CADTH Health Technology Review
Point-of-Care Testing of International Normalized Ratios for People on Oral Anticoagulants: A Rapid Qualitative Review
Rapid Review
Authors: Elijah Herington, Danielle MacDougall
Abbreviations
CPAMS
community pharmacist-led anticoagulation management services
INR
international normalized ratio
OAC
oral anticoagulant
Key Messages
The opportunity to engage in self-testing can be experienced as simultaneously liberating and constraining.
While self-testing may be appreciated as a form of point-of-care testing for international normalized ratio (INR) levels, some people engaged in self-testing were concerned with the limited amount of personalized care they received.
People using oral anticoagulants described community pharmacist-led anticoagulation management services (CPAMS) as a convenient way of testing INR levels and learning about their health needs.
Community pharmacists felt they were well-situated to provide care through CPAMS, but acknowledged the importance of ongoing training, oversight, and appropriate levels of resourcing.
Context and Policy Issues
Oral anticoagulants (OACs) are largely taken by people who have a history of blood clots (e.g., deep vein thrombosis, pulmonary embolism) or a condition that increases their risk of developing blood clots in the future (e.g., atrial fibrillation, thrombophilia). The goal of OACs is to prevent the development or increased growth of harmful blood clots without keeping blood from clotting altogether. This can be complicated given the narrow therapeutic range of OACs such as warfarin and because doses often need to be adjusted due to factors such as genetic variation, meals, and the other medications one may be taking.1
As such, the use of OACs requires ongoing practices of measuring, tracking, and managing how quickly a person’s blood clots, which is represented as an international normalized ratio (INR). Along with the people using the OACs, INR management commonly involves multiple other parties, such as primary care providers, laboratories, and pharmacists. In this model, blood must be drawn at a collection centre or medical practice and then sent to a laboratory for testing. The laboratory informs the primary care provider of the INR value who then informs the person taking the OACs and makes dosing adjustments.1 Point-of-care testing models like community pharmacist-led anticoagulation management services (CPAMS) or self-testing attempt to limit both the time it takes to receive one’s INR values and the number of parties involved. The hope is that this not only improves the cost-effectiveness of OAC management, but also improves clinical outcomes given the assumption that this decreases barriers to accessing professional management services.
The purpose of this report is to describe how people using OACs and those involved in their care understand and experience point-of-care options in the management of their INR values.
Research Question
What are the perspectives and experiences of people who take oral anticoagulants, as well as their family and health care providers, on engaging with point-of-care testing to support the management of their INR levels?
Methods
Literature Search Methods
This report is an update of a literature search strategy developed for a previous CADTH report.2 For the current report, a limited literature search was conducted on key resources including MEDLINE, Embase, and Scopus. Search filters were applied to limit retrieval to qualitative studies. The initial search was limited to English-language documents published between January 1, 2010, and November 19, 2020. For the current report, database searches were rerun on January 27, 2021, to capture any articles published since the initial search date. Additionally, a supplemental search was conducted in MEDLINE and Scopus to locate mixed method publications. The main search concepts were anticoagulants and mixed methods. The search was also limited to English-language documents published between January 1, 2010, and January 27, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Sample | People who take oral anticoagulants to support the management of their INR levels and those involved in their care (e.g., family, primary care providers, pharmacists) |
Phenomenon of interest | Point-of-care testing for INR levels in any setting (e.g., community pharmacy, home) |
Design | Any qualitative design |
Evaluation | Perspectives on, expectations around, and experiences with accessing and undergoing point-of-care testing for INR levels |
Research type | Primary qualitative studies; qualitative portions of mixed-methods studies |
INR = international normalized ratio.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2010.
Critical Appraisal of Individual Studies
Critical appraisal was conducted by the primary reviewer and followed Krefting’s3 interpretation model for assessing trustworthiness in qualitative research. Krefting’s mode of exploring trustworthiness3 asks the reviewer to consider the interactions between research methods and results as a way of evaluating the process involved in arriving at a certain result or conclusion. This is done with a particular focus on 4 guiding questions:
Were the study authors true to their study participants (credibility)?
Does the analysis make sense in light of the data presented (confirmability)?
Is the analysis consistent across study findings (dependability)?
Does the analysis found in 1 study resonate with the research question and context for this review (transferability)?
Results of the critical appraisal were not used to exclude studies from this review; rather, they were used to understand the methodological and conceptual limitations of the included publications in relation to the research question. A narrative summary is provided below; a general note on the trustworthiness (i.e., high, moderate, low) of each included publication is reported in Table 2 in Appendix 2.
Data Analysis
A descriptive thematic analysis4 intended to identify the diversity of experiences with point-of-care testing for INR levels was conducted by a single reviewer.
Preliminary analysis began at the screening stage through the use of memoing. Given the small number of included publications (n = 6), memoing continued to be used in lieu of formal coding. This second set of memos helped to describe the findings of included primary studies and note preliminary spaces of confluence between studies. A second round of memoing and diagraming used an initial, tentative set of themes to extract findings and supporting data in the studies and to explore their relationships across studies. Included studies and memos were re-read, key findings and themes were identified, and the linkages between studies were explored. Memoing and re-reading continued until themes were well-described and stable, and all relevant findings and supporting data from the included studies had been accounted for within those themes.
Summary of Included Literature
Quantity of Research Available
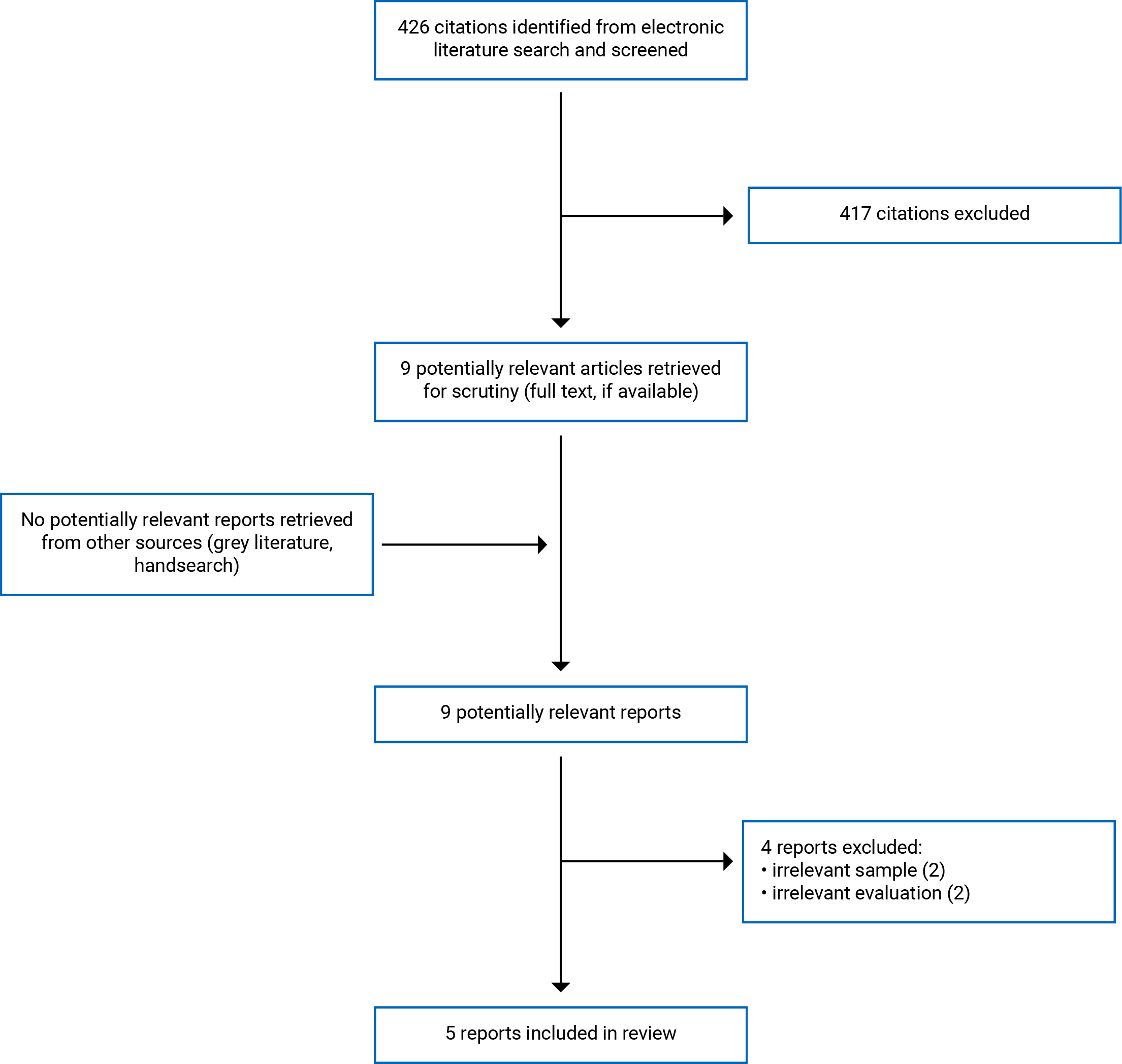
A total of 426 citations were identified in the literature search. Following screening of titles and abstracts, 417 citations were excluded and 9 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 4 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. The PRISMA5 flow chart of the study selection is presented in Appendix 1.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications and their participants are provided in Table 2 in Appendix 2.
Study Design
Five publications representing 4 studies were included in this review. Two publications, derived from 1 study, described using a mixed-methods study design.6,7 The remaining publications did not describe a study design, but all were qualitative and used 1 of the following for data analysis: thematic analysis,8 framework analysis,9 or content analysis.10 Four publications (including the qualitative portions of both mixed-methods publications) used interviews to collect data6-9 and 1 publication used text mining from blog posts.10
Country of Origin
Of the 5 publications, 3 were from the UK8-10 and 2 were from Aotearoa New Zealand.6,7
Participant Population
Across 5 publications there were a total of 43 people taking OACs engaged in self-testing,8,9 7 people taking OACs engaged in CPAMS,7 42 health care professionals providing CPAMS,6,7 and 6 health care professionals wishing to provide CPAMS.6 One study was not able to report participant characteristics given its design as a content analysis of blogs.10
Interventions
Three publications were focused on the experiences of people engaged in INR self-testing or their providers.8-10 Two publications, from 1 study, were focused on the experiences of people engaged in CPAMS or their providers.6,7
Summary of Critical Appraisal
The publications included within this review were assessed to be of a moderate to high degree of trustworthiness overall.
Of the 5 included publications, 3 were identified as being of a moderate degree of credibility and confirmability.6,7,10 One of these publications6 separated their presentation of data from their analysis by placing “data” (i.e., participant quotes) in tables cordoned off from the narrative text. While this may be a practical exercise for disciplines oriented toward the statistical representations of analysis (e.g., clinical epidemiology) or result from pressures to meet journal word limits that prevent authors from fully elaborating the connections between data and analysis in the text, their confirmability (i.e., whether an analysis makes sense in light of the presented data) was difficult to assess as a result. The remaining 27,10 provided incomplete support to their analysis. The links between data and analysis were clear at times; however, this was not consistent across the entirety of either publication. For these same reasons, both publications were considered to be of moderate credibility.
All of the included publications were assessed to have moderate to high dependability as their internal logics and ways of framing were consistent throughout the entirety of analysis. All of the publications demonstrated moderate to high transferability given their consistency with our own research question and context.
Results
Whether conducted by a pharmacist through a service like CPAMS or done by one’s self, point-of-care testing of INR levels was generally appreciated both by people taking OACs and their providers.6-10 For example, CPAMS and self-testing were described as improving the convenience of INR testing by increasing the number of sites available to conduct testing while decreasing the wait time associated with queues for blood draws and receiving the results of these blood draws.6-8,10 With this similarity in mind, we have nevertheless chosen to separate out the 2 forms of point-of-care testing in our presentation of the analysis below. While both do share crossover experiences, we found these experiences and expectations were often distinct enough to warrant this separation.
Self-Testing
Self-Testing Can Be Simultaneously Liberating and Constraining
By and large, people who had been prescribed self-testing appreciated the mobility and limited time spent in waiting rooms afforded by this form of point-of-care testing.8-10 Not being tied to a brick and mortar clinic, laboratory, or pharmacy for testing meant they could remain home if feeling ill or to travel freely for vacation and simply call in their INR values, receive a dose adjustment if necessary, and move on with their day.8,10 Some appreciated the level of independence this offered: “I travel a lot with work, so I can fly off to Germany and not worry if I’ve got to get a test in while I’m in Germany. I can just do it…so it’s definitely an independence thing (p. 610).”8
While many people may have had broadly positive experiences with self-testing and even felt a bit more “in control of [their] own destiny (p. 610),”8 it is important to think through the potential shift in responsibilities from professional care providers to people taking OACs entwined with self-testing. By being more involved in their own care, some felt as though they were engaged in a form of “apprenticeship”8 or “work”9 where they were learning to mimic the advice of their health care providers. One participant put it this way: “I’ve done this once after advice from a hospital [anticoagulation clinic], I’m in a very, very similar circumstance now, instead of bothering the hospital, I’ll do what I did last time and then test again in 2 days, and it’s worked so…(p. 611).”8 By paying close attention to how foods, for example, might interact with their medication and learning to read “all the little tell-tale [signs]”8 of their body that might indicate something is wrong (e.g., bleeding gums for 1 participant), some people even described confidence making independent adjustments themselves.8,9
While it was unclear at times from the included studies if this move beyond self-testing to self-management (e.g., dose adjustment) was prescribed or assumed, it did happen. One of the potential reasons people might opt to self-manage even if they had not been prescribed to do so could be their fear that if they reported numbers that were higher than the desired INR range, they might lose the opportunity to self-test.8 As such, not only did people take on self-management, but some described manipulating their results or simply choosing to not “bother telling anybody (p. 611)”8 when their numbers were out of range.
For those who were self-managing, this disappointment could be borne out as in Tompson’s study: “[I felt] annoyed with myself for, like, not dosing myself correctly, but I think I’ve learnt now, with a bit more experience, that it’s a pretty random drug and there’s no point in beating yourself up over it (p. e441).”9
Concerns About the Limited Amount of Personalized Care Received
While self-testing may be appreciated as a form of point-of-care testing for INR levels, some people engaged in self-testing were concerned with the limited amount of personalized care they received.
People using self-testing have to communicate their results to the clinic or community pharmacy at varying rates (depending on how close to being in range they are) and appreciate prompt feedback.8,10 Personalized contact with health care providers was noted as important. Participants would have appreciated the opportunity to meet with their clinical team to understand a bit more about how dosing decisions were made based on the INR numbers that were submitted. At present, participants felt a bit out to left field and alone because their clinicians knew nothing about them.8 This was particularly important in situations where the accuracy of the coagulometer was questioned or needed to be recalibrated.10
Learning the process of self-testing along with the operational requirements of the coagulometer could be difficult. For example, some people described having difficulty drawing enough blood for the coagulometer, which could lead to feeling a bit “hopeless,” as if they had “screwed up,” or even “a bit panicky (p. e439).”9 Those who were provided with training materials like instructional booklets or DVDs considered this to be inadequate and suggested that they would be better supported by face-to-face training opportunities.9,10 In the end, however, most described attaining some degree of confidence in their ability to self-test.8-10 This was particularly the case in situations where study participants already had a good relationship with their providers built on mutual trust.8
CPAMS
CPAMS Can Be a Convenient Way of Testing INR and Learning About Health Needs
Much like their counterparts engaged with OAC via self-testing, people using a CPAMS model to manage their OAC largely found it to be beneficial and appreciated the practicalities of more conveniently located services and shorter queues.7 However, the convenience of CPAMS was described as extending beyond these practicalities and was buffered by an appreciation for the immediacy or results. People appreciated the work of their primary care teams; however, given how busy their providers could be, the “results of tests can take time or get missed (p. 399).”7 As such, the opportunity to both quickly receive the results and have personalized conversations about them with their pharmacists helped people feel more comfortable with and knowledgeable of their own health.7 Were any complications to arise that their pharmacists felt unable to address, people using CPAMS were confident that their pharmacists would refer them back to their primary care team for clarification.7
Some people felt it was odd to be tested by the same person that they buy their deodorant from, while others expressed concern that their warfarin adjustments were dictated by an algorithm rather than the pharmacists’ clinical knowledge.7
Community Pharmacists Felt Well-Situated to Provide Care Through CPAMS
Although community pharmacists felt they were well-situated to provide care through CPAMS, they acknowledged the importance of ongoing training, oversight, and appropriate levels of resourcing.
By and large, both pharmacists who were enrolled in CPAMS and those who had not yet secured a licence to provide CPAMS were confident in their knowledge of warfarin and their ability to help navigate complications around getting people’s INR numbers within a predesignated target range.6,7 Given their location in community pharmacies where people may also be buying things such as food or over-the-counter medications, some pharmacists considered themselves “well placed to deal with things that might influence their [patient’s] therapy (p. 9).”6 This was especially important for pharmacists who either worked in more rural locations or where GPs might be in short supply.7 To ensure consistency across CPAMS sites, some pharmacists suggested that the development of an oversight body that could provide training and quality assurance would be helpful.6
Resourcing and funding were described by some pharmacists providing CPAMS as particularly concerning. Keeping up with pre-existing demands while adding this service could be difficult and may imply that some pharmacies are not suitable candidates for a program like CPAMS.6 Even where pharmacies have the human resources to provide the service, some pharmacists were concerned that people who are dealing with particularly unstable INR numbers and require more regular attention could make financing the service difficult.6
Limitations
The greatest limitation of this review is the limited literature exploring expectations, experiences, and perspectives of people taking OACs and health care professionals about point-of-care testing of INR levels. With only 3 qualitative studies focused on self-testing and 2 mixed-methods publications from 1 study focused on CPAMS, it is unlikely that all points of interest have been covered in this review. Although this does not lessen the validity of these findings, it lacks the contextual depth a qualitative review is meant to offer to the technology in question.
Furthermore, given that none of the included studies examined how things such as the pressures of gendered social roles or the physical and psychological harm of racist stereotypes may affect one’s access to or ability to engage with self-testing or CPAMS, we are unable to comment about how point-of-care testing for INR may be beneficial (or not) for people fitting any number of these categories.
Conclusions and Implications for Decision- or Policy-Making
We conducted a descriptive thematic synthesis to analyze the results of 5 publications and to describe some key features of how people use OACs, and their care providers engage with or experience, 2 forms of point-of-care testing for INR levels — self-testing and CPAMS.
Although point-of-care testing was generally appreciated across both self-testing and CPAMS, we have separated out the results of our analysis given the divergence in practices and concerns associated with each. For self-testing, people described a mixture of feeling liberated in their experience with self-testing, but also constrained by the ever-present possibility of losing their freedom to self-test. For some, this fear of losing the opportunity to self-test led them to either self-manage their OAC dosages or manipulate how and when they reported their results to the anticoagulation lab. In cases where people feel driven to self-manage, we might ask what better care could look like. Similarly, although self-testing was an appreciated form of point-of-care testing for INR levels, some people were concerned by the limited amount of personalized care they received. Without adding more layers of surveillance, is it possible to think differently about how support is provided to people who are self-testing?
Where CPAMS served as the form of point-of-care testing, people using OACs appreciated the opportunity to receive their test results rapidly and to follow up immediately with their pharmacist if there were any lingering questions. By and large, community pharmacists felt capable of both administering the test and addressing the questions their patients may have, but acknowledged the importance of ongoing training, oversight, and appropriate levels of resourcing.
References
1.Hull RD, Garcia DA, Vazquez SR. Warfarin and other VKAs: Dosing and adverse effects. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: www.uptodate.com. Accessed 2021 Jan 29.
2.Point-of-care testing of international normalized ratios for people on oral anticoagulants: a reference list. (CADTH rapid response report: reference list). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RA1152_POC%20of%20INR%20qual_Final.pdf. Accessed 2021 Jan 22.
3.Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J Occup Ther. 1991;45(3):214-222. Medline
4.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101.
5.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. Medline
6.Beyene K, Chan AHY, Barton E, et al. Pharmacists views on participating in New Zealand's community pharmacy anticoagulation management service: a mixed-methods study. Int J Clin Pharm. 2021;43(1):251-262. Medline
7.Shaw J, Harrison J, Harrison J. A community pharmacist-led anticoagulation management service: attitudes towards a new collaborative model of care in New Zealand. Int J Pharm Pract. 2014;22(6):397-406. Medline
8.Kuljis J, Money AG, Perry M, Barnett J, Young T. Technology-assisted self-testing and management of oral anticoagulation therapy: a qualitative patient-focused study. Scand J Caring Sci. 2017;31(3):603-617. Medline
9.Tompson A, Heneghan C, Fitzmaurice D, Sutton S, Harrison S, Ward A. Supporting patients to self-monitor their oral anticoagulation therapy: recommendations based on a qualitative study of patients' experiences. Br J Gen Pract. 2015;65(636):e438-e446. Medline
10.Shah SG, Robinson I. Patients' perspectives on self-testing of oral anticoagulation therapy: content analysis of patients' internet blogs. BMC Health Serv Res. 2011;11:25. Medline
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Publications
Lead author, year, location | Study objectives | Study design and data collection strategya | Inclusion criteria | Description of study participantsb | CPAMS or self-testing | Trustworthiness |
Beyene (2020) Aotearoa New Zealand6 | To explore the views of community pharmacists that provide and do not provide CPAMS to identify facilitators and barriers to uptake | Mixed methods; phone interviews | NR | Total participants = 12 CPAMS:
| CPAMS | Moderate |
Kuljis (2017) UK8 | To better understand the perceptions of individuals enrolled as “patient self-testers” at an oral anticoagulation clinic | Thematic analysis; semi-structured interviews | All participants needed to be registered and active PSTMs at a hospital-based anticoagulation clinic, speak English, aged 18 or older, able to provide informed consent to take part in the study, and used the CoaguChek INR self-testing device | Total participants = 17 Experience with self-testing ranged from 1 year to 10 years across participants | Self-testing | High |
Tompson (2015) UK9 | To learn more about the experiences of people who were self-monitoring their OAC in the hopes of identifying a set of barriers and facilitators that these people encounter and to produce a set of recommendations on how best to support such people | Framework analysis; interviews | NR | Total participants = 26 | Self-testing | High |
Shaw (2014) Aotearoa New Zealand7 | To explore the perspectives and experiences of people who participated in a CPAMS pilot | Mixed-methods; interviews | NR | 43 total participants
| CPAMS | Moderate |
Shah (2011) UK10 | To explore peoples’ experiences conducting INR self-testing | Content analysis; text mining from blogs | Blogs and blog postings written in the English language from January 2000 to October 2009 by any patient or lay carers were selected. Another criterion for the selection of blogs was that they should be currently active | NR | Self-testing | Moderate |
CPAMS = community pharmacists-led anticoagulation management service; INR = international normalized ratio; NR = not reported; OAC = oral anticoagulation therapy; POCT = point-of-care testing; PSTM = patient self-tester manager.
aFor mixed-methods studies, we only identified the data collection strategies of the qualitative components.
bFor mixed-methods studies, we only identified the participants of the qualitative components.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein do not necessarily reflect the views of Health Canada, Canada’s provincial or territorial governments, other CADTH funders, or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to requests@cadth.ca