CADTH Health Technology Review
Codeine for Acute Extremity Pain
Rapid Review
Authors: Dave K. Marchand, Charlene Argáez
Abbreviations
AE
adverse event
APAP
N-acetyl-para-aminophenol (i.e., acetaminophen, paracetamol)
CI
confidence interval
ED
emergency department
MA
meta-analysis
NRS
numerical rating scale
NSAID
nonsteroidal anti-inflammatory drug
RCT
randomized controlled trial
SR
systematic review
VAS
visual analogue scale
Key Messages
No comparative evidence was found on the use of codeine, as a single ingredient, for acute extremity pain management.
There are many types of codeine combinations drugs available, which makes a direct comparison difficult and increases the uncertainty of the results. Although the overall analysis is inconclusive, in many comparisons, codeine was no different than the comparator group in increasing patient satisfaction or in reducing pain scores, the need for additional analgesia, and the number of adverse events.
Most of the evidence is from studies without a placebo arm; therefore, it is not possible to know how much of the pain reduction was unrelated to codeine.
Most of the evidence is from studies in which patients received a single dose of a codeine combination drug and were observed for a very limited time, usually minutes to hours. This increases the uncertainty of the findings, and safety information needs to be interpreted with caution.
Context and Policy Issues
Injuries to the upper and lower extremities can result from myriad causes such as sprains, fractures, crushes, and thermal or chemical injuries. A frequent outcome of such injuries is pain, which can be classified as acute (lasting for minutes to weeks) or chronic (lasting months to years).1,2
The goals of therapy for acute extremity pain include the recognition that the patient is experiencing pain, the rapid reduction of pain intensity, and the general minimization of discomfort until the cause of the pain is treated.1,2 Therapeutic options for acute pain control include both non-pharmacological (e.g., ice, splint, sling) and pharmacological choices depending on the level of pain associated with the injury. Non-opioid analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs), N-acetyl-para-aminophenol (APAP) (i.e., acetaminophen, paracetamol), and salicylates, may be sufficient for mild to moderate pain.1 Whereas opioids (e.g., morphine, fentanyl, hydromorphone, hydrocodone, oxycodone, codeine), alone or in combination with a non-opioid, are often the next step for recalcitrant pain or as a starting point for severe pain.1,2
Opioid prescribing practices have come under scrutiny in recent years as Canada and other jurisdictions battle with an opioid epidemic.3 For this and other reasons, there has been a desire to optimize opioid prescribing in those cases in which it is possible.4 The appropriate role of codeine for pain management is being questioned and is the focus of this report.
In Canada, several formulations of codeine are available for treatment of pain. Codeine is an agonist of primarily the mu receptor5,6 in the central nervous system and in peripheral tissues such as the gastrointestinal tract.7 It is metabolized in the liver by the cytochrome P450 isoenzyme CYP2D6 to various metabolites, including morphine,1,5 which accounts for some of its analgesic effect.1,5,6 The rate of metabolism by the CYP2D6 isoenzyme is known to vary in the general population,1,5 which highlights the ranges of pain relief and side effects that can be observed when codeine is used.1,7 It is a relatively weak opioid,6 and may also be used in combination with APAP or NSAIDs to provide an additive analgesic effect.1
This report is part of a series questioning the appropriate use of codeine in pain management. A previous report summarized and critically appraised evidence available in November 2020 on codeine for pain related to osteoarthritis of the knee and hip.8 Two other summaries with critical appraisal are in progress at the time of writing for the use of codeine for acute dental pain9 and pain related to Caesarean section.10 Other related CADTH reports on codeine include 3 summaries with critical appraisals from 2019.11-13 The first sought evidence on codeine for acute pain from urological or general surgery,12 the second sought evidence on codeine for pediatric patients with acute pain,11 and the third sought evidence on codeine for acute pain in patients undergoing orthopedic surgery.13
The objective of this report is to investigate the clinical effectiveness of codeine or codeine combination products for the management of acute extremity pain.
Research Questions
What is the clinical effectiveness of codeine for patients with acute extremity pain?
What is the clinical effectiveness of codeine with acetaminophen and/or an NSAID for patients with acute extremity pain?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via OVID, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were codeine and extremity pain. Filters were applied to limit the retrieval to health technology assessments, systematic reviews (SRs), and meta-analyses (MAs), randomized controlled trials (RCTs), and non-randomized studies. The search was also limited to English language documents published between January 1, 2010, and November 23, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients (any age) with acute extremity pain presenting to primary care or an emergency department |
Interventions | Q1: Codeine alone Q2: Codeine with acetaminophen and/or an NSAID (e.g., ASA, ibuprofen, naproxen) as single products or as combination drugs (e.g., codeine-acetaminophen-caffeine combination) |
Comparators | Other opioids (e.g., tramadol, oxycodone, morphine, hydromorphone, fentanyl), 1 or more non-opioid analgesics (e.g., acetaminophen, NSAID), other opioid combinations (e.g., oxycodone with acetaminophen), or placebo |
Outcomes | Clinical effectiveness (e.g., pain control, pain scales, health-related qualify of life, mobility), safety (e.g., overdose-related adverse events such as respiratory depression and liver toxicity, other adverse events such as constipation and risk of falls, dependence/addiction, hospitalizations) |
Study designs | Health technology assessments, SRs, RCTs, non-randomized studies |
NSAID = nonsteroidal anti-inflammatory drug; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2010. Articles that included patients with pain related to osteoarthritis of the knee or hip were excluded because this particular population is the object of a stand-alone CADTH report.8 Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SR.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)14 for SRs and the Downs and Black checklist15 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
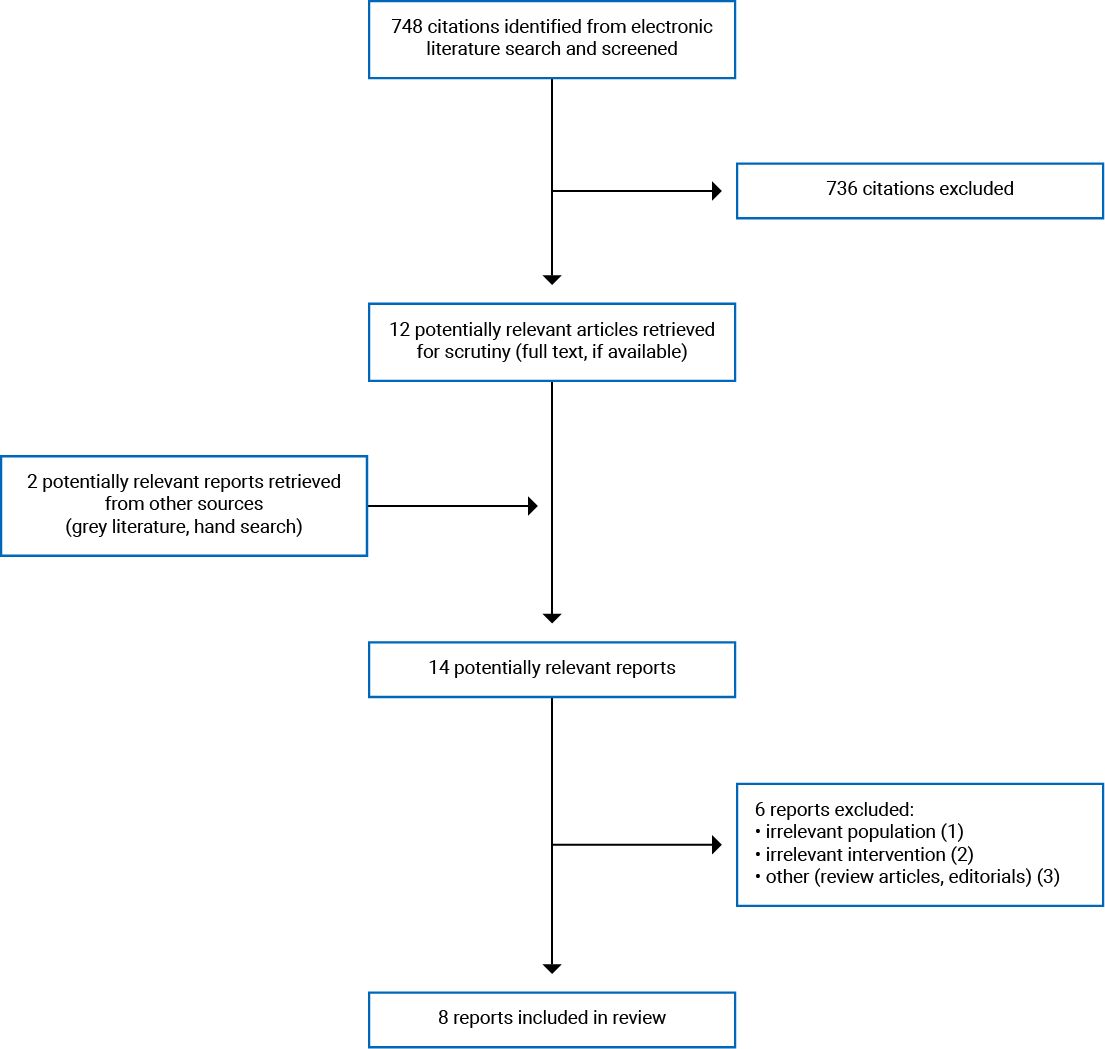
A total of 748 citations were identified in the literature search. Following screening of titles and abstracts, 736 citations were excluded and 12 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 14 potentially relevant articles, 6 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. These comprised 2 SRs, 5 RCTs, and 1 non-randomized study. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)16 flow chart of the study selection.
