CADTH Health Technology Review
Droperidol for Agitation in Acute Care
Rapid Review
Authors: Rob Edge, Charlene Argáez
Abbreviations
AAEM
American Academy of Emergency Medicine
AMSS
Altered Mental Status Scale
BARS
Behavioural Activity Rating Scale
COI
conflict of interest
ECG
electrocardiogram
ED
emergency department
EPS
extrapyramidal symptoms
ETCO2
end-tidal carbon dioxide
IM
intramuscular
LOS
length of stay
MA
meta-analysis
PICO
population, intervention, comparator, outcome
PICU
psychiatric intensive care unit
QTc
corrected QT interval
RCT
randomized controlled trial
RR
relative risk
SpO2
peripheral oxygen saturation
SR
systematic review
Key Messages
Comparative evidence supports that droperidol is as effective as haloperidol and olanzapine for the sedation of adult patients with uncontrolled aggression, anxiety, or violent behaviour in acute care settings, and a limited quantity of evidence supports the superiority of droperidol over ziprasidone and lorazepam monotherapies.
There are no statistically significant differences in adverse event frequency or severity in adult patients treated with droperidol compared with haloperidol or olanzapine.
Guidelines published in 2015 support the safety and efficacy of droperidol treatment for agitation based on high-quality relevant evidence.
These guidelines found insufficient evidence to support electrocardiogram or telemetry monitoring of patients who were administered less than 2.5 mg of droperidol.
Context and Policy Issues
Agitation, aggression, and violent behaviour commonly present in acute care settings and may be a factor in up to 2.6% of emergency department (ED) encounters in the US.1,2 Agitation is often of unknown or multifactorial etiology; however, it is commonly a result of alcohol or drug intoxication, trauma, or mental health disorders.3,4 Patients with agitation can present a risk to staff, other patients, and property. Therefore, for cases in which verbal de-escalation fails, physical restraint and sedation may be required to ensure a safe environment where further acute care diagnosis and treatment can proceed.5,6 Treatment goals for this indication are rapid and safe sedation.6
Droperidol is a butyrophenone used in acute care settings for a variety of purposes, including the rapid sedation of patients with agitation, aggression, or who are exhibiting violent behaviour.4,7 Droperidol can be administered intravenously and it can also be administered intramuscularly, which has practical advantages when safely dealing with agitated patients.7 Many antipsychotic drugs, including droperidol, haloperidol, and olanzapine, have a similar adverse event profile that includes serious events such as respiratory depression, cardiac events, and extrapyramidal symptoms (EPS).4
In 2001, a black box warning was issued by the US FDA for the use of droperidol based on post-marketing surveillance data.3,7 The black box warning emphasized careful patient selection and increased monitoring to prevent corrected QT (QTc) interval elongation in patients administered droperidol.7 QTc elongation can lead to sudden cardiac death. The extra burden placed on management of patients with droperidol has greatly decreased its use and availability in the US.7
The purpose of this report was to retrieve and review the current evidence on the safety and efficacy of droperidol for patients with agitation, aggression, or violent behaviour in acute care settings. In addition, this report aimed to retrieve and review relevant evidence-based guidelines regarding the use of droperidol in acute care settings.
Research Questions
What is the clinical effectiveness of droperidol for the management of violence and aggression in acute care settings?
What are the evidence-based guidelines regarding the use of droperidol in acute care settings?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were droperidol and acute care or agitation. No search filters were applied to limit retrieval to study type. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2010, and December 9, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adult patients in acute care settings |
Intervention | Droperidol |
Comparator | Standard care (i.e., other antipsychotic drugs, such as haloperidol or olanzapine) |
Outcomes | Research Question 1: Effectiveness (e.g., treatment agitation, aggression, violence) and safety Research Question 2: Recommendations regarding patient monitoring |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, observational comparative studies, and evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2010. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs, the Downs and Black checklist9 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
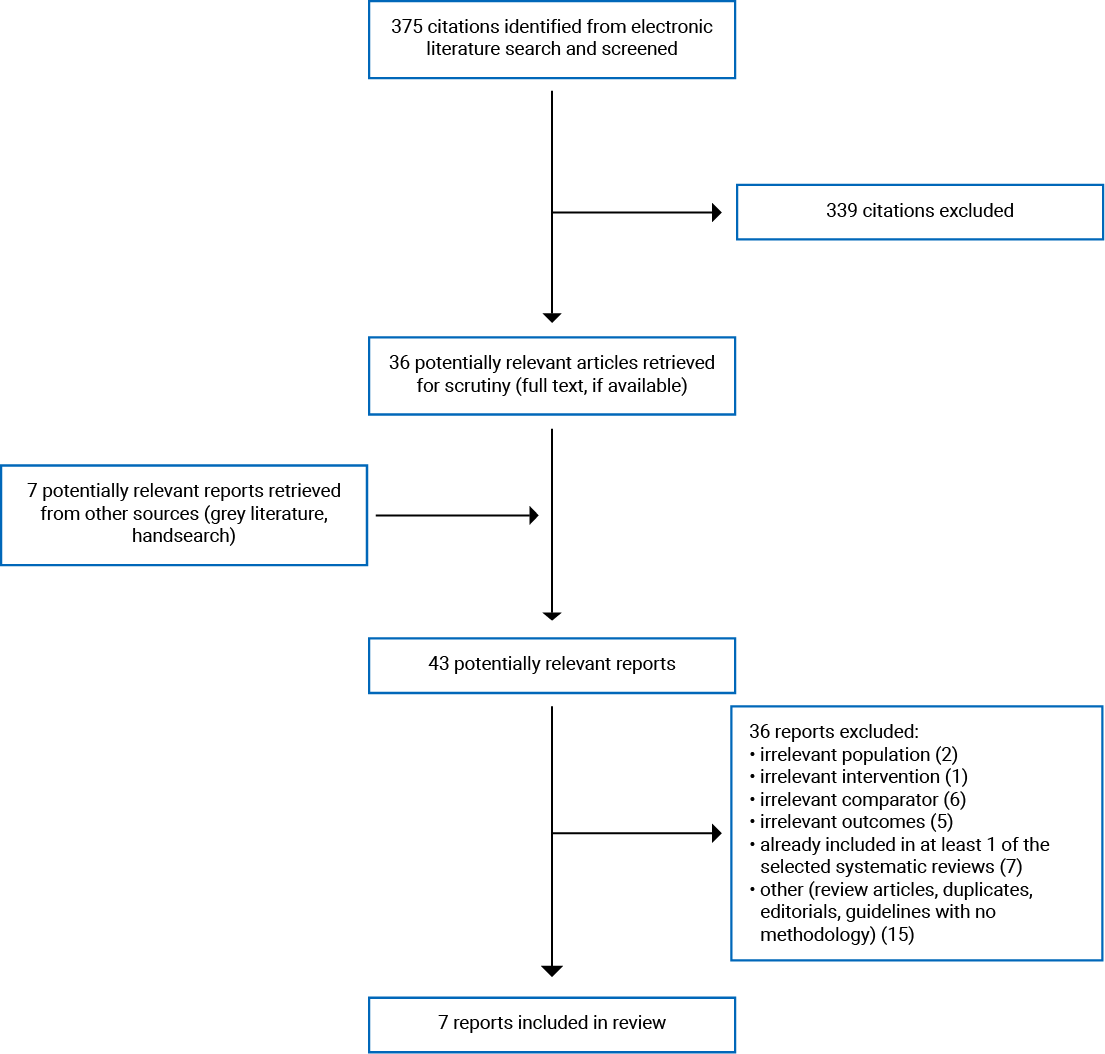
A total of 375 citations were identified in the literature search. Following screening of titles and abstracts, 339 citations were excluded and 36 potentially relevant reports from the electronic search were retrieved for full-text review. Seven potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 43 potentially relevant articles, 36 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews (SRs), 1 randomized controlled trial (RCT), 3 non-randomized studies, and 1 evidence-based guideline.
The included RCT was published in 2020 but was conducted between 2003 and 2005.2 Although the authors stated that the dataset was previously unpublished, a subset of the same authors published results of an RCT conducted in 2005 within the same ED in Minneapolis, Minnesota. This study, Martel et al. (2005),11 was identified by 1 of the 2 SRs included in this report.6,11 The potential overlap of this evidence is therefore unclear.
Furthermore, 2 relevant retrospective observational studies were conducted at the same Minneapolis ED, overlapped chronologically, and included some of the same authors. Therefore, these 2 studies may include overlapping evidence. However, as suggested by patient numbers, patient inclusion criteria, and reported outcomes, these studies were not entirely overlapping (i.e., some unique patients were included); therefore, both are included in this report.3,4 These retrospective observational studies did not overlap with the Martel et al. (2020) RCT.
Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)12 flow chart of the study selection. Appendix 5 presents the overlap of primary study evidence of the SRs included in this report.
Summary of Study Characteristics
Both SRs had broader inclusion criteria than the present review.6,13 Specifically, both SRs included studies that examined any chemical restraint intervention in acute care settings.6,13 Only the characteristics and results of the subset of relevant studies are described in this report.
Study Design
Two SRs were identified that fit the inclusion criteria presented in Table 1.6,13 Muir-Cochrane et al. was published in 2020 and identified 23 RCTs, 8 study arms of which were relevant to this report.6 Bak et al. was published in 2019 and identified 53 RCTs and 1 SR; 8 of these RCTs and the SR were relevant to this report.13
Four primary studies are included in this report: 1 RCT published in 20202 and 3 retrospective observational studies.3,4,14
One guideline with relevant recommendations was identified and included in this report.7 Recommendations were formulated by the American Academy of Emergency Medicine (AAEM) using evidence collected by a systematic literature search of all study designs, using human subjects, and published in the English language. All relevant supporting evidence was assigned a quality category based upon study design and methodology, as well as a grade based upon study design and relevance to the research question. Quality categories ranged from outstanding (highest) to unsatisfactory (lowest), while grade categories ranged from Grade A (highest) to Grade F (lowest). Recommendations were assigned a class; however, it was not clear how these related to the assigned quality and grade categories.
Country of Origin
The included SRs originated in Australia6 and the Netherlands.13 All primary studies were conducted and authored in the US.2-4,14 Two of the retrospective observational studies were conducted at the same ED in Minneapolis and had overlapping study time frames.3,4 The identified guidelines were also from the US; however, the AAEM did not specify that the recommendations were intended to apply to American emergency physicians.7
Patient Population
The SR from Australia included adult patients with uncontrolled aggression, anxiety, or violent behaviour, or patients with mental health conditions who were non-consenting to treatment.6 The SR from the Netherlands included adults with psychiatric disorders or intoxication encountered in the ED or mental health ward.13
The RCT (Martel et al. 2020)2 enrolled adults older than 18 years requiring parenteral sedation for acute agitation. The study excluded patients who were prisoners, in police custody, pregnant, breastfeeding, had a relevant allergy, or were capable of providing consent but did not consent to treatment. The authors also stated that safety considerations may have impacted enrolment.2
Two of the retrospective observation studies included adult patients in the same ED that presented with alcohol intoxication and altered mental status.3,4 Cole et al. also reported that a blood ethanol concentration greater than 80 mg/dL was required for patient inclusion.3 The third retrospective observational study included patients who behaved in a manner that posed a threat to their own well-being and/or others, were combative, or had a head injury that required prehospital physical restraint. Included patients had a median age of 31 years.14
The guidelines focused on the safety aspects of droperidol administration to patients in the ED for any indication.7
Interventions and Comparators
The 2 SRs had a broad focus on chemical restraint of adults in acute care (including droperidol) and neither SR specified a comparator.6,13 Muir-Cochrane et al. identified RCT evidence on IV and intramuscular (IM) droperidol doses of 5 mg and 10 mg.6 Bak et al. identified RCT evidence on 4 mg, 5 mg, and 10 mg doses of droperidol without distinguishing between IM and IV administration routes. In the reporting of evidence, Bak et al. reported outcomes for each drug independently without the context of the comparator used in the individual RCTs.13
The RCT compared IM administration of 5 mg droperidol, 10 mg ziprasidone, 20 mg ziprasidone, and 2 mg lorazepam.2
Two retrospective observational studies with possible overlap of included patients compared droperidol, haloperidol, and olanzapine antipsychotic drugs.3,4 The median doses for both studies were 5 mg droperidol, 5 mg haloperidol, or 10 mg olanzapine.3,4 Macht et al. compared a median droperidol dose of 2.9 mg to a median haloperidol dose of 7.9 mg following an ED protocol change from droperidol to haloperidol.14
The guidelines considered the intervention of droperidol, including whether appropriate and safe use of IM- or IV-administrated doses of droperidol less than 2.5 mg required electrocardiogram (ECG) or telemetry monitoring, and the safety of IM droperidol doses of up to 10 mg.7
Outcomes
The SR by Muir-Cochrane et al. included studies that reported any measures of aggression, agitation, or violent behaviours, and results were reported narratively. The meta-analysis (MA) component of the SR reported the combined results of 2 RCTs for the following outcomes: median time to calm, proportion of patients calm at 5 minutes, and proportion of patients calm at 10 minutes. The MA also examined if there was a significant correlation between antipsychotic drug dose and frequency of adverse events.6 Relevant outcomes in the SR by Bak et al. were proportion of patients experiencing adverse events, oversedation, EPS, acute dystonia, akathisia, hypotension or hypertension, and QTc elongation (> 500 ms).
The RCT reported the following outcomes: proportion adequately sedated at 15 minutes, severity of agitation using the Altered Mental Status Scale (AMSS), severity of agitation using the Behavioural Activity Rating Scale (BARS), the proportion of patients requiring additional sedation during the entire encounter, the proportion of patients requiring additional sedation before adequate sedation, the time until additional sedatives were administered, the ED length of stay (LOS), hospital LOS, nasal end-tidal carbon dioxide (ETCO2), peripheral oxygen saturation (SpO2), and QTc interval.2 The AMSS ranges from −4 to 4, with zero representing normal responsiveness, speech, facial expression, and no ptosis. On the AMSS scale, 4 represents an agitated patient with combative or violent responsiveness, loud outbursts of speech, agitated facial expressions, and no ptosis, while −4 represents an overly sedated patient who is unresponsive to mild prodding or shaking and has limited recognizable speech, marked relaxed facial expression with a slacked jaw, glazed eyes, and marked ptosis. Martel et al. did not report BARS outcomes but instead reported an analysis of the correlation between AMSS and BARS to demonstrate that observations were consistent.2
It is likely that Cole et al. and Klein et al. reported on an overlapping patient cohort; however, these studies focused on different outcomes.3,4 Cole et al. focused on ED LOS.3 Klein et al. also reported on ED LOS, but additionally reported the proportion of patients that required rescue sedation within 1 hour, the proportion of patients that required rescue sedation over the entire encounter, and adverse events that included the proportion of patients requiring intubation, experiencing torsades de points, cardiac arrest, akathisia, dystonia, anaphylaxis, and rash.4
Macht et al. reported on the proportion of patients requiring rescue sedation within 1 hour, QTc interval, adverse events including cardiac arrest and hypotension (SpO2 < 90 mm Hg), and events requiring intubation, bag mask ventilation, or administration of anti-dysrhythmic medication.14
The guidelines did not specify outcomes but reported a focus on therapeutic efficacy outcomes and outcomes related to ECG monitoring of patients administered droperidol.7
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The 2 SRs included in this review had important strengths, including a comprehensive systematic literature search, a PRISMA flow chart describing the literature selection, data extraction methodology, an MA, a table of study characteristics, critical appraisal methodology, and a discussion on the limitations of the study.6,13 Muir-Cochrane et al. contained additional unique strengths, including study selection that was conducted in duplicate, PICO (population, intervention, comparator, outcome)-formulated inclusion criteria, a statement of no potential conflicts of interest (COI), and an assessment of publication bias.6 Bak et al. did not formulate a PICO research question but had clear inclusion and exclusion criteria.13 The most important limitation of these SRs was a lack of critical appraisal reporting. Despite reporting an appropriate critical appraisal methodology for the included RCTs, appraisal results were not included in Bak et al. and were reported as a single numerical score in Muir-Cochrane et al. The potential bias in the body of evidence identified by these SRs was therefore unclear. The SR from Bak et al. lacked the unique strengths of Muir-Cochrane et al. and reported outcomes per study arm, removing information on the comparator used in the study, which may have removed important context. Muir-Cochrane et al. identified 2 RCTs relevant to the efficacy of droperidol that had suitable homogeneity for an MA. Bak et al. did not identify RCTs that reported the outcomes of interest on droperidol treatment for the MA, and reported only narratively on studies relevant to droperidol.13 Therefore, both MAs of the included SRs were limited by the quantity of identified evidence.6,13 The SR from Muir-Cochrane et al. reported limited comparative conclusions regarding the safety and dose of olanzapine compared to droperidol.6 In the SR by Bak et al., it was unclear whether adverse events were not reported or whether no adverse events occurred for some included RCTs.13
RCT
One RCT was identified that was not included in the SRs.2 This study had important methodological strengths including a CONSORT diagram of patient recruitment and enrolment, tabulated patient characteristics, sufficient randomization methodology, and appropriate statistical methods. The study clearly defined patient eligibility, interventions, and outcomes. Other strengths included sufficient power with no loss to follow-up, quantified adverse events, and a comprehensive discussion on the study’s limitations. A statement of no potential COIs was also provided. Although the study was published in 2020, it was conducted between 2003 and 2005, and the reporting delay may have introduced unknown bias. The delay was discussed in detail by the authors. The authors did not provide allocation concealment methodology, details regarding the role of blinded investigators, nor an analysis of potential confounders.
Non-Randomized Studies
Two of the identified retrospective observational studies, Cole et al. and Klein et al., may have reported different outcomes from a study with an overlapping patient cohort and therefore shared similar strengths and limitations regarding methodology.3,4 Both publications provided a clear objective and clear patient criteria; used appropriate statistical methods; tabulated patient characteristics; used a blinded data extractor; and provided a comprehensive discussion on the limitations of the study. Only Cole et al. reported no potential COI and accounted for concomitant administration of diphenhydramine,3 while only Klein et al. reported quantified adverse event data.4 Due to the retrospective data, neither publication was able to account for IM versus IV administration; however, Cole et al. reported that IV administration represented less than 6% of patients.
The third retrospective observational study provided a clear objective, a statement of no potential COIs, appropriate statistical methodology, and a comprehensive discussion on study limitations. The study reported adverse events quantitatively and used a data extractor that was blinded to the study protocol. The study was limited by retrospective design and did not distinguish between IM and IV administration. The study was subject to a significant potential for selection bias in that limited patient characteristics were reported on a cohort with unclear selection criteria, limited data on concomitant medications was reported, significant loss to follow-up was observed, and incomplete data on outcomes of QTc were reported.
Guidelines
Guidelines from the AAEM provided a clear objective; however, the guidelines did not specifically describe a research question or the patient population of interest. A systematic literature search was used to identify relevant evidence. Significant limitations in the reported methodology included a lack of stakeholder involvement, lack of information on other treatment options, lack of advice and implications for implementation, and unclear potential COI. Importantly, although the quality of the supporting evidence was assessed, the criteria used lacked sufficient detail and were not used to describe the body of identified evidence. Additionally, the recommendations were assigned a class that was not defined or associated with the assessed quality or the assigned grade of the supporting evidence. However, the supporting evidence was associated with each clear and unambiguous recommendation.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness and Safety of Droperidol
The 2 included SRs summarized the following body of evidence regarding the comparative safety and efficacy of droperidol for patients in acute care settings.6,13 Muir-Cochrane et al. summarized 8 RCTs relevant to droperidol.6 Two RCTs, both appraised as high-quality studies, enrolled an overlapping cohort of 361 patients and observed that IV administration of midazolam with droperidol was associated with a significantly greater number of successful sedations than IV droperidol or IV olanzapine alone. In contrast, another high-quality RCT with 91 participants found that IM droperidol was quicker and safer than IM midazolam, and the combination of droperidol and midazolam administered intramuscularly offered no advantages. Another high-quality study including 144 randomized patients with acute agitation in the ED found that IM midazolam and IM droperidol were quicker and more effective than IM ziprasidone; however, patients treated with IM midazolam required more frequent rescue sedation and experienced more frequent respiratory distress. Another RCT randomized 336 patients to receive IV midazolam concomitantly with placebo, IV droperidol, or IV olanzapine. This RCT was also appraised as a high-quality study; it found that the addition of either droperidol or olanzapine decreased the time to adequate sedation. In an MA, Muir-Cochrane et al. included 2 of the RCTs above with sufficient homogeneity, and this combined dataset did not identify a statistically significant difference between droperidol and olanzapine in terms of the proportion of adequately sedated patients at 5 minutes or 10 minutes post-administration. This analysis also identified a statistically significant increase in adverse events with an increased dose of olanzapine from 5 mg to 10 mg but not with an increased dose of droperidol from 5 mg to 10 mg. The highest reported frequency of overall adverse events was reported as 16.2% with 10 mg droperidol. Although narrative conclusions from Muir-Cochrane et al. favoured the safety and efficacy of 5 mg olanzapine in quickly producing calm in distressing situations, no significant differences to 5 mg droperidol administration in safety or efficacy were identified in this SR. Limited conclusions specific to droperidol were reported.6
Additional findings summarized by Bak et al. (2019) included safety results of an RCT that compared droperidol and olanzapine and did not identify a statistically significant difference in the frequency of cardiovascular arrhythmia adverse events.13 Bak et al. also included an MA from an SR that compared droperidol to haloperidol in 1 RCT of 228 patients in which no statistically significant difference in efficacy was identified.13 The SR from Bak et al. presented evidence that supported the authors conclusions that olanzapine, haloperidol plus promethazine, and droperidol were the most effective and safe for rapid tranquilization in the ED. With regard to QTc, the evidence supported the author’s conclusion that the prevalence of unsafe QTc following droperidol treatment is rare and comparable to other antipsychotic drugs. For some of the included RCTs in Bak et al., it was unclear whether adverse events were not reported or there were no adverse events.13 The frequencies of adverse events following droperidol administration were variable between identified studies in the 2 included SRs and included events of hypotension,6 respiratory depression,6 acute dystonia,6,13 airway obstruction,6 hypotension,6,13 arrhythmia,6 bradycardia,6 hypoventilation,6 EPS,13 akathisia,13 oversedation,6,13 and QT elongation.13
The RCT published in 2020 by Martel et al. compared 5 mg IM droperidol, 2 mg IM lorazepam, 10 mg IM ziprasidone, and 20 mg IM ziprasidone in a total of 115 randomized patients.2 For the primary outcome of proportion of adequately sedated patients (AMSS ≤ 0) at 15 minutes, droperidol was statistically superior to the other treatments. For the other efficacy outcomes of requirement for additional sedative medications and ED LOS, no statistically significant differences between groups were identified. With regard to safety outcomes, statistically significant differences in ETCO2 change and a composite outcome of ETCO2 change and hypoxemia (SpO2 < 90%) favoured droperidol. Despite favouring droperidol, this respiratory depression composite outcome was the most frequently observed adverse event observed in this report, reported in 12% of patients. No significant differences in QTc or other respiratory outcomes were identified.2 The conclusions from the authors of the study support droperidol as being more effective than lorazepam or ziprasidone for the treatment of acute agitation in the ED while causing fewer respiratory depression episodes, and with a similar QTc.2 Limited patient characteristics were reported in Martel et al. (2020); therefore, these results are of unclear generalizability and potential risk factors for adverse events were not assessed.2
Two retrospective observational studies published in 2019 compared droperidol, olanzapine, and haloperidol administered to patients in the ED intoxication unit.3,4 Cole et al. found that patients administered droperidol monotherapy for acute agitation secondary to alcohol intoxication had significantly shorter ED LOS than either comparator group.3 Adverse event data were not reported in this study other than the authors observed no cases of sudden cardiac death.3 Klein et al. observed a lower proportion of patients requiring rescue sedation who were treated with either droperidol or olanzapine compared with haloperidol in a similar patient population in the same setting.4 No significant differences in adverse event frequency were observed in this cohort of more than 15,000 patients. The authors concluded that major adverse events were rare, but they did not examine potential risk factors.4
The oldest included study, a retrospective observational study from 2014, reported on the use of droperidol compared to haloperidol for prehospital physical restraint of 532 patients with threatening behaviour.14 In this study, no statistically significant differences were observed in the proportion of patients requiring rescue sedation, QTc length, or adverse events. One patient treated with droperidol suffered cardiopulmonary arrest; however, the authors did not attribute this to torsades de pointes or droperidol administration.14
Guidelines
One set of guidelines from 2015 provided recommendations regarding droperidol administration by emergency physicians.7 Three recommendations were formulated based upon both outstanding and good quality studies comprising Grade A and Grade B evidence. The recommendations were also assigned a class to reflect the strength of each recommendation; however, these classes were not defined in the publication. The AAEM assigned a Class B strength to the first recommendation that droperidol is an efficacious treatment of agitation, headache, and nausea. The guideline committee’s second recommendation was that there is insufficient evidence to recommend mandating an ECG or telemetry monitoring for doses less than 2.5 mg given either intramuscularly or intravenously (Class A strength). A dose of less than 2.5 mg is considered off-label in the US, and the FDA black box warning does not apply to off-label dose levels.7 The third recommendation was that IM doses of up to 10 mg of droperidol appear to be as safe and effective as other medications used for sedation of agitated patients (Class B). The authors also stated that it is well established that antipsychotic drugs increase QTc in a dose-related manner, but they did not make statements about ECG or telemetry monitoring of patients administered more than 2.5 mg droperidol. Furthermore, the authors encouraged a clarification of the US FDA black box warning to address the dose of droperidol with regard to the FDA recommendation.7
Limitations
The evidence identified and included in this report contain an unclear quantity of overlap (i.e., some of the same patients were included in more than 1 publication); therefore, some evidence may be disproportionally represented. The majority of the evidence identified in this report was from RCTs included in 2 SRs.6,13 The critical appraisals conducted in the SRs were not reported in sufficient detail to assess potential bias concerns in this body of evidence. None of the identified studies reported detailed patient characteristics or analyzed the data for possible risk factors for the reported serious adverse events. Therefore, this evidence had unclear generalizability to all adult patients in acute care settings. The ethical issue of informed consent for agitated patients in acute care in the evidence included in this report may have not been appropriately addressed. Furthermore, the recommendations identified in this report are limited by a lack of context as the authors did not define the classes assigned to grade the strength of recommendations.7
Conclusions and Implications for Decision- or Policy-Making
This report identifies and summarizes evidence on the use of droperidol for agitated, aggressive, and violent adult patients in acute care settings. This body of evidence consists of 2 SRs,6,13 1 RCT,2 and 3 retrospective observational studies.3,4,14 There is considerable overlap between the RCTs included in the SRs (outlined in Appendix 5). One set of guidelines was identified that included recommendations for emergency physicians regarding management of patients with droperidol.7
There was consistent evidence that no other tested antipsychotic drug (haloperidol, olanzapine, lorazepam, or ziprasidone) demonstrated superior sedative efficacy to droperidol.2-4,6,13,14 Evidence for sedative efficacy of antipsychotic drugs for patients in acute care settings was from 2 RCTs, both with fewer than 50 patients in each study arm. Findings from these RCTs supported the superiority of droperidol over ziprasidone2,6,11 and lorazepam.2 Efficacy evidence of droperidol compared with olanzapine and haloperidol was mixed in 4 RCTs, either favouring droperidol or finding no significant difference.6,13
Potentially serious adverse events were identified in this evidence, including respiratory depression and QTc prolongation. One RCT reported statistically significant differences in adverse events favouring droperidol over lorazepam and ziprasidone in the frequency of respiratory depression events.2 The remaining comparative evidence of adverse event profiles of antipsychotic drugs did not identify any additional statistically significant differences, including evidence from 3 retrospective observational studies, 2 of which had partially overlapping cohorts of more than 10,000 patients.3,4 None of the identified studies examined potential correlations between the incidence of adverse events and patient risk factors, making the generalizability of the droperidol safety profile for all adult patients in acute care settings unclear. No identified studies had a primary outcome of safety; therefore, some studies may have been insufficiently powered to detect any differences between treatment arms.
Three evidence-based recommendations from the AAEM were formulated, one of which was relevant to patient monitoring.7 This recommendation was based upon high-quality evidence and it stated that there is currently insufficient evidence to recommend mandating an ECG or telemetry monitoring of patients administered dose levels of droperidol less than 2.5 mg, either intravenously or intramuscularly. The authors also recommended that droperidol is as efficacious as other medications used for the treatment of agitation and that IM doses up to 10 mg are comparably safe.7 No evidence was identified regarding implementation and/or potential challenges for the use of droperidol for sedating adult patients in acute care in the Canadian health care setting.
A black box warning regarding droperidol was issued by the FDA in 2001 based upon post-marketing surveillance.3,7 This warning stated that ECG monitoring should be used before administration of droperidol and that droperidol should not be administered if the QTc was longer than 440 ms in males or 450 ms in females.7 None of the identified evidence provided patient baseline QTc or examined QTc as a potential risk factor before droperidol administration. Some study authors questioned the relevance of the evidence on which the black box warning was presumably based;3,7 a future similarly powered study with a focus on examining serious adverse events and risk factors may provide the appropriate clarification.
References
1.Chan EW, Taylor DM, Knott JC, Phillips GA, Castle DJ, Kong DC. Intravenous droperidol or olanzapine as an adjunct to midazolam for the acutely agitated patient: a multicenter, randomized, double-blind, placebo-controlled clinical trial. Ann Emerg Med. 2013;61(1):72-81. Medline
2.Martel ML, Driver BE, Miner JR, Biros MH, Cole JB. Randomized double-blind trial of intramuscular droperidol, ziprasidone, and lorazepam for acute undifferentiated agitation in the emergency department. Acad Emerg Med. 2020;05:05.
3.Cole JB, Klein LR, Martel ML. Parenteral antipsychotic choice and its association with emergency department length of stay for acute agitation secondary to alcohol intoxication. Acad Emerg Med. 2019;26(1):79-84. Medline
4.Klein LR, Driver BE, Horton G, Scharber S, Martel ML, Cole JB. Rescue sedation when treating acute agitation in the emergency department with intramuscular antipsychotics. J Emerg Med. 2019;56(5):484-490. Medline
5.Calver L, Drinkwater V, Gupta R, Page CB, Isbister GK. Droperidol v. haloperidol for sedation of aggressive behaviour in acute mental health: randomised controlled trial. Br J Psychiatry. 2015;206(3):223-228. Medline
6.Muir-Cochrane E, Grimmer K, Gerace A, Bastiampillai T, Oster C. Safety and effectiveness of olanzapine and droperidol for chemical restraint for non-consenting adults: a systematic review and meta-analysis. Australas Emerg Care. 2020 Oct 10;S2588-994X(20)30081-6.
7.Perkins J, Ho JD, Vilke GM, DeMers G. American Academy of Emergency Medicine position statement: safety of droperidol use in the emergency department. J Emerg Med. 2015;49(1):91-97. Medline
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. Medline
10.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Jan 14.
11.Martel M, Sterzinger A, Miner J, Clinton J, Biros M. Management of acute undifferentiated agitation in the emergency department: a randomized double-blind trial of droperidol, ziprasidone, and midazolam. Acad Emerg Med. 2005;12(12):1167-1172. Medline
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
13.Bak M, Weltens I, Bervoets C, et al. The pharmacological management of agitated and aggressive behaviour: a systematic review and meta-analysis. Eur Psychiatry. 2019 Apr;57:78-100. Medline
14.Macht M, Mull AC, McVaney KE, et al. Comparison of droperidol and haloperidol for use by paramedics: assessment of safety and effectiveness. Prehosp Emerg Care. 2014;18(3):375-380. Medline
15.Calver L, Drinkwater V, Isbister GK. A prospective study of high dose sedation for rapid tranquilisation of acute behavioural disturbance in an acute mental health unit. BMC Psychiatry. 2013;13(no pagination). Medline
16.Calver L, Isbister GK. High dose droperidol and QT prolongation: analysis of continuous 12-lead recordings. Br J Clin Pharmacol. 2014;77(5):880-886. Medline
17.Cocchi A, Fonda P, Perosino N. [Droperidol: a double-blind clinical study]. Riv Sper Freniatr Med Leg Alien Ment. 1971;95(6):1109-1125. Medline
18.Hick JL, Mahoney BD, Lappe M. Prehospital sedation with intramuscular droperidol: a one-year pilot. Prehosp Emerg Care. 2001 Oct-Dec;5(4):391-394. Medline
19.Isbister GK, Calver LA, Page CB, Stokes B, Bryant JL, Downes MA. Randomized controlled trial of intramuscular droperidol versus midazolam for violence and acute behavioral disturbance: the DORM study. Ann Emerg Med. 2010;56(4):392-401.e391. Medline
20.Isbister GK. Droperidol or olanzapine, intramuscularly or intravenously, monotherapy or combination therapy for sedating acute behavioral disturbance. Ann Emerg Med. 2017;69(3):337-339. Medline
21.Khokhar MA, Rathbone J. Droperidol for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. 2016;12:CD002830. Medline
22.Knott JC, Taylor DM, Castle DJ. Randomized clinical trial comparing intravenous midazolam and droperidol for sedation of the acutely agitated patient in the emergency department. Ann Emerg Med. 2006 Jan;47(1):61-67. Medline
23.Resnick M, Burton BT. Droperidol vs. haloperidol in the initial management of acutely agitated patients. J Clin Psychiatry. 1984 Jul;45(7):298-299. Medline
24.Richards JR, Derlet RW, Duncan DR. Chemical restraint for the agitated patient in the emergency department: lorazepam versus droperidol. J Emerg Med. 1998 Jul-Aug;16(4):567-573. Medline
25.Rosen CL, Ratliff AF, Wolfe RE, Branney SW, Roe EJ, Pons PT. The efficacy of intravenous droperidol in the prehospital setting. J Emerg Med. 1997;15(1):13-17. Medline
26.Taylor DM, Yap CYL, Knott JC, et al. Midazolam-droperidol, droperidol, or olanzapine for acute agitation: a randomized clinical trial. Ann Emerg Med. 2017;69(3):318-326.e311. Medline
27.van Leeuwen AM, Molders J, Sterkmans P, et al. Droperidol in acutely agitated patients. A double-blind placebo-controlled study. J Nerv Ment Dis. 1977;164(4):280-283. Medline
28.Yap CYL, Taylor DM, Knott JC, et al. Intravenous midazolam-droperidol combination, droperidol or olanzapine monotherapy for methamphetamine-related acute agitation: subgroup analysis of a randomized controlled trial. Addiction. 2017 Jul;112(7):1262-1269. Medline
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Muir-Cochrane et al. (2020)6 Australia Funding: No specific funding | 23 RCTs with droperidol included in 8 RCTs | Adults with uncontrolled aggression, anxiety, violence, or with mental health conditions and non-consenting to treatment | Intervention: Chemical restraint (including droperidol) Comparator: Any reported | Outcomes: Any measure of aggression, agitation, or violent behaviours Follow-up: Any follow-up duration |
Bak et al. (2019)13 Netherlands Funding: No specific funding | 53 RCTs and 1 SR with droperidol included in 8 of the RCTs and 1 SR | Adults with psychiatric disorder or intoxication, in the ED, ward in mental health hospital, or mixed Excluded patients with delirium | Intervention: Rapid tranquilization or pharmacological intervention (including droperidol) | Outcomes:
Follow-up: At least 2 hours |
ACES = Agitation-Calmness Evaluation Scale; ED = emergency department; OASS = Overt Agitation Severity Scale; PANSS-EC = Positive and Negative Symptom Scale-Excitement Components; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes |
Randomized controlled trial | ||||
Martel et al. (2020)2 US Funding: Not reported | Adequately powered, randomized, double-blind, 4-arm trial (N = 115 patients) | Adults (≥ 18 years) requiring parenteral sedation for acute agitation Exclusions
| Interventions:
| Outcomes:
|
Non-randomized studies | ||||
Cole et al. (2019)3 US Funding: Not reported | Retrospective observational cohort study, 3 arms (N = 11,787) | Adults (≥ 18 years) presenting to the ED intoxication unit with chief complaint of alcohol intoxication or altered mental status, and ethanol > 80 mg/dL in blood. Exclusions: multiple antipsychotic drugs administered | Interventions:
Diphenhydramine was frequently administered concomitantly (droperidol 62%, olanzapine 13%, and haloperidol 87%) | Outcome: ED LOS |
Klein et al. (2019)4 US Funding: Not reported | Retrospective observational cohort study, 3 arms (N = 15,918) | Adults (≥ 18 years) presenting to the ED intoxication unit with chief complaint of altered mental status | Interventions: Initial antipsychotic drug
Diphenhydramine was frequently administered concomitantly but the frequency was not reported | Outcomes:
|
Macht et al. (2014)14 US Funding: AHRQ and NIH grants | Retrospective observational cohorts chronologically separated by ED protocol change from droperidol to haloperidol (N = 532) | Patients “behaving in a manner that poses a threat to their own well-being or others” or combative, head-injured patients requiring prehospital physical restraint Exclusions: Patients receiving droperidol as an antiemetic | Interventions:
| Outcomes:
|
AHRQ = Agency for Healthcare Research and Quality; AMSS = Altered Mental Status Scale; BARS = Behavioural Activity Rating Scale; ED = emergency department; ETCO2 = end-tidal carbon dioxide; LOS = length of stay; NIH = National Institutes of Health; SBP = systolic blood pressure; QTc = QT interval; SpO2 = peripheral oxygen saturation.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendation development and evaluation | Guideline validation |
AAEM (2015)7 | ||||||
Intended users: Emergency physicians Target population: ED patients receiving droperidol for any indication | Appropriate and safe use of droperidol for any management of patients in the ED | Efficacy, role of ECG monitoring, maximal dosing | Electronic search of droperidol and Inapsine (1995 to 2014), selection (all study designs) done in duplicate; synthesis was done by independent and joint review and discussion | Quality ranking assigned as outstanding, good, adequate, poor, or unsatisfactory based upon 2 criteria (design consideration and methodology consideration) | Evidence categorized as supportive, neutral, or opposed Quality and grade of evidence used to determine the level of recommendation | No methodology provided for internal or external review by experts or stakeholders |
AAEM = American Academy of Emergency Medicine; ED = emergency department.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 28
Strengths | Limitations |
Muir-Cochrane et al. (2020)6 | |
|
|
Bak et al. (2019)13 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; COI = conflict of interest; CONSORT = Consolidated Standards of Reporting Trials; MA = meta-analysis; PICO = population, intervention, comparator, outcome; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT = randomized controlled trial; SR = systematic review.
Table 6: Strengths and Limitations of RCT Clinical Study Using the Downs and Black Checklist9
Strengths | Limitations |
Martel et al. (2020)2 | |
|
|
Table 7: Strengths and Limitations of Non-Randomized Clinical Studies Using the Downs and Black Checklist9
Strengths | Limitations |
Cole et al. (2019)3 | |
|
|
Klein et al. (2019)4 | |
|
|
Macht et al. (2014)14 | |
|
|
Table 8: Strengths and Limitations of Guideline Using AGREE II10
Item | Assessment |
AAEM (2015)7 | |
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Unclear |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | No |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | No |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | No |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Systematic Reviews
Muir-Cochrane et al. (2020)6
Main Study Findings
RCTs comparing droperidol to another antipsychotic drug
Yap et al. (2017) (N = 92)
Quality: 13 out of 13
Midazolam-droperidol versus olanzapine or droperidol for methamphetamine-related acute agitation in the psychiatric intensive care unit (PICU)
IV midazolam-droperidol sedated significantly more patients than IV droperidol or IV olanzapine
Taylor et al. (2017) (n = 361)
Quality: 13 out of 13
Midazolam-droperidol versus olanzapine or droperidol for acute agitation in PICU
IV midazolam-droperidol sedated significantly more patients than IV droperidol or IV olanzapine
Calver et al. (2015) (N = 206)
Quality: 13 out of 13
IM droperidol versus IM haloperidol for sedation of PICU patients with aggressive behaviours
Similar sedative efficacy; haloperidol was safer
Chan et al. (2013) (N = 336)
Quality: 13 out of 13
IV droperidol and IV olanzapine were both more effective as an adjunct to IV midazolam compared to IV midazolam alone at reducing time to adequate sedation in the ED
Isbister (2017) (N = 91)
Quality: 13 out of 13
IM droperidol versus IM midazolam or IM midazolam-droperidol in the ED
IM droperidol was quicker and safer for sedation of violent and aggressive patients
The combination offered no additional benefit
Knott et al. (2006) (N = 153)
Quality: 13 out of 13
IV midazolam versus IV droperidol of acutely agitated patients in the ED
Interventions were equally effective at sedation within 10 minutes
Midazolam was faster, but more patients required airway management and further sedation
Martel et al. (2005) (N = 144)
Quality: 13 out of 13
IM midazolam versus IM droperidol or IM ziprasidone of acutely agitated patients in the ED
IM midazolam and IM droperidol were quicker and more effective than ziprasidone
More patients treated with IM midazolam required rescue sedation treatments and experienced respiratory distress
Meta-analysis
Chan et al. (2013) and Taylor et al. (2017) had sufficient homogeneity for dosing, outcome measures, and time frames for meta-analysis (I2 = 0%)
Time to sedation
Median difference: 0.1 (95% CI, −0.115 to 0.254) minutes favouring droperidol over olanzapine (not significant)
No significant difference between olanzapine and droperidol in percentage of adequately sedated patients at 5 minutes or 10 minutes
Adverse events (MA of Chan et al. and Taylor et al.), %
Droperidol 5 mg: 10.7%
Droperidol 10 mg: 16.2%
Difference between doses in frequency of adverse events was not significant (odds ratio [OR] = 0.6; 95% CI, 0.3 to 1.4)
Olanzapine 5 mg: 8.3%
Olanzapine 10 mg: 20%
Lower doses significantly decreased frequency of adverse events (OR = 0.4; 95% CI, 0.2 to 0.8)
Rate of adverse events between droperidol and olanzapine not statistically tested
Authors’ Conclusion
“This study provides clear guidance than 5 mg olanzapine delivered intramuscularly is both safe and effective in quickly producing calm in potentially distressing situations, and that it is as effective, and safer, than higher doses (p. 14).”6
“…5 mgs olanzapine produced the lowest rate of adverse events. Thus, of the three drug choices 5 mg IM olanzapine was the most effective and safest [chemical restraint] option in the short-term (p. 14).”6
The above conclusions were based upon 1 RCT in which the authors of the study had concluded that the numbers of patients experiencing adverse events were similar between groups at a 5 mg dose: droperidol (12 of 112; 10.7%) and olanzapine (9 of 109; 8.3%).
Bak et al. (2019)13
Main Study Findings
SR of Khokhar and Rathbone (2016)
Efficacy
Droperidol versus haloperidol (1 RCT; Cocchi et al. [1971], n = 228): relative risk (RR) = 1.01 (95% CI, 0.93 to 1.09)
Droperidol versus midazolam (1 RCT; Knott et al. [2006], n = 153): RR = 0.96 (95% CI, 0.72 to 1.28)
Droperidol versus olanzapine (1 RCT; Chan et al. [2013], n = 221): RR = 1.02 (95% CI, 0.94 to 1.11)
Cardiovascular arrhythmia
Droperidol versus olanzapine (1 RCT; Chan et al. [2013], n = 221): RR = 0.32 (95% CI, 0.01 to 7.88)
Data from RCTs (not direct comparator studies)
Antipsychotic drugs (IM): Percentage (or range of percentages across different studies) of patients reaching calmness
Within 15 to 20 minutes
Droperidol: 53% to 92%
Haloperidol: 67% to 91%
IV Droperidol + midazolam: 89%
IV Olanzapine: 66%
Within 2 hours
Droperidol: 98%
Droperidol + midazolam: 96%
Haloperidol: 60% to 89%
Haloperidol + promethazine: 89% to 97%
Aripiprazole: 60% to 84%
Olanzapine: 73% to 91%
Ziprasidone: 29% to 90%
Loxapine: 66% to 74%
Placebo: 28% to 44%
Antipsychotic drugs (IM): Mean time (or range of percentages across different studies) to calmness (minutes)
Droperidol: 8 to 25
Droperidol + midazolam: 25
Lorazepam: 48
Haloperidol: 30
Haloperidol + promethazine: 20 to 30
Midazolam: 20 to 24
Haloperidol + lorazepam: 44
Haloperidol + midazolam: 10
Olanzapine: 30
Olanzapine (IV): 11
Risperidone + lorazepam: 43
Adverse events (not direct comparator studies; for some RCTs it was unclear whether adverse events were not reported or there were no adverse events to report)
Oversedation
Droperidol: 1%
Lorazepam: 10%
Haloperidol: 0% to 36%
Haloperidol + promethazine: 3%
Haloperidol + midazolam: 40%
Aripiprazole: 4% to 9%
Olanzapine: 3% to 13%
Risperidone: 13%
Risperidone + lorazepam: 13%
Levomepromazine: 8%
Ziprasidone: 10%
Loxapine: 11% to 13%
Placebo: 2% to 10%
Movement disorders
EPS
Haloperidol: 6% to 55%
Haloperidol + promethazine: 0% to 74%
Haloperidol + lorazepam: 5%
Haloperidol + midazolam: 44%
Aripiprazole: 2%
Olanzapine: 0% to 5%
Risperidone: 6% to 8%
Ziprasidone: 0% to 52%
Placebo: 2% to 7%
Acute dystonia
Droperidol: 0% to 1%
Haloperidol: 0% to 17%
Haloperidol + lorazepam: 3%
Haloperidol + midazolam: 10%
Aripiprazole: 1% to 2%
Olanzapine: 0% to 4%
Haloperidol + promethazine: 0%
Risperidone: 2%
Akathisia
Haloperidol: 4% to 46%
Aripiprazole: 3%
Olanzapine: 3%
Levomepromazine: 8%
Hypotension or hypertension:
Droperidol: 0% to 4%
Droperidol + midazolam: 2% to 42%
Midazolam: 5%
Haloperidol: 0% to 17%
Haloperidol + lorazepam: 3%
Haloperidol + promethazine: 10%
Haloperidol + midazolam: 10%
Olanzapine: 0% to 4%
Levomepromazine (hypotension): 16%
Levomepromazine (hypertension): 3%
Cardiovascular adverse effects: QT elongation > 500 ms:
Droperidol: 1% to 6%
Droperidol + midazolam: 1% to 14%
Haloperidol: 0% to 6%
Aripiprazole: 0% to 6%
Olanzapine: 0% to 3%
Placebo: 0% to 8%
Authors’ Conclusion
“Droperidol has been abandoned for some years because of QT-time prolongation. However, recent studies have shown that the prevalence of exceeding unsafe QT-times is rare and not more than with other antipsychotics… The problem of QT elongation in droperidol appears a rather smaller problem and not more prevalent compared to other antipsychotics (p. 96).”13
“At an ED the context asks for a more rapid onset of calmness and medical safety equipment is at hand allowing midazolam, droperidol or droperidol plus midazolam IV or IM to be used, medications that reaches calmness very fast but also need medical attention (p. 98).”13
“Olanzapine, haloperidol plus promethazine, or droperidol are most effective and safe for use as rapid tranquilisation. Midazolam sedates most quickly. But due to increased saturation problems, midazolam is restricted to use within an emergency department of a general hospital (p. 78).”13
Summary of Findings of Included RCT Primary Clinical Studies
Martel et al. (2020)2
Main Study Findings
Difference in proportion adequately sedated at 15 minutes (95% CI):
Droperidol versus lorazepam: 33% (8% to 58%)
Droperidol versus ziprasidone (10 mg): 39% (14% to 64%)
Droperidol versus ziprasidone (20 mg): 29% (3% to 54%)
Difference in reduction in median AMSS at 15 minutes (95% CI):
Droperidol versus lorazepam: 2 (0 to 3)
Droperidol versus ziprasidone (10 mg): 1 (0 to 2)
Droperidol versus ziprasidone (20 mg): 1 (0 to 2)
BARS outcomes were reported with a Spearman rank correlation coefficient for AMSS of 0.95 (P < 0.001).
Additional sedatives required
Entire encounter:
Droperidol: 20%
Ziprasidone (10 mg): 25%
Ziprasidone (20 mg): 16%
Lorazepam: 39%
Before adequate sedation:
Droperidol: 8%
Ziprasidone (10 mg): 14%
Ziprasidone (20 mg): 13%
Lorazepam: 23%
Time until additional sedatives (minutes), median (IQR):
Droperidol: 90 (32 to 149)
Ziprasidone (10 mg): 46 (30 to 60)
Ziprasidone (20 mg): 38 (34 to 40)
Lorazepam: 60 (49 to 78)
LOS in ED, median (IQR)
Time from administration to discharge (minutes):
Droperidol: 341 (235 to 400)
Ziprasidone (10 mg): 285 (236 to 383)
Ziprasidone (20 mg): 325 (257 to 412)
Lorazepam: 379 (199 to 524)
Total time in ED (minutes):
Droperidol: 563 (477 to 615)
Ziprasidone (10 mg): 540 (438 to 720)
Ziprasidone (20 mg): 551 (455 to 640)
Lorazepam: 611 (439 to 782)
Adverse events
Respiratory outcomes
Hypoxemia (SpO2 < 90%):
Droperidol: 8%
Ziprasidone (10 mg): 7%
Ziprasidone (20 mg): 19%
Lorazepam: 23%
Change in ETCO2 (decreased > 10 mm Hg, or increased > 15 mm Hg):
Droperidol: 8%
Ziprasidone (10 mg): 32%
Ziprasidone (20 mg): 32%
Lorazepam: 45%
P = 0.03
Respiratory depression (hypoxemia or change in ETCO2 composite):
Droperidol: 12%
Ziprasidone (10 mg): 36%
Ziprasidone (20 mg): 39%
Lorazepam: 48%
P = 0.04
QT elongation (QTc), median (IQR):
Droperidol: 413 (389 to 452)
Ziprasidone (10 mg): 410 (385 to 432)
Ziprasidone (20 mg): 428 (391 to 459)
Lorazepam: 414 (380 to 429)
Authors’ Conclusion
“Droperidol was more effective than lorazepam or either dose of ziprasidone for the treatment of acute agitation in the ED and caused fewer episodes of respiratory depression (p. 1).”2
“QTc durations were similar in all groups (p. 1).”2
“Droperidol also tended to have higher AMSS scores (less sedation) once adequate sedation was achieved, suggesting that earlier reevaluation may be more feasible with droperidol than lorazepam or ziprasidone (Figure 2). This has obvious benefits in patients requiring psychiatric evaluation and on total time patients spend in the ED who require medications for agitation management. We found no difference in effectiveness or safety between lorazepam and ziprasidone. Our data align with subsequent in the intervening years demonstrating IM droperidol to be a safe, effective first-line agent for acute agitation in the ED (p. 7).”2
Summary of Findings of Included Non-Randomized Primary Clinical Studies
Cole et al. (2019)3
Main Study Findings
Entire cohort: ED LOS (minutes), mean (95% CI):
Droperidol (n = 3,790): 499 (493 to 506)
Haloperidol (n = 1,449): 524 (515 to 537)
Olanzapine (n = 6,549): 533 (528 to 539)
Cohort not administered concomitant anticholinergic agents: ED LOS (minutes), mean (95% CI):
Droperidol (n = 1,537): 468 (454 to 478)
Haloperidol (n = 204): 506 (488 to 551)
Olanzapine (n = 6,145): 530 (524 to 536)
Authors’ Conclusion
“Droperidol, when given as monotherapy for sedation of acute agitation secondary to alcohol intoxication, was associated with significantly shorter ED length of stay than either parenteral haloperidol or olanzapine. Despite olanzapine’s longer half-life, no difference in ED length of stay was observed between haloperidol or olanzapine (p. 83).”3
“No cases of sudden cardiac death occurred (p. 79).”3
Klein et al. (2019)4
Main Study Findings
Percentage difference requiring rescue sedation (within 1 hour) (95% CI):
Droperidol versus olanzapine: 0% (−1% to 1%)
Droperidol versus haloperidol: −7% (−9% to −5%)
Olanzapine versus haloperidol: −7% (−9% to −5%)
Negative percentage indicates first drug had fewer patients requiring rescue sedation
Percentage difference requiring rescue sedation (entire ED encounter) (95% CI):
Droperidol versus olanzapine: −2% (−3% to 0%)
Droperidol versus haloperidol: −9% (−11% to −7%)
Olanzapine versus haloperidol: −7% (−9% to −5%)
Negative percentage indicates first drug had fewer patients requiring rescue sedation
ED LOS (minutes), median (IQR) (entire cohort):
Droperidol (n = 4,947): 511 (393 to 647)
Haloperidol (n = 2,146): 537 (410 to 672)
Olanzapine (n = 8,825): 544 (418 to 690)
Adverse events, % (95% CI):
Intubation:
Droperidol (n = 4,947): 0.2% (0.1% to 0.3%)
Haloperidol (n = 2,146): 0.2% (0.1% to 0.5%)
Olanzapine (n = 8,825): 0.4% (0.2% to 0.6%)
Torsades de points: 0%
Cardiac arrest:
Droperidol (n = 4,947): 0%
Haloperidol (n = 2,146): 0%
Olanzapine (n = 8,825): 0.01% (0.01% to 0.06%)
Akathisia:
Droperidol (n = 4,947): 0.1% (0.03% to 0.2%)
Haloperidol (n = 2,146): 0%
Olanzapine (n = 8,825): 0.02% (0% to 0.1%)
Dystonia:
Droperidol (n = 4,947): 0.04% (0% to 0.1%)
Haloperidol (n = 2,146): 0.05% (0% to 0.3%)
Olanzapine (n = 8,825): 0.02% (0% to 0.1%)
Anaphylaxis: 0%
Rash:
Droperidol (n = 4,947): 0%
Haloperidol (n = 2,146): 0%
Olanzapine (n = 8,825): 0.02% (0% to 0.1%)
Authors’ Conclusion
“At 1 h, droperidol and olanzapine resulted in the lowest rates of rescue medication administration (11% for each) compared with haloperidol (18%). Adverse events were relatively uncommon. Our findings support that olanzapine and droperidol may be more effective than haloperidol for achieving adequate sedation in agitated patients (p. 488).”4
“Although this study was not necessarily powered to detect adverse events, we reviewed over 15,000 cases of antipsychotic administration and found that serious adverse events were rare (p. 487).”4
“There were no significant differences in major adverse events (p. 484).”4
“Diphenhydramine was given more often [than benzodiazepines] (87% of haloperidol cases, 13% of olanzapine cases, and 62% of droperidol cases)...we may have missed cases of EPS because we used diphenhydramine administration as a surrogate to search for EPS. It is also possible that EPS rates are underestimated due to the frequent co-administration of diphenhydramine, especially with droperidol and haloperidol (p. 488).”4
Macht et al. (2014)14
Main Study Findings
Difference in percentage of patients requiring rescue sedation (within 1 hour) (95% CI):
Droperidol versus haloperidol: −2.9% (−8.5% to 2.6%)
Droperidol had fewer patients requiring rescue sedation
QTc difference (ms), median (95% CI):
Droperidol versus haloperidol: 5 (−10 to 6)
Droperidol had greater median QTc
Droperidol versus haloperidol: difference in percentage of patients with the following QTc intervals (95% CI)
QTc 450 to 474 ms: 6% (−6% to 19%)
QTc 475 to 499 ms: 5% (−4% to 14%)
QTc > 500 ms: 1% (−6% to 4%)
Droperidol had more patients within each elongation interval
Adverse events: no significant differences
Intubation:
Droperidol (n = 218): 2%
Haloperidol (n = 314): 4%
Cardiac arrest:
Droperidol (n = 218): 0.4%
Haloperidol (n = 314): 0%
SpO2 < 90 mm Hg:
Droperidol (n = 218): 3%
Haloperidol (n = 314): 4%
Anti-arrhythmic:
Droperidol (n = 218): 0.5%
Haloperidol (n = 314): 2%
Bag mask ventilation:
Droperidol (n = 218): 2%
Haloperidol (n = 314): 4%
Authors’ Conclusion
“Our study did not demonstrate a statistically significant difference between droperidol and haloperidol in effectiveness, measured by use of further medications within 30 minutes of ED arrival (p. 6).”14
“Our findings suggest that droperidol does not have a worse side-effect profile than haloperidol. We do, however, recognize that a patient in the droperidol group suffered cardiopulmonary arrest. This patient had history of congenital heart disease and a median sternotomy scar from a surgery at age 3, and did not require defibrillation or anti-dysrhythmic drugs for resuscitation, suggesting that torsades de pointes was a less-likely cause of his cardiopulmonary arrest (p. 6).”14
“In this cohort of agitated patients treated with haloperidol or droperidol in the prehospital setting, there was no significant difference in QTc prolongation, adverse events, or need for repeat sedation between haloperidol and droperidol. There was a trend toward fewer adverse events and less need for repeat sedation in the droperidol group. Further study with larger patient groups is needed to better define the safest and most effective method to sedate agitated patients in the prehospital setting (p. 8).”14
Summary of Recommendations of Included Guideline
AAEM (2015)7
Recommendations and Supporting Evidence
“Droperidol is an efficacious treatment of agitation, headache, and nausea (p. 93).” - Class B (outstanding and good quality studies of Grade A and Grade B)
“There is currently insufficient evidence to recommend for mandating an electrocardiogram (ECG) or telemetry monitoring for doses < 2.5 mg given either i.m. or i.v. (p. 96).” - Class A (outstanding and good quality studies of Grade A and Grade B)
“Intramuscular doses of up to 10 mg of droperidol appear to be as safe and as effective as other medications used for sedation of agitated patients (p. 96).” - Class B (outstanding and good quality studies of Grade A and Grade B)
Quality of Evidence and Strength of Recommendations
Grade of evidence
Grade A: Randomized clinical trials or meta-analyses (multiple clinical trials) or randomized clinical trials (smaller trials) directly addressing the review issue
Grade B: Randomized clinical trials or meta-analyses (multiple clinical trials) or randomized clinical trials (smaller trials) indirectly addressing the review issue
Grade C: Prospective, controlled, non-randomized, cohort studies
Grade D: Retrospective, non-randomized, cohort, or case-control studies
Grade E: Case series, animal/model scientific investigations, theoretical analyses, or case reports
Grade F: Rational conjecture, extrapolations, unreferenced opinion in literature, or common practice
Quality of evidence
Outstanding: Design and methodology both with appropriate considerations
Good: Design or methodology with appropriate considerations
Adequate: Design with possible bias and adequate methodological consideration
Poor: Limited design or methodological considerations
Unsatisfactory: Questionable design or methodological considerations
Appendix 5: Overlap Between Included Systematic Reviews
Table 9: Overlap in Relevant Studies Between Systematic Reviews
Study citation | Muir-Cochrane et al. (2020)6 | Bak et al. (2019)13 |
Calver et al. (2013)15 | No | Yes |
Calver and Isbister (2014)16 | No | Yes |
Calver et al. (2015)5 | Yes | Yesa |
Chan et al. (2013)1 | Yes | Noa |
Cocchi et al. (1971)17 | No | Noa |
Hick et al. (2001)18 | No | Yes |
Isbister et al. (2010)19 | No | Yes |
Isbister (2017)20 | Yes | No |
Khokhar and Rathbone (2016)21a | No | Yes |
Knott et al. (2006)22 | Yes | Yesa |
Martel et al. (2005)11 | Yes | No |
Resnick and Burton (1984)23 | No | Noa |
Richards et al. (1998)24 | No | Yes |
Rosen et al. (1997)25 | Yes | No |
Taylor et al. (2017)26 | Yes | Yes |
Van Leeuwen et al. (1977)27 | No | Noa |
Yap et al. (2017)28 | Yes | No |
aKhokhar and Rathbone (2016) is itself a systematic review included in Bak et al. (2019); reference is also included in Khokar and Rathbone.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca