CADTH Health Technology Review
Rapid Testing for the Diagnosis of Pulmonary Tuberculosis and Rifampicin Resistance: A Review of Cost-Effectiveness
Rapid Review
Authors: Anusree Subramonian, Melissa Severn
Abbreviations
AFB
acid-fast bacillus
CI
confidence interval
DALY
disability-adjusted life-year
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels
GDP
gross domestic product
ICER
incremental cost-effectiveness ratio
INB
incremental net benefit
MTB/RIF
Mycobacterium tuberculosis complex and resistance to rifampicin
QALY
quality-adjusted life-year
SD
standard deviation
TB
tuberculosis
UR
uncertainty range
WTP
willingness to pay
Key Messages
The evidence regarding the cost-effectiveness of the Xpert Mycobacterium tuberculosis complex and resistance to rifampicin (Xpert MTB/RIF) test compared with smear microscopy in diagnosing tuberculosis is summarized in this report.
Results from the included 6 studies showed that Xpert MTB/RIF testing is a cost-effective option compared with sputum smear microscopy. However, the generalizability of the results to the Canadian setting are unclear because of the clinical data source populations, willingness-to-pay thresholds, and assumptions used in the analyses.
There is a lack of evidence regarding the cost-effectiveness of Xpert MTB/RIF testing compared with mycobacterial cultures or culture-based susceptibility testing.
Context and Policy Issues
Tuberculosis (TB) is a chronic multisystemic infectious disease caused by Mycobacterium tuberculosis. WHO estimates that approximately one-quarter of the world’s population is infected with M. tuberculosis.1 Globally, approximately 10 million people had TB in 2019, and there were approximately 1.2 million deaths attributable to the disease.1 The enormous health and economic burden caused by the disease make it a major public health issue. In Canada, active TB infection rates are one of the lowest in the world. There were 1,796 active cases of TB nationwide in 2017, mostly in foreign-born individuals and the Canadian Indigenous population.2
TB can affect almost all body systems, such as the central nervous system (e.g., TB meningitis), gastrointestinal tract (e.g., intestinal TB), and cardiovascular system (pericardial TB). Pulmonary TB is a debilitating disease affecting primarily the lungs. The main symptom of pulmonary TB is chronic cough that lasts for 2 weeks or longer. Other symptoms include fever, hemoptysis, anorexia, and loss of weight.3 TB is treated with antimicrobial agents such as rifampicin and isoniazid and it is completely curable with treatment with the appropriate agent for the appropriate duration. Early diagnosis and treatment are of utmost importance because TB is highly infectious, transmitted through droplet spread, and associated with long-term complications.
The diagnostic tests for TB include chest radiography, sputum smear microscopy, sputum culture, and rapid and simultaneous TB and antibiotic susceptibility testing for pulmonary TB and rifampicin resistance. The Xpert M. tuberculosis complex and resistance to rifampicin (MTB/RIF) test is a Health Canada–approved rapid diagnostic test for pulmonary TB that uses polymerase chain reaction–based nucleic acid amplification to detect M. tuberculosis and rifampicin resistance.3 The results are available within 2 hours. It uses a disposable cartridge in which the sputum sample and reagent are mixed. The cartridge is then placed in the Xpert machine and automatically processed.4 The test is automated with a minimal training requirement and the results are rapidly available; therefore, Xpert testing can be useful in settings with resource constraints where the infection rates are high, such as in the northern regions of Canada.3
The objective of the current report is to review the evidence regarding the cost-effectiveness of the rapid and simultaneous TB and antibiotic susceptibility testing for pulmonary TB and rifampicin resistance. This report is an upgrade from a CADTH report (Summary of Abstracts)5 published in June 2020. Another report focused on the diagnostic accuracy of the rapid and simultaneous tuberculosis and antibiotic susceptibility testing for pulmonary TB and rifampicin resistance.6 These reports are components of a larger CADTH Condition Level Review on tuberculosis. More information on CADTH’s Condition Level Review of tuberculosis can be found in the CADTH website
Research Question
What is the cost-effectiveness of rapid and simultaneous tuberculosis and antibiotic susceptibility testing for the detection of pulmonary tuberculosis or rifampicin resistance?
Methods
Literature Search Methods
This report is an update of a literature search strategy developed for a previous CADTH report.5 For the current report, a limited literature search was conducted on key resources including MEDLINE, the Cochrane Library, University of York Centre for Reviews and Dissemination (CRD) databases, Canadian and major international health technology agencies, as well as a focused internet search. Methodological filters were used to limit search results to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses, any types of clinical trials or observational studies, and economic studies. The initial search was limited to English-language documents published between January 1, 2015, and June 9, 2020. For the current report, database searches were rerun on October 28, 2020, to capture any articles published since the initial search date. The search of major health technology agencies was also updated to include documents published since June 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | People of any age with presumptive pulmonary TB, presumptive rifampicin-resistant TB, or presumptive multi-drug–resistant TB |
Intervention | Automated real-time nucleic acid amplification test for rapid and simultaneous detection of TB and rifampicin resistance (e.g., Xpert MTB/RIF) |
Comparator | Smear microscopy, mycobacterial cultures, or culture-based drug susceptibility testing |
Outcomes | Cost-effectiveness |
Study designs | Economic evaluations |
MTB/RIF = M. tuberculosis complex and resistance to rifampicin; TB = tuberculosis.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2015.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Drummond checklist7 for economic evaluations as a guide. The strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
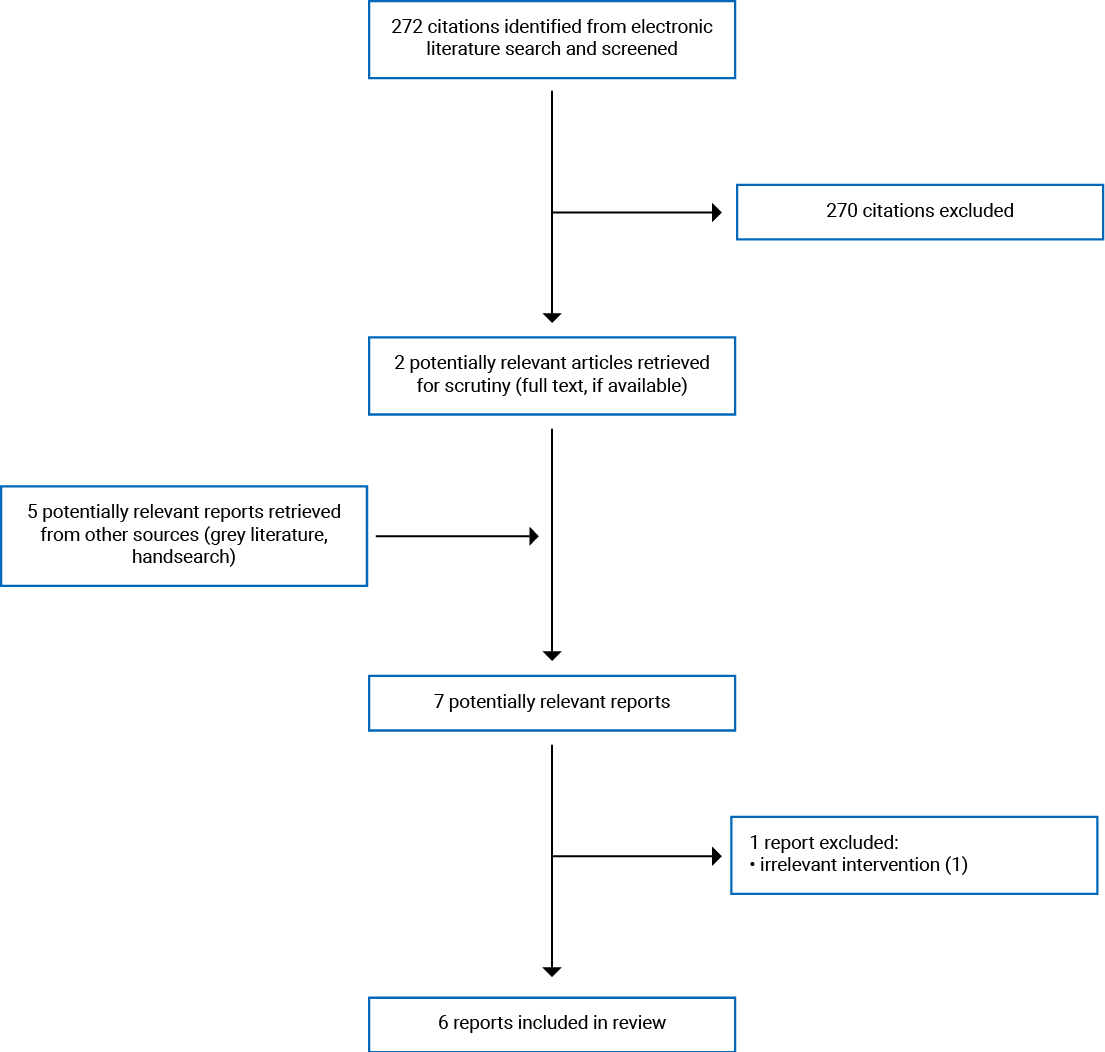
A total 272 citations were identified in the literature search. Following screening of titles and abstracts, 270 citations were excluded and 2 potentially relevant reports from the electronic search were retrieved for full-text review. Five potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 1 publication was excluded as the intervention was not relevant to this report. Six economic evaluations met the inclusion criteria and were included in this report.8-13 Appendix 1 presents the PRISMA14 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Six economic evaluations were included in this report.8-13 Among them, 1 publication was a health technology assessment that included a systematic review and meta-analysis of the clinical effectiveness of Xpert MTB/RIF testing in addition to an economic evaluation.13 Only the characteristics of the economic evaluation relevant to the report are summarized below.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The study by Khumsri et al.8 was a cost-effectiveness analysis using a societal perspective over a 1-year time horizon. A decision tree model was used for the analysis to represent a possible clinical pathway for correct TB diagnosis. Four categories of correct diagnosis were considered: true positive for TB and treated with anti-TB drugs, true positive for TB with rifampicin resistance (treated with second-line drugs for multi-drug resistance), false-negative patients treated with anti-TB drugs, and true negative patients (not treated). Clinical data were sourced from a single-centre randomized clinical study. Cost data were obtained from hospital database review and staff interviews. Utility data were obtained through the Thai version of the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) questionnaire from the clinical study participants. The key assumptions used in the study were unclear. The costs were reported in 2019 US dollars and no discount rates were used.
The study by Pooran et al.9 was a cost-effectiveness analysis using a health care provider perspective (National TB Programme), with a time horizon of 6 months. The analysis was based on a multi-centre, randomized, parallel-group trial (TB-NEAT) conducted in South Africa, Zimbabwe, Zambia, and Tanzania. The clinical states considered in the analysis were diagnosed, treatment initiated, treatment initiation on the same day of diagnosis, treatment completed, and improvement in morbidity. The clinical and cost data were obtained from the TB-NEAT trial. The costs were reported in 2014 US dollars. A discount rate of 3% was used. Assumptions considered in the model included patients who did not return for 2-month follow-up were assumed to be lost to follow-up; for patients who died during the study period, the duration between treatment initiation and death was assumed to be the treatment duration; and for symptomatic patients, a negative Xpert test or smear microscopy was assumed to be always followed up with a chest X-ray.
The study by Orlando and colleagues10 was a trial-based cost-effectiveness analysis that used a national health care perspective and a time horizon of 1 year. The analysis was based on a single-centre trial (DREAM) conducted in Mozambique among people living with HIV. The cost data were obtained from the DREAM program, Global Fund for TB therapy, and the literature. The model considered costs associated with a delay in diagnosis and health system–associated delay (e.g., due to logistics). The diagnostic pathways used in the analysis considered the statuses of undiagnosed, treated, and delayed diagnosis. The costs were reported in 2016 US dollars. A discount rate of 3% was used. All HIV-positive patients were assumed to be treated at a clinical centre with a high rate of retention to care. Patients were assumed to have follow-up visits every 3 months. Considering an infectious period of 15 days, maximum delay in diagnosis was assumed to be 105 days. Delay due to health system was assumed to be 61 days.
The study by Wilkman-Jorgensen et al.11 was a cost-utility analysis using a health care provider perspective and a time horizon of 90 years. A stochastic transmission Markov model was used. Costs were reported on 2013 US dollars. A discount rate of 3% was used. Clinical data were obtained from a descriptive study of a local TB program, the literature, and expert opinions. The cost data were obtained from proforma invoices, WHO tables for Kenyan settings (Mozambican data were not available), and from the Mozambican Ministry of Health. The different TB disease status levels considered in the model were susceptible to infection, latent infection (slow or fast progression), diseased (smear positive or negative), treated, and cured. The study assumed that there was no multi-drug–resistant TB, that the HIV incidence remained stable throughout the study period, that patients were not started on TB treatment empirically, and that there was homogenous mixing of individuals within the population.
The study by Pinto et al.12 was a cost-effectiveness analysis using a health care provider perspective (National TB Program [NTP]). The time horizon used was unclear. A deterministic decision tree simulation was used. Costs were reported in 2014 US dollars. No discounting was considered. Clinical data were sourced from a Brazilian trial (additional details not reported), and the National TB Information System. Cost data were obtained from a micro-costing analysis and from indexed prices. Treatment costs were from the literature and NTP guidelines. The study assumed that all TB patients were new cases and would undergo either sputum microscopy or Xpert testing. The probability of culture and drug susceptibility testing requested for new non-HIV TB cases was assumed as 10%. Specificity of diagnosis after both tests was assumed to be 80% and all diagnosed patients were assumed to be treated with first-line medication. Lastly, it was assumed that all symptomatic patients who tested negative in sputum microscopy or Xpert testing were diagnosed based on clinical and X-ray findings.
The study by Drobniewski et al.13 was a cost-effectiveness analysis using a provider perspective (National Health Service) and time horizons of 10 years and 20 years. An integrated transmission-dynamic and economic model was used. The infection status considered in the model included naïve, latent infection, preclinical disease, active disease, on treatment, and recovered. Cost was reported in British pounds. A discount rate of 3.5% was used. Clinical data were sourced from the systematic review and meta-analysis conducted by the authors, National TB institute of India, Health Protection Agency, and from the literature. Cost data were obtained from NHS reference costs and the British National Formulary. Utility data were sourced from Health Survey of England were estimated by the authors. Resource use parameters were obtained from WHO, National Institute for Clinical Excellence, expert opinions, and from the literature. The study authors assumed the cost incurred for transportation of tests when the testing was regional and an additional cost when the testing was local to account for the centre operating below capacity. They assumed that the patients with smear-negative disease were not initially admitted, whereas patients with smear-positive disease were always admitted.
Country of Origin
The study authors of the included studies were from Brazil,12 Italy,10 Mozambique,11 South Africa,9 Thailand,8 and the UK.13
Patient Population
Five of the included economic evaluations considered a target population of people with presumptive TB.8,9,11-13 One study involved a population of people living with HIV.10
The population of 1 study was from a local study conducted in a tertiary care hospital in Thailand and comprised 90 participants with presumptive TB.8 In the Pooran et al. study, the population were study participants of the TB-NEAT trial (N = 1,502).9 In the study by Orlando et al.,10 the population involved participants of a local study in Mozambique. In another study, the population was reported as the residents of the Ancuabe District in Mozambique.11 Additional details and characteristics of the population were not reported. The population involved in the fifth study was participants of a Brazilian trial.12 Additional details and the characteristics of the trial participants were not reported. Lastly, Drobniewski et al. considered ethnic groups in England and Wales as the study population.13 Specifically, South Asian, Black African, and Eastern European groups were considered in the evaluation. The population data were obtained from the 2011 census.
Interventions and Comparators
The intervention was Xpert MTB/RIF assay.8-13 The comparator was sputum smear microscopy in all included studies.8-13
Two studies outlined specific intervention and treatment strategies involving Xpert testing and smear microscopy.10,12 In 1 study,10 Xpert MTB/RIF testing was compared to a strategy of 4-symptom screening and smear microscopy in symptomatic patients. In the other study,12 intervention comprised an initial consultation, chest X-ray, Xpert testing of 1 sample, and HIV testing. The comparator strategy comprised initial consultation, chest X-ray, HIV testing, and sputum smear microscopy of 2 samples.
Wikman-Jorgensen et al.11 considered Xpert testing as a substitute to smear microscopy as well as an add-on to smear-negative cases. Lastly, in the study by Drobniewski et al.,13 Xpert testing in a local and regional setting were considered separately, depending on the setting of the Xpert test.
Outcomes
Five of the included studies reported results as incremental cost-effectiveness ratios (ICERs) of various outcomes.8-12 Khumsri et al.8 reported cost per quality-adjusted life-years (QALYs) and cost per diagnosis of 1,000 presumptive TB patients (ICER). In the study by Pooran et al.,9 incremental cost per clinical outcome of the culture-positive cases (ICER) were reported. The clinical outcomes considered in the analysis were diagnosed, treatment initiated, treatment initiation on the same day of diagnosis, treatment completed, and improvement in morbidity. Orlando and colleagues10 reported the ICER as cost per disability-adjusted life-years (DALYs) saved. Pinto et al.12 calculated ICER to report additional cost per detected TB case and per bacteriologically determined TB case. The fifth study, by Wilkman-Jorgensen et al.,11 reported ICER of DALY averted. Lastly, a study by Drobniewski et al.13 reported incremental QALYs and the incremental net benefit (INB) of adding Xpert testing in local and regional settings.
Summary of Critical Appraisal
The included economic evaluations had several strengths.8-13 The objectives and economic importance of the studies were described. The interventions and comparators of interest were clearly reported. The form of analysis and perspectives were described. The sources of input parameters in the analysis were mentioned.8-13 Currency, conversion rates, and price data used to report the results were described. Two9,10 of the studies used a trial-based analysis, and other 4 studies8,11-13 used modelling with parameters obtained from other sources to conduct analysis. All studies conducted sensitivity analyses and incremental effectiveness results were reported. Conclusions were consistent with the data reported and were accompanied by the appropriate caveats.8-13
In the study by Khumsri et al.,8 the input parameters were sourced from a single-centre study, and the rates were not discounted considering a shorter time horizon of 1 year. The assumptions used by the authors were unclear. In the study by Pooran et al.,9 the analyses were done using a time horizon of 6 months, which is a short time to complete treatment for TB and to measure improvement in morbidity. In the study by Wikman-Jorgensen et al.,11 some of the cost parameters used in the model were from Kenyan settings because local data were not available. This could lower the internal validity of the results. The study also assumed that there was no multi-drug–resistant TB, which may not be true in real-world clinical settings. In another study, the time horizon used was unclear, making the interpretation of results challenging.12 In the study by Drobniewski et al.,13 cost-effectiveness was assessed in 3 ethnic groups in the UK. The results of such an analysis may not be generalizable to settings where the population is multicultural and diverse. In the 2 studies9,10 that a trial-based analysis was conducted, the characteristics and demographics of the trial population were not reported. Therefore, the external validity of the results was unclear. Five studies conducted the evaluation from a provider perspective.9-13 The direct and indirect costs to the patients were not considered. Therefore, the economic benefit of the tests to the patients were unclear. Although the included studies discussed the results with limitations, there were several assumptions used that made it difficult to determine the reliability of results and whether the model would have been robust to changes in these issues. Lastly, none of the studies were conducted in Canada. Based on population, disease prevalence, and different willingness-to-pay (WTP) thresholds, generalizability to Canadian settings was unclear.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Additional details and findings from the included studies are provided in Appendix 4.
Cost-Effectiveness of Xpert Testing Compared With Smear Microscopy
Overall, the authors of the included studies concluded that Xpert testing is a cost-effective strategy compared to smear microscopy.8-13
The study by Khumsri et al.8 found that Xpert MTB/RIF test had lower total costs and higher gain of QALYs compared to sputum acid-fast bacillus (AFB) smear. Thus Xpert MTB/RIF testing was reported as dominant over a time horizon of 1 year. The cost-effectiveness plane also showed that Xpert MTB/RIF testing was more effective and less costly than sputum AFB testing, thus was reported as dominant.
Results from the study by Pooran et al9 found that the weighted average of incremental cost per clinical outcome of Xpert testing across all study sites (Tanzania, Zambia, Zimbabwe, and South Africa) ranged from US$561 for treatment initiation on the same day as diagnosis to US$4,185 for diagnosis by index test compared to smear microscopy over a 6-month time horizon. As per the cost-effectiveness acceptability curve, the WTP threshold at which a 90% probability of cost-effectiveness achieved for Xpert testing ranged from US$1,600 for treatment initiation on the same day of diagnosis to US$9,450 for diagnosed by index test. The probability of point-of-care Xpert testing being cost-effective was 90% at a WTP of US$3,820 per treatment completion (ICER US$1,210) Sensitivity analyses (tornado diagram) showed that annual test volume, expected useful life, and the purchase price of the GeneXpert machine influenced the ICER.
The results form 1 study10 among people living with HIV in Mozambique showed that Xpert MTB/RIF test was very cost-effective as the ICER (costs per DALY = US$56.54) was lower than the WTP of US$382 (1 gross domestic product [GDP] of Mozambique in 2016) using a time horizon of 1 year. One-way sensitivity analysis (tornado diagram) showed that the ICER per MTB/RIF compared with standard protocol was sensitive to the prevalence of TB in HIV-positive patients and the mortality among false-negative cases. However, strategies remained very cost-effective in all ranges of parameters used.
The cost-utility study by Wikman-Jorgensen et al.11 considered a WTP threshold of US$590 and a time horizon of 90 years. At that threshold, Xpert MTB/RIF testing was found to be cost-effective as a substitute to smear microscopy (ICER = US$122.13 per DALY averted) and as an add-on test to a smear-negative test (ICER = US$341.71 per DALY averted). In the probabilistic sensitivity analysis, Xpert MTB/RIF testing was within the WTP threshold in 60.6% of the runs. Results of the sensitivity analysis showed that the factors impacting the ICER were the risk of infection and TB prevalence.
Results from the study by Pinto et al.12 found that Xpert MTB/RIF testing resulted in 3.9% more TB diagnoses per 100,000 suspected cases and 26.1% bacteriologically confirmed cases compared with sputum smear microscopy. Thus, compared with smear microscopy, Xpert testing had an ICER of US$943 (per additional TB diagnosis) and US$356 (per additional TB diagnosis with bacteriological confirmation). Sensitivity analysis showed that the model was highly sensitive to changes in the specificity of clinical diagnosis following Xpert testing. A probabilistic simulation found a 95% probability of Xpert testing being cost-effective in all ranges of the WTP thresholds (US$100 to US$11,000)
The study by Drobniewski et al.13 reported INBs of Xpert testing compared with smear microscopy conducted in local and regional centres among 3 populations. In South Asian, Black African, and Eastern European populations, both local and regional GeneXpert testing were associated with significant INBs over time horizons of 10 and 20 years indicating cost-effectiveness with a threshold of £20,000 and £30,000. Sensitivity analyses (tornado diagram) showed that sensitivity and specificity of the test were the parameters that most influenced the INB in all populations.
Limitations
The main limitation of this report is the generalizability of the results to Canadian settings. Four of the included studies were conducted in African settings.9-12 One study was conducted in Thailand.8 In 1 study conducted in the UK, the effectiveness was calculated among 3 ethnic groups.13 Considering the differences in cost, population demography, socioeconomic status, and prevalence of TB in various subpopulations in Canada (e.g., Indigenous populations), the generalizability of the results to Canadian settings may not be possible.
Various assumptions were considered in the included studies related to the patients’ clinic visits,9 time incurred due to delay in diagnosis and health system diagnostics,10 homogenous mixing of individuals within the population,11 and additional costs incurred in local and regional testing sites.13 One study assumed that all TB patients were new patients.12 Another study assumed that there was no multi-drug–resistant TB.11 These assumptions may not be accurate in real-world settings. For example, it has been estimated that 4.1% of all newly diagnosed TB cases and 19% of recurrent TB cases are multi-drug resistant.15 Recurrent TB and multi-drug–resistant TB could be associated with additional costs and loss of QALYs related to longer treatment times and possible complications. Without considering these cost parameters in the model, the internal validity of the results could be low. Three of the studies conducted their analysis using a time horizon of 1 year or less.8-10 As TB is a chronic disease that may require long-term treatment and result in complications, a horizon of 1 year might be too short to sufficiently estimate the costs. The time horizon used in 1 study was unclear.12
Lastly, no evidence regarding the cost-effectiveness of Xpert MTB/RIF testing compared with mycobacterial cultures or culture-based susceptibility testing were found.
Conclusions and Implications for Decision- or Policy-Making
Six economic evaluations8-13 (5 cost-effectiveness analyses8-10,12,13 and 1 cost-utility analysis11) comparing the cost-effectiveness of Xpert MTB/RIF testing compared with smear microscopy were included in this report. No evidence regarding the cost-effectiveness of Xpert MTB/RIF testing compared with mycobacterial cultures or culture-based susceptibility testing were found. Overall, the authors of the included studies concluded that Xpert MTB/RIF testing was a cost-effective strategy compared with smear microscopy. The ICERs estimated by the included studies showed the cost-effectiveness of Xpert/MTB testing compared with smear microscopy and was consistent and robust across the studies.
However, the results were specific to the study settings. Findings need to be interpreted with caution considering the assumptions considered in the studies, methodological limitations, parameters considered, and limited generalizability to Canadian settings. Most of the included studies were conducted in African settings, where the prevalence of TB, social and demographic factors, and economic parameters are likely to be different from Canada. In 1 study conducted in the UK, the effectiveness was calculated among 3 ethnic groups. Considering the increased prevalence of TB in the Indigenous population, and the differences in socioeconomic parameters between Canada and the population included in the studies, the generalizability of the results to Canadian settings may not be possible.
A recently published CADTH report reviewed the diagnostic accuracy of Xpert testing.6 There was variability in the sensitivity and specificity of the tests as found in the included systematic reviews. The sensitivities of the Xpert test ranged between 62% and 85%, and the specificities ranged between 98% and 99%. Sensitivity analyses from 2 studies included in the current report found that the cost-effectiveness was influenced by the sensitivity and specificity of the test.12,13 Therefore, accurate estimates of these parameters may be important in establishing cost-effectiveness of Xpert testing. Current evidence suggests that rapid molecular testing such as Xpert MTB/RIF testing could be a cost-effective alternative to sputum smear microscopy. Economic evaluations conducted using parameters specific to Canadian settings is warranted to inform policy-making decisions.
References
1.World Health Organization. Global Tuberculosis report Geneva: World Health Organization 2020: https://www.who.int/docs/default-source/documents/tuberculosis/execsumm-11nov2020.pdf?sfvrsn=e1d925f_4. Accessed 18 Dec 2020.
2.Public Health Agency of Canada. Tuberculosis: Monitoring. 2019; https://www.canada.ca/en/public-health/services/diseases/tuberculosis/surveillance.html. Accessed 2020 December 18.
3.Pai M, Minion J, Jamieson F, Wolfe J, Behr M. Chapter 3: Canadian Tuberculosis Standards 7th Edition: 2014 – Diagnosis of active tuberculosis and drug resistance. 2014; https://www.canada.ca/en/public-health/services/infectious-diseases/canadian-tuberculosis-standards-7th-edition/edition-15.html#s3-1. Accessed 2020 December 18.
4.Centers for Disease Control and Prevention. A New Tool to Diagnose Tuberculosis: The Xpert MTB/RIF assay. https://www.cdc.gov/tb/publications/factsheets/pdf/xpertmtb-rifassayfactsheet_final.pdf. Accessed 2020 Decmber 18.
5.5Kumar D, Brett K, Argaez C. Rapid and simultaneous tuberculosis and antibiotic susceptibility testing for the diagnosis of pulmonary tuberculosis and rifampicin resistance: diagnostic accuracy and cost-effectiveness. Ottawa: CADTH; 2020 Jun. (CADTH rapid response report: summary of abstracts). CADTH rapid response report: summary of abstracts. Ottawa: CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RB1499%20GeneXpert%20Final.pdf. Accessed 2020 December 24.
6.Banerjee S, Severn M. Rapid and Simultaneous Tuberculosis and Antibiotic Susceptibility Testing for the Diagnosis of Pulmonary Tuberculosis and Rifampicin Resistance: A Review of Diagnostic Accuracy. CADTH rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/rr/2020/RC1317%20GeneXpert%20Upgrade%20Final.pdf. Accessed 2020 December 24.
7.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2020 December 24.
8.Khumsri J, Hanvoravongchai P, Hiransuthikul N, Chuchottaworn C. Cost-Effectiveness Analysis of Xpert MTB/RIF for Multi-Outcomes of Patients With Presumptive Pulmonary Tuberculosis in Thailand. Value Health Reg Issues. 2020;21:264-271. Medline
9.Pooran A, Theron G, Zijenah L, et al. Point of care Xpert MTB/RIF versus smear microscopy for tuberculosis diagnosis in southern African primary care clinics: a multicentre economic evaluation. Lancet Glob Health. 2019;7(6):e798-e807. Medline
10.Orlando S, Triulzi I, Ciccacci F, et al. Delayed diagnosis and treatment of tuberculosis in HIV+ patients in Mozambique: A cost-effectiveness analysis of screening protocols based on four symptom screening, smear microscopy, urine LAM test and Xpert MTB/RIF. PloS one. 2018;13(7):e0200523. Medline
11.Wikman-Jorgensen PE, Llenas-García J, Pérez-Porcuna TM, et al. Microscopic observation drug-susceptibility assay vs. Xpert(®) MTB/RIF for the diagnosis of tuberculosis in a rural African setting: a cost-utility analysis. Tropical medicine & international health: TM & IH. 2017;22(6):734-743. Medline
12.Pinto M, Steffen RE, Cobelens F, van den Hof S, Entringer A, Trajman A. Cost-effectiveness of the Xpert® MTB/RIF assay for tuberculosis diagnosis in Brazil. The international journal of tuberculosis and lung disease: the official journal of the International Union against Tuberculosis and Lung Disease. 2016;20(5):611-618.
13.Drobniewski F, Cooke M, Jordan J, et al. Systematic review, meta-analysis and economic modelling of molecular diagnostic tests for antibiotic resistance in tuberculosis. Health technology assessment (Winchester, England). 2015;19(34):1-188, vii-viii. Medline
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
15.World Health Organization. Global Tuberculosis Report 2017. Geneva: WHO; 2017: https://www.who.int/tb/publications/global_report/gtbr2017_main_text.pdf?ua=1. Accessed 01 Jan 2021.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Economic Evaluations
Study citation, country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach and outcomes | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Khumsri et al. (2020)8 Country: Thailand Funding source: 90th Anniversary of Chulanlongkorn University Ratchadaphisek- somphot Fund, National Research Council of Thailand | Type of analysis: Cost-effectiveness analysis Time horizon: 1 year Perspective: Societal perspective including medical and patient costs | Target population:Individuals ≥ 18 years with presumptive TB Characteristics of the patient cohort: Number of participants = 90
No statistically significant differences between groups | Intervention: Xpert MTB/RIF assay Comparator: sputum AFB smear | Model: Decision tree Clinical pathways were designed based on the clinical study Ceiling threshold: 160,000 THB (US$5,079.36) per QALY Sensitivity analysis was conducted using the Monte Carlo simulation method for uncertainty and a 1-way sensitivity analysis for the effect of costs, diagnostic tests, and the prevalence of pulmonary TB patients Outcomes: Correct diagnosis, time to get correct diagnosis, and gain in QALYs | Costs were reported in 2019 US$.a No discount rate was used Source of clinical data: A clinical study conducted in an outpatient department of a tertiary care hospital (2016 to 2017) Participants were randomized to either Xpert MTB/RIF or sputum AFB smear. All samples were tested with sputum culture and for drug susceptibility. Outcome assessment and testing was blinded. Source of cost data: Hospital database review and health care staff interviews Source of utility data: 3 patient interviews with the Thai version of EQ-5D-5L: before the first OPD visit before diagnosis, at 1 month, and 3 months later | Assumptions made by the authors were unclear and/or not reported |
Pooran et al. (2019)9 (Part of TB-NEAT study) Country: South Africa Funding source: The European and Developing Countries Clinical Trials Partnership | Type of analysis: Cost-effectiveness analysis Time horizon: 6 months Perspective: Health care provider | Target population:Individuals with presumptive TB Characteristics of the patient cohort:(from TB-NEAT trial): Number of participants = 1,502
| Intervention: Xpert MTB/RIF performed at point of care Comparator: same-day smear microscopy | Trial-based analysis Cost-effectiveness for diagnosed, treatment initiated, treatment initiation on the same day of diagnosis, treatment completed, and improvement in morbidity (numerical TB score) Univariate sensitivity analysis, probabilistic sensitivity analyses, and scenario analyses conducted WTP thresholds:
| Costs reported in 2014 US$ converted from currencies of the participating countries accruing to historic exchange rates. Discount rate: 3% Source of clinical data: TB-NEAT randomized, 2-group, parallel-group study conducted in South Africa, Zimbabwe, Zambia, and Tanzania Source of cost data: TB-NEAT trial, empirical data collected from each site Source of utility data: TB-NEAT randomized, 2-group, parallel-group study | Patients who started treatment but did not return for 2-month follow-up or were not on treatment were assumed to be lost to follow-up and/or defaulted and only costs incurred for 2 months were considered. For patients who died during the study period, length of treatment was considered as the duration between treatment initiation and death In symptomatic individuals who tested negative in Xpert MTB or smear microscopy, it was assumed that a chest X-ray was conducted |
Orlando et al. (2018)10 Country: Italy Funding source: Not reported | Type of analysis: Cost-effectiveness analysis Time horizon: 1 year Perspective: National health care perspective | Target population: People living with HIV Characteristics of patient cohort: Individuals who were HIV+ Number of patients = 1,000 Mean age = 35 years Other characteristics, demographics, and comorbidities of the cohort were not reported | Intervention: Xpert MTB/RIF for all participants Comparator: Standard 4-symptom screening and sputum smear microscopy in positive patients to symptom screening Symptoms included: fever, current cough, night sweats, and weight loss | Analysis based on a trial in Mozambique, based on DREAM program Model conducted a simulation on a sample of 1,000 HIV+ patients Economic burden due to delay in diagnosis and treatment plus health system organization delay were considered in the model Outcomes: DALYs saved 1-way sensitivity analysis and ICER calculated and completed on key parameters Threshold of effectiveness: Interventions were considered “very cost-effective” if ICER was below per capita GDP Mozambique (US$382 in 2016) and “cost-effective” if ICER was below 3 times the per capita GDP (US$1,146) | Costs were reported in 2016 US$. Discount rate: 3% Source of clinical data: Local clinical study, literature, and DREAM data Source of cost data: estimated from DREAM program, Global Fund for TB therapy, and literature | It was assumed that all HIV+ patients were treated at a clinical centre with a high rate of retention to care HIV+ patients were assumed to be seen at the clinics every 3 months when TB could be diagnosed and treated. Considering a 15-day infectious period, maximum delay in diagnosis would be 105 days A health system delay of 61 days was assumed 5 new transmitted cases were assumed to occur among HIV+ patients |
Wikman-Jorgensen et al. (2017)11 Country: Mozambique Funding source: Not reported | Type of analysis: Cost-utility analysis Time horizon: 90 years Perspective: Health care provider | Target population: Residents of the Ancuabe District in Mozambique Characteristics of the patient cohort: Not reported | Intervention: Xpert MTB/RIF Comparator: smear microscopy Strategies considered:
| Model: Stochastic transmission Markov model 1-way sensitivity analysis performed for TB prevalence, risk of infection sensitivity of the techniques for HIV-infected and not HIV-infected patients, and discount rate Monte Carlo simulation used for probabilistic sensitivity analysis WTP threshold established at 1 times the per capita GNI of Mozambique in 2013 (US$590) Cost evaluation conducted using micro-costing methods | Costs reported in 2013 US$. Discount rate: 3% yearly applied to both costs and effectiveness Source of clinical data: A descriptive study of local TB program, literature, and expert consultations Source of cost data: Proforma invoices, WHO tables for items lifetime (when Mozambique data were not available, data from Kenyan settings were used); Mozambican Ministry of Health (labour costs) | Model assumptions:
|
Pinto et al. (2016)12 Country: Brazil Funding source: InCo-TB project | Type of analysis: Cost-effectiveness analysis Time horizon: Not reported Perspective: Provider (National TB program perspective) | Target population: Individuals with presumptive TB Characteristics of the patient cohort: Not reported | Intervention: Diagnostic strategy including initial consultation, chest X-ray, Xpert testing of 1 sample, and HIV testing Comparator: Standard of care strategy (initial consultation, chest X-ray, sputum smear microscopy of 2 sputum samples, and HIV testing) In both strategies, individuals with HIV coinfection undergo drug susceptibility training. If clinical diagnosis made, patients treated with standard first-line drug regimen | Model: Deterministic decision tree simulation Input parameters: Cohort details, diagnostic parameters of the tests (sensitivity and specificity of Xpert and sputum smear microscopy), clinical diagnosis, costs associated with the strategies End points: additional TB cases diagnosed and additional TB cases confirmed using bacteriological culture Secondary end point: number of false-positive TB diagnosis avoided ICER calculated to describe additional cost per detected TB case and per bacteriologically determined TB case | Costs reported in 2014 US$.b No discounting was considered Source of clinical data: A trial of Xpert in Brazil, National TB Information system (SINAN), assumption Source of cost data: Micro-costing analysis and indexed prices. Treatment costs were from literature and NTP guidelines | Model assumptions:
|
Drobniewski et al. (2015)13 Country: UK Funding source: NIHR HTA program as project number 10/96/01 | Type of analysis: Cost-effectiveness analysis Time horizon: 10 year and 20 year Perspective: Health care provider perspective (NHS) | Target population: Individuals tested for suspected TB Ethnic groups in England and Wales (Black African, South Asian, and Eastern European) were considered Characteristics of the patient cohort: South Asian: 1,469,558 UK born; 1,515,112 foreign bornc Black African: 323,276 UK born; 666,352 foreign bornd Eastern European: 1,114,368 foreign borne | Intervention: GeneXpert (centralized and localized testing were considered) Comparator: Current practice (smear microscopy) | Model: Integrated transmission-dynamic and economic model Parameters included TB natural history, screening, and transmission data; diagnostic tests (e.g., sensitivity, specificity); costs of health care resources, treatments, and contact tracing; utility costs (QALY due to TB treatment adverse effects and case fatality risk) Probabilistic sensitivity analyses performed with 10,000 parameter sets to report incremental costs and incremental QALYs, and deterministic sensitivity analysis Outcomes: QALY loss associated with TB and treatment | Costs reported in £. Discount rate: 3.5% Source of clinical data: systematic review, literature, National TB institute of India, Health Protection Agency, and assumptions. Source of cost data: NHS reference costs, local data, and British National Formulary Source of utility data: Health survey for England, literature, and estimated by authors Source of resource use parameters: WHO, NICE, literature, assumptions, and expert opinion |
|
AFB = acid-fast bacilli; DALY = disability-adjusted life-year; GDP = gross domestic product; GNI = gross national income; HIV+ = HIV positive; HTA = Health Technology Assessment; ICER = incremental cost-effectiveness ratio; LF-LAM = lateral flow urine lipoarabinomannan assay; MTB = M. tuberculosis; MTB/RIF = M. tuberculosis complex and resistance to rifampicin; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; NIHR = National Institute of Health Research; OPD = outpatient department; QALY = quality-adjusted life-year; SSM = sputum smear microscopy; TB = tuberculosis; THB = Thai Bhat.
aCost conversion rate in 2019: 31.5 THB = US$1.
bCost conversion rate in 2014: 2.40 Brazilian reais = US$1.
cSouth Asian UK birth rate: 0.038 per annum; immigration rate: 0.07 per annum.
dBlack African UK birth rate: 0.067 per annum; immigration rate: 0.04 to 0.07 per annum.
eEastern European UK population size and birth rate not available; immigration rate: 0.11 per annum.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist7
Strengths | Limitations |
Khumsri et al. (2020)8 | |
|
|
Pooran et al. (2019)9 | |
|
|
Orlando et al. (2018)10 | |
|
|
Wikman-Jorgensen et al. (2017)11 | |
|
|
Pinto et al. (2016)12 | |
|
|
Drobniewsket al. (2015)13 | |
|
|
TB = tuberculosis; WTP = willingness to pay.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Economic Evaluations
Khumsri et al. (2020)8
Main Study Findings
Costs reported in 2018 US dollars
Threshold: US$5,079.36 per QALY
ICER calculated as: [Total Cost Xpert MTB/RIF – Total Cost Sputum AFB Smear] / [Total Outcome Xpert MTB/RIF – Total Outcome Sputum AFB Smear]
Study findings:
Base case
Costs
Xpert MTB/RIF: US$143,119.53
Sputum AFB smear: US$198,030.97
Time to get correct diagnosis (days)
Xpert MTB/RIF: mean = 1.88 (standard deviation [SD] = 1.07)
Sputum AFB smear: mean = 4.11 (SD = 2.22)
Mean difference = –2.23 days (95% confidence interval [CI], –3.047 to –1.425; P < 0.001)
Correct diagnosis per 1,000 presumptive pulmonary TB patients
Xpert MTB/RIF: n = 907
Sputum AFB Smear: n = 724
Cost-effectiveness ratio per correct diagnosis
Xpert MTB/RIF: 158.31
Sputum AFB smear: 273.52
ICER: dominant
QALYs gained per 1,000 presumptive pulmonary TB patients
Xpert MTB/RIF: 947.14
Sputum AFB Smear: 939.84
Cost-effectiveness ratio per QALY
Xpert MTB/RIF: 151.11
Sputum AFB Smear: 208.95
ICER: Dominant
Sensitivity analyses: 1,000 cohort simulations (1,000):
Average correct diagnosis
Xpert MTB/RIF: n = 673 (95% CI, 655.21 to 691.22)
Sputum AFB smear: n = 592 (95% CI, 577.34 to 605.84)
Difference = 81 patients
QALYs gained
Xpert MTB/RIF = 945.85 (95% CI, 945.7 to 945.98)
Sputum AFB Smear = 940.40 (95% CI, 940.27 to 940.53)
Difference = 5.45 years
“The probabilistic sensitivity analysis was presented by CE plane, in which the Xpert MTB/RIF method remained dominant (p. 268)”8 for correct diagnosis as well as QALYS gained.
Authors’ Conclusion
“Using Xpert MTB/RIF in the initial TB diagnosis in adult patients presumed to have TB can shorten the time to achieve a correct diagnosis. Moreover, Xpert MTB/RIF is considerably cost-effective for multi-outcomes. These study results are essential empirical evidence for policy makers who wish to evaluate the National Strategic Plan for TB in Thailand in setting up and choosing TB diagnostic tools that are significantly cost-effective and worthy (p. 270).”8
Pooran et al. (2019)9
Main Study Findings
Study findings:
Estimated outcomes and total costs of same-day smear microscopy compared to clinic-based Xpert MTB/RIF, per 1,000 individuals presenting with TB symptoms to a primary care clinic.
Diagnosed by index test
Culture-positive cases
Smear microscopy: n = 245.3
Xpert MTB/RIF: n = 253.8
Difference = 8.5 (95% CI, −37.5 to 54.5)
Treatment initiated
Culture-positive cases
Smear microscopy: n = 207.5
Xpert MTB/RIF: n = 231.8
Difference = 24.3 (95% CI, −20 to 68.5)
Total cases
Smear microscopy: n = 423.2
Xpert MTB/RIF: n = 432.1
Difference = 9.0 (95% CI, −42.0 to 59.8)
Treatment initiation on the same day of diagnosis
Culture-positive cases
Smear microscopy: n = 90.3
Xpert MTB/RIF: n = 153.6
Difference = 63.4 (95% CI, 27.3 to 99.4)
Total cases
Smear microscopy: n = 149.6
Xpert MTB/RIF: n = 225.0
Difference = 75.4 (95% CI, 33.5 to 117.3)
Treatment completed
Culture-positive cases
Smear microscopy: n = 107.8
Xpert MTB/RIF: n = 137.2
Difference = 29.4 (95% CI, –6.9 to 65.6)
Total cases
Smear microscopy: n = 226.4
Xpert MTB/RIF: n = 245.5
Difference = 19.2 (95% CI, – 26.1 to 64.3)
Improvement in morbidity
Culture-positive cases
Smear microscopy: n = 115.9
Xpert MTB/RIF: n = 134.4
Difference = 18.6 (95% CI, –18.0 to 55.1)
Total cases
Smear microscopy: n = 243.9
Xpert MTB/RIF: n = 251.0
Difference = 7.1 (95% CI, –38.7 to 52.9)
ICER (incremental cost per clinical outcome among culture-positive cases in 2014 US dollars)
Diagnosed by index test
Tanzania: US$4,254
Zambia: Xpert dominated
Zimbabwe: US$1,675
South Africa: US$1,373
All sites (weighted average): US$4,185
Treatment initiated
Tanzania: US$1,554
Zambia: US$2,699
Zimbabwe: US$1,685
South Africa: US$984
All sites (weighted average): US$1,463
Treatment initiation on the same day of diagnosis
Tanzania: US$1,107
Zambia: US$785
Zimbabwe: US$399
South Africa: US$460
All sites (weighted average): US$561
Treatment completed
Tanzania: US$521
Zambia: US$465
Zimbabwe: US$4,309
South Africa: US$8,485
All sites (weighted average): US$1,210
Improvement in morbidity
Tanzania: US$508
Zambia: US$2,024
Zimbabwe: US$1,710
South Africa: US$3,101
All sites (weighted average): US$1,918
WTP threshold (at which a 90% probability of cost-effectiveness achieved) as per the cost-effectiveness acceptability curves
Diagnosed by index test: WTP = US$9,450
Treatment initiated: WTP = US$4,450
Treatment initiation on the same day of diagnosis: WTP = US$1,600
Treatment completed: WTP = US$3,820
Improvement in morbidity: WTP = US$5,840
Authors’ Conclusion
“In summary, we have estimated the cost-effectiveness of implementing Xpert at the point of care in four different African settings. Overall, our results indicate that a point-of-care-based Xpert can offer good value for money relative to other tuberculosis diagnostic strategies, though the cost-effectiveness of this strategy is likely to be even higher given that transmission reduction and drug resistance detection were not factored into the analysis. These findings will facilitate decision making about public health strategy and resource allocation by NTPs so that cost savings and health benefits can be maximised (p. 10).”9
Orlando et al. (2018)10
Main Study Findings
Study findings:
DALYs saved:
Standard = 1,107
MTB/RIF = 1,281
Cost per DALY saved:
Delayed diagnosis ($)
Standard = 79.06
MTB/RIF = 14.18
Delayed diagnosis + health system delay
Standard = 133
MTB/RIF = 72.02
ICER per DALY saved (compared to standard strategy, excluding costs of newly transmitted infections)
MTB/RIF = 56.54
“Given that the ICER of MTB/RIF and LF-LAM / MTB/RIF protocols versus standard protocol is lower than per capita GDP of Mozambique, the diagnosis and treatment evaluated are very cost-effective (p. 6).”10
Sensitivity analyses:
ICER per DALY saved (compared to standard strategy, including costs of newly transmitted infections).
MTB/RIF versus standard strategy:
“ICER was strongly influenced by the prevalence of TB in HIV+ patients. When prevalence included the minimum value (5.05%), the ICER reached the maximum value of 123.18 as opposed to the case base of 56.54. Cost-effectiveness was sensitive to the cost of the MTB/RIF assays with a minimum value of 14.25 if the cost was lower ($7.36) than the base case (p. 8).”10
All strategies remained very cost-effective (ICER < US$382) in all ranges of parameters used.
Authors’ Conclusion
“This study showed that MTB/RIF protocol is cost-effective compared to standard and LF-LAM / MTB/RIF protocol in PLHIV [people living with HIV], especially in countries with high HIV and TB prevalence such as Mozambique (p. 13).”10
Wikman-Jorgensen et al. (2017)11
Main Study Findings
Study findings:
Xpert as substitute for smear microscopy: ICER: US$345.71 per DALY averted
Xpert MTB/RIF as add-on test to 1 smear-negative test: ICER: US$122.13 per DALY averted
Results of the sensitivity analysis showed that the factors impacting ICER were the risk of infection and TB prevalence. A 10% reduction was applied, and the ICER did not rise significantly (US$346.08 per DALY averted) when a 10% reduction was applied in the probability of completing the diagnostic pathway in the add-on strategy.
In the probabilistic sensitivity analysis, Xpert MTB/RIF was within the WTP threshold in 60.6% of the runs.
Authors’ Conclusion
“In summary, replacing SM with Xpert MTB/RIF for the evaluation of all TB suspects was most likely to be cost-effective in this rural and remote African setting. Our results reinforce the WHO recommendation of Xpert_ MTB/RIF being the first diagnostic test in every pulmonary TB suspect and add to a growing body of evidence, suggesting that SM is a technique to replace when possible (p. 741).”11
Pinto et al. (2016)12
Main Study Findings
Study findings:
Total costs per 100,000 cases of presumptive TB (2014 US dollars)
Sputum smear microscopy = US$37,713,000
Xpert MTB/RIF = US$38,902,000
Cost-effectiveness
Total TB diagnosis per 100,000 cases of presumptive TB
Sputum smear microscopy: n = 32,773
Xpert MTB/RIF: n = 34,034
Difference = 3.9%
ICER (cost per additional diagnosis) = US$943 (95% uncertainty range [UR] US$851 to US$992)
Additional TB diagnosis with bacteriological confirmation
Sputum smear microscopy: n = 12,836
Xpert MTB/RIF: n = 16,180
Difference = 26.1%
ICER = US$356 (95% UR US$292 to US$641)
“The Monte Carlo probabilistic simulation yielded a 95% probability of being cost-effective in all ranges of willingness-to-pay threshold to both outcomes (US$100–US$11 000) (p. 616).”12
Sensitivity analyses:
“Using the NRT value for SSM, the ICER would be US$1597 (95%UR 1510–2585) for each additional TB diagnosis and US$602 (95%UR 597–658) for each additional TB diagnosis with bacteriological confirmation (p. 616).”12
Authors’ Conclusion
“Our results support the Brazilian Ministry of Health’s decision to incorporate Xpert into the NTP’s diagnostic strategy. Moreover, because of the wide range of parameters and costs used, it is likely that similar results would be found in other countries, although the specific characteristics of the health system, the prevalence of the disease and health care practices should be analysed in each setting before the implementation of a new diagnostic test. Other non-economic perspectives should (p. 617).”12
Drobniewsket al. (2015)13
Main Study Findings
Study findings:
South Asian population
Cost-effectiveness plane showed that GeneXpert was associated with significant INBs compared to the current strategy, indicating cost-effectiveness with a threshold of £20,000 and £30,000. This effectiveness was observed over a 10-year horizon and 20-year horizon.
Time horizon 10 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 148.3 (95% CI, 147.5 to 149.1)
GeneXpert regional = 151.3 (95% CI, 150.5 to 152.0)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 20.3 (95% CI, 20.3 to 20.4)
GeneXpert regional = 20.2 (95% CI, 20.1 to 20.2)
Threshold QALY = £30,000
GeneXpert local = 21.8 (95% CI, 21.7 to 21.9)
GeneXpert regional = 21.7 (95% CI, 21.6 to 21.8)
Time horizon 20 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 282.9 (95% CI, 280.2 to 285.7)
GeneXpert regional = 350.4 (95% CI, 347.9 to 352.9)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 35.4 (95% CI, 35.3 to 35.6)
GeneXpert regional = 36.3 (95% CI, 36.2 to 36.5)
Threshold QALY = £30,000
GeneXpert local = 38.3 (95% CI, 38.1 to 38.4)
GeneXpert regional = 39.8 (95% CI, 39.7 to 40.0)
Black African population
Cost-effectiveness plane showed that all Xpert testing were associated with significant INBs compared to the current strategy, indicating cost-effectiveness with a threshold of £20,000 and £30,000, over 10-year time horizon and a 20-year time horizon.
Time horizon 10 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 179.4 (95% CI, 177.8 to 180.9)
GeneXpert regional = 152.2 (95% CI, 150.7 to 153.7)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 16.8 (95% CI, 16.7 to 16.9)
GeneXpert regional = 16.1 (95% CI, 16.0 to 16.2)
Threshold QALY = £30,000
GeneXpert local = 18.6 (95% CI, 18.5 to 18.7)
GeneXpert regional = 17.6 (95% CI, 17.6 to 17.7)
Time horizon 20 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 504.4 (95% CI, 499.8 to 509.0)
GeneXpert regional = 418.6 (95% CI, 414.0 to 423.1)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 33 (95% CI, 32.9 to 33.2)
GeneXpert regional = 31.1 (95% CI, 30.9 to 31.3)
Threshold QALY = £30,000
GeneXpert local = 38.1 (95% CI, 37.9 to 38.3)
GeneXpert regional = 35.3 (95% CI, 35.1 to 35.5)
Eastern European population
Cost-effectiveness plane showed that all Xpert testing were associated with significant and “modest” INBs compared to the current strategy, indicating cost-effectiveness with a threshold of £20,000 and £30,000, over a 10-year time horizon and 20-year time horizon.
Time horizon 10 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 3.8005 (95% CI, 3.7562 to 3.8449)
GeneXpert regional = 3.0969 (95% CI, 3.053 to 3.1407)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 0.8047 (95% CI, 0.8015 to 0.808)
GeneXpert regional = 0.7909 (95% CI, 0.7876 to 0.7941)
Threshold QALY = £30,000
GeneXpert local = 0.8427 (95% CI, 0.8394 to 0.8461)
GeneXpert regional = 0.8218 (95% CI, 0.8185 to 0.8252)
Time horizon 20 years
Incremental QALYs (compared to current strategy)
GeneXpert local = 8.8709 (95% CI, 8.7592 to 8.9825)
GeneXpert regional = 7.1578 (95% CI, 7.0473 to 7.2683)
INB of adding molecular testing
Threshold QALY = £20,000
GeneXpert local = 1.4228 (95% CI, 1.417 to 1.4285)
GeneXpert regional = 1.3889 (95% CI, 1.3831 to 1.3946)
Threshold QALY = £30,000
GeneXpert local = 1.5115 (95% CI, 1.5052 to 1.5178)
GeneXpert regional = 1.4604 (95% CI, 1.4542 to 1.4667)
Authors’ Conclusion
“The results of the transmission modelling suggest that all assays are cost saving and achieved an increase in QALYs compared with current practice. For the Black African and Eastern European populations, GeneXpert was likely to be the most cost-effective approach compared with current practice. For the South Asian population, the MTBDRplus assay was most favourable achieving the highest INB compared with current practice. ‘Real-life’ and ‘real clinical use’ evaluation studies, both retrospective and prospective studies within the UK, and comparable environments are needed to determine if the trial performance of these tests is maintained in real NHS use (p. 125).”13
Appendix 5: References of Potential Interest
Previous CADTH Report
1.CADTH. Rapid and Simultaneous Tuberculosis and Antibiotic Susceptibility Testing for the Diagnosis of Pulmonary Tuberculosis and Rifampicin Resistance: Diagnostic Accuracy and Cost-Effectiveness; 2020 Jun. https://www.cadth.ca/rapid-and-simultaneous-tuberculosis-and-antibiotic-susceptibility-testing-diagnosis-pulmonary
Study With Alternate Intervention
2.Lee DJ, Kumarasamy N, Resch SC, et al. Rapid, point-of-care diagnosis of tuberculosis with novel Truenat assay: cost-effectiveness analysis for India's public sector. PLoS One. 2019;14(7):e0218890. Medline
Acknowledgements: Holly Gunn, Srabani Banerjee
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca