CADTH Health Technology Review
Laxatives and Erectile Dysfunction Medications to Treat Side Effects of Opioid Agonist and Methadone Maintenance Therapy
Rapid Review
Authors: Sara D. Khangura, Andrea Ryce
Abbreviations
ED
erectile dysfunction
MMT
methadone maintenance therapy
OAT
opioid agonist therapy
OUD
opioid use disorder
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Key Messages
Opioid agonist and methadone maintenance therapies are essential medical interventions for effectively managing opioid use disorder. However, side effects, including constipation and erectile dysfunction can compromise treatment adherence and increase the risk of relapse.
No studies or guidelines describing the clinical effectiveness or recommendations for the use of laxatives or erectile dysfunction medications in the treatment of constipation or erectile dysfunction in patients undergoing OAT or MMT were identified.
Research is needed to understand the clinical effectiveness and inform guidance concerning the treatment of constipation with laxatives and the use of medications indicated for erectile dysfunction.
Context and Policy Issues
Opioid use disorder (OUD) is a health crisis in Canada1,2 and around the world.3,4 OUD is characterized by a dependency on opioid drugs and/or prescription opioid medications, and people living with OUD experience a euphoria commonly known as “getting high.”5 People of all ages and/or sociodemographic backgrounds can develop OUD; however, known risk factors include younger age (i.e., adolescents and young adults), a history of substance abuse, and/or comorbid mental illness.6 People living with OUD often experience significant morbidity and mortality, including loss of livelihood and/or social networks and supports, homelessness, increased hospitalization, and death.2,4,7,8 Increasingly, the opioid crisis is being driven by the misuse of opioid medications that are commonly prescribed for patients experiencing pain — in particular, chronic pain.8
Treatment for OUD is generally multi-modal, including both behavioural and pharmacological interventions.4,5,9 Opioid agonist therapy (OAT) and methadone maintenance therapy (MMT) are effective medical interventions for reducing the symptoms of dependency and supporting patients with OUD to reduce and abstain from their misuse of opioids.1,10 OAT and MMT medications include methadone and buprenorphine, which are longer-acting opioid medications as compared to the shorter-acting opioid drugs and medications that can cause OUD.4 OAT and MMT thereby reduce the symptoms of withdrawal without producing the effect of getting high.9 However, like all opioid medications and drugs, OAT and MMT cause side effects, such as constipation and sexual dysfunction (including erectile dysfunction [ED] in men).11 These side effects can cause discomfort and distress, and may discourage patients undergoing OAT or MMT from continuing with treatment, which can increase the risk of relapse.12,13
Constipation has been described as a common and persistent side effect of OAT and MMT.9-11 Opioid-induced constipation is a side effect common to all opioid drugs and medications, and is described as one of the most common gastrointestinal adverse effects caused by this class of drugs.14 In addition to more serious complications from chronic constipation, it can cause bloating, discomfort, and reduced quality of life for affected patients.15 Common treatments for constipation include dietary and lifestyle interventions (such as increased fibre and/or exercise) and/or laxatives (including stimulants, stool softeners, and fibre supplements).16 Although there is some information and evidence to inform the treatment of opioid-induced constipation in patients receiving prescribed opioids,17-19 less information is known to be available to inform best practices for treating OUD patients with constipation as a side effect of OAT or MMT.
Sexual dysfunction is also a side effect of opioid drugs and medications — including OAT and MMT — and can occur in both men and women.20-23 Sexual dysfunction causes a variety of deleterious symptoms, including abnormalities in sexual desire, arousal, and satisfaction,13 and sometimes resulting in ED for men.24 Sexual dysfunction and/or ED may have various underlying causes, including those of a physiologic, social, and/or psychological etiology.12,25 The association between exposure to OAT and sexual dysfunction (including ED) is well-established.12,25 Treatments for ED in the general population may include medical, mechanical, and/or surgical interventions26; however, less information is known to be available to inform best practices for the treatment of ED as a side effect of OAT or MMT in patients living with OUD.
Given the benefits that OAT and MMT can offer to patients living with OUD — as well as the known side effects of these medications and the limited information available to inform treatment to reduce their deleterious effects — there is a need to assemble and assess available evidence addressing this topic. Thus, the purpose of this report is to identify and summarize evidence and guidelines describing the clinical effectiveness and/or recommendations to inform the use of laxatives and/or ED medication for OUD patients undergoing OAT or MMT.
Research Questions
What is the clinical effectiveness of laxatives to treat constipation in patients undergoing opioid agonist therapy or methadone maintenance treatment?
What is the clinical effectiveness of erectile dysfunction medication to treat sexual dysfunction in patients undergoing opioid agonist therapy or methadone maintenance treatment?
What are the evidence-based guidelines regarding laxatives or erectile dysfunction medication for patients undergoing opioid agonist therapy or methadone maintenance treatment?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE All via Ovid, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were OAD or MMT and drug therapy for constipation and ED. Search filters were applied to part of the search to limit retrieval to guidelines. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and May 11, 2021. Internet links were provided if available.
Selection Criteria and Methods
One reviewer screened all citations and selected the studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant sources were retrieved and assessed for eligibility. The final selection of full-text sources was based on the eligibility criteria presented in Table 1.
Criteria | Description |
Population | Patients undergoing opioid agonist therapy or methadone maintenance treatment (i.e., suboxone, morphine, or naltrexone) |
Intervention | Q1: Laxatives, bulk-forming agents, and stool softeners (e.g., docusate, senna, polyethylene glycol 3350, sodium phosphate, bisacodyl, glycerine suppositories, psyllium husk) Q2: Erectile dysfunction medication (e.g., sildenafil citrate, tadalafil, vardenafil) Q3: Laxatives, bulk-forming agents, and stool softeners, or erectile dysfunction medication |
Comparator | Alternative medications for constipation or sexual dysfunction; non-pharmacological; alternative lifestyle changes; no treatment |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., change in symptoms, safety) Q3: Recommendations regarding the use of laxatives or erectile dysfunction medication in patients undergoing opioid agonist therapy or methadone maintenance treatment |
Study designs | HTAs, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
HTA = health technology assessment.
Exclusion Criteria
Articles were excluded if they did not meet the eligibility criteria outlined in Table 1, were duplicate publications, or were published before 2016. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
Critical appraisal was not undertaken because no eligible guidelines were identified.
Summary of Evidence
Quantity of Research Available
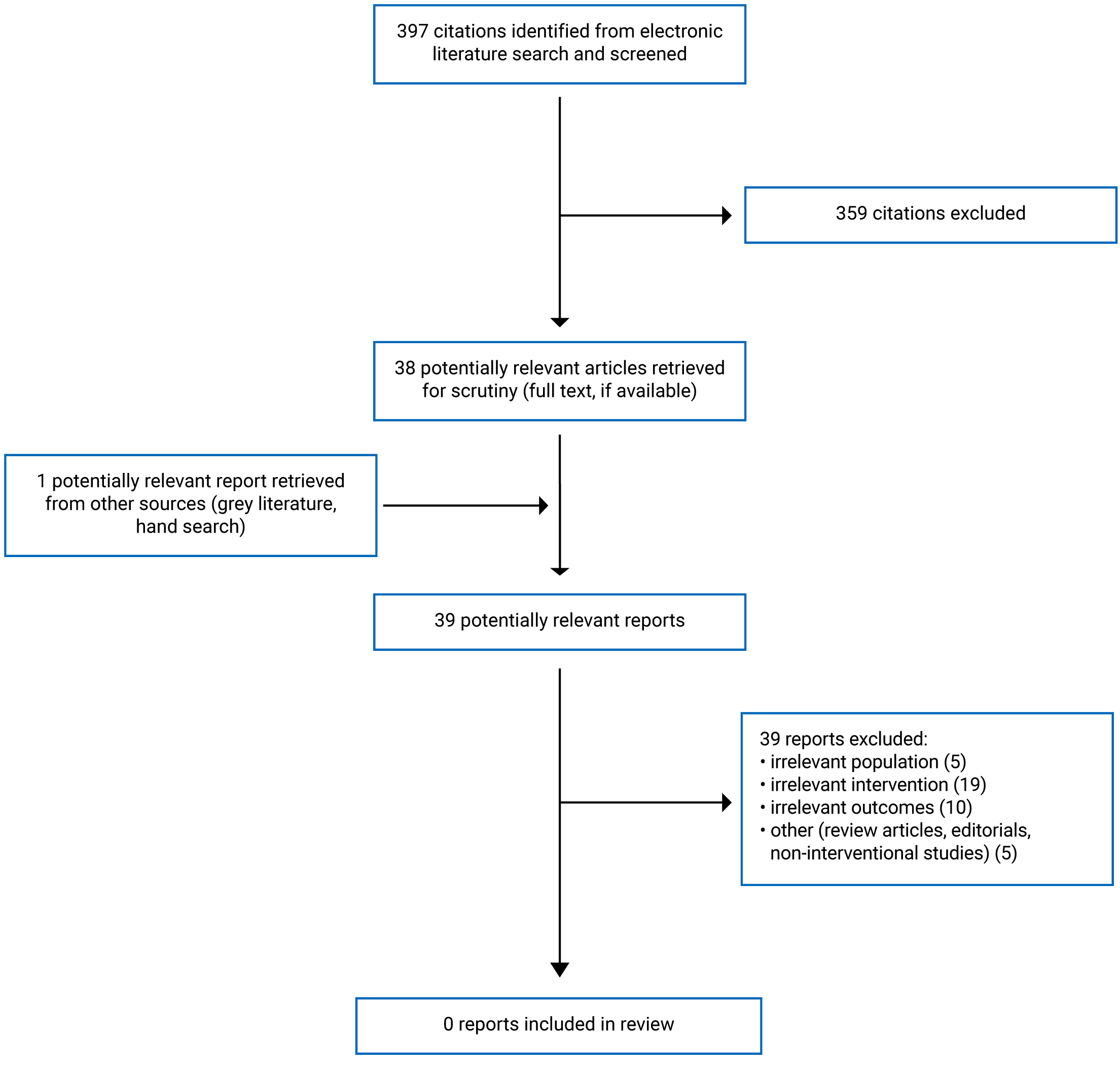
A total of 397 citations were identified in the literature search. Following screening of titles and abstracts, 359 citations were excluded and 38 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant source was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 39 publications were excluded for various reasons, and no publications met the inclusion criteria and were included in this report. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)27 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 2.
Summary of Findings
No studies assessing the clinical effectiveness of laxatives to treat constipation or ED medications to treat sexual dysfunction medications for patients undergoing OAT or MMT were identified. No evidence-based guidelines informing the use of laxatives or ED medications for patients undergoing OAT or MMT were identified; therefore, no summary is provided.
Limitations
No eligible studies nor evidence-based guidelines describing laxatives or ED medications for patients undergoing OAT and MMT were identified.
Conclusions and Implications for Decision- or Policy-Making
No evidence or evidence-based guidelines describing the use of laxatives or ED medication to treat the side effects of OAT or MMT were identified. This gap in the evidence describing treatment of the side effects of OAT and MMT has also been acknowledged in the literature reviewed for this report.22 Most of the evidence in this topic area was found to address either the clinical effectiveness of OAT and/or MMT28,29 or the side effects from prescribed opioid medications in patients living with pain.17-19,30,31 Although existing guidelines offer recommendations about the use of OAT and/or MMT to treat OUD, there were no guidelines identified informing the management or treatment of constipation or ED as side effects of OAT and/or MMT.1,8
CADTH has previously assembled a body of evidence relevant to opioids,32,33 including reports that have assessed and summarized evidence specific to the use of OAT and MMT and its effects on people living with OUD.34-38 One recent CADTH report assembled and summarized qualitative evidence describing the experiences of OUD patients and described a preference among some patients for buprenorphine as compared to methadone due to the perception of fewer side effects with the former.39 However, the CADTH reports produced to date have not addressed treatment of side effects from OAT.
Several sources were identified in this review that described investigations into the treatment of constipation as a side effect of opioid medication prescribed for patients with chronic pain17-19,30; however, there were no studies that described the treatment of constipation as a side effect of OAT or MMT. Notably, the sources identified did not describe investigation into the use of laxatives to treat opioid-induced constipation; rather, these studies assessed the use of naldemedine17,30 and methylnaltrexone.18,19
Several studies that assessed sexual dysfunction and/or ED were identified but did not meet the eligibility criteria for this review — many were observational and, as such, did not assess an intervention.12,24,25,40 Two such studies assessed measures of sexual dysfunction and/or ED and other psychological parameters in men living with OUD and receiving MMT as compared to men not receiving MMT. Authors of both studies reported finding significantly more sexual dysfunction and/or ED and psychological morbidity among patients receiving MMT.12,25 Another study reported a significant correlation between psychological distress and ED in patients receiving MMT.24 Authors of these and other studies addressing sexual dysfunction and/or ED have highlighted the importance of multiple variables that often contribute to the problem of sexual dysfunction and ED — in this case, among patients receiving OAT and MMT.12,24,25,40 The complexity of ED is likely to contribute to the challenge of effective treatment, and may be compounded in patients receiving OAT and/or MMT given the psychological, sociological, and other comorbidities that can occur in these patients.
Several other studies were identified that investigated the use of alternative therapies20,22,23,41,42 and/or antidepressant drugs41-43 as primary study interventions for the treatment of ED as a side effect of MMT as opposed to investigating ED medication. One such study reported an improvement in ED for MMT patients receiving Rosa damascena oil as compared to those randomized to placebo.22 Another double-blind, placebo-controlled randomized trial reported that ginseng produced a benefit to both male and female patients with sexual dysfunction as a side effect of MMT.20 Yet another study randomized MMT patients to either crocin or placebo and measured psychological parameters after 8 weeks (including ED); the authors reported a statistically significant improvement in patients receiving the active intervention.42 Nonetheless, the treatment of ED using medications developed for the condition itself (e.g., sildenafil citrate, tadalafil, vardenafil) was not described in the studies identified by this review.
Given the importance of OAT and MMT in the context of the opioid crisis, and the risk that side effects such as constipation and/or ED may pose to treatment adherence, there is a need for more research investigating best practices and interventions to inform the management of care and ensure optimal patient outcomes.
References
1.Korownyk C, Perry D, Ton J, et al. Managing opioid use disorder in primary care: PEER simplified guideline. Can Fam Physician. 2019;65(5):321-330. PubMed
2.Rieb LM, Samaan Z, Furlan AD, et al. Canadian Guidelines on Opioid Use Disorder Among Older Adults. Can Geriatr J. 2020;23(1):123-134. PubMed
3.Llanes C, Alvarez AI, Pastor MT, Garzon MA, Gonzalez-Garcia N, Montejo AL. Sexual Dysfunction and Quality of Life in Chronic Heroin-Dependent Individuals on Methadone Maintenance Treatment. J. 2019;8(3):07.
4.Schuckit MA. Treatment of Opioid-Use Disorders. N Engl J Med. 2016;375(4):357-368. PubMed
5.Strain E. Pharmacotherapy for opioid use disorder. In: UpToDate, ed. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Jun 1.
6.Strain E. Opioid use disorder: Epidemiology, pharmacology, clinical manifestations, course, screening, assessment, and diagnosis. In: UpToDate, ed. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Jun 1.
7.NSW Clinical Guidelines: Treatment of Opioid Dependence – 2018. North Sydney (AU): New South Wales Ministry of Health; 2018: https://www.health.nsw.gov.au/aod/Publications/nsw-clinical-guidelines-opioid.pdf. Accessed 2021 Jun 1.
8.Bruneau J, Ahamad K, Goyer ME, et al. Management of opioid use disorders: a national clinical practice guideline. Cmaj. 2018;190(9):E247-E257. PubMed
9.Opioid agonist therapy. Toronto (ON): Centre for Addiction and Mental Health.; 2016: https://www.camh.ca/-/media/files/oat-info-for-clients.pdf. Accessed 2021 Jun 1.
10.Tetrault JM, Fiellin DA. Current and potential pharmacological treatment options for maintenance therapy in opioid-dependent individuals. Drugs. 2012;72(2):217-228. PubMed
11.Opioid Agonist Therapy Guidelines for Manitoba Pharmacists. Winnepeg (MB): College of Pharmacists of Manitoba.; 2020: https://cphm.ca/wp-content/uploads/Resource-Library/Opioid-Agonist-Therapy/OAT-Guidelines-MB-Pharmacists.pdf. Accessed 2021 May 31.
12.Agha-Mohammadhasani P, Mokhtaree M, Nazari A, Rahnama A. Comparison of Sexual Function and Serum Testosterone Levels in Men Opiate Addicts, under Methadone Maintenance Therapy, and Healthy Men. Addict. 2018;10(2):76-85. PubMed
13.Babakhanian M, Haghdoost AA, Afshari M, Taghizadeh F, Moosazadeh M. Methadone Replacement Therapy and Sexual Disorders among Opium Dependent Iranian Men: A Meta-Analysis Study. Addict. 2017;9(1):1-10. PubMed
14.Nelson AD, Camilleri M. Opioid-induced constipation: advances and clinical guidance. Ther Adv Chronic Dis. 2016;7(2):121-134. PubMed
15.Mehta V, Alaward S, Kuravinakop S, Nikolic S. Effect of a fixed-dose opioid agonist/antagonist on constipation in patients on long-term opioids for non-malignant pain unable to tolerate laxatives. Pain physician. 2014;17(5):415-424. PubMed
16.Constipation. Patient Care & Health Information 2019; https://www.mayoclinic.org/diseases-conditions/constipation/diagnosis-treatment/drc-20354259. Accessed 2021 Jun 11.
17.Brower V. Naldemedine effective in treating opioid-induced constipation. Lancet Oncol. 2017;18(6):e306. PubMed
18.Chamberlain BH, Rhiner M, Slatkin NE, Stambler N, Israel RJ. Subcutaneous methylnaltrexone for opioid-induced constipation in advanced-illness patients with or without active cancer. Pain manag. 2020;10(2):73-84. PubMed
19.Mehta N, O'Connell K, Giambrone GP, Baqai A, Diwan S. Efficacy of methylnaltrexone for the treatment of opiod-induced constipation: a meta-analysis and systematic review. Postgrad Med. 2016;128(3):282-289. PubMed
20.Farnia V, Alikhani M, Ebrahimi A, Golshani S, Sadeghi Bahmani D, Brand S. Ginseng treatment improves the sexual side effects of methadone maintenance treatment. Psychiatry Res. 2019;276:142-150. PubMed
21.Zamboni L, Franceschini A, Portoghese I, Morbioli L, Lugoboni F, Group G. Sexual Functioning and Opioid Maintenance Treatment in Women. Results From a Large Multicentre Study. Front Behav Neurosci. 2019;13:97. PubMed
22.Farnia V, Tatari F, Alikhani M, et al. Rosa Damascena oil improved sexual function and testosterone in male patients with opium use disorder under methadone maintenance therapy-results from a double-blind, randomized, placebo-controlled clinical trial. Drug Alcohol Depend. 2017;176:117-125. PubMed
23.Farnia V, Tatari F, Alikhani M, et al. Rosa Damascena oil improved methadone-related sexual dysfunction in females with opioid use disorder under methadone maintenance therapy - results from a double-blind, randomized, and placebo-controlled trial. J Psychiatr Res. 2017;95:260-268. PubMed
24.Cheng CM, Lin YC, Chang KC. Psychological Distress is Correlated with Erectile Dysfunction Among Patients Receiving Methadone Maintenance in Taiwan. J Dual Diagn. 2017;13(4):312-316. PubMed
25.Gerra G, Manfredini M, Somaini L, Maremmani I, Leonardi C, Donnini C. Sexual Dysfunction in Men Receiving Methadone Maintenance Treatment: Clinical History and Psychobiological Correlates. Eur Addict Res. 2016;22(3):163-175. PubMed
26.MacGill M. What's to know about erectile dysfunction? 2017; https://www.medicalnewstoday.com/articles/5702. Accessed 2021 Jun 1.
27.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
28.Klein JW. Pharmacotherapy for Substance Use Disorders. Med Clin North Am. 2016;100(4):891-910. PubMed
29.Ronsley C, Nolan S, Knight R, et al. Treatment of stimulant use disorder: A systematic review of reviews. PLoS ONE. 2020;15(6):e0234809. PubMed
30.Anonymous. Naldemedine (Symproic) for opioid-induced constipation. Med Lett Drugs Ther. 2017;59(1535):196-198. PubMed
31.Moss J. Identifying and Treating Opioid Side Effects: The Development of Methylnaltrexone. Anesthesiology. 2019;130(1):142-148. PubMed
32.Evidence on Opioids. Evidence Bundle 2021; https://cadth.ca/evidence-bundles/opioid-evidence-bundle. Accessed 2021 Jun 1.
33.Treating Opioid Use Disorder. Research Gaps. Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/treating_opioid_use_disorder.pdf. Accessed 2021 Jun 2.
34.Injectable Opioid Agonist Treatment for Patients with Opioid Dependence: A Review of Clinical and Cost-Effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RC1277-iOAT%20Final.pdf. Accessed 2021 Jun 2.
35.Telehealth-delivered opioid agonisttherapy for the treatment of adults with opioid use disorder: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2018: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1026%20opioid%20agonist%20therapy%20Final.docx.pdf. Accessed 2021 Jun 11.
36.Buprenorphine formulations for the treatment of opioid use disorders: a review of comparative clinical effectiveness, cost-effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://cadth.ca/sites/default/files/pdf/htis/2017/RC0908%20Buprenorphine%20Formulations%20Final.pdf. Accessed 2021 Jun 2.
37.Buprenorphine/Naloxone Versus Methadone for the Treatment of Opioid Dependence: A Review of Comparative Clinical Effectiveness, Cost-Effectiveness and Guidelines. (CADTH Rapid response report: peer-reviewed summary with critical appraisal). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/htis/sep-2016/RD0032_Suboxone_Final.pdf. Accessed 2021 Jun 2.
38.Crushed Buprenorphine or Buprenorphine-Naloxone for Opioid Dependency: A Review of the Clinical Effectiveness and Guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2016: https://cadth.ca/sites/default/files/pdf/htis/july-2016/RC0794-Crushed%20Suboxone%20Final.pdf. Accessed 2021 Jun 2.
39.Opioid agonist treatments for opioid use disorder: a rapid qualitative review. . (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1100%20Buprenorphine%20for%20OUD%20Final.pdf. Accessed 2021 Jun 2.
40.Ramli FF, Shuid AN, Pakri Mohamed RM, Tg Abu Bakar Sidik TMI, Naina Mohamed I. Health-Seeking Behavior for Erectile Dysfunction in Methadone Maintenance Treatment Patients. Int J Environ Res Public Health. 2019;16(21):01.
41.Ramli FF, Azizi MH, Syed Hashim SA. Treatments of Sexual Dysfunction in Opioid Substitution Therapy Patients: A Systematic Review and Meta-Analysis. Int J Med Sci. 2021;18(11):2372-2380. PubMed
42.Khalatbari-Mohseni A, Banafshe HR, Mirhosseini N, Asemi Z, Ghaderi A, Omidi A. The effects of crocin on psychological parameters in patients under methadone maintenance treatment: a randomized clinical trial. Subst Abuse Treat Prev Policy. 2019;14(1):9. PubMed
43.Yee A, Loh HS, Ong TA, Ng CG, Sulaiman AH. Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Trial of Bupropion as Treatment for Methadone-Emergent Sexual Dysfunction in Men. AJMH. 2018;12(5):1705-1718. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Additional References
1.NSW Clinical Guidelines: Treatment of Opioid Dependence – 2018. North Sydney (AU): New South Wales Ministry of Health; 2018: https://www.health.nsw.gov.au/aod/Publications/nsw-clinical-guidelines-opioid.pdf. Accessed 2021 Jun 11.
Guideline in the Appendix (p. 124) describing constipation as a side effect of OAT, but not including formal guidance on its management and/or treatment:
2.Ramli FF, Shuid AN, Pakri Mohamed RM, et al. Health-Seeking Behavior for Erectile Dysfunction in Methadone Maintenance Treatment Patients. Int J Environ Res Public Health. 2019;16(21):01.
Observational study of MMT patients with self-reported data describing health-seeking behaviour, including the decision to use, and perceived effectiveness of, medication for ED (medications unspecified):
Previous CADTH Reports
3.Treating Opioid Use Disorder. Research Gaps. Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/pdf/treating_opioid_use_disorder.pdf. Accessed 2021 Jun 2.
4.Injectable Opioid Agonist Treatment for Patients with Opioid Dependence: A Review of Clinical and Cost-Effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/pdf/htis/2020/RC1277-iOAT%20Final.pdf. Accessed 2021 Jun 2.
5.Telehealth-delivered opioid agonisttherapy for the treatment of adults with opioid use disorder: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2018: https://cadth.ca/sites/default/files/pdf/htis/2019/RC1026%20opioid%20agonist%20therapy%20Final.docx.pdf. Accessed 2021 Jun 11.
6.Buprenorphine formulations for the treatment of opioid use disorders: a review of comparative clinical effectiveness, cost-effectiveness and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://cadth.ca/sites/default/files/pdf/htis/2017/RC0908%20Buprenorphine%20Formulations%20Final.pdf. Accessed 2021 Jun 2.
7.Buprenorphine/Naloxone Versus Methadone for the Treatment of Opioid Dependence: A Review of Comparative Clinical Effectiveness, Cost-Effectiveness and Guidelines. (CADTH Rapid response report: peer-reviewed summary with critical appraisal). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/htis/sep-2016/RD0032_Suboxone_Final.pdf. Accessed 2021 Jun 2.
8.Crushed Buprenorphine or Buprenorphine-Naloxone for Opioid Dependency: A Review of the Clinical Effectiveness and Guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2016: https://cadth.ca/sites/default/files/pdf/htis/july-2016/RC0794-Crushed%20Suboxone%20Final.pdf. Accessed 2021 Jun 2.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca