CADTH Health Technology Review
Codeine for Acute Dental Pain and Acute Pain Related to Dental Procedures
Rapid Review
Authors: Sara D. Khangura, Charlene Argáez
Abbreviations
AE
adverse event(s)
AMSTAR
A MeaSurement Tool to Assess systematic Reviews
CI
confidence interval
NNH
number needed to harm
NNT
number needed to treat
NSAID
nonsteroidal anti-inflammatory drug
PID
pain intensity difference
RCT
randomized controlled trial
SD
standard deviation
SPID
sum of pain intensity difference
SPID6
sum of pain intensity at 6 hours
SR
systematic review
TOTPAR
total pain relief
VAS
visual analogue scale
Key Messages
Two overviews of systematic reviews, 4 systematic reviews, and 9 randomized controlled trials were identified comparing codeine or codeine combination drugs with placebo and/or other drugs in the management of acute dental pain.
As compared to placebo, codeine was generally shown to offer a benefit to patients experiencing acute dental pain.
When compared to other drugs and/or drug combinations — particularly those that were acetaminophen- or ibuprofen-based — codeine generally was not found to be as clinically effective for the management of acute dental pain, with the potential exception of tooth sensitivity following dental bleaching, where 1 study reported that acetaminophen plus codeine was statistically significantly superior to ibuprofen or placebo.
Increased adverse events were observed with codeine-containing drugs as compared to other drugs and/or placebo.
Studies included in this review demonstrated both strengths and limitations, some of which limit the extent to which the findings from these studies were relevant to this report and/or can be generalized.
Context and Policy Issues
Acute dental pain and acute pain related to dental procedures is common, whether caused by a dental condition or following an invasive dental procedure.1 Acute dental pain can be debilitating and can cause anxiety about seeking dental treatment; consequently, the effective management of acute dental pain is a priority for dental professionals.2
There are multiple analgesic drugs used to treat acute dental pain, with a large body of literature describing their effects, as well as relative benefits and risks.3 In general, the literature divides analgesic drugs for the treatment of acute dental pain into 2 groups: opioids and non-opioids.4 With a variety of benefit/risk profiles to both opioid and non-opioid analgesics,5 the use of opioids in dentistry — including codeine — is a source of debate among experts, primarily because of the potential for misuse and other adverse effects.6,7
Codeine is a commonly used opioid analgesic in dentistry, which, like all opioids, has the potential for misuse.8 Codeine converts to morphine,9 which is primarily responsible for its analgesic effect.2 It is often used in combination with other analgesic drugs and has been described as a “weak opioid” — being acknowledged and classified accordingly by the WHO (p133).9 Studies have demonstrated that codeine is less clinically effective than other drugs for managing acute dental pain — in particular, nonsteroidal anti-inflammatory drugs (NSAIDs) and/or acetaminophen9,10 In addition, codeine can produce a variety of adverse reactions, including nausea, vomiting, dizziness, drowsiness, and other reactions, with the risk of an adverse reaction increasing alongside the dose of the medication.9 In particular, there are warnings against the use of codeine in pediatric populations, as well as breastfeeding women and the elderly, because of an increased risk in some individuals with the CYP2D6 polymorphism, who metabolize codeine more rapidly and in whom serious adverse events (AEs) have occurred.6,8,9
Nonetheless, it has been acknowledged that there remains a potential role for the use of codeine in the management of acute dental pain, probably in combination with other analgesics.5 There is also a possible pharmacoeconomic benefit; a recent economic analysis identified the addition of codeine to ibuprofen as offering a distinct advantage in the management of acute dental pain.11 Indeed, authors of another study of analgesic use among Canadian patients with dental pain described cost as a factor; codeine was characterized as being more affordable for patients as compared to more effective and expensive drugs such as acetaminophen and/or ibuprofen.12
Given the potential benefits and harms of codeine, a review of the literature will offer insight into its clinical effectiveness and provide an update to the evidence needed for decision-makers to consider the best use of codeine for the management of acute dental pain.
Research Questions
What is the clinical effectiveness of codeine for patients with acute dental pain or pain related to dental procedures?
What is the clinical effectiveness of codeine with acetaminophen and/or a nonsteroidal anti-inflammatory drug for patients with acute dental pain or pain related to dental procedures?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via OVID, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were codeine and dental pain. Filters were applied to limit retrieval to systematic reviews (SRs), health technology assessments, and meta-analyses, randomized clinical trials, and non-randomized studies. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2011 and January 4, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for eligibility. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients (any age) with acute dental pain or acute pain related to dental procedures |
Intervention | Q1: Codeine alone, administered orally Q2: Codeine with acetaminophen and/or a nonsteroidal anti-inflammatory drug (NSAID; e.g., acetylsalicylic acid, ibuprofen, naproxen) as single products or as combination drugs (e.g., codeine-acetaminophen-caffeine combination), administered orally |
Comparator | Other opioids (e.g., tramadol, oxycodone, morphine, hydromorphone, fentanyl), 1 or more non-opioid analgesics (e.g., acetaminophen, NSAID), other opioid combinations (e.g., oxycodone with acetaminophen), or placebo, administered orally |
Outcomes | Clinical effectiveness (e.g., pain control, pain scales, health-related quality of life), safety (e.g., overdose-related adverse events such as respiratory depression and liver toxicity, other adverse events such as constipation, dependence/addiction, hospitalizations) |
Study designs | HTAs, SRs, meta-analyses, RCTs, non-randomized studies |
HTA = health technology assessment; NSAID = nonsteroidal anti-inflammatory drug; Q = question; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2011. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Studies with no comparison group or with mixed indications that did not report data relevant for this review separately were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)13 for SRs, and the Downs and Black checklist14 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
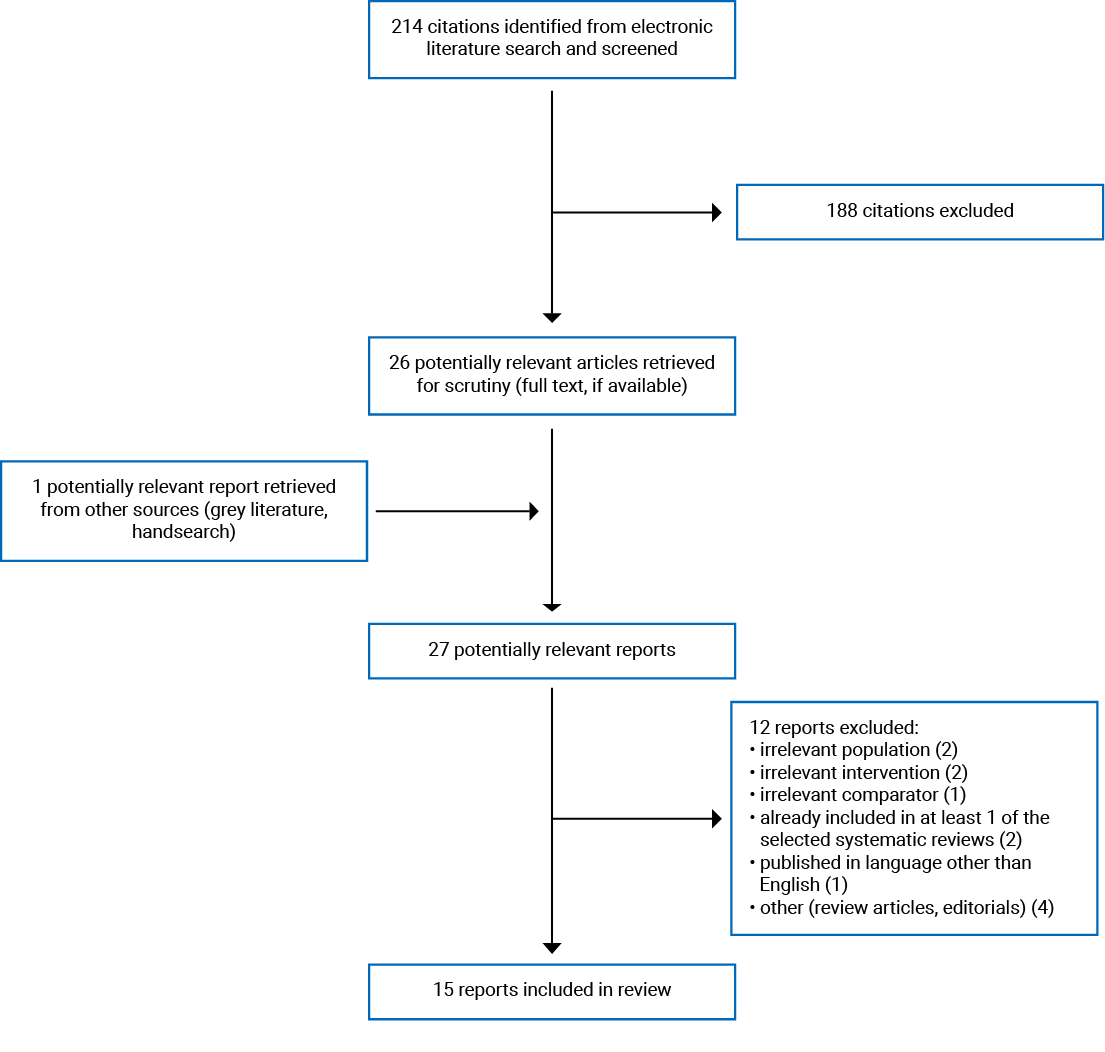
A total of 214 citations were identified in the literature search. Following the screening of titles and abstracts, 188 citations were excluded and 26 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 12 publications were excluded for various reasons and 15 publications met the eligibility criteria for inclusion in this report. These comprised 2 overviews of SRs, 4 SRs, and 9 randomized controlled trials (RCTs). The included overviews of SRs and the SRs were broader in scope than the research questions and selection criteria for the current review; thus, only the SRs and primary studies that could be ascertained as meeting the selection criteria for the present review are described in this report. One of the 9 RCT reports15 described 2 separate trials using similar methods and 2 of the RCT reports16,17 described data from 2 independent follow-up time periods for the same trial. Appendix 1 presents the PRISMA18 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Study Design
Two overviews of SRs published in 201119 and 201520 were identified. Both overviews sought Cochrane SRs only and either reported no detail as to the time frame or dates of the search20 or described a 15-year time frame for the search (start and end dates were not reported).19 One overview of SRs included 35 SRs19 (1 of which could be ascertained as eligible for inclusion in this report) and the other overview of SRs included 10 SRs20 (1 of which could be ascertained as eligible for inclusion in this report). There was no overlap across the 2 overviews in the 2 SRs eligible for this review.
Four SRs were included in the review,21-24 3 of which conducted meta-analyses.21,23,24 One of the SRs was published in 2019 and included 10 RCTs, 5 of which reported data eligible for this review.21 Another SR was also published in 2019 and included 3 RCTs, 1 of which reported data eligible for inclusion in the current review.22 A third SR was published in 2015, including 14 RCTs, 6 of which reported data eligible for this review.23 And lastly, 1 SR was published in 2013, including 119 RCTs, 3 of which reported data eligible for inclusion in this review.24 All of the included SRs limited their included primary studies to RCTs, only.21-24 One SR reported an assessment of methodological quality of included RCTs.21 There was no overlap in the primary studies containing data eligible for this review across the SRs included.
All15,25-30 but 116,17 of the RCTs were single-centre and double-blind. Five of the RCTs were 2-arm studies,25-28,30 2 were 3-arm,15,29 and 1 RCT described in 2 reports had 5 treatment groups.16,17 Several of the reports described a randomization procedure using computer-generated sequencing,15,16,25,28 while another RCT described the use of a random table of numbers27 and another, the use of a random draw system.29 Three of the RCTs did not provide details regarding the methods or procedures used to generate the random sequence.17,26,30 One of the RCTs28 described a split-mouth, crossover-type design. In this RCT, patients underwent 2 surgical procedures — 1 for each of 2 third molar extractions — and were randomly assigned to the intervention or control for preoperative treatment of pain in the first surgery. For the second surgery, the preoperative medication was changed to the other treatment arm, so that each patient experienced both the intervention and the placebo for 1 of each of the procedures.28
Country of Origin
Both overviews of SRs were led by co-authors from the UK,19,20 as was 1 of the SRs.24 Other SRs were led by investigators based in Australia,21 Hong Kong,23 as well as 1 led by co-authors from Italy, Saudi Arabia, and the US.22 Three RCTs were conducted in Brazil;25,27,29 1 each in Italy,28 New Zealand,26 and South Africa30; and 4 RCTs reported in 3 publications were carried out in the US.15-17
Patient Population
Most of the studies described patients with acute pain following a dental procedure.15-17,19-24,26,28-30 Both of the overviews of SRs19,20 and 1 SR21 described patients with post-operative pain more generally, including multiple types of surgical procedures (i.e., not only dental). Eleven studies15-17,19-21,23,24,26,28,30 described pain following third molar extraction, with the others describing acute abscess,25,27 acute pain following dental implant surgery,22 and acute dental sensitivity following a series of tooth-bleaching procedures.29
Interventions and Comparators
One study was identified describing an investigation into the use of codeine only for patients with acute dental pain or pain related to dental procedures (an overview of SRs describing the clinical effectiveness of multiple types of single dose oral analgesics),19 including 1 SR describing data comparing codeine (60 mg) with placebo in the treatment of dental pain.
All of the remaining 14 included studies in this review described investigation into the use of codeine in combination with other agents — most often with acetaminophen/paracetamol or 1 of several types of NSAID — sometimes with (an) additional agent(s). One overview of SRs investigated the clinical effectiveness of non-prescription, over-the-counter, oral medications.20 The overview included 1 SR relevant to this review and authors of the overview described 1 primary study from that SRs that met the eligibility criteria of the overview (a placebo-controlled trial of an over-the-counter ibuprofen and codeine product for post-operative pain in adults).20 All of the SRs described combination products with codeine,21-24 3 of which compared against placebo21,23,24 and 1 of which compared against another combination product.22 All 4 of the SRs included combinations of acetaminophen/paracetamol and codeine using various procedures for dosage and timing.21-24 Three of the SRs included studies investigating combinations of both acetaminophen + codeine, and ibuprofen + codeine; whereas 1 SR limited its investigation into a comparison of acetaminophen/codeine against acetaminophen/caffeine, without including any NSAID combinations.22 Two of the SRs included codeine combinations with acetylsalicylic acid.21,23 Other agents added to some of the codeine combinations included butalbital,23 doxylamine succinate,24 and caffeine.21,23,24
All 9 of the RCTs assessed combinations of acetaminophen/paracetamol and codeine,15-17,25-30 and 1 RCT investigated the use of an NSAID combined with codeine and acetaminophen.26 Several of the studies assessed codeine combinations as a comparator, rather than as the intervention of interest for the study,15-17,25 but these reports still included data of relevance eligible for this review. All but 128 of the RCTs compared codeine combinations against other active treatments.15-17,25-27,29,30 In addition to the 1 RCT that compared a codeine combination against placebo only, several other RCTs included placebo arms in their trials.15-17,28,29
Outcomes
Efficacy
Fourteen of the included studies provided data on efficacy outcomes15-17,19,21-30 and 10 of the included studies provided data on safety outcomes.15-17,21,23,25-28,30 The 1 study with no data reported on any outcomes was an overview of SRs that reported no reliable or eligible data of relevance to codeine in the treatment of acute dental pain.20
Efficacy outcomes reported include pain; pain severity and/or pain intensity;15,21-23,25-28,30 pain relief;15,19,23,24,30 the use of rescue medication or remedication;16,17,19,27,28 self-reported, perceived effectiveness of the study medication;16,17 and number needed to treat (NNT),19,31 defined in 1 SR as the number of patients that would need to be treated with the active medication to produce a benefit for 1 patient.24 Notably, pain was measured by the studies in this review using a variety of comparisons and measures across multiple time frames of follow-up. One study assessed dental sensitivity resulting from teeth bleaching procedures.29 Measures of efficacy outcomes included visual analogue scales (VAS) — for example, 0 to 10,22 1 to 10,29 or 0 to 10025,26,30 — and 4- and 5-point Likert pain scales15-17,30 and other continuous measures of pain — for example, 0 to 100.21 Several studies reported on the sum of pain intensity difference (SPID)15,23 and total pain relief (TOTPAR)15,17,23,24 by summing pain intensity and pain relief scores, respectively, across various time frames of the included studies and calculating mean values across treatment groups.
Of note, several studies also reported on outcomes not eligible for inclusion in this report; for instance, tooth whitening,29 or the association of an analgesic with patient anxiety.30 Because of their lack of relevance to clinical effectiveness for acute pain, these and other ineligible outcomes from otherwise eligible studies were not described in this report of findings.
Safety
Of the 9 studies in this review that reported on safety outcomes,15-17,21,23,25,27,28,30 all described AEs and/or experiences. Four studies reported on any AE,15-17,21 1 RCT reported on serious AEs,17 and 2 studies reported on treatment-emergent or drug-related AEs.17,21 Two studies reported AEs in a category described only as “Other.”25,27 In addition to reports of AEs, 2 studies reported on number needed to harm (NNH); both describing NNH with regard to the occurrence of any AE.25,27 Measures for safety outcomes were generally numbers of patients experiencing an AE and/or the number of occurrences of an AE.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Summary of Critical Appraisal
Overviews of Systematic Reviews and Systematic Reviews
The 2 overviews of SRs19,20 demonstrated several strengths, primarily because of they limited inclusion to Cochrane systematic reviews (which are known to be conducted using high methodological standards).32,33 Both overviews of SRs reported methods that were aligned with the Cochrane SR method, including clearly reported selection criteria, published protocols, dual eligibility screening and data abstraction, consideration of the implications of funding sources for included SRs on the findings of the overview, and consideration of heterogeneity and risk of bias on the findings. One limitation was a lack of elaboration concerning the rationale for limiting to Cochrane reviews only, and the potential implications this could have for their objectives; e.g., missing any relevant SRs that were not Cochrane reviews. In addition, search dates and time frames were not explicated in either overview.19,20 As well, there was a notable lack of information reported about SRs that were excluded; i.e., 1 overview did not report any information on excluded SRs19 and the other listed citations for the excluded SRs, but did not explain the reasons for excluding each SR,20 which leaves the reader unable to assess the rationale for the exclusion of each of the SRs.
While the AMSTAR13 assessments indicated that the 4 included SRs in this review were of low or critically low quality, their reports demonstrated both strengths and limitations.21-24 Whereas only 1 of the systematic reviews made mention of a protocol (although, it failed to include any details or reference to the document),23 all of the systematic reviews reported the use of 2 or more electronic databases to search for eligible studies and all included some description of support and/or funding for the review's conduct and/or publication.21-24 Most of the systematic reviews described the population, intervention, comparator, and outcome (PICO) components within the inclusion criteria21-23 and 2 of the systematic reviews described electronic search strategies that were run less than 24 months before the publication of the report, grey literature and handsearch methods, and an assessment of risk of bias.21,22 Dual screening and selection of sources was reported for 3 of the reviews.21-23 Other strengths included the application of dual data abstraction, a description of publication bias,21 and a detailed list of excluded primary studies.34
Limitations of the included SRs included no explicit description of an a priori method or clear and explicit reference to a protocol;21-24 no description of the methods used for data abstraction;22-24 no explicit reporting of funding sources for included primary studies,21-24 and no description of risk of bias assessments.23,24 Of the 2 SRs that reported an assessment of risk of bias, 1 conducted a GRADE assessment, indicating that the included RCTs (both those eligible and not eligible for this review) were generally of high quality, with a mean score of 7.7 (standard deviation [SD], 1.1) out of a possible 11 points using the PEDro risk of bias scale.21 The other SR tabulated the scores from their assessment using the study quality assessment tool of the NICE‒National Institute for Health and Care Excellence; i.e., the Quality Assessment of Controlled Intervention Studies tool.22 No overall assessment of the quality of the evidence was offered, but of the 14 criteria in the tool applied, the 1 RCT from which data eligible for this review were available met 13 of the requirements, suggesting that the risk of bias was not a significant concern for this study.22 These missing features make it difficult for the reader to assess the extent to which the findings are reliable and/or valid. Other important limitations included a lack of discussion around the potential impacts of heterogeneity and/or risk of bias on the findings of the reviews,21-24 which helps the reader to understand and interpret the applicability of the findings of the review.
Randomized Controlled Trials
The 9 RCTs included in this review demonstrated more strengths than limitations and were generally well-reported; notably, all made some reference to CONSORT35 in their reports,15-17,25-30 with 2 specifically indicating the use of CONSORT guidelines to inform the methods for their study.28,29 Several studies did not report (or did not consistently report) actual P values, reporting them categorically instead (e.g., P < 0.05).15-17,29 Other studies did not report on any AE experienced by patients during the study.26,28,29 Several studies included either limited data describing patient characteristics that could potentially confound study findings28,30 or no information describing patient characteristics.29 Other reporting deficits included interventions not being clearly described29 and some estimates of random variability missing.15 Clarity and completeness in reporting RCT data are critical for the reader to be able to assess the extent to which a study was conducted rigorously and whether the data are valid and reliable.
Components necessary to assess the external validity of the 9 RCTs were neither explicitly nor clearly reported in any of the study reports.15-17,25-30 Specifically, the extent to which those invited to participate, and those who agreed to participate, in the studies were representative of the source population from which they were selected was not clearly explicated.15-17,25-30 Establishing external validity is important to ensure that the findings from a study are generalizable, outside of the study context, to the broader population.
Indicators of internal validity were present in all of the included RCTs,15-17,25-30 with some studies reporting more detail and demonstrating more evidence of internal validity, and others reporting less detail. All of the studies reported randomizing patients and blinding them to the study interventions,15-17,25-30 while only 1 did not blind those measuring the outcomes to the study medications; i.e., single-blind design.30 There was no obvious data dredging for any of the studies and the statistical methods appeared appropriate, as reported.15-17,25-30 Other shortfalls in reporting features of internal validity across more than 1 of the RCTs included a lack of clarity concerning patient compliance with medication,15-17,27,28 a lack of clarity concerning whether patients from various treatment groups were recruited from the same population, and16,17,29 uncertainty as to whether confounding was accounted for in the analyses and/or interpretation of the study findings.15,27-29 Internal validity is necessary to establish confidence in the findings and to demonstrate that the findings are associated with the interventions under study as opposed to extraneous factors that may be affecting the study patients, interventions, and/or setting.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 tabulates and details the main study findings and authors’ conclusions.
Clinical Effectiveness of Codeine
Efficacy
Pain Relief
There was 1 study in this review that described the clinical effectiveness of codeine (60 mg) alone (i.e., not in combination with another agent) for the management of dental pain.19 The study was an overview of SRs that reported on efficacy using 50% maximum pain relief as the outcome of interest in comparing codeine (60 mg) to placebo for the treatment of dental pain.19 A limited amount of data specific to patients experiencing dental pain was reported, but did indicate that whereas 14% of patients receiving codeine (60 mg) achieved 50% maximum pain relief, 9% of placebo patients achieved this outcome; i.e., relative benefit 1.5 (95% confidence interval [CI], 1.1 to 2.1).
Number Needed to Treat
Authors of the overview highlighted the relatively high NNT using codeine (60 mg) was 21 (95% CI, 12 to 96) to achieve 50% maximum pain relief; i.e., 1 of the highest NNTs reported in the overview.19 Authors emphasized that this was considered to be a reliable result because of the large patient sample size from which the estimates were generated (i.e., N = 1,146).19
Remedication
Authors of the overview also reported that the mean time to remedication with codeine (60 mg) used as a single-drug intervention was less than 3 hours, which was 1 of the lowest (i.e., least beneficial) of the drugs assessed for treating dental pain in the overview.19
Clinical Effectiveness of Codeine With Acetaminophen and/or a Nonsteroidal Anti-inflammatory Drug
Efficacy
Pain, Pain Intensity and/or Pain Severity — Codeine Combination Drugs Versus Placebo
One SRs pooled data across RCTs describing the efficacy of a variety of codeine-containing combination drugs against placebo, using immediate and short-term follow-up — i.e., 3 hours, and 4 to 6 hours, respectively — following a single dose.21 In the immediate term, a statistically significant benefit was reported favouring the codeine combination drugs as compared to placebo; i.e., pooled data across 4 RCTs evaluating 211 patients demonstrated a mean difference between pain scores (measured using a 0 to 100 pain scale) of −12.7 (95% CI, −18.5 to −6.9).21 In the short-term, however, no statistically significant difference was found when investigators pooled data across 3 RCTs evaluating 155 patients; i.e., mean difference of −4.3 (95% CI, −11.6 to 3.0).21 This SR also described an RCT that compared various doses of paracetamol and codeine against placebo and found a clinically significant benefit in pain scores at 12 hours follow-up for the codeine-containing drugs; i.e., paracetamol (1,000 mg) and codeine (60 mg) versus placebo, −31.0 (95% CI, −39.1 to −22.9) and paracetamol (500 mg) and codeine (30 mg) versus placebo, −16.0 (−24.1 to −7.9).21
Another SR investigated multiple combination analgesics compared with placebo for post-operative dental pain in patients following third molar extraction — many of which contained codeine.23 Authors calculated the adjusted SPID at 6 hours for all of the included studies, where higher scores represented superiority of the analgesic effect.23 Pain intensity in codeine-containing combinations, as characterized by calculating the mean across adjusted SPID at 6 hours (SPID6) scores, ranged from 0.86 for 1 study of acetaminophen (1 g) and codeine phosphate (30 mg) versus placebo to 3.64 for 3 studies investigating acetaminophen (600 mg) and codeine phosphate (60 mg) versus placebo.23
One recently-published series of 2 RCTs characterized pain severity in 228 and 230 patients, respectively, following third molar extraction(s) using the SPID at 4, 6, and 8 hours, as well as measuring peak pain intensity difference (PID), to compare acetaminophen (600 mg) and codeine phosphate (60 mg) versus placebo.15 In both trials, the authors reported the statistically significant superiority of acetaminophen (600 mg) and codeine phosphate (60 mg) against placebo at 4, 6, and 8 hours, as well as a statistically significant benefit in peak PID.15
Another RCT compared preoperative treatment with a single dose of paracetamol (500 mg) and codeine (30 mg) versus placebo in 32 patients preparing to undergo 2 procedures for third molar extraction.28 Patients were randomized to 1 of the 2 interventions for the first procedure and were switched to the other intervention for the second procedure, with follow-up occurring for 3 days post-surgery.28 A statistically significant difference favouring paracetamol (500 mg) and codeine (30 mg) was found between the groups on day 1 of follow-up (P = 0.001), but not on days 2 and 3 of follow-up.28 Study investigators also reported a statistically significant difference in the time to first use of analgesic medication following the surgery (P = 0.004), with patients in the paracetamol (500 mg) and codeine (30 mg) group taking their first post-operative dose of analgesia at 414.33 minutes (SD, 131.26) and placebo patients at 288.67 minutes (SD, 116.63).
One RCT reported across 2 papers was conducted in 588 patients with acute dental pain following the extraction of third molars.16,17 Study patients were randomized to 1 of 5 arms, receiving either a once-daily dose of etoricoxib (120 mg or 90 mg), ibuprofen (600 mg) every 6 hours, acetaminophen (600 mg) and codeine (60 mg) every 6 hours, or placebo. The daily recall of average pain measure on days 2 and 3 indicated that acetaminophen (600 mg) and codeine (60 mg) was more effective than placebo on day 2, but had a similar effect to placebo as of day 3.16 Authors also highlighted that the differences from placebo in the etoricoxib arms were approximately twice that of the difference versus placebo in the acetaminophen (600 mg) and codeine (60 mg) arm.16 Likewise, the daily recall of worst pain measure for acetaminophen (600 mg) and codeine (60 mg) was found to be similar to placebo on days 2 and 3.16
Pain and Pain Intensity — Codeine Combination Drugs Versus Acetaminophen or Acetaminophen Combination Drugs
One SR described a comparison of acetaminophen (300 mg) and codeine (30 mg) against acetaminophen (300 mg) and caffeine (20 mg) in patients with post-operative dental pain and reported a difference of 1.67 in pain scores (using a VAS scale of 0 to 10) at 6 hours follow-up (clinical and/or statistical significance not reported).22 This SR also reported some findings narratively, including that pain scores measured at 3, 6, and 12 hours were lower in the acetaminophen (300 mg) and codeine (30 mg) group, and that there were no differences found at all other follow-up intervals.22 Authors concluded that there was a small benefit of the codeine-containing combination, as compared to the caffeine-containing combination.22
One RCT compared treatment with paracetamol (1,000 mg) versus paracetamol (1,000 mg) and codeine (30 mg) every 6 hours for 3 days in 39 patients with acute apical abscess.25 Study investigators measured pain using a VAS (0 to 100) at baseline, 6, 12, 24, 48, and 72 hours, and reported no statistically significant differences between patient groups at any follow-up time point.25 Authors concluded that both medications were effective for pain control in this patient population.25
Pain Intensity — Codeine Combination Drugs Versus NSAIDs or NSAID Combination Drugs
The recently published series of 2 RCTs characterizing pain severity using SPID and peak PID15 also described the statistically significant superiority of naproxen sodium (440 mg) to acetaminophen (600 mg) and codeine phosphate (60 mg) in SPID at 6 and 8 hours (although no statistically significant difference was observed at 4 hours) in the first of the 2 trials, with no statistically significant differences in peak PID between the drugs.15 In the second trial, no statistically significant difference was found between the drugs in peak PID or SPID at any follow-up time point.15 These findings were similar to those reported in the 5-arm RCT reported across 2 papers,16,17 where it was reported that no statistically significant difference between etoricoxib (120 mg) and acetaminophen (600 mg) and codeine (60 mg) was found in peak PID from baseline at 6 hours (P = 0.199).17
Pain and Pain Intensity — Codeine Combination Drugs Versus Other Drugs or Combination Drugs
One RCT investigated the use of paracetamol (1,000 mg), ibuprofen (400 mg), and codeine (60 mg) against paracetamol (1,000 mg) and ibuprofen (400 mg) administered every 6 hours in 131 patients undergoing third molar extraction.26 VAS scores were presented graphically and could not therefore be abstracted for inclusion in this report, but authors did indicate that no significant differences between groups were found.26 Study investigators also measured Global Pain Scale levels post-operatively using a questionnaire, corroborating the VAS scores in finding no statistically significant difference between the groups. Authors concluded that the addition of codeine to this medication regimen in these patients proffered no benefit.26
Another RCT randomized 26 patients with acute periradicular abscess to either codeine (30 mg) and acetaminophen (500 mg) or tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg) every 4 hours for 3 days, measuring pain using a VAS (0 to 100) at baseline, 6, 12, 48, and 72 hours.27 Study authors reported no statistically significant differences between the drug combinations at any of the follow-up time points.27 Similarly, another RCT randomized 100 patients to either Stilpane (i.e., paracetamol 320 mg and codeine 8 mg) or Tramacet (paracetamol 325 mg and tramadol 37.5mg) every 6 hours for the treatment of post-operative pain following third molar extraction.30 Authors reported on the SPID and VAS outcome measures at 3, 6, and 48 hours, as well as 5 days following the surgery and found no statistically significant differences between the groups on either measure at any point in follow-up.30
Pain Relief — Codeine Combination Drugs Versus Placebo
One SR investigated multiple combinations of analgesics (many of which contained codeine) compared with placebo for post-operative dental pain in patients following third molar extraction.23 Authors calculated adjusted scores characterizing TOTPAR at 6 hours for all of the included studies, where higher scores represented superiority of the analgesic effect.23 Total pain relief in codeine-containing combinations, reported using the calculated mean of adjusted TOTPAR6 scores, was found to range from 1.43 in 1 study of acetaminophen (1 g) and codeine phosphate (30 mg) versus placebo to 6.70 in another study comparing acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg) to placebo.23
Another SR described pain relief in patients with pain from third molar extractions using multiple over-the-counter analgesic combinations (some of which contained codeine) as compared to placebo.24 Authors reported on the proportion of study patients achieving 50% max TOTPAR at 4 or 6 hours (i.e., a calculated measure of TOTPAR relative to baseline; authors reported only that “...50%maxTOTPAR was calculated using standard methods.” (p22))24 Using 50% max TOTPAR, the study reported relative benefit values of 2.7 (95% CI, 1.8 to 4.8) for paracetamol (1,000), codeine (base15), and doxylamine succinate (10) as compared to placebo; and 6.2 (95% CI, 0.9 to 45) for paracetamol (1,000), caffeine (50), and codeine (base13), and 34 (95% CI 4.9 to 23.9) for ibuprofen (400) and codeine (25.6) compared to placebo.24 Of note, this SR did not specify the units of measure for the drug combinations described, and the units “base13” and “base15” were neither explained nor elaborated.
The recently published series of 2 RCTs comparing acetaminophen (600 mg) and codeine phosphate (60 mg) with placebo15 also described pain relief using TOTPAR at 4, 6, and 8 hours, as well as measuring peak pain relief. In both the first and second trials, the authors described the statistically significant superiority of acetaminophen (600 mg) and codeine phosphate (60 mg) against placebo at all follow-up time points, as well as a statistically significant benefit in peak pain relief.15 The studies also investigated time to onset of pain relief, indicating a statistically significant benefit in both trials for acetaminophen (600 mg) and codeine phosphate (60 mg), with a median of 1.0 hours until some relief, as compared to placebo, and with a median of greater than 8 hours to some relief in both trials.15
Pain Relief — Codeine Combination Drugs Versus NSAIDs or NSAID Combination Drugs
In the first of 2 RCTs comparing acetaminophen (600 mg) and codeine phosphate (60 mg) with naproxen sodium (440 mg),15 authors reported statistically significant superiority of the NSAID with regard to TOTPAR at all follow-up time points; however, no significant difference was found between the drugs in terms of peak pain relief.15 The study also reported on time to onset of relief, indicating no difference in either absolute or statistical terms between naproxen sodium (440 mg) and acetaminophen (600 mg) and codeine phosphate (60 mg). In the second trial, authors reported no statistically significant difference between the drugs in TOTPAR at 4 hours or peak pain relief, but did find a statistically significant benefit of naproxen sodium (440 mg) in TOTPAR at both 6 and 8 hours of follow-up.15 As it concerns the median time to some relief, authors found a statistically significant benefit in the second trial favouring acetaminophen (600 mg) and codeine phosphate (60 mg), as compared to naproxen sodium (440 mg) (1.0 hours versus 2.0 hours, respectively).
The RCT published across 2 papers16,17 also reported on pain relief in the 588 patients, finding a statistically significant benefit for etoricoxib (120 mg and 90 mg) versus acetaminophen (600 mg) and codeine (60 mg) in TOTPAR6 scores (P ≤ 0.001 for both etoricoxib dosages, respectively).17 Likewise, a statistically significant benefit in the patient’s global assessment of study medication across a 24 hour time span was observed between both doses of etoricoxib (120 mg and 90 mg), as compared with acetaminophen (600 mg) and codeine (60 mg) (P ≤ 0.05), as well as at the 24 hour mark (P = 0.007 and P = 0.014, respectively).17 However, the time to perceptible pain relief was described by the authors as being “similar” (p5) between the etoricoxib arms and the acetaminophen (600 mg) and codeine (60 mg) group.17
Use of Rescue Medication — Codeine Combination Drugs Versus Placebo
Patient use of rescue medication in codeine combination drugs compared with placebo was reported in 4 of the included RCTs.15-17,28 The 1 report of 2 RCTs describing a comparison of acetaminophen (600 mg) and codeine phosphate (60 mg) against placebo for pain from third molar extraction reported that, in the first of the 2 trials, 85% of the patients in the acetaminophen (600 mg) and codeine phosphate (60 mg) group, and 91% of patients in the placebo arm, took backup medication (the significance of the difference between the groups was not reported).15 Further, study investigators measured the hours until use of rescue medication, reporting a statistically significant benefit (narratively only) in the median number of hours for the acetaminophen (600 mg) and codeine phosphate (60 mg) group (i.e., 3.4 hours), as compared to patients receiving placebo (i.e., 1.1 hours).15 Findings in the second trial with regard to this outcome were similar15 (see Appendix 4 for details).
The 2 reports of 1 RCT describing both acetaminophen (600 mg) and codeine (60 mg) against placebo in the treatment of patients following third molar extraction reported on the use of rescue medication within the first 24 hours of the first dose of study medication17 and on days 2 and 3 of the study.16 Specifically, study authors reported that 35.5% of patients receiving acetaminophen (600 mg) and codeine (60 mg) required rescue medication in the 6 hours following the first dose of study medication,17 followed by 23.2% on day 2 and 19.6% on day 3.16 In the placebo group, 65.2% of patients receiving placebo required rescue medication in the first 6 hours,17 followed 55.6% on day 2 and 21.7% on day 3.16 The authors did not characterize the significance of the difference between the groups in the first 6 hours, but did specify that acetaminophen (600 mg) and codeine (60 mg) was found to be significantly more beneficial than placebo on day 2 (odds ratio, 0.23; 95% CI, 0.10 to 0.54) but not on day 3 (odds ratio 0.89; 95% CI, 0.34 to 2.37).16
Notably, another RCT comparing the preoperative treatment of patients preparing to undergo third molar extraction with either paracetamol (500 mg) and codeine (30 mg), or placebo, described the number of patients who used rescue medication, as well as the number of rescue medication tablets taken, and reported no statistically significant difference in either outcome between the groups (P = 0.364 and P = 0.104, respectively).28
Use of Rescue Medication — Codeine Combination Drugs Versus NSAIDs
Patient use of rescue medication in codeine combination drugs compared with NSAIDs was described in 3 of the included RCTs.15-17 The 1 report of 2 RCTs describing a comparison of naproxen sodium (440 mg) versus acetaminophen (600 mg) and codeine phosphate (60 mg) reported that, in the first of the 2 trials, 62% of patients in the naproxen sodium (440 mg) group and 85% of the patients in the acetaminophen (600 mg) and codeine phosphate (60 mg) group took backup medication (statistical significance of the difference between groups was not reported).15 Regarding the median hours before the use of rescue medication, the authors reported a statistically significant benefit (narratively, only) for the naproxen sodium (440 mg) group (i.e., 5.9 hours) compared to the acetaminophen (600 mg) and codeine phosphate (60 mg) patients (i.e., 3.4 hours).15 Findings in the second trial with regard to these outcomes were similar (see Appendix 4 for details).15
The 2 reports of 1 RCT comparing acetaminophen 600 mg and codeine 60 mg against etoricoxib 120 mg and etoricoxib 90 mg reported that, whereas 35.5% of patients receiving acetaminophen 600 mg and codeine 60 mg required rescue medication in the 6 hours following the first dose of study medication, only 12.4% and 8.4% of patients receiving etoricoxib 120 mg and etoricoxib 90 mg, respectively, required rescue medication.17 Authors described acetaminophen 600 mg and codeine 60 mg as demonstrating inferiority against both doses of etoricoxib with regard to this outcome.36 On days 2 and 3, 23.2% and 19.6% of patients, respectively, in the acetaminophen 600 mg)and codeine 60 mg group required rescue medication, as compared to 17.7% and 16.7% in the etoricoxib 120 mg group, respectively, and 22.6% and 13.8% in the etoricoxib 90 mg group, respectively.16 Authors indicated that both etoricoxib groups were “better” (p5) compared to acetaminophen 600 mg and codeine 60 mg) in the 6-hour follow-up,17 with no characterization of the significance of the differences between the acetaminophen 600 mg and codeine 60 mg and the etoricoxib groups described for this outcome on days 2 or 3.16 The median time to use of rescue medication in the first 6 hours of study assessments was also reported for each group,17 with authors indicating that the time for both etoricoxib doses was “longer” (p5) (i.e., better) as compared to that for the codeine-containing drug.17 Median time to rescue medication was not reported for days 2 and 3 of follow-up.16
Use of Rescue Medication — Codeine Combination Drugs Versus Other Drugs
One RCT comparing codeine (30 mg) and acetaminophen (500 mg) against tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg) for the treatment of pain in patients with acute periradicular abscess reported that 40% of patients in both groups took additional medication.27 Authors also reported the number of additional tablets taken, finding that, on average, patients in the codeine (30 mg) and acetaminophen (500 mg) group took 1.5 additional tablets compared to 1.6 additional tablets in the tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg) group (no characterization of the significance of the difference between groups was reported).27
The RCT comparing paracetamol 1,000 mg and ibuprofen 400 mg, with or without codeine 60 mg, in patients with acute pain from third molar extraction reported the use of rescue medication in 1 patient (1.5%) in the codeine group and 2 (3.0%) in the non-codeine group; authors did not comment on the significance of this difference.26
Pain Intensity and Relief
One report of an RCT described the sum of hourly pain relief and hourly PID from baseline, with authors finding no statistically significant difference between the codeine-containing Stilpane and the non‒codeine-containing Tramacet (P > 0.05 at all follow-up time points).30
Sensitivity
Dental sensitivity was reported in 1 RCT assessing the efficacy of paracetamol 500 mg and codeine 30 mg compared to ibuprofen 400 mg or placebo in patients preparing to undergo a series of 2 tooth-bleaching procedures.29 Using an analogue visual scale of pain, study investigators collected scores immediately following each procedure for each patient, summed these scores across the 2 procedures, and calculated mean values of global immediate sensitivity for each treatment group. The mean global immediate sensitivity scores for patients receiving paracetamol 500 mg and codeine 30 mg was 1.0 (SD, 0.2); for ibuprofen 400 mg, it was 4.8 (SD, 0.9); and for those receiving placebo, it was 4.7 (1.0). The scores were statistically significantly different (P < 0.001) in favour of paracetamol 500 mg and codeine 30 mg versus both comparison arms and the authors concluded that the codeine-containing medication was superior to ibuprofen and placebo for the pre-treatment of dental sensitivity in patients preparing to undergo tooth bleaching.29
Patient Self-Reported Perception of Medication Effectiveness
The recently published report of 2 trials comparing acetaminophen 600 mg and codeine phosphate 60 mg versus placebo also reported on the findings of a global evaluation for pain relief with 45% of patients in the acetaminophen 600 mg and codeine phosphate 60 mg group reporting good, very good, or excellent relief, compared to 12% of patients in the placebo group in the first trial; and 54% of patients in the acetaminophen 600 mg and codeine phosphate 60 mg group reporting good, very good, or excellent relief compared to 13% of patients in the placebo group.15 As it concerns the comparison of acetaminophen 600 mg and codeine phosphate 60 mg to naproxen sodium 440 mg, 59% of patients in the naproxen sodium 440 mg group reported good, very good, or excellent relief compared to the 45% of patients in the acetaminophen 600 mg and codeine phosphate 60 mg group in the first trial.15 The second trial identified the same proportion of patients in the naproxen sodium 440 mg arm (i.e., 59%) reporting good, very good, or excellent relief compared to 54% of patients in the acetaminophen 600 mg and codeine phosphate 60 mg group.15 Another report of an RCT comparing Stilpane and Tramacet described a measure of patient-reported medication efficacy collected at 6 hours and characterized using a scale from “poor” to “excellent.”30 Authors reported narratively that there was no statistically significant difference found between the codeine-containing Stilpane and the non‒codeine-containing Tramacet for this measure.30
However, the 5-arm RCT reporting across 2 papers16,17 reported on the patient's global assessment of study medication, demonstrating a statistically significant benefit for etoricoxib (120 mg and 90 mg) against acetaminophen (600 mg) and codeine (60mg) (P ≤ 0.05) across a 24-hour time span and again at the 24-hour mark (P = 0.007 and P = 0.014, respectively).17 Likewise, the patient's global assessment of study medication on days 2 and 3 was found to statistically significantly favour etoricoxib as compared to acetaminophen (600 mg) and codeine (60 mg) (P < 0.01).16
Number Needed to Treat
One SR describing several comparisons of codeine-containing combination drugs against placebo for the treatment of post-operative dental pain in patients following third molar extraction reported on NNT.24 The NNT to achieve 50% max TOTPAR for ibuprofen (400) and codeine (25.6) versus placebo was 1.7 (95% CI, 1.5 to 1.9) and for paracetamol (1,000), caffeine (50), and codeine (base13) versus placebo was 4.2 (95% CI, 2.5 to 1.4).24These numbers were not reported with units in the SR.
Safety
Of the 9 studies reporting safety data, the most commonly reported AEs included nausea (9 studies);15-17,21,23,25,27,28,30 dizziness (9 studies);15-17,21,23,25,27,28,30 headache (9 studies);15-17,21,23,25,27,28,30 vomiting (6 studies);15-17,21,28,30 drowsiness (4 studies);21,23,25,27 rash (3 studies);15,23,30 somnolence (3 studies);15,17,30 and emesis (2 studies).25,27 Other AEs were reported in only 1 study each; i.e., tiredness, cold sweats and dizziness, gastrointestinal upset;21 earache, numbness in the legs, dry mouth, hot feeling, sweating, restlessness, tiredness;23 nervousness, syncope, dyspepsia, infection;15 insomnia, pruritis;30 alveolar osteitis and hyperhidrosis.17
Adverse Events — Codeine Combination Drugs Versus Placebo
The SR of RCTs describing the clinical effectiveness of a variety of codeine-containing combination drugs against placebo in patients with post-operative pain described the relative risk regarding a variety of AEs.21 Authors reported finding no statistically significant difference between patients in experiencing any AE, treatment-emergent AEs, tiredness, nausea, dizziness, cold sweats and dizziness, gastrointestinal upset, vomiting, or headache.21 Conversely, the recently published report of 2 RCTs comparing acetaminophen (600 mg) and codeine phosphate (60 mg) versus placebo found that the number of patients in the active treatment group experiencing at least 1 AE was statistically significantly higher (P ≤ 0.02).15 Similarly, patients receiving acetaminophen (600 mg) and codeine phosphate (60 mg) were more likely to experience nausea, vomiting, dizziness, and somnolence as compared to patients receiving placebo.15 Likewise, the 5-arm trial describing a comparison of acetaminophen (600 mg) and codeine (60 mg) against placebo also reported a statistically significantly greater proportion of patients in the codeine-containing group experiencing nausea and vomiting (P ≤ 0.002) in the first 24 hours after use of the drug.17 The difference between experiences of AE on days 2 and 3 was not described quantitatively; however, the authors did highlight that patients in the acetaminophen (600 mg) and codeine (60 mg) arm experienced the greatest proportion of AEs compared to all the other study groups (including placebo).16 Another RCT described an assessment of AEs, but reported finding none among either the group of patients receiving paracetamol (500 mg) and codeine (30 mg) or those receiving placebo.28 Finally, 1 SR of RCTs comparing codeine combination drugs against placebo did report on the proportions of patients experiencing AEs by drug combination, but it was not clear whether the authors were reporting the data for the active treatment arms, only, as opposed to comparatively across the active and placebo groups;23 thus, these data were abstracted and tabulated (Appendix 4) but are not summarized further.
Adverse Events — Codeine Combination Drugs Versus Acetaminophen
The RCT comparing paracetamol 1,000 mg with and without codeine 30 mg in patients with acute apical abscess found no statistically significant difference between groups, with 12 and 11 patients, respectively, reported as having experienced an AE (P > 0.05).25
Adverse Events — Codeine Combination Drugs Versus NSAIDs/NSAID Combination Drugs
The recently published report of 2 RCTs comparing acetaminophen (600 mg) and codeine phosphate (60 mg) against naproxen sodium (440 mg) found that, in the first of the 2 trials, the number of patients in the codeine-containing arm of the trial experiencing at least 1 AE was statistically significantly higher as compared to patients receiving placebo (P ≤ 0.02).15 Similarly, patients receiving acetaminophen (600 mg) and codeine phosphate (60 mg) were described as being more likely to experience nausea, vomiting, dizziness, and somnolence as compared to patients receiving naproxen sodium (440 mg), with a statistically significant difference reported in the second of the 2 trials for patients experiencing dizziness (P = 0.01).15 Likewise, the 5-arm trial describing a comparison of acetaminophen (600 mg) and codeine (60 mg) against 2 doses of etoricoxib (120 mg and 90 mg) also reported a statistically significantly greater proportion of patients in the codeine-containing group experiencing 1 or more AEs, drug-related AEs, and nausea and vomiting (P ≤ 0.001) in the first 24 hours after use of the study drugs.17 The difference between experiences of AEs on days 2 and 3 were not described quantitatively; however, authors did highlight that patients in the acetaminophen (600 mg) and codeine (60 mg) arm experienced the greatest proportion of AEs compared to all other groups (including both doses of etoricoxib).16
Adverse Events — Codeine Combination Drugs Versus Other Drugs
The RCT comparing codeine 30 mg and acetaminophen 500 mg against tramadol hydrochloride 37.5 mg)and acetaminophen 500 mg described the assessment of several AEs, reporting no statistically significant difference between the groups with regard to any.27 Likewise, the South African RCT describing a comparison of Stilpane versus Tramacet described no statistically significant difference between the groups with regard to the assessment of multiple AEs.30
Number Needed to Harm
The RCT comparing paracetamol 1,000 mg with and without codeine 30 mg in patients with acute apical abscess found no statistically significant difference (described narratively, only) between groups in their analyses of NNH, reporting that “the Number Needed to Harm (NNH) value was 47.6” (p5/8).25 Similarly, another RCT comparing codeine 30 mg and acetaminophen 500 mg against tramadol hydrochloride 37.5 mg and acetaminophen 500 mg reported the same NNH value of 1.25 for both groups.27
Limitations
There were several limitations to this review, primarily the limited number of included studies identified and amount of available data to answer the first research question concerning the use of codeine as a single-drug intervention in the management of acute dental pain; i.e., only 1 eligible study was identified, reporting a limited amount of data.19 Nonetheless, the authors of this overview did highlight that the findings reported specific to codeine in the treatment of acute dental pain were based on data from 15 studies, describing more than 1,000 patients and so were deemed to be reliable.19 Related to this, the SR studies identified lacked alignment in their scope and focus with the questions posed in this review, rendering only a few of the primary studies they described relevant to this report.19-24 Reporting was unclear or lacked critical information in 2 of the SRs, making the data presented difficult to interpret.23,24 Further, of the 4 SR included in this review, 3 included primary studies that were published in the 1980s and 1990s. It is unclear the extent to which changes in practice in that time may affect the interpretation of this data. Finally, the small sample sizes of some of the RCTs, combined with missing information and/or methodological limitations of many of the RCTs included in this review, may impact the extent to which the findings can be generalized to other populations.
Conclusions and Implications for Decision- or Policy-Making
While opioids are acknowledged as having a limited role in managing dental pain,5 their relative risks of dependency, addiction, and AEs are problematic.37 Despite codeine being considered a “weak opioid” (p133),9 those in dentistry acknowledge that the use of opioids to manage dental pain in patients has contributed to the opioid crisis37 and that there may be more clinically effective alternatives, such as NSAIDs and acetaminophen, for example.10
In the literature, codeine as a single-drug therapy in the management of pain has generally been found to be less effective than other analgesics9 and the findings of this review corroborate these conclusions; 1 study was found indicating that codeine (60 mg) for the treatment of dental pain had 1 of the highest NNTs of all the drugs assessed in the overview and 1 of the shortest time frames to remedication.19 Further to this, the addition of codeine to acetaminophen or ibuprofen regimens was not found to add benefit to patients with dental pain,25,26 but was found to be associated with increases in AEs.25
On the other hand, codeine in combination with other drugs has demonstrated some clinical effectiveness in the treatment of acute dental pain — specifically when compared to placebo.15-17,21,28 Nonetheless, when compared to other combination drugs (e.g., NSAIDs or acetaminophen-based combinations), codeine combination drugs were found by studies included in this review to either compare less favourably regarding the effects on measures of pain15-17,26 or to add no benefit.15-17,22,25,26 These findings are supported by a recent overview of SRs describing multiple types of drugs for dental pain, including opioids, and highlighting ibuprofen and acetaminophen as the most clinically effective and beneficial.3
In addition to the apparently limited role for codeine in the treatment of dental pain, opioids have been singled out as the analgesics most strongly associated with AEs.3 Many of the studies in this review corroborate this conclusion, demonstrating that codeine and codeine combination drugs have been shown to be more harmful than other non-opioid drugs and combinations.15-17
The 1 apparent exception with regard to these findings and conclusions was the study of dental sensitivity in patients undergoing tooth bleaching, which found a statistically significant benefit in the pre-procedural administration of an acetaminophen and codeine combination as compared to an NSAID or placebo.29 Notably, the difference between nociceptive pain and the pain caused from tooth bleaching could be a factor, as could be the contribution of acetaminophen, the small size of the study, and the fact that no safety data were reported,29 making it unrealistic to draw conclusions from this finding alone and indicating that more research would be necessary to identify the role of codeine in the pre-treatment of patients preparing to undergo tooth bleaching.
Finally, the 2 studies comparing codeine against other opioid-containing drugs found no differences in measures of dental pain in patients.27,30 Likewise, the studies found codeine versus opioid-containing drugs to have similar safety profiles.27,30
In conclusion, the findings of this review seem to generally agree with a consensus in much of the literature as it concerns the relative benefit and value of codeine in the management of dental pain; i.e., the small contribution that codeine may offer to dental patients with acute pain may be outweighed by the risks and safety concerns (including AEs and concerns around misuse of the drug). In the broader context of an opioid crisis, alternatives to codeine and other opioids — such as ibuprofen- and acetaminophen-based products — are preferred and recommended by many in the dental community.6,7,9
References
1.Renton T. Dental (Odontogenic) Pain. Rev Pain. 2011;5(1):2-7. Medline
2.Becker DE. Pain management: Part 1: Managing acute and postoperative dental pain. Anesth Prog. 2010;57(2):67-78; quiz 79-80. Medline
3.Moore PA, Ziegler KM, Lipman RD, Aminoshariae A, Carrasco-Labra A, Mariotti A. Benefits and harms associated with analgesic medications used in the management of acute dental pain: An overview of systematic reviews. J Am Dent Assoc. 2018;149(4):256-265.e253. Medline
4.Kim SJ, Seo JT. Selection of analgesics for the management of acute and postoperative dental pain: a mini-review. J Periodontal Implant Sci. 2020;50(2):68-73. Medline
5.Hersh EV, Moore PA, Grosser T, et al. Nonsteroidal Anti-Inflammatory Drugs and Opioids in Postsurgical Dental Pain. J Dent Res. 2020;99(7):777-786. Medline
6.Teoh L. Managing acute dental pain without codeine. Aust Prescr. 2020;43(2):64. Medline
7.Laniado N, Hersh EV, Badner VM, Saraghi M. Prescribing Analgesics for Postoperative Dental Pain. Compend Contin Educ Dent (Jamesburg, NJ: 1995). 2020;41(9):466-473; quiz 474.
8.Codeine: drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021 www.uptodate.com. Accessed 2021 Jan 25.
9.Iedema J. Cautions with codeine. Aust Prescr. 2011;34(5):133-135.
10.Dionne RA, Gordon SM, Moore PA. Prescribing Opioid Analgesics for Acute Dental Pain: Time to Change Clinical Practices in Response to Evidence and Misperceptions. Compend Contin Educ Dent. 2016;37(6):372-378;quiz379.
11.Bolanos-Diaz R, Regalado-Rafael R. Economic evaluation of ibuprofen/codeine combination versus ibuprofen alone for acute pain treatment in Peru. J Pharm Health Serv Res. 2011;2(4):227-232.
12.Moeller J, Farmer J, Quiñonez C. Patterns of analgesic use to relieve tooth pain among residents in British Columbia, Canada. PLoS One. 2017;12(5):e0176125. Medline
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
15.Cattry E, Troullos E, Paredes-Diaz A. Efficacy and safety of naproxen sodium 440 mg versus acetaminophen 600 mg/codeine phosphate 60 mg in the treatment of postoperative dental pain. Am J Dent. 2020;33(2):106-112. Medline
16.Brown JD, Daniels SE, Bandy DP, et al. Evaluation of multiday analgesia with etoricoxib in a double-blind, randomized controlled trial using the postoperative third-molar extraction dental pain model. Clin J Pain. 2013;29(6):492-498. Medline
17.Daniels SE, Goulder MA, Aspley S, Reader S. A randomised, five-parallel-group, placebo-controlled trial comparing the efficacy and tolerability of analgesic combinations including a novel single-tablet combination of ibuprofen/paracetamol for postoperative dental pain. Pain. 2011;152(3):632-642. Medline
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
19.Moore RA, Derry S, McQuay HJ, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults. Cochrane Database Syst Rev. 2011(9):CD008659. Medline
20.Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L. Non-prescription (OTC) oral analgesics for acute pain - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015(11):CD010794. Medline
21.Abdel Shaheed C, Maher CG, McLachlan AJ. Efficacy and Safety of Low-dose Codeine-containing Combination Analgesics for Pain: Systematic Review and Meta-Analysis. Clin J Pain. 2019;35(10):836-843. Medline
22.Abou-Atme YS, Melis M, Zawawi KH. Efficacy and safety of acetaminophen and caffeine for the management of acute dental pain: a systematic review. Saudi Dent J. 2019;31(4):417-423. Medline
23.Au AHY, Choi SW, Cheung CW, Leung YY. The efficacy and clinical safety of various analgesic combinations for post-operative pain after third molar surgery: A systematic review and meta-analysis. PLoS One. 2015;10 (6) (no pagination)(e0127611).
24.Moore RA, Derry C. Efficacy of OTC analgesics. Int J Clin Pract. 2013;67(SUPPL. 178):21-25. Medline
25.da Silva PB, Mendes AT, Cardoso MBF, et al. Comparison between isolated and associated with codeine acetaminophen in pain control of acute apical abscess: a randomized clinical trial. Clin Oral Investig. 2020;10:10. Medline
26.Best AD, De Silva RK, Thomson WM, Tong DC, Cameron CM, De Silva HL. Efficacy of Codeine When Added to Paracetamol (Acetaminophen) and Ibuprofen for Relief of Postoperative Pain After Surgical Removal of Impacted Third Molars: A Double-Blinded Randomized Control Trial. J Oral Maxillofac Surg. 2017;75(10):2063-2069. Medline
27.Santini MF, Rosa RAD, Ferreira MBC, Fischer MI, Souza EM, So MVR. Comparison of two combinations of opioid and non-opioid analgesics for acute periradicular abscess: a randomized clinical trial. J Appl Oral Sci. 2017;25(5):551-558. Medline
28.Cristalli MP, LaMonaca G, De Angelis C, Pranno N, Annibali S. Efficacy of preoperative administration of paracetamol-codeine on pain following impacted mandibular third molar surgery: A randomized, split-mouth, placebo-controlled, double-blind clinical trial. Pain Res Manag. 2017;2017 (no pagination)(9246352).
29.de Oliveira SN, de Assuncao IV, Borges BCD. Efficacy of ibuprofen and codeine + paracetamol to reduce immediate bleaching sensitivity caused by in-office tooth bleaching: A randomized, controlled, double-blind clinical trial. Am J Dent. 2018;31(4):195-198. Medline
30.Outhoff K, Dippenaar JM, Nell M, Royds M, Greeff OBW. A randomised clinical trial comparing the analgesic and anxiolytic efficacy and tolerability of Stilpane and Tramacet after third molar extraction: Clinical trail. South Afr J Anaesthesia Analgesia. 2015;21(2):22-27.
31.Hussey EK, Kapur A, O'Connor-Semmes R, et al. Safety, pharmacokinetics and pharmacodynamics of remogliflozin etabonate, a novel SGLT2 inhibitor, and metformin when co-administered in subjects with type 2 diabetes mellitus. BMC Pharmacol Toxicol. 2013;14 (no pagination)(25).
32.Goldkuhle M, Narayan VM, Weigl A, Dahm P, Skoetz N. A systematic assessment of Cochrane reviews and systematic reviews published in high-impact medical journals related to cancer. BMJ Open. 2018;8(3):e020869. Medline
33.Petticrew M, Wilson P, Wright K, Song F. Quality of Cochrane reviews. Quality of Cochrane reviews is better than that of non-Cochrane reviews. BMJ (Clinical research ed). 2002;324(7336):545-545. Medline
34.Bonato LL, Quinelato V, Pinheiro ADR, et al. ESRRB polymorphisms are associated with comorbidity of temporomandibular disorders and rotator cuff disease. Int J Oral Maxillofac Surg. 2016;45(3):323-331. Medline
35.Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. Medline
36.Daniels SE, Bandy DP, Christensen SE, et al. Evaluation of the dose range of etoricoxib in an acute pain setting using the postoperative dental pain model. Clin J Pain. 2011;27(1):1-8. Medline
37.Thornhill MH, Suda KJ, Durkin MJ, Lockhart PB. Is it time US dentistry ended its opioid dependence? J Am Dent Assoc. 2019;150(10):883-889. Medline
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Overviews of Systematic Reviews
Study citation, country, funding source | Numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Moore et al. (2015)20 UK | 10 Cochrane SRs included in the overview, 1 of which could be ascertained as containing data relevant to this review | Adults with acute post-operative pain | Intervention: Non-prescription, OTC ibuprofen + codeine (dose and administration NR) Comparator: Placebo | Insufficient data of relevance to this review was reported to describe eligible outcomes. |
Moore et al. (2011)19 UK | 35 Cochrane SRs included in the overview, 1 of which could be ascertained as containing data relevant to this review | Adults with acute post-operative pain | Interventions: Single-dose, oral codeine 60 mg Comparator: Placebo | Efficacy: 50% maximum pain relief Mean time to remedication Safety: NR (i.e., no data specific to dental pain reported) Follow-up: 4hr to 6hr |
hr = hour(s); NR = not reported; OTC = over the counter; SR = systematic review.
Table 3: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Abdel Shaheed et al. (2019)21 Australia Supported by the Therapeutic Goods Administration (Canberra, Australia) | 10 RCTs included in the SR, 5 of which reported data eligible for this review | Post-operative dental pain | Intervention: Combination: acetylsalicylic acid (375 mg) and codeine (15 mg) and caffeine (30 mg), single dose; ibuprofen (200 mg) and codeine (12.8 mg), 2 tabs, single dose; ibuprofen (200 mg) and codeine (15 mg), single dose; ibuprofen (400 mg) and codeine (30 mg), single dose; ibuprofen (800 mg) and codeine (60 mg), single dose; paracetamol (1,000 mg) and codeine (60 mg), single dose (a second dose could be taken); paracetamol (500 mg) and codeine (15 mg), 2 tabs, single dose; paracetamol (500 mg) and codeine (30 mg), single dose (a second dose could be taken) Comparator: Placebo | Efficacy: Acute nociceptive pain, 0 to 100 continuous pain scale Safety: AEs: Any, treatment-emergent, drowsiness, tiredness, nausea, dizziness, cold sweats and dizziness, GI upset, vomiting, headache Follow-up: 3hr to 12hr (efficacy outcomes); NR (safety outcomes) |
Abou-Atme et al. (2019)22 Italy, Saudi Arabia, US | 3 RCTs included in the SR, 1 of which reported data eligible for inclusion in this review | 76 pts with post-operative pain from dental implant surgery | Intervention: Combination acetaminophen (300 mg) and caffeine (20 mg), 1 dose 30 min. before and after surgery Comparator: Combination acetaminophen (300 mg) and codeine (30 mg), 1 dose 30 min. before and after surgery | Efficacy: Post-operative pain, VAS 0-10 Safety: NR Follow-up: 30 min., 3 hr, 6 hr, 12 hr, 1 d, 2 d, 3d, 7d post-medication |
Au et al. (2015)23 Hong Kong | 14 RCTs included in the SR; 8 of which reported data eligible for this review | Patients with post-operative pain following third molar extraction | Intervention: Combination, single dose: acetaminophen (650 mg) and codeine phosphate (60 mg) acetaminophen (600 mg) and codeine phosphate (60 mg) acetaminophen (300 mg) and codeine phosphate (30 mg) acetaminophen (1 g) and codeine phosphate (30 mg) acetylsalicylic acid (650 mg) and codeine phosphate (60 mg) acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg) and codeine phosphate (15 mg) ibuprofen (400 mg) and codeine phosphate (25.6 mg) Comparator: Placebo | Efficacy: Post-operative pain intensity (0 to 4 pain scale where 0 = no pain, 4 = severe pain): SPID6 scores from baseline across a 6-hr time frame adjusted SPID6 (difference between SPID6 of active medication minus SPID6 of placebo) post-operative pain relief (0 to 4 pain scale where 0 = no relief; 4 = complete relief): TOTPAR6 (sum of total pain relief scores across a 6-hr time frame) adjusted TOTPAR6 (difference between TOTPAR6 of active medication minus TOTPAR6 of placebo) Safety: AEs: Drowsiness, dizziness, earache, headache, nausea, numbness in legs, dry mouth, hot feeling, sweating, restlessness, tiredness, rash Follow-up: 6 hr (primary efficacy end points); NR (safety outcomes) |
Moore and Derry (2013)24 UK | 119 RCTs included in the SR, 3 of which reported data eligible for inclusion in this review | 361 patients with post-operative pain following third molar extraction | Intervention:a Combination: paracetamol (1,000 and codeine (base15) and doxylamine succinate (10); ibuprofen (400) and codeine (25.6); paracetamol (1,000) and caffeine (50) and codeine (base13); administration NR Comparator: placebo | Efficacy: Pain relief; i.e., 50% max TOTPAR (mean total pain relief values for active and placebo arms converted into % max TOTPAR by division into the maximum value) NNT (calculated using 50% max TOTPAR) Success rate (max. possible success rate being 100%; success rate = 100 × (active response ‒ placebo response/(100 ‒placebo response) Failure rate (max. possible success rate being 100%; failure rate = 100 – (success rate) Safety: NR Follow-up: 4hr or 6hr |
aNote: The units of measurement were not specified in the report of findings, nor were base13 and base15 explained by the authors of the study.
AE = adverse event(s); d = day(s); GI = gastrointestinal; hr = hour(s); mg = milligram(s); min. = minute(s); NNT = number needed to treat; NR = not reported; pts = patients; RCT = randomized controlled trial; SPID = sum of pain intensity difference; SPID6 = sum of pain intensity difference at 6 hours; SR = systematic review; TOTPAR = total pain relief; TOTPAR6 = total pain relief at 6 hours; VAS = visual analogue scale.
Table 4: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Cattry et al. (2020)15 US Funding source NR (reference is made to a “sponsor” (p107), who is not explicitly identified in the article) | 2 RCTs, single-centre, double-blind, double-dummy | 460 pts with at least moderate post-operative dental pain following removal of impacted third molars were randomized in 2 trials: Study 1 — Efficacy analyses All: 225 pts; Intervention: 90 pts; Active comparator: 91 pts; Placebo: 44 pts Study 1 — Safety analyses All: 228 pts; Intervention: 91 pts; Active comparator: 92 pts; Placebo: 45 pts Study 2 — Efficacy and safety analyses All: 230 pts; Intervention: 92 pts; Active comparator: 91 pts; Placebo: 47 pts Mean age, yr (SD) Study 1: 23.6 (6.80); Study 2: 21.3 (5.0) Sex, % female Study 1: 66; Study 2: 50 Baseline pain intensity, n (%) Study 1: Moderate: 165 (73); Severe: 60 (27) Study 2: Moderate: 192 (83); Severe: 38 (17) | Intervention: Naproxen sodium (440 mg), single dose Comparators: Acetaminophen (600 mg) and codeine phosphate (60 mg), single dose Placebo, single dose | Efficacy Pain severity: 0 to 4 continuous scale Pain relief: 0 to 5 continuous scale Safety Adverse events: Any body system Nausea, vomiting, dizziness, somnolence, headache, nervousness, syncope, dyspepsia, infection, rash Follow-up: 4 hr, 6 hr, 8 hr (efficacy outcomes); NR (safety outcomes) |
da Silva et al. (2020)25 Brazil Funding source NR | RCT, single centre, double blind | 39 pts seeking urgent care for acute apical abscess Intervention: 19 pts; Comparator: 20 pts Mean age, yr (SD) Intervention: 42.6 (15.5); Comparator: 44.3 (13.5) Sex, % female Intervention: 63.2; Comparator: 70 Baseline pain score, median (25th/75th percentile) Intervention: 85 (65/91); Comparator: 82 (63/98) | Intervention: Paracetamol (1,000 mg), every 6hr for 3d Comparator: Paracetamol (1,000 mg) and codeine (30 mg), every 6 hr for 3 d Other: All pts also received amoxicillin (500 mg) every 8hr for 7d as antibiotic treatment for their condition | Efficacy Pain (VAS, 0-100) Safety Adverse events: Dizziness, drowsiness, nausea, headache, emesis, other Follow-up: 6 hr, 12 hr, 24 hr, 48 hr, 72 hr |
de Oliveira et al. (2018)29 Brazil Funding source NR | RCT, single centre, double blind | 60 volunteers undergoing teeth-bleaching procedure across 2 sessions per pt, were randomized Intervention: 20 pts; Active comparator: 20 pts; Placebo: 20 pts Pt characteristics: NR | Intervention: Paracetamol (500 mg) and codeine (30 mg), administered 1hr before each bleaching session; N doses NR Comparator: Ibuprofen (400 mg), administered 1hr before each bleaching session; N doses NR Placebo, administered 1hr before each bleaching session; N doses NR | Efficacy Sensitivity, measured by global immediate sensitivity using a self-reported, analogue visual scale of pain (EVA), 1 to 10 Safety: NR Follow-up: “immediate” |
Best et al. (2017)26 New Zealand Funding source NR | RCT, single centre, double blind | 131 adult patients requiring removal of at least 1 mandibular third molar with an anticipated need for bone removal were randomized Intervention Randomized: 64 pts; Analyzed: 63 pts Comparator Randomized: 67 pts; Analyzed: 67 pts Mean age, yr (SD) Intervention: 23.0 (3.4); Comparator: 24.1 (5.9) Sex, % female Intervention: 60.9; Comparator: 67.2 Dental Anxiety, n (%) Intervention: 11 (17.5); Comparator: 13 (19.4) | Intervention Paracetamol (1,000 mg) and ibuprofen (400 mg) and codeine (60 mg) Comparator Paracetamol (1,000 mg) and ibuprofen (400 mg) | Efficacy Post-operative pain: VAS (100 mm) Post-operative pain questionnaire (experience of post-operative pain, treatment adherence, use of rescue medication) Safety Adverse events: Use of rescue medication Follow-up: Immediately post-surgery, every 3 hours for 48 hours post-surgery, 3 days post-surgery |
Cristalli et al. (2017)28 Italy Funding source NR | RCT, single centre, double blind | 32 patients requiring removal of 2 mandibular third molars across 2 procedures were randomized to:
Mean age, yr (SD) All: 22.65 (2.74) Sex, % female All: 57 Surgery duration, min (SD) Intervention: 30.47 (12.03); Control: 34.76 (12.21) | Intervention Paracetamol (500 mg) and codeine 30 mg), single dose administered pre-operatively in the first procedure (placebo administered in the second procedure) Comparator Placebo, single dose administered pre-operatively (paracetamol (500 mg) and codeine 30 (mg) administered in the second procedure) | Efficacy Post-operative pain: NRS-11: Time interval to first post-operative use of analgesic medication Use of rescue medication Number of rescue medication tablets taken Safety Adverse events: Nausea, vomiting, headaches, dizziness Follow-up: 1d, 2 d, 3 d, 1 wk |
Santini et al. (2017)27 Brazil Funding provided through grants from the Coordination for the Improvement of Higher Education Personnel (CAPES) | RCT, single centre, double blind | 26 pts seeking emergency care for acute periradicular abscess were randomized Intervention Randomized: 13 pts; Analyzed (efficacy): 10 pts; Analyzed (safety): 10 pts Comparator Randomized: 13 pts; Analyzed (efficacy): 8 pts; Analyzed (safety): 10 pts Mean age, yr (SD) Intervention: 41.6 (12.7); Comparator: 45.1 (16.7) Sex, % female Intervention: 80; Comparator: 60 Initial pain score (VAS 0 to 100), median (25th/75th percentiles) Intervention: 90 (71.2/100); Comparator: 81.5 (72.2/98.5) Difference b/w groups, Mann–Whitney U test P = 0.760 | Intervention Codeine (30 mg) and acetaminophen (500 mg), every 4 hr for 3d Comparator Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg), every 4 hr for 3d Other Amoxicillin (500 mg) every 8 hr for 7d for pts with systemic symptoms | Efficacy Pain Use of additional medication NNH Safety Adverse reactions Dizziness, drowsiness, nausea, headache, emesis, others Follow-up: Initial, 6 hr, 12 hr, 24 hr, 48 hr, 72 hr |
Outhoff et al. (2015)30 South Africa Funding provided by Aspen Pharmacare | RCT, single centre, single blind | 100 patients with moderate to severe pain following third molar extraction were randomized Intervention Randomized: 52 pts; Analyzed: 52 pts Comparator Randomized: 48 pts; Analyzed: 48 pts Mean age, yr All: 22; Intervention: NR; Comparator: NR Sex, % female Intervention: 67.3; Comparator: 58.3 | Intervention Stilpane (paracetamol (320 mg) and codeine (8 mg)) Comparator Tramacet (paracetamol (325 mg) and tramadol (37.5 mg)) | Efficacy Pain intensity: 0 to 4 point Likert scale; 0 to 100 mm VAS Pain relief: 0 to 5 point Likert scale; Self-reported, medication efficacy: 0 to 5 point Likert scale (0 = poor; 5 = excellent); Time to pain relief: Stopwatch-measured Safety Adverse reactions: Nausea, vomiting, somnolence, dizziness, headache, insomnia, pruritus, rash Follow-up: 30 min, hourly b/w 1hr and 6 hr, 48 hr, 5 d |
Brown et al. (2013)16 US Funding source NR; Support provided by Merck Sharp & Dohme Corporation | RCT, multi-centre, double blind | 588 pts experiencing moderate to severe pain 5hr following completion of the extraction of ≥ 2 third molars (one of which must have been impacted in the mandible) were randomized Intervention 1 Randomized: 97 pts; Completed: 95 pts Intervention 2 Randomized: 191 pts; Completed: 188 pts Active comparator 1 Randomized: 192 pts; Completed: 189 pts Active comparator 2 Randomized: 62 pts; Completed: 56 pts Placebo Randomized: 46 pts; Completed: 45 pts Dosed, Day 2/Day3, n pts (%) Intervention 1: 59 (61.5)/42 (43.8) Intervention 2: 143 (75.3)/88 (46.8) Active comparator 1: 163 (84.9)/123 (64.4) Active comparator 2: 35 (62.5)/24 (42.9) Placebo: 35 (76.1)/16 (34.8) Pt Characteristics: NR (i.e., reported earlier in Daniels et al. [2011] that follows) | Intervention 1 Etoricoxib (120 mg), once daily Intervention 2 Etoricoxib (90 mg), once daily Active Comparator 1 Ibuprofen (600 mg), every 6 hr Active Comparator 2 Acetaminophen (600 mg) and codeine (60 mg), every 6 hr Placebo Other Acetaminophen (325 mg), up to 4 times daily as rescue medication | Efficacy Post-operative pain: Daily recall of average and worst pain, 0 to 10 numerical rating scale (0 = “no pain;” 10 = “pain as bad as you can imagine”) Self-reported medication effectiveness: Patient’s global assessment of study medication, 0 to 4 categorical scale (0 = poor; 4 = excellent) Use of rescue medication: % pts Safety Adverse experiences Any, headache, dizziness, nausea, vomiting Follow-up: 2d (24 hr), post first dose; 3d (36 hr), post first dose; 14d, post first dose |
Daniels et al. (2011)17 US Funded by Merck & Co. Inc. | RCT, multi-centre, double blind | 588 pts requiring extraction of ≥ 2 third molars (1 of which must have been impacted in the mandible) were randomized Intervention 1: 97 pts Intervention 2: 191 pts Active comparator 1: 192 pts Active comparator 2: 62 pts Placebo: 46 pts Sex, % female Intervention 1: 51.5; Intervention 2: 59.2; Active comparator 1: 59.9; Active comparator 2: 59.7; Placebo: 54.3 Age in yr, mean (SD) Intervention 1: 21.8 (3.5); Intervention 2: 21.8 (3.6); Active comparator 1: 21.6 (3.8); Active comparator 2: 20.5 (2.8); Placebo: 21.0 (3.0) Baseline pain intensity, n pts (%) Moderate Intervention 1: 49 (50.5); Intervention 2: 98 (51.3); Active comparator 1: 106 (55.2); Active comparator 2: 30 (48.4); Placebo: 21 (45.7) Severe Intervention 1: 48 (49.5); Intervention 2: 93 (48.7); Active comparator 1: 86 (44.8); Active comparator 2: 32 (51.6); Placebo: 25 (54.3) | Intervention 1 Etoricoxib (120 mg), once daily Intervention 2 Etoricoxib (90 mg), once daily Active Comparator 1 Ibuprofen (600 mg), every 6 hr Active Comparator 2 Acetaminophen (600 mg) and codeine (60 mg), every 6 hr Placebo Other Hydrocodone bitartrate (5 mg) and acetaminophen (500 mg) as rescue medication | Efficacy Pain intensity: Measured using a 0 to 3 point Likert scale (0 = none; 3 = severe) Pain relief: TOTPAR6 measured using a 0 to 4 point Likert scale (0 = none; 4 = complete) Self-reported medication effectiveness: Patient’s global assessment of study medication, 0 to 4 categorical scale (0 = poor; 4 = excellent) Use of rescue medication: Time and amount taken Speed of analgesic response: Time to perceptible response; time to meaningful response using a double stopwatch method Safety Adverse experiences Any, drug-related, serious, nausea, vomiting, dizziness, alveolar osteitis, headache, somnolence, hyperhidrosis, discontinuation of study medication Follow-up: 16 pre-specified time points until 24hr; 14d (safety outcomes only) |
b/w = between; CAPES = Coordination for the Improvement of Higher Education Personnel; d = day(s); EVA = analogue visual scale of pain; hr = hour(s); mg = milligram(s); mm = millimetre; N/n = number; NNH = number needed to harm; NR = not reported; NRS-11 = Numerical Rating Scale-11; pt(s) = patient(s); RCT = randomized controlled trial; SD = standard deviation; TOTPAR6 = total pain relief at 6 hours; VAS = visual analogue scale; wk = week; yr = year(s).
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Overviews of Systematic Reviews Using AMSTAR 213
Strengths | Limitations |
Moore et al. (2011)19 | |
The inclusion criteria described the required PICO components, including time frame for follow-up. A protocol was published before conducting the overview. The selection of eligible study designs was described. Study selection and data extraction were performed in duplicate. Included reviews were described in adequate detail for an overview. Authors addressed funding and potential conflict of interest for included reviews. Heterogeneity was addressed. The risk of bias was reportedly low due to the limitation to Cochrane reviews only. The authors reported the source of funding for the overview and stated their conflicts of interest (but not how these were managed during the overview). | Authors explained that only Cochrane reviews were sought and included but did not elaborate a justification as to why this decision was made. Search dates were not reported. Excluded reviews were neither listed nor described. Risk of bias assessments were not described; the authors stated only that included reviews satisfied AMSTAR requirements. |
Moore et al. (2015)20 | |
The inclusion criteria described the required PICO components. A protocol was published before conducting the overview. The selection of eligible study designs was described. Study selection and data extraction were performed in duplicate. Citations for excluded reviews were listed. Included reviews were described in adequate detail for an overview. Risk of bias was reportedly low due to the limitation to Cochrane reviews only. Heterogeneity was addressed. The authors addressed funding and potential conflicts of interest for included reviews. The authors reported the source of funding for the overview and stated they had no conflicts of interest. | The authors explained that only Cochrane reviews were sought and included but did not elaborate on a justification as to why this decision was made. Search dates were not reported. Reasons for excluding individual reviews were not described. Risk of bias assessments was not described; the authors stated only that included reviews satisfied AMSTAR requirements. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = patient, intervention, comparator, outcome.
Table 6: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 213
Strengths | Limitations |
Abdel Shaheed et al. (2019)21 | |
The review’s eligibility criteria described the required PICO components. More than 2 electronic databases were searched. Reference lists of included studies were handsearched. The search was conducted less than 24 months before publication of the review. Study selection and data extraction were performed in duplicate. The risk of bias assessments were conducted for included studies. Publication bias was investigated and its potential impact on the meta-analyses was mentioned. The source of support for the review was reported and the authors declared no conflicts of interest. | There was no explicit mention of a protocol or methods established a priori. Rationales for limitation to RCTs only and English-language only were not included. There was no mention of grey literature searches, consultation with content experts, or searches of trial registries/databases Excluded studies were neither listed, nor were the reasons for ineligibility for individual studies described. Funding sources for included primary studies were not reported. Elaboration of heterogeneity (beyond reporting the I2 statistic) among included primary studies was not reported, nor was an explicit justification for conducting meta-analyses. The impact of risk of bias of included studies was not explicitly incorporated into the interpretation and conclusions. |
Abou-Atme et al. (2019)22 | |
The review’s eligibility criteria described the required PICO components. More than 2 electronic databases were searched. Reference lists of included studies were handsearched; grey literature and trial registry searches were conducted. The search was conducted less than 24 months before publication of the review. The search was not limited to English-only sources. The study selection was performed in duplicate. Risk of bias assessments were conducted for included studies. A rationale for not conducting meta-analyses was provided. The authors reported no funding in support of the review. | There was no explicit mention of a protocol or methods established a priori. Rationale for limitation to RCTs only was not included. Methods for data abstraction were not described. Excluded studies were neither listed, nor were the reasons for ineligibility described. Funding sources for included primary studies were not reported. The impact of risk of bias of included studies was not explicitly incorporated into the interpretation and conclusions. Conflicts of interest for the review co-authors were not reported. |
Au et al. (2015)23 | |
The research questions and inclusion criteria included the required PICO components. There is mention (but no description) of a protocol. More than 2 electronic databases were searched. No language or date limitations were put on the first round of the electronic database search. The study selection was performed in duplicate. A list of studies excluded in the third round of the search, including details as to the rationale for exclusion, was included. Some assessment and consideration of heterogeneity was reported. The authors reported no sources of support or funding, and no conflicts of interest. | There was no clear mention of an a priori method or design informing the review and eligibility and selection criteria appear to have been added iteratively. Rationale for limitations applied iteratively to the PICOS criteria was not included. Methods for data abstraction were not described. Neither a list of included studies, nor details describing the characteristics of included studies, were reported — findings were reported by drug combination. The reporting of outcome definitions and safety outcomes is unclear. The authors did not report an assessment of risk of bias. Funding sources for included primary studies were not reported (although an acknowledgement that some RCTs were funded by pharmaceutical companies is included). Elaboration of heterogeneity (beyond reporting the I2 statistic) among included primary studies was not reported. The impact of possible risk of bias of included studies was not incorporated into the interpretation and conclusions. |
Moore et al. (2013)24 | |
More than 2 electronic databases were searched. Some assessment/consideration of heterogeneity was reported Funding for the production of the report is described. | There was no explicit mention of a protocol or methods established a priori. Eligibility criteria were not clearly reported. Details of the search (e.g., keywords, strategy) were not reported. Rationale for limitation to RCTs only was not included. Methods for study selection and data abstraction were not described. Excluded studies were neither listed, nor were the reasons for ineligibility described. Neither a list of included studies, nor details describing the characteristics of included studies, were reported — findings were reported by drug combination. The authors did not report assessment of risk of bias. Elaboration of heterogeneity (beyond reporting the I2 statistic) among included primary studies was not reported. Impact of possible risk of bias of included studies was not incorporated into the interpretation/conclusions. Funding sources for included primary studies were not reported. One author reported sources of support, funding, and potential conflicts of interest without a description about how these were managed/mitigated. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = patient, intervention, comparator, outcome; RCT = randomized controlled trial.
Table 7: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist14
Strengths | Limitations |
Cattry et al. (2020)15 | |
Reporting
| Reporting
|
Internal validity (bias)
| Internal validity (bias)
|
Internal validity (confounding)
| Internal validity (confounding)
|
External validity
| |
da Silva et al. (2020)25 | |
Reporting
| External validity
|
Internal validity (bias)
| |
Internal validity (confounding)
| |
de Oliveira et al. (2018)29 | |
Reporting
| Reporting
|
Internal validity (confounding)
| Internal validity (confounding)
|
Internal validity (bias)
| External validity
|
Best et (al. (2017)26 | |
Reporting
| Reporting
|
Internal validity (confounding)
| Internal validity (confounding)
|
Internal validity (bias)
| External validity
|
Cristalli et al. (2017)28 | |
Reporting
| Reporting
|
Internal validity (bias)
| Internal validity (bias)
|
Internal validity (confounding)
| Internal validity (confounding)
|
External validity
| |
Santini et al. (2017)27 | |
Reporting
| Reporting
|
Internal validity (bias)
| Internal validity (bias)
|
Internal validity (confounding)
| Internal validity (confounding)
|
External validity
| |
Outhoff et al. (2015)30 | |
Reporting
| Reporting
|
Internal validity (bias)
| Internal validity (bias)
|
Internal validity (confounding)
| Internal validity (confounding)
|
External validity
| |
Reporting
| Reporting
|
Internal validity (bias)
| Internal validity (bias)
|
Internal validity (confounding)
| Internal validity (confounding)
|
External validity
| |
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Overviews of Systematic Reviews
Moore et al. (2015)20
Main study findings
The report described insufficient data and/or information describing codeine in the treatment of dental pain; i.e.:
“Within a review of ibuprofen plus codeine, we found information on one trial of an OTC combination product (Ibuprofen + codeine 2015), but concluded that the amount of information was too small to make the estimate of efficacy reliable.” (p11)
Authors’ conclusion
“The lack of any information on the efficacy of low dose codeine combination therapies is a major gap in knowledge. While the doses of codeine may be small in individual doses, this possibly represents substantial population consumption, and we need to know that there is some benefit in terms of analgesic efficacy in individuals as a balance to possible harm to the community.” (p13)
Moore et al. (2011)19
Main study findings
Efficacy: 50% maximum pain relief
Number (N) (%) patients achieving outcome
Codeine (60 mg): 79/573 (14)
Placebo: 52/573 (9)
Relative benefit (95% confidence interval [CI]: 1.5 (1.1 to 2.1)
NNT (95% CI): 21 (12 to 96)
Mean time to remedication (hour [hr]): < 3
Authors’ conclusion
No conclusions specific to codeine for the treatment of dental pain were reported.
Summary of Findings of Included Systematic Reviews and Meta-Analyses
Abdel Shaheed et al. (2019)21
Main study findings
Acute Nociceptive Pain (continuous pain scale, 0 to 100)
Immediate term (3 hr after single dose)
Mean difference (95% CI), pooled results (4 studies, N = 211 patients [pts]): –12.7 (–18.5 to –6.9)
Mean (standard deviation [SD]), 4 individual studies
Ibuprofen (200 mg) and codeine (15 mg)
Treatment (number [n] = 32 pts): 30.4 (22.2)
Placebo (n = 13 pts): 42.8 (22.2)
Ibuprofen (400 mg) and codeine (30 mg)
Treatment (n = 26 pts): 27.6 (22.2)
Placebo (n = 13 pts): 42.8 (22.2)
Ibuprofen (200 mg) and codeine (15 mg)
Treatment (n = 36 pts): 27.5 (22.2)
Placebo (n = 35 pts): 43.8 (22.2)
Acetylsalicylic acid (375 mg) and codeine (15 mg) and caffeine (30 mg)
Treatment (n = 30 pts): 15.0 (20.0)
Placebo (n = 26 pts): 23.8 (16.3)
Short-term (4 hr to 6 hr after a dose)
Mean difference (95% CI), pooled results (3 studies, N = 155 pts): ‒4.3 (‒11.6 to 3.0)
Mean (SD), 3 individual studies
Ibuprofen (200 mg) and codeine (15 mg)
Treatment (n = 32 pts): 28.5 (22.2)
Placebo (n = 13 pts): 32.0 (22.2)
Ibuprofen (400 mg) and codeine (30 mg)
Treatment (n = 26 pts): 20.8 (22.2)
Placebo (n = 13 pts): 32.0 (22.2)
Ibuprofen (200 mg) and codeine (15 mg)
Treatment (n = 36 pts): 30.0 (22.2)
Placebo (n = 35 pts): 31.3 (22.2)
12hr Follow-up
Mean (SD)
Paracetamol (1,000 mg) and codeine (60 mg)
Treatment (n = 44 pts): 15 (22.2)
Placebo (n = 85 pts): 46 (22.2)
Mean difference (95% CI), clinical significance (yes/no): ‒31.0 (‒39.1 to ‒22.9), yes
Paracetamol (500 mg) and codeine (30 mg)
Treatment (n = 43 pts): 30 (22.2)
Placebo (n = 85 pts): 46 (22.2)
Mean difference (95% CI), clinical significance (yes/no): ‒16.0 (‒24.1 to ‒7.9), yes
Safety
Adverse Events
Any
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tabs for post-operative dental pain
Treatment (n = 169 pts), n pts: 97
Placebo (n = 55 pts), n pts: 35
Relative risk (95% CI), statistical significance (yes/no): 0.90 (0.71 to 1.14), no
Paracetamol (500 mg) and codeine (15 mg), 2 tabs, for post-operative dental pain
Treatment (n = 113 pts), n pts: 72
Placebo (n = 55 pts), n pts: 35
Relative risk (95% CI), statistical significance (yes/no): 1.00 (0.78 to 1.28), no
Treatment-emergent
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tabs for post-operative dental pain
Treatment (n = 169 pts), n pts: 59
Placebo (n = 55 pts), n pts: 23
Relative risk (95% CI), statistical significance (yes/no): 0.83 (0.57 to 1.21), no
Paracetamol (500 mg) and codeine (15 mg), 2 tabs, for post-operative dental pain
Treatment (n = 113 pts), n pts: 45
Placebo (n = 55 pts), n pts: 23
Relative risk (95% CI), statistical significance (yes/no): 0.95 (0.65 to 1.40), no
Tiredness
Ibuprofen (200 mg) and codeine (15 mg) for post-operative dental pain
Treatment (n = 36 pts), n pts: 1
Placebo (n = 35 pts), n pts: 0
Relative risk (95% CI), statistical significance (yes/no): 2.92 (0.12 to 69.32), no
Nausea
Ibuprofen (200 mg) and codeine (15 mg) for post-operative dental pain
Treatment (n = 36 pts): 1
Placebo (n = 35 pts), n pts: 0
Relative risk (95% CI), statistical significance (yes/no): 2.92 (0.12 to 69.32), no
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tablets for post-operative dental pain
Treatment (n = 169 pts), n pts: 50
Placebo (n = 55 pts), n pts: 18
Relative risk (95% CI), statistical significance (yes/no): 0.90 (0.58 to 1.41), no
Paracetamol (500 mg) and codeine (15 mg), 2 tablets, for post-operative dental pain
Treatment (n = 113 pts), n pts: 37
Placebo (n = 55 pts), n pts: 18
Relative risk (95% CI), statistical significance (yes/no): 1.00 (0.63 to 1.59), no
Dizziness
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tablets for post-operative dental pain
Treatment (n = 169 pts), n pts: 23
Placebo (n = 55 pts), n pts: 3
Relative risk (95% CI), statistical significance (yes/no): 2.50 (0.78 to 7.99), no
Paracetamol (500 mg) and codeine (15 mg), 2 tablets, for post-operative dental pain
Treatment (n = 113 pts), n pts: 14
Placebo (n = 55 pts), n pts: 3
Relative risk (95% CI), statistical significance (yes/no): 2.27 (0.68 to 7.58), no
Cold sweats and dizziness
Acetylsalicylic acid (375 mg) and codeine (15 mg) and caffeine (30 mg) for post-operative dental pain
Treatment (n = 26 pts), n pts: 0
Placebo (n = 30 pts), n pts: 3
Relative risk (95% CI), statistical significance (yes/no): 0.38 (0.04 to 3.48), no
Gastrointestinal (GI) upset
Acetylsalicylic acid (375 mg) and codeine (15 mg) and caffeine (30 mg) for post-operative dental pain
Treatment (n = 26 pts), n pts: 3
Placebo (n = 30 pts), n pts: 0
Relative risk (95% CI), statistical significance (yes/no): 8.04 (0.43 to 148.71), no
Vomiting
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tabs for post-operative dental pain
Treatment (n = 169 pts), n pts: 35
Placebo (n = 55 pts), n pts: 13
Relative risk (95% CI), statistical significance (yes/no): 0.88 (0.50 to 1.53), no
Paracetamol (500 mg) and codeine (15 mg), 2 tablets, for post-operative dental pain
Treatment (n = 113 pts), n pts: 25
Placebo (n = 55 pts), n pts: 13
Relative risk (95% CI), statistical significance (yes/no): 0.94 (0.52 to 1.68), no
Headache
Ibuprofen (200 mg) and codeine (12.8 mg), 2 tablets for post-operative dental pain
Treatment (n = 169 pts), n pts: 32
Placebo (n = 55 pts), n pts: 10
Relative risk (95% CI), statistical significance (yes/no): 1.04 (0.55 to 1.98), no
Paracetamol (500 mg) and codeine (15 mg), 2 tablets, for post-operative dental pain
Treatment (n = 113 pts), n pts: 21
Placebo (n = 55 pts), n pts: 10
Relative risk (95% CI), statistical significance (yes/no): 1.02 (0.52 to 2.02), no
Authors’ conclusion
“There is low to moderate level evidence that combination analgesic products containing low-dose codeine provide small to moderate pain relief for acute and chronic pain conditions in the immediate short-term with limited trial data on use beyond 24 hours. Further research examining regular use of these medicines is needed with more emphasis on measuring potential harmful effects.” (p836)
Abou-Atme et al. (2019)22
Main study findings
Post-operative pain
Data reported quantitatively
6 hr post-operatively, visual analogue score (VAS) score (0 to 10)
Acetaminophen (300 mg) and codeine (30 mg): 4.39
Acetaminophen (300 mg) and caffeine (20 mg): 6.06
Difference b/w groups (clinical/statistical significance): 1.67 (not reported [NR])
Information reported qualitatively only
3 hr, 6 hr, 12 hr post-operatively (clinical/statistical significance)
Pain lower in the combination acetaminophen (300 mg) and codeine (30 mg) group (NR)
All other follow-up intervals (clinical/statistical significance)
No difference in reported level of pain between treatment groups.
Authors’ conclusion
“The results of the studies included in this review suggest that the combination of acetaminophen and caffeine is... slightly inferior to acetaminophen and codeine.” (p421)
Au et al. (2015)23
Main study findings
Post-operative pain intensity
Sum of pain intensity difference at 6 hours [SPID6], mean (SD) a
Acetaminophen (650 mg) and codeine phosphate (60 mg) versus (vs.) placebo, 1 study (N = 31 pts): 4.66 (1.65)
Acetaminophen (600 mg) and codeine phosphate (60 mg) vs. placebo, 2 studies (N = 75 pts): 4.48 (0.84)
Acetaminophen acid (300 mg) and codeine phosphate (30 mg) vs. placebo, 2 studies (N = 255 pts): 3.47 (2.01)
Acetaminophen (1 g) and codeine phosphate (30 mg) vs. placebo, 1 study (N = 113 pts): 1.00 (0.14)
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 38 pts): 2.2 (0.4)
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital, (50 mg) and codeine phosphate (15 mg) vs. placebo, 1 study (N = 41 pts): 3.46 (0.37)
Ibuprofen (400 mg) and codeine phosphate (25.6 mg) vs. placebo, 1 study (N = 169 pts): 1.23 (0.14)
Adjusted SPID6, calculated mean
Acetaminophen (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 31 pts): 3.01
Acetaminophen (600 mg) and codeine phosphate (60 mg) vs. placebo, 3 studies (N = 75 pts): 3.64
Acetaminophen (300 mg) and codeine phosphate (30 mg) vs. placebo, 2 studies (N = 255 pts): 1.46
Acetaminophen (1 g) and codeine phosphate (30 mg) vs. placebo, 1 study (N = 113 pts): 0.86
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 38 pts): 1.80
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg) and codeine phosphate (15 mg) vs. placebo, 1 study (N = 41 pts): 3.09
Ibuprofen (400 mg) and codeine phosphate (25.6 mg) vs. placebo, 1 study (N = 169 pts): 1.09
Post-operative pain relief
Total pain relief at 6 hours (TOTPAR6), mean (SD)a
Acetaminophen (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 31 pts): 13.37 (8.3)
Acetaminophen (600 mg) and codeine phosphate (60 mg) vs. placebo, 2 studies (N = 75 pts): 10.28 (4.08)
Acetaminophen (300 mg) and codeine phosphate (30 mg) vs. placebo, 2 studies (N = 255 pts): 6.51 (3.27)
Acetaminophen (1 g) and codeine phosphate (30 mg) vs. placebo, 1 study (N = 113 pts): 1.87 (0.44)
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 38 pts): 6.9 (2.5)
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg) vs. placebo, 1 study (N = 41 pts): 9.07 (2.37)
Ibuprofen (400 mg) and codeine phosphate (25.6 mg) vs. placebo, 1 study (N = 169 pts): 2.23 (0.44)
Adjusted TOTPAR6, mean
Acetaminophen (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 31 pts): 5.07
Acetaminophen (600 mg) and codeine phosphate (60 mg) vs. placebo, 2 studies (N = 75 pts): 6.20
Acetaminophen (300 mg) and codeine phosphate (30 mg) vs. placebo, 2 studies (N = 255 pts): 3.24
Acetaminophen (1 g) and codeine phosphate (30 mg) vs. placebo, 1 study (N = 113 pts): 1.43
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg) vs. placebo, 1 study (N = 38 pts): 4.40
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg) vs. placebo, 1 study (N = 41 pts): 6.70
Ibuprofen (400 mg) and codeine phosphate (25.6 mg) vs. placebo, 1 study (N = 169 pts): 1.79
Safety
Adverse event (AEs), % pts experiencing the outcome
Drowsiness
Acetaminophen (650 mg) and codeine phosphate (60 mg), n = 31 pts: 9.70
Acetaminophen (600 mg) and codeine phosphate (60 mg), n = 48 pts: 6.25
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 1.46
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg), n = 39 pts: 9.80
Dizziness
Acetaminophen (600 mg) and codeine phosphate (60 mg), n = 48 pts: 4.16
Acetaminophen (300 mg) and codeine phosphate (3 0mg), n = 274 pts: 2.12
Acetaminophen (1 g) and codeine phosphate (30 mg), n = 113 pts: 12.40
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg), n = 39 pts: 4.90
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 6.25
Ibuprofen (400 mg) and codeine phosphate (25.6 mg), n = 169 pts: 12.40
Earache
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.00
Headache
Acetaminophen (650 mg) and codeine phosphate (60 mg), n = 31 pts: 9.70
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 0.70
Acetaminophen (1 g) and codeine phosphate (30 mg), n = 113 pts: 18.60
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg), n = 39 pts: 22
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.00
Ibuprofen (400 mg) and codeine phosphate (25.6 mg), n = 169 pts: 18.60
Nausea
Acetaminophen (650 mg) and codeine phosphate (60 mg), n = 31 pts: 9.70
Acetaminophen (600 mg) and codeine phosphate (60 mg), n = 48 pts: 10.40
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 11
Acetaminophen (1 g) and codeine phosphate (30 mg), n = 113 pts: 32.70
Acetylsalicylic acid (650 mg) and codeine phosphate (60 mg), n = 39 pts: 19.50
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.01
Ibuprofen (400 mg) and codeine phosphate (25.6 mg), n = 169 pts: 32.70
Numbness in the legs
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 0.36
Dry mouth
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 0.70
Hot feeling
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.01
Sweating
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg) and codeine phosphate (15 mg), n = 48 pts: 2.01
Restlessness
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.01
Tiredness
Acetylsalicylic acid (325 mg), caffeine (40 mg), butalbital (50 mg), and codeine phosphate (15 mg), n = 48 pts: 2.01
Rash
Acetaminophen (300 mg) and codeine phosphate (30 mg), n = 274 pts: 0.36
a Note: The authors did not specify whether parenthesized values were standard deviation, so an assumption on the part of the review author was made.
Authors’ conclusion
No conclusions specific to codeine in the treatment of dental pain were reported.
Moore et al. (2013)24
Main study findings
Pain relief
Achievement of 50% maximum (max) total pain relief (TOTPAR), % patients
Paracetamol (1,000) and codeine (base15) and doxylamine succinate (10) vs. placebo
Active: 21
Placebo: 8
Relative benefit of active treatment (95% CI): 2.7 (1.8 to 4.8)
Ibuprofen (400) and codeine (25.6) vs. placebo:
Active: 62
Placebo: 2
Relative benefit of active treatment (95% CI): 34 (4.9 to 23.9)
Paracetamol (1,000) and caffeine (50) and codeine (base13) vs. placebo
Active: 29
Placebo: 4
Relative benefit of active treatment (95% CI): 6.2 (0.9 to 45)
Number needed to treat (NNT) (95% CI)
Paracetamol (1,000) and codeine (base15) and doxylamine succinate (10) vs. placebo: NR
Ibuprofen (400) and codeine (25.6) vs. placebo: 1.7 (1.5 to 1.9)
Paracetamol (1,000) and caffeine (50) and codeine (base13) vs. placebo: 4.2 (2.5 to 14)
Success rate (categorical range by %, reported graphically only)
Paracetamol (1,000) and codeine (base15) and doxylamine succinate (10) vs. placebo: NR
Ibuprofen (400) and codeine (25.6) vs. placebo: NR
Paracetamol (1,000) and caffeine (50) and codeine (base13) vs. placebo: 20 to 30
Failure rate (categorical range by %, reported graphically only)
Paracetamol (1,000) and codeine (base15) and doxylamine succinate (10) vs. placebo: NR
Ibuprofen (400) and codeine (25.6) vs. placebo: NR
Paracetamol (1,000) and caffeine (50) and codeine (base13) vs. placebo: 70 to 80
Authors’ conclusion
“In general, OTC [over-the counter] analgesics containing codeine tended to use significantly lower doses of codeine and higher doses of other constituents; presumably to minimise codeine-related side effects.” (p23)
“Combination analgesics with ibuprofen (paracetamol or codeine) had the highest success rates in acute pain studies.” (p24)
Summary of Findings of Included Primary Clinical Studies
Cattry et al. (2020)15
Main study findings
Efficacy
Study 1
Pain severity — SPID, least mean square (SD): a statistically significant superiority to placebo; b statistically significant superiority to active comparator
4 hr
Naproxen sodium (440 mg): 2.6 (3.1)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1.9 (3.1) a
Placebo: ‒0.5 (3.2)
6 hr
Naproxen sodium (440 mg): 3.6 (4.6) a,b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.1 (4.6)a
Placebo: ‒0.8 (4.6)
8 hr
Naproxen sodium (440 mg): 4.3 (6.0)a,b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.1 (6.0) a
Placebo: −1.0 (3.2)
Pain relief — TOTPAR, least mean square (SD): a statistically significant superiority to placebo; b statistically significant superiority to active comparator
4 hr
Naproxen sodium (440 mg): 6.6 (4.7) a,b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 5.1 (4.6)a
Placebo: 1.3 (4.7)
6 hr
Naproxen sodium (440 mg): 9.4 (6.8) a, b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 6.2 (6.9) a
Placebo: 1.9 (6.9)
8 hr
Naproxen sodium (440 mg): 11.5 (8.9)a, b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 6.9 (8.9)a
Placebo: 2.5 (9.1)
Peak pain intensity difference (PID), least mean square (SD): a statistically significant superiority to placebo
Naproxen sodium (440 mg): 1.1 (1.0)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0.9 (1.0)a
Placebo: 0.1 (0.9)
Peak pain relief, least mean square (SD): a statistically significant superiority to placebo
Naproxen sodium (440 mg): 2.4 (1.4)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.2 (1.4)a
Placebo: 0.7 (1.4)
Median time to onset of some relief (hr): a statistically significant superiority to placebo, b statistically significant superiority to active comparator)
Naproxen sodium (440 mg): 1.0a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1.0a
Placebo: > 8
Median time to rescue (hr): a statistically significant superiority to placebo; b statistically significant superiority to active comparator)
Naproxen sodium (440 mg): 5.9a,b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 3.4a
Placebo: 1.1
Patients who took backup medication, n (%)
Naproxen sodium (440 mg): 56 (62)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 77 (85)
Placebo: 40 (91)
Global evaluation for pain relief, % pts
Naproxen sodium (440 mg):
Good, Very Good, Excellent: 59
Poor, Fair: 41
Acetaminophen (600 mg) and codeine phosphate (60 mg)
Good, Very Good, Excellent: 45
Poor, Fair: 55
Placebo
Good, Very Good, Excellent: 12
Poor, Fair: 89
Study 2
Pain severity — SPID, least mean square (SD): a statistically significant superiority to placebo
4 hr
Naproxen sodium (440 mg): 1.4 (2.8)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1.7 (2.7)a
Placebo: –1.4 (2.8)
6 hr
Naproxen sodium (440 mg): 2.2 (4.4)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.0 (3.9)a
Placebo: –2.2 (4.5)
8 hr
Naproxen sodium (440 mg): 2.8 (6.0)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.0 (4.9)a
Placebo: –3.2 (5.7)
Pain relief — TOTPAR, least mean square (SD); a statistically significant superiority to placebo; b statistically significant superiority to active comparator
4 hr
Naproxen sodium (440 mg): 5.8 (4.4)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 5.4 (4.2)a
Placebo: 1.6 (3.0)
6 hr
Naproxen sodium (440 mg): 8.7 (7.1)a, b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 7.0 (6.1)a
Placebo: 2.2 (4.6)
8 hr
Naproxen sodium (440 mg): 11.1 (9.7)a, b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 8.1 (7.8)a
Placebo: 2.5 (5.9)
Peak PID, least mean square (SD): a statistically significant superiority to placebo
Naproxen sodium (440 mg): 0.8 (0.9)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0.9 (0.7)a
Placebo: 0.0 (0.9)
Peak pain relief, least mean square (SD): a statistically significant superiority to placebo
Naproxen sodium (440 mg): 2.2 (1.5)a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2.2 (1.2)a
Placebo: 0.9 (1.2)
Median time to onset of some relief (hr): a statistically significant superiority to placebo); b statistically significant superiority to active comparator
Naproxen sodium (440 mg): 2.0a
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1.0a,b
Placebo: > 8
Median time to rescue (hr); a statistically significant superiority to placebo; b statistically significant superiority to active comparator
Naproxen sodium (440 mg): 6.5a, b
Acetaminophen (600 mg) and codeine phosphate (60 mg): 3.7a
Placebo: 1.5
Patients who took backup medication, n (%)
Naproxen sodium (440 mg): 51 (55)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 70 (77)
Placebo: 45 (96)
Global evaluation for pain relief, % ptsa
Naproxen sodium (440 mg):
Good, Very Good, Excellent: 59
Poor, Fair: 40
Acetaminophen (600 mg) and codeine phosphate (60 mg)
Good, Very Good, Excellent: 54
Poor, Fair: 47
Placebo
Good, Very Good, Excellent: 13
Poor, Fair: 87
Note: Proportion values for groups per treatment arm do not always add to 100 because of rounding.
Safety
AEs, n pts (%) reporting at least 1 occurrence
Study 1
Any body system
Naproxen sodium (440 mg): 6 (7)
Acetaminophen (600 mg) and codeine phosphate (60 mg)
23 (25)
Difference between naproxen sodium (440 mg) and placebo groups: P ≤ 0.02
Placebo: 4 (9)
Nausea
Naproxen sodium (440 mg): 1 (1)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 8 (9)
Placebo: 1 (2)
Vomiting
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 5 (5)
Placebo: 1 (2)
Dizziness
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 7 (8)
Placebo: 1 (2)
Somnolence
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 7 (8)
Placebo: 0
Headache
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1 (1)
Placebo: 1 (2)
Nervousness
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 0
Syncope
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1 (1)
Placebo: 0
Dyspepsia
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 1 (1)
Placebo: 0
Infection
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 0
Rash
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 0
Study 2
Any body system
Naproxen sodium (440 mg): 28 (30)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 37 (41)
Placebo: 25 (53)
Nausea
Naproxen sodium (440 mg): 11 (12)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 21 (23)
Placebo: 12 (26)
Vomiting
Naproxen sodium (440 mg): 7 (8)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 12 (13)
Placebo: 8 (17)
Dizziness
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 11 (12)
Difference vs. naproxen sodium (440 mg): P = 0.01
Placebo: 5 (11)
Somnolence
Naproxen sodium (440 mg): 5 (5)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 13 (14)
Difference vs. naproxen sodium (440 mg): P = 0.053
Placebo: 4 (9)
Headache
Naproxen sodium (440 mg): 7 (8)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 5 (5)
Placebo: 6 (13)
Nervousness
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 2 (4)
Syncope
Naproxen sodium (440 mg): 0
Acetaminophen (600 mg) and codeine phosphate (60 mg): 2 (2)
Placebo: 0
Dyspepsia
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 0
Infection
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 0
Rash
Naproxen sodium (440 mg): 2 (2)
Acetaminophen (600 mg) and codeine phosphate (60 mg): 0
Placebo: 1 (2)
Authors’ conclusion
“These studies provide dental and medical professionals with scientific evidence of the superior efficacy and safety of nonprescription doses of naproxen sodium compared to the combination of acetaminophen and codeine phosphate in the treatment of post-operative dental pain. Naproxen sodium can be prescribed as an alternative pain treatment to opioids for dental pain and should be considered as first-line therapy for acute pain management.” (p111)
da Silva et al. (2020)25
Main study findings
Efficacy
Pain, VAS (0 to 100), median (25th/75th percentiles)
Initial
Paracetamol (1,000 mg): 85 (65/91)
Paracetamol (1,000 mg) and codeine (30 mg): 82 (63/98)
Difference between groups, Mann–Whitney U test: P = 0.877
6 hr
Paracetamol (1,000 mg): 45 (8/78)
Paracetamol (1,000 mg) and codeine (30 mg): 52 (22/75)
Difference between groups, Mann–Whitney U test: P = 0.332
12 hr
Paracetamol (1,000 mg): 25 (5/69)
Paracetamol (1,000 mg) and codeine (30 mg): 36 (10/70)
Difference between groups, Mann–Whitney U test: P = 0.545
24 hr
Paracetamol (1,000 mg): 24 (1/54)
Paracetamol (1,000 mg) and codeine (30 mg): 25 (10/64)
Difference between groups, Mann–Whitney U test: P = 0.608
48 hr
Paracetamol (1,000 mg): 15 (0/44)
Paracetamol (1,000 mg) and codeine (30 mg): 18 (5/35)
Difference between groups, Mann–Whitney U test: P = 0.607
72 hr
Paracetamol (1,000 mg): 0 (0/24)
Paracetamol (1,000 mg) and codeine (30 mg): 5 (0/17)
Difference between groups, Mann–Whitney U test: P = 0.246
Safety
AEs, n cases
Dizziness
Paracetamol (1,000 mg): 1
Paracetamol (1,000 mg) and codeine (30 mg): 3
Difference between groups, Chi-square test: P = 0.606
Number needed to harm (NNH) for paracetamol (1,000 mg) and codeine (30 mg): 10
Drowsiness
Paracetamol (1,000 mg): 3
Paracetamol (1,000 mg) and codeine (30 mg): 7
Difference between groups, Chi-square test: P = 0.278
NNH for paracetamol (1,000 mg) and codeine (30 mg): 5
Nausea
Paracetamol (1,000 mg): 2
Paracetamol (1,000 mg) and codeine (30 mg): 8
Difference between groups, Chi-square test: P = 0.067
NNH for paracetamol (1,000 mg) and codeine (30 mg): 3.4
Headache
Paracetamol (1,000 mg): 4
Paracetamol (1,000 mg) and codeine (30 mg): 3
Difference between groups, Chi-square test: P = 0.494
NNH for paracetamol (1,000 mg): 16.7
Emesis
Paracetamol (1,000 mg): 0
Paracetamol (1,000 mg) and codeine (30 mg): 2
Difference between groups, Chi-square test: P = 0.488
NNH for paracetamol (1,000 mg) and codeine (30 mg): 10
Other
Paracetamol (1,000 mg): 3
Paracetamol (1,000 mg) and codeine (30 mg): 4
Difference between groups, Chi-square test: P = 0.432
NNH for paracetamol (1,000 mg) and codeine (30 mg): 25
Authors’ conclusion
“Both medications were effective for pain control in acute apical abscess cases.” (p1)
“Our results revealed that both groups were similar regarding the frequency of adverse effects... However, NNH calculation demonstrated that isolated acetaminophen is more advantageous because from 47.6 patients administering acetaminophen association at least one adverse effect more than isolated might report.” (p7)
de Oliveira et al. (2018)29
Main study findings
Sensitivity
Global immediate sensitivity, analogue visual scale of pain (EVA), mean (SD)
Paracetamol (500 mg) and codeine (30 mg): 1.0 (0.2)
Ibuprofen (400 mg): 4.8 (0.9)
Placebo: 4.7 (1.0)
Difference between paracetamol (500 mg) and codeine (30 mg) vs. ibuprofen (400 mg), analysis of variance (ANOVA) and Tukey’s post-hoc tests: P < 0.01
Difference between paracetamol (500 mg) and codeine (30 mg) vs. placebo, method NR, ANOVA and Tukey’s post-hoc tests: P < 0.01
Authors’ conclusion
“The use of codeine + paracetamol 1 hour before in-office tooth bleaching can drastically reduce immediate sensitivity.” (p195)
Best et al. (2017)26
Main study findings
Efficacy
Post-operative pain
VAS scores
Presented graphically only
Authors report narratively that there were no significant differences between groups.
Post-operative pain questionnaire, Global Pain Level
Paracetamol (1,000 mg) and ibuprofen (400 mg) and codeine (60 mg), n (%)
No pain: 7 (10.9)
Mild: 37 (57.8)
Moderate: 16 (25.9)
Severe: 3 (4.7)
Excruciating (agony): 1 (1.6)
Paracetamol (1,000 mg) and ibuprofen (400 mg), n (%)
No pain: 6 (9.0)
Mild: 30 (44.8)
Moderate: 25 (37.3)
Severe: 5 (7.5)
Excruciating (agony): 1 (1.5)
Difference b/w groups: P = 0.52
Linear mixed model results
Pain scores statistically significantly associated with reported baseline pain level
Pain scores increased (i.e., worsened) over time
No differences in pain levels between groups
Use of rescue medication, n (%) pts
Paracetamol (1,000 mg) and ibuprofen (400 mg) and codeine (60 mg) (n = 64): 1 (1.6)
Paracetamol (1,000 mg) and ibuprofen (400 mg) (n = 67): 2 (3.0)
Authors’ conclusion
“This study confirmed the hypothesis that the addition of codeine 60 mg every 6 hours to a regimen of paracetamol 1,000 mg every 6 hours and ibuprofen 400 mg every 8 hours does not improve analgesia after mandibular third molar surgery involving bone removal.” (p2068)
Cristalli et al. (2017)28
Main study findings
Efficacy
Post-operative pain intensity
Numerical Rating Scale-11 score, mean (SD)
Day 1
Paracetamol (500 mg) and codeine (30 mg): 3.18 (2.18)
Placebo: 4.65 (2.73)
Difference between groups: P = 0.001
Day 2
Paracetamol (500 mg) and codeine (30 mg): 2.22 (1.88)
Placebo: 2.53 (2.12)
Difference between groups: P = 0.134
Day 3
Paracetamol (500 mg) and codeine (30 mg): 1.81 (1.77)
Placebo: 2.01 (2.31)
Difference between groups: P = 0.468
Pain scores comparison by receipt of intervention or placebo in the first or second procedures, respectively, mean (SD)
Paracetamol (500 mg) and codeine (30 mg) in the first surgery: 3.05 (1.75)
Paracetamol (500 mg) and codeine (30 mg) in the second surgery: 2.09 (2.02)
Difference between groups receiving paracetamol (500 mg) and codeine (30 mg) in the first vs. second procedure: P = 0.419
Placebo in the first surgery: 3.48 (2.62)
Placebo in the second surgery: 5.48 (2.52)
Difference between groups receiving placebo in the first vs. second procedure: P = 0.011
Minutes to first post-operative use of analgesic medication, mean (SD)
Paracetamol (500 mg) and codeine (30 mg): 414.33 (131.26)
Placebo: 288.67 (116.63)
Difference between groups: P = 0.004
Rescue medication
Use of rescue medication, n pts
Paracetamol (500 mg) and codeine (30 mg): 8
Placebo: 6
Difference b/w groups: P = 0.364
Number of rescue medication tablets taken, mean (SD)
Paracetamol (500 mg) and codeine (30 mg): 1.24 (1.82)
Placebo: 1.47 (1.66)
Difference b/w groups: P = 0.104
Safety
Adverse events recorded at 1wk: None reported among any study patients.
Authors’ conclusion
“The preoperative administration of paracetamol-codeine significantly reduced the intensity of postoperative pain and increased the time to the first request of rescue therapy compared to placebo.” (p5)
Santini et al. (2017)27
Main study findings
Efficacy
Pain
VAS (0 to 100 mm), median (25th/75th percentiles)
Initial
Codeine (30 mg) and acetaminophen (500 mg): 90.5 (71.25/100)
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 88.5 (74.25/99.5)
Difference between groups, Mann–Whitney U test: P = 0.733
6 hr
Codeine (30 mg) and acetaminophen (500 mg): 10.5 (0/60.5)
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 9.5 (0.5/62.25)
Difference between groups, Mann–Whitney U test: P = 0.59
12 hr
Codeine (30 mg) and acetaminophen (500 mg): 6 (0/36.5)
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 5.5 (0/62.5)
Difference between groups, Mann–Whitney U test: P = 0.545
48 hr
Codeine (30 mg) and acetaminophen (500 mg): 0 (0/7.7)
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 0.5 (0/28)
Difference between groups, Mann–Whitney U test: P = 0.312
72hr
Codeine (30 mg) and acetaminophen (500 mg): 0 (0/4)
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 0 (0/20)
Difference between groups, Mann–Whitney U test: P = 0.427
Use of additional medication, % pts
Codeine (30 mg) and acetaminophen (500 mg): 40
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 40
Number of additional tablets taken, average
Codeine (30 mg) and acetaminophen (500 mg): 1.5
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 1.6
Safety
Adverse reactions, n pts
Dizziness
Codeine (30 mg) and acetaminophen (500 mg): 5
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 4
Difference between groups, Chi-square test: P = 0.999
Drowsiness
Codeine (30 mg) and acetaminophen (500 mg): 8
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 6
Difference between groups, Chi-square test: P = 0.628
Nausea
Codeine (30 mg) and acetaminophen (500 mg): 6
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 4
Difference between groups, Chi-square test: P = 0.656
Headache
Codeine (30 mg) and acetaminophen (500 mg): 1
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 1
Difference between groups, Chi-square test: P = 0.999
Emesis
Codeine (30 mg) and acetaminophen (500 mg): 2
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 2
Difference between groups, Chi-square test: P = 0.999
Others
Codeine (30 mg) and acetaminophen (500 mg): 1
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 0
Difference between groups, Chi-square test: P = 0.999
NNH
Codeine (30 mg) and acetaminophen (500 mg): 1.25
Tramadol hydrochloride (37.5 mg) and acetaminophen (500 mg): 1.25
Authors’ conclusion
“The present randomized clinical trial indicated that Tr/Ac [tramadol hydrochloride 37.5 mg and acetaminophen 500 mg] and Co/Ac [codeine 30 mg and acetaminophen 500 mg] treatment presented similar analgesic efficacy when used to control pain caused by APA [acute periradicular abscess].” (p557)
Outhoff et al. (2015)30
Main study findings
Efficacy
Pain intensity
SPID (from baseline), mean (SD)
3 hr following first dose
Stilpane: –3.46 (1.64)
Tramacet: –3.05 (2.12)
Difference between groups: P = 0.6878
6 hr following first dose
Stilpane: –6.58 (14.10)
Tramacet: –3.51 (20.05)
Difference between groups: P = 0.3873
48 hr (± 24hr) following first dose
Stilpane: –86.54 (36.36)
Tramacet: –90.14 (39.65)
Difference between groups: P = 0.3001
5 days (d) (± 2d) following first dose
Stilpane: –252.69 (86.99)
Tramacet: –250.14 (91.57)
Difference between groups: P = 0.5436
VAS (0 to 100mm), difference from baseline, mean (SD)
3 hr following first dose
Stilpane: –55.32 (24.21)
Tramacet: –52.38 (23.28)
Difference between groups: P = 0.8931
6 hr following first dose
Stilpane: –61.25 (27.67)
Tramacet: –60.76 (23.05)
Difference between groups: P = 0.7862
48 hr (± 24hr) following first dose
Stilpane: –68.02 (23.74)
Tramacet: –71.21 (15.95)
Difference between groups: P = 0.0960
5 d (± 2d) following first dose
Stilpane: –73.50 (20.59)
Tramacet: –70.63 (20.84)
Difference between groups: P = 0.8572
Pain relief
Assessment of total pain relief (TOTPAR) from baseline, mean (SD)
3 hr following first dose
Stilpane: 5.58 (1.58)
Tramacet: 5.54 (1.93)
Difference between groups: P = 0.9204
6 hr following first dose
Stilpane: 15.52 (13.59)
Tramacet: 17.88 (19.22)
Difference b/w groups: P = 0.4782
48hr (± 24hr) following first dose
Stilpane: 145.56 (44.06)
Tramacet: 157.0 (30.83)
Difference between groups: P = 0.1387
5d (± 2d) following first dose:
Stilpane: 413.25 (96.35)
Tramacet: 430.33 (80.34)
Difference between groups: P = 0.3401
Pain intensity and relief
Sum of hourly pain relief and hourly pain intensity difference (SPRID) from baseline, mean (SD)
3 hr following first dose
Stilpane: 2.45 (1.72)
Tramacet: 2.82 (2.06)
Difference between groups: P = 0.9656
6 hr following first dose
Stilpane: 9.28 (27.02)
Tramacet: 14.70 (38.69)
Difference between groups: P = 0.3925
48 hr (± 24hr) following first dose
Stilpane: 59.36 (43.10)
Tramacet: 67.20 (43.83)
Difference between groups: P = 0.7348
5d (± 2d) following first dose
Stilpane: 160.89 (93.12)
Tramacet: 180.53 (78.64)
Difference between groups: P = 0.7432
Patient-reported medication efficacy
Poor to excellent, % pts
6 hr following first dose
Stilpane: Excellent = 22; Very good = 40; Good = 33; Fair = 4; Poor = 2
Tramacet: Excellent = 10; Very good = 38; Good = 38; Fair = 13; Poor = 2
Difference between groups: Reported narratively as not statistically significant
Time to pain relief
Perceptible pain relief at 1hr, % pts
Stilpane: approximately 70
Tramacet: approximately 70
Meaningful pain relief at 1 hr, % pts
Stilpane: approximately 35
Tramacet: approximately 35
Safety
Adverse reactions, % pts
Nausea
Stilpane: 9.6
Tramacet: 12.5
Vomiting
Stilpane: 5.8
Tramacet: 6.3
Somnolence
Stilpane: 15.4
Tramacet: 14.6
Dizziness
Stilpane: 1.9
Tramacet: 6.3
Headache
Stilpane: 1.9
Tramacet: 2.1
Insomnia
Stilpane: 1.9
Tramacet: 2.1
Pruritus
Stilpane: 5.8
Tramacet: 2.1
Rash
Stilpane: 0
Tramacet: 4.2
Authors’ conclusion
“Despite their distinctive compositions and mechanisms of action, Stilpane® and Tramacet® are equally effective and well-tolerated combination analgesics in eligible patients experiencing moderate to severe acute pain.” (p22)
Brown et al. (2013)16
Main study findings
Efficacy
Post-operative pain:
Daily recall of average pain, (0 to 10 scale), difference from placebo, least squares mean (95% CI)
Etoricoxib (120 mg)
Day 2: –1.40 (–2.09 to –0.71)
Day 3: –0.61 (–1.44 to –0.12)
Etoricoxib (90 mg):
Day 2: –1.29 (–1.92 to –0.66)
Day 3: –0.78 (–1.22 to 0.00)
Ibuprofen (2,400 mg)
Day 2: –1.11 (–1.75 to –0.48)
Day 3: –0.28 (–0.89 to –0.33)
Acetaminophen (600 mg) and codeine (60 mg)
Day 2: –0.87 (–1.63 to –0.11)
Day 3: –0.45 (–1.18 to 0.29)
Daily recall of worst pain on days 2 and 3, (0 to 10 scale), difference from placebo, least squares mean (95% CI)
Etoricoxib (120 mg)
Day 2: –1.42 (–2.42 to –0.43)
Day 3: –0.37 (–1.22 to 0.49)
Etoricoxib (90 mg)
Day 2: –0.97 (–1.89 to –0.06)
Day 3: –0.78 (–1.71 to 0.14)
Ibuprofen (2,400 mg)
Day 2: –0.79 (–1.71 to 0.12)
Day 3: 0.21 (–0.65 to 1.06)
Acetaminophen (600 mg) and codeine (60 mg)
Day 2: –0.48 (–1.58 to 0.62)
Day 3: –0.62 (–1.65 to 0.40)
Self-reported medication effectiveness:
Patient’s global assessment of study medication on day 2, % pts
Etoricoxib (120 mg)
Excellent: 34
Very good: 33
Good: 17
Fair: 12
Poor: 4
Etoricoxib (90 mg)
Excellent: 30
Very good: 39
Good: 19
Fair: 8
Poor: 5
Ibuprofen (2,400 mg)
Excellent: 25
Very good: 39
Good: 21
Fair: 11
Poor: 4
Acetaminophen (600 mg) and codeine (60 mg)
Excellent: 15
Very good: 31
Good: 33
Fair: 18
Poor: 4
Placebo
Excellent: 11
Very good: 5
Good: 14
Fair: 27
Poor: 43
Patient’s global assessment of study medication on day 3, % pts
Etoricoxib (120 mg)
Excellent: 36
Very good: 31
Good: 21
Fair: 7
Poor: 6
Etoricoxib (90 mg)
Excellent: 30
Very good: 41
Good: 17
Fair: 7
Poor: 5
Ibuprofen (2,400 mg)
Excellent: 26
Very good: 34
Good: 26
Fair: 10
Poor: 5
Acetaminophen (600 mg) and codeine (60 mg)
Excellent: 15
Very good: 32
Good: 32
Fair: 19
Poor: 2
Placebo
Excellent: 12
Very good: 7
Good: 9
Fair: 30
Poor: 42
Use of rescue medication on day 2, n pts (%)
Etoricoxib (120 mg): 17 (17.7)
Etoricoxib (90 mg): 43 (22.6)
Ibuprofen (2,400 mg): 44 (22.9)
Acetaminophen (600 mg) and codeine (60 mg)
13 (23.2):
Difference compared to placebo, odds ratio (95% CI), statistical significance, yes/no: 0.23 (0.10 to 0.54), yes
Placebo
26 (55.6)
Use of rescue medication on day 3, % pts
Etoricoxib (120 mg): 16 (16.7)
Etoricoxib (90 mg): 26 (13.8)
Ibuprofen (2,400 mg): 34 (17.8)
Acetaminophen (600 mg) and codeine (60 mg)
11 (19.6)
Difference compared to placebo, odds ratio (95% CI), statistical significance, yes/no: 0.89 (0.34 to 2.37), no
Placebo: 10 (21.7)
Safety
Adverse experiences on days 2 or 3, % pts
Any
Etoricoxib (120 mg): 10.3
Etoricoxib (90 mg): 8.4
Ibuprofen (2,400 mg): 10.4
Acetaminophen (600 mg) and codeine (60 mg): 17.7
Placebo: 8.7
Headache
Etoricoxib (120 mg): 1.0
Etoricoxib (90 mg): 1.6
Ibuprofen (2,400 mg): 0.5
Acetaminophen (600 mg) and codeine (60 mg): 6.5
Placebo: 6.5
Dizziness
Etoricoxib (120 mg): NR
Etoricoxib (90 mg): 0.5
Ibuprofen (2,400 mg): 1.0
Acetaminophen (600 mg) and codeine (60 mg): NR
Placebo: 2.2
Nausea
Etoricoxib (120 mg): 1.0
Etoricoxib (90 mg): 1.0
Ibuprofen (2,400 mg): 2.1
Acetaminophen (600 mg) and codeine (60 mg): 9.7
Placebo: 2.2
Vomiting
Etoricoxib (120 mg): NR
Etoricoxib (90 mg): NR
Ibuprofen (2,400 mg): 0.5
Acetaminophen (600 mg) and codeine (60 mg): 8.1
Placebo: NR
Discontinued medication due to AE, n pts (%)
Etoricoxib (120mg): 0 (0)
Etoricoxib (90mg): 1 (0.5)
Ibuprofen (2400mg): 1 (0.5)
Acetaminophen (600 mg) and codeine (60 mg): 3 (5.4)
Placebo: 0 (0)
Authors’ conclusion
“Pain control was most favorable for the etoricoxib doses and ibuprofen. Global Assessments of Study Medication continued to differentiate the treatments and demonstrated greater efficacy for etoricoxib on Days 2 and 3 compared with placebo and [acetaminophen (600mg) and codeine (60mg)]” (p492)
Daniels et al. (2011)17
Main study findings
Efficacy
Pain intensity
Peak pain intensity difference from baseline over the 6 hr following the first dose of study medication, mean (median)
Etoricoxib (120 mg)
1.86 (2)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P = 0.199
Etoricoxib (90 mg): 1.92 (2)
Ibuprofen (2,400 mg): 1.80 (2)
Acetaminophen (600 mg) and codeine (60 mg): 1.76 (2)
Placebo: 0.67 (1)
Pain relief
Overall analgesic effect, TOTPAR6, least squares mean (95% CI)
Etoricoxib (120 mg)
15.73 (14.57 to 16.89)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.001
Etoricoxib (90 mg)
16.10 (15.28 to 16.93)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.001
Ibuprofen (2,400 mg): 15.67 (14.85 to 16.50)
Acetaminophen (600 mg) and codeine (60 mg): 11.83 (10.38 to 13.28)
Placebo: 5.08 (3.39 to 6.76)
Subgroup analysis of TOTPAR6 by baseline pain intensity score, least squares mean (95% CI)
Etoricoxib (120 mg)
Moderate: 16.58 (14.96 to 18.21)
Severe: 14.86 (13.22 to 16.51)
Etoricoxib (90 mg)
Moderate: 16.11 (14.96 to 17.26)
Severe: 16.12 (14.94 to 17.30)
Ibuprofen (2,400 mg)
Moderate: 16.39 (15.29 to 17.50)
Severe: 14.88 (13.54 to 16.11)
Acetaminophen (600 mg) and codeine (60 mg)
Moderate: 11.00 (8.92 to 13.08)
Severe: 12.58 (10.57 to 14.59)
Placebo
Moderate: 6.85 (4.36 to 9.33)
Severe: 3.52 (1.24 to 5.80)
Time to perceptible pain relief in minutes,a median (95% CI)
Etoricoxib (120 mg): 0.48 (0.45 to 0.57)
Etoricoxib (90 mg): 0.47 (0.43 to 0.48)
Ibuprofen (2,400 mg): 0.46 (0.38 to 0.50)
Acetaminophen (600 mg) and codeine (60 mg)
0.43 (0.35 to 0.57)
Difference vs. etoricoxib: reported narratively as “similar” (p5)
Placebo: > 4 (not estimable)
Peak pain relief over the 6 hr following the first dose of study medication, mean (median)
Etoricoxib (120 mg)
3.23 (4)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.05
Etoricoxib (90 mg)
3.34 (4)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.05
Ibuprofen (2,400 mg): 3.26 (4)
Acetaminophen (600 mg) and codeine (60 mg): 3.02 (3)
Placebo: 1.43 (1)
Self-reported medication effectiveness
Patient’s global assessment of study medication over 24 hr, mean (median)
Etoricoxib (120 mg)
2.73 (3)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.05
Etoricoxib (90 mg)
2.72 (3)
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P ≤ 0.05
Ibuprofen (2,400 mg): 2.59 (3)
Acetaminophen (600 mg) and codeine (60 mg)
2.31 (2): Placebo
1.11 (1)
Patient’s global assessment of study medication at 24 hr, % pts
Etoricoxib (120 mg)
Excellent, Very Good or Good: 86
Fair to Poor: 14
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P = 0.007
Etoricoxib (90 mg)
Excellent, Very Good, or Good: 87
Fair to Poor: 13
Difference vs. acetaminophen (600 mg) and codeine (60 mg): P = 0.014
Ibuprofen (2,400 mg)
Excellent, Very Good, or Good: 83
Fair to Poor: 17
Acetaminophen (600 mg) and codeine (60 mg)
Excellent, Very Good, or Good: 74
Fair to Poor: 26
Placebo
Excellent, Very Good, or Good: 30
Fair to Poor: 70
Rescue medication
Dose of study medication, n (%)
Etoricoxib (120 mg): 12 (12.4)
Etoricoxib (90 mg): 16 (8.4)
Ibuprofen (2,400 mg): 22 (11.5)
Acetaminophen (600 mg) and codeine (60 mg)
22 (35.5)
Difference vs. etoricoxib: reported narratively as inferior to both etoricoxib dosages (p5)
Placebo: 30 (65.2)
Time to use of rescue medication, hr (95% CI))
Etoricoxib (120 mg) : > 6 (not estimable)
Etoricoxib (90 mg) : > 6 (not estimable)
Ibuprofen (2,400 mg): > 6 (not estimable)
Acetaminophen (600 mg) and codeine (60 mg)
> 6 (not estimable)
Difference vs. etoricoxib: reported narratively as a statistically significantly shorter amount of time than either dosages of etoricoxib (p5)
Placebo: 2.13 (1.67 to 4.20)
Safety
Adverse experiences
One or more, n pts (%)
Etoricoxib (120 mg): 28 (28.9)
Etoricoxib (90 mg): 54 (28.3)
Ibuprofen (2,400 mg): 57 (29.7)
Acetaminophen (600 mg) and codeine (60 mg): 35 (56.5)
Difference vs. etoricoxib: P ≤ 0.001
Placebo: 12 (25.1)
Drug-related, n pts (%)
Etoricoxib (120 mg): 12 (12.4)
Etoricoxib (90 mg): 21 (11.0)
Ibuprofen (2,400 mg): 18 (9.4)
Acetaminophen (600 mg) and codeine (60 mg)
30 (48.4)
Difference vs. etoricoxib: P ≤ 0.001
Placebo: 6 (13.0)
Serious, n pts (%)
Etoricoxib (120 mg): 0 (0)
Etoricoxib (90 mg): 0 (0)
Ibuprofen (2,400 mg): 0 (0)
Acetaminophen (600 mg) and codeine (60 mg): 0 (0)
Placebo: 0 (0)
Most common adverse experiences (> 3.0% incidence)
Nausea, n pts (%)
Etoricoxib (120 mg): 4 (4.1)
Etoricoxib (90 mg): 6 (3.1)
Ibuprofen (2,400 mg): 10 (5.2)
Acetaminophen (600 mg) and codeine (60 mg)
23 (37.1)
Difference vs. etoricoxib: P ≤ 0.001
Difference vs. placebo: P ≤ 0.002
Placebo: 3 (6.5)
Vomiting, n pts (%)
Etoricoxib (120 mg): 1 (1.0)
Etoricoxib (90 mg): 2 (1.0)
Ibuprofen (2,400 mg): 2 (1.0)
Acetaminophen (600 mg) and codeine (60 mg)
15 (24.2)
Difference vs. etoricoxib: P ≤ 0.001
Difference vs. placebo: P ≤ 0.002
Placebo: 1 (2.2)
Dizziness, n pts (%)
Etoricoxib (120 mg): 0 (0.0)
Etoricoxib (90 mg): 4 (2.1)
Ibuprofen (2,400 mg): 3 (1.6)
Acetaminophen (600 mg) and codeine (60 mg): 10 (16.1)
Placebo: 2 (4.2)
Alveolar osteitis, n pts (%)
Etoricoxib (120 mg): 3 (3.1)
Etoricoxib (90 mg): 8 (4.2)
Ibuprofen (2,400 mg): 8 (4.2)
Acetaminophen (600 mg) and codeine (60 mg): 1 (1.6)
Placebo: 0 (0.0)
Headache, n pts (%)
Etoricoxib (120 mg): 5 (5.2)
Etoricoxib (90 mg): 11 (5.8)
Ibuprofen (2,400 mg): 8 (4.2)
Acetaminophen (600 mg) and codeine (60 mg): 9 (14.5)
Placebo: 6 (13.0)
Somnolence, n pts (%)
Etoricoxib (120 mg): 2 (2.1)
Etoricoxib (90 mg): 4 (2.1)
Ibuprofen (2,400 mg): 6 (3.1)
Acetaminophen (600 mg) and codeine (60 mg): 5 (8.1)
Placebo: 0 (0.0)
Hyperhidrosis, n pts (%)
Etoricoxib (120 mg): 1 (1.0)
Etoricoxib (90 mg): 1 (0.5)
Ibuprofen (2,400 mg): 1 (0.5)
Acetaminophen (600 mg) and codeine (60 mg): 2 (3.2)
Placebo: 1 (2.2)
Discontinuation of study medication due to AE, n pts (%)
Etoricoxib (120 mg): 0 (0)
Etoricoxib (90 mg): 1 (0.5)
Ibuprofen (2,400 mg): 1 (0.5)
Acetaminophen (600 mg) and codeine (60 mg): 3 (4.8)
Placebo: 0 (0)
a Note: Authors of this study did report the unit of measurement for time to pain relief as “minutes;” however, the data (i.e., proportions of minutes) appear inconsistent with this and may be describing, for example, stopwatch readings or some other measure.
Authors’ conclusion
“In summary, the results of this study confirm the understanding of earlier studies that reported that NSAID [nonsteroidal anti-inflammatory drug] therapy was superior to placebo or opioid-based therapy for the treatment of postoperative dental pain. According to the primary and secondary endpoints, both etoricoxib 90 and 120 mg were superior to placebo and A/C [acetaminophen 600 mg and codeine 60 mg]; the results for etoricoxib were similar to those observed with ibuprofen. In addition, etoricoxib and ibuprofen were generally well tolerated and showed superior tolerability compared with A/C.” (p7)
Appendix 5: References of Potential Interest
Previous CADTH Reports
1.Codeine for Acute Pain: A Synopsis of the Evidence. Ottawa (ON): CADTH; 2019 Dec: https://cadth.ca/sites/default/files/pdf/htis/codeine_actute_pain_evidence_synopsis.pdf Accessed 2021 Jan 23.
2.Marchand DK, Ford C. Codeine for Acute Pain for Urological or General Surgery Patients: A Review of Clinical Effectiveness (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Dec: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1201%20Codeine%20for%20Urological%20Pts%20Final.pdf Accessed 2021 Jan 23.
3.Li KX, Ford C. Codeine for Pediatric Patients with Acute Pain: A Review of Clinical Effectiveness (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Nov: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1200%20Codeine%20for%20Pediatric%20Patients%20Final.pdf Accessed 2021 Jan 23.
4.Marchand DK, McCormack S. Codeine for Acute Pain in Patients Undergoing Orthopedic Surgery: A Review of Clinical Effectiveness (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Oct: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1199%20Codeine%20for%20Orthopaedic%20Pts%20Final.pdf Accessed 2021 Jan 23.
5.Codeine and acetaminophen for pain relief: a review of the clinical efficacy (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2012 Apr: https://www.cadth.ca/codeine-and-acetaminophen-pain-relief-review-clinical-efficacy-and-safety Accessed 2021 Jan 23.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca