all patients had measurable disease at baseline (96.6% in the lorlatinib group versus 97.3% in the crizotinib group), with approximately one-quarter of patients presenting with brain metastasis (25.5% versus 27.2%, respectively). Of patients with brain metastasis at baseline, 17 (11.4%) in the lorlatinib group and 13 (8.8%) in the crizotinib group had measurable brain disease. Most patients had an ECOG PS of 0 (45.0% in the lorlatinib group versus 38.8% in the crizotinib group) or 0 (53.0% versus 55.1%, respectively) and were classified as having adenocarcinoma (94.0% versus 95.2%, respectively) or stage IV metastatic NSCLC (90.6% versus 94.6%, respectively). Patients were classified as either never smokers (54.4% versus 63.9%, respectively) or former smokers (36.9% versus 29.3%, respectively); a greater proportion of patients in the crizotinib group were classified as never smokers, and more patients in the lorlatinib group were classified as former smokers.17
Table 7: Summary of Baseline Characteristics for the CROWN Study — Full Analysis Set
Characteristic | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Age in years,a n (%) | ||
18 to < 45 | 26 (17.4) | 35 (23.8) |
45 to < 65 | 64 (43.0) | 68 (46.3) |
≥ 65 | 59 (39.6) | 44 (29.9) |
Mean (SD) | 59.1 (13.1) | 55.6 (13.5) |
Sex, n (%) | ||
Male | 65 (43.6) | 56 (38.1) |
Female | 84 (56.4) | 91 (61.9) |
Race, n (%) | ||
White | 72 (48.3) | 72 (49.0) |
Asian | 65 (43.6) | 65 (44.2) |
Japanese | 25 (38.5) | 23 (35.4) |
Korean | 8 (12.3) | 13 (20.0) |
Chinese | 26 (40.0) | 23 (35.4) |
Other | 6 (9.2) | 6 (9.2) |
Black or African-American | 0 | 1 (0.7) |
Other | 0 | 0 |
Missing | 12 (8.1) | 9 (6.1) |
Ethnic origin, n (%) | ||
Asian | 66 (44.3) | 65 (44.2) |
Non-Asian | 83 (55.7) | 82 (55.8) |
Measurable disease at baseline, n (%) | ||
Yes | 144 (96.6) | 143 (97.3) |
No | 5 (3.4) | 4 (2.7) |
Brain disease at baseline, n (%) | ||
Yes | 38 (25.5) | 40 (27.2) |
Measurable disease | 17 (11.4) | 13 (8.8) |
Not measurable disease | 21 (14.1) | 27 (18.4) |
No | 110 (73.8) | 106 (72.1) |
No data | 1 (0.7) | 1 (0.7) |
ECOG PS,b n (%) | ||
0 | 67 (45.0) | 57 (38.8) |
1 | 79 (53.0) | 81 (55.1) |
2 | 3 (2.0) | 9 (6.1) |
Histopathological classification, n (%) | ||
Adenocarcinoma | 140 (94.0) | 140 (95.2) |
Non-adenocarcinoma | 9 (6.0) | 7 (4.8) |
TNM current stage, n (%) | ||
Stage IIIA | 1 (0.7) | 0 |
Stage IIIB | 12 (8.1) | 8 (5.4) |
Stage IV | 135 (90.6) | 139 (94.6) |
Otherc | 1 (0.7) | 0 |
Extent of disease, n (%) | ||
Locally advanced | 14 (9.4) | 8 (5.4) |
Metastatic | 135 (90.6) | 139 (94.6) |
Smoking status, n (%) | ||
Never | 81 (54.4) | 94 (63.9) |
Current | 13 (8.7) | 9 (6.1) |
Former | 55 (36.9) | 43 (29.3) |
AJCC = American Joint Committee on Cancer; FAS = full analysis set; SD = standard deviation; TNM = tumour, nodes, metastases.
aAge at screening (years) = (date of given informed consent − date of birth + 1)/365.25.
bPer independent central neuroradiological review.
cOne patient with locally advanced disease at study entry was staged according to AJCC version 8.0, instead of AJCC version 7.0 as required by protocol was therefore classified under Other.
Source: CROWN Clinical Study Report.17
Prior Treatments
In general, the prior therapies patients received were similar in each treatment group (Table 8). Prior radiotherapy (13.4% versus 13.6% in the lorlatinib and crizotinib groups, respectively) or surgery (18.1% versus 15.6%) were the most commonly reported prior anticancer therapies. Prior systemic anticancer treatments were reported infrequently among patients and were primarily received in the adjuvant treatment setting (6.7% versus 5.4%). Prior adjuvant and neoadjuvant therapies were infrequently reported among patients in the lorlatinib and crizotinib groups (6.7% versus 5.4% and 0.7% versus 0.7%, respectively). One patient in the lorlatinib group received carboplatin and paclitaxel for advanced disease violating eligibility criteria; this event was captured as an important protocol deviation.
Table 8: Summary of Prior Anticancer Treatments
Anticancer therapy status, n (%) | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Patients with at least 1 prior anticancer systemic therapy | 12 (8.1) | 9 (6.1) |
Patients with at least 1 prior anticancer radiotherapy | 20 (13.4) | 20 (13.6) |
Patients with at least 1 prior anticancer surgery | 27 (18.1) | 23 (15.6) |
Patients with adjuvant anticancer systemic therapy | 10 (6.7) | 8 (5.4) |
Patients with neoadjuvant anticancer systemic therapy | 1 (0.7) | 1 (0.7) |
Source: CROWN Clinical Study Report.17
Interventions
Patients were randomized to receive either lorlatinib or crizotinib as monotherapy. Lorlatinib was administered to patients orally at 100 mg using four 25 mg tablets once daily. Crizotinib was administered orally at a dosage of 250 mg twice daily; capsules of crizotinib were available at 200 mg or 250 mg.17
Patients were required to swallow the lorlatinib tablet or crizotinib capsule whole without manipulating or chewing before swallowing at the same time every day.17
Each cycle was specified to be 4 weeks (or 28 days) regardless of dose delays, dose interruptions, or missed doses. Treatments were administered to patients until disease progression confirmed by BICR, patient refusal, the patient was lost-to-follow-up, unacceptable toxicity, or if the study was terminated by the sponsor, whichever came first.17 Patients were eligible for treatment beyond progression (confirmed by BICR) if they were thought to still be deriving benefit from continued treatment, as long as the treating physician determined that the benefits and risks were favourable for the patient.18 Patients who received treatment beyond progression were required to undergo the same assessments during the active treatment period, including the following tumour assessments:
For patients with only documented extracranial progression, intracranial lesions stable or in response, intracranial assessments were to be performed until intracranial disease progression.
No further tumour assessments were required once intracranial disease progression was documented.
Patient Compliance
As patients self-administered treatment at home, compliance was captured and completed by the patient using a diary. The diary was to be maintained by the patient and include unchanged, missed, or changed doses of study treatments received. Patients randomized to either group were required to return bottles of lorlatinib or crizotinib at the end of each 28-day cycle during their planned visit to the investigational site. The number of tablets of lorlatinib or capsules of crizotinib were documented and recorded at each clinic visit. Study sites were required to follow up with patients on day 5 of cycle 1 (± 3 days) to confirm the patient’s understanding and compliance with treatment dosing instructions. Patients were re-trained if necessary. If patients required a dose modification, the same follow-up procedures were applied.17
Dose Modifications
Dosing of treatments was permitted to be delayed and/or reduced in the event of significant toxicity experienced by the patient. Dose modifications were based on the worst toxicity observed if multiple toxicities occurred. Patients were instructed to inform their investigators at the first occurrence of any AE. In the event of AEs, trial investigators were instructed to employ the best supportive care practices of local institutions or follow pre-specified dose modifications for lorlatinib or crizotinib.17
Doses of lorlatinib were permitted to be modified at 2 levels; the first level involved a dose reduction to 75 mg, and the second level involved a dose reduction to 50 mg. Dose reductions beyond the second level (50 mg) were not permitted. Re-escalation of doses was also not permitted unless there was a discussion with the sponsor’s medical contact. Precautions surrounding AEs of hyperlipidemia and PR-interval prolongation were pre-specified in the CROWN trial protocol as these were expected AEs that have been observed in previous studies of lorlatinib.18
Doses of crizotinib were permitted to be modified at 2 levels; the first level involved a dosage reduction to 200 mg twice daily, and the second dose level involved a dosage reduction to 250 mg once daily. Dosage reductions beyond the second level (250 mg once daily) were not permitted. Re-escalation of crizotinib was not permitted except in specific circumstances. Precautions surrounding AEs of nausea and vomiting, diarrhea, bradycardia, pneumonitis, pneumonia, renal cysts, and severe visual loss were pre-specified.18
Patients were required to permanently discontinue study treatment if dose interruptions lasted longer than 6 weeks due to ongoing treatment-related toxicities. Patients who discontinued treatment permanently due to severe toxicity were to remain in the trial for ongoing tumour assessments until RECIST 1.1–defined disease progression as assessed by BICR. However, patients were able to continue treatment after a dose interruption of greater than 6 weeks if there was a discussion of the clinical circumstances with the sponsor’s medical monitor.18
If patients overdosed on study treatment (took > 100 mg of lorlatinib or > 250 mg twice daily of crizotinib), they were required to report this to the sponsor regardless of whether AEs were observed.18
Concomitant Treatments
Concomitant medications were permitted at any time during the trial if they were considered necessary for the patient’s well-being. Concomitant medications solely for supportive care (e.g., antiemetics, analgesics, megestrol acetate for anorexia, bisphosphonates, or RANK ligands for metastatic bone disease or osteoporosis) were permitted. Patients who were already on treatment with RANK ligands (i.e., denosumab) before study entry were required to be at a stable dose before randomization. No treatments were prohibited during the post-treatment follow-up phase. Other anticancer treatments, investigational therapies, radiation therapy (except for palliative radiotherapy to specific sites of disease), and herbal remedies with known anticancer properties were not permitted.18
The primary enzymes involved in the metabolism of lorlatinib include CYP3A and UGT1A4, along with involvement of other CYP enzymes in the metabolism, inhibition, and induction of lorlatinib (i.e., CYP2C19, CYP2C8, CYP3A, and CYP2B6). As inhibition or induction of these enzymes may alter the systemic exposure of lorlatinib to patients, safety precautions for certain concomitant medications were pre-specified.18
The CYP3A enzyme is predominantly involved in the metabolism of crizotinib. Concomitant medications that are CYP3A inhibitors or inducers may be expected to alter the plasma concentrations of crizotinib in patients; therefore, concurrent use of potent CYP3A inhibitors or inducers were not permitted in the trial. However, topical use of CYP3A inhibitors were permitted. Other CYP isoforms (i.e., CYP1A2, 2C8, 2C9, 2C19, and 2D6) may also be inhibited by crizotinib. In addition, treatments that operate through CYP3A4 were also limited during the trial.18
Outcomes
A list of the efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in the following section. A detailed discussion and critical appraisal of the HRQoL outcome measures are provided in Appendix 3.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | Included in statistical hierarchy | Outcome definition used in the CROWN trial |
|---|---|---|
Primary end point | ||
PFS by BICR | Yes | The time from date of randomization to the date of the first documentation of disease progression per RECIST 1.1 criteria and based on BICR assessment, or death due to any cause, whichever occurs first |
Secondary end point | ||
OS | Yes | The time from randomization to the date of death due to any cause |
Exploratory end points | ||
PFS by investigator assessment | No | Defined in a similar manner as the primary end point of PFS assessed by BICR; however, disease progression was derived programmatically from the target lesion measurements, nontarget lesion status, and new lesions recorded on the case report form |
ORR by BICR | No | The percentage of patients with a best overall confirmed response (CR or PR) according to RECIST 1.1 criteria; both CR and PR must have been confirmed by repeat assessments performed no less than 4 weeks after the criteria for response were met |
ORR by investigator assessment | No | Defined in a similar manner as ORR based on BICR assessment; however, the best overall response per the investigator was derived programmatically from the target lesion measurements, nontarget lesion status, and new lesions recorded on the case report form |
IC-ORR by BICR | No | Defined in the same manner as ORR per BICR, but based only on intracranial disease in the subgroup of patients with at least 1 intracranial lesion |
IC-TTP by BICR | No | The time from date of randomization to the date of the first documentation of progression of intracranial disease, based on either new brain metastases or progression of existing brain metastases |
DOR by BICR | No | Defined, for patients with a confirmed objective response per RECIST 1.1, as the time from the first documentation of objective tumour response (CR or PR) to the first documentation of disease progression or death due to any cause, whichever occurs first |
IC-DOR by BICR | No | Defined in the same manner as DOR per BICR, except that it is conducted only in patients with a confirmed IC-ORR |
TTR by BICR | No | Defined, for patients with a confirmed objective response, as the time from the date of randomization to the first documentation of objective response (CR or PR) which is subsequently confirmed |
IC-TTR by BICR | No | Defined in the same manner as TTR per BICR assessment, except that is only conducted in patients with a confirmed IC-OR |
Health-related quality of life | ||
EORTC QLQ-C30 | No | Version 3.0 of the EORTC QLQ-C30 was administered to patients. The survey consists of 30 questions including 5 function scales (physical, role, cognitive, emotional, and social), 1 global health status/global quality-of-life scale, 3 symptom scales (fatigue, pain, nausea, and vomiting), and 6 single items that assess additional symptoms (dyspnea, appetite loss, sleep disturbance, constipation, and diarrhea) and financial impact. Scales and single items of the survey range in score from 0 to 100, with higher scores on the functional and global health status/quality-of-life scales indicating higher levels of functioning and health status/quality of life, respectively. Higher scores on the symptom scales or items represent a greater presence of symptoms. |
EORTC QLQ-LC13 | No | The lung cancer–specific module consists of 13 questions including 1 multi-item scale and 9 single items assessing symptoms (dyspnea, cough, hemoptysis, and site-specific pain), side effects (sore mouth, dysphagia, peripheral neuropathy, and alopecia), and pain medication use. Higher scores indicate a greater presence of symptoms. A TTD analysis of pain in the chest, dyspnea, or cough, individually from the EORTC QLQ-LC13 and as a composite end point, was defined as the time from randomization to the first time a patient’s score showed a ≥ 10-point increase after baseline in any of the 3 symptoms. |
EQ-5D-5L | No | The EQ-5D-5L is a questionnaire for assessing a patient’s health status in terms of a single index value or utility score. The 2 components of the questionnaire include a descriptive system that allows patients to rate their level of problems (none, slight, moderate, severe, extreme/unable) in 5 areas (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), and a Visual Analogue Scale that allows patients to rate their overall health status from 0 (worst imaginable) to 100 (best imaginable). |
BICR = blinded independent central review; CR = complete response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; EQ-5D-5L = EQ-5D 5-Levels questionnaire; IC-DOR = intracranial duration of response; IC-ORR = intracranial objective response rate; IC-TTP = intracranial time to progression; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST = Response Evaluation Criteria in Solid Tumor Version 1.1; TTR = time to response.
Source: Statistical Analysis Plan.18
Safety Assessments
Adverse events were graded using the Common Terminology Criteria for Adverse Events Version 4.03. Safety end points were summarized while patients were on treatment (unless otherwise specified).18
Statistical Analysis
Sample Size
The statistical analysis plan specified that approximately 280 patients, 140 in each treatment group, were to be randomized in the CROWN trial. As of February 28, 2019, a total of 196 patients were randomized into the study. The primary objective of the study was to determine whether lorlatinib was superior to crizotinib in prolonging PFS based on RECIST 1.1 criteria as determined by a BICR. The trial was required to have 177 PFS events to have at least 90% power to detect an HR of 0.611 using a 1-sided stratified log-rank significance level of 0.025 and a 2-look group sequential design with a Lan-DeMets (O’Brien-Fleming) alpha spending function to determine the efficacy boundaries.18 Assuming an HR of 0.611 would indicate the superiority of lorlatinib, the median PFS was estimated to be 18 months in the lorlatinib group and 11 months in the crizotinib group. A 15% dropout rate was assumed within each treatment group at 30 months, along with a nonuniform patient accrual over a period of approximately 15 months with a follow-up period of approximately 18 months after randomization of the last patient.18
The expected sample size was planned to allow for a comparison of OS dependent on the observed statistical significance of lorlatinib over crizotinib for PFS.18 A total of 198 deaths were required to have 70% power using a 1-sided stratified log-rank test at a 1-sided significance level of 0.025, and a 3-look group sequential design with Lan-DeMets (O’Brien-Fleming) alpha spending function to determine the efficacy boundaries. The 198 OS events were expected to result in an HR of 0.70, which would support improved efficacy of lorlatinib over crizotinib and result in an expected median OS of 68.6 months and 48 months in the lorlatinib and crizotinib groups, respectively. A 15% dropout rate was assumed with each treatment group for OS at 120 months, with a follow-up of approximately 110 months after randomization of the last patient.18
Interim and Final Analyses
Interim and final analyses for PFS were pre-specified in the statistical analysis plan of the CROWN trial. The interim analysis was to be performed after approximately 133 PFS events (75% of 177 events) had occurred per BICR and was to be conducted by an independent statistician. A final analysis of PFS was specified only if the boundary for efficacy was not crossed at the interim analysis. The final analysis of PFS was specified to occur when 177 PFS events occurred according to a BICR, and to be performed by the sponsor’s clinical team.18
The nominal significance levels for the interim and final efficacy analyses for PFS were determined using the Lan-DeMets procedure with an O’Brien-Fleming stopping boundary; the overall significance level was preserved at 0.025 (1-sided). The superiority of lorlatinib over crizotinib was considered to have been met if the value of the test statistic exceeded the efficacy boundary (z < −2.337; P < 0.01) at the interim analysis (Table 10).18 However, as the number of observed events may not necessarily be the same as the number of expected events, the efficacy boundaries were specified to be updated based on the observed number of PFS events at the time of the interim analysis using pre-specified alpha spending functions. At the data cut-off date of March 20, 2020, the interim analysis was performed after 127 PFS events had occurred (72% of the 177 events planned for the final analysis of PFS). The efficacy boundaries were updated to reflect the number of PFS events that occurred, and are provided in Table 11; a P value of 0.0081 was used to determine statistical significance at the time of the interim analysis for PFS.17
Table 10: Planned Efficacy Boundaries for PFS
Analysis | Events, n (%) | z score | P value (1-sided) |
|---|---|---|---|
Interim | 133 (75%) | < −2.337 | < 0.01 |
Final | 177 (100%) | < −2.012 | < 0.022 |
PFS = progression-free survival.
Source: CROWN protocol.18
Table 11: Updated Efficacy Boundaries for PFS and OS
Analysis | Events, n (%) | z score | P value (1-sided) |
|---|---|---|---|
PFS per BICR (interim analysis) | 127 (72%) | < −2.402 | 0.0081 |
OS (interim analysis 1) | 51 (26%) | < −4.264 | < 0.0001 |
BICR = blinded independent central review; OS = overall survival; PFS = progression-free survival.
Source: CROWN Clinical Study Report.17
As the secondary end point of the trial, OS was specified to be analyzed using a hierarchical testing procedure dependent on statistical significance of PFS favouring lorlatinib.18 A maximum of 3 analyses for OS were planned:
at the time of the interim/final analysis for PFS (where PFS exceeded the efficacy boundary)
at 70% of the 198 expected OS events
at 100% of the 198 expected OS events (the final analysis).
An alpha spending function according to Lan-DeMets (O’Brien-Fleming) independent of the function used for the primary efficacy analysis was used to preserve the 0.025 overall level of significance across the repeated testing of the OS in the interim and final analyses. The nominal P values used for declaration of statistical significance at the time of the analysis of OS were dependent on the number of OS events occurring at the time of the analyses and the alpha spent for OS at the time of the earlier analyses. Early stopping of the trial was permitted for a superior OS result, such that PFS, the primary end point, was shown to be statistically significantly favouring lorlatinib. The interim analyses for OS were to be performed by an independent statistician.18 At the time of data cut-off (March 20, 2020), 51 OS events (26% of the 198 events planned at the end of the study) had occurred, and efficacy boundaries for OS were updated based on Lan-DeMets (O’Brien-Fleming), which included a P value of < 0.0001 (Table 11).17
Analysis Populations
The full analysis set (FAS) included all patients who were randomized to the CROWN trial. Patients were analyzed according to the treatment group to which they were randomized. This analysis set was used for evaluate efficacy end points and patient characteristics.18 The FAS was considered equivalent to the intention-to-treat population.
The safety analysis set included all patients who received at least 1 dose of study treatment. Patients were classified according to the treatment they actually received.18
The patient-reported analysis set included patients in the FAS who completed a patient-reported outcome (PRO) assessment at baseline and at least 1 post-baseline assessment. This analysis set was used for the analyses of change from baseline scores and TTD in patient-reported pain in the chest, dyspnea, and cough in the EORTC QLQ-LC13. The analysis sets were separate for the EORTC QLQ-C30, EORTC QLQ-LC13, and EQ-5D-5L descriptive system and EQ VAS questionnaires.18
Primary End Point of Progression-Free Survival According to a BICR
The primary objective of the study was to determine whether lorlatinib was superior to crizotinib in prolonging PFS based on RECIST 1.1 criteria as determined by a BICR.18
The following protocol was used to censor PFS:
Patients were censored on the date of their last adequate tumour assessment if they:
did not experience an event (progression or death)
started a new anticancer treatment before experiencing a PFS event (progression or death)
experienced a PFS event after 2 or more missed tumour assessments.
Patients were censored on the day of randomization if they:
did not have a baseline tumour assessment
did not have any post-baseline tumour assessments.
The analyses of PFS were conducted using the FAS and a BICR with a 1-sided log-rank test stratified by the factors used for randomization (i.e., presence of brain metastases and ethnic origin). The significance of the log-rank test was preserved at a 1-sided 0.025 alpha at the interim and/or final analyses.18 The Kaplan-Meier method was used to estimate the PFS times of each treatment group, with corresponding 95% CIs calculated according to Brookmeyer and Crowley30 and results displayed graphically where appropriate. The CIs for the 25th, 50th and 75th percentiles were reported. A Cox proportional hazards model was used to determine HRs and corresponding 95% CIs. The log(-log) method according to Kalbfleisch and Prentice31 was used to estimate the CI for the survival function. The standard error (SE) was estimated using the Greenwood formula.18
Sensitivity Analyses for Progression-Free Survival
Sensitivity analyses were performed for the primary outcome of PFS per BICR and were considered exploratory.18 These analyses were conducted in the same manner as the primary analysis of this outcome and included:
counting all events of disease progression and deaths as PFS events regardless of missing assessments or timing of the event (i.e., not censoring due to start of new anticancer therapy before event or due to missed assessments)18
an unstratified analysis18
a stratified analysis using the 2 randomization stratification factors and baseline ECOG PS value from the case report forms18
multivariable Cox proportional hazards models to explore the potential influences of baseline patient characteristics (e.g., age, gender, ethnic origin, presence of brain metastasis at baseline per BICR intracranial assessment, smoking status, ECOG PS, extent of disease, and histology) on PFS.18
Secondary End Points
All secondary end points were analyzed using the FAS. Unless otherwise specified, tumour assessments for secondary end points were conducted by a BICR.18
Progression-Free Survival According to the Investigator
Analysis of PFS by investigator assessment was conducted using the same methods for PFS per BICR.18
Overall Survival
A 1-sided stratified log-rank test was used for the analysis of OS. A Cox proportional hazards model stratified for the presence of brain metastases and ethnic origin was used to estimate the HR for OS, and the corresponding 95% CI was calculated using the log(-log) method according to Kalbfleisch and Prentice.31 The Kaplan-Meier method was used to determine the OS of each treatment group, with CIs calculated according to Brookmeyer and Crowley30 and displayed graphically. The CIs for the 25th, 50th, and 75th percentiles were reported. To account for alpha spending, a repeated CI was calculated. The OS rate was estimated at 12, 24, and 36 months, with corresponding 2-sided 95% CIs. The estimate of the SE was computed using the Greenwood formula.18
Censoring for OS was conducted if:
patients were alive
patients withdrew consent
patients were lost-to-follow-up.
Sensitivity Analyses for Overall Survival
Sensitivity analyses for OS were considered exploratory and conducted in the same manner as the primary analysis for OS and included:
an unstratified analysis18
a stratified analysis using the 2 randomization stratification factors and baseline ECOG PS18
multivariable Cox proportional hazards models to explore the potential influences of baseline patient characteristics (e.g., age, gender, race, ethnic origin, presence of brain metastasis at baseline per BICR of intracranial assessment, smoking status, ECOG PS, disease stage, extent of disease, and histology) on OS.18
Subsequent Therapies
The statistical analysis plan of the CROWN trial pre-specified analyses that would correct for the receipt of subsequent anticancer therapies by patients. It was acknowledged that subsequent anticancer therapies had the potential to affect estimates of OS; although the impact was considered uncertain. Based on the type, frequency, or distribution of subsequent therapies, analyses were pre-specified to correct for effects of subsequent treatments.18
Objective Response Rate
In the analysis of ORR, patients without a documented CR or PR were considered nonresponders. The ORR was determined by a BICR and investigator assessment. To determine the ORR, the number of patients with a CR or PR was divided by the number of patients randomized to each treatment group and the corresponding exact 2-sided 95% CIs were calculated. The Cochran-Mantel-Haenszel test was used to provide a comparison of ORRs between the treatment groups with the corresponding 2-sided 95% CI.18
Subgroup Analyses
Subgroup analyses were pre-specified and performed on the following groups for PFS, OS, and ORR17:
age (< 65 years versus ≥ 65 years)
gender (male versus female)
ethnic origin (Asian versus non-Asian, from an interactive voice response system)
presence of baseline brain metastasis (yes versus no, from BICR intracranial assessment)
smoking status (never versus current/former)
ECOG PS (0 or 1 versus 2)
extent of disease (locally advanced versus metastatic)
histology (adenocarcinoma versus non-adenocarcinoma).
Exploratory End Points
Intracranial Objective Response Rate
A modified version of RECIST 1.1 was used to assess intracranial disease. Assessment of IC-ORR was conducted by a BICR. The IC-ORR was summarized in a manner similar to ORR with at least 1 baseline measurable intracranial lesion. Surgery or radiotherapy of extracranial lesions was stated not to affect the determination of IC-ORR.18
Intracranial Time to Progression
The IC-TTP was assessed by a BICR among the subgroups of patients with and without brain metastases at baseline. The same censoring rules used for PFS were applied to the analysis of IC-TTP, except that patients who died without experiencing disease progression were not censored, as death was not considered an event. Patients were also not censored in cases of surgery or radiotherapy if the surgery or radiotherapy involved an extracranial lesion. A 1-sided stratified log-rank test was conducted to test for treatment differences between treatment groups. The Kaplan-Meier method was used to summarize IC-TTP in each treatment group with corresponding 95% CIs, and the results were displayed graphically where appropriate. The CIs were reported for the 25th, 50th, and 75th percentiles. The Cox proportional hazards model was used to calculate treatment HRs and the corresponding 95% CIs.18
Probability of a First Event Being a CNS Progression, Non-CNS Progression, or Death
The competing risk approach to estimating cumulative incidence functions by treatment group was used to evaluate the probability of a first event being a CNS progression per BICR intracranial assessment, a non-CNS progression per BICR, or death. The time to first event being a competing event (which included a “CNS progression” or “non-CNS progression” or “death”) was defined as the time from randomization until the date of that specific event. Patients were censored on the date of their last tumour assessment if they did not have any competing events.18
Duration of Response
The censoring rules for analysis of DOR were the same as described for PFS. The Kaplan-Meier estimates were presented for each treatment group, including summary statistics (i.e., median DOR time, 2-sided 95% CI) depending on the number of patients who achieved a CR or PR and who subsequently had an event in each treatment group. The median DOR and associated CIs were calculated according to Brookmeyer and Crowley.30
Intracranial DOR
The IC-DOR was summarized in the subgroup of patients with at least 1 measurable intracranial lesion. Censoring rules for IC-DOR were the same as those described for PFS, except that surgery or radiotherapy for an extracranial lesion was not considered.18
Time to Tumour Response
Simple descriptive statistics (i.e., mean, SD, median, range, and interquartile range) were used to summarize TTR.18
Intracranial Time to Tumour Response
Intracranial TTR was summarized using simple descriptive statistics (i.e., mean, SD, median, range, and interquartile range).18
Testing of the Proportional Hazard Assumption
Testing of the proportional hazard assumption was conducted to evaluate the validity of the models for time-to-event outcomes (i.e., PFS and OS). Analyses were conducted by plotting Schoenfeld residuals for the stratified Cox proportional regression models to graphically investigate violations of the proportional hazard assumption. Based on this form of analysis, a non-zero slope was considered evidence of departure of the proportional hazard assumption. The proportional hazard assumption was also formally tested using Schoenfel residual test, using a P value of less than 0.05 as evidence of departure of the proportional hazard assumption. Visual examination of the proportional hazard assumption within each stratum was conducted by plotting log(–log[S(t)]) versus log(t), where S(t) was the estimated survival function for PFS at a specified time, t. In cases where there was evidence of large departures from the proportional hazard assumption, then PFS per BICR assessment was also analyzed based on restricted mean survival time differences.18,32
Patient-Reported Outcomes
Patient-reported outcomes were assessed using the EORTC QLQ-C30 (version 3.0), EORTC QLQ-LC13 (version 3.0), and EQ-5D-5L. The EORTC QLQ-C30, EORTC QLQ-LC13, and EQ-5D-5L were scored according to their respective validation papers and user guides. Higher scores on the EORTC QLQ-C30 represented “better” levels of functioning and/or “worse” level of symptoms. A minimal important difference (MID) of 10 points was used as the threshold for determining improvement or worsening from baseline in the EORTC QLQ-C30. Higher scores on the EORTC QLQ-LC13 represented “worse” level of symptoms. Higher scores in the EQ-5D-5L represented “better” self-rated health. Completion rates were summarized for each questionnaire, as well as summaries of descriptive statistics including change from baseline, mean, SE, and 95% CIs.18
A TTD analysis was conducted for pain in the chest, dyspnea, and cough individually and as a composite end point. This was defined as the time from randomization to the first time a patient’s score showed an increase of 10 points or more after baseline in any of the 3 symptoms. A stratified 1-sided log-rank test was used to compare the TTD in the 3 symptoms and composite end point between the treatment groups. Estimates of TTD were produced using Kaplan-Meier methods in each treatment group, including medians with associated 95% CIs calculated according to Brookmeyer and Crowley. The Cox proportional hazards model was used to determine treatment effects. Censoring occurred at the last day a patient completed a subscale assessment if they had not deteriorated, and death was not considered an event for the TTD.18
Results
Patient Disposition
A summary of the disposition of patients in the CROWN trial is provided in Table 12. The number of patients screened for eligibility was not reported, although the sponsor did report that 129 patients were considered screened failures. The reasons for screen failures were not collected.33 A total of 149 patients were randomized to the lorlatinib group and 142 patients were randomized to the crizotinib group. In the treatment phase, fewer patients in the lorlatinib group discontinued from the study than in the crizotinib group (30.9% versus 78.2%, respectively). The main reasons for discontinuation from the study in the respective treatment groups were disease progression (17.4% versus 58.5%), followed by AEs (6.7% versus 8.5%), withdrawal by the patient (2.7% versus 5.6%), and death (4.0% versus 2.8%). During the long-term follow-up phase, fewer patients in the lorlatinib group discontinued from the trial (18.1%) than in the crizotinib group (32.7%). The main reasons for study discontinuation in both treatment groups were death (15.4% versus 19.0%, respectively) and withdrawal by the patient (2.7% versus 12.2%, respectively). A total of 122 patients (81.9%) in the lorlatinib group remain ongoing in the trial, compared to 99 patients (67.3%) in the crizotinib group.17
Table 12: Patient Disposition of the CROWN Trial
Disposition | Description | |
|---|---|---|
Lorlatinib | Crizotinib | |
Screened, N | NR | NR |
Randomized, N (%) | 149 (100.0) | 142 (100.0) |
Treated, N (%) | 149 (100.0) | 142 (100.0) |
Not treated, N (%) | 0 | 5 (3.4) |
Treatment phase | ||
Discontinued from study, N (%) | 46 (30.9) | 111 (78.2) |
Reason for discontinuation, N (%) | ||
Adverse events | 10 (6.7) | 12 (8.5) |
Death | 6 (4.0) | 4 (2.8) |
Lost to follow-up | 0 | 0 |
Progressive disease | 26 (17.4) | 83 (58.5) |
Protocol deviation | 0 | 0 |
Sponsor termination | 0 | 0 |
Withdrawal by patient | 4 (2.7) | 8 (5.6) |
Medication error | 0 | 0 |
Global deterioration | 0 | 3 (2.1) |
Other | 0 | 1 (0.7) |
Ongoing | 103 (69.1) | 31 (21.8) |
Long-term follow-up phase | ||
Discontinued from study, N (%) | 27 (18.1) | 48 (32.7) |
Reason for discontinuation, N (%) | ||
Death | 23 (15.4) | 28 (19.0) |
Lost to follow-up | 0 | 2 (1.4) |
Study terminated by sponsor | 0 | 0 |
Withdrawal by patient | 4 (2.7) | 18 (12.2) |
Other | 0 | 0 |
Ongoing | 122 (81.9) | 99 (67.3) |
Analysis sets, N (%) | ||
FAS | 149 (100.0) | 147 (100.0) |
Safety | 149 (100.0) | 142 (96.6) |
PRO | ||
EORTC QLQ-C30 | 148 (99.3) | 140 (95.2) |
EORTC QLQ-LC13 | 146 (98.0) | 139 (94.6) |
EQ-5D-5L | 148 (99.3) | 140 (95.2) |
EQ VAS | 147 (98.7) | 138 (93.9) |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer 13; EQ-5D-5L = EQ-5D 5-Levels questionnaire; EQ VAS = EQ-5D Visual Analogue Scale; FAS = full analysis set; NR = not reported; PRO = patient-reported outcome.
Source: CROWN Clinical Study Report.17
Protocol Deviations
Important protocol deviations were reported among similar proportions of patients in both the lorlatinib and crizotinib groups (43.0 versus 41.5%, respectively). Most important protocol deviations were due to informed consent (17.2%), procedures and tests (12.8%), and investigational product (10.1%). Similar proportions of important protocol deviations were reported across both treatment groups, and no important protocol deviation was reported for greater than 20% of patients.
Protocol Amendments
The original protocol of the CROWN trial, dated October 5, 2016, was amended a total of 4 times. The amendments were mainly to do with clarifications and minor updates. During the fourth amendment of the protocol, dated October 4, 2019, a change was made to the design of the study based on a primary end point of PFS assessed by BICR. The original design of the trial specified a planned futility analysis for PFS to occur when approximately 60% of events had occurred. However, the amendment replaced the futility analysis with an interim analysis to be conducted when approximately 75% of events had occurred. Accordingly, changes were made to the sample size calculations of the trial and the efficacy boundaries at the interim and final analysis of PFS were determined. The stated rationale for the change was based on the observation that PFS events in the CROWN trial were occurring at a rate slower than originally expected, and on the availability of alternative treatment options for patients.18
Exposure to Study Treatments
Duration and Dose Intensity
The mean duration of treatment was 16.6 months (SD = 8.32) in the lorlatinib group compared to 10.4 months (SD = 6.90) in the crizotinib group (Table 13). The median duration of treatment was not estimable (NE) in the lorlatinib group and 9.6 months (95% CI, 7.6 to 11.1) in the crizotinib group. At the data cut-off date, more patients in the lorlatinib group remained on treatment than in the crizotinib group (69.1% versus 21.8%, respectively).
As the duration of treatment was longer in the lorlatinib group, the dose intensity and cumulative dose intensity were greater in this group compared to the crizotinib group. The relative dose intensity was similar in the treatment groups.
Table 13: Summary of Exposure to Study Treatment — Safety Analysis Set
Exposure | Lorlatinib N = 149 | Crizotinib N = 142 |
|---|---|---|
Duration of treatment (months), mean (SD)a | 16.6 (8.32) | 10.4 (6.90) |
Treatment duration, n (%) | ||
≥ 6 months | 126 (84.6) | 97 (68.3) |
≥ 12 months | 113 (75.8) | 49 (34.5) |
≥ 18 months | 67 (45.0) | 19 (13.4) |
Kaplan-Meier estimates of time to event (months), median (95% CI)b | NE (NE to NE) | 9.6 (7.6 to 11.1) |
Cumulative dose (mg),c mean (SD) | 46,106.7 (24,414.31) | 146,237.7 (98,040.64) |
Dose intensity (mg/week),d mean (SD) | 661.2 (78.83) | 3,371.4 (311.80) |
Relative dose intensity (%),e mean (SD) | 94.5 (11.26) | 96.3 (8.91) |
NE = not estimable; SD = standard deviation.
aDuration of treatment was defined as duration (months) = (last dose date − first dose date + 1)/30.4375.
bBased on the Brookmeyer and Crowley method.
cCumulative dose = sum of the actual dose levels (mg) of treatment received.
dDose intensity (mg/week) = (cumulative dose [mg])/(actual duration of treatment [weeks]).
eRelative dose intensity (%) = 100 × (dose intensity [mg/week])/(7 × 100 [mg/week]) for lorlatinib; relative dose intensity (%) = 100 × (dose intensity [mg/week])/(7 × 2 × 250 [mg/week]) for crizotinib.
Source: CROWN Clinical Study Report.17
Dose Modifications
A summary of the dose reductions and interruptions that occurred in the trial by treatment group is provided in Table 14. A dose reduction was defined as a non-zero dose that was less than the prior dose. Dose reductions were reported in 41 patients (27.5%) in the lorlatinib group and 32 patients (22.5%) in the crizotinib group. The proportion of patients requiring 1 dose reduction was similar between the lorlatinib (16.1%) and crizotinib (16.2%) groups; and the proportion of patients requiring 2 dose reductions was greater in the lorlatinib group (11.4% versus 6.3%, respectively). All dose reductions were due to AEs in the lorlatinib group, and almost all were due to AEs in the crizotinib group.
Dose interruptions were defined as a temporary discontinuation of dosing for more than 1 day. At least 1 dose interruption occurred in 79 patients (53.0%) in the lorlatinib group and 68 patients (47.9%) in the crizotinib group. The proportions of patients requiring any number of dose interruptions was similar across both treatment groups. Most patients in either treatment group required only 1 or 2 dose interruptions, and the majority of dose interruptions were due to AEs (49.0% in the lorlatinib group versus 44.4% in the crizotinib group). The dose interruptions due to “other” reasons were related to mistakes or oversight from patients and medical procedure protocols that required dose interruptions (6.7% in the lorlatinib group and 11.3% in the crizotinib group).
Table 14: Summary of Dose Modifications — Safety Analysis Set
Dose modification, n (%) | Lorlatinib (N = 149) | Crizotinib (N = 142) |
|---|---|---|
Patients with at least 1 dose reduction based on investigator prescriptiona | ||
Patients, n (%) | 41 (27.5) | 32 (22.5) |
1 reduction | 24 (16.1) | 23 (16.2) |
2 reductions | 17 (11.4) | 9 (6.3) |
Reasons for dose reduction | ||
AEs | 41 (27.5) | 30 (21.1) |
Patients with at least 1 dose interruptionb | ||
Patients, n (%) | 79 (53.0) | 68 (47.9) |
1 interruption | 44 (29.5) | 32 (22.5) |
2 interruptions | 17 (11.4) | 19 (13.4) |
3 interruptions | 10 (6.7) | 11 (7.7) |
≥ 4 interruptions | 8 (5.4) | 6 (4.2) |
Reasons for dose interruption | ||
Adverse events | 73 (49.0) | 63 (44.4) |
Other | 10 (6.7) | 16 (11.3) |
Note: Dose modification could be attributed to more than 1 reason if multiple dose reductions or interruptions occurred for different reasons.
aDose reduction was defined as a non-zero planned dose that was less than the prior planned dose and was administered for more than 1 day.
bDose interruption was defined as a 0 mg dose administered for more than 1 day.
Source: CROWN Clinical Study Report.17
Concomitant Treatments
Most patients in each treatment group received concomitant medications (96.6% versus 95.1%, respectively); however, the frequency of some concomitant medications differed by treatment group. Rosuvastatin calcium (38.9%), paracetamol (36.9%), furosemide (28.9%), and rosuvastatin (24.8%) were the most commonly reported (≥ 20%) concomitant medications in the lorlatinib group, compared to paracetamol (39.4%) and metoclopramide (21.8%), which were most commonly reported in the crizotinib group.17
Subsequent Therapies
At the cut-off date, |||||||||||||| in the crizotinib group had received subsequent therapy compared with patients in the lorlatinib group (Table 15). |||||||||||||| in the crizotinib group |||||||| had received at least 1 type of follow-up systemic anticancer treatment compared with patients in the lorlatinib group ||||||||. |||||||||||||| in the crizotinib group received 1 |||||||||||||||||||||||||| or 2 subsequent therapies |||||||||||||||||||||||| compared to the patients in the lorlatinib group and |||||||||||||||||||||| of patients in each treatment group received 3 or more subsequent therapies. Radiotherapy was received by |||| of patients in the crizotinib group versus |||| of patients in the lorlatinib group, and no patients in either treatment group received subsequent anticancer surgery.17
The first and second subsequent therapy was |||||||||||||||| an ALK TKI compared with chemotherapy with or without an anti-angiogenic therapy, an immunotherapy or other (Table 16). A subsequent TKI was |||||||||||||| in the crizotinib group (|||||| compared with the lorlatinib group ||||||||; alectinib (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||) and brigatinib (|||||||||||||||||||||| ||||||||||||) were |||||||||||||||| reported as a first subsequent TKI in the crizotinib group compared with the lorlatinib group, whereas crizotinib (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||) and ceritinib (||||||||||||||||||||||||||||||||||||||||) were ||||||||||| reported as a first subsequent ALK TKI in the lorlatinib group. Chemotherapy with or without an anti-angiogenic therapy was |||||||||||||| in the lorlatinib group (|||||| compared with the crizotinib group (|||||||||||||||||||| in either group received either immunotherapy (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||) or other (||||||||||||||||||||||||).17
An ALK TKI as a second subsequent therapy was |||||||||||||| in the lorlatinib group (||||||||||||||||||||||||||||||||||||||||||||||||||). Alectinib (||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||) and brigatinib (||||||||||||||||||) were both |||||||||||||| as a second subsequent TKI in the lorlatinib group compared with the crizotinib group, whereas ceritinib (|||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||) and lorlatinib (||||||||||||||||||) were |||||||||||||| as a second subsequent ALK TKI in the crizotinib group compared with the lorlatinib group. Chemotherapy with or without an anti-angiogenic was |||||||||||||| in the crizotinib group (|||||| compared to the lorlatinib group ||||||)17
|||||||||||||| received a third subsequent systemic anticancer therapy. A third subsequent ALK TKI was |||||||||||||| in the crizotinib group (||||) compared with the lorlatinib group (|||||| Chemotherapy with or without an anti-angiogenic therapy was reported in |||| |||||||||||||||||| in the lorlatinib group and |||||||||||||||||||||||| in the crizotinib group.17
Table 15: Summary of Patients Receiving Subsequent Anticancer Therapies in the CROWN Trial [Redacted]
|||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| |
|---|---|---|
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Note: This table has been redacted at the sponsor’s request.
Source: CROWN Clinical Study Report.17
Table 16: Breakdown of Subsequent Anticancer Therapies Administered to Patients in the CROWN Trial [Redacted]
|||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| |
|---|---|---|
|||||||||||||||||||| | |||||||||||||||||||| | |||||||||||||||||||| |
Note: This table has been redacted as per the sponsor’s request.
Source: CROWN Clinical Study Report.17
Efficacy
At the data cut-off date (March 20, 2020), the CROWN trial met its primary end point and demonstrated a statistically significant difference in PFS that favoured treatment with lorlatinib over crizotinib. The median PFS follow-up duration was 18.3 months (95% CI, 16.4 to 20.1) in the lorlatinib group and 14.8 months (95% CI, 12.8 to 18.4) in the crizotinib group. Based on pre-specified statistical criteria, this was considered the final analysis for PFS, and no formal testing for PFS was planned for future time points.17 At the time of this analysis, OS, which was hierarchically tested depending on the statistical significance of PFS, did not show any statistically significant difference between the lorlatinib and crizotinib treatment groups.17 A detailed summary of the results for the primary and secondary end points of the CROWN trial are reported in Table 17. A summary of the results of intracranial efficacy end points, which were assessed as exploratory outcomes, are reported in Table 18.
The sponsor assessed the proportional hazards for PFS by performing tests for statistical significance using log(-log(Survival)) plots and a plot of Schoenfeld residuals from stratified Cox proportional regression models. The sponsor provided the log(-log(Survival)) plots and a plot of Schoenfeld residuals; however, the results of proportional hazards tests were not reported.
Table 17: Summary of Efficacy End Points in the CROWN Trial — Full Analysis Set
Outcomes | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
PFS according to BICR | ||
Events, n (%) | 41 (27.5) | 86 (58.5) |
Progressive disease | 32 (21.5) | 82 (55.8) |
Death | 9 (6.0) | 4 (2.7) |
Median (months), (95% CI)a | NE (NE to NE) | 9.3 (7.6 to 11.1) |
Stratified HR (95% CI)b,c | 0.28 (0.191 to 0.413) | |
Stratified log-rank 1-sided P valued | < 0.0001e | |
OS | ||
Events, n (%) | 23 (15.4) | 28 (19.0) |
Median, months (95% CI)a | NE (NE to NE) | NE (NE to NE) |
Stratified HR (95% CI)c | 0.72 (0.414 to 1.249) | |
ORR per BICR | ||
ORR, n (%) | 113 (75.8) | 85 (57.8) |
95% CI | 68.2 to 82.5 | 49.4 to 65.9 |
BOR, n (%) | ||
CR | 4 (2.7) | 0 |
PR | 109 (73.2) | 85 (57.8) |
SD | 19 (12.8) | 41 (27.9) |
Non-CR/Non-PD | 3 (2.0) | 3 (2.0) |
PD | 10 (6.7) | 7 (4.8) |
Not evaluable | 4 (2.7) | 11 (7.5) |
DOR per BICRf | N = 113 | N = 85 |
Events, n (%) | 18 (15.9) | 45 (52.9) |
Progressive disease | 14 (12.4) | 45 (52.9) |
Death | 4 (3.5) | 0 |
Median, months (95% CI)a | NE (NE to NE) | 11.0 (9.0 to 12.9) |
Range (minimum to maximum) | 0.9 to 31.3 | 1.1 to 27.5 |
TTR per BICR | ||
Mean, months (SD) | 2.13 (1.370) | 2.12 (1.252) |
BICR = blinded independent central review; BOR = best overall response; CI = confidence interval; CR = complete response; DOR = duration of response; HR = hazard ratio; NE = not estimable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PD = progressive disease; PR = partial response; SD = standard deviation; TTR = time to response.
aBased on the Brookmeyer and Crowley method.
bStratified by presence of brain metastases (yes or no) and ethnic origin (Asian or non-Asian) at randomization from interactive response technology stratification values.
cHazard ratio based on Cox proportional hazards model; under proportional hazards; a HR < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to crizotinib.
dClopper-Pearson method used.
eP value was based on stratified log-rank test.
fPatients with confirmed CR or PR in the FAS.
Source: CROWN Clinical Study Report.17
Table 18: Summary of Exploratory Intracranial-Specific Efficacy End Points Based on BICR Assessment (Modified RECIST 1.1) — Full Analysis Set
End points | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
IC-TTPa | ||
Events, n (%) | 5 (3.4) | 45 (30.6) |
Median, months (95% CI)b | NE (NE to NE) | 16.6 (11.1 to NE) |
Stratified HR (95% CI)c d | 0.07 (0.026 to 0.170) | |
Stratified log-rank 1-sided P valuee | < 0.0001f | |
IC-TTP among patients with brain metastasis | ||
Number of patients contributing to the analysis | 38 | 40 |
Events, n (%) | 4 (10.5) | 26 (65.0) |
Median, months (95% CI) | NE (NE to NE) | 7.3 (3.7 to 9.3) |
Stratified HR,c d (95% CI) | 0.08 (0.026 to 0.227) | |
1-sided P valuee | < 0.0001f | |
IC-TTP among patients without brain metastasis | ||
Number of patients contributing to the analysis | 38 | 40 |
Events, n (%) | 1 (000.9) | 19 (17.8) |
Median, months (95% CI)b | NE (NE to NE) | NE (16.6 to NE) |
Stratified HR (95% CI)c d | 0.03 (0.004 to 0.230) | |
1-sided P valuee | < 0.0001f | |
Risk of CNS progression | ||
Number of patients contributing to the analysis | 38 | 40 |
CNS progression without prior non-CNS progressive disease | ||
Events | 4 (2.7) | 35 (23.8) |
Cause-specific stratifiedc analysis HRd (95% CI) | 0.06 (0.022 to 0.182) | |
log-rank 1-sided P valuef | < 0.0001f | |
Non-CNS progression without prior CNS progressive disease | ||
Events | 29 (19.5) | 54 (36.7) |
Cause-specific stratifiedc analysis HRd (95% CI) | 0.30 (0.185 to 0.474) | |
log-rank 1-sided P valuef | < 0.0001f | |
Death without prior CNS or non-CNS progressive disease | ||
Events | 9 (6.0) | 4 (2.7) |
Cause-specific stratifiedc analysis HRd (95% CI) | 1.66 (0.501 to 5.500) | |
log-rank 1-sided P valuef | 0.7966f | |
IC-ORR among patients with brain metastasis | ||
Number of patients contributing to the analysis | 38 | 40 |
IC-ORR, n (%) | 25 (65.8) | 8 (20.0) |
95% CIh | 48.6 to 80.4 | 9.1 to 35.6 |
IC-ORR among patients with at least 1 measurable brain metastasis | ||
Number of patients contributing to the analysis | 17 | 13 |
IC-ORR, n (%) | 14 (82.4) | 3 (23.1) |
95% CIh | 56.6 to 96.2 | 5.0 to 53.8 |
IC-DOR among patients with brain metastases at baseline and confirmed CR or PR | ||
Number of patients contributing to the analysis | 25 | 8 |
Median, months (95% CI) | NE (NE to NE) | 9.4 (6.0 to 11.1) |
IC-DOR among patients with at least 1 measurable brain metastasis and confirmed CR or PR | ||
Number of patients contributing to the analysis | 14 | 3 |
Median, months (95% CI) | NE (NE to NE) | 10.2 (9.4 to 11.1) |
IC-TTR among patients with brain metastases at baseline and confirmed CR or PR | ||
Number of patients contributing to the analysis | 25 | 8 |
Mean (SD) | 3.04 (2.800) | 2.21 (0.844) |
IC-TTR among patients with at least 1 measurable brain metastasis at baseline and confirmed CR or PR | ||
Number of patients contributing to the analysis | 25 | 8 |
Mean (SD) | 2.39 (0.886) | 1.86 (0.083) |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; CR = complete response; HR = hazard ratio; IC-DOR = intracranial duration of response; IC-ORR = intracranial objective response rate; IC-TTP = intracranial time to progression; IC-TTR = intracranial time to response; NE = not estimable; PR = partial response; RECIST = Response Evaluation Criteria in Solid Tumors Version 1.1; SD = standard deviation.
aPatients with confirmed CR or PR in the full analysis set.
bBased on Brookmeyer and Crowley method.
cStratified by presence of brain metastases (yes or no) and ethnic origin (Asian or non-Asian) at randomization from interactive response technology stratification values.
dHazard ratio based on Cox proportional hazards model; under proportional hazards; an HR < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to crizotinib.
eP value was based on stratified log-rank test.
fP value was not adjusted for multiplicity.
gPatients with brain metastases at baseline.
hClopper-Pearson method used.
Source: CROWN Clinical Study Report.17
Primary End Point: Progression-Free Survival per BICR
A lower proportion of patients experienced a PFS event in the lorlatinib group (27.5%) than in the crizotinib group (58.5%). The majority of the PFS events were progression events (21.5% versus 55.8%, respectively), with deaths representing 6.0% and 2.7%, respectively). A statistically significant improvement in PFS was demonstrated in the lorlatinib group compared to the crizotinib group, corresponding to a 72% reduction in the risk of progression or death (stratified HR = 0.28; 95% CI, 0.191 to 0.413; stratified 1 sided log-rank P < 0.001). The median PFS in the lorlatinib group was NE (95% CI, NE to NE) compared to 9.3 months (95% CI, 7.6 to 11.1) in the crizotinib group (Figure 3).17
More patients in the lorlatinib group were censored in the analysis of PFS than in the crizotinib group (72.5% versus 41.5%, respectively). The primary reasons for censoring were due to patients continuing without an event (62.4% in the lorlatinib group versus 15.6% in the crizotinib group), beginning a new anticancer therapy (6.7% versus 16.3%, respectively) or withdrawing from the trial (2.0% versus 9.5%, respectively) (Table 19).17
Figure 3: Kaplan-Meier Plot of PFS (Primary Analysis) per BICR Assessment (RECIST 1.1) — Full Analysis Set
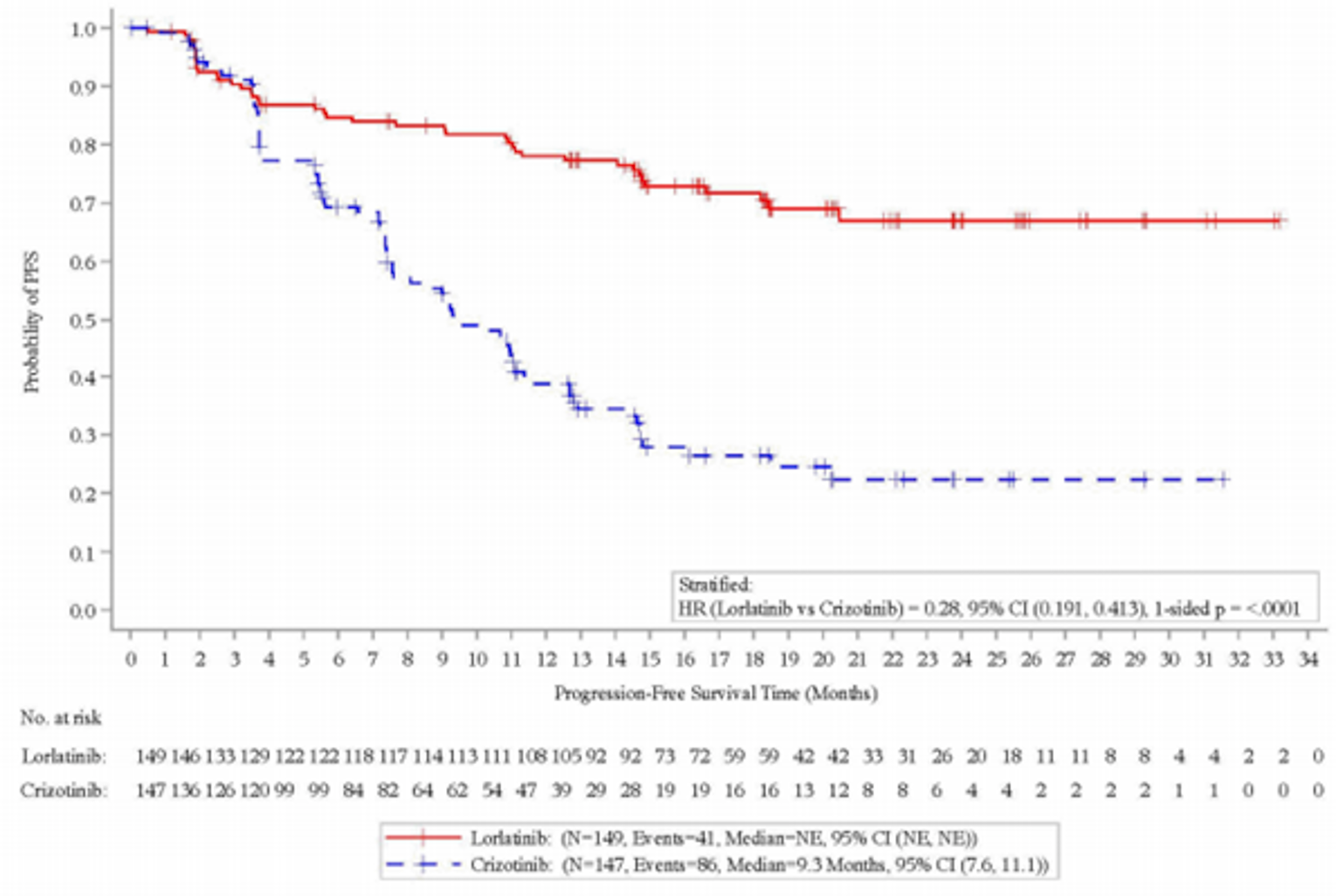
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; NE = not estimable; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; vs. = versus.
Source: CROWN Clinical Study Report.17
Table 19: Censoring for Primary Analysis of PFS per BICR — Full Analysis Set
Censored patients | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Censored patients, n (%) | 108 (72.5) | 61 (41.5) |
Reasons for censoring, n (%) | ||
No adequate baseline assessment | 0 | 0 |
Start of new anticancer therapy | 10 (6.7) | 24 (16.3) |
Event after ≥ 2 missing or inadequate post-baseline assessments | 1 (0.7) | 0 |
Withdrawal of consent | 3 (2.0) | 14 (9.5) |
Lost to follow-up | 1 (0.7) | 0 |
No adequate post-baseline tumour assessment | 0 | 0 |
Ongoing without an event | 93 (62.4) | 23 (15.6) |
BICR = blinded independent central review; PFS = progression-free survival.
Source: CROWN Clinical Study Report.17
Subgroup Analysis
Subgroup analyses are depicted in Figure 4. All subgroup analyses supported the primary analysis of PFS, which favoured treatment with lorlatinib over crizotinib.17
Figure 4: Forest Plot of PFS per BICR Assessment (RECIST 1.1) by Subgroups — Full Analysis Set
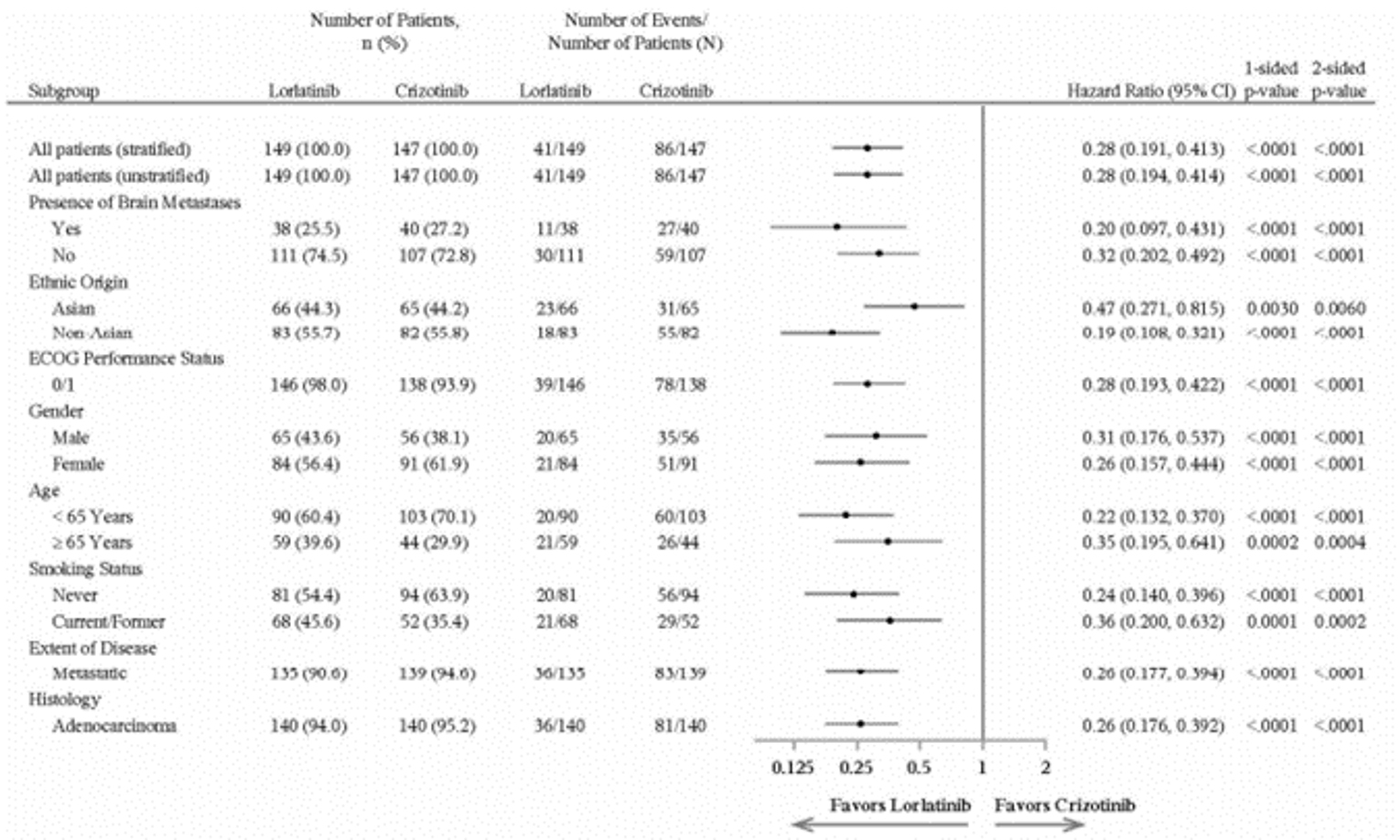
CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Note: Presence of brain metastases subgroup was based on modified RECIST 1.1 BICR baseline data. Hazard ratios were not calculated due to insufficient numbers of events (< 10 events on either treatment group within the defined subset), as dictated by the statistical analysis plan, for patients who had an ECOG Performance Status of 2 (2 versus 8), extent of locally advanced (5 versus 3) or histology of non-adenocarcinoma (5 versus 5). Stratified by presence of brain metastases (yes or no) and ethnic origin (Asian or non-Asian) at randomization. Percentages were calculated based on the number of patients in the FAS in each treatment group. Plot presented on a log scale (base = 2). P values were not adjusted for multiplicity.
Source: CROWN Clinical Study Report.17
Secondary End Point: Overall Survival
At the time of the interim analysis, the majority of patients in both treatment groups were alive. Of the 198 OS events required for the final analysis of OS, 51 (26%) occurred at the time of the primary analysis (final) of PFS, including 23 (15.4%) in the lorlatinib group and 28 (19.0%) in the crizotinib group (Figure 5). The statistical boundary of efficacy for OS was not crossed. The median OS was NE in either treatment group. Preliminary results for OS demonstrated an HR of 0.72 (95% CI, 0.414 to 1.249), which were not statistically significant.17
Similar proportions of patients were censored in the lorlatinib (84.6%) and crizotinib (81.0%) groups in the analysis of OS (Table 20). The reasons for censoring were primarily patients remaining alive (81.9% in the lorlatinib group versus 67.3% in the crizotinib group) and withdrawal of consent (2.7% versus 12.2%, respectively).17
Figure 5: Kaplan-Meier Plot of Overall Survival — Full Analysis Set
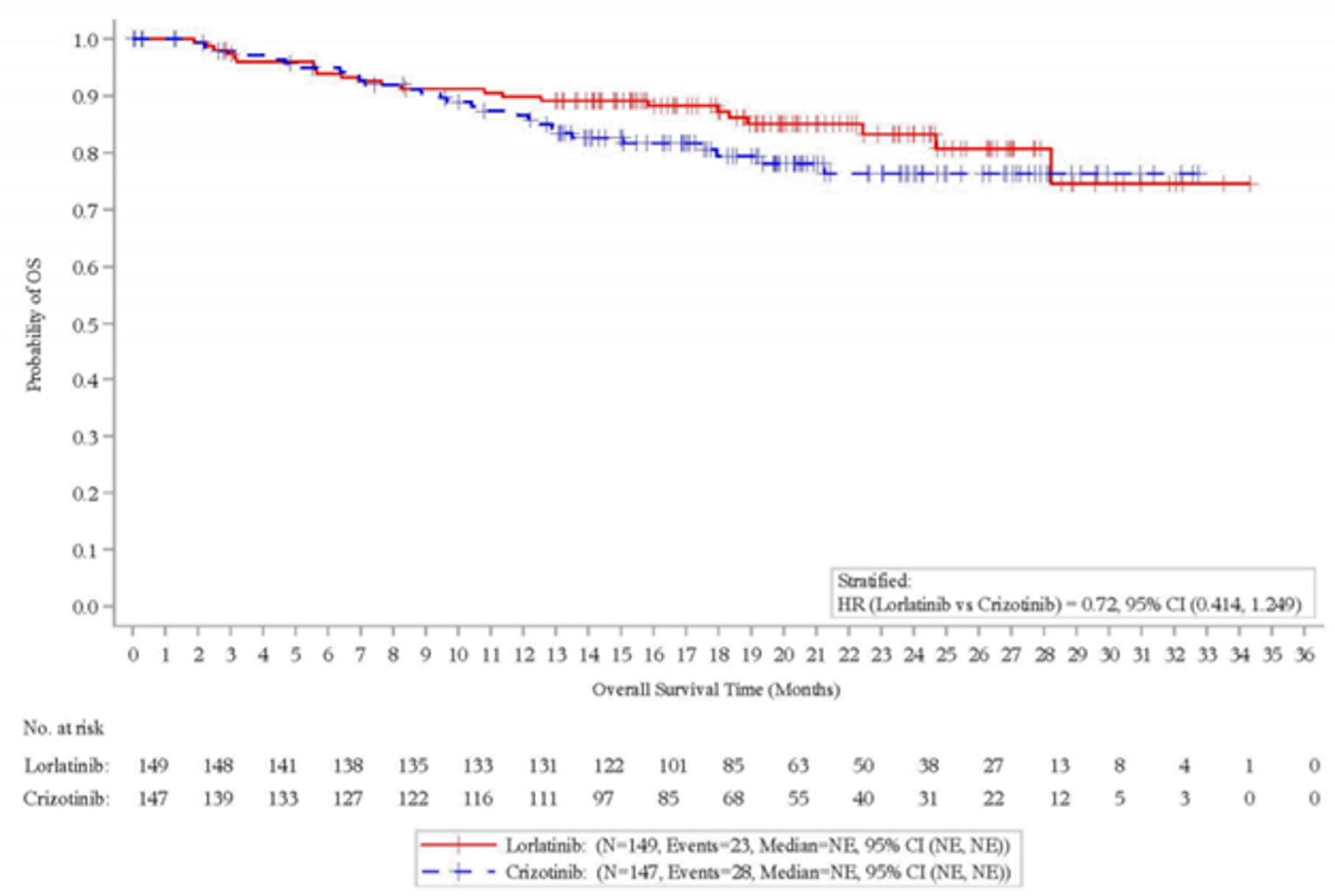
CI = confidence interval; HR = hazard ratio; NE = not estimable; OS = overall survival.
Source: CROWN Clinical Study Report.17
Table 20: Censoring for Overall Survival Analysis — Full Analysis Set
Censored patients | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Censored patients, n (%) | 126 (84.6) | 119 (81.0) |
Reasons for censoring, n (%) | ||
Withdrawal of consent | 4 (2.7) | 18 (12.2) |
Lost to follow-up | 0 | 2 (1.4) |
Alive | 122 (81.9) | 99 (67.3) |
Source: CROWN Clinical Study Report.17
Exploratory End Point: Progression-Free Survival per Investigator Assessment
The results for PFS assessed by investigator were consistent with the results for PFS assessed by a BICR. Results favoured the lorlatinib group over the crizotinib group (HR = 0.21; 95% CI, 0.144 to 0.307). The median PFS was NE in the lorlatinib group (95% CI, NE to NE) and 9.1 months (95% CI, 7.4 to 10.9) in the crizotinib group (Figure 6).17
More patients in the lorlatinib group were censored (73.2%) than in the crizotinib group (29.3%) (Table 21). Censoring was mainly due to patients continuing without an event (64.4% in the lorlatinib group versus 15.6% in the crizotinib group), withdrawal of consent (2.0% versus 7.5%, respectively), and starting a new anticancer therapy (3.4% versus 5.4%, respectively).17
Figure 6: Kaplan-Meier Plot of PFS Based on Derived Investigator Assessment (RECIST 1.1) — Full Analysis Set
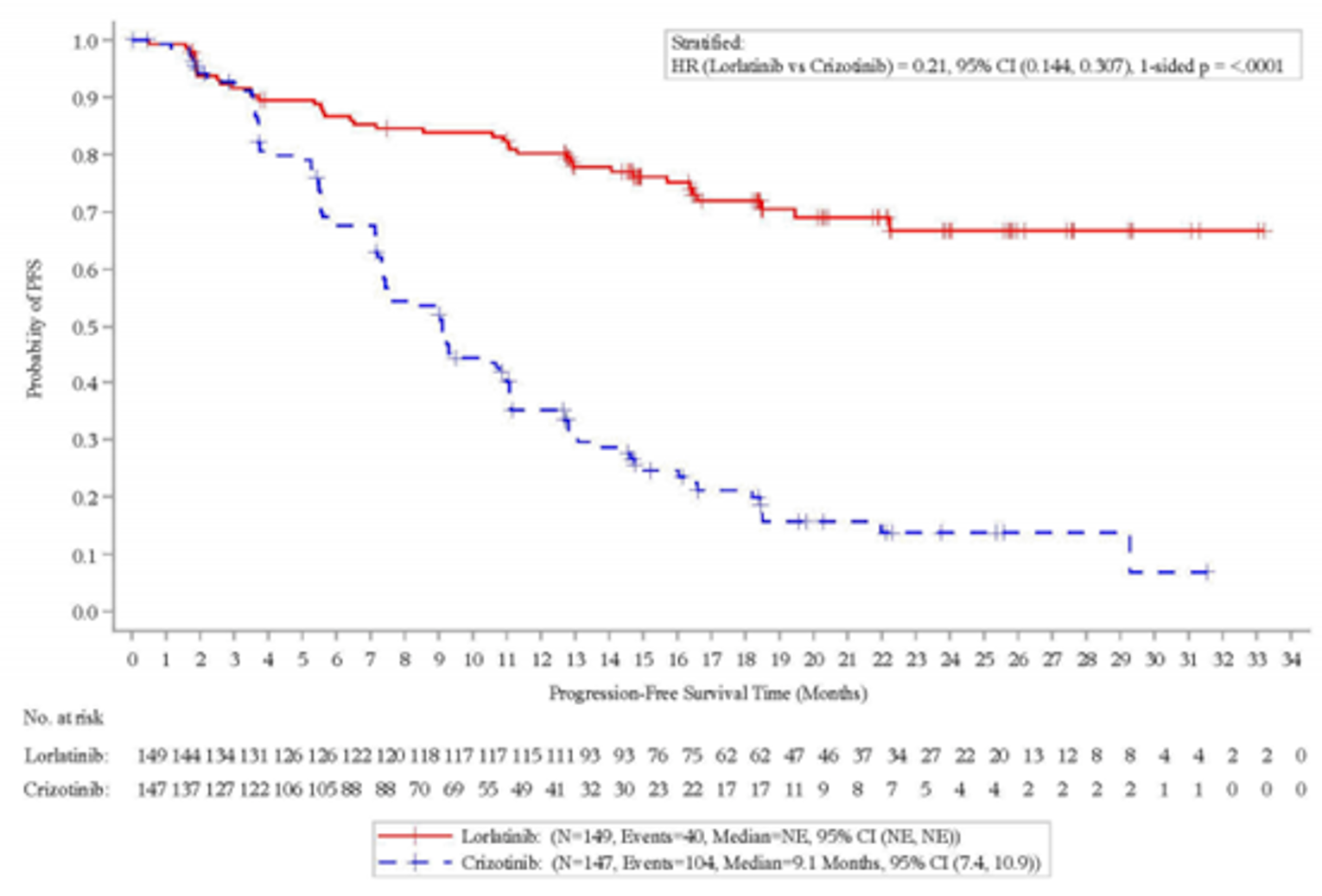
CI = confidence interval; HR = hazard ratio; NE = not estimable; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: CROWN Clinical Study Report.17
Table 21: Censoring for Secondary End Point PFS by Investigator — Full Analysis Set
Censored patients | Lorlatinib (N = 149) | Crizotinib (N = 147) |
|---|---|---|
Censored patients, n (%) | 109 (73.2) | 43 (29.3) |
Reasons for censoring, n (%) | ||
No adequate baseline assessment | 1 (0.7) | 0 |
Start of new anticancer therapy | 5 (3.4) | 8 (5.4) |
Event after ≥ 2 missing or inadequate post-baseline assessments | 2 (1.3) | 1 (0.7) |
Withdrawal of consent | 3 (2.0) | 11 (7.5) |
Lost to follow-up | 2 (1.3) | 0 |
No adequate post-baseline tumour assessment | 0 | 0 |
Ongoing without an event | 96 (64.4) | 23 (15.6) |
PFS = progression-free survival.
Source: CROWN Clinical Study Report.17
Exploratory End Point: ORR per BICR
The ORR was numerically higher in the lorlatinib group at 75.8% (95% CI, 68.2 to 82.5) compared to 57.8% (95% CI, 49.4 to 65.9) in the crizotinib group. Similarly, more patients in the lorlatinib group than in the crizotinib group achieved a CR (2.7% versus 0, respectively) or PR (73.2% versus 57.8%, respectively).17
Exploratory End Point: DOR per BICR
The median DOR was NE (95% CI, NE to NE) in the lorlatinib group, and 11.0 months (95% CI, 9.0 to 12.9) in the crizotinib group.17 There was a large amount of censoring in the analysis of DOR; 84.1% of patients in the lorlatinib group and 47.1% in the crizotinib group were censored, mainly due to patients continuing without an event (75.2% versus 22.4%, respectively), or starting a new anticancer therapy (5.2% versus 18.8%, respectively). Fewer patients in the lorlatinib group (15.9%) had an event compared with the crizotinib group (52.9%), and most were events of progressive disease (12.4% versus 52.9%, respectively).
Exploratory End Point: Time to Tumour Response per BICR (RECIST 1.1)
Among patients with a confirmed objective response (CR or PR) per BICR assessment, the mean TTR was similar in the treatment groups, at 2.13 months in the lorlatinib group (SD = 1.370) and 2.12 months (SD = 1.252) in the crizotinib group.17
Exploratory End Point: Intracranial Time to Progression per BICR (Modified RECSIT 1.1)
The time to CNS progression was numerically longer in patients treated in the lorlatinib group than the crizotinib group (Figure 7). The median IC-TTP was NE (95% CI, NE to NE) in the lorlatinib group and 16.6 months (95% CI, 11.1 to NE) in the crizotinib group (HR = 0.07; 95% CI, 0.026 to 0.170; nominal 1-sided P < 0.0001).17
In the subset of patients with brain metastases at baseline, fewer patients in the lorlatinib group than in the crizotinib group experienced an event (10.5% versus 65.0%, respectively). The median IC-TTP per BICR was NE in the lorlatinib group (95% CI, NE to NE) and 7.3 months (95% CI, 3.7 to 9.3) in the crizotinib group (Table 22). The stratified HR was 0.08 (95% CI, 0.026 to 0.227) (Figure 8).17
In the subset of patients without brain metastases at baseline, 1 patient (0.9%) in the lorlatinib group experienced an event compared to 19 patients (17.8%) in the crizotinib group (Table 23). The median IC-TTP among patients without brain metastases at baseline was NE in either treatment group. The stratified HR favoured the lorlatinib group over the crizotinib group (HR = 0.03; 95% CI, 0.004 to 0.230) (Figure 9).17
Figure 7: Kaplan-Meier Plot of IC-TTP Based on BICR Assessment (Modified RECIST 1.1) — Full Analysis Set
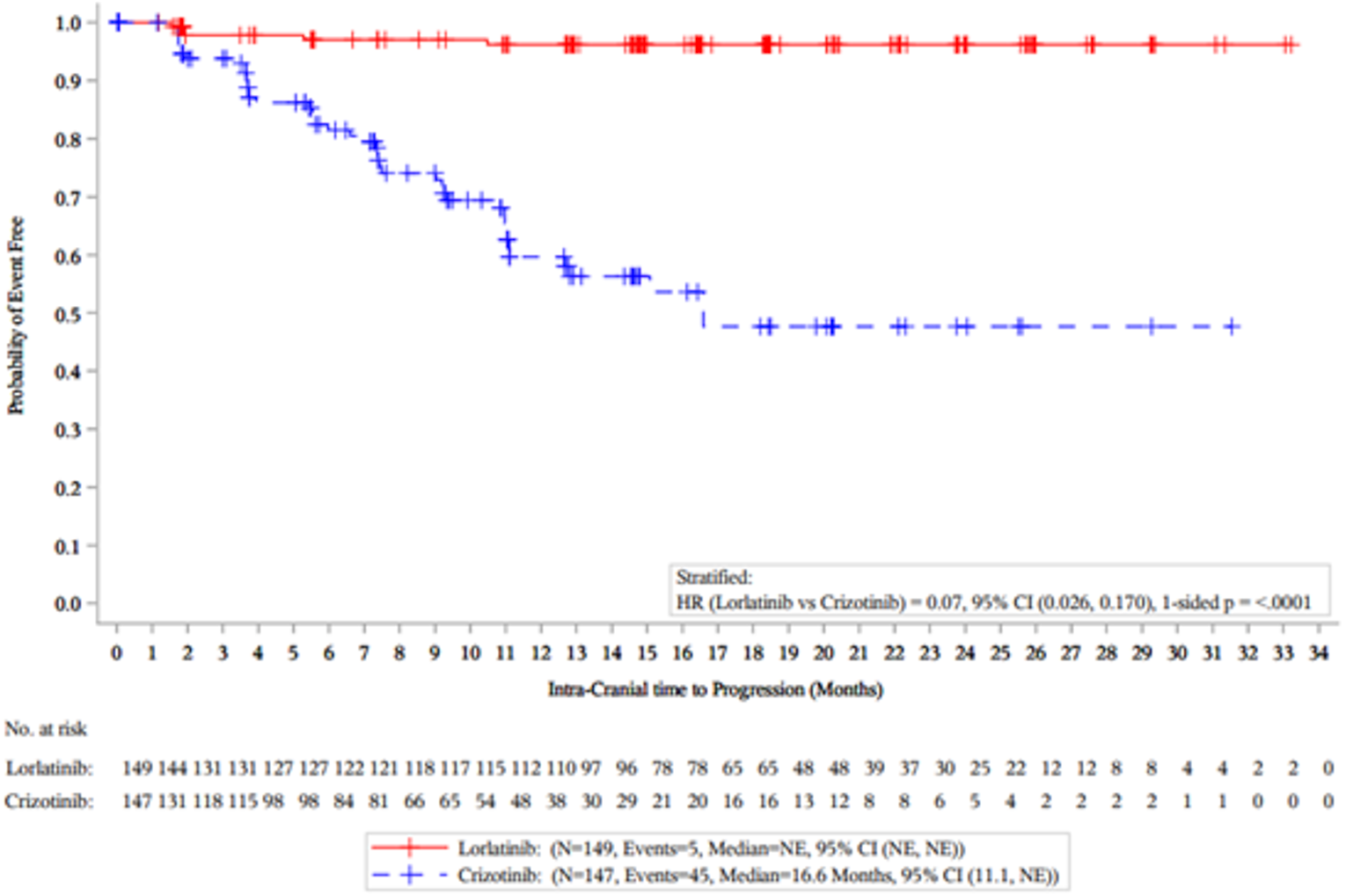
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; IC-TPP = intracranial time to progression; NE = not estimable; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: CROWN Clinical Study Report.17
Table 22: Summary IC-TTP Based on BICR Assessment (Modified RECIST 1.1) — Patients With Brain Metastases at Baseline in the Full Analysis Set
IC-TTP patients | Lorlatinib (N = 38) | Crizotinib (N = 40) |
|---|---|---|
Events, n (%) | 4 (10.5) | 26 (65.0) |
Median, months (95% CI)a | NE (NE to NE) | 7.3 (3.7 to 9.3) |
Stratified HR,b c (95% CI) | 0.08 (0.026 to 0.227) | |
1-sided P valued | < 0.0001e | |
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; IC-TPP = intracranial time to progression; NE = not estimable; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
aBased on Brookmeyer and Crowley method.
bStratified by ethnic origin (Asian or non-Asian) at randomization from interactive response technology stratification values.
cHazard ratio based on Cox proportional hazards model; under proportional hazards, an HR < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to crizotinib.
dP value was based on a stratified log-rank test.
eP value was not adjusted for multiplicity.
Source: CROWN Clinical Study Report.17

|||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| |
|---|---|---|
|||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||| |
Note: This table has been redacted at the sponsor’s request.
aBased on Brookmeyer and Crowley method.
bStratified by ethnic origin (Asian or non-Asian) at randomization from interactive response technology stratification values.
cHazard ratio based on a Cox proportional hazards model; under proportional hazards, a hazard ratio < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to Crizotinib.
dP value was based on a stratified log-rank test.
eP value was not adjusted for multiplicity.
Source: CROWN Clinical Study Report.17

Alumni Exploratory End Point: Probability of First Event Being a CNS Progression, Non-CNS Progression, or Death per BICR (RECIST 1.1 and Modified RECIST 1.1)
Time to CNS progression and time to development of CNS metastases were end points specified in the CADTH protocol as being of interest to patients and clinicians, but these end points were not reported in the CROWN trial. However, the CROWN trial did report results for the probability that a patient’s first event was a CNS progression, non-CNS progression, or death, and data on these end points were considered clinically important by the clinical experts consulted by CADTH. The probability of a first event being a CNS progression after adjusting for non-CNS progression and death was lower (i.e., favoured) in the lorlatinib group compared with the crizotinib group (HR = 0.06; 95% CI, 0.022 to 0.182). The probability of a first event being a non-CNS progression after adjusting for CNS progression or death was also lower in the lorlatinib group than in the crizotinib group (HR = 0.30; 95% CI, 0.185 to 0.474). There was no difference in the probability of a first event being death after adjusting for prior CNS or non-CNS progression between the treatment groups (Table 24).17
Table 24: Summary of Risk of CNS Progression by BICR (RECIST 1.1) — Full Analysis Set
Patients with event, n (%) | Lorlatinib N = 38 | Crizotinib N = 40 | Cause-specific stratifieda analysis, HRb (95% CI) | Log-rank 1-sided P valuec |
|---|---|---|---|---|
CNS progression without prior non-CNS progressive disease | 4 (2.7) | 35 (23.8) | 0.06 (0.022 to 0.182) | < 0.0001 |
Non-CNS progression without prior CNS progressive disease | 29 (19.5) | 54 (36.7) | 0.30 (0.185 to 0.474) | < 0.0001 |
Death without prior CNS or non-CNS progressive disease | 9 (6.0) | 4 (2.7) | 1.66 (0.501 to 5.500) | 0.7966 |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; HR = hazard ratio.
aStratified by presence of brain metastases (yes or no) and ethnic origin (Asian or non-Asian) at randomization from interactive response technology stratification values.
bHR based on a Cox proportional hazards model; under proportional hazards, an HR < 1 indicates a reduction in hazard rate in favour of lorlatinib compared to Crizotinib.
cP values were not adjusted for multiplicity.
Source: CROWN Clinical Study Report.17
Exploratory End Point: Intracranial ORR per BICR (Modified RECIST 1.1)
Patients With Any (Measurable or Nonmeasurable) Brain Metastases at Baseline
A total of 38 patients in the lorlatinib group and 40 patients in the crizotinib group had any measurable or nonmeasurable brain metastasis. Among these patients, the IC-ORR was numerically higher in the lorlatinib group (65.8%; 95% CI, 48.6 to 80.4) than in the crizotinib group (20.0%; 95% CI, 9.1 to 35.6) (Table 25). More patients in the lorlatinib group had an intracranial CR than patients in the crizotinib group (60.5% versus 15.0%, respectively).17
Table 25: Summary of IC-ORR Based on BICR (Modified RECIST 1.1) — Patients With Brain Metastases at Baseline in the Full Analysis Set
Response | Lorlatinib (N = 38) | Crizotinib (N = 40) |
|---|---|---|
IC-ORR, n (%) | 25 (65.8) | 8 (20.0) |
95% CIa | 48.6 to 80.4 | 9.1 to 35.6 |
Confirmed BOR, n (%) | ||
CR | 23 (60.5) | 6 (15.0) |
PR | 2 (5.3) | 2 (5.0) |
Stable disease | 1 (2.6) | 5 (12.5) |
Non-CR and/or non-PD | 10 (26.3) | 17 (42.5) |
Progressive disease | 2 (5.3) | 7 (17.5) |
Not evaluable | 0 | 3 (7.5) |
BICR = blinded independent central review; BOR = best overall response; CR = complete response; IC = intracranial; ORR = objective response rate; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
aClopper-Pearson method used.
Source: CROWN Clinical Study Report.17
Patients With at Least 1 Measurable Brain Metastasis at Baseline
A total of 17 patients in the lorlatinib group and 13 patients in the crizotinib groups had at least 1 measurable brain metastasis (Table 26). Among these patients, the IC-ORR was numerically higher in the lorlatinib group (82.4%; 95% CI, 56.6 to 96.2) than in the crizotinib group (23.1%; 95% CI, 5.0 to 53.8). The proportion of patients achieving an intracranial complete response (IC-CR) was higher in the lorlatinib group than the crizotinib group (70.6% versus 7.7%, respectively).17
Table 26: Summary of IC-ORR based on BICR (Modified RECIST 1.1) — Patients With at Least 1 Measurable Brain Metastasis in the Full Analysis Set
Response | Lorlatinib (N = 17) | Crizotinib (N = 13) |
|---|---|---|
IC-ORR, n (%) | 14 (82.4) | 3 (23.1) |
95% CIa | 56.6 to 96.2 | 5.0 to 53.8 |
Confirmed BOR, n (%) | ||
Complete response | 12 (70.6) | 1 (7.7) |
Partial response | 2 (11.8) | 2 (15.4) |
Stable disease | 1 (5.9) | 5 (38.5) |
Progressive disease | 2 (11.8) | 2 (15.4) |
Not evaluable | 0 | 3 (23.1) |
BICR = blinded independent central review; BOR = best overall response; CI = confidence interval; IC = intracranial; ORR = objective response rate; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
aClopper-Pearson method used.
Source: CROWN Clinical Study Report.17
Exploratory End Point: Intracranial DOR per BICR (Modified RECIST 1.1)
Among patients with any measurable or nonmeasurable brain metastases at baseline who had a confirmed CR or PR, the median IC-DOR was NE (95% CI, NE to NE) in the lorlatinib group and 9.4 months (95% CI, 6.0 to 11.1) in the crizotinib group (Table 27).17
Among patients with at least 1 measurable brain metastasis who had confirmed CR or PR, the median IC-DOR was NE (95% CI, NE to NE) in the lorlatinib group and 10.2 months (95% CI, 9.4 to 11.1) in the crizotinib group (Table 28).17
Table 27: Summary of IC-DOR Based on BICR Assessment (Modified RECIST 1.1) — Patients With Any Brain Metastases at Baseline and Confirmed CR or PR in the Full Analysis Set
IC-DOR | Lorlatinib (N = 25) | Crizotinib (N = 8) |
|---|---|---|
Event, n (%) | 3 (12.0) | 4 (50.0) |
Disease progression | 1 (4.0) | 2 (25.0) |
Death | 2 (8.0) | 2 (25.0) |
IC-DOR (months), median (95% CI) | NE (NE to NE) | 9.4 (6.0 to 11.1) |
IC-DOR (months), range | 1.9 to 31.4 | 3.5 to 11.1 |
Response duration ≥ 12 months, n (%) | 18 (72.0) | 0 |
BICR = blinded independent central review; CI = confidence interval; CR = complete response; DOR = duration of response; IC = intracranial; NE = not estimable; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: CROWN Clinical Study Report.17
Table 28: Summary of IC-DOR Based on BICR (Modified RECIST 1.1) — Patients With at Least 1 Measurable Brain Metastasis and Confirmed CR or PR in the Full Analysis Set
IC-DOR | Lorlatinib (N = 14) | Crizotinib (N = 3) |
|---|---|---|
Event, n (%) | 2 (14.3) | 2 (66.7) |
Disease progression | 0 | 1 (33.3) |
Death | 2 (14.3) | 1 (33.3) |
IC-DOR (months), median (95% CI) | NE (NE to NE) | 10.2 (9.4 to 11.1) |
IC-DOR (months), range | 3.9 to 31.4 | 5.4 to 11.1 |
Response duration ≥ 12 months, n (%) | 11 (78.6) | 0 |
BICR = blinded independent central review; CI = confidence interval; CR = complete response; DOR = duration of response; IC = intracranial; NE = not estimable; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: CROWN Clinical Study Report.17
Exploratory End Point: Intracranial TTR per BICR (Modified RECIST 1.1)
Among patients with any baseline brain metastasis who had a confirmed CR or PR, the mean IC-TTR was numerically longer in the lorlatinib group at 3.04 months (SD = 2.800) than in the crizotinib group at 2.21 months (SD = 0.844). Among patients with at least 1 measurable brain metastasis at baseline, the mean IC-TTR was numerically longer in the lorlatinib group at 2.39 months (SD = 0.886) compared to the crizotinib group at 1.86 months (SD = 0.083) (Table 29).17
Table 29: Summary of IC-TTR Based on BICR (Modified RECIST 1.1) — Full Analysis Set
Time to tumour response (months) | Lorlatinib (N = 25) | Crizotinib (N = 8) |
|---|---|---|
Patients with any brain metastases at baseline and confirmed CR or PR, mean (SD) | 3.04 (2.80) | 2.21 (0.84) |
Patients with at least 1 measurable brain metastasis and confirmed CR or PR, mean (SD) | 2.39 (0.89) | 1.86 (0.08) |
BICR = blinded independent central review; CR = complete response; IC-TTR = intracranial time to response; PR = partial response; SD = standard deviation; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; SD = standard deviation.
Source: CROWN Clinical Study Report.17
Patient-Reported Outcomes
Data for PROs are presented in this report for the first 18 cycles of treatment because the number of patients completing PRO assessments in each treatment group was smaller during later treatment cycles (≤ 20%). Patient attrition was due primarily to patients experiencing disease progression. Due to the small sample sizes in each treatment group at later cycles, the sponsor expressed concern regarding the interpretability of the data.17
Completion Rates
More than 90% of patients completed at least 1 question of the EORTC QLQ-C30 and QLQ-LC13 questionnaires at each assessment time point. More than 88% of patients completed the entire questionnaire (all questions answered) until the data cut-off date. After cycle 19, less than 50% of patients were eligible for completion of the questionnaires in the lorlatinib group, resulting in small sample sizes; in the crizotinib group, less than 50% of the sample were eligible for completion of the questionnaires after cycle 11. Compliance in the EQ-5D-5L questionnaire was also high, with more than 90% of patients completing at least 1 question of the or the entire questionnaire until cycle 38. In the lorlatinib group, less than 50% of patients were eligible for completion of the survey after cycle 19. In the crizotinib group, less than 50% of patients were eligible for completion of the survey after cycle 11.17
EORTC QLQ-C30 Functional and Symptoms Scales
At baseline, the mean scores for the global quality-of-life scale were 64.6 (SE ± 1.82) in the lorlatinib group and 59.8 (SE ± 1.90) in the crizotinib group. Numerically, there was a greater overall improvement in global quality of life from baseline up until the data cut-off date; the estimated mean global quality-of-life score was 70.79 (95% CI, 63.57 to 78.01) in the lorlatinib group and 66.79 (95% CI, 60.36 to 73.22) in the crizotinib group; and the estimated mean difference between the lorlatinib and crizotinib groups was 4.65 (95% CI, 1.14 to 8.16; P = 0.0096) (Figure 10). This between-group difference did not meet the pre-specified threshold for the MID of at least 10 points. A similar proportion of patients in the lorlatinib and crizotinib groups achieved an improvement of 10 points or more (41.8% versus 42.6%, respectively) or a stable score (39.7% versus 38.1%, respectively) in the global quality-of-life subscale.
The mean changes from baseline scores were numerically higher in the lorlatinib group compared to the crizotinib group for the QLQ-C30 functioning subscales (physical functioning, role functioning, emotional functioning, social functioning), except for the cognitive functioning scale, for which the change from baseline scores were numerically higher in the crizotinib group over the lorlatinib group.17 For the symptoms sales (fatigue, pain, nausea and vomiting, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), the mean changes from baseline scores were numerically lower in the lorlatinib group for the fatigue, nausea and vomiting, insomnia, appetite loss, constipation, diarrhea, and financial difficulties subscales, except for the pain and dyspnea subscales, which were numerically higher in the lorlatinib group compared to the crizotinib group. For all functioning and symptom domain subscales of the EORTC QLQ-C30, none of the between-group differences met the MID (≥ 10 points) threshold.17
Figure 10: Plot of Mean Change From Baseline (± SE) Over Time for EORTC QLQ-C30
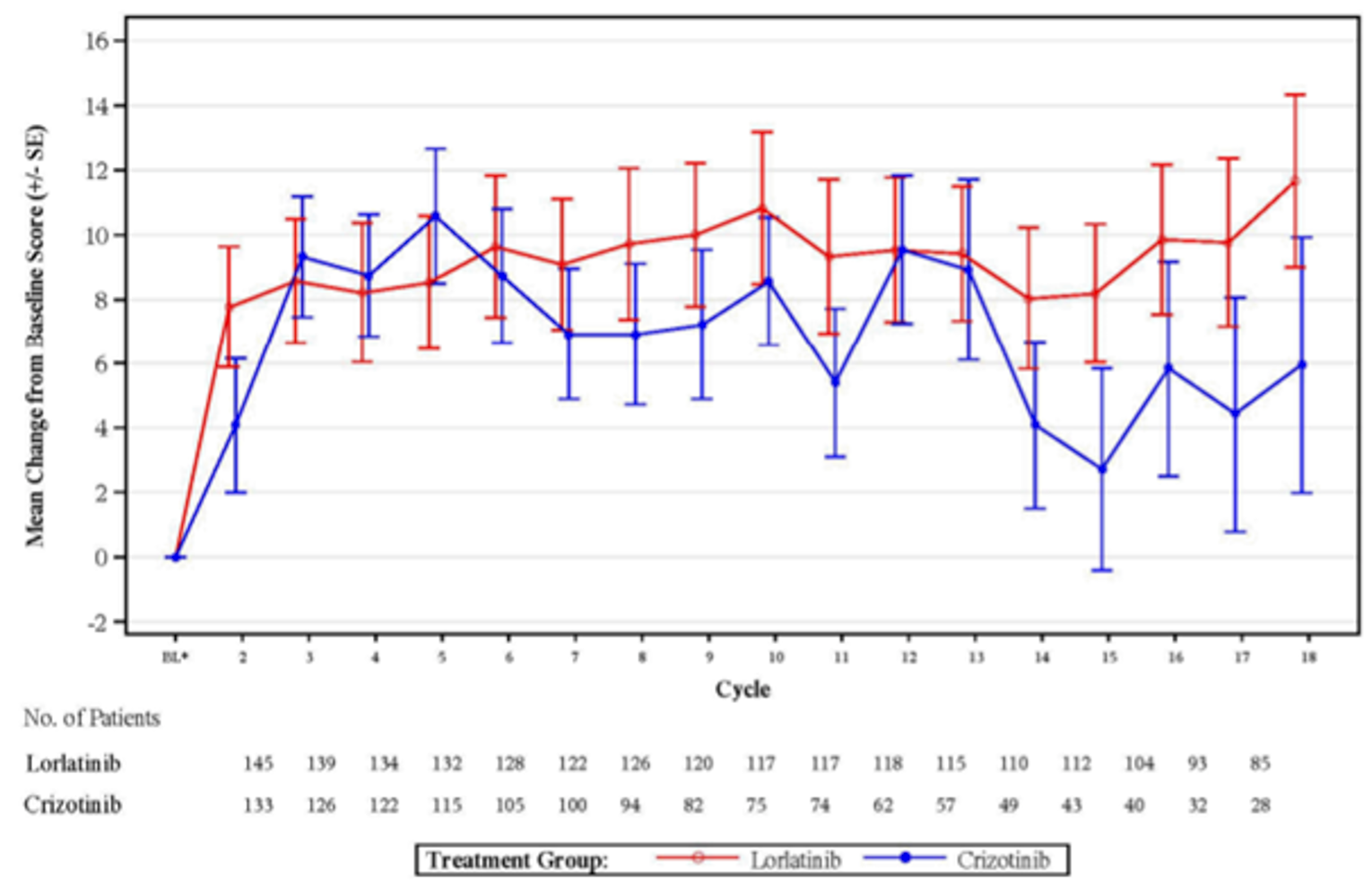
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SE = standard error.
Note: Baseline was defined as the last assessment performed on or before date of the first dose of study treatment. Based on EORTC QLQ-C30 PRO analysis set within each treatment group. Mean change from baseline is shown through cycle 18 to correspond with the median follow-up time
Source: CROWN Clinical Study Report.17
EORTC QLQ-LC13 Symptom Scales and Time to Deterioration
Time to deterioration in EORTC QLQ-LC13 symptom scales was evaluated for individual symptoms, including pain in the chest, dyspnea, and cough, and as a composite end point of these 3 symptoms. Pain in the chest, dyspnea, and cough were chosen as they are commonly reported disease-related symptoms experienced by patients with lung cancer. The mean scores for pain in the chest, dyspnea, and cough at baseline were similar between the lorlatinib and crizotinib groups. The TTD in the composite end point of lung cancer symptoms (cough, dyspnea, or pain in the chest) was not different between the 2 treatment groups; the median TTD was 3.3 months (95 CI, 2.1 to 4.7) in the lorlatinib group and 3.7 months (95% CI, 0.211 to 0.382) in the crizotinib group (HR = 1.09, 95% CI, 0.822 to 1.444; 1-sided P value = 0.7293) (Figure 11).17 Similarly, the TTD in individual symptoms was not different between the 2 treatment groups for the pain in the chest, dyspnea, and cough scales.17
Figure 11: Kaplan-Meier Plot of Time to Deterioration in Composite of Pain in the Chest, Dyspnea, and Cough
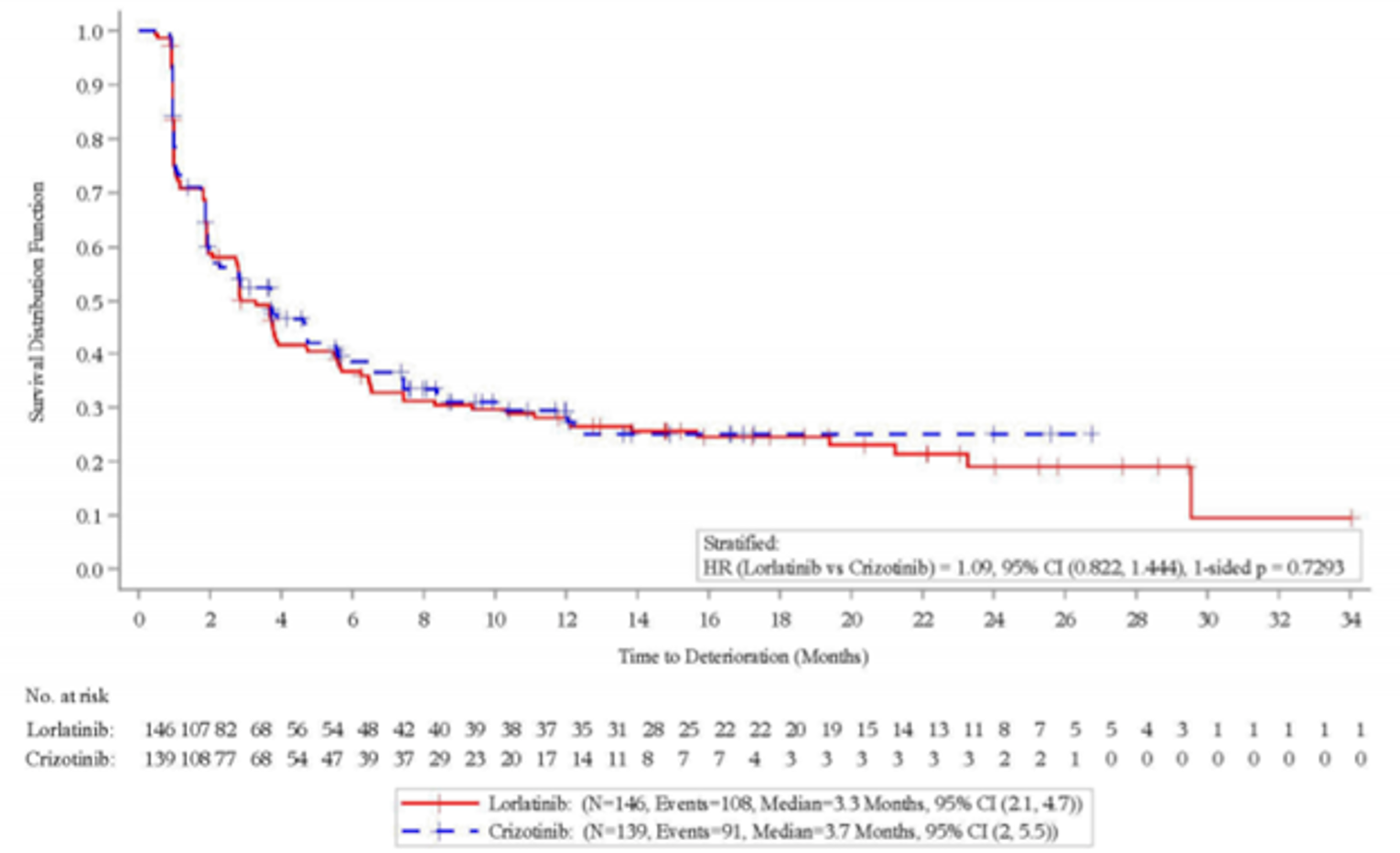
CI = confidence interval; HR = hazard ratio.
Source: CROWN Clinical Study Report.17
EQ-5D VAS and Index Values
The mean scores of patients in the lorlatinib and crizotinib groups |||||||||||| for the EQ-5D-5L and EQ VAS scores (|||||||||||||||||||||||||||||||||) and index values (mean = |||||||||||||||| versus ||||||||||||||||) at baseline and throughout the trial until cycle 38. The proportion of patients reporting slight, moderate, severe, or extreme problems in the functional dimensions of the questionnaire (mobility, self-care, usual activities, pain or discomfort, anxiety or depression) was ||| in both treatment groups at baseline; the proportion of patients reporting slight, moderate, severe, or extreme problems |||||||||||||||||||||||||| in later cycles from baseline.17
Harms
Only those harms identified in the CADTH review protocol are reported below. A summary of harms data is provided in Table 30. Further details regarding AEs are provided in the text that follows.
Table 30: Summary of All Adverse Events — Safety Analysis Set
Adverse events | Lorlatinib | Crizotinib |
|---|---|---|
Patients evaluable for AEs, n | 149 | 142 |
Number of AEs, n | 2,023 | 1,729 |
Patients with AEs, n (%) | 149 (100.0) | 140 (98.6) |
Patients with SAEs, n (%) | 51 (34.2) | 39 (27.5) |
Patients with maximum grade 3 or 4 AEs, n (%) | 108 (72.5) | 79 (55.6) |
Patients with maximum grade 5 AEs, n (%) | 7 (4.7) | 7 (4.9) |
Patients discontinued from study due to AEs,a n (%) | 7 (4.7) | 8 (5.6) |
Patients discontinued study treatment due to AEs,b n (%) | 10 (6.7) | 13 (9.2) |
Patients with dose reduced or temporary discontinuation due to AEs, n (%) | 79 (53.0) | 71 (50.0) |
AE = adverse event; SAE = serious adverse event.
Note: Included data from the first dose of study treatment through end of study follow-up (infinite lag) or start of new anticancer therapy, whichever occurred first. Except for the number of AEs, patients were counted only once per treatment in each row. Serious adverse events determined defined according to the investigator's assessment using the Medical Dictionary for Regulatory Activities, version 23.0 coding.
aPatients who had an AE record that caused study discontinuation.
bPatients who had an AE record that caused treatment discontinuation.
Source: CROWN Clinical Study Report.17
Adverse Events
All patients in the lorlatinib group (100%) and almost all patients in the crizotinib group (98.6%) experienced an AE, most of which were grade 1 or 2. The most common AEs in the lorlatinib group were hypercholesterolemia (70.5%), hypertriglyceridemia (63.8%), edema (55.0%), increased weight (38.3%), peripheral neuropathy (33.6%), cognitive effects and diarrhea (21.5% each), and dyspnea (20.1%); all these AEs occurred more frequently in the lorlatinib group, except for diarrhea, which was more common in the crizotinib group. The most common AEs in the crizotinib group were nausea (52.1%), diarrhea (52.1%), edema (39.4%), vision disorder (39.4%), vomiting (38.7%), increased ALT (33.8%), constipation (29.6%), increased AST (27.5%), and decreased appetite (24.6%); all these AEs occurred more frequently in the crizotinib group, except for edema, which occurred more frequently in the lorlatinib group.17
Approximately three-quarters of the AEs in the lorlatinib group were grade 3 or 4 (72.5%) compared to just over half of AEs in the crizotinib group (55.7%). The grade 3 or 4 AEs that occurred more frequently in the lorlatinib group were increased weight (16.8%), hypercholesterolemia (15.4%), and hypertriglyceridemia (12.8%). The most common grade 3 AEs in the crizotinib group included neutropenia (8.5%), increased gamma-glutamyl transferase, decreased neutrophil count, hypoalbuminemia (4.2% each), increased ALT, increased AST, increased blood creatine phosphokinase, and increased lipase (3.5% each). Neutropenia was the only grade 3 event to occur more frequently in the crizotinib group than in the lorlatinib group (8.5% versus 0.7%, respectively). Grade 4 AEs were generally infrequent in both treatment groups; hypertriglyceridemia (7.4%) was the most common grade 4 AE in the lorlatinib group, and decreased neutrophil count (2.8%) was the most common grade 4 event in the crizotinib group (Table 31).
Table 31: Summary of Any-Cause Adverse Events of Any Grade — Safety Analysis Set
Adverse events | Lorlatinib (N = 149) | Crizotinib (N = 142) | ||||
|---|---|---|---|---|---|---|
Any-grade AE | Grade 3 AE | Grade 4 AE | Any-grade AE | Grade 3 AE | Grade 4 AE | |
Any AE, n (%) | 149 (100.0) | 87 (58.4) | 21 (14.1) | 140 (98.6) | 67 (47.2) | 12 (8.5) |
Most common events,a n (%) | ||||||
Hypercholesterolemia | 105 (70.5) | 23 (15.4) | 1 (0.7) | 5 (3.5) | 0 | 0 |
Hypertriglyceridemia | 95 (63.8) | 19 (12.8) | 11 (7.4) | 8 (5.6) | 0 | 0 |
Edema | 82 (55.0) | 6 (4.0) | 0 | 56 (39.4) | 2 (1.4) | 0 |
Weight increase | 57 (38.3) | 25 (16.8) | 0 | 18 (12.7) | 3 (2.1) | 0 |
Peripheral neuropathy | 50 (33.6) | 3 (2.0) | 0 | 21 (14.8) | 1 (0.7) | 0 |
Cognitive effects | 32 (21.5) | 3 (2.0) | 0 | 8 (5.6) | 0 | 0 |
Diarrhea | 32 (21.5) | 2 (1.3) | 0 | 74 (52.1) | 1 (0.7) | 0 |
Dyspnea | 30 (20.1) | 4 (2.7) | 0 | 23 (16.2) | 3 (2.1) | 0 |
Anemia | 29 (19.5) | 4 (2.7) | 0 | 11 (7.7) | 4 (2.8) | 0 |
Fatigue | 29 (19.5) | 2 (1.3) | 0 | 46 (32.4) | 4 (2.8) | 0 |
Arthralgia | 28 (18.8) | 1 (0.7) | 0 | 16 (11.3) | 0 | 0 |
Hypertension | 27 (18.1) | 15 (10.1) | 0 | 3 (2.1) | 0 | 0 |
Vision disorder | 27 (18.1) | 0 | 0 | 56 (39.4) | 1 (0.7) | 0 |
Alanine aminotransferase increase | 26 (17.4) | 4 (2.7) | 0 | 48 (33.8) | 5 (3.5) | 1 (0.7) |
Constipation | 26 (17.4) | 0 | 0 | 42 (29.6) | 1 (0.7) | 0 |
Pain in extremity | 26 (17.4) | 0 | 0 | 12 (8.5) | 0 | 0 |
Headache | 25 (16.8) | 0 | 0 | 25 (17.6) | 1 (0.7) | 0 |
Pyrexia | 25 (16.8) | 1 (0.7) | 1 (0.7) | 18 (12.7) | 2 (1.4) | 0 |
Cough | 24 (16.1) | 0 | 0 | 26 (18.3) | 0 | 0 |
Mood effects | 24 (16.1) | 2 (1.3) | 0 | 7 (4.9) | 0 | 0 |
Back pain | 22 (14.8) | 1 (0.7) | 0 | 16 (11.3) | 0 | 0 |
Gamma-glutamyl transferase increase | 22 (14.8) | 8 (5.4) | 1 (0.7) | 22 (15.5) | 6 (4.2) | 0 |
Nausea | 22 (14.8) | 1 (0.7) | 0 | 74 (52.1) | 3 (2.1) | 0 |
Aspartate aminotransferase increase | 21 (14.1) | 3 (2.0) | 0 | 39 (27.5) | 5 (3.5) | 0 |
Vomiting | 19 (12.8) | 1 (0.7) | 0 | 55 (38.7) | 2 (1.4) | 0 |
Sleep effects | 17 (11.4) | 1 (0.7) | 1 (0.7) | 14 (9.9) | 0 | 0 |
Upper respiratory tract infection | 17 (11.4) | 1 (0.7) | 0 | 11 (7.7) | 2 (1.4) | 0 |
Blood creatine phosphokinase increase | 16 (10.7) | 2 (1.3) | 0 | 24 (16.9) | 5 (3.5) | 1 (0.7) |
Chest pain | 16 (10.7) | 2 (1.3) | 0 | 20 (14.1) | 1 (0.7) | 0 |
Dizziness | 16 (10.7) | 0 | 0 | 20 (14.1) | 0 | 0 |
Hyperlipidemia | 16 (10.7) | 2 (1.3) | 1 (0.7) | 0 | 0 | 0 |
Myalgia | 16 (10.7) | 0 | 0 | 5 (3.5) | 0 | 0 |
Hyperglycemia | 15 (10.1) | 5 (3.4) | 0 | 5 (3.5) | 0 | 0 |
Rash | 15 (10.1) | 0 | 0 | 11 (7.7) | 0 | 0 |
Lipase increase | 14 (9.4) | 3 (2.0) | 2 (1.3) | 17 (12.0) | 5 (3.5) | 1 (0.7) |
Amylase increase | 13 (8.7) | 0 | 0 | 16 (11.3) | 1 (0.7) | 0 |
Neutropenia | 10 (6.7) | 1 (0.7) | 0 | 21 (14.8) | 12 (8.5) | 0 |
Blood creatinine increase | 9 (6.0) | 2 (1.3) | 0 | 19 (13.4) | 3 (2.1) | 0 |
Dysgeusia | 8 (5.4) | 0 | 0 | 23 (16.2) | 0 | 0 |
Hypoalbuminemia | 8 (5.4) | 1 (0.7) | 0 | 18 (12.7) | 6 (4.2) | 0 |
Blood alkaline phosphatase increase | 7 (4.7) | 0 | 0 | 18 (12.7) | 2 (1.4) | 0 |
Decreased appetite | 5 (3.4) | 0 | 0 | 35 (24.6) | 4 (2.8) | 0 |
Sinus bradycardia | 4 (2.7) | 0 | 0 | 15 (10.6) | 0 | 0 |
Blood lactate dehydrogenase increase | 3 (2.0) | 1 (0.7) | 0 | 15 (10.6) | 0 | 0 |
Neutrophil count decrease | 3 (2.0) | 0 | 0 | 16 (11.3) | 6 (4.2) | 4 (2.8) |
Bradycardia | 2 (1.3) | 0 | 0 | 17 (12.0) | 0 | 0 |
AE = adverse event.
Note: Patients were only counted once per treatment per event. Included data from the first dose of study treatment through end of study follow-up (infinite lag) or start of new anticancer therapy, whichever occurred first. Decreasing order of frequency relative to lorlatinib any grade. With any AE row included all patients without cut-off. Medical Dictionary for Regulatory Activities version 23.0 coding applied.
aFrequency ≥ 10% in any treatment group.
Source: CROWN Clinical Study Report.17
Serious Adverse Events
In general, SAEs were more commonly reported in the lorlatinib group than in the crizotinib group (34.2% versus 27.5%, respectively) although the majority of SAEs occurred in 1 patient. The most common SAEs of any grade in the lorlatinib group were pneumonia (4.7%), dyspnea, respiratory failure (2.7% each), cognitive effects and pyrexia (2.0% each). In the crizotinib group, the most common SAEs of any grade were pneumonia (3.5%) and pyrexia (2.1%). Grade 3 or 4 SAEs occurred more frequently in the lorlatinib group than in the crizotinib group (22.8% versus 17.6%, respectively). The most common grade 3 SAEs in the lorlatinib group were dyspnea (2.7%) and respiratory failure (2.0%); and the most common grade 3 SAE in the crizotinib group was pneumonia (2.1%). All grade 4 SAEs occurred at a low frequency of less than 2% of patients.17
Table 32: Summary of Serious Adverse Events — Safety Analysis Set
Serious adverse events | Lorlatinib (N = 149) | Crizotinib (N = 142) | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 3 | Grade 4 | Any grade | Grade 3 | Grade 4 | |
Any serious adverse event, n (%) | 51 (34.2) | 28 (18.8) | 6 (4.0) | 39 (27.5) | 19 (13.4) | 6 (4.2) |
Most common events,a n (%) | ||||||
Pneumonia | 7 (4.7) | 2 (1.3) | 1 (0.7) | 5 (3.5) | 3 (2.1) | 1 (0.7) |
Dyspnea | 4 (2.7) | 4 (2.7) | 0 | 0 | 0 | 0 |
Respiratory failure | 4 (2.7) | 3 (2.0) | 0 | 0 | 0 | 0 |
Cognitive effects | 3 (2.0) | 1 (0.7) | 0 | 0 | 0 | 0 |
Pyrexia | 3 (2.0) | 0 | 1 (0.7) | 3 (2.1) | 2 (1.4) | 0 |
Note: Patients were only counted once per treatment per event. Included data from the first dose of study treatment through end of study follow-up (infinite lag) or start of new anticancer therapy, whichever occurred first. Decreasing order of frequency relative to lorlatinib any grade. With any adverse events row included all patients without cut-off. Medical Dictionary for Regulatory Activities version 23.0 coding applied.
aFrequency of 2% or more in any treatment group.
Source: CROWN Clinical Study Report.17
Dose Modifications
A summary of dose interruptions and modifications is provided in the Exposure to Study Treatments section of this report. Further details regarding AEs resulting in dose reductions and interruptions are provided in Table 33. Adverse events that resulted in dose reductions occurred in 31 patients (20.8%) in the lorlatinib group and 22 patients (15.5%) in the crizotinib group. The most commonly occurring AEs that resulted in a dose reduction in the lorlatinib group were edema (5.4%), hypertriglyceridemia (4.0%), and peripheral neuropathy (3.4%). The most commonly occurring AEs resulting in a dose reduction in the crizotinib group were edema and decreased neutrophil count (3.5% each). Peripheral neuropathy was the most common grade 3 AEs resulting in dose reductions in the lorlatinib group, occurring in 1.3% of patients; in the crizotinib group the most common grade 3 AE was decreased neutrophil count (2.1%). No grade 4 AEs resulted in dose reductions in either treatment group.17
Dose interruptions resulting from AEs occurred in a similar proportion of patients in the lorlatinib (49.0%) and crizotinib (47.2%) treatment groups, of which 32.9% and 36.6% were attributable to grade 3 or 4 AEs. The most common AEs of any grade that resulted in a dose interruption in the lorlatinib group included hypertriglyceridemia (7.4%) edema (5.4%), pneumonia (4.7%), and cognitive effects (4.0%). In the crizotinib group, the most common AEs of any grade resulting in dose interruption were due to decreased neutrophil count (7.0%), increased ALT (4.3%), and pneumonia (3.5). Grade 3 AEs resulting in dose interruption occurred in less than 3% of patients in the lorlatinib group, and the most common grade 4 AE was hypertriglyceridemia, which occurred in 5.4% of patients. In the crizotinib group, the grade 3 AEs that resulted in dose interruption were neutropenia (7.7%) and decreased neutrophil count decrease (4.2%). Grade 4 AEs resulted in a dose interruption in less than 3% of patients due to decreased neutrophil count (2.8%) and pneumonia (0.7%).17
Table 33: Summary of Adverse Events Resulting in Dose Reductions — Safety Analysis Set
Adverse events | Lorlatinib (N = 149) | Crizotinib (N = 142) | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 3 | Grade 4 | Any grade | Grade 3 | Grade 4 | |
Any adverse event, n (%) | 31 (20.8) | 9 (6.0) | 0 | 22 (15.5) | 7 (4.9) | 0 |
Most common event,a n (%) | ||||||
Edema | 8 (5.4) | 1 (0.7) | 0 | 5 (3.5) | 1 (0.7) | 0 |
Hypertriglyceridemia | 6 (4.0) | 0 | 0 | 0 | 0 | 0 |
Peripheral neuropathy | 5 (3.4) | 2 (1.3) | 0 | 0 | 0 | 0 |
Cognitive effects | 3 (2.0) | 1 (0.7) | 0 | 0 | 0 | 0 |
Hypercholesterolemia | 3 (2.0) | 0 | 0 | 0 | 0 | 0 |
Mood effects | 3 (2.0) | 0 | 0 | 0 | 0 | 0 |
Neutropenia | 0 | 0 | 0 | 3 (2.1) | 2 (1.4) | 0 |
Neutrophil count decrease | 0 | 0 | 0 | 5 (3.5) | 3 (2.1) | 0 |
Note: Patients were only counted once per treatment per event. Included data from the first dose of study treatment through end of study follow-up (infinite lag) or start of new anticancer therapy, whichever occurred first. Decreasing order of frequency relative to lorlatinib any grade. With any adverse event row included all patients without cut-off. Medical Dictionary for Regulatory Activities version 23.0 coding applied.
aFrequency ≥ 2% in any treatment group.
Source: CROWN Clinical Study Report.17
Table 34: Summary of Adverse Events Resulting in Dose Interruptions — Safety Analysis Set
Adverse events | Lorlatinib (N = 149) | Crizotinib (N = 142) | ||||
|---|---|---|---|---|---|---|
Any grade | Grade 3 | Grade 4 | Any grade | Grade 3 | Grade 4 | |
Any adverse event, n (%) | 73 (49.0) | 35 (23.5) | 14 (9.4) | 67 (47.2) | 42 (29.6) | 10 (7.0) |
Most common events,a n (%) | ||||||
Hypertriglyceridemia | 11 (7.4) | 2 (1.3) | 8 (5.4) | 0 | 0 | 0 |
Edema | 8 (5.4) | 4 (2.7) | 0 | 2 (1.4) | 1 (0.7) | 0 |
Pneumonia | 7 (4.7) | 1 (0.7) | 2 (1.3) | 5 (3.5) | 2 (1.4) | 1 (0.7) |
Cognitive effects | 6 (4.0) | 0 | 0 | 0 | 0 | 0 |
Hypercholesterolemia | 5 (3.4) | 4 (2.7) | 1 (0.7) | 0 | 0 | 0 |
Mood effects | 5 (3.4) | 1 (0.7) | 0 | 0 | 0 | 0 |
ALT increase | 4 (2.7) | 3 (2.0) | 0 | 6 (4.2) | 4 (2.8) | 0 |
Neutropenia | 1 (0.7) | 1 (0.7) | 0 | 11 (7.7) | 11 (7.7) | 0 |
Neutrophil count decrease | 0 | 0 | 0 | 10 (7.0) | 6 (4.2) | 4 (2.8) |
Note: Patients were only counted once per treatment per event. Included data from the first dose of study treatment through end of study follow-up (infinite lag) or start of new anticancer therapy, whichever occurred first. Decreasing order of frequency relative to lorlatinib any grade. With any adverse event row included all patients without cut-off. Medical Dictionary for Regulatory Activities version 23.0 coding applied.
aFrequency ≥ 3% in any treatment group.
Source: CROWN Clinical Study Report.17
Withdrawals Due to Adverse Events
Adverse events leading to permanent treatment discontinuation occurred in 10 patients (6.7%) in the lorlatinib group and 13 patients (9.2%) in the crizotinib group. Grade 3 AEs resulting in permanent treatment discontinuation occurred in 6 patients (4.0%) and 7 patients (4.9%) in the lorlatinib and crizotinib groups, respectively. Grade 4 AEs resulting in permanence discontinuation from study treatment occurred in 2 patients (1.3%) in the lorlatinib group and 1 patient (0.7%) in the crizotinib group. The most common AE that resulted in permanent discontinuation of lorlatinib was cognitive effects (N = 2; 1.3%). The most common AEs resulting in permanent discontinuation of crizotinib were pleural effusion (N = 3; 2.1%) and pneumonitis (N = 2; 1.4%).17
Mortality
Deaths occurred in similar proportions of patients in the lorlatinib and crizotinib groups: 23 patients (15.4%) and 18 patients (19.7%), respectively. Most deaths were attributed to disease progression, which occurred in 17 patients (11.4%) in the lorlatinib group and 23 patients (16.2%) in the crizotinib group. Two deaths in the lorlatinib group were considered by the investigator to be treatment-related; both of these patients had a history of prior heart disease and diabetes. One patient died of cardiac failure approximately 2 months after receiving their last dose of lorlatinib, and the second patient died of respiratory failure in the context of infectious pneumonia.17 The cause of death of 3 patients, including 1 in the lorlatinib group and 2 in the crizotinib group, was categorized as unknown. The cause of 2 deaths, including 1 patient in each treatment group, were categorized as other; 1 of these patients experienced worsening of decompensatio cordis, and the other patient experienced sepsis.
Three deaths in the lorlatinib group were related to SAEs, but they were not considered by the sponsor in the overall count of grade 5 AEs as they occurred after the patients began new anticancer therapies.17
Notable Harms
A list of AEs of special interest in the CROWN trial are reported in Table 35. The AEs of special interest in the CROWN trial aligned with notable harms listed in the CADTH systematic review protocol. In general, these AEs were more common in the lorlatinib group, except for vision disorder and increased liver function test, which were more common in the crizotinib group than in the lorlatinib group (39.4% versus 18.1% and 37.3% versus 20.8%, respectively). The most common AEs of special interest were hypercholesterolemia (70.5% in the lorlatinib group versus 3.5% in the crizotinib group), hypertriglyceridemia (63.8% versus 5.6%, respectively), edema (55.0% versus 39.4%, respectively), weight gain (38.3% versus 12.7%, respectively), peripheral neuropathy (33.6% versus 14.8%, respectively), cognitive effects (21.5% versus 5.6%, respectively), increased liver function test (20.8% versus 37.3%), and mood effects 16.1% versus 4.9%).17
Table 35: Adverse Events of Special Interest in the CROWN Trial
Adverse event | Any grade AE, n (%) | |
|---|---|---|
Lorlatinib (N = 149) | Crizotinib (N = 142) | |
Hypercholesterolemia | 105 (70.5) | 5 (3.5) |
Hypertriglyceridemia | 95 (63.8) | 8 (5.6) |
Edema | 82 (55.0) | 56 (39.4) |
Peripheral neuropathy | 50 (33.6) | 21 (14.8) |
CNS effects | ||
Cognitive effects | 32 (21.5) | 8 (5.6) |
Mood effects | 24 (16.1) | 7 (4.9) |
Speech effects | 7 (4.7) | 0 |
Psychotic effects | 5 (3.4) | 0 |
Vision disorder | 27 (18.1) | 56 (39.4) |
Pneumonitis | 2 (1.3) | 4 (2.8) |
Weight gain | 57 (38.3) | 18 (12.7) |
Liver function test increased | 31 (20.8) | 53 (37.3) |
QT prolongation | 5 (3.4) | 8 (5.6) |
Atrioventricular block | 4 (2.7) | 0 |
Pancreatitis | 23 (15.4) | 26 (18.3) |
CNS = central nervous system.
Source: CROWN Clinical Study Report.17
Critical Appraisal
Internal Validity
The CROWN trial was a multinational, multi-centre, open-label, group sequential superiority trial. Open-label trials by design are associated with biases that may affect patient outcomes and reporting, and favour investigational products over standard of care, as patients and investigators are aware of the assigned treatment of patients. However, the choice of an open-label design was considered appropriate given that crizotinib has been a standard treatment for patients with metastatic ALK-positive NSCLC, and clinicians are likely knowledgeable of toxicity profiles. The primary end point of the CROWN trial, PFS, may have been affected by bias from an open-label trial design. However, BICR was implemented for the assessment of PFS, as well as other end points that involved judgment of patient clinical progression (i.e., ORR and DOR), which mitigated the potential for bias introduced through the trial design. The risk of bias from an open-label design is likely to be of greater concern for subjective end points, such as HRQoL and safety, as the knowledge of treatment assignment from patients and investigators could have influenced the reporting and assessment of these outcomes.
Patients were randomized to the CROWN trial in a 1:1 ratio using an interactive web-based response technology system. Randomization was stratified by the presence of brain metastases and ethnic origin.17 This method of randomization was considered to result in a low risk of bias, as relatively equal proportions of patients were randomly assigned to receive either lorlatinib or crizotinib. The clinical experts consulted by CADTH indicated that presence of brain metastases is a particularly important factor for consideration in this patient population, and was accounted for in the randomization scheme to avoid an imbalance of this disease characteristic between the treatment groups. Overall, baseline demographic and clinical characteristics of patients were well balanced across the groups, with some exceptions (age and smoking status). The clinical experts suggested that it is unlikely that these slight imbalances affected patient outcomes.
The primary and secondary end points of the CROWN trial were PFS and OS. Both end points were considered in power calculations, and OS was tested hierarchically at the time of the data cut-off depending on the statistical significance of PFS. Other secondary and exploratory end points were not included in the statistical hierarchy. The statistically significant findings on subgroup analyses, such as in patients with brain metastasis were likely subject to multiplicity and inflated type I error rate. At the data cut-off date, the interim analysis for PFS had crossed the pre-specified efficacy boundary and demonstrated a statistically significant difference in favour of lorlatinib in prolonged PFS, and the analysis was therefore considered final by the sponsor. However, OS data were deemed immature, as only 26% of the 198 OS events required for the final analysis of OS had occurred.17 However, improvements in PFS may not always correlate to a difference in OS in the assessment of oncology treatment benefit. In fact, mainly due to disease progression, a higher proportion of patients in the crizotinib group than in the lorlatinib group (17.4% versus 58.5%, respectively) withdrew from the study. This would largely bias the estimate of OS in the final analysis. Further evidence is therefore required to confirm the superiority of lorlatinib over crizotinib in treatment efficacy with respect to OS. The next analysis for OS, occurring once 70% of events have occurred, was projected to occur in early 2025, assuming that the number of OS events expected to occur for this analysis happen by the end of 2024.33
At the data cut-off date, |||||||||||||| in the crizotinib group compared with the lorlatinib group had received a subsequent systemic anticancer therapy. There were disproportional differences in the frequency and type of subsequent systemic anticancer therapies administered to patients. For example, while an ALK TKI was the |||||||||||||||| administered subsequent therapy received by patients in both the lorlatinib and crizotinib groups (||||||||||||||||||||||||||||||||||||||||||), |||||||||||||| in the lorlatinib group received subsequent treatment with chemotherapy with or without an anti-angiogenic therapy compared with patients in the crizotinib group (||||||||||||||||||||||||||||||||||||||||).33 These differences in subsequent therapies are expected to introduce bias into the efficacy analyses of OS and other patient outcomes. However, the direction and extent of this bias is difficult to predict.
Treatment crossover was not permitted within the CROWN trial. However, at the data cut-off date, |||||||||||||| in the lorlatinib group discontinued treatment and received crizotinib as a first subsequent therapy and |||||||||||||||| received crizotinib as a second subsequent therapy; |||||||||||||||| discontinued in the crizotinib group and received lorlatinib as a first subsequent therapy, |||||||||||| received lorlatinib as a second subsequent therapy, and |||||||||||||| received it as a third subsequent therapy.17,33 Treatment crossover may introduce bias into efficacy analyses as effects of previous treatment may carry over into the next line of therapy. However, as there were |||||||||||||| in both treatment groups who received subsequent treatment with the assigned therapy of the opposite treatment group, it is unlikely that biases related to crossover affected efficacy results of the trial.
Most patients in each treatment group received concomitant medications (96.6% in the lorlatinib group versus 95.1% in the crizotinib group). although the frequencies of some types of concomitant medications received by patients varied across treatment groups. The clinical experts consulted by CADTH for this review indicated that the differences in concomitant medications may be indicative of real-world practices. For example, the greater use of statins in the lorlatinib group than in the crizotinib group may be indicative of AEs related to cholesterol in the lorlatinib group. While differences in the types of concomitant medications were observed between the lorlatinib and crizotinib groups, these differences were considered unlikely to affect efficacy outcomes.
Statistical analyses of OS and PFS were conducted using Cox proportional hazards models, which rely on the assumption of proportional hazards in both treatment groups. The sponsor assessed proportional hazards for PFS by performing tests for statistical significance using log(-log(Survival)) plots and a plot of Schoenfeld residuals from stratified Cox proportional regression models. However, the sponsor did not conduct a formal assessment of the proportional hazards assumption and did not provide a conclusion regarding its violation. Based on the plots provided, it is possible that there was a potential for violation of the assumption for the analysis of PFS. An analysis of proportional hazards for OS was not reported, and it is not known whether the analysis of OS violated the proportional hazards assumption; the data for OS were immature.
In general, due to patients continuing in the trial, the analyses of efficacy end points involved censoring of many patients. While data for the primary end point, PFS, was considered mature, large amounts of censoring may indicate that longer-term data are required to capture the true benefit of lorlatinib compared to crizotinib. Particularly, longer-term data would benefit analyses of OS as the median had not been reached in either treatment group. Results of exploratory end points (i.e., PFS according to investigator assessment, ORR, DOR, and IC-TTP) at the data cut-off date favoured treatment with lorlatinib over crizotinib; however, as the trial was not powered to formally test these outcomes, the obtained results should be considered as supportive evidence only.
Data on HRQoL were captured using the EORTC QLQ-C30, EORTC QLQ-LC13, and EQ-5D-5L. The EORTC QLQ-C30 had demonstrated adequate reliability and validity among lung cancer patients. The EORTC QLQ-LC13 is a lung cancer–specific module that may better reflect the changes in HRQoL among patients with lung cancer compared to general HRQoL questionnaires. The EQ-5D-5L is a generic tool used to measure HRQoL of patients across many diseases; the validity and reliability of this tool has been demonstrated across many patient populations. It uncertain whether the EQ-5D-5L is best equipped to capture the impacts of treatment and disease on lung cancer patients, especially among a subgroup of ALK-positive advanced or metastatic patients who are likely to develop brain metastases. The development of brain metastases may affect their HRQoL differently than it would patients for whom the likelihood of developing such metastases and associated side effects is lower. In particular, the EORTC QLQ-C30, EORTC QLQ-LC13, and EQ-5D-5L showed a lack of reliability regarding assessment of cognitive function (Appendix 3). It is possible that the HRQoL instruments used in the CROWN trial may not have adequately captured the impact of patient disease and treatment specifically related to cognitive function.
A summary of dose exposure showed that patients in the lorlatinib group received treatment for a longer mean period of time than patients in the crizotinib group. Consequently, the dose intensity and cumulative dose intensity were greater in patients treated with lorlatinib compared to those treated with crizotinib. These differences in exposure of treatment between the treatment groups are likely to have resulted in improved treatment effects in the lorlatinib group. However, the longer exposure to treatment should also be considered when interpreting safety and HRQoL data, as longer exposure to treatment may influence toxicities and quality of life for patients.
External Validity
The CROWN trial compared lorlatinib to crizotinib for patients with ALK-positive metastatic NSCLC. Lorlatinib was administered at a dose of 100 mg orally once daily, while crizotinib was administered at a dose of 250 mg twice daily orally; these doses are in alignment with Health Canada–approved indications. At the time of the trial’s inception, crizotinib was considered the standard of care. However, newer-generation TKIs such as alectinib and brigatinib have demonstrated improved efficacy and ability to penetrate the blood-brain barrier. They have become the standards of care for patients in the first-line treatment setting of locally advanced and metastatic ALK-positive NSCLC and are therefore more relevant comparators against lorlatinib. The comparative efficacy and safety of these treatments is not known because they have not been directly compared in RCTs. As such, the sponsor provided an ITC that compared lorlatinib to these treatments. Three ITCs published in the literature that compared lorlatinib to other ALK TKIs were also identified by the CADTH team. The ITCs are summarized and critically appraised in the Indirect Evidence section.
The majority of patients in the CROWN trial had an ECOG PS score of 0 or 1. The generalizability of the efficacy results (i.e., improvement in PFS) to those patients with a poorer ECOG PS remains unknown. Moreover, the study excluded patients with potential vascular or cardiac diseases, or patients with unfavourable lab testing on renal, liver, pancreatic, or bone marrow function. In reality, the safety profile of lorlatinib for patients with those comorbidities or abnormal testing may be even worse, particularly in the event that lorlatinib increased the risk of hypercholesterolemia and hypertriglyceridemia compared to crizotinib. The CROWN trial allowed for the enrolment of patients with brain metastases, who accounted for 25.5% of the lorlatinib group and 27.2% of the crizotinib group.17 Inclusion of patients with brain metastases is highly relevant as many patients with ALK-positive metastatic NSCLC develop brain metastases. Given the limitations of subgroup analysis results, intracranial-specific efficacy end points showed numerically improved patient outcomes in the lorlatinib group over the crizotinib group. The clinical experts consulted by CADTH recognized the results of the CROWN trial for patients with brain metastases.
In general, the baseline characteristics of patients in the CROWN trial were considered representative of patients typically treated in clinical practice. However, the clinical experts consulted by CADTH noted that ALK-positive NSCLC is more common in younger patients with a history of light smoking or no smoking history. In the CROWN trial, 36.9% of patients in the lorlatinib group and 29.3% of patients in the crizotinib group were reported to have been former smokers at baseline. While this is unlikely to have affected patient outcomes in the CROWN trial, the clinical experts suggested that the proportions of patients captured as former smokers may be lower in clinical practice. The clinical experts noted that the eligibility criteria for RCTs are typically more restrictive and may not capture the breadth of patients that clinicians see in clinical practice. It is unclear whether the treatment effects of lorlatinib are generalizable to patients who were excluded from the CROWN trial.
The CROWN trial allowed for enrolment of patients with brain metastases, who accounted for 25.5% of the lorlatinib group and 27.2% the crizotinib group.17 The CROWN trial demonstrated improved PFS among all patients, including those with brain metastases. In addition, intracranial-specific efficacy end points (IC-ORR, IC-TTP, IC-DOR, and IC-TTR) showed numerically improved results suggestive of improved patient outcomes in the lorlatinib group over the crizotinib group. The clinical experts consulted by CADTH supported the results of the CROWN trial, which suggested improved efficacy with lorlatinib for patients with brain metastases.
In the CROWN trial, assessments of efficacy were conducted every 8 weeks while on treatment until disease progression. The clinical experts consulted by CADTH indicated that patients are typically assessed every 3 months for response in their first year of treatment, and imaging for brain metastases generally occur every 6 months. Assessments for efficacy were conducted more frequently in the CROWN trial, which may have allowed for greater detection of treatment response in patients. It is not expected that the frequency of assessments in the CROWN trial negatively affected patient outcomes; however, the assessments were likely conducted too frequently and are not reflective of clinical practice.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The CROWN trial compared lorlatinib to crizotinib for the first-line treatment of adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC. Crizotinib was considered the standard of care for patients with ALK-positive locally advanced or metastatic NSCLC; however, other treatments such as alectinib or brigatinib have been introduced for treatment of these patients and are also considered relevant comparators in the first-line treatment setting. This section summarizes and critically appraises the available indirect evidence comparing lorlatinib to other relevant treatments for ALK-positive advanced or metastatic NSCLC.
A supplemental search of the medical literature for publicly available ITCs was conducted by CADTH. A focused literature search for network meta-analyses (NMAs) dealing with non–small cell lung cancer was run in MEDLINE All (1946–) on July 21, 2021. No limits were applied to the search. Three published ITCs were identified in the CADTH literature search: Chuang et al. (2021),19 Wang et al. (2021),20 and Ando et al. (2021).21
The sponsor conducted a systematic literature review to identify relevant studies for its submitted ITC. A systematic literature review by BresMed was conducted on October 31, 2019. Details of the systematic literature review are included in Table 36. Inclusion criteria for the systematic literature review were stated to be subject to the “80% rule,” under which 80% of the patients in a study must have met the inclusion criteria of the systematic literature review. Studies were limited to patients treated in the first-line setting; and studies that included patients who were not treatment-naive were not considered unless there were subgroup analysis involving patients who were treatment-naive.18 A grey literature search was also conducted to identify conference proceedings for studies that were ongoing or completed but unpublished. The search for grey literature was restricted to the proceedings published between 2018 and 2019. In addition, the bibliographies of key systematic reviews and meta-analysis articles were screened by the sponsor to ensure all relevant clinical studies were captured.18
Ando et al. (2021)21 conducted a systematic literature review to identify relevant literature for their NMA. The systematic literature review conducted on May 6, 2021, used 4 databases to capture published reports from 1946 to date. In addition to the 4 databases, the search strategy used for PubMed was also used in the Embase, CENTRAL, and SCOPUS databases. The reference lists of retrieved studies were also checked for relevant studies and the corresponding authors of studies were contacted when sufficient information or data could not be retrieved from the literature. To avoid publication bias, a manual search for relevant articles was conducted to supplement studies found in the literature search. No details regarding restrictions on searches were provided.
Wang et al. (2021) conducted a literature search to identify publications for inclusion into their NMA. Publications were captured if they were published until January 2021. In addition to publications retrieved from the literature search, reference lists of selected studies were hand-searched. Although Wang et al. (2021) did not specify inclusion criteria related to study design, based on studies included in the NMA, the CADTH team assumed that results were limited to RCTs.
Chuang et al. (2021) conducted a comprehensive literature search to identify publications for inclusion into their NMA. All databases were searched from inception until December 12, 2020. Abstracts in the main oncology congresses databases, including the American Society of Clinical Oncology, the American Association for Cancer Research, the European Society for Medical Oncology, and the World Conference on Lung Cancer, were reviewed. Reference lists of studies were also searched to identify any additional relevant literature.
Description of Indirect Treatment Comparisons
A description of the study selection methods used to identify relevant studies in each of the ITCs are reported in Table 36. All ITCs included studies of adult patients with advanced or metastatic ALK-positive NSCLC who were treated in the first-line setting; however, some of these also included patients who had received previous treatment for metastatic disease with chemotherapy or a previous ALK inhibitor. In these studies, the proportion of patients who had received previous treatment was generally less than 20%. All the ITCs compared lorlatinib with alectinib, brigatinib, and crizotinib; other comparators included ceritinib, ensartinib, and chemotherapy. In the sponsor’s ITC,18 quality assessments were performed based on the recommendations of the National Institute for Health and Care Excellence (NICE). while the published ITCs19-21 conducted quality assessments using the Cochrane Collaboration risk of bias tool.
Table 36: Study Selection Criteria and Methods for ITCs
Selection criteria | Sponsor’s ITC | Wang et al. (2021) | Chuang et al. (2021) | Ando et al. (2021) |
|---|---|---|---|---|
Population | Adult patients Advanced or metastatic NSCLC Treatment-naive patients (first-line setting) | ALK inhibitor–naive or previously untreated (ALK inhibitor–naive and chemotherapy-naive) advanced NSCLC | Adult patients Advanced or metastatic ALK-positive NSCLC Treatment-naive | Adult patients (≥ 18 years) Histological or cytological confirmation of advanced or metastatic ALK-positive NSCLC At least 1 measurable lesion evaluated in accordance with the RECIST 1.1 criteria in solid tumours ECOG PS 0 to 2 No previous exposure to ALK-targeted therapy |
Intervention | Lorlatinib/PF-06463922 Crizotinib/PF-02341066 Ceritinib/LDK378 Alectinib Brigatinib/AP26113 Ensartinib/X-396 Belizatinib/TSR-011 ASP3026 X-376 CEP-28122 CEP-37440 Entrectinib/RXDX-101 Retaspimycin/IPI-504 Pemetrexed | Lorlatinib Alectinib Brigatinib Crizotinib | Crizotinib Ceritinib Alectinib Brigatinib Lorlatinib Entrectinib Ensartinib | Lorlatinib (100 mg daily orally) Brigatinib (180 mg once daily) Alectinib (300 mg or 600 mg twice daily orally) Ceritinib (750 mg daily orally) Crizotinib (250 mg twice daily orally) Platinum-based chemotherapy |
Comparator | Any interventions listed here | Any interventions listed here | Any interventions listed here | Any interventions listed here |
Outcome | Response – tumour and intracranial Survival – tumour and intracranial Blood-brain barrier penetration Intracranial time to progression Duration of response Time to tumour response Quality of life Tolerability Safety | PFS OS Response rates AEs | PFS OS ORR AEs | PFS OS ORR AEs (any grade and grade ≥ 3) SAEs (any grade and grade ≥ 3) Increased AST/ALT levels (any grade and grade ≥ 3) Nausea (any grade and grade ≥ 3) Diarrhea (any grade and grade ≥ 3) Pneumonitis (any grade and grade ≥ 3) |
Study design | RCTs irrespective of blinding status Non-RCTs (single-arm studies, prospective or retrospective cohort studies, long-term follow-up studies, systematic reviews, and meta-analyses of RCTs and non-RCTs) | Not reported | Phase II and III RCTs | Phase III parallel group RCTs |
Publication characteristics | No data limits for publication date or language of publication were imposed | Publications were limited by English language | No data limits for publication date or language of publication were imposed | No details provided |
Exclusion criteria | Population
Intervention
Comparators
Outcomes
Study design
| Studies were excluded if they did not report outcomes of interest | Exclusion criteria were not explicitly stated; although studies that did not fit the listed inclusion criteria were excluded | Exclusion criteria included studies that did not fit the inclusion criteria listed |
Databases searched | Electronic databases
Grey Literature | Cochrane Controlled Trial Register Embase MEDLINE Science Citation Index | Embase MEDLINE PubMed Embase Classic Cochrane Library Clinicaltrials.gov | PubMed Cochrane Library Embase SCOPUS |
Selection process | Two independent reviewers from BresMed screened titles and abstracts independently Uncertainty on screened studies was checked by a senior reviewer Studies were reviewed at full text by 2 independent reviewers from BresMed Uncertainty was checked and judged by an independent third reviewer | All potentially relevant articles were reviewed by 2 independent reviewers | 2 independent reviewers screened articles | 2 reviewers screened through studies independently |
Data extraction process | Data were extracted by a BresMed reviewer and checked independently by a second reviewers | Not reported | 2 independent reviewers performed data extraction A third reviewer was available to resolve discrepancies through discussion | Data were extracted independently by 2 reviewers A third reviewer was consulted to resolve discrepancies when necessary |
Quality assessment | RCTs were assessed for quality based on recommendations in the NICE sponsor’s submission template | Studies were assessed using methods described in the Cochrane Collaboration Handbook | RCTs were assessed for quality using the RoB tool recommended by the Cochrane Handbook for Systematic Reviews Interventions by 2 reviewers independently A third reviewer was available to resolve discrepancies through discussion | RCTs were assessed using the RoB2 recommended by the Cochrane Collaboration |
AE = adverse event; ALK = anaplastic lymphoma kinase; ALT = alanine transaminase; AST = aspartate transaminase; ITC = indirect treatment comparison; NICE = National Institute for Health and Care Excellence; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RoB = risk of bias; RoB2 = risk of bias tool 2; SAE = serious adverse event.
Source: Sponsor’s ITC,18 Ando et al. (2021),21 and Wang et al. (2021).20
Methods of Sponsor’s Indirect Treatment Comparison
Objectives
The aim of the sponsor’s submitted ITC was to compare the relative efficacy of lorlatinib with alternative treatments for patients with ALK-positive advanced or metastatic NSCLC in the first-line treatment setting.
Study Selection Methods
A literature search was conducted based on the criteria reported in Table 36. Studies were screened by title and abstract, and the full-text screen resulted in the inclusion of 50 articles that captured 8 RCTs, and 75 articles that captured 54 non-RCTs. The following 8 RCTs were retrieved from the systematic literature review and considered for inclusion into the sponsor’s ITC: ALEX, J-ALEX, ALESIA, ALTA-1L, ASCEND-4, ASCEND-8, PROFILE 1014, and PROFILE 1029. The CROWN trial was also considered for inclusion, as well as another study identified by the sponsor, the eXalt3 trial. The 54 non-RCTs were not considered for inclusion into the ITC due to their study design.
ITC Analysis Methods
Details of the methodology used for the sponsor’s ITC are provided in Table 37.
Table 37: Sponsor’s ITC Analysis Methods
Detail | Sponsor’s ITC |
|---|---|
ITC methods | NMAs were conducted using a Bayesian approach to capture the uncertainty in model parameters while preserving correlation between treatment effects. Relative treatment effects were estimated using the Markov chain Monte Carlo methods. Both fixed and random effects were fitted to the data. Models were compared for goodness of fit. |
Priors | Two prior distributions were used to assess the sensitivity of the results to the choice of prior distribution. The prior distributions were non-informative and in line with those specified in the NICE Decision Support Unit Technical Support Document 2 to allow the posterior distribution to be primarily driven by the data. |
Assessment of model fit | Clinical plausibility of the estimated relative treatment effects and goodness-of-fit statistics (i.e., DIC and total residual deviance) were compared to the number of unique data points. To determine whether samples within each chain were highly correlated, autocorrelation plots were used to assess autocorrelation. A suitable thinning interval was applied, if needed, to ensure the chain was mixing well and was representative of the posterior distribution. |
Assessment of consistency | An assessment of consistency was not possible for this NMA as there were no closed loops in any of the networks. |
Assessment of convergence | A burn-in of 50,000 iterations was used, assessed by running 3 chains using different starting values and checking convergence using the Brooks-Gelman-Rubin statistic and plots of posterior density. A further 50,000 iterations were generated after convergence was achieved to estimate treatment effects and credible intervals. |
Outcomes |
|
Sensitivity analyses | Sensitivity analyses were conducted that excluded studies enrolling exclusively Asian patients; the ALESIA, J-ALEX, ASCEND-8, and PROFILE 1029 trials enrolled exclusively Asian patients and were excluded from the sensitivity analysis; this sensitivity analysis was conducted for both OS and PFS. Some trials enrolled patients who were not treatment-naive; sensitivity analyses were conducted that excluded patients who had received prior therapy for metastatic disease; all trials had available PFS data for subgroups of patients who were treatment-naive except for the eXalt3 trial; for OS, all trials except the ALTA-1L and eXalt3 trial had available OS data for subgroups of patients who were treatment-naive; trials that did not report PFS or OS data for subgroups of patients who were treatment-naive were excluded from this analysis A sensitivity analysis was conducted to determine the effect of brain metastasis at baseline on PFS; all trials except for the ASCEND-8, PROFILE 1029, and eXalt3 trials reported data for patients with brain metastasis; ASCEND-8, PROFILE 1029, and eXalt3 trials were excluded from this analysis. |
Subgroup analysis | None conducted |
Methods for pairwise meta-analysis | Pairwise comparisons were represented using HRs and RRs with associated 95% credible intervals for each comparator |
AE = adverse event; HR = hazard ratio; IC = intracranial; ITC = indirect treatment comparison; NMA = network meta-analysis; NICE = National Institute for Health and Care Excellence; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RR = relative risk; TTP = time to progression.
Source: Sponsor’s ITC.18
Treatments
Treatments included in the studies of the ITC were lorlatinib, alectinib, brigatinib, ceritinib, crizotinib, ensartinib, and chemotherapy. Included single trials evaluated lorlatinib (CROWN), brigatinib (ALTA-1L), and ensartinib (eXalt3); these oral treatments were administered at 100 mg daily, 170 mg daily, and 225 mg daily, respectively. Three trials assessed alectinib (ALEX, J-ALEX, and ALESIA) at doses of 600 mg twice daily orally or 300 mg twice daily orally. Two trials provided information about ceritinib (ASCEND-4 and ASCEND-8) and assessed ceritinib at 3 doses: 750 mg twice daily, 600 mg twice daily, and 450 mg twice daily, all administered orally. Crizotinib was included in 8 trials (CROWN, ALEX, ALESIA, J-ALEX, ALTA-1L, PROFILE 1014, PROFILE 1029, and eXalt3), all of which assessed crizotinib at 250 mg twice daily orally. Chemotherapy regimens were included in 3 trials (PROFILE 1014, PROFILE 1029 and ASCEND-4), which assessed the same regimen of pemetrexed (500 mg/m2) in combination with carboplatin (area under the curve of 5 mg/min/mL or 6 mg/min/mL) or cisplatin (75 mg/m2) administered intravenously every 3 weeks. The J-ALEX trial was included in the NMA as a separate node; comparisons to alectinib at 300 mg were therefore made separately. Multiple doses of ceritinib were also assessed in the ASCEND-4 and ASCEND-8 trials, including 750 mg, 600 mg, and 450 mg. The different doses of ceritinib were also assessed as separate nodes.
Crossover was not permitted in the CROWN, ALEX, ALESIA, J-ALEX ASCEND-8, or eXalt3 trials.18 The presence of treatment crossover was considered as it may introduce bias into the assessments of efficacy. Crossover was permitted in the ALTA-1L, ASCEND-4, PROFILE 1014, and PROFILE 1029 trials. In the ALTA-1L trial, 35 patients (25.5%) randomized originally to the crizotinib group crossed over to receive brigatinib. The sponsor noted that, while no methods to adjust for crossover were reported in the primary publication of the ALTA-1L trial, investigations reported in the sponsor’s submission to NICE deemed the rank-preserving structural failure time (RPSFT) method to be the most appropriate method of adjusting for crossover in the assessment of OS and such an analysis was conducted on a later data cut-off date of the ALTA-1L trial. Therefore, HRs from the NICE submission were used in the sponsor’s NMA for scenarios that did and did not include treatment crossover. The ASCEND-4 trial reported 80 patients (43.3%) randomized to the chemotherapy group who crossed over to receive ceritinib. Similar to crossover scenarios for brigatinib in the ALTA-1L trial, the RPSFT method was used to adjust for crossover for OS as a sensitivity analysis in the sponsor’s submission to NICE. Information from these crossover analyses were used in the sponsor’s NMA. In the PROFILE 1014 trial, 72.4% of patients randomized to chemotherapy crossed over to receive crizotinib. To account for crossover in the PROFILE 1014 trial, the sponsor used the RPSFT methodology. In the PROFILE 1029 trial, 70% of patients randomized to receive chemotherapy crossed over to receive crizotinib. No adjustments for crossover were conducted for this trial. The sponsor noted that removal of trials that included crossover (without RPSFT adjustment) was not possible, as it resulted in a disconnected network. Sensitivity analyses were performed when crossover-adjusted data were substituted into the network, where available, for OS.
End Points
OS and PFS were the primary end points analyzed in the ITC.
Overall Survival: OS data were available from all trials except the J-ALEX and ASCEND-8 trials; exclusion of these trials did not break the overall network. In addition, no OS data were available for ceritinib at 600 mg and 450 mg, or for alectinib at 300 mg. The overall network for OS is depicted in Figure 12.
Figure 12: OS Network for Sponsor’s ITC
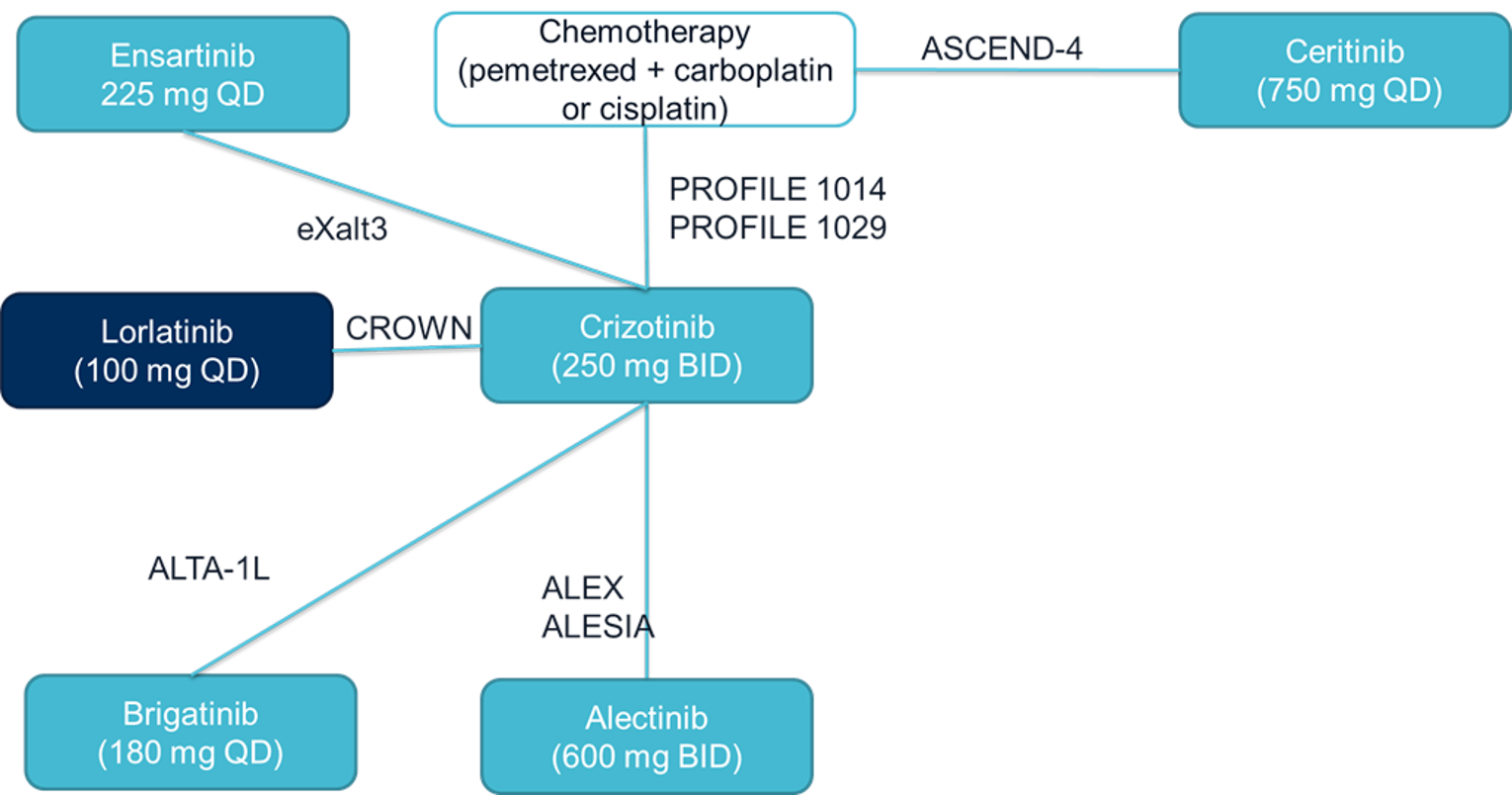
BID = twice daily; OS = overall survival; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Overall Survival Sensitivity Analyses: Sensitivity analyses for OS were conducted that excluded Asian patients. The ALESIA, J-ALEX, ASCEND-8, and PROFILE 1029 trials enrolled only Asian patients; therefore, these trials were excluded from the sensitivity analysis.
Another sensitivity analysis only included patients who were treatment-naive. The ALTA-1L and eXalt3 trials were therefore excluded as they did not report OS data for subgroups of patients who did not receive prior treatment.
Progression-Free Survival: PFS data assessed by independent radiological review were available for all 8 trials; and PFS data assessed by investigators were available in 6 of the trials (CROWN, ALEX, ALESIA, J-ALEX, ALTA-1L, and ASCEND-4). Of the studies included in the NMA, PFS data reported by race subgroup were available from 7 trials (CROWN, ALEX, ALTA-1L, ASCEND-4, ASCEND-8, PROFILE 1014, and eXalt3).
However, as intracranial PFS was an outcome interest; this outcome was only reported for the CROWN trial, based on patient-level data for IC-TTP and OS.
Data for IC-TTP were available from all trials except the ASCEND-4, ASCEND-8, and eXalt3 trials.
The overall network for PFS is depicted in Figure 13.
Figure 13: PFS Network for Sponsor’s ITC
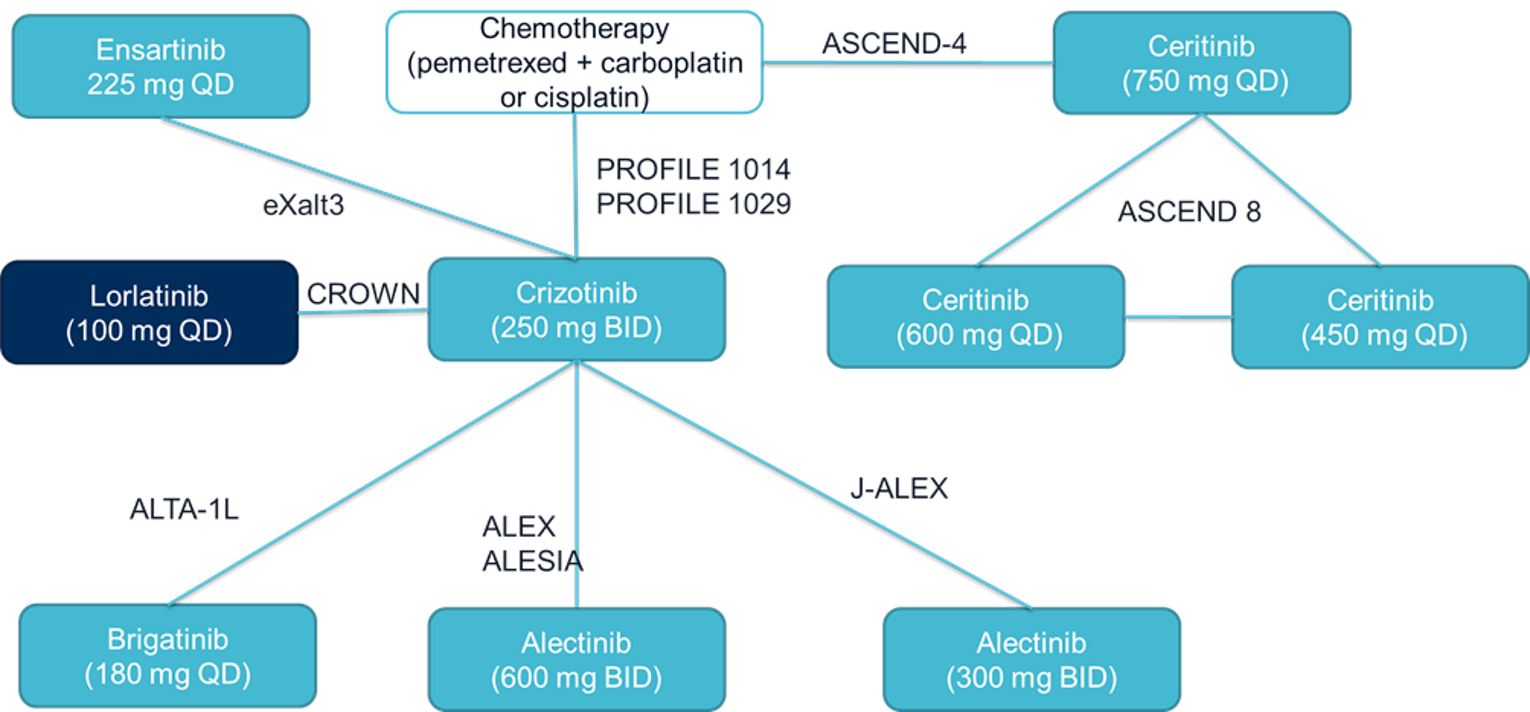
BID = twice daily; PFS = progression-free survival; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Progression-Free Survival Sensitivity Analysis: Three trials — ALESIA, J-ALEX, and PROFILE 1029 — enrolled only Asian patients. These trials were excluded from the sensitivity analyses.
Additional sensitivity analyses were also conducted on patients who did not receive any prior treatment. All trials had available PFS data for subgroups of patients who were treatment-naive except for the eXalt3 trial, which was excluded from this analysis.
Subgroup PFS data for patients with brain metastases were available in all trials except the ASCEND-8, PROFILE 1029, and eXalt3 trials. These trials were excluded in sensitivity analyses to determine the effect of brain metastases at baseline on PFS.
Other End Points
Other end points for consideration in the sponsor’s ITC included ORR, IC-ORR, IC-CR, intracranial progression response (IC-PR), grade 3 and 4 AEs, and discontinuations due to AEs. These end points were binary end points considered in the sponsor’s ITC. The availability of data for each of these binary end points is reported in Table 38.
Data for ORR was reported in all trials and assessed by independent radiological review, except in the ALEX and ALESIA trials, for which data reported for ORR were assessed by an investigator. All studies were included in the network for ORR (Figure 14).
Data for IC-ORR was reported in all studies except for J-ALEX, ASCEND-8, and PROFILE 1029. Removal of these trials did not disconnect the overall network (Figure 15).
Data for IC-CR was reported in most trials, except the J-ALEX, ASCEND-8, PROFILE 1014, and PROFILE 1029 trials. Excluding the studies that did not report IC-CR resulted in a disconnected link between chemotherapy and ceritinib; the remaining links in the network remained connected (Figure 16).
Data for IC-PR was only reported in the CROWN, ASCEND-4, ASCEND-8, and eXalt3 trials. However, because the counts for IC-PR were zero for both treatment groups in the eXalt3 trial, the eXalt3 trial was excluded from the network. Overall, due to lack of available data, comparisons for IC-PR were not feasible (Figure 17).
A network diagram for grade 3 and 4 AEs is depicted in Figure 18. Data regarding grade 3 and 4 AEs were available in all trials except the ASCEND-8, PROFILE 1029, and eXalt3 trials. Removal of trials not reporting grade 3 and 4 AEs did not result in a disconnected network. The network diagram for AEs resulting in treatment discontinuation is depicted in Figure 19. Because all trials reported data regarding AEs resulting in treatment discontinuation, all trials were included in the network.
Table 38: Binary End Point Data Reported by Included Studies in the Sponsor’s ITC
Study name | Trial name | Treatment 1 | Treatment 2 | 100% Asian studies | ORR IRR | IC-ORR IRR | IC complete response | IC progression response | Grade 3 and 4 AEs | AEDC |
|---|---|---|---|---|---|---|---|---|---|---|
Shaw (2020) | CROWN | Lorlatinib | Crizotinib | No | Yes | Yes | Yes | Yes | Yes | Yes |
Camidge (2019) | ALEX | Alectinib | Crizotinib | No | Yes (INV only) | Yes | Yes | No | Yes | Yes |
Zhou (2019) | ALESIA | Alectinib | Crizotinib | Yes | Yes (INV only) | Yes | Yes | No | Yes | Yes |
Hida (2017) | J-ALEX | Alectinib | Crizotinib | Yes | Yes | No | No | No | Yes | Yes |
Camidge (2018) | ALTA-1L | Brigatinib | Crizotinib | Yes | Yes | Yes | Yes | No | Yes | Yes |
Soria (2017) | ASCEND-4 | Ceritinib | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Cho (2019) | ASCEND-8 | Ceritinib (3 doses) | No | Yes | No | No | Yes | No | Yes | |
Solomon (2018) | PROFILE 1014 | Chemotherapy | Crizotinib | No | Yes | Yes | No | No | Yes | Yes |
Wu (2018) | PROFILE 1029 | Chemotherapy | Crizotinib | Yes | Yes | No | No | No | No | Yes |
Horn (2020) | eXalt3 | Ensartinib | Crizotinib | No | Yes | Yes | Yes | Yesa | No | Yes |
AE = adverse event; AEDC = discontinuation due to adverse events; IC = intercranial; INV = investigator-assessed; IRR = independent radiological review; ITC = indirect treatment comparison; ORR = objective response rate; PFS = progression-free survival.
Note: Bold text indicates comparison not possible.
aZero counts for both arms so trial is excluded.
Source: Sponsor’s ITC.18
Figure 14: ORR Network Diagram in Sponsor’s ITC
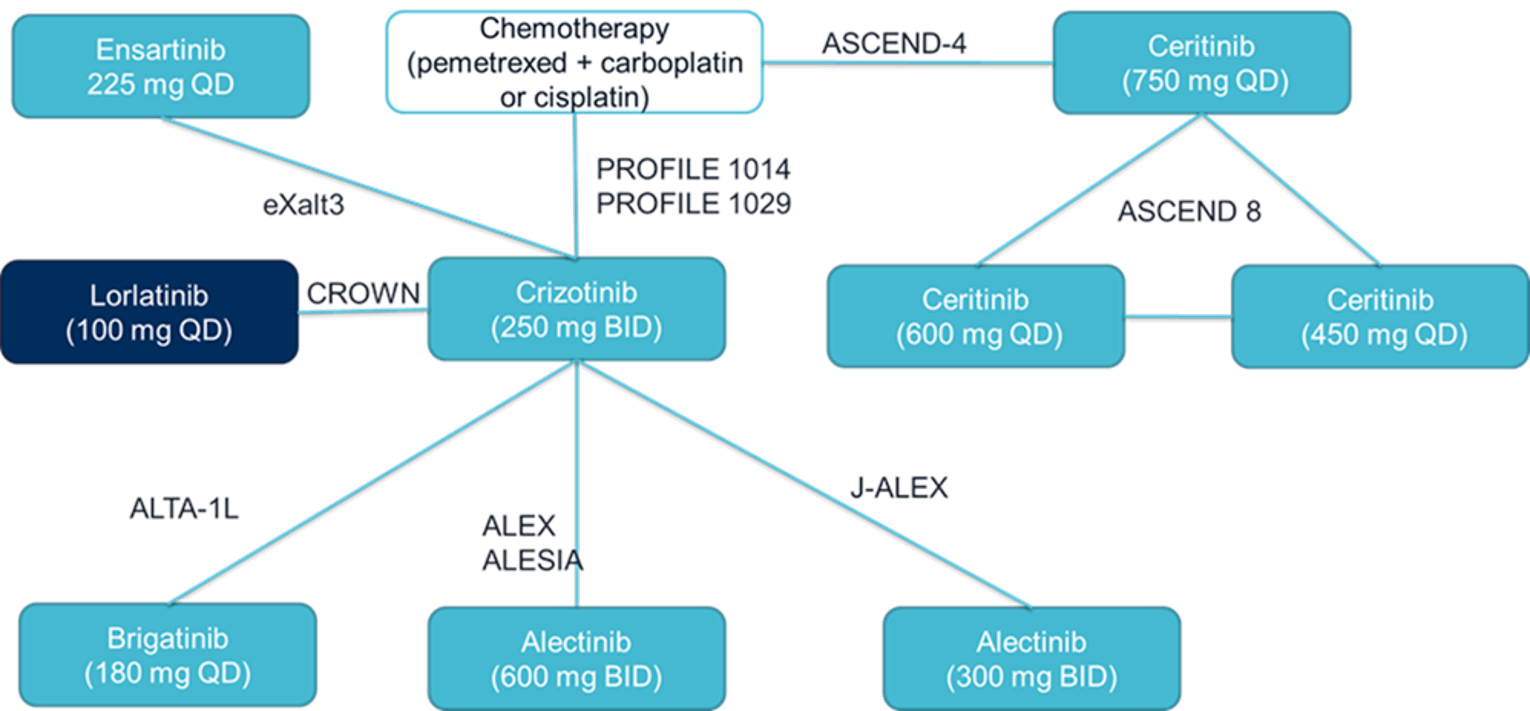
BID = twice daily; ORR = objective response rate; QD = once a day.
Source: Sponsor’s indirect treatment comparsion.18
Figure 15: IC-ORR Network Diagram in Sponsor’s ITC
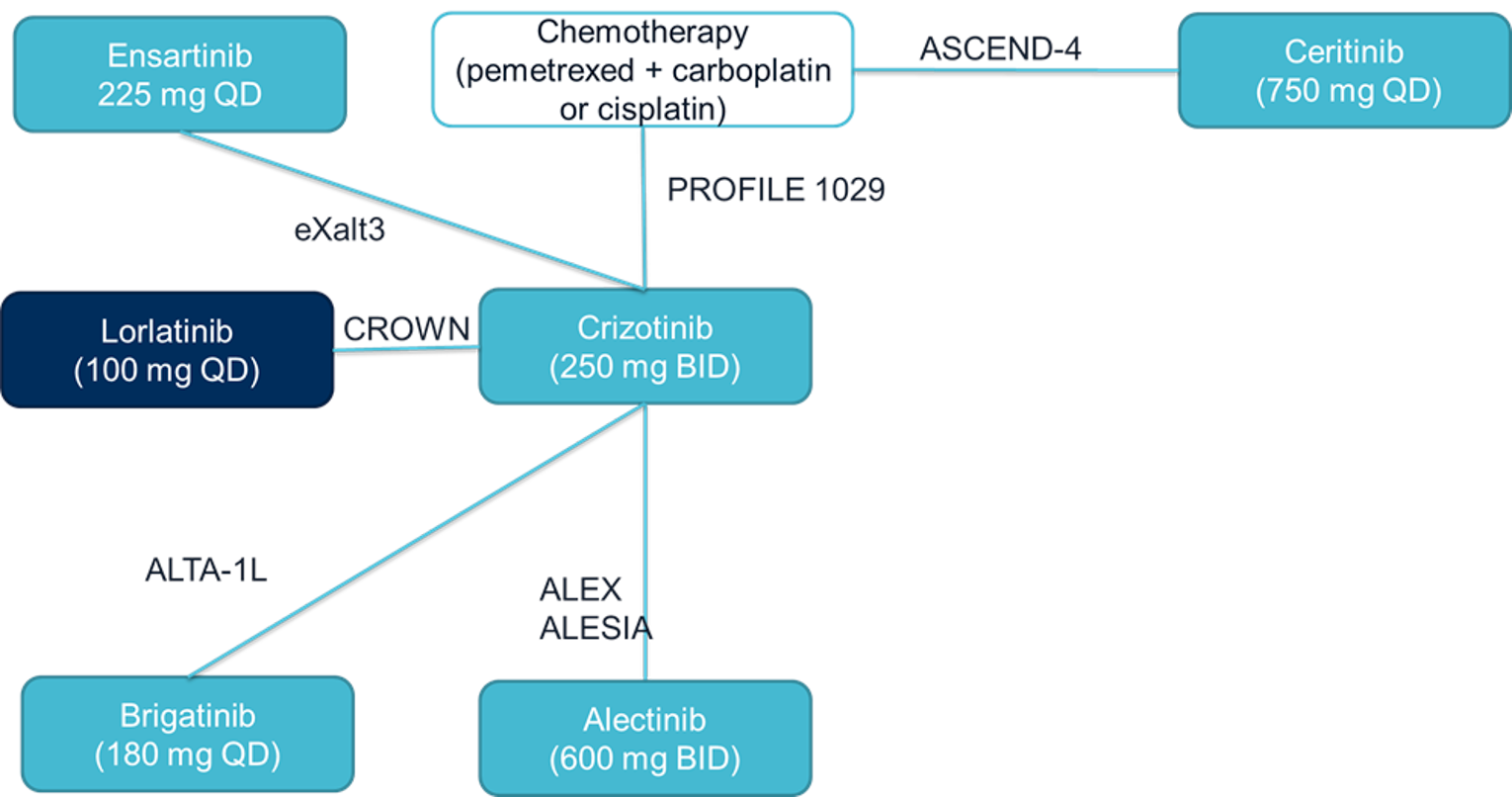
BID = twice daily; IC = intracranial; ORR = objective response rate; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Figure 16: IC-Complete Response Network Diagram in Sponsor’s ITC
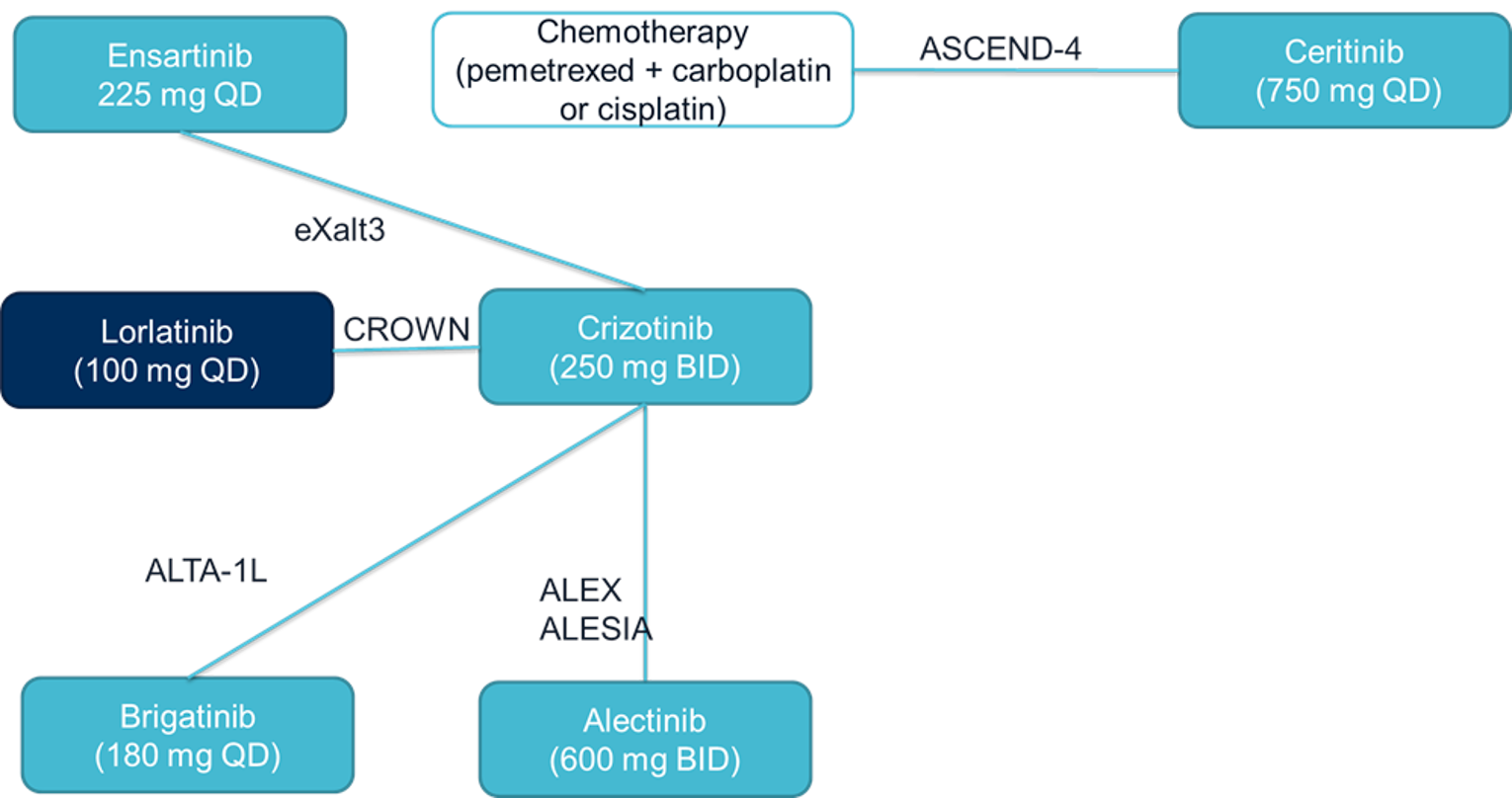
BID = twice daily; IC = intracranial; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Figure 17: IC-Progression Response Network Diagram in Sponsor’s ITC
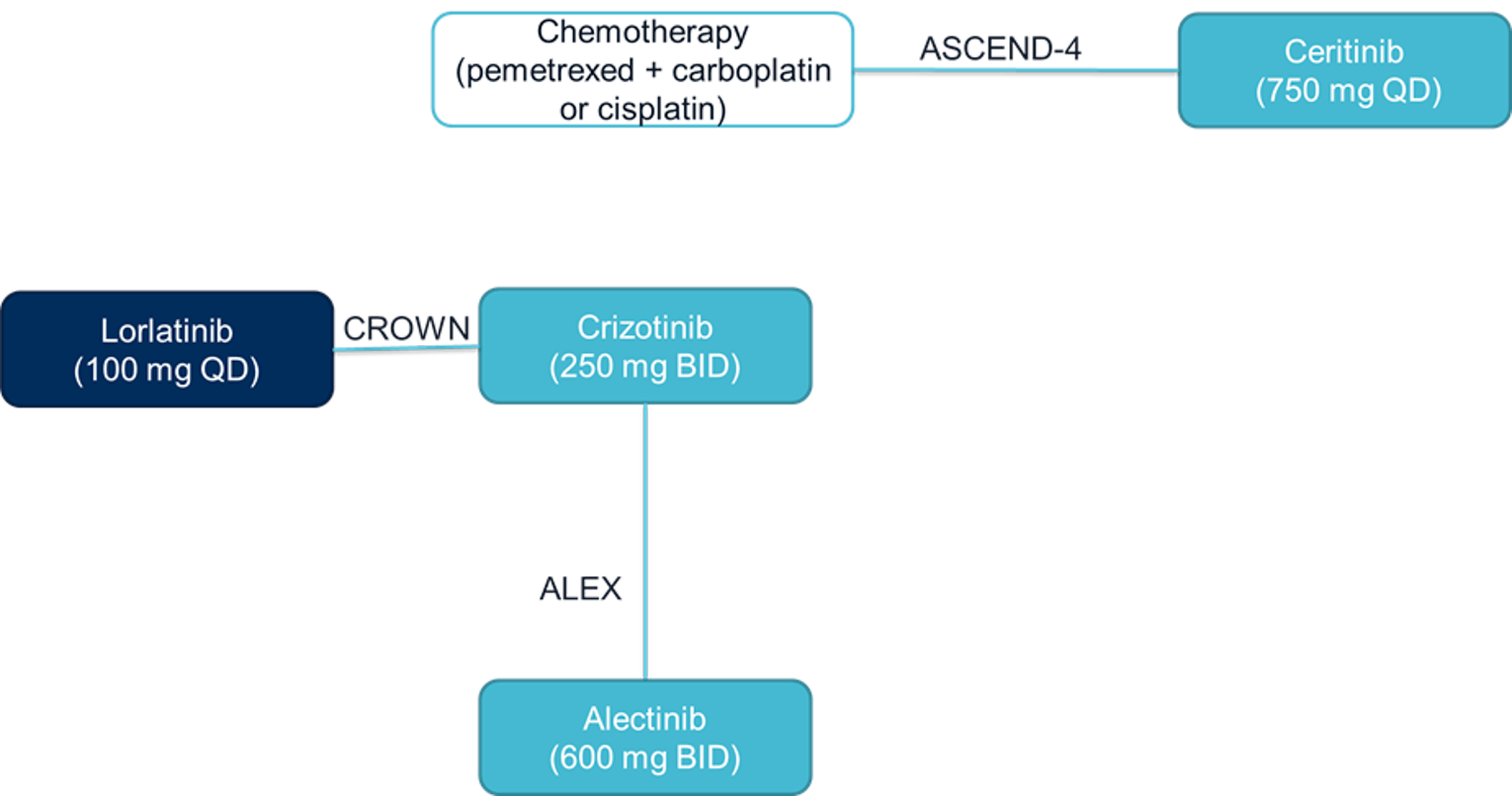
BID = twice daily; IC = intracranial; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Figure 18: Grade 3 and Grade 4 AEs Network Diagram in Sponsor’s ITC
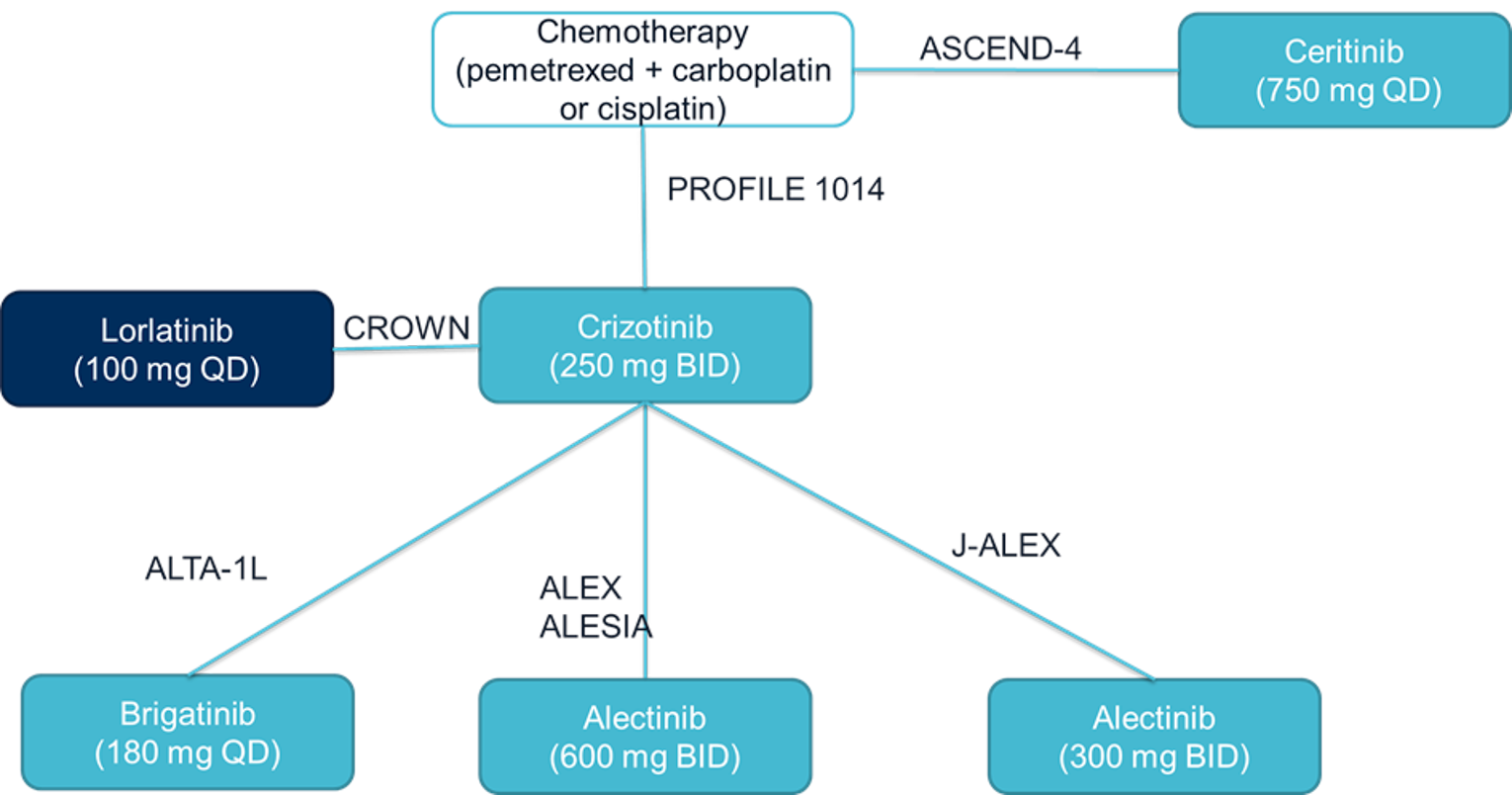
AE = adverse event; BID = twice daily; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Figure 19: AEs Resulting in Discontinuation Network Diagram in Sponsor’s ITC
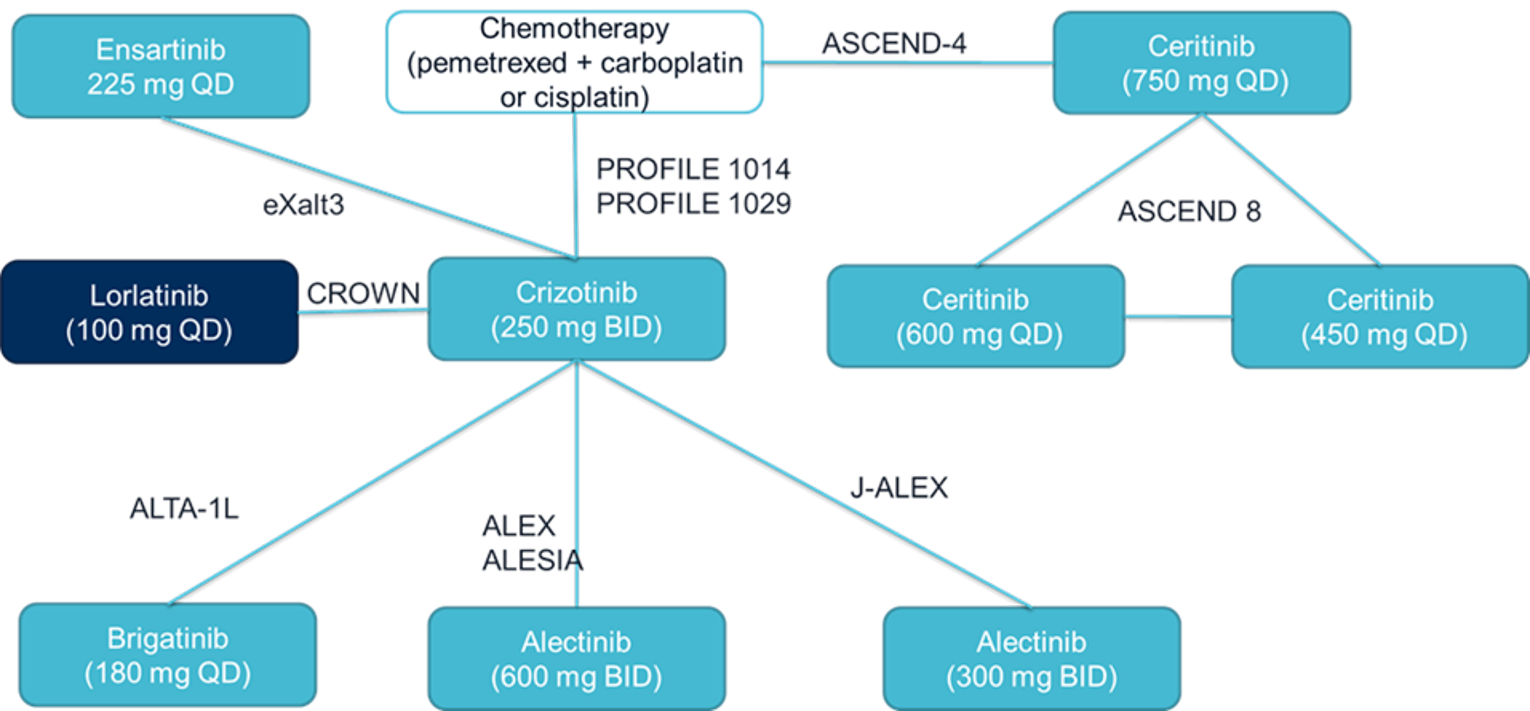
BID = twice daily; QD = once a day.
Source: Sponsor’s indirect treatment comparison.18
Both OS and PFS were estimated using published HRs and associated 95% CIs for data inputs. If only Kaplan-Meier curves were available, data from the Kaplan-Meier curves were digitized using methods by Guyot et al. (2012) to generate pseudo-patient-level data, and then estimate HRs. The proportional hazards assumption was assessed through visual inspection of Kaplan-Meier curves for both OS and PFS in each trial. For PFS, the sponsor treated the assumption as reasonable based on Kaplan-Meier plots as there was no clear change in HRs over time. The sponsor stated the proportional hazards assumption was reasonable for OS as well.18
Analyses of other end points (i.e., ORR, IC-ORR, IC-CR, IC-PR, grade 3 and 4 AEs, and AEs resulting in treatment discontinuation) used the number of patients with an event and the total number of patients in each treatment group of a study. Treatment effects were assessed using ORs and associated 95% CrIs.18
Results of Sponsor’s Indirect Treatment Comparison
Summary of Included Studies
Ten trials were included for analyses in the sponsor’s ITC, including CROWN, ALEX, J-ALEX, ALESIA, ALTA-1, ASCEND-4, ASCEND-8, PROFILE 1014, PROFILE 1029, and eXalt3. A summary of trial characteristics is provided in Table 39. Six of the included trials included treatment of patients in the first line, while the remaining included patients in multiple lines of therapy. Three of the trials enrolled Asian populations. All trials provided data on OS and PFS data except for the J-ALEX and ASCENT-8 trials, which did not have available OS data.
A summary of inclusion and exclusion criteria of the RCTs included in the ITC is provided in Table 40. Trials included in the ITC were published between 2017 and 2020. Enrolled patients included adults with stage IIIB or IV ALK-positive NSCLC (CROWN, ALEX, J-ALEX, ALESIA, ALTA-1L, ASCEND-8, and eXalt3); the remaining trials included patients with advanced, metastatic, or recurrent disease. Patients in all trials were naive to previous treatment with ALK inhibitors. Three trials (J-ALEX, ALTA-1L, and eXalt3) included patients who could have received prior treatment with chemotherapy and who were chemotherapy-naive, and 1 trial (ASCEND-8) included patients who could have received prior treatment with any treatment (including crizotinib) or who were naive to any treatment. All trials enrolled patients with an ECOG PS of 0 to 2. All trials permitted the enrolment of patients with brain metastases; however, some trials included criteria about patients with brain metastases, often specifying that their CNS disease must be asymptomatic and stable. All trials specified that disease must be measurable using RECIST 1.1 criteria; the CROWN trial was the only trial to specify patients must have had at least 1 extracranial measurable target lesion. Tumour requirements were not reported for the eXalt3 trial.
Table 39: Overview of Included RCTs Identified in the Sponsor’s Systematic Literature Review
Study name | Trial name | Study design, study setting, blinding, and study phase | Intervention and comparator | Treatment line | Asian-only population | OS available | PFS available |
|---|---|---|---|---|---|---|---|
Shaw (2020) | CROWN | RCT parallel Open-label Multi-centre internationala Phase III | Lorlatinib vs. crizotinib | First-line | No | Yes | Yes |
Camidge (2019) | ALEX | RCT parallel Open-label Multi-centre internationalb Phase III | Alectinib vs. crizotinib | First-line | No | Yes | Yes |
Zhou (2019) | ALESIA | RCT parallel Open-label Multi-centre internationalc Phase III | Alectinib vs. crizotinib | First-line | Yes | Yes | Yes |
Hida (2017) | J-ALEX | RCT parallel Open-label Multi-centre (Japan) Phase III | Alectinib vs. crizotinib | Mixed | Yes | No | Yes |
Camidge (2018) | ALTA-1L | RCT Open-label Multi-centre internationald Phase III | Brigatinib vs. crizotinib | Mixed | No | Yes | Yes |
Soria (2017) | ASCEND-4 | RCT crossover Open-label Multi-centre internationale Phase III | Ceritinib vs. chemotherapy | First-line | No | Yes | Yes |
Cho (2019) | ASCEND-8 | RCT parallel Open-label Multi-centre internationalf Phase I | Ceritinib (3 doses) | Mixed | No | No | Yes |
Solomon (2018) | Profile 1014 | RCT Open-label Multi-centre internationalg Phase III | Chemotherapy vs. crizotinib | First-line | No | Yes | Yes |
Wu (2018) | Profile 1029 | RCT crossover Open-label Multi-centre internationalh Phase III | Chemotherapy vs. crizotinib | First-line | Yes | Yes | Yes |
Horn (2020) | eXalt3 | RCT Open-label Multi-centre internationali Phase III | Ensartinib vs. crizotinib | Mixed | No | Yes | Yes |
OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; vs. = versus.
aArgentina, Australia, Belgium, Canada, China, Czech Republic, France, Germany, Hong Kong, India, Italy, Japan, Mexico, Netherlands, Poland, Russia, South Korea, Singapore, Spain, Taiwan, Turkey, the UK, and the US.
bAustralia, Bosnia and Herzegovina, Brazil, Canada, Chile, China, Costa Rica, Egypt, France, Germany, Guatemala, Israel, Italy, South Korea, Mexico, New Zealand, Poland, Portugal, Russian Federation, Serbia, Singapore, Spain, Switzerland, Taiwan, Thailand, Ukraine, the UK, and the US.
cChina, South Korea, and Thailand.
dAt 124 centres in 20 countries.
eAustralia, New Zealand, Austria, Brazil, China, Colombia, Denmark, France, Germany, Greece, India, Ireland, Italy, Japan, South Korea, Lebanon, Mexico, Netherlands, Norway, Portugal, Russian Federation, Singapore, Spain, Sweden, Taiwan, Thailand, Turkey, and the UK.
fPatients were recruited from 87 centres across 24 countries.
gAustralia, Austria, Belgium, Brazil, Canada, Chile, China, Finland, France, Germany, India, Ireland, Italy, Japan, South Korea, Luxembourg, Mexico, Netherland, Norway, Peru, Portugal, Russian Federation, Singapore, South Africa, Spain, Switzerland, Taiwan, Ukraine, the UK, and the US.
hChina, Malaysia, and Thailand.
iArgentina, Australia, Belgium, Brazil, Canada, China, Czechia, France, Germany, Hong Kong, Israel, Italy, Netherlands, Peru, Poland, Russia, South Korea, Spain, Turkey, the UK, and the US.
Source: Sponsor’s indirect treatment comparison.18
Table 40: Summary of Inclusion and Exclusion Criteria of Included RCTs in Sponsor’s ITC
Study name | Trial name | Disease stage | Line of treatment | ECOG PS | CNS metastases | Tumour requirement | Age |
|---|---|---|---|---|---|---|---|
Shaw (2020) | CROWN | IIIB/IV ALK-positive NSCLC | ALK inhibitor–naive | 0 to 2 | Asymptomatic treated or untreated CNS metastases permitted | ≥ 1 extracranial measurable target lesion (RECIST 1.1) with no prior radiation required | ≥ 18 years (or ≥ 20 years as required by local regulation) |
Camidge (2019) | ALEX | IIIB/IV ALK-positive NSCLC | ALK inhibitor–naive | 0 to 2 | CNS metastases allowed if asymptomatic | Measurable disease (RECIST 1.1) | ≥ 18 years |
Zhou (2019) | ALESIA | IIIB/IV ALK-positive NSCLC | ALK inhibitor–naive | 0 to 2 | CNS metastases allowed if asymptomatic | Measurable disease (RECIST 1.1) | ≥ 18 years |
Hida (2017) | J-ALEX | IIIB/IV ALK-positive NSCLC | ALK inhibitor–naive ± prior chemo | 0 to 2 | Permitted | ≥ 1 measurable target lesion (RECIST 1.1) | ≥ 20 years |
Camidge (2018) | ALTA-1L | IIIB/IV ALK-positive NSCLC | ALK inhibitor–naive ± prior chemo | 0 to 2 | Permitted if asymptomatic and neurologically stable with no increasing dose of steroids or anticonvulsants within 7 days before randomization | ≥ 1 measurable target lesion (RECIST 1.1) | ≥ 18 years |
Soria (2017) | ASCEND-4 | Advanced or metastatic non-squamous ALK- rearranged NSCLC | ALK inhibitor–naive | 0 to 2 | Permitted if clinically and neurologically stable with no increasing steroids within 2 weeks before screening | Measurable disease (RECIST 1.1) | ≥ 18 years |
Cho (2019) | ASCEND-8 | IIIB/IV NSCLC harbouring an ALK rearrangement | ALK inhibitor–naive ± prior treatment (including crizotinib) | 0 to 2 | Could have asymptomatic or neurologically stable CNS metastases | At least 1 measurable lesion (RECIST 1.1) | ≥ 18 years |
Solomon (2018) | PROFILE 1014 | Locally advanced, recurrent, or metastatic non-squamous ALK-positive NSCLC | ALK inhibitor–naive | 0 to 2 | CNS metastases permitted if treated and neurologically stable with no ongoing requirement for corticosteroids for at least 2 weeks before study entry | Must have had measurable disease (RECIST 1.1) | ≥ 18 years (or ≥ 20 or ≤ 65 years as required by local regulation) |
Wu (2018) | PROFILE 1029 | Locally advanced, recurrent, or metastatic non-squamous NSCLC positive for an ALK rearrangement | ALK inhibitor–naive | 0 to 2 | Brain metastases were eligible if appropriately treated and neurologically stable for at least 2 weeks before enrolment | Measurable disease (RECIST 1.1) | 18 to 70 years |
Horn (2020) | eXalt3 | Stage IIIB/IV NSCLC | ALK inhibitor–naive ± prior chemo | 0 to 2 | Permitted | NR | NR |
ALK = anaplastic lymphoma kinase; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; NR = not reported; NSCLC = non–small cell lung cancer; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; RCT = randomized controlled trial.
Source: Sponsor’s ITC.18
The J-ALEX, ALTA-1L, ASCEND-8, and eXalt3 trials enrolled patients who had received prior treatment; a summary of prior treatments received by these patients is provided in Table 41. In all trials, previous treatment with ALK inhibitors was not permitted, except for the ASCENT-8 trial, which allowed previous treatment with crizotinib. Previous treatment with chemotherapy was allowed within all 4 trials; previous treatment with chemotherapy was the only previous treatment permitted within the J-ALEX, ALTA-1L, and eXalt3 trials.18
There were no imbalances in the proportions of patients who received prior treatments across treatment groups, except for the ASCEND-8 trial, in which more patients randomized to receive ceritinib at 600 mg received a prior treatment than patients randomized to the 450 mg or 750 mg ceritinib groups. Across the trials, the proportions of patients with previous therapy were similar, at between 41% and 24%. Following the 80% rule used by the sponsor for its systematic literature review, patients in studies were required to fit 80% of eligibility criteria of the systematic literature review; the majority of patients enrolled in these trials were therefore treatment-naive.18
Table 41: Summary of Prior Treatments for RCTs That Enrolled Patients With Prior Treatments Included in the Sponsor’s Indirect Treatment Comparison
Study name | Trial name | Line of treatment | Treatment | N in study | N (%) strictly first-line | Inclusion |
|---|---|---|---|---|---|---|
Hida (2017) | J-ALEX | ALK inhibitor–naive ± prior chemo | Alectinib | 103 | 66 (64%) | Patients who were chemotherapy-naive or who had received 1 previous chemotherapy regimen |
Crizotinib | 104 | 67 (64%) | ||||
Camidge (2018) | ALTA-1L | ALK inhibitor–naive ± prior chemo | Brigatinib | 137 | 101 (74%) | Patients who had not previously received ALK-targeted therapy (although they could have received chemotherapy) |
Crizotinib | 138 | 101 (73%) | ||||
Cho (2019) | ASCEND-8 | ALK inhibitor–naive ± prior treatment (including crizotinib) | Ceritinib 450 mg | 108 | 73 (68%) | Eligible patients who were either treatment-naive (except for neoadjuvant/adjuvant systemic therapy, excluding regimens containing an ALK inhibitor) or were previously treated with at least 1 systemic anticancer therapy (including crizotinib) |
Ceritinib 600 mg | 87 | 51 (59%) | ||||
Ceritinib 750 mg | 111 | 74 (67%) | ||||
Horn (2020) | eXalt3 | ALK inhibitor–naive ± prior chemo (no chemo subgroup) | Ensartinib | 143 | 109 (76%) | Patients who had not received prior ALK inhibitors and no more than 1 chemotherapy regimen |
Crizotinib | 147 | 105 (71%) |
ALK = anaplastic lymphoma kinase; RCT = randomized controlled trial.
Source: Sponsor’s indirect treatment comparison.18
Study Characteristics
A summary of the baseline characteristics of patients in the trials included in the sponsor’s ITC is provided in Table 42. In general, baseline characteristics of patients included in the trials were balanced, with some exceptions. In the CROWN trial, patients in the lorlatinib group had a higher median age (61 years) compared to the crizotinib group (56 years). The proportions of males across both trials were similar, ranging between 37% and 61%; however, the ALTA-1L, ASCEND-4, and ASCEND-8 trials were characterized by differences in the proportions of males and females between treatment groups.18 Across all trials the proportion of patients who were never smokers was greater than the proportion of patients who were current or former smokers. Patient ECOG PS scores were similar across treatment groups in all trials, and all trials enrolled mostly patients with ECOG PS of 0 or 1. The proportions of patients with brain metastases in the trials ranged between 25% and 40% and there were imbalances in the proportion of patients with brain metastases between treatment groups in the PROFILE 1029, J-ALEX, and eXalt3 trials. The proportion of patients classified as Asian were similar across treatment groups in all trials except the ALTA-1L trial. Some trials enrolled slightly more than one-third Asian patients (CROWN, ALEX, ASCEND-8, ALTA-1L, PROFILE 1014, ASCEND-4, and eXalt3), and others exclusively Asian patients (J-ALEX, ALESIA, and PROFILE 1029). The smoking status of patients within trials was relatively similar between treatment groups, except for the CROWN, ALESIA, ALTA-1L, and ASCEND-4 trials.18
The inclusion criteria of the sponsor’s systematic review specified that included studies must include patients who were previously untreated or receiving treatment in the first line. However, only 4 trials included 100% of patients who did not receive prior systemic therapy for metastatic disease (CROWN, ALEX, PROFILE 1029, and PROFILE 1014). The remaining trials included patients who received prior treatments, although only the J-ALEX, ALTA-1L, ASCEND-8, and eXalt3 trials specified enrolment of patients with prior therapy in the eligibility criteria. These trials are described in the preceding section.18
Table 42: Summary of Baseline Characteristics of RCTs Included in the Sponsor’s ITC
Trial name | Treatment/ comparator | N | Age, median (range) | Gender, % (female:male) | Brain metastasis, % | Race (Asian), % | Smoking, % | ECOG PS (0 or 1), % | Prior chemotherapy, % | |
|---|---|---|---|---|---|---|---|---|---|---|
Never smoker | Current smoker | |||||||||
CROWN | Lorlatinib | 149 | 61 (30 to 90) | 56:44 | 26 | 44 | 54 | 46 | 98 | 0 |
Crizotinib | 147 | 56 (26 to 84) | 62:38 | 27 | 44 | 64 | 35 | 94 | 0 | |
ALEX | Alectinib | 152 | 58 (25 to 88) | 55:45 | 42 | 45 | 61 | 40 | 93 | 0 (NR) |
Crizotinib | 151 | 54 (18 to 91) | 58:42 | 38 | 46 | 65 | 35 | 93 | 0 (NR) | |
ASCEND-8 | Ceritinib 450 mg | 73a | 55 (26 to 87) | 56:44 | 33 | 40 | 64 | 36 | NR | 4 |
Ceritinib 600 mg | 51a | 52 (21 to 81) | 39:61 | 29 | 37 | 59 | 39 | NR | 12 | |
Ceritinib 750 mg | 74a | 51 (22 to 87) | 47:53 | 28 | 35 | 66 | 34 | NR | 8 | |
ALESIA | Alectinib | 125 | 51 (43 to 59) | 49:51 | 35 | 100 | 67 | 33 | 97 | 6 |
Crizotinib | 62 | 49 (41 to 59) | 45:55 | 37 | 100 | 73 | 28 | 98 | 15 | |
ALTA-1L | Brigatinib | 137 | 58 (27 to 86) | 50:50 | 29 | 43 | 61 | 39 | 96 | 26 |
Crizotinib | 138 | 60 (29 to 86) | 41:59 | 30 | 36 | 54 | 46 | 96 | 27 | |
PROFILE 1014 | Crizotinib | 172 | 52 (22 to 76) | 60:40 | 26 | 45 | 62 | 39 | 94 | 0 |
Chemotherapy | 171 | 54 (19 to 78) | 63:37 | 27 | 47 | 65 | 35 | 95 | 0 | |
PROFILE 1029 | Crizotinib | 104 | 48 (24 to 67) | 52:48 | 20 | 100 | 75 | 25 | 96 | 0 |
Chemotherapy | 103 | 50 (23 to 69) | 58:42 | 31 | 100 | 70 | 30 | 96 | 0 | |
J-ALEX | Alectinib | 103 | 61 (27 to 85) | 60:40 | 14 | 100 | 54 | 46 | 98 | 36 |
Crizotinib | 104 | 60 (25 to 84) | 61:39 | 28 | 100 | 59 | 41 | 98 | 36 | |
ASCEND-4 | Ceritinib | 189 | 55 (22 to 81) | 54:46 | 31 | 40 | 57 | 43 | 94 | 5 |
Chemotherapy | 187 | 54 (22 to 80) | 61:39 | 33 | 44 | 65 | 35 | 93 | 5 | |
eXalt3 | Ensartinib | 143 | 54 (25 to 86) | 50:50 | 33 | 54 | 59 | 41 | 95 | 24 |
Crizotinib | 147 | 53 (26 to 90) | 48:52 | 39 | 57 | 64 | 0 | 95 | 29 | |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; NR = not reported; RCT = randomized controlled trial.
aTreatment-naive population: the intention-to-treat population of this study includes patients with prior crizotinib.
Source: Sponsor’s ITC.18
Risk of Bias Assessment
Two independent reviewers conducted a quality assessment of the included RCTs. The quality assessment criteria were based on recommendations in the NICE sponsor’s submission template. The quality assessment included aspects of randomization, allocation concealment, baseline characteristics, blinding, patient withdrawals, outcome selection and reporting bias, and statistical analyses in studies. The following questions were used as guidance:
Was randomization carried out appropriately?
Was the concealment of treatment allocation adequate?
Were the groups similar at the outset of the study in terms of prognostic factors?
Were the care providers, participants, and outcome assessors blind to treatment allocation?
Were there any unexpected imbalances in dropouts between groups?
Is there any evidence to suggest that the authors measured more outcomes than they reported?
Did the analysis include an intention-to-treat analysis? If so, was this appropriate and were appropriate methods used to account for missing data?
Responses to these questions were reported as either yes, no, or unclear. Based on the sponsor’s assessment, trials included in the NMA (ALEX, J-ALEX, ASCEND-4, ASCEND-8, ALESIA, ALTA-1L, PROFILE 1014, and PROFILE 1029) were rated as having high quality regarding randomization, baseline characteristics, withdrawals, measurement of outcomes, and statistical analyses. All studies except for the ALTA-1L, PROFILE 1014, and PROFILE 1029 trials were rated as having high-quality allocation concealment. All studies were rated as having very low quality regarding blinding.
Results
Progression-Free Survival
Three models were assessed for PFS, including 2 random-effects models and 1 fixed-effect model. Based on the deviance information criterion, the fixed-effects model had the best fit to the data and was used in the primary analysis and sensitivity analyses. Random-effects models resulted in treatment estimates with wide CrIs. A summary of PFS results is provided in Table 43. Lorlatinib was favoured against all treatments except for alectinib at a dose of 300 mg.
Sensitivity Analyses: Among subgroups of patients who were treatment-naive, results were consistent with the primary analysis; lorlatinib was favoured compared to all treatments except for alectinib at 300 mg. For the analyses that removed studies that enrolled only Asian patients, lorlatinib was favoured over all treatments, although alectinib at 300 mg was not included in this analysis. Ensartinib was not included in the analysis of PFS for patients with brain metastasis. Among the subset of patients with brain metastasis, lorlatinib was favoured over ceritinib (750 mg), crizotinib, and chemotherapy, but not over alectinib at 600 mg and 300 mg and brigatinib. Ensartinib and ceritinib at 600 mg and 450 mg were not included in this analysis.
Results for IC-TTP favoured lorlatinib against brigatinib, crizotinib, and chemotherapy, but not alectinib at 600 mg. Alectinib at 300 mg, ceritinib at any dose, and ensartinib were not included in this analysis.
Table 43: PFS Results of Sponsor’s ITC
Treatment | PFS ITT: FE, HR (95% CrI) | PFS INV: FE, HR (95% CrI) | PFS treatment-naive: FE, HR (95% CrI) | PFS remove 100% Asian FE, HR (95% CrI) | PFS brain metastasis subgroup FE, HR (95% CrI) | IC-TTP FE, HR (95% CrI) |
|---|---|---|---|---|---|---|
Alectinib (600 mg) | 0.61 (0.38 to 0.99) | 0.57 (0.36 to 0.90) | 0.61 (0.38 to 0.98) | 0.56 (0.34 to 0.93) | 0.76 (0.33 to 1.78) | 0.45 (0.16 to 1.27) |
Alectinib (300 mg) | 0.82 (0.36 to 1.85) | 0.62 (0.34 to 1.13) | 0.90 (0.44 to 1.85) | NR | 2.55 (0.29 to 22.81) | NR |
Brigatinib | 0.57 (0.34 to 0.95) | 0.48 (0.29 to 0.81) | 0.51 (0.28 to 0.94) | 0.57 (0.34 to 0.95) | 0.82 (0.31 to 2.12) | 0.23 (0.07 to 0.75) |
Ceritinib (750 mg) | 0.22 (0.13 to 0.37) | NR | 0.22 (0.13 to 0.37) | 0.23 (0.13 to 0.40) | 0.12 (0.04 to 0.33) | NR |
Ceritinib (450 mg) | 0.31 (0.15 to 0.66) | NR | 0.31 (0.15 to 0.66) | 0.32 (0.15 to 0.70) | NR | NR |
Ceritinib (600 mg) | 0.25 (0.12 to 0.54) | NR | 0.25 (0.12 to 0.54) | 0.26 (0.12 to 0.58) | NR | NR |
Crizotinib | 0.28 (0.19 to 0.41) | 0.21 (0.14 to 0.31) | 0.28 (0.19 to 0.41) | 0.28 (0.19 to 0.41) | 0.20 (0.10 to 0.43) | 0.07 (0.03 to 0.18) |
Ensartinib | 0.55 (0.32 to 0.93) | NR | NR | 0.55 (0.32 to 0.93) | NR | NR |
Chemotherapy | 0.12 (0.08 to 0.19) | NR | 0.12 (0.08 to 0.19) | 0.13 (0.08 to 0.20) | 0.08 (0.03 to 0.21) | 0.04 (0.01 to 0.11) |
CrI = credible interval; FE = fixed effect; HR = hazard ratio; IC-TTP = intracranial time to progression; INV = investigator; ITT = intention-to-treat; NR = not reported; PFS = progression-free survival.
Note: Results in bold indicate the base-case analyses. All estimates are vs. lorlatinib.
Source: Sponsor’s indirect treatment comparison.18
Overall Survival
Three models, including 2 random-effects models and 1 fixed-effect model, were assessed for best fit for OS. Based on the deviance information criterion, the fixed-effect model had the best fitted data. Random-effects models also resulted in treatment-effect estimates with wide CrIs. Fixed-effects models were used as the primary analysis and for sensitivity analyses.
Analyses for OS were also conducted with adjustment for treatment crossover; a network diagram illustrating the unadjusted and crossover-adjusted HRs is depicted in Figure 20. After adjustment for crossover, lorlatinib was found to be favoured over chemotherapy (HR = 0.58; 95% CrI, 0.07 to 0.85), but not over any other treatment. Comparisons between lorlatinib and alectinib at 600 mg, brigatinib, crizotinib, ensartinib were similar to results of the primary unadjusted analysis for OS. However, comparisons between lorlatinib and brigatinib or ceritinib at 750 mg and chemotherapy were not similar to unadjusted results. The direction of the effect compared to brigatinib was closer to the null versus comparisons to ceritinib at 750 mg and chemotherapy, which were further from the null.
Lorlatinib was not favoured over any treatments (Table 44).
Sensitivity Analyses: The sponsor noted that adjusted OS results provided a fairer comparison across all trials. Therefore, sensitivity analyses were conducted using the adjusted fixed-effects models.
Among the subset of patients who were treatment-naive, lorlatinib was favoured over chemotherapy; no differences were found between lorlatinib and alectinib at 600 mg, ceritinib at 750 mg, or crizotinib. Brigatinib and ensartinib were not included in the analysis of assessments of treatment-naive patients. When studies that included exclusively Asian patients were removed, lorlatinib was favoured over chemotherapy, but not over any other treatments. Among the subset of patients with brain metastases, lorlatinib was not favoured over alectinib at 600 mg, crizotinib, or chemotherapy; the remaining treatments were not included in this analysis.
Table 44: OS Results of Sponsor’s ITC
Treatment | OS ITT: FE, HR (95% CrI) | OS adjusted for crossover: FE, HR (95% CrI) | OS first-line subgroup: FE, HR (95% CrI) | OS remove 100% Asian FE, HR (95% CrI) | OS brain metastases subgroup FE, HR (95% CrI) |
|---|---|---|---|---|---|
Alectinib (600 mg) | 1.21 (0.63 to 2.35) | 1.21 (0.63 to 2.33) | 1.21 (0.63 to 2.34) | 1.04 (0.53 to 2.06) | 1.26 (0.42 to 3.72) |
Brigatinib | 0.79 (0.38 to 1.63) | 0.83 (0.32 to 2.10) | NR | 0.83 (0.33 to 2.11) | NR |
Ceritinib (750 mg) | 0.79 (0.38 to 1.64) | 0.34 (0.09 to 1.23) | 0.34 (0.09 to 1.25) | 0.34 (0.10 to 1.24) | NR |
Crizotinib | 0.72 (0.41 to 1.26) | 0.72 (0.42 to 1.25) | 0.72 (0.41 to 1.25) | 0.72 (0.41 to 1.25) | 0.75 (0.30 to 1.90) |
Ensartinib | 0.82 (0.38 to 1.76) | 0.82 (0.38 to 1.76) | NR | 0.82 (0.38 to 1.76) | NR |
Chemotherapy | 0.58 (0.31 to 1.07) | 0.25 (0.07 to 0.85) | 0.25 (0.07 to 0.85) | 0.25 (0.07 to 0.85) | 0.97 (0.32 to 2.90) |
CrI = creditable interval; FE = fixed effect; HR = hazard ratio; ITT = intention-to-treat; NR = not reported; OS = overall survival.
Note: Results in bold indicate the base-case analyses.
Source: Sponsor’s indirect treatment analysis.18
Figure 20: Network Diagram for OS With Unadjusted and Crossover-Adjusted HRs and CIs
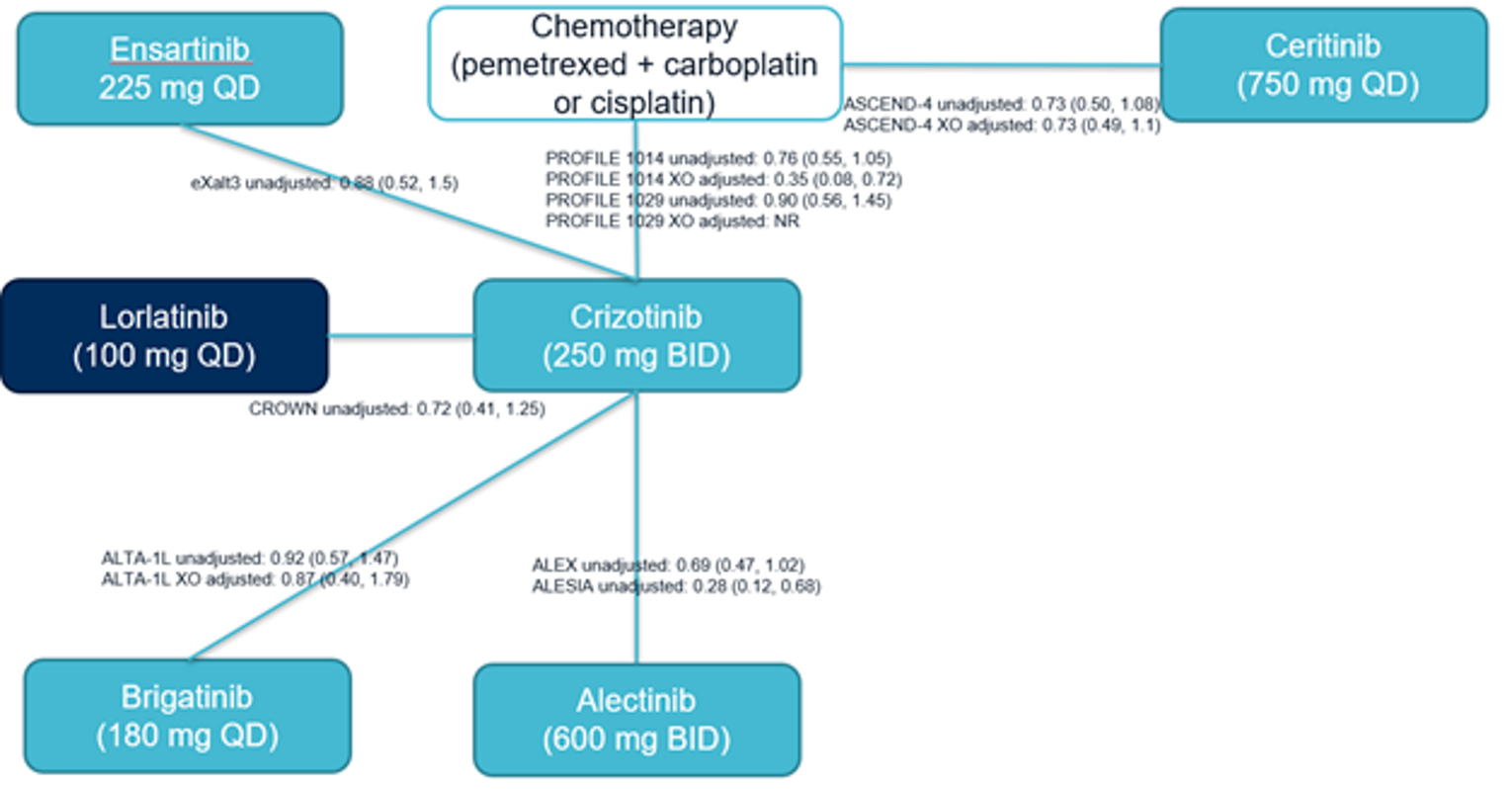
BID = twice daily; CI = confidence interval; HR = hazard ratio; NR = not reported; OS = overall survival; QD = once a day; XO = crossover.
Source: Sponsor’s indirect treatment comparison.18
Other Binary End Points
The networks for the other binary end points were small; therefore, only fixed-effects analyses were conducted for these end points (Table 45). For the ORR, IC-ORR, and IC-CR end points, an OR of greater than 1 indicated an improved response when treated with lorlatinib versus a comparator treatment. For the IC-PR end point, an effect value less than 1 favoured lorlatinib, as this was considered a “negative” event. For safety end points, including grade 3 and 4 AEs and AEs resulting in treatment discontinuation, ORs greater than 1 suggested greater AEs with lorlatinib group compared to the comparator treatment.
For ORR, lorlatinib was favoured over crizotinib (OR = 2.31; 95% CrI, 1.41 to 3.82) and chemotherapy (OR = 10.92; 95% CrI, 5.87 to 20.54), but not any other therapy. For IC-ORR, lorlatinib was favoured over ceritinib at 750 mg (OR = 23.25; 95% CrI, 4.23 to 134.14), crizotinib (OR = 8.14; 95% CrI, 2.98 to 24.36) and chemotherapy (OR = 76.80; 95% CrI, 18.09 to 353.31). Intracranial complete response was favoured with lorlatinib when compared with crizotinib (OR = 9.30; 95% CrI, 3.25 to 30.18). Lorlatinib was not favoured against any treatment when considering IC-PR.
Regarding safety, the odds of grade 3 and 4 AEs occurring were higher in the lorlatinib group than alectinib at 300 mg (OR = 6.49; 95% CrI, 3.01 to 14.00) or 600 mg (OR = 3.32; 95% CrI, 1.80 to 6.15) and crizotinib (OR = 2.11; 95% CrI, 1.30 to3.44). The ORs for the remaining comparisons against lorlatinib were all greater than 1, suggesting that lorlatinib was not favoured when considering grade 3 and 4 AEs. Regarding AEs resulting in treatment discontinuation, lorlatinib was favoured against chemotherapy (OR = 0.31; 95% CrI, 0.11 to 0.91).
Table 45: Results of Binary End Points in Sponsor’s ITC
Treatment | ORR BICR ITT: FE, OR (95% CrI) | IC-ORR BICR ITT: FE, OR (95% CrI) | IC-CR ITT: FE, OR (95% CrI) | IC-PR ITT: FE, OR (95% CrI) | AEDC ITT: FE, OR (95% CrI) | Grade 3 and 4 AE ITT: FE, OR (95% CrI) |
|---|---|---|---|---|---|---|
Alectinib (600 mg) | 1.46 (0.69 to 3.12) | 1.45 (0.43 to 5.09) | 1.11 (0.28 to 4.58) | 0.25 (0.02 to 2.08) | 0.77 (0.27 to 2.18) | 3.32 (1.80 to 6.15) |
Alectinib (300 mg) | 0.77 (0.25 to 2.18) | NR | NR | NR | 1.91 (0.57 to 6.59) | 6.49 (3.01 to 14.00) |
Brigatinib | 1.43 (0.70 to 2.92) | 0.76 (0.18 to 3.29) | 0.58 (0.06 to 3.78) | NR | 0.50 (0.15 to 1.64) | 1.67 (0.84 to 3.36) |
Ceritinib (750 mg) | 1.50 (0.69 to 3.26) | 23.25 (4.23 to 134.14) | NR | NR | 0.37 (0.10 to 1.33) | 1.32 (0.61 to 2.87) |
Ceritinib (450 mg) | 1.30 (0.44 to 3.91) | NR | NR | NR | 0.59 (0.06 to 7.22) | NR |
Ceritinib (600 mg) | 1.76 (0.57 to 5.44) | NR | NR | NR | 0.41 (0.04 to 5.15) | NR |
Crizotinib | 2.31 (1.41 to 3.82) | 8.14 (2.98 to 24.36) | 9.30 (3.25 to 30.18) | 0.23 (0.03 to 1.11) | 0.71 (0.29 to 1.67) | 2.11 (1.30 to 3.44) |
Ensartinib | 1.51 (0.71 to 3.19) | 1.08 (0.13 to 7.93) | 2.67 (0.21 to 28.07) | NR | 0.51 (0.14 to 1.77) | 1.65 (0.57 to 4.74) |
Chemotherapy | 10.92 (5.87 to 20.54) | 76.80 (18.09 to 353.31) | NR | NR | 0.31 (0.11 to 0.91) | 1.87 (0.98 to 3.60) |
AEDC = discontinuation due to adverse events; BICR = blinded independent central review; CrI = credible interval; FE = fixed effect; IC-CR = intracranial complete response; IC-ORR = intracranial objective response rate; IC-PR = intracranial progressed response; ITT = intention-to-treat; NR = not reported; OR = odds ratio.
Source: Sponsor’s indirect treatment comparison.18
Critical Appraisal of the Sponsor’s ITC
The sponsor’s NMA compared the efficacy and safety of lorlatinib to crizotinib, alectinib, brigatinib, chemotherapy, ceritinib, and ensartinib. The doses for all treatments cross studies were the same, except for alectinib and ceritinib. For alectinib, doses of 300 mg and 600 mg were assessed using data from the ALEX and J-ALEX trials, respectively. For ceritinib, doses of 450 mg, 600 mg, and 750 mg were assessed using data from the ASCEND-8 and ASCEND-4 trials. The ASCEND-8 trial was a dose-ranging trial that assessed ceritinib at 3 different doses: 450 mg with a low-fat meal, 600 mg with a low-fat meal, and 750 mg fasted. Alectinib has been previously reviewed by CADTH for the same indication as this review for lorlatinib, and received a positive recommendation. Based on the previous CADTH review and approval by Health Canada, the most relevant dose for consideration for alectinib is 600 mg. This was confirmed by clinical experts consulted by CADTH for this review to be the standard dose of alectinib used in clinical practice. As 450 mg is the standard dose for ceritinib,34 the 450 mg dose of ceritinib is considered the most relevant comparison to lorlatinib. Overall, the clinical experts agreed that many of the treatments included in the sponsor’s ITC were not commonly used as first-line therapy for patients with ALK-positive metastatic NSCLC, including ensartinib and chemotherapy; of the listed treatments in the sponsor’s ITC, alectinib and brigatinib were the most important comparators to lorlatinib.
The sponsor’s ITC included mostly phase III RCTs. The ASCEND-8 trial was a phase I open-label, dose-ranging, active-controlled trial. The remaining trials included in the sponsor’s ITC were phase III open-label, active-controlled trials that reported PFS as the primary outcome. Inclusion of a phase I trial is likely to have introduced uncertainty into comparisons conducted within the NMA. The clinical experts consulted by CADTH also questioned the appropriateness of including the ASCEND-8 trial in the NMA due to its trial design, and agreed that only the ASCEND-4 trial, a phase III RCT comparing ceritinib at 750 mg to chemotherapy, should have been included in the sponsor’s ITC. Inclusion of the phase I trial may have broadened the evidence base of the sponsor’s ITC, potentially strengthening the network of the trials included in the NMA. However, potential introduction of biases due to the phase I trial should also be acknowledged.
Treatment crossover was allowed in some trials, which may introduce bias into the efficacy analyses of these trials and within the NMA. Crossover was not permitted in the CROWN, ALEX, ALESIA, J-ALEX, ASCEND-8, or eXalt3 trials. The sponsor noted that treatment crossover, which was reported in the ALTA-1L, ASCEND-4, PROFILE 1014, and PROFILE 1029 trials, affected the effect estimates of the NMA. Therefore, the analyses for OS were adjusted for crossover using published reports of adjusted OS data using the RPSFT method. The adjustment for crossover was considered appropriate to allow for more fair comparisons between treatments across trials. However, the RPSFT method is based on multiple assumptions, and its use may bias the estimated difference in OS toward the null, and such an estimation is still an artifact of a selected statistical model.
The baseline characteristics of patients were mostly balanced within and across trials. Based on input from clinical experts consulted by CADTH, the differences in baseline characteristics were not considered to have strongly affected any comparisons within the NMA. However, the clinical experts noted that the presence of brain metastasis at baseline was likely the most important baseline characteristic for consideration in the overall comparisons within the network. Comparisons of inclusion criteria of trials included in the sponsor’s ITC revealed some variations in previous treatments patients received before receiving trial treatments; patients were mostly treatment-naive, but 4 trials (J-ALEX, ALTA-1L, ASCEND-8, and eXalt3) allowed for enrolment of patients with prior treatment. The sponsor applied an 80% rule under which the majority of patients in the studies should have been treatment-naive. However, 24% to 41% of patients in the J-ALEX, ALTA-1L, ASCEND-8, and eXalt3 studies had received prior therapy, which may be another source of heterogeneity across the trials.
Important treatment-effect modifiers were identified by the sponsor, as they may have introduced heterogeneity in treatment comparisons. Heterogeneity was observed across the studies with respect to the presence of brain metastases at baseline, enrolment of patients with prior therapy, and enrolment of patients only from Asia. The sponsor explored the impact of these factors by conducting sensitivity analyses. The sensitivity analyses produced results similar to those of the primary analyses, which used intention-to-treat populations in the studies.
The sponsor conducted a risk of bias assessment of the trials included in the ITC. In general, the trials were assessed as having a low risk of bias. All studies were assessed by the sponsor to be of high quality regarding randomization, allocation concealment, baseline characteristics, patient withdrawals, outcome selection and reporting bias, and statistical analyses. Blinding was the only factor for which all studies had a high risk of bias, as all studies were open-label, which are at greater risk for bias in favour of investigational treatments. In addition, 3 studies (ALTA-1L, PROFILE 1014, and PROFILE 1029) were rated as having a medium risk of bias regarding allocation concealment. In general, based on the sponsor’s assessment, there was little concern over the quality of the studies included in the ITC. However, it is possible that the risk of bias assessment conducted by the sponsor was more lenient, as risk of bias assessments conducted by other authors on the ITCs, which included the same trials (reported in the following section), were more conservative.
The primary analysis of the sponsor’s NMA was conducted using fixed-effects models for the analyses of OS and PFS. The use of fixed-effects models assumes the same treatment effect for each study. The sponsor also conducted analyses using random-effects models, which are usually preferred when numerous studies are included in an NMA as they may better accommodate the heterogeneity across trials. However, as the number of trials included in each comparison within the sponsor’s NMA was small, with many including only 1 trial, the use of fixed-effects models was considered to be appropriate. In addition, based on lower (i.e., better) deviance information criterion values with fixed-effects models and wide CrIs of effect estimates resulting from the random-effects models, the fixed-effects models were preferred.
The primary end points of interest in the NMA were OS and PFS; the latter was assessed by BICR and definitions of both were consistent across trials. The sponsor also conducted NMAs for additional end points, including PFS per investigator assessment, intracranial progression-free survival, IC-TTP, ORR, IC-ORR, IC-CR, IC-PR, grade 3 and 4 AEs, and AEs resulting in treatment discontinuation; however, for many of these end points, the networks were limited in terms of the small number of studies included and the data available for comparisons. In particular, the networks for investigator-assessed PFS, OS exclusively assessed for first-line patients, OS among patients with brain metastasis, and IC-PR had missing data from 4 or more studies. The sponsor noted that interpretation of the data for these networks posed a challenge as the limited data available for these comparisons were not consistent with the analyses of other scenarios in the sponsor’s ITC.
The sponsor assessed the proportional hazards for OS and PFS by visually examining the proportionality in published Kaplan-Meier plots, concluding that the proportional hazards assumption was reasonable for both OS and PFS. While this is not a formal method of testing for the assumption, it was considered acceptable as they did not have access to the individual patient-level data of all studies included in the NMA.
The end points in the sponsor’s ITC allowed for comparisons of efficacy and safety. All studies included in the sponsor’s ITC reported PFS as the primary end point. When PFS was compared, lorlatinib was favoured over most treatments. Lorlatinib was not favoured in comparisons of OS. In the CROWN trial, OS data were not mature at the time of the analysis for PFS. It is likely that bias from immature OS data affected comparisons of this outcome in the NMA. For lorlatinib, only 26% of the OS events had occurred in the CROWN trial at the data cut-off date. Further, the OS assessment could have been significantly affected by crossover as mentioned previously. The sponsor also assessed 2 safety end points (total AEs of grade 3 and 4 AEs and AEs resulting in treatment discontinuation). However, these comparisons were not conducted separately for individual AEs of special interest, such as CNS effects. Therefore, it is possible that variations in certain AEs known to be common with specific treatments were not captured. In addition, AEs of lower grades were not captured. While lower-grade AEs may not require as intensive management compared to grade 3 or 4 AEs, they may still be relevant for consideration of patient’s overall tolerability to treatments, and consideration of only grade 3 or 4 AEs may underestimate the prevalence of certain AEs, which may be common but are more likely to present as grade 1 or 2.
While the sponsor did not include comparisons of HRQoL, it noted that the ALESIA, ASCEND-8, ALTA-1L, and J-ALEX trials did not report data for HRQoL end points.18 Lack of comparisons of HRQoL were likely due to lack of available data.
Methods of the Indirect Treatment Comparison by Ando et al. (2021)
Objectives
The primary aim of the NMA by Ando et al. (2021) was to compare the safety and efficacy of lorlatinib to alectinib in patients with ALK-positive advanced NSCLC who had not previously received an ALK inhibitor. The NMA also compared lorlatinib to brigatinib, ceritinib, crizotinib, and platinum-based chemotherapy.
Study Selection Methods
A literature search was conducted based on details in Table 46. After removal of duplicates, 1,051 studies were identified from the systematic literature search. Eight studies (PROFILE 1014, PROFILE 1029, ALEX, J-ALEX, ALESIA, ASCEND-4, ALTA-1L, and CROWN) were chosen for inclusion in the NMA based on the criteria used in the systematic literature review.
Indirect Treatment Comparison Analysis Methods
Details of the NMA conducted by Ando et al. (2021) are reported in Table 46.
Table 46: ITC Analysis Methods by Ando et al. (2021)
Analysis | Description |
|---|---|
ITC methods | A Bayesian NMA was conducted in accordance with a methodology developed by the National Center for Medical Research. Standard Bayesian modelling as described by Dias et al. were used; this modelling is dependent on assumptions of inconsistency and heterogeneity among studies included in the NMA |
Priors | A non-informative prior distribution prior was used. Gibbs sampling was used to evaluate the posterior distribution of the effect size based on the Markov chain Monte Carlo method |
Assessment of model fit | Not applicable |
Assessment of consistency | Heterogeneity was assessed using the I2 statistic; an I2 value of > 50% was considered to indicate a high degree of heterogeneity; a pairwise meta-analysis using a random-effects model was performed to calculate the I2 statistic among included studies with the same direct comparison |
Assessment of convergence | A total of 50,000 iterations were used with a burn-in of 10,000 iterations; The Brooks-Gelman-Rubin diagnostic method was used to assess for convergent diagnosis for all comparisons; convergence of models was assessed both visually and using Brooks-Gelman-Rubin diagnostics |
Outcomes | Progression-free survival Overall survival Objective response rate |
Sensitivity analyses | Sensitivity analyses were conducted based on the presence of conceptual heterogeneity among the studies included in the NMA; studies considered heterogenous were excluded |
Subgroup analysis | Patients with brain metastasis Patients with an Eastern Cooperative Oncology Group Performance Status of 0 to 1 Patients who were Asian and non-Asian |
Methods for pairwise meta-analysis | Hazard ratios, odds ratios, and relative risks were used to represent effect size, with corresponding 95% credible intervals |
NMA = network meta-analysis.
Source: Ando et al. (2021).21
Results of the ITC
Summary of the Included Studies
The following 8 trials were included in the NMA by Ando et al. (2021)21: PROFILE 1014, PROFILE 1029, ALEX, J-ALEX, ALESIA, ASCEND-4, ALTA-1L, and CROWN. A network of studies is depicted in Figure 21.
Figure 21: Network Diagram of Studies Included in the NMA by Ando et al. (2021)
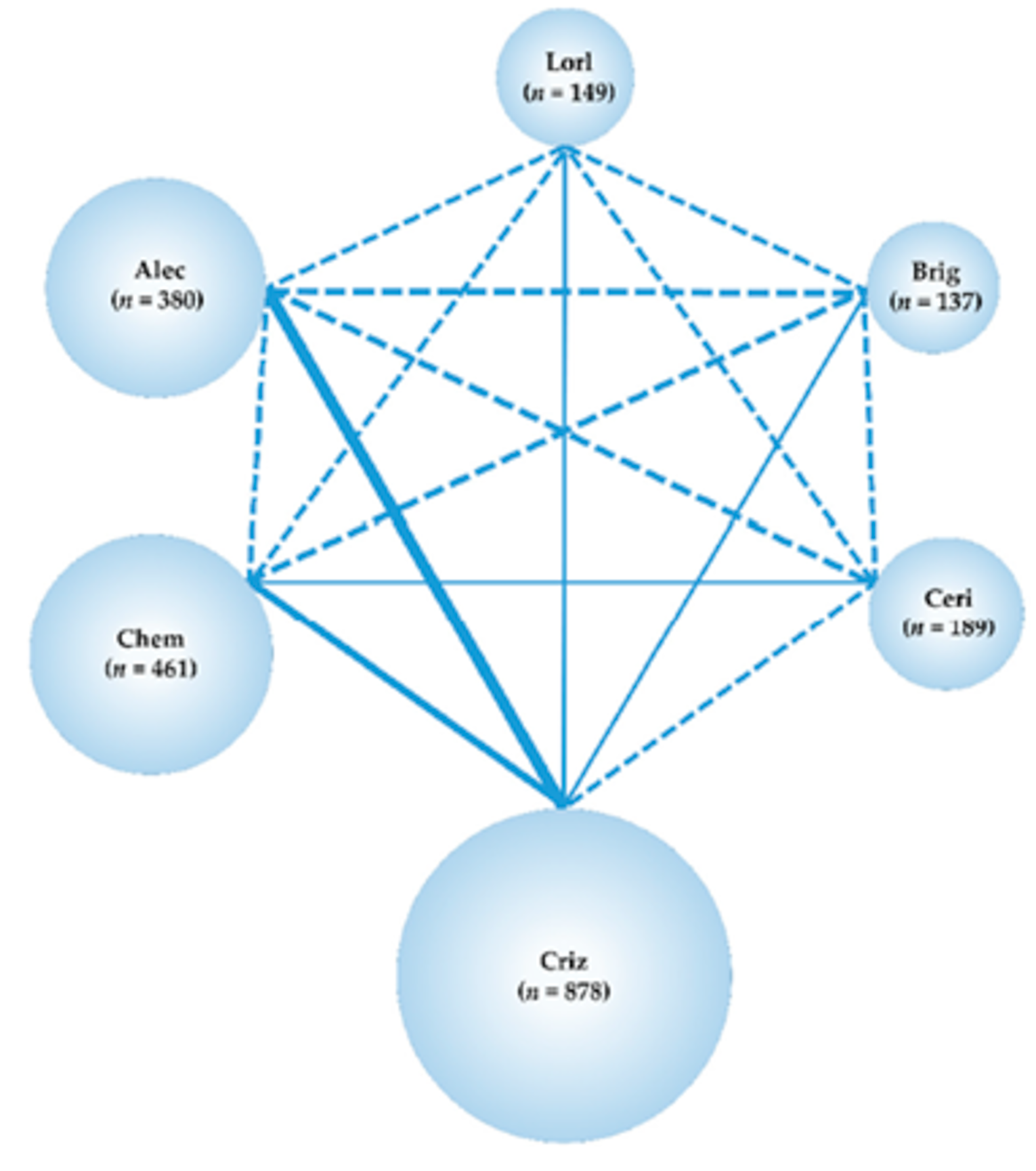
Alec = alectinib; Brig = brigatinib; Ceri = ceritinib; Chem = chemotherapy; Criz = crizotinib; Lorl = lorlatinib; NMA = network meta-analysis; RCT = randomized controlled trial.
Note: Network map of the 6 treatment groups (i.e., lorlatinib, brigatinib, alectinib, ceritinib, crizotinib, and chemotherapy). The RCTs included in the NMA are shown as solid lines, and the width of a solid line corresponds to the number of included trials. Dashed lines indicate that there are no head-to-head RCTs and that treatment comparisons will be attempted. N is the number of patients in each group.
Source: Ando et al. (2021).21
Study Characteristics
As these studies were also included in the sponsor’s ITC, a summary of trial characteristics is reported. Briefly, all trials enrolled adult patients aged 18 years or older (20 years for the J-ALEX trial) with metastatic ALK-positive NSCLC and an ECOG PS of 0, 1, or 2. There were slight differences in eligibility criteria of the studies regarding prior treatments. The PROFILE 1014, PROFILE 1029, ALEX, ALESIA, and CROWN trials enrolled patients who did not receive any systemic treatment for advanced disease, the ASCEND-4 study enrolled patients who were untreated with any systemic anticancer therapy, the J-ALEX trial enrolled patients who were chemotherapy-naive or who received 1 previous chemotherapy regimen, and the ALTA-1L trial enrolled patients who did not previously receive ALK-targeted therapy.
A summary of baseline characteristics is presented before Table 42.
Risk of Bias Assessment
Ando et al. (2021) assessed the quality of studies retrieved from their systematic literature review. Studies were assessed using the risk of bias tool 2 as recommended by the Cochrane Collaboration. The following parameters were used to assess for bias:
the randomization process
deviations from intended interventions
missing outcome data
measurement of the outcome
selection of the reported result.
These criteria were assessed as having either low risk, some concern, or high risk. Two researchers assessed the risk of bias independently, with conflicts resolved by a third researcher.
Regarding randomization, all studies were rated as having a low risk of bias, except for the PROFILE 1029 study, which was noted as having inadequate descriptions of details related to randomization and judged as having some concerns of bias related to this domain. All studies were rated as having some concern regarding deviations from intended interventions. All studies were rated as having a low risk of bias related to missing outcome data. All studies were rated as having some concern regarding bias in measurement of the outcome. Regarding bias in selection of the reported results, all studies were rated as having a low risk of bias. Overall, all studies were rated as having some concern, which was mainly due to trials being open-label and having bias due to deviations from intended interventions and bias in measurement of outcomes. As none of the studies were rated as having a high risk of bias, the authors concluded that the studies were considered to be of good quality.
Assessment of Proportional Hazards
The main outcomes of these studies were PFS and OS, which relied on the use of Cox proportional hazards models. The authors did not mention any assessment of the proportional hazards assumption.
Results
Progression-Free Survival
The results of the comparisons of treatments to lorlatinib for PFS conducted by Ando et al. (2021)21 are depicted in Figure 22. All comparisons favoured treatment with lorlatinib for PFS (versus chemotherapy: HR = 0.121; 95% CrI, 0.078 to 0.187; versus crizotinib: HR = 0.280; 95% CrI, 0.191 to 0.411; versus ceritinib: HR = 0.220; 95% CrI, 0.131 to 0.367; and versus brigatinib: HR = 0.572; 95% CrI, 0.326 to 0.997), except for alectinib (HR = 0.742; 95% CrI, 0.466 to 1.180).
Figure 22: Comparative Efficacy of Lorlatinib and Existing Therapeutics for PFS in Patients — Ando et al. (2021)
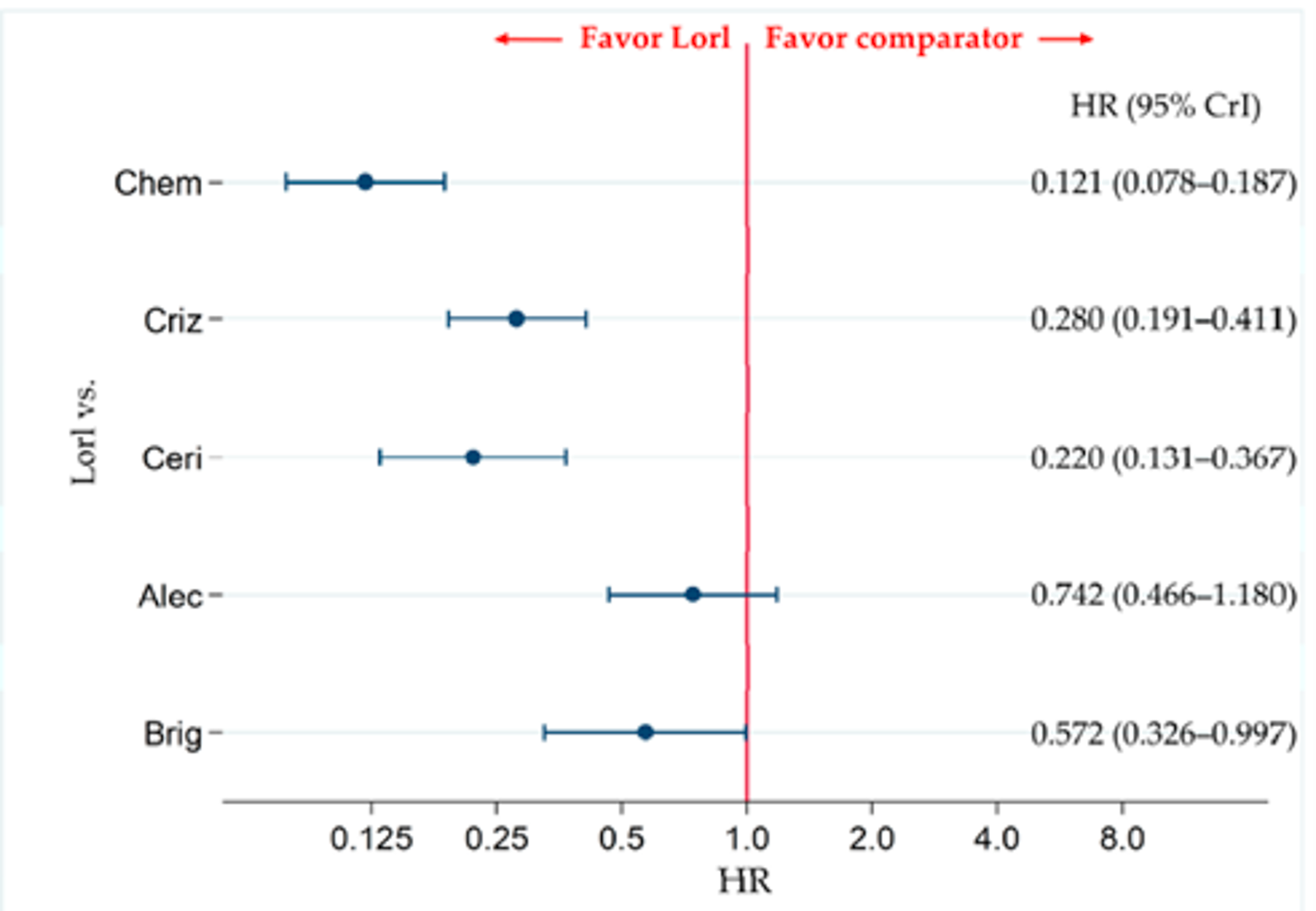
Alec = alectinib; Brig = brigatinib; Ceri = ceritinib; Chem = chemotherapy; Criz = crizotinib; CrI = credible interval; Lorl = lorlatinib; HR = hazard ratio; PFS = progression-free survival; vs. = versus.
Note: All 8 studies were included for analyzing PFS in the overall participant group. A comparison of PFS in ALK-p ALK inhibitor–naive advanced NSCLC patients treated with lorlatinib and each of the other 5 therapeutic agents including chemotherapy, crizotinib, ceritinib, alectinib, and brigatinib as comparator is presented. Comparisons are expressed as lorlatinib versus each of the comparators. Data are expressed as HRs and 95% CrIs.
Source: Ando et al. (2021).21
Subgroup analyses of Asian versus non-Asian patients: The PROFILE 1014, ASCEND-4, ALEX, ALTA-1L, and CROWN studies were included to analyze PFS in non-Asian patients. All studies were included to analyze Asian patients.21 In the subgroup of non-Asian patients, lorlatinib was favoured over all comparators: chemotherapy (HR = 0.101; 95% CrI, 0.052 to 0.193), crizotinib (HR = 0.190; 95% CrI, 0.112 to 0.324), ceritinib (HR = 0.229; 95% CrI, 0.107 to 0.489), alectinib (HR = 0.388; CrI, 0.195 to 0.769), and brigatinib (HR = 0.352; 95% CrI, 0.169 to 0.732). In the subgroup of Asian patients, lorlatinib was favoured over chemotherapy (HR = 0.196; 95% CrI, 0.107 to 0.363), crizotinib (HR = 0.471; 95% CrI, 0.270 to 0.818), and ceritinib (HR = 0.298; 95% CrI, 0.298; 95% CrI, 0.137 to 0.643), but not over alectinib (HR = 1.423; 95% CrI, 0.748 to 2.708) or brigatinib (HR = 1.148; CrI, 0.456 to 2.860).21
Presence of brain metastasis versus without brain metastasis: The assessment of PFS in the subgroup of patients with and without brain metastases included the PROFILE 1014, PROFILE 1029, ASCEND-4, ALEX, J-ALEX, ALTA-1L, and CROWN studies. The authors noted that the ALESIA study was not included in this subgroup analysis because the ALESIA trial only reported data for PFS for patients with brain metastasis based on assessment by an independent review committee. However, the analysis of PFS in the NMA by Ando et al. (2021)21 was based on investigator-assessed PFS. Due to discrepancies between PFS assessed by investigators and independent review committees, the ALESIA study was excluded from this subgroup analysis.21
In the subgroup of patients with brain metastasis, lorlatinib was favoured over chemotherapy (HR = 0.108; 95% CrI, 0.047 to 0.248), crizotinib (HR = 0.200; 95%CrI, 0.097 to 0.414), and ceritinib (HR = 0.155; 95% CrI, 0.060 to 0.398), but not over alectinib (HR = 0.542; 95% CrI, 0.229 to 1.285) or brigatinib (HR = 1.003; 95% CrI, 0.333 to 2.979). In the subgroup of patients without brain metastases, lorlatinib was favoured over chemotherapy (HR = 0.135; 95% CrI, 0.081 to 0.226), crizotinib (HR = 0.320; 95% CrI. 0.205 to 0.501), ceritinib (HR = 0.283; 95% CrI, 0.152 to 0.523) and brigatinib (HR = 0.445; 95% CrI, 0.227 to 0.864), but not over alectinib (HR = 0.705; 95% CrI, 0.402 to 1.234).21
An ECOG PS of 0 or 1 versus 2: The authors noted that a comparison of patients with an ECOG PS of 0 or 1 versus 2 was not possible as the CROWN and ASCEND-4 trials did not provide PFS data for the subgroups of patients with an ECOG PS of 2. Instead, the authors conducted a subgroup analysis of patients with an ECOG PS of 0 to 1.21 The PROFILE 1014, PROFILE 1029, ALEX, J-ALEX, ALESIA, ALTA-1L, and CROWN trials were included in the subgroup analysis of patients with an ECOG PS of 0 to 1 for PFS. In the subgroup of patients with an ECOG PS of 0 to 1, lorlatinib was favoured over chemotherapy (HR = 0.121; 95% CrI, 0.077 to 0.190) and crizotinib (HR = 0.280; 95% CrI, 0.188 to 0.416), but not over alectinib (HR = 0.774; 95% CrI, 0.486 to 1.233), brigatinib (HR = 0.562; 95% CrI, 0.310 to 1.025).21
Overall Survival
The results for the comparisons of treatments to lorlatinib for OS conducted by Ando et al. (2021)21 are depicted in Figure 23. Six of the 8 studies (PROFILE 1014, ASCEND-4, ALEX, ALESIA, ALTA-1L, and CROWN) were included in the analysis for OS. Lorlatinib was not favoured over any of the comparator treatments.21 Subgroup analyses for OS were not conducted by Ando et al., as no corresponding data for the subgroup analyses were reported.21
Figure 23: Comparative Efficacy of Lorlatinib and Existing Therapeutics for OS — Ando et al. (2021)
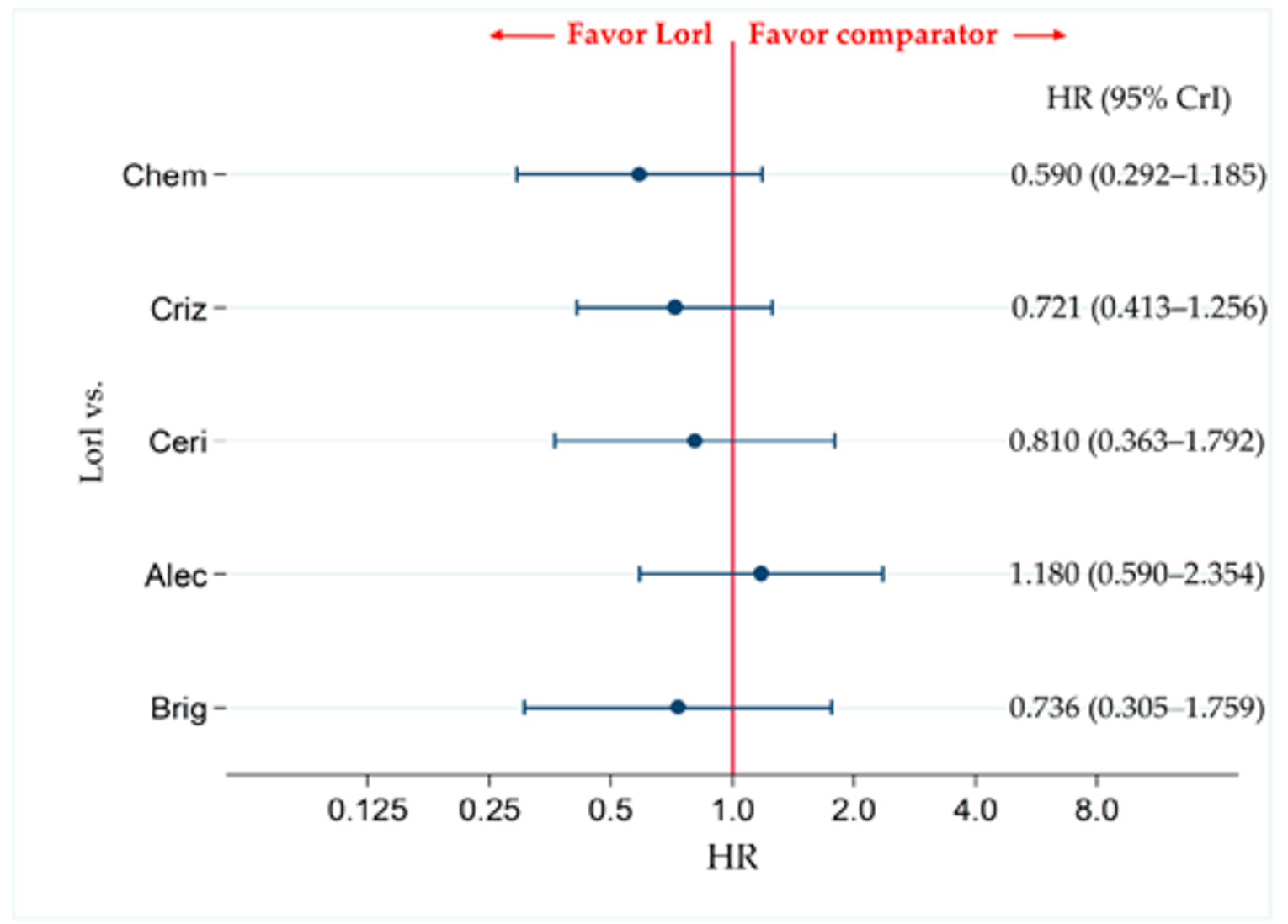
Alec = alectinib; Brig = brigatinib; Ceri = ceritinib; Chem = chemotherapy; Criz = crizotinib; CrI = credible interval; HR = hazard ratio; Lorl = lorlatinib; OS = overall survival; vs. = versus.
Note: A comparison of OS in ALK-p ALK inhibitor–naive advanced NSCLC patients treated with lorlatinib and each of the other 5 therapeutic agents including chemotherapy, crizotinib, ceritinib, alectinib, and brigatinib as comparator is presented. Comparisons are expressed as lorlatinib versus each of the comparator agents. Data are expressed as HRs and 95% CrIs.
Source: Ando et al. (2021).21
Objective Response Rate
The proportions of patients achieving an objective response (CR plus PR) was assessed by Ando et al. (2021)21 as a secondary efficacy end point. All 8 studies were included in this analysis. Lorlatinib was favoured over chemotherapy (OR = 10.49; 95% CrI, 5.583 to 19.61) and crizotinib (OR = 2.292; 95% CrI, 1.391 to 3.769), but not over alectinib (OR = 1.102; 95% CrI, 0.572 to 2.115), ceritinib (OR = 1.454; 95% CrI, 0.668 to 3.140), or brigatinib (OR = 1.424; 95% CrI, 0.699 to 2.886).21
Grade 3 or Higher Adverse Events
Grade 3 or higher AEs was the primary safety end point for the analysis by Ando et al. (2021).21 Data published were stated not to be sufficient for comparison between all treatments. Only 5 of the studies were included in this analysis: ALEX, J-ALEX, ALESIA, ALTA-1L, CROWN. A depiction of results from this analysis is presented in Figure 24. Both crizotinib (RR = 1.300; 95% CrI, 1.085 to 1.554) and alectinib (RR = 1.918; 95% CrI, 1.486 to 2.475) were favoured over lorlatinib. Neither lorlatinib nor brigatinib were favoured over each other (RR = 1.181; 95% CrI, 0.900 to 1.546).21
Figure 24: Comparative Safety of Grade 3 or Higher Adverse Events — Ando et al. (2021)
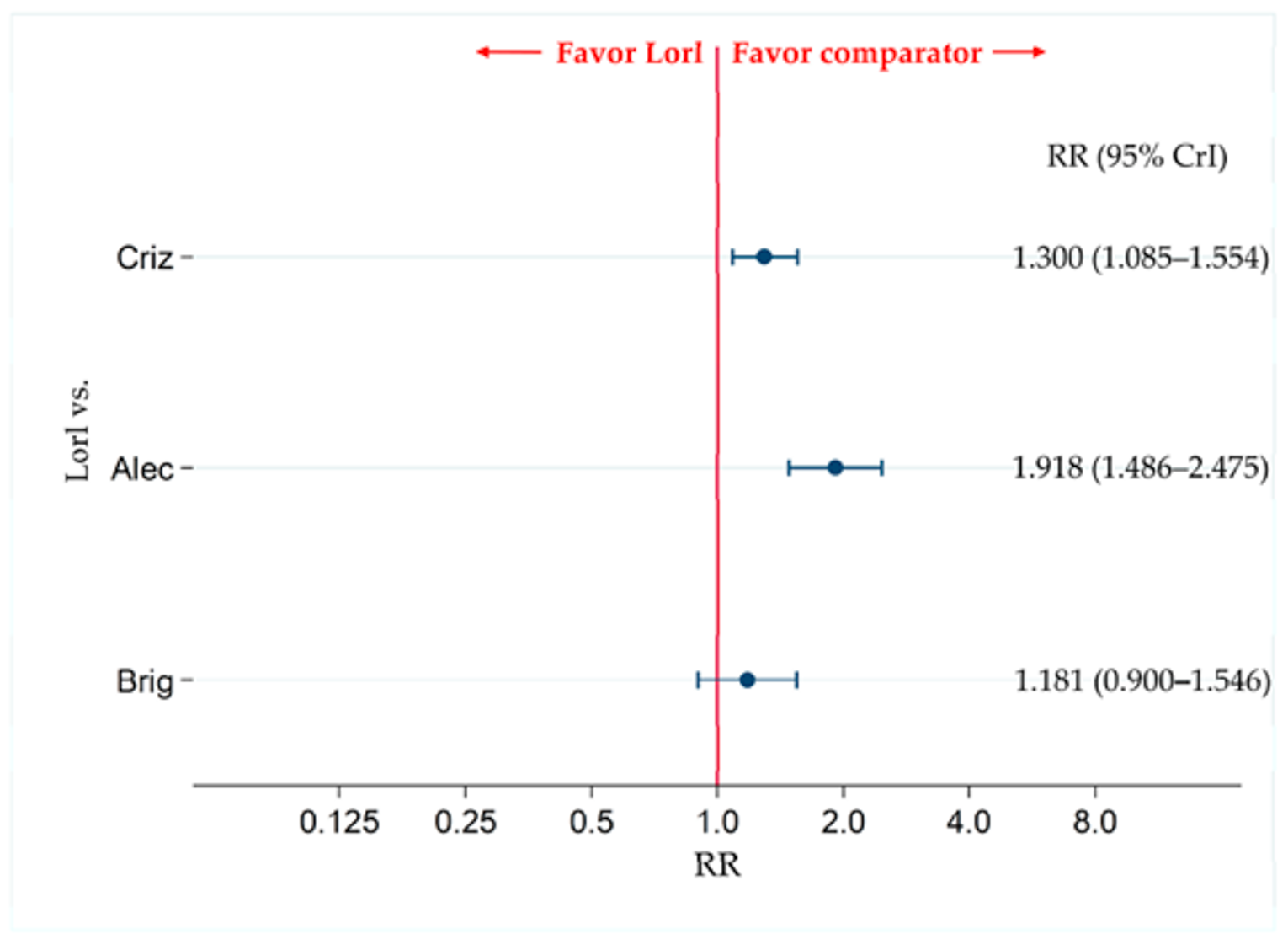
Alec = alectinib; Brig = brigatinib; Criz = crizotinib; CrI = credible interval; Lorl = lorlatinib; RR = relative risk; vs. = versus.
Note: Comparison of safety assessing grade ≥ 3 AEs for ALK-positive ALK inhibitor–naive advanced NSCLC patients treated with lorlatinib and each of the other 3 therapeutic agents, including crizotinib, alectinib, and brigatinib, as comparators is presented. Comparisons are expressed as lorlatinib versus each of the comparator agents. Data are expressed as RRs and 95% CrIs.
Source: Ando et al. (2021).21
Any-Grade Adverse Events
Five of the 8 studies were included in the analysis for AEs of any grade: ALEX, J-ALEX, ALESIA, ALTA-1L, and CROWN. No treatments were favoured between lorlatinib and alectinib (RR = 1.018; 95% CrI, 0.985 to 1.051), lorlatinib and brigatinib (RR = 1.041; 95% CrI, 1.001 to 1.083), or lorlatinib and crizotinib (RR = 1.010; 95% CrI, 0.985 to 1.035).21
Any-Grade Serious Adverse Events
Four studies were included in the analysis for SAES of any grade: ALEX, J-ALEX, ALESIA, and CROWN. No treatments were favoured between lorlatinib and alectinib (RR = 1.614; 95% CrI, 1.041 to 2.503) or lorlatinib and crizotinib (RR = 1.249; 95% CrI, 0.881 to 1.768).21
Grade 3 or Higher Serious Adverse Events
Two studies were included in the analysis for grade 3 or higher SAEs: CROWN and ALEX. No treatments were favoured between lorlatinib and alectinib (RR = 1.255; 95% CrI, 0.737 to 2.146) or lorlatinib and crizotinib (RR = 1.219; 95% CrI, 0.816 to 1.818).21
Nausea
All 8 studies were included in the analysis for any-grade nausea. Lorlatinib was favoured over chemotherapy (RR = 0.274; 95% CrI, 0.178 to 0.424) and crizotinib (RR = 0.280; 95% CrI, 0.186 to 0.421), and ceritinib (RR = 0.221; 95% CrI, 0.139 to 0.352), but not brigatinib (RR = 0.597; 95% CrI, 0.353 to 1.002) or alectinib (RR = 1.284; 95% CrI, 0.764 to 2.153).
In the analysis of grade 3 or higher nausea, 7 of the 8 studies were included: PROFILE 1014, ASCEND-4, ALEX, J-ALEX, ALESIA, ALTA-1L, and CROWN. Lorlatinib was not favoured over chemotherapy (RR = 0.211; 95% CrI, 0.011 to 3.840), crizotinib (RR = 0.322; 95% CrI, 0.032 to 3.197), ceritinib (RR = 0.415; 95% CrI, 0.018 to 9.110), alectinib (RR = 1.487; 95% CrI, 0.097 to 22.690) or brigatinib (RR = 0.645; 95% CrI, 0.036 to 11.140).
Diarrhea
All 8 studies were included in the analysis for any-grade diarrhea. Lorlatinib was favoured over crizotinib (RR = 0.410; 95% CrI, 0.290 to 0.580), ceritinib (RR = 0.273; 95% CrI, 0.142 to 0.522), and brigatinib (RR = 0.456; 95% CrI, 0.301 to 0.688). However, chemotherapy (RR = 2.127; 95% CrI, 1.304 to 3.456) and alectinib (RR = 1.869; 95% CrI, 1.167 to 2.988) were both favoured over lorlatinib.
In the analysis of grade 3 or higher diarrhea, 6 of the 8 studies were included: PROFILE 1014, ASCEND-4, ALEX, J-ALEX, ALTA-1L, and CROWN. Lorlatinib was not favoured over chemotherapy (RR = 7.531; 95% CrI, 0.291 to 189.60), crizotinib (RR = 1.928; 95% CrI, 0.173 to 21.020), ceritinib (RR = 1.635; 95% CrI, 0.045 to 57.010), alectinib (RR = 11.620; 95% CrI, 0.482 to 275.70), or brigatinib (RR = 2.874; 95% CrI, 0.142 to 56.560).
Increased Alanine Transaminase
Due to a lack of data, only 5 of 8 studies were included in the analysis of any-grade and grade 3 or higher increase in ALT: ALEX, J-ALEX, ALESIA, ALTA-1L, and CROWN. Regarding any-grade increase in ALT, lorlatinib was favoured over crizotinib (RR = 0.520; 95% CrI, 0.342 to 0.786), but not over alectinib (RR = 0.869; 95% CrI, 0.538 to 1.399) or brigatinib (RR = 0.866; 95% CrI, 0.476 to 1.563). Regarding grade 3 or higher increase in ALT, lorlatinib was not favoured over crizotinib (RR = 0.639; 95% CrI, 0.181 to 2.220), alectinib (RR = 2.447; 95% CrI, 0.584 to 10.18), or brigatinib (RR = 4.248; 95% CrI, 0.639 to 27.77).
Increased Aspartate Transaminase
Four of 8 studies were included in the analysis of any-grade and grade 3 or higher increase in AST: ALEX, J-ALEX, ALTA-1L, and CROWN. Regarding any-grade increase in AST, lorlatinib was favoured over crizotinib (RR = 0.510; 95% CrI, 0.315 to 0.819), but not over alectinib (RR = 1.089; 95% CrI, 0.591 to 2.006) or brigatinib (RR = 0.553; 95% CrI, 0.291 to 1.046). Regarding grade 3 or higher increase in AST, lorlatinib was not favoured over crizotinib (RR = 0.569; 05% CrI, 0.137 to 2.135), alectinib (RR = 1.269; 95% CrI, 0.254 to 6.300), or brigatinib (RR = 2.268; 95% CrI, 0.271 to 18.61).
Pneumonitis
In the analysis of both any-grade and grade 3 or higher pneumonitis, only 2 of the 8 trials could be included: the ALEX and CROWN trials. Regarding any-grade pneumonitis, lorlatinib was not favoured over either crizotinib (RR = 0.946; 95% CrI, 0.135 to 6.569) or alectinib (RR = 1.881; 95% CrI, 0.145 to 25.02). Similarly, regarding grade 3 or higher pneumonitis, lorlatinib was not favoured over either crizotinib (RR = 0.318; 95% CrI, 0.011 to 8.930) or alectinib (RR = 2.250; 95% CrI, 0.029 to 177.2).
Critical Appraisal of the Indirect Treatment Comparison
In general, baseline characteristics of patients were balanced. Some variations in baseline characteristics were noted across trials. For example, a few trials included patients who had previously received treatment for ALK-positive metastatic NSCLC. In addition, the authors noted that some trials enrolled exclusively Asian patients, and that variations were evident in patients with brain metastases at baseline. However, in general, the authors suggested that heterogeneity in baseline characteristics across trials was low but non-negligible in its impact on the comparisons within the ITC.
Ando et al. (2021) also conducted an analysis of heterogeneity using the I2 statistic for studies that compared the same treatments. The analysis revealed an I2 value of 0.0% (P = 0.583) for the PROFILE 1014 and PROFILE 1029 studies, which both compared crizotinib to chemotherapy; the I2 value suggested no difference in the between-study heterogeneity. The comparison between alectinib and crizotinib was assessed through 3 studies, (ALEX, J-ALEX, and ALESIA); the I2 value was 65.0% (P = 0.057), which indicated a significant amount of between-study heterogeneity. The heterogeneity across these trials comparing alectinib and crizotinib may be partly due to the differences in baseline characteristics, as the ALEX trial enrolled patients who previously received chemotherapy, and may also be due to different doses of alectinib, the J-ALEX trial administered alectinib at 300 mg, and the ALEX and ALESIA studies administered alectinib at 600 mg. It is possible that a large amount of heterogeneity may introduce uncertainty into estimates obtained from the NMA.
Ando et al. (2021) conducted subgroup analyses to determine the effect of certain effect modifiers on the efficacy of lorlatinib when compared to other treatments. Subgroup analyses included subgroups of patients who were Asian versus non-Asian, with brain metastasis versus without brain metastasis, and with an ECOG PS of 0 or 1 versus 2. Due to limited data for OS, subgroup analyses were stated to only be possible for PFS. Analyses revealed the efficacy of lorlatinib may differ among specific subgroups. However, as the trials included in the NMA were not powered for analyses in specific subgroups, results of subgroup analyses in the NMA should be interpreted with caution.
As discussed previously, the NMA by Ando et al. (2021) included both the ALEX and J-ALEX trials, which compared alectinib to crizotinib. Alectinib was administered to patients at 600 mg in the ALEX trial, but 300 mg in the J-ALEX trial. The authors conducted the NMA while considering the efficacy of both doses of alectinib to be equivalent, and both trials provided data for comparisons that involved alectinib. Because the Health Canada–approved dose of alectinib, and the dose used in Canadian clinical practice, is 600 mg, it may not be appropriate to consider the 2 different doses of alectinib as equivalent. Data for the 2 doses of the treatment may introduce uncertainty into comparisons that involve alectinib, as the safety and efficacy of alectinib at different doses may not be equivalent.
Sensitivity analyses for PFS were conducted by Ando et al. (2021) to assess the impact of heterogeneity observed in the trials included in their NMA. Sensitivity analyses included removal of studies that included patients who previously received chemotherapy, including the ALEX and ALTA-1L trials. The results of the sensitivity analyses were consistent with the primary analysis of the NMA (results of the sensitivity analyses are not reported here). The authors concluded that, based on these results, receiving prior treatment with chemotherapy would not affect the final conclusions obtained from the NMA. Consultation with clinical experts for this review also suggested that efficacy of a TKI would not likely be affected by prior treatment with chemotherapy.
Ando et al. (2021) conducted random-effects modelling for their NMA. Random-effects models may be more useful in accounting for heterogeneity, which may be present among patients across trials. However, a random-effects model may also overestimate the error. The overall size of the network for this NMA was limited, and few studies were used to inform each treatment comparison. Random-effects models may be useful when many studies are present, as there is likely more heterogeneity to capture in larger networks. In this instance, the use of a random-effects model may have introduced greater uncertainty to the estimates. In fact, this may be observed in the wide CrIs, which were associated with effect estimates for both efficacy and safety comparisons.
The risk of bias was assessed for studies included in the NMA. While most studies were reported to have a low risk of bias in most categories using the risk of bias tool 2, all studies were noted to have some concern for bias, although most of the concern was related to the open-label designs of all of the trials. None of the studies were reported to have a high risk of bias. While it is possible that biases may have affected each study, it is unlikely that these biases would greatly affect the comparisons made within the NMA.
Ando et al. (2021) assessed both efficacy and safety outcomes. In particular, the authors conducted an analysis of safety end points that assessed AEs of any grade and grade 3 or higher. In addition, the authors compared AEs that may be of particular interest to patients and clinicians, including diarrhea, nausea, increased AST and/or ALT, and pneumonitis. Consideration of certain AEs may be important for both patients and clinicians, as tolerance to treatments may play an important role in choice of therapy. The authors did not conduct comparisons of HRQoL in their NMA, likely due to a lack of available data.
Methods of the Indirect Treatment Comparison by Wang et al. (2021)
Objectives
The aim of the ITC conducted by Wang et al. (2021)20 was to evaluate the efficacy and safety of lorlatinib, alectinib, and brigatinib for ALK-positive advanced NSCLC in the first line.
Study Selection Methods
A literature search was based on details in Table 36. Studies were screened for relevance by 2 reviewers independently. A total of 412 records were retrieved from the literature search. After title and abstract and then full-text screening, 5 studies were included.
Indirect Treatment Comparison Analysis Methods
Details of the methodology for the NMA conducted by Wang et al. (2021)20 can be found in Table 47.
Table 47: ITC Analysis Methods — Wang et al. (2021)
Analysis | Description |
|---|---|
ITC methods | Analyses were conducted using Bayesian methodology; a normal likelihood with identity link model was applied for outcomes of OS and PFS; summary measures (i.e., log HRs and SEs) from studies were used; Markov chain Monte Carlo methods were used to estimate HRs and 95% CrIs for OS and PFS; data for these estimations were derived from HRs and associated 95% CIs reported in the trials |
Priors | Not reported |
Assessment of model fit | Not reported |
Assessment of consistency | Not reported |
Assessment of convergence | Not reported |
Outcomes | OS PFS |
Sensitivity analyses | None |
Subgroup analysis | Age (< 65 years vs. ≥ 65 years) Sex (female vs. male) Race (Asian vs. non-Asian) Smoking status (never smoker vs. current or former smoker) |
Methods for pairwise meta-analysis | HRS and RRs were used to represent effect size with corresponding 95% CrIs |
CrI = credible interval; HR = hazard ratio; OS = overall survival; PFS = progression-free survival; RR = relative risk; SE = standard error; vs. = versus.
Source: Wang et al. (2021).20
Results of the Indirect Treatment Comparison
Summary of the Included Studies
The following trials were included in the ITC conducted by Wang et al. (2021)20: ALTA-1L, ALEX, CROWN, ALESIA, and J-ALEX. Trial and baseline characteristics of these studies have been described above. The network diagram of the NMA is depicted in Figure 25.
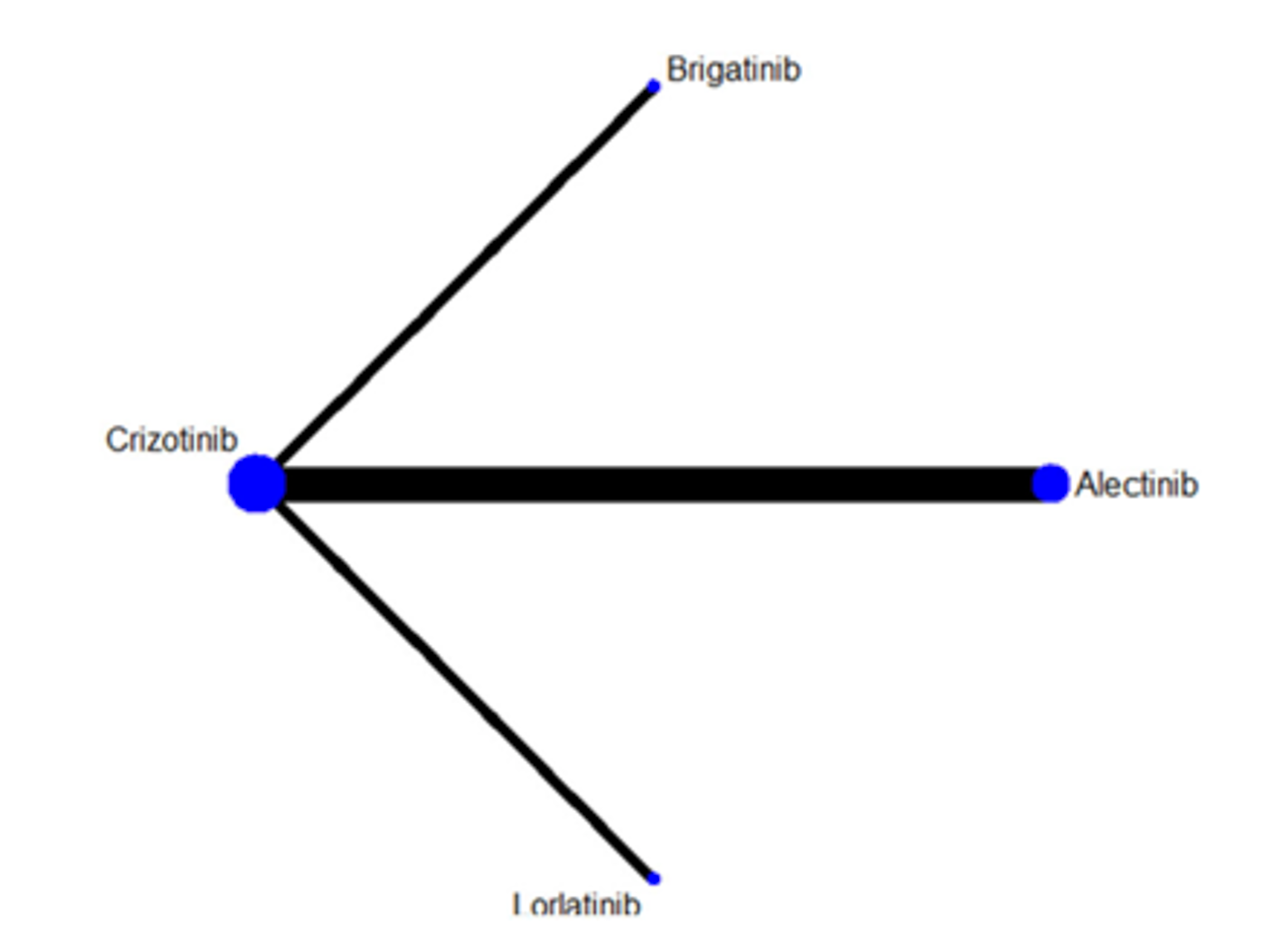
Risk of Bias
Wang et al. (2021)20 conducted a quality assessment of studies included in their NMA using methods and categories described in the Cochrane Collaboration Handbook. Two reviewers conducted the quality assessment independently. Disagreements were resolved through a group discussion until a consensus was reached. The quality assessment involved 7 domains, including sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting bias, and other bias. Categories were assigned a judgment of high, low, or unclear risk.
All trials were rated as having a low risk of bias regarding randomization, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Regarding allocation concealment, the ALESIA, ALEX, AND J-ALEX trials were assessed as having a low risk of bias; however, the ALTA-1L and CROWN trial were assessed as having a high risk of bias.20 All trials were considered to have a high risk of bias regarding blinding, as they were all open-label trials.
Results
Progression-Free Survival
The results of the fixed-effects NMA for PFS are reported in Figure 26. Results indicated that lorlatinib was favoured over both brigatinib and alectinib among patients who were ALK inhibitor– and chemotherapy-naive. Lorlatinib was favoured over brigatinib among patients who were ALK inhibitor–naive but was not favoured over alectinib. A subgroup analysis for PFS among patients who were ALK inhibitor–naive is depicted in Figure 27. In general, subgroup analysis revealed that neither lorlatinib nor alectinib was favoured in the following subgroups: age, sex, smoking status, ECOG PS, and brain metastases. However, among non-Asian patients, lorlatinib was favoured over alectinib. Subgroup analysis revealed that neither lorlatinib nor brigatinib were favoured in the sex and smoking status subgroups. However, lorlatinib seemed to be favoured over brigatinib among patients who were younger than 65 years, Asian or non-Asian, with an ECOG PS of 0 or 1, and without CNS metastasis.20
Figure 26: Network Meta-Analysis for PFS — Wang et al. (2021)
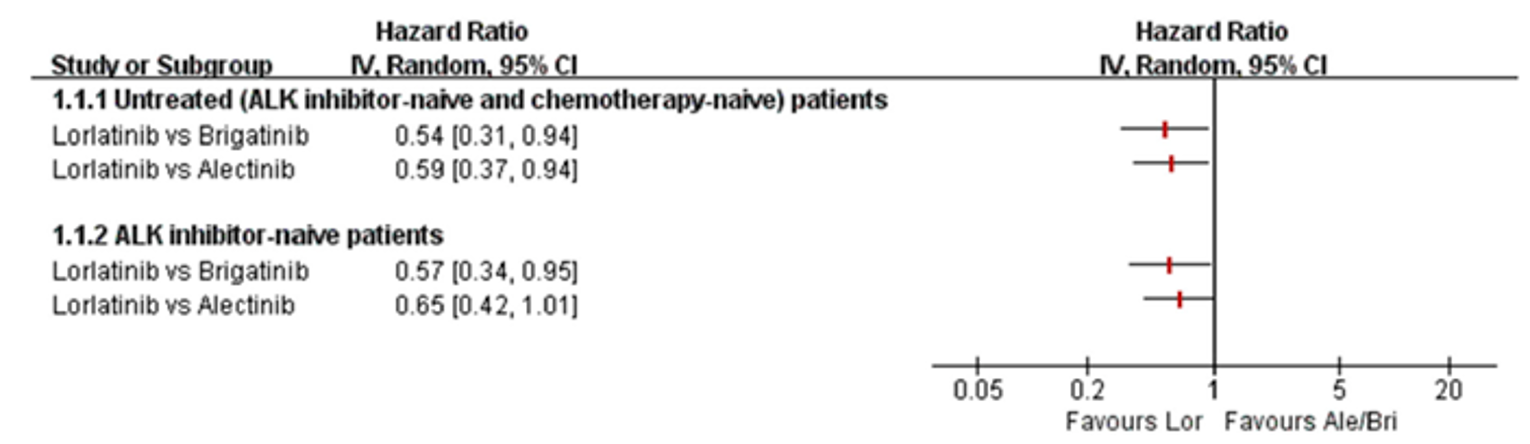
Ale = alectinib; ALK = anaplastic lymphoma kinase; Bri = brigatinib; CI = confidence interval; Lor = lorlatinib; vs = versus.
Source: Wang et al. (2021).20
Figure 27: Subgroup Analysis Among Patients Who Were ALK Inhibitor–Naive — Wang et al. (2021)
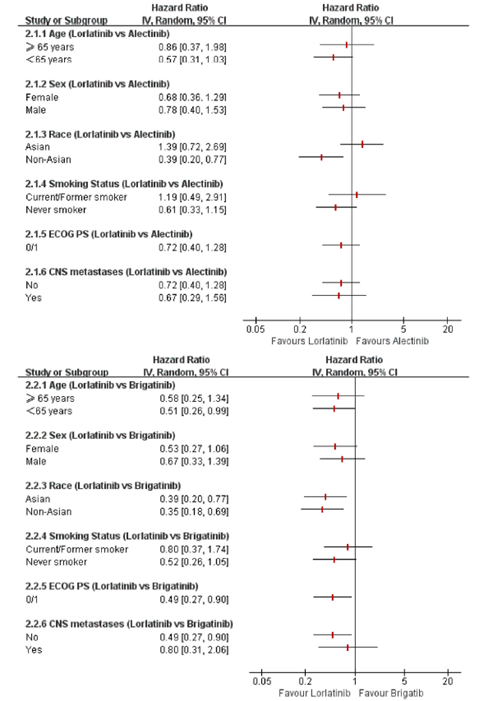
ALK = anaplastic lymphoma kinase; CI = confidence interval.
Source: Wang et al. (2021).20
Response Rate
Wang et al. (2021)20 reported finding no differences between lorlatinib, alectinib or brigatinib in overall confirmed response rate and intracranial confirmed response rate analysis.
Overall Survival
Wang et al. (2021)20 reported finding no differences between lorlatinib, alectinib or brigatinib in OS.
Safety
Wang et al. (2021)20 conducted an analysis for safety involving assessments of AEs, AEs leading to treatment discontinuation, and AEs leading to dose reduction. In all cases, none of the treatments (lorlatinib, alectinib, and brigatinib) were favoured over another.
Critical Appraisal of the ITC
As the studies included in the ITC conducted by Wang et al. (2021) were included in the sponsor’s ITC, critical appraisal of baseline characteristics has already been described. Briefly, variations were noted in the types of patients enrolled in the trials. For example, some patients were noted to be naive to systemic treatments for metastatic NSCLC; however, some patients may have received prior treatment with an ALK inhibitor and/or chemotherapy. In addition, there were some variations in the proportion of Asian and non-Asian patients. The authors did not discuss the impact of heterogeneity in baseline characteristics, and no formal assessment of heterogeneity was reported.
The subgroup analyses conducted by Wang et al. (2021) assessed the impact of baseline characteristics on treatment effect on patients who had not previously received an ALK inhibitor. The subgroup analyses may be useful in identifying potential effect modifiers affecting efficacy or lorlatinib and other comparators. However, the subgroup analyses were based on data obtained from the publications of the trials included in the NMA, which were not powered for detection of treatment effects. Subgroup analyses in the NMA should therefore be interpreted with caution.
Wang et al. (2021) conducted Bayesian modelling using fixed effects in their NMA. Random effects may be useful to account for heterogeneity that is present across trials included in an NMA. However, the error estimated within random-effects models may be overestimated if only a few trials are included in an NMA. The use of fixed-effects models was considered appropriate by the CADTH team due to the low number of studies included in the NMA and the limited number of trials informing each comparison.
Similar to the NMA conducted by Ando et al. (2021), Wang et al. (2021) included both the ALEX and J-ALEX trials, which assessed alectinib as an intervention. However, the ALEX trial assessed alectinib at 600 mg, whereas the J-ALEX trial assessed alectinib at 300 mg. The Health Canada–approved dose of alectinib, and the dose used in Canadian clinical practice, is 600 mg. Data for the 2 different doses of the treatment may introduce uncertainty to comparisons that involve alectinib, as the safety and efficacy of alectinib at different doses may not be equivalent.
The Wang et al. (2021) NMA assessed the following efficacy outcomes: PFS, OS, response rates, and intracranial response rates. As PFS was the primary end point in all trials included in the NMA, the primary results presented in the publication by Wang et al. (2021) were based on PFS. Results for other efficacy end points (i.e., OS and response rates) were also briefly discussed; however, the results were not available in the publication. As OS was not mature at the time of the data cut-off for the CROWN trial, comparisons to lorlatinib for OS made in the NMA were likely affected by bias. Comparisons for OS would likely be more compelling with more mature data. Wang et al. (2021) also assessed safety end points, including AEs, AEs resulting in treatment discontinuation, and AEs leading to dose reduction; the results for safety analyses were also not presented in the publication. However, inclusion of such analyses was considered beneficial as safety end points may be important for patients and clinicians when choosing a therapy. Outcomes involving HRQoL were not assessed, likely due to a lack of available data.
Cox proportional hazards models were used for analyses of PFS and OS in the trials included in the NMA. However, no assessment of whether the proportional hazards assumptions were valid were reported by the authors. Violation of the proportional hazards assumption may introduce uncertainty into analyses conducted in the NMA. As no data were reported regarding assessment of the assumption, it is not possible to know the impact of this decision.
Methods of the ITC (Chuang et al. [2021])
Objectives
The aim of the ITC conducted by Chuang et al. (2021)19 was to evaluate the efficacy — in terms of PFS, response rate, and safety, and in terms of grade 3 to 5 AEs — of ALK inhibitors for the first-line treatment of ALK-positive patients using published phase III RCTs.
Study Selection Methods
A literature search was conducted based on details reported in Appendix 3. After removal of duplicates, 918 studies were identified using the comprehensive literature search. Six studies were chosen for inclusion in the NMA.
ITC Analysis Methods
Details of the methodology used for the ITC conducted by Chuang et al. (2021) are reported in Table 48.
Table 48: ITC Analysis Methods — Chuang et al. (2021)
Analysis | Description |
|---|---|
ITC methods | The NMA was conducted using frequentist methods; a contrast-based analysis was performed for multiple treatment comparisons using the restricted maximum likelihood approach in which a treatment contrast (e.g., treatment A vs. treatment B) was used as an observation unit in the network map; different parameters were used to contrast 2 treatments (A and B) in RCTs that contained the same 2 treatments (A and B) in other RCTs; this was done to split the unit; parameters were estimated jointly within the same model to determine the difference; fixed-effects models were used; the same true effect size was then assumed for all trials in the study |
Priors | NA |
Assessment of model fit | NA |
Assessment of consistency | Not reported |
Assessment of convergence | NA |
Outcomes | Progression-free survival Objective response rate Grade ≥ 3 adverse events |
Sensitivity analyses | None |
Subgroup analysis | Progression-free survival among patients without brain metastases Progression-free survival among patients with brain metastases |
Methods for pairwise meta-analysis | Hazard ratios and relative risks were used to represent effect size with corresponding 95% credible intervals |
NA = not applicable; NMA = network meta-analysis; RCT = randomized controlled trial.
Source: Chuang et al. (2021).19
Results of the Indirect Treatment Comparison
Summary of the Included Studies
The following trials were included in the NMA by Chuang et al. (2021): CROWN, ALTA-1L, ALEX, J-ALEX, ALESIA, eXalt3. The network of studies included in the NMA is depicted in Figure 28. These studies were included in the sponsor’s ITC and are summarized here. Due to a lack of available information, ensartinib was not included in the network for safety and subgroup analyses.
Figure 28: Network Diagrams for Comparisons of PFS, ORR, and Grade 3 to Grade 5 AEs in the NMA by Chuang et al. (2021)
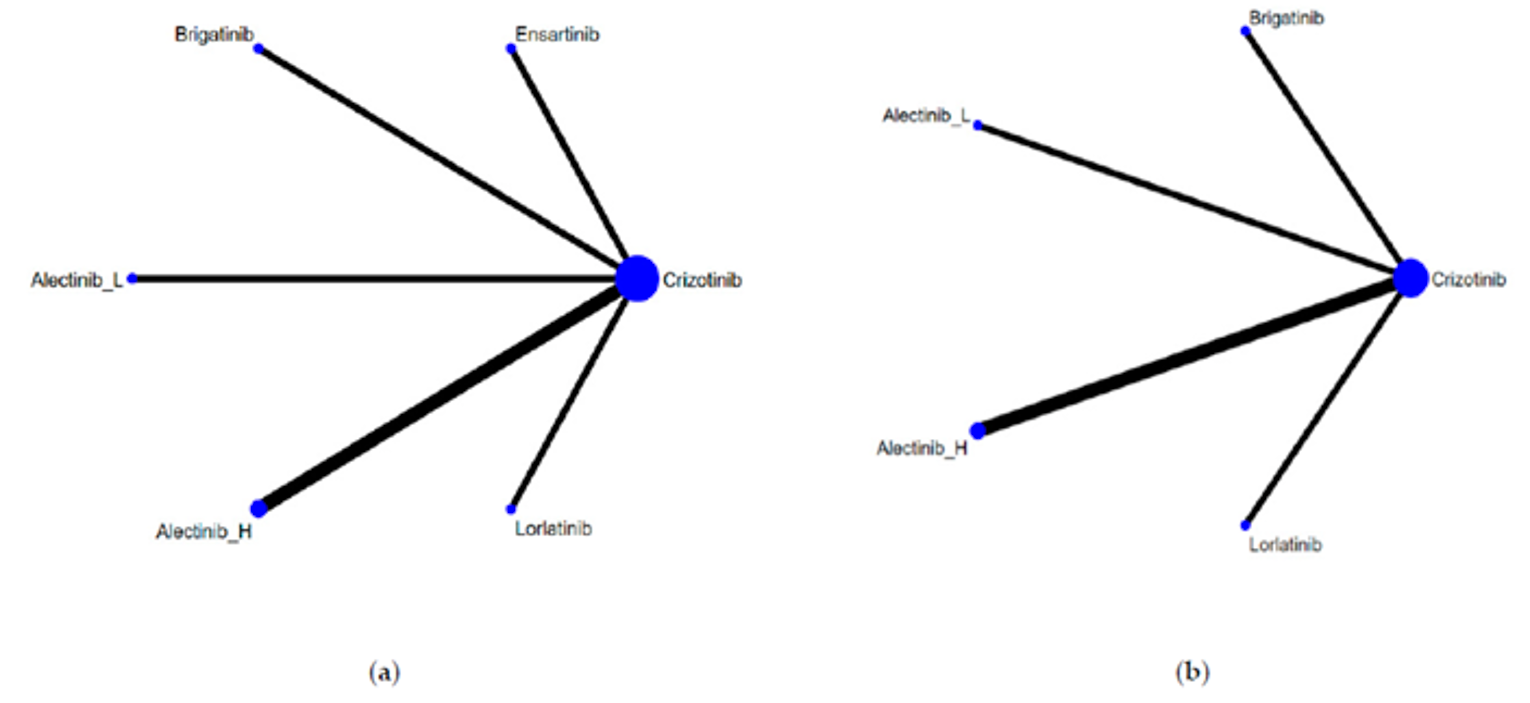
AE = adverse event; Alectinib_H = alectinib high dose (600 mg); alectinib_L = alectinib low dose (300 mg); NMA = network meta-analysis; ORR = objective response rate; PFS = progression-free survival.
Note: Network constructions for comparisons in PFS, ORR, and grade 3 to 5 AEs: (a) Network constructions for PFS and ORR; (b) Network constructions for PFS subgroup analysis and grade 3 to 5 AEs.
Source: Chuang et al. (2021).19
Risk of Bias Assessment
Chuang et al. (2021) assessed the risk of bias using the risk of bias tool and the following parameters: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. These listed criteria were assessed as having a low, unclear, or high risk of bias.
In general, based on the assessment by Chuang et al. (2021), there was an unclear risk of bias among studies. The ALESIA, ALEX, and J-ALEX trials were rated as having a low risk of bias regarding random sequence generation, while the ALTA-1L, CROWN, and eXalt3 trials were rated as having an unclear risk of bias. Similarly, the ALESIA, ALEX, and J-ALEX trials were rated as having a low risk of bias regarding allocation concealment, while the ALTA-1L, CROWN and eXalt3 trials were rated as having an unclear risk of bias. All studies were rated as having a high risk of bias regarding blinding as all trials were open-label. All studies were rated as having a low risk of bias regarding blinding of outcome assessment; this was due to the use of BICR for assessment of end points in trials. All studies were rated as having a low risk of bias regarding incomplete outcome data, except for the eXalt3 trial, which was rated as having an unclear risk of bias. The ALTA-1L and CROWN trials were rated as having a low risk of bias regarding selective reporting; the remaining trials (ALESIA, ALEX, J-ALEX, and eXalt3) were rated as having an unclear risk of bias. All studies were rated as having an unclear risk of bias regarding other biases.
The eXalt3 trial was rated as having an unclear risk of bias for most criteria on the risk of bias tool. The authors noted that this was mainly due to a lack of published data on the trial; information was obtained from the protocol available on clinicaltrials.gov as limited data were published in the report from the 2020 annual meeting of the World Conference on Lung Cancer. The unclear risk of bias among most trials for sequence generation, allocation concealment, and selective reporting was reported to be due to a lack of detailed information.
Results
A summary of results for PFS and ORR conducted using the NMA is provided in Figure 29.
Figure 29: Summary of Effects for PFS and ORR — Chuang et al. (2021)

Alectinib_H = alectinib high dose (600 mg); alectinib_L = alectinib low dose (300 mg); HR = hazard ratio; CI = confidence interval; vs = versus.
Note: (a) Pairwise comparisons for PFS; (b) pairwise comparisons for ORR; (c) pairwise comparisons for PFS among patients with baseline brain metastases; (d) pairwise comparisons for PFS among patients without baseline brain metastasis.
Source: Chuang et al. (2021).19
Progression-Free Survival
Lorlatinib was favoured over crizotinib (HR = 0.28; 95% CrI, 0.19 to 0.41), ensartinib (HR = 0.54; 95% CrI, 0.32 to 0.92), and brigatinib (HR = 0.57; 95% CrI, 0.32 to 0.95), but not over alectinib at 600 mg (HR = 0.68; 95% CrI, 0.42 to 1.08) or 300 mg (HR = 0.76; 95% CrI, 0.34 to 1.28).
Subgroup Analyses
Subgroup analyses were conducted among patients with and without brain metastases. Results of the subgroup analyses suggested that, among patients with brain metastases, lorlatinib was favoured over crizotinib (HR = 0.25; 95% CI, 0.14 to 0.44), but not over brigatinib (HR = 0.79; 95% CI, 0.33 to 1.94), or alectinib at 600 mg (HR = 0.75; 95% CI, 0.34 to 1.66) or 300 mg (HR = 0.79; 95% CI, 0.33 to 1.94). Among patients without brain metastases, lorlatinib was favoured over crizotinib (HR = 0.32; 95% CI 0.20 to 0.51) and brigatinib (HR = 0.49; 95% CI, 0.27 to 0.91), but not over alectinib at 600 mg (HR = 0.74; 95% CI, 0.42 to 1.30) or 300 mg (HR = 0.82; 95% CI, 0.82 to 1.66).
Objective Response Rate
For ORR, lorlatinib was favoured over crizotinib (RR = 1.31; 95% CI, 1.11 to 1.55). Lorlatinib was not favoured over ensartinib (RR = 1.18; 95% CI, 0.94 to 1.48), brigatinib (RR = 1.11; 95% CI, 0.94 to 1.48), or alectinib at 600 mg (RR = 1.16; 95% CI, 0.96 to 1.40) or 300 mg (RR = 1.13; 95% CI, 0.92 to 1.39).
Grade 3 or Higher AEs
In terms of safety, lorlatinib had a greater risk of grade 3 or higher AEs compared to crizotinib (RR = 1.27; CrI 1.07 to 1.52), and alectinib at 600 mg (RR = 1.62; 95% CrI, 1.24 to 2.12) and 300 mg (RR = 2.09; 95% CrI, 1.48 to 2.95), but not brigatinib (RR = 1.07; 95% CrI, 0.84 to 1.37).
Critical Appraisal of the Indirect Treatment Comparison
All studies included in the ITC by Chuang et al. (2021)19 were included in the sponsor’s ITC. The critical appraisal of baseline characteristics has been described. Heterogeneity across the studies related to study protocols, patient baseline characteristics and response evaluation bias was acknowledged by Chuang et al. (2021).19 Variations in patients who were treatment-naive, the presence of brain metastases, and the proportion of Asian and non-Asian patients should be considered. The authors described that trials that enrolled Asian populations, including the J-ALEX and ALESIA trials, demonstrated improved efficacy compared to crizotinib and that further investigations were warranted to understand the disease status and environments of Asian and Western populations.19 The authors noted that their ITC was specific to patients who were naive to previous ALK inhibitors, reducing the potential for bias in their NMA.
A subgroup analysis was conducted to assess the comparative efficacy of PFS among patients with and without brain metastases at baseline. The presence of brain metastases at baseline was noted as a source of heterogeneity. Such analyses may be useful in identifying potential effect modifiers. However, as the trials were not powered for assessments of efficacy among this subgroup of patients, the results of the analyses conducted in this NMA for this subgroup should also be interpreted with caution.
The NMA by Chuang et al. (2021)19 included alectinib as a comparator. Studies that assessed alectinib did so at 2 doses: 600 mg and 300 mg. The Health Canada–approved dose of alectinib is 600 mg; this is also the dose typically used in clinical practice. There is uncertainty whether the 2 different doses of alectinib can be considered equivalent in terms of both efficacy and safety; a higher dose may be associated with greater toxicities. The CADTH team considered it appropriate that the authors considered the 2 doses of alectinib as separate comparisons.
The ITC assessed efficacy outcomes of PFS and ORR. Data for OS in the trials were immature or not reported, making extrapolation of long-term efficacy impossible. Comparisons of grade 3 or higher AEs were assessed; considerations of safety are important as tolerability of treatments are important for patients and physicians when choosing therapy.
Chuang et al. (2021)19 used fixed-effects models due to the limited amount of published data. Random-effects models may be better suited for accommodating for heterogeneity across studies. However, in this NMA the treatment of interest was evaluated in only 1 trial, and the number of trials included in each comparison was low. Fixed-effects models were therefore considered appropriate.
Summary
Four ITCs were summarized and critically appraised, 1 submitted by the sponsor,18 and 3 identified through a CADTH supplementary literature search.19-21 The ITCs used different methodologies, including both frequentist and Bayesian approaches, and both fixed- and random-effects models. Advantages and disadvantages to both methods have been stated, mainly emphasizing the differences in how heterogeneity was assessed across studies, and its impact on the accuracy and precision of comparative treatment-effect estimates in the NMA. In particular, models that used random effects tended to result in wide CrIs. The characteristics across the trials were largely comparable, although variations in Asian and non-Asian patients, patients with brain metastases, and receipt of prior systemic therapies were noted. The comparators included in the NMAs differed slightly across each ITC; all studies compared lorlatinib with alectinib, brigatinib, and crizotinib. Other comparisons with lorlatinib included chemotherapy, ceritinib, and ensartinib. All ITCs included studies for alectinib that assessed doses of both 600 mg and 300 mg. Alectinib is approved for use in Canada at 600 mg. Some of the ITCs combined data regarding alectinib at both the 600 mg and 300 mg doses, while other ITCs assessed each dose as a separate network node. All ITCs included analyses of efficacy and safety. In general, lorlatinib was favoured for PFS over chemotherapy, crizotinib, ceritinib, and ensartinib; but the results of comparisons of PFS between lorlatinib and brigatinib or alectinib were not as clear. Results for other efficacy end points (i.e., OS and ORR) were also unclear due to lack of available data. Safety analyses suggested that there may be greater risk for toxicities in lorlatinib compared to other alternative treatments. The ITCs suffered mainly from clinical heterogeneity in patient characteristics and methodological heterogeneity due to differences in trial design that introduced uncertainty into effect estimates between treatment comparisons. As such, based on the indirect evidence reviewed, the true magnitude of comparative efficacy and safety estimates between the treatments assessed is not known.
Discussion
Summary of Available Evidence
One multi-centre, multinational, open-label, randomized, active-controlled, phase III group sequential superiority trial met the criteria of the CADTH systematic review.17 A total of 296 patients were randomized in the CROWN trial; 149 were randomized to receive lorlatinib and 147 patients were randomized to receive crizotinib. The study enrolled patients who had previously untreated ALK-positive local advanced or metastatic NSCLC, with or without brain metastases. The study results were based on pre-specified interim analyses of PFS and OS, and the OS data were considered immature at the data cut-off date (March 20, 2020). The study reached its primary end point of PFS according to an O’Brien-Fleming early-stop rule (alpha = 0.025) but is ongoing for follow-up of OS. The mean age of patients was 58 years, with slightly more female patients (56.4% in the lorlatinib group and 61.9% in the crizotinib group). Most patients were White (48.2% and 49.0% in the lorlatinib and crizotinib groups, respectively) or Asian (43.6% versus 44.2%, respectively). Brain metastases were reported in 25.5% of patients in the lorlatinib group and 27.2% of patients in the crizotinib group. Most patients had an ECOG PS of 0 (45.0% in the lorlatinib group versus 38.8% in the crizotinib group) or 1 (53.0% versus 55.1%, respectively), adenocarcinoma type of NSCLC (94.0% versus 95.2%, respectively), and stage IV metastatic disease (90.6% versus 94.6%, respectively). Patients were classified as either never smokers (54.4% in the lorlatinib group versus 63.9%) or former smokers (36.9% versus 29.3%).17
In addition to the systematic review, 1 sponsor-submitted ITC18 and 3 other ITCs19-21 identified through a supplementary literature search conducted by CADTH were summarized and appraised for this review.
Interpretation of Results
Efficacy
The CROWN trial demonstrated a statistically significant improvement in PFS in patients treated with lorlatinib over crizotinib. At the data cut-off date, the analysis of PFS was considered final by the sponsor based on the early-stopping rule. PFS is considered a clinically meaningful end point for patients, and the clinical experts consulted by CADTH confirmed that the results were clinically meaningful and supported improved patient outcomes with lorlatinib over crizotinib among all patient subgroups, including those with and without brain metastases. Fewer patients in the lorlatinib group (30.9%) than in the crizotinib group (78.2%) discontinued from the CROWN trial and the reasons for discontinuation were mainly due to disease progression, which occurred less frequently in the lorlatinib group than in the crizotinib group (17.8% versus 58.5%, respectively). Data for OS were hierarchically tested upon statistical significance of PFS and did not show a statistically significant difference between the groups. However, at the time of the data cut-off date, only 26% of the 198 OS events required for the final analysis of OS had occurred.17 Two additional analyses of OS are planned: when approximately 70% of events have occurred and at the final analysis. The CROWN trial was stopped early for benefit, creating the potential for the difference in PFS between lorlatinib and crizotinib to be overestimated at the time of interim analysis, even though approximately 70% of PFS events required for final analysis had accumulated at the early data cut-off date.35-37 This is a concern as OS data were immature at the interim analysis and final analysis of this outcome could be complicated or biased with disproportional dropouts between the treatment groups, largely due to, for example, a lack of efficacy or withdrawal due to disease-specific AEs. Although PFS is considered a clinically meaningful end point, whether a statistically significant and better improvement in PFS corresponds with an associated improvement in OS is still uncertain. It is not uncommon in oncology trials for an improvement in PFS to fail to translate into a final improvement in OS benefit. Other efficacy end points (i.e., ORR and DOR) favoured the lorlatinib group over the crizotinib group. In general, longer-term data are required to capture the long-term benefit of lorlatinib on patient outcomes.
Additional efficacy end points among subgroups of patients with brain metastases were also analyzed in the trial (i.e., IC-ORR, IC-DOR, IC-TTP, and IC-TTR). The results of these end points suggested improvements in patient outcomes when patients were treated with lorlatinib rather than crizotinib. The results of additional analyses of the probability of a first event being a CNS progression suggested that patients in the lorlatinib group had a lower probability of a first PFS event being a CNS progression. These data suggest that lorlatinib shows efficacy in patients with and without brain metastases and has the potential to delay the incidence of brain metastases and progression of brain metastases. The CROWN trial was not powered to assess these intracranial efficacy end points, and the results are considered exploratory. However, the data may be useful for patients and clinicians when considering a first-line treatment option in patients with ALK-positive NSCLC, particularly those with brain metastases. The efficacy of lorlatinib among patients with brain metastases was highlighted by both clinician and patient groups providing input for this review. While these analyses are limited by their exploratory nature, the clinicians consulted by CADTH both agreed they were clinically meaningful, as delayed progression of brain metastases is an important cause of patient morbidity and mortality.
HRQoL was assessed as an exploratory end point in the CROWN trial. No clinically meaningful differences (MID ≥ 10 points) between the lorlatinib and crizotinib treatment groups were observed in all subscales of the EORTC QLQ-C30 and QLQ-LC13 based on mean changes from baseline scores to the end of the study period. Similar results were observed for the EQ-5D-5L and EQ VAS. The TTD analysis conducted for symptom scales of pain in the chest, dyspnea, and cough in the EORTC QLQ-C30 also showed no differences between the treatment groups.
At the time of the CROWN trial’s inception, crizotinib was considered an appropriate comparator. However, new ALK inhibitors have been approved for use among this patient population in the first line, including alectinib and brigatinib. The clinical experts consulted by CADTH confirmed that alectinib and brigatinib were the most relevant comparators against lorlatinib. Four ITCs that compared lorlatinib to alectinib and brigatinib, as well as other therapies (i.e., ceritinib, crizotinib, chemotherapy, ensartinib) were summarized and critically appraised. As the primary end point of all trials included in each ITC was PFS, and the trials were powered for this end point, the discussion of efficacy will primarily focus on PFS. In the sponsor’s ITC, lorlatinib was favoured over ceritinib, crizotinib, ensartinib, chemotherapy, brigatinib, and alectinib at 600 mg, but not alectinib at 300 mg. The remaining ITCs also favoured treatment with lorlatinib except when compared against alectinib. In addition, CrIs between comparisons of lorlatinib and brigatinib, while not including 1 (which would indicate no difference), were close to the threshold. While the ITCs may suggest that lorlatinib is preferred over other therapies, the relative efficacy of lorlatinib against brigatinib and alectinib remains uncertain. The indirect evidence had significant limitations inherent in NMAs, including considerable clinical and methodological heterogeneity (e.g., the recognized differences in study population in terms of prior therapies) across different trials in the network. Moreover, the analysis of OS in all the ITCs could have suffered significant limitations. The RPFST method was used to handle varied crossovers in the trials. The method itself can only be valid when certain assumptions are met, and the estimated difference in OS could often be biased toward the null, which made it difficult to interpret the nonsignificant findings reported in the ITCs. Whether there was truly no difference or the estimate of difference in OS had been biased remains inconclusive. This casts further uncertainty on the comparative efficacy between lorlatinib versus all other ALK TKIs in regard to OS. Without direct evidence it is not possible to determine the ideal first-line ALK inhibitor for patients with ALK-positive metastatic NSCLC.
Harms
In general, toxicities were more commonly reported among patients treated in the lorlatinib group than in the crizotinib group. The most common AEs in the lorlatinib group were hypercholesterolemia (70.5% versus 3.5% in the crizotinib group), hypertriglyceridemia (63.8% versus 5.6%), edema (55.0% versus 39.4%), increased weight (38.3% versus 12.7%), peripheral neuropathy (33.6% versus 14.8%), cognitive effects (21.5% versus 5.6%), diarrhea (21.5% versus 52.1%), and dyspnea (20.1% versus 16.2%). The clinical experts consulted by CADTH noted that the AEs reported in the CROWN trial may have underestimated the cognitive side effects that have been commonly reported among patients treated with lorlatinib. Neurologic AEs have also been highlighted in the Health Canada product monograph for lorlatinib.1 Adverse events related to CNS effects were reported in a greater proportion of patients in the lorlatinib group compared to the crizotinib group (cognitive effects: 21.5% versus 5.6%; mood effects: 16.1% versus 4.9%; speech effects: 4.7% versus 0; psychotic effects: 3.4% versus 0, respectively). The clinical experts consulted by CADTH noted that the separate analysis of each type of CNS effect may have underestimated the frequency and severity of AEs affecting the brain and cognition. When lorlatinib is used in clinical practice, it may be beneficial for clinicians to consider the neurologic toxicities of lorlatinib and patient’s past medical history.
While more AEs were reported in the lorlatinib group, which may warrant greater monitoring of patients, in particular regarding cognitive AEs, the proportions of patients requiring dose modifications and interruptions were similar across both treatment groups. Dose reductions occurred in 20.8% of patients in the lorlatinib group compared to 15.5% of patients in the crizotinib group, and dose interruptions occurred in 49.0% and 47.2% of patients, respectively. Ultimately, the toxicities of lorlatinib are likely manageable, as similar proportions of patients discontinued treatment due to AEs in the lorlatinib (6.7%) and crizotinib (9.2%) groups.
The HRQoL data from the CROWN trial also suggested an increased severity of cognitive AEs. No differences were observed in the EORTC QLQ-C30 scores between patients in the lorlatinib and crizotinib groups, but the mean change from baseline scores in the physical, role emotional, and social functioning subscales of the QLQ-C30 were numerically higher in the lorlatinib group than in the crizotinib group. The mean change from baseline scores in the cognitive functioning scores were numerically higher in the crizotinib group than in the lorlatinib group.17 While no meaningful differences in HRQoL were observed through the EORTC QLQ-C30, EORTC QLQ-LC13 or EQ-5D-5L questionnaires, it was noted that the reliability of these tools in capturing cognitive AEs is not well established. Because there were no other commonly used and validated tools for the assessment of cognitive AEs at the time of the trial’s inception, these questionnaires may have underestimated the impact of both disease and treatment on patient HRQoL, specifically regarding cognitive effects.
The ITCs that were summarized and critically appraised compared AEs associated with other comparators, including other ALK TKIs and chemotherapy. Considerations of AE profiles are relevant for patients and clinicians when choosing a therapy, and tolerability may aid in the success of patient’s treatment. The sponsor’s ITC included comparisons of grade 3 and 4 AEs and AEs resulting in treatment discontinuation. The remaining ITCs included comparisons of any-grade AEs, grade 3 or higher AEs, SAEs, AEs resulting in treatment discontinuation, and specific AEs (e.g., nausea, diarrhea, ALT and/or AST increase, and pneumonitis). In general, results appeared to suggest that the incidence of AEs was greater among patients treated with lorlatinib. In particular, the toxicities of lorlatinib were consistently found to be greater compared to alectinib, especially when the dose of 300 mg was assessed separately from the 600 mg dose. This result may be due to the reduced dose exposure of alectinib at 300 mg, which may be correlated to reduced toxicities. The safety comparisons presented in the ITCs may not have accounted for the specific toxicities associated with each treatment that play a pivotal role in choice of therapy for patients.
Conclusions
One ongoing, phase III, open-label, randomized superiority trial (CROWN) provided evidence regarding the efficacy and safety of lorlatinib as first-line treatment in adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic NSCLC. Compared to crizotinib, patients treated with lorlatinib showed a statistically significant improvement in PFS that was considered clinically meaningful by the clinical experts consulted by CADTH. A consistent improvement in PFS was observed in all patient subgroups assessed, most notably patients with brain metastasis. The intracranial efficacy outcomes assessed in the trial (IC-ORR, IC-TTP, IC-DOR, and IC-TTR), although exploratory, also showed a consistent treatment benefit for lorlatinib. These results suggest that, compared to crizotinib, lorlatinib may have an improved ability to penetrate the blood-brain barrier and may be an option for patients with brain metastasis. Due to immaturity of the trial data, no evidence was available on OS. The trial is ongoing, and longer-term data are needed to determine whether the observed PFS benefit will translate to an improvement in OS. Lorlatinib may have a poorer safety profile compared to crizotinib, as grade 3 and 4 AEs were higher (by approximately 17%) in patients treated with lorlatinib, although this did not appear to result in a higher rate of dose modification or interruption, or treatment discontinuation. In particular, lorlatinib was associated with a higher incidence of neurologic AEs (i.e., cognitive and mood effects), and patients and clinicians should be aware of this association before initiating treatment with lorlatinib. Results for HRQoL did not suggest any clinically meaningful differences between the treatment groups. In general, the results of the CROWN trial support the use of lorlatinib as another first-line treatment option for patients with ALK-positive locally advanced or metastatic NSCLC.
Comparison of efficacy and safety between lorlatinib and other TKIs, specifically alectinib and brigatinib, were emphasized to be more relevant in the Canadian first-line treatment setting of advanced or metastatic ALK-positive NSCLC. The ITCs included in this review showed that, similar to lorlatinib, both alectinib and brigatinib have improved PFS when compared to crizotinib and therefore are more likely to be choices for first-line therapy compared with crizotinib. However, given the limitations of the ITCs, primarily related to clinical and methodological heterogeneity across included trials, the magnitude and direction of comparative estimates of efficacy and safety between lorlatinib, alectinib, and brigatinib are uncertain.
References
1.Lorbrena (lorlatinib): tablets, 25 and 100 mg, oral [product monograph]. In: Kirkland (QC): Pfizer Canada ULC; 2021.
2.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. Can Med Assoc J. 2020;192(9):E199-E205. PubMed
3.cancer.org. Lung cancer survival rates https://www.cancer.org/cancer/lung-cancer/detection-diagnosis-staging/survival-rates.html. Published 2021. Accessed.
4.Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363(18):1693-1703. PubMed
5.Shaw AT, Solomon BJ, Besse B, et al. ALK Resistance Mutations and Efficacy of Lorlatinib in Advanced Anaplastic Lymphoma Kinase-Positive Non–Small-Cell Lung Cancer. J Clin Oncol. 2019;37(16):1370-1379. PubMed
6.Griesinger F, Roeper J, Pöttgen C, Willborn KC, Eberhardt WEE. Brain metastases in ALK-positive NSCLC - time to adjust current treatment algorithms. Oncotarget. 2018;9(80):35181-35194. PubMed
7.Pacheco JM, Gao D, Smith D, et al. Natural History and Factors Associated with Overall Survival in Stage IV <em>ALK</em>-Rearranged Non–Small Cell Lung Cancer. J Thorac Oncol. 2019;14(4):691-700. PubMed
8.CADTH. Brigatinib (Alunbrig) ALK + NSCLC - pERC Final Recommendation https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/10230BrigatinibALK%2BNSCLC_fnRec_EC21Apr2021_final.pdf. Published 2021. Accessed2021.
9.CADTH. Brigatinib (Alunbrig) NSCLC - pERC Final Recommendation. https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10167BrigatinibNSCLC_FnRec_approvedbyChair_NOREDACT_Post_01AUG2019_final.pdf. Published 2019. Accessed2021.
10.CADTH. Lorlatinib (Lorbrena) NSCLC - pERC Final Recommendation. https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10183LorlatinibNSCLC_FnRec_ApprovedbyChair_Post_30Jan2020_final.pdf. Published 2020. Accessed 2021, 2021.
11.CADTH. Alectinib (Alecensaro) NSCLC (first line) - pERC Final Recommendation. https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_1stln_fn_rec.pdf. Published 2018. Accessed2021.
12.CADTH. Alectinib (Alecensaro) NSCLC (second line) - pERC Final Recommendation. https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_2ln_fn_rec.pdf. Published 2018. Accessed2021.
13.CADTH. Alectinib (Alecensaro) NSCLC - pERC Final Recommendation https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_fn_rec.pdf. Published 2017. Accessed2021.
14.CADTH. Ceritinib (Zykadia) NSCLC - Final Recommendation. https://www.cadth.ca/sites/default/files/pcodr/pcodr_ceritinib_zykadia_nsclc_fn_rec.pdf. Published 2015. Accessed2021.
15.CADTH. Ceritinib (Zykadia) - pERC Final Recommendation https://www.cadth.ca/sites/default/files/pcodr/pcodr_ceritinib_zykadia_nsclc_resub_fn_rec.pdf. Published 2017. Accessed2021.
16.CADTH. Crizotinib Resubmission First Line NSCLC - Final Recommendation https://www.cadth.ca/sites/default/files/pcodr/pcodr_xalkori_1stln_nsclc_fn_rec.pdf. Published 2015. Accessed2021.
17.Clinical Study Report: B7461006. A phase 3, randomized, open label study of lorlatinib (PF-06463922) monotherapy versus crizotinib monotherapy in the first line treatment of patients with advanced ALK-positive non-small cell lung cancer [internal sponsor's report]. In: Melbourne (AU): Pfizer Inc.; 2020.
18.Drug Reimbursement Review sponsor submission: Lorbrena (lorlatinib): tablets, 25 and 100 mg, oral [internal sponsor's package]. In: Kirkland (QC): Pfizer Canada ULC; 2021 Sep.
19.Chuang CH, Chen HL, Chang HM, et al. Systematic Review and Network Meta-Analysis of Anaplastic Lymphoma Kinase (ALK) Inhibitors for Treatment-Naive ALK-Positive Lung Cancer. Cancers (Basel). 2021;13(8):19. PubMed
20.Wang L, Sheng Z, Zhang J, et al. Comparison of lorlatinib, alectinib and brigatinib in ALK inhibitor-naive/untreated ALK-positive advanced non-small-cell lung cancer: a systematic review and network meta-analysis. J Chemother. 2021:1-10. PubMed
21.Ando K, Manabe R, Kishino Y, et al. Comparative efficacy and safety of lorlatinib and alectinib for ALK-rearrangement positive advanced non-small cell lung cancer in asian and non-asian patients: A systematic review and network meta-analysis. Cancers (Basel). 2021;13(15). PubMed
22.Committee; CCSA. Canadian Cancer Statistics: A 2020 special report on lng cancer Toronto, ON2020.
23.NCCN. NCCN Clinical Practice Guidelines in Oncology: Non-small cell lung cancer version 5.2021 https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Published 2021. Accessed August 2021.
24.ULC PC. Xalkori Product Mongraph Kirkland, Quebec, Canada2021.
25.Limited H-LR. Alecensaro product Monograph 2021.
26.Inc. TC. Alunbrig Product Monograph. 2021.
27.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
28.Grey matters: a practical tool for searching health-related grey literature. In: Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 1800 Jan 1.
29.Shaw AT, Bauer TM, de Marinis F, et al. First-Line Lorlatinib or Crizotinib in Advanced ALK-Positive Lung Cancer. N Engl J Med. 2020;383(21):2018-2029. PubMed
30.Brookmeyer R, Crowley J. A Confidence Interval for the Median Survival Time. Biometrics. 1982;38(1):29-41.
31.Kalbfleisch JD, Prentice RL. The Statistical Analysis of Failure Time Data. 2nd Ed. ed. Hoboken Wiley Interscience 2002.
32.Zhang X. Comparison of restricted mean survival times between treatments based on a stratified Cox model. Bio-Algorithms and Med-Systems. 2013;9(4):183-189.
33.Pfizer Canada response to August 19, 2021 DRR request for additional information regarding Lorlatinib DRR review: OPTIONAL BRIEF DESCRIPTION OF INFO REQUESTED [internal additional sponsor's information]. In: City (PROV): Sponsor name; 2021.
34.Cho BC, Obermannova R, Bearz A, et al. Efficacy and Safety of Ceritinib (450 mg/d or 600 mg/d) With Food Versus 750-mg/d Fasted in Patients With ALK Receptor Tyrosine Kinase (ALK)-Positive NSCLC: Primary Efficacy Results From the ASCEND-8 Study. J Thorac Oncol. 2019;14(7):1255-1265. PubMed
35.Bassler D, Briel M, Montori VM, et al. Stopping Randomized Trials Early for Benefit and Estimation of Treatment Effects: Systematic Review and Meta-regression Analysis. JAMA. 2010;303(12):1180-1187. PubMed
36.Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ: British Medical Journal. 2012;344:e3863. PubMed
37.Wilcox RA, Djulbegovic B, Guyatt GH, Montori VM. Randomized Trials in Oncology Stopped Early for Benefit. J Clin Oncol. 2008;26(1):18-19. PubMed
38.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
39.Eortc Quality of Life. FAQs. https://qol.eortc.org/faq/. Accessed 2021 Apr 14.
40.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
41.EORTC QLC-C30 scoring manual. In: Brussels (BE): European Organisation for Research and Treatment of Cancer (EORTC); 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2021 Apr 16.
42.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
43.Paiva CE, Carneseca EC, Barroso EM, et al. Further evaluation of the EORTC QLQ-C30 psychometric properties in a large Brazilian cancer patient cohort as a function of their educational status. Support Care Cancer. 2014;22(8):2151-2160. PubMed
44.Luo N, Fones CS, Lim SE, Xie F, Thumboo J, Li SC. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-c30): validation of English version in Singapore. Qual Life Res. 2005;14(4):1181-1186. PubMed
45.Ozturk A, Sarihan S, Ercan I, Karadag M. Evaluating quality of life and pulmonary function of long-term survivors of non-small cell lung cancer treated with radical or postoperative radiotherapy. Am J Clin Oncol. 2009;32(1):65-72. PubMed
46.Brabo EP, Paschoal ME, Biasoli I, et al. Brazilian version of the QLQ-LC13 lung cancer module of the European Organization for Research and Treatment of Cancer: preliminary reliability and validity report. Qual Life Res. 2006;15(9):1519-1524. PubMed
47.Marzorati C, Monzani D, Mazzocco K, Pavan F, Monturano M, Pravettoni G. Dimensionality and Measurement Invariance of the Italian Version of the EORTC QLQ-C30 in Postoperative Lung Cancer Patients. Front Psychol. 2019;10:2147. PubMed
48.Arrieta O, Luvian-Morales J, Turcott JG, Onate-Ocana LF. Quality of life and anorexia/cachexia in lung cancer: validation of the Spanish version of the FAACT instrument. Qual Life Res. 2018;27(10):2709-2718. PubMed
49.Ahn MJ, Tsai CM, Hsia TC, et al. Cost-effectiveness of bevacizumab-based therapy versus cisplatin plus pemetrexed for the first-line treatment of advanced non-squamous NSCLC in Korea and Taiwan. Asia Pac J Clin Oncol. 2011;7 Suppl 2:22-33. PubMed
50.Chie WC, Yang CH, Hsu C, Yang PC. Quality of life of lung cancer patients: validation of the Taiwan Chinese version of the EORTC QLQ-C30 and QLQ-LC13. Qual Life Res. 2004;13(1):257-262. PubMed
51.Koukouli S, Stamou A, Alegakis A, Georgoulias V, Samonis G. Psychometric properties of the QLQ-C30 (version 3.0) in a sample of ambulatory Cretan cancer patients. European Journal of Cancer Care. 2009;18(5):447-456. PubMed
52.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
53.Osoba D, Zee B, Pater J, Warr D, Kaizer L, Latreille J. Psychometric properties and responsiveness of the EORTC quality of Life Questionnaire (QLQ-C30) in patients with breast, ovarian and lung cancer. Qual Life Res. 1994;3(5):353-364. PubMed
54.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
55.Bedard G, Zeng L, Zhang L, et al. Minimal important differences in the EORTC QLQ-C30 in patients with advanced cancer. Asia Pac J Clin Oncol. 2014;10(2):109-117. PubMed
56.Aggarwal J, Chakraborty S, Ghosh Laskar S, et al. Reference Data for Standardized Quality of Life Questionnaires in Indian Patients with Brain Metastases from Non-small Cell Lung Cancer: Results from a Prospective Study. Cureus. 2017;9(4):e1149. PubMed
57.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30a(5):635-642. PubMed
58.Franceschini J, Jardim JR, Fernandes AL, Jamnik S, Santoro IL. Reproducibility of the Brazilian Portuguese version of the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire used in conjunction with its lung cancer-specific module. Jornal Brasileiro De Pneumologia: Publicacao Oficial Da Sociedade Brasileira De Pneumologia E Tisilogia. 2010;36(5):595-602.
59.Arrieta O, Nunez-Valencia C, Reynoso-Erazo L, et al. Health-related quality of life in patients with lung cancer: validation of the Mexican-Spanish version and association with prognosis of the EORTC QLQ-LC13 questionnaire. Lung Cancer. 2012;77(1):205-211. PubMed
60.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
61.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
62.Ameri H, Yousefi M, Yaseri M, Nahvijou A, Arab M, Akbari Sari A. Mapping the cancer-specific QLQ-C30 onto the generic EQ-5D-5L and SF-6D in colorectal cancer patients. Expert Rev Pharmacoecon Outcomes Res. 2019;19(1):89-96. PubMed
63.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. In: Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2020 Oct 13.
64.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946–)
EMBASE (1974–)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: July 21, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(lorlatinib* or loratinib* or lorbrena* or lorviqua* or PF-06463922 or PF06463922 or PF-6463922 or PF6463922 or OSP71S83EU or TE9WI16FEU).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*lorlatinib/ or (lorlatinib* or loratinib* or lorbrena* or lorviqua* or PF-6463922 or PF6463922 or PF-06463922 or PF06463922).ti,ab,kw,dq.
3 use oemezd
(conference review or conference abstract).pt.
4 not 5
2 or 6
remove duplicates from 7
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – lorlatinib or Lorbrena or Lorviqua | lung or NSCLC]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – lorlatinib or Lorbrena or Lorviqua | lung or NSCLC]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – lorlatinib or Lorbrena or Lorviqua | lung or NSCLC]
Grey Literature
Search dates: July 15 – July 21, 2021
Keywords: lorlatinib, Lorbrena, Lorviqua, loratinib, non–small cell lung cancer, NSCLC, lung
Limits: None
Updated: Search updated prior to the meeting of CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC).
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Note this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Felip E, Shaw AT, Bearz A, et al. Intracranial and extracranial efficacy of lorlatinib in patients with ALK-positive non-small-cell lung cancer previously treated with second-generation ALK TKIs. Ann Oncol. 2021;32(5):620-630. | Study design |
Solomon BJ, Besse B, Bauer TM, et al. Lorlatinib in patients with ALK-positive non-small-cell lung cancer: results from a global phase 2 study. Lancet Oncol. 2018;19(12):1654-1667. | Study design |
Shaw AT, Felip E, Bauer TM, et al. Lorlatinib in non-small-cell lung cancer with ALK or ROS1 rearrangement: an international, multicentre, open-label, single-arm first-in-man phase 1 trial. Lancet Oncol. 2017;18(12):1590-1599. | Study design |
Appendix 3: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire – core 30 items (EORTC QLQ-C30)
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module (EORTC QLQ-LC13)
European Quality of Life Scale – 5 Dimensions – 5 Levels (EQ-5D-5L)
Findings
Table 51: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A 30-item, patient-reported, cancer-specific, quality of life questionnaire using 4- and 7-point Likert scales. | Validity, reliability, and responsiveness: Evidence of validity, reliability, and responsiveness in populations with lung cancer. Limited evidence supporting adequate validity, reliability, and responsiveness in patients with NSCLC and ALK. | Patients with cancer
Patients with NSCLC: MID is estimated to range from 5 to 7 units in patients with NSCLC and brain metastases |
EORTC QLQ-LC13 | A 13-item lung cancer–specific questionnaire to be used in conjunction with the QLQ-C30 to address symptoms associated with lung cancer and its standard treatment. Composed of 2 basic elements: (1) the EORTC QLQ-C30, covering general aspects of HRQL, and (2) additional disease- or treatment-specific questionnaire modules. | Validity, reliability, and responsiveness: Evidence of validity, reliability, and responsiveness in populations with lung cancer. Limited evidence supporting adequate validity, reliability, and responsiveness in patients with NSCLC and ALK. | Patients with NSCLC: MID is estimated to range from 3 to 6 units in patients with NSCLC and brain metastases |
EQ-5D-5L | Patient-reported, generic quality of life instrument using a 5-point ordinal scale to assess health in 5 dimensions. | Validity, reliability, and responsiveness: Validity demonstrated in the general population. No literature was identified that assessed validity, reliability, or responsiveness in patients with ALK-positive NSCLC. | No MID identified in populations with ALK-positive NSCLC |
ALK = anaplastic lymphoma kinase–positive; EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire – core 30 items; EORTC QLQ-LC13 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; EQ-5D-5L = European Quality of Life Scale – 5 Dimensions – 5 Levels; HRQoL = health-related quality of life; MID = minimal important difference; NSCLC = non–small cell lung cancer.
EORTC QLQ-C30
Description
The EORTC QLQ-C30 is one of the most commonly used PRO measures in oncology clinical trials.38 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials in response to treatment.39 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item quality-of-life scale, as outlined in Table 52. The first 2 versions of the questionnaire have been previously validated in patients with cancer.40 Version 3.0 of the questionnaire is the most current version and has been in use since December of 1997.41 It is available in 90 languages and is intended for use in adult populations only. The global quality of life scale is also known as Global Health Scale.42
Table 52: EORTC QLQ-C30 Scales
Functional scales (15 questions) | Symptom scales (7 questions) | Single-item symptom scales (6 questions) | Global quality of life (2 questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global quality of Life (2) |
Role function (2) | Pain (2) | Insomnia (1) | — |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | — |
Emotional function (4) | — | Constipation (1) | — |
Social function (2) | — | Diarrhea (1) | — |
— | — | Financial impact (1) | — |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period to assess function and symptoms.41 Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”) with scores on these items ranging from 1 to 4. For the 2 items that form the global QoL scale, the response format is a 7-point Likert-type scale with anchors at 1 = “very poor” and 7 = “excellent.”
Raw scores for each scale are computed as the average of the items that contribute to a particular scale.41 This scaling approach is based on the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of one unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scales would reflect an improvement. According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.
Psychometric Properties
Validity
Data from 6 prospective studies were combined to assess the validity of the EORTC QLQ-C30 in in 986 lung cancer patients in Brazil.43 Construct validity was assessed by cross-sectional correlational evidence and discriminative evidence. Convergent validity was assessed by testing a priori hypotheses about strength of Pearson’s correlation between QLQ-C30 subscales and other scales, including the World Health Organization (WHO) QoL-bref, the Hospital Anxiety and Depression Scale (HADS), and the Edmonton Symptom Assessment System (ESAS). Evidence of convergent validity was defined as a correlation of ≥0.40 between items and their scales. It was hypothesized that the various scales would be at least moderately correlated with each other’s respective scales. Results showed that convergent and divergent validity were adequate, with index values of 91.6% and 97.4% respectively.43 In general, moderate to strong correlations (r > 0.40) were found between the subscales of the EORTC QLQ-C30 and its respective dimensions on the WHOQOL-bref, the HADS, and the ESAS instruments. There were poor correlations between the EORTC QLQ-C30’s social functioning domain and the respective domains on the WHOQOL-bref. In terms of known-group validity, the EORTC QLQ-C30 was able to differentiate groups of patients with distinct performance statuses and types of treatment.43
Another cross-sectional study aimed to validate the EORTC QLQ-C30 and the LC13 in 112 patients with advanced lung cancer in a palliative care setting. Construct validity was evaluated using multi-trait analysis, with evidence of convergent validity defined as a correlation of 0.40 or higher between an item and its own hypothesized scale. Criterion validity was evaluated through variance and correlation with various clinical measures including stage of cancer, performance status, spirometry, blood tests, and the 6-minute walk test. Concurrent validity was examined by comparing the correlation with other scales measuring the same constructs; strong correlations were described as > 0.60. Construct validity was confirmed to be present among all the scales except cognitive functioning. Concurrent and criterion validity were supported for most of the functioning and symptom scales. Performance on the physical functioning, emotional, and global QoL were able to be predicted from various clinical measures (r2 = 0.70, 0.59, and 0.50, respectively).
One cross-sectional study aimed to validate the EORTC QLQ-C30 in a convenience sample of cancer patients in Singapore.44 Most patients had breast and colorectal cancers, but leukemia, lung cancer, lymphoma, germ cell tumour, and other cancers were also included. Construct validity was assessed by cross-sectional correlational evidence and discriminative evidence. First, convergent validity was assessed using Spearman’s correlations between QLQ-C30 and Short Form-36 (SF-36) scales, hypothesizing moderate to strong correlation (defined as correlation coefficient of 0.35 to 0.5, and > 0.5, respectively) between scales of these 2 instruments measuring similar dimensions of HRQoL. Results showed moderate to strong correlations between the QLQ-C30 and SF-36 scales, ranging from 0.35 to 0.67 across the assessed scales. Next, known-groups approach was used to compare 6 QLQ-C30 scale scores between patients reporting mild and severe symptoms, as well as by stage of disease and presence of comorbid conditions. With the exception of emotional functioning, the remaining 5 scales showed better scores in patients with mild symptoms than those with severe symptoms (P < 0.05 for all other comparisons). Patients in early stages of cancer (or with no comorbid conditions) generally had better QLQ-C30 scores than those in advanced disease stages (or with comorbid conditions); however, none of these differences were statistically significant.
A recent cross-sectional study in Kenya was conducted to evaluate the psychometric properties of the EORTC QLQ-C30, using the English or Kiswahili version in 100 patients with cancer.42 Most patients had breast cancer, followed by prostate, Kaposi sarcoma, lung, and other cancers. Construct validity was assessed by examining the interscale correlations among the subscales of EORTC QLQ-C30. The interscale correlations were weak to strong with an absolute magnitude ranging from 0.07 to 0.73. Notably, with the exception of cognitive functioning, emotional functioning, nausea and vomiting, dyspnea, appetite loss, constipation, and diarrhea, the GHS correlated moderately with the remaining subscales (r ≥ 0.30). Cross-cultural validity was evaluated but not reported here.
Another study in Turkey aimed to assess the validity and reliability of the EORTC QLQ-C30 in 28 patients who survived NSCLC post-radiation therapy for ≥ 2 years.45 In terms of construct validity, all interscale correlations were statistically significant, with the strongest positive correlation between the domains of physical and role functioning (r = 0.59, P = 0.01), and physical and cognitive functioning (r = 0.37, P = 0.05). In terms of convergent validity, the highest correlation of EORTC QLQ-C30 and the Karnofsky performance scale during the questionnaire was found to be with physical functioning (r = 0.41, P < 0.02) and constipation (r = 0.44, P = 0.01).
This questionnaire has also been translated and validated in numerous other languages including Portuguese,46 Italian,47 Spanish,48 Chinese49,50 and Cretan51 for use in populations with lung cancer.
Reliability
The Brazilian and Singaporean cross-sectional studies above also assessed reliability by calculating Cronbach alpha for all QLQ-C30 scales.43,44 The Cronbach alpha was 0.70 or greater for 6 of the 9 assessed QLQ-C30 scales in both studies; The scales that did not meet the minimum reliability limit included the domains of cognitive functioning, physical functioning,44 social functioning,43 and nausea and vomiting.
The Kenyan study described above assessed the internal consistency of each scale of the questionnaire using Cronbach alpha coefficients.42 With the exception of the cognitive function scale, all of the scales had a Cronbach alpha ≥ 0.70
The Turkish study described above found that 7 of 9 scales of the questionnaire were found to have a Cronbach’s alpha ≥ 0.70 ranging from 0.56 for social functioning and 0.93 for role functioning.
The cross-sectional study by Nicklasson and Bergman also assessed the reliability of the EORTC QLQ-C30 in 112 advanced lung cancer patients with chest malignancies in the palliative care setting.52 The minimum reliability limit (Cronbach’s alpha ≥ 0.70) was reached for all multi-item scales, except for cognitive functioning.52
Responsiveness
One study by Osoba et al.53 aimed to assess the responsiveness of the EORTC QLQ-C30 in 160 lung cancer patients who received chemotherapy. The QLQ-C30 showed responsiveness to changes in disease state and treatment to chemotherapy in the expected direction. Patients with metastatic disease and those who received chemotherapy had diminished scores in the domains of physical and social role functions, and global quality of life, and had greater fatigue and nausea and vomiting compared with before chemotherapy.53
Minimal Important Difference
For use in clinical trials, scores on the EORTC QLQ-C30 can be compared between different groups of patients or within a group of patients over time. One study from 1998 conducted in patients with breast cancer and small-cell lung cancer estimated a clinically relevant change in score on any scale of the EORTC QLQ-C30 to be 10 points.54 The estimate was based on a study that used an anchor-based approach to estimate the MID, in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Participants who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported being “very much” changed had corresponding changes of more than 20 points.
In 2014, a Canadian study estimated the MID for EORTC QLQ-C30 in 369 patients with advanced cancer who completed the questionnaire at baseline and 1-month post-radiation.55 The most common cancer type was breast cancer, followed by lung, prostate, gastrointestinal, renal cell, and other cancers. The MID was estimated using both anchor- and distribution-based methods for improvement and deterioration. Two anchors of overall health and overall QoL were used, both taken directly from the EORTC QLQ-C30 (questions 29 and 30) where patients rated their overall health and QoL themselves. Improvement and deterioration were categorized as an increase or decrease by 2 units to account for the natural fluctuation of patient scoring. With these 2 anchors, the estimated MIDs across all EORTC QLQ-C30 scales ranged from 9.1 units to 23.5 units for improvement, and from 7.2 units to 13.5 units for deterioration. Distribution-based estimates were closest to 0.5 SD.
In 2017, a study in India aimed to derive a reference dataset for Indian patients with NSCLC and brain metastases and estimated the MID.56 The authors determined that estimated MID for the various functional and symptom scales ranged from 5 to 7 units.56 Distribution-based estimates were closest to 0.2 SD.
EORTC QLQ-LC13
The EORTC QLQ-LC13 is a 13-item lung cancer–specific questionnaire module that is a modular supplement to the QLQ-C30 for assessing the quality of life of lung cancer patients in clinical trials.57 The EORTC QLQ-LC13 is composed of 2 basic elements: the EORTC QLQ-C30, as the general HRQoL questionnaire, and additional disease- or treatment-specific questionnaire modules.57 There have been multiple international field studies to evaluate the psychometric properties of the EORTC QLQ-C30 supplemented by the EORTC QLQ-LC13.57
This questionnaire has been translated into numerous other languages including Portuguese,46,58 Spanish,59 and Chinese50 and has been deemed reliable and valid for use in patient populations with lung cancer.
Psychometric Properties
Validity
A study by Nicklasson and Bergman52 aimed to validate the EORTC QLQ-C30 and the LC13 in 112 patients with advanced lung cancer in a palliative care setting. Construct validity was evaluated using multi-trait analysis, with evidence of convergent validity defined as a correlation of 0.40 or higher between an item and its own hypothesized scale. Criterion validity was evaluated through variance by and correlation with various clinical measures including stage of cancer, performance status, spirometry, blood tests, and the 6-minute walk test. Concurrent validity was examined by comparing the correlation with other scales measure the same constructs; strong correlations were described as greater than 0.60. Construct validity was confirmed to be present among all the symptom scales and were consistent with previous studies. Concurrent and criterion validity were supported for most of the functioning and symptom scales.
Reliability
The same cross-sectional study above assessed the reliability of the EORTC QLQ-LC13 in 112 advanced lung cancer patients with chest malignancies in the palliative care setting. The minimum reliability limit (Cronbach’s alpha > 0.70) was reached for all multi-item scales, except for cognitive functioning.
EQ-5D-5L
The European Quality of Life Scale (EQ-5D) is a generic HRQoL instrument that may be applied to a wide range of health conditions and treatments.60,61 The first of 2 parts of the EQ-5D is a descriptive system that classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D-5L has 5 possible levels for each domain and respondents are asked to choose the level that reflects their health state for each of the 5 domains resulting in 3,125 possible health states.62 A scoring function can be used to assign a value to self-reported health states from a set of population-based preference weights.60,61 The second part is a 20 cm Visual Analogue Scale (EQ VAS) that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ VAS which best represents their health on that day. Hence, the EQ-5D produces 3 types of data for each respondent:
a profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 15121 and 33211
a population preference-weighted health index score based on the descriptive system
a self-reported assessment of health status based on the EQ VAS.
The EQ-5D index score is generated by applying a multi-attribute utility function to the descriptive system.63 Different utility functions are available that reflect the preferences of specific populations (e.g., US or UK). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.
The EQ-5D-5L is validated in the general population and has an estimated MID between 0.037 and 0.069 based on scoring algorithms for 6 countries (Canada, China, Spain, Japan, England, and Uruguay).64
No literature was identified that assessed validity, reliability, or responsiveness in patients with ALK-positive NSCLC. No MID information was identified in populations with ALK-positive NSCLC.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
ALK
anaplastic lymphoma kinase
BIA
budget impact analysis
CNS
central nervous system
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
RDI
relative dose intensity
ToT
time on treatment
TKI
tyrosine kinase inhibitor
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Lorlatinib (Lorbrena), oral tablets |
Submitted price | Lorlatinib, 100 mg: $337.33 per tablet Lorlatinib, 25 mg: $112.44 per tablet |
Indication | As monotherapy for the first-line treatment of adult patients with ALK-positive locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer. |
Health Canada approval status | NOC |
Health Canada review pathway | Other: Expedited pathway — Project ORBIS |
NOC date | June 7, 2021 |
Reimbursement request | As per indication |
Sponsor | Pfizer Canada |
Submission history | Previously reviewed: No |
ALK = anaplastic lymphoma kinase; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | As first-line treatment for patients with ALK-positive advanced non–small cell lung cancer |
Treatment | Lorlatinib |
Comparators | Crizotinib Alectinib Brigatinib |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (30 years) |
Key data sources | CROWN trial: efficacy estimates (PFS, intracranial progression-free survival (CNS-PFS), OS, and time on treatment) for lorlatinib and crizotinib Network meta-analysis: hazard ratios for PFS and OS for alectinib and brigatinib compared to crizotinib Time on treatment for alectinib and brigatinib was derived using estimates of mean treatment duration obtained from the literature |
Submitted results | Results from sequential analysis indicated that the 2 optimal treatments (i.e., on the cost-effectiveness frontier) are lorlatinib and crizotinib. The ICER for lorlatinib was $128,964 per QALY when compared to crizotinib (incremental costs = $338,070; incremental QALYs = 2.62). |
Key limitations | There was substantial uncertainty in the extrapolated long-term OS outcomes for all treatments due to immature OS data reported in the CROWN trial. Evidence from the NMA was uncertain due to limited number of included studies and heterogeneity across studies in terms of trial design and eligibility criteria. The sponsor did not consider any potential waning of treatment effects, which may benefit lorlatinib as the modelled survival benefit for lorlatinib persists over the entire time horizon. Feedback from clinical experts consulted by CADTH indicated that OS benefits and treatment durations derived for alectinib and brigatinib in the sponsor’s model lacked face validity and were expected to be comparable for the 2 treatments. Estimates for resources required to manage CNS progression, subsequent treatment distributions, and dose intensities did not reflect standard of care in Canada. |
CADTH reanalysis results | CADTH corrected the sponsor’s model by applying a 20% variance to parameters without known standard errors and used a gamma distribution for cost data. The CADTH base case assumed equivalence of OS benefit and time on treatment for alectinib and brigatinib, and incorporated revised estimates for resources required to manage CNS progression, subsequent treatment distribution, and dose intensity for alectinib. In the CADTH base case, crizotinib, brigatinib, lorlatinib are on the cost-effectiveness frontier. The ICER for brigatinib compared to crizotinib is $116,289 per QALY, and the ICER for lorlatinib compared to brigatinib is $147,368 per QALY. The probability of lorlatinib being cost-effective at a WTP threshold of $50,000 per QALY is 1.4% compared to crizotinib, brigatinib, and alectinib. A price reduction of at least 42% is required for lorlatinib to be considered an optimal treatment option at a WTP threshold of $50,000 per QALY gained. The results are highly sensitive to assumptions regarding survival outcomes. |
ALK = anaplastic lymphoma kinase; CNS = central nervous system; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; NMA = network meta-analysis; PFS = progression-free survival; QALY = quality-adjusted life-year; WTP = willingness to pay.
Conclusions
The CROWN trial provided evidence that first-line treatment with lorlatinib among patients with anaplastic lymphoma kinase (ALK)–positive non–small cell lung cancer (NSCLC) led to a statistically significant and clinically meaningful improvement in progression-free survival (PFS) when compared to crizotinib. Data for overall survival (OS) in the trial were highly immature thus no evidence is currently available; additional data are expected. Due to a lack of head-to-head studies comparing lorlatinib to relevant comparators, the sponsor performed a network meta-analysis (NMA) to indirectly compare lorlatinib to alectinib and brigatinib and to derive relative estimates of efficacy. The efficacy estimates obtained from the indirect evidence are uncertain due to clinical and methodological heterogeneity across studies, particularly in terms of baseline patient characteristics and differences in trial design. The sponsor’s economic results were highly influenced by the parametric survival models used to extrapolate long-term outcomes and by assumptions on the benefit of lorlatinib relative to the comparator treatments.
CADTH identified several limitations within the sponsor’s economic analysis. Substantial uncertainty was observed in the long-term extrapolated outcomes for all treatments due to immature trial data and uncertainty in results derived from the NMA. Moreover, the sponsor did not apply treatment waning in the model, which could benefit lorlatinib as the extrapolated OS benefit for lorlatinib relative to comparators in the sponsor’s model persists over the entire time horizon. CADTH also noted additional structural uncertainty because the use of a partitioned survival model (PSM) does not explicitly account for progression. This structural assumption could introduce a post-progression survival bias that likely favours lorlatinib. The revised CADTH base case was derived by assuming 20% variance to parameters without known standard errors, applying a gamma distribution for costs, assuming equivalence of OS and time on treatment (ToT) for alectinib and brigatinib, revising estimates for resources required to manage central nervous system (CNS) progression and subsequent treatment distribution, and using a dose intensity for alectinib that aligns with clinical practice. CADTH performed scenario analyses by varying the following parameters: OS benefit for lorlatinib relative to alectinib and brigatinib, parametric survival models for OS extrapolation beyond the trial duration, treatment-waning assumptions, resource use estimates for CNS progression, and utility values.
In the CADTH base case, crizotinib, brigatinib, and lorlatinib were on the cost-effectiveness frontier. The incremental cost-effectiveness ratio (ICER) for brigatinib compared to crizotinib is $116,289 per quality-adjusted life-year (QALY), and the ICER for lorlatinib compared to brigatinib is $147,368 per QALY. Although CADTH’s base case resulted in a higher ICER for lorlatinib than the sponsor’s base case ($128,964 per QALY versus $147,368 per QALY), both analyses provided consistent results, indicating that, at the submitted price, lorlatinib was not cost-effective at a $50,000 per QALY willingness-to-pay (WTP) threshold. A price reduction of at least 42% would be required to make lorlatinib an optimal treatment option at a WTP threshold of $50,000 per QALY relative to the comparator treatments.
Results were highly sensitive to assumptions regarding the relative difference in OS between alectinib and brigatinib, OS benefit for lorlatinib relative to alectinib and brigatinib, treatment-waning assumptions, and the parametric models used to extrapolate long-term outcomes. However, several limitations could not be addressed in the CADTH base-case and scenario analyses due to data limitations and constraints introduced by the submitted model structure.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the drug plans that participated in the CADTH review process (specifically, information that pertains to the economic submission). No patient input and no input from clinician groups was received.
Two patient groups, the CanCertainty Coalition and Lung Cancer Canada, provided input. Patient input indicated that the current standard of treatment for patients with ALK-positive NSCLC is targeted therapy, which includes the tyrosine kinase inhibitors (TKIs) crizotinib, ceritinib, and alectinib. Patient input reported that chemotherapy has been a long-standing and well-documented standard of care for patients with lung cancer, with options available for oral chemotherapy as a take-home cancer drug. Patient input described that those with the ALK-positive mutation commonly present with brain metastases at diagnosis, which is debilitating and negatively affects quality of life, has a poorer prognosis, and lowers survival rates. Patient input reported that lorlatinib is another targeted therapy that can be administered orally with active manageable side effects and, unlike chemotherapy, it allows patients to be independent, functional, and active in their daily lives. Patient input further reported that other benefits offered by lorlatinib included long-term remission and delayed progression.
Registered clinician input was received from Lung Cancer Canada and the Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee. Registered clinicians indicated that the 2 standard-of-care treatments in Canada for patients with ALK-positive locally advanced or metastatic NSCLC are alectinib and brigatinib, as crizotinib and ceritinib are no longer commonly used. Registered clinicians described that current treatment goals for patients in practice include prolonging disease progression, increasing the duration of treatment response, reducing loss of cognition and memory, reducing the severity of symptoms, and minimizing adverse events (AEs). Important outcomes of treatment also include improving quality of life and maintaining independence. Although treatment goals can largely be achieved with alectinib in the first-line setting, lorlatinib is an alternative option in the first-line setting because it addresses an unmet need by extending PFS and OS. Lorlatinib may also fulfill an unmet need in later lines of therapy (e.g., second-line onward). Registered clinicians indicated that routine lung cancer tests, including ALK testing, would help identify which patients are best suited for lorlatinib. Additionally, clinical response is determined by a response rate, an improvement in symptoms, or major motor milestones. Treatment response is assessed every few cycles of treatment, as required.
Feedback from the drug plans indicated that currently available treatment options for the indicated population include alectinib, brigatinib, and crizotinib, as alectinib and brigatinib have demonstrated superiority to crizotinib. Despite this, drug plans raised concerns about the fact that the CROWN trial did not consider all relevant comparators but compared lorlatinib to crizotinib. Drug plans are unclear whether switching treatment to lorlatinib is possible for patients who are currently being treated with crizotinib, alectinib, or brigatinib. Drug plans anticipate a potential change in the place in therapy for alectinib and brigatinib with the introduction of lorlatinib, as well as for other drugs in subsequent lines of therapy, and they are unsure about the sequential use of TKIs after lorlatinib. In regard to the budget impact of lorlatinib, drug plans noted that the price of lorlatinib should not be more than the prices of alectinib or brigatinib, although oral medications are funded differently across jurisdictions.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included alectinib and brigatinib as comparators in the submitted economic evaluation. Hazard ratios (HRs) for the relative efficacy for alectinib and brigatinib were derived using an NMA.
The sponsor’s model considered the impact of TKIs on CNS progression, OS, and quality of life.
Based on the information provided by the sponsor, crossover was not permitted in the CROWN trial. For alectinib and brigatinib, the sponsor applied crossover-adjusted HRs for OS and PFS benefits. These adjusted HRs were also applied to the CADTH base case.
Several of these concerns were addressed in CADTH reanalyses:
The sponsor included crizotinib as a comparator in the submitted economic evaluation. CADTH undertook a scenario analysis in which crizotinib was removed as a relevant comparator.
CADTH was unable to address the following concerns raised from stakeholder input:
CADTH was unable to assess the effects of subsequent TKIs on PFS and OS due to the limitation of PSM. The PSM does not allow to explicitly account for subsequent therapies as additional health states.
Based on information provided by the sponsor, some patients who discontinued study treatment in the crizotinib arm of the CROWN trial received lorlatinib in subsequent lines of therapy, and some patients who discontinued study treatment in the lorlatinib arm received crizotinib in subsequent lines of therapy.
Economic Review
The current review is for lorlatinib (Lorbrena) for the first-line treatment for patients with ALK-positive advanced NSCLC.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for lorlatinib with the current standards of care (i.e., crizotinib, alectinib, and brigatinib) for the first-line treatment for patients with ALK-positive advanced NSCLC.1 The target population for the sponsor’s economic evaluation aligns with the reimbursement request and Health Canada–indicated population.
Lorlatinib is available as 25 mg and 100 mg tablets. The recommended dosage for lorlatinib is 100 mg administered orally once daily until disease progression or unacceptable toxicity. At the submitted price of $112.44 for a 25 mg tablet of lorlatinib or $337.33 for a 100 mg tablet of lorlatinib, and based on the sponsor’s distribution of doses, the 28-day cycle cost is $8,982.1 The per-cycle costs for the comparator treatments were $7,011 for crizotinib, $9,030 for alectinib, and $8,068 for brigatinib.1
The clinical outcomes of interest were QALYs and life-years.1 The model simulated costs and clinical outcomes for each treatment regimen over a lifetime horizon (30 years) from the perspective of Canada’s publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.1
Model Structure
The sponsor used a PSM consisting of 4 health states: progression-free, non–CNS-progressed disease, CNS-progressed disease, and death (Figure 1, Appendix 3).2 Unlike most PSMs, an additional health state was added by the sponsor to capture the impact of lorlatinib on intracranial progression. All patients enter the model in the progression-free health state, where they receive either lorlatinib or a comparator treatment. Patients may either remain progression-free or their disease may progress (non-CNS or CNS progression), or they may die. Non–CNS-progressed patients could remain in the same state, experience CNS progression, or move to death. Patients with CNS-progressed disease could either remain alive with CNS progression or transition to death. Death is modelled as an absorbing state. The sponsor further divided the alive states by treatment status (on or off treatment) as ToT was modelled independent of PFS.1
Model Inputs
The baseline characteristics of the modelled patient cohort were based on the CROWN trial,3 which compared the efficacy of lorlatinib with crizotinib for the first-line treatment for patients with advanced ALK-positive NSCLC. The mean baseline age of patients in the CROWN trial was 57.4 years.
Efficacy outcomes (OS, CNS-PFS, PFS) for lorlatinib and crizotinib were based on the CROWN trial. Survival curves were extrapolated beyond the observed trial duration by fitting parametric survival models to the patient-level data. Curve selection was based on the clinical plausibility of long-term extrapolations, consistency of extrapolation across end points, consistency across treatments, and statistical goodness-of-fit measures (Akaike information criterion and Bayesian information criterion). However, the sponsor noted that some data from the CROWN trial were considered immature and goodness-of-fit measures were used where appropriate. Independent models were used to extrapolate efficacy outcomes for lorlatinib and crizotinib.1
An NMA was performed of HRs for PFS and OS for alectinib and brigatinib compared to crizotinib. The HRs were then applied to the baseline survival curves for crizotinib to extrapolate survival outcomes for alectinib and brigatinib. The sponsor indicated that an NMA could not be performed to derive HRs for CNS-PFS because these data are not commonly reported in the included trials (of note: CNS-PFS is the same as intracranial PFS [IC-PFS] referred to in the CADTH Clinical Review). The sponsor’s model assumed that the estimated HR for PFS for a given treatment versus crizotinib derived from the NMA is equal to the HR for CNS-PFS.1
The ToT curves for lorlatinib and crizotinib were derived from the patient data from the CROWN trial. For alectinib and brigatinib, ToT was estimated from the median treatment duration reported in the literature.4 Patients in all treatment arms could continue to receive treatment after progression if the modelled ToT curve was greater than the PFS curve.
The sponsor’s model incorporated relevant all-cause AEs of grade 3 and above that were observed in more than 2% of patients in at least 1 of the treatment arms of the CROWN trial. AE treatment costs were extracted from the Ontario Case Costing Initiative.5 Additional resource use was determined based on clinical expert opinion. The sponsor calculated the total AE costs based on the annual incidence rate of each AE and its annual costs.
The sponsor applied a crosswalk algorithm to derive EQ-5D 3-Levels (EQ-5D-3L) questionnaire data from the EQ-5D 5-Levels (EQ-5D-5L) questionnaire data collected in the CROWN trial. Utility values for progression-free and progressed health states were derived using the EQ-5D-3L data. Utility values derived by treatment status (on or off treatment) and health state were applied in the sponsor’s base case. A multiplier sourced from literature6 was applied to utility values to account for the impact of CNS progression. An annual utility decrement for AEs and age-related utility adjustment7 was obtained from literature and incorporated in the model. The model assumed that the duration of all AEs in the model was 5 days.
Costs were measured from a publicly funded health systems perspective. Unit costs for were sourced from the Ontario Drug Benefit (ODB) Formulary schedule of benefits and the Ontario Nurses Collective Agreement.8 Treatment costs for lorlatinib were based on dose distributions from the CROWN trial. For all other treatments, the sponsor’s model applied the relative dose intensity (RDI) to account for dose interruptions and reductions or noncompliance.
Resource use (frequency and proportion of patients requiring each resource) was based on clinical expert opinion to reflect current standard of care in Canada.
One-time costs of subsequent treatment were applied to patients upon progression. For lorlatinib, alectinib, and brigatinib, it was assumed that 100% of patients received chemotherapy upon progression. For crizotinib, the sponsor assumed that patients received alectinib (90%), ceritinib (5%), lorlatinib (5%), or chemotherapy (5%) upon progression. The proportion of patients who received subsequent treatment was determined as the proportion of patients who transition out of the “progression-free” state in each cycle without dying. This proportion was estimated based on the proportion of progression events (exclusive of death) for the full population and was assumed to be constant over time and across all treatment arms. Subsequent treatment distributions were elicited from clinical experts in Canada, whereas durations and dosing schedules9-14 were sourced from the literature and product monographs.
The sponsor’s model applied a one-time end-of-life cost to all patients transitioning to death that was obtained from a study by Cheung et al. (2015).15 The study by Cheung et al. used population-level health administrative databases to identify costs of end-of-life cancer care among adult patients in Canada. In addition, a one-off cost of ALK testing ($133) was applied to 100% of patients in all treatment arms upon entry into the model.16 Sensitivity and specificity were not considered in the sponsor’s model.
Summary of Sponsor’s Economic Evaluation Results
Base-Case Results
The sponsor presented results from a probabilistic analysis based on 2,000 iterations. CADTH noted that there was a difference between the deterministic and probabilistic results despite the increased number of iterations, which appeared to be primarily driven by immature OS data and uncertainty surrounding the HRs of the NMA. The probabilistic findings are presented in Table 3. Results from deterministic analysis are presented in Table 12. The submitted analyses were based on the publicly available prices of the comparators and subsequent treatments.
Results from a sequential analysis showed that brigatinib was extendedly dominated by alectinib, and alectinib was extendedly dominated by lorlatinib. Lorlatinib was associated with an ICER of $128,964 per QALY gained compared to crizotinib (Table 3). For lorlatinib, 83% of the incremental QALYs gained compared to crizotinib were accrued beyond the trial follow-up period and were based on extrapolated survival outcomes.
Table 3: Summary of the Sponsor’s Economic Evaluation Results — Probabilistic Analysis
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
Crizotinib | 250,238 | 3.48 | Reference |
Lorlatinib | 588,308 | 6.10 | 128,964 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Only treatments included on the cost-effectiveness frontier are included. Full results are reported in Appendix 3.
Source: Sponsor’s pharmacoeconomic report.1
The probability of lorlatinib being cost-effective compared to alectinib, brigatinib, and crizotinib was 0.5% at a WTP threshold of $50,000 per QALY. A breakdown of costs and QALYs by health state is presented in Table 13, Appendix 3. A breakdown by cost category is described in Table 15, Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor performed a series of scenario analyses by varying the discount rate, time horizon, study perspective, and utility values and incorporating drug wastage for subsequent treatments and sources used to determine subsequent treatment durations (Table 16, Appendix 3). However, these analyses were only provided as pairwise comparisons, and are therefore of limited use to CADTH for this review. Results from the sponsor’s scenario analyses showed that the cost-effectiveness findings were influenced by changes to the time horizon, perspective of analysis, and applying an RDI for lorlatinib.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Uncertainty associated with the long-term comparative efficacy: In the sponsor’s model, survival outcomes (OS, PFS, CNS-PFS) for lorlatinib and crizotinib were extrapolated using data from the CROWN trial; HRs for PFS and OS benefits for alectinib and brigatinib (versus crizotinib) were derived based on an NMA. Data from the CROWN trial — specifically the OS data for both lorlatinib and crizotinib, and the CNS-PFS (derived via intracranial time to progression) data for lorlatinib — were immature. This immaturity in the data results in significant uncertainty in the extrapolated survival outcomes beyond the trial duration. There was substantial variation in the predicted proportion of patients alive at 10 years for lorlatinib (36% to 71%) and crizotinib (18% to 55%) based on alternative extrapolated parametric distributions for OS, despite similar models’ goodness of fit. Significant uncertainty was also observed in the predicted proportion of patients alive and free of intracranial progression at 10 years for lorlatinib (45% to 87%) based on alternative extrapolated parametric distributions for CNS-PFS. Although the sponsor’s base case was based on conservative survival estimates (relative to other distributions provided), the validity of the extrapolated outcomes remains unknown due to the lack of long-term data.
Efficacy for alectinib and brigatinib was derived using an NMA. However, evidence from the NMA was uncertain due to clinical and methodological heterogeneity across included studies related to differences in baseline patient characteristics (patient’s race, presence of brain metastases, and previous history of therapy) and trial design (treatment crossover and dosing). Moreover, when results from the NMA were used with the CROWN trial, the extrapolated outcomes for alectinib and brigatinib lacked face validity. The clinical experts consulted by CADTH indicated that the differences in the derived OS benefit for alectinib and brigatinib were not aligned with clinical expectations; in practice, the OS benefit was considered comparable between alectinib and brigatinib. Furthermore, published evidence suggests that that there are no significant differences in PFS between the brigatinib and alectinib arms, although this is based on a slightly different population.17
Feedback from clinical experts consulted by CADTH indicated that the extrapolated OS benefit for lorlatinib relative to alectinib and brigatinib may be overestimated. CADTH noted that, because the median follow-up times are longer for alectinib and brigatinib in the sponsor’s model (163 weeks and 107 weeks, respectively) than for lorlatinib (79 weeks), the extrapolated survival benefits beyond trial duration were much greater for lorlatinib than for alectinib and brigatinib. Given that 83% of survival for lorlatinib was realized beyond trial duration based on extrapolated survival outcomes, CADTH tested the assumptions on the exploration of long-term outcomes through scenario analyses.
The identified uncertainty related to long-term survival outcomes is reflected in the limitations identified within the CADTH Clinical Review with respect to the identified comparative clinical evidence and discrepancy between deterministic and probabilistic results. The sources of uncertainty in the extrapolated outcomes and CADTH reanalyses to address these limitations include the following:
CADTH performed a reanalysis assuming equal HRs for OS for alectinib and brigatinib as part of the CADTH base case.
CADTH performed 1-way scenario analyses using alternative parametric models to predict OS beyond the trial duration, assuming equivalence of OS for lorlatinib, alectinib, and brigatinib.
Model structure is inappropriate: The sponsor acknowledged that the OS and PFS data are highly immature, particularly for lorlatinib; however, the sponsor indicated that it was inappropriate to extrapolate such outcomes to inform a state-transition model because this would result in greater uncertainty than using the partitioned survival approach. Although the PSM approach is commonly used in previous health technology assessments of oncology treatments, it does not explicitly model progression, and would therefore inaccurately reflect the long-term impact of lorlatinib beyond the trial duration. This concern is likely to be conflated with immature data. Structural assumptions imposed by the PSM (non–mutually exclusive OS and PFS curves) could introduce a post-progression survival bias that favours lorlatinib.
CADTH could not address this limitation.
Treatment waning was not incorporated: The sponsor did not incorporate treatment waning for any of the treatments considered in the model. This assumption could benefit lorlatinib as the extrapolated OS benefit for lorlatinib relative to comparators in the sponsors model persists over the entire time horizon of the model (30 years). The clinical experts consulted by CADTH advised that ALK inhibitors, including lorlatinib, are likely to become less effective over time, although it is unclear when the decline in treatment effect would be observed.
CADTH performed scenario analysis by incorporating treatment waning in the model.
The ToT assumptions do not align with clinical practice or expectation: The sponsor estimated ToT for alectinib and brigatinib from the median treatment duration reported in literature. The extrapolated median ToT was higher for alectinib (2.29 years) compared with brigatinib (1.99 years). Clinical experts consulted by CADTH advised that treatment durations for both treatments are comparable in clinical practice.
CADTH performed a reanalysis by assuming equal ToT for alectinib and brigatinib.
Inappropriate costs of subsequent therapy and management of CNS progression: In the sponsor’s model, resource use estimates and assumptions applied to estimate costs of subsequent therapy and management of CNS progression were based on expert opinion. The sponsor’s model assumed that 50% of patients who progress on subsequent chemotherapy would receive third- or fourth-line immunotherapy. The clinical experts consulted by CADTH advised that this proportion was expected to be lower based on clinical practice. They also suggested revisions to resource use estimates for CNS progression to reflect the standard of care in Canada.
Based on input provided by clinical experts, CADTH revised the proportion of patients receiving third- or fourth-line immunotherapy and resource use estimates for CNS progression as part of its reanalysis.
CADTH also identified the following limitations in the sponsor’s model; however, these are not expected to have a significant impact on cost-effectiveness findings.
Underestimation of survival benefit of comparators: The sponsor’s model did not incorporate survival benefits resulting from subsequent therapies for progressed patients. According to the clinical experts consulted by CADTH, this limitation would likely underestimate the survival of patients in comparator treatments arms. However, the use of a PSM makes it difficult to incorporate additional subsequent treatment states to capture the survival benefits of subsequent therapies for progressed patients.
CADTH was unable to address this limitation due to the constraint of the structure of the submitted model.
Important adverse events were not considered: The sponsor’s model incorporated all-cause AEs of grade 3 and above that were observed in more than 2% of patients in at least 1 treatment arm of the CROWN trial. The clinical experts consulted by CADTH indicated that the economic model should also capture the impact of ALK inhibitors on neurological AEs (such as mood or cognitive disorder), early pulmonary toxicity, weight gain, and fatigue.
Because data pertaining to these AEs were unavailable for alectinib and brigatinib in the data sources used by the sponsor, CADTH was unable to include these AEs in its reanalysis. However, inclusion of these AEs is unlikely to have a significant impact on incremental costs or QALYs due to the low incidence of these events.
Relative dose intensity: The sponsor applied the RDI approach for crizotinib, alectinib, and brigatinib, and incorporated a detailed dosing distribution for lorlatinib based on the CROWN trial. The sponsor applied an RDI for lorlatinib as part of scenario analysis. The clinical experts consulted by CADTH indicated that the RDI values for alectinib and lorlatinib in the sponsor’s model were not aligned with clinical practice.
Revised RDI values were used as part of CADTH reanalysis. CADTH also performed a scenario analysis by assuming the RDI was equal to 100% (no dose interruptions) for all treatments to account for the limitations with the use of RDI as a composite input.
Distribution for costs: The sponsor applied a normal distribution for costs in the probabilistic sensitivity analysis.
CADTH considered this inappropriate, as a normal distribution may not capture the skewness of cost data, and corrected for this in the reanalysis by using a gamma distribution.
CADTH also appraised several key assumptions made by the sponsor (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Due to a lack of data, the sponsor assumed that the HRs for PFS derived from the NMA were applicable to CNS-PFS end points. | CADTH was unable to assess whether this assumption is appropriate, and how it may affect the cost-effectiveness findings due to the lack of an alternative data source. |
The sponsor’s model assumed that patients in all treatment arms could continue to receive treatment beyond progression if the ToT curves are greater than the PFS curves. | Acceptable. However, clinical experts consulted by CADTH indicated that treatment with crizotinib, alectinib, and brigatinib is not typically given beyond progression and that, if used, treatment beyond progression is short. CADTH explored the impact of this assumption as part of scenario analyses. |
The proportion of patients who received subsequent treatments was estimated based on the proportion of PFS events that were not death for the full population and was assumed to be constant over time and across all treatment arms. | Appropriate. |
The sponsor assumed a 10% SE of uncertainty in cases where the SE for an input parameter was not reported in the original data source. | Inappropriate. Due to paucity of data, a wider variation in SE (i.e., 20%) should be applied. CADTH replaced 10% SE with 20% in all reanalyses. |
HR = hazard ratio; IC = intracranial; PFS = progression-free survival; NMA = network meta-analysis; SE = standard error; ToT = time on treatment.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH could not address the limitations resulting from immature trial data and model structure. The CADTH base case was derived by applying the following corrections to the sponsor’s base case: a 20% variance (20% of the mean values) for parameters without known standard errors, and a gamma distribution for cost data. In addition, the CADTH base case assumed equivalence of OS benefit and ToT for alectinib and brigatinib, and incorporated revised estimates for resources required to manage CNS progression, subsequent treatment distribution, and dose intensity for alectinib.
Table 5 details each change made to derive the CADTH revised base case, which was conducted in a stepwise approach to emphasize the impact of each change. The summary of results from the reanalysis are presented in Table 6.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Variance for parameters without known standard errors | 10% of the mean values | 20% of the mean values |
2. Distribution applied for cost data | Normal | Gamma |
Changes to derive the CADTH base case | ||
1. OS for alectinib and brigatinib | Median HR for OS (95% CI):
| HR for OS for brigatinib is assumed equal to alectinib; i.e., Median HR for OS 995% CI):
|
2. Time on treatment | Median ToT (years):
| ToT curve modelled for brigatinib was applied to both alectinib and brigatinib Median ToT (years):
|
3. Resource use estimates for patients who experience CNS progression | Proportion of CNS-progressed patients who undergo WBRT = 10% | Proportion of CNS-progressed patients who undergo WBRT = 25% |
4. Subsequent treatment distribution: proportion of patients on third- or fourth-line immunotherapy | 50% | 10% |
5. RDI for alectinib | RDI = 95.6%, as per the ALEX trial4 | RDI = 85%, based on inputs provided by clinical experts |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 + 5 | |
CI = confidence interval; CNS = central nervous system; HR = hazard ratio; OS = overall survival; RDI = relative dose intensity; ToT = time on treatment; WBRT = whole-brain radiotherapy; vs. = versus.
Results from the CADTH revised base case showed that alectinib was extendedly dominated by brigatinib; however, the ICERs for alectinib and brigatinib compared to crizotinib were comparable. The sequential analysis shows that the ICER for brigatinib compared to crizotinib was $116,289 per QALY and the ICER for lorlatinib compared to brigatinib was $147,368 per QALY. The probability of lorlatinib being cost-effective compared to crizotinib, alectinib, and brigatinib at a WTP threshold of $50,000 was 1.4%. Stepped analysis showed that the sponsor’s base-case results were influenced most by the assumptions regarding the relative difference in OS between alectinib and brigatinib (Table 17, Appendix 4). Disaggregated results from the CADTH revised base case are presented in Table 18 (Appendix 4).
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER vs. reference ($/QALY) | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor-corrected base case | ||||
Crizotinib | 250,431 | 3.59 | Reference | — |
Alectinib | 511,238 | 5.06 | 177,724 | Extendedly dominated through crizotinib and lorlatinib |
Brigatinib | 413,984 | 4.45 | 190,259 | Extendedly dominated through crizotinib and lorlatinib |
Lorlatinib | 589,455 | 6.12 | 134,027 | 134,027 |
CADTH base case | ||||
Crizotinib | 252,599 | 3.59 | Reference | — |
Alectinib | 421,908 | 5.04 | 117,021 | Extendedly dominated through crizotinib and brigatinib |
Brigatinib | 422,491 | 5.05 | 116,289 | 116,289 |
Lorlatinib | 581,212 | 6.13 | 129,478 | 147,368 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Scenario Analysis Results
CADTH performed a scenario analysis to evaluate the impact of the following model parameters and assumptions: OS benefit for lorlatinib relative to alectinib and brigatinib, alternative PSMs to extrapolate OS, applying treatment waning, estimates for resources required for CNS-progressed patients, incorporating RDI for lorlatinib, using alternative utility values, and a revised comparator set. A description of the scenario analyses undertaken by CADTH is presented in Appendix 4.
Results from scenario analysis are presented in Table 22, Appendix 4. Results were most sensitive to the assumptions regarding OS benefit for lorlatinib relative to alectinib and brigatinib, and incorporated a treatment-waning assumption and the parametric models used to extrapolate long-term OS. For all but 2 of these analyses, the sequential ICER for lorlatinib was greater than in the CADTH base case. The ICER for lorlatinib increased to $318,255 per QALY when treatment waning was incorporated for alectinib, brigatinib, and lorlatinib. However, the ICER for lorlatinib decreased when an RDI approach using estimates provided by clinical experts was incorporated for lorlatinib. Results were robust to changes in CNS progression, resource use estimates, and utility values.
A price-reduction analysis was performed based on the sponsor’s and CADTH’s revised base-case analyses (Table 7). Results from the price-reduction analysis showed that a reduction of at least 42% is required for lorlatinib to be cost-effective compared to crizotinib, brigatinib, and alectinib at a WTP threshold of $50,000 per QALY. Alectinib and brigatinib were extendedly dominated in all price-reduction scenarios, and their ICERs are therefore not reported. If alternative pricing arrangements are in place for any of the comparator treatments, the price reduction reported by CADTH may not accurately reflect the price reduction required to achieve an ICER of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for lorlatinib vs. comparators ($ per QALY)a | |
|---|---|---|
Price reduction | Sponsor base case | CADTH base-case reanalysis |
No price reduction | If WTP < $128,964 per QALY, crizotinib is optimal If WTP > $128,964 per QALY, lorlatinib is optimal | If WTP < $116,289 per QALY, crizotinib is optimal If WTP > $116,289 per QALY and < $147,368 per QALY, brigatinib is optimal If WTP > $147,368 per QALY, lorlatinib is optimal |
10% | If WTP < $107,694 per QALY, crizotinib is optimal If WTP > $107,694 per QALY, lorlatinib is optimal | If WTP < $109,404 per QALY, crizotinib is optimal If WTP > $109,404 per QALY, lorlatinib is optimal |
20% | If WTP < $90,619 per QALY, crizotinib is optimal If WTP > $90,619 per QALY, lorlatinib is optimal | If WTP < $88,985 per QALY, crizotinib is optimal If WTP > $88,985 per QALY, lorlatinib is optimal |
30% | If WTP < $72,481 per QALY, crizotinib is optimal If WTP > $72,481 per QALY, lorlatinib is optimal | If WTP < $71,250 per QALY, crizotinib is optimal If WTP > $71,250 per QALY, lorlatinib is optimal |
40% | If WTP < $54,234 per QALY, crizotinib is optimal If WTP > $54,234 per QALY, lorlatinib is optimal | If WTP < $51,687 per QALY, crizotinib is optimal If WTP > $51,687 per QALY, lorlatinib is optimal |
42% | If WTP < $50,610 per QALY, crizotinib is optimal If WTP > $50,610 per QALY, lorlatinib is optimal | If WTP < $48,903 per QALY, crizotinib is optimal If WTP > $48,903 per QALY, lorlatinib is optimal |
50% | If WTP < $35,422 per QALY, crizotinib is optimal If WTP > $35,422 per QALY, lorlatinib is optimal | If WTP < $33,315 per QALY, crizotinib is optimal If WTP > $33,315 per QALY, lorlatinib is optimal |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness to pay.
aAlectinib and brigatinib are extended dominated by lorlatinib in all scenarios.
Issues for Consideration
A study by Li et al. evaluated the cost-effectiveness of lorlatinib compared to crizotinib in patients with previous, untreated, advanced ALK-positive NSCLC.18 The analysis was performed from a US payer perspective, over a time horizon of 30 years, using efficacy data (OS and PFS) from an interim analysis of the CROWN trial. The ICER of lorlatinib compared to crizotinib reported in this study was much larger than those reported in the sponsor’s and CADTH’s base cases (Li et al.: $409,667 per QALY; sponsor’s base case: $128,96 per QALY; CADTH’s base case: $147,368 per QALY). CADTH could not identify the reason for such a large difference, although hypothesize that it may be due to differences in extrapolated survival outcome assumptions.
Lorlatinib, alectinib, and brigatinib are TKIs. The clinical experts consulted by CADTH advised that TKIs, including lorlatinib, may be used as subsequent therapy among patients who experience disease progression, which may lead to increased health system costs. The economic submission did not allow for the consideration of any benefits associated with subsequent TKI use; the sponsor’s PSM approach only allowed incorporation of the impact of subsequent therapies on costs. However, at present, TKIs are not commonly accessible as later-line treatments. If TKIs are used sequentially in practice, the budget impact of treatment of ALK-positive NSCLC will be greater than is currently estimated.
Overall Conclusions
Evidence from the CROWN trial showed that, compared to crizotinib, first-line treatment with lorlatinib led to a clinically meaningful and statistically significant improvement in PFS among patients with ALK-positive NSCLC. However, the OS data in the trial were immature and additional data are expected that may result in numerical differences to the current evidence. Because of the lack of head-to-head studies comparing lorlatinib to alectinib and brigatinib, the sponsor submitted an NMA. However, the indirect evidence is associated with uncertainty due to clinical and methodological heterogeneity across included studies in terms of baseline patient characteristics (race, presence of brain metastases, and previous history of therapy) and differences trial design. Furthermore, due to data limitations, the HRs for CNS-PFS for alectinib and brigatinib were based on PFS efficacy end points and may not accurately represent the population to which the PFS data are modelled. In the sponsor’s economic evaluation, the majority of the survival benefits for all treatment arms accrued beyond the trial duration. As a result, the sponsor’s cost-effectiveness estimates were influenced by the parametric models used to extrapolate long-term outcomes and assumptions on the relative benefit for the comparator treatments.
CADTH identified several limitations within the sponsor’s economic analysis. Substantial uncertainty was observed in the extrapolated OS and CNS-PFS outcomes, particularly for lorlatinib, due to immature trial data for these end points. Moreover, when results from the NMA were combined with those from the CROWN trial, clinical expert feedback indicated that the extrapolated survival outcomes lacked face validity. The sponsor did not incorporate treatment waning in the model, which could overestimate the survival benefit for lorlatinib relative to the comparators. CADTH also noted additional structural uncertainty because the use of a PSM does not explicitly account for progression. This structural assumption could introduce a post-progression survival bias that favours lorlatinib. Clinical experts consulted by CADTH also indicated that estimates used for resources required to manage CNS progression, subsequent treatment distribution, and dose intensities did not reflect clinical practice.
CADTH was unable to address all the limitations identified but made several corrections and revisions to the sponsor’s base case to derive the CADTH base case. CADTH corrected the sponsor’s model to apply more appropriate variance and distributions for specific parameters and incorporated alternative assumptions regarding OS, resources required to manage CNS progression, and subsequent treatment distribution, and used a dose intensity for alectinib that aligns with clinical practice.
In the CADTH base case, crizotinib, brigatinib, and lorlatinib were on the cost-effectiveness frontier. The ICER for brigatinib compared to crizotinib is $116,289 per QALY, and the ICER for lorlatinib compared to brigatinib is $147,368 per QALY. Although CADTH’s base case resulted in a higher ICER for lorlatinib compared with the sponsor’s base case ($128,964 per QALY versus $147,368 per QALY), both analyses provided consistent results, indicating that, at the submitted price, lorlatinib was not cost-effective at a WTP threshold of $50,000 per QALY. A price reduction of at least 42% would be required to make lorlatinib an optimal treatment option at a WTP threshold of $50,000 per QALY relative to the comparator treatments.
Further exploration of survival outcomes, duration of treatment effect, resource use, and utilities were assessed in scenario analyses. Results were highly sensitive to assumptions regarding the relative difference in OS between alectinib and brigatinib, OS benefit for lorlatinib relative to alectinib and brigatinib, application of treatment waning, and the parametric model used to extrapolate long-term outcomes. Results were robust to changes in resource use estimates for CNS progression, subsequent treatment distribution, and utility values. However, several limitations could not be addressed in the CADTH base-case and scenario analyses due to data limitations and constraints introduced by the submitted model structure.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lorbrena (lorlatinib): tablets, 25 and 100 mg, oral. Kirkland (QC): Pfizer Canada ULC; 2021 Jun 18.
2.Camidge DR, Kim HR, Ahn MJ, et al. Brigatinib Versus Crizotinib in Advanced ALK Inhibitor-Naive ALK-Positive Non-Small Cell Lung Cancer: Second Interim Analysis of the Phase III ALTA-1L Trial. J Clin Oncol. 2020;38(31):3592-3603. PubMed
3.Shaw AT, Bauer TM, de Marinis F, et al. First-Line Lorlatinib or Crizotinib in Advanced ALK-Positive Lung Cancer. N Engl J Med. 2020;383(21):2018-2029. PubMed
4.Mok T, Camidge DR, Gadgeel SM, et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann Oncol. 2020;31(8):1056-1064. PubMed
5.Ontario Case Costing Initiative (OCCI). Ontario Case Costing Initiative (OCCI). 2021: https://data.ontario.ca/en/dataset/ontario-case-costing-initiative-occi. . Accessed 2021 Sep 20.
6.Roughley A, Damonte E, Taylor-Stokes G, Rider A, Munk VC. Impact of Brain Metastases on Quality of Life and Estimated Life Expectancy in Patients with Advanced Non-Small Cell Lung Cancer. Value Health. 2014;17(7):A650. PubMed
7.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
8.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Jul 12.
9.National Institute for Health and Care Excellence. Brigatinib for ALK-positive advanced non-small-cell lung cancer that has not been previously treated with an ALK inhibitor. (Technology appraisal guidance 670) 2021; https://www.nice.org.uk/guidance/ta670. Accessed 2021 May 26.
10.Novello S, Mazières J, Oh IJ, et al. Alectinib versus chemotherapy in crizotinib-pretreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer: results from the phase III ALUR study. Ann Oncol. 2018;29(6):1409-1416. PubMed
11.Shaw AT, Kim TM, Crinò L, et al. Ceritinib versus chemotherapy in patients with ALK-rearranged non-small-cell lung cancer previously given chemotherapy and crizotinib (ASCEND-5): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017;18(7):874-886. PubMed
12.Kim DW, Tiseo M, Ahn MJ, et al. Brigatinib in Patients With Crizotinib-Refractory Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer: A Randomized, Multicenter Phase II Trial. J Clin Oncol. 2017;35(22):2490-2498. PubMed
13.CADTH pCODR Expert Review Committee (pERC) final recommendation: nivolumab (Opdivo). Ottawa (ON): CADTH; 2016 Jun 3: https://www.cadth.ca/sites/default/files/pcodr/nivolumab_opdivo_nsclc_fn_cgr.pdf. Accessed 2021 Sep 24.
14.CADTH pCODR Expert Review Committee (pERC) final recommendation: pembrolizumab (Keytruda). Ottawa (ON): CADTH; 2016 Nov 3: https://www.cadth.ca/sites/default/files/pcodr/pcodr_pembrolizumab_keytruda_nsclc_fn_cgr.pdf. Accessed 2021 Sep 24.
15.Cheung MC, Earle CC, Rangrej J, et al. Impact of aggressive management and palliative care on cancer costs in the final month of life. Cancer. 2015;121(18):3307-3315. PubMed
16.Johnston KM, Sheffield BS, Yip S, Lakzadeh P, Qian C, Nam J. Costs of in-house genomic profiling and implications for economic evaluation: a case example of non-small cell lung cancer (NSCLC). J Med Econ. 2020;23(10):1123-1129. PubMed
17.Ando K, Akimoto K, Sato H, et al. Brigatinib and Alectinib for ALK Rearrangement-Positive Advanced Non-Small Cell Lung Cancer With or Without Central Nervous System Metastasis: A Systematic Review and Network Meta-Analysis. Cancers (Basel). 2020;12(4). PubMed
18.Li S, Li J, Peng L, Li Y, Wan X. Cost-Effectiveness of Lorlatinib as a First-Line Therapy for Untreated Advanced Anaplastic Lymphoma Kinase-Positive Non-Small Cell Lung Cancer. Front Oncol. 2021;11:684073. PubMed
19.CADTH Pharmacoeconomic Report: brigatinib (Alunbrig). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/pcodr/Reviews2021/10230BrigatinibALK%2BNSCLC_fnEGR_REDACT-ABBREV_EC21Apr2021_final.pdf. Accessed 2021 Sep 20.
20.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lorbrena (lorlatinib): tablets, 25 and 100 mg, oral. Kirkland (QC): Pfizer Canada ULC; 2021 Jun 18.
Appendix 1: Cost-Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost-Comparison Table for Non–Small Cell Lung Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Lorlatinib (Lorbrena) | 25 mg 100 mg | Tablet | $112.4443 $337.3333 | 100 mg once daily | 337.33 | 123,126 |
Kinase inhibitors | ||||||
Alectinib (Alecensaro) | 150 mg | Capsule | 42.1666 | 600 mg twice daily | 337.33 | 123,126 |
Brigatinib (Alunbrig) | 30 mg 90 mg 180 mg | Capsule | 112.32 336.9643b 336.9643b | 90 mg daily for 7 days; 180 mg daily thereafter | 336.96 | 122,990 |
Crizotinib (Xalkori) | 200 mg 250 mg | Tablet | 130.0000 | 250 mg twice daily | 260.00 | 94,900 |
Note: All prices are from the Ontario Exceptional Access Program (accessed August 2021), unless otherwise indicated, and do not include dispensing fees.
aSponsor-submitted price.
bBased on CADTH review of brigatinib (Alunbrig).19
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | No | See CADTH appraisal section |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | See CADTH appraisal section |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | See CADTH appraisal section |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
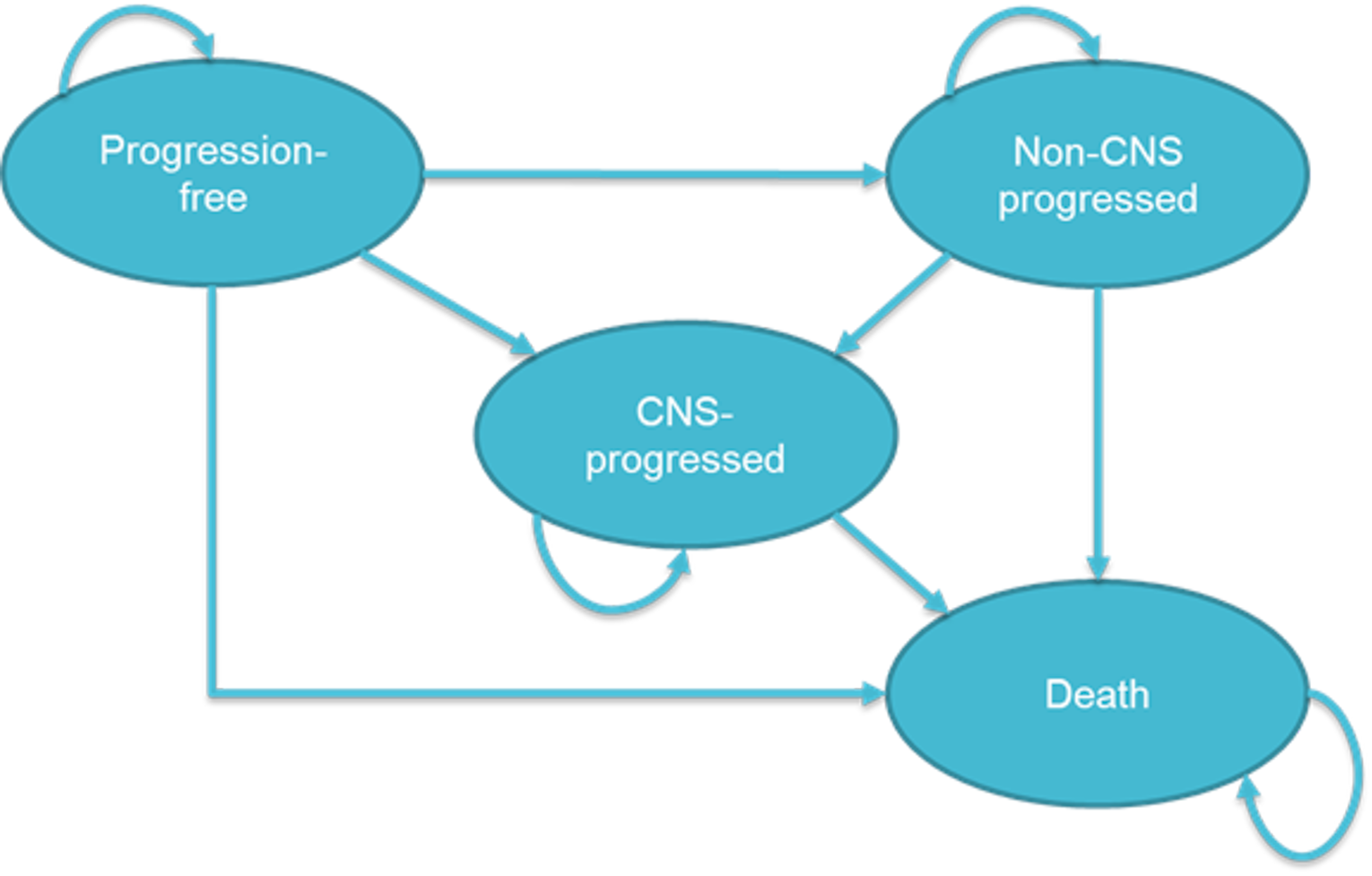
Table 10: Health State Occupancy
Health state | Occupancy at time T |
|---|---|
Progression-free on treatment | MIN (PFST, ToTT) |
Progression-free off treatment | MAX (0, PFST minus ToTT) |
Non–CNS progressed on treatment | MAX (0, MIN [CNS-PFST, ToTT] minus PFST) |
Non–CNS progressed off treatment | MAX (0, CNS-PFST minus MAX [PFST, ToTT]) |
CNS progressed on treatment | MAX (0, ToTT minus CNS-PFST) |
CNS progressed off treatment | OST minus MAX (CNS-PFST, ToTT) |
Death | 1 minus OST |
CNS = central nervous system; MAX = maximum; MIN = minimum; OS = overall survival; PFS = progression-free survival; T = time; ToT = time on treatment.
Note: The CNS-PFS, PFS, and ToT curves in the model are capped to be less than OS at any given time.
Detailed Results of the Sponsor’s Base Case
Table 11: Summary of the Sponsor’s Economic Evaluation Results — Probabilistic Analysis
Drug | Total costs ($) | Total QALYs | Total LYs | ICER vs. reference | Sequential ICER ($ per QALY) |
|---|---|---|---|---|---|
Crizotinib | $250,238 | 3.48 | 5.63 | Ref. | Reference |
Brigatinib | $412,992 | 4.36 | 6.45 | 185,791 | Extendedly dominated through crizotinib and lorlatinib |
Alectinib | $511,149 | 4.96 | 7.54 | 176,245 | Extendedly dominated through crizotinib and lorlatinib |
Lorlatinib | $588,308 | 6.1 | 8.20 | 128,964 | $128,964 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 12: Summary of the Sponsor’s Economic Evaluation Results — Deterministic Analysis
Drug | Total costs ($) | Total QALYs | Total LYs | ICER vs. reference | Sequential ICER ($/QALY) |
|---|---|---|---|---|---|
Crizotinib | $248,918 | 3.38 | 5.47 | Reference | Reference |
Brigatinib | $419,611 | 4.2 | 6.11 | $208,162 | Extendedly dominated through crizotinib and lorlatinib |
Alectinib | $512,608 | 4.85 | 7.33 | $179,381 | Extendedly dominated through crizotinib and lorlatinib |
Lorlatinib | $578,403 | 6.21 | 8.21 | $116,426 | $116,426 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Cost and QALY Breakdown by Health State — Probabilistic Results
Treatments | Progression-free | Non–CNS progressed | CNS progressed | Death | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | |
Lorlatinib | $478,034 | 3.45 | $77,792 | 2.38 | $15,506 | 0.27 | $16,976 | — | $588,308 | 6.10 |
Crizotinib | $106,890 | 1.01 | $51,400 | 0.45 | $73,549 | 2.03 | $18,399 | — | $250,238 | 3.48 |
Alectinib | $295,485 | 2.00 | $107,484 | 0.87 | $90,702 | 2.10 | $17,478 | — | $511,149 | 4.96 |
Brigatinib | $261,937 | 2.03 | $67,026 | 0.80 | $66,079 | 1.53 | $17,950 | — | $412,992 | 4.36 |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 14: Cost and QALY Breakdown by Health State — Deterministic Results
Treatments | Progression-free | Non–CNS progressed | CNS progressed | Death | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | |
Lorlatinib | $514,090 | 3.48 | $46,981 | 2.74 | $0 | 0.00 | $17,331 | — | $578,403 | 6.21 |
Crizotinib | $108,172 | 1.00 | $49,507 | 0.44 | $72,577 | 1.95 | $18,661 | — | $248,918 | 3.38 |
Alectinib | $295,235 | 1.98 | $126,704 | 0.88 | $72,726 | 1.99 | $17,943 | — | $512,608 | 4.85 |
Brigatinib | $270,292 | 2.02 | $66,960 | 0.86 | $63,921 | 1.32 | $18,438 | — | $419,611 | 4.20 |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 15: Cost Breakdown by Cost Category — Probabilistic Results
Treatments | Treatment costs | Administration costs | Subsequent treatment costs | ALK testing costs | Resource use costs | EOL costs | AE costs |
|---|---|---|---|---|---|---|---|
Lorlatinib | $495,189 | $0 | $20,217 | $133 | $55,298 | $16,976 | $496 |
Crizotinib | $103,471 | $0 | $45,468 | $133 | $82,438 | $18,399 | $330 |
Alectinib | $381,884 | $0 | $20,697 | $133 | $90,356 | $17,478 | $603 |
Brigatinib | $294,731 | $0 | $20,590 | $133 | $79,350 | $17,950 | $238 |
AE = adverse event; ALK = anaplastic lymphoma kinase; EOL = end of life; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 16: Results From Scenario Analysis — Probabilistic Analysis (1,000 Iterations)
Scenario | Base-case setting | Pairwise ICER | ||
|---|---|---|---|---|
Crizotinib (vs. lorlatinib) | Alectinib (vs. lorlatinib) | Brigatinib (vs. lorlatinib) | ||
Base case | — | $128,964 | $67,622 | $100,444 |
Discount rates for costs and QALYs: 3% | 1.50% | $135,275 | $65,396 | $105,008 |
Discount rates for costs and QALYs: 0% | $124,209 | $68,276 | $96,601 | |
Time horizon: 10 years | 30 years | $182,553 | $74,389 | $136,885 |
Time horizon: 20 years | $136,399 | $64,397 | $102,899 | |
Time horizon: 40 years | $124,652 | $59,862 | $98,983 | |
Perspective: Societal | Non-societal | $143,165 | $74,678 | $115,437 |
RDI: Exclude and detailed dosing for lorlatinib | Include | $140,771 | $79,872 | $89,445 |
Utility: TA563 (ALEX) | CROWN (by health state and treatment status) | $132,278 | $68,468 | $98,451 |
Utility: TA670 (ALTA 1L) | $139,833 | $69,191 | $108,932 | |
Drug wastage subsequent treatments: Exclude | Include | $132,771 | $71,918 | $103,344 |
Source of subsequent treatment durations: TA670 | Literature (based on second-line cost-effectiveness model for lorlatinib) | $100,582 | $66,524 | $98,636 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus; RDI = relative dose intensity.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses
Note this appendix has not been copy-edited.
Table 17: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER vs. reference ($ per QALY) | Sequential ICER ($ per QALY) |
|---|---|---|---|---|---|
Sponsor’s base case | Crizotinib | $250,238 | 3.48 | Reference | — |
Alectinib | $412,992 | 4.36 | $185,791 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $511,149 | 4.96 | $176,245 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $588,308 | 6.10 | $128,964 | $128,964 | |
Sponsor’s corrected base case | Crizotinib | $250,431 | 3.59 | Reference | — |
Alectinib | $413,984 | 4.45 | $190,259 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $511,238 | 5.06 | $177,724 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $589,455 | 6.12 | $134,027 | $134,027 | |
CADTH reanalysis 1 OS for alectinib and brigatinib | Crizotinib | $250,488 | 3.49 | Reference | — |
Alectinib | $424,893 | 4.93 | $121,079 | $121,079 | |
Brigatinib | $508,598 | 4.95 | $177,696 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $588,311 | 6.14 | $127,643 | $135,482 | |
CADTH reanalysis 2 Time on treatment | Crizotinib | $250,115 | 3.48 | Reference | — |
Alectinib | $414,032 | 4.36 | $187,672 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $461,926 | 4.92 | $147,241 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $587,228 | 6.19 | $124,418 | $124,418 | |
CADTH reanalysis 3 Resource use estimates for patients who experience CNS progression | Crizotinib | $251,856 | 3.45 | Reference | — |
Alectinib | $416,096 | 4.36 | $181,129 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $512,440 | 4.91 | $178,448 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $590,868 | 6.09 | $128,502 | $128,502 | |
CADTH reanalysis 4 Subsequent treatment distribution | Crizotinib | $249,931 | 3.49 | Reference | — |
Alectinib | $406,369 | 4.34 | $183,806 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $503,683 | 4.95 | $173,803 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $583,200 | 6.15 | $125,246 | $125,246 | |
CADTH reanalysis 5 Relative dose intensity (RDI) for alectinib | Crizotinib | $249,898 | 3.48 | Reference | — |
Alectinib | $413,757 | 4.34 | $191,109 | Extendedly dominated through crizotinib and lorlatinib | |
Brigatinib | $467,128 | 4.92 | $150,679 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $585,721 | 6.12 | $127,214 | $127,214 | |
CADTH base case (reanalysis 1+2+3+4+5) | Crizotinib | $252,599 | 3.59 | Reference | — |
Alectinib | $421,908 | 5.04 | $117,021 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $422,491 | 5.05 | $116,289 | $116,289 | |
Lorlatinib | $581,212 | 6.13 | $129,478 | $147,368 |
CNS = central nervous system; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Note: The CADTH reanalysis is based on publicly available prices of the comparator treatments.
Table 18: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. reference) | Incremental (sequential) |
|---|---|---|---|---|
Discounted LYs | ||||
Crizotinib | Progression-free | 1.22 | NA | NA |
Non–CNS progressed | 0.62 | NA | NA | |
CNS progressed | 3.82 | NA | NA | |
Total | 5.66 | NA | NA | |
Alectinib | Progression-free | 2.39 | 1.18 | NA |
Non–CNS progressed | 1.15 | 0.53 | NA | |
CNS progressed | 4.02 | 0.19 | NA | |
Total | 7.56 | 1.90 | NA | |
Brigatinib | Progression-free | 2.46 | 1.24 | 0.07 |
Non–CNS progressed | 1.17 | 0.55 | 0.03 | |
CNS progressed | 3.93 | 0.10 | −0.09 | |
Total | 7.56 | 1.90 | 0.00 | |
Lorlatinib | Progression-free | 4.23 | 3.01 | 1.77 |
Non–CNS progressed | 3.44 | 2.82 | 2.27 | |
CNS progressed | 0.56 | –3.26 | −3.36 | |
Total | 8.23 | 2.57 | 0.67 | |
Discounted QALYs | ||||
Crizotinib | Progression-free | 1.00 | NA | NA |
Non–CNS progressed | 0.45 | NA | NA | |
CNS progressed | 2.14 | NA | NA | |
Total | 3.59 | NA | NA | |
Alectinib | Progression-free | 1.98 | 0.97 | NA |
Non–CNS progressed | 0.85 | 0.40 | NA | |
CNS progressed | 2.22 | 0.07 | NA | |
Total | 5.04 | 1.45 | NA | |
Brigatinib | Progression-free | 2.03 | 1.02 | 0.05 |
Non–CNS progressed | 0.86 | 0.42 | 0.02 | |
CNS progressed | 2.16 | 0.02 | −0.05 | |
Total | 5.05 | 1.46 | 0.01 | |
Lorlatinib | Progression-free | 3.44 | 2.44 | 1.42 |
Non–CNS progressed | 2.39 | 1.94 | 1.53 | |
CNS progressed | 0.30 | –1.85 | −1.87 | |
Total | 6.13 | 2.54 | 1.08 | |
Discounted costs ($) | ||||
Crizotinib | Treatment costs | $103,512 | NA | NA |
Administration costs | $0 | NA | NA | |
Subsequent treatment costs | $45,146 | NA | NA | |
ALK testing costs | $132 | NA | NA | |
Resource use costs | $84,954 | NA | NA | |
EOL costs | $18,510 | NA | NA | |
AE costs | $344 | NA | NA | |
Total | $252,599 | NA | NA | |
Alectinib | Treatment costs | $297,766 | $194,254 | NA |
Administration costs | $0 | $0 | NA | |
Subsequent treatment costs | $13,136 | −$32,010 | NA | |
ALK testing costs | $132 | $0 | NA | |
Resource use costs | $92,738 | $7,783 | NA | |
EOL costs | $17,589 | −$920 | NA | |
AE costs | $548 | $203 | NA | |
Total | $421,908 | $169,310 | NA | |
Brigatinib | Treatment costs | $299,169 | $195,657 | $1,403 |
Administration costs | $0 | $0 | $0 | |
Subsequent treatment costs | $13,129 | −$32,017 | −$7 | |
ALK testing costs | $132 | $0 | $0 | |
Resource use costs | $92,233 | $7,278 | −$505 | |
EOL costs | $17,589 | −$920 | $0 | |
AE costs | $239 | −$105 | −$309 | |
Total | $422,491 | $169,892 | $582 | |
Lorlatinib | Treatment costs | $494,268 | $390,756 | $195,099 |
Administration costs | $0 | $0 | $0 | |
Subsequent treatment costs | $12,848 | −$32,298 | −$281 | |
ALK testing costs | $132 | $0 | $0 | |
Resource use costs | $56,395 | −$28,560 | −$35,838 | |
EOL costs | $17,072 | −$1,438 | −$517 | |
AE costs | $498 | $153 | $258 | |
Total | $581,212 | $328,613 | $158,721 | |
Treatment | ICER vs. reference ($) | Sequential ICER ($) | ||
Crizotinib | Reference | Reference | ||
Alectinib | $117,021 | Extendedly dominated through crizotinib and brigatinib | ||
Brigatinib | $116,289 | $116,289 | ||
Lorlatinib | $129,478 | $147,368 | ||
AE = adverse event; ALK = anaplastic lymphoma kinase; EOL = end of life; ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; vs. = versus.
Detailed Results of CADTH Base Case
Table 19: Results From CADTH Reanalysis — Deterministic
Drug | Total costs ($) | Total QALYs | Total LYs | ICER vs. reference | Sequential ICER ($ per QALY) |
|---|---|---|---|---|---|
Crizotinib | $250,497 | 3.38 | 5.47 | Reference | Reference |
Alectinib | $420,899 | 4.82 | 7.33 | $118,957 | Extendedly dominated through crizotinib and lorlatinib |
Brigatinib | $421,870 | 4.83 | 7.33 | $118,440 | Extendedly dominated through crizotinib and lorlatinib |
Lorlatinib | $571,160 | 6.21 | 8.21 | $113,311 | $113,311 |
ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; vs. = versus.
Table 20: Cost and QALY Breakdown by Health State From CADTH Reanalysis — Deterministic Results
Treatments | Progression-free | Non–CNS progressed | CNS progressed | Death | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | |
Lorlatinib | $514,090 | 3.48 | $39,738 | 2.74 | $0 | 0.00 | $17,331 | — | $571,160 | 6.21 |
Crizotinib | $108,172 | 1.00 | $49,135 | 0.44 | $74,528 | 1.95 | $18,661 | — | $250,497 | 3.38 |
Alectinib | $263,609 | 1.98 | $64,703 | 0.85 | $74,644 | 1.99 | $17,943 | — | $420,899 | 4.82 |
Brigatinib | $270,292 | 2.02 | $59,552 | 0.86 | $74,083 | 1.95 | $17,943 | — | $421,870 | 4.83 |
CNS = central nervous system; QALY = quality-adjusted life-year.
Table 21: Cost and QALY Breakdown by Health State From CADTH Reanalysis — Probabilistic Results
Treatments | Progression-free | Non–CNS progressed | CNS progressed | Death | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | Costs | QALYs | |
Lorlatinib | $476,049 | 3.44 | $71,855 | 2.39 | $16,236 | 0.30 | $17,072 | — | $581,212 | 6.13 |
Crizotinib | $106,690 | 1.00 | $51,357 | 0.45 | $76,042 | 2.14 | $18,510 | — | $252,599 | 3.59 |
Alectinib | $251,376 | 1.98 | $68,250 | 0.85 | $84,694 | 2.22 | $17,589 | — | $421,908 | 5.04 |
Brigatinib | $257,412 | 2.03 | $65,430 | 0.86 | $82,059 | 2.16 | $17,589 | — | $422,491 | 5.05 |
CNS = central nervous system; QALY = quality-adjusted life-year.
CADTH Scenario Analysis
CADTH performed the following scenario analyses:
OS benefit for lorlatinib relative to alectinib, brigatinib: CADTH assumed equivalence of OS for lorlatinib, alectinib and brigatinib by equating the OS for alectinib and brigatinib to that modelled for lorlatinib.
Alternate parametric models for OS extrapolation: CADTH performed scenario analyses using alternate parametric models to extrapolate OS for lorlatinib and crizotinib beyond trial duration. CADTH tested the impact of applying exponential, gamma and log-logistic models as the OS curves predicted by these models were believed to be clinically plausible.
Treatment waning: CADTH tested the impact of applying treatment waning to the extrapolated OS outcomes for alectinib, brigatinib and lorlatinib by assuming that the OS benefit for lorlatinib, alectinib and brigatinib is equal to that for crizotinib from year 5 onwards.
Assuming ToT equal to PFS: CADTH tested the impact of treatment discontinuation assumption by setting the ToT curves for alectinib and brigatinib to be equal to their respective PFS curves. This assumption was not applied to patients receiving crizotinib as the median ToT for these patients was lesser than the median PFS, which aligns with clinical expectations as patients on crizotinib could stop treatment before progression due to the high toxicity associated with the treatment. CADTH did not test this assumption for lorlatinib as clinical experts indicated that treatment with lorlatinib could continue beyond progression due to data from the CROWN trial suggesting improved response among patients with brain metastases.
CNS-progression resource use estimates: CADTH tested the impact of assuming that 100% of CNS-progressed patients incurred costs associated with management of CNS progression. To test this, the proportion of CNS-progressed patients receiving WBRT, stereotactic radiotherapy and surgical rejection was scaled to sum to a 100%. This was implemented by increasing the proportion of patients receiving WBRT to 40%. Estimates were not revised for SRT and surgical resection as these are not accessible in all Canadian provinces based on inputs from clinical experts consulted by CADTH.
RDI for lorlatinib: CADTH tested the impact of the RDI for lorlatinib using estimates provided by clinical experts. CADTH also tested the impact of applying a RDI of 100% (assuming no dose interruptions) for all treatments.
Utility values: CADTH tested the impact of incorporating utility values from the CROWN trial stratified by health state, treatment status, and treatment arm.
Comparator: CADTH tested the impact of removing crizotinib as a relevant standard of care for ALK+ NSCLC in the Canadian setting.
Table 22: Results From CADTH Scenario Analyses
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER vs. reference ($ per QALY) | Sequential ICER |
|---|---|---|---|---|---|
CADTH Base Case | Crizotinib | $252,599 | 3.59 | Reference | — |
Alectinib | $421,908 | 5.04 | $117,021 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $422,491 | 5.05 | $116,289 | $116,289 | |
Lorlatinib | $581,212 | 6.13 | $129,478 | $147,368 | |
CADTH Scenario Analysis 1 OS benefit for lorlatinib compared to alectinib and brigatinib | Crizotinib | $252,383 | 3.59 | Reference | — |
Alectinib | $424,250 | 5.39 | $95,650 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $424,931 | 5.4 | $95,168 | $95,168 | |
Lorlatinib | $583,209 | 6.13 | $129,976 | $216,169 | |
CADTH Scenario Analysis 2A Exponential model used to predict OS for lorlatinib and crizotinib | Crizotinib | $252,037 | 3.61 | Reference | — |
Alectinib | $422,544 | 5.09 | $114,790 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $423,232 | 5.11 | $114,042 | $114,042 | |
Lorlatinib | $584,925 | 6.16 | $130,119 | $152,948 | |
CADTH Scenario Analysis 2B Gamma model used to predict OS for lorlatinib and crizotinib | Crizotinib | $251,437 | 3.55 | Reference | — |
Alectinib | $419,168 | 5.03 | $113,287 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $420,155 | 5.04 | $112,964 | $112,964 | |
Lorlatinib | $586,294 | 6.16 | $128,143 | $148,392 | |
CADTH Scenario Analysis 2C Log-logistic model used to predict OS for lorlatinib and crizotinib | Crizotinib | $265,105 | 4.68 | Reference | — |
Alectinib | $441,402 | 6.53 | $95,552 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $442,561 | 6.54 | $95,464 | $95,464 | |
Lorlatinib | $603,765 | 7.46 | $122,146 | $176,428 | |
CADTH Scenario Analysis 3 Treatment waning | Crizotinib | $252,919 | 3.55 | Reference | — |
Alectinib | $406,104 | 4.17 | $246,191 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $406,471 | 4.18 | $242,324 | $242,324 | |
Lorlatinib | $547,232 | 4.63 | $273,537 | $318,255 | |
CADTH Scenario Analysis 4 ToT for alectinib and brigatinib relative to PFS | Crizotinib | $251,293 | 3.56 | Reference | — |
Alectinib | $380,454 | 4.97 | $91,700 | $91,700 | |
Brigatinib | $385,718 | 4.98 | $94,431 | Extendedly dominated through crizotinib and lorlatinib | |
Lorlatinib | $582,520 | 6.18 | $126,323 | $166,508 | |
CADTH Scenario Analysis 5 CNS resource use | Crizotinib | $253,830 | 3.61 | Reference | — |
Alectinib | $421,219 | 5.03 | $117,092 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $421,710 | 5.05 | $116,244 | $116,244 | |
Lorlatinib | $579,766 | 6.08 | $131,567 | $152,986 | |
CADTH Scenario Analysis 6A RDI for lorlatinib (85%) | Crizotinib | $250,609 | 3.53 | Reference | — |
Alectinib | $418,283 | 4.97 | $116,620 | Extendedly dominated by crizotinib and lorlatinib | |
Brigatinib | $419,211 | 4.98 | $116,686 | Extendedly dominated by crizotinib and lorlatinib | |
Lorlatinib | $528,308 | 6.12 | $107,492 | $107,492 | |
CADTH Scenario Analysis 6B RDI = 100% for all treatments | Crizotinib | $255,433 | 3.55 | Reference | — |
Alectinib | $473,218 | 4.99 | $151,032 | Extendedly dominated by crizotinib and lorlatinib | |
Brigatinib | $474,195 | 4.98 | $153,118 | Dominated by alectinib | |
Lorlatinib | $607,203 | 6.18 | $133,613 | $133,613 | |
CADTH Scenario Analysis 7 Utility values stratified by health state, treatment status, and treatment arm. | Crizotinib | $252,246 | 3.55 | Reference | — |
Alectinib | $420,674 | 5.08 | $110,592 | Extendedly dominated through crizotinib and brigatinib | |
Brigatinib | $421,509 | 5.09 | $110,157 | $110,157 | |
Lorlatinib | $581,276 | 6.1 | $128,977 | $157,481 | |
CADTH Scenario Analysis 8 Removing crizotinib as a relevant comparator. | Alectinib | $421,908 | 5.04 | Reference | — |
Brigatinib | $422,491 | 5.05 | $41,233 | $41,233 | |
Lorlatinib | $581,212 | 6.13 | $145,994 | $147,368 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 23: Summary of Key Take-Aways
Key Take-aways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor assessed the budget impact of the introduction of lorlatinib for adult patients with ALK-positive locally advanced or metastatic non–small cell lung cancer (NSCLC) from the drug program perspective in the Canadian setting (excluding Quebec), over a 3-year time horizon.20 Drug acquisition costs, dispensing fees, and subsequent treatment costs were included.20 The sponsor used an epidemiological approach to estimate the number of newly diagnosed advanced stage NSCLC patients per year who would be eligible for treatment with lorlatinib, which required assessing the published literature to derive estimates for the prevalence and incidence of lung cancer in Canada, estimating the proportion of patients with lung cancer by type (small cell versus NSCLC), deriving the patient breakdown by stage at diagnosis (I & II, III, and IV), estimating the proportion of NSCLC patients developing metastatic disease and the proportion of early stage patients who would develop a metastatic recurrence, and estimating the prevalence of attrition factors for NSCLC.20 Finally, the proportion of patients with an ALK-positive mutation was applied to derive the number of newly diagnosed metastatic patients eligible for treatment with lorlatinib.20
In the reference scenario, the sponsor assumed that patients could only receive alectinib and crizotinib in year 1, followed by the introduction of brigatinib in years 2 and 3. In the new drug scenario, lorlatinib was assumed to displace alectinib and brigatinib over the 3-year time horizon, totally displacing crizotinib, while capturing ||||% of the market share by the end of year 3.20
Key inputs to the budget impact analysis (BIA) are documented in Table 24.
The sponsor’s BIA also included the following key assumptions:
Crizotinib is a relevant treatment option and reimbursed in the first-line setting.20
Lorlatinib is expected to take most of the market share over the first 3 years.20
Table 24: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Prevalence of lung cancer | 0.16% |
Proportion of lung cancer that is non–small cell lung cancer | 88% |
Annual change (decrease) in lung cancer incidence rate | −1.70% |
Annual change (decrease) in lung cancer death rate | −1.80% |
NSCLC Stage I | 20% |
NSCLC Stage II | 8% |
NSCLC Stage III | 20% |
NSCLC Stage IV | 49% |
NSCLC Stage Unknown | 2% |
Metastasis by 5 years (NSCLC Stage I) | 39% |
Metastasis by 5 years (NSCLC Stage II) | 39% |
Metastasis by 5 years (NSCLC Stage III) | 80% |
Metastasis by 5 years (NSCLC Stage IV) | 100% |
Metastasis by 5 years (NSCLC Stage Unknown) | 100% |
Metastatic non–small cell lung cancer with ALK-positive | 3.8% |
Reasons for attrition (Trial) | 5% |
Reasons for attrition (Refuse) | 5% |
Reasons for attrition (Advanced) | 10% |
Reasons for attrition (Adv. Effects) | 7% |
Number of patients eligible for drug under review | 317 / 315 / 313 |
Market uptake (3 years) | |
Uptake (reference scenario) Alectinib Brigatinib Crizotinib | |||||||||||||||||||||||||||||| |||||||||||||||||||| |||||||||||||||||||| |
Uptake (new drug scenario) Lorlatinib Alectinib Brigatinib Crizotinib | |||||||||||||||||||||||||||||| |||||||||||||||||||| |||||||||||||||||||| |||||||||||||||||||| |
Cost of treatment (per patient) | |
Cost of treatment per day Lorlatinib Alectinib Brigatinib Crizotinib | $337.33 $337.28 $336.96 $260.00 |
NSCLC = non–small cell lung cancer.
Source: Sponsor’s submitted budget impact analysis.20
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s base-case analysis suggest that the introduction of lorlatinib in patients with NSCLC would result in cost savings of $223,425 in year 1, $11,695,462 in year 2, $24,555,011 in year 3, for a total incremental budget saving of $36,473,898 over the 3-year time horizon.20
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Median time on treatment may underestimate drug costs associated with lorlatinib, alectinib, and brigatinib: In the submitted pharmacoeconomic analysis, the sponsor adjusted total drug acquisition costs for lorlatinib, alectinib, and brigatinib based on the median ToT in the CROWN trial (approximately 17 months or 521 days for lorlatinib) and based on published literature (888 days for alectinib11 and 758 days for brigatinib4). The clinical experts consulted by CADTH indicated that the sponsor’s estimated treatment duration may have underestimated treatment costs since the median ToT for lorlatinib was expected to be longer for all treatments. To align with CADTH’s pharmacoeconomic base case, which revised the median ToT for all treatments, the median ToT for lorlatinib, alectinib and brigatinib was revised in CADTH’s BIA base case (i.e., 36 months or 1,095 days for lorlatinib and 26 months or 791 days for alectinib and brigatinib, respectively).
CADTH addressed this limitation by changing the median ToT with lorlatinib to 36 months (i.e., 1,095 days) and the median ToT to 26 months (i.e., 791 days). In a scenario analysis, CADTH examined the impact of the median ToT for each treatment based on the sponsor’s base-case estimates.
The anticipated market share for lorlatinib in the new drug scenario is likely overestimated: The sponsor anticipated that lorlatinib would capture ||||%, ||||% and ||||% of the market share distribution, respectively, over Years 1, 2, and 3. The clinical experts consulted by CADTH indicated that lorlatinib’s place in therapy could be extended to later lines of therapy and therefore, the experts felt that the sponsor’s anticipated market share uptake for lorlatinib were likely overestimated for the first-line treatment only as per its indication. The experts noted that it remains uncertain whether lorlatinib will be used in later lines of therapy.
CADTH addressed this limitation by revising the market shares for lorlatinib in the new drug scenario to 10%, 20% and 30%, respectively, over the 3-year time horizon to reflect its anticipated uptake in the first-line setting.
The estimated eligible population size is uncertain due to the uncertainty in several epidemiological inputs: The sponsor undertook an epidemiological approach to estimate the size of the population eligible for treatment with lorlatinib. As part of this approach, the sponsor assumed that the incidence of lung cancer would decrease by 1.7% per year, over the 3-year time horizon. The clinical experts consulted by CADTH indicated that this was unlikely as the incidence was expected to remain constant over time. Additionally, the sponsor assumed that the proportion of patients eligible for coverage across Canada (except Quebec) was approximately 81% based on a weighted average. However, CADTH’s clinical experts indicated that the majority (90%) of patients would likely be eligible for treatment.
CADTH addressed this limitation by revising the proportion of patients eligible for coverage to 90% and revising the estimated annual change in incidence to 1% to reflect that the incidence would remain unchanged. In a scenario analysis, CADTH explored the impact of all (100%) patients eligible for treatment coverage.
The dose intensities of all treatments did not align with the expected doses administered in Canadian clinical practice: The sponsor applied relative dose intensities for lorlatinib, brigatinib, crizotinib, and alectinib based on the CROWN trial, which underestimated drug costs, as each treatment was assigned less than a full dose intensity. For instance, the clinical experts consulted by CADTH indicated that the loading dose for brigatinib would be administered at a full dose of 100%, alectinib would be administered an RDI of 80 to 85%, and the dose intensity for lorlatinib was expected to be the same as for alectinib.
CADTH addressed this limitation by changing the dose intensities to 85% for lorlatinib in week 1 and onwards, 85% for alectinib, and 100% for the brigatinib loading dose.
The market share distribution in the reference scenario did not reflect clinical expectations: In the submitted BIA, the sponsor assumed that crizotinib was a relevant and available treatment option in the first-line setting and assumed that patients would continue to receive crizotinib in year 1. The clinical experts consulted by CADTH indicated that crizotinib is not the appropriate standard-of-care treatment, as alectinib and brigatinib have demonstrated superiority over crizotinib and are the current standard-of-care treatments for the first-line setting in Canadian clinical practice. As such, no market shares are expected to be assigned to crizotinib in the reference scenario. The experts further indicated that while brigatinib would have no market share in year 1, its market share would increase to 30% in year 2 and 40% in year 3, with alectinib capturing the remaining market share.
CADTH addressed this limitation by revising the market shares in the reference scenario to 0% for crizotinib across all 3 years, 0% for brigatinib in year 1, and 30% for brigatinib in years 2 and 3.
CADTH Reanalyses of the Budget Impact Analysis
A table noting the changes made to the sponsor’s BIA as part of the CADTH reanalysis is available in Table 25.
Table 25: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Treatment duration (i.e., median time on treatment) | Lorlatinib = 521 days Alectinib = 888 days Brigatinib = 758 days | Lorlatinib = 1,095 days Alectinib = 791 days Brigatinib = 791 days |
2. Market share new drug scenario | Lorlatinib: |||||||||||||||||||| Alectinib: |||||||||||||||||||| Brigatinib: |||||||||||||||||||| Crizotinib: |||||||||||||||||||| | Lorlatinib: 10% / 20% / 30% Alectinib: 90% / 45% / 40% Brigatinib: 0% / 35% / 30% Crizotinib: 0% / 0% / 0% |
3. Population size | Annual change in lung cancer incidence rate = –1.70% Proportion eligible to receive treatment = 81% | Annual change in incidence rate = 1% (constant) Proportion eligible to receive treatment = 90% |
4. Relative dose intensity | Alectinib = 95.6% | Alectinib = 85% |
5. Market share reference scenario | Alectinib: |||||||||||||||||||| Brigatinib: |||||||||||||||||||| Crizotinib: |||||||||||||||||||| | Alectinib: 100% / 70% / 60% Brigatinib: 0% / 30% / 40% Crizotinib: 0% / 0% / 0% |
CADTH base case | Reanalyses 1 + 2 + 3 + 4 + 5 | |
Applying these changes resulted in an increase in the budget impact under the drug plan perspective to $459,404 in year 1, $1,407,996 in year 2, $6,246,895 in year 3, for a total budget impact of $8,114,296 over 3 years. The results of the CADTH stepwise reanalyses are presented in summary format in Table 26, and a more details breakdown of the CADTH base case is presented in Table 27.
Table 26: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | −$36,473,898 |
CADTH reanalysis 1 | $14,939,122 |
CADTH reanalysis 2 | −$8,932,290 |
CADTH reanalysis 3 | −$43,303,273 |
CADTH reanalysis 4 | −$31,583,420 |
CADTH reanalysis 5 | −$36,317,056 |
CADTH base case | $8,114,296 |
CADTH also conducted additional scenario analyses to address the remaining uncertainty regarding the potential size of the eligible population:
Applied a median ToT for alectinib, and brigatinib based on their respective PFS curves (median ToT becomes 1.69 years or 617 days for alectinib and brigatinib) calculate their respective drug costs.
Explored the impact of increasing the proportion of patients eligible for treatment to 100%.
Assumed alternate RDI values for lorlatinib (85%), alectinib (85%), brigatinib loading dose (85%) and brigatinib maintenance dose (85%), based on the feedback from CADTH’s clinical experts.
Assumed alternate RDI values; given the limitations associated with the composite RDI input, an RDI of 100% was assumed for all treatments.
Applied a 42% price reduction on the submitted price of lorlatinib to reflect the point at which the ICER was cost-effective within the $50,00 per QALY threshold.
Table 27: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $84,026,927 | $39,094,104 | $76,415,653 | $93,643,412 | $209,153,168 |
New drug | — | $38,870,679 | $64,720,190 | $69,088,401 | $172,679,270 | |
Budget impact | — | −$223,425 | −$11,695,46 | −$24,555,011 | −$36,473,898 | |
CADTH base case | Reference | $76,218,314 | $41,112,408 | $83,147,970 | $91,838,536 | $216,098,914 |
New drug | — | $41,571,813 | $84,555,966 | $98,085,431 | $224,213,210 | |
Budget impact | — | $459,404 | $1,407,996 | $6,246,895 | $8,114,286 | |
CADTH scenario analysis 1 | Reference | $76,218,314 | $41,112,408 | $70,420,019 | $71,953,946 | $183,486,373 |
New drug | — | $41,571,813 | $73,100,810 | $81,483,476 | $196,156,098 | |
Budget impact | — | $459,404 | $2,680,792 | $9,529,530 | $12,669,725 | |
CADTH scenario analysis 2 | Reference | $84,687,015 | $45,680,454 | $92,386,633 | $102,042 | $240,109,904 |
New drug | — | $46,190,903 | $93,951,073 | $108,983,812 | $249,125,788 | |
Budget impact | — | $510,449 | $1,564,441 | $6,940,994 | $9,015,884 | |
CADTH scenario analysis 3 | Reference | $76,218,314 | $41,112,408 | $83,147,970 | $91,838,536 | $216,098,914 |
New drug | — | $41,113,057 | $83,160,512 | $95,255,683 | $219,529,252 | |
Budget impact | — | $649 | $12,543 | $3,417,147 | $3,430,339 | |
CADTH scenario analysis 4 | Reference | $105,431,898 | $48,354,774 | $97,706,702 | $107,807,577 | $253,869,053 |
New drug | — | $48,355,537 | $97,706,685 | $111,842,076 | $257,904,297 | |
Budget impact | — | $763 | -$17 | $4,034,499 | $4,035,244 | |
CADTH scenario analysis 5 | Reference | $76,218,314 | $41,112,408 | $83,147,970 | $91,838,536 | $216,098,914 |
New drug | — | $39,655,180 | $78,725,907 | $86,263,043 | $204,644,130 | |
Budget impact | — | −$1,457,229 | −$4,422,062 | −$5,575,493 | −$11,454,784 |
Stakeholder Input
Patient Group Input
CanCertainty
Authors of the submission: Robert Bick, Co-Lead, CanCertainty, and Kevin Moore, Epidemiologist
About CanCertainty
The CanCertainty Coalition is the united voice of more than 30 Canadian patient groups, cancer health charities, and caregiver organizations from across the country, joining together with oncologists and cancer care professionals to significantly improve the affordability and accessibility of cancer treatment.
For more information about the CanCertainty Coalition, please visit: https://www.cancertaintyforall.ca/
Information Gathering
Lorlatinib is indicated for patients with non-small cell lung cancer (NSCLC) whose tumours have mutations of anaplastic lymphoma kinase (ALK). As an orally administered oncology drug, lorlatinib is not automatically funded by certain provincial governments. In Ontario and the Atlantic provinces, only individuals over the age of 65 are automatically covered for oral oncology medication. For the small number of patients under 65 living in these provinces, their diagnosis could lead to severe economic hardships. However, if lorlatinib is fully funded by all provinces, these patients will instead be able to focus on their treatment and spending time with their family and friends.
Our data collection efforts aimed to estimate the number of patients who are at risk of severe financial burden as a result of their diagnosis. To do this, we calculated the number of ALK-positive NSCLC cases in Canada each year among the under 65 population who do not have private or automatic public prescription drug coverage. As lorlatinib is indicated as a monotherapy for first-line treatment, it was sufficient to calculate the ALK-positive NSCLC rate in Canada. Calculating remission rates from first and second-line treatment was not required. Lorlatinib was originally trialled as a third-line treatment for patients who developed resistance to crizotinib and one of several second-line treatments. After positive trial results, lorlatinib is now indicated as a monotherapy for first-line treatment.
ALK mutations are rare. We estimate that about 420 Canadians are diagnosed with ALK-positive NSCLC each year. Of these 420 cases, 105 will be under the age of 65. Depending on where these individuals live, their oral oncology medication may not be covered by their provincial government. For the 32 patients under 65 living in British Columbia, Alberta, Saskatchewan, and Manitoba, oral oncology medication is automatically covered. Residents of Ontario and the Atlantic provinces under the age of 65 are not automatically covered under public plans. Their route to treatment access is not simple. By our estimations, 6 of these Ontario cancer patients will not have private health insurance. Before they can receive their medication these patients will have to navigate a complicated process of funding applications, approval delays, locating a pharmacy, and waiting for their medication in the mail. They will incur out of pocket costs and sizeable portion of their income will go towards their medication. This is a small number of patients to be impacted by such a restrictive policy.
Lung cancer incidence data was sourced from the Canadian Cancer Society (Statistics Canada) (Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto, ON: Canadian Cancer Society; 2020. Available at: cancer.ca/Canadian-Cancer-Statistics-2020-EN ) in collaboration with the provincial and territorial cancer registries. In their 2020 special report on lung cancer, the Canadian Cancer Society provided lung cancer data for all of Canada (excluding Quebec) broken down into age groups (refer to Figure 2 in the report). We applied the age-specific lung cancer incidence rates to the 2016 population demographics (Statistics Canada. (2020) Annual Demographic Estimates: Canada, Provinces and Territories [Data Visualisation Tool]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501) of each province to arrive at the number of new lung cancer cases each year by age and province.
The ALK mutation has only been identified in patients with NSCLC, specifically patients with the NSCLC subtype adenocarcinoma (Koivunen, J. P., Mermel, C., Zejnullahu, K., Murphy, C., Lifshits, E., Holmes, A. J., et al (2008). EML4-ALK Fusion Gene and Efficacy of an ALK Kinase Inhibitor in Lung Cancer. Clinical Cancer Research, 14(13), 4275–4283. doi:10.1158/1078-0432.ccr-08-0168 ). In the same 2020 special report, the Canadian Cancer Society provided the percent distribution of lung cancer cases by specific histological type. We used lung cancer incidence data along with histological distributions to estimate the number of adenocarcinoma cases each year by age and province. The ALK mutation is present in approximately 3% of adenocarcinoma cases (Dearden, S., Stevens, J., Wu, Y.-L., & Blowers, D. (2013). Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap). Annals of Oncology, 24(9), 2371–2376. doi:10.1093/annonc/mdt205). With these percentages, we estimated the number of yearly lung cancer cases with the ALK mutation by age and province. In other words, this is the estimated number of Canadian residents who will become eligible for lorlatinib each year.
We measured “potential financial toxicity” using data on lack of private drug coverage. The Canadian Life and Health Insurance Association (Sutherland, Greg, and Thy Dinh. Understanding the Gap: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. Published in Canada | All rights reserved | Agreement No. 40063028 | *Incorporated as AERIC Inc.) provides data on “extended health coverage.” For each province, we extracted the percentage of individuals under the age of 65 without private drug coverage AND without automatic public drug coverage. These province specific percentages were applied to the ALK-positive NSCLC case rates to arrive at the final estimation: the number of yearly ALK-positive NSCLC cases among the under 65 population without private or automatic public prescription drug coverage.
Assuming Lorlatinib is ultimately funded by the provinces and territories, the following chart details the number of patients in each province/territory that would face financial barriers in accessing this treatment.
Table 1: Number of Patients Who Would Face Financial Barriers Accessing Treatment
Province | Populationi | Cases of ALK-positive NSCLCii | Without private drug coverageiii | |||
|---|---|---|---|---|---|---|
Over 65 | Under 65 | Over 65 | Under 65 | Over 65 | Under 65 | |
Totaliv | 5,133,226 | 24,170, | 236 | 80 | 0 | 7.0 |
BC | 986,936 | 4,160,776 | 45 | 15 | 0 | 0 |
AB | 610,974 | 3,810,902 | 28 | 11 | 0 | 0 |
SK | 191,020 | 987,661 | 9 | 3 | 0 | 0 |
MB | 221,666 | 1,157,597 | 10 | 3 | 0 | 0 |
ON | 2,594,358 | 12,139,656 | 120 | 40 | 0 | 6.1 |
NB | 171,262 | 610,214 | 8 | 2 | 0 | 0.5 |
NS | 208,825 | 770,526 | 10 | 3 | 0 | 0.3 |
PE | 31,957 | 127,668 | 1 | 0 | 0 | 0.1 |
NL | 116,228 | 405,875 | 5 | 2 | 0 | 0.1 |
(i) From Stats Canada for the year 2016 to align with incidence calculations.
(ii) Age-specific incidence rates were sourced for all age groups (10-year increments).
(iii) Province specific private drug coverage rates provided by The Canadian Life and Health Insurance Association.
(iv) Excluding Quebec (who do not report cancer cases in the same manner) and the territories (for whom we do not have health insurance data).
Limitations
We calculated these estimates to highlight an issue, not to be absolutely precise.
Just because someone younger than 65 does not have private insurance does not mean that they are without financial support for their oral oncology medication. In each province, multiple programs exist to support individuals with high drug costs. Based on our experience as a patient advocacy group, we made the assumption that individuals with private health insurance incur less cost when prescribed oral oncology drugs.
The ALT mutation rates were not sourced from a Canadian population. Differing demographics across the provinces may skew the actual case counts.
Disease Experience
The access problems are so difficult that in many hospitals and cancer centres across Canada, such as those in Ontario, a new type of social worker known as a drug access navigator has been established (and funded) to assist patients and clinicians navigate the byzantine treatment access structures. In Ontario, the organization that supports these navigators is known as the Oncology Drug Access Navigators of Ontario (ODANO). They describe the problem that their association works to resolve as follows: Drugs are an important part of cancer treatment, yet patients often have difficulty accessing coverage for the most effective medicines. The complexity of cancer drug coverage in Canada can overwhelm patients and families.
And
For example, although cancer drugs administered in hospitals and clinics are often offered free of charge to patients, half of all new cancer drugs are taken at home and, therefore, many are not covered by the public health system. Unfortunately, many of our patients do not have any private insurance. If a patient is fortunate enough to have private coverage, many drug plans require a 20% co-payment, which can quickly become a financial burden to patients on expensive medications.
British Columbia, Alberta, Saskatchewan, Manitoba, Quebec, NWT, Yukon, and Nunavut cover the reimbursement of oral cancer drugs for all in need. Ontario and the Atlantic provinces do not.
In Ontario and Atlantic provinces, with respect to access to approved cancer treatments, there is institutional discrimination against those who are young, uninsured and who have cancer requiring take-home cancer treatment. With 60% of all new cancer drugs being developed with oral formulations, this issue urgently needs to be resolved through policy change. Traditionally, cancer treatments were administered to patients by an IV in the hospital. Over the past 15 or so years, an increasing number of effective cancer treatments can be taken at home by pill or injection. Take-home cancer medications are now a fundamental part of today’s cancer treatments and should be recognized equally within our health care systems. Patients requiring an intravenous treatment can start that medication as soon as needed and don’t face any financial or administrative burdens provided the drug is included on the provincial formulary.
However, when take-home cancer medications are prescribed, patients in Ontario and the Atlantic provinces, who are under 65, and lack adequate private insurance, have to apply to a variety of funding assistance programs and ultimately pay a significant deductible or co-pay from their personal savings. In some cases, the cost to the patient might be as high as $23,400 annually, based upon Nova Scotia’s Family Pharmacare Program. To qualify for assistance programs, patients and their families have to submit significant amounts of personal and financial information and often face weeks of stressful delay in starting their cancer treatment until the paperwork and approvals are resolved.
Even for patients with private drug insurance, the reality is that many face significant co-pays, deductibles or annual/lifetime caps. For example, some private insurance plans have a cap of $2,000 for prescription drugs for the entire year. The majority of take-home cancer drugs cost more than $20,000 per year. Two-tiered pharmacare in Ontario and the Atlantic Provinces discriminates on the basis of age, income, geography, cancer type, and cancer treatment, and is financially ruining many lives.
A survey (Strategic Directions. Cancertainty & Strategic Directions IVR Report. 2017. Available at: https://d3n8a8pro7vhmx.cloudfront.net/cancertainty/pages/119/attachments/original/1490212245/CanCertaintySurvey_October2016.pdf) of over 1,600 Nova Scotians, commissioned by the CanCertainty Coalition, demonstrates that drug coverage for cancer patients is a serious and growing problem.
More than half (57 percent) of Nova Scotians expect the provincial health care system will pay for take-home cancer medications. In reality, patients will ultimately pay a significant deductible or co-pay from their personal funds.
Three out of five people in Nova Scotia (60 percent) said they would consider leaving the province if faced with having to pay for their cancer drugs. Only seven percent could afford monthly drug costs of over $200.
Experiences With Currently Available Treatments
Take-home cancer drugs (THCD) are medications used for the active treatment of cancer and are usually dispensed for administration in the home (e.g., oral chemotherapy). These drugs have become a standard treatment for many cancers and present opportunities for patients, providers, and the health system. However, flaws in our current drug coverage system result in some patients not being able to access these treatments.
The term “financial toxicity” describes the distress and hardship arising from the financial burden of cancer treatment. Even in counties with government funded universal healthcare, financial toxicity is an issue for cancer patients and their families. Financial toxicity comes in many forms: out of pocket costs, lost income, travel expenses etc. Patients may deal with their financial burden by delaying or foregoing care. They may take less medication than prescribed, utilize over-the-counter drugs in place of prescribed medications, decline procedures, and skip appointments in an attempt to defray costs. The combination of high drug prices, particularly of oral targeted anticancer drugs, and increased cost sharing has made patients more vulnerable to medication non-adherence. Patients who are younger, have lower income, and are uninsured appear to be at greater risk of medication non-adherence. Although government funded public healthcare exists in many very high development index countries, financial toxicity is still common among cancer patients and caregivers. The evidence suggests that those with a shorter time since diagnosis, not currently working, and with more severe cancers have higher rates of financial toxicity, including stress and strain (Longo, C.J., Fitch, M.I., Banfield, L. et al. Financial toxicity associated with a cancer diagnosis in publicly funded healthcare countries: a systematic review. Support Care Cancer 28, 4645–4665 (2020). https://doi.org/10.1007/s00520-020-05620-9).
An unfunded oral oncology drug is financially toxic compared to a funded IV oncology drug. The disease experience of cancer patients that require oral drugs is a dual track of disease and economic hardships. After receiving their diagnosis, deciding on a medication, and dealing with the side effects, patients in Ontario and the Atlantic provinces have to consider the financial side of their diagnosis. “Hearing that you have cancer is devastating. Finding out that you can’t pay for the medication that will make you well is catastrophic. It doesn’t have to be this way” (Lisa Machado, Ontario).
The financial side of cancer treatment is unnecessarily burdensome. “When you are going through any kind of sickness, whatever the severity of it, the last thing you should have to worry about is your medication cost” (Ed, Ontario). In addition to dealing with cancer, and not being well enough to work, patients in Ontario and the Atlantic provinces spend days on end, sometimes months, wading through paperwork in order to get approval for coverage of the oral chemotherapy that has kept them alive. Because some cancer treatments are not automatically funded, treatment is delayed for many patients. They wait weeks for government approval before dealing with insurance companies and pharmacies to receive their prescription. Patients often pay out of pocket for the first few weeks of their treatment, which they may not be reimbursed for. “My doctor prescribed a new drug that is not covered by the government therefore I had to find insurance to cover it which costs around $5000.00 a month, I came up with insurance to cover it but I had to pay the pharmacy first then the insurance would reimburse me some time later. My problem I do not have the $5000 to pay out let alone wait till they reimburse me” (Sharon, Ontario).
“Cancer isn’t fair, but access to treatment should be!” (Tammy, Ontario).
Experience With Drug Under Review
CanCertainty’s focus for this submission is on issues related the distress and hardship arising from the financial burdens associated with cancer treatment. If lorlatinib were to be reimbursed for patients with ALT-positive NSCLC who have progressed on previous treatments, there would be some patients under 65 in Ontario and Atlantic Canada that would face significant financial and administrative barriers in accessing treatment.
Anything Else?
Equitable Access
We recommend that pCODR, when assessing and reporting on implementation issues with respect to lorlatinib, examine the issues of equitable access across all Canadian jurisdictions.

Safety
With respect to implementation, we believe pCODR should also examine the issue of safety with respect to take-home cancer drugs. From 2006 to 2001, it is estimated that Ontario’s computerized provider entry system, the Oncology Patient Information System (OPIS) prevented 8,500 adverse drug events, 5,000 physician office visits, 750 hospitalizations, 57 deaths, and saved millions in annual healthcare costs. But, this system is only used for only IV Drugs (eHealth Ontario. Cancer Care Ontario and eHealth Ontario Partner to Deliver Safer Chemotherapy Treatment. Toronto, ON: 2011. Available at: https://ehealthontario.on.ca/en/news/view/cancer-care-ontario-ehealth-ontario-partner-to-deliver-safer-chemotherapy). As a result, patients requiring take-home cancer drugs (THCD) in Ontario are (currently) subject to significant safety challenges, and health systems are subject to significant annual costs (physician office visits, hospitalizations etc).
In Ontario, dispensing and delivery models for THCD have been documented to be inconsistent and pose serious safety concerns for patients and their families. Some patients receive their medication from hospital pharmacies, some from specialty pharmacies, and some from community pharmacies that lack specialization and training in the handling of toxic cancer medications. This contrasts with the robust guidelines and clear processes that have been developed for intravenous cancer drugs (IVCD) where delivery is more comprehensive, organized, safer and patient-centred than THCD. There are numerous known safety and quality deficits related to the current method of community dispensing of THCD including incorrect dosing and handling, limited monitoring and non-adherence (which can lead to under or overdosing), serious toxicity, morbidity, and mortality. Patient lives and well-being are at stake. Ontario urgently needs to reform its systems for THCD dispensing that embed high-quality, safe practices that recognize the unique aspects of these drugs.
In April 2017, Cancer Care Ontario organized the Oncology Pharmacy Task Force with the mandate to advise Cancer Care Ontario (CCO) on how to enhance the current system for THCD delivery to optimize quality and safety; and subsequently, to deliver a report to the Ministry of Health and Long-Term Care (MOHLTC) based on the findings of the Task Force. The Task Force included representatives from patient advocacy groups, pharmacy and pharmacist associations, regulatory and standard setting organizations, and subject matter experts. On March 25th, 2019 the report was completed and published on the CCO website, but there has been no follow up or action taken to the many important recommendations. The report Enhancing the Delivery of Take-Home Cancer Drugs in Ontario (March 2019) can be found at: https://www.cancercareontario.ca/sites/ccocancercare/files/guidelines/full/1_CCO_THCD_Report_25Apr2019.pdf
CanCertainty suggests that pCODR examine the issues of safety and dispensing when examining and reporting on issues concerning pan-Canadian implementation of lorlatinib.
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed exclusively using CanCertainty resources and personnel and contract personnel.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
Data was collected and analyzed using CanCertainty personnel/contract personnel.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 2: Conflict of Interest Declaration for CanCertainty
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AstraZeneca | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Robert Bick
Position: Co-Lead
Patient Group: CanCertainty
Date: July 8, 2021
Lung Cancer Canada
Author of the submission: Shem Singh
About Lung Cancer Canada
Lung Cancer Canada is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research and advocacy. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer. https://www.lungcancercanada.ca/
Lung Cancer Canada is registered with CADTH.
Information Gathering
Data collection: The information was collected through interviews, questionnaires, and environmental scanning of advanced stage ALK+ non-small cell lung cancer (NSCLC) patients and caregivers. The thoughts and experiences of the patients and caregivers have been included in the submission. The information was accessed June – July 2021.
Demographic data:
ALK+ NSCLC is found to be more common in non-smokers, younger adults, and those with Asian ethnicity. All of these patients are ALK positive and have experience with lorlatinib. Specific treatment experience can be found Place in Therapy section.
Table 3: Demographic Data of Patients and Caregivers
Gender | Age | Patient/Caregiver | Source | Location |
|---|---|---|---|---|
Female | 59 | Patient | Interview | Spain |
Male | N/A | Patient | Interview | USA |
Male | 62 | Caregiver | Environ Scan | Online |
Male | 69 | Caregiver | Environ Scan | Online |
Female | N/A | Caregiver | Questionnaire | USA |
Female | N/A | Patient | Questionnaire | USA |
Female | 55 | Patient | Interview | Canada |
Female | 44 | Patient | Interview | USA |
Male | N/A | Patient | Interview | Canada |
Female | N/A | Caregiver | Interview | Canada |
Female | 42 | Patient | Interview | Canada |
Female | 35 | Patient | Interview | United Kingdom |
Male | N/A | Caregiver | Interview | Canada |
Female | 51 | Patient | Interview | Canada |
Male | 73 | Patient | Questionnaire | Canada |
Male | 54 | Patient | Interview | Switzerland |
Male | 57 | Patient | Questionnaire | Philippines |
Disease Experience
12 years ago, life was busy and full for AM who was building her career when she noticed a lump in her neck. Further testing revealed a diagnosis of advanced lung cancer and her world was turned upside down. She thought that someone was playing a bad joke on her. But when her new reality set in and facing a terminal diagnosis, she decided that no matter what, she was going to fight to survive. It has been almost 12 years since her diagnosis and AM has defied the odds thanks to advancements in lung cancer treatments, specifically targeted treatments. She has been fortunate to have access to new treatments. In recent years, ALK positive lung cancer had a number of advancements that have allowed AM to live 12 years. However, there is still a large unmet need. In first line, although there are a number of treatments, there is still no cure. New treatments with increased efficacy are needed to increase the chance for a longer life. In second line and beyond, treatments are needed to overcome resistant mutations. Lorlatinib is a new treatment that has the potential to achieve both.
ALK-positive lung cancer patients make up 2 - 4% of NSCLC cases. NSCLC is the most common type of lung cancer occurring in 80 – 85% of cases. This type of lung cancer is typically found in younger patients and never smokers. In Canada, the current standard of care for this group of patients is targeted therapy. This form of treatment has helped improve patient outcomes and quality of life. Take SA’s spouse for example who was diagnosed with ALK + lung cancer in 2014. After 5 years on ceritinib and then 7 months on alectinib, he developed progression in the lung and brain and was placed on lorlatinib in 2019. Since starting treatment he has a lot more energy and says this is the best TKI he has been on. He walks every day, runs, plays the piano, skies in the winter, and is currently working part-time. He has a good quality of life. Lorlatinib had given him, AM, and many other patients the ability to live and live well. Lorlatinib has a profile that is effective in first line but also able to cover resistant mutations beyond.
Patients with the ALK mutation commonly present with brain metastases at diagnosis, this has been observed in about 30% of patients. This involvement can be quite debilitating, affecting the quality of life, resulting in a poorer prognosis and reducing already low survival rates even further. While there are options to treat the ALK mutation in the first line, there is also an unmet need to provide treatments that are not just effective in treating the tumours but also effective in treating brain involvement. This will reduce the need for other treatments that can result in cognitive side effects further impacting the patient’s quality of life.
Lorlatinib is an ALK tyrosine kinase inhibitor used for the treatment of patients with ALK-positive non-small cell lung cancer (NSCLC) and has been approved by the FDA and many other countries. This form of treatment has the potential to improve patient outcomes and have more survivors like AC and SA’s spouse. The input below will highlight the profound responses patients have on this treatment which hugely improved the quality of their lives – in both first line therapy and beyond. Patients are living longer and better on this treatment and we hope this form of treatment is considered by CADTH as a first-line treatment for this group of patients.
When JE received the devastating news of having lung cancer in 2017, she was told she didn’t have long to live, about 1 year to 18 months, so she and her spouse told their young kids that mummy was dying. Thankfully, the next day results from genetic testing showed she had the ALK mutation and would be able to receive targeted therapy. This changed everything for her and her family. She is currently on lorlatinib, doing well and thankful to have more time with her loved ones.
Experiences With Currently Available Treatments
The current standard of treatment for patients with ALK-positive NSCLC is targeted therapy and includes crizotinib, ceritinib or alectinib. Chemotherapy though a viable option has limited benefits and is well known for its toxic side effects. The patient experience with these forms of treatment have been well documented in previous submissions.
Targeted Therapy (ALK Inhibitors – Crizotinib, Ceritinib and Alectinib)
These treatments are known to improve patient outcomes by shrinking tumour sizes, have manageable side effects and prolong survival. They are given via the oral route which is easier on patients as it reduces the need for hospital visits and the burden on love ones. Patients are functional, independent and active on these forms of treatment allowing them to go back to work, travel, enjoy activities, and spend time with their loved ones, thus maintaining a high quality of life.
Crizotinib
Crizotinib was one of the first efficacious options for treating ALK+ NSCLC. Many of the patients interviewed in previous submissions have been active and highly functioning and said the side effects were manageable. These include nausea, vomiting, diarrhea, visual disturbances, edema, and fatigue. Some patients did find the side effects intolerable. One patient said crizotinib was challenging and affected her quality of life. She was so nauseous that getting out of bed was difficult. Another patient had to discontinue crizotinib due to liver dysfunction. JH was on crizotinib for 11 months and developed severe edema and was in a lot of pain. She also developed numbness in her hands and feet and visual disturbances. JE had severe leg edema on crizotinib and progressed after one year. She also had severe GI issues which severely affected her well-being and ability to socialize. It was difficult sometimes to go out. She also had visual flashes which made it difficult to drive at night.
For patients with brain metastasis at diagnosis, crizotinib may not provide adequate protection as data has shown that crizotinib may not effectively protect and treat CNS involvement and delay or prevent metastasis to the brain as it may not cross the blood-brain barrier. A treatment that would address any CNS involvement would be preferred as this reduces the need for other treatments such as radiation therapy that may result in cognitive deficits. This was the case for GI who was diagnosed in 2015 with metastasis to the brain. She was treated with crizotinib but did not help the brain tumour and she subsequently had to be treated with radiation therapy.
Ceritinib
JH was on ceritinib for 2 years, it worked very well, and she showed no evidence of disease for about a year, but the side effects were really challenging. The treatment came with a lot of gastrointestinal issues including cramps and diarrhea which severely affected her quality of life and ability to go out and socialize. This form of treatment is known to come with GI side effects which are well documented in previous submissions. SA’s spouse was on ceritinib for 5 years but stopped due to progression. Another patient unfortunately also progressed after 18months.
Alectinib
Alectinib is the current standard of care for ALK+ NSCLC patients. It is has been shown to be efficacious in treating these groups of patients and has shown better efficacy and lower toxicity compared to crizotinib. It has been found to also be effective in treating patients' brain metastases, reducing or eliminating the need for whole-brain radiation. It is generally very well tolerated with manageable side effects.
Within 6 weeks of treatment, alectinib reduced one patient’s tumour by 70%. She felt great and had few side effects. Another patient was on alectinib for a year and had a huge reduction in the size of her tumours and was termed stable. Within a month of being on the treatment, her symptoms had subsided. Some patients however were not able to tolerate this treatment.
Patients have come to expect efficacy with ALK inhibitors which makes it a preferred option for treating this group of patients.
Chemotherapy
Chemotherapy has been a long-standing and well documented standard of care for patients with lung cancer. Chemotherapy while a viable option has limited benefits and is known for having toxic side effects that leave patients unable to be fully functional or active and dependent on their loved ones. The side effects are well documented. Patients like JH who were treated with chemotherapy experienced side effects that interfered with daily activities. She was quite unwell and not capable of doing much physically and needed help taking care of the children. She couldn’t be involved in a lot of the activities she normally did. Some patient’s experienced minimal symptoms, while others reported side effects consistent with those in the survey of those on chemotherapy such as nausea, vomiting, and extreme fatigue.
Impact on Caregivers
The impact of lung cancer is felt not only by the patients but also by their loved ones. The diagnosis and treatment of lung cancer has a major impact on the life of the patient, and many caregivers spend time providing care and support to their loved ones. With many caregivers playing a central role in the management of care of their loved ones such as being involved in the daily activities, medical care, providing informational, financial, or emotional support, there is a need for more durable treatments that would help decrease the demand on the caregivers and allow patients return to life. This would allow many caregivers to continue working, not having to take time off work to care for their loved ones thus reducing physical and financial burdens on the family.
For patients on targeted therapy, this is an oral medication with manageable side effects. Patients can be independent, functional, and active. They can get out of bed, go for their appointments by themselves and even go back to work, and this allows caregivers to continue working and be productive. Unlike chemotherapy, an IV treatment, where caregivers are faced with the need to help take their loved ones to their appointments, as well as having to juggle other needs on the home and work front. Oral therapies can decrease the mental health burden of caregivers. Stress is a commonly reported by caregivers. To ensure the care of their loved ones, some caregivers lost time at work resulting in reduced productivity. Both mental health stress and financial stress is not captured in HTA economic considerations but have a considerable impact on economy overall.
Improved Outcomes
Recent advancements in the treatment of lung cancer have changed the paradigm for lung cancer patients. They have allowed patients to hope for a better tomorrow and even plan for the possible future. These outcomes which play a huge role in a patient’s treatment decision include the following:
Improving the symptoms of their lung cancer
Allowing patients have a good quality of life.
Having manageable side effects
Giving patients long-term remission and delaying progression
Allowing patients live longer while maintaining their functionality and independence so they are not a burden on their loved ones
Experience With Drug Under Review
Lung Cancer Canada was only able to gather the experience from one patient taking lorlatinib in the 1st line from Spain. While the requested submission is for the 1st line treatment of ALK + NSCLC, the thoughts, and experiences of patients treated with lorlatinib in other lines is also discussed. The table below summarizes the input received.
Table 4: Input Received From Patients and Caregivers
Gender | Age | Patient/ Caregiver | Year of Diagnosis | 1st line | Currently on Treatment | Duration on treatment | Source of Treatment |
|---|---|---|---|---|---|---|---|
F (SO) | 59 | Patient | 2018 | Yes | Yes | 4 years | Clinical Trial |
M (MK) | N/A | Patient | 2013 | No | Yes | 52 months | Clinical Trial |
M (LT) | 62 | Caregiver | 2016 | No | Yes | 3 years | N/A |
M(FL) | 69 | Caregiver | 2015 | No | Yes | 2 months | Insurance |
F (SA) | N/A | Caregiver | 2014 | No | Yes | 18 months | N/A |
F (AC) | N/A | Patient | 2018 | No | Yes | 3 months | Insurance |
F (JH) | 55 | Patient | 2013 | No | Yes | 3 years | Access Program |
F (GI) | 44 | Patient | 2015 | No | Yes | 3 years | Insurance |
M (GL) | N/A | Patient | 2019 | No | Yes | 3 months | Access Program |
F (HE) | N/A | Caregiver | 2019 | No | Yes | 3 months | Access Program |
M (AJ) | 54 | Patient | 2019 | No | Yes | 6 months | Public Coverage |
F (AM) | 42 | Patient | 2009 | No | Yes | 5 years | Access program |
F (RE) | 35 | Patient | 2020 | No | Yes | 3 months | Public Program |
M (TM) | N/A | Caregiver | 2017 | No | Yes | 1 year | Access Program |
F (JE) | 51 | Patient | 2017 | No | Yes | 1 year | Access Program |
M (TE) | 73 | Patient | 2013 | No | Yes | 6 weeks | Access program |
M (RP) | 57 | Patient | 2018 | No | Yes | 10 months | N/A |
Lorlatinib was effective in shrinking the tumours and maintaining stable disease. It also improved symptoms.
When SO was diagnosed in 2018 she was placed on lorlatinib. After two months of treatment the tumour had shrunk by 50%, by the 4th month the swollen lymph nodes had disappeared. She is still on treatment to date and doing well.
MK has been on lorlatinib for 52 months, his tumours have shrunk and he remains stable. A tumour in the neck was recently discovered, this is planned to be surgically removed. AC was diagnosed in 2018 and started lorlatinib in February 2021 after developing progression in her lymph nodes, liver and bones. Her last scan showed almost all cancer has resolved aside from a residual tumour in her hip. Prior to taking lorlatinib GI was deteriorating as fluid had built up around her heart and she was struggling to breathe and the fluid had to be drained. She thought she would not make it. She was lucky to get access to lorlatinib as it had just been approved by the FDA. 2-3 days after starting lorlatinib she started to feel better, her breathing improved, her health got better and by two weeks she was back to her normal self.
HE was terrified and scared when her spouse was deteriorating rapidly as a result of his lung cancer. He had lost a lot of weight, his speech was slurred, and was walking with difficulty. He was then placed on lorlatinib and is doing much better. He is yet to have a follow-up scan but feels much better, has gained back the weight and his speech and walking have improved. The improvements in her spouse’s health have allowed her to go back to work.
AJ was diagnosed in 2019 and initially placed on alectinib. In early 2020, he developed chest pain and difficulty breathing and was unable to sleep unless he sat upright. He went to the hospital and a CT scan found that he had developed pulmonary embolism, fluid in his lungs, and a bleeding tumour in his lungs. After treatment of his complications, he was placed on ceritinib but this treatment did not work and he was deteriorating rapidly and had progressed to the brain. He had one round of chemotherapy while waiting for genetic testing results which was also not successful in treating the cancer. He even developed hiccups and constipation which led to him developing a hernia. He was in really bad shape and had lost about 20 kg. He was subsequently placed on lorlatinib. He felt the results immediately and by the second day, his breathing had improved. Follow-up scans showed the tumours had shrunk and brain metastasis completely resolved. He is glad to be alive thanks to lorlatinib.
Lorlatinib works beyond first line. This JE’s 3rd treatment and says it’s the best so far at treating her cancer. Follow-up scans showed she has had a complete response to this treatment.
Lorlatinib is a durable form of treatment
Lorlatinib was and still is the 1st line treatment for SO who had been on the treatment for about 4 years. MK has been on lorlatinib longer than all of the 3 TKI’s and chemotherapy he has been treated with combined. He has been on lorlatinib for 52 months. AM has been on lorlatinib for 5 years, and JH and GI for over 3 years.
Lorlatinib is a durable treatment option
Worked on brain metastasis
MK developed brain metastasis while on ceritinib and was subsequently taken off the treatment. This was treated with radiation, then he was placed on alectinib and taken off after 3 months as it did not have much effect on the tumour. In 2017, he was placed on lorlatinib, which managed his brain metastases and he is still on this treatment, The dose was decreased to 75 mg due to memory issues and neuropathy. In September 2020 he progressed and the dose was increased back to 100mg and this has stopped the progression to date. Lorlatinib also stopped SA’s spouse's brain metastasis. Brain metastases is a significant concern for lung cancer patients and is a common development. Whole brain radiation is a viable treatment for brain metastases but it carries risk of permanent cognitive side effects including memory loss. Lorlatinib’s efficacy in the brain is highly significant and valuable to patient quality of life.
Has manageable size effects – Dose reduction was also effective
Most patients said the side effects of lorlatinib were manageable. However, a number of patients mentioned the dose was reduced due to side effects and the treatment was still effective on their cancer. Common side effects include fatigue, constipation, nausea/vomiting, diarrhea, numbness/tingling of arms/legs, swelling ankles/feet/hands, trouble sleeping, weight gain, high cholesterol levels, and memory issues.
SO developed high cholesterol levels which is treated with medication. In 2019, the treatment was suspended for two months due to high liver enzymes. Since then her dose was reduced from 100 mg to 75 mg. During the two months off treatment, she did not progress. She also has constipation (she eats plums to help with this) and neuropathy which she tries to combat with cold showers and walks on the beach.
MK developed memory issues, brain fog and neuropathy around his fingertips. This lead to the reduction of the treatment dose to 75 mg and he is still on that dose to date. Asides memory issues, says he has been alive for 52 months and is enjoying his life. For AC the side effects are manageable and does not cause fatigue.
JH developed some nerve discomfort but this disappeared after 2 months. She also developed some memory loss with treatment but says it is not worse than the deficits she experienced with her other treatments. About a year into treatment with lorlatinib, GI noticed some cognitive symptoms, this included memory loss, prone to anger and a personality change. This resulted in a reduction of her treatment of 100 mg to 75 mg and the cognitive symptoms resolved. Everything was back to normal apart from the occasional forgetfulness but for the most part the treatment was really tolerable.
AJ developed leg and calf edema and stiffness in his fingers and this has improved with time. Other side effects were manageable. He has had mild memory issues with this treatment.
When treated with lorlatinib, AM developed a number of side effects that were quite unexpected. She experienced vivid dreams, memory loss, insomnia and weight gain. The dreams did go away with time however the insomnia had to be managed with treatment and is still ongoing. She sometimes sleeps for just 2 hours a day. Other side effects she developed include high cholesterol levels and tachycardia. The cholesterol levels and insomnia are managed with medication.
Rebecca developed diarrhea and slurred speech with her treatment soon after taking lorlatinib but combats this by taking her pill at night before she goes to bed. She also had short-term memory issues which also improved by taking the drug at night.
Allow patients to maintain a good quality of life – Patients are able to maintain social interactions, work, have energy and be independent.
Since taking lorlatinib SO has led a totally normal life. She did stop working on the insistence of her medical team due to her stressful job. She continues to interact socially with friends and family, asides from the social isolation due to the pandemic.
On lorlatinib, SA’s spouse has plenty of energy and says it’s the best TKI he has taken. He walks every day, runs, plays the piano, plays golf, skies in winter and is working part-time. He has a good quality of life. AC continues to work full time, take care of the home and yard, spend time with family and friends, travel. She is able to make plans for the future and live a completely normal life since her diagnosis. GI was back to running about 3 miles a day and doing all the things she loved, she had more energy and her physical health felt really great. AM has been able to maintain a good quality of life with lorlatinib but recently developed shortness of breath which was investigated and a scan showed there is no progression. She feels more like she did before she had cancer and is currently stable.
RE feels much better on lorlatinib compared to alectinib which was her first treatment (she progressed after only 3 months). It gave her a lot of energy and was able to go back to the gym, play badminton and go rock climbing. She was unable to be involved in these activities while on alectinib as she was fatigued a lot of the time. She hopes to stay well and long enough to take care of her young daughter.
Other than increased cholesterol levels RP has manageable side effects that have allowed him to be fully functional working from home. For him, the arrival of lorlatinib was quite timely as he had progressed on alectinib and had to be treated for a collapsed lung and had to be admitted to the hospital for 34 days to drain fluid from his lungs.
Lorlatinib gave patients their life back – It allowed patients a feeling that they were returning to life.
MK was in really bad shape before taking lorlatinib. In his words, “I was basically about to die at that point.” He was bedridden, extremely fatigued in addition the previous treatment chemotherapy had made him very sick. Within 2 weeks of starting lorlatinib he rebounded and had more energy. Like many of the patients interviewed MK had been on crizotinib, ceritinib, alectinib, and even chemotherapy and says this is the best treatment he has ever been on. Lorlatinib gave him his life back.
The treatment has been fantastic for JH. She has way more energy and is able to carry out chores such as painting, gardening, and walking the dog.
In JE’s words, “I love it”. Unlike alectinib that left her feeling like a zombie, she feels like her old self on lorlatinib. She is able to socialize, participate in tasks and has more energy, her spouse is happy to see how much better she is on lorlatinib. Life is good at the moment and they hope the effects of the treatment are long-lasting.
Increased energy was a common reported outcome of taking lorlatinib. All patients interviewed reported increased feelings of hope and mental wellness as lorlatinib enabled living close to a new good normal.
Dosage
Lorlatinib which is given via the oral route was is preferred by patients. It is also a once-daily pill which is easy to swallow unlike some of the other ALK inhibitors that are given two or three times a day or multiple pills at a time.
Companion Diagnostic Test
ALK+ testing is currently a standard in many provinces across the country. Lorlatinib does not require additional companion diagnostics.
Anything Else?
There has been great progress in the treatment of lung cancer in the last decade with ALK positive NSCLC having a number of viable treatment options and patient expectations for treatments are very high.
Patients are able to stay functional, independent and physically active with manageable side effects, and the dosage modality makes it easier not just for the patients but also for their loved ones/caregivers. Lorlatinib is a targeted therapy that has shown durable responses and helps delay progression. It is effective on brain metastasis, thus allowing some patients to delay or avoid the side effects of whole brain radiation. It was evident that lorlatinib increased the hope and mental well being of all the patients and caregivers. The value of independence, increased mental wellbeing, time off work for caregivers and return to work for patients are uncaptured in economic evaluations but all impact the overall economy and need to be considered.
The current submission is for first line treatment. Both the FDA and Health Canada have just recently approved lorlatinib in the first line so it was difficult to find first line patients for this submission. However the experiences of this treatment in all lines of therapy have been well documented. The practice of using targeted therapies for those with actionable mutations is a well established, and well recognized best practice globally. Many other jurisdictions (eg NICE) have approved public reimbursement beyond first line. Lorlatinib is proven to be efficacious in all lines. We encourage CADTH to recommend reimbursement in first line but to also consider it for all other lines of treatment. It is a broad spectrum line-agnostic treatment that is fills the treatment gaps and aligns with patient values.
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 5: Conflict of Interest Declaration for Lung Cancer Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Pfizer | — | — | — | X |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Name: Christina Sit
Position: Director Programs and Stakeholder Relations
Patient Group: Lung Cancer Canada
Clinician Group Input
Lung Cancer Canada
Authors of the submission: Dr Geoffrey Liu; Dr Kevin Jao; Dr Paul Wheatley-Price; Dr Stephanie Snow; Dr Rosalyn Juergens; Dr Nicole Bouchard; Dr Callista Philips; Dr Zhaolin Xu; Dr Barb Melosky; Dr Sunil Yadev; Dr Catherine Labbe; Dr Donna Maziak; Dr David Dawe; Dr Dave Stewart; Dr Ron Burkes; Dr Quincy Chu; Dr Jeff Rothenstein; St Parneet Cheema; Dr Silvana Spadafora; Dr Randeep Sangha; Dr Mahmoud Abdelsalam.
About Lung Cancer Canada
Please describe the purpose of your organization. Include a link to your website (if applicable).
Lung Cancer Canada is a national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research and advocacy. Based in Toronto, Ontario, Lung Cancer Canada has a wide reach that includes both regional and pan-Canadian initiatives. Lung Cancer Canada is a member of the Global Lung Cancer Coalition and is the only organization in Canada focused exclusively on lung cancer.
Information Gathering
Please describe how you gathered the information included in the submission.
Information gathered for this submission was based on relevant published clinical data and expert evidence-based review amongst lung cancer medical oncologists across Canada.
Current treatments
Describe the current treatment paradigm for the disease
Focus on the Canadian context. Please include drug and non-drug treatments. Drugs without Health Canada approval for use in the management of the indication of interest may be relevant if they are routinely used in Canadian clinical practice. Are such treatments supported by clinical practice guidelines? Treatments available through special access programs are relevant. Do current treatments modify the underlying disease mechanism? Target symptoms?
Response: In Canada, locally advanced incurable or metastatic incurable ALK-rearranged non-small cell lung cancer (henceforth termed incurable ALK-positive NSCLC) is a unique subgroup of lung cancer patients that represent only 2-4% of all incurable lung cancers in Canada. These patients are very different than the typical lung cancer patient. There are two Canadian sources of data that describe the Canadian population with ALK-positive NSCLC:
A 2016 study of six Canadian cancer centres (Burnaby Hospital, BC Cancer Agency, The Ottawa Hospital, Lakeridge Health, Jewish General Hospital, and Princess Margaret Cancer Centre) reported a case series of 49 patients. Mean age was 53 (Standard deviation 12.5) years; 53% were female; 67% were never-smokers; 53% were white while 22% were of Asian descent (Kayaniyii et al, 2016). In this earlier study, in an era of limited ALK-tyrosine kinase inhibitor options, median overall survival (OS) was only 23.7 months (30.1 month follow-up time) from the time of diagnosis of incurable lung cancer.
In a recently updated single institution analysis at Princess Margaret (PM) Cancer Centre of 147 incurable ALK-positive NSCLC patients (Chotai et al, 2021), incurable ALK-positive patients were younger by about 8 years than the regular lung cancer patient (median age, 59.2 years), at an age where patients are typically still employed full-time and often still supporting dependents (children or elderly parents). The majority were never-smokers (76%). All ethnicities were affected (35% Caucasian, 47% Asian, 23%); 57% were female. Median OS had improved to 47 months in this more updated, recent cohort (Chotai et al). Patients are commonly sick at the time of presentation (23% presented with ECOG performance status 2 or higher (Chotai et al, 2021).
In the pre-tyrosine kinase inhibitor (TKI) era, patients had worse outcome than the typical lung cancer patient (Yang, 2012), but this dramatically changed with the introduction of multiple ALK TKIs. Today incurable ALK-positive NSCLC patients enjoy one of best overall survivals amongst lung cancer patients: the median OS from the date of diagnosis of the incurable locally advance or metastatic state is 78 months in a US real-world cohort (Pacheco, 2019) and 89 months in a French multicentre real-world cohort (Duruisseaux, 2017). Early access to ALK-TKIs to allow sequencing of these drugs has been one big difference between the US and French real-world cohorts and the aforementioned Canadian cohorts, to explain the poorer OS in the Canadian cohorts. Canadian patients and their physicians continue to be hampered with access to subsequent lines of ALK TKI therapy.
The distribution of metastatic burden is also different in incurable ALK-positive patients, when compared to other NSCLC subtypes. There is a high cumulative incidence of pleural-pericardial disease and brain metastases (Figure 2; Chotai et al, 2021). Both types of metastases have significant impact on patient well-being and can lead to additional non-drug therapies: for pleural-pericardial disease, talc pleurodesis, pericardial window procedures, and indwelling pleural catheters are often needed, when TKI/drug therapy is unable to control pleural-pericardial disease; whole brain or localized stereotactic radiation (and occasionally surgical resection) with all of its incumbent short and long term side effects, are necessary when TKI/drug therapy is unable to control CNS metastases or there is lack of access to such TKI agents.
Figure 2: Cumulative Incidence Plots of Various Metastatic Disease Sites in Canadian ALK-Positive NSCLC
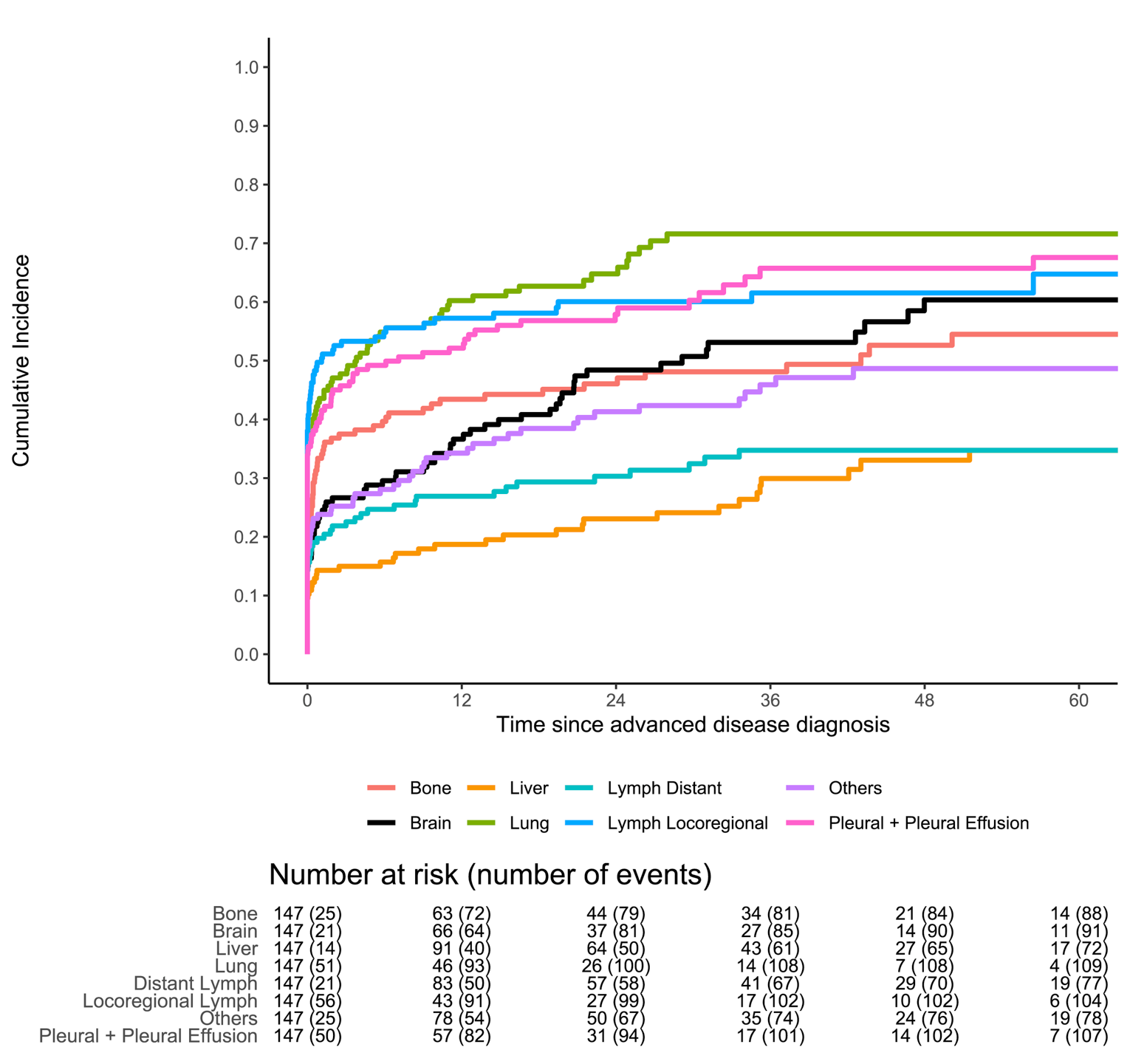
A major reason for a long median overall survival in these patients in the US and Europe has been the use of sequential TKI therapy, interspersed with chemotherapy and local palliative management. Figure 3 demonstrates this using Swimmer’s plots in our own Canadian PM data (Chotai et al, 2021). These swimmer’s plots demonstrate the benefit that sequencing ALK-TKI agents one after the other has on prolonging overall survival, using the five available TKI drugs in Canada are: crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib.
Figure 3: Swimmer’s Plots of 147 Canadian (PM) Incurable ALK-Rearranged NSCLC Patients, Anchored on The Date of Diagnosis of Incurable Disease
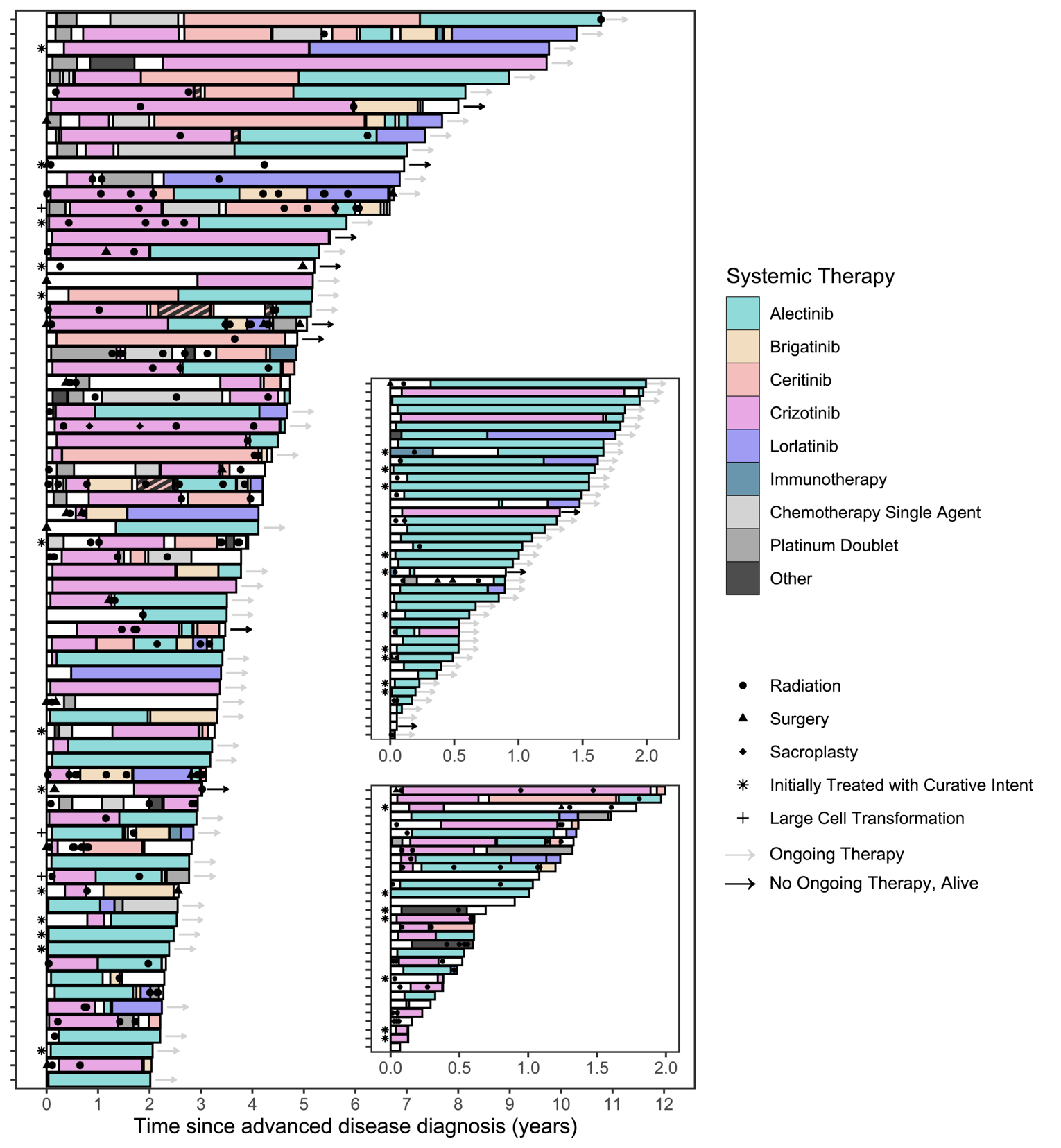
Of the two insets, the upper one includes all patients who has less than two years of follow-up are still alive. The bottom inset includes all patients who died less than two years after diagnosis of incurable disease. (Chotai Et Al, 2021)
Biologically, when resistance to one drug occurs, mechanisms of resistance in the ALK setting are varied, including secondary mutations in ALK and the development of oncogenic pathways that bypass ALK signaling. However, the use of molecular profiling at the time of development of resistance to an ALK-TKI is still in its infancy and not generally funded in the public system, nor is there consensus on the benefit of profiling new biopsy material at every timepoint of TKI failure. Instead, there has been a Canadian (and indeed international) pragmatic drug sequencing approach initially that first involved first-generation drugs (crizotinib, ceritinib), followed by second-generation drugs (alectinib, brigatinib), and then third-generation drugs (lorlatinib). More recently, first generation drugs are no longer used for newly diagnosed incurable ALK-positive NSCLC patients and more recently diagnosed patients have started with second generation ALK-targeting agents. When one drug stops working, another ALK-TKI is started. If a drug fails to work, rapid clinical deterioration is common-place when the disease is not under control; as such it only takes weeks to a few months to determine whether the next sequencing drug is indeed clinically benefiting the patient.
A common approach has also been to utilize the best first-line therapy available to patients at the time of diagnosis of incurable state. Up until earlier this year, this standard has been alectinib. With CADTH approval of brigatinib in the first-line setting, there are now two standards available. In this current situation in Canada, after first-line alectinib or brigatinib, no second or subsequent line of ALK-TKI has received a positive recommendation by CADTH.
The original old standard of crizotinib first-line has not been in use (unless forced to use it due to access problems) since the ALEX trial demonstrated superiority of PFS with alectinib over crizotinib in the first-line setting. This inferiority of crizotinib to newer ALK-TKI agents was further re-confirmed in the ALTA-1L (compared to brigatinib), eXalt-3 (compared to ensartinib), and CROWN (compared to lorlatinib) trials. Ceritinib fell out of favour because of its gastrointestinal symptomatic and (asymptomatic) hepatic laboratory adverse events; although ceritinib was later found to have improved tolerability and a better adverse event profile when administered with a low-fat meal and at a lower dose (450mg/day instead of 750mg/day), by then the ALEX trial results had been reported, and clinicians moved towards a second-generation standard (alectinib, and more recently, both alectinib and brigatinib). It should be noted that there are still pockets of patients who remain on crizotinib as first-line and/or ceritinib as first- or second-line TKI, given that some patients benefit from these earlier agents for years. However, crizotinib and ceritinib are not typically used in the first-line incurable ALK-positive setting any more in Canada.
Choice is an important matter in this unique treatment setting. When patients are on a targeted drug potentially for months to years, what would have been a Grade 1 toxicity could still impact our patients functionally long term. As our patients are typically full time employed and taking care of dependents (elderly parents or school-aged children), the ability to change drugs due to toxicities, is an important factor. Up until recently, the management of these patients has been typically similar to how internists treat hypertension, diabetes, asthma or other chronic conditions – one selects the agent that is most likely to have manageable toxicities and a high chance of efficacy, considering the comorbidities and lifestyle of the specific patient. After administration, efficacy and toxicity are evaluated. One then switches agents as needed to another agent, if efficacy or toxicity management is suboptimal and benefit-risk discussion with the patient has been performed. Figure 4 summarizes differences in toxicities of these ALK-TKI agents in a heat-map, showing that there are differences in toxicities across agents in the real-world Canadian setting. Figure 5 demonstrates that when patients are stable clinically, their health utility scores, which are summary values that are tied loosely to health-related quality of life, are stable and high; the scores in this figure are generated from the Canadian reference population in Canadian ALK-positive NSCLC patients.
Figure 4: Mean Health Utility Scores of Patients Over Time by Tyrosine Kinase Inhibitor Treatment While Clinically and Radiologically Stable on Their TKI Therapy
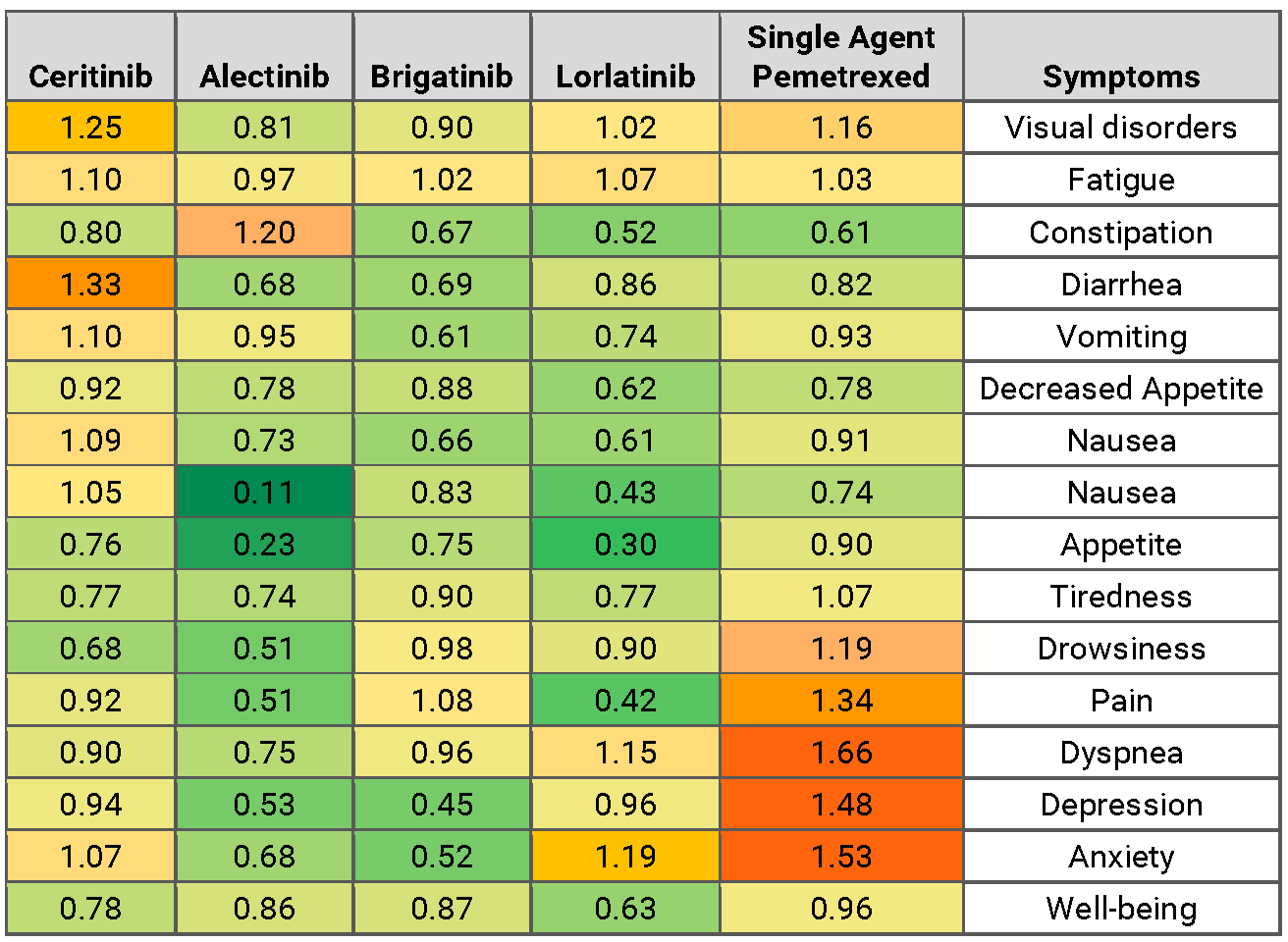
HUS values in each treatment group were modelled using locally estimated scatterplot smoothing. When fewer than 15% of the original number of patients were present, the line becomes dotted to reflect potential survivor bias. The first 6 weeks of treatment is marked with a box, “treatment initiation”, to represent the typical length of time required for patients to respond to therapy. Adapted From Tse BC Et Al, 2020 (Canadian PM Real-World Data).
Figure 5: Proportion of Patients With Clinically Relevant Toxicities Leading to Treatment Modifications With Different ALK-TKIs
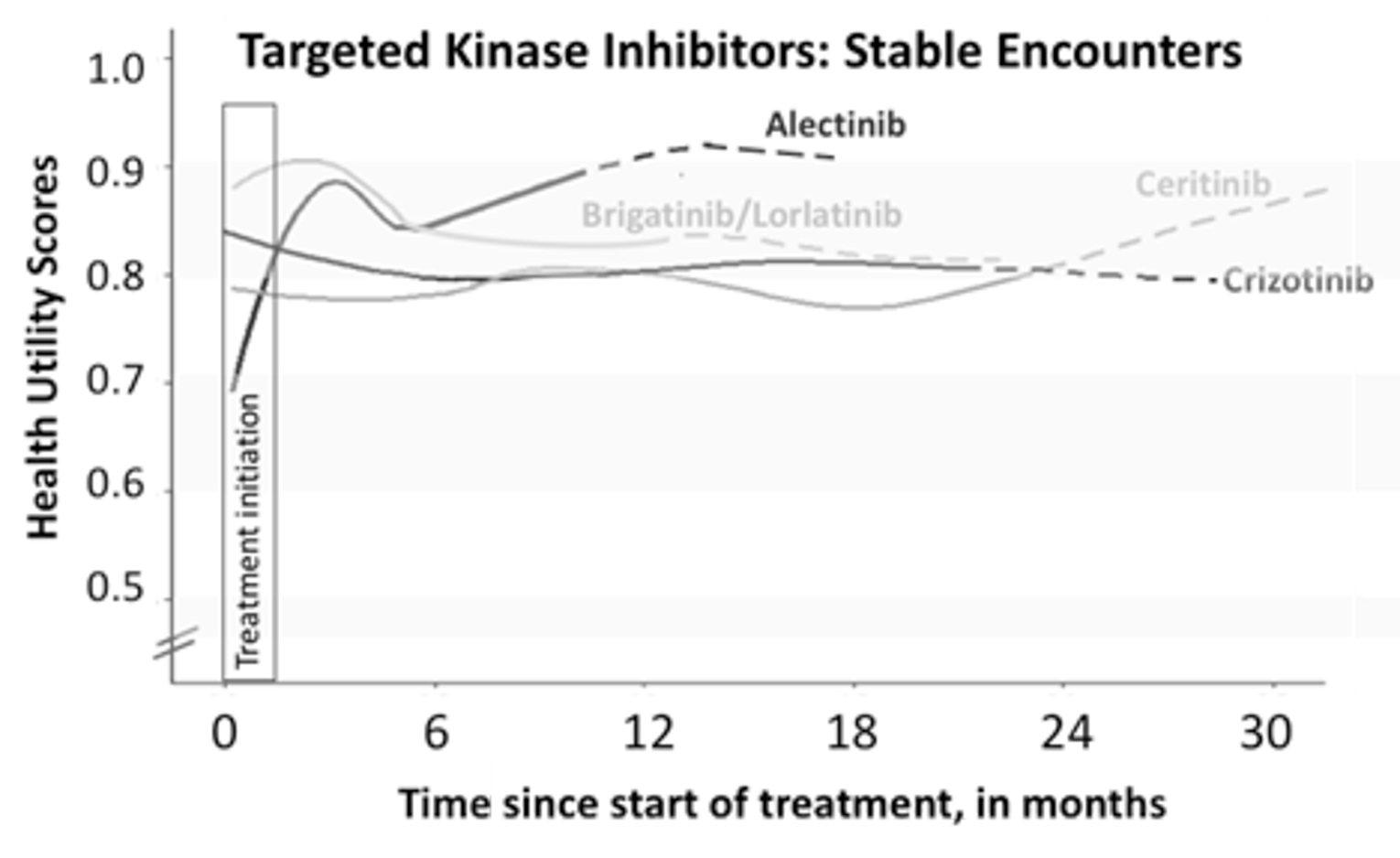
Standard errors of the proportions are presented.
Adapted from Schmid et al, 2021.
As each ALK TKI has a unique set of toxicities, the ability to change to another agent to minimize adverse events becomes important. Figure 6 shows the real-world Canadian (PM) data on treatment modifications across all the available TKIs. Being reported are the proportions of patients with toxicities leading to:
Any treatment modification, counting maximum one event per agent per patient
Temporary treatment interruptions, counting maximum one event per agent per patient
Dose reduction, counting maximum one event per agent per patient. In reviewing clinician notes, because of variability in availability to switch TKI agents (due to drug access issues), dose reduction occurred more frequently in some settings as opposed to switching drugs, even when the clinician/patient preferred the latter option.
Permanent discontinuations (note that data may underestimate discontinuations due to toxicity for the more recent agents, because the number average duration of treatment with these newer agents is shorter than for the older agents).
In summary, it is clear that there is a need for Canadian patients to access different ALK-TKIs for sequencing purposes both for efficacy and toxicity purposes, based on this real-world data.
When special access and compassionate programs close in the absence of public reimbursement, access to the later generation ALK-TKI agents, such as brigatinib and lorlatinib, outside of first-line use will be greatly diminished. Inequity will occur as some provinces may have special alternative funding mechanisms while others will not. The risk to this unique and small population of patients is that while US, Asian, and European patients will continue to have long overall survival times of 6.5-7.5 years (which may improve further with the availability of newer agents), Canadian patients will regress even further and have less than the current 3.9 years of median overall survival (from PM data). Note that even this 3.9 year median overall survival is due partly to the fact that PM has opened 23 trials for ALK+ patients (to increase early access to all ALK TKIs) and this median OS value is based on an era in which there was relative availability of ALK TKI through compassionate and special access programs. That generation of access through clinical trials and compassionate/special access programs is coming to an end; there is significant concern that Canadian patient overall survival may actually worsen as a result. While there is hope that the latest generation of ALK TKIs can benefit the newly diagnosed ALK patient, existing incurable ALK patients will be left with fewer options.
Figure 4 shows the relative severity of mean patient reported symptoms and toxicities, when compared to crizotinib. The mean values from the Likert scales of individual PRO-CTCAE (patient reported outcomes of the common terminology criteria for adverse events) and ESAS (Edmonton Systems Assessment Scales) items were first normalized to crizotinib values and presented in a heat map where the green spectrum means less-severe symptoms compared to crizotinib, while the orange-red spectrum means more severe symptoms, and yellow is neutral. Adapted from Tse BC et al, 2020 (Canadian real-world PM data).
Figure 6: Relative Severity of Mean Patient Reported Symptoms and Toxicities, When Compared to Crizotinib
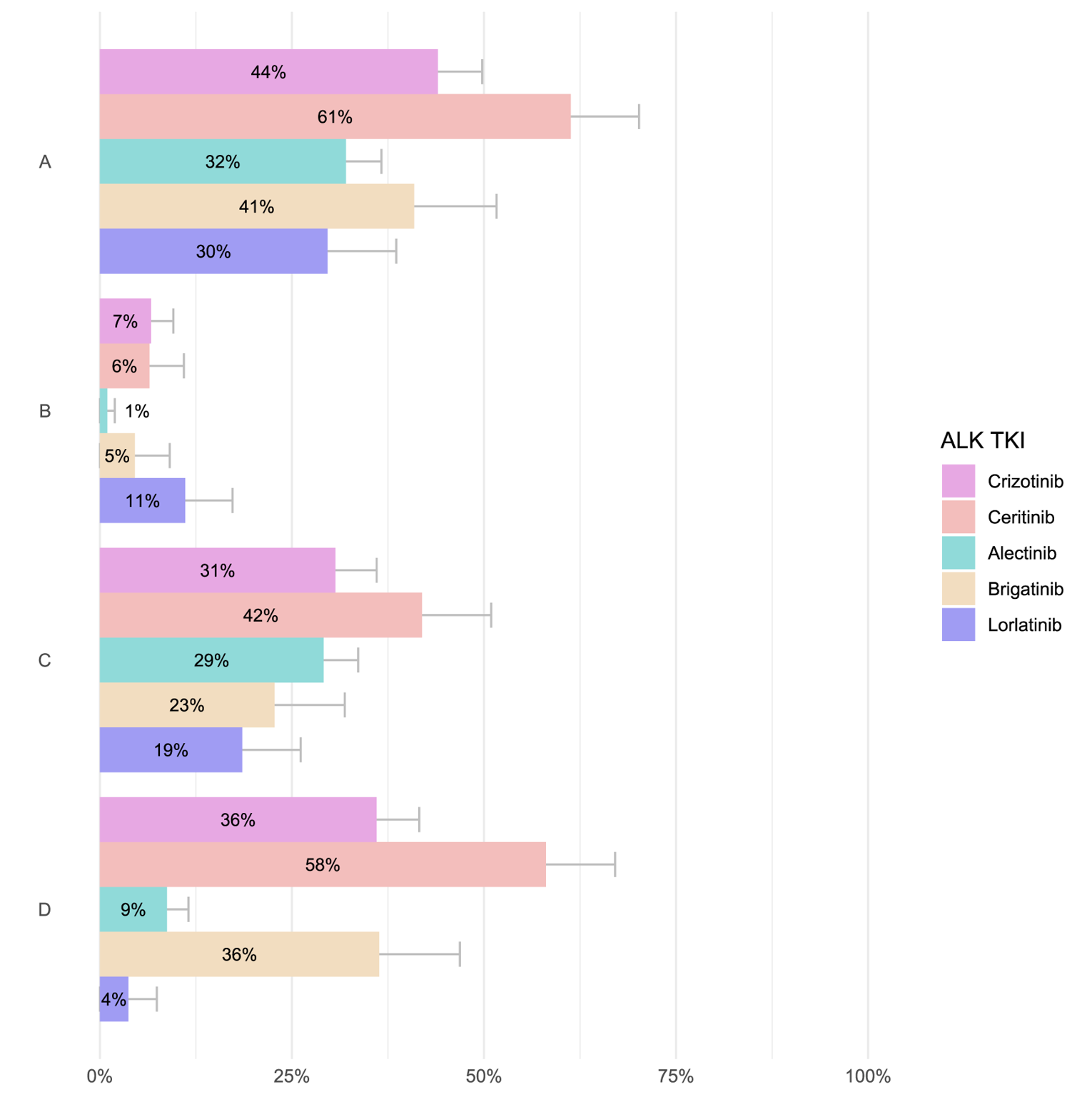
References in this section (alphabetical order)
Chotai S et al. (accepted for 2021 World Conference in Lung Cancer), Real-World Sequencing of ALK-TKIs in Advanced Stage ALK-positive NSCLC patients in Canada.
Duruisseaux M et al. Oncotarget. 2017; 8:21903-21917
Kayaniyil S et al. Curr Oncol. 2016 Dec;23(6):e589-e597
Pacheco JM, et al. J Thorac Oncol. 2019;14:691-700
Schmid et al. (accepted for 2021 World Conference in Lung Cancer), Real-world clinically-relevant toxicities of ALK TKIs in a cohort of patients with advanced/metastatic ALK+ NSCLC.
Tse BC et al. Curr Oncol. 2020 Dec; 27:e552-e559.
Yang P, et al. J Thorac Oncol. 2012;7:90-97
Treatment Goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Response: The important goals that an ideal treatment for incurable ALK-positive NSCLC patients would address are, in order of importance:
Prolong life
Delay disease progression
Maintain or improve health-related quality of life
Reduce severity of disease-related symptoms
Minimize adverse events specific to the patient
Reduce loss of cognition, memory, and other sequelae of CNS metastases and its local treatments
Maintain independence
Treatment Gaps (Unmet Needs)
Considering the treatment goals under the Treatment Goals section, please describe goals (needs) that are not being met by currently available treatments.
Examples: Not all patients respond to available treatments. Patients become refractory to current treatment options. No treatments are available to reverse the course of disease. No treatments are available to address key outcomes. Treatments are needed that are better tolerated. Treatment are needed to improve compliance. Formulations are needed to improve convenience.
Response: There are multiple areas of unmet need.
For the first unmet need, there is a need for more effective anti-cancer agents for first line ALK-TKIs. This falls in the category of “Not all patients respond or respond long enough to available therapies”. Currently, the agents with positive recommendations from CADTH are alectinib and brigatinib that are currently being used clinically in the first-line setting. Crizotinib and ceritinib are no longer being used in the first-line or any-line setting, as explained under the Current Treatments section.
Alectinib and brigatinib have median progression-free survivals of 34 months (investigator-assessed, ALEX trial) or 24 months (blinded independent review, ALTA-1L), and hazard ratios of 0.43-0.49 when compared to crizotinib. Any agent that improves on these median progression-free survivals and/or hazard ratios would satisfy this unmet need. This is especially true in the current Canadian situation where there are no CADTH-recommended ALK-TKIs after use of alectinib or brigatinib; in essence, a Canadian patient reliant on the public health care system has one shot at an ALK-TKI. In this case, the ALK-TKI with the best efficacy results amongst all of the ALK-TKIs would satisfy the need for improved efficacy outcomes. Lorlatinib satisfies these criteria by having a HR of 0.28 and a median PFS that has not been reached yet.
Please note that ALK-positive patients represent a unique subgroup of NSCLC patients. It would be inappropriate to compare outcomes in incurable ALK-positive NSCLC patients with outcomes of incurable non-ALK-positive NSCLC patients, and use this argument that ALK-positive patients already do better than other NSCLC patients and thus there is no unmet need for more efficacious agents. If that logic was appropriate, then one would argue that there would be no unmet need for any new agents in metastatic breast, colorectal, and prostate cancer, because each of these incurable cancers all have better survival outcomes than lung and pancreatic cancer.
For the second unmet need, there is a need for effective anti-cancer agents for second and subsequent line ALK-TKIs post-first line ALK-TKI. This falls in the category of “Patients become refractory to current treatment options.” The rationale for this is explained under the Current Treatments section and illustrated in the Canadian setting through real-world evidence shown in Figure 3 above. These data demonstrate the benefit of sequencing ALK-TKI drugs to maximize the chance for long term control (or prolonged survival) in incurable ALK-positive NSCLC patients. Lorlatinib is the ALK TKI with evidence of efficacy in the second and subsequent line treatment after failure of alectinib, brigatinib, ceritinib, and/or crizotinib, including patients who have failed multiple prior lines of ALK TKI agents.
For the third unmet need, there is a need for effective anti-cancer agents that improve on the targeting of existing brain metastases and/or protection of the brain from developing new metastases. This falls into the category of “Not all patients respond or respond in a specific metastatic disease site long enough to currently available therapies.” Current evidence and practice support the concept that systemic chemotherapy is not used to treat brain metastases in NSCLC because it is unreliable in its ability to control the brain metastases and often ineffective (Ernani and Stinchcombe, 2019). Local therapy consists of surgery in very selected cases, often when the space occupying aspect requires immediate attention. Steroids are only a temporizing measure, and is effective only in reducing the peri-lesional edema; it is not a long-term solution, and is also wrought with complications (hyperglycemia, psychotropic effects, muscle wasting, etc.). Whole brain radiotherapy had been the standard of care for several decades, but is fraught with significant long term toxicities. In the past, it was the general opinion that the long term cognitive and memory deficits were unlikely to be clinically relevant because NSCLC patients had such short lifespans after the diagnosis of brain metastases.
However, in the era of ALK-TKI agents and ALK-positive NSCLC where relatively longer term survival is expected, both acute and long term toxicities of brain metastases and its local therapies can be devastating, especially to younger, active, employed patients that are typical of this patient population. Even with stereotactic radiotherapy (sometimes performed multiple times due to new lesions or eventual progressing previously treated brain metastases), the physical and psychological toll on patients and their families is enormous. Empiric evidence shows an increase in symptoms in ALK-positive patients after the development of brain metastases (Guérin et al, 2015), and there is evidence that brain metastases lead to significant quality of life interference of patient reported outcomes in the community setting (Walker et al, 2016).
Ideally complete remission of these brain lesions would be desired. Both alectinib (ALEX) and brigatinib (ALTA-1L) have intracranial complete responses of 45% in all brain lesions, and 28-38% intracranial complete response rates amongst patients with measurable brain metastases. The 12-month intracranial failure rates are 7.8-9.4%. Improvements in these values in another anti-cancer agent would satisfy this third unmet need. In the CROWN trial, the intracranial response among patients with measurable brain metastases was 82% with 71% of patients achieving a compete response. Lorlatinib’s 12-month cumulative incidence of CNS progression was particularly impressive, at only 2.8%.
For the fourth unmet need, there is a need for choice in effective anti-cancer agents targeting ALK, where the toxicity profiles of new agents are different from that of the currently available ALK-TKI agents. This falls into the category of “Alternative treatments are needed that are better tolerated in individual patients that would allow proper individualization of therapy”. The addition of lorlatinib to the funded list of ALK-TKIs would provide choice for clinicians and patients and allow individualization of care. This is especially important when dealing with potential adverse events and drug toxicities that would need to be addressed over years of exposure to these ALK-TKI agents. Agents that satisfy this unmet need should also have low permanent discontinuation rates, as demonstrated for lorlatinib in the CROWN trial. Greater detail of rationale is also provided under the Current Treatments section and accompanying real world evidence is shown in Figure 4.
The fifth unmet need falls into the “formulations to improve convenience” category. For some patients, the convenience of a single pill a day is important (loraltinib, brigatinib) as opposed to up to 8 pills in divided doses (twice daily), as in the case of alectinib.
References in this section:
Ernani and Stinchcombe. J Oncol Practice. 2019; 15:563-570.
Guérin et al. J Med Econ. 2015; 18:312-322.
Walker et al. Clin Lung Cancer. 2018; 19:139-147.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response: For newly diagnosed incurable ALK-positive NSCLC patients, the greatest need are agents with improved efficacy, different adverse event profiles, and low permanent discontinuation rates. Lorlatinib meets this unmet need. (see CROWN trial data). For patients already on an ALK-inhibitor, the greatest need is a choice of additional efficacious and tolerable TKI agents for subsequent lines of ALK therapy. Lorlatinib meets this unmet need. (see Figure 3 above). For patients intolerant to their current ALK-inhibitor, the greatest need is for an alternative agent, equally efficacious (or better) but with a different toxicity profile. Lorlatinib meets this unmet need. (see CROWN data, compared to ALEX and ALTA-1L toxicity data).
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: Lorlatinib directly inhibits the oncogenic driver, ALK, and influences the underlying carcinogenic mechanism. It has been studied as both first-line and second and subsequent lines of treatment, but always as monotherapy. Its use in the proposed setting is not expected to cause a shift in the current treatment paradigm, but as an additional ALK-TKI agent, with accumulating evidence that lorlatinib is the best in class among the currently available ALK-TKI agents. Lorlatinib is considered to have superior pre-clinical coverage of resistant secondary mutations in the ALk gene, and thus could theoretically prevent the development of such resistant secondary mutations as a means of developing drug resistance in the clinical setting. This may partially explain the apparent superior results (better HR for PFS when compared to crizotinib in CROWN, when compared with alectinib in the ALEX trial and brigatinib in the ALTA-1L trial, in cross-trial comparisons). Lorlatinib was specifically designed to penetrate the blood-brain barrier better than other ALK-TKIs. Intracranial data from the CROWN trial supports the striking efficacy of lorlatinib in the intracranial setting (see under the Treatment Gaps (Unmet Need) section for details). Lorlatinib will substitute for existing ALK TKIs in the first line setting in patients who are newly diagnosed with incurable ALK-positive NSCLC. Lorlatinib will serve as a later/last TKI line of therapy in incurable ALK-positive NSCLC patients who have progressed on other first- or second-generation ALK-TKIs.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: Chemotherapy is no longer considered appropriate as a first-line alternative treatment of incurable ALK-positive NSCLC after the PROFILE (crizotinib) and ASCEND (ceritinib) trials. Crizotinib is no longer considered appropriate as a first-line alternative treatment of incurable ALK-positive NSCLC after ALEX, ALTA-1L, eXalt3, and CROWM trials. Ceritinib is generally not used by clinicians due to its high gastrointestinal adverse events and hepatotoxicities. The choices for first-line incurable ALK-positive NSCLC are now alectinib (ALEX trial), brigatinib (ALTA-1L trial), and lorlatinib (CROWN trial). Among these agents, lorlatinib has the strongest indication of being “best in class” by having a PFS HR of 0.28 versus crizotinib overall, an intracranial response amongst measureable disease of 71%, a 12-month cumulative incidence rate of brain metastasis of 2.8%, while maintaining a HR for extracranial control of 0.3 versus crizotinib; each of these results are generally better than what was shown in ALEX and ALTA-1L. However, alternatives must be considered because each agent has a unique toxicity profile, and with the likely use of these agents over years, individualization of patient management and inclusion of patient preference in the decision-making process should be considered. However, in patients who do not have strong preferences for alternative drugs, and who do not have particular relative or absolute contraindications to any of these drugs, use of lorlatinib in the first-line would be a preferred choice in many clinical settings. It would also be appropriate for patients to commence on brigatinib or alectinib in the first line, and for reasons explained in detail earlier, be able to access lorlatinib in the second line (if they did not receive lorlatinib in the first line)
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: After lorlatinib is given (in first or subsequent lines of therapy), there are no further ALK-TKIs that are CADTH-recommended. The next line of therapy will be chemotherapy: platinum-based doublet (if the patient can tolerate) or single agent monotherapy (in patients who may not tolerate platinum agents). Use of immunotherapy either concurrently with chemotherapy or as a subsequent line of therapy can be considered, but efficacy of immunotherapy in ALK+ NSCLC may be low. This sequence is not a significant departure from current standards in the post-alectinib or post-brigatinib setting, where the same subsequent treatment options are available after first-line alectinib or first-line brigatinib. Each specific ALK-TKI is generally used only in one line of therapy. Although there is anecdotal evidence of benefit in specific situations when re-using an ALK-TKI at a later line of therapy (Shaw et al, 2018), it is generally not done outside of a research setting.
References in this section:
Shaw et al, N Engl J Med 2016;374:54-61
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: Patients with ALK rearrangements/fusions are most likely to respond to treatment with lorlatinib. There is not one subgroup of incurable ALK-positive patients (by clinico-demographic or molecular-pathologic features) that would be expected to be more or less suited for treatment with lorlatinib. This same group of patients are most in need of an intervention (See under the Treatment Gaps (Unmet Needs) section for details). All patients, regardless of disease characteristics would best be treated with lorlatinib; however, patients who have baseline brain metastases could benefit the most, given the superb intracranial control observed in CROWN with lorlatinib. Lorlatinib may also be a better choice than brigatinib in patients who have significant dyspnea or who are hypoxic at baseline, given the risks of EOPE (early onset pulmonary events) in patients treated with brigatinib.
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify). Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: ALK-positive NSCLC is not challenging to diagnose in routine clinical practice. Canadian standards for routine lung biomarker testing have included ALK fusions for more than a half-decade now. The testing is either through immunohistochemical staining, through fluorescent in-site hybridization, or through molecular profiling, typically as part of a biomarker panel. A Canada-wide cross-validation pathology study of ALK testing helped establish standards across Canada (Cutz et al, 2014). Misdiagnosis is rare. Incurable patients who are pre-symptomatic should be considered for treatment with lorlatinib or other CADTH-approved ALK-TKIs, given that there is reason to believe that TKI-untreated incurable ALK-positive NSCLC patients have worse outcomes than patients without these ALK-rearrangerments/fusions in the pre-TKI era (Yang et al, 2012).
References in this section
Cutz et al. J Thorac Oncol. 2014;9:1255-63
Yang P, et al. J Thorac Oncol. 2012;7:90-97
Which patients would be least suitable for treatment with the drug under review?
Response: Patients without ALK-rearrangements/fusions would be least suitable for use of lorlatinib.
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
If so, how would these patients be identified?
Response: Yes it is possible to identify patients who are most likely to exhibit a response to treatment with lorlatinib. These patients have ALK rearrangements/fusions, as identified through the processes under the Place in Therapy section.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response:
Best overall response rate based on radiological assessment (Complete Response, Partial Response, Stable Disease, Progressive Disease)
Clinical symptom control and health-related quality of life, including time to clinical deterioration
Progression-free survival
Intra-cranial progression-free survival
Extra-cranial progression-free survival
Overall survival
The aforementioned outcomes are aligned with the outcomes typically used in clinical trials and reported in the CROWN trial.
Early assessment of therapeutic response or benefit involves outcomes (1) and (2); longer-term evidence of efficacy is demonstrated through outcomes (3) through (5).
Although the ultimate assessment of treatment benefit is with outcome (6), with generally long median OS in the ALK-positive population and the use of sequential therapies to achieve long term prolongation of OS, it is also the outcome most confounded by subsequent therapies when trying to assign attribution of benefit of different therapies. The more pragmatic assessments will involve progression-free survivals (i.e. outcomes (3) through (5)).
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth). Attainment of major motor milestones. Ability to perform activities of daily living. Improvement in symptoms. Stabilization (no deterioration) of symptoms.
Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: Radiological response by RECIST criteria (CR, PR) including disease stabilization (SD) is strongly correlated with clinical response and clinical benefit in the majority of incurable ALK-positive NSCLC patients receiving ALK-TKIs; this is the case with lorlatinib (quality of health data) (Mazieres et al, 2021). Canadian (PM) data demonstrated that disease progression was associated with a mean HUS decrease of 0.065 (95%CI 0.113-0.065), whilst stable disease on any ALK TKI was associated with excellent health utility scores: the mean overall HUS for each TKI ranged from 0.805 to 0.858, and longitudinally from 0.774 to 0.912, with higher values associated with alectinib, brigatinib, and lorlatinib. Further, HUS was inversely correlated to multiple PRO-CTCAE and ESAS symptoms and toxicities: rho values ranged from --0.094 to -0.557 (P<0.001 for each correlation; all data from Tse et al, 2020).
Given that disease controls rates are extremely high (CR+PR+SD = 89% in CROWN lorlatinib arm), and radiological disease control has been shown by Tse et al (2020) to be associated with clinical benefit, all of the following list would constitute clinically meaningful response would include all of the following:
Improvement in health utility and global quality-of-life indices
Lack of deterioration over time in health related quality-of-life scores
Reduction in the frequency, severity, and functional dysfunction associated with disease symptoms
Ability to perform activities of daily living
Stabilization (no deterioration) of symptoms
Lorlatinib and other ALK TKIs are sometimes termed “Lazarus drugs” because they are useful even in individuals who have really poor performance status, patient who are hospitalized, and sometimes near death. Thus, the majority of responding patients have symptomatic improvement, if they were symptomatic at baseline. Figure 7 shows Canadian data indicating similar overall survival by ECOG performance status at the time of diagnosis; these data support the concept that even the very sick incurable ALK-positive NSCLC patients at baseline benefit from ALK TKIs.
Figure 7: Kaplan-Meier Curves and Median Overall Survival in Patients With Good ECOG Performance Status Compared To Patients With Poor Performance Status
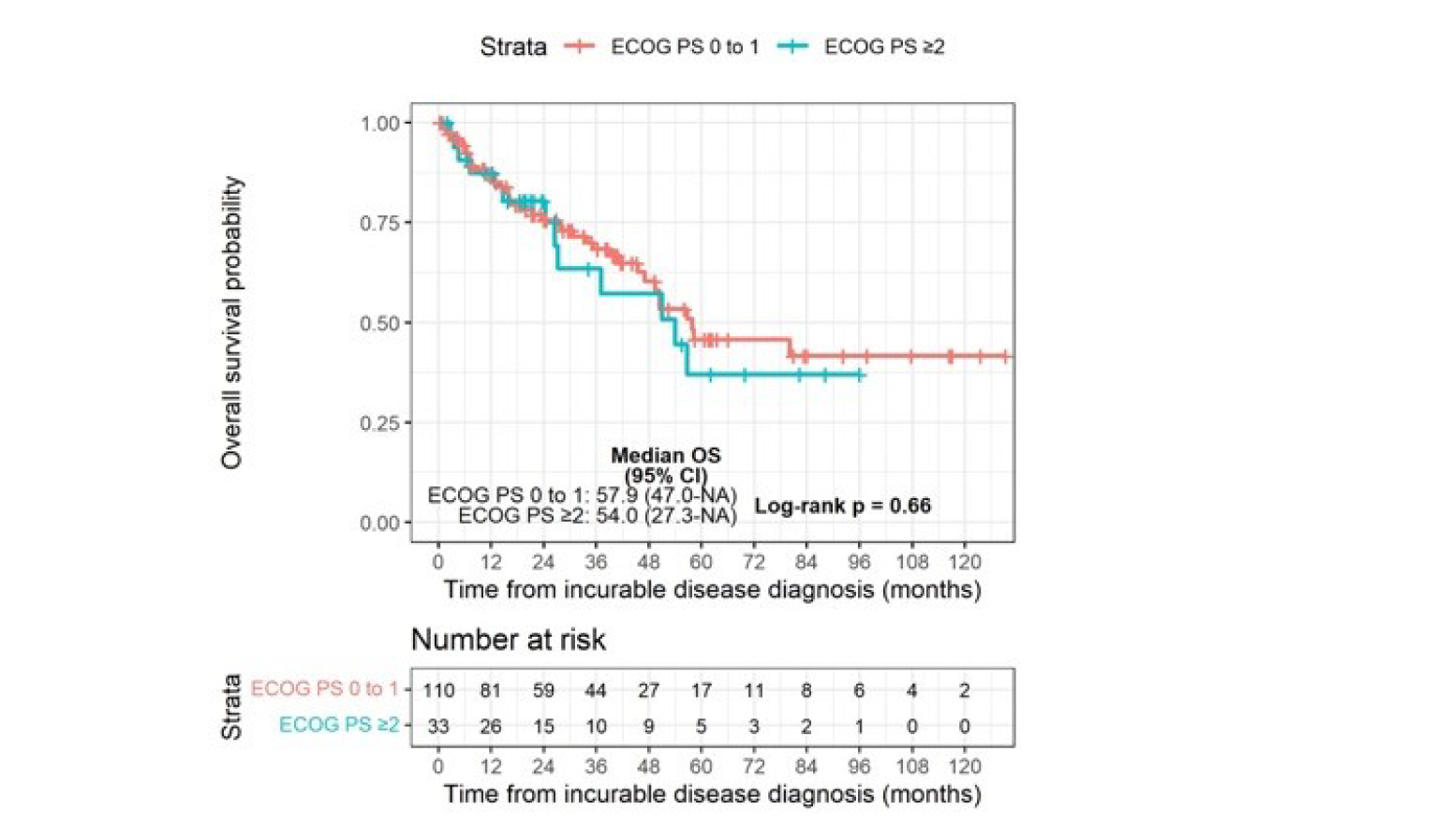
Canadian (PM) data showing Kaplan-Meier curves and median overall survival in patients with good ECOG performance status of 0-1 at diagnosis (red line) compared to patients with poor performance status of ≥ 2 at diagnosis (blue line). Graph includes all 143 patients with known baseline ECOG performance status, irrespective of treatment given. (Schmid et al, manuscript in preparation).
References in this section
Mazieres J et al. 2020 World Conference on Lung Cancer; January 28-31, 2021; Virtual. Abstract MA11.08.
Schmid S, Cheng S, Chotai S, Zhan L, Hueniken K, Balaratnam K, Khan K, Patel D, Grant B, Raptis r, Xu W, Shepherd FA, Sacher AG, Leighl N, Bradbury PA, Liu G. Real-world treatment sequencing, clinically relevant toxicities, health utilities, and survival outcomes in patients with advanced ALK-rearranged Non-small-cell Lung Cancer. Manuscript in Preparation.
Tse BC et al. Curr Oncol. 2020 Dec; 27:e552-e559.
How often should treatment response be assessed?
Response: There is no current standard for how often treatment response should be assessed, in the absence of new or progressive symptoms that trigger interim radiological imaging. Because lorlatinib, along with other ALK-TKIs such as alectinib and brigatinib, are expected to work for years in the first-line setting, radiological assessment of treatment response is required within 2-3 months of initiation of lorlatinib, and thereafter, radiological evaluation every 3-6 months in the absence of symptomatic progression would be considered reasonable.
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility). Certain adverse events occur (specify type, frequency, and severity). Additional treatment becomes necessary (specify).
Response: The primary reason for discontinuation would be disease progression. Additional reasons include Grade 3 or higher toxicities, or even in some cases Grade 1-2 toxicities, if these toxicities significantly adversely influence the quality of life and function of the patients. Minor progression or oligoprogression that requires local management (palliative radiation, surgical resection) need not result in permanent discontinuation; treatment beyond progression was built into the original clinical trials, including CROWN, and should be left to the discretion of the treating oncologist.
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Response: Community setting would be appropriate for treatment with the oral TKI agent, lorlatinib, under the supervision of the prescribing oncologist.
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
If so, which specialties would be relevant?
Response: Not applicable. This is an oncology drug.
Additional Information
Is there any additional information you feel is pertinent to this review?
Response: None
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (Section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
None.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
None.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Geoffrey Liu
Position: Professor of Medicine, University of Toronto; Medical Oncologist, University Health Network
Date: 06-07-2021
Table 6: Declaration for Lung Cancer Canada Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Takeda | — | — | — | X |
Roche | — | — | X | — |
Pfizer | — | — | X | — |
Astra Zeneca | — | — | — | X |
Bristol Myers Squibb | X | — | — | — |
Boehringer Ingelheim | — | — | X | — |
AbbVie | — | X | — | — |
Merck | — | X | — | — |
EMD Serono | X | — | — | — |
Novartis | — | — | X | — |
Glaxo Smith Kline | X | — | — | — |
Declaration for Clinician 2
Name: Rosalyn Juergens
Position: Medical Oncologist and Head of Department of Clinical Trials at the Juravinski Cancer Centre
Date: 06-07-2021
Table 7: Declaration for Lung Cancer Canada Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | — | X | — | — |
Bristol-Myers Squibb | X | — | — | — |
Merck Sharp and Dohme | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 3
Name: Paul Wheatley-Price
Position: Medical Oncologist, The Ottawa Hospital Cancer Centre; Professor, University of Ottawa
Date: 06-07-2021
Table 8: Declaration for Lung Cancer Canada Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | — | X | — | — |
Bayer | X | — | — | — |
Boehringer Ingelheim | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Merck | — | X | — | — |
Novartis | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Quincy Chu
Position: Medical Oncologist, Cross Cancer Institute, Alberta
Date: 06-07-2021
Table 9: Declaration for Lung Cancer Canada Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AbbVie | X | — | — | — |
Amgen | X | — | — | — |
Astra Zeneca | — | — | — | X |
Boehringer Ingelheim | — | X | — | — |
Bristol-Myers Squibb | — | X | — | — |
Eisai | X | — | — | — |
Merck | — | — | X | — |
Novartis | — | X | — | — |
Pfizer | — | X | — | — |
Roche | — | X | — | — |
Declaration for Clinician 5
Name: Ronald Burkes
Position: Medical Oncologist, Mount Sinai Hospital; Professor, University of Toronto
Date: 06-07-2021
Table 10: Declaration for Lung Cancer Canada Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 6
Name: Randeep Sangha
Position: Medical Oncologist, Cross Cancer Institute; Associate Professor, University of Alberta
Date: 06-07-2021
Table 11: Declaration for Lung Cancer Canada Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 7
Name: Donna Maziak
Position: Professor and Thoracic Surgeon, University of Ottawa
Date: 06-07-2021
Table 12: Declaration for Lung Cancer Canada Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Jeffrey Rothenstein
Position: Medical Oncologist, Lakeridge Health, Oshawa
Date: 06-07-2021
Table 13: Declaration for Lung Cancer Canada Clinician 8
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Declaration for Clinician 9
Name: Callista Phillip
Position: Medical Oncologist and Clinical Lead; Oncology Clinic, Joseph Brant Hospital
Date: 06-07-2021
Table 14: Declaration for Lung Cancer Canada Clinician 9
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | X | — | — | — |
Bayer | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 10
Name: David Dawe
Position: Medical Oncologist, CancerCare Manitoba
Date: 06-07-2021
Table 15: Declaration for Lung Cancer Canada Clinician 10
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | — | — | X | — |
Merck | X | — | — | — |
Boehringer-Ingelheim | X | — | — | — |
Declaration for Clinician 11
Name: Stephanie Snow
Position: Medical Oncologist, QEII hospital; Associate Professor, Dalhousie University
Date: 06-07-2021
Table 16: Declaration for Lung Cancer Canada Clinician 11
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Amgen | X | — | — | — |
Astra Zeneca | — | — | X | — |
Bayer | — | X | — | — |
Boehringer Ingelheim | X | — | — | — |
Bristol-Myers Squibb | — | — | X | — |
Eisai | X | — | — | — |
Merck | — | — | X | — |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Purdue | X | — | — | — |
Roche | — | — | X | — |
Taiho | X | — | — | — |
Takeda | — | X | — | — |
Declaration for Clinician 12
Name: Parneet Cheema
Position: Medical Oncologist, William Osler Health Centre
Date: 06-07-2021
Table 17: Declaration for Lung Cancer Canada Clinician 12
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Merck | X | — | — | — |
Novartis | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 13
Name: Mahmoud Abdelsalam
Position: Medical Oncologist, The Moncton Hospital
Date: 06-07-2021
Table 18: Declaration for Lung Cancer Canada Clinician 13
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bristol-Myers Squibb | — | X | — | — |
Declaration for Clinician 14
Name: Barbara Melosky
Position: Medical Oncologist, BC Cancer
Date: 06-07-2021
Table 19: Declaration for Lung Cancer Canada Clinician 14
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
GlaxoSmithKline | — | X | — | — |
Merck | X | — | — | — |
Declaration for Clinician 15
Name: Dr Catherine Labbé
Position: Pulmonologist and Program Director
Date: 06-07-2021
Table 20: Declaration for Lung Cancer Canada Clinician 15
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
BMS | — | X | — | — |
Astra Zeneca | — | X | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 16
Name: Zhaolin Xu
Position: Pathologist, QEII Health Sciences Centre
Date: 06-07-2021
Table 21: Declaration for Lung Cancer Canada Clinician 16
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | X | — | — | — |
Declaration for Clinician 17
Name: Dr. Cheryl Ho
Position: Medical Oncologist, BC Cancer Agency
Date: 06/07/2021
Table 22: Declaration for Lung Cancer Canada Clinician 17
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bayer | X | — | — | — |
Roche | — | — | — | X |
Declaration for Clinician 18
Name: Dr. Normand Blais
Position: Medical Oncologist, Hôpital Notre Dame du CHUM
Date: 06/07/2021
Table 23: Declaration for Lung Cancer Canada Clinician 18
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Novartis | X | — | — | — |
Declaration for Clinician 19
Name: Dr. Sunil Yadav
Position: Professor and Medical Oncologist, Saskatoon Cancer Centre
Date: 06/07/2021
Table 24: Declaration for Lung Cancer Canada Clinician 19
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Bristol-Myers-Squibb | X | — | — | — |
Astra Zeneca | X | — | — | — |
Merck | — | — | X | — |
Roche | — | X | — | — |
Takeda | X | — | — | — |
Declaration for Clinician 20
Name: Dr. Kevin Jao
Position: Medical Oncologist, Hôpital du Sacré-Cœur-de-Montréal
Date: 06-07-2021
Table 25: Declaration for Lung Cancer Canada Clinician 20
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 21
Name: Dr. Nicole Bouchard
Position: Pulmonologist, Sherbrooke University Hospital
Date: 06-07-2021
Table 26: Declaration for Lung Cancer Canada Clinician 21
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Astra Zeneca | X | — | — | — |
Bristol-Myers-Squibb | X | — | — | — |
Merck | X | — | — | — |
Bayer | X | — | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Declaration for Clinician 22
Name: Silvana Spadafora
Position: Medical Oncologist
Date: 06-07-2021
Table 27: Declaration for Lung Cancer Canada Clinician 22
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee (Lung DAC)
Authors of the submission: Dr. Gail Darling, Dr. Andrew Robinson, Dr. Natasha Leighl, Dr. Peter Ellis, Dr. Mohammad Rassouli
About Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee (Lung DAC)
Please describe the purpose of your organization. Include a link to your website (if applicable).
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Please describe how you gathered the information included in the submission.
This input was jointly discussed at a DAC meeting.
Current Treatments
Describe the current treatment paradigm for the disease.
Focus on the Canadian context. Please include drug and non-drug treatments. Drugs without Health Canada approval for use in the management of the indication of interest may be relevant if they are routinely used in Canadian clinical practice. Are such treatments supported by clinical practice guidelines? Treatments available through special access programs are relevant. Do current treatments modify the underlying disease mechanism? Target symptoms?
Response: Current treatments include alectinib, and brigatinib (compassionate access) in previously treated ALK-positive NSCLC.
Treatment Goals
What are the most important goals that an ideal treatment would address?
Examples: Prolong life, delay disease progression, improve lung function, prevent the need for organ transplant, prevent infection or transmission of disease, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, improve health-related quality of life, increase the ability to maintain employment, maintain independence, reduce burden on caregivers.
Response: Prolong, delay disease progression, delay CNS disease progression, reduce loss of cognition, reduce the severity of symptoms, minimize adverse effects, and improve health-related quality of life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals under the Treatment Goals section, please describe goals (needs) that are not being met by currently available treatments.
Examples: Not all patients respond to available treatments. Patients become refractory to current treatment options. No treatments are available to reverse the course of disease. No treatments are available to address key outcomes. Treatments are needed that are better tolerated. Treatment are needed to improve compliance. Formulations are needed to improve convenience.
Response: Currently the needs stated under the Treatment Goals section are being met by alectinib. Longer control of symptomatic disease and longer PFS/OS are still important goals of therapy.
Which patients have the greatest unmet need for an intervention such as the drug under review?
Would these patients be considered a subpopulation or niche population? Describe characteristics of this patient population. Would the drug under review address the unmet need in this patient population?
Response: ALK-positive NSCLC patients, especially those with CNS metastases. These are usually young to very young patients, non-smokers. Although lorlatinib will be appropriate for first line (1L) therapy; the unmet need for these patients will be after failure of currently available options.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Is there a mechanism of action that would complement other available treatments, and would it be added to other treatments? Is the drug under review the first treatment approved that will address the underlying disease process rather than being a symptomatic management therapy? Would the drug under review be used as a first-line treatment, in combination with other treatments, or as a later (or last) line of treatment? Is the drug under review expected to cause a shift in the current treatment paradigm?
Response: Lorlatinib is an active 1L agent. Given funding is available for other active 1L agents, the unmet need may be in the 2L setting.
Please indicate whether or not it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug under review. Please provide a rationale from your perspective.
If so, please describe which treatments should be tried, in what order, and include a brief rationale.
Response: Alectinib is currently the 1L preferred ALK TKI. Lorlatinib is an active drug which has shown to be effective and beneficial in 1L and represents an alternate treatment option.
How would this drug affect the sequencing of therapies for the target condition?
If appropriate for this condition, please indicate which treatments would be given after the therapy has failed and specify whether this is a significant departure from the sequence employed in current practice. Would there be opportunity to treat patients with this same drug in a subsequent line of therapy? If so, according to what parameters?
Response: If lorlatinib is used in 1L, it will replace other ALK TKIs. Post lorlatinib, it would be nice to have other ALK TKIs available. If lorlatinib is used 1L and stopped due to global progression/drug failure, it will not be used again.
Which patients would be best suited for treatment with the drug under review?
Which patients are most likely to respond to treatment with the drug under review? Which patients are most in need of an intervention? Would this differ based on any disease characteristics (e.g., presence or absence of certain symptoms, stage of disease)?
Response: ALK-positive NSCLC
How would patients best suited for treatment with the drug under review be identified?
Examples: Clinician examination or judgement, laboratory tests (specify), diagnostic tools (specify). Is the condition challenging to diagnose in routine clinical practice? Are there any issues related to diagnosis? (e.g., tests may not be widely available, tests may be available at a cost, uncertainty in testing, unclear whether a scale is accurate or the scale may be subjective, variability in expert opinion.) Is it likely that misdiagnosis occurs in clinical practice (e.g., underdiagnosis)? Should patients who are pre-symptomatic be treated considering the mechanism of action of the drug under review?
Response: Through reflex testing that’s already in place
Which patients would be least suitable for treatment with the drug under review?
Response: All ALK-positive advanced NSCLC patients have the potential to benefit
Is it possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review?
If so, how would these patients be identified?
Response: Yes – via ALK testing; the majority of patients in the pivotal trial exhibited response
What outcomes are used to determine whether a patient is responding to treatment in clinical practice?
Are the outcomes used in clinical practice aligned with the outcomes typically used in clinical trials?
Response: Response rate, improvement in symptoms
What would be considered a clinically meaningful response to treatment?
Examples: Reduction in the frequency or severity of symptoms (provide specifics regarding changes in frequency, severity, and so forth). Attainment of major motor milestones. Ability to perform activities of daily living. Improvement in symptoms. Stabilization (no deterioration) of symptoms. Consider the magnitude of the response to treatment. Is this likely to vary across physicians?
Response: All of the above except attainment of major motor milestones
How often should treatment response be assessed?
Response: Patients should be assessed every 2-3 cycles with imaging every 2-6 months as clinically indicated.
What factors should be considered when deciding to discontinue treatment?
Examples: Disease progression (specify; e.g., loss of lower limb mobility). Certain adverse events occur (specify type, frequency, and severity). Additional treatment becomes necessary (specify).
Response: symptomatic disease progression, intolerable side effects
What settings are appropriate for treatment with the drug under review?
Examples: Community setting, hospital (outpatient clinic), specialty clinic
Response: Outpatient administration; inpatient also acceptable at times
For non-oncology drugs, is a specialist required to diagnose, treat, and monitor patients who might receive the drug under review?
If so, which specialties would be relevant?
Response: Not applicable
Additional information
Is there any additional information you feel is pertinent to this review?
Response: In additional to the data in 1L, this drug provides benefit to patients who failed currently available 1L ALK TKIs and should be reconsidered.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (Place in Therapy) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat support to the DAC in completing this input.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician that contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Gail Darling
Position: Cardiothoracic Surgeon/Ontario Cancer Lead
Date: 10-June-2021
Table 28: Declaration for OH-CCO Lung DAC Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Andrew Robinson
Position: Medical Oncologist/Lung DAC member
Date: 10-June-2021
Table 29: Declaration for OH-CCO Lung DAC Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Peter Ellis
Position: Medical Oncologist/Lung DAC member
Date: 10-June-2021
Table 30: Declaration for OH-CCO Lung DAC Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Natasha Leighl
Position: Medical Oncologist/Lung DAC member
Date: 10-June-2021
Table 31: Declaration for OH-CCO Lung DAC Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Mohammad Rassouli
Position: Medical Oncologist/Lung DAC member
Date: 10-June-2021
Table 32: Declaration for OH-CCO Lung DAC Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.