CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Esophageal carcinoma, gastroesophageal junction adenocarcinoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
5-FU
5-fluorouracil
AE
adverse event
BICR
blinded independent central review
CAPOX
capecitabine and oxaliplatin
CCC
Colorectal Cancer Canada
CI
confidence interval
CPS
combined positive score
DOR
duration of response
EAC
esophageal adenocarcinoma
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EGJ
esophagogastric junction
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-OES18
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Cancer Module
EQ-5D-5L
EQ-5D 5-Levels
ESCC
esophageal squamous cell carcinoma
FAS
full analysis set
FOLFIRI
irinotecan, 5-fluorouracil, and oxaliplatin
FOLFOX
5-fluorouracil, oxaliplatin, and leucovorin
GEJ
gastroesophageal junction
GI
gastrointestinal
HER2
human epidermal growth factor receptor 2
HR
hazard ratio
HRQoL
health-related quality of life
ITT
intention to treat
MAIC
matching-adjusted indirect comparison
ORR
objective response rate
OS
overall survival
PD-1
programmed cell death protein 1
PD-L1
programmed cell death ligand 1
PFS
progression-free survival
PRO
patient-reported outcome
QoL
quality of life
RECIST 1.1
Response Evaluation Criteria in Solid Tumors Version 1.1
SD
standard deviation
VAS
Visual Analogue Scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda) IV infusion over 30 minutes |
Indication | Pembrolizumab, in combination with platinum- and fluoropyrimidine-based chemotherapy, is indicated for the first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the esophagogastric junction (tumour centre 1 cm to 5 cm above the gastric cardia) |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project Orbis |
NOC date | June 4, 2021 |
Sponsor | Merck Canada Inc. |
HER2 = human epidermal growth factor receptor 2; NOC = Notice of Compliance.
Introduction
In Canada, esophageal cancer is ranked 19th among all cancer types based on incidence and 10th based on mortality.8 There are 2 distinct histological subtypes: esophageal adenocarcinoma (EAC) and esophageal squamous cell carcinoma (ESCC).9,10 EAC typically occurs in the distal esophagus and gastroesophageal junction (GEJ).11 Adenocarcinoma of the GEJ is further classified into Siewert type I (1 cm to 5 cm above the GEJ), Siewert type II (1 cm above and up to 2 cm below the GEJ), and Siewert type III (2 cm to 5 cm below the GEJ).12
Signs and symptoms of esophageal cancer include dysphagia (difficulty swallowing), frequent chocking on food, unexplained weight loss, indigestion or heartburn, coughing or hoarseness, nausea or vomiting, fatigue, and chest pain, pressure, or burning.8,13,14
The current standard treatment for locally advanced and unresectable or metastatic cancer of the esophagus and GEJ is systemic chemotherapy. Standard first-line chemotherapy regimens typically include a fluoropyrimidine and a platinum (usually cisplatin or oxaliplatin).15-18 Examples of fluoropyrimidine- and platinum-based chemotherapy used in the first-line setting include: cisplatin and 5-fluorouracil [5-FU], capecitabine and cisplatin, capecitabine and oxaliplatin (CAPOX), and 5-FU, oxaliplatin, and leucovorin (FOLFOX). Patients with advanced cancer of the EAC or GEJ may be treated with irinotecan, 5-FU, and oxaliplatin (FOLFIRI),;9 however, this is not commonly used in the first-line setting. Other less common first-line treatments include paclitaxel or docetaxel doublet regimens, paclitaxel or docetaxel triplet regimens, and epirubicin.
Pembrolizumab is a selective humanized monoclonal antibody that enhances immune system detection of tumours and facilitates tumour regression via the programmed cell death protein 1 (PD-1) pathway. The recommended dose for pembrolizumab is 200 mg every 3 weeks or 400 mg every 6 weeks administered as an IV infusion until disease progression, unacceptable toxicity, or to a maximum of 24 months. The Health Canada–approved indication of interest is pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or human epidermal growth factor receptor 2 (HER2)-negative adenocarcinoma of the esophagogastric junction (EGJ; tumour centre 1 cm to 5 cm above the gastric cardia). The CADTH reimbursement request aligns with this Health Canada indication. Refer to the Introduction of the main body of this report for more details.
The objective of this clinical review is to review the beneficial and harmful effects of pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy as per the indication previously highlighted.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review. As well, issues identified by the Provincial Advisory Group that may impact their ability to implement a recommendation are summarized. Refer to the Stakeholder Perspectives Section of the main body of this report for more details.
Patient Input
Three patient groups, including Colorectal Cancer Canada (CCC), the Gastrointestinal (GI) Society, and My Gut Feeling (Stomach Cancer Foundation of Canada), co-created 1 patient input for this review.
According to the patient and caregiver respondents (N = 33), most patients were diagnosed with EAC (77.42%) and 12.90% of patients were diagnosed with ESCC. All patient and caregiver respondents, except 1 patient, reported experiencing the following symptoms before diagnosis: trouble swallowing, heartburn, weight loss, fatigue, worsening indigestion, frequent choking on food, hiccups, and indigestion.
Two patient respondents had experience with the drug under review (pembrolizumab) and reported the following treatment-related side effects: abdominal pain, diarrhea, rash, shortness of breath, and constipation (1 patient); fatigue, itching and some allergic reactions (the other patient). One patient respondent noted that pembrolizumab manages coughing, back pain, hoarseness, and vomiting less effectively than existing therapies. However, both respondents reported that pembrolizumab did manage certain symptoms better than existing therapies including pain behind the breastbone or in the throat, black stool, and weight loss (1 patient); fatigue and vomiting (the other patient). Both patients indicated that they expected the following key outcomes to be improved by pembrolizumab: prolonged overall survival (OS), delayed need for chemotherapy, and convenient route of administration.
Patient and caregiver respondents highlighted that given the poor and short survival rate for most patients with esophageal cancer, it is necessary for patients to have access to new effective therapies that prolong OS, improve quality of life (QoL), reduce disease symptoms, and have tolerable side effects. It was also noted that given the severity of disease symptoms, improved QoL is an important outcome to consider in this setting. Additionally, when asked to indicate trade-offs in respect to treatment outcomes in choosing a new therapy, almost all patient and caregiver respondents indicated that they were willing to take a drug that has been proven to improve QoL even if it would not prolong OS.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts agreed that the full patient population included in the indication (adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ [tumour centre 1 cm to 5 cm above the gastric cardia]) should be eligible for treatment with pembrolizumab. However, the clinical experts noted that some patients are more likely to respond to treatment with pembrolizumab than others (e.g., ESCC histology and programmed cell death ligand 1 [PD-L1] with a combined positive score [CPS] ≥ 10). The clinical experts identified patients with autoimmune diseases are at increased risk of autoimmune disease flares and immune-related adverse events (AEs) when treated with immunotherapy. However, the clinical experts agreed that for patients with well-controlled autoimmune diseases, immunotherapy may still represent an appropriate treatment option for these patients after a discussion of the risks and benefits between clinician and patient. The clinical experts reiterated that the full patient population included in the indication should be eligible for treatment with pembrolizumab.
According to the clinical experts, pembrolizumab added to chemotherapy has the potential to represent a standard of care for patients with esophageal cancer or GEJ Siewert type I. The clinical experts felt that pembrolizumab added to chemotherapy would certainly be a standard of care for patients with ESCC and for patients with a CPS of 10 or greater. The clinical experts also felt that pembrolizumab added to chemotherapy was an appropriate treatment option for patients with GEJ Siewert type I who are HER2 negative, EAC, and tumours with a CPS of less than 10.
The clinical experts identified prolonged life and improved health-related quality of life (HRQoL) to be important outcomes and goals for treatment. The clinical experts noted that not all patients respond to available treatment options and patients ultimately become refractory to current therapies. As a result, there is a need for more effective treatment options with manageable safety profile.
To the clinical experts, a clinically meaningful response to treatment would be an improved OS and a reduction in the frequency or severity of symptoms (improved QoL). The clinical experts expressed that for patients treated with immunotherapy, a long-term plateau of the survival curve would also be considered a significant benefit since current median survival for this patient population is less than 12 months. As well, the clinical experts stated that if the addition of an agent to an established regimen was not detrimental to QoL and improved survival, that would also be considered a clinically meaningful response to treatment.
Clinician Group Input
Overall, 2 clinician group inputs were provided for the review: 1 joint submission by 6 clinicians on behalf of the medical advisory board of My Gut Feeling, the Canadian GI Oncology Evidence Network, and the medical advisory board of CCC; and 1 joint submission from 4 clinicians on behalf of the Ontario Health-Cancer Care Ontario GI Drug Advisory.
Both clinician groups emphasized that all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would greatly benefit from this treatment. The clinician group emphasized that all patients with locally advanced unresectable or metastatic esophageal carcinoma or HER2-negative GEJ adenocarcinoma have a poor prognosis; therefore, all patients should be eligible for the addition of pembrolizumab to first-line platinum and fluoropyrimidine chemotherapy.
The clinician groups identified prolonged life and improved or maintained HRQoL as the goals of treatment. Delaying progression of disease and ensuring adequate nutritional intake were additional goals of treatment identified by the Ontario Health-Cancer Care Ontario GI Drug Advisory clinicians.
To the clinician groups, a clinically meaningful response to treatments would be a reduction in symptoms or at minimum, a stabilization of symptoms (e.g., less pain, weight gain/cessation of weight loss, less fatigue). Additionally, an overall improvement in the ability to perform daily activities and a reduction in the caregiver burden would also be considered clinically meaningful responses to treatment.
In summary, while the clinician groups and clinical experts noted that patients with PD-L1 with a CPS of 10 or greater, and ESCC patients with PD-L1 with a CPS of 10 or greater are more likely to respond to pembrolizumab than the intention-to-treat (ITT) population (any PD-L1 CPS and esophageal cancer or GEJ Siewert type I), all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would benefit from pembrolizumab, and as a result, both the clinician groups and the clinical experts expressed that the full patient population in the indication submitted for reimbursement (i.e., esophageal cancer and HER2-negative GEJ Siewert type I) should be eligible for treatment with pembrolizumab.
Drug Program Input
The Provincial Advisory Group identified the following jurisdictional implementation issues: relevant comparators, consideration for initiation of therapy, consideration for discontinuation of therapy, generalizability, care provision, system issues, and economic considerations. The clinical experts consulted by CADTH weighed evidence from the KEYNOTE-590 trial and other clinical considerations to provide responses to the Provincial Advisory Group’s drug program implementation questions. Refer to Table 4: Summary of Drug Plan Input and Clinical Expert Response for more details.
Clinical Evidence
Pivotal Study and Protocol Selected Study (KEYNOTE-590)
Description of Study
The KEYNOTE-590 study is an ongoing phase III, randomized, double-blind, placebo-controlled, multi-centre, superiority study comparing pembrolizumab in combination with cisplatin and 5-FU to placebo in combination with cisplatin and 5-FU for the first-line treatment of patients with locally advanced unresectable or metastatic adenocarcinoma or ESCC or advanced or metastatic Siewert type I adenocarcinoma of the GEJ. Refer to Table 6: Details of Included Study.1
One co-primary outcome is OS among patients with ESCC whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), patients with ESCC, patients whose tumours are PD-L1 with a CPS of 10 or greater, and all patients. The second co-primary outcome is progression-free survival (PFS) per Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1) among patients with ESCC, patients whose tumours are PD-L1 with a CPS of 10 or greater, and all patients. Secondary and exploratory outcomes included: objective response rate (ORR), duration of response (DOR), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module (EORTC QLQ-OES18), safety, and EQ5D-5 Levels questionnaire (EQ-5D-5L).1
The demographic and baseline characteristics were well-balanced between groups, except for age (65 years or older) and stage IVB (distant lymph nodes and/or other organs) disease. There were more patients 65 years or older in the pembrolizumab in combination with cisplatin and 5-FU group (46.1%) compared with the placebo in combination with cisplatin and 5-FU group (39.9%). There were more patients with a current disease stage of iv B in the pembrolizumab in combination with cisplatin and 5-FU group (17.4%) compared with the placebo in combination with cisplatin and 5-FU group (10.9%). The majority (99.7%) had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1 (39.9% and 59.8%, respectively) and had metastatic disease (91.2%). Most patients were male (83.4%), had an ESCC primary diagnosis (73.2%), and about half were Asian (53.4%), enrolled in Asia (52.5%), and had tumour expressed PD-L1 with a CPS of 10 or greater (51.1%). Refer to Table 7: Summary of Baseline Characteristics, ITT Population.1
The results for both PFS and OS are deemed final based on interim analysis since both primary end points were met with a pre-specified stopping boundary for statistical significance. However, the study is ongoing; therefore, long-term efficacy and safety data are anticipated to be available in the future.3
Efficacy Results
As of the data cut-off date (July 2, 2020), the median follow-up duration for patients in the pembrolizumab in combination with cisplatin and 5-FU group was 12.6 months (range = 0.1 to 33.6) and the median follow-up duration for patients in the placebo combination with cisplatin and 5-FU group was 9.8 months (range = 0.1 to 33.6).1
In all patients, there was a 27% reduction in the risk of death in favour of pembrolizumab in combination with cisplatin and 5-FU. The OS hazard ratio (HR) was 0.73 (95% confidence interval [CI]:, 0.62 to 0.86) with P < 0.0001, crossing the boundary for statistical significance. The median OS was 12.4 months (95% CI, 10.5 to 14.0) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 9.8 months (95% CI, 8.8 to 10.8) for the placebo in combination with cisplatin and 5-FU group. A statistically significant OS benefit in favour of pembrolizumab in combination with cisplatin and 5-FU was also observed in patients with ESCC whose tumours express PD-L1 with a CPS of 10 or greater, patients with ESCC, and patients whose tumours express PD-L1 with a CPS of 10 or greater.1
In all patients, there was a 35% reduction in risk of death and disease progression in favour of pembrolizumab in combination with cisplatin and 5-FU. The PFS HR was 0.65 (95% CI, 0.55 to 0.76) with P < 0.0001, crossing the boundary for statistical significance. The median PFS was 6.3 months (95% CI, 6.2 to 6.9) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 5.8 months (95% CI, 5.0 to 6.0) for the placebo in combination with cisplatin and 5-FU group. A statistically significant PFS benefit in favour of pembrolizumab in combination with cisplatin and 5-FU was also observed in patients with ESCC and patients whose tumours express PD-L1 with a CPS of 10 or greater.1
In the patient-reported outcome (PRO) full analysis set (FAS) population (i.e., all randomized patients who have at least 1 PRO assessment available for the specific end point and have received at least 1 dose of the study intervention), the least squares mean change from baseline to week 18 in EQ-5D visual analogue scale (VAS) was similar between the 2 groups. The mean change from baseline in global health status/QoL (using the EORTC QLQ-C30 scale) remained stable over time for the pembrolizumab in combination with cisplatin and 5-FU group compared with the placebo in combination with cisplatin and 5-FU group, and the median time to deterioration for global health status/QoL was not reached for both groups.1
Refer to Table 2 and Table 14.
Harms Results
Overall, any AEs, treatment-related AEs, grade 3 to 5 AEs, and any serious AEs were comparable between the pembrolizumab in combination with cisplatin and 5-FU group and the placebo in combination with cisplatin and 5-FU (Table 2) group. The most commonly reported AEs were nausea (67.3% versus 62.7%), anemia (50.5% versus 56.2%), decreased appetite (44.3% versus 38.1%), fatigue (40.3% versus 34.1%), and constipation (40.0% versus 40.3%).
Although the number of events was infrequent, deaths due to AEs and deaths due to treatment-related AEs were similar between the 2 groups.
Of note, immune-mediated AEs and infusion reactions (25.7% versus 11.6%), hypothyroidism (10.8% versus 6.5%) and hyperthyroidism (5.7% versus 0.8%), pneumonitis (6.2% versus 0.5%), grade 3 or greater treatment-related AEs (71.9% versus 67.6%), serious treatment-related AEs (31.6% versus 26.2%), and discontinuation due to treatment-related AEs (19.5% versus 11.6%) were higher among the pembrolizumab in combination with cisplatin and 5-FU group.1
Refer to Table 2: Summary of Key Results from Pivotal and Protocol Selected and Table 27 Additional Harms Outcomes.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Study
Outcomes | KEYNOTE-590 | |
|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU | |
OS: Co-primary outcome, ITT population | ||
OS: Patients with ESCC and PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 94/143 (65.7) | 121/143 (84.6) |
Median OS, months (95% CI)a | 13.9 (11.1 to 17.7) | 8.8 (7.8 to 10.5) |
HR (Cox regression model)b (95% CI) | 0.57 (0.43 to 0.75) | |
P value (stratified log-rank test)c | < 0.0001 | |
12-month OS rate, % (95% CI)a | 54.5 (46.0 to 62.3) | 33.6 (26.0 to 41.3) |
OS: Patients with ESCC | ||
Events (deaths), n/N (%) | 190/274 (69.3) | 222/274 (81.0) |
Median OS, months (95% CI)a | 12.6 (10.2 to 14.3) | 9.8 (8.6 to 11.1) |
HR (Cox regression model)b (95% CI) | 0.72 (0.60 to 0.88) | |
P value (stratified log-rank test)c | 0.0006 | |
12-month OS rate, % (95% CI)a | 51.0 (44.9 to 56.8) | 37.9 (32.2 to 43.7) |
OS: Patients with PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 124/186 (66.7) | 165/197 (83.8) |
Median OS, months (95% CI)a | 13.5 (11.1 to 15.6) | 9.4 (8.0 to 10.7) |
HR (Cox regression model) (95% CI)d | 0.62 (0.49 to 0.78) | |
P value (stratified log-rank test)e | < 0.0001 | |
12-month OS rate, % (95% CI)a | 53.8 (46.3 to 60.6) | 37.1 (30.3 to 43.8) |
OS: All patients | ||
Events (deaths), n/N (%) | 262/373 (70.2) | 309/376 (82.2) |
Median OS, months (95% CI)a | 12.4 (10.5 to 14.0) | 9.8 (8.8 to 10.8) |
HR (Cox regression model)f (95% CI) | 0.73 (0.62 to 0.86) | |
P value (stratified log-rank test)g | < 0.0001 | |
12-month OS rate, % (95% CI)a | 50.6 (45.4 to 55.6) | 39.4 (34.4 to 44.3) |
EQ-5D: Exploratory outcome | ||
EQ-5D VAS: FAS population | ||
Change from baseline to week 18, LS mean (95% CI)h | –2.29 (–4.35 to –0.24) | –3.49 (–5.61 to –1.37) |
Difference in LS means (95% CI), P valueh | 1.20 (–1.61 to 4.01), 0.4016 | |
EQ-5D VAS: Patients with ESCC and PD-L1 CPS ≥ 10, FAS population | ||
Change from baseline to week 18, LS mean (95% CI)i | –4.46 (–7.94 to –0.97) | –4.35 (–8.06 to –0.65) |
Difference in LS means (95% CI), P valuei | –0.10 (–4.96 to 4.76), 0.9668 | |
EQ-5D VAS: Patients with ESCC, FAS population | ||
Change from baseline to week 18, LS mean (95% CI)i | –3.78 (–6.19 to –1.38) | –3.47 (–5.97 to –0.97) |
Difference in LS means (95% CI), P valuei | –0.31 (–3.64 to 3.01), 0.8532 | |
EQ-5D VAS: Patients with PD-L1 CPS ≥ 10, FAS population | ||
Change from baseline to week 18, LS mean (95% CI)j | –3.38 (–6.42 to –0.35) | –3.78 (–6.87 to –0.69) |
Difference in LS means (95% CI), P valuej | 0.40 (–3.70 to 4.49), 0.8490 | |
PFS: Co-primary outcome, ITT population | ||
PFS: Patients with ESCC | ||
Events (deaths), n/N (%) | 219/274 (79.9) | 244/274 (89.1) |
Median PFS, months (95% CI)a | 6.3 (6.2 to 6.9) | 5.8 (5.0 to 6.1) |
HR (Cox regression model)l (95% CI) b | 0.65 (0.54 to 0.78) | |
P value (stratified log-rank test)c | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 24.1 (19.0 to 29.6) | 11.9 (8.2 to 16.3) |
PFS: Patients with PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 140/186 (75.3) | 174/197 (88.3) |
Median PFS, months (95% CI)a | 7.5 (6.2 to 8.2) | 5.5 (4.3 to 6.0) |
HR (Cox regression model) (95% CI)l | 0.51 (0.41 to 0.65) | |
P value (stratified log-rank test)m | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 30.3 (23.5 to 37.5) | 9.2 (5.5 to 14.2) |
PFS: All patients | ||
Events (deaths), n (%) | 297/373 (79.6) | 333/376 (88.6) |
Median PFS, months (95% CI)a | 6.3 (6.2 to 6.9) | 5.8 (5.0 to 6.0) |
HR (Cox regression model) (95% CI)f | 0.65 (0.55 to 0.76) | |
P value (stratified log-rank test)g | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 24.9 (20.4 to 29.6) | 11.9 (8.7 to 15.7) |
Harms outcomes | N = 370 | N = 370 |
Any adverse event, n (%) | 370 (100.0) | 368 (99.5) |
Grade ≥ 3k adverse event, n (%) | 318 (85.9) | 308 (83.2) |
Treatment-related adverse eventn, n (%) | 364 (98.4) | 360 (97.3) |
Grade ≥ 3 treatment-related adverse event, n (%) | 266 (71.9) | 250 (67.6) |
Any serious adverse event, n (%) | 205 (55.4) | 204 (55.1) |
Serious treatment-related adverse evento, n (%) | 117 (31.6) | 97 (26.2) |
Any adverse event leading to discontinuation, n (%) | 90 (24.3) | 74 (20.0) |
Discontinuation due to treatment-related adverse event | 72 (19.5) | 43 (11.6) |
Death due to adverse event | 28 (7.6) | 38 (10.3) |
Death due to treated-related adverse event | 9 (2.4) | 5 (1.4) |
Notable harms/harms of special interest | N = 370 | N = 370 |
Immune-mediated adverse events and infusion reactions | 95 (25.7) | 43 (11.6) |
Hypothyroidism | 40 (10.8) | 24 (6.5) |
Hyperthyroidism | 21 (5.7) | 3 (0.8) |
Pneumonitis | 23 (6.2) | 2 (0.5) |
Colitis | 8 (2.2) | 6 (1.6) |
Adrenal Insufficiency | 4 (1.1) | 2 (0.5) |
Hepatitis | 5 (1.4) | 0 (0.0) |
Hypophysitis | 3 (0.8) | 0 (0.0) |
Nephritis | 1 (0.3) | 2 (0.5) |
Type 1 diabetes mellitus | 1 (0.3) | 0 (0.0) |
5-FU = 5-fluorouracil; CI = confidence interval; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; ESCC = esophageal squamous cell carcinoma; FAS = full set analysis; HR = hazard ratio; ITT = intention to treat; LS = least square; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival; OS = overall survival; VAS = visual analogue scale.
aFrom product-limit (Kaplan–Meier) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by geographic region (Asia, rest of the world) and ECOG Performance Status (0, 1).
cOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world) and ECOG Performance Status (0, 1).
dBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by geographic region (Asia vs. rest of the world) and tumour histology (adenocarcinoma vs. squamous cell carcinoma).
eOne-sided P value based on log-rank test stratified by geographic region (Asia vs. rest of the world) and tumour histology (adenocarcinoma vs. squamous cell carcinoma).
fStratified by geographic region (Asia, rest of the world), tumour histology (adenocarcinoma, squamous cell carcinoma), and ECOG Performance Status (0, 1).
gOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world), tumour histology (adenocarcinoma, squamous cell carcinoma), and ECOG Performance Status (0, 1).
hBased on a constrained longitudinal data analysis (cLDA) model with the patient-reported outcome scores as the response variable with covariates for treatment by study visit interaction, stratification factors geographic region (Asia, rest of the world), tumour histology (adenocarcinoma, squamous cell carcinoma), and ECOG Performance Status (0, 1).
iBased on a cLDA model with the patient-reported outcome scores as the response variable with covariates for treatment by study visit interaction, stratification factors, geographic region (Asia, rest of the world), and ECOG Performance Status (0, 1).
jBased on a cLDA model with the patient-reported outcome scores as the response variable with covariates for treatment by study visit interaction, stratification factors, geographic region (Asia, rest of the world), and tumour histology (adenocarcinoma, squamous cell carcinoma).
kGrades are based on National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03.
lBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by geographic region (Asia, rest of the world) and tumour histology (adenocarcinoma, squamous cell carcinoma).
mOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world) and tumour histology (adenocarcinoma, squamous cell carcinoma).
nDetermined by the investigator to be related to the drug.
oSerious adverse events up to 90 days of last dose are included.
Source: Clinical Study Report1 manuscript under review (Sun et al. [2021]).7
Critical Appraisal
Notable limitations of the KEYNOTE-590 trial are highlighted in the following text. For a complete list of critical appraisal points, refer to Clinical Evidence Section, Critical Appraisal.
There is a potential risk of bias because of missing data on secondary and exploratory end points (e.g., DOR, EORTC QLQ-C30, EORTC QLQ-OES18, and EQ-5D-5L), particularly on the QoL measures. In addition, for subjective outcomes (e.g., in PROs), patients may also have differential recall bias. For example, drug-related AEs, such as immune-mediated events (25.7% versus 11.6%), and particularly, hypothyroidism (symptoms including fatigue, increased sensitivity to cold, muscle weakness) and hyperthyroidism (symptoms including nervousness, anxiety, fatigue, and weight loss) might have led to unblinding and the patients’ awareness of their treatment assignment, potentially leading to biased assessment of the PROs. Overall, the magnitude and direction of the impact of missing data and imbalances is unknown.
The platinum- and fluoropyrimidine-based chemotherapy used in the KEYNOTE-590 study (i.e., cisplatin and 5-FU) represents 1 of the standard first-line chemotherapies regimens, other relevant treatment regimens (listed in the systematic review protocol) are not considered in the KEYNOTE-590 study. The overall beneficial effect of the combination therapy with pembrolizumab was present. However, it would remain uncertain if such benefit could be generalizable to different combinations of chemotherapies regimens. Moreover, the study excluded patients with poor ECOG PS scores (> 1). This further compromised the generalizability of the findings on efficacy and particularly, safety to those patients who may receive this first-line combination therapy in practice.
The reported OS and PFS results are deemed final based on interim analysis according to pre-specified stopping criteria. However, whether the “actual” final efficacy results would conform with these interim results is unknown. There are case reports that discuss the early stop of a trial to claim statistical significance according to pre-specified stopping rule that had suffered type I error with the interim results and the estimates of effects could not be the repeated at the final analysis after the trial was completed.20-22
Indirect Comparisons
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search. The sponsor conducted a feasibility assessment3 estimating the comparative efficacy and safety of pembrolizumab plus cisplatin and 5-FU versus other competing interventions using data obtained from a systematic literature review.
The submitted feasibility assessment was summarized and critically appraised by the CADTH clinical review team and can be found in Appendix 5. Ultimately, the CADTH clinical review team concluded that a standard network meta-analysis was not feasible due to lack of network connectivity, and that an unanchored matching-adjusted indirect comparison (MAIC) would likely be biased, and it would not be possible to quantify or identify the direction of the bias.
Other Relevant Evidence
The following 2 studies (KEYNOTE-062 and KEYNOTE-859) were identified as relevant because they met the systematic review protocol; however, were a mixed population (i.e., all HER2-negative GEJ patients were enrolled without any Siewert classification, whereas only patients with HER2-negative Siewert type I GEJ are of relevance to the reimbursement request).
It is also important to note that the trials did not include patients with ESCC or adenocarcinoma of the esophagus, which is a relevant population for the reimbursement request. For the KEYNOTE-062 study, patients must be PD-L1 positive (i.e., CPS ≥ 1), whereas PD-L1 status is not an eligibility criterion for reimbursement in for this submission. Both trials used alternative platinum- and fluoropyrimidine-based chemotherapy backbones for the intervention and comparator compared to the KEYNOTE-590 study. In the KEYNOTE-062 study, cisplatin and 5-FU or cisplatin and capecitabine were offered as the chemotherapy backbone for the intervention and comparator, while in the KEYNOTE-859 study, cisplatin and 5-FU or oxaliplatin and capecitabine were offered.
The KEYNOTE-062 study is a phase III, randomized, partially blinded, multi-centre study comparing pembrolizumab as monotherapy and in combination with cisplatin and 5-FU or cisplatin and capecitabine versus placebo in combination with cisplatin and 5-FU or cisplatin and capecitabine as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma. The results from the pre-specified subgroup analysis of the primary location (GEJ) were only available for OS and safety data were reported for the entire study population (gastric and GEJ adenocarcinoma).
In the overall study population (patients with gastric and GEJ adenocarcinoma), there is no difference in OS between the pembrolizumab combination and chemotherapy groups for patients with PD-L1 a CPS of 1 or greater (OS HR = 0.85; 95% CI, 0.7 to 1.03). The pre-specified OS subgroup analysis of the primary location for GEJ were consistent with the overall study population results (OS HR = 0.96; 95% CI, 0.67 to 1.36). The GEJ subgroup OS results were exploratory, underpowered, and not reflective of the entire reimbursement population, and therefore should be interpreted with caution. Results for the primary location (GEJ adenocarcinoma) subgroup for other important efficacy outcomes were not available. In the overall population (patients with gastric and GEJ adenocarcinoma), more AEs leading to discontinuation and immune-mediated AEs and infusion reactions were reported in the pembrolizumab combination group compared to the chemotherapy group (27.6% versus 18.0%, and 24.0% versus 7.8%, respectively).23
KEYNOTE-859 is a phase III, multi-centre study comparing pembrolizumab in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) versus placebo in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma. Currently, only study design details are available.24 The study is still ongoing, and no results are available at this time.3
Refer to Clinical Evidence Section, Other Relevant Evidence for more details.
Conclusions
Compared to placebo in combination with cisplatin and 5-FU, first-line treatment with pembrolizumab in combination with cisplatin and 5-FU showed a clinically meaningful and statistically significant overall and PFS benefit in adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia). While patients with PD-L1 with a CPS of 10 or greater, and patients with ESCC with PD-L1 with a CPS of 10 or greater are more likely to respond to pembrolizumab than the ITT population (any PD-L1 CPS and esophageal cancer or GEJ Siewert type I), all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would benefit from pembrolizumab, and as a result, clinicians expressed that the full patient population in the indication (adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ [tumour centre 1 cm to 5 cm above the gastric cardia]) should be eligible for treatment with pembrolizumab. Discontinuation due to treatment-related AEs, serious treatment-related AEs, and immune-mediated AEs and infusion reactions were more frequently reported in patients treated with pembrolizumab in combination with cisplatin and 5-FU compared to patients treated with placebo in combination with cisplatin and 5-FU. Although there was no clinically meaningful deterioration in QoL, there remains uncertainty in PROs and QoL due to the limitations discussed (i.e., missing data, recall bias). The study is ongoing; therefore, long-term efficacy and safety data are anticipated to be available in the future. In addition, study eligibility included only patients with ECOG PS 0 or 1. Therefore, the benefit and safety profile are unknown in those patients with an ECOG PS greater than 1 in real-world clinical practice, who are also likely to receive this combination therapy.
The platinum- and fluoropyrimidine-based chemotherapy used in the KEYNOTE-590 study (i.e., cisplatin and 5-FU) represents 1 of the standard of first-line chemotherapies regimens. The KEYNOTE-062 and KEYNOTE-859 studies used alternative platinum- and fluoropyrimidine-based chemotherapy backbones for the intervention and comparator compared to the KEYNOTE-590 study (cisplatin and 5-FU or cisplatin and capecitabine for the KEYNOTE-062 study and cisplatin and 5-FU or oxaliplatin and capecitabine for the KEYNOTE-859 study). However, both trials had a mixed population (i.e., all HER2-negative GEJ patients were enrolled without any Siewert classification, whereas only patients with HER2-negative Siewert type I GEJ are of relevance to the reimbursement request) and both trials did not include patients with ESCC or adenocarcinoma of the esophagus, which is a relevant population for the reimbursement request. Based on clinical expert opinion, it would be reasonable to use other platinum- and fluoropyrimidine-based chemotherapy backbones apart from cisplatin and 5-FU.
Introduction
Disease Background
Esophageal cancer initiates in the cells of the esophagus. In Canada, esophageal cancer is ranked 19th among all cancer types based on incidence and 10th based on mortality.8 In 2020, it was estimated that a total of 2,400 Canadians would be diagnosed with esophageal cancer and 2,300 Canadians would die from esophageal cancer.25 Esophageal cancer is among 1 of the cancers with a high proportion of metastatic disease (stage IV) at first diagnosis (39.9%),8 with a relative 5-year survival rate for metastatic esophageal cancer of 5%.26
There are 2 distinct histological subtypes: EAC which begins in the glandular cells and ESCC which begins in the squamous (flat, thin) cells.9,10 EAC typically occurs in the distal esophagus and GEJ.11 Adenocarcinoma of the GEJ is further classified into: Siewert type I (1 cm to 5 cm above the GEJ), Siewert type II (1 cm above and up to 2 cm below the GEJ), and Siewert type III (2 cm to 5 cm below the GEJ).12
Although ESCC is the most common subtype diagnosed globally, EAC has become more predominant across the Western countries.10 In Canada, the incidence of EAC has been increasing (10.9 cases per million in 1992 compared to 26.8 cases per million in 2010), while the incidence of ESCC has been declining (18.2 cases per million in 1992 compared to 14.7 cases per million in 2010).10 It is estimated that by 2026, the incidence of EAC would be 4.8 per 100,000 in men and 0.8 per 100,000 in women and the incidence of ESCC would be 1.3 per 100,000 in men and 0.6 per 100 women.27
Signs and symptoms of esophageal cancer include dysphagia (difficulty swallowing), frequent chocking on food, unexplained weight loss, indigestion or heartburn, coughing or hoarseness, nausea or vomiting, fatigue, and chest pain, pressure, or burning.4,8,13 As a result, patients’ QoL is negatively affected.28
The recommended diagnostic work-up includes an esophagogastroduodenoscopy with biopsy to establish the tumour’s location and histology, followed by a CT scan of the thorax, abdomen, and pelvis to establish the tumour’s location, depth of penetration into the esophageal wall, invasion into adjacent structures, and involvement of regional and non-regional lymph node, and metastatic disease. Blood work is also recommended to identify end-organ dysfunction.15
Standards of Therapy
The current standard treatment for locally advanced and unresectable or metastatic cancer of the esophagus and GEJ is systemic chemotherapy. Patients with advanced or metastatic EAC and GEJ are treated similarly to gastric adenocarcinoma.15-18 In fact, phase III clinical trials for metastatic gastric cancer include patients with GEJ.15-18,23,24 HER2 status is evaluated for patients with EAC or GEJ, as targeted therapy (trastuzumab-based treatment) is recommended for patients who are HER2 positive.29
As noted by the clinical experts, standard first-line chemotherapy regimens include a fluoropyrimidine and a platinum (usually cisplatin or oxaliplatin)15-18 for patients with advanced ESCC and patients with HER2-negative EAC or GEJ. Examples of fluoropyrimidine- and platinum-based chemotherapy used in the first-line setting include: cisplatin and 5-FU, capecitabine and cisplatin, CAPOX, and FOLFOX. Patients with advanced cancer of the EAC or GEJ may be treated with FOLFIRI19; however, this is not commonly used in the first-line setting. Other less common first-line treatments include paclitaxel or docetaxel doublet regimens, paclitaxel or docetaxel triplet regimens, and epirubicin.
The clinical experts identified prolonged life and improved HRQoL as the goals of treatment. Similarly, the clinician groups identified prolonged life and improved or maintained HRQoL as the goals of treatment. Delaying progression of disease and ensuring adequate nutritional intake were additional goals of treatment identified by a clinical group, while access to new effective therapies that prolong OS, improve QoL, reduce disease symptoms, and have tolerable side effects were noted as important for patient and caregiver respondents.
Drug
Pembrolizumab is a selective humanized monoclonal antibody that enhances immune system detection of tumours and facilitates tumour regression via the PD-1 pathway. The Health Canada recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks administered as an IV infusion until disease progression, unacceptable toxicity, or to a maximum of 24 months. Health Canada has issued market authorization for pembrolizumab in various indications such as classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma, urothelial carcinoma, endometrial carcinoma, melanoma, non–small cell lung carcinoma, renal cell carcinoma, head and neck squamous cell carcinoma, and colorectal cancer.5
The Health Canada–approved indication of interest is pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia).5 The CADTH reimbursement request aligns with this Health Canada indication. Refer to Table 3.
Table 3: Key Characteristics of Pembrolizumab
Item | Pembrolizumab |
|---|---|
Mechanism of action | Exerts dual ligand blockade of the PD-1 pathway on antigen or tumour cells and reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment |
Indicationa | In combination with platinum- and fluoropyrimidine-based chemotherapy, is indicated for the first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the esophagogastric junction (tumour centre 1 cm to 5 cm above the gastric cardia) |
Route of administration | IV |
Recommended dose | 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity, disease progression, or to a maximum of 24 months |
Serious adverse effects or safety issues | Hepatic impairment Immune-mediated adverse reactions: immune-mediated pneumonitis, immune-mediated colitis, immune-mediated hepatitis, immune-mediated nephritis and renal dysfunction, immune-mediated endocrinopathies, adrenal insufficiency, hypophysitis, type 1 diabetes mellitus, thyroid disorders, severe skin reactions Infusion-related reactions Renal impairment Teratogenic risk |
Other | Given in combination with platinum- and fluoropyrimidine-based chemotherapy |
HER2 = human epidermal growth factor receptor 2; PD-1 = programmed cell death protein 1.
aHealth Canada–approved indication.
Source: Health Canada Keytruda Product Monograph.5
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Groups and Information Gathered
Three patient groups, CCC, the GI Society, and My Gut Feeling (Stomach Cancer Foundation of Canada), co-created 1 patient input for this review. CCC drafted the patient group input which was reviewed by the GI Society and My Gut Feeling (Stomach Cancer Foundation of Canada) before its submission to CADTH. All 3 patient groups collected survey data.
CCC is a charitable not-for-profit organization which is dedicated to colorectal cancer awareness and education, supports patients and caregivers, and advocates on their behalf. It aims to reduce the incidence and mortality of colorectal cancer in Canada while improving the QoL of patients, their families, and their caregivers.
The GI Society is committed to improving the lives of people with GI and liver conditions, supporting research, advocating for appropriate patient access to health care, promoting GI and liver health, and providing trusted, evidence-based information for all areas of the GI tract.
My Gut Feeling (Stomach Cancer Foundation of Canada) is a non-profit organization, founded by 2 survivors, dedicated to providing support, awareness, education, information, and advocacy to patients with stomach cancer, survivors, and caregivers. It aims to dispel misconceptions about stomach cancer and to provide information every step of the way from the time of diagnosis to living with and surviving stomach cancer. It strives to improve patients’ and caregivers’ QoL, offer a voice to patients and caregivers, and provide a peer mentorship based on personal experience with stomach cancer.
Patient input was collected through an online patient and caregiver survey co-created by the 3 patient groups (CCC, GI Society, and My Gut Feeling [Stomach Cancer Foundation of Canada)] during the period of April 23, 2021, to May 16, 2021. A total of 25 patients and 8 caregivers responded to the survey, 62.50% of respondents were male (1 respondent’s gender was unknown). Most survey respondents were from the UK and Northern Ireland (45.45%), followed by the US (36.36%), Canada (9.09%), New Zealand (3.03%), Ireland (3.03%), and Belgium (3.03%). According to the survey respondents, at the time of diagnosis, patients’ ages ranged from 20 years to 29 years (6.06%) to 70 to 79 years (3.03%); most patients (39.39%) were 50 to 59 years old at the time of their cancer diagnoses. Of all survey respondents (N = 33), 30.30% were previously treated, 24.24% were in remission, 21.21% were undergoing treatment, 6.06% were caregivers participating in the survey on behalf of a patient undergoing treatment, and 18.18% were caregivers participating on behalf of a patient who had been previously treated.
Disease Experience
According to the patient and caregiver respondents, most patients were diagnosed with adenocarcinoma (77.42%) and 12.90% of patients were diagnosed with squamous cell carcinoma. The percentage of patients diagnosed with stage III esophageal cancer was 38.71%, followed by 25.81%, 22.58%, and 3.23% of patients diagnosed with stage IV, II, and I disease, respectively. Of those patients diagnosed with stage IV disease (n = 7), 3 patients were in stage IV disease, 2 patients were clear of metastases, 1 patient had passed away, and 1 patient was in the neoadjuvant stage at the time of completing the survey. Two patients who were diagnosed with stage III disease were experiencing stage IV disease at the time of participating in the survey. According to the survey responses, patients whose cancer had spread beyond the initial diagnosis had metastases mostly in the lymph nodes (37.93%), liver (20.69%), lung (17.24%), and stomach (14.29%).
When asked if any esophageal cancer-induced symptoms were experienced before diagnosis, all patient and caregiver respondents, except 1 patient, reported experiencing symptoms including (presented here in order of most frequently reported) trouble swallowing, heartburn, weight loss, fatigue, worsening indigestion, frequent choking on food, hiccups, and indigestion.
Experiences With Currently Available Treatments
According to the patient and caregiver respondents, most patients had received chemotherapy (96.70%) followed by surgery (66.70%), radiation therapy (50.0%), endoscopic therapy (16.70%), and other targeted therapies (10.0%); more than half of the survey respondents (58.62%) felt that therapies were effective at controlling symptoms of esophageal cancer. According to the survey, the most reported side effects from therapies included fatigue (88.89%), nausea (62.96%), loss of appetite (62.96%), and low white blood cell count (51.85%). One patient respondent reported being currently on nivolumab.
Most patient and caregiver respondents (75.86%) indicated that most of their needs were being met by therapies currently available; however, 24.14% of respondents believe otherwise. The following quotes illustrate areas of unmet need.
“Short survival rates.”
“[Ability of the cancer] to continue to spread.”
“[The lack of] “metabolism of food.”
“Inability to eat enough to constitute a healthy diet.”
“It is not possible for [current drugs] to stop the growth, only prolong life.”
“The chemotherapy was tolerable but did not improve quality of life as the side effects in addition to the side effects from the surgery and need for a feeding tube really impacted my brother-in-law’s ability to go out, eat, carry on a conversation, or enjoy his family.”
Experience With Drug Under Review
Two patient respondents had experience with the drug under review; 1 patient with stage III esophageal cancer was previously treated with pembrolizumab, and another patient with stage IV esophageal cancer is currently undergoing treatment with pembrolizumab. One patient respondent noted that in addition to pembrolizumab, treatment also involved cryotherapy, radiation, and targeted therapy. The other patient respondent indicated having access to pembrolizumab via a clinical trial with no other therapy included.
The following treatment-associated side effects were reported by the 2 patient respondents: abdominal pain, diarrhea, rash, shortness of breath, and constipation (I patient); fatigue, itching, and some allergic reactions (the other patient). One patient respondent noted that pembrolizumab manages some symptoms less effectively than existing therapies including coughing, back pain, hoarseness, and vomiting. However, both respondents reported that pembrolizumab did manage certain symptoms better than existing therapies including pain behind the breastbone or in the throat, black stool, and weight loss (1 patient); fatigue and vomiting (the other patient).
While 1 patient respondent did not mention any difficulties taking pembrolizumab, the other patient respondent indicated that social issues, lifestyle changes, and anxiety were difficult to manage while taking pembrolizumab. Both patient respondents rated their overall experience with pembrolizumab as a 6 on a scale of 1 to 10 (1 being much worse and 10 being much better) compared to other treatments.
Both patient respondents did not identify any particular gap or unmet patient need associated with current therapies that pembrolizumab could help address. However, both patients indicated that they believe pembrolizumab will change their long-term health and well-being for the better.
The following quotes illustrate the importance that patient and caregiver respondents place on having access to pembrolizumab and other future immunotherapies.
“Any treatment that helps someone with esophageal cancer is a chance.”
“Many people have had a very successful story with Keytruda.”
“I would like access to anything that would extend my life.”
“I was one of the lucky ones to survive so I know how important access to new treatments are to all patients.”
Improved Outcomes
The authors of the patient input highlighted that given the poor and short survival rate for most patients with esophageal cancer, it is necessary for patients to have access to new effective therapies that prolong OS, improve QoL, reduce disease symptoms, and have tolerable side effects. It was also noted by the authors that given the severity of disease symptoms, improved QoL is an important outcome to consider in this setting. Additionally, when asked to indicate trade-offs in respect to treatment outcomes in choosing a new therapy, almost all patient and caregiver respondents (92.0%) indicated that they were willing to take a drug that has been proven to improve QoL even if it would not prolong OS. Furthermore, on a scale of 1 to 10 (1 being no side effects and 10 being severe side effects), patients and caregivers rated on average 5 for the severity of side effects to extend survival by 2 months, 6 months, and 1 year. One caregiver and 1 patient respondent indicated that they were willing to tolerate significant side effects to extend survival by 2 months. However, 2 patient respondents indicated that they were not willing to tolerate any side effects to extend their survival by 1 year. When asked about how important it is for patients along with their physicians to have a choice in deciding which drug to take on a scale of 1 to 10 (1 being not important and 10 being very important), patient and caregiver respondents rated on average 8 for the level of importance.
Two patient respondents who had experience with pembrolizumab reported that they expected the following key outcomes to be improved by pembrolizumab, including prolonging OS, delaying the need of chemotherapy, and having a convenient route of administration.
The following quote illustrates the importance of QoL and the potential impact a new therapy (pembrolizumab) can have on improving QoL.
“A good quality of life is essential for esophageal patients. Even if overall survival is not dramatically improved, the quality of life improvement from this drug can bring significant advantages enabling them to spend more time with their families with the side effects of existing treatments.”
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 3 clinical specialists with expertise in the diagnosis and management of esophageal carcinoma and GEJ adenocarcinoma.
Current Treatment Options
The current standard treatment for locally advanced and unresectable or metastatic cancer of the esophagus and GEJ is systemic chemotherapy. Patients with advanced or metastatic EAC and GEJ are treated similarly to gastric adenocarcinoma.15-18 Rare types of esophageal cancer such as GI stromal tumour, leiomyosarcoma, and neuroendocrine tumours are treated differently than patients with adenocarcinoma and squamous cell histology, whom comprise the focus of this review.
Palliative radiation, endoscopic dilatation, or stenting can improve local symptoms of dysphagia or bleeding.15-18 Early interdisciplinary care with the addition of psychologists and dieticians has been shown to improve survival compared to standard oncology care.30 Many patients derive benefit from formal palliative care consultation.31
Systemic therapy improves survival compared to best supportive care for patients with advanced cancer of the esophagus and GEJ.32 With respect to systemic therapy, HER2 is evaluated for patients with EAC or GEJ and anti-HER2 therapy is included in their treatment if positive. Palliative chemotherapy is recommended for patients with good performance status. Standard first-line chemotherapy regimens include a fluoropyrimidine and a platinum (usually cisplatin or oxaliplatin)15-18 for patients with advanced ESCC and patients with HER2-negative EAC or GEJ. Examples of fluoropyrimidine- and platinum-based chemotherapy used in the first-line setting include cisplatin and 5-FU, capecitabine and cisplatin, CAPOX, and FOLFOX. Patients with advanced cancer of the EAC or GEJ may be treated with FOLFIRI19; however, this is not commonly used in the first-line setting. Other less common first-line treatments include paclitaxel or docetaxel doublet regimens, paclitaxel or docetaxel triplet regimens, and epirubicin.
With respect to second-line therapy, patients with advanced cancer of the EAC or GEJ may be treated with irinotecan or FOLFIRI. The combination of paclitaxel ramucirumab is also a therapeutic option for patients with cancer of the GEJ in the absence of contraindications to ramucirumab. Single agent docetaxel and paclitaxel can also be used for ESCC, EAC, or GEJ in the absence of significant neuropathy.15-18
Unmet Needs
The most important goals of treatment are to prolong life and improve HRQoL.
There is a need for more effective treatment options with manageable safety profile. Patients ultimately become refractory to current therapies and not all patients respond to available options. This patient population can be frail, and nutrition is often a challenge due to dysphagia; thus, treatments are needed that are better tolerated.
Place in Therapy
In the current treatment paradigm, pembrolizumab would be used in combination with a platinum- and a fluoropyrimidine-based chemotherapy for the first-line treatment of patients with locally advanced or unresectable cancer of the esophagus or HER2-negative adenocarcinoma of the GEJ (tumour epicentre 1 cm to 5 cm above the gastric cardia). Pembrolizumab added to chemotherapy is not currently a standard of care in Canada in this patient population. However, pembrolizumab added to chemotherapy has the potential to represent a standard of care for patients with esophageal cancer or GEJ Siewert type I. The clinical experts felt that pembrolizumab added to chemotherapy would certainly be a standard of care for patients with ESCC and for patients with a CPS of 10 or greater. The clinical experts also felt that pembrolizumab added to chemotherapy was an appropriate treatment option for patients with GEJ Siewert type I who are HER2 negative, EAC, and for tumours with a CPS of less than 10.
Patient Population
The clinical experts agreed that the full patient population in the indication should be eligible for treatment with pembrolizumab (i.e., esophageal cancer and HER2-negative GEJ Siewert type I). However, the clinical expert noted that some patients are more likely to respond to treatment with pembrolizumab than others. For instance, characteristics associated with increased survival benefit to the addition of pembrolizumab to cisplatin and 5-FU include ESCC histology and a CPS of 10 or greater.
The clinical experts noted that clinician judgment would be used to identify suitable patients and that access to PD-L1 CPS testing (though not required for eligibility and is not currently available), would also be useful in identifying patients who are most likely to benefit from the addition of pembrolizumab to systemic therapy.
Clinical experts identified patients with autoimmune diseases are at increased risk of autoimmune disease flares and immune-related AEs when treated with immunotherapy. However, the clinical experts agreed that for patients with well-controlled autoimmune diseases, immunotherapy may still represent an appropriate treatment option for these patients after a discussion of the risks and benefits between clinician and patient. As well, patients requiring prednisone 10 mg per day or higher may derive less benefit from pembrolizumab. Immunotherapy is generally not started until a patient’s steroid requirement is less than the equivalent of 10 mg of prednisone per day.
Nonetheless, the clinical experts reiterated that full patient population included in the indication should be eligible for treatment with pembrolizumab.
Assessing Response to Treatment
In clinical practice, imaging (CT scan) is used to assess response and is done every 3 months as standard of care. PROs (formal and informal report of symptoms) are used as an early indication of benefit and for monitoring toxicity.
According to the clinical experts, a clinically meaningful response to treatment would be improved OS and a reduction in the frequency or severity of symptoms (improved QoL). The clinical experts noted that the definition of a clinically meaningful response may vary across physicians. For patients treated with immunotherapy, a long-term plateau of the survival curve would also be considered a significant benefit since current median survival for this patient population is less than 12 months. If the addition of an agent to an established regimen did not cause a detriment to QoL, and improved survival, that would also be considered a clinically meaningful response to treatment.
Discontinuing Treatment
Treatment of pembrolizumab is discontinued in the presence of death, disease progression on CT, deterioration in clinical status precluding continuation of treatment, withdrawal of patient consent, severe AEs, or grade 3 or higher immune-related AEs.
Prescribing Conditions
The clinical experts noted that pembrolizumab is commonly used in other tumour sites; thus, all settings in which it is currently administered would be appropriate for administration. Patients should have access to the following specialists: medical oncology, hepatology, gastroenterology, endocrinology, respirology, nephrology, and dermatology. Access to rheumatology and ophthalmology would also be ideal.
The clinical experts highlighted that some patients will be treated at community cancer centres and have therapy given by nurse practitioners or general practitioners.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Two clinician group inputs were provided for the review of pembrolizumab for the first-line treatment of locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative GEJ adenocarcinoma in combination with platinum- and fluoropyrimidine-based chemotherapy, in adult patients. One joint clinician input was provided by 6 clinicians on behalf of the medical advisory board of My Gut Feeling, the Canadian GI Oncology Evidence Network and the medical advisory board of CCC. For ease of reference, this group of clinicians will be referred to throughout the input as “clinicians from the medical advisory boards.” Two of the clinicians from the medical advisory boards practice in British Columbia, 2 clinicians practice in Alberta, 1 clinician practices in Ontario, and 1 clinician practices in Nova Scotia The medical advisory board of CCC works with patient groups to ensure their activities and health information are relevant and valuable for patients and caregivers. The medical advisory board of My Gut Feeling works with patient organizations to advise on education and awareness initiatives and issues regarding access to treatment. The Canadian GI Oncology Evidence Network is a virtual and inclusive network of Canadian GI oncology clinicians who contribute to the knowledge of GI cancer and its treatments, including participating in clinical trials, conducting observational research, and assisting with local, provincial, and national clinical guideline developments and health technology assessments.
The second joint input was provided by 4 clinicians on behalf of the Ontario Health-Cancer Care Ontario GI Drug Advisory. Ontario Health-Cancer Care Ontario Drug Advisory Committees provide evidence-based clinical and health system guidance on drug-related issues including The provincial drug reimbursement programs and the systemic treatment program.
Current Treatments
The clinicians from the medical advisory boards explained that the goal of current treatments for patients with locally advanced unresectable or metastatic esophageal or GEJ cancers is to manage symptoms and prolong survival. Patients often have symptoms such as dysphagia, odynophagia, early satiety, nausea, and vomiting. These symptoms can limit their ability to maintain adequate nutritional intake. Additionally, the tumours can lead to both acute and chronic bleeding which can be life-threatening. The clinicians advised that these symptoms often need to be addressed before patients can start therapy. Systemic therapy can be considered for patients with an adequate ECOG PS, of which the most common is cytotoxic chemotherapy. The clinician group noted the following treatment sequence:
Platinum- and fluoropyrimidine-based doublet chemotherapy (with the addition of trastuzumab if the patient has HER-2 positive adenocarcinoma)
Taxane (with the addition of ramucirumab if primary tumour is GEJ adenocarcinoma)
Irinotecan-based therapy
Trifluridine or tipiracil (if the primary tumour is GEJ adenocarcinoma)
Additionally, the clinician group stated that local therapies such as radiation therapy or endoscopic stents are also often used to help mitigate some of the symptoms. Some patients are also treated with IV iron replacement to address iron deficiency. Although there is some phase III evidence that supports the use of immunotherapy checkpoint inhibitors in later lines of therapy, Canadian patients currently do not have access through funded indications or access programs. Patients with esophageal and gastroesophageal cancers have had access to immunotherapy through clinical trials, private insurance, or out-of-pocket expenses.
The clinicians from the Ontario Health-Cancer Care Ontario noted the following treatments options in each line of therapy:
First-line therapy: FOLFOX or FOLFIRI
Second-line therapy: paclitaxel with or without ramucirumab for GEJ adenocarcinoma; FOLFOX or single agent capecitabine or weekly Taxol or radiation for ESCC
Third-line therapy: trifluridine or tipiracil for GEJ adenocarcinoma
Unmet Needs
Clinicians from the Ontario Health-Cancer Care Ontario explained that the goals of treatments are to prolong patients’ survival, delay the progression of disease, maintain QoL, and ensure adequate nutritional intake. The clinician group also noted that currently many patients do not respond to all available systemic treatments. Their DOR is very short, and they often become refractory. Even among patients who demonstrate a response, survival is quite limited. Therefore, there exists a significant unmet need for therapies that not only improve QoL, but also significantly prolong survival.
Similarly, clinicians form the medical advisory boards stated that the aim of treatments is to maintain or improve patients’ QoL and prolong survival. The clinician group emphasized that the disease presents patients with a significant symptom burden that impairs their QoL. Patients often struggle with both local symptoms such as adequate nutrition, nausea and vomiting, pain, and blood loss, and constitutional symptoms such as weight loss, weakness, and fatigue. Without therapy, patients have poor survival, which is often less than 6 months. Although current systemic therapy can prolong survival compared to best supportive care, the average survival with systemic therapy is still very modest, (approximately 11 months) as patients often experience a rapid clinical deterioration at the time of progression. This can lead to significant attrition rates between lines of therapy and only a small number of patients end up receiving systemic therapy beyond first or second line. The clinician group emphasized the importance of having access to the best therapies earlier during the course of treatment to maximize survival, reduce symptom burden, and improve overall QoL. The clinicians asserted that pembrolizumab therapy addresses this unmet need. In the KEYNOTE-590 trial, the improvement in survival was statistically and clinically significant and was maintained throughout key time points with a 12% absolute improvement in OS rates at both 12 months and 24 months from randomization.
The clinician groups were asked to identify the patient populations that have the greatest unmet need for a therapy like pembrolizumab. Both clinician groups emphasized that all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would greatly benefit from this treatment. The clinicians from the medical advisory boards noted that in the KEYNOTE-590 trial, patients with PD-L1 with a CPS of 10 or greater received the greatest benefit with pembrolizumab and chemotherapy. The clinicians from the Ontario Health-Cancer Care Ontario did not specify any additional subgroups but noted that patients with adenocarcinoma that is HER-2 positive would be excluded from this treatment as these patients would receive trastuzumab along with platinum- and fluoropyrimidine-based doublet chemotherapy.
Place in Therapy
Both clinician groups stated that pembrolizumab would be added to treatments in the first-line setting. Clinicians from the medical advisory boards specified that it would be added to platinum- and fluoropyrimidine-based doublet chemotherapy. The clinician group further commented that there are many studies in other solid tumours that have demonstrated the benefit of adding checkpoint inhibitor immunotherapy to cytotoxic chemotherapy. Similarly, the KEYNOTE-590 trial demonstrated that compared to chemotherapy alone, adding pembrolizumab improved OS, PFS, and response rates without deteriorating QoL. Adding pembrolizumab as first-line therapy would have no impact on the treatment options used in subsequent lines of therapy.
Both clinician groups advised against recommending patients to try other treatments before initiating treatment with pembrolizumab. The clinicians from the Ontario Health-Cancer Care Ontario reiterated that pembrolizumab is an addition to first-line treatment to improve overall patient outcomes. The clinicians from the medical advisory boards further commented that there is no indication in Canada for immunotherapy checkpoint inhibitors in subsequent lines of therapy. Additionally, the rapid deterioration of patients at the time of progression makes patients ineligible for further therapy beyond first line, due to decreased performance status. Therefore, the clinicians emphasized that it is important to offer the therapies during the start of treatment.
Clinicians were asked to identify how the drug might affect the sequencing of therapies for esophageal cancer. The clinicians from the medical advisory boards stated that if patients remain well enough to consider further therapy beyond first line, the subsequent lines of therapy would apply as stated above. Both groups of clinicians explained that if pembrolizumab is used as first-line therapy, immunotherapy will not be used in subsequent lines of therapy. The clinicians from the medical advisory boards further commented that there are no opportunities to treat patients with pembrolizumab or any other immunotherapy checkpoint inhibitor in subsequent lines of therapy.
Patient Population
The clinicians from the medical advisory boards stated that all patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative GEJ adenocarcinoma would benefit from pembrolizumab and platinum- and fluoropyrimidine-based doublet chemotherapy, assuming they have no contraindications to immune checkpoint inhibition such as solid tumour transplant recipient, severe and active autoimmune disease.
Both clinician groups noted that although the greatest benefit in the KEYNOTE-590 trial was observed for patients with PD-L1 with a CPS of 10 or greater and an ECOG PS of 0 to 1, OS for the entire study population was clinically and statistically significant, regardless of their histology or PD-L1 CPS status. Clinicians from the medical advisory boards therefore concluded that no population subgroup should be excluded on the basis of either histology or PD-L1 subtype. Furthermore, the clinician group re-emphasized that all patients with locally advanced unresectable or metastatic esophageal carcinoma or HER2-negative GEJ adenocarcinoma have grim prognosis and therefore all should be eligible for the addition of pembrolizumab to first-line platinum and fluoropyrimidine chemotherapy.
Clinicians were asked to explain how eligible patients would be identified. The clinicians form the medical advisory boards stated that since there is currently no indication to treat based on PD-L1 status or histology, no additional testing is required beyond what is routinely done (i.e., histological confirmation of carcinoma, radiographic work-up to determine locally advanced unresectable or metastatic staging, and HER-2 results of gastro-EAC to ensure patients are not HER-2 positive). Similarity the clinicians from Ontario Health-Cancer Care Ontario noted that although the greatest benefit is observed in patients who have PD-L1 with a CPS of 10 or greater, there is currently no routine testing conducted for this, nor is any testing expected in the future.
Furthermore, the clinicians from the medical advisory boards commented that it is very unlikely that the disease will be undiagnosed. The symptoms of the disease for new patients are often quite extreme, which leads them to immediately seek medical attention and confirm a diagnosis. For patients that have been treated with curative intent, the majority of locally advanced or metastatic recurrences occur within the first 5 years after treatment, during which is it routine for the patients to be monitored for clinical and radiographic changes.
Clinicians were asked to identify which group of patients would be least suited for pembrolizumab. The clinicians form the medical advisory boards stated that patients with a poor performance status that cannot be improved with best supportive care (e.g., nutritional support, pain control or iron replacement) would not be suited for platinum- and fluoropyrimidine-based doublet chemotherapy. Additionally, patients who are ineligible for either platinum- and fluoropyrimidine-based doublet chemotherapy or immunotherapy checkpoint inhibitors due to comorbidities would not be suitable for treatment with pembrolizumab. Pembrolizumab is also not well suited for patients with contraindications to immunotherapy such as autoimmune diseases.
Clinicians were asked to advise if it is possible to identify those patients who are most likely to exhibit a response to treatment with the drug under review. Both groups of clinicians stated that patients with ESCC and a PD-L1 with a CPS of 10 or greater would be most likely to exhibit a response to pembrolizumab. However, clinicians from the medical advisory boards noted that when pembrolizumab was added to platinum- and fluoropyrimidine-based doublet chemotherapy in the full ITT population in KEYNOTE-590 trial, the outcomes were superior in all subgroups regardless of histology and PD-L1 status. Therefore, although histology and PD-L1 status are good biomarkers that can help predict a greater benefit, they should not be used to exclude eligible patients from receiving pembrolizumab.
Assessing Response to Treatment
Clinicians were asked to report which outcomes are used to determine whether a patient is responding to treatment in clinical practice. Clinicians from the medical advisory boards responded that clinical assessments are conducted by the clinicians every 3 to 4 weeks and as needed, if a change in clinical status is observed between the formal assessments. The clinical assessments consist of an assessment of the presence and severity of symptoms, as well as an overall assessment of health and functioning. A reduction or stabilization of symptoms and improved functioning are good indicators to determine patients’ response to therapy. Additionally, radiographic assessments are conducted every 8 to 12 weeks to objectively assess for response to treatment. The clinicians further noted that in the KEYNOTE-590 trial, key trial end points included PFS, response rates, and QoL. These assessments are also conducted in routine clinical practice. Similarly, the clinicians from Ontario Health-Cancer Care Ontario stated that an improvement in symptoms and objective response on radiographic imaging are good indicators to determine patient response to treatment.
Both clinician groups responded that a clinically meaningful response to treatments would be a reduction in symptoms or at minimum, a stabilization of symptoms (e.g., less pain, weight gain or cessation of weight loss, and less fatigue). Additionally, an overall improvement in the ability to perform daily activities and a reduction in the caregiver burden would also be considered clinically meaningful responses to treatment.
Clinicians were asked to advise on how often the response to treatment should be assessed. Both groups of clinicians responded that radiographic imaging would occur every 2 to 3 months. The clinicians from the medical advisory board further noted that clinical assessments would be done every 3 to 4 weeks.
Discontinuing Treatment
Both groups of clinicians stated that treatment with pembrolizumab should be discontinued if there is evidence of disease progression or if the patient develops AEs and/or toxicities that cannot be treated with best supportive care. Additionally, the clinicians from the medical advisory board stated that treatment may also be discontinued if the patient no longer wishes to continue with the treatment.
Prescribing Conditions
Both clinician groups advised that the treatment would be administered on an outpatient basis. The clinicians from the medical advisory boards further stated that treatment would mostly likely be in a specialized cancer hospital that has expertise in chemotherapy and immunotherapy. This is standard practice in most regions in Canada.
Additional Considerations
Both clinician groups provided some additional comments for consideration. Reflecting on the results of the KEYNOTE-590 trial, the clinicians form the medical advisory groups concluded that they highly support the reimbursement of pembrolizumab. The clinicians emphasized that the results of the KEYNOTE-590 trial are very notable, as OS was quite significant and was maintained at key time points. Almost 38% of patients in the ITT population were alive at 24 months, which the clinicians commented is quite remarkable for this type of cancer. Additionally, all patients, regardless of PD-L1 status, benefited from the addition of pembrolizumab, and the control arms were representative of the current standard of care in Canada. Toxicity did not increase significantly by adding pembrolizumab and QoL was comparable among the treatment arms.
The clinicians from Ontario Health-Cancer Care Ontario advised that peer review publication and final analyses are still needed, and the publication should be based on the planned duration of the study. The clinicians asserted that PD-L1 CPS testing should be made available to identify which patient subgroup will experience the greatest benefits from pembrolizumab. Additionally, the clinicians advised that further speculation and discussions are needed to determine if FOLFOX or FOLFIRI would be an approximate chemotherapy substitute for pembrolizumab. Consideration should be given to patients treated by adjuvant nivolumab and in their subsequent lines of therapy in the metastatic setting.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. Their implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Can trial results be generalized to other first-line chemotherapy combinations if a patient is not able to tolerate or receive a platinum-based combination? | Pembrolizumab maybe added to other first-line chemotherapy combinations if a patient is not able tolerate or receive a platinum-based combination as long as the patient would otherwise be eligible for treatment with pembrolizumab. CAPOX and FOLFOX should be interchangeable chemotherapy backbones with cisplatin plus 5-FU. If not eligible for cisplatin, carboplatin would be a reasonable substitute, and this is consistent with standard practice in multiple cancer sites. If patients cannot tolerate the chemotherapy combination, and do not have any grade 3 or higher immune-related adverse events, it would be reasonable to continue with pembrolizumab monotherapy. At least 1 cycle of chemotherapy should be given concurrently with pembrolizumab. |
If treatment is discontinued before evidence of progressive disease, can pembrolizumab be administered at time of relapse? | It would be reasonable to re-administer pembrolizumab at the time of relapse, with or without chemotherapy at the discretion of the treating physician, in following instances: treatment is discontinued before disease progression or disease progression occurs during a treatment break. |
If re-treatment is permitted at time of relapse, would therapy consist of pembrolizumab monotherapy or pembrolizumab plus chemotherapy? | It would be reasonable to re-administer pembrolizumab at the time of relapse, with or without chemotherapy at the discretion of the treating physician, in the following instances: treatment is discontinued before disease progression or disease progression occurs during a treatment break. |
Would patients with CNS metastases be eligible for pembrolizumab plus chemotherapy? | Patients with CNS metastases were not included in KEYNOTE-590; thus, the magnitude of benefit for combination therapy with pembrolizumab is unclear. However, metastatic lung cancer patients with controlled CNS metastases are often treated with the combination of immunotherapy and chemotherapy. By extrapolation, it may be reasonable to treat patients with metastatic esophageal or gastroesophageal junction cancer with controlled CNS metastases who otherwise meet the inclusion criteria for KEYNOTE-590 with pembrolizumab plus chemotherapy, if they did not require steroids (equivalent of prednisone 10 mg/day or higher). |
What is the recommended definition or parameters to use in determining when to stop pembrolizumab therapy? | Treatment is discontinued in the presence of death, disease progression on CT, deterioration in clinical status precluding continuation of treatment, withdrawal of patient consent, severe adverse events, or grade 3 or higher immune-related adverse events. |
If there is disease progression during a treatment break, can pembrolizumab therapy be resumed? | It would be reasonable to re-administer pembrolizumab at the time of relapse, with or without chemotherapy, at the discretion of the treating physician, in following instances: treatment is discontinued before disease progression or disease progression occurs during a treatment break. |
If a patient cannot tolerate the chemotherapy combination, are they able to continue with pembrolizumab monotherapy? Is there a minimum number of chemotherapy cycles that must be given concurrently with pembrolizumab? | If patients cannot tolerate the chemotherapy combination, and do not have any grade 3 or higher immune-related adverse events, it would be reasonable to continue with pembrolizumab monotherapy. At least 1 cycle of chemotherapy should be given concurrently with pembrolizumab. |
Should patients with ECOG Performance Status of 2 or greater be eligible? | Patients with ECOG Performance Status of 2 or greater were not eligible for inclusion in KEYNOTE-590. Though 2 patients with an ECOG Performance Status of 2 appear to have been included in the trial, almost all patients were ECOG Performance Status 0 or 1 (747 out of 749); therefore, the magnitude of benefit in this population is uncertain. |
There is a time-limited need to allow patients currently on platinum plus fluoropyrimidine-based chemotherapy, or alternate chemotherapy, to add pembrolizumab. What time frame is appropriate to add pembrolizumab for patients on chemotherapy alone or who recently completed chemotherapy? | It would be reasonable to permit the addition of pembrolizumab as a time-limited option for patients who have not progressed on first-line therapy. Applicable first-line chemotherapy regimens would include first-line platinum plus fluoropyrimidine, or alternate doublet chemotherapy (e.g., FOLFOX,CAPOX, or FOLFIRI) and patients who had completed treatment without progression would also be suitable. There is no time frame specified as long as there is lack of progression. Patients should otherwise meet the inclusion criteria for the KEYNOTE-590. The population of patients who would fall into this category will be quite small. As these patients would be started later in therapy, consideration could be made to limit this to patients with tumours that have a PD-L1 CPS ≥ 10. |
Is companion diagnostic testing (PD-L1) not required to determine eligibility? | Although it is not required for eligibility, access to PD-L1 CPS testing would be ideal and should be performed when a patient presents with metastatic or advanced disease. PD-L1 testing results provide meaningful information for the clinician to discuss the anticipated benefits of treatment with patients and families. |
5-FU = 5-fluorouracil; CAPOX = capecitabine and oxaliplatin; CNS = central nervous system; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; FOLFIRI = irinotecan, 5-fluorouracil, and oxaliplatin; FOLFOX = 5-fluorouracil, oxaliplatin, and leucovorin; PD-L1 = programmed cell death ligand 1.
As well, the Patient Advisory Group noted that uptake of pembrolizumab in this setting versus existing systemic therapies is likely to be immediate leading to a considerable increase in budget impact in a reimbursement scenario and also noted that reimbursement of pembrolizumab in the first-line setting would likely shift other systemic therapies to later lines of therapy, representing an added cost. However, the clinical experts expressed that it would not cause a shift in the current treatment paradigm as pembrolizumab is not standard of care in Canada. Similarly, the clinician group highlighted that adding pembrolizumab as a first-line therapy would have no impact on the treatment options used in subsequent lines of therapy.
Clinical Evidence Selection
The clinical evidence included in the review of pembrolizumab is presented in 3 sections. The first section, the systematic review, includes the pivotal study provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section refers to a summary and appraisal of the feasibility assessment for indirect evidence from the sponsor found in Appendix 5. The third section includes sponsor-submitted additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review: Pivotal and Protocol Selected Studies
Objective
To perform a systematic review of the beneficial and harmful effects of pembrolizumab (200 mg every 3 weeks or 400 mg every 6 weeks) in combination with platinum- and fluoropyrimidine-based chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia).
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5: Inclusion Criteria for the Systematic Review. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the esophagogastric junction (tumour centre 1 cm to 5 cm above the gastric cardia) in the first-line setting. Subgroups:
|
Intervention | Pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapya administered as an IV infusion over 30 minutes. The recommended dose of pembrolizumab in adults is either:
|
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
AE = adverse event; ECOG = Eastern Cooperative Oncology Group; FOLFIRI = irinotecan, 5-fluorouracil, and oxaliplatin; FOLFOX = 5-fluorouracil, oxaliplatin, and leucovorin; HER2 = human epidermal growth factor receptor 2; PD-L1 = programmed cell death ligand 1.
aExamples of platinum- and fluoropyrimidine-based chemotherapy may include: cisplatin plus 5-fluorouracil, capecitabine plus cisplatin, capecitabine plus oxaliplatin, and FOLFOX.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.33
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pembrolizumab and esophageal or GEJ cancer. Clinical trials registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on June 18, 2021. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on October 10, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.34 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers will independently make the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 296 studies were identified from the literature for inclusion in the systematic review (Figure 1: Flow Diagram for Inclusion and Exclusion of Studies). The included study (KEYNOTE-590) is summarized in Table 6. A list of excluded studies and reason for exclusion is presented in Appendix 2.
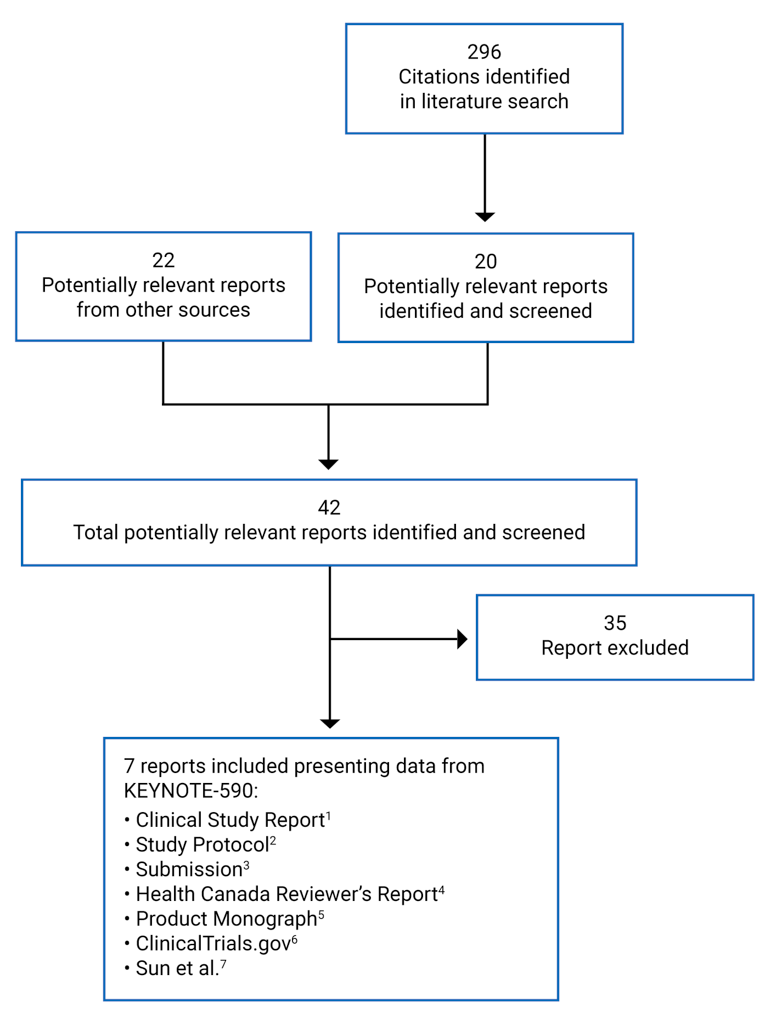
Table 6: Details of KEYNOTE-590 Study
Criteria | KEYNOTE-590 |
|---|---|
Design and population | |
Study design | Phase III, multi-centre, double-blind, placebo-controlled |
Locations | 168 sites in 26 countries across the Americas including Canada and US, Asia, Europe, Africa, and Australia |
Patient enrolment dates | July 25, 2017 to July 2, 2020 2 enrolment periods: Global Cohort and China Extension (Global Cohort and China Extension were merged for the primary analysis); combined as the Global Study Population |
Randomized (N) | Planned: 700 Actual: 749 (373 in pembrolizumab plus chemotherapy; 376 in placebo plus chemotherapy) |
Inclusion criteria | At least 18 years of age Histologically or cytologically confirmed locally advanced unresectable or metastatic adenocarcinoma or squamous cell carcinoma of the esophagus or advanced or metastatic Siewert type I adenocarcinoma of the esophagogastric junction Measurable disease per RECIST 1.1 as determined by the local site investigator or radiology assessment ECOG Performance Status of 0 or 1 Tissue sample for PD-L1 by immunohistochemistry analysis (either newly obtained or archival) |
Exclusion criteria | Resectable or potentially curable (with radiation therapy) locally advanced esophageal carcinoma as determined by local investigator Received previous therapy for advanced or metastatic adenocarcinoma or squamous cell cancer of the esophagus or advanced or metastatic Siewert type I adenocarcinoma of the esophagogastric junction Known additional malignancy that was progressing or required active treatment Immunodeficient or received chronic systemic steroid therapy or any other form of immunosuppressive therapy within 7 days before first dose of trial treatment History of organ transplant (including allogeneic stem cell transplant) Non-infectious pneumonitis that required steroids or current pneumonitis Received prior therapy with an anti-PD-1, anti-PD-L1, or anti-PD-L2 agent or with an agent directed to another co-inhibitory T-cell receptor Previously participated in a pembrolizumab clinical trial |
Drugs | |
Intervention | Pembrolizumab: 200 mg every 3 weeks administered intravenously Cisplatin: 80 mg/m2 every 3 weeks administered intravenously; maximum of 6 doses 5-FU: 800 mg/m2/day for 5 days (4,000 mg/m2 total per cycle) every 3 weeks administered intravenously |
Comparator(s) | Placebo: normal saline, every 3 weeks administered intravenously Cisplatin: 80mg/m2 every 3 weeks administered intravenously, maximum 6 doses 5-FU: 800 mg/m2/day for 5 days (4,000 mg/m2 total per cycle) every 3 weeks administered intravenously |
Phase | |
Run-in | Within 28 days before treatment randomization, potential patients were evaluated to determine if they fulfilled study entry requirements. Screening procedures were completed within 28 days before first dose of treatment, except for: laboratory tests performed within 14 days before first dose of treatment, evaluation of ECOG performed within 14 days before treatment, pregnancy test within 72 hours before randomization for women of reproductive potential, and initial tumour imaging within 21 days before randomization. |
Blinding | Pembrolizumab and placebo are blinded to the patient, study site personnel, as well as the sponsor personnel. The patient and investigator included in the treatment or clinical evaluation are not aware of the group assignments. |
Follow-up | Defined as time of randomization to the date of death or database cut-off date if patient remain alive |
Outcomes | |
Co-primary end points | Overall survival (in patients whose tumours are PD-L1 biomarker-positive [CPS ≥ 10], with ESCC, ESCC and CPS ≥ 10, and all patients) Progression-free survival (based on RECIST 1.1 as assessed by investigator in patients with ESCC, CPS ≥ 10, and all patients) |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | The results for both PFS and overall survival are final based on interim analysis since all end points were met; however, the study is ongoing. The study and results are based on a Global Study Population, whereby the 2 enrolment periods for the Global Cohort and China Extension Study were merged for the primary analyses. Crossover to pembrolizumab was not permitted. The data cut-off date was July 2, 2020 after a minimum of 13 months follow-up. |
Publications | Sun et al. (2021)7 |
5-FU = 5-fluorouracil; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; EQ-5D 5L = EQ-5D 5-Levels; ESCC = esophageal squamous cell carcinoma; irRECIST = immune-related Response Evaluation Criteria in Solid Tumors; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1; PD-L2 = programmed cell death ligand 2; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: Clinical Study Report.1
Description of Study (KEYNOTE-590)
The KEYNOTE-590 study is an ongoing, phase III, randomized, double-blind, placebo-controlled, multi-centre, superiority study comparing pembrolizumab in combination with cisplatin and 5-FU to placebo in combination with cisplatin and 5-FU for the first-line treatment of patients with locally advanced unresectable or metastatic EAC or ESCC or advanced or metastatic Siewert type I adenocarcinoma of the EGJ. The trial was conducted in 168 sites in the Americas including Canada and the US, Asia, Europe, Africa, and Australia. Trial characteristics are summarized in Table 6.
The co-primary objectives were to evaluate if pembrolizumab in combination with cisplatin and 5-FU, compared to placebo in combination with cisplatin and 5-FU, would improve:
OS among patients with ESCC whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), patients with ESCC, patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), and all patients, and
PFS per RECIST 1.1 among patients with ESCC, patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), and all patients.
A key secondary objective was to evaluate if pembrolizumab in combination with cisplatin and 5-FU, compared to placebo in combination with cisplatin and 5-FU, would improve ORR in all randomized participants. Other evaluated secondary outcomes included:
ORR among patients with ESCC whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), patients with ESCC, patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10)
DOR: patients with ESCC whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), patients with ESCC, patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), and all patients
Safety and tolerability profile
HRQoL using EORTC QLQ-C30 and EORTC QLQ-OES18 in all patients, patients with ESCC whose tumours have a CPS of 10 or greater, patients with ESCC, and patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10)
Exploratory objectives included:
Characterizing PRO utilities using the EQ-5D-5L questionnaire in all patients, patients with ESCC whose tumours have a CPS of 10 or greater, patients with ESCC, and patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10)
Evaluating PFS per immune-related RECIST in all patients, patients whose tumours are PD-L1 biomarker-positive (CPS ≥ 10), patients with ESCC, and patients with ESCC whose tumours have a CPS of 10 or greater
Studying biomarkers predictive of clinical response and resistance, safety, pharmacodynamic activity, and/or the mechanism of action of pembrolizumab and other treatments
A total of 1,020 patients were screened, and 749 patients were randomized in a 1:1 ratio to receive pembrolizumab in combination with cisplatin and 5-FU (n = 373 patients) or placebo in combination with cisplatin and 5-FU (n = 376 patients). Randomization occurred centrally using an interactive voice response/system/integrated web response system. Randomization was stratified for geographic region (Asia, rest of the world), histology (adenocarcinoma, ESCC), and ECOG PS (0, 1). The first patient was randomized on July 25, 2017, and the last patient on July 2, 2020.
This is an ongoing study with interim results using a Global Study Population, whereby the 2 enrolment periods (Global Cohort and China Extension Study) were merged. These interim results represent the final analysis, with a data cut-off date of July 2, 2020.
Populations (KEYNOTE-590)
Inclusion and Exclusion Criteria
Eligible patients had to be at least 18 years of age with histologically or cytologically confirmed locally advanced unresectable or metastatic adenocarcinoma or ESCC or advanced or metastatic Siewert type I adenocarcinoma of the GEJ. Patients had to have an ECOG PS of 0 or 1.
Patients were ineligible if they received previous therapy for advanced or metastatic adenocarcinoma or squamous cell cancer of the esophagus or advanced or metastatic Siewert type I adenocarcinoma of the EGJ, had active central nervous system metastases and/or carcinomatous meningitis, or active infection or autoimmune disease that required systemic therapy in the past 2 years. Inclusion and exclusion criteria are further described in Table 6.
Baseline Characteristics
The demographic and baseline characteristics were well-balanced between groups, except for age (65 years or older) and stage IVB disease. There were more patients 65 years or older in the pembrolizumab in combination with cisplatin and 5-FU group (46.1%) compared with the placebo in combination with cisplatin and 5-FU group (39.9%). There were more patients with a current disease stage of iv B (distant lymph nodes and/or other organs) in the pembrolizumab in combination with cisplatin and 5-FU group (17.4%) compared with the placebo in combination with cisplatin and 5-FU group (10.9%; data not reported in Table 7). The majority (99.7%) had an ECOG PS of 0 or 1 (39.9% and 59.8%, respectively) and had metastatic disease (91.2%). Most patients were male (83.4%), had an ESCC primary diagnosis (73.2%), and about half were Asian (53.4%), enrolled in Asia (52.5%), and had tumour expressed PD-L1 with a CPS of 10 or greater (51.1%).1 Refer to Table 7: Summary of Baseline Characteristics, ITT Population.
Most patients had been treated with 1 or more prior medications (94.9% in the pembrolizumab in combination with cisplatin and 5-FU group and 94.1% in the placebo in combination with cisplatin and 5-FU group); the types of prior medication were balanced between the 2 treatment groups. Refer to Table 21 for more details.
With regards to concomitant medication, a greater proportion of patients in the pembrolizumab in combination with cisplatin and 5-FU group compared with patients in the placebo in combination with cisplatin and 5-FU group had taken the following concomitant medications: drugs for constipation (55.9% versus 49.2%), antithrombotic agents (31.4% versus 25.9%), corticosteroids in dermatological preparations (17.8% versus 11.6%), anesthetics (24.3% versus 18.1%), and psychoanaleptics (15.1% versus 9.5%). Refer to Table 22 for more details on types of concomitant medication.
Table 7: Summary of Baseline Characteristics — ITT Population
Characteristic | KEYNOTE-590 | ||
|---|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU N = 373 | Placebo in combination with cisplatin and 5-FU N = 376 | Total N = 749 | |
Age, years | |||
Mean (SD) | 62.8 (9.8) | 62.0 (9.2) | 62.4 (9.5) |
Median (min, max) | 64.0 (28, 94) | 62.0 (27, 89) | 63.0 (27, 94) |
Age category | |||
< 65 years | 201 (53.9) | 226 (60.1) | 427 (57.0) |
≥ 65 years | 172 (46.1) | 150 (39.9) | 322 (43.0) |
Sex | |||
Male | 306 (82.0) | 319 (84.8) | 625 (83.4) |
Female | 67 (18.0) | 57 (15.2) | 124 (16.6) |
Race | |||
Asian | 201 (53.9) | 199 (52.9) | 400 (53.4) |
White | 139 (37.3) | 139 (37.0) | 278 (37.1) |
American Indian or Alaska Native | 9 (2.4) | 12 (3.2) | 21 (2.8) |
Multiple | 5 (1.3) | 9 (2.4) | 14 (1.9) |
American Indian or Alaska Native, White | 3 (0.8) | 6 (1.6) | 9 (1.2) |
Black or African American, White | 2 (0.5) | 3 (0.8) | 5 (0.7) |
Black or African American | 5 (1.3) | 2 (0.5) | 7 (0.9) |
Missing | 14 (3.8) | 15 (4.0) | 29 (3.9) |
Region | |||
Asia | 196 (52.5) | 197 (52.4) | 393 (52.5) |
Rest of world | 177 (47.5) | 179 (47.6) | 356 (47.5) |
Primary diagnosis | |||
Squamous cell carcinoma of the esophagus | 274 (73.5) | 274 (72.9) | 548 (73.2) |
Adenocarcinoma of the esophagus | 58 (15.5) | 52 (13.8) | 110 (14.7) |
Adenocarcinoma of the gastroesophageal junction, Siewert type I | 41 (11.0) | 50 (13.3) | 91 (12.1) |
Brain metastasis | |||
Yes | 1 (0.3) | 2 (0.5) | 3 (0.4) |
No | 372 (99. 7) | 374 (99.5) | 746 (99.6) |
ECOG Performance Status | |||
0 | 149 (39.9) | 150 (39.9) | 299 (39.9) |
1 | 223 (59.8) | 225 (59.8) | 448 (59.8) |
2 | 1 (0.3) | 1 (0.3) | 2 (0.3) |
Histology | |||
Adenocarcinoma | 99 (26.5) | 102 (27.1) | 201 (26.8) |
Squamous cell carcinoma | 274 (73.5) | 274 (72.9) | 548 (73.2) |
Disease status | |||
Metastatic | 344 (92.2) | 339 (90.2) | 683 (91.2) |
Unresectable, locally advanced | 29 (7.8) | 37 (9.8) | 66 (8.8) |
PD-L1 status | |||
CPS ≥ 10 | 186 (49.9) | 197 (52.4) | 383 (51.1) |
CPS < 10 | 175 (46.9) | 172 (45.7) | 347 (46.3) |
Not evaluable | 6 (1.6) | 6 (1.6) | 12 (1.6) |
Missing | 6 (1.6) | 1 (0.3) | 7 (0.9) |
HER2 statusa | N = 41 | N = 50 | N = 91 |
Positive | 0 (0.0) | 1 (2.0) | 1 (1.1) |
Negative | 34 (82.9) | 40 (80.0) | 74 (81.3) |
Missing | 7 (17.1) | 9 (18.0) | 16 (17.6) |
5-FU = 5-fluorouracil; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; HER2 = human epidermal growth factor receptor 2; NA = not applicable; PD-L1 = programmed cell death ligand 1; SD = standard deviation.
Note: Values are n (%) unless otherwise indicated.
Note: The data cut-off date was July 2, 2020.
aHER2 status testing (fluorescence in situ hybridization testing or immunohistochemical testing) was planned for participants with Siewert type I adenocarcinoma of the gastroesophageal junction. One patient had a positive HER2 status, but this patient is not treated with study medication.
Source: Clinical Study Report, Keytruda submission.1
Interventions (KEYNOTE-590)
Pembrolizumab in combination with cisplatin and 5-FU group was dosed at 200 mg intravenously, every 3 weeks on day 1 of each cycle to a maximum of 35 administrations (2 years). Along with pembrolizumab, patients in the pembrolizumab in combination with cisplatin and 5-FU group generally received cisplatin at a dose of 80 mg/m2 intravenously every 3 weeks on day 1 of each cycle for a maximum of 6 doses and 5-FU at a dose of 800 mg/m2 per day for 5 days every 3 weeks on day 1 to day 5 of each cycle. Although administration of cisplatin and/or 5-FU could begin 1 to 2 days following pembrolizumab or placebo, and administration of 5-FU could vary (as per local standard for 5-FU administration duration) provided that the total dose was 4,000 mg/m2 per cycle (e.g., 1,000 mg/m2 per day on each of days 1 to 4 was permitted).
Normal saline in the placebo in combination with cisplatin and 5-FU group was given every 3 weeks on day 1 of each cycle. Along with placebo, patients in the placebo in combination with cisplatin and 5-FU group generally received cisplatin at a dose of 80 mg/m2 intravenously every 3 weeks on day 1 of each cycle for a maximum of 6 doses and 5-FU at a dose of 800 mg/m2 per day for 5 days every 3 weeks on day 1 to day 5 of each cycle. Administration of cisplatin and/or 5-FU could begin 1 to 2 days following pembrolizumab or placebo, and administration of 5-FU could vary (as per local standard for 5-FU administration duration) provided that the total dose was 4,000 mg/m2 per cycle (e.g., 1,000 mg/m2 per day on each of days 1 to 4 was permitted).
Treatment was continued until confirmed progressive disease, unacceptable toxicity, intercurrent illness that prevented further administration of treatment, investigator’s decision to withdraw patient, patient withdrawal of consent, pregnancy of patient, noncompliance with trial treatment or procedure requirements, completion of 35 administrations (approximately 2 years) of treatment with study medication or achievement of a complete response, or administrative reasons. Crossover from placebo to pembrolizumab was not permitted.
Pembrolizumab or placebo dose reduction were not permitted, rather treatment could be interrupted or discontinued due to toxicity.
Outcomes (KEYNOTE-590)
Co-primary outcomes were OS (in patients with ESCC whose tumours are PD-L1 CPS ≥ 10, in patients with ESCC, in patients whose tumours are PD-L1 CPS ≥ 10, and all patients) and PFS (in patients with ESCC, in patients whose tumours are PD-L1 biomarker-positive [CPS ≥ 10] and all patients). Secondary outcomes included: ORR, DOR, EORTC QLQ-C30, EORTC QLQ-OES18, and safety. PFS, ORR, and DOR are based on RECIST 1.1 and assessed by the investigator. EQ-5D-5L was an exploratory outcome. Refer to Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol for more details. A description and critical appraisal of PROs can be found in Appendix 4.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | KEYNOTE-590 | Definition |
|---|---|---|
Efficacy | ||
Overall survival | Co-primary | Time from randomization to death of any cause in: the ESCC PD-L1 CPS ≥ 10; ESCC; PD-L1 CPS ≥ 10; and all randomized patient populations |
Progression-free survival | Co-primary | Time from randomization to first disease progression (per RECIST 1.1 by investigator assessment) or death of any cause in ESCC, PD-L1 CPS ≥ 10, and all randomized patient populations). |
EORTC QLQ-C30 | Additional secondary | Includes 30 questions, consisting of a global health status/QoL scale, a financial difficulty scale, 5 functional scales (cognitive, social, physical, emotional, and role functioning), and 8 symptom scales (fatigue, insomnia, appetite, loss, pain, constipation, diarrhea, dyspnea, and nausea and vomiting); sponsor defined a 10-point change from baseline as improvement or deterioration |
ED-5D-5L (descriptive system and VAS) | Exploratory | Consists of 2 parts: descriptive system and VAS; descriptive system includes 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety or depression and VAS is a scale ranging from 100 (best imaginable health) to 0 (worst imaginable health); no minimal important difference was provided in the sponsor’s submission |
Objective response rate | Key secondary | Proportion of patients with complete or partial response in the total population (per RECIST 1.1 by investigator assessment) |
Duration of response | Additional secondary | Time from first complete or partial response until first disease progression (RECIST 1.1 by investigator) or death by any cause. |
EORTC QLQ-OES18 | Additional secondary | Consists of 18 items with symptoms of dysphagia, pain, reflux, eating, difficulty with swallowing saliva, choking, dry mouth, taste, cough, and speech; sponsor defined a 10-point change from baseline as improvement or deterioration |
CPS = combined positive score; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; ED-5D-5L = EQ-5D 5-Levels; ESCC = esophageal squamous cell carcinoma; PD-L1 = programmed cell death ligand 1; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumors; VAS = visual analogue scale.
Source: Clinical Study Report, Keytruda submission.1
Statistical Analysis (KEYNOTE-590)
In the final protocol, there was 1 efficacy interim analysis in addition to the final analysis planned. The purpose of the interim analysis was to perform the main efficacy analysis for PFS and the interim analysis of OS, while the purpose of the final analysis was to perform the main efficacy analysis for OS. Refer to Table 23 for more details.
Interim data were reviewed by an independent data monitoring committee which could make recommendations for the ongoing conduct of the trial. It was noted that the independent data monitoring committee confirmed that the KEYNOTE-590 study met the specified efficacy and safety end points after the review of the interim analysis results performed by an unmasked independent statistician.7 As a result, the interim results in this report represent the final analysis, with a data cut-off date of July 2, 2020.
Important protocol deviations were similar between the 2 groups (7.8% in the pembrolizumab in combination with cisplatin and 5-FU group and 8.2% in placebo in combination with cisplatin and 5-FU group). The majority of important protocol deviations were related to safety reporting (reportable events and/or follow-up safety event information not reported as per timelines outlines in the protocol). None of the important protocol deviations were considered clinically important.
Protocol deviations associated with COVID-19 were reported in 4.0% of patients in the pembrolizumab in combination with cisplatin and 5-FU group and 1.9% in placebo in combination with cisplatin and 5-FU group. The majority of protocol deviations associated with COVID-19 were related to trial procedure and deemed not important. None of the protocol deviations associated with COVID-19 were considered clinically important.
All amendments to the statistical analysis plan occurred before the data lock for the planned interim analysis (July 30, 2020). Of note, changes to the primary end points were made based on results from the KEYNOTE-181 study, an open-label, phase III randomized controlled trial of patients with advanced or metastatic ESCC or adenocarcinoma of the esophagus that progressed after 1 prior therapy35 (e.g., the addition of OS in ESCC; OS in ESCC whose tumours are PD-L1 with a CPS or 10 or greater, and PFS in ESCC). As well, based on input from the US regulatory agency, PFS analysis was changed from blinded independent central review (BICR) to investigator-assessed due to the higher expected discordance rate in the assessment of disease response between investigator and BICR.
Non-parametric Kaplan–Meier method was used to estimate OS, PFS, DOR, and time to deterioration (for PROs: EORTC QLQ-C30, QLQ-OES18, and EQ-5D-5L). A stratified log-rank test was used to assess the difference in OS, PFS, and time to deterioration between the 2 groups. The stratified Miettman and Nurminen method was used to assess the difference in response rate, overall improvement, and overall improvement or stability (for PROs: EORTC QLQ-C30, QLQ-OES18, and EQ-5D-5L). Refer to Table 24 for details on statistical model, adjustment factors, censoring, and sensitivity or exploratory analysis.
If at least 1 of the hypotheses regarding superiority of pembrolizumab in combination with cisplatin and 5-FU compared with placebo in combination with cisplatin and 5-FU was significant, then the KEYNOTE-590 study was considered to have met its primary objective. Overall type I error was controlled at 2.5% (1-sided): 1.2% initially allocated to OS in patients with ESCC and PD-L1 with a CPS of 10 or greater, 1.1% to OS in patients with ESCC, 0 to OS in patients with PD-L1 with a CPS of 10 or greater, 0 to OS in all patients, 0.2% to PFS in patients with ESCC, 0 to PFS in patients with PD-L1 with a CPS of 10 or greater, and 0 to PFS in all patients. Figure 2 illustrates the reallocation of type I error and describes each hypothesis.
Figure 2: Multiplicity Diagram for Type I Error Control
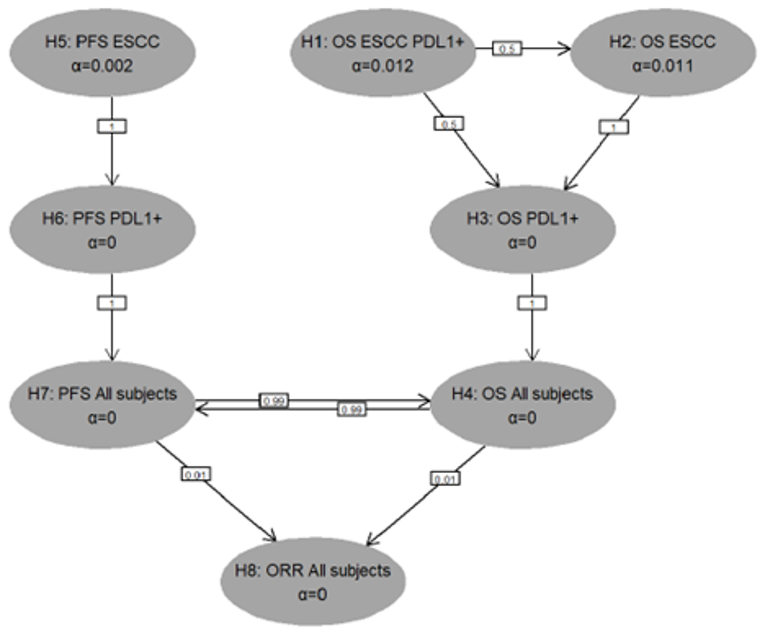
Source: Clinical Study Report, Keytruda submission.1
The sample size and PFS and OS power calculations were based on the following assumptions: PFS follows an exponential distribution with a median of 6 months in the placebo in combination with cisplatin and 5-FU group; OS follows an exponential distribution with a median of 12 months in the placebo in combination with cisplatin and 5-FU group; an enrolment period of 28 months; and a 5% annual dropout rate for PFS and OS.
For PFS with a targeted number of 460 investigator-assessed events in ESCC at the interim analysis (final for PFS), the study had 82.8% power to detect an HR of 0.7 at an overall alpha level of 0.002 (1-sided). If the PFS hypothesis was rejected in ESCC, the PFS test has 62.2% power to detect an HR of 0.7 at an alpha level of 0.002 in patients with PD-L1 with a CPS of 10 or greater. If both PFS hypotheses in ESCC and in PD-L1 with a CPS of 10 or greater are rejected, the PFS test has 76.8% power to detect an HR of 0.75 at an alpha level of 0.002 in all patients. If the PFS null hypotheses in all populations and all OS null hypotheses are rejected, the PFS test has 95.1% power to detect an HR of 0.75 at an alpha level of 0.025 in all patients.
For OS with a targeted number of 233 events and 1 interim analysis at 86% of target number of events, the study has 84.5% power at final analysis to detect an HR of 0.65 at an overall alpha level of 0.012 (1-sided) in ESCC patients with PD-L1 with a CPS of 10 or greater, and based on a target number of 455 events, the study has 88.3% power at final analysis to detect an HR of 0.72 at an overall alpha level of 0.011 (1-sided) in ESCC patients. If the OS hypothesis is rejected in ESCC with PD-L1 with a CPS of 10 or greater and is not, however, rejected in ESCC, the OS test has 89.5% power at final analysis to detect an HR of 0.65 at an overall alpha level of 0.006 (1-sided) in PD-L1 with a CPS of 10 or greater. If the OS hypothesis is rejected in ESCC and is not, however, rejected in ESCC with PD-L1 with a CPS of 10 or greater, the OS test has 92.9% power at final analysis to detect an HR of 0.65 at an overall alpha level of 0.011 (1-sided) in PD-L1 with a CPS of 10 or greater. If the OS hypotheses in ESCC with PD-L1 with a CPS of 10 or greater and in ESCC are both rejected, the OS test has 96.0% power at final analysis to detect an HR of 0.65 at an overall alpha level of 0.023 (1-sided) in PD-L1 with a CPS of 10 or greater. If OS hypotheses in ESCC with PD-L1 with a CPS of 10 or greater, in ESCC, and in PD-L1 with a CPS of 10 or greater are all rejected, the OS test has 94.1% power at final analysis to detect an HR of 0.75 at an overall alpha level of 0.023 (1-sided) in all patients. If the OS hypotheses in all populations and all PFS null hypotheses are rejected, the OS test has approximately 94.5% power at final analysis to detect an HR of 0.75 at an overall alpha level of 0.025 (1-sided) in all patients.
For ORR, based on 749 patients with at least 10 months of follow-up, the study had a 98.7% power to detect a 15%-point difference in ORR (at an alpha of 0.025) between an underlying 35% response rate in the placebo in combination with cisplatin and 5-FU group and a 50% response rate in the pembrolizumab in combination with cisplatin and 5-FU.
Results
Patient Disposition
Patient Disposition shows the patient disposition for the KEYNOTE-590 study. Of the 1,020 patients screened, a total of 749 patients were randomized and 271 patients were excluded upon screening primarily because they did not have a histologically or cytologically confirmed diagnosis of locally advanced unresectable or metastatic adenocarcinoma or ESCC or advanced or metastatic Siewert type I.1
Of the 749 patients that were randomized to receive either pembrolizumab in combination with cisplatin and 5-FU (n = 373) or placebo in combination with cisplatin and 5-FU (n = 376), 740 received treatment (n = 370 and n = 370, respectively) and 9 did not receive treatment (n = 3 and n = 6, respectively).1
At the time of the data cut-off date of July 2, 2020, a total of 687 patients discontinued treatment (n = 328 in the pembrolizumab in combination with cisplatin and 5-FU group; n = 359 in the placebo in combination with cisplatin and 5-FU group). The main reasons for discontinuation in the pembrolizumab in combination with cisplatin and 5-FU group and in the placebo in combination with cisplatin and 5-FU group were progressive disease (55.1% and 64.6%, respectively), followed by AEs (13.2% and 11.9%, respectively), and then clinical progression (9.7% and 11.1%, respectively). A total of 15 patients in the pembrolizumab in combination with cisplatin and 5-FU group completed treatment while 1 patient in the placebo in combination with cisplatin and 5-FU group completed treatment.1
The efficacy population (ITT population) included 749 patients, while the safety population included 740 patients.1
As of the data cut-off date, the median follow-up duration for patients in the pembrolizumab in combination with cisplatin and 5-FU group was 12.6 months (range = 0.1 to 33.6) and the median follow-up duration for patients in the placebo combination with cisplatin and 5-FU group was 9.8 months (range = 0.1 to 33.6).1
Item | KEYNOTE-590 | |
|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU | |
Screened, N | 1,020 | |
Excluded on screening, n | 271 | |
Randomized, n | 373 | 376 |
Received treatment | 370 (99.2) | 370 (98.4) |
Did not receive treatment | 3 (0.8) | 6 (1.6) |
Completed treatment | 15 (4.1) | 1 (0.3) |
Discontinued from study | 328 (88.6) | 359 (97.0) |
Reason for discontinuation | ||
Progressive disease | 204 (55.1) | 239 (64.6) |
Adverse events | 49 (13.2) | 44 (11.9) |
Clinical progression | 36 (9.7) | 41 (11.1) |
Withdrawal by participant | 30 (8.1) | 23 (6.2) |
Physician decision | 9 (2.4) | 10 (2.7) |
Complete response | 0 (0.0) | 1 (0.3) |
Protocol violation | 0 (0.0) | 1 (0.3) |
Continuing treatment | 27 (7.3) | 10 (2.7) |
Efficacy (ITT) populationa, n | 373 | 376 |
ITT global cohort | 355 | 356 |
ITT China cohort | 51 | 55 |
ITT ESCC | 274 | 274 |
ITT PD-L1 CPS ≥ 10 | 186 | 197 |
ITT ESCC PD-L1 CPS ≥ 10 | 143 | 143 |
Safety population, n | 370 | 370 |
5-FU = 5-fluorouracil; CPS = combined positive score; ESCC = esophageal squamous carcinoma; ITT = intention to treat; PD-L1 = programmed cell death protein 1.
Note: Values are n (%) unless otherwise indicated.
Note: The data cut-off date was July 2, 2020.
aGlobal Study Population
Source: Clinical Study Report, Keytruda submission.1
Exposure to Study Treatments
The median duration on therapy was similar between groups (5.7 months [range = 0.0 to 26.0] versus 5.1 months [range = 0.1 to 26.6]), while the median number of cycles was 8.0 months (range = 1.0 to 35.0) for the pembrolizumab in combination with cisplatin and 5-FU group compared with 7.0 months (range = 1.0 to 35.0) for the placebo in combination with cisplatin and 5-FU group. AEs leading to dose interruption was similar between the groups (66.8% versus 63.2%). Dose reduction of pembrolizumab was not permitted. Refer to Table 10 and Table 20 for more details.
Table 10: Summary of Exposure to Treatment — Safety Population
Item | Pembrolizumab in combination with cisplatin and 5-FU N = 370 | Placebo in combination with cisplatin and 5-FU N = 370 |
|---|---|---|
Duration on therapy, months | ||
Mean (SD) | 7.7 (6.8) | 5.8 (4.8) |
Median (min to max) | 5.7 (0.0 to 26.0) | 5.1 (0.1 to 26.6) |
Number of cycles | ||
Mean (SD) | 11.0 (9.4) | 8.5 (6.4) |
Median (min to max) | 8.0 (1.0 to 35.0) | 7.0 (1.0 to 35.0) |
Duration of exposure, n (%) | ||
> 0 months | 370 (100.0) | 370 (100.0) |
≥ 1 months | 326 (88.1) | 325 (87.8) |
≥ 3 months | 269 (72.7) | 260 (70.3) |
≥ 6 months | 167 (45.1) | 131 (35.4) |
≥ 9 months | 105 (28.4) | 72 (19.5) |
≥ 12 months | 79 (21.4) | 39 (10.5) |
≥ 18 months | 50 (13.5) | 13 (3.5) |
≥ 24 months | 13 (3.5) | 2 (0.5) |
Number of cycles, pembrolizumab | ||
Mean (SD) | 10.8 (9.3) | NA |
Median (min to max) | 8.0 (1.0 to 35.0) | NA |
Number of cycles, placebo | ||
Mean (SD) | NA | 8.4 (6.4) |
Median (min to max) | NA | 7.0 (1.0 to 35.0) |
Number of cycles, cisplatin | ||
Mean (SD) | 4.7 (1.7) | 4.7 (1.8) |
Median (min to max) | 6.0 (1.0 to 6.0) | 6.0 (1.0 to 6.0) |
Number of cycles, 5-FU | ||
Mean (SD) | 8.0 (7.2) | 7.1 (5.4) |
Median (min to max) | 6.0 (1.0 to 35.0) | 6.0 (1.0 to 35.0) |
Adverse event leading to dose interruption, n (%) | 247 (66.8) | 234 (63.2) |
5-FU = 5-fluorouracil; max = maximum; min = minimum; NA = not applicable; SD = standard deviation.
Note: The data cut-off date was July 2, 2020.
Note: Dose reduction of pembrolizumab is not permitted.
Source: Clinical Study Report.1
Efficacy
Overall Survival
In patients with ESCC and PD-L1 with a CPS of 10 or greater, OS HR was 0.57 (95% CI, 0.43 to 0.75; P < 0.0001). The median OS was 13.9 months (95% CI, 11.1 to 17.7) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 8.8 months (95% CI, 7.8 to 10.5) for the placebo in combination with cisplatin and 5-FU group.
In patients with ESCC, OS HR was 0.72 (95% CI, 0.60 to 0.88; P = 0.0006). The median OS was 12.6 months (95% CI, 10.2 to 14.3) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 9.8 months (95% CI, 8.6 to 11.1) for the placebo in combination with cisplatin and 5-FU group.
In patients whose tumour express PD-L1 with a CPS of 10 or greater, OS HR was 0.62 (95% CI, 0.49 to 0.78; P < 0.0001). The median OS was 13.5 months (95% CI, 11.1 to 15.6) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 9.4 months (95% CI, 8.0 to 10.7) for the placebo in combination with cisplatin and 5-FU group.
In all patients, OS HR was 0.73 (95% CI, 0.62 to 0.86; P < 0.0001). The median OS was 12.4 months (95% CI, 10.5 to 14.0) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 9.8 months (95% CI, 8.8 to 10.8) for the placebo in combination with cisplatin and 5-FU group.
In all 4 OS analyses, the HRs were statistically significant. Refer to Table 11: Summary of Efficacy Co-Primary Outcomes, Efficacy (ITT) Population for more details.
Kaplan–Meier Curves for OS are presented in Figure 3, Figure 4, Figure 5, and Figure 6.
Progression-Free Survival
In patients with ESCC, PFS HR was 0.65 (95% CI, 0.54 to 0.78; P < 0.0001). The median PFS was 6.3 months (95% CI, 6.2 to 6.9) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 5.8 months (95% CI, 5.0 to 6.1) for the placebo in combination with cisplatin and 5-FU group.
In patients whose tumour express PD-L1 with a CPS of 10 or greater, PFS HR was 0.51 (95% CI, 0.41 to 0.65; P < 0.0001). The median PFS was 7.5 months (95% CI, 6.2 to 8.2) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 5.5 months (95% CI, 4.3 to 6.0) for the placebo in combination with cisplatin and 5-FU group.
In all patients, PFS HR was 0.65 (95% CI, 0.55 to 0.76; P < 0.0001). The median PFS was 6.3 months (95% CI, 6.2 to 6.9) for the pembrolizumab in combination with cisplatin and 5-FU group compared to 5.8 months (95% CI, 5.0 to 6.0) for the placebo in combination with cisplatin and 5-FU group.
In all 3 PFS analyses, the HRs were statistically significant. Refer to Table 11: Summary of Efficacy Co-Primary Outcomes, Efficacy (ITT) Population for more details.
Kaplan–Meier curves for PFS are presented in Figure 7, Figure 8, and Figure 9.
Table 11: Summary of Efficacy Co-Primary Outcomes — Efficacy, ITT, Population
Outcomes | Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU |
|---|---|---|
OS (Co-primary outcome), ITT population | ||
OS: Patients with ESCC and PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 94/143 (65.7) | 121/143 (84.6) |
Median OS, months (95% CI)a | 13.9 (11.1 to 17.7) | 8.8 (7.8 to 10.5) |
HR (Cox regression model)b (95% CI) | 0.57 (0.43 to 0.75) | |
P value (stratified log-rank test)c | < 0. 0001 | |
12-month OS rate, % (95% CI)a | 54.5 (46.0 to 62.3) | 33.6 (26.0 to 41.3) |
OS: Patients with ESCC | ||
Events (deaths), n/N (%) | 190/274 (69.3) | 222/274 (81.0) |
Median OS, months (95% CI)a | 12.6 (10.2 to 14.3) | 9.8 (8.6 to 11.1) |
HR (Cox regression model)b (95% CI) | 0.72 (0.60 to 0.88) | |
P value (stratified log-rank test)c | 0.0006 | |
12-month OS rate, % (95% CI)a | 51.0 (44.9 to 56.8) | 37.9 (32.2 to 43.7) |
OS: Patients with PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 124/186 (66.7) | 165/197 (83.8) |
Median OS, months (95% CI)a | 13.5 (11.1 to 15.6) | 9.4 (8.0 to 10.7) |
HR (Cox regression model) (95% CI)d | 0.62 (0.49 to 0.78) | |
P value (stratified log-rank test)e | < 0.0001 | |
12-month OS rate, % (95% CI)a | 53.8 (46.3 to 60.6) | 37.1 (30.3 to 43.8) |
OS: All patients | ||
Events (deaths), n/N (%) | 262/373 (70.2) | 309/376 (82.2) |
Median OS, months (95% CI)a | 12.4 (10.5 to 14.0) | 9.8 (8.8 to 10.8) |
HR (Cox regression model)f (95% CI) | 0.73 (0.62 to 0.86) | |
P value (stratified log-rank test)g | < 0.0001 | |
12-month OS rate, % (95% CI)a | 50.6 (45.4 to 55.6) | 39.4 (34.4 to 44.3) |
PFS (Co-Primary Outcome): ITT population | ||
PFS: Patients with ESCC | ||
Events (deaths), n/N (%) | 219/274 (79.9) | 244/274 (89.1) |
Median PFS, months (95% CI)a | 6.3 (6.2 to 6.9) | 5.8 (5.0 to 6.1) |
HR (Cox regression model)a (95% CI)b | 0.65 (0.54 to 0.78) | |
P value (stratified log-rank test)c | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 24.1 (19.0 to 29.6) | 11.9 (8.2 to 16.3) |
PFS: Patients with PD-L1 CPS ≥ 10 | ||
Events (deaths), n/N (%) | 140/186 (75.3) | 174/197 (88.3) |
Median PFS, months (95% CI)a | 7.5 (6.2 to 8.2) | 5.5 (4.3 to 6.0) |
HR (Cox regression model) (95% CI)h | 0.51 (0.41 to 0.65) | |
P value (stratified log-rank test)i | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 30.3 (23.5 to 37.5) | 9.2 (5.5 to 14.2) |
PFS: All patients | ||
Events (deaths), n (%) | 297/373 (79.6) | 333/376 (88.6) |
Median PFS, months (95% CI)a | 6.3 (6.2 to 6.9) | 5.8 (5.0 to 6.0) |
HR (Cox regression model) (95% CI)f | 0.65 (0.55 to 0.76) | |
P value (stratified log-rank test)g | < 0.0001 | |
12-month PFS rate, % (95% CI)a | 24.9 (20.4 to 29.6) | 11.9 (8.7 to 15.7) |
5-FU = 5-fluorouracil; CI = confidence interval; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; ESCC = esophageal squamous cell carcinoma; HR = hazard ratio; ITT = intention to treat; OS = overall survival; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival.
aFrom product-limit (Kaplan–Meier) method for censored data.
bBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by geographic region (Asia, rest of the world) and ECOG Performance Status (0, 1).
cOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world) and ECOG Performance Status (0, 1).
dBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by geographic region (Asia vs. rest of the world) and tumour histology (adenocarcinoma vs. squamous cell carcinoma).
eOne-sided P value based on log-rank test stratified by geographic region (Asia vs. rest of the world) and tumour histology (adenocarcinoma vs. squamous cell carcinoma).
fStratified by geographic region (Asia, rest of the world), tumour histology (adenocarcinoma, squamous cell carcinoma), and ECOG Performance Status (0, 1).
gOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world), tumour histology (adenocarcinoma, squamous cell carcinoma), and ECOG Performance Status (0, 1).
hBased on Cox regression model with the Efron method of tie handling with treatment as a covariate stratified by geographic region (Asia, rest of the world) and tumour histology (adenocarcinoma, squamous cell carcinoma).
IOne-sided P value based on log-rank test stratified by geographic region (Asia, rest of the world) and tumour histology (adenocarcinoma, squamous cell carcinoma).
Source: Clinical Study Report, Keytruda submission.1
Figure 3: Kaplan–Meier Estimates of Overall Survival, Patients With ESCC, and PD-L1 CPS ≥ 10 — ITT Population
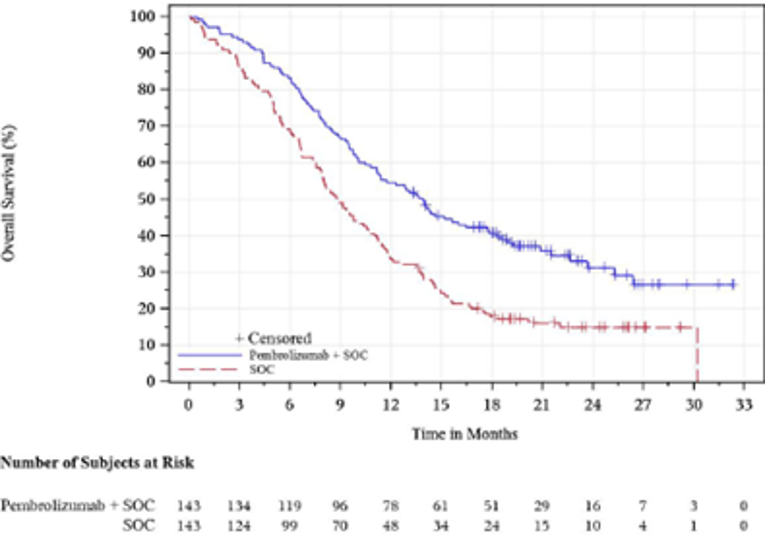
5-FU = 5-fluorouracil; CPS- = combined positive score; ESCC = esophageal squamous cell carcinoma; ITT = intent to treat; PD-L1 = programmed cell death ligand 1; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 4: Kaplan–Meier Estimates of Overall Survival in Patients With ESCC — ITT Population
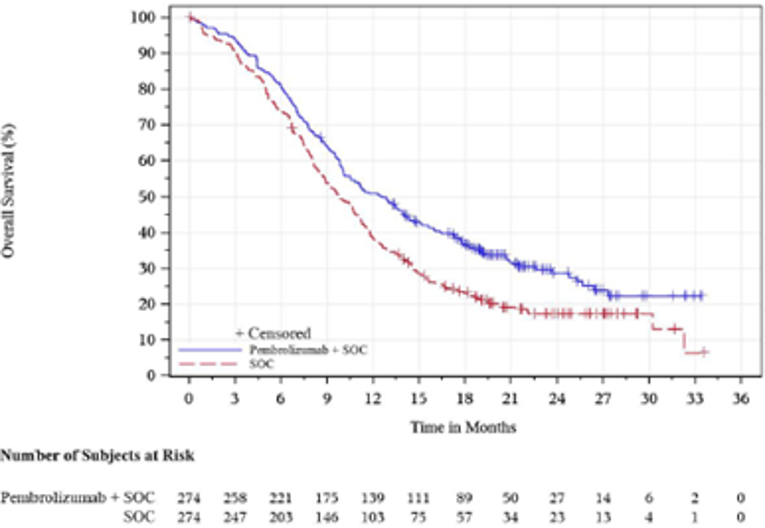
5-FU = 5-fluorouracil; ESCC = esophageal squamous cell carcinoma; ITT = intent to treat; PD-L1 = programmed cell death ligand 1; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 5: Kaplan–Meier Estimates of Overall Survival in Patients With PD-L1 CPS of 10 or Greater — ITT Population
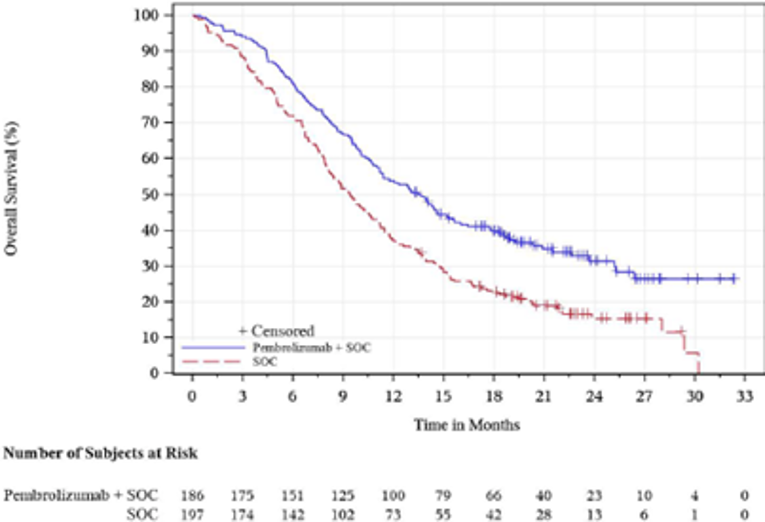
5-FU = 5-fluorouracil; CPS = combined positive score; ESCC = esophageal squamous cell carcinoma; ITT = intent to treat; PD-L1 = programmed cell death ligand 1; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 6: Kaplan–Meier Estimates of Overall Survival (All Patients)
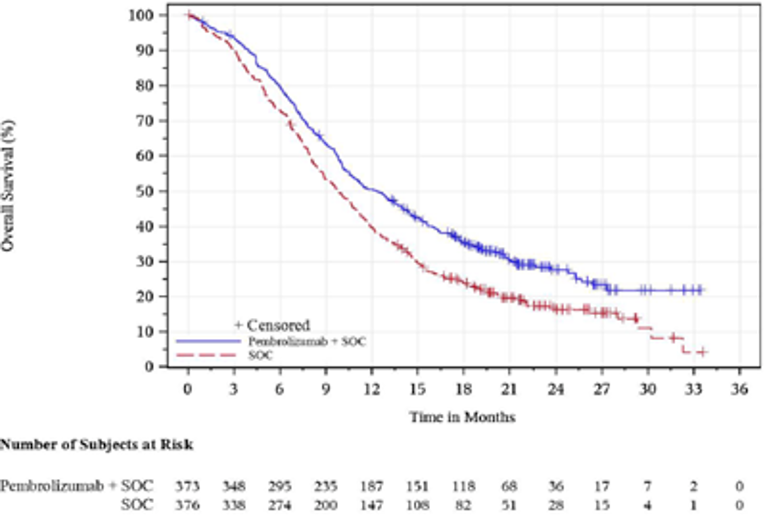
5-FU = 5-fluorouracil; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 7: Kaplan–Meier Estimates of PFS Based on Investigator Assessment per RECIST 1.1. in Patients With ESCC — ITT Population
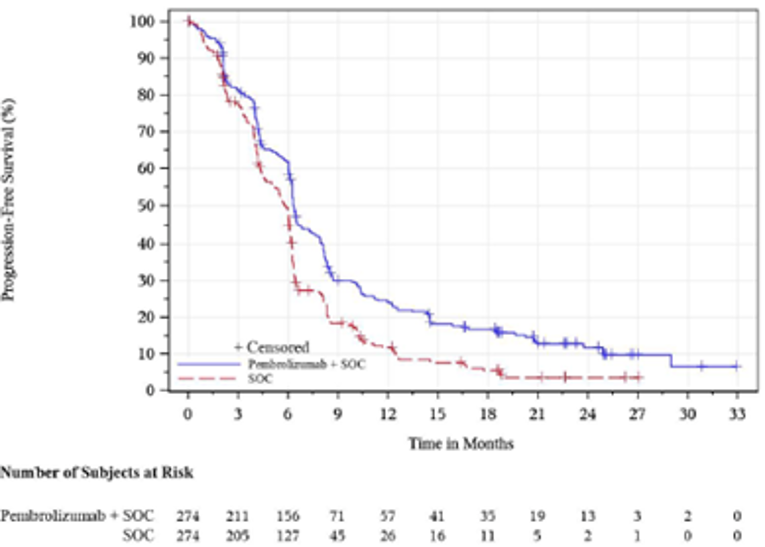
5-FU = 5-fluorouracil; ESCC = esophageal squamous cell carcinoma; ITT = intention to treat; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 8: Kaplan–Meier Estimates of PFS Based on Investigator Assessment per RECIST 1.1. in Patients With PD-L1 CPS of 10 or Greater — ITT Population
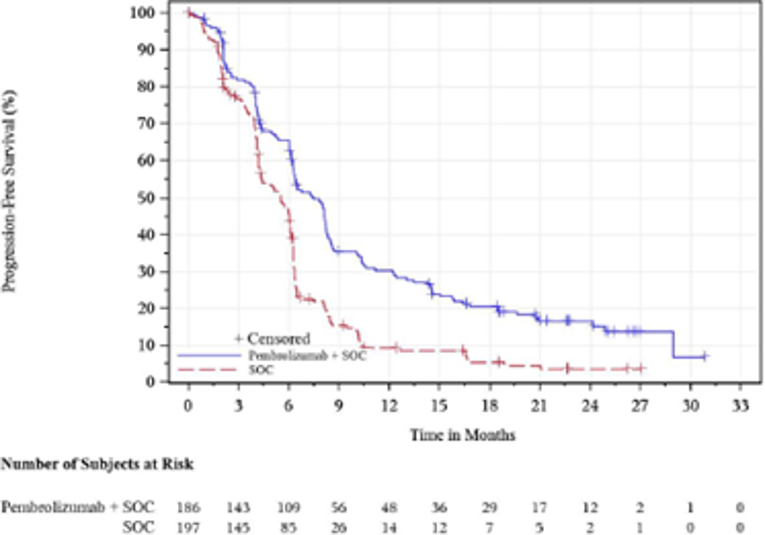
5-FU = 5-fluorouracil; CPS = combined positive score; ITT = intention to treat; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 9: Kaplan–Meier Estimates of PFS Based on Investigator Assessment per RECIST 1.1 in All Patients — ITT Population
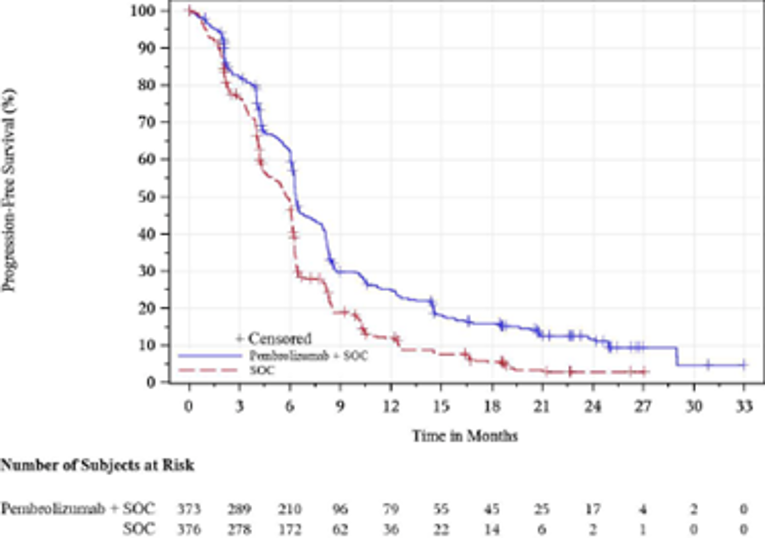
5-FU = 5-fluorouracil; ITT = intention to treat; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; SOC = cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
In general, pre-specified subgroup analyses for OS and PFS were consistent with the co-primary analysis results, with the exception of sex (female), histology (adenocarcinoma [OS only]), primary tumour site (adenocarcinoma of esophagus [OS only]), and Siewert type I. Refer to Table 12: Summary of Subgroup Analyses, All Patients, ITT Population Forrest plots of OS and PFS HRs by subgroups can be found in Figure 18 and Figure 19.
Table 12: Summary of Subgroup Analyses for All Patients — ITT Population
Subgroups | Pembrolizumab in combination with cisplatin and 5-FU N = 373 | Placebo in combination with cisplatin and 5-FU N = 376 | HR (Cox regression model)a (95% CI) |
|---|---|---|---|
Overall survival | |||
Age | |||
< 65 years | 147/201 (73.1) | 185/226 (81.9) | 0.76 (0.61 to 0.95) |
≥ 65 years | 115/172 (66.9) | 124/150 (82.7) | 0.69 (0.53 to 0.89) |
Sex | |||
Male | 216/306 (70.6) | 266/319 (83.4) | 0.70 (0.58 to 0.84) |
Female | 46/67 (68.7) | 43/57 (75.4) | 0.89 (0.59 to 1.35) |
ECOG Performance Status | |||
0 | 95/149 (63.8) | 112/150 (74.7) | 0.72 (0.55 to 0.94) |
1 | 166/223 (74.4) | 196/225 (87.1) | 0.73 (0.59 to 0.90) |
2 | 1/1 (100.0) | 1/1 (100.0) | NA |
Histology | |||
Adenocarcinoma | 72/99 (72.7) | 87/102 (85.3) | 0.74 (0.54 to 1.02) |
Squamous cell carcinoma | 190/274 (69.3) | 222/274 (81.0) | 0 0.72 (0.60 to 0.88) |
Primary tumour site | |||
Squamous cell carcinoma of the esophagus | 190/274 (69.3) | 222/274 (81.0) | 0.72 (0.60 to 0.88) |
Adenocarcinoma of the esophagus | 44/58 (75.9) | 45/52 (86.5) | 0.78 (0.51 to 1.20) |
Adenocarcinoma of the gastroesophageal junction, Siewert type I | 28/41 (68.3) | 42/50 (84.0) | 0.70 (0.43 to 1.15) |
Disease status | |||
Metastatic | 240/344 (69.8) | 279/339 (82.3) | 0.71 (0.60 to 0.85) |
Unresectable, locally advanced | 22/29 (75.9) | 30/37 (81.1) | NA |
Progression-free survival, investigator-assessed per RECIST 1.1 | |||
Age | |||
< 65 years | 168/201 (83.6) | 204/226 (90.3) | 0.69 (0.56 to 0.85) |
≥ 65 years | 129/172 (75.0) | 129/150 (86.0) | 0.62 (0.48 to 0.80) |
Sex | |||
Male | 252/306 (82.4) | 285/319 (89.3) | 0.63 (0.53 to 0.75) |
Female | 45/ 67 (67.2) | 48/ 57 (84.2) | 0.74 (0.49 to 1.12) |
ECOG Performance Status | |||
0 | 113/149 (75.8) | 135/150 (90.0) | 0.57 (0.45 to 0.74) |
1 | 183/ 223 (82.1) | 197/225 (87.6) | 0.71 (0.58 to 0.87) |
2 | 1/1 (100.0) | 1/1 (100.0) | NA |
Histology | |||
Adenocarcinoma | 78/99 (78.8) | 89/102 (87.3) | 0.63 (0.46 to 0.87) |
Squamous Cell Carcinoma | 219/274 (79.9) | 244/274 (89.1) | 0.65 (0.54 to 0.78) |
Primary tumour site | |||
Squamous cell carcinoma of the esophagus | 219/274 (79.9) | 244/274 (89.1) | 0.65 (0.54 to 0.78) |
Adenocarcinoma of the esophagus | 47/58 (81.0) | 49/52 (94.2) | 0.58 (0.38 to 0.90) |
Adenocarcinoma of the gastroesophageal junction, Siewert type I | 31/41 (75.6) | 40/50 (80.0) | 0.73 (0.45 to 1.20) |
Disease status | |||
Metastatic | 275/344 (79.9) | 305/339 (90.0) | 0.62 (0.53 to 0.74) |
Unresectable (locally advanced) | 22/29 (75.9) | 28/37 (75.7) | N A |
5-FU = 5-fluorouracil; CI = confidence interval, ECOG = Eastern Cooperative Oncology Group, HR = hazard ratio, NA = not analyzed; RECIST = Response Evaluation Criteria in Solid Tumors.
Note: All values are n/N (%).
Note: The data cut-off date was July 2, 2020.
aPembrolizumab in combination with cisplatin and 5-FU vs. placebo in combination with cisplatin and 5-FU.
Source: Clinical Study Report.1
Objective Response Rate
In all patients, confirmed ORR was higher with the pembrolizumab in combination with cisplatin and 5-FU group compared to the placebo in combination with cisplatin and 5-FU group (45.0% and 29.3% respectively). Refer to Table 13 Objective Response Rate and Duration of Response, All Patients, ITT Population .
For ORR of patients with ESCC, ESCC and a CPS of 10 or greater, and ESCC and CPS refer to Table 25.
Duration of Response
In all patients, the median DOR in the pembrolizumab in combination with cisplatin and 5-FU group was 8.3 months (range = 1.2 to 31.0) compared with the placebo in combination with cisplatin and 5-FU group (6.0 months; 1.5 to 25.0, respectively). Refer to Table 13 Objective Response Rate and Duration of Response, All Patients, ITT Population .
For DOR of patients with ESCC, ESCC and a CPS of 10 or greater, and ESCC and CPS refer to Table 25.
Table 13: Objective Response Rate and Duration of Response for All Patients — ITT Population
Outcome | Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU |
|---|---|---|
Objective response rate, investigator assessment per RECIST 1.1: all patients | ||
Number of responses, n/N | 168/373 | 110/376 |
Complete response, n (%) | 24 (6.4) | 9 (2.4) |
Partial response, n (%) | 144 (38.6) | 101(26.9) |
Stable disease, n (%) | 128 (34.3) | 174(46.3) |
Progressive disease, n (%) | 42 (11.3) | 59 (15.7) |
Could not be evaluated, n (%) | 4 (1.1) | 2 (0.5) |
No assessment, n (%) | 31 (8.3) | 31 (8.2) |
Overall response rate, % (95% CI) | 45.0 (39.9, 50.2) | 29.3 (24.7, 34.1) |
Difference in overall response rate between pembrolizumab and placebo (95% CI), P value | 15.8 (9.0 to 22.5), 0.0001 | |
Duration of response, investigator assessment per RECIST 1.1 patients with confirmed response: all patients | ||
Number of patients with response, n/N (%)a | 168/373 (45.0) | 110/376 (29.3) |
Response duration (months), median (minimum to maximum)b | 8.3 (1.2 to 31.0)c | 6.0 (1.5 to 25.0)c |
5-FU = 5-fluorouracil; CI = confidence interval; ITT = intention to treat; LS = least square: PD-L1 = programmed cell death ligand 1; RECIST = Response Evaluation Criteria in Solid Tumors.
Note: The data cut-off date was July 2, 2020.
aIncludes patients with confirmed complete response or partial response.
bFrom product-limit (Kaplan–Meier) method for censored data.
cNo progressive disease by the time of last disease assessment.
Source: Clinical Study Report.1
EQ-5D Questionnaire
In the FAS population, the compliance and completion for the EQ-5D at baseline was similar at the baseline (98.1% for both groups). Over time, compliance and completion rates declined as missing data by design (e.g., discontinued due to AE, clinical progression, physician decision, progressive disease, withdrawal by patient) increased.
Based on blinded data review, week 18 was used for the mean change from baseline analysis. At week 18, imbalances (≥ 5% differences) in missing data (i.e., discontinued due to AE, clinical progression, physician decision, progressive disease, protocol violation, withdrawal by patient, patient died) were observed between the pembrolizumab in combination with cisplatin and 5-FU group compared to the placebo in combination with cisplatin and 5-FU group (31.9% versus 38.9%, respectively). At week 18, patients not completing the questionnaire due to disease under study or to site staff error were similar (6.5% versus 4.4%, respectively).
In the FAS population, the least squares mean change from baseline to week 18 in EQ-5D VAS was similar between the 2 groups. EQ-5D was an exploratory end point, with no MID reported by the sponsor. Refer to Table 14.
For EQ-5D VAS of patients with (i) ESCC, (ii) ESCC and a CPS of 10 or greater, and (iii) ESCC and a CPS of 10 or greater refer to Table 26.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
Based on blinded data review, week 18 was used for the mean change from baseline analysis. In the FAS population, the least squares mean change from baseline to week 18 in in global health status/QoL remained was similar between the 2 groups. The mean change from baseline in global health status/QoL remained stable over time for the pembrolizumab in combination with cisplatin and 5-FU group compared with the placebo in combination with cisplatin and 5-FU group and the median time to deterioration for global health status/QoL was not reached for both groups. Refer to Figure 10, Figure 11, and Table 14.
Imbalances (≥ 5% differences) in missing data (e.g., discontinued due to AE, clinical progression, complete response, physician decision, progressive disease, protocol violation, withdrawal by patient, completed study treatment, translation not available in patient’s language, patient died) were observed at week 18 between the pembrolizumab in combination with cisplatin and 5-FU group compared to the placebo in combination with cisplatin and 5-FU group (31.7% versus 38.7%, respectively). At week 18, patients not completing the questionnaire (e.g., did not complete due to disease under study, site staff error, patient in hospital, physically unable to complete, patient refused for other reasons, with visit no record, or other) were similar (6.8% versus 4.7%, respectively).
For global health status/QoL of patients with ESCC, ESCC and a CPS of 10 or greater, and ESCC refer to Table 26, Figure 20, Figure 21, Figure 22, Figure 23, Figure 24 and Figure 25.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module
Based on blinded data review, week 18 was used for the mean change from baseline analysis. In the FAS population, the mean change from baseline in pain was in favour of the pembrolizumab in combination with cisplatin and 5-FU, the mean change from baseline in dysphagia and reflux were similar between the 2 groups, and the median time to deterioration for dysphagia, pain, and reflux was not reached for both groups. Refer to Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, Figure 17, and Table 14.
For dysphagia, pain, and reflux of patients with ESCC, ESCC and a CPS of 10 or greater, and ESCC refer to Table 26, Figure 26, Figure 27, Figure 28,Figure 29, Figure 30, Figure 31, Figure 32, Figure 33,Figure 34, Figure 35, Figure 36, Figure 37, Figure 38, Figure 39, Figure 40, Figure 41, Figure 42, and Figure 43.
Table 14: Patient-Reported Outcomes — FAS Population
Patient-reported outcome | Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU |
|---|---|---|
EQ-5D VAS: FAS populationa | ||
Change from baseline to week 18, LS mean (95% CI)b | –2.29 (–4.35 to –0.24) | –3.49 (–5.61 to –1.37) |
Difference in LS means (95% CI), P valueb | 1.20 (–1.61 to 4.01), 0.4016 | |
EORTC QLQ-C30 global health status/QoL: FAS populationc | ||
Change from baseline to week 18, LS mean (95% CI) | –1.74 (–4.24 to 0.75) | –1.64 (–4.21 to 0.92) |
Difference in LS means (95% CI), P value | –0.10 (–3.40 to 3.20), 0.9530 | |
EORTC QLQ-OES18 dysphagia: FAS populationc | ||
Change from baseline to week 18, LS mean (95% CI) | 0.78 (–3.25 to 4.81) | 3.13 (–1.02 to 7.28) |
Difference in LS means (95% CI), P value | –2.35 (–7.78 to 3.07), 0.3945 | |
EORTC QLQ-OES18 pain: FAS populationc | ||
Change from baseline to week 18, LS mean (95% CI) | –4.78 (–7.01 to –2.56) | –1.85 (–4.14 to 0.45) |
Difference in LS means (95% CI), P value | –2.94 (–5.86 to –0.02), 0.0487 | |
EORTC QLQ-OES18 reflux: FAS populationc | ||
Change from baseline to week 18, LS mean (95% CI) | –0.43 (–2.91 to 2.06) | 0.76 (–1.80 to 3.33) |
Difference in LS means (95% CI), P value | –1.19 (–4.49 to 2.10), 0.4781 | |
EORTC QLQ-C30 global health status/QoL: FAS population | ||
Improved, n/N (%), (95 CI%)d | 120/338 (35.5), (30.4 to 40.9) | 91/334 (27.2), (22.5 to 32.4) |
Stable, n/N (%), (95 CI%)d | 136/338 (40.2), (35.0 to 45.7) | 145/334 (43.4), (38.0 to 48.9) |
Improved and stable, n/N (%), (95 CI%)d | 256/338 (75.7), (70.8 to 80.2) | 236/334 (70.7), (65.5 to 75.5) |
Deteriorated, n/N (%), (95 CI%)d | 82/338 (24.3), (19.8 to 29.2) | 98/334 (29.3), (24.5 to 34.5) |
Difference in percent improved, estimate (95 CI%)e, P valuef | 8.1 (1.1 to 15.1), 0 0.0116 | |
Difference in percent improved and stable, estimate (95 CI%)e, P valuef | 4.9 (–1.8 to 11.6), 0.0747 | |
EORTC QLQ-OES18 dysphagia: FAS population | ||
Improved, n/N (%), (95 CI%)d | 152/337 (45.1), (39.7 to 50.6) | 134/329 (40.7), (35.4 to 46.3) |
Stable, n/N (%), (95 CI%)d | 81/337 (24.0), (19.6 to 29.0) | 99/329 (30.1), (25.2 to 35.4) |
Improved and stable, n/N (%), (95 CI%)d | 233/337 (69.1), (63.9 to 74.0) | 233/329 (70.8), (65.6 to 75.7) |
Deteriorated, n/N (%), (95 CI%)d | 104/337 (30.9), (26. 0 to 36.1) | 96/329 (29.2), (24.3 to 34.4) |
Difference in percent improved, estimate (95 CI%)e, P valuef | 4.4 (–3.1 to 11.9), 0.1244 | |
Difference in percent improved and stable, estimate (95 CI%)e, P valuef | –1.6 (–8.5 to 5.2), 0.6788 | |
EORTC QLQ-OES18 pain: FAS population | ||
Improved, n/N (%), (95 CI%)d | 138/337 (40.9), (35.7 to 46.4) | 126/329 (38.3), (33.0 to 43.8) |
Stable, n/N (%), (95 CI%)d | 137/337 (40.7), (35.4 to 46.1) | 133/329 (40.4), (35.1 to 45.9) |
Improved and stable, n/N (%), (95 CI%)d | 275/337 (81.6), (77.0 to 85.6) | 259/329 (78.7), (73.9 to 83.0) |
Deteriorated, n/N (%), (95 CI%)d | 62/337 (18.4), (14.4 to 23. 0) | 70/329 (21.3), (17.0 to 26.1) |
Difference in percent improved, estimate (95 CI%)e, P valuef | 2.3 (–4.9 to 9.6), 0.2640 | |
Difference in percent improved and stable, estimate (95 CI%)e, P valuef | 2.6 (–3.4 to 8.7), 0.1975 | |
EORTC QLQ-OES18 reflux, FAS population | ||
Improved, n/N (%), (95 CI%)d | 101/337 (30.0), (25.1 to 35.2) | 92/329 (28.0), (23.2 to 33.1) |
Stable, n/N (%), (95 CI%)d | 164/337 (48.7), (43.2 to 54.1) | 167/329 (50.8), (45.2 to 56.3) |
Improved and stable, n/N (%), (95 CI%)d | 265/337 (78.6), (73.9 to 82.9) | 259/329 (78.7), (73.9 to 83.0) |
Deteriorated, n/N (%), (95 CI%)d | 72/337 (21.4), (17.1 to 26.1) | 70/329 (21.3), (17.0 to 26.1) |
Difference in percent improved, estimate (95 CI%)e, P valuef | 1.8 (–5.1 to 8.6), 0.3063 | |
Difference in percent improved and stable, estimate (95 CI%)e, P valuef | –0.5 (–6.7 to 5.7), 0.5652 | |
5-FU = 5-fluorouracil; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; LS = least squares; QoL = quality of life.
Note: The data cut-off date was July 2, 2020.
Note: Improved defined as a 10 point or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by a 10 point or more improvement at a visit scheduled at least 6 weeks later.
Note: Overall improvement/stability defined as the composite of improvement and stability. Stability is defined as, when the criteria for improvement are not met, a less than 10 points worsening in score from baseline at any time during the study and confirmed by a less than 10 points worsening at a visit scheduled at least 6 weeks later.
aFAS was defined as all randomized participants who have at least 1 patient-reported outcome assessment available for the specific end point and have received at least 1 dose of the study intervention.
bBased on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors geographic region (Asia, Rest of the World) and tumour histology (Adenocarcinoma, Squamous Cell Carcinoma) and ECOG performance status (0, 1).
cBased on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors geographic region (Asia, rest of the world) and tumour histology (adenocarcinoma, squamous cell carcinoma) and ECOG Performance Status (0, 1).
dBased on binomial exact CI method.
eBased on the Miettinen and Nurminen method with population-based weighting stratified by strata. If there are 0 subjects in 1 of the treatments or sequences in a comparison for a particular stratum, then strata are combined as specified in the supplemental statistical analysis plan to ensure sufficient number of subjects in each stratum.
fOne-sided P value for testing. The H0 difference in percent = 0 vs. the H1 difference in percent greater than 0.
Source: Clinical Study Report, Keytruda submission.1
Figure 10: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ-C30 Global Health Status/QoL Over Time by Treatment Group — FAS Population
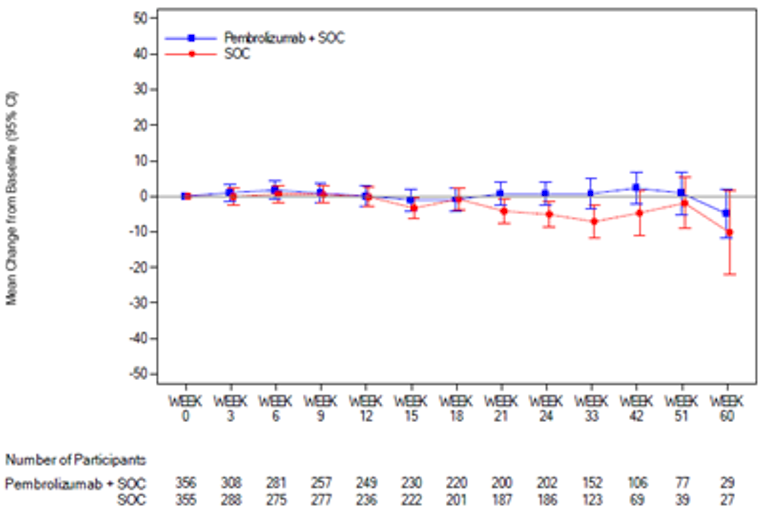
5-FU = 5-fluorouracil; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumors; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 11: Kaplan–Meier Estimates of Time to Deterioration for EORTC QLQ-C30 Global Health Status and QoL — FAS Population With Baseline
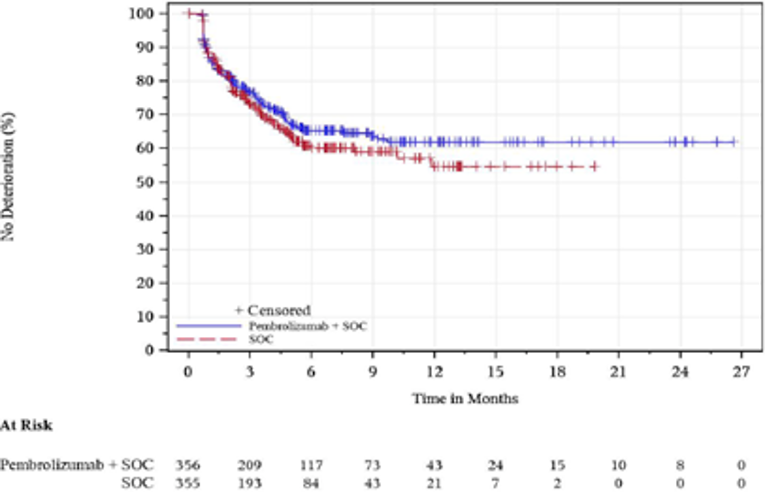
5-FU = 5-fluorouracil; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumors; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 12: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Dysphagia Over Time by Treatment Group — FAS Population
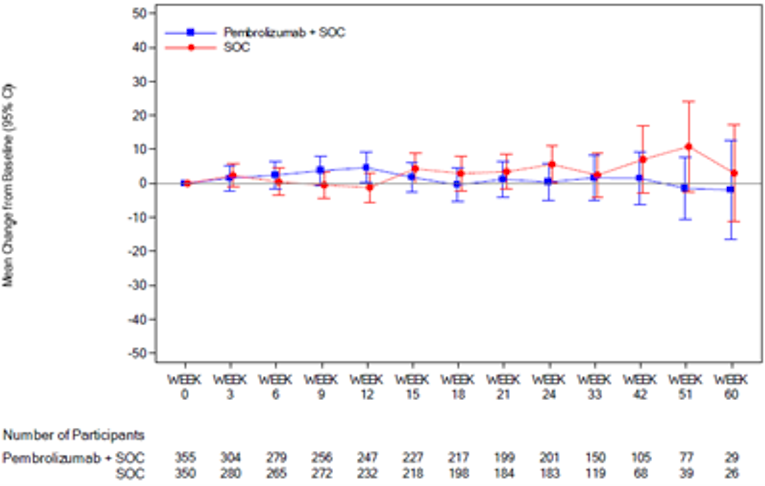
5-FU = 5-fluorouracil; CI = confidence interval; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 13: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Pain Over Time by Treatment Group — FAS Population
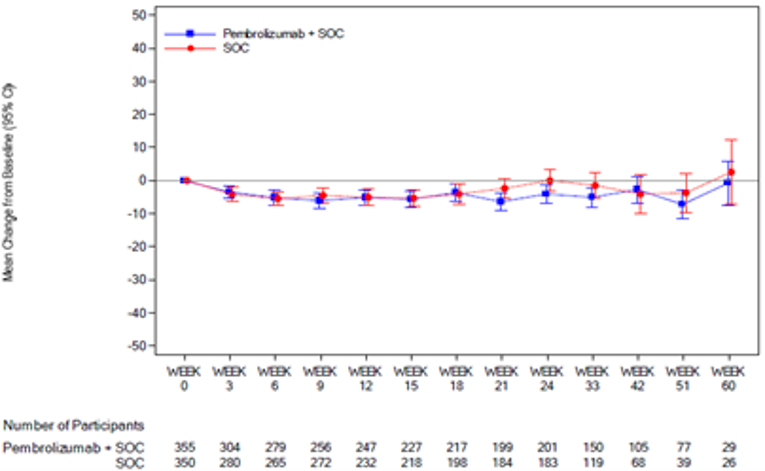
5-FU = 5-fluorouracil; CI = confidence interval; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 14: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Reflux Over Time by Treatment Group — FAS Population
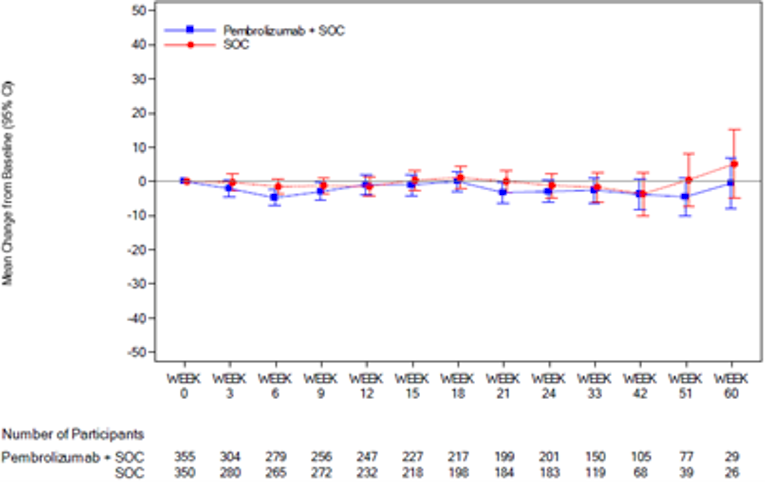
5-FU = 5-fluorouracil; CI = confidence interval; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 15: Kaplan–Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Dysphagia — FAS Population With Baseline
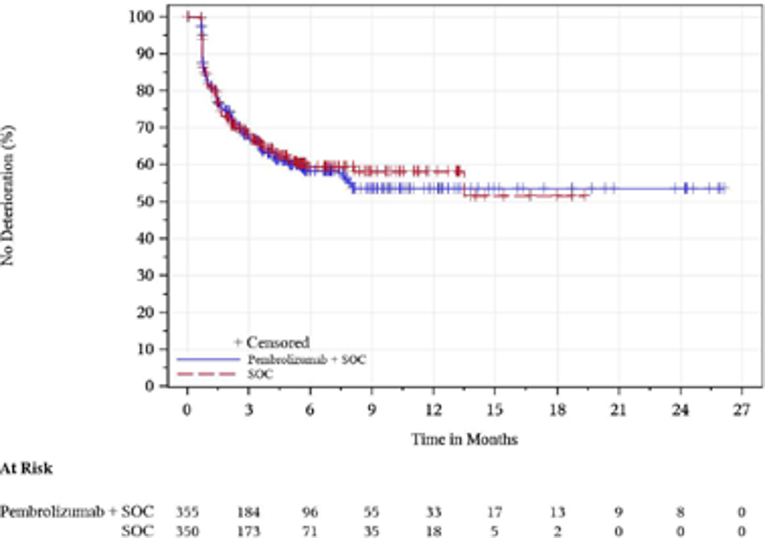
5-FU = 5-fluorouracil; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 16: Kaplan–Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Pain — FAS Population With Baseline
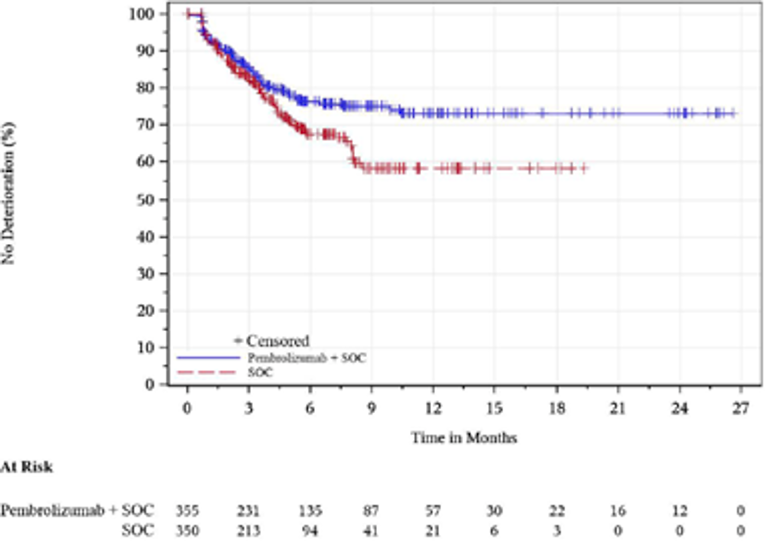
5-FU = 5-fluorouracil; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Figure 17: Kaplan–Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Reflux — FAS Population With Baseline
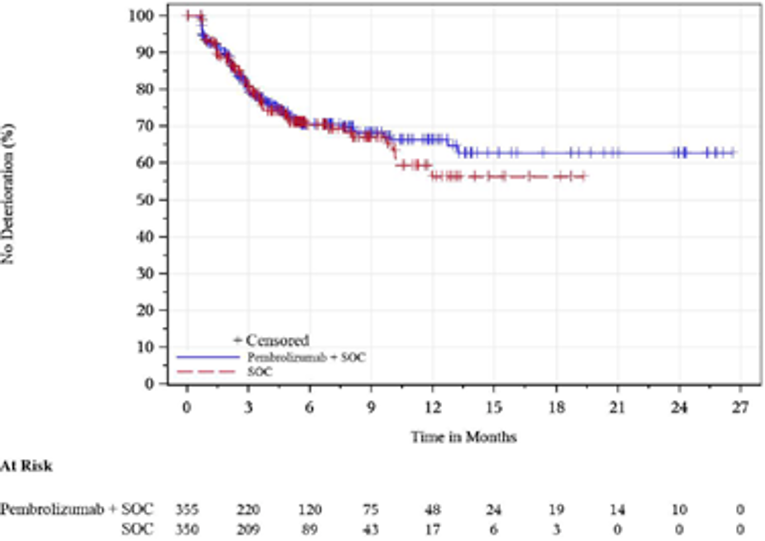
5-FU = 5-fluorouracil; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Esophageal Cancer Module; FAS = full analysis set; Pembrolizumab + SOC = pembrolizumab in combination with cisplatin and 5-FU; SOC = placebo in combination with cisplatin and 5-FU.
Note: The data cut-off date was July 2, 2020.
Source: Clinical Study Report, Keytruda submission.1
Harms (KEYNOTE-590)
Any AEs, treatment-related AEs, grade 3 to 5 AEs, and any serious AEs were comparable between pembrolizumab in combination with cisplatin and 5-FU versus placebo in combination with cisplatin and 5-FU (Table 15).
Although the number of events was infrequent, death due to AEs, and death due to treatment-related AEs were similar between the 2 groups.
The most commonly reported AEs in the pembrolizumab in combination with cisplatin and 5-FU group and the placebo in combination with cisplatin and 5-FU group were nausea (67.3% versus 62.7%, respectively), anemia (50.5% versus 56.2%, respectively), decreased appetite (44.3% versus 38.1%, respectively), fatigue (40.3% versus 34.1%, respectively), and constipation (40.0% versus 40.3%, respectively). The most frequently reported treatment-related AEs were nausea (63.0% versus 59.5%, respectively), decreased appetite (39.2% versus 32.2%, respectively), and anemia (38.6% versus 43.8%, respectively); most of which were grade 1 or 2.
Of note, immune-mediated AEs and infusion reactions were higher among the pembrolizumab in combination with cisplatin and 5-FU group (25.7% versus 11.6%, respectively), hypothyroidism (10.8% versus 6.5%, respectively) and hyperthyroidism (5.7% versus 0.8%, respectively), pneumonitis (6.2% versus 0.5%, respectively), grade 3 or higher treatment-related AE (71.9% versus 67.6%, respectively), serious treatment-related AEs (31.6% versus 26.2%, respectively), and discontinuation due to treatment-related AEs (19.5% versus 11.6%, respectively).1
Refer to Table 15: Summary of Harms and Table 27: Additional Harms Outcomes.
Harms, n (%) | KEYNOTE-590 | |
|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU N = 370 | Placebo in combination with cisplatin and 5-FU N = 370 | |
Any adverse event | 370 (100.0) | 368 (99.5) |
Grade ≥ 3a adverse event | 318 (85.9) | 308 (83.2) |
Treatment-related adverse eventb | 364 (98.4) | 360 (97.3) |
Grade ≥ 3 treatment-related adverse event | 266 (71.9) | 250 (67.6) |
Any serious adverse event | 205 (55.4) | 204 (55.1) |
Serious treatment-related adverse event,c n (%) | 117 (31.6) | 97 (26.2) |
Any adverse event leading to discontinuation | 90 (24.3) | 74 (20.0) |
Discontinuation due to treatment-related adverse event | 72 (19.5) | 43 (11.6) |
Death due to adverse event | 28 (7.6) | 38 (10.3) |
Death due to treatment-related adverse event | 9 (2.4) | 5 (1.4) |
Notable harms or harms of special interest | ||
Immune-mediated adverse events and infusion reactions | 95 (25.7) | 43 (11.6) |
Hypothyroidism | 40 (10.8) | 24 (6.5) |
Hyperthyroidism | 21 (5.7) | 3 (0.8) |
Pneumonitis | 23 (6.2) | 2 (0.5) |
Colitis | 8 (2.2) | 6 (1.6) |
Adrenal insufficiency | 4 (1.1) | 2 (0.5) |
Hepatitis | 5 (1.4) | 0 (0.0) |
Hypophysitis | 3 (0.8) | 0 (0.0) |
Nephritis | 1 (0.3) | 2 (0.5) |
Type 1 diabetes mellitus | 1 (0.3) | 0 (0.0) |
5-FU = 5-fluoruracil.
aGrades are based on National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03.
bDetermined by the investigator to be related to the drug.
cSerious adverse events up to 90 days of last dose are included.
Critical Appraisal
Internal Validity
Overall, the demographic and baseline characteristics were well-balanced between groups, with the exception of age (65 years or older) and stage IVB disease. There was a greater proportion of patients in the pembrolizumab in combination with cisplatin and 5-FU group who were 65 years of age or older compared with patients in the placebo in combination with cisplatin and 5-FU group (46.1% and 39.9%, respectively). As well, there was a greater proportion of patients in pembrolizumab in combination with cisplatin and 5-FU group with stage IVB compared with patients in the placebo in combination with cisplatin and 5-FU group (17.4% and 10.9%, respectively). These imbalances resulted in more patients who were elderly with severe disease stage in the pembrolizumab than in the placebo combination arm, which rendered the study results more likely against the study drug.
There is a potential risk of bias because of substantial missing data (ORR, DOR, EORTC QLQ-C30, EORTC QLQ-OES18, and EQ-5D-5L) particularly on the QoL measures. A total of 8.3% of proportion of patients in the pembrolizumab in combination with cisplatin and 5-FU group compared with 8.2% of patients in the placebo in combination with cisplatin and 5-FU had no post-baseline assessment available for response evaluation.
In addition, for subjective outcomes (e.g., PROs), there may have been differential recall bias. For example, drug-related AEs, such as immune-intermediate events (25.7 versus 11.6%, respectively), and particularly, hypothyroidism (i.e., symptoms including fatigue, increased sensitivity to cold, muscle weakness) and hyperthyroidism (i.e., symptoms including nervousness, anxiety, fatigue, weight loss) might have led to unblinding and the patients’ awareness of their treatment assignment, potentially leading to biased assessment of the PROs. In addition, a total of 11 inadvertent unblinding events and a total of 21 premature “emergency” unblinding events were reported by the site due to emergency safety reasons and for further medical management; these patients were not excluded from the efficacy and safety analyses. Overall, the magnitude and direction of the impact of these missing data and recall bias on QoL is unknown.
The clinical experts agreed that the OS interim results represent a clinically meaningful benefit for patients. The reported OS and PFS results are deemed final based on interim analysis according to pre-specified stopping criteria. However, whether the “actual” final efficacy results would conform with the interim results is unknown. There are case reports that discuss the early stop of a trial that claimed statistical significance according to pre-specified stopping rule that had suffered type I error with the interim results and the estimates of effects could not be repeated at the final analysis after the trial was completed.20-22 Such potential impacts, including the depletion of susceptible subjects, on OS could be more likely to occur toward the end of the trial. Therefore, the magnitude of OS benefit at final analysis may not be as large as what had been obtained at interim analysis.
The majority of patients had been treated with 1 or more prior medications (94.9% in the pembrolizumab in combination with cisplatin and 5-FU group and 94.1% in the placebo in combination with cisplatin and 5-FU group); the types of prior mediation were balanced between the 2 treatment groups.
With regards to concomitant medication, a greater proportion of patients in the pembrolizumab in combination with cisplatin and 5-FU group compared with patients in the placebo in combination with cisplatin and 5-FU group had taken the following concomitant medications: drugs for constipation (55.9% versus 49.2%, respectively), antithrombotic agents (31.4% versus 25.9%, respectively), corticosteroids in dermatological preparations (17.8% versus 11.6%, respectively), anesthetics (24.3% versus 18.1%, respectively), and psychoanaleptics (15.1% versus 9.5%, respectively). The impact of concomitant medications for the control of side effects may also have complicated the assessment of benefit on QoL.
The proportion of new anticancer medication received appeared a little higher in the placebo group (43.5% for patients in the pembrolizumab in combination with cisplatin and 5-FU group compared with 47.8% of patients in the placebo in combination with cisplatin and 5-FU group). The protocol stated that exploratory analysis to adjust for the effect of other PD-L1 therapies on OS could be performed; however, no analysis on the interim OS data were performed. Therefore, impact of other PD-L1 therapies on OS is unknown.
Approximately 1.3% of patients in the pembrolizumab in combination with cisplatin and 5-FU group and 0.8% of patients in the placebo in combination with cisplatin and 5-FU group of withdrew their participation from the trial. At total of 8.1% patients in the pembrolizumab group and 6.2% in the placebo group withdrew study medication.
Early withdrawal of the study medications and significant protocol deviations were also noted. Significant protocol deviations were similar between the pembrolizumab in combination with cisplatin and 5-FU group and the placebo in combination with cisplatin and 5-FU group (7.8% and 8.2%, respectively). Of note, protocol deviations associated with COVID-19 were higher (4.0% versus 1.9%) in the pembrolizumab than placebo combination group.
External Validity
The KEYNOTE-590 study population (first-line patients with locally advanced unresectable or metastatic adenocarcinoma or ESCC or advanced or metastatic Siewert type I adenocarcinoma of the EGJ) is considered reflective of the requested reimbursement population. The following considerations are of importance regarding the external validity of the KEYNOTE-590 study:
Population: The requested reimbursement population is carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia). Siewert type I adenocarcinoma of the EGJ (in KEYNOTE-590) is synonymous with adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia). The reimbursement request specifies that these patients must be HER2 negative. Patient populations such as patients with active CNS metastases, patients with ECOG PS 2 or greater, and patients with rare forms of esophageal cancer such as GI stromal tumour, leiomyosarcoma, and neuroendocrine tumours were excluded from the KEYNOTE-590 study. Therefore, the magnitude of benefit in these unstudied populations is uncertain. This further compromised the generalizability of the findings on efficacy and particularly, safety, to those patients who may also receive this first-line combination therapy in practice.
Intervention: The requested reimbursement population is more inclusive in terms of the pembrolizumab combination. The KEYNOTE-590 study evaluated pembrolizumab in combination with cisplatin and 5-FU compared with cisplatin and 5-FU, whereas the reimbursement request is pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy and is not limited to the chemotherapy backbone used in the KEYNOTE-590 study.
Comparator: The platinum- and fluoropyrimidine-based chemotherapy (i.e., cisplatin and 5-FU) represents 1 of the standard first-line chemotherapies regimens and is an appropriate comparator in Canada. However, other relevant treatment regimens (listed in the systematic review protocol) are not studied. It would remain uncertain if the observed benefit could be generalizable to different combinations of chemotherapies regimens.
Outcome: The follow-up duration for the pembrolizumab in combination with cisplatin and 5-FU group was 12.6 months (range = 0.1 to 33.6) and the median follow-up duration for the placebo combination with cisplatin and 5-FU group was 9.8 months (range = 0.1 to 33.6).1 The clinical experts agreed that the OS interim results represent a clinically meaningful benefit for patients.
Setting: This study is a multinational, multi-centre trial. Among the 26 countries that participated, there were 6 Canadians sites that recruited patients. Half of the patient population were enrolled in Asia (52.5%).1
Table 16 details the assessment of generalizability of evidence for pembrolizumab.
Table 16: Assessment of Generalizability of Evidence for Pembrolizumab
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | CNS metastases | Patients with known active CNS metastases were not included in KEYNOTE-590. | Thus, the magnitude of benefit for combination therapy with pembrolizumab is unclear. However, as noted by the clinical experts, patients with metastatic lung cancer with controlled CNS metastases are often treated with the combination of immunotherapy and chemotherapy. By extrapolation, it may be reasonable to treat patients with metastatic esophageal or GEJ with controlled CNS metastases who otherwise meet the inclusion criteria for KEYNOTE-590 with pembrolizumab plus chemotherapy if they do not require steroids (equivalent of prednisone 10 mg/day or higher). |
ECOG PS ≥ 2 | Patients with ECOG PS of ≥ 2 were not eligible for inclusion in KEYNOTE-590. Though 2 patients with ECOG PS = 2 appear to have been included in the trial, almost all patients were ECOG PS 0 or 1 (747 out of 749).1 | Therefore, the magnitude of benefit in this population is uncertain. | |
Other rare forms of esophageal cancer | Other rare forms of esophageal cancer such as GIST, leiomyosarcoma, and NETs were not included in KEYNOTE-590. | Thus, the benefit of pembrolizumab plus chemotherapy in this population is unknown. Of note, rare types of esophageal cancer such as GIST, leiomyosarcoma, and NETs are treated differently than patients with adenocarcinoma and squamous cell histology; this comprises the focus of this review. | |
Intolerance to platinum-based chemotherapy | By protocol design, treatment with cisplatin was to be capped at 6 cycles and treatment with 5-FU could continue for 2 years. As seen in Table 20, exposure to chemotherapy treatment reduces especially after 6 cycles in both treatment groups. The sponsor noted that this was based on the discretion of the investigator and could also be related to adverse events.3 | According to the clinical experts, if patients cannot tolerate the chemotherapy combination, and do not have any grade 3 or higher immune-related adverse events, it would be reasonable to continue with pembrolizumab monotherapy. At least 1 cycle of chemotherapy should be given concurrently with pembrolizumab. | |
Histology | There were more patients with ESCC than EAC in KEYNOTE-590 (73.2% vs. 26.8%). | The clinical experts acknowledged that even though EAC occurs more frequently than ESCC in Canada, KEYNOTE-590 included both EAC and ESCC, and the benefit is seen in the entire population. | |
Intervention | Pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy | Pembrolizumab in combination with cisplatin and 5-FU was the intervention in KEYNOTE-590. | Cisplatin plus 5-fluorouracil would be considered a standard chemotherapy backbone for this patient population. However, as noted by the clinical experts, due to the clinical efficacy of oxaliplatin-fluoropyrimidine combinations,15-18 as well as the more favourable toxicity profile of oxaliplatin vs. cisplatin, most clinicians prefer using oxaliplatin based-regimens. Oxaliplatin does not cause ototoxicity, can be used for patients with baseline renal dysfunction (CrCl ≥ 30 mL/min), and has a lower incidence of nephrotoxicity compared to cisplatin.36,37 Therefore, it is felt that FOLFOX and CAPOX should be eligible as chemotherapy backbones. |
Comparator | Platinum- and fluoropyrimidine-based chemotherapy | Placebo in combination with cisplatin and 5-FU was the comparator in KEYNOTE-590. Other relevant treatment regimens (listed in the systematic review protocol) are not considered in KEYNOTE-590. No relevant indirect treatment comparison was identified in the literature. The sponsor provided an indirect treatment comparison feasibility assessment report. Refer to Appendix 5 for the summary and critical appraisal of the feasibility assessment report. | The magnitude of benefit for pembrolizumab in combination with platinum- and fluoropyrimidine-based chemotherapy compared to other relevant treatment regimens is unknown. |
Outcomes | OS | OS was a co-primary outcome. Reported OS rates are final based on interim analysis since all end points were met. However, the study is ongoing; therefore, long-term efficacy and safety data will be available in the future. The median OS was 12.4 months (95% CI, 10.5 to 14.0) for the pembrolizumab in combination with cisplatin and 5-FU group and 9.8 months (95% CI, 8.8 to 10.8) for the placebo in combination with cisplatin and 5-FU group among all patients.1 | As noted by the clinical experts, the definition of a clinically meaningful response may vary across physicians. For patients treated with immunotherapy, a long-term plateau of the survival curve would also be considered a significant benefit as median survival for this patient population is approximately 12 months. |
QoL | EQ-5D was an exploratory outcome. There was no formal hypothesis testing, and no multiplicity adjustment was performed. No MID was reported. LS mean change from baseline to week 18 in EQ-5D VAS was similar between groups among the FAS population.1 EORTC QLQ-C30 was a secondary outcome. There was no formal hypothesis testing, and no multiplicity adjustment was performed. The mean change from baseline in the global health status/QoL scores at week 18 were similar between groups among the FAS population. The mean change from baseline in the global health status/QoL scores appeared stable over time.1 | According to the clinical experts, there was no clinically significant detriment in QoL. If the addition of an agent to an established regimen was not detrimental and improved survival, that would also be considered a clinically meaningful response to treatment. | |
Setting | Multinational, multi-centre study | Participants were enrolled from 26 countries across the Americas including Canada and US, Asia, Europe including France, Germany, and UK, Africa, and Australia. There were 8 Canadian sites, 2 of which did not enroll patients. Half of the patient population were enrolled in Asia (52.5%).1 | As noted by clinical experts, patients in France, Germany, UK, and US would likely be treated similarly to Canadian patients; therefore, the data are generalizable to the Canadian setting. |
5-FU = 5-fluorouracil; CAPOX = capecitabine and oxaliplatin; CI = confidence interval; CNS = central nervous system; CrCl = creatinine clearance; EAC = esophageal adenocarcinoma; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ESCC = esophageal squamous cell carcinoma; FAS = full analysis set; FOLFOX = 5-fluorouracil, oxaliplatin, and leucovorin; GEJ = gastesophageal junction; GIST = gastrointestinal stromal tumour; LS = least squares; MID = minimal important difference; NET = neuroendocrine tumour; OS = overall survival; QoL = quality of life; VAS = visual analogue scale.
Indirect Evidence
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search. The sponsor conducted a feasibility assessment3 of estimating the comparative efficacy and safety of pembrolizumab plus cisplatin and 5-FU versus other competing interventions using data obtained from a systematic literature review. Refer to Appendix 5 for the CADTH’s summary and critical appraisal of the feasibility assessment.
Other Relevant Evidence
The following 2 studies (KEYNOTE-062 and KEYNOTE-859) were identified as relevant because they met the systematic review protocol; however, they included a mixed population (i.e., all HER2-negative GEJ patients were enrolled without any Siewert classification, whereas only patients with HER2-negative Siewert type I GEJ are of relevance to the reimbursement request).
It is also important to note that the trials did not include patients with ESCC or adenocarcinoma of the esophagus, which is a relevant population for the reimbursement request. For the KEYNOTE-062 study, patients must be PD-L1 positive (i.e., CPS ≥ 1), whereas PD-L1 status is not an eligibility criterion for reimbursement for this submission. The results from the pre-specified subgroup analysis of the primary location (GEJ) were only available for OS and safety data are reported for the entire study population (gastric and GEJ adenocarcinoma). For the KEYNOTE-859 study, only study design details are available, and no results are available at this time. Both trials used alternative platinum- and fluoropyrimidine-based chemotherapy backbones for the intervention and comparator. In the KEYNOTE-062 study, cisplatin and 5-FU or cisplatin and capecitabine were offered as the chemotherapy backbone for the intervention and comparator, while in the KEYNOTE-859 study, cisplatin and 5-FU or oxaliplatin and capecitabine were offered.
KEYNOTE-06223,38,39
The KEYNOTE-062 study is a phase III, randomized, partially blinded, multi-centre study comparing pembrolizumab as monotherapy and in combination with cisplatin and 5-FU or cisplatin and capecitabine versus placebo in combination with cisplatin and 5-FU or cisplatin and capecitabine as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma. Patients were enrolled into the trial in 200 centres in 29 countries across the Americas (not including Canada), Asia, Africa, Europe, and Oceania.23 Refer to Table 17 for more details.
A total of 1,787 patients were screened, and 763 patients were randomized in a 1:1:1 ratio to receive pembrolizumab as monotherapy (n = 256), pembrolizumab in combination with cisplatin and 5-FU or capecitabine (n = 257), or placebo in combination with cisplatin and 5-FU or capecitabine (n = 250). There were slightly more GEJ patients in the pembrolizumab combination group than the chemotherapy group (33.1% versus 26.8%). It is unknown how many patients overall and in each group were classified as Siewert type I. With regard to the fluoropyrimidine-based chemotherapy, more patients received capecitabine than 5-FU in the pembrolizumab combination group (61.9% versus 38.1%) and the chemotherapy group (62.0% versus 38.0%).23 Refer to Table 1 of the KEYNOTE-062 publication.23 The results represent the final analysis, with a data cut-off date of March 26, 2019. In the overall study population (patients with gastric and GEJ adenocarcinoma), there was no difference in OS between the pembrolizumab combination and chemotherapy groups for patients with PD-L1 with a CPS of 1 or greater (OS HR = 0.85; 95% CI 0.7 to 1.03). The pre-specified OS subgroup analysis of the primary location for GEJ were consistent with the overall study population results (OS HR = 0.96; 95% CI 0.67 to 1.36). It is important to note that the pre-specified OS subgroup analysis of the primary location for GEJ was exploratory, underpowered, and not reflective of the entire reimbursement population, and therefore should be interpreted with caution. In the overall population (patients with gastric and GEJ adenocarcinoma), more AEs leading to discontinuation and immune-mediated AEs and infusion reactions were reported in the pembrolizumab combination group compared to the chemotherapy group (27.6% versus 18.0%, and 24.0% versus 7.8%, respectively).23
Refer to Figure 2C of the KEYNOTE-062 publication23 and Table 2 of the KEYNOTE-062 publication23 for more details.
KEYNOTE-85924,40
The KEYNOTE-859 study is an ongoing phase III, multi-centre study comparing pembrolizumab in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) versus placebo in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma. Patients must be HER2 negative.40 The trial did not include patients with ESCC or adenocarcinoma of the esophagus which is a relevant population for the reimbursement request. Enrolment is ongoing in 33 countries, with 215 study locations in the Americas (including Canada), Asia, Europe, Africa, and Oceania.40,41 Currently, only study design details are available.24 The study is still ongoing, and no results are available at this time.3 Refer to Table 17 for more details.
Table 17: Details of Other Relevant Studies — KEYNOTE-062 and KEYNOTE-859
Criteria | KEYNOTE-062 | KEYNOTE-859 |
|---|---|---|
Designs and populations | ||
Study design | Phase III, multi-centre, partially blinded, 3-arm, RCT | Phase III, multi-centre, double-blind, placebo-controlled RCT |
Locations | 200 centres in 29 countries across the Americas (including not Canada), Asia, Africa, Europe, and Oceania | 215 study locations across the Americas including Canada and US, Asia, Europe, Africa, and Oceania |
Patient enrolment dates | September 18, 2015, to May 26, 2017 | Started: November 8, 2018 Estimated completion date: September 28, 2024 |
Randomized (N) | Planned: 750 Enrolled: 763 (256 in pembrolizumab monotherapy, 257 in pembrolizumab chemotherapy, and 250 in placebo) | Planned: 1,542 Enrolled: NA |
Inclusion criteria | At least 18 years of age Histologically or cytologically confirmed diagnosis of locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma HER2 negative and PD-L1 positive Measurable disease as defined by RECIST 1.1 as determined by investigator assessment ECOG Performance Status of 0 or 1 | At least 18 years of age Histologically or cytologically confirmed diagnosis of locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma HER2 negative Measurable disease as defined by RECIST 1.1 as determined by investigator assessment ECOG Performance S of 0 or 1 Tumour tissue sample deemed adequate for PD-L1 biomarker analysis |
Exclusion criteria | Squamous cell or undifferentiated gastric cancer Received previous therapy for locally advanced, unresectable or metastatic gastric or GEJ cancer Known additional malignancy that is progressing or requires active treatment Known active CNS metastases and/or carcinomatous meningitis Active autoimmune disease that has required systemic treatment in past 2 years Immunodeficient or is receiving chronic systemic steroid therapy or any other form of immunosuppressive therapy within 7 days prior the first dose of trial drug Received prior therapy with an anti-PD-1, anti-PD-L1, or anti-PD-L2 agent Currently or previously participated in a pembrolizumab clinical trial | Squamous cell or undifferentiated gastric cancer Received previous therapy for locally advanced, unresectable or metastatic gastric or GEJ cancer Known additional malignancy that is progressing or requires active treatment Known active CNS metastases and/or carcinomatous meningitis Active autoimmune disease that has required systemic treatment in past 2 years Immunodeficient or is receiving chronic systemic steroid therapy or any other form of immunosuppressive therapy within 7 days prior the first dose of trial drug Received prior therapy with an anti-PD-1, anti-PD-L1, or anti-PD-L2 agent |
Drugs | ||
Intervention | Pembrolizumab: 200 mg IV every 3 weeks OR Pembrolizumab: 200 mg IV every 3 weeks Cisplatin: 80 mg/m2 IV on day 1 every 3 weeks; maximum 6 doses Fluoropyrimidine: 5-FU: 800 mg/m2/day IV for 5 days (4,000 mg/m2 total per cycle) every 3 weeks OR Capecitabine 1,000 mg/m2 (oral) twice per day, for 14 days every 3 weeks | Pembrolizumab: 200 mg IV every 3 weeks Cisplatin: 80mg/m2 IV every 3 weeks; maximum 6 doses 5-FU: 800 mg/m2/day IV for 5 days (4,000 mg/m2 total per cycle) every 3 weeks OR Pembrolizumab: 200 mg IV every 3 weeks Oxaliplatin: 130 mg/m2 IV on day 1 every 3 weeks Capecitabine 1,000 mg/m2 (oral) twice per day, for 14 days every 3 weeks |
Comparator(s) | Placebo: normal saline IV, every 3 weeks Cisplatin: 80 mg/m2 IV on day 1 every 3 weeks; maximum 6 doses 5-FU: 800 mg/m2/day IV for 5 days (4,000 mg/m2 total per cycle) every 3 weeks OR capecitabine 1,000 mg/m2 (oral)twice per day, for 14 days every 3 weeks | Placebo: normal saline IV, every 3 weeks Cisplatin: 80 mg/m2 IV every 3 weeks; maximum 6 doses 5-FU: 800 mg/m2/day IV for 5 days (4,000 mg/m2 total per cycle) every 3 weeks OR Placebo: normal saline IV, every 3 weeks Oxaliplatin: 130 mg/m2 IV on day 1 every 3 weeks Capecitabine 1,000 mg/m2 (oral) twice per day, for 14 days every 3 weeks |
Phase | ||
Run-in | Within 21 days before treatment randomization, potential patients were evaluated to determine if they fulfill the entry requirements. Screening procedures were completed within 21 days before first dose of treatment except for: laboratory tests performed within 10 days before first dose of treatment, evaluation of ECOG performed within 3 days before treatment, or pregnancy test within 72 hours before randomization for women of reproductive potential. | Within 28 days before randomization, initial tumour imaging |
Blinding | Pembrolizumab monotherapy is open label and patient, trial site personnel, sponsor, or designee are not blinded to treatment as only 1 type of treatment is administered. Pembrolizumab combination and placebo combination is blinded to the patient, trial site personnel, and sponsor. | Double blinded (completed details NR) |
Follow-up | Median (range) follow-up: 29.4 (22.0 to 41.3) months | Details NR |
Outcomes | ||
Co-primary end points | Overall survival in patients with PD-L1 CPS ≥ 1 (intention-to-treat population) and PD-L1 CPS of ≥ 10 Progression-free survival per RECIST 1.1 by BICR in patients with PD-L1 CPS of ≥ 1 | Overall survival |
Secondary and exploratory end points | Secondary:
| Secondary:
|
Notes | Re-treatment of pembrolizumab was permitted. Data cut-off date of March 26, 2019. These results represent the final analysis. | Ongoing study, results are not available at this time. Re-treatment of pembrolizumab was permitted. |
Publications | ||
5-FU = 5-fluorouracil; BICR = blinded independent central review; CNS = central nervous system; CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-STO22 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Gastric Cancer Module; GEJ = gatresophageal junction; HER2 = human epidermal growth factor receptor 2; IV = IV; NA = not applicable; NR = not reported; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1; PD-L2 = programmed cell death ligand 2; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: KEYNOTE-062 Publication, Shitara et al. (2020)23 and KEYNOTE-859 Publication, Tabernero et al. (2021).24
Discussion
Summary of Available Evidence
The CADTH clinical review report included input from patient groups, clinical experts, and drug programs, 1pivotal phase III randomized controlled trial, 2 supporting phase III randomized controlled trials, and 1 indirect treatment comparison feasibility assessment report.
The KEYNOTE-590 study is an ongoing phase III, randomized, double-blind, placebo-controlled, multi-centre, superiority study comparing pembrolizumab in combination with cisplatin and 5-FU to placebo in combination with cisplatin and 5-FU for the first-line treatment of patients with locally advanced unresectable or metastatic adenocarcinoma or ESCC or advanced or metastatic Siewert type I adenocarcinoma of the GEJ.
The KEYNOTE-062 study is a phase III, randomized, partially blinded, multi-centre study comparing pembrolizumab as monotherapy and in combination with cisplatin and 5-FU or cisplatin and capecitabine versus placebo in combination with cisplatin and 5-FU or cisplatin and capecitabine as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma.
The KEYNOTE-859 study is an ongoing phase III, multi-centre study comparing pembrolizumab in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) versus placebo in combination with chemotherapy (cisplatin and 5-FU or oxaliplatin and capecitabine) as first-line treatment for patients with advanced gastric or GEJ adenocarcinoma.
No indirect treatment comparisons were included in the sponsor’s submission to CADTH or identified in the literature search; however, the sponsor conducted a feasibility assessment3 of estimating the comparative efficacy and safety of pembrolizumab plus cisplatin and 5-FU versus other competing interventions using data obtained from a systematic literature review.
Interpretation of Results
Efficacy
In Canada, esophageal cancer is ranked 19th among all cancer types based on incidence and 10th based on mortality.8 Esophageal cancer is among 1 of the cancers with a high proportion of metastatic disease (stage IV) at first diagnosis (39.9%),8 with a relative 5-year survival rate for metastatic esophageal cancer of 5%.26 Patient and caregiver respondents expressed the need for have access to new effective therapies that prolong OS, improve QoL, reduce disease symptoms, and have tolerable side effects given the poor and short survival rate for most patients with esophageal cancer.
The clinical experts identified prolonged life and improved HRQoL as the goals of treatment. Similarly, the clinician groups identified prolonged life and improved or maintained HRQoL as the goals of treatment. Delaying progression of disease and ensuring adequate nutritional intake were additional goals of treatment identified by a clinical group.
Both the clinical groups and clinical experts agreed that a clinically meaningful and statistically significant survival benefit in favour of pembrolizumab in combination with cisplatin and 5-FU was observed in the KEYNOTE-590 study for the entire study population, ESCC histology, and PD-L1 with a CPS of 10 or greater. The reported OS and PFS results are deemed “final” based on interim analysis according to pre-specified stopping criteria. However, whether the ”actual” final efficacy results would conform with the interim results is unknown.
Both the clinical groups and clinical experts acknowledged that while patients with PD-L1 with a CPS of 10 or greater, and patients with ESCC with PD-L1 with a CPS of 10 or greater are more likely to respond to pembrolizumab than the ITT population (any PD-L1 CPS and esophageal cancer or GEJ Siewert type I), all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would benefit from pembrolizumab. They agreed that the full patient population in the indication should be eligible for treatment with pembrolizumab (i.e., esophageal cancer and HER2-negative GEJ Siewert type I).
With regards to PROs for the FAS population, the mean change from baseline in global health status/QoL (using the EORTC QLQ-C30 scale) remained stable over time for the pembrolizumab in combination with cisplatin and 5-FU group compared with the placebo in combination with cisplatin and 5-FU group, and the median time to deterioration for global health status/QoL was not reached for both groups. EQ-5D was an exploratory outcome with no minimal important difference reported. Similar least squares mean change from baseline to week 18 in EQ-5D VAS was reported between the 2 groups. Although there was no clinically meaningful deterioration in QoL, there remains uncertainty in PROs and QoL due to the limitations discussed (i.e., missing data, recall bias). However, the magnitude and direction of the impact of these issues on the QoL assessment is unknown. As well, there is a potential risk of bias because of missing data, concomitant medication use, and differential recall bias due to patients’ awareness of treatment assignments as a consequence of drug-related AEs. The clinical experts noted, among other clinically meaningful responses (e.g., improved survival, reduction in severity of symptom, improved QoL), that if the addition of an agent to an established regimen improved survival and was not detrimental to QoL, that would also be considered a clinically meaningful response to treatment. In contrast, clinician groups expressed that a clinically meaningful response to treatments would be a reduction in symptoms or at minimum, a stabilization of symptoms (e.g., less pain, weight gain or cessation of weight loss, less fatigue), as well as an overall improvement in the ability to perform daily activities and a reduction in the caregiver burden.
With regards to investigator-assessed PFS and the protocol amendment to change PFS analysis from BICR to investigator-assessed due to the higher expected discordance rate in the assessment of disease response between investigator and BICR, the clinical experts noted that it is common to see discordance between BICR and investigator assessments in outcomes that have some subjectivity. The clinical experts acknowledged that while it is generally viewed that BICR as the more reliable measurement of response because the trial is blinded, the independent investigators response is still an adequate measure.
Although OS and PFS subgroup analysis results were pre-specified, they are considered exploratory and not powered to detect a difference, except for ESCC (histology and primary tumour site because ESCC was included in the statistical analysis plan); and therefore, should be interpretated with caution. The clinical experts acknowledged that although the possibility of sex differences in immunotherapy response has been highlighted in numerous previous publications,42 they discouraged different treatment recommendations based on sex.
The clinical experts agreed that while it is preferred to have a longer DOR, the 15.8% difference in ORR is a relatively large and a 6.4% complete response rate for the pembrolizumab in combination with cisplatin and 5-FU group was considered to be impressive for metastatic disease.
Of note, the study eligibility included only patients with ECOG 0 or 1, as a result, the benefit and safety profile are unknown in those patients with ECOG greater than 1, in real-world clinical practice who are also likely to receive this combination therapy.
As noted by the clinical experts, standard first-line chemotherapy regimens include a fluoropyrimidine and a platinum (usually cisplatin or oxaliplatin)15-18 for patients with advanced ESCC and HER2-negative patients with EAC or GEJ. Examples of fluoropyrimidine- and platinum-based chemotherapy used in the first-line setting include: cisplatin and 5-FU, capecitabine and cisplatin, CAPOX, and FOLFOX. While the platinum- and fluoropyrimidine-based chemotherapy used in the KEYNOTE-590 study (i.e., cisplatin and 5-FU) represents 1 of the standard of first-line chemotherapies regimens, the clinical experts agreed that CAPOX and FOLFOX should be interchangeable chemotherapy backbones with cisplatin and 5-FU. If the patient is not eligible for cisplatin, carboplatin would be a reasonable substitute, which is consistent with standard practice in multiple cancer sites. The KEYNOTE-062 and KEYNOTE-859 studies used alternative platinum- and fluoropyrimidine-based chemotherapy backbones for the intervention and comparator compared to the KEYNOTE-590 study (cisplatin and 5-FU or cisplatin and capecitabine for KEYNOTE-062 and cisplatin and 5-FU or oxaliplatin and capecitabine for KEYNOTE-859). However, both trials had a mixed population (i.e., all HER2-negative GEJ patients were enrolled without any Siewert classification, whereas only patients with HER2-negative Siewert type I GEJ are of relevance to the reimbursement request) and both trials did not include patients with ESCC or adenocarcinoma of the esophagus, which is a relevant population for the reimbursement request. As well, for KEYNOTE-062, patients must be PD-L1 positive (i.e., CPS ≥ 1), whereas PD-L1 status is not an eligibility criterion for reimbursement in for this submission. Although GEJ subgroup OS analysis results were available for KEYNOTE-062, the results should be interpreted with caution because the GEJ subgroup OS analysis was exploratory, underpowered, and not reflective of the entire reimbursement population.
No indirect treatment comparisons comparing pembrolizumab to other relevant treatments were included in the sponsor’s submission to CADTH or identified in the literature search. The sponsor submitted an indirect treatment comparison feasibility assessment. A critical appraisal of the sponsor’s feasibility study was conducted by CADTH acknowledged that a standard network meta-analysis was not feasible due to lack of network connectivity, and that an unanchored MAIC would likely be biased, and it would not be possible to quantify or identify the direction of the bias.
Harms
The majority of patients in the trial reported treatment-related AEs; however, more discontinuation due to treatment-related AEs was reported in patients in the pembrolizumab in combination with cisplatin and 5-FU group. Many patients experienced grade 3 or greater AEs, and approximately half of the patients in the trial reported a serious AE; however, more serious treatment-related AEs were reported in patients in the pembrolizumab in combination with cisplatin and 5-FU group. More immune-mediated AEs and infusion reactions were reported in the pembrolizumab in combination with cisplatin and 5-FU group and among the AEs of special interest, there were more hypothyroidism, hyperthyroidism, and pneumonitis events reported in the pembrolizumab in combination with cisplatin and 5-FU group.
Overall, the clinical experts agreed that the pembrolizumab in combination with cisplatin and 5-FU toxicity profile appeared to be manageable. The clinical experts noted that monitoring and management of immune-related AEs is required. However, the clinical experts highlighted that serious side effects from PD-1 monotherapy are rare and are well described in previous clinical trials23,35,43; therefore, they felt that the vast majority of patients tolerate these agents well. Although pembrolizumab in combination with cisplatin and 5-FU is a novel combination for the treatment of the indication under review, pembrolizumab is not a novel agent in oncology (i.e., there are various Health Canada–approved indications in oncology) and therefore, AEs and immune-mediated AEs (such as hypothyroidism, hyperthyroidism, pneumonitis, colitis, adrenal insufficiency, hepatitis, hypophysitis, nephritis, and type 1 diabetes mellitus) specific to pembrolizumab are known to clinicians and therefore can be better managed.
Other Considerations
The clinical experts highlighted that pembrolizumab added to chemotherapy is not currently a standard of care in Canada in this patient population. However, they expressed that pembrolizumab added to chemotherapy has the potential to represent a standard of care for patients with esophageal cancer or GEJ Siewert type I. The clinical experts felt that pembrolizumab added to chemotherapy would certainly be a standard of care for patients with ESCC and for patients with a CPS of 10 or greater. The clinical experts also felt that pembrolizumab added to chemotherapy was an appropriate treatment option for patients with GEJ Siewert type I who are HER2 negative, EAC, and for tumours with a CPS of less than 10.
Although ESCC is the most common subtype diagnosed globally, EAC has become more predominant across the Western countries including Canada.10,27 The clinical experts acknowledged that even though EAC is seen more than ESCC in Canada, the KEYNOTE-590 study included both EAC and ESCC, and the benefit of pembrolizumab is seen in the entire population. As a result, the clinical experts emphasized that the full patient population (i.e., esophageal cancer and HER2-negative GEJ Siewert type I) should be eligible for pembrolizumab.
The clinical experts agreed it would be reasonable to permit the addition of pembrolizumab as a time-limited option for patients who have not progressed on first-line therapy. Applicable first-line chemotherapy regimens would include first-line platinum plus fluoropyrimidine, or alternate doublet chemotherapy (e.g., FOLFOX or CAPOX or FOLFIRI) and patients who had completed treatment without progression would also be suitable. The clinical experts agreed that there is no time frame specified as long as there is lack of progression; however, patients should otherwise meet the inclusion criteria for the KEYNOTE-590 study. The clinical experts noted that the population of patients who would fall into this category will be quite small. The clinical experts suggested that as these patients would be started later in therapy, consideration could be made to limit this to patients with tumours that have a PD-L1 with a CPS of 10 or greater.
The clinical experts noted that PD-L1 IHC 22C3 pharmDx is currently the only commercially available PD-L1 test validated for pembrolizumab and that PD-L1 status is not a requirement for reimbursement eligibility.3 While the clinical experts and clinician groups expressed that the full patient population in the indication should be eligible for treatment with the drug under review (i.e., esophageal cancer and HER2-negative GEJ Siewert type I), the clinical experts highlighted that access to PD-L1 CPS testing would be ideal as testing results provide meaningful information for the clinician to discuss the anticipated benefits of treatment with patients and families. The clinician group highlighted, however, that there is currently no routine testing conducted for this, nor is any testing expected in the future.
Reported OS and PFS results are final based on interim analysis. However, the long-term efficacy and safety of pembrolizumab in combination with cisplatin and 5-FU compared to placebo combination with cisplatin and 5-FU is unknown. The study is ongoing and therefore long-term efficacy and safety data are anticipated to be available in the future.
Conclusions
Compared to placebo in combination with cisplatin and 5-FU, first-line treatment with pembrolizumab in combination with cisplatin and 5-FU showed a clinically meaningful and statistically significant overall and PFS benefit in adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ (tumour centre 1 cm to 5 cm above the gastric cardia). While patients with PD-L1 with a CPS of 10 or greater, and ESCC patients with PD-L1 with a CPS of 10 or greater are more likely to respond to pembrolizumab than the ITT population (any PD-L1 CPS and esophageal cancer or GEJ Siewert type I), all patients with esophageal cancers and EGJ adenocarcinomas (Siewert type I) would benefit from pembrolizumab, and as a result, clinicians expressed that the full patient population in the indication (adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the EGJ [tumour centre 1 cm to 5 cm above the gastric cardia]) should be eligible for treatment with pembrolizumab. Discontinuation due to treatment-related AEs, serious treatment-related AEs, and immune-mediated AEs and infusion reactions were more frequently reported in patients treated with pembrolizumab in combination with cisplatin and 5-FU compared to patients treated with placebo in combination with cisplatin and 5-FU. Although there was no clinically meaningful deterioration in QoL, there remains uncertainty in PROs and QoL due to the limitations discussed (i.e., missing data, recall bias). The study is ongoing and therefore long-term efficacy and safety data are anticipated to be available in the future. In addition, study eligibility included only patients with ECOG PS 0 or 1. Therefore, the benefit and safety profile are unknown in those patients with ECOG greater than 1, who, in real-world clinical practice, are also likely to receive this combination therapy.
The platinum- and fluoropyrimidine-based chemotherapy used in the KEYNOTE-590 study (i.e., cisplatin and 5-FU) represents 1 of the standard of first-line chemotherapies regimens. The KEYNOTE-062 and KEYNOTE-859 studies used alternative platinum- and fluoropyrimidine-based chemotherapy backbones for the intervention and comparator compared to the KEYNOTE-590 study (cisplatin and 5-FU or cisplatin and capecitabine for KEYNOTE-062 and cisplatin and 5-FU or oxaliplatin and capecitabine for KEYNOTE-859). However, both trials had a mixed population (i.e., all patients with HER2-negative GEJ were enrolled without any Siewert classification, whereas only patients with HER2-negative Siewert type I GEJ are of relevance to the reimbursement request) and neither trials did included patients with ESCC or adenocarcinoma of the esophagus, which is a relevant population for the reimbursement request. Based on clinical expert opinion, it would be reasonable to use other platinum- and fluoropyrimidine-based chemotherapy backbones apart from cisplatin and 5-FU.
References
1.Clinical Study Report: P590V01MK3475. A randomized, double-blind, placebo-controlled phase III clinical trial of pembrolizumab (MK-3475) in combination with cisplatin and 5-fluorouracil versus placebo in combination with cisplatin and 5-fluorouracil as first-line treatment in subjects with advanced/metastatic esophageal carcinoma (KEYNOTE-590) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme Corp.; 2020.
2.Study Protocol. A randomized, double-blind, placebo-controlled phase III clinical trial of pembrolizumab (MK-3475) in combination with cisplatin and 5-fluorouracil versus placebo in combination with cisplatin and 5-fluorouracil as first-line treatment in subjects with advanced/metastatic esophageal carcinoma (KEYNOTE-590) [internal sponsor's report]. Whitehouse Station (NJ): Merck Sharp & Dohme Corp.; 2020.
3.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [internal sponsor's package]. Kirkland (QC): Merck Canada Inc.; 2021 Jun 8.
4.Health Canada reviewer's report: Keytruda (pembrolizumab) [internal sponsor's report]. Ottawa (ON): Therapeutics Products Directorate, Health Canada; 2021.
5.Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2021.
6.Merck Sharp & Dohme Corp. NCT03189719: first-line esophageal carcinoma study with chemo vs. chemo plus pembrolizumab (MK-3475-590/KEYNOTE-590). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT03189719. Accessed 2021 Jun 30.
7.Sun JM, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759-771. PubMed
8.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2018. Toronto (ON): Canadian Cancer Society; 2018: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2018-canadian-cancer-statistics-special-report/2018-canadian-cancer-statistics-special-report-en.pdf?rev=b253d476a7d24e10aa07233e32d9f204&hash=484A8A4E445DA1E915DC358C0715057F. Accessed 2021 May 25.
9.Canadian Cancer Society. What is esophageal cancer? 2021; https://cancer.ca/en/cancer-information/cancer-types/esophageal/what-is-esophageal-cancer. Accessed 2021 May 25.
10.Cattelan L, Ghazawi FM, Le M, et al. Epidemiologic trends and geographic distribution of esophageal cancer in Canada: A national population-based study. Cancer Medicine. 2020;9(1):401-417. PubMed
11.Jain S, Dhingra S. Pathology of esophageal cancer and Barrett's esophagus. Ann Cardiothorac Surg. 2017;6(2):99-109. PubMed
12.Siewert JR, Stein HJ. Carcinoma of the gastroesophageal junction - classification, pathology and extent of resection. Dis Esophagus. 1996;9(3):173-182.
13.Mayo Clinic. Esophageal cancer: symptoms and causes. 2020; https://www.mayoclinic.org/diseasesconditions/esophageal-cancer/symptoms-causes/syc-20356084. Accessed 2021 Aug 5.
14.Johns Hopkins Sidney Kimmel Comprehensive Cancer Center. Warning signs of esophageal cancer. https://www.hopkinsmedicine.org/kimmel_cancer_center/cancers_we_treat/esophageal_cancer/warning-signs.html. Accessed 2021 Aug 5.
15.Esophageal cancer. Edmonton (AB): Cancer Care Alberta; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gi009-esophageal.pdf. Accessed 2021 Aug 5.
16.BC Cancer Agency. Esophageal and esophagogastric junction. 2013; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-guidelines/gastrointestinal/esophageal-esophagogastric-junction. Accessed 2021 Jun 25.
17.Provincial esophageal cancer and gastro-esophageal junction cancer treatment guidelines. Regina (SK): Saskatchewan Cancer Agency; 2018: http://www.saskcancer.ca/images/pdfs/health_professionals/clinical_resources/clinical_practice_guidelines/upper-gastro_intestinal_cancer/Esophageal%20Cancer%20and%20Gastro-esophageal%20Junction%20Cancer%20Treatment%20Guidelines%20December%202018.pdf. Accessed 2021 Jun 25.
18.Lordick F, Mariette C, Haustermans K, Obermannova R, Arnold D. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27:v50-v57. PubMed
19.Guimbaud R, Louvet C, Ries P, et al. Prospective, randomized, multicenter, phase III study of fluorouracil, leucovorin, and irinotecan versus epirubicin, cisplatin, and capecitabine in advanced gastric adenocarcinoma: a French intergroup (Fédération Francophone de Cancérologie Digestive, Fédération Nationale des Centres de Lutte Contre le Cancer, and Groupe Coopérateur Multidisciplinaire en Oncologie) study. J Clin Oncol. 2014;32(31):3520-3526. PubMed
20.Wilcox RA, Djulbegovic B, Guyatt GH, Montori VM. Randomized trials in oncology stopped early for benefit. J Clin Oncol. 2008;26(1):18-19. PubMed
21.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-1187. PubMed
22.Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. The dangers of stopping trials early. BMJ. 2012;344:e3863. PubMed
23.Shitara K, Van Cutsem E, Bang YJ, et al. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol. 2020;6(10):1571-1580. PubMed
24.Tabernero J, Bang YJ, Van Cutsem E, et al. KEYNOTE-859: a Phase III study of pembrolizumab plus chemotherapy in gastric/gastroesophageal junction adenocarcinoma. Future Oncol. 2021;12:12. PubMed
25.Canadian Cancer Society. Esophageal cancer statistics. 2021; https://cancer.ca/en/cancer-information/cancer-types/esophageal/statistics. Accessed 2021 May 25.
26.Canadian Cancer Society. Survival statistics for esophageal cancer. 2021; https://cancer.ca/en/cancer-information/cancer-types/esophageal/prognosis-and-survival/survival-statistics. Accessed 2021 May 25.
27.Otterstatter MC, Brierley JD, De P, et al. Esophageal cancer in Canada: trends according to morphology and anatomical location. Can J Gastroenterol. 2012;26(10):723-727. PubMed
28.Smyth EC, Lagergren J, Fitzgerald RC, et al. Oesophageal cancer. Nat Rev Dis Primers. 2017;3:17048-17048. PubMed
29.Muro K, Lordick F, Tsushima T, et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic oesophageal cancer: a JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019;30(1):34-43. PubMed
30.Lu Z, Fang Y, Liu C, et al. Early interdisciplinary supportive care in patients with previously untreated metastatic esophagogastric cancer: a phase III randomized controlled trial. J Clin Oncol. 2021;39(7):748-756. PubMed
31.Higginson IJ, Finlay IG, Goodwin DM, et al. Is there evidence that palliative care teams alter end-of-life experiences of patients and their caregivers? J Pain Symptom Manage. 2003;25(2):150-168. PubMed
32.Janmaat VT, Steyerberg EW, van der Gaast A, et al. Palliative chemotherapy and targeted therapies for esophageal and gastroesophageal junction cancer. Cochrane Database Syst Rev. 2017;11(11):CD004063. PubMed
33.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
34.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Jun 24.
35.Kojima T, Shah MA, Muro K, et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 2020;38(35):4138-4148. PubMed
36.Oxaliplatin: 5 mg/mL oxaliplatin 50 mg / 10 mL, 100 mg / 20 mL, 200 mg / 40 mL sterile concentrate for intravenous infusion [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2020: https://pdf.hres.ca/dpd_pm/00057007.PDF. Accessed 2021 Jun 30.
37.Cisplatin injection: sterile solution 1 mg/mL (10 mg, 50 mg, 100 mg cisplatin per vial) [product monograph]. Toronto (ON): Teva Canada Limited; 2016: https://pdf.hres.ca/dpd_pm/00036984.PDF. Accessed 2021 Jun 30.
38.Merck Sharp & Dohme Corp. NCT02494583: Study of pembrolizumab (MK-3475) as first-line monotherapy and combination therapy for treatment of advanced gastric or gastroesophageal junction adenocarcinoma (MK-3475-062/KEYNOTE-062). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2015: https://clinicaltrials.gov/ct2/show/NCT02494583. Accessed 2021 Jun 30.
39.Van Cutsem E, Valderrama A, Bang YJ, et al. Quality of life with first-line pembrolizumab for PD-L1-positive advanced gastric/gastroesophageal junction adenocarcinoma: results from the randomised phase III KEYNOTE-062 study. ESMO Open. 2021;6(4):100189. PubMed
40.Merck Sharp & Dohme Corp. NCT03675737: Pembrolizumab (MK-3475) plus chemotherapy versus placebo plus chemotherapy in participants gastric or gastroesophageal junction (GEJ) adenocarcinoma (MK-3475-859/KEYNOTE-859). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2018: https://clinicaltrials.gov/ct2/show/NCT03675737. Accessed 2021 Jun 30.
41.Tabernero J, Bang YJ, Van Cutsem E, et al. Pembrolizumab plus chemotherapy for previously untreated, HER2-negative unresectable or metastatic advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: KEYNOTE-859. J Clin Oncol. 2021;39(3 Suppl):TPS263-TPS263.
42.Conforti F, Pala L, Bagnardi V, et al. Cancer immunotherapy efficacy and patients' sex: a systematic review and meta-analysis. Lancet Oncol. 2018;19(6):737-746. PubMed
43.Shah MA, Kojima T, Hochhauser D, et al. Efficacy and safety of pembrolizumab for heavily pretreated patients with advanced, metastatic adenocarcinoma or squamous cell carcinoma of the esophagus: the phase 2 KEYNOTE-180 study. JAMA Oncol. 2019;5(4):546-550. PubMed
44.Kato K, Shah M, Enzinger P, et al. A phase 3 study of chemotherapy + pembrolizumab versus chemotherapy + placebo as first-line therapy for patients with advanced esophageal or esophagogastric junction (E/EGJ) cancer: KEYNOTE-590 - Trial in progress. Ann Oncol. 2018;29(Supplement 5):v14-v15.
45.Wang H, Xuan TT, Chen Y, et al. Investigative therapy for advanced esophageal cancer using the option for combined immunotherapy and chemotherapy. Immunotherapy. 2020;12(10):697-703. PubMed
46.McCaw ZR, Ludmir EB, Wei LJ. Quantifying the long-term survival benefit of pembrolizumab for patients with advanced gastric cancer. JAMA Oncol. 2021;7(4):632-633. PubMed
47.Minami H, Kiyota N, Omori T. Did the randomized phase III KEYNOTE-181 study of pembrolizumab for esophageal cancer yield negative or positive results? J Clin Oncol. 2021:JCO2003262. PubMed
48.Nakamagoe K, Yamada T, Okune S, Moriwaki T, Tamaoka A. Fisher syndrome as an immune-related adverse event after using pembrolizumab but not nivolumab. Acta Neurol Belg. 2021;28:28. PubMed
49.Alsina M, Smyth EC. Safety and preliminary signs of efficacy with the combination of pembrolizumab plus oxaliplatin and S-1 in Japanese gastric cancer patients. Ann Transl Med. 2020;8(24):1696. PubMed
50.Narita Y, Kadowaki S, Muro K. Immune checkpoint inhibitor plus anti-HER2 therapy: a new standard for HER2-positive oesophagogastric cancer? Lancet Oncol. 2020;21(6):741-743. PubMed
51.Anonymous. Pembrolizumab (Keytruda) for cancers with biomarkers. Med Lett Drugs Ther. 2018;60(1537):e8-e9. PubMed
52.Lemery S, Keegan P, Pazdur R. First FDA approval agnostic of cancer site - When a biomarker defines the indication. N Engl J Med. 2017;377(15):1409-1412. PubMed
53.Aprile G, Silvestris N, Antonuzzo L, Scartozzi M. Metastatic gastric cancer in the last two decades: goals achieved and future promises. Future Oncol. 2015;11(19):2633-2636. PubMed
54.Gil Z, Billan S. Pembrolizumab-chemotherapy for advanced oesophageal cancer. Lancet. 2021;398(10302):726-727. PubMed
55.Landre T, Des Guetz G, Chouahnia K, Fossey-Diaz V, Culine S. Immune checkpoint inhibitors for patients aged >= 75 years with advanced cancer in first- and second-line settings: a meta-analysis. Drugs Aging. 2020;37(10):747-754. PubMed
56.Tabernero J, Van Cutsem E, Bang Y, et al. Pembrolizumab with or without chemotherapy versus chemotherapy for first-line treatment of advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: The Phase 3 KEYNOTE-062 Study. Ann Oncol. 2019;30(Supplement 4):iv152-iv153.
57.Tabernero J, Van Cutsem E, Bang Y-J, et al. Pembrolizumab with or without chemotherapy versus chemotherapy for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: The phase III KEYNOTE-062 study. J Clin Oncol. 2019;37(18 Suppl):LBA4007-LBA4007.
58.Alakus H, Bruns C. Pembrolizumab for advanced esophageal carcinoma. [German]. Onkologe. 2018;24(1):76-78.
59.Shah MA, Bennouna J, Doi T, et al. KEYNOTE-975: A randomized, double-blind, placebo-controlled phase 3 trial of pembrolizumab vs placebo in participants with esophageal carcinoma receiving concurrent definitive chemoradiotherapy. Cancer Res. 2020;80(16 Suppl):CT282.
60.Kojima T, Muro K, Francois E, et al. Pembrolizumab versus chemotherapy as second-line therapy for advanced esophageal cancer: Phase III KEYNOTE-181 study. J Clin Oncol. 2019;37(4 Suppl):2-2.
61.Bang YJ, Kang YK, Catenacci DV, et al. Pembrolizumab alone or in combination with chemotherapy as first-line therapy for patients with advanced gastric or gastroesophageal junction adenocarcinoma: results from the phase II nonrandomized KEYNOTE-059 study. Gastric Cancer. 2019;22(4):828-837. PubMed
62.Shah MA, Kojima T, Enzinger PC, et al. Pembrolizumab for patients with previously treated metastatic adenocarcinoma or squamous cell carcinoma of the esophagus: Phase 2 KEYNOTE-180 study. J Clin Oncol. 2018;36(15 Suppl):4049-4049.
63.Mansoor W, Kulkarni AS, Kato K, et al. Health-related quality of life (HRQoL) of pembrolizumab plus chemotherapy versus chemotherapy as first-line therapyin patients with advanced esophageal cancer: The phase III KEYNOTE-590 study. J Clin Oncol. 2021;39(3 Suppl):168-168.
64.Aschenbrenner DS. New esophageal cancer indication for pembrolizumab. Am J Nurs. 2019;119(11):21. PubMed
65.Kato K, Shah MA, Enzinger P, et al. KEYNOTE-590: Phase III study of first-line chemotherapy with or without pembrolizumab for advanced esophageal cancer. Future Oncol. 2019;15(10):1057-1066. PubMed
66.Akyala AI, Verhaar AP, Peppelenbosch MP. Immune checkpoint inhibition in gastric cancer: A systematic review. J Cellular Immunotherapy. 2018;4(2):49-55.
67.European Organisation for Research and Treatment of Cancer (EORTC). EORTC Quality of Life. Questionnaires. Brussels (BE): EORTC: https://qol.eortc.org/questionnaires/. Accessed 2021 Jul 8.
68.Braun DP, Gupta D, Grutsch JF, Staren ED. Can changes in health related quality of life scores predict survival in stages III and IV colorectal cancer? Health Qual Life Outcomes. 2011;9(1):62. PubMed
69.Snyder CF, Blackford AL, Sussman J, et al. Identifying changes in scores on the EORTC-QLQ-C30 representing a change in patients' supportive care needs. Qual Life Res. 2015;24(5):1207-1216. PubMed
70.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
71.Dai Z, Lang W, Yang H, et al. Validation of EORTC QLQ-OES18 for Chinese patients with esophageal cancer. Dis Esophagus. 2017;30(10):1-7. PubMed
72.EuroQol Research Foundation. EQ-5D-5L: about. 2017; https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/. Accessed 2021 Jul 8.
73.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
74.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
75.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
76.European Organisation for Research Treatment of Cancer (EORTC). EORTC Quality of Life. FAQ. https://qol.eortc.org/faq/. Accessed 2021 May 25.
77.European Organisation for Research Treatment of Cancer (EORTC). EORTC QLQ-C30 scoring manual. Brussels (BE): EORTC; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf?bcs-agent-scanner=e1284245-c178-0a43-a29d-2949b50384ee. Accessed 2021 Jul 8.
78.Brunelli C, Mosconi P, Boeri P, et al. Evaluation of quality of life in patients with malignant dysphagia. Tumori. 2000;86(2):134-138. PubMed
79.Huang CC, Lien HH, Sung YC, Liu HT, Chie WC. Quality of life of patients with gastric cancer in Taiwan: validation and clinical application of the Taiwan Chinese version of the EORTC QLQ-C30 and EORTC QLQ-STO22. Psychooncology. 2007;16(10):945-949. PubMed
80.Onate-Ocana LF, Velazquez-Monroy N, Vazquez L, et al. Clinical validation of the EORTC QLQ-OG25 questionnaire for the evaluation of health-related quality of life in Mexican patients with esophagogastric cancers. Psychooncology. 2012;21(7):745-753. PubMed
81.Tomaszewski KA, Puskulluoglu M, Biesiada K, Bochenek J, Nieckula J, Krzemieniecki K. Validation of the polish version of the eortc QLQ-C30 and the QLQ-OG25 for the assessment of health-related quality of life in patients with esophagi-gastric cancer. J Psychosoc Oncol. 2013;31(2):191-203. PubMed
82.Oñate-Ocaña LF, Alcántara-Pilar A, Vilar-Compte D, et al. Validation of the Mexican Spanish version of the EORTC C30 and STO22 questionnaires for the evaluation of health-related quality of life in patients with gastric cancer. Ann Surg Oncol. 2009;16(1):88-95. PubMed
83.King MT. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res. 1996;5(6):555-567. PubMed
84.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
85.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
86.Bjordal K, de Graeff A, Fayers PM, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. 2000;36(14):1796-1807. PubMed
87.Blazeby JM, Conroy T, Hammerlid E, et al. Clinical and psychometric validation of an EORTC questionnaire module, the EORTC QLQ-OES18, to assess quality of life in patients with oesophageal cancer. Eur J Cancer. 2003;39(10):1384-1394. PubMed
88.European Organisation for Research Treatment of Cancer (EORTC). EORTC Quality of Life. Oesophageal. https://qol.eortc.org/questionnaire/qlq-oes18/. Accessed 2021 Jul 8.
89.Chie WC, Tsai CJ, Chiang C, Lee YC. Quality of life of patients with oesophageal cancer in Taiwan: validation and application of the Taiwan Chinese (Mandarin) version of the EORTC QLQ-OES18: a brief communication. Qual Life Res. 2010;19(8):1127-1131. PubMed
90.Forootan M, Tabatabaeefar M, Maghsoodi N, Ardeshiri M, Fatemi M, Rahimzadeh H. Adaptation of a quality of life questionnaire for Iranian patients with esophageal cancer. Indian J Palliat Care. 2014;20(2):123-127. PubMed
91.Fujita T, Okada N, Sato T, Mayanagi S, Kanamori J, Daiko H. Translation, validation of the EORTC esophageal cancer quality-of-life questionnaire for Japanese with esophageal squamous cell carcinoma: analysis in thoraco-laparoscopic esophagectomy versus open esophagectomy. Jpn J Clin Oncol. 2016;46(7):615-621. PubMed
92.EQ-5D-5L user guide. Rotterdam (NL): EuroQol Research Foundation; 2021: https://euroqol.org/publications/user-guides/. Accessed 2021 Jul 8.
93.Lorenzen S, Schuster T, Porschen R, et al. Cetuximab plus cisplatin-5-fluorouracil versus cisplatin-5-fluorouracil alone in first-line metastatic squamous cell carcinoma of the esophagus: a randomized phase II study of the Arbeitsgemeinschaft Internistische Onkologie. Ann Oncol. 2009;20(10):1667-1673. PubMed
94.Moehler M, Maderer A, Thuss-Patience PC, et al. Cisplatin and 5-fluorouracil with or without epidermal growth factor receptor inhibition panitumumab for patients with non-resectable, advanced or metastatic oesophageal squamous cell cancer: a prospective, open-label, randomised phase III AIO/EORTC trial (POWER). Ann Oncol. 2020;31(2):228-235. PubMed
95.Moehler MH, Thuss-Patience PC, Brenner B, et al. Cisplatin/5-FU (CF) +/− panitumumab (P) for patients (pts) with non-resectable, advanced, or metastatic esophageal squamous cell cancer (ESCC): An open-label, randomized AIO/TTD/BDGO/EORTC phase III trial (POWER). J Clin Oncol. 2017;35(15 Suppl):4011-4011.
96.Ross P, Nicolson M, Cunningham D, et al. Prospective randomized trial comparing mitomycin, cisplatin, and protracted venous-infusion fluorouracil (PVI 5-FU) With epirubicin, cisplatin, and PVI 5-FU in advanced esophagogastric cancer. J Clin Oncol. 2002;20(8):1996-2004. PubMed
97.Cleary JM, Horick NK, McCleary NJ, et al. FOLFOX plus ziv-aflibercept or placebo in first-line metastatic esophagogastric adenocarcinoma: A double-blind, randomized, multicenter phase 2 trial. Cancer. 2019;125(13):2213-2221. PubMed
98.Yoon HH, Bendell JC, Braiteh FS, et al. Ramucirumab combined with FOLFOX as front-line therapy for advanced esophageal, gastroesophageal junction, or gastric adenocarcinoma: a randomized, double-blind, multicenter Phase II trial. Ann Oncol. 2016;27(12):2196-2203. PubMed
99.Gong J, Zhang X, Lu M, et al. Efficacy of paclitaxel plus cisplatin in advanced esophageal squamous cell cancer: Further analysis of single center, prospective study. J Clin Oncol. 2013;31(15 Suppl):e15174-e15174.
100.Li YH, Jiang W, Wang F, et al. Efficacy and safety of rhLTα-Da with cisplatin and fluorouracil in patients with metastatic esophageal squamous cell carcinoma: A randomized, multicenter, open-labelled, controlled, phase IIb trial. J Clin Oncol. 2016;34(15 Suppl):4036-4036.
101.Bristol-Myers Squibb. NCT03143153: A study to evaluate efficacy in subjects with esophageal cancer treated with nivolumab and ipilimumab or nivolumab combined with fluorouracil plus cisplatin versus fluorouracil plus cisplatin (CheckMate 648). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/results/NCT03143153. Accessed 2021 Jul 15.
102.Bristol-Myers Squibb. NCT02872116: Efficacy study of nivolumab plus ipilimumab or nivolumab plus chemotherapy against chemotherapy in stomach cancer or stomach/esophagus junction cancer (CheckMate649). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/record/NCT02872116. Accessed 2021 Jul 15.
103.Lee SJ, Kim S, Kim M, et al. Capecitabine in combination with either cisplatin or weekly paclitaxel as a first-line treatment for metastatic esophageal squamous cell carcinoma: a randomized phase II study. BMC Cancer. 2015;15(1):693. PubMed
104.Hironaka S, Tsubosa Y, Mizusawa J, et al. Phase I/II trial of 2-weekly docetaxel combined with cisplatin plus fluorouracil in metastatic esophageal cancer (JCOG0807). Cancer Sci. 2014;105(9):1189-1195. PubMed
105.Wolff K, Wein A, Reulbach U, et al. Weekly high-dose 5-fluorouracil as a 24-h infusion and sodium folinic acid (AIO regimen) plus irinotecan in patients with locally advanced nonresectable and metastatic adenocarcinoma or squamous cell carcinoma of the oesophagus: a phase II trial. Anticancer Drugs. 2009;20(3):165-173. PubMed
106.Ojima T, Nakamori M, Nakamura M, et al. Phase I/II study of divided-dose docetaxel, cisplatin and fluorouracil for patients with recurrent or metastatic squamous cell carcinoma of the esophagus. Dis Esophagus. 2017;30(2):1-7. PubMed
107.Huang J, Zhou Y, Zhang H, et al. A phase II study of biweekly paclitaxel and cisplatin chemotherapy for recurrent or metastatic esophageal squamous cell carcinoma: ERCC1 expression predicts response to chemotherapy. Med Oncol. 2012;30(1):343. PubMed
108.Tamura S, Imano M, Takiuchi H, et al. Phase II study of docetaxel, cisplatin and 5-fluorouracil (DCF) for metastatic esophageal cancer (OGSG 0403). Anticancer Res. 2012;32(4):1403-1408. PubMed
109.Kim JY, Do YR, Park KU, et al. A multi-center phase II study of docetaxel plus cisplatin as first-line therapy in patients with metastatic squamous cell esophageal cancer. Cancer Chemother Pharmacol. 2010;66(1):31-36. PubMed
110.Tanaka Y, Yoshida K, Sanada Y, Osada S, Yamaguchi K, Takahashi T. Biweekly docetaxel, cisplatin, and 5-fluorouracil (DCF) chemotherapy for advanced esophageal squamous cell carcinoma: a phase I dose-escalation study. Cancer Chemother Pharmacol. 2010;66(6):1159-1165. PubMed
111.Rossman JF, Falkson CI, Xu R, et al. Phase II trial of docetaxel and carboplatin in patients with advanced squamous carcinoma of the esophagus (E2298): a trial of the Eastern Cooperative Oncology Group. Gastrointest Cancer Res. 2011;4(1):9-14. PubMed
112.Osaka Y, Shinohara M, Hoshino S, et al. Phase II study of combined chemotherapy with docetaxel, CDDP and 5-FU for highly advanced esophageal cancer. Anticancer Res. 2011;31(2):633-638. PubMed
113.Zhang X, Shen L, Li J, Li Y, Li J, Jin M. A phase II trial of paclitaxel and cisplatin in patients with advanced squamous-cell carcinoma of the esophagus. Am J Clin Oncol. 2008;31(1):29-33. PubMed
114.Takahashi H, Arimura Y, Yamashita K, et al. Phase I/II study of docetaxel/cisplatin/fluorouracil combination chemotherapy against metastatic esophageal squamous cell carcinoma. J Thorac Oncol. 2010;5(1):122-128. PubMed
115.Lee J, Im YH, Cho EY, et al. A phase II study of capecitabine and cisplatin (XP) as first-line chemotherapy in patients with advanced esophageal squamous cell carcinoma. Cancer Chemother Pharmacol. 2008;62(1):77-84. PubMed
116.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2021 May 26.
117.Seruga B, Ocana A, Amir E, Tannock IF. Failures in phase III: causes and consequences. Clin Cancer Res. 2015;21(20):4552-4560. PubMed
118.22 case studies where phase 2 and phase 3 trials had divergent results. Silver Spring (MD): U.S. Food and Drug Administration; 2017: https://www.fda.gov/media/102332/download. Accessed 2021 Jun 15.
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 21, 2021
Alerts: Biweekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits: Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,ot,kf,hw,rn,nm.
exp Esophageal Neoplasms/
((esophag* or oesophag* or gastroesophag* or GE junction* or EG junction* or GEJ or EGJ or upper gastr* or upper GI or gastric*) adj5 (cancer* or neoplas* or tumo?r* or carcinoma* or adenocarcinoma* or squamous or malignan* or metast*)).ti,ab,kf.
2 or 3
1 and 4
5 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kw,dq.
7 or 8
esophagus tumour/ or exp esophagus cancer/
((esophag* or oesophag* or gastroesophag* or GE junction* or EG junction* or GEJ or EGJ or upper gastr* or upper GI or gastric*) adj5 (cancer* or neoplas* or tumo?r* or carcinoma* or adenocarcinoma* or squamous or malignan* or metast*)).ti,ab,kw,dq.
10 or 11
9 and 12
13 not (conference abstract or conference review).pt.
14 use oemezd
6 or 15
remove duplicates from 16
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Keytruda OR pembrolizumab OR lambrolizumab | esophageal OR gastroesophageal OR oesophageal OR esophagogastric]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – Keytruda, pembrolizumab, esophageal, oesophageal, gastroesophageal, esophagogastric]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – Keytruda, pembrolizumab]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Keytruda, pembrolizumab, esophageal, oesophageal, gastroesophageal, esophagogastric]
Grey Literature
Search dates: June 17, 2021 – June 22, 2021
Keywords: Keytruda, pembrolizumab, lambrolizumab, esophageal, oesophageal, gastroesophageal, esophagogastric, oesophagogastric
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Reference | Reason for exclusion |
|---|---|
Abstract, No Outcomes Reported, Preceded Unpublished Manuscript | |
Case Report | |
Duplicate | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Editorial/Letter/Commentary/Correspondence | |
Meta-Analysis | |
Mixed Population | |
Mixed Population | |
Mixed Population, Abstract, Preceded Full Publication | |
Mixed Population, Abstract, Preceded Full Publication | |
Not relevant intervention | |
Not relevant intervention | |
Not Relevant Population, Not Relevant Intervention | |
Not Relevant Population, Not Relevant Intervention | |
Not Relevant Population, Not Relevant Intervention | |
Not Study Design | |
Not Study Design, Not Relevant Population, Not Relevant Intervention | |
Not Study Design, Not Relevant Population, Not Relevant Intervention | |
Poster, Study Design, No Outcomes Reported, Mixed Population | |
Presentation, Not Relevant Intervention | |
Presentation, Preceded unpublished manuscript | |
Presentation, Preceded Unpublished Manuscript | |
Review Article | |
Study Design, No Outcomes Reported, Mixed Population | |
Study Design, No Outcomes Reported, Mixed Population | |
Study design, No Outcomes Reported, Preceded unpublished manuscript | |
Study Design, No Outcomes Reported, Preceded Unpublished Manuscript | |
Systematic Review |
Note: This table has not been copy-edited.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 20: Summary of Exposure to Treatment by Regimen Component, Safety Population
Number of cycles | Pembrolizumab in combination with cisplatin and 5-FU (N=370) | Placebo in combination with cisplatin and 5-FU (N=370) | ||||
|---|---|---|---|---|---|---|
Pembrolizumab | Cisplatin | 5-FU | Placebo | Cisplatin | 5-FU | |
≥1 | 370 (100.0) | 369 (99.7) | 370 (100.0) | 370 (100.0) | 370 (100.0) | 370 (100.0) |
≥2 | 339 (91.6) | 335 (90.5) | 337 (91.1) | 337 (91.1) | 331 (89.5) | 333 (90.0) |
≥3 | 321 (86.8) | 314 (84.9) | 316 (85.4) | 317 (85.7) | 312 (84.3) | 314 (84.9) |
≥4 | 292 (78.9) | 282 (76.2) | 289 (78.1) | 285 (77.0) | 274 (74.1) | 282 (76.2) |
≥5 | 267 (72.2) | 245 (66.2) | 262 (70.8) | 265 (71.6) | 241 (65.1) | 260 (70.3) |
≥6 | 240 (64.9) | 206 (55.7) | 232 (62.7) | 235 (63.5) | 205 (55.4) | 227 (61.4) |
≥7 | 213 (57.6) | 0 (0.0) | 138 (37.7) | 204 (55.1) | 0 (0.0) | 135 (36.5) |
≥8 | 194 (52.4) | 0 (0.0) | 126 (34.1) | 176 (47.6) | 0 (0.0) | 116 (31.4) |
≥9 | 175 (47.3) | 0 (0.0) | 107 (28.9) | 139 (37.6) | 0 (0.0) | 94 (25.4) |
≥10 | 143 (38.6) | 0 (0.0) | 84 (22.7) | 111 (30.0) | 0 (0.0) | 75(20.3) |
≥11 | 132 (35.7) | 0 (0.0) | 74 (20.0) | 97 (26.2) | 0 (0.0) | 68 (18.4) |
≥12 | 116 (31.4) | 0 (0.0) | 62 (16.8) | 86 (23.2) | 0 (0.0) | 60 (16.2) |
≥13 | 105 (28.4) | 0 (0.0) | 54 (14.6) | 72 (19.5) | 0 (0.0) | 48 (13.0) |
≥14 | 96 (25.9) | 0 (0.0) | 50 (13.5) | 59 (15.9) | 0 (0.0) | 36 (9.7) |
≥15 | 88 (23.8) | 0 (0.0) | 43 (11.6) | 53 (14.3) | 0 (0.0) | 32 (8.6) |
≥16 | 82 (22.2) | 0 (0.0) | 39 (10.5) | 42 (11.4) | 0 (0.0) | 25 (6.8) |
≥17 | 80 (21.6) | 0 (0.0) | 38 (10.3) | 40 (10.8) | 0 (0.0) | 23 (6.2) |
≥18 | 76 (20.5) | 0 (0.0) | 38 (10.3) | 35 (9.5) | 0 (0.0) | 19 (5.1) |
≥19 | 70 (18.9) | 0 (0.0) | 36 (9.7) | 26 (7.0) | 0 (0.0) | 13 (3.5) |
≥20 | 66 (17.8) | 0 (0.0) | 33 (8.9) | 26 (7.0) | 0 (0.0) | 12 (3.2) |
≥21 | 57 (15.4) | 0 (0.0) | 28 (7.6) | 21 (5.7) | 0 (0.0) | 10 (2.7) |
≥22 | 52 (14.1) | 0 (0.0) | 25 (6.8) | 21 (5.7) | 0 (0.0) | 10 (2.7) |
≥23 | 50 (13.5) | 0 (0.0) | 24 (6.5) | 18 (4.9) | 0 (0.0) | 8 (2.2) |
≥24 | 48 (13.0) | 0 (0.0) | 23 (6.2) | 17 (4.6) | 0 (0.0) | 8 (2.2) |
≥25 | 45 (12.2) | 0 (0.0) | 21 (5.7) | 12 (3.2) | 0 (0.0) | 6 (1.6) |
≥26 | 45 (12.2) | 0 (0.0) | 19 (5.1) | 9 (2.4) | 0 (0.0) | 5 (1.4) |
≥27 | 41 (11.1) | 0 (0.0) | 17 (4.6) | 8 (2.2) | 0 (0.0) | 5 (1.4) |
≥28 | 38 (10.3) | 0 (0.0) | 16 (4.3) | 6 (1.6) | 0 (0.0) | 4 (1.1) |
≥29 | 34 (9.2) | 0 (0.0) | 16 (4.3) | 5 (1.4) | 0 (0.0) | 4 (1.1) |
≥30 | 30 (8.1) | 0 (0.0) | 13 (3.5) | 5 (1.4) | 0 (0.0) | 4 (1.1) |
≥31 | 28 (7.6) | 0 (0.0) | 13 (3.5) | 5 (1.4) | 0 (0.0) | 4 (1.1) |
≥32 | 22 (5.9) | 0 (0.0) | 9 (2.4) | 4 (1.1) | 0 (0.0) | 3 (0.8) |
≥33 | 18 (4.9) | 0 (0.0) | 9 (2.4) | 4 (1.1) | 0 (0.0) | 3 (0.8) |
≥34 | 15 (4.1) | 0 (0.0) | 8 (2.2) | 2 (0.5) | 0 (0.0) | 2 (0.5) |
=35 | 14 (3.8) | 0 (0.0) | 8 (2.2) | 2 (0.5) | 0 (0.0) | 2 (0.5) |
Mean (SD) | 10.8 (9.3) | 4.7 (1.7) | 8.0 (7.2) | 8.4 (6.4) | 4.7 (1.8) | 7.1 (5.4) |
Median (Range) | 8 (1-35) | 6.0 (1-6) | 6.0 (1-35) | 7.0 (1-35) | 6.0 (1-6) | 6.0 (1-35) |
5-FU = 5-fluorouracil, SD = standard deviation.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Table 21: Prior Types of Medication
Prior medications | KEYNOTE-590 | |
|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU (N=370) | Placebo in combination with cisplatin and 5-FU (N=370) | |
No prior medications | 19 (5.1) | 22 (5.9) |
One or more prior medications | 351 (94.9) | 348 (94.1) |
Antiemetics and antinauseants | 164 (44.3) | 171 (46.2) |
Drugs for acid related disorders | 199 (53.8) | 213 (57.6) |
Drugs for constipation | 58 (15.7) | 51 (13.8) |
Drugs for functional gastrointestinal disorders | 65 (17.6) | 77 (20.8) |
Drugs for functional gastrointestinal disorders | 65 (17.6) | 77 (20.8) |
Mineral supplements | 69 (18.6) | 71 (19.2) |
Blood substitutes and perfusion solutions | 142 (38.4) | 136 (36.8) |
Calcium channel blockers | 37 (10.0) | 51 (13.8) |
Diuretics | 48 (13.0) | 48 (13.0) |
Analgesics | 177 (47.8) | 163 (44.1) |
Anesthetics | 41 (11.1) | 37 (10.0) |
Psycholeptics | 93 (25.1) | 88 (23.8) |
Corticosteroids for systemic use | 136 (36.8) | 135 (36.5) |
Thyroid therapy | 27 (7.3) | 25 (6.8) |
A5-FU = 5-fluorouracil.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Table 22: Concomitant Medication
Concomitant medications* | KEYNOTE-590 | ||
|---|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU (N=370) | Placebo in combination with cisplatin and 5-FU (N=370) | Total (N=740) | |
Antidiarrheals, intestinal anti-inflammatory/anti-infective agents | 98 (26.5) | 91 (24.6) | 189 (25.5) |
Antiemetics and antinauseants | 353 (95.4) | 360 (97.3) | 713 (96.4) |
Bile and liver therapy | 14 (3.8) | 9 (2.4) | 23 (3.1) |
Digestives, including enzymes | 11 (3.0) | 11 (3.0) | 22 (3.0) |
Drugs for acid related disorders | 327 (88.4) | 334 (90.3) | 661 (89.3) |
Drugs for constipation | 207 (55.9) | 182 (49.2) | 389 (52.6) |
Drugs for functional gastrointestinal disorders | 264 (71.4) | 273 (73.8) | 537 (72.6) |
Drugs for diabetes | 50 (13.5) | 58 (15.7) | 108 (14.6) |
Minerals supplements | 225 (60.8) | 210 (56.8) | 435 (58.8) |
Other alimentary tract and metabolism products | 34 (9.2) | 27 (7.3) | 61 (8.2) |
Stomatological preparations | 37 (10.0) | 37 (10.0) | 74 (10.0) |
Vitamins | 114 (30.8) | 106 (28.6) | 220 (29.7) |
Anti-bacterials for systemic use | 203 (54.9) | 204 (55.1) | 407 (55.0) |
Antimycotics for systemic use | 31 (8.4) | 30 (8.1) | 61 (8,2) |
Antivirals for systemic use | 15 (4.1) | 24 (6.5) | 39 (5.3) |
Endocrine therapy | 39 (10.5) | 35 (9.5) | 74 (10.0) |
Immunostimulants | 116 (31.4) | 132 (35.7) | 248 (33.5) |
Anti-anemic preparations | 78 (21.1) | 62 (16.8) | 140 (18.9) |
Antihemorrhagics | 39 (10.5) | 49 (13.2) | 88 (11.9) |
Antithrombotic agents | 116 (31.4) | 96 (25.9) | 212 (28.6) |
Blood substitutes and perfusion solutions | 322 (87.0) | 309 (83.5) | 631 (85.3) |
Agents acting on the renin-angiotensin system | 79 (21.4) | 84 (22.7) | 163 (22.0) |
Beta blocking agents | 50 (13.5) | 42 (11.4) | 92 (12.4) |
Calcium channel blockers | 62 (16.8) | 75 (20.3) | 137 (18.5) |
Cardiac therapy | 40 (10.8) | 45 (12.2) | 85 (11.5) |
Diuretics | 190 (51.4) | 180 (48.6) | 370 (50.0) |
Lipid modifying agents | 61 (16.5) | 68 (18.4) | 129 (17.4) |
Vasoprotectives | 33 (8.9) | 21 (5.7) | 54 (7.3) |
Antifungals for dermatological use | 52 (14.1) | 46 (12.4) | 98 (13.2) |
Antiseptics and disinfectants | 46 (12.4) | 38 (10.3) | 84 (11.4) |
Corticosteroids, dermatological preparations | 66 (17.8) | 43 (11.6) | 109 (14.7) |
Emollients and protectives | 38 (10.3) | 20 (5.4) | 58 (7.8) |
Urologicals | 23 (6.2) | 28 (7.6) | 51 (6.9) |
Anti-inflammatory and antirheumatic products | 151 (40.8) | 150 (40.5) | 301 (40.7) |
Drugs for treatment of bone diseases | 24 (6.5) | 19 (5.1) | 43 (5.8) |
Muscle relaxants | 31 (8.4) | 38 (10.3) | 69 (9.3) |
Analgesics | 262 (70.8) | 261 (70.5) | 523 (70.7) |
Anesthetics | 90 (24.3) | 67 (18.1) | 157 (21.2) |
Antiepileptics | 59 (15.9) | 71 (19.2) | 130 (17.6) |
Psychoanaleptics | 56 (15.1) | 35 (9.5) | 91 (12.3) |
Psycholeptics | 218 (58.9) | 201 (54.3) | 419 (56.6) |
Antihistamines for systemic use | 129 (34.9) | 140 (37.8) | 269 (36.4) |
Cough and cold preparations | 110 (29.7) | 92 (24.9) | 202 (27.3) |
Drugs for obstructive airway diseases | 71 (19.2) | 60 (16.2) | 131 (17.7) |
Ophthalmologicals | 28 (7.6) | 19 (5.1) | 47 (6.4) |
Corticosteroids for systemic use | 340 (91.9) | 328 (88.6) | 668 (90.3) |
Thyroid therapy | 54 (14.6) | 44 (11.9) | 98 (13.2) |
5-FU = 5-fluorouracil.
Note: Data cut-off date was July 2, 2020.
*Concomitant medications with an incidence ≤ 5% in one or more treatment groups.
Source: Clinical Study Report.1
Table 23: Summary of Interim and Final Analyses Strategy in KEYNOTE-590
Analyses | Key end points | Timing | Estimated time after first patient randomized | Primary purpose of analysis |
|---|---|---|---|---|
Interim | PFS in ESCC PFS in PD-L1 CPS≥10 PFS in all patients OS in ESCC with PD-L1 CPS≥10 OS in ESCC OS in PD-L1 CPS≥10 OS in all patients | (1) Enrolment is complete with a minimum follow-up of 13 months and (2) ~ 460 investigator assessed PFS events have been observed in ESCC and (3) ~391 deaths have occurred in ESCC. At this time ~200 deaths are expected to have occurred in ESCC with PD-L1 CPS≥10 and ~ 267 deaths are expected to have occurred in PD-L1 CPS≥10 | ~35 months | Final PFS analysis Interim OS analysis |
Final | OS in ESCC with PD-L1 CPS≥10 OS in PD-L1 CPS≥10 OS in ESCC OS in all patients | (1) A minimum follow-up of 9 months after interim analysis and (2) ~233 deaths have occurred in ESCC with PD-L1 CPS≥10 and (3) ~ 455 deaths have occurred in ESCC. At this time ~311 deaths are expected to have occurred in PDL1 CPS≥10 | ~44 months | Final OS analysis |
CPS = combined positive score; ESCC = esophageal squamous cell carcinoma; PD-L1 = programmed death ligand 1; PFS = progression-free survival; OS = overall survival.
Source: Clinical Study Report.1
Table 24: Statistical Analysis of Efficacy End Points in KEYNOTE-590
End point | Statistical model | Adjustment factors | Censoring | Sensitivity or exploratory analyses |
|---|---|---|---|---|
KEYNOTE-590 | ||||
Overall survival |
| Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Censored at patient’s last known alive date | Exploratory analyses to adjust for the effect of crossover to other PD-1 therapies |
Progression-free survival |
| Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Three censoring scenarios:
|
|
Objective response rate | Stratified Miettinen and Nurminen method (for comparison of ORR) with strata weighting by sample size | Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Patients with missing data are considered non-responders | Sensitivity analysis using RECIST 1.1 by BICR |
Duration of response | Non-parametric Kaplan-Meier method | Only patients who achieved CR or PR are included | Three censoring scenarios:
| Sensitivity analysis using RECIST 1.1 by BICR |
EORTC QLQ-C30 |
| Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Two censoring scenarios for time to deterioration:
| None |
QLQ-OES18 |
| Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Two censoring scenarios for time to deterioration:
| None |
ED-5D-5L (descriptive system and VAS) |
| Stratified by geographic region (Asia, rest of world), histology (adenocarcinoma, squamous cell carcinoma), ECOG Performance Status (0, 1) | Two censoring scenarios for time to deterioration:
| None |
BICR = Blinded independent central review; CR = complete response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core Module; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Module; EQ-5D-5L = EQ-5D 5-Level; HR = hazard ratio; ITT = intent to treat; ORR = objective response rate; OS = overall survival; PD = progressive disease; PD-1 = Programmed cell death protein 1; PFS = progression-free survival; PR = partial response; PRO = patient-reported outcome; irRECIST = immune-related Response Evaluation Criteria in Solid Tumors; VAS = visual analogue scale.
Source: Clinical Study Report.1
Figure 18: Forest Plot of Overall Survival Hazard Ratio by Subgroup Factor. Efficacy (ITT) Population
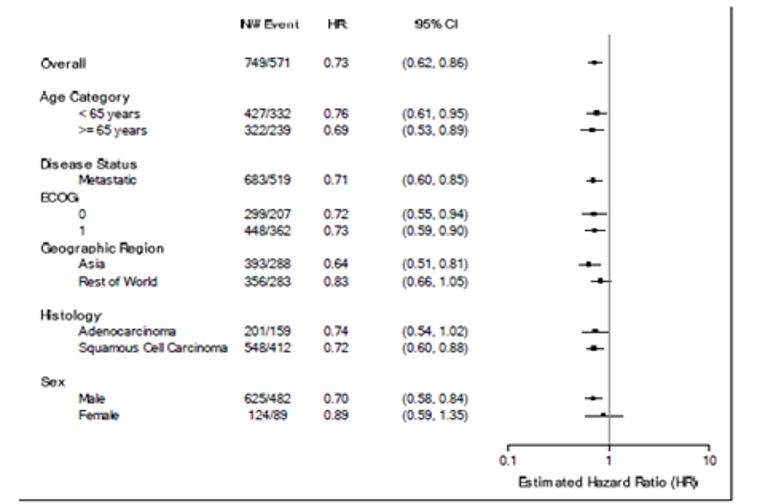
CI = confidence interval, ECOG = Eastern Cooperative Oncology Group, HR = hazard ratio; ITT = intent to treat
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Figure 19: Forest Plot of PFS Hazard Ratio by Subgroup Factor Based on Investigator Assessment per RECIST 1.1, ITT Population
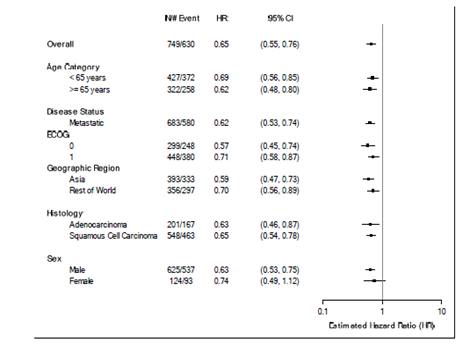
CI = confidence interval, ECOG = Eastern Cooperative Oncology Group, HR = hazard ratio; ITT = intent to treat.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Table 25: Objective Response Rate and Duration of Response for Patients With ESCC and PD-L1 CPS of 10 or Greater, Patients with ESCC, and Patients with PD-L1 CPS of 10 or Greater, ITT Population
Outcomes | Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU |
|---|---|---|
Objective response rate, investigator assessment per RECIST 1.1 – Patients with ESCC and PD-L1 CPS ≥10 | ||
Number of Responses, n/N (%) | 73/143 (51.0) | 40/143 (28.0) |
Complete Response, n (%) | 10 (7.0) | 3 (2.1) |
Partial Response, n (%) | 63 (44.1) | 37 (25.9) |
Stable Disease, n (%) | 43 (30.1) | 69 (48.3) |
Progressive Disease, n (%) | 16 (11.2) | 20 (14.0) |
Could not be evaluated, n (%) | 2 (1.4) | 0 (0.0) |
No Assessment, n (%) | 9 (6.3) | 14 (9.8) |
Overall Response Rate, % (95% CI) | 51.0 (42.6, 59.5) | 28.0 (20.8, 36.1) |
Difference in Overall Response Rate between pembrolizumab and placebo (95% CI), P value | 22.8 (11.6, 33.4), P <0.0001 | |
Objective response rate, investigator assessment per RECIST 1.1 – Patients with ESCC | ||
Number of Responses, n/N (%) | 120/274 (43.8) | 85/274 (31.0) |
Complete Response, n (%) | 21 (7.7) | 4 (1.5) |
Partial Response, n (%) | 99 (36.1) | 81 (29.6) |
Stable Disease, n (%) | 97 (35.4) | 126 (46.0) |
Progressive Disease, n (%) | 32 (11.7) | 39 (14.2) |
Could not be evaluated, n (%) | 3 (1.1) | 0 (0.0) |
No Assessment, n (%) | 22 (8.0) | 24 (8.8) |
Overall Response Rate, % (95% CI) | 43.8 (37.8, 49.9) | 31.0 (25.6, 36.9) |
Difference in Overall Response Rate between pembrolizumab and placebo (95% CI), P value | 12.8 (4.7, 20.7), P= 0.0009 | |
Objective response rate, investigator assessment per RECIST 1.1 – Patients with PD-L1 CPS ≥10 | ||
Number of Responses, n/N (%) | 95/186 (51.1) | 53/197 (26.9) |
Complete Response, n (%) | 11 (5.9) | 5 (2.5) |
Partial Response, n (%) | 84 (45.2) | 48 (24.4) |
Stable Disease, n (%) | 55 (29.6) | 98 (49.7) |
Progressive Disease, n (%) | 21 (11.3) | 27 (13.7) |
Could not be evaluated, n (%) | 3 (1.6) | 1 (0.5) |
No Assessment, n (%) | 12 (6.5) | 18 (9.1) |
Overall Response Rate, % (95% CI) | 51.1 (43.7, 58.5) | 26.9 (20.8, 33.7) |
Difference in Overall Response Rate between pembrolizumab and placebo (95% CI), P value | 24.0 (14.3, 33.2), P <0.0001 | |
Duration of response, investigator assessment per RECIST 1.1 in Patients with Confirmed Response – Patients with ESCC and PD-L1 CPS ≥10 | ||
Number of patients with response, n/N (%)† | 73/143 (51.0) | 40/143 (28.0) |
Response duration (months), median (min, max)‡ | 10.4 (2.2+ - 28.9+) | 4.4 (1.5+ - 25.0+) |
Duration of response, investigator assessment per RECIST 1.1 Patients with Confirmed Response – Patients whose tumours are PD-L1 CPS ≥10 | ||
Number of patients with response, n/N (%)† | 95/186 (51.1) | 53/197 (26.9) |
Response duration (months), median (min, max)‡ | 10.4 (1.9 - 28.9+) | 5.6 (1.5+ - 25.0+) |
Duration of response, investigator assessment per RECIST 1.1 Patients with Confirmed Response – Patients with ESCC | ||
Number of patients with response, n/N (%)† | 120/274 (43.8) | 85/274 (31.0) |
Response duration (months), median (min, max)‡ | 9.1 (1.2+ - 31.0+) | 6.1 (1.5+ - 25.0+) |
CPS = combined positive score; ESCC = esophageal squamous cell carcinoma; ITT = intention to treat; LS = least square; PD-L1 = programmed death ligand 1; RECIST = Response Evaluation Criteria in Solid Tumors; 5-FU = 5-fluorouracil.
Data cut-off date: July 2, 2020
†Includes patients with confirmed complete response or partial response.
‡From product-limit (Kaplan-Meier) method for censored data.
"+" indicates there is no progressive disease by the time of last disease assessment.
Data cut-off date: July 2, 2020
Source: Clinical Study Report1
Table 26: Patient-Reported Outcomes for Patients With ESCC and PD-L1 CPS of 10 or Greater, Patients With ESCC, and Patients With PD-L1 CPS of 10 or Greater, FAS Population
Patient-reported outcome | Pembrolizumab in combination with cisplatin and 5-FU | Placebo in combination with cisplatin and 5-FU | |
|---|---|---|---|
EQ-5D VAS - Patients with ESCC and PD-L1 CPS ≥10, FAS Population | |||
Change from Baseline to week 18, LS mean (95% CI)^ | -4.46 (-7.94, -0.97) | -4.35 (-8.06, -0.65) | |
Difference in LS Means (95% CI), P value^ | -0.10 (-4.96, 4.76), 0.9668 | ||
EQ-5D VAS - Patients with ESCC, FAS Population | |||
Change from Baseline to week 18, LS mean (95% CI)^ | -3.78 (-6.19, -1.38) | -3.47 (-5.97, -0.97) | |
Difference in LS Means (95% CI), P value^ | -0.31 (-3.64, 3.01), 0.8532 | ||
EQ-5D VAS - Patients with PD-L1 CPS ≥10, FAS Population | |||
Change from Baseline to week 18, LS mean (95% CI)* | -3.38 (-6.42, -0.35) | -3.78 (-6.87, -0.69) | |
Difference in LS Means (95% CI), P value* | 0.40 (-3.70, 4.49), 0.8490 | ||
EORTC QLQ-C30 Global Health, Patients with ESCC and PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 47/130 (36.2), (27.9, 45.0) | 35/130 (26.9), (19.5, 35.4) | |
Stable, n/N (%), (95 CI%†) | 54/130 (41.5), (33.0, 50.5) | 48/130 (36.9), (28.6, 45.8) | |
Improved + Stable, n/N (%), (95 CI%†) | 101/130 (77.7), (69.6, 84.5) | 83/130 (63.8), (55.0, 72.1) | |
Deteriorated, n/N (%), (95 CI%†) | 29/130 (22.3), (15.5, 30.4) | 47/130 (36.2), (27.9, 45.0) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 9.5 (-1.8, 20.7), 0.0498 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 13.3 (2.2, 24.2), 0 .0097 | ||
EORTC QLQ-C30 Global Health, ESCC, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 86/251 (34.3), (28.4, 40.5) | 68/249 (27. 3), (21.9, 33.3) | |
Stable, n/N (%), (95 CI%†) | 105/251 (41.8), (35.7, 48.2) | 104/249 (41.8), (35.6, 48.2) | |
Improved + Stable, n/N (%), (95 CI%†) | 191/251 (76.1), (70.3, 81.2) | 172/249 (69.1), (62.9, 74.8) | |
Deteriorated, n/N (%), (95 CI%†) | 60/251 (23.9), (18.8, 29.7) | 77/249 (30.9), (25. 2, 37.1) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 6.8 (-1.3, 14.8), 0.0503 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 7.0 (-0.8, 14.8), 0.0402 | ||
EORTC QLQ-C30 Global Health, PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 63/170 (37.1), (29.8, 44.8) | 49/174 (28.2), (21.6, 35.5) | |
Stable, n/N (%), (95 CI%†) | 68/170 (40.0), (32.6, 47.8) | 67/174 (38.5), (31.2, 46.2) | |
Improved + Stable, n/N (%), (9 5CI%†) | 131/170 (77.1), (70.0, 83.1) | 116/174 (66.7), (59.1, 73.6) | |
Deteriorated, n/N (%), (95 CI%†) | 39/170 (22.9), (16.9, 30.0) | 58/174 (33.3), (26.4, 40.9) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 8.7 (-1.2, 18.5), 0.0420 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 10.4 (0.8, 19.8), 0.0167 | ||
EORTC QLQ-OES18 Dysphagia, ESCC and PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 67/129 (51.9), (43.0, 60.8) | 43/127 (33.9), (25. 7, 42.8) | |
Stable, n/N (%), (95 CI%†) | 32/129 (24.8), (17.6, 33.2) | 46/127 (36.2), (27.9, 45.2) | |
Improved + Stable, n/N (%), (95 CI%†) | 99/129 (76.7), (68.5, 83.7) | 89/127 (70.1), (61.3, 77.9) | |
Deteriorated, n/N (%), (95 CI%†) | 30/129 (23.3), (16.3, 31.5) | 38/127 (29.9), (22.1, 38.7) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 19.0 (7.0, 30.5), 0.0011 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 6.9 (-3.8, 17.4), 0.1017 | ||
EORTC QLQ-OES18 Pain, ESCC and PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 48/129 (37.2), (28.9, 46.2) | 38/127 (29.9), (22.1, 38.7) | |
Stable, n/N (%), (95 CI%†) | 60/129 (46.5), (37.7, 55.5) | 56/127 (44.1), (35.3, 53.2) | |
Improved + Stable, n/N (%), (95 CI%†) | 108/129 (83.7), (76.2, 89.6) | 94/127 (74.0), (65.5, 81.4) | |
Deteriorated, n/N (%), (95 CI%†) | 21/129 (16.3), (10.4, 23.8) | 33/127 (26.0), (18.6, 34.5) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 5.6 (-5.5, 16.8), 0.1597 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 9.2 (-0.9, 19.3), 0.0370 | ||
EORTC QLQ-OES18 Reflux, ESCC and PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 34/129 (26.4), (19.0, 34.8) | 33/127 (26.0), (18.6, 34.5) | |
Stable, n/N (%), (95 CI%†) | 70/129 (54.3), (45.3, 63.1) | 66/127 (52.0), (42.9, 60.9) | |
Improved + Stable, n/N (%), (95 CI%†) | 104/129 (80.6), (72.7, 87.0) | 99/127 (78.0), (69.7, 84.8) | |
Deteriorated, n/N (%), (95 CI%†) | 25/129 (19.4), (13.0, 27.3) | 28/127 (22.0), (15.2, 30.3) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | -0.7 (-11.4, 10.1), 0.5487 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 2.7 (-7.3, 12.7), 0.2947 | ||
EORTC QLQ-OES18 Dysphagia, ESCC, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 121/249 (48.6), (42.2, 55.0) | 104/246 (42.3), (36.0, 48.7) | |
Stable, n/N (%), (95 CI%†) | 61/249 (24.5), (19.3, 30.3) | 77/246 (31.3), (25.6, 37. 5) | |
Improved + Stable, n/N (%), (95 CI%†) | 182/249 (73.1), (67.1, 78.5) | 181/246 (73.6), (67.6, 79.0) | |
Deteriorated, n/N (%), (95 CI%†) | 67/249 (26.9), (21.5, 32.9) | 65/246 (26.4), (21.0, 32.4) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 6.2 (-2.6, 14.9), 0.0833 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | -0.5 (-8.2, 7.2), 0.5469 | ||
EORTC QLQ-OES18 Pain, ESCC, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 97/249 (39.0), (32.9, 45.3) | 86/246 (35.0), (29.0, 41.3) | |
Stable, n/N (%), (95 CI%†) | 109/249 (43.8), (37.5, 50.2) | 106/246 (43.1), (36.8, 49.5) | |
Improved + Stable, n/N (%), (95 CI%†) | 206/249 (82.7), (77.5, 87.2) | 192/246 (78.0), (72.3, 83.1) | |
Deteriorated, n/N (%), (95 CI%†) | 43/249 (17.3), (12.8, 22.5) | 54/246 (22.0), (16.9, 27.7) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 3.9 (-4.4, 12.2), 0.1766 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 4.7 (-2.3, 11.7), 0.0938 | ||
EORTC QLQ-OES18 Reflux, ESCC, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 70/249 (28.1), (22.6, 34.1) | 68/246 (27.6), (22.2, 33.7) | |
Stable, n/N (%), (95 CI%†) | 131/249 (52.6), (46.2, 58.9) | 127/246 (51.6), (45.2, 58.0) | |
Improved + Stable, n/N (%), (95 CI%†) | 201/249 (80.7), (75.3, 85.4) | 195/246 (79.3), (73.7, 84.2) | |
Deteriorated, n/N (%), (95 CI%†) | 48/249 (19.3), (14.6, 24.7) | 51/246 (20.7), (15.8, 26.3) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 0.1 (-7.7, 8.0), 0.4877 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 1.2 (-5.9, 8.2), 0.3692 | ||
EORTC QLQ-OES18 Dysphagia, PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 82/169 (48.5), (40.8, 56.3) | 60/169 (35.5), (28.3, 43.2) | |
Stable, n/N (%), (95 CI%†) | 40/169 (23.7), (17.5, 30.8) | 59/169 (34.9), (27.8, 42.6) | |
Improved + Stable, n/N (%), (95 CI%†) | 122/169 (72.2), (64.8, 78.8) | 119/169 (70.4), (62.9, 77.2) | |
Deteriorated, n/N (%), (95 CI%†) | 47/169 (27.8), (21.2, 35.2) | 50/169 (29.6), (22.8, 37.1) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 13.2 (2.7, 23.5), 0.0071 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 2.1 (-7.5, 11.6), 0.3309 | ||
EORTC QLQ-OES18 Pain, PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 69/169 (40.8), (33.3, 48.6) | 56/169 (33.1), (26.1, 40.8) | |
Stable, n/N (%), (95 CI%†) | 71/169 (42.0), (34.5, 49.8) | 73/169 (43.2), (35.6, 51.0) | |
Improved + Stable, n/N (%), (95 CI%†) | 140/169 (82.8), (76.3, 88.2) | 129/169 (76.3), (69.2, 82.5) | |
Deteriorated, n/N (%), (95 CI%†) | 29/169 (17.2), (11.8, 23.7) | 40/169 (23.7), (17.5, 30.8) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 7.1 (-2.9, 16.9), 0.0820 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 6.5 (-2.2, 15.2), 0.0701 | ||
EORTC QLQ-OES18 Reflux, PD-L1 CPS ≥10, FAS Population | |||
Improved, n/N (%), (95 CI%†) | 52/169 (30.8), (23.9, 38.3) | 44/169 (26.0), (19.6, 33.3) | |
Stable, n/N (%), (95 CI%†) | 83/169 (49.1), (41.4, 56.9) | 89/169 (52.7), (44.9, 60.4) | |
Improved + Stable, n/N (%), (95 CI%†) | 135/169 (79.9), (73.0, 85.6) | 133/169 (78.7), (71.7, 84.6) | |
Deteriorated, n/N (%), (95 CI%†) | 34/169 (20.1), (14.4, 27.0) | 36/169 (21.3), (15.4, 28.3) | |
Difference in % Improved, Estimate (95 CI%)‡, P value § | 4.5 (-5.1, 14.0), 0.1802 | ||
Difference in % Improved + Stable, Estimate (95 CI%)‡, P value § | 1.4 (-7.4, 10.1), 0.3775 | ||
CI = confidence interval; CPS = combined positive score; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core Module; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Module; FAS = Full Analysis Set; PD-L1 = Programmed cell death 1 ligand 1; 5-FU = 5-fluorouracil.
Note: Data cut-off date: July 2, 2020.
*Based on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors geographic region (Asia, rest of the world) and tumour histology (Adenocarcinoma, Squamous Cell Carcinoma) and ECOG Performance Status (0, 1).
^Based on a cLDA model with the PRO scores as the response variable with covariates for treatment by study visit interaction, stratification factors geographic region (Asia, rest of the world) and ECOG Performance Status (0, 1)
†Based on binomial exact CI method.
‡Based on Miettinen & Nurminen method with population-based weighting stratified by strata. If there are 0 subjects in one of the Treatment/sequence in a comparison for a particular stratum, then strata are combined as specified in the sSAP to ensure sufficient number of subjects in each stratum.
§One-sided P value for testing. H0: difference in % = 0 versus H1: difference in % > 0.
Improved defined as a 10 point or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by a 10 point or more improvement at a visit scheduled at least 6 weeks later.
Overall improvement/stability defined as the composite of improvement and stability. Stability is defined as, when the criteria for improvement are not met, a less than 10 points worsening in score from baseline at any time during the study and confirmed by a less than 10 points worsening at a visit scheduled at least 6 weeks later.
Source: Clinical Study Report.1
EORTC QLQ-C30 Global Health Status/QoL
Figure 20: Change From Baseline and 95% CI for the EORTC QLQ-C30 Global Health Status and QoL Over Time by Treatment Group, ESCC With PD-L1 CPS of 10 or Greater, FAS Population
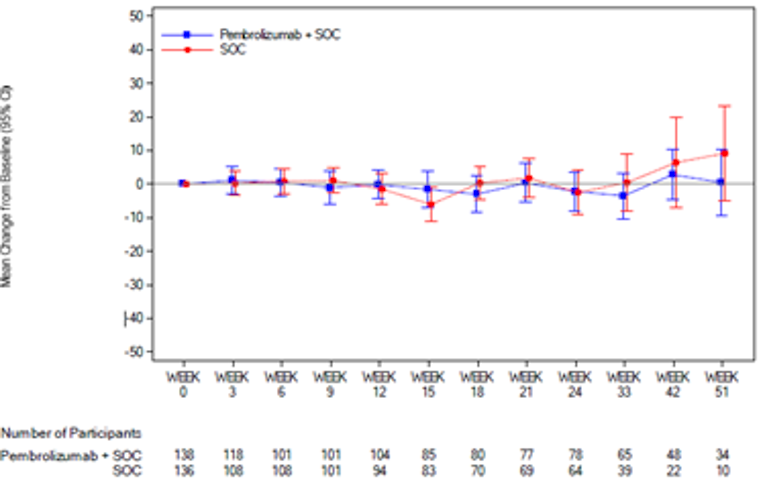
Figure 21: Change From Baseline and 95% CI for the EORTC QLQ-C30 Global Health Status and QoL Over Time by Treatment Group, ESCC, FAS Population
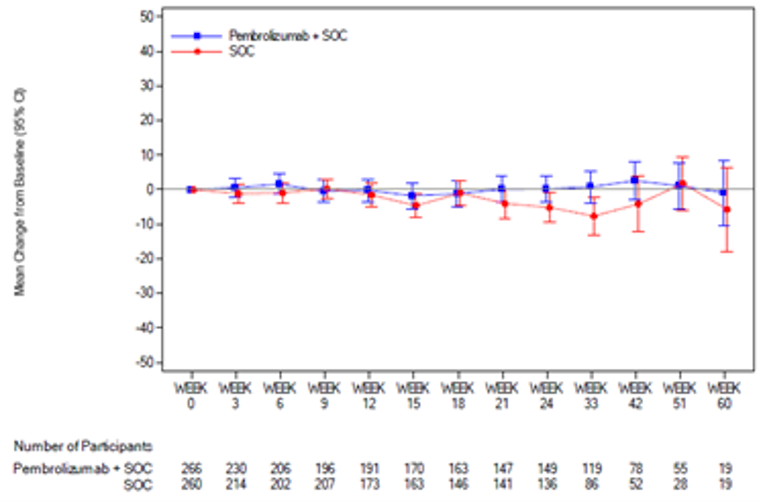
Figure 22: Change From Baseline and 95% CI for the EORTC QLQ-C30 Global Health Status and QoL Over Time by Treatment Group, PD-L1 CPS of 10 or Greater, FAS Population
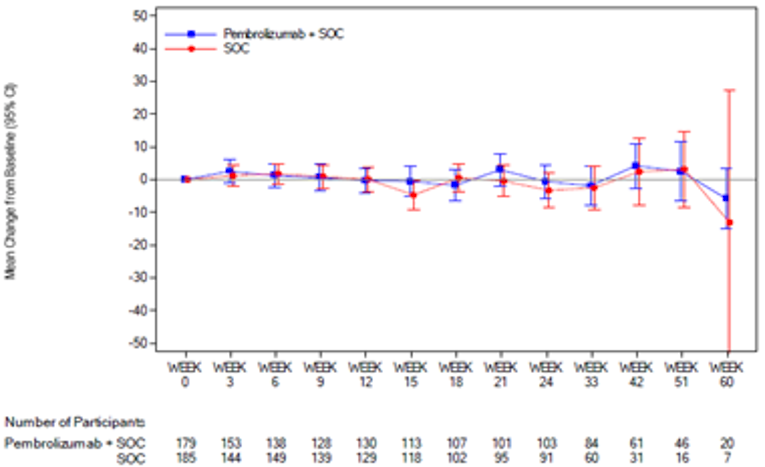
Figure 23: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-C30 Global Health, ESCC, and PD-L1 CPS or 10 or Greater, FAS Population With Baseline
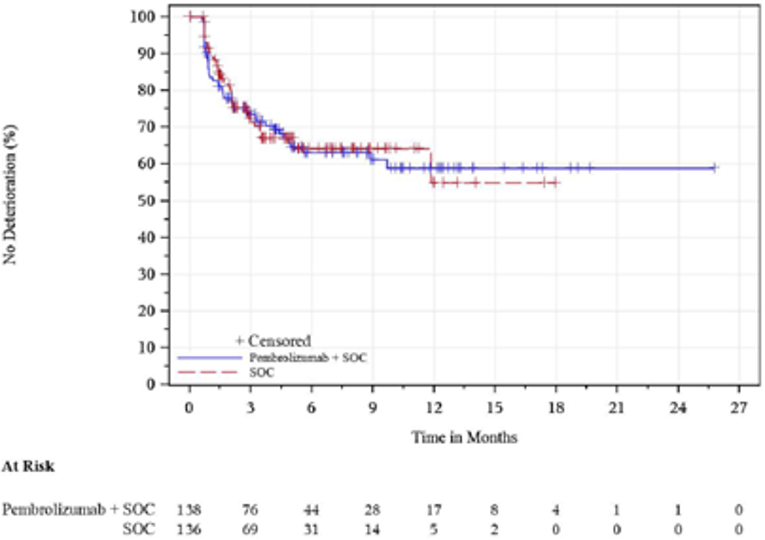
Figure 24: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-C30 Global Health Status and QoL, ESCC FAS Population With Baseline
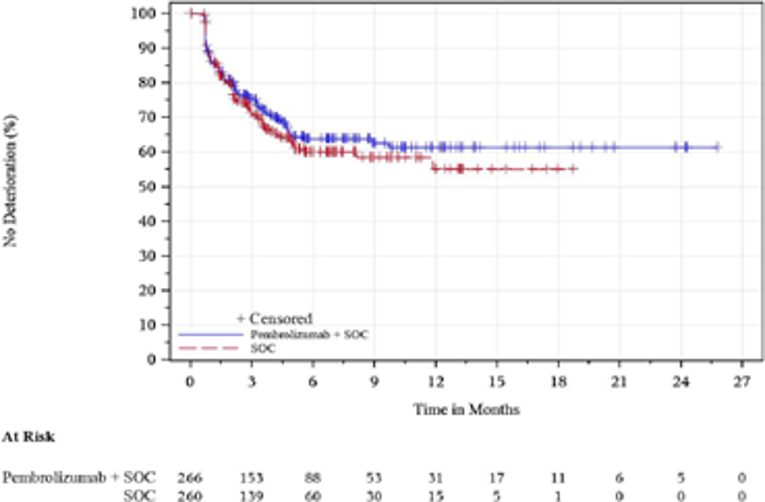
Figure 25: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-C30 Global Health Status and QoL, PD-L1 CPS of 10 or Greater, FAS Population With Baseline
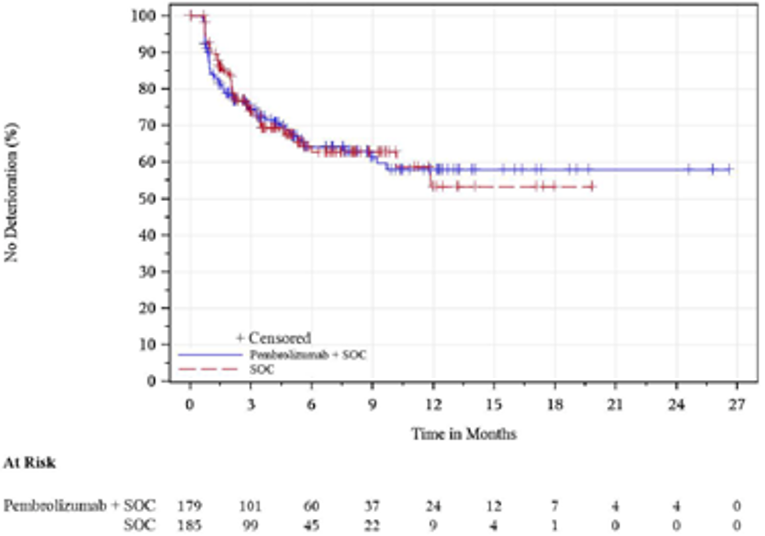
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core Module; ESCC = Esophageal squamous cell carcinoma; FAS = Full Analysis Set; PD-L1 = Programmed cell death 1 ligand 1; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumors; Pembrolizumab + SOC = Pembrolizumab in combination with cisplatin and 5-FU; SOC = Placebo in combination with cisplatin and 5-FU; 5-FU = 5-fluorouracil.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
EORTC QLQ OES-18
Figure 26: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Dysphagia Over Time by Treatment Group, ESCC With PD-L1 CPS of 10 or Greater, FAS Population
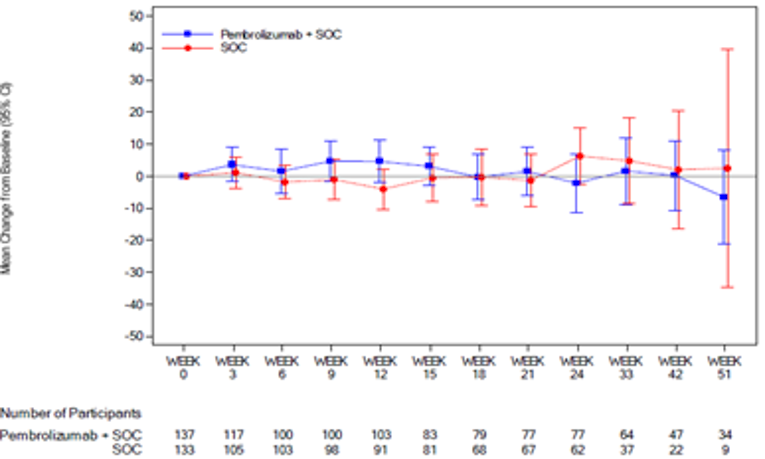
Figure 27: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Pain Over Time by Treatment Group, ESCC With PD-L1 CPS of 10 or Greater, FAS Population
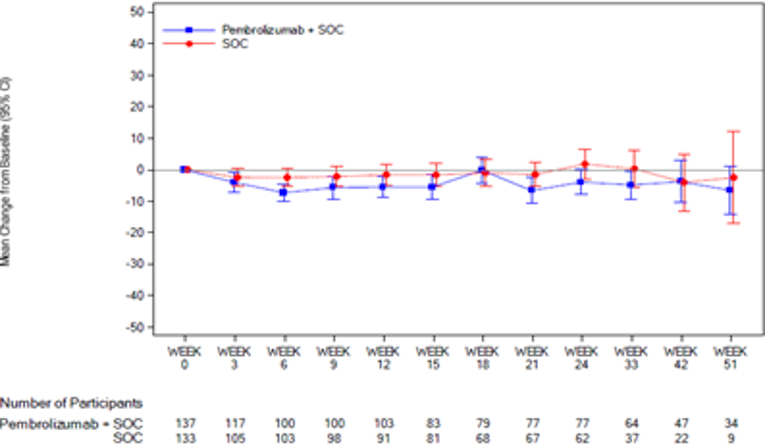
Figure 28: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Reflux Over Time by Treatment Group, ESCC With PD-L1 CPS of 10 or Greater, FAS Population
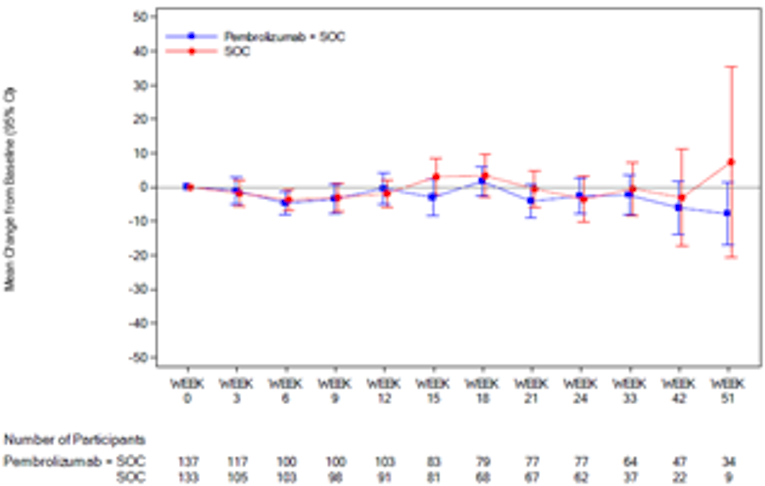
Figure 29: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Dysphagia Over Time by Treatment Group, ESCC, FAS Population
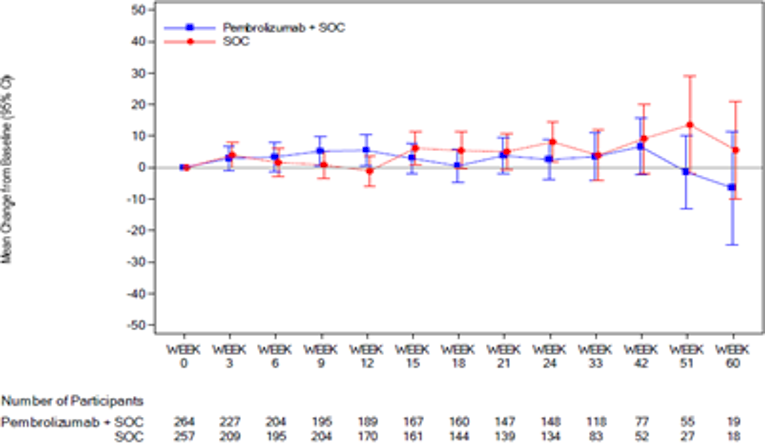
Figure 30: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Pain Over Time by Treatment Group, ESCC, FAS Population
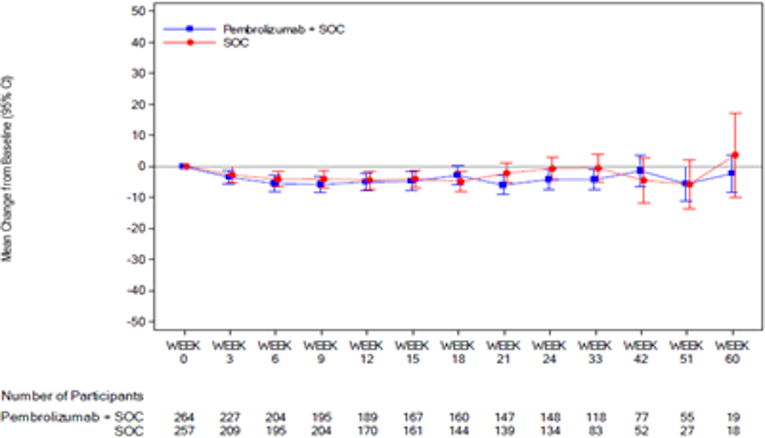
Figure 31: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Reflux Over Time by Treatment Group, ESCC, FAS Population
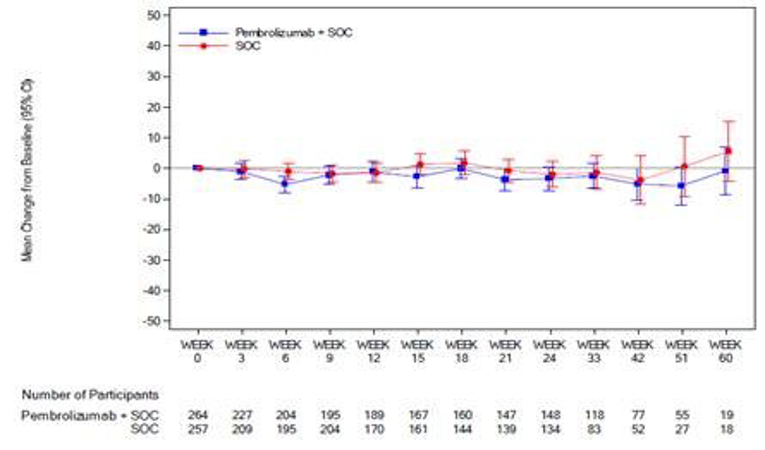
Figure 32: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Dysphagia Over Time, PD-L1 CPS of 10 or Greater, FAS Population
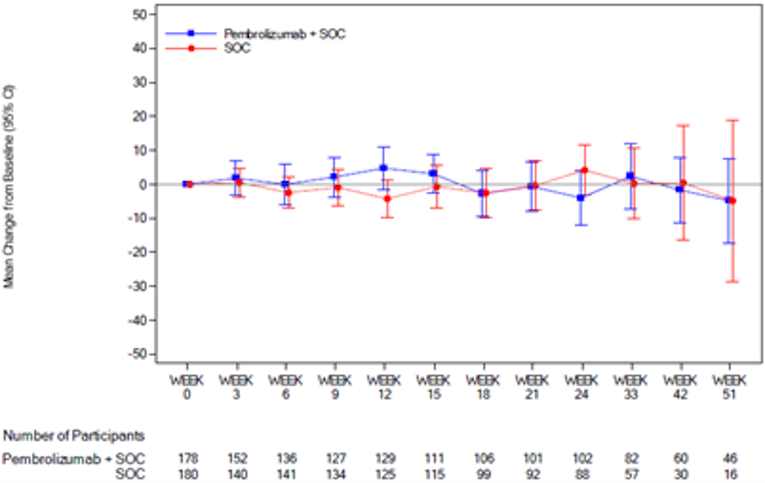
Figure 33: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Pain Over Time, PD-L1 CPS of 10 or Greater, FAS Population
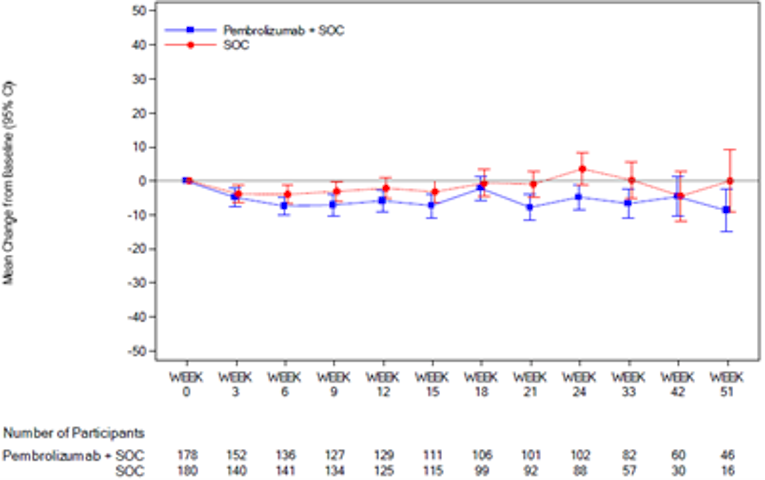
Figure 34: Empirical Mean Change From Baseline and 95% CI for the EORTC QLQ OES-18 Reflex Over Time, PD-L1 CPS of 10 or Greater, FAS Population
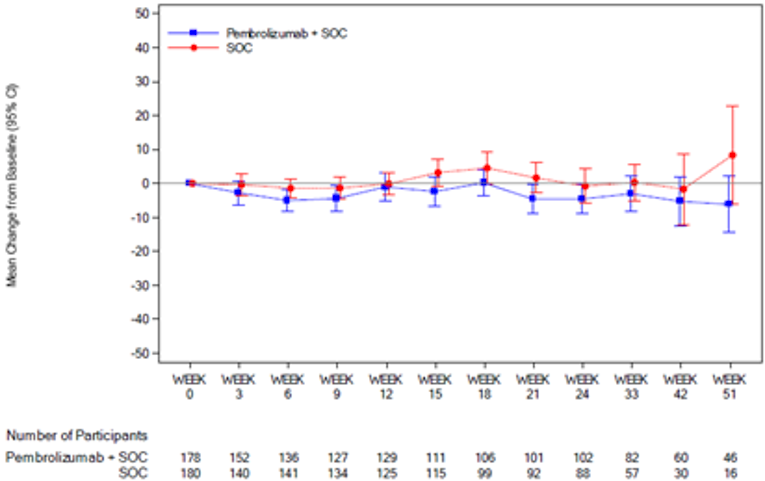
CI = confidence interval; CPS = combined positive score; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Module; FAS = Full Analysis Set; PD-L1 = Programmed cell death 1 ligand 1; Pembrolizumab + SOC = Pembrolizumab in combination with cisplatin and 5-FU; SOC = Placebo in combination with cisplatin and 5-FU; 5-FU = 5-fluorouracil.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Figure 35: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Dysphagia, ESCC With PD-L1 CPS of 10 or Greater, FAS Population at Baseline
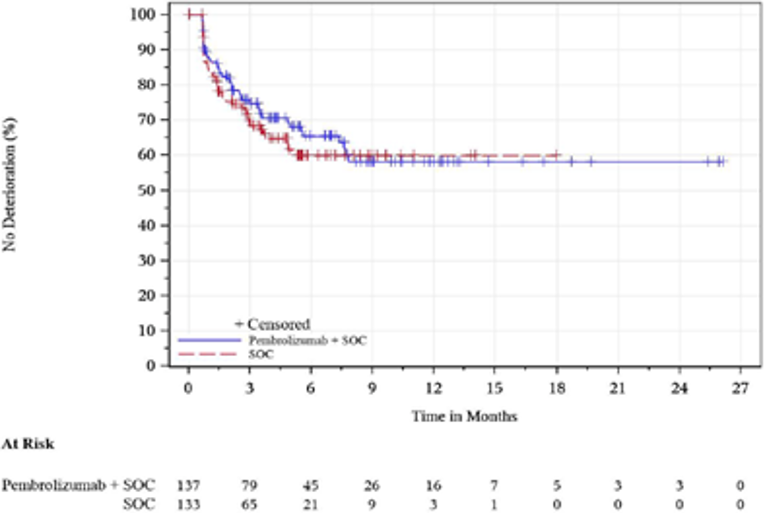
Figure 36: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Pain, ESCC With PD-L1 CPS of 10 or Greater, FAS Population at Baseline
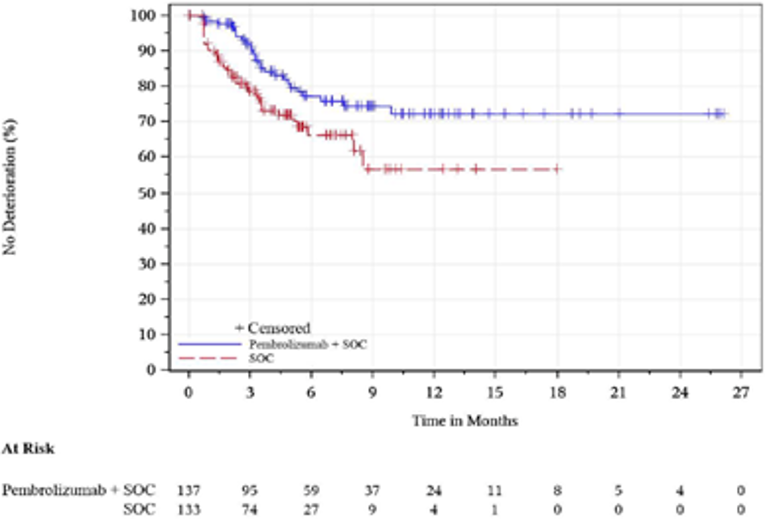
Figure 37: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Reflux, ESCC With PD-L1 CPS of 10 or Greater, FAS Population at Baseline
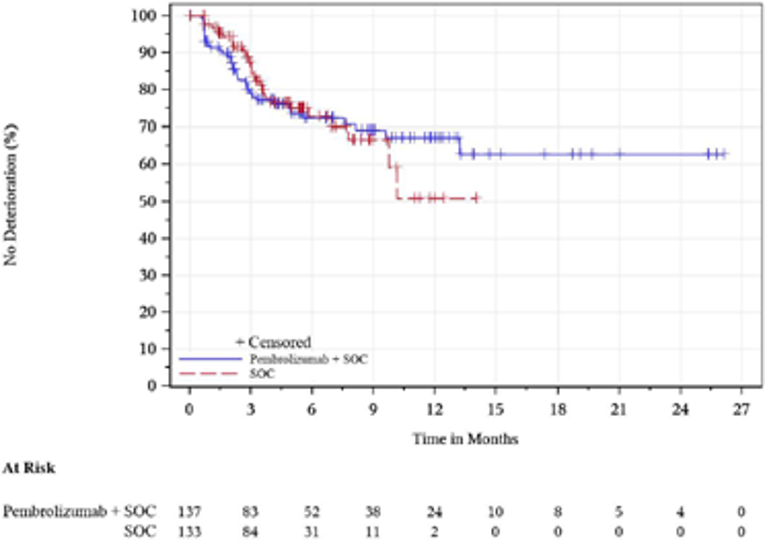
Figure 38: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Dysphagia, ESCC, FAS Population With Baseline
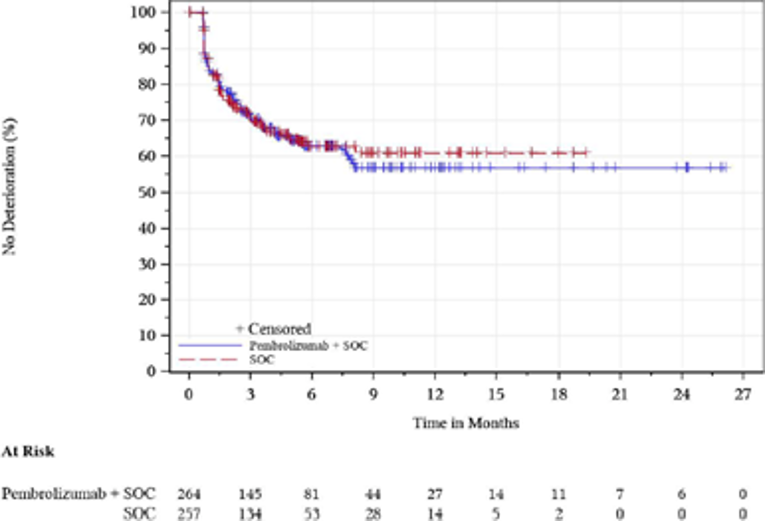
Figure 39: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Pain, ESCC, FAS Population With Baseline
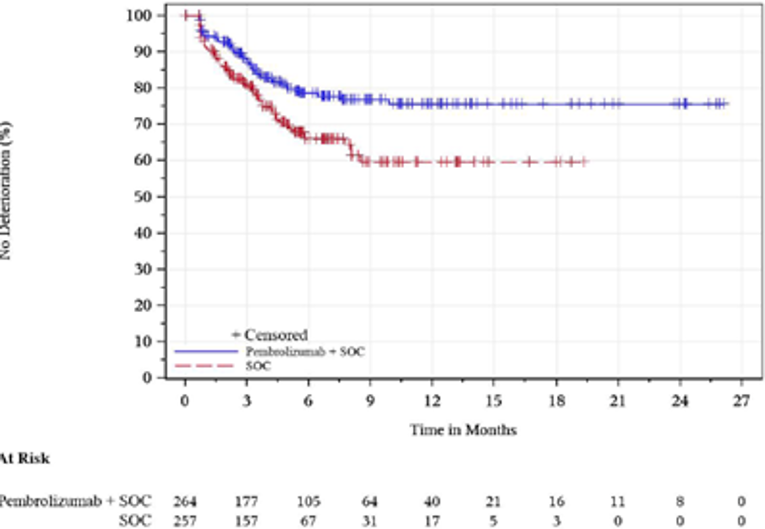
Figure 40: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Reflux, ESCC, FAS Population With Baseline
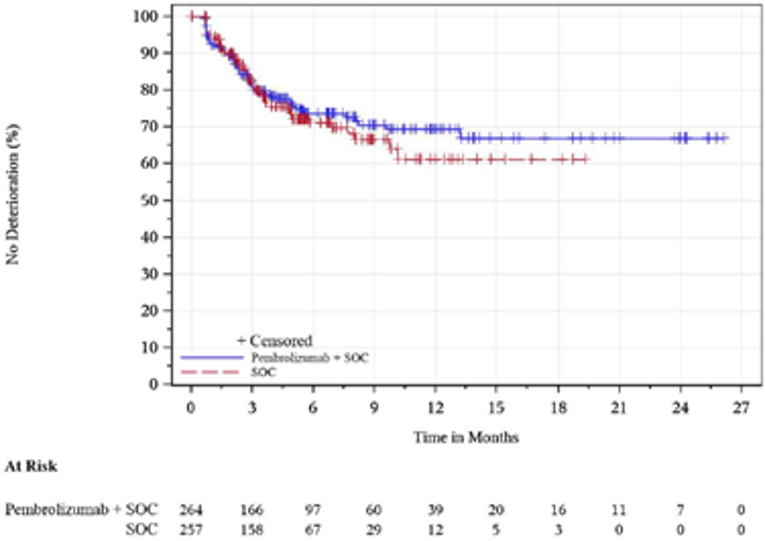
Figure 41: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Dysphagia, PD-L1 CPS of 10 or Greater, FAS Population With Baseline
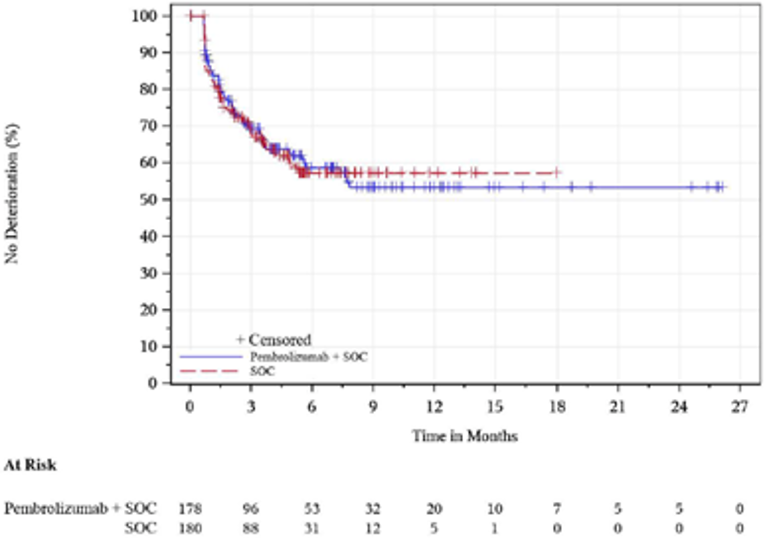
Figure 42: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Pain, PD-L1 CPS of 10 or Greater, FAS Population With Baseline
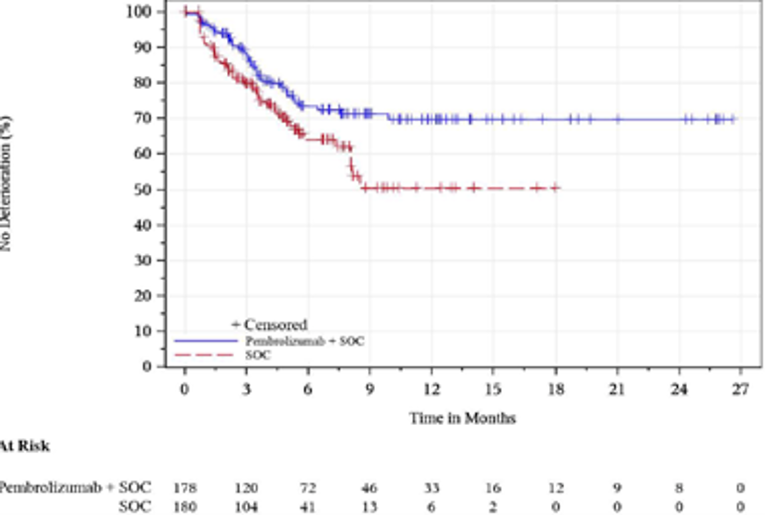
Figure 43: Kaplan-Meier Estimates of Time to Deterioration for EORTC QLQ-OES18 Reflux, PD-L1 CPS of 10 or Greater, FAS Population With Baseline
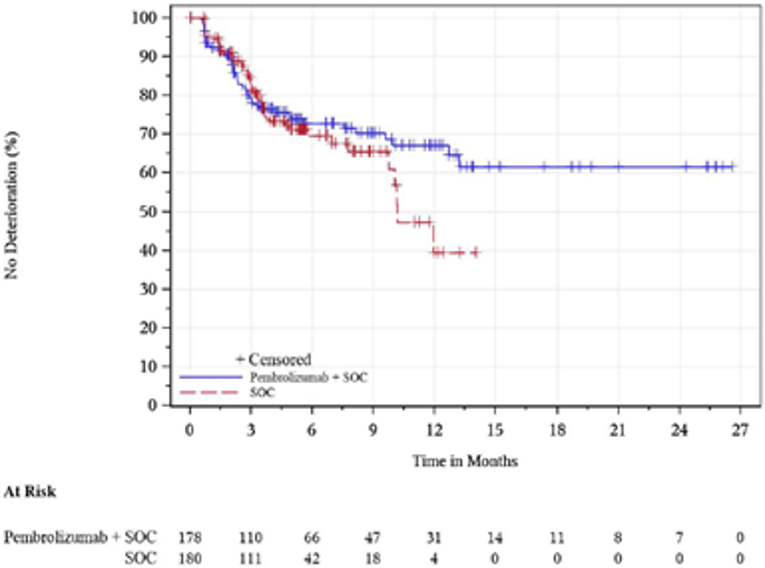
CPS = combined positive score; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Module; FAS = Full Analysis Set; PD-L1 = Programmed cell death 1 ligand 1; Pembrolizumab + SOC = Pembrolizumab in combination with cisplatin and 5-FU; SOC = Placebo in combination with cisplatin and 5-FU; 5-FU = 5-fluorouracil.
Note: Data cut-off date was July 2, 2020.
Source: Clinical Study Report.1
Table 27: Additional Harms Outcomes, Adverse Events Leading to Death and Treatment Discontinuation
Adverse event | KEYNOTE-590 | |
|---|---|---|
Pembrolizumab in combination with cisplatin and 5-FU (N=370) | Placebo in combination with cisplatin and 5-FU (N=370) | |
Adverse events leading to death reported up to 90 days after last dose in > 0% in either group | ||
Pneumonia | 6 (1.6) | 10 (2.7) |
Pneumonia aspiration | 3 (0.8) | 2 (0.5) |
Pulmonary sepsis | 3 (0.8) | 0 (0.0) |
Death | 2 (0.5) | 7 (1.9) |
Acute kidney injury | 1 (0.3) | 0 (0.0) |
Acute myocardial infarction | 1 (0.3) | 0 (0.0) |
Acute respiratory failure | 1 (0.3) | 1 (0.3) |
COVID-19 | 1 (0.3) | 0 (0.0) |
Cardio-respiratory arrest | 1 (0.3) | 0 (0.0) |
Clostridium difficile colitis | 1 (0.3) | 0 (0.0) |
Diarrhea | 1 (0.3) | 1 (0.3) |
Febrile neutropenia | 1 (0.3) | 1 (0.3) |
Hepatic failure | 1 (0.3) | 0 (0.0) |
Interstitial lung disease | 1 (0.3) | 1 (0.3) |
Multiple organ dysfunction syndrome | 1 (0.3) | 1 (0.3) |
Esophageal fistula | 1 (0.3) | 0 (0.0) |
Oesophagobronchial fistula | 1 (0.3) | 0 (0.0) |
Pneumonitis | 1 (0.3) | 0 (0.0) |
Pulmonary embolism | 1 (0.3) | 0 (0.0) |
Sudden cardiac death | 1 (0.3) | 0 (0.0) |
Upper gastrointestinal hemorrhage | 1 (0.3) | 2 (0.5) |
Aspiration | 0 (0.0) | 1 (0.3) |
Cardiac arrest | 0 (0.0) | 2 (0.5) |
Cerebral hemorrhage | 0 (0.0) | 1 (0.3) |
Cerebrovascular accident | 0 (0.0) | 1 (0.3) |
Gastrointestinal hemorrhage | 0 (0.0) | 1 (0.3) |
Haematemesis | 0 (0.0) | 1 (0.3) |
Respiratory failure | 0 (0.0) | 1 (0.3) |
Sepsis | 0 (0.0) | 3 (0.8) |
Tracheal hemorrhage | 0 (0.0) | 1 (0.3) |
Adverse events leading to treatment discontinuation of pembrolizumab/placebo in >0% in either group | ||
Blood and lymphatic system disorders | 2 (0.5) | 1 (0.3) |
Febrile neutropenia | 1 (0.3) | 1 (0.3) |
Neutropenia | 1 (0.3) | 0 (0.0) |
Thrombocytopenia | 1 (0.3) | 0 (0.0) |
Cardiac disorders | 5 (1.4) | 3 (0.8) |
Angina unstable | 1 (0.3) | 0 (0.0) |
Cardiac arrest | 0 (0.0) | 2 (0.5) |
Cardiac failure | 2 (0.5) | 0 (0.0) |
Cardio-respiratory arrest | 1 (0.3) | 0 (0.0) |
Coronary artery stenosis | 1 (0.3) | 0 (0.0) |
Pericarditis | 0 (0.0) | 1 (0.3) |
Congenital, familial and genetic disorders | 1 (0.3) | 0 (0.0) |
Tracheo-esophageal fistula | 1 (0.3) | 0 (0.0) |
Gastrointestinal disorders | 7 (1.9) | 4 (1.1) |
Colitis | 1 (0.3) | 0 (0.0) |
Diarrhea | 2 (0.5) | 0 (0.0) |
Duodenitis | 1 (0.3) | 0 (0.0) |
Dysphagia | 1 (0.3) | 0 (0.0) |
Gastrointestinal hemorrhage | 0 (0.0) | 1 (0.3) |
Esophageal fistula | 1 (0.3) | 0 (0.0) |
Pneumatosis intestinalis | 0 (0.0) | 1 (0.3) |
Upper gastrointestinal hemorrhage | 1 (0.3) | 2 (0.5) |
General disorders and administration site conditions | 3 (0.8) | 6 (1.6) |
Death | 2 (0.5) | 5 (1.4) |
Multiple organ dysfunction syndrome | 0 (0.0) | 1 (0.3) |
General disorders and administration site conditions | 3 (0.8) | 6 (1.6) |
Sudden cardiac death | 1 (0.3) | 0 (0.0) |
Hepatobiliary disorders | 3 (0.8) | 0 (0.0) |
Autoimmune hepatitis | 1 (0.3) | 0 (0.0) |
Hepatic failure | 1 (0.3) | 0 (0.0) |
Hepatitis | 1 (0.3) | 0 (0.0) |
Infections and infestations | 6 (1.6) | 12 (3.2) |
Clostridium difficile colitis | 1 (0.3) | 1 (0.3) |
Extradural abscess | 0 (0.0) | 1 (0.3) |
Pneumonia | 4 (1.1) | 9 (2.4) |
Pulmonary sepsis | 1 (0.3) | 0 (0.0) |
Sepsis | 0 (0.0) | 1 (0.3) |
Injury, poisoning and procedural complications | 2 (0.5) | 2 (0.5) |
Infusion-related reaction | 2 (0.5) | 0 (0.0) |
Subdural haematoma | 0 (0.0) | 1 (0.3) |
Tracheal hemorrhage | 0 (0.0) | 1 (0.3) |
Investigations | 4 (1.1) | 3 (0.8) |
Alanine aminotransferase increased | 1 (0.3) | 0 (0.0) |
Aspartate aminotransferase increased | 1 (0.3) | 0 (0.0) |
Blood creatinine increased | 2 (0.5) | 3 (0.8) |
Platelet count decreased | 1 (0.3) | 0 (0.0) |
Metabolism and nutrition disorders | 1 (0.3) | 0 (0.0) |
Cachexia | 1 (0.3) | 0 (0.0) |
Nervous system disorders | 3 (0.8) | 4 (1.1) |
Cerebral infarction | 0 (0.0) | 1 (0.3) |
Cerebrovascular accident | 1 (0.3) | 2 (0.5) |
Encephalopathy | 1 (0.3) | 0 (0.0) |
Peripheral sensory neuropathy | 1 (0.3) | 0 (0.0) |
Subarachnoid hemorrhage | 0 (0.0) | 1 (0.3) |
Renal and urinary disorders | 5 (1.4) | 4 (1.1) |
Acute kidney injury | 4 (1.1) | 2 (0.5) |
Renal failure | 0 (0.0) | 1 (0.3) |
Tubulointerstitial nephritis | 1 (0.3) | 1 (0.3) |
Respiratory, thoracic and mediastinal disorders | 13 (3.5) | 7 (1.9) |
Acute respiratory failure | 1 (0.3) | 1 (0.3) |
Aspiration | 0 (0.0) | 1 (0.3) |
Interstitial lung disease | 2 (0.5) | 1 (0.3) |
Pneumonia aspiration | 2 (0.5) | 2 (0.5) |
Pneumonitis | 6 (1.6) | 0 (0.0) |
Pulmonary embolism | 1 (0.3) | 0 (0.0) |
Pulmonary oedema | 0 (0.0) | 1 (0.3) |
Respiratory failure | 1 (0.3) | 1 (0.3) |
Vascular disorders | 0 (0.0) | 2 (0.5) |
Aortic thrombosis | 0 (0.0) | 1 (0.3) |
Dry gangrene | 0 (0.0) | 1 (0.3) |
5-FU = 5-fluorouracil.
Note: Data cut-off date of July 2, 2020.
Source: Clinical Study Report.1
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and minimal important difference):
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Version 3.0
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Cancer Module US English Version 1.0
EQ-5D 5-Levels questionnaire US English Version 1.1
Findings
Table 28: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | Cancer-specific measure of HRQoL 30-item self-administered questionnaire, consisting of a global health status/QoL scale, a Financial Difficulty scale, 5 functional scales (cognitive, social, physical, emotional, and role functioning), and 8 symptom scales (fatigue, insomnia, appetite, loss, pain, constipation, diarrhea, dyspnea, and nausea and vomiting).67,68 | Psychometric properties assessed in patients with esophageal and esophagogastric cancer. Validity: Construct validity assessed through convergent/ divergent and known-group validity; results suggested overall good construct validity. Reliability: Internal consistency (based on Cronbach alpha coefficient) and test–retest reliability were assessed; results suggested moderate to good internal consistency and good reproducibility. Responsiveness: No relevant studies found. | Not identified in the literature in patients with esophageal or gastric cancer. Sponsor defined a 10‑point change from baseline as improvement/ deterioration. A MID of 10-point change for improvement and worsening was suggested for the EORT QLQ-C30 in patients with breast and colorectal cancer.69 In addition, in patients with various cancer types,70 small and median improvements over time were generally classified as 4 or 5 to 9 points (small improvement) and as greater than 9 points to not evaluable (median improvements). Small and median deteriorations were generally classified as greater than 5 to less than 13 points (small deterioration) and as 10 or greater to less than 18 points (median deterioration).70 |
EORTC QLQ‑OES18 | Supplement of QLQ-C30 to assess HRQoL in patients with esophageal cancer; consisting of a 18-item self-administered questionnaire including 4 multi-item scales of dysphagia (3 items); eating (4 items); reflux (2 items); pain (3 items); and 6 single-item scales of trouble swallowing saliva; choking; dry mouth; taste; cough; speech.71 | Psychometric properties assessed in patients with esophageal cancer. Validity: Construct validity assessed through convergent/ divergent and known-group validity; results suggested overall good construct validity. Reliability: Internal consistency (based on Cronbach alpha coefficient) was assessed; results suggested moderate to good internal consistency Responsiveness: No relevant studies found. | Not identified in the literature in patients with esophageal or gastric cancer. Sponsor defined a 10‑point change from baseline as improvement/ deterioration, with no references for this definition provided. |
EQ-5D-5L | Generic, utility-based measure of HRQoL, consisting of an index score and a VAS. Index score: The tool consists of 5 dimensions: mobility, self-care, usual activity, pain/ discomfort and anxiety/ depression; each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. VAS: The tool assessed patient’s self-rated health on a vertical visual analogue scale.72 | Validity: Not identified in the literature in patients with esophageal or gastric cancer. Reliability: No relevant studies found. Responsiveness: No relevant studies found. | No relevant studies found in the literature in patients with esophageal or gastric cancer. No MID was provided in the sponsor’s submission. A Canadian MID of 0.037 ± 0.0001 for the EQ-5D-5L was suggested for the Canadian-specific scoring algorithm.73 MID ranges for the EQ-5D-5L from 8 to 12 based on ECOG Performance Status and from 7 to 10 based on FACT quality of life quintiles were suggested for patients with various advanced cancers.74 |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-OES18 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Cancer Module; EQ-5D-5L = European Quality of Life 5-Five Dimensions 5-Levels; HRQoL = health-related quality of life; MID = minimal important difference; QoL = quality of life; VAS = visual analogue scale.
EORTC QLQ-C30
Description
The EORTC QLQ-C30, is one of the most commonly used PRO measures in oncology clinical trials.67,75 It is a multi-dimensional, cancer-specific, evaluative measure of health-related quality of life (HRQoL). It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials, in response to treatment.76 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item QoL scale, as outlined in Table 29. Version 3.0 of the questionnaire, used in the included trials in this report, is the most current version.77 It is available in 118 different languages on the EORTC Study group website and is intended for use in adult populations only.67
Table 29: Scales of EORTC QLQ-C30
Functional scales (15 questions) | Symptom scales (7 questions) | Single-item symptom scales (6 questions) | Global Quality of Life (2 questions) |
|---|---|---|---|
Physical function (5) | Fatigue (3) | Dyspnea (1) | Global Quality of Life (2) |
Role function (2) | Pain (2) | Insomnia (1) | |
Cognitive function (2) | Nausea and vomiting (2) | Appetite loss (1) | |
Emotional function (4) | Constipation (1) | ||
Social function (2) | Diarrhea (1) | ||
Financial impact (1) |
Scoring
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4.77 For the 2 items that form the global QoL scale, however, the response format is a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).77
Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of one unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scale would reflect an improvement. According to the EORTC QLQ-C30’s scoring algorithm, if there are missing items for a scale (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least one-half of the items. In calculating the scale score, the missing items are simply ignored — an approach that assumes that the missing items have values equal to the average of those items for what the respondent completed.77
Psychometric Properties
Validity
Brunelli et al. (2000)78 conducted a validation of the EORTC QLQ-C30 instrument in patients with advanced esophageal cancer who receiving palliative treatment of malignant dysphagia in Italy. In addition, 3 studies79-81 assessed the validity of the EORTC QLQ-C30 in patients with gastric cancer in Taiwan (Huan et al. [2007]79) and Mexico (Onate-Ocana et al. [200982]) and in patients with esophagogastric cancer in Poland (Tomaszewski et al. [2013]81).
The study by Brunelli et al. (2000)78 enrolled 109 patients, but final analyses were based on 98 patients as information was lacking on more than 50% of the items on the EORTC QLQ-C30 questionnaire for 11 patients. Most patients had dysphagia; 44% and 25% of patients, respectively, had difficulty swallowing solid food and difficulty swallowing liquid and soft food, 29% of patients had little or no difficulty swallowing. The authors investigated convergent validity by assessing the correlation between an item and its own scale using Spearman’s correlation coefficient (r). As hypothesized, the convergent item-scale validity was moderately high (r > 0.40) for all items suggesting good convergent validity.78
Tomaszewski et al. (2013)81 assessed the psychometric properties of the EORTC QLQ-C30 in patients with esophageal or gastric cancer, including neoplasms located at the esophagogastric junction. The study enrolled 98 patients in Poland (all patients completed the EORTC QLQ-C30 questionnaire) divided into 2 groups: curative intention treatment (neoadjuvant or adjuvant treatment) (N = 57) and palliative treatment (N = 41). Most patients had gastric cancer (84.7%), followed by patients with esophageal cancer (14.3%) and esophagogastric junction cancer (1%). Construct validity was assessed via convergent and divergent validities evaluating the correlation between each item and its own scale and the correlation between each item and any other scale, respectively. Validity was judged to be good when the correlation between an item and its own scale was significantly higher than its correlation with any other scale using Pearson’s product-moment correlation. In addition, the scales of the EORTC QLQ-C30 and the QLQ-OG25 were compared, and it was hypothesized that scales in the EORTC QLQ-C30 and QLQ-OG25 would not relate to each other (Pearson r < 0.40) unless they were conceptually related (Pearson r > 0.40). The QLQ-OG25 module is a fully EORTC validated and EORTC approved disease-specific module with 22 questions for patients with esophagogastric cancer.67 Overall, results showed good convergent validity with coefficients showing moderate to high values (r ≥ 0.40). As expected, correlations between each item and any other scales were low suggesting good divergent validity. As hypothesized, scales between the EORTC QLQ-C30 and the QLQ-OG25 had low correlations, except for those with clinical overlap. For example, as expected, moderate to high correlations were noted between the anxiety and emotional functioning scales (r = 0.74) of both questionnaires and between the nausea and vomiting scale of the EORTC QLQ-C30 and the dysphagia and eating restrictions scales of the QLQ-OG25 (r = 0.62 and r = 0.65, respectively).81
Known-group comparison was assessed by Tomaszewski et al. (2013),81 comparing the EORTC QLQ-C30 scores between subgroups of patients that were expected to differ in respect to their clinical status (including disease site [esophagus versus stomach], treatment type [curative intention versus palliative], and physical function sores [good versus poor]). Differences between groups were tested with t-test or Mann-Whitney test as applicable. Results showed that the disease site did influence the responses given in more than half of the scales including global health status, physical functioning, and role functioning. Single items of the EORTC QLQ-C30 that distinguished between disease sites were fatigue, pain, dyspnea, insomnia, and appetite loss. Unexpectantly, treatment intention did not influence the scores in the EORTC QLQ-C30 questionnaire. The authors suggested this may have been because patients seemed to focus mainly on having cancer rather than on whether their cancer could be cured or not. The EORTC QLQ-C30 showed significantly better HRQoL scores in patients with better physical functioning.81
Reliability
Brunelli et al. (2000)78 assessed internal consistency with the Cronbach alpha coefficient. Overall, values of the coefficients demonstrated moderate to good internal consistency, ranging from 0.61 for the cognitive scale to 0.86 for the fatigue scale, while all the other scales ranged from 0.70 to 0.85.78
Tomaszewski et al. (2013)81 assessed internal consistency with the Cronbach alpha coefficient. Overall, results suggested moderate to good internal consistency given most multi-item-scale correlations had Cronbach alpha coefficient values of > 0.7, except the cognitive functioning scales which had a correlation value below 0.70, with an alpha coefficient of 0.62.81
Tomaszewski et al. (2013)81 assessed test–retest reliability in 35 randomly selected patients, who were asked to complete the questionnaire twice. Test–retest reliability was evaluated using Interclass Correlations (ICC) between baseline and retest 2 weeks late; a correlation of >0.80 was considered “good” with a significance level at p < 0.05. Results suggested good reliability of the CLC-C30 questionnaire with ICC ranging from 0.82 to 0.91.81
MID
A MID for the EORTC QLQ-C30 questionnaire was not identified in the literature for patients with esophageal or gastric cancer. The sponsor did not explicitly identify a MID but it was noted in the sponsor’s submission that an improvement in the EORTC QLQ-C30 instrument was defined as a 10 point or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by a 10 point or more improvement at a visit schedule at least 6 weeks later.1 Also, overall improvement/ stability was defined in the sponsor’s submission as the composite of improvement and stability. Stability was defined as, when the criteria for improvement are not met, a less than 10 points worsening in score from baseline at any time during the study and confirmed by a less than 10 points worsening at a visit scheduled at least 6 weeks later.1 Deterioration was defined as the time to first onset of 10 or more decrease from baseline with confirmation under right-censoring rule (the last observation).1 The submitted clinical study report1 of the KEYNOTE-590 trial reported that the aforementioned definitions were guided by the results of 3 studies.70,83,84 Osoba et al. (1998)84 suggested categorizing changes of EORTC QLQ-C30 scores of 5 to 10 points as small differences, 10 to 20 points as moderate differences, and greater than 20-point differences as large in patients who received chemotherapy for either breast cancer or small cell lung cancer.84 King et al. (1996)83 suggested that a change of EORTC QLQ-C30 scores of 5 points may be relatively small, while a change of 15 points may be relatively large in patients receiving treatment for various types of cancer. While King et al. (1996)83 reported that their findings were not based on the most current version of the EORTC QLQ-C30, Osoba et al. (1998)84 did not explicitly report which version of the EORTC QLQ-C30 was used but referenced version 1.0.85 The findings of both studies were not further summarized here given potential biases arising from differences across EORTC QLQ-C30 versions which may impact the assessment of HRQoL. The guidelines by Cocks et al. (2012)70 combined study results obtained via a systematic review of published studies with blinded expert opinions using meta-analytic techniques to estimate large, medium, and small mean changes over time in patients with various cancer types. While it is not reported by the authors which versions of the EORTC QLQ-C30 were utilized in the include studies, the literature search conducted by the authors was dated post 1998, which may imply that the majority of included studied used the most current version of the EORTC QLQ-C30 questionnaire, version 3.0, which, according to the EORTC QLQ-C30 Scoring Manual,77 was tested in EORTC field studies by Bjordal et al.86 in 2000.77 Cocks et al. (2012)70 reported that based on 118 included articles (selected from 911 identified articles in the literature search) 1,232 mean changes in HRQoL over time were combined in the meta-analysis with timescales ranging from 4 days to 5 years. The findings of the study suggested that generally, most median improvements were classified as subscale changes of greater than 9 points; with changes ranging from greater than 7 points (cognitive functioning subscale) to greater than 13 points (appetite loss subscale). It was noted that the upper limit for medium improvements could not generally be estimated. Most small improvements were categorized as changes varying between 4 or 5 and 9 points; with changes ranging from greater than 3 (financial difficulties subscale) to between 7 and 13 points (appetite loss subscale). Regarding deteriorations, most medium deteriorations were classified as subscale changes of 10 or greater and less than 18 points; with changes ranging from greater than 7 points (cognitive functioning subscale) to between 14 and 26 points (appetite loss subscale). Most small deteriorations were categorized as subscale changes of greater than 5 and less than 13 points; with changes raging between 1 and 7 points for the cognitive functioning subscale to between 7 and 14 points for the role functioning subscale. It was reported by Cocks et al. (2012)70 that large improvements or deteriorations were not evaluable.
More recently in 2015, a Canadian study estimated the MIDs of EORTC QLQ-C30 scales using data from 193 newly diagnosed breast and colorectal cancer patients.69 The Supportive Care Needs Survey-Short Form-34 (SCNS-SF34) was used as an anchor; mean changes in EORTC QLQ-C30 scales associated with improvement, worsening, and no-change in supportive care based on the SCNS-SF34 was then calculated. MIDs were assessed for the following scales: Physical function, role function, emotional function, global health/QoL (i.e., GHS), pain, and fatigue. For improvement, MIDs associated with a statistically significantly improved supportive care needs ranged from 10 to 32 points. For worsening, MIDs associated with a statistically significantly worsening of supportive care needs ranged from nine to 21 points. The range for unchanged supportive care needs was from 1-point worsening to 16-point improvement in EORTC QLQ-C30 score.69 Based on this, the authors suggested a 10-point change in EORTC QLQ- C30 score represented changes in supportive care needs, and therefore should be considered for clinical use.69
EORTC QLQ-OES18
Description
The EORTC QLQ-OES18 is a disease-specific module that was developed by the EORTC QoL Group to assess QoL in patients with esophageal cancer.87 It is to be administered in addition to the EORTC QLQ-C30 instrument to address esophageal cancer-specific symptoms.1 The EORTC QoL Group initially developed the EORTC QLQ-OES24 version (contains 24 questions) which it later refined to the EORTC QLQ-OES18 version (contains 18 questions).87 It has received formal approval and has undergone validation testing by the EORTC QoL Study Group.88 Approved translated versions are available from the EORTC QoL Study Group’s website in 56 languages.88
The EORTC QLQ-OES18 includes 18 questions: 6 single-item subscales relating to saliva swallowing, choking, dry mouth, taste, coughing, and talking. It also includes 12 items grouped into 4 subscales: dysphagia (3 items), eating (4 items), reflux (2 items), and pain (3 items).71
Scoring
The EORTC QLQ-OES18 uses a 1-week recall period in assessing function and symptoms. All questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. Computation of scores is done in similar manner as for the EORTC QLQ-C30 (see previous section). Responses to the questionnaire are transformed into a 0–100 scale, with higher scores implying a high level of symptoms or a high level of functioning.71
Psychometric Properties
Validity
Blazeby et al. (2003)87 conducted a clinical and psychometric validation of the EORTC QLQ-OES18 instrument in patients with esophageal cancer, on behalf of the EORTC GI and QoL Group. In addition, 4 studies (Chie et al. [2010],89 Dai et al. [2017],71 Forootan et al. [2014],90 Fujita et al. [2016]91) translated and subsequently validated the EORTC QLQ-OES18 questionnaire in patients with esophageal cancer. The authors of the article by Fujita et al. (2016)91 confirmed that their translated version of the EORTC QLQ-OES18 instrument into Japanese language had been accepted by the EORTC QoL Study Group for use in Japan and is currently available on the EORTC QoL Study Group’s website.91 The authors of the studies by Chie et al. (2010)89 and Dai et al., (2017)71 stated that their translations of the EORTC QLQ-OES18 questionnaire into Taiwan Chinese and Chinese languages, respectively, were done according to the guidelines of the EORTC; however, it was not reported if their translated versions had been approved for use by the EORTC QoL Study Group. The study by Forootan et al. (2014)90 neither reported if their translation of the EORTC QLQ-OES18 questionnaire into Iranian language had been done according to the guidelines of the EORTC nor if it had received the EORTC QoL Study Group’s approval. Since it is unclear if the translated versions of the EORTC QLQ-OES18 by Chie et al. (2010),89 Dai et al. (2017),71 Forootan et al. (2014)90 are approved by the EORTC QLQ-OES18 Study Group, these studies were not further summarized in here, given potential biases arising from translations which may impact the assessment of HRQoL.
The study by Blazeby et al. (2003)87 tested the validity of the EORTC QLQ-OES18 questionnaire in patients undergoing treatment for esophageal cancer. The study assessed 491 patients; 267 patients receiving treatment with curative intent and 224 patients receiving treatment with palliative intent. Initially, 591 patients were enrolled into the study, but 100 patients were excluded because the timing of the assessments was outside the pre-specified time intervals of the study. Patients were enrolled in 6 countries (UK, France, Germany, Sweden, Australia, and Spain). Construct validity was assessed by comparing the EORTC QLQ-OES18 module with the core questionnaire, EORTC QLQ-C30, for all patients before and after treatment using Spearman’s correlation coefficient (r). It was hypothesized that scales in the EORTC QLQ-OES18 module would not relate to generic aspects of QoL in the EORTC QLQ-C30 questionnaire, unless they addressed similar themes (e.g., pain). Most scales of the EORTC QLQ-OES18 instrument had low correlation with the EORTC QLQ-C30 questionnaire, except the esophageal pain and the eating scales which were moderately correlated with the QLQ-C30 pain scale (r = 0.58) and the social function and fatigue scales of the QLQ-C30 (r = 0.48 and r = 0.46 after treatment), respectively. The authors noted that both these moderate association would be expected given the connection between challenges with eating and its social consequences.87
Known-group validity was assessed by determining the extent to which the module was able to discriminate between groups of patients with different clinical status. Overall, the EORTC QLQ-OES18 instrument was able to discriminate between clinically distinct groups of patients. Patients who received potential curative treatment scored better than patients receiving treatment with palliative intent.87
Responsiveness was assessed by comparing treatment-induced differences in QoL scores over time in 4 patient subgroups (patients receiving esophagectomy, curative chemotherapy ± radiotherapy, endoscopic palliation, and palliative chemotherapy ± radiotherapy). Overall, the EORTC QLQ-OES18 questionnaire was sensitive to clinical changes in health over time and was able to discriminate between these subgroups of patients. For example, patients who were assessed 3 months after receiving esophagectomy reported worse functional aspects of QoL (physical, social, role and cognitive function) and more problems with fatigue, nausea and vomiting, pain, appetite loss, diarrhea, dry mouth, and loss of taste than before treatment; whereas patients who received chemotherapy and radiotherapy with curative intent, reported problems eating (may be related to dry mouth or pain) after treatment while dysphagia scores had not changed.87
The study by Fujita et al. (2016)91 tested the validity of the EORTC QLQ-OES18 instrument in Japanese patients with esophageal cancer of the SCC type who have undergone thoracic esophagectomy with 3-field lymph node dissection for curative purpose with both thoracoscopic and thoracotomy esophagectomy and either laparoscopic gastric or laparotomy gastric pull-up. A total of 56 Japanese patients were included; the final data were based on 50 patients who filled out the questionnaires; 70% and 15% of patients, respectively, were treated with the thoracoscopic and thoracotomy approaches; 72% and 28% of patients, respectively, underwent laparoscopic and laparotomy surgical approaches.91
Construct validity was assessed via convergent and discriminant validity using Spearman’s correlation coefficient (r). For convergent validity it was hypothesized that the correlation between an item and its own scale would be moderately high (r ≥ 0.40) and for discriminant validity the correlation between an item and any of the other scales should be low. If the correlation of an item with another scale exceeded the correlation with its own scale a definite scaling error was assumed. Results showed that correlations between an item and its own scale were high for the following scales: dysphagia scale (r ranged from 0.83 to 0.84), eating scale (r ranged from 0.69 to 0.84), reflux scale (r ranged from 0.71 to 0.88), and pain scale (r ranged from 0.67 to 0.90). Generally, single items not included in any scale were not significantly correlated with other scales, except 5 single items (trouble swallowing saliva, choked when swallowing, dry mouth, trouble with taste, trouble with coughing, and trouble with talking) which correlated with the dysphagia scale (r > 0.5) and another 3 single items (chocked when swallowing, dry mouth, and trouble with taste), which correlated with the eating scale (r > 0.6). Further, results indicated a substantial correlation between theoretically linked scales (the dysphagia and eating scales [r = 0.62] and the eating and reflux scales [r = 0.49]) and showed weak correlation between independent scales. Overall, the results suggested good convergent and discriminant validity.91
Reliability
Blazeby et al. (2003)87 assessed internal consistency with the Cronbach alpha coefficient. Values above 0.7 were regarded as acceptable and greater than 0.8 as good. The EORTC QLQ-OES18 questionnaire showed moderate to good reliability. The Cronbach alpha coefficient was above 0.70 in 60% for all scales; it was lowest in the reflux and pain scales and highest in the eating and dysphagia scales.87
Fujita et al. (2016)91 assessed internal consistency with the Cronbach alpha coefficient. Values ≥ 0.7 were regarded as acceptable and greater than 0.8 as good. Cronbach alpha coefficients for the internal consistency of the 4 scales (dysphagia, eating, reflux, and pain) were all satisfactory with values above 0.70 and pain having the highest coefficient with a value of 0.85.91
MID
A MID for EORTC QLQ-OES18 was not identified in the literature for patients with esophageal or gastric cancer. It was noted in sponsor’s submission that an improvement in the EORTC QLQ-C30 instrument was defined as a 10 point or more increase in score (in the positive direction) from baseline at any time during the study and confirmed by a 10 point or more improvement at a visit schedule at least 6 weeks later.1 Also, overall improvement/ stability was defined in the sponsor’s submission as the composite of improvement and stability. Stability was defined as, when the criteria for improvement are not met, a less than 10 points worsening in score form baseline at any time during the study and confirmed by a less than 10 points worsening at a visit scheduled at least 6 weeks later.1 Deterioration is defined as the time to first onset of 10 or more decrease from baseline with confirmation under right-censoring rule (the last observation).1 No sources for references for the aforementioned MID definitions in patients with esophageal cancer were provided by the sponsor.
EQ-5D-5L
Description
The EQ-5D is a generic, utility-based measure of HRQoL. The EQ-5D is a 2-part questionnaire, consisting of the EQ-5D descriptive system and the EQ-5D VAS.92
For the descriptive system of the EQ-5D, respondents are asked to indicate their health status that day (i.e., a one‑day recall) on 5 dimensions (mobility, self-care, usual activities, pain/ discomfort, and anxiety/depression). The EQ-5D-5L was created by the EuroQol Group in 2009 to enhance the instrument’s sensitivity and to reduce ceiling effects, as compared to the EQ-5D-3L.92
The 5-level version of the EQ-5D has response options for each of the 5 dimensions that reflect 3 possible levels of functioning.
Level 1: No problems
Level 2: Slight problems
Level 3: Moderate problems
Level 4: Sever problems
Level 5: Extreme problems
The rating on each dimension is combined to create a descriptive health profile (referred to as the health state description) that is a vector of the levels. For example, an individual with no health problems on any dimension would have a health profile of 11111, while a person with extreme problems on all dimensions would have a health profile of 55555. The numerical values assigned to the levels 1, 2, 3, 4, or 5 for each dimension reflect rank order categories of function. There are 3,125 unique health states that exist for the EQ-5D-5L.92 The EQ-5D-5L is available in 150 different languages.92
Scoring
Index Scores
The health profile (health state description or vector) defined by the EQ-5D-5L questionnaire is used to create an overall index score. To create the EQ-5D-5L index score, a scoring algorithm (a mathematical equation termed a utility function) is applied to the vector. Various scoring algorithms for the EQ-5D-5L have been derived by determining the societal preferences for its 3,125 health states (i.e., by assessing how much value society places on each health state) using techniques such as the standard gamble or TTO. In all scoring algorithms of the EQ-5D-5L, a score of 0 represents the health state “dead” and 1.0 reflects “full health.” Negative scores are also possible for those health states that society (not the individual patient) considers to be “worse than dead.”92
VAS Scores
The EQ-5D VAS is a distinct component of the EQ-5D questionnaire. The VAS score is determined by asking respondents to rate their health that day on a vertical line, with anchors (end points) labelled “Worst imaginable health state” at 0 and “Best imaginable health state” at 100. While the EQ-5D index score reflects societal preferences for the health state, the VAS captures the individual’s own value or judgment of his or her present health state. The EQ-5D VAS scores are not used to create utility scores but provide complementary information to the EQ-5D-5L index score.92
Psychometric Properties
Validity
No study was found assessing the psychometric properties related to validity for EQ-5D in patients with esophageal or gastric cancer.
Reliability
No study was found assessing the psychometric properties related to reliability for EQ-5D in patients with esophageal or gastric cancer.
MID
McClure et al. (2017)73 obtained the MID for the EQ-5D-5L by calculating the average absolute difference between the index score of the baseline health state and the index score of all single-level transitions from the baseline state. A single-level transition was defined as a change in a single dimension to the next worse/better level, while holding all other dimensions constant. Such single-level transitions across all 3,125 health states were averaged to arrive at MIDs for 6 countries (Canada, China, Spain, Japan, England, and Uruguay) by applying country-specific scoring algorithms. For Canada, transitions between levels 3 and 4 were excluded from the average to form a constant distribution of MID values across the range of baseline scores. This analysis resulted in a Canadian-specific MID of 0.037 ± 0.0001.
Pickard et al. (2007)74 estimated the MID of the EQ-5D VAS based on cross-sectional data collected from 534 patients with advanced (stage III or IV) cancer of the bladder, brain, breast, colon or rectum, head or neck, liver or pancreas, kidney, lung, lymphoma, ovary, or prostate. Using both anchor- based and distribution-based methods, estimates of the MID ranged from 8 to 12 based on the ECOG Performance Status, and from 7 to 10 based on FACT quality of life questionnaire quintiles.
A MID for EQ-5D-5L was not identified in the literature for patients with esophageal or gastric cancer. No MID was provided in the sponsor’s submission.
Appendix 5: Summary of Sponsor’s Provided Feasibility Assessment for Pembrolizumab for Advanced Esophageal Cancer
Note that this appendix has not been copy-edited.
The sponsor conducted a feasibility assessment3 of estimating the comparative efficacy and safety of pembrolizumab plus cisplatin and 5-FU versus other competing interventions using data obtained from a systematic literature review (SLR).3 The feasibility assessment report3 and the SLR3 were prepared for the sponsor by PRECISIONheor and were provided with the sponsor’s submission to CADTH. The pivotal trial in the sponsor’s submission, KEYNOTE-590,65 was a phase III randomized controlled trial comparing pembrolizumab plus cisplatin and 5-FU with cisplatin and 5-FU.3 In order to support submissions to health technology assessment agencies, the sponsor noted that it would be of interest to compare the relative efficacy and safety of pembrolizumab plus cisplatin and 5-FU to currently relevant comparator treatments in clinical practice.
The objective was to evaluate the feasibility of estimating the comparative efficacy and safety of pembrolizumab plus cisplatin and 5-FU versus relevant competing interventions other than the trial comparator treatment.3 A SLR3 was conducted to identify relevant literature for the feasibility assessment. Studies that were eligible for inclusion in the SLR evaluated patients with a histologically or cytologically confirmed diagnosis of locally advanced unresectable or metastatic adenocarcinoma or SCC of the esophagus or advanced or metastatic adenocarcinoma of the GEJ, Siewert type I. Key exclusion criteria included resectable disease, previous therapy for advanced esophagus or advanced/ metastatic Siewert type 1 adenocarcinoma of the GEJ, and HER2 positive tumours. Eligible interventions included pembrolizumab plus cisplatin and 5-FU, 5-FU or capecitabine with cisplatin or oxaliplatin, 5-FU or capecitabine with cisplatin or oxaliplatin plus epirubicin, FOLFOX, FOLFIRI, paclitaxel or docetaxel doublet or triplet regimens, nivolumab plus cisplatin and 5-FU, nivolumab plus ipilimumab, and any of the previously mentioned drugs as monotherapy. Studies could be randomized controlled trials and nonrandomized clinical trials.
The outcomes of interest included OS, PFS, DOR, ORR, drug-related AEs, grade 3-5 AEs (all drug related), discontinuation due to AEs, serious AEs, and PROs (e.g., EQ-5D, EORTC QLQ-C30, EORTC QLQ-OES18). A number of databases were searched (Embase, MEDLINE, and Cochrane Registry of Controlled Trials) clinical trials registries (clinicaltrials.gov) and relevant conference websites. Study selection and assessment of study quality (Cochrane Risk of Bias assessment) were conducted by 2 independent reviewers and disagreements between reviewers were resolved through discussion. The data base searches were executed on December 22, 2020, with no year restriction. A total of 5,543 citations were identified through database searching and 3,394 citations were screened after duplicates had been removed. Out of 343 citations selected for full text review, 22 unique trials (including the study report from the pivotal trial, KEYNOTE-59065) were included. Full PRISMA diagram was provided for each step of the study review process, and a list of excluded studies based on full text review was provided in the report.3
Of the 22 trials meeting the criteria for the SLR, 8 trials were excluded from the feasibility assessment (i.e., 3 trials93-95 including the intervention cisplatin with 5-FU were excluded based on the fact that this comparator intervention was already captured in the index trial (submitted pivotal trial, KEYNOTE-59065) and the studies did not connect to any additional interventions of interest; 5 studies96-100 were excluded based on a lack of reported patient characteristics for the population of interest).3 The sponsor noted that 14 studies were included in the feasibility assessment, which are summarized in Table 30. It was noted by the sponsor that no studies evaluating nivolumab combinations were included in the feasibility assessment as no data had been published or presented at the time of conducting the feasibility assessment (the feasibility assessment was prepared for the sponsor by PRECISIONheor on May 4, 2021).3 It was noted that once data from CheckMate 648101 or CheckMate 649102 would be available the feasibility of conducting an unanchored MAIC or a network meta-analysis (NMA) would be reconsidered.3 CheckMate 648101 (NCT03143153; primary completion date January 18. 2021) is a multi-centre, open-label phase III randomized controlled trial comparing nivolumab plus ipilimumab or nivolumab combined with 5-FU plus cisplatin versus 5-FU plus cisplatin in patients with unresectable advanced, recurrent, or metastatic previously untreated ESCC. CheckMate 649102 (NCT02872116; primary completion date May 27, 2020) is a multi-centre, open-label, phase III randomized controlled trial comparing nivolumab plus chemotherapy against chemotherapy in patients with previously untreated advanced or metastatic gastric or GEJ cancer. The clinical experts consulted by CADTH noted that regimens containing nivolumab are currently not used in Canadian clinical practice in the target population for this review.
The sponsor discussed the feasibility of conducting a NMA, an unanchored MAIC, and a naïve treatment comparison. Key requirements for each of these methods (NMA, unanchored MAIC, and naïve treatment comparison) were summarized. Briefly, key conditions for an NMA included one network of trials where each trial has at least one intervention (or placebo) in common with another trial while assuming no differential effect of prognostic factors. If there is a lack of network connectivity, an unanchored MAIC was reported to be feasible if access to individual patient data (IPD) for the index intervention is available. However, it was noted that the validity of comparative effect estimates obtained via an unanchored MAIC depends on the degree of overlap in the study populations between the index trial and comparator trials and the extent that it is possible to up or down-weight patients to achieve an appropriate match to the comparator trials. An unanchored MAIC should adjust for all effect modifiers and prognostic factors assuming the absolute treatment effect is constant at any level of effect modifiers and prognostic factors (assumes all effect modifiers and prognostic factors are known). A naïve indirect treatment comparison requires no imbalance between the studies with respect to prognostic factors or in terms of treatment effect modifiers. For a summary of a comparison for feasibility assessment steps for NMAs versus unanchored MAICs the sponsor provided Table 31.3
The sponsor presented a network diagram of studies included in the feasibility assessment which demonstrated a lack of network connectivity, Figure 44. Since the studies included in the feasibility assessment did not form a connected network, the sponsor noted that it would not be feasible to perform an NMA. As IPD data were available for the index trial (KEYNOTE-590)65 the sponsor proceeded to summarize and assess between-study differences in order to evaluate the feasibility of conducting an unanchored MAIC between the index intervention of the KEYNOTE-590 trial,65 pembrolizumab plus cisplatin plus 5-FU, and the following comparators: cisplatin plus capecitabine, paclitaxel plus capecitabine, carboplatin plus docetaxel, irinotecan plus 5-FU plus oxaliplatin FOLFIRI, cisplatin plus paclitaxel, cisplatin plus docetaxel plus 5-FU, and cisplatin plus docetaxel.3
The sponsor assessed differences in trial characteristics based on eligibility criteria, patient characteristics, outcome definitions, reported outcomes, and treatment regimens across the included studies. Trial characteristics and eligibility criteria of the trials included in the feasibly assessment are summarized in Table 32 Study Characteristics of Trials Included in Feasibility AssessmentTable 32 and Table 33. All 14 trials were either phase I or phase II single-arm trials, except the index trial, KEYNOTE-590,65 and the study by Lee et al. (2015),103 which were randomized phase III and phase II trials, respectively. The following key inconsistencies in trial eligibility criteria across the included studies were noted by the sponsor. Most trials exclusively allowed patients with esophageal SCC, whereas KEYNOTE-59065 enrolled patients with adenocarcinoma or SCC of the esophagus as well as patients with GEJ, Siewert type 1. Two comparator trials, Hironaka et al. (2014)104 and Wolff et al. (2009)105 also enrolled patients with adenocarcinoma and adenosquamous carcinoma/adenocarcinoma, respectively. Most studies included patients with ECOG PS 0 to 2, whereas KEYNOTE-590,65 Hironaka et al. (2014),104 and Ojima et al. (2017)106 included patients with ECOG PF 0 to 1.
Baseline patient characteristics are summarized in Table 34, Table 35,Table 36. Across the 14 included studies there was some variation in median age, which ranged from 56 years in Huang et al. (2013)107 to 67 years in Ojima et al. (2017).106 All studies enrolled more males than females and the proportion of male patients ranged from 76% in Tamura et al. (2012)108 to 100% in Kim et al. (2010).109 In terms of the extent of disease, the KEYNOTE-590 trial65 included 91.2% of patients with metastatic disease and 8.8% of patients with unrespectable locally advanced disease.1 The majority of patients across studies had metastatic disease except in Lee et al. (2008), Lee et al. (2015),103 and Tanaka et al. (2019),110 which included 82%, 93% and 50% of patients with locally advanced disease, respectively. Key differences in patients’ baseline characteristic across the included studies included:
Race: KEYNOTE-59065 was conducted in multiple centres internationally (53.4% of patients were Asian, 37.1% were White, few patients American Indian or Alaska Native, or multiple)1 whereas the comparator trials were conducted in centres across Asian countries only, except for 2 studies, Rossman et al. (2011)111 and Wolff et al. (2009)105 which were conducted in US and South Africa, and Germany, respectively.
Histology: KEYNOTE-59065 included 73.2% of patients with SCC of the esophagus, 14.7% of patients with adenocarcinoma of the esophagus, and 12.1% of patients with adenocarcinoma of the GEJ, Siewert type 1.1 The target population in the reimbursement request for this review aligns with the study population of the KEYNOTE-590 trial. All comparator trials exclusively enrolled patients with SCC of the esophagus, except Hironaka et al. (2014)104 and Wolff et al. (2009)105 which included 4% and 54% of patients with adenocarcinoma of the esophagus, respectively.
ECOG PS: KEYNOTE-59065 included 59.8% of patients with ECOG PS of 1, 39.9% of patients with ECOG PS of 0 and 0.3% of patients with ECOG PS of 2. In 6 comparator studies (Rossman et al. [2011],111 Huang et al. [2013],107 Kim et al. [2010],109 Osaka et al. [2011],112 Wolff et al. [2009],105 and Zhang et al. [2008]113) the majority of patients had ECOG PS of 1 (percentages ranging from 51% to in Zhang et al. [2008]113 to 90% in Kim et al. [2010]109). In 4 comparator studies (Hironaka et al. [2014],104 Tamura et al. [2012],108 Ojima et al. [2017],106 Takahashi et al. [2010]114) the majority of patients had ECOG PS of 0 (percentages ranging from 71% in Hironaka et al. [2014]104 to 86% in Tamura et al. [2012]108). In 2 studies (Tanaka et al. [2010]110 and Lee et al. [2008]) almost all patients had ECOG PS 0/ 1. ECOG PS of 2 was only present in patients in Osaka et al. (2011)112 (40%), Rossman et al. (2011) (16%), Wolff et al. (2009)105 (17%), Zhang et al. (2006)113 (18%), and in few patients in Kim et al. (2010)109 and Lee et al. (2008).
Primary tumour site: KEYNOTE-59065 included 12.1% of patients with tumours in the GEJ and 87.9% of patients with tumours in the esophagus. All comparator trials exclusively included patients with tumours in the esophagus.
Outcome availability and definitions from the included studies are summarized in Table 37and Table 38. Key differences in outcome availability and outcome definitions across the included studies included:
ORR: All studies reported ORR, however, only KEYNOTE-59065 and Zhang et al. (2008)113 defined ORR. Nine studies, including KEYNOTE-590,65 used RECIST criteria to assess response, whereas Lee et al. (2008) used the WHO criteria and 4 studies (Rossman et al. [2011],111 Tamura et al. [2012],108 Tanaka et al. [2010],110 and Wolff et al. [2009]105) did not report the criteria used to evaluate response.
OS: All studies, except Tanaka et al. (2010)110 reported OS, however, only KEYNOTE-590,65 Wolff et al.(2009),105 and Zhang et al. (2008)113 provided explicit definitions.
PFS: Nine studies reported PFS, however, definitions for PFS were only reported in KEYNOTE-59065 and Zhang et al. (2008113
Time to progression: Three studies reported TTP. A definition for TTP was reported in Zhang et al. (2008).113
Safety: KEYNOTE-59065 reported general and treatment-related grade 3-5 AEs, treatment-related serious AEs, and discontinuation due to AEs. Lee et al. (2008) and Lee et al. (2015)103 only reported grade 3-4 AEs and other comparator studies reported individual AEs.
HRQoL: KEYNOTE-59065 and Lee et al. (2015)103 assessed HRQoL utilizing the EORTC QLQ-OES18. However, Lee et al. (2015)103 only provided a brief description of HRQoL outcomes rather than reporting results for HRQoL measures. The KEYNOTE-590 trial65 also used the EORTC QLQ-C30 and EQ-5D to evaluate HRQoL.
Treatment regimens of studies included in the feasibility assessment are summarized in Table 39. Key differences in treatment regimens administered across the included studies included:
Capecitabine plus cisplatin: Two included studies used capecitabine plus cisplatin with different dosing schedules: Lee et al. (2008)115 (capecitabine: 1,250 mg/ m2 per oral dose twice a day on day 1 to day 14 every 21-day treatment cycle; cisplatin: 60 mg/ m2 on day 1 of every 21-day treatment cycle) and Lee et al. (2015)103 (capecitabine: 1,000 mg/ m2 per oral dose twice a day on day 1 to day 14 every 21-day treatment cycle; cisplatin: 75 mg/ m2 on day 1 of every 21-day cycle). In the submitted economic model the following treatment regimen was assumed for capecitabine plus cisplatin which differed to what was used in Lee et al. (2008)115 and Lee et al. (2015)103: capecitabine: 1,000 mg/ m2 per oral dose twice a day on day 1 to day 14 every 21-day treatment cycle; cisplatin: 80 mg/ m2 on day 1 of every 21-day treatment cycle.116
Cisplatin plus paclitaxel: Two included studies used cisplatin plus paclitaxel with different dosing schedules: Huang et al. (2013)107 (cisplatin: 50 mg/ m2 on day 2 of every 14-day treatment cycle; paclitaxel: 150 mg/ m2 on day 1 of every 14-day treatment cycle) and Zhang et al. (2008)113 (cisplatin: 75 mg/ m2 on day 1 of every 21-day cycle; paclitaxel: 175 mg/ m2 on day 1 of every 21-day cycle). The submitted economic model did not include the cisplatin plus paclitaxel combination as comparator treatment.116
Cisplatin plus docetaxel plus 5-FU: Six included studies used cisplatin plus docetaxel plus 5-FU with different dosing schedules: 3 studies (Tamura et al. [2012],108 Osaka et al. [2011],112 and Takahashi et al. [2010]114) administered docetaxel at a dose of 60 mg/ m2, on day 1 of every 21-day cycle; whereas the other 3 studies administered docetaxel at a dose of 30-40 mg/ m2 on day 1 and day 15 (Hironaka et al. [2014]104 and Tanaka et al. [2010]110) or day 8 (Ojima et al. [2017]106) every 28-day cycle. The submitted economic model did not include the cisplatin plus docetaxel plus 5-FU combination as comparator treatment.116
Summary tables of efficacy results reported in the included studies are presented in Table 40. Median OS was evaluated in 13 studies65,103-115 ranging from 6.7 months in Rossman et al. (2011)111 to 13.6 months in Wolff et al. (2009).105 Median PFS was also reported in 12 studies65,103-109,111,113-115 ranging from 3.2 months in Rossman et al. (2011)111 to 7 months in Takahashi et al. (2010)114 and Zhang et al. (2008).113 ORR was reported in 13 studies65,103,104,106-115 ranging from 15.6% in Rossman et al. (2011)111 to 88.9% in Tanaka et al. (2010).110 DOR among responders was reported in 3 studies (KEYNOTE-590,65 Lee et al. [2008],115 and Lee et al. [2015]103) ranging from 4 months in Lee et al. (2015)103 to 8.3 months in the pembrolizumab plus cisplatin and 5-FU group of the KEYNOTE-590 trial.65 Only KEYNOTE-59065 reported AEs, drug-related AEs, grade 3 to 5 AEs, drug-related grade 3 to 5 AEs, SAEs, drug-related SAEs, discontinuation due to AEs, discontinuation due to SAEs, and discontinuation due to drug-related AEs. Decrease in neutrophil count, anemic, and neutropenia were the most commonly reported grade 3 to 5 AEs in both treatment groups in KEYNOTE-59065 (anemia: 17.0% and 21.9% in the pembrolizumab plus cisplatin plus 5-FU and cisplatin plus 5-FU groups, respectively; neutropenia: 14.6% and 16.5% in the pembrolizumab plus cisplatin plus 5-FU and cisplatin plus 5-FU groups, respectively).1 Lee et al. (2008)115 and Lee et al. (2015)103 reported grade 3 or 4 AEs. In both of these studies, grade 3 to 4 neutropenia was the most common AE and the proportion of patients experiencing neutropenia ranged from 34.8% in Lee et al. (2015)103 to 73.3% in Lee et al. (2008). HRQoL was evaluated with EORTC QLQ-OES18 in KEYNOTE-59065 and Lee et al. (2015).103 However, Lee et al. (2015)103 did not report specific HRQoL scores and only stated that “reflux improved after capecitabine plus cisplatin chemotherapy.”103 KEYNOTE-59065 additionally used EORTC QLQ-C30 and EQ-5D; the least squares mean changes from baseline were similar between the 2 treatment groups.3
Having summarized and reviewed the between-trial differences in the 14 studies included in the feasibility assessment, the sponsor noted the following concerns with conducting an unanchored MAIC. Matching to comparator trials would lead to a weight of 0 for non-Asian patients as well as those Asian patients without ESCC in the KEYNOTE-590 trial,65 resulting in a large reduction in the effect sample size (ESS) and high degree of uncertainly around the treatment effects estimates due to these being influenced by relative few patients. Furthermore, the sponsor noted that in case a sufficiently large ESS were achievable and the bias due to potential residual imbalances between populations were assumed to be minimal, it remained unclear how generalizable the comparative effect estimates would be to the present target population, given that ethnicity, histology, and tumour location have been identified as effect modifiers (although the sponsor noted that there is some controversy around the role of ethnicity as effect modifier). Given that the review of between-study differences determined that key differences were present between studies, the sponsor noted that treatment effect estimates obtained via a naïve indirect treatment comparison would be subject to a serious risk of bias.3
Key Critical Appraisal Points Conducted by the CADTH Clinical Review Team
Overall, the comparator treatments to pembrolizumab plus cisplatin and 5-FU considered in the submitted feasibility assessment were appropriate for the Canadian clinical practice setting. The feasibility assessment included 14 studies that evaluated the following comparator interventions: cisplatin plus capecitabine, paclitaxel plus capecitabine, carboplatin plus docetaxel, FOLFIRI, cisplatin plus paclitaxel, cisplatin plus docetaxel plus 5-FU, and cisplatin plus docetaxel. These comparator treatments aligned with the comparators listed in the protocol of the CADTH conducted systemic literature review for this submission, except for FOLFOX and epirubicin plus 5-FU which were listed in the CADTH protocol but not included in the feasibility assessment due to a lack of reported patient characteristics for the population of interest in studies evaluating FOLFOX and epirubicin plus 5-FU. The clinical experts consulted by CADTH agreed that in Canada, FOLFOX is the most commonly used comparator treatment, whereas 5-FU with cisplatin is the most commonly used treatment around the world in the present target setting. While no trial including FOLFOX was assessed in the feasibility assessment it was agreed by the clinical experts that it is reasonable to assume similar efficacy between platinum-containing regimens (e.g., the cisplatin plus 5-FU [the KEYNOTE-590 trial65 comparator], cisplatin plus capecitabine, oxaliplatin plus capecitabine, and FOLFOX). It was also agreed by the clinical experts that FOLFIRI is used in Canada in patients who are platinum ineligible. FOLFIRI could not be considered equivalent to platinum-containing regimens according to the clinical experts. The clinical experts noted that epirubicin is not commonly used in Canadian clinical practice in the target setting.
The sponsor conducted a feasibility assessment using data obtained from a SLR.3 The SLR3 was provided with the sponsor’s submission to CADTH. The SLR was based on published results up to December 22, 2020. This CADTH report is current as of 2021.
Given there was no common comparator between the index trial, KEYNOTE-590,65 and the comparator trials and a high degree of heterogeneity in the baseline patient characteristics between studies, the sponsor’s rationale to assess the feasibility of an unanchored MAIC comparison appears reasonable. The CADTH clinical review team noted that an unanchored MAIC will only provide an unbiased comparison between an intervention of interest and the comparators if (1) all prognostic and effect modifying factors are known and included in the weighting process and (2) if it is reasonable to assume that all sourced of heterogeneity between the studies can be explained by the factors identified for the weighting process as opposed to other sources of heterogeneity, such as a difference related to the study design, outcomes, or treatment regimens. Unanchored MAICs are rarely able to fulfill these strict assumptions and it is very difficult to quantify or identify the direction of the resulting bias (relative treatment effect estimates from unanchored MAICs my over-und underestimate the true treatment effects).
The comparator trials included in the feasibility assessment were all small single-arm phase II trials (sample sizes ranged from N = 25 in Wolff et al. [2009]105 to N = 62 in Hironaka et al. [2014]104), except for Lee et al. (2015)103 (N = 94) which was a randomized phase II trial. The magnitude of the treatment effect estimates observed in a small study sample may not be replicable in a larger study sample or generalizable to the target population in real-world clinical practice. Phase II trials are hypothesis generating only and may not accurately predict harm and/or effectiveness of treatments.117,118 The primary objective of phase II (randomized or nonrandomized) trials is to document the safety outcomes and investigate if the estimate of effect for a new drug is large enough to use it in confirmatory phase III trials. An unanchored MAIC would compare the weighted treatment effects of the drug in the index trial, i.e., pembrolizumab plus cisplatin and 5-FU, to the treatment effect of a comparator (as reported directly from the comparator trial). The high uncertainty in the magnitude of treatment effects obtained in the small phase II comparator trials, would substantially limit the ability to interpret the relative treatments effects between pembrolizumab plus cisplatin and 5-FU and comparator interventions.
FOLFIRI is a relevant comparator to pembrolizumab plus cisplatin and 5-FU in the target setting of this review in patients who are platinum ineligible. The clinical experts consulted by CADTH noted that FOLFIRI could not be considered equivalent to platinum-containing regimens. The feasibility assessment included one trial by Wolff et al. (2009)105 that evaluated FOLFIRI. The trial by Wolff et al. (2009)105 was a small (N = 25) single-arm phase II trial evaluating FOLFIRI in patients with either locally advanced or metastatic adenocarcinomas or squamous cell carcinomas of the esophagus in Germany. The very small sample size and the phase II trial design of the study by Wolff et al. (2009)105 would introduce a high degree of uncertainty in the comparative treatment effects between pembrolizumab plus cisplatin and 5-FU and FOLFIRI.
In conclusion, the CADTH clinical review team agreed with the sponsor’s assessment that since the studies included in the feasibility assessment did not form a connected network it would not be feasible to perform a standard NMA. Given the previously mentioned key limitations the CADTH clinical review team confirmed that the results of an indirect comparison of pembrolizumab plus cisplatin and 5-FU to relevant comparators via an unanchored MAIC would likely be biased and it would not be possible to quantify or identify the direction of the bias. This would substantially limit the ability to interpret the comparative results between pembrolizumab plus cisplatin and 5-FU and relevant comparators.
Table 30: Summary of Trials Included in the Feasibility Assessment
Trial | Description |
|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | |
KEYNOTE-59065 | KEYNOTE-590 is an ongoing phase III double-blind, multi-centre, randomized controlled trial evaluating the efficacy and safety of pembrolizumab with cisplatin and 5-FU as compared to placebo with cisplatin and 5-FU. Patients were recruited internationally from Australia and countries in Asia, Europe, North America, and South America. Previously untreated patients with an ECOG score of 0-1 and locally advanced unresectable or metastatic adenocarcinoma or squamous cell carcinoma of the esophagus or advanced/metastatic Siewert type I adenocarcinoma of the GEJ were eligible for inclusion. Co-primary end points were OS and PFS per RECIST 1.1 between treatment arms and secondary end points included ORR per RECIST 1.1 and HRQoL between treatment arms. The most recent data cut-off was July 2, 2020 with a median follow-up of 13.4 months for patients receiving pembrolizumab plus cisplatin and 5-FU and 9.8 months in patients receiving placebo plus cisplatin and 5-FU. |
Capecitabine plus cisplatin | |
Lee 2008115 | A phase II single-arm trial evaluating capecitabine plus cisplatin as first-line chemotherapy in 45 patients with advanced esophageal squamous cell carcinoma. Patients were recruited from a single centre in South Korea. The primary objective was to evaluate the response rate per WHO criteria and secondary objectives were OS, TTP, and safety. The ORR was 57.8% with 0 CR and 26 PRs. The median duration of response in responders was 4.6 months. Median follow-up was 25.7 months, median TTP was 4.7 months, and median OS was 11.2 months. The most common grade 3/4 non-hematological adverse event was anorexia (9.4%) and the most common grade 3/4 hematological adverse event was neutropenia (17.3%). |
Lee 2015103 | A phase II, open-label trial evaluating capecitabine plus cisplatin as first-line treatment in 46 patients with metastatic esophageal squamous cell carcinoma. Patients were recruited from a single centre in South Korea. The primary objective of this study was to assess the response rate per RECIST 1.0 and secondary objectives included assessment of PFS, OS, toxicity, and HRQoL. The ORR was 57% with a median follow-up of 23 months. Median PFS was 5.1 months and median OS was 10.5 months. |
FOLFIRI | |
Wolff 2009105 | A phase II single-arm trial evaluating FOLFIRI as first-line treatment in 25 patients with either locally advanced or metastatic adenocarcinomas or squamous cell carcinomas of the esophagus. Patients were recruited from a single centre in Germany. The primary objective of this study was to assess median survival time from treatment initiation until the time of death or the last evaluation, secondary end points were the response rate (CR and PR in accordance with WHO criteria) and the proportion of patients with SD. Median survival was 13.6 months and the ORR was 33% with all patients achieving PR. |
Carboplatin plus docetaxel | |
EE298111 | A phase II single-arm trial evaluating docetaxel and carboplatin as first-line treatment in 32 patients with advanced squamous cell carcinoma of the esophagus. Patients were recruited from centres in the US and South Africa. The primary objective of this study was to assess the response rate. The ORR was 15.6%, one (3%) patient achieved complete response and 4 others (13%) achieved partial response. The most common grade 3 and 4 toxicities were leukopenia (78%) and neutropenia (84%). |
Cisplatin plus paclitaxel | |
Huang 2013107 | A phase II single-arm trial evaluating cisplatin and paclitaxel as first-line treatment in 46 patients with recurrent or metastatic esophageal squamous cell carcinoma. Patients were recruited from centre(s) in China. The primary objective of this study was to determine ORR and safety. The median follow-up was 18.2 months. The ORR was 56.5%, 2 (4.3%) patients achieved CR and 24 others (52.2%) achieved PR. The median PFS and OS were 5.6 months and 17.0 months, respectively. Hematological toxicity was most common; grade 3 and 4 neutropenia were observed in 37.0% and 23.9% of patients, respectively. |
Zhang 2008113 | A phase II single-arm trial evaluating cisplatin and paclitaxel as first-line treatment in 35 patients with unresectable and/or recurrent and/or metastatic esophageal squamous cell carcinoma. Patients were recruited from centres in China. The primary objective of this study was to determine response and survival rates. The median follow-up was 18.2 months. The ORR was 48.6%, one (2.8%) patient achieved CR and 16 others (45.7%) achieved PR. The median OS was 13.0 months, and the most common adverse events were neutropenia and nausea. |
Cisplatin plus docetaxel plus 5-FU | |
Hironaka et al. (2014)104 | A phase I/II single-arm trial evaluating cisplatin and docetaxel and 5-FU as first-line treatment in 62 patients with stage IV B or recurrent esophageal squamous cell carcinoma, adenosquamous carcinoma, and adenocarcinoma. Patients were recruited from centres in Japan. The primary objective of this study was to determine response and safety. The median follow-up was 15.6 months. The ORR was 62.3%, 0 patients achieved CR and 33 (62.3%) others achieved PR. The median PFS and OS were 5.8 months and 11.1 months, respectively. Common grade 3/4 adverse events were neutropenia (25%), anemia (36%), hyponatremia (29%), anorexia (24%), and nausea (11%). |
OGSG 0403108 | A phase II single-arm trial evaluating cisplatin plus docetaxel plus 5-FU as first-line treatment in 29 patients with metastatic squamous cell carcinoma of the esophagus. Patients were recruited from centres in Japan. The primary end point was ORR and the secondary end points were tolerability, OS, and PFS. The ORR was 34.5%, 3 patients achieved CR and 7 others achieved PR. The median PFS and OS were 85 days and 318 days, respectively. Grade 3 or 4 leukopenia or neutropenia occurred in 15 patients (52%) and 22 patients (76%). |
Ojima 2017106 | A phase I/II single-arm trial evaluating cisplatin plus docetaxel plus 5-FU as first-line treatment in 48 patients with recurrent/metastatic esophageal squamous cell carcinoma. Patients were recruited from centres in Japan. The primary objective of this study was to determine response, and the secondary end points were to evaluate OS, PFS, and treatment-related toxicity. The ORR was 62.5%, 6 (12.5%) patients achieved CR and 24 (50%) others achieved PR. The median PFS and OS were 6 months and 13 months, respectively. |
Osaka 2011112 | A phase II single-arm trial evaluating cisplatin plus docetaxel plus 5-FU as first-line treatment in 30 patients with advanced esophageal squamous cell carcinoma. Patients were recruited from a single centre in Japan. The ORR was 83.3%, 4 (13.3%) patients achieved CR and 21 (70%) others achieved PR. The median OS was 271 days. |
Takahashi 2010114 | A phase I/II single-arm trial evaluating cisplatin and docetaxel and 5-FU as first-line treatment in 51 patients with metastatic or recurrent squamous cell carcinoma of esophagus. Patients were recruited from a single centre in Japan. The primary end points of this study were ORR and descriptive summaries of adverse events. Secondary end points including PFS and OS. The ORR was 66.6%, 2 (5.1%) patients achieved CR and 24 (61.5%) others achieved PR. The median PFS and OS were 7 months and 13 months, respectively. |
Tanaka 2010110 | A phase I single-arm trial evaluating cisplatin plus docetaxel plus 5-FU as first-line treatment in 18 patients with advanced unresectable or recurrent squamous cell carcinoma of esophagus. Patients were recruited from a single centre in Japan. The ORR was 88.9%, 6 (33.3%) patients achieved CR and 10 (55.6%) others achieved PR. |
Cisplatin plus docetaxel | |
Kim 2010109 | A phase II, single-arm trial evaluating cisplatin plus docetaxel as first-line treatment in 30 patients with metastatic squamous cell esophageal cancer. Patients were recruited from centres in Korea. The ORR was 33.3%, 3 (7.7%) patients achieved CR and 10 (25.6%) others achieved PR. The median PFS and OS were 5 months and 8.3 months, respectively. |
5-FU, fluorouracil; CR, complete response; ECOG, Eastern Cooperative Oncology Group; EGJ, esophagogastric junction; FOLFIRI: irinotecan, 5-FU, oxaliplatin; FOLFOX: folinic acid, 5-FU, oxaliplatin; HRQoL, health-related quality of life; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; RECIST, Response Evaluation Criteria in Solid Tumors; TTP, time to progression; WHO, World Health Organization.
Table 31: Comparison of Feasibility Assessment Steps for Network Meta-Analysis Versus Unanchored Matching-Adjusted Indirect Comparisons, and Rationale for Changes Given Underlying Assumptions of Unanchored Matching-Adjusted Indirect Comparisons
Steps | Feasibility assessment steps for NMA | Feasibility assessment steps for unanchored MAIC | Description of change and rationale |
|---|---|---|---|
A | Assessment of the treatment (doses/schedules) or outcome definitions that are expected to modify relative treatment effects | Assessment of outcome definitions that are expected to modify relative treatment effects Should index trial definitions be adapted to align with external source(s)? | Remove treatments and align outcome definitions
May not be feasible to change the definitions in index trial if differences depending on data collection and/or tools to measure outcome |
B | Assessment of the distribution of study and patient characteristics that are expected to modify relative treatment effects | Assessment of the distribution of study and patient characteristics that are expected to modify absolute or relative treatment effects Should patients from the index trial be excluded to align with inclusion from external sources(s)? | Assessment of not only effect modifiers but also prognostic factors
|
C | Assessment of the baseline risk (placebo-response) that is also associated with the relative treatment effects | -- | Not applicable: Comparisons of baseline risk across the trials in an NMA require multiple trials with a placebo, which is not applicable to unanchored MAIC |
D | Assessment of observed treatment effects | Assessment of how the observed absolute effects are reported | Unlike with an NMA where evaluation of relative effects may be helpful to justify model choice (i.e., fixed versus random effects), for an unanchored MAIC the way the aggregate data are published will inform what comparisons are possible (which outcomes can be evaluated) and/or what assumptions are necessary (e.g., if only medians are reported rather than Kaplan-Meier curves) |
IPD, individual patient data; MAIC, matching-adjusted indirect comparison; NMA, network meta-analysis; RCT, randomized controlled trial.
Figure 44: Network Diagram of Studies Included in Feasibility Assessment
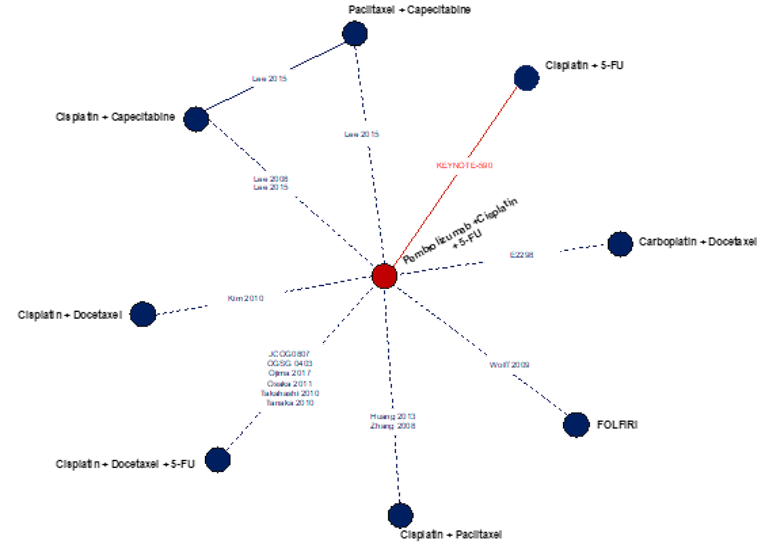
5-FU = 5-fluorouracil.
Note: Nodes connected by dashed lines were not compared in a head-to-head fashion by means of a randomized controlled trial.
Table 32: Study Characteristics of Trials Included in Feasibility Assessment
Trial ID | N | Study design | Phase | Masking | Treatment | Population source | Region | Study period | Median follow-up months (Range) |
|---|---|---|---|---|---|---|---|---|---|
KEYNOTE-590 | 749 | RCT | III | Double blind | Pembrolizumab + 5-FU + cisplatin | Multi-centre | Global (Asia, Australia, Europe, North America, and South America) | July 2017 - ongoing | Pembro arm: 12.6 (0.1 - 33.6) Placebo arm: 9.8 (0.1 – 33.6) |
Placebo + 5-FU + cisplatin | |||||||||
Lee 2015103 | 94 | RCT | II | Open label | Cisplatin + capecitabine | Single centre | South Korea | October 2008 - October 2018 | 23 |
Lee 2008 | 45 | Single-arm | II | Open label | Cisplatin + capecitabine | Single centre | South Korea | October 2003 - October 2006 | 25.7 (10.8 - 42.6) |
Wolff 2009105 | 25 | Single-arm | II | Open label | FOLFIRI | Single centre | Germany | — | 10 |
Kim 2010109 | 30 | Single-arm | II | Open label | Cisplatin + docetaxel | Single centre | Korea | — | 7.5 |
EE298111 | 32 | Single-arm | II | Open label | Carboplatin + docetaxel | Multi-centre | US and South Africa | — | — |
Huang 2013107 | 46 | Single-arm | II | Open label | Cisplatin + paclitaxel | — | China | — | 18.2 |
Zhang 2008113 | 39 | Single-arm | II | Open label | Cisplatin + paclitaxel | — | China | — | — |
Hironaka et al. (2014)104 | 62 | Single-arm | I/II | Open label | Cisplatin + docetaxel + 5-FU | Multi-centre | Japan | — | 15.6 |
OGSG 0403108 | 29 | Single-arm | II | Open label | Cisplatin + docetaxel + 5-FU | Multi-centre | Japan | — | — |
Ojima 2017106 | 48 | Single-arm | I/II | Open label | Cisplatin + docetaxel + 5-FU | — | Japan | — | — |
Osaka 2011112 | 30 | Single-arm | II | Open label | Cisplatin + docetaxel + 5-FU | Single centre | Japan | — | — |
Takahashi 2010114 | 51 | Single-arm | I/II | Open label | Cisplatin + docetaxel + 5-FU | Single centre | Japan | — | Mean: 13.3 |
Tanaka 2010110 | 18 | Single-arm | I | Open label | Cisplatin + docetaxel + 5-FU | Single centre | Japan | — | — |
5-FU, fluorouracil; RCT, randomized controlled trial, FOLFOX, folinic acid, 5-FU, oxaliplatin; FOLFIRI, folinic acid, 5-FU, irinotecan.
Table 33: Eligibility Criteria of Trials Included in Feasibility Assessment
Trial ID | Age (years) | Disease criteria | Previous therapy | Included histology | Excluded histology | Performance score |
|---|---|---|---|---|---|---|
KEYNOTE-590 | ≥18 | Locally advanced unresectable or metastatic | No previous therapy for advanced or metastatic disease | Esophageal adenocarcinoma, squamous cell carcinoma, or GEJ adenocarcinoma Siewert type I | — | ECOG 0-1 |
Lee 2008 | 18 - 75 | Advanced | No previous therapy or 5-FU-based adjuvant chemotherapy >12 months before study entry | Esophageal squamous cell carcinoma | Esophageal or EGJ adenocarcinoma | ECOG 0-2 |
Lee 2015103 | ≥18 | Metastatic or recurrent | No previous therapy for metastatic disease or only adjuvant chemotherapy >6 months before study entry | Esophageal squamous cell carcinoma | Esophageal adenocarcinoma or small cell carcinoma | ECOG 0-2 |
Wolff 2009105 | 18-75 | Locally advanced or metastatic | No previous systemic therapy | Esophageal adenocarcinoma or squamous cell carcinoma | — | ECOG 0-2 |
Kim 2010109 | 18-75 | Metastatic or recurrent | No previous systemic therapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
EE298111 | ≥18 | Advanced | No prior chemotherapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
Huang 2013107 | -- | Metastatic or recurrent | No previous systemic therapy or neoadjuvant or adjuvant chemotherapy <12 months before study entry | Esophageal squamous cell cancer | — | — |
Zhang 2008113 | 18-75 | Unresectable, recurrent, or metastatic | No previous systemic therapy or adjuvant chemotherapy <6 months before study entry | Esophageal squamous cell cancer | — | ECOG 0-2 |
Hironaka et al. (2014)104 | 20-75 | Metastatic or recurrent | No previous systemic therapy or neoadjuvant or adjuvant chemotherapy <6 months before study entry | Esophageal squamous cell carcinoma, adenosquamous carcinoma, and adenocarcinoma | — | ECOG 0-1 |
OGSG 0403108 | 20-75 | Metastatic | No previous treatment for cancer including surgery, chemotherapy, and radiotherapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
Ojima 2017106 | ≥20 | Metastatic or recurrent | No previous systemic therapy or adjuvant chemotherapy <1 month before study entry | Esophageal squamous cell cancer | — | ECOG 0-1 |
Osaka 2011112 | 20-80 | Advanced | No previous systemic therapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
Takahashi114 2010 | 20-80 | Metastatic or recurrent | No previous systemic therapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
Tanaka 2010110 | ≥18 | Advanced unresectable or recurrent | No previous systemic therapy | Esophageal squamous cell cancer | — | ECOG 0-2 |
ECOG, Eastern Cooperative Oncology Group; EGJ, esophagogastric junction.
Table 34: Patient Characteristics of Included Trials — Age, Sex, Race or Ethnicity
Trial ID | Treatment | N | Population | Median age (Range) | Male n, (%) | Caucasian n, (%) | Black n, (%) | Asian n, (%) |
|---|---|---|---|---|---|---|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | ||||||||
KEYNOTE-590 | Pembrolizumab + Cisplatin + 5-FU | 373 | Overall | 64 (28-94) | 306 (82) | 139 (37.3) | 5 (1.3) | 201 (53.9) |
Cisplatin + 5-FU | 376 | Overall | 62 (27-89) | 319 (84.8) | 139 (37) | 2 (0.5) | 199 (52.9) | |
Pembrolizumab + Cisplatin + 5-FU | 274 | ESCC | 64 (32-94) | 222 (81) | 70 (25.5) | 5 (1.8) | 183 (66.8) | |
Cisplatin + 5-FU | 274 | ESCC | 63 (35-89) | 232 (84.7) | 69 (52.2) | 0 | 181 (66.1) | |
Capecitabine plus cisplatin | ||||||||
Lee 2008 | Capecitabine + Cisplatin | 45 | Overall | 62 (47-72) | 44 (97.8) | — | — | — |
Lee 2015 | (Capecitabine + Cisplatin) and (Capecitabine + Paclitaxel) | 94 | Overall | 63 (34-82) | 92 (97.9)** | — | — | — |
Capecitabine + Paclitaxel | 48 | Overall | 63 (34-82) | 47 (97.9)** | — | — | — | |
Capecitabine + Cisplatin | 46 | Overall | 62 (46-76) | 45 (97.8)** | — | — | — | |
FOLFIRI | ||||||||
Wolff 2009 | FOLFIRI | 24 | Overall | 58 (44-75) | 19 (79) | — | — | — |
Carboplatin plus docetaxel | ||||||||
E2298 | Carboplatin + Docetaxel | 32 | Overall | 64 (41-80) | 25 (78) | 16 (50) | 16 (50) | — |
Cisplatin plus paclitaxel | ||||||||
Huang 2013 | Paclitaxel + Cisplatin | 46 | Overall | 56.2 (42-71) | 38 (82.6) | — | — | 46 (100) |
Zhang 2008 | Paclitaxel + Cisplatin | 39 | Overall | 58 (41-72) | 36 (92) | — | — | 39 (100) |
Cisplatin plus docetaxel plus 5-FU | ||||||||
JCOG0807 | Cisplatin + Docetaxel + 5-FU | 55 | Overall | 61 (44-75) | 49 (89.1) | — | — | 55 (100) |
OGSG 0403 | Cisplatin + Docetaxel + 5-FU | 29 | Overall | 61 (38-73) | 22 (76)** | — | — | 29 (100) |
Ojima 2017 | Cisplatin + Docetaxel + 5-FU | 48 | Overall | 67 (48-84) | 44 (92)** | — | — | 48 (100) |
Osaka 2011 | Cisplatin + Docetaxel + 5-FU | 30 | Overall | 58.1 (40-73)* | 26 (87)** | — | — | 30 (100) |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 39 | Overall | 65.2 (44-79)* | 34 (87) | — | — | 39 (100) |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 12 | Overall | 63.9 (53-74)* | 10 (83) | — | — | 12 (100) |
Tanaka 2010 | Cisplatin + Docetaxel + 5-FU | 18 | Overall | 62.8 (50-79) | 15 (83.3) | — | — | 18 (100) |
Cisplatin plus docetaxel | ||||||||
Kim 2010 | Cisplatin + Docetaxel | 39 | Overall | 65 (46-75) | 39 (100) | — | — | 39 (100) |
5-FU = 5-Fluorouracil; ESCC = Esophageal squamous cell cancer.
*Mean reported.
**Calculated.
*^ Mean (SD) reported.
Table 35: Patient Characteristics of Included Trials — Extent of Disease
Trial ID | Treatment | N | Population | Locally advanced, n (%) | Metastatic, n (%) | Locally recurrent, n (%) | Other, n (%) |
|---|---|---|---|---|---|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | |||||||
KEYNOTE-590 | Pembrolizumab + Cisplatin + 5-FU | 373 | Overall | 29 (7.8) | 344 (92.2) | — | — |
Cisplatin + 5-FU | 376 | Overall | 37 (9.8) | 339 (90.2) | — | — | |
Pembrolizumab + Cisplatin + 5-FU | 274 | ESCC | 21 (7.7) | 253 (92.3) | — | — | |
Cisplatin + 5-FU | 274 | ESCC | 30 (10.9) | 244 (89.1) | — | — | |
Capecitabine plus cisplatin | |||||||
Lee 2008 | Capecitabine + Cisplatin | 45 | Overall | 37 (82.2) | — | — | — |
Lee 2015 | (Capecitabine + Cisplatin) and (Capecitabine + Paclitaxel) | 94 | Overall | 59 (62.8) | 90 (96) | 35 (37.2) | — |
Capecitabine + Paclitaxel | 48 | Overall | 30 (62.5) | 47 (98) | 18 (37.5) | — | |
Capecitabine + Cisplatin | 46 | Overall | 43 (93.4) | 3 (6.5) | 17 (37) | — | |
FOLFIRI | |||||||
Wolff 2009 | FOLFIRI | 24 | Overall | 3 (12) | 21 (88) | — | — |
Carboplatin plus docetaxel | |||||||
E2298 | Carboplatin + Docetaxel | 32 | Overall | — | 23 (72) | — | — |
Cisplatin plus paclitaxel | |||||||
Huang 2013 | Cisplatin + Paclitaxel | 46 | Overall | 7 (15.2) | 39 (84.8) | — | — |
Zhang 2008 | Cisplatin + Paclitaxel | 39 | Overall | — | — | — | — |
Cisplatin plus docetaxel plus 5-FU | |||||||
JCOG0807 | Cisplatin + Docetaxel + 5-FU | 55 | Overall | — | 55 (100) | — | — |
OGSG 0403 | Cisplatin + Docetaxel + 5-FU | 29 | Overall | — | 29 (100) | — | — |
Ojima 2017 | Cisplatin + Docetaxel + 5-FU | 48 | Overall | — | 48 (100) | — | — |
Osaka 2011 | Cisplatin + Docetaxel + 5-FU | 30 | Overall | — | 25 (83.3) | — | — |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 39 | Overall | — | 16 (41)* | 23 (59) | — |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 12 | Overall | — | 9 (75)* | 3 (25) | — |
Tanaka 2010 | Cisplatin + Docetaxel + 5-FU | 18 | Overall | 9 (50) | 9 (50) | — | — |
Cisplatin plus docetaxel | |||||||
Kim 2010 | Cisplatin + Docetaxel | 39 | Overall | 39 (100) | — | — | |
5-FU = 5-Fluorouracil; ESCC = Esophageal squamous cell cancer.
*Calculated.
Table 36: Patient Characteristics of Included Trials — ECOG Performance Scores
Trial ID | Treatment | N | Population | Performance scoring scale | Performance score, n (%) | Performance score 1, n (%) | Performance score 2, n (%) |
|---|---|---|---|---|---|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | |||||||
KEYNOTE-590 | Pembrolizumab + Cisplatin + 5-FU | 373 | Overall | ECOG | 149 (39.9) | 223 (59.8) | 1 (0.3) |
KEYNOTE-590 | Cisplatin + 5-FU | 376 | Overall | ECOG | 150 (39.9) | 225 (59.8) | 1 (0.3) |
KEYNOTE-590 | Pembrolizumab + Cisplatin + 5-FU | 274 | ESCC | ECOG | 103 (37.6) | 171 (62.4) | — |
KEYNOTE-590 | Cisplatin + 5-FU | 274 | ESCC | ECOG | 105 (38.3) | 169 (61.7) | — |
Capecitabine plus cisplatin | |||||||
Lee 2008 | Capecitabine + Cisplatin | 45 | Overall | ECOG | — | — | 4 (8.9) |
Lee 2015 | (Capecitabine + Cisplatin) and (Capecitabine + Paclitaxel) | 94 | Overall | ECOG | — | — | — |
Lee 2015 | Capecitabine + Paclitaxel | 48 | Overall | ECOG | — | — | — |
Lee 2015 | Capecitabine + Cisplatin | 46 | Overall | ECOG | — | — | — |
FOLFIRI | |||||||
Wolff 2009 | FOLFIRI | 24 | Overall | ECOG | 3 (12) | 17 (71) | 4 (17) |
Carboplatin plus docetaxel | |||||||
E2298 | Carboplatin + Docetaxel | 32 | Overall | ECOG | 5 (16) | 22 (68) | 5 (16) |
Cisplatin plus paclitaxel | |||||||
Huang 2013 | Cisplatin + Paclitaxel | 46 | Overall | ECOG | 12 (26.1) | 33 (71.7) | 1 (2.2) |
Zhang 2008 | Cisplatin + Paclitaxel | 39 | Overall | ECOG | 12 (31) | 20 (51) | 7 (18) |
Cisplatin plus docetaxel plus 5-FU | |||||||
JCOG0807 | Cisplatin + Docetaxel + 5-FU | 55 | Overall | ECOG | 39 (70.9) | 16 (29.1) | — |
OGSG 0403 | Cisplatin + Docetaxel + 5-FU | 29 | Overall | ECOG | 25 (86.2)* | 4 (13.8)* | 0* |
Ojima 2017 | Cisplatin + Docetaxel + 5-FU | 48 | Overall | ECOG | 40 (83.3)* | 8 (9.6)* | 0* |
Osaka 2011 | Cisplatin + Docetaxel + 5-FU | 30 | Overall | ECOG | — | 18 (60) | 12 (40) |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 39 | Overall | ECOG | 29 (74.4)* | 10 (25.6)* | — |
Takahashi 2010 | Cisplatin + Docetaxel + 5-FU | 12 | Overall | ECOG | 10 (83.3)* | 2 (16.7)* | — |
Tanaka 2010 | Cisplatin + Docetaxel + 5-FU | 18 | Overall | ECOG | — | — | 0 |
Cisplatin plus docetaxel | |||||||
Kim 2010 | Cisplatin + Docetaxel | 39 | Overall | ECOG | 2 (5) | 35 (90) | 2 (5) |
5-FU, 5-Fluorouracil; ECOG, Eastern Cooperative Oncology Group; ESCC = Esophageal squamous cell cancer.
*Calculated.
Table 37: Outcome Definitions of Studies Included in Feasibility Assessment
Trial ID | Overall survival definition | Progression-free survival definition | ORR definition | Criteria used | HRQoL | HRQoL measure used |
|---|---|---|---|---|---|---|
KEYNOTE-590 | Time from randomization to death due to any cause | Time from randomization to disease progression or death, whichever occurs first | Percentage of patients who have CR or PR | RECIST 1.1 | Yes | EORTC QLQ-C30; EORTC QLQ-OES18; EQ-5D |
Lee 2008 | — | TTP | — | WHO | No | -- |
Lee 2015103 | — | — | — | RECIST 1.0 | Yes | EORTC QLQ-OES18 |
Wolff 2009105 | Time from treatment initiation until the time of death or the last evaluation, | TTP | — | — | No | — |
Kim 2010109 | — | — | — | RECIST | No | — |
EE298111 | — | — | — | — | No | — |
Huang 2013107 | — | — | — | RECIST 1.0 | No | — |
Zhang 2008113 | Date of when treatment began to the date of death, or up to the most recent follow-up visit | The time to progression was measured from the date the treatment began to the date of progression | CR was defined as the disappearance of all target lesions persisting for more than 4 weeks. A partial response was defined as a minimum of a 30% decrease in the sum of the longest diameter of target lesions persisting for more than 4 weeks. | RECIST | No | — |
Hironaka et al. (2014)104 | — | — | — | RECIST 1.0 | No | — |
OGSG 0403108 | — | — | — | — | No | — |
Ojima 2017106 | — | — | — | RECIST 1.0 | No | — |
Osaka 2011112 | — | — | — | RECIST | No | — |
Takahashi 2010114 | — | — | — | RECIST | No | — |
Tanaka 2010110 | — | — | — | — | No | — |
CR, complete response; EORTC QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core Module; EORTC QLQ-OES18, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Oesophageal Module; PR, partial response, RECIST, Response Evaluation Criteria in Solid Tumors; TTP, time to progression; WHO, World Health Organization.
Table 38: Outcome Availability and Definitions of Studies Included in Feasibility Assessment
Trial ID | OS | PFS | ORR | Adverse events | Reported adverse events | HRQoL | ||
|---|---|---|---|---|---|---|---|---|
Median | KM | Median | KM | |||||
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | ||||||||
KEYNOTE-590 | YES | YES | YES | YES | YES | YES | Drug-related AEs Grade 3-5 AEs (all drug related) Serious AEs (all drug related) Discontinuation due to AEs | YES |
Capecitabine plus cisplatin | ||||||||
Lee 2008 | YES | YES | —* | —* | YES | YES | Grade 3-4 AEs (all) | — |
Lee 2015103 | YES | YES | YES | YES | YES | YES | Grade 3-4 AEs (all) | YES |
FOLFIRI | ||||||||
Wolff 2009105 | YES | YES | YES | — | YES* | YES | Individual AEs | — |
Carboplatin plus docetaxel | ||||||||
EE298111 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
Cisplatin plus paclitaxel | ||||||||
Huang 2013107 | YES | YES | YES | — | YES | YES | Individual AEs | — |
Zhang 2008113 | YES | YES | YES | — | YES | YES | Individual AEs | — |
Cisplatin plus docetaxel plus 5-FU | ||||||||
Hironaka et al. (2014)104 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
OGSG 0403108 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
Ojima 2017106 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
Osaka 2011112 | YES | YES | — | — | YES | YES | Individual AEs | — |
Takahashi 2010114 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
Tanaka 2010110 | — | — | — | — | YES | YES | Individual AEs | — |
Cisplatin plus docetaxel | ||||||||
Kim 2010109 | YES | YES | YES | YES | YES | YES | Individual AEs | — |
AE, adverse event; HRQoL, health-related quality of life; KM, Kaplan-Meier; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
*= TTP was reported instead of PFS (KM curve available).
Table 39: Treatment Regimens of Studies Included in Feasibility Assessment
Trial | Regimen | Agent | Dosing and schedule |
|---|---|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | |||
KEYNOTE-59065 | Pembrolizumab + Cisplatin + 5-FU | Pembrolizumab | IV (200mg; D1, Q3W; UDP) |
Cisplatin | IV (80mg/m2; D1; Q3W; UDP) | ||
5-FU | IV (800mg/m2; D1-5; Q3W; UDP) | ||
Cisplatin + 5-FU | Cisplatin | IV (80mg/m2; D1; Q3W; UDP) | |
5-FU | IV (800mg/m2; D1-5; Q3W; UDP) | ||
Capecitabine plus cisplatin | |||
Lee 2008115 | Cisplatin + Capecitabine | Capecitabine | PO (1,250mg/m2; D1-14 BID; Q3W; UDP) |
Cisplatin | IV (60mg/m2; D1; Q3W; UDP) | ||
Lee 2015103 | Cisplatin + Capecitabine | Capecitabine | PO (1,000mg/m2; D1-14 BID; Q3W; UDP) |
Cisplatin | IV (75mg/m2; D1; Q3W; UDP) | ||
FOLFIRI | |||
Wolff 2009105 | FOLFIRI | Irinotecan | IV (80mg/m2; D1,D8,D15,D22,D29,D36; Cycle length: 57 days; UDP) |
Sodium folic acid | IV (500mg/m2; D1,D8,D15,D22,D29,D36; Cycle length: 57 days; UDP) | ||
5-FU | IV (2000mg/m2; D1,D8,D15,D22,D29,D36; Cycle length: 57 days; UDP) | ||
Carboplatin plus docetaxel | |||
EE298111 | Carboplatin + Docetaxel | Docetaxel | IV (75mg/m2; D1; Cycle length: 3 weeks; Max no. cycles: 6 cycles) |
Carboplatin | IV (6AUC; D1; Cycle length: 3 weeks; Max no. cycles: 6 cycles) | ||
Cisplatin plus paclitaxel | |||
Huang 2013107 | Cisplatin + Paclitaxel | Paclitaxel | IV (150mg/m2; D1; Cycle length: 14 days; UDP) |
Cisplatin | IV (50mg/m2; D2; Cycle length: 14 days; UDP) | ||
Zhang 2008113 | Cisplatin + Paclitaxel | Paclitaxel | IV (175mg/m2; D1; Cycle length: 21 days; Max no. cycles: 6 cycles) |
Cisplatin | IV (75mg/m2; D1; Cycle length: 21 days; Max no. cycles: 6 cycles) | ||
Cisplatin plus docetaxel plus 5-FU | |||
Hironaka et al. (2014)104 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (30-40mg/m2; D1, D15; Cycle length: 4 weeks; UDP or intolerable AEs) |
Cisplatin | IV (80mg/m2; D1; Cycle length: 4 weeks; UDP or intolerable AEs) | ||
5-FU | IV (800mg/m2; D1-D5; Cycle length: 4 weeks; UDP or intolerable AEs) | ||
OGSG 0403108 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (60mg/m2; D1; Cycle length: 4 weeks; UDP) |
Cisplatin | IV (70mg/m2; D1; Cycle length: 4 weeks; UDP) | ||
5-FU | IV (600mg/m2; D1-D5; Cycle length: 4 weeks; UDP) | ||
Ojima 2017106 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (30-40mg/m2; D1, D8; Cycle length: 4 weeks; UDP or intolerable AEs) |
Cisplatin | IV (12mg/m2; D1-D5; Cycle length: 4 weeks; UDP or intolerable AEs) | ||
5-FU | IV (600mg/m2; D1-D5; Cycle length: 4 weeks; UDP or intolerable AEs) | ||
Osaka 2011112 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (60mg/m2; D1; Cycle length: 3-4 weeks; Twice) |
Cisplatin | IV (60mg/m2; D1; Cycle length: 3-4 weeks; Twice) | ||
5-FU | IV (800mg/m2; D1-D5; Cycle length: 3-4 weeks; Twice: 1 cycle) | ||
Takahashi 2010114 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (40/50/60mg/m2; D1; Cycle length: 3 weeks; UDP) |
Cisplatin | IV (70mg/m2; D1; Cycle length: 3 weeks; UDP) | ||
5-FU | IV (700mg/m2; D1-D5; Cycle length: 3 weeks; UDP) | ||
Tanaka 2010110 | Cisplatin + Docetaxel + 5-FU | Docetaxel | IV (30-40mg/m2; D1, D15; Cycle length: 28 days; UDP) |
Cisplatin | IV (40mg/m2; D1, D15; Cycle length: 28 days; UDP) | ||
5-FU | IV (400mg/m2; D1-D5 and D15-D19; Cycle length: 28 days; UDP) | ||
Cisplatin plus docetaxel | |||
Kim 2010109 | Cisplatin + Docetaxel | Docetaxel | IV (70mg/m2; D1; Cycle length: 21 days; UDP or intolerable AEs) |
Cisplatin | IV (70mg/m2; D1; Cycle length: 21 days; UDP or intolerable AEs) | ||
5-FU, fluorouracil; BID, twice daily; IV, intravenous; PO, oral; Q3W, every 3 weeks; UDP, until disease progression.
Table 40: Survival and Response Outcomes for the Trials Included in the Feasibility Assessment
Trial | Regimen | N | Median OS (95% CI), months | Median PFS (95% CI), months | ORR, n (%) | CR, n (%) | PR, n (%) | SD, n (%) | PD, n (%) | Median DOR (95% CI), months | |
|---|---|---|---|---|---|---|---|---|---|---|---|
Pembrolizumab plus cisplatin and 5-FU versus placebo plus cisplatin and 5-FU | |||||||||||
KEYNOTE-59065 | Pembrolizumab + Cisplatin + 5-FU | 373 | 12.4 (10.5-14) | 6.3 (6.2-6.9) | 168 (45) | 24 (6.4) | 144 (38.6) | 128 (34.3) | 42 (11.3) | 8.3 (1.2+ - 31+) | |
Cisplatin + 5-FU | 376 | 9.8 (8.8-10.8) | 5.8 (5.0-6.0) | 110 (29.3) | 9 (2.4) | 101 (26.9) | 174 (46.3) | 59 (15.7) | 6 (1.5+ - 25+) | ||
Capecitabine plus cisplatin | |||||||||||
Lee 2008115 | Cisplatin + Capecitabine | 45 | 11.2 (8.5-13.9) | 4.7 (2.5-7)* | 26 (57.8) | 0 (0) | 26 (57.8) | 6 (13.3) | 6 (13.3) | 4.6 (1-15.6) | |
Lee 2015103 | Cisplatin + Capecitabine | 46 | 10.5 (9.2-11.9) | 5.1 (4.0-6.2) | 26 (57) | 0 (0) | 26 (57) | 10 (22) | 3 (7) | 4 (1-31) | |
FOLFIRI | |||||||||||
Wolff 2009105 | FOLFIRI | 24 | 13.6 (7.1-20.1) | 6.6 (1.6-24.6)** | -- | -- | 8 (33) | 9 (38) | 2 (8) | -- | |
Carboplatin plus docetaxel | |||||||||||
EE298111 | Carboplatin + Docetaxel | 32 | 6.7 | 3.2 | 5 (15.6) | 1 (3) | 4 (13) | 13 (41) | 9 (28) | -- | |
Cisplatin plus paclitaxel | |||||||||||
Huang 2013107 | Cisplatin + Paclitaxel | 46 | 17 (12.3-23.7) | 5.6 (2.8-8.4) | 26 (56.5) | 2 (4.3) | 24 (52.2) | 16 (34.8) | 3 (6.5) | -- | |
Zhang 2008113 | Paclitaxel + Cisplatin | 39 | 13 (10.5-15.4) | 7 (4.83-9.16) | 17 (48.6) | 1 (2.8) | 16 (45.7) | 15 (42.9) | 3 (8.5) | -- | |
Cisplatin plus docetaxel plus 5-FU | |||||||||||
Hironaka et al. (2014)104 | Cisplatin + Docetaxel + 5-FU | 53 | 11.1 (9.4-13.8) | 5.8 (4.6-7.4) | 33 (62.3) | 0 | 33 (62.3) | 8 (15.1) | 9 (17) | -- | |
OGSG 0403108 | Cisplatin + Docetaxel + 5-FU | 29 | 318 (240-421)*** | 85 (81-159)*** | 10 (34.5) | -- | 7 (24.1) | -- | -- | -- | |
Ojima 2017106 | Cisplatin + Docetaxel + 5-FU | 48 | 13 (9.7-16.3) | 6 (3.7-8.3) | 30 (62.5) | 6 (12.5) | 24 (50) | 10 (20.8) | 8 (16.7) | -- | |
Osaka 2011112 | Cisplatin + Docetaxel + 5-FU | 30a | 271*** | -- | 25 (83.3) | 4 (13.3) | 21 (70) | 2 (6.7) | 0 | -- | |
29b | -- | -- | 21 (72.4) | 3 (10.3) | 18 (62.1) | 5 (17.2) | 0 | -- | |||
25c | -- | -- | 18 (72) | 3 (12) | 15 (60) | 6 (24) | 0 | -- | |||
Takahashi 2010114 | Cisplatin + Docetaxel + 5-FU | 39 | 13 | 7 | 26 (66.6) | 2 (5.1) | 24 (61.5) | 12 (30.8) | 1 (2.6) | -- | |
Tanaka 2010110 | Cisplatin + Docetaxel + 5-FU | 18 | -- | -- | 16 (88.9) | 6 (33.3) | 10 (55.6) | 1 (5.6) | 1 (5.6) | -- | |
Cisplatin plus docetaxel | |||||||||||
Kim 2010109 | Cisplatin + Docetaxel | 39 | 8.3 (7.3-9.4) | 5 (2.7-7.3) | 13 (33.3) | 3 (7.7) | 10 (25.6) | 11 (28.2) | 10 (25.6) | -- | |
5-FU, fluorouracil; CI, confidence interval; CR, complete response; DOR, duration of response; ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease.
*TTP reported instead of PFS, **Median (range); ***Days reported; aPatients with radiological evaluation of primary lesion response; bPatients with radiological evaluation of lymph node response; cPatients with radiological evaluation of distant organ response.
Pharmacoeconomic Review
Abbreviations
5-FU
5-fluorouracil
AE
adverse event
BIA
budget impact analysis
CAPOX
capecitabine and oxaliplatin
CPS
combined positive score
EC
esophageal cancer
EGJ
esophagogastric junction
FOLFOX
5-fluorouracil, oxaliplatin, and leucovorin
HER2
human epidermal growth factor receptor 2
ICER
incremental cost-effectiveness ratio
OS
overall survival
PD-L1
programmed cell death ligand 1
PFS
progression-free survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
ToT
time on treatment
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), IV infusion |
Submitted price | Pembrolizumab IV infusion: $4,400 per 4 mL vial |
Indication | First-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the esophagogastric junction (tumour centre 1 cm to 5 cm above the gastric cardia) |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project Orbis |
NOC date | June 4, 2021 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed and is currently under review for multiple indications at CADTH. The following indications were reviewed in 2020 or were ongoing at the completion of this review: Indication: Refractory or relapsed classical Hodgkin lymphoma Recommendation date: Under review Recommendation: Under review Indication: Head and neck squamous cell carcinoma Recommendation date: December 22, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level Indication: Renal cell carcinoma Recommendation date: April 2, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level Indication: Squamous non–small cell lung cancer Recommendation date: January 3, 2020 Recommendation: Recommended on the condition of cost-effectiveness being improved to an acceptable level |
HER2 = human epidermal growth factor receptor 2; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients (aged 18 years and older) with locally advanced unresectable or metastatic, cancer of the esophagus or HER2-negative esophagogastric junction; aligns with reimbursement request |
Treatments | Pembrolizumab in combination with 5-FU and cisplatin |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs and LYs |
Time horizon | Lifetime (20 years) |
Key data source | KEYNOTE-590 trial was used to inform PFS, OS, TTD, and health utility values |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
5-FU = 5-fluorouracil; CAPOX = capecitabine and oxaliplatin; FOLFOX = 5-FU and oxaliplatin and leucovorin; HER2 = human epidermal growth factor receptor; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; TTD = time to death; WTP = willingness to pay.
aDue to limitations with the use of a blended comparator, and concerns with the validity of the sponsor’s calculations, the blended comparator was not considered within the CADTH reanalysis.
Conclusions
Evidence from the KEYNOTE-590 trial indicated that compared to placebo in combination with cisplatin and 5-fluorouracil (5-FU), first-line treatment with pembrolizumab in combination with cisplatin and 5-FU showed a clinically meaningful and statistically significant overall and progression-free survival (PFS) benefit in adult patients with locally advanced unresectable or metastatic, cancer of the esophagus or human epidermal growth factor receptor (HER2)-negative esophagogastric junction (EGJ; tumour centre 1 cm to 5 cm above the gastric cardia), based on the data currently analyzed. As the study is ongoing, additional long-term efficacy and safety information are anticipated. Survival models used to extrapolate overall survival (OS) data drove the modelled cost-effectiveness of pembrolizumab in combination with chemotherapy compared to chemotherapy.
CADTH identified several limitations within the sponsor’s economic analysis, specifically the uncertainty associated with the use of interim PFS and OS data from the KEYNOTE-590 trial and application of these data within a partitioned survival model, the assumptions regarding comparators and background chemotherapy, an inappropriate source for end-of-life cost, and overestimated proportion of patients who are likely to receive subsequent treatments post-progression.
CADTH undertook a revised base case that was derived by correcting drug administration fees for the 5-fluorouracil, oxaliplatin, and leucovorin (FOLFOX) and capecitabine and oxaliplatin (CAPOX) regimens (considered in blended chemotherapy), as well as the leucovorin dose, and using publicly listed prices for 5-FU, oxaliplatin, and leucovorin. Canadian end-of-life costs specific to esophageal adenocarcinoma were also incorporated, reducing the proportion of patients requiring subsequent treatments to 10% as suggested by the clinical experts consulted by CADTH, and a treatment-waning assumption was applied to account for the uncertainty resulting from the use of interim analysis.
Although CADTH’s base case resulted in a higher incremental cost-effectiveness ratio (ICER) than the sponsor’s base case ($170,819 per quality-adjusted life-year [QALY] versus $142,861 per QALY), both analyses provided consistent results, suggesting that pembrolizumab in combination with a chemotherapy backbone was associated with higher costs and improved QALYs but was not cost-effective at a $50,000 per QALY willingness-to-pay threshold compared to 5-FU in combination with cisplatin at the submitted price. A price reduction of at least 75% would be required to make pembrolizumab an optimal treatment option at a willingness-to-pay threshold of $50,000 per QALY. The cost-effectiveness of pembrolizumab in combination with 5-FU and cisplatin was highly sensitive to statistical approaches used to fit the OS data, with the ICERs ranging from $176,963 per QALY to $306,332 per QALY.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process, specifically, information that pertains to the economic submission.
Three patient groups (Colorectal Cancer Canada, Gastrointestinal Society, and My Gut Feeling [Stomach Cancer Foundation of Canada]) used an online patient and caregiver survey to capture patient perspectives on pembrolizumab for first-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER-2 negative gastroesophageal junction adenocarcinoma in combination with platinum- and fluoropyrimidine-based chemotherapy. The survey collected patient input from 25 patients and 8 caregivers from the UK and Northern Ireland, US, Canada, New Zealand, Ireland, and Belgium. The participants reported several symptoms of esophageal cancer (EC) that affect quality of life, including trouble swallowing, heartburn, weight loss, fatigue, worsening indigestion, frequent choking on food, hiccups, and indigestion. Treatments include chemotherapy (96.7%), surgery (66.7%), radiation therapy (50.0%), endoscopic therapy (16.7%), and other targeted therapies (10.0%). The majority of patients and caregivers reported improvement in symptoms of EC under standard care with some common side effects, including fatigue, nausea, loss of appetite, and low white blood cell count. Patients expressed a desire for new treatments that prolong life, increase metabolism, stop tumour growth, and improve quality of life (such as the ability to consume food, go out, and carry on a conversation). Almost all patients and caregivers expressed a willingness to take a drug that improves quality of life even if OS is not prolonged. Patients are willing to tolerate some side effects to extend survival. One patient with stage III EC and 1 with stage IV EC had experience with the drug under review. While taking pembrolizumab, 1 patient reported side effects such as abdominal pain, diarrhea, rash, shortness of breath, and constipation. The other patient reported fatigue, itching, and some allergic reactions. The symptoms reported less effectively managed under pembrolizumab compared to existing therapies include coughing, back pain, hoarseness, and vomiting. The symptoms reported as better managed under pembrolizumab include pain behind the breastbone or in the throat, black stool, weight loss, fatigue, and vomiting.
Input was received from 2 groups: the Ontario Health Cancer Care Ontario Gastrointestinal Drug Advisory, and a joint submission on behalf of My Gut Feeling, the Canadian Gastrointestinal Oncology Evidence Network, and Colorectal Cancer Canada. Clinicians noted some treatment gaps; specifically, that not all patients respond to the available systemic treatments or are refractory to the available treatments, while others respond for only a short duration. Clinician also noted pembrolizumab will be an addition to currently available treatment in the first-line setting as it can assist patients achieve the treatment goals of prolonging life, delaying disease progression, and maintaining a good weight, quality of life, and nutrition. The clinician input also noted that in the KEYNOTE-590 study interim analysis, the best benefit was reported in patients with a programmed cell death ligand 1 (PD-L1) combined positive score (CPS) score of 10 or greater, but this testing is not routine in current practice, nor expected to be in the future, thus the treatment should not be restricted to this subgroup.
The drug plans noted that health care providers are familiar with the preparation, administration, and monitoring of pembrolizumab infusions. The drug plans also noted there is a time-limited need to allow the addition of pembrolizumab to treatment of patients who are currently on a platinum- and fluoropyrimidine-based chemotherapy, which means the number of patients on pembrolizumab may be higher than estimated. The reimbursement of pembrolizumab in the first-line setting would also likely shift other systemic therapies to later lines of therapy, which may result in higher budget impact than estimated.
The following concerns were addressed in the sponsor's economic model.
Clinical benefits such as delaying disease progression, prolonging OS, and adverse events (AEs) associated with pembrolizumab in combination with 5-FU and cisplatin were considered.
A subgroup analysis for patients with PD-L1 with a CPS of 10 or greater was conducted by the sponsor.
Drug administration fees for pembrolizumab were considered in the sponsor’s model.
In addition, CADTH addressed the following concern.
The impact of pembrolizumab on subsequent lines of systematic therapies was a noted concern. CADTH performed scenario analyses assessing alternate assumptions regarding subsequent treatments.
CADTH was unable to address the following concern raised from stakeholder input.
The drug plans expressed concern about the timing to add and the financial impact of prescribing pembrolizumab to patients who are currently on platinum- and fluoropyrimidine-based chemotherapy.
Economic Review
The current review is for pembrolizumab (Keytruda) for the first-line treatment of locally advanced unresectable or metastatic esophageal and HER2-negative EGJ cancer.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for pembrolizumab in combination with 5-FU and cisplatin for the first-line treatment of locally advanced unresectable or metastatic esophageal and HER2-negative EGJ cancer. Comparators included 5-FU combined with cisplatin and blended chemotherapy which consisted of 5-FU in combination with cisplatin (13%), capecitabine in combination with cisplatin (7%), FOLFOX (64%), and CAPOX (17%).1 The modelled population was in line with the reimbursement request and Health Canada–approved indication.
Pembrolizumab is available as powder for solution for infusion (100 mg/4 mL vial). The recommended dosage is pembrolizumab 200 mg every 3 weeks in combination with 5-FU 800 mg/m2 every 3 weeks (days 1 to 5) and cisplatin 80 mg/m2 infusion over 2 hours, every 3 weeks.2 At the submitted price of $4,400 per 4 mL vial, the per cycle cost of pembrolizumab was estimated to be $8,800, assuming 100% dose intensity. When used in combination with 5-FU and cisplatin, at the sponsor’s assumed dose intensities, the total regimen cost per cycle was $8,472.27. The total regimen costs per cycle for 5-FU in combination with cisplatin and blended chemotherapy were $282.66 and $1,102.55, respectively, per the sponsor’s submitted analysis (CADTH corrections altered these estimates to $461.59 and $273.21, respectively). The sponsor considered vial sharing (50%) and relative dose intensity (RDI) in the first-line drug cost calculation.1
The clinical outcome was QALYs and life-years. The economic analysis was undertaken over a time horizon of 20 years from the perspective of a Canadian publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.1
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: progression-free, progressive disease, and death (Appendix 3; Figure 1). The proportion of patients who were progression-free, who experienced progressive disease, or who were dead at any time over the model horizon was derived from non-mutually exclusive survival curves. All patients entered in the progression-free state and were assumed to receive treatments until disease progression and/or the development of treatment-limiting or treatment-related AEs. Patients could discontinue treatment but remain in the progression-free health state based on the time-on-treatment (ToT) curve and, upon discontinuation, the cost of treatment would no longer be incurred. At the end of each weekly cycle, the proportion of patients with progressive disease or death was derived based on the area under the survival curves. Specifically, OS was partitioned to estimate the proportion of patients in the death state, while the PFS was used to estimate the proportion of patients in the progression-free health state. The difference between the OS curve and PFS curve was partitioned at each time point to estimate the proportion of patients in the progressive disease health state. Disease progression was determined by investigator assessment according to Response Evaluation Criteria in Solid Tumors Version 1.1 criteria.1
Model Inputs
The modelled population reflected the baseline characteristics of European participants of the KEYNOTE-590 trial, a multi-centre, randomized, double-blind, placebo-controlled, phase III study of pembrolizumab plus chemotherapy (5-FU and cisplatin) versus placebo plus chemotherapy in patients with previously untreated advanced or metastatic EC. The submitted model assumed a mean age of 61.4 years, mean body surface area of 1.84 m2 (standard deviation = 0.20), mean weight of 71.22 kg (standard deviation = 13.49).1
PFS, OS, and ToT curves for pembrolizumab in combination with 5-FU and cisplatin and 5-FU and cisplatin were generated using patient-level data from the KEYNOTE-590 trial (the data cut-off date was July 2, 2020).1 The sponsor used piecewise models to predict PFS and OS after the end of the trial follow-up. Kaplan–Meier data from the KEYNOTE-590 trial was used to inform PFS for the first 10 months of the model duration; thereafter, PFS was extrapolated using a log-logistic parametric survival model. Similarly, OS was informed directly from the Kaplan–Meier data up to 40 months; thereafter, a log-logistic model was fitted to patient-level data to inform long-term extrapolation. This distribution was selected based on clinical validity and statistical fit. The sponsor assumed that PFS and OS for other chemotherapies incorporated in the blended chemotherapy regimens was equal to those receiving 5-FU and cisplatin. The model accounted for grade 3 or higher all-cause and treatment-related AEs that were reported in at least 5% of in any treatment arm of the KEYNOTE-590 trial. The occurrence of AEs for blended chemotherapy were assumed to be the same as the 5-FU and cisplatin arm.1
Health utility values were based on a linear mixed-effects models fitted with EuroQol 5-Dimensions 5-Levels questionnaire data collected in the KEYNOTE-590 trial, which were adapted to the Canadian population using Canadian tariffs. The linear mixed-effects models also included the presence or absence of any grade 3 or higher AEs to estimate AE disutility. The sponsor estimated health state utilities based on time to death, which reflects the decline in the quality of life for patients with advanced or metastatic cancer as they approach death (i.e., 0 to 29, 30 to 89, 90 to 179, 180 to 359, or ≥ 360 days until death).1
Costs included drug (acquisition, administration), health state, disease management, AEs, and terminal care. The HER2 testing costs were not included in the model because the tests have already been used in clinical practice for EGJ adenocarcinoma. Drug acquisition cost for pembrolizumab in combination with 5-FU and cisplatin and comparators was calculated as a function of the unit drug cost, dosing schedule, RDI reported in the KEYNOTE-590 trial, and proportion of patients on treatments. Unit drug costs were sourced from recent CADTH pan-Canadian Oncology Drug Review economic guidance. For the blended chemotherapy, the drug acquisition and administration costs were estimated as the weighted average by individual chemotherapy treatment. ToT survival curves for modelled first-line treatments were used to estimate the proportion of patients on each drug treatment over time. ToT Kaplan–Meier data for the pembrolizumab in combination with 5-FU and cisplatin and 5-FU in combination with cisplatin arms in the KEYNOTE-590 trial are mature; data extrapolation using survival models were therefore not required. The sponsor model applied maximum treatment duration of 35 cycles (105 weeks) to pembrolizumab and 5-FU and 6 cycles (18 weeks) to cisplatin as indicated in the KEYNOTE-590 trial protocol. Treatment duration for blended chemotherapy was assumed to be the same as either the 5-FU ToT or cisplatin ToT in the 5-FU in combination with cisplatin arm. Drug administration costs included costs associated with vial administration for IV therapies.1
The model also considered the costs of subsequent therapies among patients who discontinued first-line treatment. The proportion of patients receiving different subsequent treatments after discontinuation for the pembrolizumab in combination with 5-FU and cisplatin and 5-FU in combination with cisplatin arms was based Canadian local estimates. Patients received subsequent therapies for different treatment durations based on data from the KEYNOTE-590 study. The model also considered disease management costs, including CT scans, full blood count, renal function tests, hepatic function tests, and medical consultations. Unit costs for resource use elements were obtained from local estimates. Costs for each AE were obtained from the published literature and the Ontario Case Costing Initiative database. Terminal care costs were applied to patients who transitioned to the “death” health state; the cost estimate was obtained from an economic evaluation study by Verma and Rocchi which reported the end-of-life costs due to metastatic breast cancer in the last 3 months before death.1
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically with 5,000 iterations with the deterministic and probabilistic results being similar. The probabilistic findings are presented below. The submitted analyses were based on the publicly available prices of the comparator treatments.
Base-Case Results
Pembrolizumab in combination with 5-FU and cisplatin was associated with an ICER of $142,861 per QALY compared to 5-FU and cisplatin over a 20-year time horizon (Table 3). The blended chemotherapy comparator was dominated by 5-FU and cisplatin as it was more costly and generated the same QALYs. At a willingness-to-pay value of $50,000 per QALY, the probability of pembrolizumab in combination with 5-FU and cisplatin being cost-effective was 0% compared to 5-FU and cisplatin.1
The main cost driver was drug acquisition cost, followed by subsequent treatment cost and drug administration cost. Pembrolizumab in combination with 5-FU and cisplatin was associated with 0.67 additional life-years relative to 5-FU in combination with cisplatin. At the end of the model time horizon (i.e., 20 years), the model estimated that approximately 2.9%, 0.8%, and 0.8% of the patients are alive in the pembrolizumab in combination with 5-FU and cisplatin, 5-FU in combination with cisplatin, and blended chemotherapy groups, respectively.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
5-FU and cisplatin | 71,289 | 1.21 | Reference |
Pembrolizumab in combination with 5-FU and cisplatin | 180,106 | 1.97 | 142,861 |
5-FU = 5-fluorouracil; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Only treatments that are on the efficiency frontier are reported in the main body. Blended chemotherapy was dominated by the 5-FU and cisplatin regimen.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor performed scenario analyses by considering alternative parametric survival models, using alternative cut-off for piecewise modelling, varying the time at which the treatment effect started to wane, deriving utility scores from the UK algorithm, removing disutility due to AEs, assuming a 100% RDI, and using alterative time horizon or discount rates. Cost-effectiveness results were robust to changes in most parameters and assumptions. The blended chemotherapy comparators were dominated by 5-FU and cisplatin in most scenarios except when alternative sources of AE rates were considered. The scenarios with the greatest impact on the ICER were alternative parametric models for modelling OS. Compared to 5-FU and cisplatin, the estimated ICERs of pembrolizumab in combination with 5-FU and cisplatin ranged between $83,620 per QALY (using a piecewise Gompertz distribution to predict long-term OS) and $252,076 per QALY (using a 1-piece log-logistic to predict long-term OS).1
A subgroup analysis of patients with PD-L1 with a CPS of 10 or greater provided findings consistent with the sponsor’s base case. Compared to 5-FU and cisplatin, the blended chemotherapy comparator was dominated, and the ICER of pembrolizumab in combination with 5-FU and cisplatin was reduced to $106,185 per QALY.1
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Uncertainty in the long term survival benefits of pembrolizumab in combination with 5-FU and cisplatin: The clinical experts agreed that the interim OS results represent a clinically meaningful benefit for patients. The reported PFS and OS results are deemed final based on an interim analysis according to pre-specified stopping criteria. However, whether the actual final efficacy results would conform with the interim results is unknown. There are case reports of stopping a trial early to claim statistical significance according to pre-specified stopping rule and the type I error with the interim results could not be repeated at the final analysis after the trial was completed.3-5 Such potential impacts, including the depletion of susceptible subjects, on OS could be more likely to occur toward the end of the trial. Therefore, the magnitude of OS benefit at final analysis may not be as large as what had been obtained at interim analysis. Although the sponsor used the best fitted survival model (log-logistic) to predict long-term PFS and OS data, CADTH noted that this parametric survival model did not fit PFS data well based on visual inspection when extrapolated over the lifetime horizon.
CADTH also noted additional uncertainty associated with the estimated survival benefits of pembrolizumab in combination with 5-FU and cisplatin due to the sponsor’s use of a partitioned survival model. While this modelling approach is appropriate for the decision question and could provide comparable estimates to the state transition approach, it introduces structural assumptions about the relationship between PFS and OS (i.e., non-mutually exclusive curves) with immature data.6 This uncertainty could not be adjusted for in CADTH’s reanalysis due to the submitted model structure. These assumptions are likely to introduce a post-progression survival bias that favours pembrolizumab in combination with 5-FU and cisplatin. CADTH was not able to estimate the full extent to which the post-PFS survival benefit estimated in the model was due to the efficacy of pembrolizumab in combination with 5-FU and cisplatin versus being due to the structural bias within the model, but attempted to address this concern within the confines of the submitted model structure.
CADTH was unable to fully assess the concerns identified within this limitation. CADTH applied a treatment-waning effect, as defined within the sponsor’s model, as part of the CADTH base case, and assessed the impact of alternative parametric survival models to extrapolate PFS and OS data beyond the trial follow-up period within scenario analyses. The cost-effectiveness of pembrolizumab in combination with chemotherapy was sensitive to alternate survival data and treatment effect assumptions.
Relevant backbone chemotherapies were not considered for combination use with pembrolizumab: Clinical experts consulted by CADTH indicated that pembrolizumab may also be prescribed with FOLFOX or CAPOX; however, the sponsor’s model considered pembrolizumab in combination with cisplatin and 5-FU. It remains unclear how the type of backbone therapy may affect the cost-effectiveness of pembrolizumab.
CADTH addressed this limitation by replacing 5-FU and cisplatin with CAPOX and mFOLFOX in scenario analyses.
Inappropriate source of end-of-life care cost: The sponsor obtained the end-of-life care cost from a study conducted by Verma and Rocchi,7 which reported the 3-month end-of-life cost incurred among postmenopausal patients with hormone-sensitive metastatic breast cancer who had failed tamoxifen and subtracted 3-month progressive disease management costs from the cost. CADTH was concerned about the sponsor’s approach as a terminal cost varies according to the type of cancer. Moreover, if the net or attributable cost of end-of-life care was not used, it is unnecessary to remove disease management costs incurred at the end-of-life to avoid double counting. The sponsor’s approach was likely to overestimate the cost of end-of-life but underestimate the ICER because more patients with no 5-FU in combination with cisplatin transitioned to death compared to those treated with pembrolizumab in combination with 5-FU and cisplatin.
CADTH addressed this limitation by using an alternative Canadian end-of-life cost8 that captures all publicly funded health services provided to patients with esophageal adenocarcinoma who were in the terminal phase in its reanalysis.
Proportion of patients receiving subsequent treatments not reflective of current practice in Canada: The sponsor’s economic model used Canadian local estimates to inform the proportion of patients receiving different subsequent treatments after discontinuation for the pembrolizumab in combination with 5-FU and cisplatin and 5-FU in combination with cisplatin groups. This might overestimate the ICER as the sponsor assumed that all patients who progressed and did not transition to death would receive subsequent treatments. Based on feedback from the clinical experts, approximately 10% of patients in each treatment arm would receive subsequent therapies.
As part of CADTH’s base case, CADTH assumed 10% of patients with disease progression would receive subsequent treatments. CADTH also explored the use of the sponsor submitted subsequent treatment distributions from the KEYNOTE-590 trial as part of scenario analyses.
An additional limitation was identified but was not considered to be key limitations:
Use of blended comparator is inappropriate: Although clinical experts consulted by CADTH agreed that these chemotherapy regimens reflect the treatment availability and use in Canada, each treatment should be considered individually, and assessed in a sequential analysis. While the submitted model had the functionality to compare the costs of pembrolizumab in combination with 5-FU and cisplatin and the individual regimens, these analyses lacked regimen-specific comparative efficacy and safety parameters for the individual treatment regimens. As such, the interpretation of the economic value of pembrolizumab in combination with 5-FU and cisplatin was restricted to a comparison with the blended comparator and the cost-effectiveness of pembrolizumab in combination with 5-FU and cisplatin relative to the individual regimens is unknown.
CADTH was unable to address the uncertainty in the cost-effectiveness of pembrolizumab in combination with 5-FU and cisplatin compared to each individual chemotherapy regimen due the lack of comparative efficacy and safety data for these regimens. As a result, CADTH removed the blended comparator arm and compared pembrolizumab in combination with 5-FU and cisplatin to 5-FU in combination with cisplatin.
Health utility values not adjusted for the baseline utility: While a time-to-death approach was acceptable for the estimation of health utility in this submission based on recent evidence suggesting that progression may not be a good proxy for health-related quality of life for patients receiving immune-oncology agents,9,10 CADTH was concerned that the sponsor did not adjust for baseline utility in either the time-to-death or progression-based approach. Although economic data from randomized controlled trials usually rest on the assumption that baseline characteristics between the groups are well-balanced, there may be imbalance in mean baseline utility between trial arms. This imbalance may cause misleading ICERs as the ICERs can be very sensitive to small changes in QALYs as a result of imbalance in mean baseline utility.11
CADTH was unable to assess the impact of the limitation related to the omission of baseline utility adjustment; however, it was likely to have a minimal impact on ICERs because the sponsor’s model assumed the same health utility values across treatment groups. CADTH assessed the impact the approach to incorporate health utilities as a scenario analysis.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (See Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patient characteristics (i.e., age, gender, weight, body surface area) are based on European patients who participated in the KEYNOTE-590 trial. | The clinical experts consulted by CADTH found this assumption acceptable. |
OS, PFS, and AE inputs for the blended chemotherapy comparator were assumed equal to the 5-FU in combination with cisplatin arm of the KEYNOTE-590 trial. | Acceptable. Given the lack of comparative efficacy of the non-trial comparators and pembrolizumab in combination with 5-FU and cisplatin, it was reasonable to assume equal efficacy of included non-trial comparators. |
The sponsor used a time-to-death approach to estimate health utility values and reflect the decline in the quality of life for patients with advanced or metastatic cancer as they approach death. The sponsor also assumed the choice of the treatments did not affect health utility values. | Acceptable. CADTH acknowledged that progression status may not always be a good proxy for health-related quality of life, especially for patients receiving immune-oncology agents where there can be issues with pseudo-progression10 when the action of the treatment is mistaken for disease progression. In addition, a large proportion of missing utility data are expected when the patient deteriorates, and the disease progresses toward death because most trials collect utility data for up to 1 year or end of treatment, at time of discontinuation, and at the fixed interval after the treatment discontinuation follow-up visit. |
Time on treatment of individual drugs in the blended chemotherapy was to be the same as either the 5-FU duration or cisplatin duration in the 5-FU in combination with cisplatin arm. | Acceptable. |
5-FU = 5-fluorouracil; AE = adverse event; OS = overall survival; PFS = progression-free survival.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH could not adequately address the uncertainty resulting from the immature PFS and OS data. The CADTH base case was derived by correcting drug administration fees for FOLFOX and CAPOX considered in the blended chemotherapy and leucovorin dose, using publicly listed prices for 5-FU, oxaliplatin, and leucovorin, using the Canadian end-of-life cost specific to esophageal adenocarcinoma, and reducing the proportion of patients requiring subsequent treatments to 10%, as suggested by the clinical experts consulted by CADTH. In addition, CADTH applied a treatment-waning assumption to account for the potential uncertainty resulting from the use of interim analysis and removed the blended chemotherapy comparator due to the lack of evidence on comparative efficacy and safety of each individual regimen to pembrolizumab in combination with 5-FU and cisplatin. Table 5 details the change made to derive the CADTH base case, and the summary results of the CADTH base case are presented in Table 6. Additional results are shown in Appendix 4 (Table 13 and Table 14).
Results from CADTH's base case suggested that pembrolizumab with 5-FU and cisplatin was associated with higher costs ($100,545) and increased QALYs (0.59 QALYs), with an ICER of $170,819 per QALY compared to 5-FU in combination with cisplatin. The estimated ICER was higher than that reported in the sponsor's base case due to the assumption that treatment effect of pembrolizumab and backbone chemotherapy wanes over time. The probability that pembrolizumab in combination with 5-FU and cisplatin is cost-effective was 0 at the willingness-to-pay threshold of $50,000 per QALY. Approximately 92% of the incremental QALYs and 22% of incremental costs came from the extrapolation beyond the trial follow-up period.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
ToT data used in drug administration cost calculation for FOLFOX and CAPOX as part of the blended chemotherapy | ToT data for FOLFOX were used for CAPOX and ToT data for CAPOX were used for FOLFOX | CADTH corrected the ToT data for FOLFOX and CAPOX |
Listed price (cost per mg) for 5-FU, oxaliplatin, and leucovorin | 5-FU: $0.003 per mg Oxaliplatin: $10.20 per mg Leucovorin: $0.05 per mg | 5-FU: $0.03 per mg Oxaliplatin: $0.73 per mg Leucovorin: $0.15 per mg |
Leucovorin dose | 200 mg/m2 | 400 mg/m2 as per Ontario Health12 |
Changes to derive the CADTH base case | ||
1. Use an inappropriate terminal care cost | Use a 3-month terminal care cost for metastasis breast cancer ($26,020) | Use a 6-month terminal care cost for esophageal adenocarcinoma ($9,362) |
2. Percentage of patients who progressed and received subsequent treatments not reflective of Canadian practice | All living patients who progressed were assumed to receive subsequent treatments | Assume 10% of living patients who progressed to receive subsequent treatments |
3. Treatment-waning assumption | Treatment effect of pembrolizumab in combination with 5-FU and cisplatin was assumed to sustain beyond the trial | Assume a treatment-waning effect with starting and ending times at 2 and 5 years as considered in the sponsor’s scenario analysis |
4. Inclusion of the blended chemotherapy comparator | Consider the blended chemotherapy as one of the comparators | Remove the blended chemotherapy comparator |
CADTH base case | 1 + 2 + 3 + 4 | |
5-FU = 5-fluorouracil; CAPOX = capecitabine and oxaliplatin; FOLFOX = 5-FU and oxaliplatin and leucovorin; ToT = time on treatment.
aAs the lowest cost chemotherapy regimen is 5-FU and cisplatin, and chemotherapy regimens were considered equivalent, blended chemotherapy is always dominated by 5-FU and cisplatin and was therefore not included in CADTH reanalyses.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER vs. Reference | Sequential ICER |
|---|---|---|---|---|
Sponsor-corrected base case | ||||
5-FU and cisplatin | 72,653 | 1.21 | Ref. | Ref. |
Pembrolizumab and 5-FU and cisplatin | 181,579 | 1.98 | 142,422 | 142,422 |
CADTH base case | ||||
5-FU and cisplatin | 28,826 | 1.21 | Ref. | Ref. |
Pembrolizumab and 5-FU and cisplatin | 129,370 | 1.80 | 170,819 | 170,819 |
5-FU = 5-fluorouracil; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Scenario Analysis Results
Based on CADTH's base case, a series of scenario analyses were conducted. These analyses explored the impact of the following model parameters and assumptions: parameter survival models to assess the uncertainty of PFS and OS data reported in the interim analysis of the KEYNOTE-590 trial; choice of backbone chemotherapies; approach to estimate health utility values; end-of-life care costs; treatment duration; drug wastage; RDI; proportion of patients receiving subsequent treatments; patient subgroup (PD-L1 CPS ≥ 10); and a perspective of analysis.
Results from scenario analyses (Appendix 4, Table 15) demonstrated that the cost-effectiveness findings were largely sensitive to parametric models used to extrapolate OS data. The ICERs increased from $176,963 per QALY (Scenario 4: Alternative survival models for OS; piecewise log-logistic with cut-off at 32 weeks) to $306,332 per QALY (Scenario 6: Alternative survival models for OS; piecewise Weibull with cut-off at 40 weeks). The ICERs were also influenced by how treatment duration was estimated, and the approach used to estimate health utility values. If PFS curves were used to reflect treatment duration for all treatments (Scenario 10), the ICER increased to $192,960 per QALY. Using a traditional progression-based approach to estimate health utility increased the ICER to $188,121 per QALY. Cost-effectiveness findings were found to be robust to the changes in survival models used to predict long-term PFS data, vial-sharing assumption, and the percentage of patients whose disease progressed and required subsequent treatments.
CADTH undertook a price reduction analysis based on the sponsor's base case and the CADTH base case (Table 7). The results show that a price reduction of 75% is required for pembrolizumab in combination with 5-FU and cisplatin to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for pembrolizumab plus 5-FU and cisplatin vs. 5-FU and cisplatin | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $142,861 | $170,819 |
10% | $129,524 | $154,203 |
20% | $116,612 | $138,464 |
30% | $105,047 | $122,765 |
40% | $92,481 | $105,557 |
50% | $80,033 | $89,444 |
60% | $67,019 | $73,425 |
70% | $54,637 | $57,163 |
75% | $48,546 | $49,085 |
5-FU = 5-fluorouracil; ICER = incremental cost-effectiveness ratio; vs. = versus.
Issues for Consideration
According to an interim analysis of the KEYNOTE-590 trial, pembrolizumab in combination with 5-FU and cisplatin might provide greater clinical benefits and be more cost-effective for patients with PD-L1 with a CPS of 10 or greater. However, as the PD-L1 testing is not routinely performed in current practice in Canada, clinical experts consulted by CADTH advised that funding for pembrolizumab should not be restricted to this subgroup.
The wholesale price of pembrolizumab is $1,100 per mL. It is also available in powder form for IV solution and comes in a 2 mL vial, priced at $2,200. However, the sponsor submitted a reimbursement request only for a 100 mg solution in 4 mL vials.13
As noted in the clinician input received for this review, there is potential use of pembrolizumab in patients who are currently on platinum- and fluoropyrimidine-based chemotherapy, or alternate chemotherapy. There is no time frame specified for patients currently on chemotherapy or those who have not progressed. If pembrolizumab was used in this expanded population, the budget impact would be higher than estimated. However, this expanded population is not part of Health Canada indication, and the size of this population is unknown.
Pembrolizumab is funded using weight-based dosing in multiple jurisdictions.14,15 CADTH was not able to assess alternate dosing approaches as part of this review.
Overall Conclusions
Evidence from the KEYNOTE-590 trial indicated that compared to placebo in combination with cisplatin and 5-FU, first-line treatment with pembrolizumab in combination with cisplatin and 5-FU showed a clinically meaningful and statistically significant overall and PFS benefit in adult patients with locally advanced unresectable or metastatic cancer of the esophagus or HER2-negative EGJ (tumour centre 1 cm to 5 cm above the gastric cardia), based on the data currently analyzed. As the study is ongoing, additional long-term efficacy and safety information are anticipated. Survival models used to extrapolate OS data drove the modelled cost-effectiveness of pembrolizumab in combination with chemotherapy compared to chemotherapy.
CADTH identified several limitations within the sponsor’s economic analysis, specifically the uncertainty associated with the use of interim PFS and OS data from the KEYNOTE-590 trial and application of these data within a partitioned survival model, the assumptions regarding comparators and background chemotherapy, an inappropriate source for end-of-life cost, and overestimated proportion of patients who are likely to receive subsequent treatments post-progression.
CADTH was unable to address all the limitations identified, but made several corrections and revisions to sponsor’s base case to derive the CADTH base case. CADTH corrected drug administration fees for FOLFOX and CAPOX (considered in blended chemotherapy), the leucovorin dose, and using publicly listed prices for 5-FU, oxaliplatin, and leucovorin, while also incorporating a Canadian end-of-life cost specific to esophageal adenocarcinoma, reducing the proportion of patients requiring subsequent treatments to 10% as suggested by the clinical experts consulted by CADTH, and applying a treatment-waning assumption to account for the uncertainty resulting from the use of interim analysis. CADTH undertook further scenario analyses to explore the impact of alternate parameter survival models for PFS and OS data, assumptions regarding the costs of backbone and blended chemotherapy regimens, an alternate approach to estimate health utility values, alternate dose intensity and drug use assumptions, and perspective of the analysis.
Although CADTH’s base case resulted in a higher ICER than the sponsor’s base case ($170,819 per QALY versus $142,861 per QALY), both analyses provided consistent results, suggesting that pembrolizumab in combination with a chemotherapy backbone was associated with higher costs and improved QALYs but was not cost-effective at a $50,000 per QALY willingness-to-pay threshold compared to 5-FU in combination with cisplatin at the submitted price. A price reduction of at least 75% would be required to make pembrolizumab an optimal treatment option at a willingness-to-pay threshold of $50,000 per QALY.
The cost-effectiveness of pembrolizumab in combination with a chemotherapy backbone was highly sensitive to the statistical approaches used to fit the OS data, with the ICERs ranging from $176,963 per QALY (Scenario 4: Alternative survival models for OS; piecewise log-logistic with cut-off at 32 weeks) to $306,332 per QALY (Scenario 6: Alternative survival models for OS; piecewise Weibull with cut-off at 40 weeks). Cost-effectiveness findings were found to be robust to the changes in survival models used to predict long-term PFS data, vial-sharing assumption, and the percentage of patients whose disease progressed and required subsequent treatments. A scenario based on PD-L1 status should be interpreted with caution given the lack of publicly funded testing and the clinical experts’ feedback that this marker should not be a determinant as to whether pembrolizumab could be used to treat a patient with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2-negative adenocarcinoma of the esophagogastric junction.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2021 May 26.
2.Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2021.
3.Wilcox R, Djulbegovic B, Guyatt G, Montori V. Randomized trials in oncology stopped early for benefit. J Clin Oncol. 2008;26(1):18-19. PubMed
4.Bassler D, Briel M, Montori V, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-1187. PubMed
5.Guyatt G, Briel M, Glasziou P, Bassler D, Montori V. The dangers of stopping trials early. BMJ. 2012;344:e3863. PubMed
6.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU Technical Support Document 19). Sheffield (GB): Decision Support Unit, ScHARR, University of Sheffield; 2017: http://nicedsu.org.uk/wp-content/uploads/2017/06/Partitioned-Survival-Analysis-final-report.pdf. Accessed 2021 Aug 22.
7.Verma S, Rocci A. Economic evaluation of antiaromatase agents in the second-line treatment of metastatic breast cancer. Support Care Cancer. 2003;11(11):728-734. PubMed
8.Thein HH, Jembere N, Thavorn K, et al. Estimates and predictors of health care costs of esophageal adenocarcinoma: a population-based cohort study. BMC Cancer. 2018;18(1):694. PubMed
9.Hernandez-Villafuerte K, Fischer A, Latimer N. Challenges and methodologies in using progression free survival as a surrogate for overall survival in oncology. Int J Technol Assess Health Care. 2018;34(3):300-316. PubMed
10.Huang B. Some statistical considerations in the clinical development of cancer immunotherapies. Pharm Stat. 2018;17(1):49-60. PubMed
11.Manca A, Hawkins N, Sculpher M. Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ. 2005;14(5):487-496. PubMed
12.Cancer Care Ontario. Drug formulary: funded evidence-informed regimens. 2021; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2021 Aug 11.
13.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Aug 11.
14.BC Cancer Drug Manual: pembrolizumab [product monograph]. Vancouver (BC): BC Cancer Provincial Health Service Authority; 2021: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Pembrolizumab_monograph.pdf. Accessed 2021 Mar 1.
15.Cancer Care Ontario. Drug Formulary: pembrolizumab. 2021; https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/44411. Accessed 2021 Aug 23.
16.Government of British Columbia. BC PharmaCare formulary search. 2021; https://pharmacareformularysearch.gov.bc.ca. Accessed 2021 Aug 11.
17.Formulary: September 2021. Halifax (NS): Nova Scotia Department of Health; 2021: https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf. Accessed 2021 Aug 18.
18.Epirubicin hydrochloride injection: 2 mg/mL [product monograph]. Kirkland (QC): Pfizer Canada Inc.; 2018: https://www.pfizer.ca/sites/default/files/201802/2018.01.23_Epirubicin_PM_E_Level_3.pdf. Accessed 2021 Aug 19.
19.Epirubicin for injection: 2 mg/mL (2 mg Epirubicin Hydrochloride/ mL) [product monograph]. Toronto (ON): Teva Canada Limited; 2014: https://pdf.hres.ca/dpd_pm/00026770.PDF. Accessed 2021 Aug 19.
20.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab): powder for solution for infusion 50 mg, solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2021 May 26.
21.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
22.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2019. Toronto (ON): Canadian Cancer Society; 2019: www.cancer.ca/Canadian-Cancer-Statistics-2019-EN. Accessed 2021 Aug 10.
23.Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian cancer statistics 2017. Toronto (ON): Canadian Cancer Society; 2017: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2017-statistics/2017_canadian-cancer-statistics_en.pdf. Accessed 2021 Aug 23.
24.pan-Canadian Oncology Drug Review Final Economic Guidance Report: Atezolizumab (Tecentriq) for small cell lung cancer. Ottawa (ON): CADTH; 2020 Jan 30: https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10156AtezolizumabSCLC_fnEGR_NOREDACT-ABBREV_Post_30Jan2020_final.pdf. Accessed 2021 Aug 10.
25.pan-Canadian Oncology Drug Review Final Economic Guidance Report: Panitumumab (Vectibix) for left sided metastatic colorectal cancer Ottawa (ON): CADTH; 2018 Mar 29: https://cadth.ca/sites/default/files/pcodr/pcodr_panitumumab_vectibix_ls_mcrc_fn_egr%20.pdf. Accessed 2021 Aug 10.
26.pan-Canadian Oncology Drug Review Initial Economic Guidance Report: Pertuzumab-trastuzumab for early breast cancer. Ottawa (ON): CADTH; 2018 Oct 4: https://www.cadth.ca/sites/default/files/pcodr/pcodr_pertuzumab-trastuzumab_perjeta-herceptin-combo_ebc_in_egr.pdf. Accessed 2021 Aug 10.
27.pan-Canadian Oncology Drug Review Final Economic Guidance Report: Pembrolizumab (Keytruda) for squamous non-small cell lung cancer. Ottawa (ON): CADTH; 2020 Jan 3: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10176PembrolizumabSQ-NSCLC_fnEGR_NOREDACT-ABBREV_Post_03Jan2020_final.pdf. Accessed 2021 Aug 10.
28.pan-Canadian Oncology Drug Review Final Economic Guidance Report: Ramucirumab (Cyramza) for gastric cancer. Ottawa (ON): CADTH; 2015 Oct 29: https://www.cadth.ca/sites/default/files/pcodr/pcodr_ramucirumab_cyramza_gc_fn_egr.pdf. Accessed 2021 Aug 10.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Regimens Used in the First-Line Treatment of Locally Advanced Unresectable or Metastatic Esophageal Carcinoma or HER2 Negative Adenocarcinoma of the Esophagogastric Junction
Treatment | Strength/ concentration | Form | Price per vial / mg ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 100 mg/4mL | 4 mL Vial IV infusion | 4,400.0000a | 200 mg Q3W or 400 mg Q6W | 419.05 | 11,733 |
Pembrolizumab plus CISPFU Q3W | 12,582 | |||||
Pembrolizumab plus CISPFU Q5.42W | 12,370 | |||||
Pembrolizumab plus CAPECISP | 12,478 | |||||
Pembrolizumab plus CAPOX | 12,180 | |||||
Pembrolizumab plus mFOLFOX | 12,708 | |||||
Cisplatin-5-fluorouracil (CISPFU) | ||||||
Cisplatin | 1 mg/mL | 50 mg 100 mg Vial for IV infusion | 135.0000 270.0000 | 80 mg/m2 Q3W Or Q5.42W | 19.29 14.46 | 540 405 |
Fluorouracil (5-FU) | 50 mg / mL | 100 mL Vial for IV infusion | 160.9000 | 800 mg/m2/day on Days 1 to 5 or 1,000 mg/m2 on days 1 to 4 Q3W Or Q5.42W | 11.03 8.27 | 309 232 |
CISPFU Q3W Or Q5.42W | 30.32 22.74 | 849 637 | ||||
Cisplatin-capecitabine (CAPECISP) | ||||||
Cisplatin | 1 mg/mL | 50 mL 100 mL Vial for IV infusion | 135.0000 270.0000 | 60 or 80 mg/m2 Q3W | 19.29 | 540 |
Capecitabine (Xeloda) | 150 mg 500 mg | Tablet | 0.4575 1.5250 | 1,000 mg/m2 twice daily on Days 1 to 14 Q3W | 7.32 | 205 |
CAPECISP | 26.61 | 745 | ||||
Oxaliplatin-capecitabine (CAPOX) | ||||||
Oxaliplatin | 5 mg/mL | 10 mL 20 mL 40 mL Vial for IV infusion | 36.2700 72.5400 145.0800 | 130 mg/m2 Q3W | 8.64 | 242 |
Capecitabine (Xeloda) | 150 mg 500 mg | Tablet | 0.4575 1.525 | 1,000 mg/m2 twice daily on Days 1 to 14 Q3W | 7.32 | 205 |
CAPOX | 15.96 | 447 | ||||
Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin (mFOLFOX) | ||||||
Oxaliplatin | 5 mg/mL | 10 mL 20 mL 40 mL Vial for IV infusion | 36.2700 72.5400 145.0800 | 85 mg/m2 Q2W | 10.36 | 290 |
Leucovorin | 10 mg/mL | 5 mL 50 mL Vial for IV infusion | 68.9400 74.4100b | 400 mg/m2 Q2W | 10.63 | 298 |
Fluorouracil (5-FU) | 50 mg/mL | 10 mL 100 mL Vial for IV infusion | 16.0900 160.9000 | 400 mg/m2 IV bolus Q2W | 2.30 | 64 |
Fluorouracil (5-FU) | 50 mg/mL | 10 mL 100 mL Vial for IV infusion | 16.0900 160.9000 | 2,400 mg/m2 IV continuous infusion Q2W | 11.49 | 322 |
mFOLFOX | 34.78 | 974 | ||||
Q2W = every 2 weeks; Q3W = every 3 weeks, 5-FU = 5 – Fluorouracil.
Note: All prices are IQVIA Delta PA wholesale list prices13 (accessed July 2021), unless otherwise indicated, and do not include dispensing fees or markups. Wastage of excess medication in vials is included in costs. Recommended dosage is based on Cancer Care Ontario monographs,12 unless otherwise indicated. For dosing that depends on weight or body surface area, CADTH assumed mean body weight of 71 kg and mean body surface area was 1.8 m2. Total cost estimates per regimen are based on the cheapest combination of the component drugs.
aSponsor’s submitted price for each dosage.
bBritish Columbia Formulary list price,16 as reported by IQVIA Delta PA (August 2021).
bNova Scotia Formulary,17 as reported by IQVIA Delta PA (August 2021).
Table 9: CADTH Cost Comparison Table for First-Line Treatment of Esophageal Carcinoma for Patients Not Candidates for Platinum Therapy
Treatment | Strength/ concentration | Form | Price per vial ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Folinic Acid (Leucovorin)-Fluorouracil-Irinotecan (FOLFIRI) | ||||||
Irinotecan | 20 mg/mL | 2 mL 5 mL 25 mL Vial for IV infusion | 208.3400 8.1000 2,604.375 | 180 mg/m2 Q2W | 2.31 | 65 |
Leucovorin | 10 mg/mL | 5 mL 50 mL Vial for IV infusion | 68.9400 74.4100 | 400 mg/m2 Q2W | 10.63 | 298 |
Fluorouracil (5-FU) | 50 mg/mL | 100 mL Vial for IV infusion | 160.9000 | 400 mg/m2 IV bolus Q2W | 2.30 | 64 |
Fluorouracil (5-FU) | 50 mg/mL | 100 mL Vial for IV infusion | 160.9000 | 2,400 mg/m2 IV continuous infusion Q2W | 11.49 | 322 |
FOLFIRI | 26.73 | 749 | ||||
Pembrolizumab plus FOLFIRI | 12,482 | |||||
Q2W = every 2 weeks.
Note: All prices are IQVIA Delta PA wholesale list prices13 (accessed July 2021), unless otherwise indicated, and do not include dispensing fees or markups but do assume wastage of excess medication in vials. Doses are from the Cancer Care Ontario Drug Formulary regimen database.12 Mean body weight was assumed to be 71.22 kg, while mean body surface area was 1.84 m2. Total cost estimates per regimen are based on the cheapest combination of the component drugs.
Table 10: CADTH Cost Comparison Table for Other First-Line Treatment of Esophageal Carcinoma
Treatment | Strength/ concentration | Form | Price per vial ($) | Recommended dosage | Average daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Epirubicin-Cisplatin-Capecitabine (ECX) | ||||||
Epirubicin | 2 mg/mL | 25 mL 100 mL Vial for IV infusiona | 200.9100 779.5400 | 50 mg /m2 Q3W | 19.13 | 536 |
Cisplatin | 1 mg/mL | 50 mL 100 mL Vial for IV infusion | 135.0000 270.0000 | 60 mg /m2 Q3W | 19.29 | 540 |
Capecitabine | 150 mg 500 mg | Tablet | 0.4575 1.5250 | 625 mg /m2 twice daily | 7.02 | 196 |
ECX | 45.44 | 1,272 | ||||
Pembrolizumab plus ECX | 13,006 | |||||
Epirubicin-Oxaliplatin-Capecitabine (EOX) | ||||||
Epirubicin | 2 mg/mL | 25 mL 100 mL Vial for IV infusiona | 200.9100 779.5400 | 50 mg /m2 Q3W | 19.13 | 536 |
Oxaliplatin | 5 mg/mL | 10 mL 20 mL 40 mL Vial for IV infusion | 36.2700 72.5400 145.0800 | 130 mg /m2 Q3W | 8.64 | 242 |
Capecitabine | 150 mg 500 mg | Tablet | 0.4575 1.525 | 625 mg /m2 twice daily | 7.02 | 196 |
EOX | 34.79 | 974 | ||||
Pembrolizumab plus EOX | 12,707 | |||||
QW3 = every 3 weeks; Q2W = every 2 weeks; 5-FU = 5-fluorouracil.
Note: All prices are IQVIA Delta PA wholesale list prices13 (accessed July 2021), unless otherwise indicated, and do not include dispensing fees or markups but do assume wastage of excess medication in vials. Doses are from the Cancer Care Ontario Drug Formulary regimen database.12 Mean body weight was assumed to be 71.22 kg, while mean body surface area was 1.84 m2. Total cost estimates per regimen are based on the cheapest combination of the component drugs. Cost estimate is based on the cheapest combination of the available forms.
aOther sizes are available as per product monographs18,19 but price was not available for 5 mL, 10 mL, 50 mL and 75 mL vials.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | See CADTH appraisal section. |
Model has been adequately programmed and has sufficient face validity | No | The submitted economic model has a minor programming error — incorrect link to time-to-treatment columns for drug administration cost calculation for the blended chemotherapy. The submitted economic model did not explicitly account for the proportion of patients who progressed and required subsequent treatments. It was assumed that all patients whose disease progressed in each cycle would receive subsequent therapies. This assumption was inconsistent with that was used in the budget impact analysis, whereby approximately 47% of patients were assumed to receive second-line treatments. |
Model structure is adequate for decision problem | Yes | Acceptable. A partitioned survival model is commonly used in oncology submissions; however, the model structure may produce a post-progression survival bias in favour of pembrolizumab in combination with 5-FU and cisplatin. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | See CADTH appraisal section. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | Acceptable. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | Acceptable. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
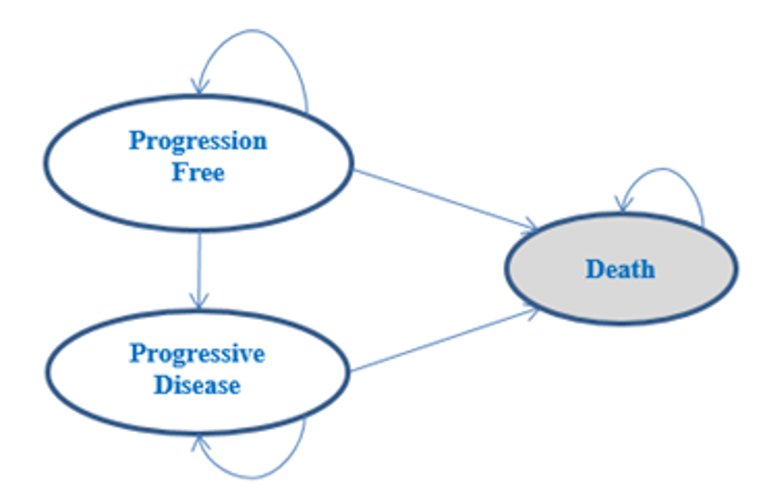
Detailed Results of the Sponsor’s Base Case
Table 12: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
5-FU + cisplatin | 71,289 | 1.21 | Reference |
Blended chemotherapy | 74,721 | 1.21 | Dominated by 5-FU + cisplatin |
Pembrolizumab + 5-FU + cisplatin | 180,106 | 1.97 | 142,861 |
5-FU = fluorouracil; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. 5-FU + cisplatin) | Incremental (sequential) |
|---|---|---|---|---|
Discounted LYs | ||||
5-FU + cisplatin | Pre-progression | 0.60 | NA | NA |
Post-progression | 0.84 | NA | NA | |
Total | 1.44 | NA | NA | |
Pembrolizumab + 5-FU + cisplatin | Pre-progression | 0.91 | 0.31 | 0.31 |
Post-progression | 1.20 | 0.36 | 0.36 | |
Total | 2.11 | 0.67 | 0.67 | |
Discounted QALYs | ||||
5-FU + cisplatin | Pre-progression | 0.51 | NA | NA |
Post-progression | 0.64 | NA | NA | |
Total | 1.15 | NA | NA | |
Pembrolizumab + 5-FU + cisplatin | Pre-progression | 0.78 | 0.27 | 0.27 |
Post-progression | 0.91 | 0.27 | 0.27 | |
Total | 1.68 | 0.54 | 0.54 | |
Discounted costs ($) | ||||
5-FU + cisplatin | Acquisition | $2,728 | NA | NA |
Administration | $3,248 | NA | NA | |
Disease management | $3,763 | NA | NA | |
Subsequent treatment | $3,051 | NA | NA | |
AEs | $6,920 | NA | NA | |
End-of-life | $9,101 | NA | NA | |
Total | $28,811 | NA | NA | |
Pembrolizumab + 5-FU + cisplatin | Acquisition | $98,360 | $95,632 | $95,632 |
Administration | $6,249 | $3,001 | $3,001 | |
Disease management | $5,507 | $1,744 | $1,744 | |
Subsequent treatment | $3,995 | $944 | $944 | |
AEs | $6,316 | -$603 | -$603 | |
End-of-life | $8,941 | -$159 | -$159 | |
Total | $129,368 | $100,558 | $100,558 | |
ICER vs. reference ($) | Sequential ICER ($) | |||
5-FU + cisplatin | Ref. | Ref. | ||
Pembrolizumab + 5-FU + cisplatin | 169,598 | 169,598 | ||
5-FU = fluorouracil; AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; Ref. = reference; vs. = versus.
Note: results are based on deterministic results.
Detailed Results of CADTH Base Case
Table 14: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | 5-FU + cisplatin | 71,289 | 1.21 | Ref. |
Blended chemotherapy | 74,721 | 1.21 | Dominateda | |
Pembrolizumab + 5-FU + cisplatin | 180,106 | 1.97 | 142,861 | |
Sponsor’s corrected base case | Blended chemotherapy | 70,543 | 1.21 | Ref. |
5-FU + cisplatin | 72,653 | 1.21 | Dominateda | |
Pembrolizumab + 5-FU + cisplatin | 181,579 | 1.98 | 145,181 | |
CADTH reanalysis 1 | Blended chemotherapy | 54,340 | 1.21 | Ref. |
5-FU + cisplatin | 56,451 | 1.21 | Dominateda | |
Pembrolizumab + 5-FU + cisplatin | 165,849 | 1.98 | 145,442 | |
CADTH reanalysis 2 | Blended chemotherapy | 42,897 | 1.21 | Ref. |
5-FU + cisplatin | 45,008 | 1.21 | Dominateda | |
Pembrolizumab + 5-FU + cisplatin | 145,528 | 1.98 | 133,700 | |
CADTH reanalysis 3 | Blended chemotherapy | 70,363 | 1.21 | Ref. |
5-FU + cisplatin | 72,474 | 1.21 | Dominateda | |
Pembrolizumab + 5-FU + cisplatin | 181,233 | 1.80 | 188,697 | |
CADTH base case (1+2+3)b | 5-FU + cisplatin | 28,826 | 1.21 | Ref. |
Pembrolizumab + 5-FU + cisplatin | 129,370 | 1.80 | 170,819 |
5-FU = fluorouracil; CAPOX = capecitabine + oxaliplatin ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
adominated by 5-FU + cisplatin.
bPer CADTH reanalysis 4, Blended chemotherapy was removed as a comparator.
Scenario Analyses
Table 15: Summary of CADTH Scenario Analyses
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor's corrected base case | |||
5-FU + cisplatin | 71,289 | 1.21 | Reference |
Blended chemotherapy | 74,721 | 1.21 | Dominated by 5-FU + cisplatin |
Pembrolizumab + 5-FU + cisplatin | 180,106 | 1.98 | 142,861 |
CADTH's base case | |||
5-FU + cisplatin | 28,826 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,370 | 1.80 | 170,819 |
CADTH's scenario analysis 1: Assuming mFOLFOX as backbone chemotherapies | |||
5-FU + cisplatin | 28,823 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,631 | 1.80 | 171,878 |
CADTH's scenario analysis 2: Assuming CAPOX as backbone chemotherapies | |||
5-FU + cisplatin | 28,824 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 127,970 | 1.80 | 168,546 |
CADTH's scenario analysis 3: Alternative survival models for OS – 1-piece log-logistic | |||
5-FU + cisplatin | 28,821 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 128,980 | 1.66 | 222,025 |
CADTH's scenario analysis 4: Alternative survival models for OS – piecewise log-logistic with cut-off at 32 weeks | |||
5-FU + cisplatin | 28,832 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,320 | 1.78 | 176,963 |
CADTH's scenario analysis 5: Alternative survival models for OS – piecewise (log-logistic for pembrolizumab + backbone chemotherapy [CAPOX] and exponential for 5-FU + cisplatin) | |||
5-FU + cisplatin | 28,020 | 0.92 | Reference |
Pembrolizumab + 5-FU + cisplatin | 127,949 | 1.27 | 283,832 |
CADTH's scenario analysis 6: Alternative survival models for OS – piecewise, Weibull with cut-off at 40 weeks | |||
5-FU + cisplatin | 28,082 | 0.94 | Reference |
Pembrolizumab + 5-FU + cisplatin | 127,932 | 1.26 | 306,332 |
CADTH's scenario analysis 7: Alternative survival models for PFS – piecewise, log-logistic with cut-off at 37 weeks | |||
5-FU + cisplatin | 28,808 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,242 | 1.80 | 171,138 |
CADTH's scenario analysis 8: Alternative survival models for PFS – piecewise, Weibull with cut-off at 10 weeks | |||
5-FU + cisplatin | 28,859 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,417 | 1.80 | 172,265 |
CADTH's scenario analysis 9: Alternative survival models for PFS – piecewise, exponential with cut-off at 10 weeks | |||
5-FU + cisplatin | 28,851 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,424 | 1.80 | 170,652 |
CADTH's scenario analysis 10: Using PFS to reflect ToT for pembrolizumab | |||
5-FU + cisplatin | 28,821 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 142,669 | 1.80 | 192,960 |
CADTH's scenario analysis 11: Using a progression-based approach to estimate health utility | |||
5-FU + cisplatin | 28,830 | 1.14 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,376 | 1.68 | 188,121 |
CADTH's scenario analysis 12: Assuming a relative dose intensity for first-line drugs equal to 1 | |||
5-FU + cisplatin | 29,929 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 137,568 | 1.80 | 182,236 |
CADTH's scenario analysis 13: Assuming no vial sharing | |||
5-FU + cisplatin | 28,964 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 129,512 | 1.80 | 171,136 |
CADTH's scenario analysis 14: Assuming 47% of patients whose disease progressed receiving subsequent treatments | |||
5-FU + cisplatin | 40,112 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin | 144,145 | 1.80 | 176,989 |
CADTH's scenario analysis 15: Focusing on patients with PD-L1 positive subgroup | |||
5-FU + cisplatin | 28,797 | 1.19 | Reference |
Pembrolizumab + 5-FU + cisplatin | 138,109 | 2.02 | 132,155 |
CADTH's scenario analysis 16: Adopting a societal perspective | |||
5-FU + cisplatin | 200,123 | 1.21 | Reference |
Pembrolizumab + 5-FU + cisplatin) | 295,083 | 1.80 | 160,869 |
5-FU = fluorouracil; CAPOX = capecitabine + oxaliplatin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
aDominated by 5-FU + cisplatin.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
BIA = budget impact analysis.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an incidence-based budget impact analysis (BIA),20 assessing the expected budgetary impact of the introduction of pembrolizumab, in combination with platinum- and fluoropyrimidine-based chemotherapy, for the neoadjuvant treatment of patients with locally advanced unresectable or metastatic EC or HER2-negative gastroesophageal junction (GEJ) adenocarcinoma. The analysis was done from the perspective of a Canadian drug plan payer over a 3-year time horizon; the base year was assumed to be 2021 and the 3-year time horizon ran from 2022 to 2024.
The sponsor estimated population size using an epidemiology-based approach, with data obtained from various sources including: Canadian Cancer Society statistics and sponsor-conducted opinion survey of Canadian medical oncologists (N=11).20-23 The costs were obtained from publicly available drug reviews.24-28 The BIA outcomes were estimated using the number of patients expected to be treated each week, which was modelled to increase over time. For second-line treatments, the duration on treatment was based on the sponsor’s extrapolations of PFS curves associated with each treatment KEYNOTE-590 trial. The curves captured a delay in progression to second-line treatments with the use of pembrolizumab. Thus, the number of patients receiving second-line treatment was lower in the scenario in which pembrolizumab is reimbursed.
The treatment costs accrued by pembrolizumab and comparators were based on Kaplan-Meier ToT data using the KN590 trial. The market share of pembrolizumab increased from 0% to ||||% over a ||||-week period based on a linear model. Non-compliance was captured through RDI estimates lower than 100%, which are assumed to represent missed or delayed doses instead of lower doses than planned/recommended for all treatments. Drug costs were obtained from publicly available drug reviews.24-28 No drug wastage was assumed. A summary of the sponsor’s derivation of the eligible population size is presented in Figure 2, and key inputs to the BIA are documented in Table 17.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
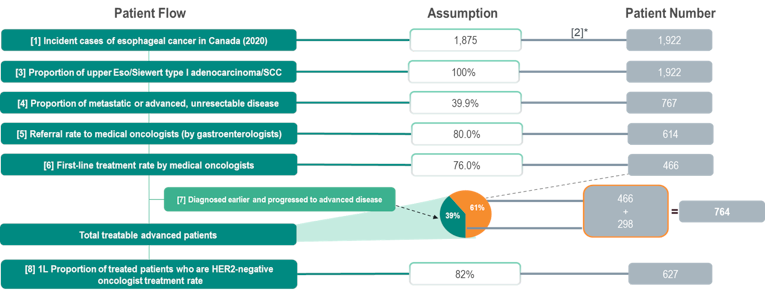
1L = first-line; Eso = esophageal; SCC = squamous cell carcinoma; HER2 = human epidermal growth factor receptor 2.
* Assuming 1% yearly growth rate (based on average annual incidence) and listing date of July 1, 2022.
Source: Sponsor’s budget impact analysis.20
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | First-line treatment of adult patients with locally advanced unresectable or metastatic carcinoma of the esophagus or HER2 negative adenocarcinoma of the esophagogastric junction |
Number of patients eligible for drug under review | 627 / 633 / 640 |
Market uptake | |
Uptake (reference scenario) Pembrolizumab + 5-FU + Cisplatin Cisplatin + 5-FU Capecitabine +Cisplatin FOLFOX CAPOX FOLFIRI Clinical trials | 0.0% / 0.0% / 0.0% 10%/ 10%/ 10% 6%/ 6%/ 6%/ 50%/ 50%/ 50%/ 13%/ 13%/ 13% 16%/ 16%/ 16%/ 5%/ 5%/ 5%/ |
Uptake (new drug scenario) Pembrolizumab + 5-FU + Cisplatin Cisplatin + 5-FU Capecitabine +Cisplatin FOLFOX CAPOX FOLFIRI Clinical trials | ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% ||||||||% / ||||||||%/ ||||||||% |
Cost of 1L treatment (per patient)a | |
Cost of treatment course Pembrolizumab + 5-FU + Cisplatin Cisplatin + 5-FU Capecitabine +Cisplatin FOLFOX CAPOX FOLFIRI | $||||||||b $|||||||| $|||||||| $|||||||| $|||||||| $|||||||| |
Cost of 2L treatment (per patient)a | |
Cost of treatment course Ramucirumab + Paclitaxel Irinotecan monotherapy Docetaxel monotherapy Paclitaxel monotherapy | $10,437.72 $322.00 $1,575.96 $50.08 |
CAPECISP = Cisplatin-capecitabine, CAPOX = Oxaliplatin-capecitabine, CISPFU = Cisplatin-5-Fluorouracil, FOLFIRI = Folinic Acid (Leucovorin)-Fluorouracil-Irinotecan, FOLFOX = Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin, HER2 = human epidermal growth factor receptor 2; 1L = first line, 2L = second line.
aCost estimation assumed average weight of 71.22 kg, body surface area of 1.84 m2, no drug wastage, and adjusted for relative dose intensity.
bAssuming pembrolizumab dose regimen of 200 mg every 3 weeks.20
Source: Sponsor’s Budget Impact Analysis (Table 5).20
Table 18: Sponsor’s Estimation of RDI
Drug | Relative dose intensity |
|---|---|
Pembrolizumab combination therapy | |
Pembrolizumab | ||||||||% |
Cisplatin | ||||||||% |
5-FU | ||||||||% |
Comparators | |
Cisplatin | ||||||||% |
5-FU | ||||||||% |
Capecitabine | ||||||||% |
Oxaliplatin | ||||||||% |
Leucovorin | ||||||||% |
Irinotecan | ||||||||% |
Source: Sponsor’s Budget Impact Analysis.20
Summary of the Sponsor’s Budget Impact Analsyis Results
The sponsor estimated the net 3-year budget impact to the public drug plans of introducing pembrolizumab for the first-line treatment of locally advanced unresectable or metastatic carcinoma of the esophagus or HER2 negative adenocarcinoma of the esophagogastric junction in adults to be $71,576,510 (Year 1: $5,605,604; Year 2: $26,008,998; Year 3: $39,961,908).20
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumptions regarding comparators and market share differ between the CUA and BIA: In the submitted BIA,20 the sponsor assumed treatments that accrue market share include CISPFU, CAPECISP, FOLFOX, CAPOX, FOLFIRI, and clinical trials. In the economic evaluation,1 the assumed treatments in the blended chemotherapy arm that accrue market share include CISPFU, CAPECISP, FOLFOX, and CAPOX. The sponsor acknowledged that FOLFIRI is for patients who are not candidates for platinum therapy but assumes that FOLFIRI captures 16% of market share in the BIA report. According to the clinical experts consulted by CADTH for this review, FOLFIRI is most typically used in the treatment of gastric cancer and not commonly used in the first-line setting for EAC and GEJC. CADTH notes that gastric cancer is outside the scope of this review. The sponsor also assumes that clinical trials capture 5% of market share in the submitted BIA report. However, the treatments that accrued market share in the economic evaluation exclude FOLFIRI and clinical trials altogether. Moreover, the sponsor’s assumptions on market share captured by relevant treatments differ between the CUA and BIA.
In CADTH reanalysis, the same proportion of market shares as assumed in the CUA were adopted to ensure alignment.
The proportion of patients moving to second-line treatment do not represent clinical practice: The sponsor assumed second-line treatment rates of 44% for pembrolizumab combination therapy and 48% for all other comparator regimens. According to the clinical experts consulted by CADTH for this review, very few patients with advanced or metastatic esophageal carcinoma are healthy enough to transition to second-line treatments in clinical practice. The clinical experts estimated that, in practice, the proportion of patients transitioning to second-line treatments may be in the range of 10% to 15%.
In CADTH reanalysis, a second-line treatment rate of 10% based on the first-line treatment received was assumed.
The sponsor reported outdated unit prices: The sponsor obtained unit prices of comparators using literature dated from 2015 to 2019.24-28 The sponsor’s adopted unit price of 5-FU, oxaliplatin, leucovorin, and irinotecan do not reflect current publicly available prices.
There is uncertainty in the assumed referral rate and HER2-nagtive treatment rate: The sponsor assumed a referral rate to medical oncologist of 80% and HER2 negative oncology treatment rate of 82%. Feedback from clinical experts consulted for this review by CADTH indicated the assumed referral rate and HER2- treatment rate may be underestimated, based on their experience in Canadian practice.
In CADTH reanalysis, referral rate to medical oncologists was assumed to be 85% and HER2-negative oncologist treatment rate was assumed to be 90% based on feedback from the clinical experts.
There is uncertainty in assumptions around speed of uptake: The sponsor assumed that pembrolizumab-chemotherapy combination captures ||||||% of the current market by |||||| weeks. The slope of the uptake is assumed to be linear, but a half-cycle correction is then applied, thus the 3 year growth in the submitted BIA is not linear. The clinical experts consulted by CADTH considered the speed of uptake to be uncertain. The budget impact is sensitive to rate of market uptake, which is based on the sponsor’s assumptions.
CADTH explored the impact of assuming slower market uptake rate by arbitrarily assuming 100% market share of pembrolizumab at 154 weeks (3 years) in a scenario analysis; this equated to a year 3 market share of 85% given the sponsor’s half-cycle correction approach.
The budget impact model has limited transparency and flexibility: The sponsor’s submitted BIA model is overly complex, using circular referencing and hard coding which increases validity issues when making changes to the model and ensuring consistency throughout the budget impact model. Furthermore, the model lacks transparency and has limited flexibility to allow the reviewers to assess the impact of changing the sponsor’s base assumptions on estimated budgetary impact.
CADTH could not address this limitation. CADTH notes that the results presented should be treated with a degree of caution as the validity of the model calculations could not be thoroughly appraised.
CADTH Reanalyses of the Budget Impact Analysis
Based on the limitations identified, CADTH corrected the sponsor’s base case by updating unit price for 5-FU, oxaliplatin, leucovorin and irinotecan, and updating leucovorin dose to 400 mg/m2 for FOLFOX. CADTH revised the corrected BIA base case by aligning market share proportions with the CUA, decreasing the second-line treatment rate to 10%, increasing the referral rate to 85% and increasing HER2-negative treatment rate to 90%.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Unit price change | Sponsor assumed unit price of $0.0030 for 5-FU, $10.2000 for oxaliplatin, $0.0500 for leucovorin and $0.5000 for irinotecan. | CADTH assumed unit price of $0.0322 for 5-FU, $0.7254 for oxaliplatin, $0.1488 for leucovorin and $0.0810 for irinotecan. |
2. Leucovorin dose change | Recommended leucovorin dose is 200 mg/m2 for mFOLFOX | Recommended leucovorin dose is 400 mg/m2 for mFOLFOX based on Cancer Care Ontario monographs12 |
Changes to derive the CADTH base case | ||
1. Align market share proportions | Sponsor assumed accrued market share of 10% for CISPFU, 6% for CAPECISP, 50% for FOLFOX, 13% for CAPOX, 16% for FOLFIRI and 5% for clinical trials. | For alignment with CUA, CADTH assumed accrued market share of 12.5% for CISPFU, 6.7% for CAPECISP, 64.2% for FOLFOX and 16.6% for CAPOX. |
2. Second-line treatment rates | Sponsor assumed 2L treatment rates of 44% for pembrolizumab combination therapy and 48% for all other comparator regimens | Based on feedback from clinical expert, CADTH assumed 2L treatment rate of 10% |
3. Referral rate | Sponsor assumed a referral rate of 80% to medical oncologists | Based on feedback from clinical expert, CADTH assumed a referral rate of 85% to medical oncologists |
4. HER2-negative treatment rate | Sponsor assumed HER2-negative oncologist treatment rate of 82% | Based on feedback from clinical expert, CADTH assumed HER2-negative oncologist treatment rate of 90% |
CADTH base case | CADTH reanalysis 1 + 2 + 3 + 4 | |
CAPECISP = Cisplatin-capecitabine, CISPFU = Cisplatin-5-Fluorouracil, FOLFIRI = Folinic Acid (Leucovorin)-Fluorouracil-Irinotecan, FOLFOX = Folinic Acid (Leucovorin)-Fluorouracil-Oxaliplatin, HER2 = human epidermal growth factor receptor 2.
Applying these changes increased the total 3-year budget impact of reimbursing pembrolizumab, in combination with platinum- and fluoropyrimidine-based chemotherapy is $7,281,922 in year 1, $33,335,288 in year 2, $50,440,428 in year 3. After 3 years since entering the market, the total anticipated budget impact of pembrolizumab is $91,057,638. The results of the CADTH step-wise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21.
Table 20: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case, as provided | $71,576,510 |
CADTH correction 1 | $76,156,676 |
CADTH correction 2 | $71,536,244 |
Sponsor’s base case, corrected | $76,036,844 |
Stepped analysis | |
CADTH reanalysis 1 | $76,100,101 |
CADTH reanalysis 2 | $78,020,156 |
CADTH reanalysis 3 | $80,789,147 |
CADTH reanalysis 4 | $83,455,073 |
CADTH base case (1+2+3+4) | $91,057,638 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 21. The scenario analysis involved:
Assuming sponsor’s assumptions on market share and redistributing market share of clinical trials to FOLFOX
Assuming 100% of referral rate to medical oncologists
Assuming slower uptake (i.e., market share of pembrolizumab of 100% at 154 weeks)
Assuming 100% HER2-negative oncologist treatment rate
Assuming 70% HER2-negative oncologist treatment rate
Assuming 100% on Q6W dosing
Assuming no transitioning to second-line treatments (0% second-line treatment rate based on the first-line treatment received)
Assuming a price reduction of 75% (per CADTH economic evaluation reanalysis)
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is sensitive to the size of assumptions on referral rate to medical oncologist, HER2-negative treatment rate, and the price of pembrolizumab. If 100% referral rate is assumed, the expected budget impact is estimated to be $107,126,633 over 3 years. If 100% HER2-negative treatment rate is assumed, the expected budget impact is estimated to be $101,175,153 over 3 years. If the price reduction identified as part of the economic evaluation is achieved, the budget impact is reduced to $23,265,169 over 3 years.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case, as provided | Reference | $5,513,690 | $5,513,690 | $5,513,690 | $5,513,690 | $44,891,194 |
New drug | $5,513,690 | $17,603,020 | $39,558,368 | $53,792,626 | $116,467,704 | |
Budget impact | $0 | $5,605,604 | $26,008,998 | $39,961,908 | $71,576,510 | |
Submitted base case, as corrected | Reference | $3,823,935 | $10,081,111 | $11,614,782 | $11,876,786 | $37,396,613 |
New drug | $3,823,935 | $16,207,415 | $39,409,353 | $53,992,756 | $113,433,458 | |
Budget impact | $0 | $6,126,304 | $27,794,571 | $42,115,969 | $76,036,844 | |
CADTH base case | Reference | $1,687,588 | $3,331,060 | $3,714,594 | $3,787,156 | $12,520,399 |
New drug | $1,687,588 | $10,612,982 | $37,049,883 | $54,227,584 | $103,578,037 | |
Budget impact | $0 | $7,281,922 | $33,335,288 | $50,440,428 | $91,057,638 | |
CADTH scenario analysis: exclude market share of clinical trials | Reference | $1,718,838 | $3,376,006 | $3,759,482 | $3,832,492 | $12,686,819 |
New drug | $1,718,838 | $10,652,551 | $37,067,508 | $54,238,595 | $103,677,492 | |
Budget impact | $0 | $7,276,545 | $33,308,025 | $50,406,102 | $90,990,672 | |
CADTH scenario analysis: 100% referral rate | Reference | $1,985,397 | $3,918,895 | $4,370,111 | $4,455,478 | $14,729,881 |
New drug | $1,985,397 | $12,485,861 | $43,588,097 | $63,797,158 | $121,856,514 | |
Budget impact | $0 | $8,566,967 | $39,217,986 | $59,341,680 | $107,126,633 | |
CADTH scenario analysis: 100% market share of pembrolizumab at 154 weeks | Reference | $1,687,588 | $3,331,060 | $3,714,594 | $3,787,156 | $12,520,399 |
New drug | $1,687,588 | $8,248,722 | $27,039,486 | $51,037,500 | $88,013,295 | |
Budget impact | $0 | $4,917,661 | $23,324,892 | $47,250,343 | $75,492,897 | |
CADTH scenario analysis: 100% HER2-negative treatment rate | Reference | $1,875,097 | $3,701,178 | $4,127,327 | $4,207,951 | $13,911,554 |
New drug | $1,875,097 | $11,792,202 | $41,166,536 | $60,252,872 | $115,086,707 | |
Budget impact | $0 | $8,091,024 | $37,039,209 | $56,044,920 | $101,175,153 | |
CADTH scenario analysis: 70% HER2-negative treatment rate | Reference | $1,312,568 | $2,590,825 | $2,889,129 | $2,945,566 | $9,738,088 |
New drug | $1,312,568 | $8,254,542 | $28,816,575 | $42,177,010 | $80,560,695 | |
Budget impact | $0 | $5,663,717 | $25,927,446 | $39,231,444 | $70,822,607 | |
CADTH scenario analysis: 100% Q6W dosing | Reference | $1,687,588 | $3,331,060 | $3,714,594 | $3,787,156 | $12,520,399 |
New drug | $1,687,588 | $10,612,982 | $37,049,883 | $54,227,584 | $103,578,037 | |
Budget impact | $0 | $7,281,922 | $33,335,288 | $50,440,428 | $91,057,638 | |
CADTH scenario analysis: 0% 2L treatments rate | Reference | $954,104 | $1,111,778 | $1,125,402 | $1,136,631 | $4,327,915 |
New drug | $954,104 | $8,419,968 | $34,616,462 | $51,749,820 | $95,740,354 | |
Budget impact | $0 | $7,308,190 | $33,491,060 | $50,613,189 | $91,412,439 | |
CADTH scenario analysis: Price reduction by 75% | Reference | $1,687,588 | $3,331,060 | $3,714,594 | $3,787,156 | $12,520,399 |
New drug | $1,687,588 | $5,192,286 | $12,216,924 | $16,688,769 | $35,785,567 | |
Budget impact | $0 | $1,861,226 | $8,502,330 | $12,901,613 | $23,265,169 |
Note: The scenario analyses are carried out on CADTH base case.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.