Summary of Study Characteristics
Two SRs,17,18 5 RCTs,19-23 and 1 non-randomized study24 were identified and included in this review. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Both SRs17,18 had broader inclusion criteria than this review. Specifically, 1 SR17 was a review of Cochrane SRs on the efficacy of over-the-counter analgesics in the context of acute post-operative pain; however, none of the included SRs evaluated the comparison of interest for this report, namely the clinical effectiveness of codeine alone or in combination preparations compared with other opioids, non-opioids, or placebo for the management of acute extremity pain. The other SR18 reviewed general pain management for acute pain after foot and ankle surgery. Only the characteristics and results of the subset of relevant studies will be described in this report.
Study Design
One SR,17 published in 2015, included Cochrane reviews of RCTs. Authors searched the Cochrane Database of SRs Issue 4 on the Cochrane Library for relevant SRs. The other SR18 with relevant content was published in 2015. Authors searched multiple electronic databases for eligible SRs, MAs, literature reviews, RCTs, and trials published between January 1946 and February 2013, for evidence on pain management after elective foot and ankle surgery. The SR contained 1 primary RCT study which was identified as relevant to this report and did not overlap with the other SR, as demonstrated in Appendix 5.
The 5 RCTs19-23 were of double-blind design, and followed patients for 90 minutes,22 120 minutes,19,23 or 24 hours.20,21
The non-randomized study24 was a prospective cohort study that followed patients for 120 minutes.
Country of Origin
The primary authors of 1 SR were from the UK,17 whereas those of the other SR18 and 3 RCTs19-21 were from the US. The primary authors of the remaining 2 RCTs were from Australia22 and Canada.23 The primary author of the non-randomized study was from Italy.24
Among the RCTs, 2 were multi-centre studies, the first conducted at 2 urban sites in the US,19 and the other at 3 urban centres in Australia.22
Patient Population
One SR17 sought evidence on the efficacy and safety of single-dose oral analgesics for acute post-operative pain in patients 15 years of age or older; the other SR18 included studies of adults with foot and ankle surgery pain.
The Chang et al. (2017) RCT19 was set at an urban emergency department (ED) and enrolled adult patients with moderate to severe acute extremity pain. It recruited 416 eligible patients (104 in each group); the mean age was 37 years and 43% to 54% were female, depending on the intervention group.
The Graudins et al. (2016) RCT22 was set at 3 urban EDs and enrolled adults aged 18 years to 75 years with acute moderate pain from a limb injury, such as upper or lower limb sprain, fracture, crush, or skin wound, but digital injuries were excluded. Authors defined moderate pain as a score of 4 to 7 on a visual analogue scale (VAS).22 The study recruited 185 eligible patients, divided into 3 intervention groups; the mean age ranged from 31 years to 35 years and 25.4% to 35.5% were female, depending on the intervention group.22
The Chang et al. (2015)20 and Chang et al. (2014)21 RCTs were set at an academic urban ED and enrolled adults aged 21 years to 64 years with acute musculoskeletal extremity pain. Both studies recruited 240 eligible patients (120 per group).20,21 The mean age in the 2015 RCT20 groups were 38 years and 39 years and both groups were 56% female. The mean age in the 2014 RCT21 groups were 34 years and 37 years, and the groups were 43% and 52% female.
The Le May et al. (2013)23 RCT was set at an urban pediatric tertiary care ED and enrolled children aged 7 years to 18 years with acute pain due to a musculoskeletal injury to a limb. Authors recruited 83 eligible patients, divided into 2 intervention groups. Mean ages of the groups were 10.9 years and 11.2 years; 45% and 46% were female.
The non-randomized study24 was set at an urban tertiary care ED and enrolled adults older than 18 years with pain to an extremity due to localized trauma or inflammation. Authors enrolled 200 patients, divided into 2 intervention groups. Mean ages were 28.0 years and 69.2 years; 46.9% and 51.7% were female.24 .
Interventions and Comparators
One SR17 sought evidence on any analgesic product available without prescription in the jurisdiction of the study compared to placebo, whereas the other SR18 compared a variety of pharmacological interventions (e.g., opioids, gabapentin, NSAIDs, ketamine, APAP, corticosteroids) to one another or a control group or used no comparator.
The Chang et al. (2017) RCT19 compared 4 analgesic drug combinations to one another. These were ibuprofen 400 mg and APAP 1,000 mg, oxycodone 5 mg and APAP 325 mg, hydrocodone 5 mg and APAP 300 mg, as well as codeine 30 mg and APAP 300 mg.19
The Graudins et al. (2016) RCT22 compared 3 analgesic drug combinations to one another. These were APAP 1,000 mg, ibuprofen 400 mg, and thiamine (i.e., vitamin B1) 100 mg; APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg; as well as APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg.
Chang et al. (2015)20 compared oxycodone 5 mg and APAP 325 mg versus codeine 30 mg and APAP 300 mg, both dosed every 4 hours, if needed, for 3 days. Chang et al. (2014)21 compared hydrocodone 5 mg and APAP 500 mg versus codeine 30 mg and APAP 300 mg, also dosed every 4 hours, if needed, for 3 days.
The Le May et al. (2013)23 RCT compared 2 drug combinations: a codeine suspension 1 mg/kg (to a maximum of 60 mg) and ibuprofen chew tablets 10 mg/kg (to a maximum of 600 mg) versus a placebo suspension and ibuprofen chew tablets 10 mg/kg (to a maximum of 600 mg).
The non-randomized study24 compared ketorolac 15 mg versus the combination of APAP 1,000 mg and codeine 60 mg.
Outcomes
One SR17 considered patient-reported pain relief, whereas the other SR18 considered post-operative pain scores, supplemental analgesic requirements, and adverse events (AEs).
The outcomes of interests in the RCTs were pain scores using a numerical rating scale (NRS),19-21 or a VAS,22,23 the need for additional analgesia,22 patient satisfaction,20,21 and AEs.20-23
The non-randomized study sought outcomes on pain scores using a NRS.24
Summary of Critical Appraisal
The strengths and limitations of the SRs17,18 were assessed using the relevant components of AMSTAR 214; however, because none of the primary studies included in 1 SR17 were relevant to this report, a number of the checklist items were not applicable. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
In both SRs,17,18 the research questions and the inclusion criteria were well described, and the study selection was completed in duplicate. The studies included in the Wang et al. (2015)18 SR were partially described, although greater detail regarding the population characteristics (such as age, gender, type of surgery, and presence of complications during surgery) could have been provided. One SR17 reported how many reviewers were involved in data extraction, provided a justification of their choice of included study designs, and provided a list of excluded studies; however, the other did not,18 possibly resulting in missed studies. Although the authors searched at least 2 databases, their restrictions (i.e., language, study design) were not justified; they did not search the reference lists of included studies, they did not consult experts in the field, nor did they search the grey literature.18 It is possible this may have also resulted in missed studies. One SR17 established methods before the conduct of the review, reducing the risk of reporting bias; however, it is unclear if their protocol was registered with an international register of SRs. The second SR18 made no mention of a written protocol, thus it is unknown if any changes to the protocol were made throughout the review process or if there was selective reporting of SR results. The authors declared conflicts of interests related to this SR18; however, they did not discuss how these were managed during the review design, data interpretation and analysis, or authorship.
RCTs
Strengths of all RCTs19-23 included clear descriptions of objectives, interventions, main outcomes, population characteristics, and eligibility criteria. Major findings were described in a way that allowed verification of analyses and conclusions, the time period over which patients were recruited was specified, and the data analyses were planned at the outset. The randomization method was mentioned for 4 RCTs.19-21,23 Although blinding of the patients and investigators was reported by all RCTs,19-23 blinding was confirmed by 1 RCT.22
One RCT19 did not collect information on AEs. Four RCTs20-23 sought evidence after a single dose of the intervention and with a limited observation window (30 minutes to 24 hours); therefore, their safety data need to be interpreted with caution.
Two RCTs19,23 collected information on concurrent non-pharmacological interventions that may have had an impact on pain levels (e.g., ice, splints, slings, elastic bandage, casts), whereas 3 other RCTs20-22 did not, introducing uncertainly whether the use of concurrent non-pharmacological interventions impacted the overall findings among all groups.
Although 4 RCTs19-22 reported being adequately powered to detect a between-group clinically meaningful difference (i.e., defined by the authors as a NRS difference of 1.319-21; VAS difference of 1.523), 1 RCT22 did not explicitly state their power calculations.
Due to poor recruitment, Graudins et al. (2016)22 changed the upper age of enrolment eligibility from 65 years to a maximum 75 years after 16 months of enrolment. At the same time, the definition of acute pain was increased from less than 8 hours to less than 48 hours.22 These changes may have introduced a bias, and it is not clear if the participants enrolled before and after the changes differed in other important characteristics. Furthermore, it was not reported if the data before and after the changes were analyzed separately.
Chang et al. (2015)20 and Chang et al. (2014)21 asked patients to recall their pain level during a telephone follow-up 24 hours after ED discharge, introducing the possibility of recall bias. Both studies also found patient non-compliance with the interventions; authors of 1 RCT21 based their conclusions on the analysis of treatment (i.e., per-protocol analysis), meaning the comparisons among treatment groups may have been biased due to dropouts.
The recruitment in Le May et al. (2013)23 took place on weekdays between 10:00 a.m. and 4:00 p.m., which may not necessarily follow the unpredictable nature of acute extremity injury. The characteristics of the population admitted to the hospital outside these hours may be have been different, which may have introduced a recruitment bias and reduced the generalizability to the population at-large.
Non-Randomized Study
Strengths identified in the non-randomized study24 include clear descriptions of objectives, interventions, main outcomes, population characteristics, and eligibility criteria. The study used a prospective cohort design yet did not discuss losses to follow-up or provide patient characteristics for withdrawals and dropouts.24 Although none of the primary outcomes were statistically significant, all of the statistically significant results from this study arose from analyses in which it was not clear if they were planned a priori.24 These unplanned analyses may have generated results in the absence of a true effect and are thus unreliable. The evidence was also garnered from a single dose of the intervention or comparator with limited time for observation of AEs (120 minutes); therefore, the safety profile needs to be interpreted with caution.
Summary of Findings
A detailed summary of findings and authors’ conclusions is provided in Appendix 4.
Clinical Effectiveness of Codeine for Patients With Acute Extremity Pain
No relevant evidence regarding codeine, as a single ingredient, for patients with acute extremity pain was identified; therefore, no summary can be provided.
Clinical Effectiveness of Codeine With Acetaminophen and/or an NSAID for Patients With Acute Extremity Pain
Pain Scores
Information regarding pain score outcomes with codeine combination products in patients with acute extremities pain was available from 1 SR,18 5 RCTs,19-23 and 1 non-randomized study.24
One relevant publication was identified in the SR18 and found that flurbiprofen 50 mg every 4 hours to 6 hours was superior (P < 0.01) at decreasing post-surgical foot and ankle pain between zero and 24 hours compared with codeine 30 mg and APAP 300 mg every 4 hours to 6 hours.18 However, there was no difference between 25 hours and 96 hours.18
The Chang et al. (2017) RCT19 compared 4 combinations of analgesics to one another: ibuprofen 400 mg and APAP 1,000 mg, oxycodone 5 mg and APAP 325 mg, hydrocodone 5 mg and APAP 300 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the absolute pain score decrease at 1 hour and 2 hours, or in the mean pain score decrease at 1 hour and 2 hours.19 Authors also analyzed a subset of patients with a baseline NRS score of 10 (i.e., worst possible pain) or a documented fracture and found no particular drug combination was better than another at decreasing the pain score of this subgroup at 2 hours.19
The Graudins et al. (2016) RCT22 compared 3 combinations of analgesics to one another: APAP 1,000 mg, ibuprofen 400 mg, and thiamine 100 mg (the non-opioid group); APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg (the codeine group); as well as APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg (the oxycodone group). Authors reported no between-group differences (i.e., statistically non-significant) in the mean pain score decrease at 30 minutes (primary outcome).22
The Chang et al. (2015) RCT20 compared 2 combinations of analgesics to one another: oxycodone 5 mg and APAP 325 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the mean pain score decrease at 2 hours or in the percentage of patients experiencing a decrease in pain score of at least 50%.20
The Chang et al. (2014) RCT21 compared 2 combinations of analgesics to one another: hydrocodone 5 mg and APAP 500 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the mean pain score decrease at 2 hours or in the percentage of patients experiencing a decrease in pain score of at least 50%.21
The Le May et al. (2013) RCT23 compared 2 combinations of pediatrically formulated analgesics to one another: codeine 1 mg/kg and ibuprofen 10 mg/kg, as well as a placebo and ibuprofen 10 mg/kg. Authors reported no between-group differences (i.e., statistically non-significant) in the mean pain scores at 60 minutes, 90 minutes, and 120 minutes.23
The Buccelletti et al. (2014) non-randomized study24 compared ketorolac 15 mg with the combination of APAP 1,000 mg and codeine 60 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the NRS pain score reduction at 30 minutes, in the analgesic effect in non-traumatic pain at 30 minutes or 120 minutes, or in the analgesic effect in traumatic pain at 30 minutes or 120 minutes.24 Yet, authors found that APAP 1,000 mg and codeine 60 mg was superior to ketorolac 15 mg at 120 minutes in cases of pain of fracture or muscular origin (P = 0.030 and P = 0.044, respectively).24 However, these results stemmed from unplanned retrospective analyses and are thus unreliable. Authors also reported on the use of these drug combinations for acute pain based on anatomic origin; however, there are discrepancies in data reporting precluding the full analysis of these results.
Rescue Analgesia
Information regarding the use of rescue analgesia with codeine combination products in patients with acute extremities pain was available from 2 RCTs.19,22
The Chang et al. (2017) RCT19 compared 4 combinations of analgesics to one another: ibuprofen 400 mg and APAP 1,000 mg, oxycodone 5 mg and APAP 325 mg, hydrocodone 5 mg and APAP 300 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the number of patients requiring rescue analgesic or the rescue dose required, in morphine equivalents.19
The Graudins et al. (2016) RCT22 compared 3 combinations of analgesics to one another: APAP 1,000 mg, ibuprofen 400 mg, and thiamine 100 mg (the non-opioid group); APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg (the codeine group); as well as APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg (the oxycodone group). Authors reported that 3 of 61 (4.9%) in the non-opioid group and zero patients in both the codeine and oxycodone groups required additional analgesia within 30 minutes (primary outcome).22 Authors reported that 18.0%, 11.3%, and 3.4% of patients in the non-opioid, codeine, and oxycodone groups, respectively, required additional analgesia within 90 minutes.22
Patient Satisfaction
Information regarding pain score outcomes with codeine combination products in patients with acute extremities pain was available from 3 RCTs.20-22
The Graudins et al. (2016) RCT22 compared 3 combinations of analgesics to one another: APAP 1,000 mg, ibuprofen 400 mg, and thiamine 100 mg (the non-opioid group); APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg (the codeine group); as well as APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg (the oxycodone group). Authors reported that 45 of 61 (73.8%), 47 of 62 (75.8%), and 39 of 59 (66.1%) patients in the non-opioid, codeine, and oxycodone groups, respectively, were satisfied with their initial analgesia.22
The Chang et al. (2015) RCT20 compared 2 combinations of analgesics to one another: oxycodone 5 mg and APAP 325 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in overall patient satisfaction or in percentage of patients who would want the same analgesic combination should they experience a similar degree of pain in the future.20
The Chang et al. (2014) RCT21 compared 2 combinations of analgesics to one another: hydrocodone 5 mg and APAP 500 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in overall patient satisfaction or in percentage of patients who would want the same analgesic combination should they experience a similar degree of pain in the future.21
Adverse Events
Information regarding AE outcomes with codeine combination products in patients with acute extremities pain was available from 1 SR,18 5 RCTs,20-23 and 1 non-randomized study.24
One relevant publication was identified in the SR18 which found no difference (statistical data not reported) in AEs between flurbiprofen 50 mg every 4 hours to 6 hours for 96 hours compared with codeine 30 mg and APAP 300 mg.18
The Graudins et al. (2016) RCT22 compared 3 combinations of analgesics to one another: APAP 1,000 mg, ibuprofen 400 mg, and thiamine 100 mg (the non-opioid group); APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg (the codeine group); as well as APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg (the oxycodone group). Authors reported 2, 1, and 10 AEs in the non-opioid (n = 61), codeine (n = 62), and oxycodone (n = 59) groups, respectively.22 types of AEs were heartburn and light-headedness in the non-opioid group; not specified in the codeine group; and light-headedness, nausea, the combination of light-headedness and nausea, and drowsiness in the oxycodone group.22
The Chang et al. (2015) RCT20 compared 2 combinations of analgesics to one another: oxycodone 5 mg and APAP 325 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the occurrence of AEs.20 Types of AEs in the oxycodone group were nausea (12%), vomiting (4%), constipation (0%), diarrhea (1%), pruritus (5%), rash (2%), dizziness (10%), drowsiness (28%), and confusion (1%).20 Types of AEs in the codeine group were nausea (12%), vomiting (2%), constipation (0%), diarrhea (3%), pruritus (4%), rash (3%), dizziness (13%), drowsiness (22%), and confusion (1%).20
The Chang et al. (2014) RCT21 compared 2 combinations of analgesics to one another: hydrocodone 5 mg and APAP 500 mg, as well as codeine 30 mg and APAP 300 mg. Authors reported no between-group differences (i.e., statistically non-significant) in the occurrence of AEs.21 Types of AEs in the hydrocodone group were nausea (10%), vomiting (2%), constipation (0%), diarrhea (0%), pruritus (3%), rash (1%), dizziness (14%), drowsiness (28%), and confusion (2%).21 Types of AEs in the codeine group were nausea (10%), vomiting (1%), constipation (0%), diarrhea (5%), pruritus (3%), rash (0%), dizziness (5%), drowsiness (29%), and confusion (1%).21
The Le May et al. (2013) RCT23 compared 2 combinations of pediatrically formulated analgesics to one another: codeine 1 mg/kg and ibuprofen 10 mg/kg, as well as a placebo and ibuprofen 10 mg/kg. Authors reported 1 side effect (nausea) in the codeine and ibuprofen group and zero in the and ibuprofen group.23 Furthermore, they reported zero AEs for either group.23
The Buccelletti et al. (2014) non-randomized study24 compared ketorolac 15 mg with the combination of APAP 1,000 mg and codeine 60 mg. Authors reported zero AEs for either group.24
Limitations
A number of limitations were identified in the critical appraisal as shown in Appendix 3; however, additional limitations exist. The main limitations of this report are related to the limited amount of evidence identified for the drug and population of interest, the heterogeneity of the interventional drug combinations, and the limited follow-up periods.
Although evidence was found for codeine combination drugs, no comparative evidence was identified regarding the use of codeine as a single ingredient. Therefore, the therapeutic appropriateness and safety of codeine, as a single ingredient, for acute extremities pain remains unanswered from this body of literature.
In addition, despite being generally well conducted, 1 SR17 did not contain any relevant literature, whereas the other SR18 yielded 1 relevant primary study with limited results reported.
Heterogeneity regarding differences in treatment was apparent in the codeine combination interventions of the primary study included in the SR,18 and among the RCTs19-23 and the non-randomized study24 included in this report (e.g., codeine 30 mg and APAP 300 mg; APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg; codeine 1 mg/kg and ibuprofen 10 mg/kg; APAP 1,000 mg and codeine 60 mg). Furthermore, many of the studies did not have an equivalent dose of APAP in the comparator groups (e.g., 300 mg, 325 mg, 500 mg, 1,000 mg). The additional dose of APAP introduces uncertainly which may have impacted the overall findings among all groups. Furthermore, the primary study included in the SR,18 3 of the RCTs,19-21 and the non-randomized study24 did not have a placebo arm; therefore, it is not possible to know how much of the pain reduction is unrelated to the codeine administered.
Heterogeneity was also apparent regarding the populations, in which 1 RCT23 was conducted in children and 2 RCTs20,21 had primarily Hispanic and African American participants; therefore, the results of these studies may not generalize to other populations.
An additional source of variability was the follow-up period (minutes to hours) of the primary study included in the SR,18 and among the RCTs19-23 and the non-randomized study24 included in this report. Although codeine analgesic effects present rapidly in individuals with normal metabolic activity, this may not have been long enough to detect longer-term outcomes (e.g., constipation, risk of falls); therefore, the safety results need to be interpreted with caution. In addition, although RCTs are a robust study design for establishing the safety and efficacy of pharmaceuticals, they generally exclude considerable portions of the potentially treatable population, thus limiting the generalizability of their findings.
None of the studies investigated patient’s CYP2D6 phenotype. The Clinical Pharmacogenetics Implementation Consortium has demonstrated that 8% to 23% of the population have a phenotype that metabolizes codeine at an “increased” (1% to 2%), “reduced” (2% to 11%), or “low or no” (5% to 10%) activity level.25 Individuals with low or no CYP2D6 activity will experience poor analgesia from codeine, whereas those with increased CYP2D6 activity will experience exaggerated effects.25,26 Phenotypes also vary by ethnic group. As an example, although the prevalence of increased enzyme activity is 1% to 2% in the general population,25 it has been estimated to be 1% in Asians,27 0.5% to 1% in Hispanics,28 5% to 10% in Caucasians,27 3% in African Americans,28 and 16% to 28% in North Africans, Ethiopians, and Arabs.28 Two RCTs20,21 were conducted at hospitals that attend to underserved minority populations (mostly Hispanic and African American); therefore, the results of these studies may not generalize to other populations.
Other potential clinical effectiveness outcomes (e.g., mobility) and safety outcomes (e.g., overdoses, liver toxicity, risks of falls, misuse) were not examined in this report due to a lack of relevant data. This gap would suggest the need for future research.
Conclusions and Implications for Decision or Policy-Making
This report identified clinical effectiveness evidence regarding the use of codeine or codeine with APAP and/or NSAIDs in patient with acute extremity pain. Two SRs,17,18 5 RCTs,19-23 and 1 non-randomized study24 were identified and included in this review.
The identified literature were heterogenous regarding the codeine combination drugs tested and length of follow-up. Although the overall results are inconclusive, all RCTs19-23 and the non-randomized study24 found no statistically significant differences in pain scores between codeine combination drugs and their respective comparators. One relevant publication was identified in the SR18 and found that the codeine combination drug was inferior to flurbiprofen at decreasing post-surgical foot and ankle pain between zero and 24 hours.18 However, there was no difference between 25 hours and 96 hours.18
Data on the use of rescue analgesia were inconclusive and conflicting. One RCT19 reported no statistically significant differences in the number of patients requiring rescue between the codeine combination drug group and the 3 comparator groups, whereas another RCT22 reported that 18.0%, 11.3%, and 3.4% of patients in the non-opioid, codeine, and oxycodone groups, respectively, required additional analgesia.
Data on patient satisfaction were also conflicting. Two RCTs20,21 reported no statistically significant differences in overall patient satisfaction between the codeine combination drug group and their respective comparators, whereas another RCT22 reported that 45 of 61 (73.8%), 47 of 62 (75.8%), and 39 of 59 (66.1%) patients in the non-opioid, codeine, and oxycodone groups, respectively, were satisfied with their initial analgesia.
Similarly, the identified literature were heterogenous and revealed mixed conclusions regarding AEs. Four studies18,20,21,24 found no differences between codeine combination drug groups and their respective comparators. One RCT22 reported 2, 1, and 10 AEs in the non-opioid (n = 61), codeine (n = 62), and oxycodone groups (n = 59), respectively, whereas another RCT23 reported 1 side effect in the codeine combination drug group compared to zero in the placebo combination group. Several studies garnered evidence from a single dose of the intervention and with limited time for observation of AEs; therefore, the safety profile needs to be interpreted with caution.
None of the studies investigated patient’s CYP2D6 isoenzyme phenotype, an important confounder that affects drug effectiveness and safety.
The limitations of the included studies, especially heterogeneity (e.g., drug combinations tested, follow-up period), should be considered when interpreting the results. Although some results highlighted in this review indicate that codeine is noninferior to many comparators, these findings come with a high degree of uncertainty. The lack of homogeneity and consensus in the identified literature suggests that more comparative studies are required in patients with acute extremity pain.
References
1.Bailey B. Chapter 14: acute pain. In: Jovaisas B, ed. Compendium of therapeutic choices. Fifth ed. Ottawa (ON): Canadian Pharmacists Association; 2007:198-208.
2.Baumann TJ, Strickland J. Chapter 62: pain management. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: a pathophysiologic approach. Seventh ed. New York (NY): McGraw-Hill Education; 2008:989-1004.
3.Morin KA, Eibl JK, Franklyn AM, Marsh DC. The opioid crisis: past, present and future policy climate in Ontario, Canada. Subst Abuse Treat Prev Policy. 2017;12(1):45. Medline
4.Kyriacou DN. Opioid vs nonopioid acute pain management in the emergency department. JAMA. 2017;318(17):1655-1656. Medline
5.Sweetman SC, ed Martindale: The complete drug reference. London, UK: Pharmaceutical Press; 2011.
6.United States Pharmacopeia Dispensing Information. Drug information for the health care professional. Vol 1. Montvale (NJ): Thomson Healthcare, Micromedex,; 2005.
7.Ćelić I, Bach-Rojecky L, Merćep I, Soldo A, Petrak AK, Bučan A. Resolving issues about efficacy and safety of low-dose codeine in combination analgesic drugs: a systematic review. Pain Therap. 2020;9(1):171-194. Medline
8.Li Y, Argáez C. Codeine for pain related to osteoarthritis of the knee and hip: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2020 Dec: https://cadth.ca/sites/default/files/pdf/htis/2020/RC1323%20Codeine%20for%20Osteoarthritis%20Pain%20Final.pdf. Accessed 2021 Jan 03.
9.Canadian Agency for Drugs and Technologies in Health. Codeine for acute dental pain and pain related to dental procedures: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2021 (in progress).
10.Canadian Agency for Drugs and Technologies in Health. Codeine for pain related to caesarean section: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2021 (in progress).
11.Li KX, Ford C. Codeine for pediatric patients with acute pain: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Nov: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1200%20Codeine%20for%20Pediatric%20Patients%20Final.pdf. Accessed 2021 Jan 03.
12.Marchand DK, Ford C. Codeine for acute pain for urological or general surgery patients: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Nov: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1201%20Codeine%20for%20Urological%20Pts%20Final.pdf. Accessed 2021 Jan 03.
13.Marchand DK, McCormack S. Codeine for acute pain in patients undergoing orthopedic surgery: a review of clinical effectiveness. (CADTH rapid response reports: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Oct: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1199%20Codeine%20for%20Orthopaedic%20Pts%20Final.pdf. Accessed 2021 Jan 03.
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
17.Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L. Non-prescription (OTC) oral analgesics for acute pain - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;11. Medline
18.Wang J, Liu GT, Mayo HG, Joshi GP. Pain management for elective foot and ankle surgery: a systematic review of randomized controlled trials. J Foot Ankle Surg. 2015;54(4):625-635. Medline
19.Chang AK, Bijur PE, Esses D, Barnaby DP, Baer J. Effect of a single dose of oral opioid and nonopioid analgesics on acute extremity pain in the emergency department: a randomized clinical trial. JAMA. 2017;318(17):1661-1667. Medline
20.Chang AK, Bijur PE, Lupow JB, Gallagher EJ. Comparative analgesic efficacy of oxycodone/acetaminophen vs codeine/acetaminophen for short-term pain management following ED discharge. Pain Med. 2015;16(12):2397-2404. Medline
21.Chang AK, Bijur PE, Munjal KG, John Gallagher E. Randomized clinical trial of hydrocodone/acetaminophen versus codeine/acetaminophen in the treatment of acute extremity pain after emergency department discharge. Acad Emerg Med. 2014;21(3):227-235. Medline
22.Graudins A, Meek R, Parkinson J, Egerton-Warburton D, Meyer A. A randomised controlled trial of paracetamol and ibuprofen with or without codeine or oxycodone as initial analgesia for adults with moderate pain from limb injury. EMA - Emergency Medicine Australasia. 2016;28(6):666-672. Medline
23.Le May S, Gouin S, Fortin C, Messier A, Robert MA, Julien M. Efficacy of an ibuprofen/codeine combination for pain management in children presenting to the emergency department with a limb injury: a pilot study. J Emerg Med. 2013;44(2):536-542. Medline
24.Buccelletti F, Marsiliani D, Zuccala G, et al. Paracetamol-codeine compared to ketorolac for pain control in the Emergency Department. Eur Rev Med Pharmacol Sci. 2014;18(20):3139-3143. Medline
25.Dean L. Dean L. Codeine Therapy and CYP2D6 Genotype. 2012 Sep 20 [Updated 2017 Mar 16]. In: Pratt VM, Scott SA, Pirmohamed M, et al., editors. Medical Genetics Summaries [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2012-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK100662/. Accessed 2021 Jan 04.
26.Kirchheiner J, Schmidt H, Tzvetkov M, et al. Pharmacokinetics of codeine and its metabolite morphine in ultra-rapid metabolizers due to CYP2D6 duplication. Pharmacogenomics J. 2007;7(4):257-265. Medline
27.Purdue Pharma. Codeine Contin: codeine monohydrate – codeine sulfate trihydrate. In: Repchinsky C, ed. Compendium of Pharmaceutical and Specialties. Ottawa (ON): Canadian Pharmacists Association; 2013:681-682.
28.Roxane Laboratories. Codeine sulfate tablets for oral use (package insert). Columbus (OH): Roxane Laboratories; 2010: https://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=fa3ed180-298a-4f9d-9d05-15182d7218bf Accessed 2021 Jan 04.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Systematic review of SRs | ||||
Moore et al. (2015)17 UK Funding source: National Institute for Health Research | Study design: Systematic review of relevant Cochrane SRs of RCTs Number of studies included: 10 Cochrane SRs were identified; however, none were relevant to this report | Adults (15 years or older) with acute post-operative pain | Intervention: Variety of analgesics available without prescription in the UK Comparator: PBO | Outcomes:
Follow-up: 4 to 6 hours, or more |
Systematic review | ||||
Wang et al. (2015)18 US Funding source: NR | Study design: Systematic review of relevant SRs, MAs, literature reviews, RCTs, and trials. Number of studies included: 45 RCTs were identified; 1 was relevant to this report | Adult patients with foot and ankle surgery pain managed by analgesics | Intervention: Variety of pharmacological interventions (e.g., opioids, gabapentin, NSAIDs, ketamine, APAP, corticosteroids) Comparator: Above drugs compared to one another, a control group, or none | Outcomes:
Follow-up: NR |
AE = adverse event; APAP = N-acetyl-para-aminophenol (i.e., acetaminophen, paracetamol); NSAID = nonsteroidal anti-inflammatory drug; MA = meta-analysis; NR = not reported; PBO = placebo; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
RCTs | ||||
Chang et al. (2017)19 US Funding source: National Institute on Aging, National Institutes of Health | Study design: Randomized, in blocks of 8, double-blind clinical trial (NCT02455518) conducted at 2 urban EDs from July 2015 to August 2016 | Adult patients with moderate to severe acute extremity pain Number of patients: 416 (104 per intervention group) Mean age, years:
Sex, female:
| Interventions:
Comparator: 1 combination vs. another | Outcomes: Between-group difference in pain intensity, using an 11-point NRS Follow-up: 2 hours after ingestion |
Graudins et al. (2016)22 Australia Funding source: NR | Study design: Randomized, in blocks of 18, double-blind clinical trial (ACTRN12610000588099) conducted at 3 urban EDs from October 2010 to October 2013 | Adults, aged 18 to 75 years, with acute moderate pain (VAS score 4 to 7) from limb injury (e.g., upper or lower limb sprain, fracture, crush, or skin wound), but excluding digital injuries Number of patients: 185 (non-opioid: n = 61; COD: n = 62; OCOD: n = 59) Mean age, years:
Sex, female:
| Interventions:
Comparator: 1 combination vs. another | Outcomes:
Follow-up: 90 minutes |
Chang et al. (2015)20 US Funding source: NR | Study design: Prospective, randomized, double-blind clinical trial (NCT01402375) at 1 urban ED from May 2013 to January 2014 | Adults, 21 to 64 years, with acute musculoskeletal extremity pain Number of patients: 240 (120 per group) Mean age, years:
Sex, female:
| Intervention: OCOD 5 mg and APAP 325 mg every 4 hours as needed, for 3 days Comparator: COD 30 mg and APAP 300 mg every 4 hours as needed, for 3 days | Outcomes:
Follow-up: 1 day following ED discharge |
Chang et al. (2014)21 US Funding source: NR | Study design: Prospective, randomized, double-blind clinical trial (NCT01402375) at 1 urban ED from January 2012 to August 2012 | Adults, 21 to 64 years, with acute musculoskeletal extremity pain Number of patients: 240 (120 per group) Mean age, years:
Sex, female:
| Intervention: HCOD 5 mg and APAP 300 mg every 4 hours, as needed, for 3 days Comparator: COD 30 mg and APAP 300 mg every 4 hours, as needed, for 3 days | Outcomes:
Follow-up: 1 day following ED discharge |
Le May et al. (2013)23 Canada Funding source:
| Study design: Randomized, in blocks of 6, double-blind, placebo-controlled clinical trial at 1 urban ED from February 2008 to November 2009 (limited to weekdays between 10:00 a.m. and 4:00 p.m.) | Children, 7 years to 18 years, with acute pain due to a musculoskeletal injury to a limb Number of patients: 83 (COD: n = 42; PBO: n = 41) Mean age, years:
Sex, female:
| Intervention: COD suspension 1 mg/kg (maximum 60 mg) and IBP chew tablets 10 mg/kg (maximum 600 mg) Comparator: PBO suspension and IBP chew tablets 10 mg/kg (maximum 600 mg) | Outcomes:
Follow-up: 120 minutes |
Non-randomized studies | ||||
Buccelletti et al. (2014)24 Italy Funding source: NR | Study design: Prospective cohort study in a single tertiary care ED, lasting 5 months | Adults, older than 18 years, with pain to an extremity due to localized trauma or inflammation Number of patients: 200 (COD: n = 87, KET: n = 113) Age range, years:
Sex, female:
| Intervention: KET 15 mg Comparator: APAP 1,000 mg and COD 60 mg | Outcomes: NRS pain level Follow-up: 2 hours |
ACTRN = Australian and New Zealand Clinical Trials Registry; AE = adverse event; APAP = N-acetyl-para-aminophenol (i.e., acetaminophen, paracetamol); COD = codeine; ED = emergency department; HCOD = hydrocodone; IBP = ibuprofen; IQR = interquartile range; KET = ketorolac; NA = not applicable; NCT = National Clinical Trial; NR = not reported; NRS = numerical rating scale; OCOD = oxycodone; PBO: placebo; SD = standard deviation; SE = side effect; THI = thiamine (i.e., vitamin B1); VAS = visual analogue scale.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 214
Strengths | Limitations |
Moore et al. (2015)17 | |
|
|
Wang et al. (2015)18 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; RCT = randomized controlled trial; SR = systematic review.
Table 5: Strengths and Limitations of RCT Clinical Studies Using the Downs and Black Checklist15
Strengths | Limitations |
Chang et al. (2017)19 | |
|
|
Graudins et al. (2016)22 | |
|
|
Chang et al. (2015)20 | |
|
|
Chang et al. (2014)21 | |
|
|
Le May et al. (2013)23 | |
|
|
AE = adverse event; ITT = intention to treat; NR = not reported; NRS = numerical rating scale; VAS.
Table 6: Strengths and Limitations of Non-Randomized Clinical Studies Using the Downs and Black Checklist15
Strengths | Limitations |
Buccelletti et al. (2014)24 | |
|
|
AE = adverse event; NRS = numerical rating scale.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Systematic Review
Wang et al. (2015)18
Main Study Findings
1 primary RCT from 1997 reported on post-operative flurbiprofen 50 mg (n = 29) versus APAP 300 mg and codeine 30 mg (n = 24) every 4 to 6 hours for 96 hours.
Pain scores:
Zero to 24 hours: Decreased pain score (absolute values not reported) in the flurbiprofen group (P < 0.01)
25 to 96 hours: Not significant (statistical data not reported)
AEs: Not significant (statistical data not reported)
Authors’ Conclusion
Not reported for this SR
Summary of Findings of Included Primary Clinical Studies: RCTs
Chang et al. (2017)19
Main Study Findings
Decrease in mean NRS pain score at 2 hours:
Ibuprofen 400 mg and APAP 1,000 mg: 4.3 (95% CI, 3.6 to 4.9)
Oxycodone 5 mg and APAP 325 mg: 4.4 (95% CI, 3.7 to 5.0)
Hydrocodone 5 mg and APAP 300 mg: 3.5 (95% CI, 2.9 to 4.2)
Codeine 30 mg and APAP 300 mg: 3.9 (95% CI, 3.2 to 4.5)
There was no difference in change in pain by treatment group from baseline to 2 hours (P = 0.053)
Decrease in mean NRS pain score at 1 hour:
Ibuprofen 400 mg and APAP 1,000 mg: 2.9 (95% CI, 2.4 to 3.5)
Oxycodone 5 mg and APAP 325 mg: 3.1 (95% CI, 2.6 to 3.7)
Hydrocodone 5 mg and APAP 300 mg: 2.4 (95% CI, 1.8 to 3.0)
Codeine 30 mg and APAP 300 mg: 2.7 (95% CI, 2.1 to 3.3)
There was no difference in change in pain by treatment group at 1 hour (P = 0.13)
Between-group difference in mean change in NRS pain score at 1 hour:
Ibuprofen 400 mg and APAP 1,000 mg versus codeine 30 mg and APAP 300 mg: 0.2 (99.2% CI, –0.6 to 1.0)
Oxycodone 5 mg and APAP 325 mg versus codeine 30 mg and APAP 300 mg: 0.4 (99.2% CI, –0.4 to 1.2)
Hydrocodone 5 mg and APAP 300 mg versus codeine 30 mg and APAP 300 mg: –0.3 (99.2% CI, –1.1 to 0.5)
No significant differences (statistical data not reported)
Between-group difference in mean change in NRS pain score at 2 hours:
Ibuprofen 400 mg and APAP 1,000 mg versus codeine 30 mg and APAP 300 mg: 0.4 (99.2% CI, –0.6 to 1.3)
Oxycodone 5 mg and APAP 325 mg versus codeine 30 mg and APAP 300 mg: 0.5 (99.2% CI, –0.4 to 1.4)
Hydrocodone 5 mg and APAP 300 mg versus codeine 30 mg and APAP 300 mg: –0.3 (99.2% CI, –1.3 to 0.6)
No significant differences (statistical data not reported)
Number of patients requiring rescue analgesic within 2 hours:
Ibuprofen 400 mg and APAP 1,000 mg (n = 101): 18 (17.8%)
Oxycodone 5 mg and APAP 325 mg (n = 104): 14 (13.5%)
Hydrocodone 5 mg and APAP 300 mg (n = 103): 18 (17.5%)
Codeine 30 mg and APAP 300 mg (n = 103): 23 (22.3%)
There was no difference in the distribution of rescue analgesia (P = 0.42)
Dose of rescue analgesia, in morphine equivalent units:
Ibuprofen 400 mg and APAP 1,000 mg: 1.6 (SD = 3.5)
Oxycodone 5 mg and APAP 325 mg: 1.1 (SD = 2.7)
Hydrocodone 5 mg and APAP 300 mg: 1.7 (SD = 3.2)
Codeine 30 mg and APAP 300 mg: 2.0 (SD = 3.4)
There was no difference in the dose of rescue analgesia, in morphine equivalent units (P = 0.27)
Decrease, at 2 hours, in the mean NRS pain score of a subset of patients with baseline NRS = 10 or a documented fracture:
Ibuprofen 400 mg and APAP 1,000 mg (n = 52): 4.4 (95% CI, 3.6 to 5.1)
Oxycodone 5 mg and APAP 325 mg (n = 48): 4.5 (95% CI, 3.7 to 5.3)
Hydrocodone 5 mg and APAP 300 mg (n = 50): 3.9 (95% CI, 3.1 to 4.6)
Codeine 30 mg and APAP 300 mg (n = 49): 4.1 (95% CI, 3.3 to 4.9)
There was no difference in change in pain by treatment group from baseline to 2 hours (P = 0.69)
Authors’ Conclusion
“For patients presenting to the ED with acute extremity pain, there were no statistically significant or clinically important differences in pain reduction at 2 hours among single-dose treatment with [ibuprofen] and [APAP] or with 3 different opioid and [APAP] combination analgesics (p. 12).”19
Graudins et al. (2016)22
Main Study Findings
Intervention groups:
Non-opioid group: APAP 1,000 mg, ibuprofen 400 mg, and thiamine 100 mg
Codeine group: APAP 1,000 mg, ibuprofen 400 mg, and codeine 60 mg
Oxycodone group: APAP 1,000 mg, ibuprofen 400 mg, and oxycodone 10 mg
Mean decrease in VAS, at 30 minutes:
Non-opioid group, n = 61: –13.5 mm
Codeine group, n = 62: –16.1 mm
Oxycodone group, n = 59: –16.2 mm
Difference in mean change in VAS, at 30 minutes:
Non-opioid group versus codeine group: –2.6 (95% CI, –8.8 to 3.6)
Non-opioid group versus oxycodone group: –2.7 95% CI, (–9.3 to 3.9)
Codeine group versus oxycodone group: 0.1 (95% CI, –6.6 to 6.4)
Mean decrease in VAS, at 60 minutes:
Non-opioid group, n = 49 of 61: –23.2 mm
Codeine group, n = 49 of 62: –30.7 mm
Oxycodone group, n = 47 of 59: –26.1 mm
Mean decrease in VAS, at 90 minutes:
Non-opioid group, n = 32 of 61: –18.7 mm
Codeine group, n = 30 of 62: –33.3 mm
Oxycodone group, n = 32 of 59: –31.7 mm
Number of patients who reported satisfaction with initial analgesia:
Non-opioid group: n = 45
Codeine group: n = 47
Oxycodone group: n = 39
Number of patients requiring additional analgesia within 90 minutes:
Non-opioid group: n = 11 of 61 (18.0%)
Codeine group: n = 7 of 62 (11.3%)
Oxycodone group: n = 2 of 59 (3.4%)
Number of patients reporting AEs, within 90 minutes; type:
Non-opioid group: n = 2 of 61 (3.3%); heartburn, light-headedness
Codeine group: n = 1 of 62 (1.6%); not specified
Oxycodone group: n = 10 of 59 (16.9%); light-headedness (n = 4), light-headedness and nausea (n = 4), nausea (n = 2), drowsiness (n = 1)
Authors’ Conclusion
“[…] the present study found that the non-opioid, [codeine] and [oxycodone] groups were all noninferior, at the primary outcome time of 30 min. This supports the initial use of a non-opioid combination for moderate pain from limb injury (p. 672).”22
Chang et al. (2015)20
Main Study Findings
Mean change in NRS score 2 hours after the most recent dose:
Oxycodone 5 mg and APAP 325 mg, n = 111: 4.5 (SD = 2.4)
Codeine 30 mg and APAP 300 mg, n = 104: 4.2 (SD = 2.4)
There was no significant difference (95% CI, –0.4 to 0.9)
Percentage of patients experiencing a 50% or greater decrease in pain score:
Oxycodone 5 mg and APAP 325 mg: 66%
Codeine 30 mg and APAP 300 mg: 61%
There was no significant difference (95% CI, –8% to 17%)
Percentage of patients who were satisfied overall with the analgesic received:
Oxycodone 5 mg and APAP 325 mg: 89%
Codeine 30 mg and APAP 300 mg: 88%
There was no significant difference (95% CI, –8% to 10%)
Percentage of patients who would want the same analgesic, should they experience a similar degree of pain in the future:
Oxycodone 5 mg and APAP 325 mg: 83%
Codeine 30 mg and APAP 300 mg: 82%
There was no significant difference (95% CI, –10% to 12%)
AEs:
Oxycodone 5 mg and APAP 325 mg, n = 111: nausea (12%), vomiting (4%), constipation (0%), diarrhea (1%), pruritus (5%), rash (2%), dizziness (10%), drowsiness (28%), and confusion (1%)
Codeine 30 mg and APAP 300 mg, n = 104: nausea (12%), vomiting (2%), constipation (0%), diarrhea (3%), pruritus (4%), rash (3%), dizziness (13%), drowsiness (22%), and confusion (1%)
There were no significant between-group differences with any of the AEs
Authors’ Conclusion
“[…] our hypothesis that [oxycodone]/[APAP] (5 mg/325 mg) would provide analgesia superior to [codeine]/[APAP] (30 mg/300 mg) was rejected. Although pain within each group was reduced by more than half over a 2-hour period, the between-group difference in analgesic effect was neither clinically nor statistically significant. Side effects and patient satisfaction were also similar (p. 2403).”20
Chang et al. (2014)21
Main Study Findings
Mean change in NRS score 2 hours after the most recent dose:
Hydrocodone 5 mg and APAP 500 mg (n = 88): 3.9 (SD = 2.5)
Codeine 30 mg and APAP 300 mg (n = 93): 3.5 (SD = 2.6)
There was no significant difference (95% CI, –0.3 to 1.2)
Percentage of patients experiencing a 50% or greater decrease in pain score: Reported as having no significant difference between groups (statistical data not reported)
Percentage of patients who were satisfied overall with the analgesic received:
Hydrocodone 5 mg and APAP 500 mg: 83%
Codeine 30 mg and APAP 300 mg: 71%
There was no significant difference (95% CI, –0.7 to 24)
Percentage of patients who would want the same analgesic, should they experience a similar degree of pain in the future:
Hydrocodone 5 mg and APAP 500 mg: 69%
Codeine 30 mg and APAP 300 mg: 71%
There was no significant difference (95% CI, –15 to 12)
AEs:
Hydrocodone 5 mg and APAP 500 mg: nausea (10%), vomiting (2%), constipation (0%), diarrhea (0%), pruritus (3%), rash (1%), dizziness (14%), drowsiness (28%), and confusion (2%)
Codeine 30 mg and APAP 300 mg: nausea (10%), vomiting (1%), constipation (0%), diarrhea (5%), pruritus (3%), rash (0%), dizziness (5%), drowsiness (29%), and confusion (1%)
There were no significant between-group differences with any of the AEs
Authors’ Conclusion
“[…]we found that [hydrocodone]/[APAP] [(5 mg/500 mg)] did not provide clinically or statistically superior outpatient pain relief compared to [codeine]/[APAP] [(30 mg/300 mg)], when assessed at 24 hours following discharge from the ED in patients presenting with acute extremity pain. Similarly, there were no clinically or statistically important differences in side-effect profiles or patient satisfaction (p. 234).”21
Le May et al. (2013)23
Main Study Findings
Mean difference in pain scores between codeine and ibuprofen versus placebo and ibuprofen groups at 3 time points:
60 minutes: 0.2 (95% CI, –0.8 to 1.2; P = 0.99)
90 minutes: –0.1 (95% CI, –1.3 to 1.0; P = 0.55)
120 minutes: –0.3 (95% CI, –1.7 to 1.1; P = 0.60)
There were no significant between-group differences
Side effects:
Codeine 1 mg/kg and ibuprofen 10 mg/kg: nausea (n = 1)
Placebo and ibuprofen 10 mg/kg: zero
AEs: Zero reported for both groups
Authors’ Conclusion
“The addition of [codeine] to [ibuprofen] did not significantly improve pain management of children with a musculoskeletal trauma. Pain control provided by the medications remained suboptimal for most patients (p. 540).”23
Summary of Findings of Included Primary Clinical Studies: Non-Randomized Study
Buccelletti et al. (2014)24
Main Study Findings
Reduction in NRS pain score between ketorolac 15 mg versus APAP 1,000 mg and codeine 60 mg at 30 minutes: No difference (statistical data not reported)
Analgesic effect between ketorolac 15 mg versus APAP 1,000 mg and codeine 60 mg in non-traumatic pain at 2 time points:
30 minutes: no significant difference (P = 0.908)
120 minutes: no significant difference (P = 0.635)
Analgesic effect between ketorolac 15 mg versus APAP 1,000 mg and codeine 60 mg in traumatic pain at 2 time points:
30 minutes: no significant difference (P = 0.770)
120 minutes: no significant difference (P = 0.482)
Analgesic efficacy of APAP and codeine versus ketorolac based on anatomic source of pain at 120 minutes:
Fractures: APAP 1,000 mg and codeine 60 mg exerted higher analgesic activity compared to ketorolac 15 mg (P = 0.030)
Muscular: APAP 1,000 mg and codeine 60 mg exerted significantly higher analgesic activity compared to ketorolac 15 mg (P = 0.044)
Analgesic efficacy of APAP and codeine versus ketorolac for acute pain overall, at 120 minutes, and based on anatomic source:
Overall: APAP 1,000 mg and codeine 60 mg exerted higher analgesic activity compared to ketorolac 15 mg in acute pain (P = 0.002)
2 hours: APAP 1,000 mg and codeine 60 mg exerted higher analgesic activity compared to ketorolac 15 mg in acute pain (Note: the P value reported by authors [P = 0.029] was for results at 30 minutes versus 2 hours)
Anatomic source: APAP 1,000 mg and codeine 60 mg exerted higher analgesic activity compared to ketorolac 15 mg in acute pain, originating from any anatomic site except the arms (P = 0.03)
Side effects: Zero reported for both groups
Authors’ Conclusion
“Those results clearly show that the combination [APAP/codeine] is a good alternative to [ketorolac] in most of the settings analyzed by this study (p. 3142).”24
Appendix 5: Overlap Between Included Systematic Reviews
Table 7: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Moore et al. (2015)17 | Wang et al. (2015)18 |
Soulier SM, et al. J Foot Ankle Surg. 1997;36(6):414-17. | X |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca