CADTH Health Technology Review
Interventions to Influence the Use of Antibiotics for Acute Upper Respiratory Tract Infections
Rapid Review
Authors: Wade Thompson, Suzanne McCormack
Abbreviations
AOM
acute otitis media
CDSS
clinical decision support system
CI
confidence interval
CRP
C-reactive protein
GP
general practitioner
GRADE
Grading of Recommendations Assessment, Development and Evaluation
IQR
interquartile range
LRTI
lower respiratory tract infection
OR
odds ratio
PICO
patient, intervention, comparison, outcome
POCT
point-of-care test(ing)
RCT
randomized controlled trial
RR
relative risk
RTI
respiratory tract infection
SR
systematic review
Strep A
group A Streptococcus
URTI
upper respiratory tract infection
Key Messages
Thirteen systematic reviews (SRs) were identified. Two of these SRs addressed delayed antibiotic prescribing and 12 of these SRs investigated family medicine interventions. Delayed antibiotic prescribing reduced antibiotic use for upper respiratory tract infections (URTIs) compared to immediate prescribing and did not appear to impact patient satisfaction or re-consultation rates; however, there was less evidence on clinical outcomes, health care utilization, or antibiotic resistance. One systematic review concluded that there was no difference between delayed and immediate antibiotics for many clinical outcomes, but that immediate antibiotics may modestly improve symptoms for acute otitis media (AOM) and sore throat compared with delayed antibiotics.
Various family medicine interventions were evaluated; however, there were generally few relevant primary studies in each of these reviews for most of the interventions. Rapid or point-of-care tests to guide the treatment of URTIs appeared to reduce antibiotic prescribing compared to control or usual care; however, there was relatively little evidence on clinical outcomes for these tests. One systematic review on procalcitonin-guided treatment suggested that this intervention led to no difference in the number of days with restricted activities or rates of treatment failure compared to control, while another systematic review found that C-reactive protein (CRP) point-of-care tests to guide antibiotic prescribing resulted in no difference in recovery or time to resolution of the symptoms; however, this was based on only 2 randomized controlled trials (RCTs). Evidence was mixed on different patient- or provider-directed interventions, such as education, training, and tools. In some of the primary studies from the eligible SRs, these interventions reduced antibiotic prescribing; while in others, they had no effect on antibiotic prescribing.
Context and Policy Issues
Acute upper respiratory tract infections (URTIs) result from viral or bacterial pathogens that infect the upper airways.1 URTIs comprise a range of conditions and symptoms such as cough, sore throat, acute otitis media (AOM), pharyngitis, tonsillitis, rhinitis, common cold, influenza, and sinusitis.1 While serious complications are rare, patients can develop pneumonia and associated adverse sequelae.1 A substantial proportion of health care visits to primary care and other family medicine settings are due to suspected URTIs.2
Most URTIs are viral in origin, meaning they are unlikely to benefit from antibiotics and can often be effectively managed remotely with supportive treatments. Despite this knowledge, antibiotics are often inappropriately prescribed.3,4 A descriptive analysis in Ontario estimated unnecessary antibiotic prescribing in primary care at rates of 48.4% for acute sinusitis and 52.6% for acute bronchitis.5 Further, more than 80% of unnecessary antibiotic prescriptions were attributed to respiratory tract conditions and infections.5 Overprescribing contributes to excessive use, unwanted side effects (e.g., allergic reactions, gastrointestinal symptoms, emergency department visits),6 and antibiotic resistance.7 Antibiotic resistance is a global public health threat and its reduction is a priority.8
Initiatives such as Choosing Wisely aim to reduce antibiotic overuse and advise against using antibiotics for URTIs that are viral in origin.7 However, while the risks of inappropriate and overuse are established, antibiotic prescribing is challenging and providers must balance the pressure of diagnostic uncertainty, time constraints, and patient expectations and preferences against the undesirable consequences of overprescribing.8 Thus, there is interest in management approaches that aid decision-making and reduce excessive prescribing and use.
Various interventions are available that address inappropriate antibiotic prescribing and the pressures of providing in-person care for patients with URTIs. These include delayed (post-dated) antibiotic prescriptions9 and different interventions to guide the use of antibiotics (e.g., clinical decision support tools, rapid point-of-care testing [POCT], viral prescription pads).10 The desired outcome is to reduce the overprescribing of antibiotics and antibiotic resistance, and potentially to improve clinical outcomes (e.g., reduce harms from antibiotics) and reduce health care utilization such as hospital and emergency department visits.
Changes to health care service delivery and organization due to the COVID-19 pandemic mean providers in primary care face difficulty in caring for patients with URTIs.7 Practical guidance and interventions continue to be required to assist clinicians in making care decisions for patients with upper respiratory tract symptoms. Resources such as the Using Antibiotics Wisely campaign's updated The Cold Standard toolkit provide resources for clinicians to support virtual and in-person management.11 However, there continues to be an interest and need for evaluating contemporary evidence to identify which interventions might be most effective for supporting shared decision-making and optimizing the care of people with URTIs.
This report aims to summarize the evidence regarding the clinical effectiveness of delayed antibiotic prescription-filling interventions and other family medicine interventions to influence the use of antibiotics for suspected acute URTIs.
Research Questions
What is the clinical effectiveness of a delayed antibiotic prescription filling intervention to influence the use of antibiotics for suspected acute upper respiratory tract infections?
What is the clinical effectiveness of other family medicine interventions to influence the use of antibiotics for suspected acute upper respiratory tract infections?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were URTIs and antibiotics. Search filters were applied to limit retrieval to health technology assessments, SRs, meta-analyses, or network meta-analyses. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and December 14, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | People of any age with suspected acute URTIs (e.g., cough, sore throat, AOM, uncomplicated pharyngitis, tonsillitis, rhinitis, common cold, influenza, uncomplicated sinusitis) |
Intervention | Q1: Delayed antibiotic prescription filling Q2: Family medicine interventions to influence the use of antibiotics, used alone or in combinations, such as but not limited to: • clinical decision rules, tool, or score charts (e.g., FeverPAIN score) • point-of-care testing (e.g., C-reactive protein, procalcitonin, streptococcal antigen, multi-viral PCR), • alternate “prescriptions” (e.g., “prescriptions” for lifestyle measure, comfort care) |
Comparator | Q1 and Q2: Standard of care (e.g., immediate antibiotic prescription filling; no prescribed antibiotics) |
Outcomes | Q1 and Q2: Clinical benefits (e.g., fever, pain, swelling, quality of life, number of consultations for the same illness) and harms (e.g., over-or underprescribing, hospital admissions, emergency department visits, morbidity [e.g., complications], mortality) |
Study Designs | HTAs and SRs |
AOM = acute otitis media; HTA = health technology assessment; PCR = polymerase chain reaction; Q = question; SR = systematic review; URTI = upper respiratory tract infections.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published prior to 2017. SRs in which all relevant studies were captured in other more recent, or more comprehensive, SRs were excluded. Primary studies in SRs were not considered relevant for the report if they only included patients with lower respiratory tract infection ([LRTI], e.g., pneumonia) or a mixture of patients with LRTI and URTI and did not report outcomes for URTI separately. Further, primary studies in SRs were not considered relevant if they took place in settings other than family medicine/general practice (GP) settings or primary care clinics (e.g., studies were not considered relevant if they took place in the emergency department or a pediatric clinic).
Critical Appraisal of Individual Studies
The included SRs were critically appraised by one reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2).12 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
A total of 382 citations were identified in the literature search. Following the screening of titles and abstracts, 343 citations were excluded and 39 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 30 publications were excluded for various reasons and 13 publications met the inclusion criteria and were included in this report. These were all SRs. One SR was on delayed antibiotic prescribing,13 one SR was on delayed antibiotic prescribing and family medicine interventions,14 and 11 SRs were on family medicine interventions.15-25 Some primary studies were included in more than one SR. The 2 SRs on delayed antibiotic prescribing reported on 4 of the same RCTs.26-29 Two of the SRs on family medicine interventions reported on the same 3 primary studies30-32 but reported outcomes differently from one another and 1 reported an additional outcome. Another 2 SRs reported on 1 of the same primary studies.33 A table of primary study overlap is provided in Appendix 5.
Appendix 1 presents the PRISMA34 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
All 13 eligible studies were SRs and all had broader inclusion criteria than the present report. Specifically, the SRs reported on a mixture of both LRTI and URTI, and/or a variety of clinical settings (e.g., emergency department, pediatric clinics, and primary care). One SR by Mortazhejri et al.14 conducted in 2020 (search date November 2016) examined studies on both delayed antibiotics (7 RCTs) and interventions aimed at patients and the public (6 studies comprising different interventions and settings) for URTIs. Only 4 of the studies on patient and public interventions were relevant for this report; they were all RCTs.
Another SR by Spurling et al.13 on delayed antibiotics for respiratory tract infections (RTIs) was a living SR initially published in 2017 (search date May 2017) and with a most recent search of November 2020. No additional studies had been identified since the 2017 search. This SR contained 11 RCTs in total, which broadly addressed RTIs in a variety of clinical settings. Five RCTs were relevant for this report, which addressed URTIs in a family medicine setting.
Eleven SRs addressed family medicine interventions. The SR by Carvalho et al.21 was published in 2020 (search date February 2020) and contained 22 studies in total, which covered a range of RTIs in different settings. Two studies (one pre-post and one cohort study) were relevant for this report. Cohen et al. published an SR22 in 2020 (search date June 2019), which contained 5 RCTs in different settings. Three of these RCTs were relevant to this report. Another 2020 SR (search date March 2019) by Fraser et al.25 contained 38 primary studies on sore throat in a variety of settings and 3 RCTs were relevant for this report, as they were conducted in a family medicine setting specifically. Van Hecke et al. conducted an SR24 in 2020 (search date January 2020), which contained 35 studies on a range of different POCTs in different outpatient settings. Two of these studies (1 RCT 1 one retrospective chart review) were relevant for this report, as they were on URTI in family medicine.
In 2019, Burstein et al. conducted an SR20 (search date January 2016), which contained 34 studies addressing antibiotic use in a broad range of conditions and settings. One controlled before-after study on URTIs was relevant from this SR. Another 2019 SR (search date April 2018) was conducted by Health Information and Quality Authority19 and contained 13 primary studies on a range of RTIs. Five of those studies (1 before-after study, 1 cross-sectional study, 1 observational study, 2 RCTs) were relevant for this report, as they were specifically on URTI.
In 2018, Deniz et al. conducted an SR16 (search date June 2017) containing a total of 7 studies in either primary care or secondary care settings. Three observational longitudinal studies conducted in primary care were relevant for this report. Kochling et al. also conducted an SR in 201817 (search date August 2016), which contained 17 studies on any RTI, and 3 RCTs from this SR were relevant for this report (specifically investigating URTIs). Lane et al. conducted an SR in 201815 (search date April 2016), which included 3 primary studies (1 RCT, 1 cohort study with a historical control, and 1 retrospective cohort study). McDonagh et al. conducted an SR in 201823 (search date January 2018), which was an update to a 2016 Agency for Healthcare Research and Quality comparative effectiveness report.35 This SR contained 96 studies on any RTI in a mixture of settings. The results were not reported in a way that allowed for determination of the relevance of primary studies.
One SR from 2017 (search date February 2017) was conducted by Schuetz et al.18 This SR contained 32 studies, in total, on different RTIs in a mixture of settings. Two of those RCTs were relevant for this report; the outcome data from this SR on URTI specifically was reported in a separate publication by Odermatt et al.36
As described, all SRs had broader inclusion criteria than the present review. Only the characteristics and results of the subset of relevant studies will be described further in this report.
Country of Origin
The SRs were conducted in Canada,14 Australia,13 Portugal,21 France,22 the UK,15,24,25 the US,20,23 Ireland,19 the Netherlands,16 Germany,17 and Switzerland.17
Patient Population
For the primary studies in the Mortazhejri et al. SR14 on delayed antibiotics, the patient population was those patients in any age group with URTI seeking treatment in a general/family practice setting. Two of the eligible RCTs were conducted in children (n = 315 and n = 81), 1 in adults (n = 149), and 4 were conducted in both children and adults (n = 129, n = 716, n = 556, and n = 398). In the Spurling et al. SR,13 among 5 eligible primary studies, 1 RCT was conducted in children (n = 712) with sore throat, 1 (n = 398) was in adults with uncomplicated RTI, 1 (n = 191) was in adults and children with cough, 1 was among children with AOM (n = 315), and 1 (n = 129) was among adults and children with the common cold.
With respect to family medicine interventions, relevant studies from SRs were those conducted in family medicine, GP, or the primary care clinic setting. The 2 relevant primary studies in the Carvalho et al. SR21 were conducted in the general population (children and adults). One study was on patients with sinusitis (comprising 438 visits) and another on those with sinusitis or pharyngitis (comprising 240 visits).
In the Cohen et al. SR,22 the 3 relevant RCTs were all conducted among patients with acute sore throat or a clinical diagnosis of pharyngitis or tonsilitis. One RCT was conducted in those greater than or equal to 3 years of age (mean age 31, n = 424), 1 in adults (age not reported, n = 533), and 1 in patients aged 14 to 60 years (mean age 32, n = 557). The relevant primary studies in the SR by Fraser et al.25 were the same 3 from Cohen et al.; however, these SRs reported outcomes differently.
The 4 relevant RCTs from the Mortazhejri et al. SR14 included 2 RCTs (n = 558 and n = 499) among children, 1 among patients with no age reported (n = 914), and 1 among adults (n = 2923) — this SR focused on URTI in general, but the authors did not specify the type of RTI in the primary studies.
The SR by Van Hecke et al.24 included 2 relevant reports, which were both conducted among children with acute sore throat (n = 1,307 and n = 176).
The population in the 1 relevant report from the Burstein et al. SR was one with URTI but was not further described (although the authors noted that all studies in their SR targeted adults).20
In the Health Information and Quality Authority SR, 1 study was conducted in patients of all ages with either acute sinusitis, tonsilitis, or otitis media (n = 367 GPs, patient characteristics was not described), 1 was conducted in adults with acute cough or sore throat (n = 120), 1 was conducted among 4,264 adults with RTI in general (authors reported URTI results separately, but the number of patients with URTI was not reported), another was conducted among 258 adults with either LRTI or rhinosinusitis (reported separately, but the number with rhinosinusitis was unclear), and 1 study among 560 patients with acute rhinosinusitis did not report the age of patients.19
All 3 relevant studies in the Deniz et al. SR16 were conducted among children with AOM. For the 3 relevant studies in the Kochling et al. SR, 1 was conducted among patients aged 14 to 60 with acute pharyngitis (n = 557); 1 was among patients older than or 21 years (n = 914) with either runny nose, blocked nose, cough, or sore throat; and 1 was among patients older than 16 years with acute cough (n=1,651).17
In the SR by Lane et al.,15 1 primary study was conducted among 22 medical residents and examined prescribing for URTI and bronchitis (results were reported separately for each) but did not provide patient characteristics; another study looked at 28,301 patient encounters (for 69 physicians) on febrile respiratory illness, but patient characteristics were not provided; and a third study was conducted among patients with influenza-like illness (in 27 GP practices), but patient characteristics were not provided.
The primary studies in the McDonagh et al. SR23 were not reported individually based on the type of RTI and setting — the authors noted that among the 96 studies in their SR, 21 studies were among patients with AOM, 32 studies were on sore throat, 7 studies were on rhinitis, 22 studies were on sinusitis, and 16 studies were on cough and common cold.
In the SR by Schuetz et al., 1 relevant RCT was conducted among people with upper or lower RTIs (n = 458, mean age 40 years), while the other relevant RCT was also conducted among people with upper or lower RTIs (n = 571, mean age 40 years).18 The patients with URTI (n = 644) from both studies were reported in a separate publication — an individual patient meta-analysis by Odermatt et al.36
Interventions and Comparators
The delayed antibiotic interventions in the Mortazhejri et al. SR14 included a mixture of different approaches, including delayed prescriptions, patient-led delayed prescriptions (prescription given to patient at time of initial visit and patients given instructions to fill the prescription after a given time), post-dated prescriptions, delayed collection (a prescription was not provided at the time of visit but kept at office reception or the pharmacy for the patient to fill if symptoms were not improved after 2 to 7 days [depending on study]), and delayed re-contact. The comparator was not described for each study, but for the SR patient, intervention, comparator, and outcome (PICO) question, the comparator was noted to be usual care or no intervention. In the Spurling et al. SR, the intervention was delayed antibiotic use (use or advice to use antibiotics more than 48 hours after initial consultation) and the comparators were immediate antibiotic use and no antibiotic use.13
The family medicine interventions varied. In the Carvalho et al. SR, the intervention was e-health tools.21 The intervention in 1 relevant primary study was a best practice alert, while in the other relevant study the intervention was a multi-component intervention for providers comprised of didactic teaching, guideline use, and a clinical decision support system (CDSS) integrated into the electronic medical record. The comparator in both studies was the pre-intervention period.
In the Cohen et al. SR, the intervention of interest was rapid tests alone or in combination with scoring systems and the comparator was management based on clinical grounds with or without scoring systems.22 In the Fraser et al. SR, the intervention was rapid POCTs for group A Streptococcus (Strep A) with or without clinical scoring systems compared to antibiotic prescribing based on clinical judgment and/or clinical scoring tools alone.25
In the Mortazhejri et al. SR,14 the intervention of interest was patient-centred interventions, which varied depending on the study. Interventions in the relevant primary studies included patient education sessions, pamphlets, websites, and pamphlets plus videos. The comparator was no intervention or usual care.
The SR by Van Hecke et al. investigated diagnostic POCTs for various diseases.24 In the relevant studies, the intervention was POCTs for sore throat (one study was OSOM Strep A Test, the other was latex agglutination antigen detection method). The comparator in 1 study was usual care, while the comparator in the other study was the pre-intervention period.
In the 1 relevant study in the Burstein et al. SR, the intervention was a mixture of brochures and a media campaign aimed at patients, plus small group education sessions and algorithms for providers implemented in 1 community.20 The comparator was communities not receiving the intervention.
The intervention of interest in the Health Information and Quality Authority SR was CRP POCTs either with or without communication, training, and education, while the comparator was standard care alone.19 In the Deniz et al. SR, the intervention of interest was guidelines on AOM, while the comparator was a pre-guideline introduction.16
The Kochling et al. SR studied various primary care interventions to reduce antibiotic prescriptions.17 The interventions of interest in the relevant studies were a rapid antigen Strep A test in one study, a multi-component intervention in another study (communication training for physicians, handouts for patients, waiting room poster), and patient education on causes of URTI in another study. The comparator was usual care in 2 studies, while the comparator was education on influenza vaccination in the other study.
The intervention of interest in the Lane et al. SR was the use of real-time epidemiological data to improve prescribing by reducing diagnostic uncertainty.15 The comparator was a pre-intervention period in one study, a historical control in another study, and was described as “control” in one RCT.
The SR by McDonagh et al. investigated various interventions to reduce inappropriate antibiotic use compared to standard care (no strategy of improving antibiotic use); however, no relevant reports could be identified from this SR because of the way the results were reported.23
Finally, the intervention in the Schuetz et al. SR was the use of procalcitonin measurements to guide antibiotic decisions and the comparator was standard care.18
Outcomes
In the Mortazhejri et al. SR,14 the outcomes of interest were prescription or use of antibiotics, patient satisfaction with the consultation, and reconsultation for the same illness. In the Spurling et al. SR, the outcomes of interest were clinical outcomes (e.g., malaise, fever, pain), antibiotic use, patient satisfaction, adverse effects of antibiotics, complications of the disease, and reconsultation.13
For family medicine interventions, antibiotic use was reported as an outcome in the SRs by Carvalho et al.,21 Cohen et al.,22 Fraser et al.,25 Mortazhejri et al.,14 Van Hecke et al.,24 Burstein et al.,20 Health Information and Quality Authority,19 Deniz et al.,16 Kochling et al.,17 Lane et al.,15 and Schuetz et al.18 (outcome data from Odermatt et al.36). Guideline adherence was an outcome in the Carvalho et al. SR,21 while inappropriate antibiotic prescription rate was an outcome in the Fraser et al. SR.25 Cohen et al. reported the outcome of recovery, defined as substantial improvement or complete recovery at day 7.22 Health Information and Quality Authority examined time to resolution of symptoms as an outcome.19 The rate of reconsultation was reported by Cohen et al.,22 Mortazhejri et al.,14 Van Hecke et al.,24 and Health Information and Quality Authority 19 Patient satisfaction was reported by Mortazhejri et al.14 and Health Information and Quality Authority 19 Cohen et al. reported on the rate of complications attributed to the index infection.22 As aforenoted, the Schuetz et al.18 SR reported on outcomes for patients with both LRTI and URTI — Odermatt et al. was a separate publication based on this SR, which reported on patients with URTI, only, and reported the number of days with restricted activity and the treatment failure rate at 28 days.36
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
Delayed Antibiotics
Overall, the reviews contributing data on delayed antibiotics had few sources of potential bias. The main weaknesses that were identified related to under-reporting the rationale for study inclusion criteria, lack of context provided for the impact of risk of bias and heterogeneity on the review results, and non-critical weaknesses with the search strategies. Details are available in Table 4 and the following summary.
The 2 eligible systematic reviews13,14 reported their research questions and inclusion criteria in detail following the PICO format. They included a reference to a protocol published a priori. Both reviews explicitly listed eligible study designs and exclusions but did not provide a rationale for the criteria utilized.
Both reviews employed comprehensive literature searches with some limitations. One review14 did not conduct the search within 24 months of publication of the review (the search was conducted in November 2016 and the review was published in 2020), meaning that studies published since 2016 were not captured in this review., Further, the authors did not search reference lists or include a grey literature search.14 The other SR is a living SR and had an up-to-date search but did not outline a formal grey literature search.13
Both reviews performed study selection and data extraction in duplicate and provided a formal list of excluded studies (with reasons for exclusion) and described the included studies in detail.
Both reviews used appropriate tools for assessing the risk of bias — the Effective Practice and Organisation of Care (EPOC) risk-of bias assessment guide adapted by study design14 and the Cochrane risk-of-bias tool,13 respectively. One review did not assess the potential impact of risk of bias on the pooled results14; the other review planned sensitivity analysis based on risk-of-bias assessments.13 Both reviews accounted for the impact of the risk of bias in interpreting and discussing the results of the review and documented primary study funding sources.
Criteria and statistical approaches for pooling were appropriate in both reviews, but 1review lacked details about the specific analytical approach.13 Both reviews formally assessed and investigated sources of heterogeneity; however, the scope of planned and executed analyses investigating factors contributing to heterogeneity was narrow in both cases. Both reviews planned to assess publication bias using funnel plots, but this was not possible because of the number of included studies. One review further considered publication bias13 within the Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessments, and unpublished data were sought and used. Both reviews detailed funding sources and declared no conflicts of interest.
Family Medicine Interventions
The reviews contributing data on family medicine interventions had varying degrees of bias. Several critical and non-critical weaknesses were identified with select reviews, including under-reporting of details of and rationale for study inclusion criteria or study characteristics, incomplete efforts to identify studies through alternative search approaches, lack of duplicate selection or extraction, lack of disclosure of excluded studies, inadequate assessment of the risk of bias, inappropriate methods for quantitative synthesis, lack of consideration of the risk of bias and publication bias in quantitative synthesis, and lack of consideration of the risk of bias and heterogeneity in the interpretation of review findings. Details are available in Table 5 and the following summary.
The 12 reviews reporting on family medicine interventions mostly included sufficient detail about scope and inclusion criteria, including all of the PICO components. Some reviews were either missing sufficient detail about main inclusion criteria (mainly comparators where relevant)17,20,21 or were lacking detail (e.g., time frame for follow-up) or clarity in their presentation.15
Registered protocols were available for most of the included reviews, although not all described deviations from the protocol (if applicable).14-16,18,21-25 Some reviews either stated that the review was not pre-registered or did not reference a protocol or a priori methods, making it challenging to assess whether analyses were pre-planned.17,19,20
Most reviews listed the eligible study designs, including specific trial or study design features, for inclusion; however, only one review explicitly included a rationale for included and excluded study designs.24
Most reviews included a comprehensive literature search strategy; however, almost all were missing at least one desired component, such as searching trial registries, scanning reference lists, consulting topic experts, or including a formal grey literature search strategy. The search in 1 review was not conducted within the desired time frame of 24 months.14
Except for 2 reviews, all others conducted study selection in duplicate. The 2 reviews noted conducted initial screening using one reviewer, with selections checked by a second, potentially increasing the likelihood of missing relevant studies.15,23 Apart from 4 reviews, most conducted data extraction in duplicate. Two23,25 used a single review for data extraction, with results checked by another, potentially increasing the likelihood of recording errors. Methods of data extraction, including the number of reviewers involved, were unclear for 2 reviews.20,24 Most reviews did not include a comprehensive list of excluded studies with reasons for exclusion, making it challenging to assess the accuracy and completeness of study selection. In most cases, review authors noted the number of excluded studies and aggregate reasons for exclusion in text or the PRISMA diagram of the review.
Most reviews described the characteristics of the included studies in adequate detail. However, specific information about interventions and comparators, and time frame of follow-up for various outcomes, were often missing. Several studies had more serious omissions. One did not adequately describe the study design, comparators, details of the interventions, and follow-up time frame.20 The Odermatt et al. publication36 reported outcomes from the Schuetz et al.18 SR — the characteristics of the relevant studies were well-described in the original Schuetz et al. publication; however, the studies were not described in detail in the Odermatt et al. publication (although the characteristics of the patients were described).
A satisfactory tool or approach for assessing the risk of bias was employed in most cases. One review used a scale that did not assess all relevant domains, notably failing to consider allocation concealment and selective outcome reporting.21 One review used a set of predefined criteria in place of a formal tool, which addressed most potential sources of bias except for bias resulting from multiple measurements and bias due to methods used to ascertain exposures and outcomes.23 Another SR extended the Cochrane risk-of-bias tool for RCTs to non-randomized studies.24 One review did not formally assess the risk of bias.20 Five reviews disclosed primary study funding sources,14,18,19,22,25 while the others failed to report this information. The Odermatt et al. publication (reporting outcomes from the Schuetz et al. SR) did not include detail on study quality, although this was formally assessed in the original Schuetz et al. SR.18
Of the 6 reviews that conducted meta-analysis, most used appropriate methods for combining results statistically, including a formal assessment of the appropriateness of pooling based on study similarity and a description of the type of meta-analytic model.14,18,19,22,25 One review pooled randomized and non-randomized studies without providing a rationale.24 Of these reviews, one formally planned to assess the potential impact of risk of bias on the pooled analyses through sensitivity analysis22 and 1 planned sensitivity analysis based on the main quality indicators.18 The other reviews did not formally assess the potential impact of risk of bias on the pooled results. In one SR13 examining clinical outcomes for delayed prescribing versus immediate prescribing, the sample size and event rates for clinical symptoms were relatively low, making it difficult to draw firm conclusions on these outcomes. The difference in pain between the 2 groups in some of the primary studies may have been clinically relevant but were not statistically significant. Most reviews did not formally assess publication bias. Two reviews either formally assessed publication bias or provided a rationale for why it was not feasible, sought unpublished data, and considered publication bias in their GRADE assessments of the certainty of the evidence.18,19 Some reviews pursued unpublished studies or data, or considered publication bias informally as part of the GRADE assessments.14,22,25
In interpreting and discussing the results of the review, 6 reviews accounted for risk of bias by directly discussing the potential impact of methodological considerations on the results, incorporating risk of bias considerations in assessments of the certainty of the findings (e.g., GRADE) or in establishing a hierarchy of the importance of findings.14,17-19,22,25 The remaining reviews either summarized the risk of bias results without putting them in context with the results or failed to discuss the risk of bias in interpreting the results.15,16,20,21,24 A satisfactory explanation for and discussion of the heterogeneity observed in the results was presented by some reviews, including a description of the relevant sources of heterogeneity and their potential implications or factoring heterogeneity into assessments of the certainty of the findings (e.g., GRADE).14,17-19,22,25 Other reviews failed to discuss heterogeneity, mentioned it briefly without discussing implications, or limited the discussion of heterogeneity to select possible sources when other factors may have impacted the findings.15,16,20,21,24 All included reviews disclosed any conflicts of interest, or lack thereof, and relevant funding sources.
Summary of Findings
Delayed Antibiotic Prescriptions
Antibiotic Use
In a meta-analysis of 6 RCTs involving 1,788 patients, Mortazhejri et al. reported that patients in the delayed antibiotic group were less likely to use antibiotics compared to those in the immediate prescription group (odds ratio [OR] = 0.09; 95% confidence interval [CI], 0.03 to 0.23).14 The authors conducted subgroup analysis comparing delayed patient-led or post-dated prescriptions (i.e., patients received at index consultation) to immediate prescription, and delayed collection (prescription not provided at time of visit but kept at office reception or pharmacy for patient to fill if symptoms had not improved after 2 to 7 days [depending on the study]) to immediate prescriptions, and found both approaches had similar effects in reducing antibiotic use compared to immediate prescriptions. The authors concluded that delayed antibiotic prescriptions significantly reduced the use of antibiotics for URTIs. Spurling et al. also investigated various delayed prescription strategies.13 Four of the RCTs in the Spurling et al. SR were also included in the meta-analysis from Mortazhejri et al.14 Relevant RCTs from the Spurling et al. SR all demonstrated significantly reduced antibiotic use for both delayed prescriptions received at the time of consultation and delayed collection compared to immediate antibiotics.13 In 2 studies, the odds of antibiotic use were lower for delayed prescriptions at time of visit compared to immediate prescription; the OR for antibiotic use was 0.20 (95% CI, 0.09 to 0.44) in one study and 0.04 (95% CI, 0.01 to 0.13) in another study. In another 4 studies, the odds of antibiotic use were lower for delayed collection versus immediate antibiotics; the 4 relevant studies had ORs of 0.03 (95% CI, 0.01 to 0.09), 0.00 (95% CI, 0.00 to 0.07), 0.00 (95% CI, 0.00 to 0.02), and 0.05 (95% CI, 0.02 to 0.08). In this SR, 1 relevant RCT reported that delayed prescriptions at time of visit increased antibiotic use compared to no antibiotic prescription (OR = 3.47; 95% CI, 1.34 to 9.01), while delayed collection increased antibiotic use in 2 studies (OR = 2.14; 95% CI, 0.81 to 5.66, in 1 study; OR = 3.18; 95% CI, 1.85 to 5.46, in the other study). The authors concluded that delayed prescriptions markedly reduced the use of antibiotics compared to immediate antibiotics and the least antibiotic use was in the no-antibiotic group.13
Patient Satisfaction
Four RCTs from the Mortazhejri et al. SR reported on patient satisfaction.14 Compared to patients receiving immediate antibiotics, those receiving delayed antibiotics were more satisfied in 1 study (OR = 1.47; 95% CI 0.32, to 6.85), less satisfied in 2 studies (OR = 0.61, 95% CI, 0.25 to 1.49; and OR = 0.32; 95% CI, 0.16 to 0.65), and there was no difference in 1 study (P = 0.14, no further detail provided). Spurling et al. also compared the number of patients satisfied with delayed antibiotics versus immediate antibiotics.13 Among relevant RCTs, the ORs comparing delayed versus immediate antibiotics crossed 1 in 4 studies, suggesting no difference in patient satisfaction between delayed antibiotics or immediate antibiotics. In one study, the odds of satisfaction were decreased in the delayed group compared to the immediate antibiotic group (OR = 0.32; 95% CI, 0.16 to 0.65). The authors of this SR13 concluded that delayed prescriptions did not result in different satisfaction levels compared to immediate antibiotics and that satisfaction was high in both groups.
Reconsultation
Four RCTs in the Mortazhejri et al. SR reported on the intention to re-consult and 1 RCT reported on the actual reconsultation rate.14 There was no difference in the proportion of patients intending to re-consult in the delayed antibiotic group versus the immediate antibiotic group in 2 studies (73% versus 65% in 1 study [OR = 1.50; 95% CI, 0.71 to 3.17] and 69% versus 86% in the other study [OR = 0.62; 95% CI, 0.19 to 2.06]). In 2 studies, the proportion intending to re-consult was lower in the delayed antibiotic group (57% versus 79% in 1study [OR = 0.35; 95% CI, 0.22 to 0.55] and 63% versus 83% [OR = 0.35; 95% CI, 0.20 to 0.62] in the other study). In 1 RCT, there was no difference in the actual reconsultation rate between groups at one month (P = 0.56, no other data provided). While the findings were mixed, these results suggest that delayed antibiotics appear to have either no effect on, or slightly reduce, the intention to re-consult. The authors of the SR did not comment on or make an overall conclusion about the effect of delayed antibiotics on reconsultation rates.
Clinical Symptoms
The Spurling et al. SR reported on pain, malaise, and fever.13 Two RCTs in this SR reported the number of participants with pain on days 3 to 6 in the delayed antibiotic group versus the immediate antibiotic group. In 1 study, there was a numerically greater proportion of participants with pain in the delayed group (13/61 [21%]) compared to the immediate antibiotic group (9/58 [16%]) (OR = 1.47; 95% CI, 0.58 to 3.77); however, this was not statistically significant. In another primary study, the proportion of participants with pain was numerically higher in the delayed antibiotic group than in the immediate antibiotic group (28/111 [25%] versus 15/101 [15%]), but this difference was not statistically significant (OR = 1.93; 95% CI, 0.96 to 3.88). One study in this SR found that a higher proportion of patients experienced pain on day 3 in the delayed antibiotic group (45/150 [30%]) compared to the immediate antibiotic group (19/135 [14%]) (OR = 2.62; 95% CI, 1.44 to 4.76). Finally, 1 RCT in the Spurling et al. SR found no difference in the proportion of patients with fever on days 3 to 6 in the delayed antibiotic group (5/67 [7%]) compared to the immediate antibiotics group (6/62 [10%]) (OR = 0.75; 95% CI, 0.22 to 2.60).13 The authors of the SR concluded that, for many clinical outcomes, there was no significant difference between delayed and immediate antibiotics. However, they noted that symptoms for AOM and sore throat may have been modestly improved by immediate antibiotics compared with delayed antibiotics.
Adverse Effects of Antibiotics
One RCT in the Spurling et al. SR found no difference in the proportion of patients experiencing vomiting in the delayed antibiotic group compared to the control group (15/179 [8%] versus 18/215 [8%], OR = 1.00; 95% CI, 0.49 to 2.05).13 Three RCTs in the Spurling et al. SR reported on rates of diarrhea in the delayed antibiotic group versus immediate — in 2 studies, there was no difference in the proportion of patients experiencing diarrhea in the delayed antibiotic group compared to the immediate group (11/67 versus 12/62 [OR = 0.82; 95% CI, 0.33 to 2.02] in 1 study and 23/179 versus 23/215 [OR = 1.23; 95% CI, 0.67 to 2.28] in another study). One study reported a lower rate of diarrhea in the delayed antibiotic group compared to the immediate antibiotic group (14/150 [9%] versus 25/135 [19%], OR= 0.45; 95% CI, 0.22 to 0.91). Two studies found no difference in the rates of rash for delayed antibiotics versus immediate — the rates in one study were 11/180 (6%) versus 14/215 (7%) (OR = 0.93; 95% CI, 0.41 to 2.1) and the rates in other study were 8/150 (5%) versus 6/135 (4%) (OR = 1.21; 95% CI, 0.41 to 3.58). The authors of the SR did not comment on this specifically; however, these results suggest that there appears to be no difference in the rates of adverse effects of antibiotics for delayed antibiotics compared to immediate antibiotics, with one study suggesting possible lower rates of diarrhea for the delayed antibiotic strategy.
Family Medicine Interventions
Antibiotic Use and Prescribing
One pre-post study in the Carvalho et al. SR examined antibiotic use, finding that a best practice alert reduced antibiotic prescriptions at sinusitis visits in the year following its introduction compared to the year before (86% before introduction versus 62% after, P < 0.01).21 The authors of this primary study concluded that clinical reminders in the electronic medical record could be an effective tool to reduce inappropriate antibiotic use.
Cohen et al. examined the number of participants provided with an antibiotic prescription for sore throat with rapid test-guided therapy with or without clinical scoring systems compared to treating on clinical grounds with or without a scoring system.22 All RCTs reported lower prescription rates for rapid test-guided approaches — 1 RCT reported rates of 86/213 versus 124/211 (risk difference = –18%; 95% CI, –28 to –9), 1 RCT reported 167/367 versus 263/385 (risk difference = –23%; 95% CI, –30 to –16), 1 RCT reported 98/223 versus 133/208 (risk difference = –20%; 95% CI, –0.29 to –0.11), and another reported RCT 63/196 versus 155/274 (risk difference = –24%; 95% CI, –33 to –16). These authors also meta-analyzed 2 RCTs comparing antibiotic dispensing rates for rapid tests with or without scoring systems to those for treating on clinical grounds with or without scoring systems and reported lower dispensing rates in the rapid test group (156/445) compared to the clinical grounds group (197/455) (risk difference= –7%, 95% CI, –17 to –2). The authors concluded that rapid testing to guide antibiotic treatment for sore throat probably reduces antibiotic prescription rates but may have little or no impact on dispensing (although there were statistically fewer antibiotics dispensed in the rapid testing arm).
Fraser et al.25 reported on the same 3 RCTs as Cohen et al.22; however, Fraser et al. reported results by individual study arm in each RCT. In 1 RCT, the number of participants receiving antibiotics was lower for those receiving rapid Strep A test-guided therapy plus clinical criteria (Centor) compared to clinical criteria alone (123/281 [44%] versus 168/262 [64%]). In another RCT, the authors reported the number of participants provided with an antibiotic prescription was lower when therapy was guided by a rapid Strep A test plus clinical score (18% received immediate prescriptions plus 23% received delayed) compared to a clinical score alone (16% received immediate prescriptions plus 41% received delayed). Finally,1 RCT reported the number of participants who received antibiotics with use of a rapid Strep A test plus decision rule (39/102, 38%) versus the rapid test alone (32/120, 27%) versus the decision rule alone (94/170, 55%) versus usual care (82/141, 58%). The authors in this SR concluded that antibiotic prescription rates or use was higher in control arms compared to those incorporating POCTs.
Mortazhejri et al.14 examined antibiotic prescribing for various interventions directed at patients. In 1 RCT, there was no difference in the number of antibiotics prescribed per patient for an education pamphlet and video compared to control (mean difference ‒0.3, P = 0.23). In another RCT, there was no difference in antibiotic prescriptions for a pamphlet versus control (OR = 1.20; 95% CI, 0.84 to 1.72). Another RCT found reduced odds of receiving an antibiotic prescription at index consultation for booklets on RTIs aimed at parents of children compared to control (OR = 0.29; 95% CI, 0.14 to 0.60). Finally, 1 RCT reported no difference in antibiotic prescriptions between an interactive website and control (relative risk [RR] = 1.02; 95% CI, 0.82 to 1.43). The authors concluded that the effect of interventions varied depending on the type of material provided.
Van Hecke et al. examined antibiotic prescribing for POCTs to treat sore throat versus control.24 One RCT reported antibiotic-prescribing rates of 261/581 for POCT versus 364/726 for usual care (RR = 0.90; 95% CI, 0.80 to 1.01), suggesting no difference in antibiotic-prescribing rates for these strategies. In a pre-post study described in this SR, the use of a POCT reduced antibiotic prescription rates post-implementation (34/68 versus 65/108 pre-implementation, RR = 0.48; 95% CI, 0.33 to 0.69). The authors concluded that POCT did not reduce antibiotic prescribing in RCTs but did show an effect in non-randomized studies.
In the Burstein et al. SR, 1 controlled before-after study reported that a multi-faceted intervention led to a 16% reduction in antibiotic prescriptions for URTIs compared to a 2% reduction in the control group (P < 0.06).20 The authors concluded that the intervention led to a modest reduction in antibiotic prescriptions for URTIs.
Health Information and Quality Authority examined antibiotic prescribing at index consultations for the use of CRP POCTs compared to usual care.19 In a meta-analysis of 2 RCTs, the authors reported antibiotic prescription rates of were lower for the CRP group compared to the usual care group (80/260 versus 109/250, RR = 0.72; 95% CI, 0.58 to 0.90). In a meta-analysis of 2 non-randomized studies, the authors reported lower antibiotic prescription rates for CRP compared to usual care (183/335 versus 287/345, RR = 0.65; 95% CI, 0.59 to 0.73). The authors concluded that the use of CRP POCT to guide the management of patients with RTIs leads to reduced antibiotic prescribing at index consultation.
The Deniz et al. SR reported on 2 pre-post studies comparing antibiotic prescription rates before and after the introduction of a guideline on AOM.16 In one study, antibiotic prescription rates fell by 12% and in another study there was no change. The authors of this SR concluded that the introduction of guidelines seems to have a modest impact on antibiotic prescription rates, at best.
Kochling et al. examined different primary care interventions.17 In 1 RCT, the OR for the prescription of an antibiotic dropped to 0.58 (95% CI, 0.43 to 0.78) 6 weeks after a multi-component intervention was introduced and increased to 1.52 (95% CI, 1.19 to 1.95) in the usual care group. At 12 months, the OR was 0.72 (95% CI, 0.54 to 0.97) for the intervention group and 1.31 (95% CI, 1.01 to 1.71) in usual care group. The authors stated that these ORs corresponded to a 60% relative reduction in antibiotic prescription rates at 6 weeks and a persistent 40% relative reduction at 12 months for the intervention compared to usual care. In another RCT, a rapid antigen test for Strep A reduced antibiotic prescribing compared to usual care (123/281 versus 168/262, rate difference = ‒20%). Another RCT in this SR reported no difference in the rate of antibiotic prescriptions for patients receiving education on causes of URTI compared to those receiving control education (94/457 versus 81/457, rate difference = 3%).
Lane et al. examined the effect of locally relevant epidemiological data provided to prescribers on antibiotic-prescribing rates.15 In 1 cohort study with a historical control, the antibiotic-prescribing rates fell to 9% from 26% (P = 0.01) in the 3 years following the introduction of a surveillance program compared to the control period. In another study, antibiotic-prescribing rates were lower when prescribers received epidemiological data during a pandemic compared to a non-pandemic period (antibiotics prescribed at 3054/7789 visits versus 9741/20512, OR = 0.72; 95% CI, 0.68 to 0.77). One RCT found no difference in antibiotic-prescribing rates when GPs were proved with a heat map and decision support tool compared to control (41% prescription rate for intervention versus 41% for control, P = 0.90). The authors concluded that surveillance systems could support antibiotic decision-making but that few interventions had been evaluated and existing studies were methodologically weak.
Odermatt et al.36 reported outcomes of an individual patient meta-analysis based on the Schuetz et al. SR.18 This publication included individuals with URTI from 2 RCTs in the Schuetz et al. SR, which examined procalcitonin to guide antibiotic prescribing compared to control. These authors found that procalcitonin-guided interventions reduced antibiotic prescription rates compared to control (59/332 versus 159/312, OR = 0.2; 95% CI, 0.1 to 0.3). The authors also found that the mean number of days exposed to antibiotics was lower in the procalcitonin group versus control (1.2 days [standard deviation 2.8] versus 3.7 days [4.0]). The authors concluded that procalcitonin-guided therapy reduced antibiotic exposure in URTI patients without compromising outcomes (which are reported in the sections Days With Restricted Activity and Treatment Failure at 28 Days that follow).
Guideline Adherence
One study in the Carvalho et al. SR examined antibiotic-prescribing guideline adherence among providers receiving a multi-component intervention versus a historical control. The authors found that guideline adherence was 91% following the intervention compared to 77% in the control group.21
Recovery
One RCT in the Health Information and Quality Authority SR reported that no difference was found in recovery at 7 days for the use of CRP POCT to guide antibiotic prescribing compared to usual care (27/118 versus 31/125, RR = 1.03; 95% CI, 0.89 to 1.18).19
Time to Resolution of Symptoms
Two RCTs in the Health Information and Quality Authority SR examined the median time to resolution of symptoms for the use of CRP POCT to guide antibiotic prescribing compared to usual care. Both studies reported no difference in the time to resolution of symptoms.19
Reconsultation
The Cohen et al. SR meta-analyzed 2 RCTs that compared reconsultation for the use of rapid test-guided therapy with or without scoring systems to those for treatment on clinical grounds with or without scoring systems.22 There was no difference in reconsultation rates between the 2 groups (59/571 versus 51/590, OR 1.12 = 95% CI, 0.57 to 2.21).
The Mortazhejri et al. SR14 examined various patient-directed interventions and identified 2 RCTs that examined reconsultation rate. One study found no difference in reconsultation rates over 1 year for patients receiving an online program compared to control (19% versus 19%, OR = 0.93; 95% CI, 0.73 to 1.16). Another study found that the intention to re-consult was lower for patients receiving an interactive booklet compared to control (55% versus 76%, OR = 0.34; 95% CI, 0.20 to 0.57).
One RCT from the Van Hecke et al. SR found that reconsultation events were lower for POCT-guided treatment of sore throat compared to usual care (RR = 4.70; 95% CI, 2.94 to 7.51). No further data were provided, so the direction of RR and definition of outcome were unclear).24
The Health Information and Quality Authority SR found 2 RCTs on the reconsultation rate for the CRP-guided treatment of URTIs compared to usual care.19 In 1 study, the reconsultation rate was 33/129 in the CRP group and 23/129 in the usual care group (RR = 1.43; 95% CI, 0.89 to 2.30). In another study, the reconsultation rate was 165/894 in the CRP group and 149/812 in the usual care group (RR = 1.01; 95% CI, 0.82 to 1.23).
Patient Satisfaction
In the Mortazhejri et al. SR, 1 RCT reported no difference in satisfaction for patients receiving an interactive booklet compared to control (90% versus 94%) (OR = 0.64; 95% CI, 0.33 to 1.22).14
In the Health Information and Quality Authority SR, 1 RCT found that the proportion of patients satisfied with care was higher for those receiving CRP POCT-guided antibiotic therapy compared to usual care (90/118 [76%] versus 79/125 [63%]).19 In another RCT, there was no difference in patient satisfaction for CRP-POCT testing versus usual care (RR = 1.01; 95% CI, 0.86 to 1.16 [event rates not reported]).
Complication Attributed to Index Infection
In the Cohen et al. SR, the authors examined the number of participants with a complication attributed to the index infection for the use of rapid tests with or without scoring systems to guide the treatment of sore throat compared to treatment on clinical grounds with or without scoring systems.22 In 1 RCT, the rate of complications was 2/213 in the rapid testing group and 0/211 in the clinical grounds group; in the other RCT, there were no events in either group.
Days With Restricted Activity
Schuetz et al. (data from Odermatt et al.36) compared procalcitonin-guided antibiotic therapy to usual care and found no difference in the median number of days with restricted activity between the 2 groups (4.2 days [IQR 5 to 14] versus 4.3 days [IQR 5 to 13]) in a meta-analysis of 2 RCTs.18 The authors concluded there was no difference in the number of days with restricted activities between the groups.
Treatment Failure at 28 Days
Schuetz et al. (data from Odermatt et al.36) also examined treatment failure at 28 days for procalcitonin-guided antibiotic therapy compared to usual care.18 There was no difference in the rate of treatment failure between the 2 groups (110/132 versus 106/132) (OR = 1.0; 95% CI, 0.7 to 1.4) based on a meta-analysis of 2 RCTs. The authors concluded there was no difference in the rate of treatment failure.
Limitations
Delayed Antibiotics
Several primary studies in the SRs on delayed antibiotics examined antibiotic use and patient satisfaction; however, there were fewer data on clinical outcomes such as symptoms, health care utilization, quality of life, and hospitalizations, as well as on antibiotic resistance and appropriateness of prescribing. Further, studies focused on rates of prescribing or use without information on whether antibiotics were over-or underprescribed.
The eligible SRs included studies with a mixture of patient populations (adults, children); however, it was unclear whether there were any differences in outcomes based on the population (Moratzhejri et al. did not investigate this14 and Spurling et al. noted no difference in outcomes for children compared to adults, but it was not possible to determine whether this was true for URTI in primary care specifically).13 The RCTs in the 2 SRs were conducted in Western countries; however, only one trial was conducted in Canada. The study populations were not described in detail in the SRs, making it challenging to understand the generalizability of the patient populations to the Canadian context. Further, antibiotic-prescribing practices (e.g., types of antibiotics prescribed, baseline use of antibiotics)17 and health care system differences between countries make the generalizability of these studies to the Canadian context unclear.
Family Medicine Interventions
The SRs of family medicine interventions reported on antibiotic use and prescribing, and 4 SRs reported on reconsultation rates, but like the studies on delayed antibiotic interventions, there were less data on other clinical outcomes. Similar to the studies on delayed antibiotic interventions, family medicine interventions focused on rates of prescribing or use without information on whether antibiotics were over- or underprescribed.
There was little evidence on clinical outcomes, health care utilization, and antibiotic resistance. One study in one SR reported on recovery and time to resolution of symptoms, 1 SR reported on complications attributed to index infection,22 while 1 SR reported on days with restricted activity.18 In some of the SRs, the interventions of interest were quite broad (e.g., “primary care interventions” in the Kochling et al. SR17), making it difficult to draw conclusions about the effect of the interventions across the review. Few of the SRs reported on the same types of interventions, further challenging the ability to draw conclusions on the body of evidence. There was more relevant evidence on different diagnostic tests (e.g., rapid Strep A tests, CRP) compared to patient and provider-directed interventions (e.g., education, tools); however, there were generally few relevant studies available for each individual intervention. The patient or provider-directed interventions also differed from one another in the included components, making it challenging to draw conclusions across studies. Another limitation was that some of the SRs included relatively few primary studies with poor methodological quality. For example, in the Lane et al. SR,5 only 3 primary studies were found, which the authors concluded were methodologically weak. In many of the SRs, few primary studies were relevant for this report, making it challenging to draw conclusions about the evidence. Further, only 1 primary study in the 11 SRs on family medicine interventions was conducted in Canada. Given possible differences in primary care systems and antibiotic-prescribing practices in other contexts, it is unclear whether the results of the eligible SRs are generalizable to the Canadian primary care context.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 SR13 examining delayed antibiotics for URTIs, 1 SR examining both delayed antibiotics and patient-directed interventions to reduce unnecessary antibiotic use in URTIs,14 and 11 SRs15-25 examining various family medicine interventions to influence the use of antibiotics for URTIs.
Delayed Antibiotics
Delayed antibiotic prescriptions appeared to significantly reduce the use of URTIs compared to immediate antibiotic prescriptions in the 2 SRs13,14 examining this — this applied to both delayed prescriptions provided at the time of visit and delayed collection (prescription not provided at time of visit but kept at office reception or pharmacy for patient to fill if symptoms not improved after, for example, 2 days). Based on the individual studies from the SRs, delayed antibiotics generally did not appear to show any difference in patient satisfaction compared to immediate antibiotics, while results were mixed on the reconsultation rate. The intent to re-consult was lower in the delayed antibiotic group compared to immediate antibiotics (in 2 RCTs from one SR14), there was no difference in intent to re-consult in 2 RCTs from the same SR,14 and there was no difference in the actual reconsultation rate (in 1 RCT from one SR).14 The effect of delayed antibiotic prescribing on clinical symptoms of URTIs was less clear — 1 SR13 concluded that symptoms of AOM and sore throat might have been modestly improved by immediate antibiotics compared to delayed antibiotics; however, this was based on 1 RCT examining malaise and fever, and 2 RCTs examining pain in URTI.
Family Medicine Interventions
Various family medicine interventions were identified and the effects appeared to differ based on the individual interventions. Different rapid tests or POCTs were examined in eligible SRs,18,19,22 which all appeared to reduce antibiotic prescribing. A well-conducted SR on rapid testing for group A strep (with or without scoring systems) to guide the treatment of sore throat suggested that this intervention reduced antibiotic-prescribing rates compared to treatment on clinical grounds, but rapid testing led to a smaller reduction in antibiotic dispensing.22 Another well-conducted SR suggested that CRP POCT-guided treatment reduced antibiotic prescribing for URTIs at index consultations compared to usual care.19 One SR further reported that procalcitonin-guided antibiotic therapy in URTIs reduced antibiotic exposure compared to control. There were less data on other outcomes, in particular clinical outcomes.18 The use of CRP POCTs to guide antibiotic prescribing in URTIs led to no difference in recovery or time to resolution of symptoms in 1 SR; however, this was based on only 2 RCTs.19 In 1 SR,22 there was no difference in reconsultation rates for rapid Strep A tests (2 studies), while in another SR there was no difference in reconsultation rates for CRP POCT (2 studies) compared to usual care.19 One RCT in 1 SR found that a POCT for sore throat reduced re-consultations compared to usual care.24 The use of procalcitonin testing to guide therapy led to no difference in the number of days with restricted activities or rates of treatment failure compared to control based on 1 meta-analysis of 2 RCTs in 1 SR.18,36
There was more heterogeneity in findings for different patient or provider-directed interventions, such as education or tools. For example, 1 SR found no difference in antibiotic prescribing for 3 different patient-directed interventions (compared to either no intervention or usual care) but found that a pamphlet on RTIs aimed at parents of children reduced antibiotic prescribing compared to usual care in 1 study.14 Two SRs each identified 1 primary study (i.e., 2 primary studies in total) that found that multi-component interventions involving provider interventions (e.g., education, training, decision support tools), as well as patient-directed interventions (e.g., handouts, posters), may reduce antibiotic prescribing compared to control and usual care. However, the only relevant study in 1 SR was a controlled before-after study20 and the authors of the other SR were unsure whether the reduction in antibiotic prescribing was clinically meaningful for 1 of the primary studies.17 One SR found few studies examining the effect of infection surveillance systems to support antibiotic decision-making, noting that available evidence was methodologically weak. Finally, 2 studies on the effect of guidelines for the treatment of AOM had mixed results and the authors of this SR suggested that this intervention may have a modest impact on antibiotic prescribing, at best.16 Results on reconsultation were mixed for patient-directed interventions — in 1 SR, there was no difference in the reconsultation rate in 1 study and a reduction in intention to re-consult in another.14
Implications
There is increasing awareness of the overuse of antibiotics. Strategies are needed to mitigate potentially inappropriate antibiotic use; for example, the use of antibiotics to treat URTIs that are viral in origin.7 Strategies aimed at influencing antibiotic use should reduce such inappropriate antibiotic use while ideally either improving or not compromising clinical outcomes or health care utilization. In this report, most of the available evidence pertained to how interventions impacted overall antibiotic prescribing and use. There was evidence that delayed antibiotics reduced antibiotic prescribing and use compared to immediate antibiotics, while rapid test/POCT-guided therapy was shown to reduce antibiotic prescribing compared to usual care for URTIs. Thus, these strategies appear to be useful to implement in order to reduce antibiotic-prescribing rates for URTI. Delayed antibiotic prescriptions also do not appear to have a negative effect on patient satisfaction or reconsultation rates. However, it was less clear whether delayed antibiotics or rapid/POCTs had an impact on clinical outcomes, health care utilization, and antibiotic resistance, as there was little or no available evidence on these outcomes.
There was variability in the effectiveness of patient and provider-directed interventions to influence prescribing, such as patient education and provider training.14,17,20 The utility of such interventions may depend on the context and type of material provided and the delivery method. Given the heterogeneity in findings and limited evidence on different patient and provider-directed interventions, policy-makers may wish to carefully examine the comparability of primary studies with their health care context when considering implementing such interventions. Similar to delayed antibiotic-prescribing interventions, there was limited evidence on clinical outcomes, antibiotic resistance, and health resource utilization with patient and provider-directed interventions.
Overall, syntheses of evidence specifically on URTI in primary care settings (family medicine, GP) will be helpful to provide more clear evidence on the effect of interventions to influence antibiotic prescribing for URTIs in this setting. Further, more data on clinical outcomes, antibiotic resistance, and health care utilization would help to improve the understanding of the effects of interventions aimed at influencing antibiotic prescribing for URTIs.
References
1.Thomas M, Bomar PA. Upper respiratory tract infection. Treasure Island (FL): StatPearls Publishing; 2020: https://www.ncbi.nlm.nih.gov/books/NBK532961/. Accessed 2020 Oct 28.
2.Finley C, Chan D, Garrison S, et al. What are the most common conditions in primary care? Systematic review. Can Fam Phys. 2018;64(11).
3.Hutchinson J, Jelinski S, Hefferton D, Desaulniers G, Parfrey P. Role of diagnostic labeling in antibiotic prescription. Can Fam Physician. 2001;47. Medline
4.Dolk FCK, Pouwels KB, Smith DRM, Robotham JV, Smieszek T. Antibiotics in primary care in England: which antibiotics are prescribed and for which conditions? J Antimicrob Chemother. 2021;73(suppl_2).
5.Schwartz K. Unnecessary antibiotic prescribing in a Canadian primary care setting: a descriptive analysis using routinely collected electronic medical record data. CMAJ Open. 2020:E360. Medline
6.Smith SM, Fahey T, Smucny J, Becker LA. Antibiotics for acute bronchitis. Cochrane Database Syst Rev. 2017;6:CD000245. Medline
7.Leis JA, Born KB, Theriault G, Ostrow O, Grill A, Johnston KB. Using antibiotics wisely for respiratory tract infection in the era of covid-19. BMJ. 2020;371. Medline
8.Handle with care: preserving antibiotics now and into the future. Ottawa (ON): Public Health Agency of Canada; 2019: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/preserving-antibiotics/Final_CPHO_Report_EN_June6_2019.pdf. Accessed 2021 Jan 21.
9.Choosing Wisely Canada. Delayed prescription. 2018; https://choosingwiselycanada.org/wp-content/uploads/2018/10/Delayed-Prescription-EN-.pdf. Accessed 2021 Jan 21.
10.Lee C, Jafari M, Brownbridge R, Phillips C, Vanstone JR. The viral prescription pad - a mixed methods study to determine the need for and utility of an educational tool for antimicrobial stewardship in primary health care. BMC Fam Pract. 2020;21(1):1-12. Medline
11.Choosing Wisely Canada. The Cold standard: second edition. 2020; https://choosingwiselycanada.org/perspective/the-cold-standard/. Accessed 2021 Jan 21.
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. Medline
13.Spurling GK, Del Mar CB, Dooley L, Foxlee R, Farley R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst Rev. 2017;9:CD004417. Medline
14.Mortazhejri S, Hong PJ, Yu AM, et al. Systematic review of patient-oriented interventions to reduce unnecessary use of antibiotics for upper respiratory tract infections. Syst Rev. 2020;9(106). Medline
15.Lane I, Bryce A, Ingle SM, Hay AD. Does locally relevant, real-time infection epidemiological data improve clinician management and antimicrobial prescribing in primary care? A systematic review. Fam Pract. 2018;35(5):542-550. Medline
16.Deniz Y, van Uum RT, de Hoog MLA, Schilder AGM, Damoiseaux R, Venekamp RP. Impact of acute otitis media clinical practice guidelines on antibiotic and analgesic prescriptions: a systematic review. Arch Dis Child. 2018;103(6):597-602. Medline
17.Kochling A, Loffler C, Reinsch S, et al. Reduction of antibiotic prescriptions for acute respiratory tract infections in primary care: a systematic review. Implement Sci. 2018;13(1):47. Medline
18.Schuetz P, Wirz Y, Sager R, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017;10:CD007498. Medline
19.Health Technology Assessment of C-reactive protein point-of-care testing to guide antibiotic prescribing for acute respiratory tract infections in primary care settings. Dublin (IE): Health Information and Quality Authority; 2019: https://www.hiqa.ie/sites/default/files/2019-05/HTA_C-reactive_Protein_Point_of_Care_Testing-FullReport.pdf. Accessed 2021 Jan 21.
20.Burstein VR, Trajano RP, Kravitz RL, Bell RA, Vora D, May LS. Communication interventions to promote the public's awareness of antibiotics: a systematic review. BMC Public Health. 2019;19(1):899. Medline
21.Carvalho É, Estrela M, Zapata-Cachafeiro M, Figueiras A, Roque F, Herdeiro M. E-health tools to improve antibiotic use and resistances: a systematic review. Antibiotics (Basel, Switzerland). 2020;9(8). Medline
22.Cohen JF, Pauchard JY, Hjelm N, Cohen R, Chalumeau M. Efficacy and safety of rapid tests to guide antibiotic prescriptions for sore throat. Cochrane Database Syst Rev. 2020;6:CD012431. Medline
23.McDonagh MS, Peterson K, Winthrop K, Cantor A, Lazur BH, Buckley DI. Interventions to reduce inappropriate prescribing of antibiotics for acute respiratory tract infections: summary and update of a systematic review. J Int Med Res. 2018;46(8):3337-3357. Medline
24.Van Hecke O, Raymond M, Lee JJ, et al. In-vitro diagnostic point-of-care tests in paediatric ambulatory care: a systematic review and meta-analysis. PLoS One. 2020;15(7):e0235605. Medline
25.Fraser H, Gallacher D, Achana F, et al. Rapid antigen detection and molecular tests for group A streptococcal infections for acute sore throat: systematic reviews and economic evaluation. Health Technol Asses. 2020;24(31):1-232. Medline
26.Arroll B, Kenealy T, Kerse N. Do delayed prescriptions reduce the use of antibiotics for the common cold? A single-blind controlled trial. J Fam Pract. 2002;51(4). Medline
27.Little P, Williamson I, Warner G, Gould C, Gantley M, Kinmonth A. Open randomised trial of prescribing strategies in managing sore throat. BMJ. 1997;314(7082). Medline
28.Little P, Gould C, Williamson I, Moore M, Warner G, Dunleavey J. Pragmatic randomised controlled trial of two prescribing strategies for childhood acute otitis media. BMJ. 2001;322. Medline
29.de la Poza Abad M, Mas Dalmau G, Moreno Bakedano M, et al. Prescription strategies in acute uncomplicated respiratory infections: a randomized clinical trial. JAMA Intern Med. 2016;176(1). Medline
30.Little P, Hobbs FDR, Moore M, et al. Clinical score and rapid antigen detection test to guide antibiotic use for sore throats: randomised controlled trial of PRISM (primary care streptococcal management). BMJ. 2013;347. Medline
31.Llor C, Mandrel J, Balagué-Corbella M, Gómez M, Cots JM. Impact on antibiotic prescription of rapid antigen detection testing in acute pharyngitis in adults: a randomised clinical trial. Br J Gen Pract. 2011;61(586):e244-e251. Medline
32.Worrall G, Hutchinson J, Sherman G, Griffiths J. Diagnosing streptococcal sore throat in adults: randomized controlled trial of in-office aids. Can Fam Physician. 2007;53(4). Medline
33.Llor C, Bjerrum L, Arana J, et al. C-reactive protein testing in patients with acute rhinosinusitis leads to a reduction in antibiotic use. Fam Pract. 2012;29(6). Medline
34.Liberates A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
35.McDonagh M, Peterson K, Winthrop K, Cantor A, Holzhammer B, Buckley DI. Improving antibiotic prescribing for uncomplicated acute respiratory tract infections. Rockville (MD): Agency for Healthcare Research and Quality; 2016: https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/antibiotics-respiratory-infection_research.pdf. Accessed 2021 Jan 21.
36.Odermatt J, Friedli N, Kutz A, et al. Effects of procalcitonin testing on antibiotic use and clinical outcomes in patients with upper respiratory tract infections. An individual patient data meta-analysis. Clin Chem Lab Med. 2017;56(1):170-177. Medline
37.Ginzburg R, Conway J, Waltermaurer E, Song W, Jellinek-Cohen S. Using clinical decision support within the electronic health record to reduce incorrect prescribing for acute sinusitis. J Patient Cent Res Rev. 2018;5(3). Medline
38.Rubin M, Bateman K, Alder S, Donnelly S, Stoddard G, Samore M. A multifaceted intervention to improve antimicrobial prescribing for upper respiratory tract infections in a small rural community. Clin Infect Dis. 2005;40(4). Medline
39.Hingorani R, Mahmood M, Alweis R. Improving antibiotic adherence in treatment of acute upper respiratory infections: a quality improvement process. J Community Hosp Intern Med Perspect. 2015;5(3). Medline
40.Dowell J, Pitkethly M, Bain J, Martin S. A randomised controlled trial of delayed antibiotic prescribing as a strategy for managing uncomplicated respiratory tract infection in primary care. Br J Gen Pract. 2001;51(464). Medline
41.Little P, Moore M, Kelly J, et al. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: pragmatic, factorial, randomised controlled trial. BMJ. 2014. Medline
42.Pshetizky Y, Naimer S, Shvartzman P. Acute otitis media--a brief explanation to parents and antibiotic use. Fam Pract. 2003;20(4). Medline
43.Worrall G, Kettle A, Graham W, Hutchinson J. Postdated versus usual delayed antibiotic prescriptions in primary care: reduction in antibiotic use for acute respiratory infections? Can Fam Physician. 2010;56(10). Medline
44.Altiner A, Brockmann S, Sielk M, Wilm S, Wegscheider K, Abholz H. Reducing antibiotic prescriptions for acute cough by motivating GPs to change their attitudes to communication and empowering patients: a cluster-randomized intervention study. J Antimicrob Chemother. 2007;60(3). Medline
45.Bjerrum L, Gahrn-Hansen B, Munck A. C-reactive protein measurement in general practice may lead to lower antibiotic prescribing for sinusitis. Br J Gen Pract. 2004;54(506). Medline
46.Briel M, Schuetz P, Mueller B, et al. Procalcitonin-guided antibiotic use vs a standard approach for acute respiratory tract infections in primary care. Arch Intern Med. 2021;168(18):2000-2007. Medline
47.Burkhardt O, Ewig S, Haagen U, et al. Procalcitonin guidance and reduction of antibiotic use in acute respiratory tract infection. Eur Respir J. 2010;36(3). Medline
48.Cals J, Schot M, de Jong S, Dinant G, Hopstaken R. Point-of-care C-reactive protein testing and antibiotic prescribing for respiratory tract infections: a randomized controlled trial. Ann Fam Med. 2010;8(2). Medline
49.Francis NA, Butler CC, Hood K, Simpson S, Wood F, Nuttall J. Effect of using an interactive booklet about childhood respiratory tract infections in primary care consultations on reconsulting and antibiotic prescribing: a cluster randomised controlled trial. BMJ. 2009;339. Medline
50.Hebert C, Beaumont J, Schwartz G, Robicsek A. The influence of context on antimicrobial prescribing for febrile respiratory illness: a cohort study. Ann Intern Med. 2012;157(3). Medline
51.Lee M, Pan D, Huang J, et al. Results from a patient-based health education intervention in reducing antibiotic use for acute upper respiratory tract infections in the private sector primary care setting in Singapore. Antimicrob Agents Chemother. 2017;61(5). Medline
52.Kavanagh K, O'Shea E, Halloran R, Cantillon P, Murphy A. A pilot study of the use of near-patient C-Reactive Protein testing in the treatment of adult respiratory tract infections in one Irish general practice. BMC Fam Pract. 2011;12. Medline
53.Little P, Stuart B, Francis N, et al. Effects of internet-based training on antibiotic prescribing rates for acute respiratory-tract infections: a multinational, cluster, randomised, factorial, controlled trial. Lancet. 2013;382(9899). Medline
54.Little P, Stuart B, Andreou P, et al. Primary care randomised controlled trial of a tailored interactive website for the self-management of respiratory infections (Internet Doctor). BMJ Open. 2016;6(4). Medline
55.Malecki M. Rapid strip tests as a decision-making tool about antibiotic treatment in children – a prospective study. Pediatr Pol. 2017;92(2):149-155.
56.Meier F, Howland J, Johnson J, Poisson R. Effects of a rapid antigen test for group A streptococcal pharyngitis on physician prescribing and antibiotic costs. Arch Intern Med. 1990;150(8). Medline
57.Rios L, Mallafre M, Gonzalez-Hidalgo R, Collado A, Carbonell J, Colomes L. Aplicación de una pauta terapéutica revisada de otitis media en una consulta pediátrica. Revista de Calidad Asistencial. 2001;18(1):5-8.
58.Shah N, Ridgway JP, Konchak C, Fahrenbach J, Brown EC, Robicsek A. 163. What's going around? A prospective cluster randomized trial to evaluate a novel, real-time, syndromic surveillance tool's effect on clinical decision making amongst primary care providers. Open Forum Infect. 2021;1(suppl_1).
59.Taylor J, Kwan-Gett T, McMahon EJ. Effectiveness of a parental educational intervention in reducing antibiotic use in children: a randomized controlled trial. Pediatr Infect Dis J. 2005;24(6):489-493. Medline
60.Temte J, Shult P, Kirk C, Amspaugh J. Effects of viral respiratory disease education and surveillance on antibiotic prescribing. Fam Med. 1999;31(2). Medline
61.Thompson P, Gilbert R, Long P, Saxena S, Sharland M, Wong I. Has UK guidance affected general practitioner antibiotic prescribing for otitis media in children? J Public Health (Oxf). 2008;30(4). Medline
62.Tyrstrup M, Beckman A, Mölstad S, et al. Reduction in antibiotic prescribing for respiratory tract infections in Swedish primary care- a retrospective study of electronic patient records. BMC Infect Dis. 2016;16(1):1-10. Medline
Appendix 1: Selection of Included Studies
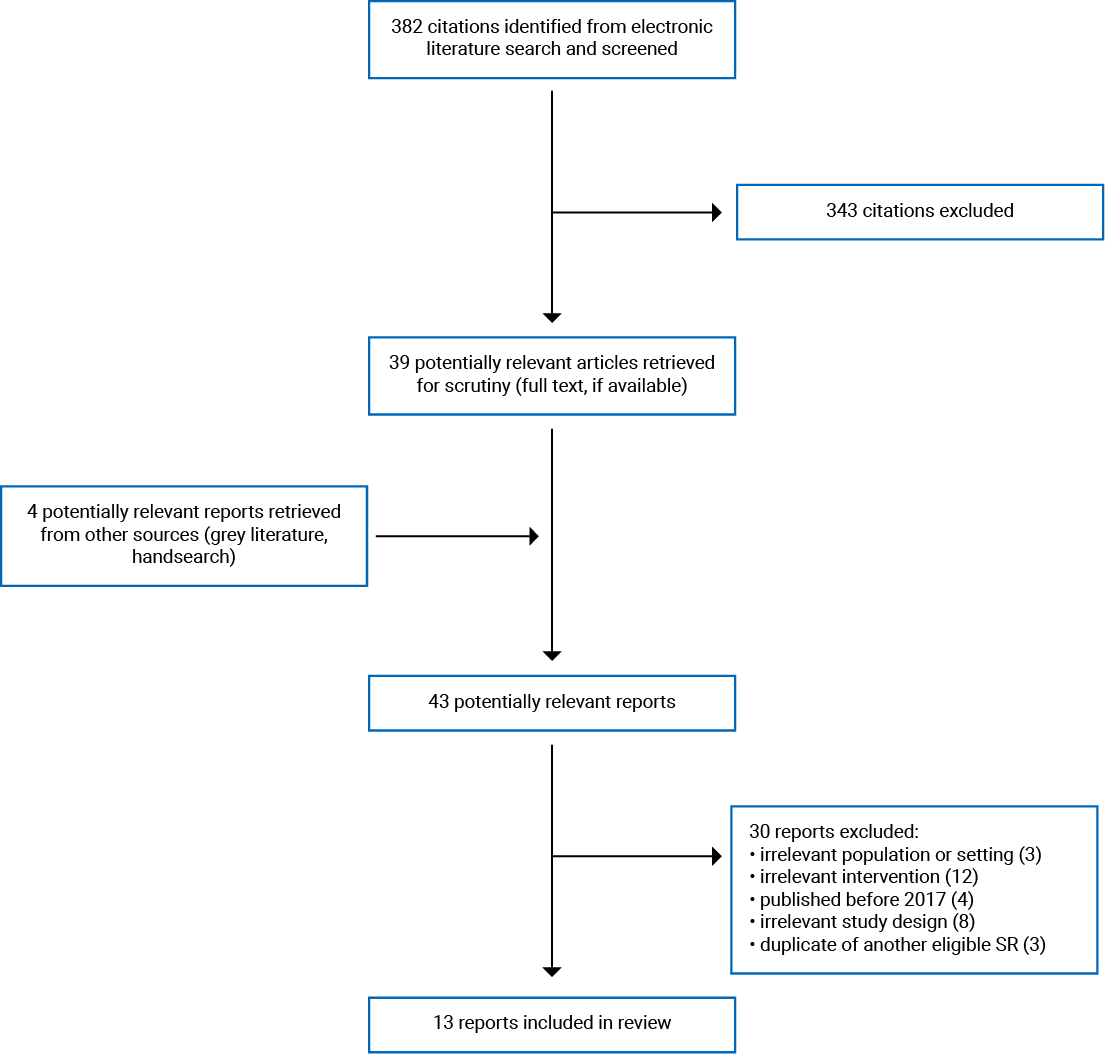
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews on Delayed Antibiotics
Study citation, country, funding source | Objective, study designs, databases searched, search date, number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Mortazhejri et al. (2020)14 Canada No funding | Objective: “Identify the interventions directed at patients to reduce unnecessary use of antibiotics to better understand ones that are more effective” (p.2) Study Designs: RCTs, quasi-RCTs, CBA, ITS conducted in GP setting Databases: MEDLINE, Embase, CENTRAL, CINAHL, Web of Science Search Date: October to November 2016 Number of Studies: 13 studies in total 7 RCTs relevant to the present report (on delayed antibiotic prescriptions in primary care) | Members of general public or patients of any age group with URTI who sought treatment in GP setting Delayed antibiotic studies: 2 studies in children (n = 81 and n = 315), 1 study in adults (n = 149), 4 studies in all patients (n = 129, n = 716, n = 556, n = 398); patients presenting to general/family practice with URTIs RCTs conducted in UK, Israel, Spain, Canada | Intervention: Any intervention directed to patients, parents of patients, public, or healthy individuals to reduce unnecessary use of antibiotics Authors separated into delayed antibiotic prescriptions and interventions directed at patients and public (education session, mass media education, pamphlets, website, and videos) Comparator: No intervention, standard or usual care | Prescription or use of antibiotics by patients for URTI in primary care Patient satisfaction with consultation Reconsultation for same illness Follow-up not specified |
Spurling et al. (2017)13 Australia Supported by Bond University, Australia; the Discipline of General Practice at the University of Queensland, Australia; General Practice Education and Training Limited, Australia | Objective: “To evaluate the effects on clinical outcomes, antibiotic use, antibiotic resistance, and patient satisfaction of advising a delayed prescription of antibiotics in respiratory tract infections.” (p.1) Study Designs: RCTs Databases: MEDLINE, Embase, Cochrane Library, CINAHL, Web of Science Search Date: November 2020 (original 2017 publication searched to May 2017; however, this is a living systematic review and most the recent search from November 2020 with no new studies added since 2017 publication) Number of Studies: 11 studies in total (any RTI in range of settings: pediatric clinics, ED, primary care) 5 studies relevant for this report (URTI only and in primary care) | 1 RCTs (n = 712) adults and children with sore throat 1 RCTs (n = 398) among adults (mean age 42 years) with uncomplicated RTI 1 RCT (n = 191) adults and children with cough 1 RCT (n = 315) among children with AOM 1 RCT (n = 129) among adults and children with common cold RCTs conducted in Spain, New Zealand, Scotland, UK | Intervention: Delayed antibiotics (use or advice to use antibiotics more than 48 hours after initial consultation) Comparator: No antibiotics or immediate antibiotics | Clinical outcomes for sore throat, AOM, cough, cold Antibiotic use Patient satisfaction Antibiotic resistance Adverse effects of antibiotics Complications of disease Reconsultation Follow-up not specified |
AOM = acute otitis media; CBA = controlled before-after; ED = emergency department; ITS = interrupted time series; RCT = randomized controlled trial; RTI = respiratory tract infection; URTI = upper respiratory tract infection.
Table 3: Characteristics of Included Systematic Reviews on Family Medicine Interventions
First author, publication year, country | Objective, study designs, databases searched, search date, number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Carvalho (et al. 2020)21 Portugal Funded by the operational program Competitiveness and Internationalisation in its FEDER/FNR component, and by the Foundation for Science and Technology in its State Budget component | Objective: Assess influence of e-health tools, in particular, and CDSSs, on antibiotic use Study Designs: Randomized and non-randomized trials, observational studies; including both primary care and hospital-based interventions Databases: PubMed, EMBASE Search Date: February 2020 Number of Studies: 22 studies in total (on any RTI in different settings: hospital, pediatric clinics, primary care) 2 studies relevant to this report based on URTI only and in primary care (1 pre-post study, 1 cohort study) | Both studies were in the general population (children and adults) 1 study on sinusitis (54 providers and 438 visits) and 1 study on sinusitis and pharyngitis (27 physicians, 1 nurse, and 240 visits) Studies conducted in US | Intervention: e-health tools (varied between studies) 1 study: best practice alert 1 study: didactic teaching, guidelines, CDSS integrated in EMR Comparator: Pre-intervention period | Antibiotic prescription practices Adherence to guidelines concerning antibiotic prescriptions Follow-up not reported |
Cohen et al. (2020)22 France Funded by the French Ministry of Health, France Research grant PHRC regional, AOR 12089 (2012) | Objective: “Assess the efficacy and safety of strategies based on rapid tests to guide antibiotic prescriptions for sore throat in primary care settings.” (p. 7) Study Designs: RCTs (individual participant and cluster) Databases: CENTRAL, MEDLINE, Embase, CINAHL, LILACS, Web of Science Search Date: June 2019 Number of Studies: 5 RCTs in total (on sore throat in primary care settings, which included pediatrician office and family medicine office) 3 RCTs relevant for this report (family medicine office only) | Ambulatory care participants of all ages with chief complaint of acute sore throat or clinical diagnosis of pharyngitis or tonsilitis 1 study included children and adults (≥ 3 years, n = 424, mean age 31) 1 study, adults only (≥ 19 years, n = 533, mean age NR) 1 study included patients aged 14 to 60 years (n = 557, mean age 32) RCTs conducted in UK, Spain, Canada | Intervention: Use of a rapid test (rapid antigen detection test = enzyme immune assay), alone or in combination with a scoring system Comparator: Management on clinical grounds | Antibiotic use Duration of sore throat symptoms Duration of other symptoms Quality of life Complication due to index infection Reconsultation Hospital admission Satisfaction Adverse events from rapid test Follow-up not reported |
Fraser et al. (2020)25 UK Funded by HTA programme at NIHR‒National Institute for Health Research) in the UK | Objective: Systematically review evidence for POCTs for group A Streptococcus in primary care and hospital settings Study Designs: No limitation Databases: MEDLINE, Embase, Cochrane Library, DARE, Web of Science, PROSPERO Search Date: March 2019 Number of Studies: 38 studies in total (included both various primary settings and secondary care) 3 RCTs relevant for this report (family medicine, only) | People aged ≥ 5 years presenting with sore throat Mean age in 29 to 31 years in 1 RCT, mean age 32 years in 1 RCT, patients aged ≥ 19 years in 1 RCT RCTs conducted in UK, Spain, Canada | Intervention: Rapid POCTs for strep A bacterium with or without clinical scoring tools Comparator: Antibiotic prescribing based on clinical judgment and clinical scoring tools alone | Antibiotic-prescribing rates Inappropriate antibiotic decision Follow-up not reported |
Mortazhejri et al. (2020)14 Canada No funding | Objective: “Identify the interventions directed at patients to reduce unnecessary use of antibiotics to better understand ones that are more effective” (p.2) Study Designs: RCTs, quasi-RCTs, CBA, ITS conducted in GP setting Databases: MEDLINE, Embase, CENTRAL, CINAHL, Web of Science Search Date: October to November 2016 Number of Studies: 13 studies in total (mixture of interventions and settings) 4 studies relevant for this report (4 RCTs in primary care for URTI) | Patients of any age group with URTI who sought treatment in GP setting Patient/public interventions: 1 RCT (n = 558) among children, 1 RCT among patients (age NR, n = 914), 1 RCT among adults (n = 2,923), 1 among children (n = 499) RCTs conducted in UK and US | Intervention: Any intervention directed to patients, parents of patients, public, or healthy individuals to reduce unnecessary use of antibiotics Authors separated into delayed antibiotic prescriptions and interventions directed at patients/public (education session, pamphlets, website, and videos) Comparator: No intervention, standard or usual care | Prescription or use of antibiotics by patients for URTI in primary care Patient satisfaction with consultation Reconsultation for same illness Follow-up not reported |
Van Hecke et al. (2020)24 UK Funded by NIHR‒National Institute for Health Research Community Healthcare MedTech and In Vitro Diagnostics Co-operative at Oxford Health NHS Foundation Trust | Objective: “Describe the clinical impact of all in-vitro diagnostic POCTs on patient outcomes and healthcare processes in pediatric ambulatory care” (p.1) Study Designs: RCTs and non-randomized studies Databases: MEDLINE, Embase, PubMed, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Web of Science Search Date: January 2020 Number of Studies: 35 studies (included various POCTs in range of ambulatory settings: GP, hospital, pharmacy, ED) 2 studies relevant for this report (on URTI, only, and in primary care) | Participants were children first presenting to ambulatory care settings 2 studies on acute sore throat: 1 RCT (n = 1,307) in primary care clinic, 1 retrospective record review (n = 176) in community health centre RCT in Poland and retrospective chart review in US | Intervention: Rapid antigen test for Strep A for sore throat Comparator: Usual care in RCT Period before implementation in retrospective record review | Patient outcomes (mortality, morbidity) Decision-making/clinical management decisions (hospital attendance, referral) Antibiotic prescribing Additional diagnostic testing Follow-up not reported |
Burstein et al. (2019)20 US No funding | Objective: Systematically identify, characterize, and evaluate the messaging approaches used in educational interventions to increase antibiotic awareness Study Designs: No limits; studies had to have been conducted in the US and had patient or public education component and formally evaluated program Databases: Pubmed, Google Scholar, Embase, CINAHL, Scopus Search Date: January 2016 Number of Studies: 34 studies in total (antibiotic use in a broad range of conditions and settings) 1 controlled before-after study relevant for this report (specifically evaluated intervention for URTI) | Setting in 1 relevant study described as “rural community” in US Authors noted that all interventions in SR targeted adults Specific characteristics of population not described | Intervention: In 1 relevant study, intervention was office-based informational brochures, media campaign about antibiotic resistance for patients, as well as small group sessions overviewing antibiotic resistance and appropriate antibiotic use plus algorithms for providers implemented in one community in the state of Utah Comparator: Communities in the state not receiving intervention | Appropriateness of antibiotic prescriptions, adherence to recommended treatment, drug resistance patterns, health care utilization Follow-up not reported |
Health Information and Quality Authority (2019)19 Ireland Funding not reported; however, report released by Health Information and Quality Authority in Ireland | Objective: Determine whether use of CRP POCT for acute RTIs in primary care leads to a significant reduction in antibiotic prescribing without compromising patient safety Study Designs: RCTs, cluster RCTs, non-randomized studies, observational studies Databases: MEDLINE, Embase, CINAHL, Cochrane Library Search Date: April 2018 Number of Studies: 13 studies in total (on any RTI) 5 studies relevant to this report (URTI specifically): 1 before-after study, 1 cross-sectional study, 1 observational study; 2 RCTs reporting on RTIs in general that reported subgroup of patients with URTI | 1 study in patients of all ages (acute sinusitis, tonsilitis, otitis media) (n = 367 GPs; number of patients NR) 1 study in adult patients, only (acute cough or sore throat; n = 120) 1 study did not report age criteria (acute rhinosinusitis; n = 560) 1 study in adult patients (RTI in general but report URTI separately; n= 4,264 but number of patients with URTI specifically unclear) 1 study in adult patients (LRTI and rhinosinusitis; both reported separately; n = 258; number with rhinosinusitis unclear) Studies conducted in Ireland; Belgium, Spain, Poland, UK, Netherlands; Spain; Netherlands; Denmark | Intervention: CRP POCT (with or without communication training, education, other biomarkers) Comparator: Standard care alone | Antibiotic prescriptions at index and 28 days Substantial improvement or complete recovery at 7 and 28 days Mortality at 28 days Time to resolution of symptoms Complications resulting in reconsultation ADRs Hospitalizations Patient satisfaction Physician satisfaction QoL |
Deniz et al. (2018)16 Netherlands Funded by Netherlands Organisation for Health Research and Development | Objective: Review the effects of guidelines on the prescription of antibiotics and analgesics for children with AOM Study Designs: No limits; studies had to evaluate effects of introducing national AOM practice guidelines on antibiotic use Databases: PubMed, Embase, Cochrane Library Search Date: June 2017 Number of Studies: 7 studies in total (in either primary care or secondary care) 3 studies relevant to this report (conducted in primary care); all studies were observational longitudinal studies and evaluated antibiotic prescribing before and after guideline introduction | 1 study of children aged 1 to 12 years 1 study of children aged 3 months to 15 years 1 study of children aged 2 to 15 years Studies conducted in Sweden, UK, Spain | Intervention: Guideline recommendations (“wait-and-see” in 2 guidelines, and antibiotic recommendation in 1 guideline) Comparator: Pre-guideline introduction | Antibiotic prescription rates Follow-up not reported |
Kochling et al. (2018)17 Germany No funding | Objective: Summarize evidence on the effectiveness of interventions in primary care to reduce antibiotic prescriptions in patients ≥ 13 years for acute RTI Study Designs: RCTs Databases: MEDLINE, Cochrane Library Search Date: August 2016 Number of Studies: 17 studies in total (on any RTI) 3 studies relevant for this report (report on URTI, only) | 1 RCT in patients aged 14 to 60 years with acute pharyngitis 1 RCT in patients ≥ 21 years presenting with runny nose, blocked nose, cough, or sore throat for 7 days or less 1 RCT in patients > 16 years with first episode of acute cough (no cough in previous 8 weeks) RCTs conducted in Germany, Singapore, Spain | Intervention: 1 study rapid antigen Strep A test 1 study communicating training for physicians, handouts for patients, and waiting room poster 1 study of patient education on causes of URTIs Comparator: 2 studies = usual care 1 study = education on influenza vaccination (control education) | Antibiotic prescription rate Reconsultation rate Days to recovery from RTI Rate of inappropriate antibiotic prescriptions Follow-up not reported |
Lane et al. (2018)15 UK Funded by National Institute for Health Research School for Primary Care Research, UK | Objective: Determine whether locally relevant, real-time syndromic or microbiological infection epidemiology can improve prescribing by reducing diagnostic uncertainty Study Designs: No limits; studies had to involve dissemination of information to primary care clinicians that was locally relevant and in real time related to common infections Databases: MEDLINE, Embase, Web of Science, CINAHL, grey literature Search Date: April 2016 Number of Studies: 3 studies (1 cluster RCT, 1 cohort with historical control, 1 retrospective cohort) | 1 study in family practice residents (n = 14) 1 study in 69 physicians in 26 practices — intervention comprised 7,789 patient visits and compared to pre-intervention period (20,512 visits) 1 study in 27 GP practices Authors did not report details of patients Studies conducted in US | Intervention Educational and surveillance program in 1 study Heavy media coverage, regular updates to physicians, epidemiological data in 1 study Syndromic heat map from EMR data provided to GPs with POC clinical decision support tool in 1 study Comparator Pre-intervention period, control group (not further described) | Antibiotic prescription rates Referral rates Harms of intervention Adherence to guidelines Follow-up not reported |
McDonagh et al. (2018)23 US Funded by the Agency for Healthcare Research and Quality | Objective: Summarize a large, complex, comparative effectiveness review of the evidence of effectiveness of all potential interventions designed to reduce inappropriate antibiotic use for acute RTIs, while not causing adverse consequences (updates a 2016 AHRQ CER) Study Designs: RCTs and comparative observational studies Databases: MEDLINE and Cochrane Library Search Date: January 2018 Number of Studies: 96 studies in total (on any RTI and mixture of primary care settings: GP, emergency departments, hospital outpatient clinics); not possible to judge which primary studies relevant for report 21 studies on AOM 32 studies on sore throat, pharyngitis, or tonsilitis 7 studies on rhinitis 22 studies on sinusitis 16 studies on cough and common cold | Studies took place in outpatient setting (mixture of GP, emergency departments, hospital) but results not reported or summarized based on setting or type of infection Population characteristics not reported based on type of RTI or setting 28 studies (30%) population of interest was adults 68 studies (71%) in children or children and adults 34 (35%) of studies in US | Intervention Interventions targeting patient, clinician, both, and those with specific age group or diagnosis Interventions targeted population or individuals and had different durations, frequencies, and intensity Authors grouped in patient or caregiver interventions, clinician interventions; further classified as educational/behavioural interventions, strategies to improve communication, clinical strategies (prediction rules, POCTs), system-level strategies (reminders, audit and feedback, financial or regulatory incentives, antimicrobial stewardship programs), multi-faceted approaches Comparator Standard care (no strategy of improving appropriate use of antibiotics) | Grouped evidence into following categories:
Follow-up not reported |
Schuetz et al. (2017)18 Switzerland Supported by National Institute for Health Research, via Cochrane Infrastructure and Cochrane Programme Grants funding | Objective: “Assess the safety and efficacy of using procalcitonin for starting or stopping antibiotics over a large range of patients with varying severity of ARIs and from different clinical settings” Study Designs: RCTs Databases: MEDLINE, Embase, CENTRAL, Cochrane Library Search Date: February 2017 Number of Studies: 32 studies in total (in any RTI and mixture of settings: primary care, medical wards ICU, ED) 2 studies relevant for this report (on URTI, only, and in primary care) Outcome data came from Odermatt et al. (2018),36 which was an individual patient data meta-analysis conducted using the 2 relevant studies from the SR conducted by Schuetz et al. (2017)18 | One RCT (n = 458) in Switzerland among people (mean age 39.5 years) with upper or lower ARIs in primary care (data available for URTI, only) One RCT (n = 571) in Germany (mean age 40 years) among adults with upper or lower ARIs in primary care (data available for URTI, only) N = 644 with URTI from both trials included for meta-analysis | Intervention: Guiding antibiotic decisions with repeated PCT measurements in one RCT (PCT < 0.1 μg/L, bacterial infection considered highly unlikely and antibiotics discouraged; PCT > 0.25 μg/L, bacterial infection considered likely and antibiotics recommended. For PCT 0.1 to 0.25 μg/ L, bacterial infection considered unlikely and antibiotics not recommended. When antibiotics withheld, a second measurement of PCT was taken within 6 to 24 hours. Antibiotics recommended if second measurement was > 0.25 μg/L or if the PCT level had increased from the first measurement by > 50% and the participant showed no clinical improvement Guiding antibiotic decisions with a single measurement only in the other RCT (based on PCT< 0.25 μg/L) Comparator: Standard care | All-cause mortality at 30 days Treatment failure within 28 days (symptoms of ongoing or relapsing infection at 28 days) Antibiotic use Number of days with restricted activities Antibiotic-related side effects |
ADR = adverse drug reaction; AOM = acute otitis media; ARI = acute respiratory infection: CBA = controlled before-after studies; CDSS = clinical decision support system; CER = comparative effectiveness research; CRP = C-reactive protein; DARE = Database of Abstracts of Reviews of Effects; ED = emergency department; EMR = electronic medical record; GP = general practitioner/practice; HTA = health technology assessment; ICU = intensive care unit; ITS = interrupted time series; LRTI = lower respiratory tract infection; NR = not reported; PCT = procalcitonin; POC = point of care; POCT = point-of-care test(ing); QoL = quality of life; RCT = randomized controlled trial; RTI = respiratory tract infection; SR = systematic review; Strep A = group A Streptococcus; URTI = upper respiratory tract infection.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews on Delayed Antibiotics Using AMSTAR 212
Item | Mortazhejri et al. (2020)14 | Spurling et al. (2017)13 |
1. Did the research questions and inclusion criteria for the review include the components of PICO? | •• | •• |
2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | •• | •• |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | X | •• |
4. Did the review authors use a comprehensive literature search strategy? | • | • |
5. Did the review authors perform study selection in duplicate? | •• | •• |
6. Did the review authors perform data extraction in duplicate? | •• | •• |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | •• | •• |
8. Did the review authors describe the included studies in adequate detail? | •• | •• |
9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | •• | •• |
10. Did the review authors report on the sources of funding for the studies included in the review? | •• | •• |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | •• | •• |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | X | •• |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | •• | •• |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | •• | •• |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | X | •• |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | •• | •• |
•• = Yes; • = Partial Yes; X = No; AMSTAR = A MeaSurement Tool to Assess systematic Reviews; PICO = patient, intervention, comparison, outcome; RoB = risk of bias.
Table 5: Strengths and Limitations of Systematic Reviews on Family Medicine Interventions Using AMSTAR 212
Item | Carvalho et al. (2020)21 | Cohen et al. (2020)22 | Fraser et al. (2020)25 | Mortazhejri et al. (2020)14 | Van Hecke et al. (2020)24 | Burstein et al. (2019)20 | Health Information and Quality Authority et al. (2019)19 | Deniz et al. (2018)16 | Kochling et al. (2018)17 | Lane et al. (2018)15 | McDonagh et al. (2018)23 | |
1. Did the research questions and inclusion criteria for the review include the components of PICO? | X | •• | •• | •• | •• | X | •• | •• | X | • | •• | •• |
2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | •• | •• | •• | •• | •• | X | X | •• | X | •• | •• | •• |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | X | X | X | X | •• | X | X | X | X | X | X | X |
4. Did the review authors use a comprehensive literature search strategy? | • | • | •• | • | • | • | • | • | X | • | • | • |
5. Did the review authors perform study selection in duplicate? | •• | •• | •• | •• | •• | •• | •• | •• | •• | X | X | •• |
6. Did the review authors perform data extraction in duplicate? | •• | •• | X | •• | X | •• | •• | •• | •• | •• | X | •• |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | X | •• | •• | •• | X | X | X | X | X | X | X | •• |
8. Did the review authors describe the included studies in adequate detail? | • | • | •• | •• | • | X | •• | •• | •• | •• | •• | •• |
9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | X | •• | • | •• | X | X | •• | •• | •• | •• | •• | •• |
10. Did the review authors report on the sources of funding for the studies included in the review? | X | •• | •• | •• | X | X | •• | X | X | X | X | •• |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | N/A | •• | •• | •• | X | N/A | •• | N/A | N/A | N/A | N/A | •• |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | N/A | •• | X | X | X | N/A | X | N/A | N/A | N/A | N/A | X |
13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | X | •• | •• | •• | X | X | •• | X | •• | X | •• | •• |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | X | X | •• | •• | X | X | •• | X | •• | X | •• | X |
15. If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | N/A | X | X | X | X | N/A | •• | N/A | N/A | N/A | N/A | •• |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | •• | •• | •• | •• | •• | •• | •• | •• | •• | •• | •• | •• |
•• = Yes; • = Partial Yes; X = No; AMSTAR = A MeaSurement Tool to Assess systematic Reviews; N/A = Not applicable; PICO = patient, intervention, comparison, outcome; RoB = risk of bias.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Findings of Included Systematic Reviews on Delayed Antibiotic Prescribing
Systematic Review | Measurement of outcome, intervention and comparator | Findings | Authors’ conclusions |
Antibiotic use | |||
Mortazhejri et al. (2020)14 | Delayed prescription versus immediate prescription (meta-analysis of 6 RCTs involving n = 1,788 participants) | Participants in delayed antibiotic group less likely to use antibiotics versus those in immediate prescription group (OR 0.09; 95% CI, 0.03 to 0.23) | “Our meta-analysis revealed that almost all studies with delayed prescription significantly reduced use of antibiotics for URTIs. Our subgroup analysis showed that the prescriptions that were given at a later time and the prescriptions that were given at the index consultation had similar effects in reducing antibiotic use in patients.” (p. 13) |
Subgroup analysis exploring timing of prescription: (1) prescription given at the time of the visit with instructions to wait for a few days before filling it (delayed patient-led and post-dated); (2) prescription not given at the time of the visit and patients were asked to return to collect the prescription after a few days (delayed collection) | Participants less likely to use antibiotics versus immediate prescription (OR 0.15; 95% CI, 0.03 to 0.72); after removing 1 study, which was a source of heterogeneity in sensitivity analysis: OR 0.08 (95% CI, 0.04 to 0.14) Participants less likely to use antibiotics for delayed collection versus immediate prescription (OR 0.05; 95% CI, 0.03 to 0.06) | ||
Spurling et al. (2017)13 (Not possible to report results of meta-analysis due to inclusion of non-eligible studies) | Delayed (prescription at time of visit) versus immediate antibiotics | 32/67 vs 55/67 (OR 0.20; 95% CI, 0.09 to 0.44) in 1 study 32/98 vs 46/50 (OR 0.04; 95% CI, 0.01 to 0.13) in 1 study | “Delayed and no antibiotic strategies markedly reduced the use of antibiotics for RTIs compared to immediate antibiotics.” (p. 17) “The number needed to treat to prevent one antibiotic prescription using the delay strategy was 1.6 compared to immediate antibiotics.” (p. 17) [conclusions based on meta-analysis which included non-eligible studies] “Delayed antibiotics for people with acute respiratory infection reduced antibiotic use compared to immediate antibiotics, but was not shown to be different to no antibiotics in terms of symptom control and disease complications. Where clinicians feel it is safe not to prescribe antibiotics immediately for people with respiratory infections, no antibiotics with advice to return if symptoms do not resolve is likely to result in the least antibiotic use while maintaining similar patient satisfaction and clinical outcomes to delaying prescription of antibiotics. Where clinicians are not confident in using a no antibiotic strategy, a delayed antibiotics strategy may be an acceptable compromise in place of immediate prescribing to significantly reduce unnecessary antibiotic use for RTIs, and thereby reduce antibiotic resistance, while maintaining patient safety and satisfaction levels.” (p. 2) |
Delayed prescription collection versus immediate antibiotics | 23/100 vs 46/51 (OR 0.03; 95% CI, 0.01 to 0.09) in 1 study 43/95 vs 92/92 (OR 0.00; 95% CI, 0.00 to 0.07) in 1 study 55/176 vs 210/211 (OR 0.00; 95% CI, 0.00 to 0.02) in 1 study 36/150 vs 132/151 (OR 0.05; 95% CI, 0.02 to 0.08) in 1 study | ||
Delayed (prescription at time of visit) versus no antibiotics | 32/98 vs. 6/49 (OR 3.47; 95% CI, 1.34 to 9.01) in 1 study | “The least antibiotic use was in the no antibiotic group, followed by delayed and then immediate antibiotic groups.” (p. 17) | |
Delayed prescription collection versus no antibiotics | 23/100 vs. 6/49 (OR 2.14; 95% CI, 0.81 to 5.66) 55/176 vs. 23/184 (OR 3.18; 95% CI, 1.85 to 5.46) | ||
Patient satisfaction | |||
Mortazhejri et al. (2020)14 | Satisfaction with the consultation or satisfaction with the treatment approach | Delayed 96% vs. 94% in immediate in 1 study (OR 1.47; 95% CI, 0.32 to 6.85) Delayed 93% vs. 96% in immediate in one study (OR 0.61; 95% CI, 0.25 to 1.49) Delayed 77% vs. 91% in immediate in 1 study (OR 0.32; 95% CI, 0.16 to 0.65) No difference between different variants of delayed prescriptions in 1 study P value for difference in satisfaction was 0.14 in another study (no further data reported) | “…two studies from the UK reported less satisfaction in the intervention group compared to the control group, though the results were statistically significant in only one study. One study from New Zealand reported higher satisfaction (though this was not statistically significant) in the intervention group. In the Little et al. study from the UK, there was no significant difference in satisfaction between different variants of delayed prescription. Poza Abad et al. from Spain reported no significant difference in satisfaction between delayed collection, delayed patient-led, and immediate prescription groups.” (p. 11) |
Spurling et al. (2017)13 (Not possible to report results of meta-analysis due to inclusion of non-eligible studies) | Number of participants satisfied for delayed versus immediate antibiotics | 64/67 vs. 58/62 (OR 1.47; 95% CI, 0.32 to 6.85) in 1 study 170/198 vs. 83/101 (OR 1.32; 95% CI, 0.69 to 2.52) in 1 study 71/73 vs. 75/75 (OR 0.19; 95% CI, 0.01 to 4.01) in 1 study 165/177 vs. 202/211 (OR 0.61; 95% CI, 0.25 to 1.49) in 1 study 115/150 vs. 123/135 (OR 0.32; 95% CI, 0.16 to 0.65) in 1 study | “Delaying prescribing did not result in significantly different levels of patient satisfaction compared with immediate provision of antibiotics” (p. 2) “Patient satisfaction was highest in the immediate antibiotic group, with 91% being moderately satisfied, very satisfied, or extremely satisfied with the consultation. The delayed antibiotic group was more satisfied (87%) than the no antibiotic group (83%). These high satisfaction results may reflect patient involvement in studies, where treating physicians were more thorough in their explanations than usual (Hawthorne effect).” (p. 17) |
Spurling et al. (2017)13 (Not possible to report results of meta-analysis because of inclusion of non-eligible studies) | Number of participants satisfied for delayed vs. no antibiotics | 170/198 vs. 78/99 (OR 1.63; 95% CI, 0.87 to 3.06) in 1 study 165/177 vs. 166/184 (OR 1.49; 95% CI, 0.70 to 3.19) in 1 study | |
Reconsultation | |||
Mortazhejri et al. (2020)14 | Within 1 month of consultation in one study Other studies reported intention to re-consult in future | No difference in reconsultation rate within 1 month (P=0.56) Intention to re-consult Delayed 73% vs. immediate 65% (OR 1.50, 95% CI 0.71 to 3.17) in one study Delayed 57% vs. immediate 79% in another study (OR 0.35, 95% CI 0.22 to 0.55) Delayed 63% vs. immediate 83% (OR 0.35, 95% CI 0.20 to 0.62) in one study Delayed 69% vs. immediate 86% (OR 0.62, 95% CI 0.19 to 2.06) | “Two studies from the UK and one study from Spain reported less intention to re-consult in the intervention groups; however, the results were statistically significant only in two studies. One study from New Zealand reported greater intention to re-consult in the intervention group though this was not statistically significant. In the Little et al. study (from the UK), there was no significant difference in reconsultation between different variants of delayed prescription.” (p. 13) |
Pain | |||
Spurling et al. (2017)13 (Not possible to report results of meta-analysis because of inclusion of non-eligible studies) | Number of participants with pain on days 3 to 6 for delayed vs. immediate antibiotics | 13/61 in delayed group vs. 9/58 in immediate (OR 1.47; 95% CI, 0.58 to 3.77) in 1 study 28/111 in delayed group vs. 15/101 in immediate (OR 1.93; 95% CI, 0.96 to 3.88) in 1 study | “Results for clinical outcomes were often heterogeneous. For most outcomes there was no evidence of difference between delayed antibiotics and both immediate and no antibiotic prescribing strategies.” (p. 17) “Symptoms for acute otitis media and sore throat were modestly improved by immediate antibiotics compared with delayed antibiotics.” (p. 2) “All strategies appear to have similar safety with no advantage for delayed antibiotics over either no antibiotics or immediate antibiotics for disease complications.” (p. 17) “There were no differences in complication rates.” (p.2) |
Pain severity on day 3 for delayed versus immediate antibiotics | SMD 0.41 (95% CI, 0.13 to 0.68) in 1 study | ||
Malaise | |||
Spurling et al. (2017)13 (Not possible to report results of meta-analysis because of inclusion of non-eligible studies) | Number of participants with malaise on day 3 for delayed vs. immediate antibiotics | 45/150 delayed vs. 19/135 for immediate (OR 2.62, 95% CI, 1.44 to 4.76) in 1 study | “For many clinical outcomes, there were no differences between prescribing strategies. Symptoms for acute otitis media and sore throat were modestly improved by immediate antibiotics compared with delayed antibiotics.” “However, both studies [including one relevant for report] found in favour of immediate antibiotics. One study included participants with otitis media.” (p. 15) |
Malaise severity on day 3 for delayed vs. immediate antibiotics | SMD 0.31 (95% CI, 0.07 to 0.54) in 1 study | ||
Fever | |||
Spurling et al. (2017)13 (Not possible to report results of meta-analysis because of inclusion of non-eligible studies) | Number of participants with fever on days 3 to 6 for delayed vs. immediate antibiotics | 5/67 in delayed vs. 6/62 in immediate (OR 0.75; 95% CI, 0.22 to 2.60) in 1 study | “There was no evidence of differences in the number of participants with fever on Days 3 to 6 (participants presented with the common cold and otitis media).” (p. 17) |
Fever severity on day 3 for delayed vs. immediate antibiotics | SMD –0.24 (95% CI, –0.48 to –0.00) in 1 study | ||
Adverse effects of antibiotics | |||
Spurling et al. (2017)13 (Not possible to report results of meta-analysis because of inclusion of non-eligible studies) | Vomiting for delayed vs. immediate antibiotics | 15/179 vs. 18/215 (OR 1.00; 95% CI, 0.49 to 2.05) in 1 study | Not commented on specifically; authors noted heterogeneity in results which “may be due to differences in antibiotic prescribing recommendations for different RTIs.” (p. 16) |
Diarrhea for delayed vs. immediate antibiotics | 11/67 vs. 12/62 (OR 0.82;95% CI 0.33, to 2.02) in 1 study 23/179 vs. 23/215 (OR 1.23; 95% CI, 0.67 to 2.28) in 1 study 14/150 vs. 25/135 (OR 0.45; 95% CI, 0.22 to 0.91) in 1 study | ||
Rash for delayed vs. immediate antibiotics | 11/180 vs. 14/215 (OR 0.93; 95% CI, 0.41 to 2.11) in 1 study 8/150 vs. 6/135 (OR 1.21; 95% CI, 0.41 to 3.58) in 1 study | ||
CI = confidence interval; OR = odds ratio; RCT = randomized controlled trial; SMD = standardized mean difference; URTI = upper respiratory tract infection; vs. = versus.
Note: Outcomes are described as delayed antibiotic intervention versus comparator (immediate or no antibiotic) in all cases.
Table 7: Summary of Findings Included Systematic Reviews on Family Medicine Interventions
Systematic review and topic | Description of outcome | Findings | Authors’ conclusions |
Antibiotic use | |||
Carvalho et al. (2020)21 (E-health interventions) | Prescription reduction in year after introduction of best practice alert compared to year before best practice alert | Prescriptions for antibiotics at sinusitis visits reduced from 86.3% to 61.7% (P <0.01) in1 study | From primary study abstract: “Clinical reminders within the EHR can be an effective tool to reduce inappropriate antibiotic use and improve providers’ decisions regarding the correct antibiotic choices for patients with acute sinusitis”37 |
Mortazhejri et al. (2020)14 (Interventions directed at patients and the public) | Antibiotic prescriptions in intervention vs. control group | No difference in antibiotic use between education pamphlet and video vs. control in number of antibiotics per patient (mean difference ‒0.3, P = 0.23) in 1 study No difference in antibiotic prescriptions for pamphlet versus control (OR 1.20; 95% CI, 0.84 to 1.72) Reduced odds of receiving antibiotic prescription at index consultation for booklets on RTI aimed at parents of children compared to control (OR 0.29; 95% CI, 0.14 to 0.60) No difference in antibiotic prescriptions between intervention (interactive website) and control (RR 1.02; 95% CI, 0.82 to 1.43) | “The effect of interventions in the information and education group varied highly among different types of educational materials.” (p. 13) |
Cohen et al. (2020)22 (rapid tests for sore throat) (Not possible to report on meta-analysis for all results as some include non-eligible studies) | Number of participants provided with an antibiotic prescription for rapid tests (+/- scoring system) vs. clinical grounds (+/- scoring system) | 86/213 vs. 124/211 (RD –0.18; 95% CI, –0.28 to –0.09) in 1 study 167/367 vs. 263/385 (RD –0.23; 95% CI, –0.30 to –0.16) in 1 study 98/223 vs. 133/208 (RD –0.20; 95% CI, –0.29 to –0.11) in 1 study 63/196 vs. 155/274 (RD –0.24; 95% CI, –0.33 to –0.16) in 1 study | “Rapid testing to guide antibiotic treatment for sore throat in primary care probably reduces antibiotic prescription rates by 25% (absolute risk difference), but may have little or no impact on antibiotic dispensing. More studies are needed to assess the efficacy and safety of rapid test-guided antibiotic prescribing, notably to evaluate patient-centred outcomes and variability across subgroups (e.g. adults versus children).” (p. 2) |
Number of participants with an antibiotic dispensed for rapid tests (+/- scoring system) vs. clinical grounds (+/- scoring system) (meta-analysis of 2 studies) | 156/445 vs. 197/455 (RD –0.07; 95% CI, –0.17 to –0.02) | ||
Number of participants provided with an antibiotic prescription for rapid tests alone vs. clinical grounds + scoring system | 28/106 vs. 83/150 (RD –0.29; 95% CI, –0.40 to –0.17) in 1 study | ||
Number of participants provided with an antibiotic prescription for rapid tests alone vs. clinical grounds without scoring system | 28/106 vs. 72/124 (RD –0.32; 95% CI, –0.44 to –0.20) in 1 study | ||
Number of participants provided with an antibiotic prescription for rapid tests + scoring system vs. clinical grounds + scoring system Meta-analysis from 2 studies | 287/670 vs. 470/476 (RD –0.21; 95% CI, –0.26 to –0.16) | ||
Number of participants with an antibiotic dispensed for rapid tests + scoring system vs. clinical grounds + scoring system Meta-analysis of 2 studies | 156/445 vs. 197/455 (RD –0.07; 95% CI, –0.17 to 0.02) | ||
Number of participants provided with an antibiotic prescription for rapid tests + scoring system vs. clinical grounds alone | 34/90 vs. 72/124 (RD –0.20; 95% CI, –0.34 to –0.07) | ||
Fraser et al. (2020)25 (Rapid tests for sore throat); reports same 3 RCTs as Cohen et al.22 | Number participants provided with an antibiotic prescription for rapid Strep A test plus clinical score (FeverPAIN) vs. clinical score alone | 38/213 (18%) immediate and 48/213 (23%) delayed vs. 33/211 (16%) immediate and 87/211 (41%) in 1 study | “There were three RCTs that reported on antibiotic use. All three trials found higher antibiotic prescription rates or use in control arms with no POCT than this with a point-of-care test” (p. 111) |
Number of participants given antibiotics for rapid Strep A test plus clinical criteria (Centor) vs. clinical criteria alone (Centor) | 123/281 (44%) vs. 168/262 (64%) in 1 study | ||
Number of participants who received antibiotics for decision rule (modified Centor) plus rapid test vs. rapid test alone vs. decision rule alone vs. usual care | 39/102 (38%) vs. 32/120 (27%) vs. 94/170 (55%) vs. 82/141 (58%) | ||
Van Hecke et al. (2020)24 (POCT for sore throat) | Immediate antibiotic prescribing for POCT in sore throat versus control | POCT vs. usual care 261/581 vs. 364/726 (RR 0.90; 95% CI, 0.80 to 1.01) in 1 RCT POCT vs. pre-implementation of POCT 34/68 vs. 65/108 (RR 0.48; 95% CI, 0.33 to 0.69) in 1 study | “Strep A POCT did not reduce immediate antibiotic prescribing in RCTs but did show an effect in non-randomized studies.” (p. 20) |
Burstein et al. (2019)20 (Communication interventions) | URTIs treated with an antibiotic for community receiving a multi-faceted intervention (office-based informational brochures and media campaign about antibiotic resistance for patients, plus small group sessions and printed algorithms for providers) compared to communities not receiving intervention | Compared to baseline, proportion of URTIs treated with antibiotics fell by 16% for intervention group vs. 2% for control group (P < 0.006) in 1 study | From abstract of primary study: “A multifaceted intervention involving the repetitive use of printed algorithms resulted in modest improvements in antibiotic prescribing for outpatient URTIs.”38 |
Health Information and Quality Authority (2019)19 (CRP POCT) | Antibiotic prescribing at index consultation for CRP testing vs. usual care (meta-analysis of 2 RCTs) | 80/260 vs. 109/250 (RR 0.72; 95% CI, 0.58 to 0.90) | “Overall, the pooled [estimates] shows a significant reduction in antibiotic prescribing between the CRP POCT group and the usual care group” (p. 75) “Overall, our results suggest that C-reactive protein POCT, when used to guide management of patients who present with symptoms of acute RTI, leads to reduced antibiotic prescribing both at index consultation” (p. 81) |
Antibiotic prescribing at index consultation for CRP testing vs. usual care (meta-analysis of 2 non-randomized studies) | 183/335 vs. 287/345 (RR 0.65; 95% CI, 0.59 to 0.73) | ||
Difference in antibiotic prescribing between CRP POCT group and usual care group | Reduced odds of antibiotic prescribing in CRP group (OR 0.43; 95% CI, 0.33 to 0.58) | ||
Deniz et al. (2018)16 (Guidelines for AOM) | Antibiotic prescription rates after introduction of guidelines compared to before | Antibiotic prescription rates fell by 12% in 1 study and there was no change in 1 study | “The introduction of national AOM clinical practice guidelines seems to have at best a modest impact on antibiotics and analgesics prescription rates for childhood AOM” (p. 601; based on studies in both primary and secondary care) |
Kochling et al. (2018)17 (Primary care interventions in general; did not meta-analyze) | Antibiotic prescriptions for intervention (communication training for physicians, waiting room poster, and handouts for patients) vs. usual care | OR for the prescription of an antibiotic dropped to 0.58 (95% CI, 0.43 to 0.78) after 6 weeks in intervention group vs. increasing to 1.52 (95% CI, 1.19 to 1.95) in usual care group OR was 0.72 (95% CI, 0.54 to 0.97) at 12 months in the intervention group and 1.31 (95% CI, 1.01 to 1.71) in usual care group These ORs correspond to a 60% relative reduction in antibiotic prescription rates at 6 weeks and a persistent 40% relative reduction at 12 months | “Despite a large difference in baseline prescription rates and increased Abx prescription rates in the intervention group (+ 0.3%) and control group (+ 10.1%) within 1 year after baseline, this trial reported statistically relevant reductions after adjusting for seasonal effects and confounding variables such as severity of disease (intervention group: adjusted OR = 0.72, 95% CI 0.54–0.97, p = 0.028; control group: adjusted OR = 1.31, 95% CI 1.01–1.71, p = 0.044). This reduction does not satisfy our conditions for a meaningful change (difference in differences − 9.8%).” (p. 22) |
Prescribed antibiotics for intervention (RADT for Strep A) vs. usual care | 123/281 (44%) vs. 168/262 (64%) RD= –20% | “Llor et al. implemented a more effective intervention: After initial consultation, the Abx prescription rate was 44% in the IG (p < 0.001) as compared to 64% in the CG due to RADTs.” (p. 17) | |
Prescribed antibiotics for intervention (patient education on causes of URTI) vs. control (patient education influenza vaccination) | 94/457 (21%) vs. 81/457 (18%) RD = 3% | “Hui Min Lee et al. did not find significantly reduced Abx prescriptions by means of patient education on causes of upper RTIs compared to CG (20.6 vs. 17.7% in the CG, OR = 1.20, p = 0.313).” (p. 16) | |
Lane et al. (2018)15 (Locally relevant real-time infection epidemiological data) | Antibiotic-prescribing rates after 3-year surveillance program compared to before | 8.6% vs. 26.4% (P = 0.01) in 1 study | “This review demonstrates the wide variety of surveillance systems and data sources that could support primary care antimicrobial decision-making. We found few had been evaluated, but those that had shown promising, albeit methodologically weak, evidence that providing locally relevant, real-time epidemiological information improved antimicrobial prescribing in primary care.” (p. 545-6) |
Antibiotic-prescribing rates during pandemic period (where prescribers received epidemiological data and updates) vs. non-pandemic period as a control | 3,054/7,789 visits (39%) in pandemic period vs. 9,741/2,0512 visits (48%) in non-pandemic period (OR 0.72; 95% CI, 0.68 to 0.77) | ||
Antibiotic-prescribing rates for GPs receiving heat map and decision support tool versus control arm | 41% for intervention vs. 41% for control (P = 0.90) | ||
Schuetz et al. (2017)18 (procalcitonin) (Includes data from Odermatt et al. 2018)36 | Initiation of antibiotic therapy in procalcitonin-guided therapy group versus control group (meta-analysis of 2 studies) | 59/332 (18%) vs. 159/312 (51%) (OR 0.2; 95% CI, 0.1 to 0.3) | “Procalcitonin guided antibiotic therapy in the primary care setting was associated with reduced antibiotic exposure in URTI patients without compromising outcomes.” (p. 171) |
Total antibiotic exposure in days (mean, SD) in procalcitonin-guided therapy group vs. control group (meta-analysis of 2 studies) | 1.2 days (2.8) vs. 3.7 days (4.0) | ||
Guideline adherence | |||
Carvalho et al. (2020)21 (E-health interventions) | Adherence with guidelines among providers receiving intervention (didactic teaching, antibiotic guidelines, and CDSS integrated into EHR) compared to historical control | 91% for intervention group vs. 77% for control in 1study | From primary study abstract: “Our low-cost interventions led to a significant improvement in ARI treatment guideline adherence.”39 |
Inappropriate antibiotic prescriptions | |||
Fraser et al. (2020)25 (rapid tests for sore throat) | Antibiotic appropriateness in acute sore throat for RADT plus scoring system compared to clinical criteria only | From 1 primary study: “Ninety-eight per cent (59/60) of patients with a positive RADT result were given antibiotics and 31% (69/225) of those with a negative test result received antibiotics. The authors determined that treatment was inappropriate (based on culture results) in 43% of patients (226/526), with 210 unnecessary prescriptions and 16 untreated cases. A total of 153 of these cases occurred in the control arm and 73 were in the RADT arm; however, the category of inappropriate decision (overprescribing or underprescribing) is not reported by trial arm.” (p. 82) | Not commented on specifically |
Recovery | |||
Health Information and Quality Authority (2019)19 (CRP POCT) | Proportion with substantial improvement or complete recovery at day 7 for CRP group vs. usual care | 27/118 vs. 31/125 (RR 1.03; 95% CI, 0.89 to 1.18) in 1 study | Not commented on specifically |
Time to resolution of symptoms | |||
Health Information and Quality Authority (2019)19 (CRP POCT) | Median time to symptom resolution in CRP group vs. usual care | 14 days (IQR 10 to 28) vs. 14 days (IQR 7 to > 28) in 1 study 5 days (IQR 3 to 7) vs. 4 days (IQR 3 to 8) in 1 study | “…no attempt was made to pool these data as the definition of resolution of symptoms differed between studies. All of the studies reported no significant difference in the time to resolution of symptoms between the CRP POCT and usual care groups” (p. 77) |
Re-consulation | |||
Cohen et al. (2020)22 (Rapid tests for sore throat) | Number of participants in need of reconsultation for rapid tests (+/- scoring system) vs. clinical grounds (+/- scoring system) Meta-analysis of 2 studies | 59/571 vs. 51/590 (OR 1.12; 95% CI, 0.57 to 2.21) | Not commented on specifically |
Mortazhejri et al. (2020)14 (Interventions directed at patients and the public) | Reconsultation rate within 1 year after enrolment for online program vs. control (OR < 1 suggests less reconsultation) | Intervention 19% vs. control 19% (OR 0.93; 95% CI, 0.73 to 1.16) in 1 study | Not commented on specifically |
Intention to re-consult for interactive booklet vs. control | Intervention 55% vs. control 76% (OR 0.34; 95% CI, 0.20 to 0.57) in 1 study | ||
Van Hecke et al. (2020)24 (POCT for sore throat) | Reconsultation events for POCT in sore throat vs. usual care | Decreased subsequent visits for POCT vs. usual care (RR 4.70; 95% CI, 2.94 to 7.51) in 1 study | “One RCT found a statistically significant effect [of Strep A POCT test] on decreasing subsequent visits compared to usual care” (p. 20) |
Health Information and Quality Authority (2019)19 (CRP POCT) | Reconsultation rate in CRP group vs. usual care | 33/129 vs. 23/129 (RR 1.43; 95% CI, 0.89 to 2.30) in 1 study 165/894 vs. 149/812 (RR 1.01; 95% CI, 0.82 to 1.23) in 1 study | ”While the point estimates for reconsultation exceeded that of usual group in all but one study, this difference was not statistically significant in any study.” (p. 78) |
Patient satisfaction | |||
Mortazhejri et al. (2020)14 (Interventions directed at patients and the public) | Satisfaction with consultation for interactive booklet vs. control (OR < 1 suggests less satisfaction in intervention group) | Intervention 90% vs. control 94% (OR 0.64; 95% CI, 0.33 to 1.22) | Not commented on specifically |
Health Information and Quality Authority (2019)19 (CRP POCT) | Number of patients satisfied in CRP group vs. usual care | 90/118 vs. 79/125 (RR of non-event 0.64; 95% CI, 0.43 to 0.96) in 1 study | “Although in one study, Cals et al. 2010, patients were more often satisfied in the CRP POCT group than in the usual care group” (p. 79) |
Satisfaction with care in CRP group vs. usual care | RR 1.01; 95% CI, 0.86 to 1.16) in 1 study | “…there was no significant difference between the CRP POCT group and the control group” (p. 79) | |
Complication attributed to index infection | |||
Cohen et al. (2020)22 (Rapid tests for sore throat) (Not possible to report on meta-analysis results as it included non-eligible studies) | Number of participants with a complication attributed to the index infection for rapid tests (+/- scoring system) vs. clinical grounds (+/- scoring system) | 2/213 vs. 0/211 (OR 5.00; 95% CI, 0.24 to 105) in 1 study 0/223 vs. 0/208 in 1 study | Not commented on specifically |
Days with restricted activity | |||
Schuetz et al. (2017)18 (procalcitonin) | Median days with restricted activity for procalcitonin-guided care vs. control Mean days with restricted activity for procalcitonin-guided care vs. control | Median 8 (IQR 5 to 14) vs.8 (IQR 5 to 13) Mean 8.5 versus 8.3 (OR= 0.2; 95% CI, ‒0.4 to 0.9) | “…days with restricted activities did not differ between groups” (p. 172) |
Treatment failure at 28 days | |||
Schuetz et al. (2017)18 (procalcitonin) (Includes data from Odermatt et al. (2018)36 | Proportion with treatment failure at 28 days for procalcitonin-guided care versus control Meta-analysis of 2 RCTs (Treatment failure defined as symptoms of ongoing or relapsing infection at 28 days) | 110/132 (33%) vs. 106/132 (34%) (OR 1.0; 95% CI, 0.7 to 1.4) | “Overall, no difference in treatment failure defined as symptoms of ongoing or relapsing infection at 28 days was found between groups” (p. 172) |
AOM = acute otitis media; CDSS = clinical decision support systems; CRP = C-reactive protein; CI = confidence interval; EHR = electronic health record; GP = general practitioner; IQR = interquartile range; MD = mean difference; OR = odds ratio; POCT = point-of-care test; RADT = rapid antigen detection test; RCT = randomized controlled trial; RD = risk difference; RR = relative risk; SD = standard deviation; RTI = respiratory tract infection; Strep A = group A Streptoccoccus; URTI = upper respiratory tract infection; vs. = versus.
Note: Outcomes described as intervention versus comparator in all cases.
Appendix 5: Overlap Between Included Systematic Reviews
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews on Delayed Antibiotics
Primary study citation | Mortazhejri et al. (2020)14 | Spurling et al. (2017)13 |
Arroll et al. (2002)26 | Yes | Yes |
Dowell et al. (2001)40 | No | Yes |
Little et al. (1997)27 | Yes | Yes |
Little et al. (2001)28 | Yes | Yes |
Little et al. (2014)41 | Yes | No |
De la Poza Abad et al. (2016)29 | Yes | Yes |
Pshetizky et al. (2003)42 | Yes | No |
Worrall et al. (2010)43 | Yes | No |
Table 9: Overlap in Relevant Primary Studies Between Included Systematic Reviews on Family Medicine Interventions
Primary study citation | Carvalho et al. (2020)21 | Cohen et al. (2020)22 | Fraser et al. (2020)25 | Mortazhejri et al. (2020)14 | Van Hecke et al. (2020)24 | Burstein et al. (2019)20 | Health Information and Quality Authority (2019)19 | Deniz et al. 2018)16 | Kochling et al. (2018)17 | Lane et al. (2018)15 | Schuetz et al. (2017)18 |
Altiner et al. (2007)44 | No | No | No | No | No | No | No | No | Yes | No | No |
Bjerrum et al. (2004)45 | No | No | No | No | No | No | Yes | No | No | No | No |
Briel et al. (2021)46 | No | No | No | No | No | No | No | No | No | No | Yes |
Burkhardt et al. (2010)47 | No | No | No | No | No | No | No | No | No | No | Yes |
Cals et al. (2010)48 | No | No | No | No | No | No | Yes | No | No | No | No |
Francis et al. (2009)49 | No | No | No | Yes | No | No | No | No | No | No | No |
Ginzburg et al. (2018)37 | Yes | No | No | No | No | No | No | No | No | No | No |
Hebert et al. (2012)50 | No | No | No | No | No | No | No | No | No | Yes | No |
Hingorani et al. (2015)39 | Yes | No | No | No | No | No | No | No | No | No | No |
Hui Min Lee et al. (2017)51 | No | No | No | Yes | No | No | No | No | Yes | No | No |
Kavanagh et al. (2011)52 | No | No | No | No | No | No | Yes | No | No | No | No |
Little et al. ( 2013a)30 | No | Yes | Yes | No | No | No | No | No | No | No | No |
Little et al. (2013b)53 | No | No | No | No | No | No | Yes | No | No | No | No |
Little et al. (2016)54 | No | No | No | Yes | No | No | No | No | No | No | No |
Llor et al. (2011)31 | No | Yes | Yes | No | No | No | No | No | No | No | No |
Llor et al. (2012)33 | No | No | No | No | No | No | Yes | No | Yes | No | No |
Malecki et al. (2017)55 | No | No | No | No | Yes | No | No | No | No | No | No |
Meier et al. (1990)56 | No | No | No | No | Yes | No | No | No | No | No | No |
Rios et al. (2001)57 | No | No | No | No | No | No | No | Yes | No | No | No |
Rubin et al. (2005)38 | No | No | No | No | No | Yes | No | No | No | No | No |
Shah et al. (2021)58 | No | No | No | No | No | No | No | No | No | Yes | No |
Taylor et al. (2005)59 | No | No | No | Yes | No | No | No | No | No | No | No |
Temte et al. (1999)60 | No | No | No | No | No | No | No | No | No | Yes | No |
Thompson et al. (2008)61 | No | No | No | No | No | No | No | Yes | No | No | No |
Tystrup et al. (2016)62 | No | No | No | No | No | No | No | Yes | No | No | No |
Worrall et al. (2007)32 | No | Yes | Yes | No | No | No | No | No | No | No | No |
Appendix 6: Additional References
Relevant Systematic Reviews Published Between 2015 and 2017
1.Coxeter P, Del Mar B, McGregor L, Beller EM, Hoffmann TC. Interventions to facilitate shared decision making to address antibiotic use for acute respiratory infections in primary care. Cochrane Database Syst Rev. 2015;2015(11): CD010907. Medline
2.McDonagh M, Peterson K, Winthrop K, Cantor A, Holzhammer B, Buckley DI. Improving Antibiotic Prescribing for Uncomplicated Acute Respiratory Tract Infections. Rockville (MD): Agency for Healthcare Research and Quality; 2016: https://effectivehealthcare.ahrq.gov/products/antibiotics-respiratory-infection/research. Accessed 2021 Jan 21.
3.O'Sullivan JW, Harvey RT, Glasziou PP, McCullough A. Written information for patients (or parents of child patients) to reduce the use of antibiotics for acute upper respiratory tract infections in primary care. Cochrane Database Syst Rev. 2016;11:CD011360. Medline
4.Wallace E, Uijen MJ, Clyne B, Zarabzadeh A, Keogh C, Galvin R, et al. Impact analysis studies of clinical prediction rules relevant to primary care: a systematic review. BMJ Open. 2016;6(3):e009957. Medline
Systematic Reviews Excluded Because Study Population, Type of Infection, and Setting Were Unclear
5.Egilmezer E, Walker GJ, Bakthavathsalam P, et al. Systematic review of the impact of point-of-care testing for influenza on the outcomes of patients with acute respiratory tract infection. Rev Med Virol. 2018;28(5):e1995 Medline
6.Lee JJ, Verbakel JY, Goyder CR, et al. The clinical utility of point-of-care tests for influenza in ambulatory care: a systematic review and meta-analysis. Clin Infect Dis. 2019;69(1):24-33. Medline
7.Tonkin-Crine SK, Tan PS, van Hecke O, et al. Clinician-targeted interventions to influence antibiotic prescribing behaviour for acute respiratory infections in primary care: an overview of systematic reviews. Cochrane Database Syst Rev. 2017;9:CD012252. Medline
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca