CADTH Health Technology Review
Gravity Drainage Versus Forced Suction Drainage for Patients With Excess Fluid in Pleural or Peritoneal Spaces
Rapid Review
Authors: Yan Li, Charlene Argáez
Abbreviations
MA
meta-analysis
NRS
non-randomized studies
PAL
prolonged air leak
RCT
randomized controlled trial
SR
systematic review
Key Messages
The evidence for chest drainage with gravity compared with forced suction was mixed. Two randomized controlled trials included in 2 systematic reviews with meta-analysis suggested that there is no difference between chest drainage with gravity versus forced suction regarding the risk of prolonged air leak, or post-operative pneumothorax and the duration of chest tube drainage, or hospital stay, following lung cancer surgery. However, 1 randomized controlled trial included in a systematic review with meta-analysis suggested that chest drainage with gravity resulted in a shorter duration of chest tube drainage and hospital stay compared to forced suction following lung cancer surgery.
One guideline suggests that chest drainage with forced suction does not provide additional benefits for patients undergoing lung surgery compared to gravity drainage.
There is a lack of relevant literature and guidelines on the clinical effectiveness or use of abdominal space drainage with gravity or forced suction.
Context and Policy Issues
The sampling of a small quantity of fluid for diagnostic intents or the removal of a large quantity of fluid for therapeutic purposes from the pleural space (i.e., between the lungs and chest wall) and the peritoneal space (i.e., abdominal cavity) is known as thoracentesis and paracentesis, respectively.1,2 Some causes for excess fluid in the pleural space — pleural effusion — include trauma (e.g., puncture wounds), surgical complications, infection (e.g., tuberculosis), and disease (e.g., cancer, heart failure).3 Common causes for excess fluid — ascites — in the peritoneal space include cirrhosis, cancer, infection, dialysis, and heart disease.4
For the drainage of excess fluid, a needle or tube is inserted into the pleural or peritoneal space.1,2 Health care providers may attach a syringe to the needle to aspirate directly or attach the tube to a water-seal drain with or without forced suction.5 The water seal acts as a one-way valve, which allows air to escape and prevents it from reentering the patient.3 When no suction is applied to the water-seal drain, it is using the force of gravity to drain fluid.3 Alternatively, the water-seal drain can be attached to external wall suction, which typically expedites the drainage of fluid and air.6 However, it is uncertain if forced suction results in direct patient benefits and/or complications.6
The aim of this report is to summarize and critically appraise the relevant clinical evidence and evidence-based guidelines regarding the clinical effectiveness or use of pleural or peritoneal space drainage with gravity or forced suction.
Research Questions
What is the comparative clinical effectiveness of draining pleural or peritoneal spaces with gravity compared with forced suction?
What are the evidence-based guidelines regarding the drainage of pleural or peritoneal spaces using gravity or forced suction?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pleural and peritoneal spaces and drainage. No search filters were applied to limit retrieval to study type. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2015 and December 8, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with excess fluid in either pleural spaces (i.e., pleural effusion) or excess fluid in peritoneal spaces |
Intervention | Gravity drainage (e.g., low intervention drainage, low suction pressure drainage) |
Comparators | Q1: Forced suction drainage (e.g., moderate to high suction pressure, wall-mounted suction) Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., safety, risks, complications, change in condition, quality of life) Q2: Recommendations regarding the choice in suction device for removing excess fluid from pleural or peritoneal spaces; Recommendations regarding the amount of suction to use in pleural or peritoneal space drainage |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2015. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for systematic reviews and the Appraisal of Guidelines for Research & Evaluation AGREE II instrument8 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
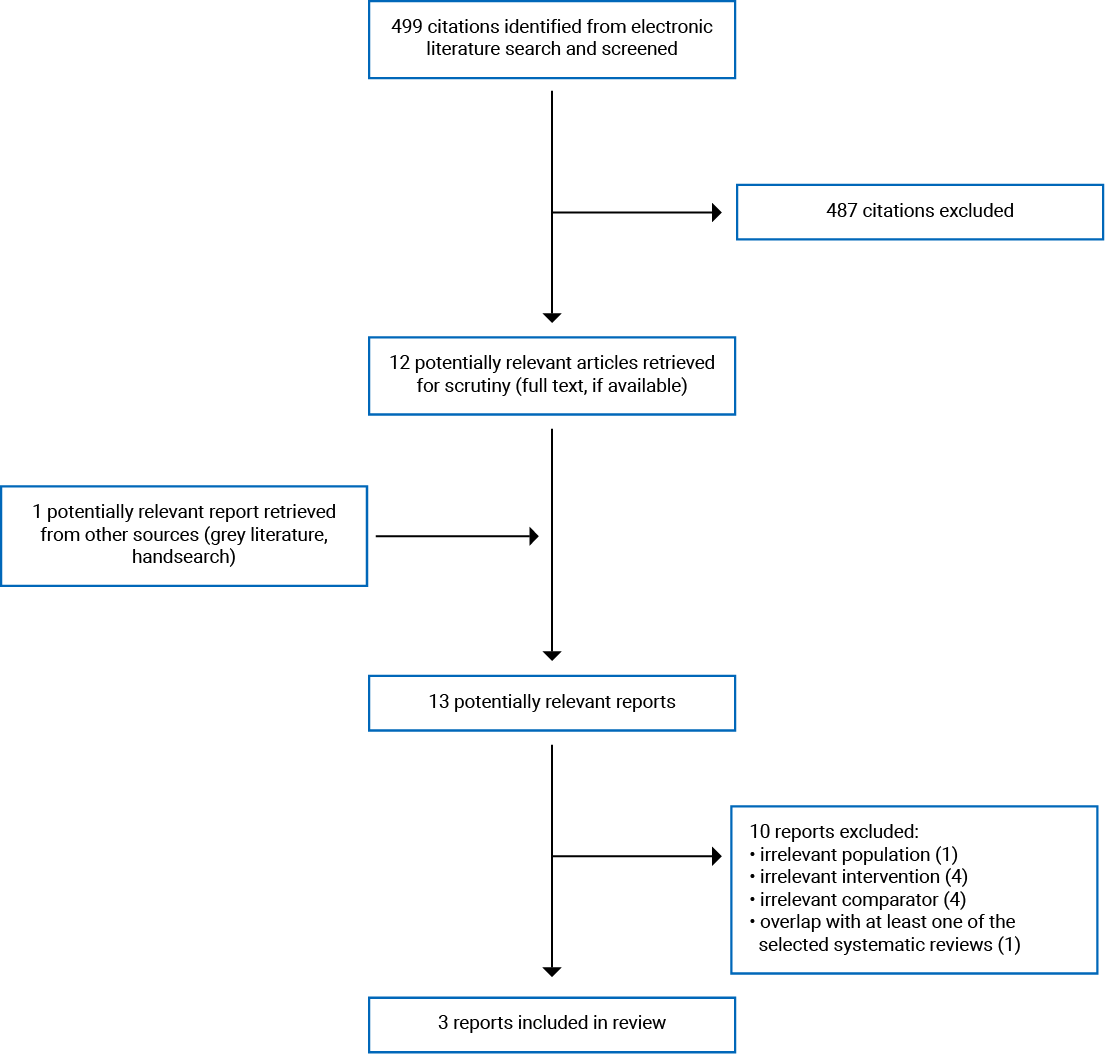
A total of 499 citations were identified in the literature search. Following the screening of titles and abstracts, 487 citations were excluded and 12 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 10 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 2 SRs with meta-analyses (MAs)9,10 and 1 evidence-based guideline.11 Appendix 1 presents the PRISMA12 flow chart of the study selection.
Summary of Study Characteristics
Two SRs with MA9,10 and 1 evidence-based guideline11 were identified with relevance to the research questions and inclusion criteria of this report. With broader inclusion criteria than the present review, 1 SR with MA10 also included other chest tube management interventions (i.e., post-operative chest tube milking, use of digital recording protocol, early chest tube removal). Only the characteristics and results of the subset of relevant studies will be described in this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Published in 20199 and 2017,10 1 of the 2 identified SRs with MA included 109 randomized controlled trials (RCTs) and the other included 35 studies (29 RCTs and 6 non-randomized studies [NRS]).10 Two RCTs and 3 RCTs included in the SR with MA authored by Zhou et al.9 and Deng et al.,10 respectively, were relevant to this report. These SRs with MA9,10 had 2 overlapping RCTs. A table of primary study overlap is provided in Appendix 5. Authors of both SRs with MA9,10 limited their search to English publications. Time frames for the literature searches were from inception to August 30, 20179 or from January 1, 1996 to January 1, 2016.10
The included evidence-based guideline,11 developed by the Society for Translational Medicine, was published in 2017. This guideline was informed by systematic searches conducted in various databases (i.e., PubMed, Scopus, Web of Science).11 The search date, time frame, and types of studies screened were not reported. The quality of the evidence (ranging from A [high] to C [low]) and strength of recommendations (ranging from 1 [strong] to 2 [weak]) were assessed using the American College of Physicians Task Force approach (detailed rating system reported in Appendix 2). Decisions on the recommendations were reached through discussion among guideline authors.11
Country of Origin
The first authors of the included SRs with MA9,10 and evidence-based guideline11 were from China.
Patient Population
The 2 identified SRs with MA did not specify the age-related inclusion criteria.9,10 While Zhou et al.9 included studies involving patients who have undergone lung surgery specifically for a benign or malignant condition, Deng et al.10 included patients who have undergone lung cancer surgery. The 3 relevant RCTs identified from the SRs with MA involved patients who have undergone lung cancer surgery.9,10 The number of study participants in the 3 RCTs was 91 (47 with suction versus 44 with no suction), 239 (116 with suction versus 123 with no suction), and 78 (46 with suction versus 32 with no suction).9,10 Population details (e.g., mean age) were not reported for the subgroups in the SRs with MA that are relevant to this report.9,10
The target population covered by the identified guideline was patients (age unspecified) undergoing lobectomy (benign or malignant condition not specified).11 The intended users of this guideline are surgeons and health care professionals providing care for patients undergoing lung surgeries.11
Interventions and Comparators
The 2 SRs with MA included primary studies that compared chest drainage with forced suction versus no forced suction (e.g., simple water-seal).9,10 Furthermore, the 2 SRs with MA did not have a requirement for a specific follow-up duration.9,10 Both SRs with MA9,10 also included primary studies comparing forced suction versus initial forced suction on the first day of surgery followed by no forced suction on subsequent days, which was a comparison outside the scope of this report. The forced suction pressure used in the 3 relevant RCTs identified from the SRs with MA were −15 cmH20 to −20 cmH20, −20 cmH20, or not reported9,10
The identified guideline contained recommendations regarding the post-operative management of chest tubes (i.e., timing of chest tube removal, number of chest tubes, chest tube clearance, chest tube suctioning, techniques to remove chest tubes, electronic drainage systems).11 Recommendations relevant for this report pertained to the use of routine chest tube suctioning.11
Outcomes
The authors of the 2 SRs with MA reported various outcomes including prolonged air leak (PAL), duration of chest tube drainage, and length of hospital stay.9,10 The SR with MA authored by Zhou et al.9 also reported on post-operative pneumothorax.
The identified guideline considered various outcomes including PAL, drainage time, length of hospital stay, and post-operative pneumothorax.11
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews and Meta-Analyses
As per AMSTAR II criteria,7 the 2 included SRs with MA9,10 shared some methodological strengths such as clearly stated objectives, inclusion criteria, key search terms, and search time frames. The authors of both SRs with MA searched multiple databases, provided a list of included studies, and used χ2 test and I2 statistics to assess for heterogeneity.9,10 Details of study selection were explicitly stated and risk of bias of included studies was assessed using an appropriate tool in the SR with MA authored by Zhou et al.9 Furthermore, data extraction was conducted in duplicate in this SR with MA, which decreases the risk for inconsistencies.9 Publication bias was not detected using Begg’s test and funnel plots in this SR with MA.9 Finally, Zhou et al. conducted a random-effects MA, disclosed their funding sources, and declared that they have no conflicts of interest.9
Regarding methodological limitations, while the exclusion criteria were explicitly stated for both SRs with MA, a list of excluded studies and rationale for exclusion was not reported.9,10 The age eligibility criteria were not explicitly stated and justification was not provided for the exclusion of non-English publications or the choice of included study designs in the 2 SRs with MA.9,10 Grey literature searches were not reported in both SRs with MA, which may have resulted in an increased risk of missing relevant, non-indexed studies.9,10 Additionally, the use of an a priori study protocol or the time frame requirements for follow-up were not reported for either SR with MA.9,10 The assessment of publication bias, details of study selection, risk of bias evaluation for included studies, and methods for statistical combination of results were not reported in the SR with MA authored by Deng et al.10 Furthermore, study screening was not performed in duplicate in this SR with MA.10 Finally, although Deng et al. declared that they have no conflicts of interest, funding sources were not disclosed.10
Evidence-Based Guidelines
The authors of the identified guideline provided a clear description of their objectives, specified the target populations and users, provided unambiguous and easily identifiable recommendations, presented monitoring criteria for the recommendations, and sought review by external experts.11 The guideline development group comprised experts from multidisciplinary areas and the views of the funding sources did not appear to have influenced the guideline’s contents.11 The supporting evidence, together with the quality of evidence, used to inform the recommendations were provided.11 However, the authors of this guideline did not seek the views and preferences of the target population, describe facilitators or barriers to their application, provide tools for putting recommendations into practice, or explicitly describe procedures for guideline updates.11
Summary of Findings
The overall findings of the included studies and guideline follow. Two SRs with MA9,10 and 1 evidence-based guideline11 met the inclusion criteria for this report. The 2 SRs with MA9,10 had 2 overlapping RCTs. Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Draining Pleural Spaces With Gravity Versus Forced Suction
Evidence regarding the comparative clinical effectiveness of draining pleural spaces with gravity (e.g., low intervention drainage, low suction pressure drainage) compared with forced suction (e.g., moderate to high suction pressure, wall-mounted suction) was available from 2 SRs with MA.9,10 Pooled findings and overall conclusions from the 2 SRs with MA9,10 were outside the scope of this report.
Prolonged Air Leak
The 2 SRs with MA9,10 included 2 overlapping RCTs that reported on PAL. There was no statistically significant difference in PAL between participants receiving forced suction versus no forced suction after lung cancer surgery.9,10
Duration of Chest Tube Drainage
The 2 SRs with MA9,10 included 1 overlapping RCT and the SR with MA authored by Deng et al.10 included 1 RCT that reported on the duration of chest tube drainage. In the overlapping RCT, there was no statistically significant difference in the duration of chest tube drainage between participants receiving forced suction versus no forced suction after lung cancer surgery.9,10 However, in the RCT included in the SR with MA by Deng et al.,10 there was a statistically significant mean difference of 1.33 days (95% confidence interval, 1.19 to 1.47) in the duration of chest tube drainage between forced suction versus no forced suction groups after lung cancer surgery favouring no forced suction (i.e., shorter duration of chest tube drainage).10
Length of Hospital Stay
The 2 SRs with MA9,10 included 1 overlapping RCT and the SR with MA authored by Deng et al.10 included 1 RCT that reported on the length of hospital stay. In the overlapping RCT, there was no statistically significant difference in the length of hospital stay between participants receiving forced suction versus no forced suction after lung cancer surgery.9,10 However, in the RCT included in the SR with MA by Deng et al.,10 there was a statistically significant mean difference of 1.61 days (95% confidence interval, 1.35 to 1.87) in the length of hospital stay between forced suction versus no forced suction groups after lung cancer surgery favouring no forced suction (i.e., shorter length of hospital stay).10
Post-operative Pneumothorax
The 2 SRs with MA9,10 included 2 overlapping RCTs that reported on post-operative pneumothorax. There was no statistically significant difference in post-operative pneumothorax between participants receiving forced suction versus no forced suction after lung cancer surgery.9,10
Clinical Effectiveness of Draining Peritoneal Spaces With Gravity Versus Forced Suction
No relevant evidence was identified regarding the drainage of peritoneal spaces using gravity or forced suction; therefore, no summary can be provided.
Guidelines
One identified evidence-based guideline provided recommendations regarding the drainage of pleural spaces using gravity or forced suction.11 This guideline states that forced suctioning does not provide additional benefits for patients who have undergone a lung lobectomy (strength of recommendation: weak; quality of evidence: high).11 Finally, no relevant evidence-based guidelines were identified regarding the drainage of peritoneal spaces; therefore, no summary can be provided.
Limitations
Limitations were identified in the critical appraisal (details in Appendix 3); however, additional limitations exist.
The authors of both SRs with MA9,10 also included primary studies comparing forced suction versus initial forced suction on the first day of surgery followed by no forced suction on subsequent days. These primary studies were excluded from this report, as all study participants received forced suction on the first day of surgery. Despite stopping forced suction for some participants starting on the second day, it was uncertain if the initial day of forced suctioning had a beneficial or harmful effect. Furthermore, while the 2 SRs with MA were published recently in 20199 and 2017,10 the 3 relevant RCTs identified from these SRs with MA date back to 2005 or 2008. As these 3 primary studies were conducted in Greece, the UK, or the US, the findings may not be generalizable to the Canadian setting. Additionally, as the critical appraisal was conducted for the included SRs with MA, the quality of the included primary studies relevant to this report is unclear. Finally, no relevant evidence was identified regarding the comparative clinical effectiveness of draining peritoneal spaces with gravity or forced suction.
The identified guideline was developed for use in China; therefore, the generalizability of the recommendations to the Canadian context is unclear.11 Additionally, no relevant evidence-based guidelines were identified regarding the drainage of peritoneal spaces for the removal of excess fluid. Overall, considering the limitations mentioned, the findings and recommendations summarized in this report need to be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 2 SRs with MA9,10 regarding the comparative clinical effectiveness of draining pleural spaces with gravity compared with forced suction. Furthermore, 1 evidence-based guideline11 was identified regarding the drainage of pleural spaces using gravity or forced suction. No relevant literature or evidence-based guidelines were identified regarding the clinical effectiveness or use of peritoneal space drainage with gravity or forced suction.
The overall findings from the identified literature were inconclusive. Specifically, 2 SRs with MA9,10 included 2 overlapping RCTs that detected no statistically significant differences in PAL and post-operative pneumothorax between forced suction versus no forced suction groups after lung cancer surgery.9,10 Furthermore, in 1 overlapping RCT included in both SRs with MA, no statistically significant differences were detected in the duration of chest tube drainage and length of hospital stay between forced suction versus no forced suction groups.9,10 However, the SR with MA authored by Deng et al.10 included 1 RCT that detected statistically significant differences in the duration of chest tube drainage and length of hospital stay between forced suction versus no forced suction groups favouring no forced suction. One evidence-based guideline suggests that forced suctioning does not result in additional benefits for patients undergoing a lung lobectomy (strength of recommendation: weak; quality of evidence: high).11
Although the 2 identified SRs with MA9,10 were published within the past 3 years, the 3 included RCTs date back to 2008 or 2005. Furthermore, the 2 SRs with MA9,10 shared methodological limitations such as not reporting if a grey literature search was conducted or whether an a priori study protocol was used. The limitations of the overall body of evidence (e.g., paucity of recently published primary studies, SRs and RCTs conducted outside of Canada) should be considered when interpreting the findings of this report.
Further research investigating comparative clinical effectiveness of drainage with gravity versus forced suction, particularly with large multinational controlled clinical trials with Canadian representation, would provide clinicians with an additional knowledge base regarding the removal of excess fluid from pleural or peritoneal spaces. As well, guidelines developed with rigorous methodology that are specific to the local context would provide additional guidance for Canadian clinicians.
References
1.Runyon B. Diagnostic and therapeutic abdominal paracentesis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2019 Nov: www.uptodate.com. Accessed 2021 Jan 11.
2.Feller-Kopman D. Management of nonmalignant pleural effusions in adults. In: Post TW, ed. UptoDate. Waltham (MA): UpToDate; 2020 Aug: www.uptodate.com. Accessed 2021 Jan 11.
3.Salmon N, Lynch S, Muck K. Chest tube management. San Diego (CA): RN.com; AMN Healthcare Education Services; 2013: https://lms.rn.com/getpdf.php/1933.pdf. Accessed 2021 Jan 12.
4.Johns Hopkins Medicine. Ascites. 2021; https://www.hopkinsmedicine.org/health/conditions-and-diseases/ascites Accessed 2021 Jan 12.
5.Wang C, Lyu M, Zhou J, Liu Y, Ji Y. Chest tube drainage versus needle aspiration for primary spontaneous pneumothorax: which is better? J Thorac Dis. 2017;9(10):4027-4038. Medline
6.Lang P, Manickavasagar M, Burdett C, et al. Suction on chest drains following lung resection: evidence and practice are not aligned. Eur J Cardiothorac Surg. 2016;49(2):611-616. Medline
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
8.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Jan 11.
9.Zhou J, Chen N, Hai Y, et al. External suction versus simple water-seal on chest drainage following pulmonary surgery: an updated meta-analysis. Interact Cardiovasc Thorac Surg. 2019;28(1):29-36. Medline
10.Deng B, Qian K, Zhou JH, Tan QY, Wang RW. Optimization of chest tube management to expedite rehabilitation of lung cancer patients after video-assisted thoracic surgery: a meta-analysis and systematic review. World J Surg. 2017 Aug;41(8):2039-2045. Medline
11.Gao S, Zhang Z, Aragon J, et al. The Society for Translational Medicine: clinical practice guidelines for the postoperative management of chest tube for patients undergoing lobectomy. J Thorac Dis. 2017;9(9):3255-3264. Medline
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
13.Qiu T, Shen Y, Wang MZ, et al. External suction versus water seal after selective pulmonary resection for lung neoplasm: a systematic review. PLoS One. 2013;8(7):e68087. Medline
14.Deng B, Tan QY, Zhao YP, Wang RW, Jiang YG. Suction or non-suction to the underwater seal drains following pulmonary operation: meta-analysis of randomised controlled trials. Eur J Cardiothorac Surg. 2010;38(2):210-215. Medline
15.Coughlin SM, Emmerton-Coughlin HM, Malthaner R. Management of chest tubes after pulmonary resection: a systematic review and meta-analysis. Can J Surg. 2012;55(4):264-270. Medline
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Zhou et al. (2019)9 China Funding Sources: National Natural Science Foundation of China and National Program for Key Science &Technology Projects of Sichuan Province, China | Objective: To compare the effects of chest drainage with no forced suction (i.e., simple water-seal) and forced suction Study design: SR with MA of RCTs Literature search strategy: The search was conducted in PubMed, Embase, and Web of Science for literature published in English from inception to August 30, 2017. Grey literature search NR. Number of studies included: Of 10 identified studies, 2 RCTs were relevant to this report Quality assessment tool: Risk of bias assessed as per Cochrane Handbook for Systemic Reviews of Interventions | Patients (age-related inclusion criteria NR) who have undergone lung surgery for a benign or malignant condition | Interventions: Chest drainage with no forced suction (i.e., simple water-seal) Comparator: Chest drainage with forced suction | Outcomes: PAL and post-operative pneumothorax, duration of chest tube drainage, and hospital stay Follow-up: Follow-up duration NR |
Deng et al. (2017)10 China Funding Source: NR | Objective: To determine optimal chest tube management after lung cancer surgery Study design: SR with MA of RCTs and NRS Literature search strategy: The search was conducted in PubMed, Embase, MEDLINE, and Web of Science for literature published in English from January 1, 1996 to January 1, 2016. Grey literature search NR. Number of studies included: Of 35 identified studies, 3 RCTs were relevant to this report Quality assessment tool: Quality of evidence assessed as per recommendation the American Academy of Orthopaedic Surgeons evidence-based practice committee | Patients (age-related inclusion criteria NR) who have undergone lung cancer surgery | Eligible Interventions: Post-operative chest tube milking, use of digital recording protocol, early chest tube removal, chest drainage with no forced suction (i.e., simple water-seal) Relevant Interventions: Chest drainage with no forced suction Comparator: Chest drainage with forced suction | Outcomes: Duration of chest tube drainage and hospital stay Follow-up: Follow-up duration NR |
MA = meta-analysis; NR = not reported; NRS = non-randomized study; PAL = prolonged air leak; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
Society for Translational Medicine (2017)11 | ||||||
Intended users: Surgeons and health care professionals providing care for patients undergoing lung surgeries Target population: Patients (age unspecified) undergoing lobectomy (benign or malignant condition not specified) China | The guideline provided recommendations regarding post-operative management of chest tubes (i.e., timing of chest tube removal, number of chest tubes, chest tube clearance, chest tube suctioning, techniques to remove chest tubes, electronic drainage systems). Recommendations relevant for this report pertained to the use of routine chest tube suctioning | Persistent air leak, drainage time, length of hospital stay, pneumothorax | Literature searches were conducted in various databases (i.e., PubMed, Scopus, Web of Science). Date and time frame of search and types of studies screened NR | Evidence quality was assessed using the American College of Physicians Task Force approach A: High-quality evidence B: Moderate-quality evidence C: Low-quality evidence | Recommendations were drafted by 1 author and any discrepancies were resolved through discussions Strength of recommendations as per the American College of Physicians Task Force: 1: Strong recommendation 2: Weak recommendation | Recommendations were reviewed by an external panel of experts |
NR = not reported.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 27
Strengths | Limitations |
Zhou et al. (2019)9 | |
|
|
Deng et al. (2017)10 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NR = not reported.
Table 5: Strengths and Limitations of Guideline Using AGREE II8
Item | Society for Translational Medicine (2017)11 |
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, and so forth) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, and so forth) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for the management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Findings of Included Systematic Reviews
Main study findings | Authors’ conclusion |
Zhou et al. (2019)9 | |
Two included primary RCTs published in 2008 and 2005 compared chest drainage with forced suction vs. no forced suction (i.e., simple water-seal) after lung cancer surgery. Prokakis et al., 2008 Forced suction pressure: −15 cmH20 to −20 cmH20 PAL (defined as > 7 days of air leak): • RR: 0.75 (95% CI, 0.21 to 2.61) Post-operative pneumothorax: • RR: 0.62 (95% CI, 0.24 to 1.61) Duration of chest tube drainage: • RR: 0.20 (95% CI, −1.04 to 1.44) Length of hospital stay: • RR: 0.90 (95% CI, −1.14 to 2.94) Alphonso et al., 2005 Forced suction pressure: − 20 cmH20 PAL (defined as > 6 days of air leak): • RR: 0.73 (95% CI, 0.33 to 1.65) Post-operative pneumothorax: • RR: 0.71 (95% CI, 0.12 to 4.15) Duration of chest tube drainage: • RR: NR Length of hospital stay: • RR: NR | Pooled findings and overall conclusions were outside the scope of this report. |
Deng et al. (2017)10 | |
Three included primary RCTs published in 2008 or 2005 compared chest drainage with forced suction vs. no forced suction (i.e., simple water-seal) after lung cancer surgery. Antanavicius et al., 2005 Forced suction pressure: NR Duration of chest tube drainage: • MD: 1.33 days (95% CI, 1.19 to 1.47) • Favours no forced suction (i.e., shorter duration of chest tube drainage) Length of hospital stay: • MD: 1.61 days (95% CI, 1.35 to 1.87) • Favours no forced suction (i.e., shorter length of hospital stay) | Pooled findings and overall conclusions were outside the scope of this report. |
CI = confidence interval; cmH2O = centimetre of water; MD = mean difference; NR = not reported; PAL = prolonged air leak; RCT = randomized controlled trial; RR = risk ratio; vs. = versus.
Table 7: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
Society for Translational Medicine (2017)11 | |
“Routine chest tube suction offers no advantage for patients undergoing lobectomy, and may only be indicated in case of progressive subcutaneous emphysema (p. 3259).”11 • These recommendations were informed by 3 SRs with MA.13-15 | 2A: Weak recommendation, high-quality evidence |
MA = meta-analysis; SR = systematic review.
Appendix 5: Overlap Between Included Systematic Reviews
Table 8: Overlap in Relevant Primary Studies between Included Systematic Reviews
Primary study citation | Zhou et al. (2019)9 | Deng et al. (2017)10 |
Prokakis C, et al. World J Surg. 2008 Nov;32(11):2336-42. | Yes | Yes |
Alphonso N, et al. Eur J Cardiothorac Surg. 2005 Mar;27(3):391-4. | Yes | Yes |
Antanavicius G, et al. Am Surg. 2005 May;71(5):416-9. | No | Yes |
Appendix 6: References of Potential Interest
Systematic Review – Overlap with Other Systematic Reviews
1.Lang P, Manickavasagar M, Burdett C, et al. Suction on chest drains following lung resection: evidence and practice are not aligned. Eur J Cardiothorac Surg. 2016 Feb;49(2):611-616. Medline
Randomized Controlled Trials
Alternative Comparator - Gravity versus Syringe Suction (Low Pressure)
2.Lentz RJ, Shojaee S, Grosu HB, et al. The Impact of Gravity vs Suction-driven Therapeutic Thoracentesis on pressure-related complications: the GRAVITAS multicenter randomized controlled trial. Chest. 2020 Mar;157(3):702-711. Medline
Alternative Intervention and Comparator – Syringe Suction versus Vacuum Bottle
3.Senitko M, Ray AS, Murphy TE, et al. Safety and tolerability of vacuum versus manual drainage during thoracentesis: a randomized trial. J Bronchology Interv Pulmonol. 2019 Jul;26(3):166-171. Medline
Alternative Comparator – Forced Suction versus Initial Forced Suction then No Forced Suction
4.Gocyk W, Kuzdzal J, Wlodarcyck J, et al. Comparison of suction versus nonsuction drainage after lung resections: a prospective randomized trial. 2016 Dec. Ann Thorac Surg. 2016 Oct;102(4):1119-24. Medline
Non-Randomized Study – No Comparator
5.Sagar AES, Landaeta MF, Adrianza AM, et al. Complications following symptom-limited thoracentesis using suction. Eur Respir J. 2020 Nov;56(5). Medline
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca