CADTH Health Technology Review
Point-of-Care Testing and N-Acetylcysteine for Acute Acetaminophen Overdose
Rapid Review
Authors: Khai Tran, Jennifer Horton
Abbreviations
GRADE
Grades of Recommendation Assessment, Development and Evaluation
NAC
N-acetylcysteine
UW
University of Wisconsin
Key Messages
Evidence on the clinical utility and cost-effectiveness of point-of-care devices could not be identified.
Two evidence-based guidelines recommend a 2-bag regimen of N-acetylcysteine, consisting of both a loading dose and maintenance dose, administered by IV for patients with acute acetaminophen overdose.
Context and Policy Issues
Acetaminophen, also called paracetamol or N-acetyl-p-aminophenol, is a popular drug used to temporarily reduce pain and fever.1 It is available in different strengths and forms, and for a wide range of populations, from children to elderly people.1 The maximum amount of acetaminophen allowed per day is 4,000 mg for adults and children aged 12 years and older.1 Although acetaminophen is safe when used as directed, long-term use and exceeding the maximum recommended daily dose can cause acetaminophen toxicity and liver damage.1
Due to the popularity and accessibility of acetaminophen, the risk of acetaminophen overdose, either by accident or on purpose, is relatively common and it is the leading cause of acute liver failure in Canada and around the world.1 Approximately 4,500 individuals are hospitalized each year in Canada due to acetaminophen overdose, and about 6% of patients hospitalized for acetaminophen overdose develop liver injuries including acute liver failure that may require a liver transplant or lead to death.1
The diagnosis of liver toxicity is based on serum levels of acetaminophen and other laboratory tests including liver function tests and a coagulation profile.2 The Rumack-Matthew nomogram, based on large data of patients not treated with antidote, plots acetaminophen concentration against time of ingestion as a predictor of hepatotoxicity and mortality.2,3 When the serum concentration of acetaminophen is above the curve at 200 mg/L at 4 hours and 25 mg/L at 16 hours, patients would have 60% incidence of severe hepatotoxicity and 5% rate of mortality.3 With 300 mg/L serum acetaminophen concentration at 4 hours and 37.5 mg/L at 16 hours, the incidence of severe hepatotoxicity would be up to 90%, and the rate of mortality would be up to 24%.3 Using this approach, patients with serum acetaminophen concentration greater than 140 mg/L at 4 hours after ingestion are considered having possible risk of hepatotoxicity, and treatment with N-acetyl-cysteine (NAC) is required.2,3 NAC has been indicated in Canada as an acetaminophen poisoning antidote.4
Several analytical methods for determining acetaminophen levels in human serum/plasma have been reported in the literature including high-performance liquid chromatography,5 UV-visible spectrophotometry,6 spectrofluorometric,7 and gas chromatography-mass spectrometry.8 When a patient is admitted to hospital or emergency department with actual or suspected acetaminophen overdose, blood samples are taken and sent to central laboratory for analysis of acetaminophen levels in the blood, and the diagnosis is delayed while waiting for the laboratory results. Point-of-care tests, also called bed-side tests or near-patient tests, are quick screening tests that could potentially improve the management of these patients. Several point-of-care tests for acetaminophen detection are reported in the literature,9,10 however, their clinical utility compared with laboratory-based diagnostic tests is unclear.
This report aims to review the clinical utility and cost-effectiveness of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose. The report also summarizes the recommendations from evidence-based guidelines regarding the administration of IV N-acetylcysteine for patients with acute acetaminophen overdose.
Research Questions
What is the clinical utility of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose?
What is the cost-effectiveness of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose?
What are the evidence-based guidelines regarding the administration of IV N-acetylcysteine for patients with acute acetaminophen overdose?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were acetaminophen, overdose, and n-acetylcysteine. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses; randomized controlled trials, controlled clinical trials, or any other type of clinical trial; economic studies; and guidelines. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and June 15, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with suspected acute acetaminophen overdose. |
Intervention | Q1, Q2: Any point-of-care device to measure acute acetaminophen overdose. Q3: IV NAC for acute acetaminophen overdose. |
Comparator | Q1, Q2: Laboratory-based diagnostic tests or any other diagnostic tests that measure acute acetaminophen overdose. Q3: Not applicable. |
Outcomes | Q1: Clinical utility (e.g., time to overdose treatment, incidence of overdose-related adverse events, safety, overdose-related mortality). Q2: Cost-effectiveness (e.g., cost-benefit of point-of-care testing vs. usual diagnostic test, costs associated with acetaminophen toxicity treatment, QALYs gained, ICERs). Q3: Recommendations regarding the use of IV NAC for patients with acute acetaminophen overdose. |
Study designs | HTA, SR, RCT, non-randomized studies, economic evaluations, and evidence-based guidelines. |
HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; NAC = N-acetylcysteine; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument11 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
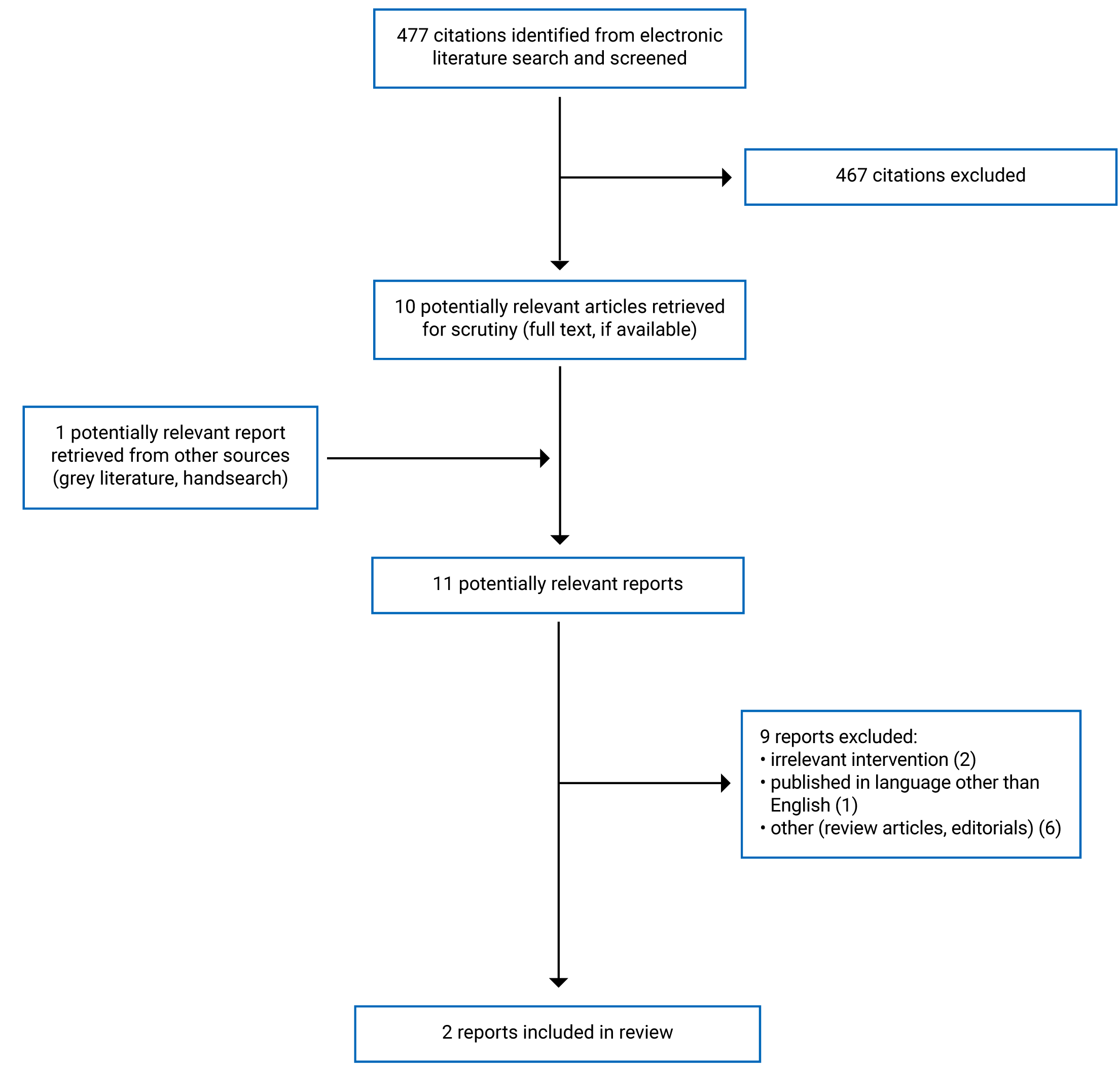
A total of 477 citations were identified in the literature search. Following screening of titles and abstracts, 467 citations were excluded and 10 potentially relevant report from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 9 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These were both evidence-based guidelines. Appendix 1 presents the PRISMA12 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The detailed characteristics of the included guidelines by Chiew et al. (2020)13 and the University of Wisconsin (UW) Health (2019)14 are provided in Appendix 2 (Table 2).
Study Design
Both included guidelines13,14 were clinical practice guidelines, which were developed to provide recommendations on the use of NAC for the management of acetaminophen overdose. A systematic search of the literature was conducted, and the quality of evidence and the strength of recommendations were assessed and graded using the Grades of Recommendation Assessment, Development and Evaluation (GRADE) in both guidelines. The UW Health guideline14 rated the level of evidence from high to very low, and the recommendations as either strong or conditional. The wordings are presented in the footnotes of Table 2 in Appendix 2. The guideline by Chiew et al, (2020)13 did not provide the rating scheme for the strength of the evidence and recommendations. Recommendations in both guidelines were developed by expert panels, and the guidelines were reviewed by external reviewers and were published either on their websites or peer-reviewed journals.
Country of Origin
The guidelines were conducted by authors from Australia and New Zealand,13 and the US.14
Patient Population
The target population of both guidelines13,14 are adult and pediatric patients with acetaminophen overdose. The intended guideline users were health care providers involved in the management of acute acetaminophen overdose.
Interventions and Comparators
The dosing regimens of NAC for treatment of acetaminophen overdose were considered in both guidelines.13,14
Outcomes
Both guidelines13,14 considered evidence based on efficacy and safety outcomes of NAC for the treatment of acetaminophen overdose for the development of the recommendations. The clinical efficacy outcomes of NAC included lowering acetaminophen plasma concentration, lowering liver enzyme levels, and therefore preventing liver toxicity.15 The common adverse events of IV NAC were anaphylactoid reactions, such as rash, pruritus, angioedema, bronchospasm, tachycardia, and hypotension.15
Summary of Critical Appraisal
The detailed quality assessments of the included guidelines13,14 (Table 3) are presented in Appendix 3.
Both guidelines13,14 were explicit in terms of scope and purpose (i.e., objectives, health questions and populations), and had clear presentation (i.e., specific, and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). In terms of stakeholder involvement, both guidelines13,14 clearly defined target users and the development groups; however, it was unclear if the views and preferences of the patients were sought in the guideline by Chiew et al. (2020).13 For rigour of development, both guidelines13,14 reported systematic methods used to search for evidence, criteria for selecting evidence, explicit link between recommendations and the supporting evidence, and methods of formulating the recommendations. Both guidelines13,14 considered health benefits, side effects, and risks in formulating the recommendations, were peer-reviewed before publication, and provided a procedure for updating. Both guidelines13,14 used GRADE methodology to assess and grade their recommendations. For clarity, the recommendations in both guidelines13,14 are specific and unambiguous, provide different options for management of the condition, and are easily identifiable. For applicability, both guidelines13,14 were explicit in terms of facilitators and barriers to application (e.g., confirmed acetaminophen ingestion/management in a clinical setting, and seeking advice from a poisons information centre), advice and/or tools on how the recommendations can be put into practice (e.g., acetaminophen management flow charts), and resource implications (e.g., considering costs in recommendations). However, neither guideline13,14 presented monitoring and or auditing criteria for auditing or monitoring the use of the guideline. For editorial independence, competing interests of guideline development group members were reported, but it was unclear if the views of the funding body have influenced the content of the guidelines. Overall, both included guidelines13,14 were of good methodological quality.
Summary of Findings
The summary of guideline recommendations is presented in Appendix 4 (Table 4).
Clinical Utility of Point-of-Care Devices
No clinical utility studies of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose were identified; therefore, no summary can be provided.
Cost-Effectiveness of Point-of-Care Devices
No cost-effectiveness studies of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose were identified; therefore, no summary can be provided.
Guidelines
The Australia and New Zealand guideline by Chiew et al. (2020)13 recommends NAC administered as a 2-bag regimen. Initial loading dose is 200 mg/kg over 4 hours followed by 100 mg/kg over 16 hours; this is a strong recommendation based on low-level evidence. For patients with initial acetaminophen concentration greater than double the nomogram line, the second bag in the 2-bag regimen should be doubled (i.e., 200 mg/kg IV NAC over 16 hours). Patients with initial acetaminophen concentration that is greater than or equal to triple the nomogram line may benefit from higher NAC doses; this is a strong recommendation based on low-level evidence. NAC should be continued if the concentration of acetaminophen is greater than 10 mg/L (66 µmol/L) or alanine transferase is elevated and increasing (> 50 units/L); this is a strong recommendation based on low-level evidence.
The UW Health guideline14 recommends enteral NAC regimens be preferred over IV regimens because the enteral regimen is equally efficacious and less expensive, unless the patient is unable to tolerate an enteral regimen; this is a strong recommendation based on high-level evidence. For IV administration, the NAC dosing is 150 mg/kg load over 1 hour, followed by a continuous infusion at 12.5 mg/kg/hour for 20 hours or more; this is a conditional recommendation based on low-level evidence. NAC treatment may be discontinued when acetaminophen concentration is below 10 mg/L and aspartate aminotransferase has decreased to less than 1,000 units/L; this is a conditional recommendation based on moderate-level evidence.
Limitations
This review did not identify any clinical utility studies or economic evaluation studies of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose, therefore no conclusions can be formed on these research questions. There were no significant methodological limitations of both included guidelines. The recommendations from the Australia and New Zealand guideline by Chiew et al. (2020)13 were mostly based on low-level evidence. Both included guidelines were conducted in Australia and New Zealand, and the US, and it is unclear whether the recommendations could be generalized to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 evidence-based guidelines13,14 regarding the administration of IV NAC for patients with acute acetaminophen overdose. No relevant evidence was identified regarding the clinical utility or cost-effectiveness of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose.
Both guidelines recommend a 2-bag NAC IV regimen for the management of acetaminophen overdose. The NAC dose and the length of infusion were slightly different between guidelines. For instance, the Australia and New Zealand guideline13 slows the loading dose of NAC (i.e., 200 mg/kg for 4 hours), while the UW Health guideline14 recommends a loading dose of 150 mg/kg over 1 hour. For continuous infusion, the guideline by Chiew et al. (2020)13 recommends 100 mg/kg over 16 hours, while the UW Health guideline14 recommends 12.5 mg/kg/hour for 20 hours or more. However, conditions for the discontinuation of NAC treatment in both guidelines were similar (i.e., acetaminophen concentration is below 10 mg/L or liver enzyme levels return to normal). For patients with acetaminophen concentration many times higher than the nomogram line, a threshold for acetaminophen toxicity in the Rumack-Matthew graph plotting serum acetaminophen concentration against hours after ingestion, the Australian and New Zealand guideline13 suggests an even higher doses of continuous infusion of NAC (i.e., 200 mg/kg for 16 hours, instead of 160 mg/kg for 16 hours). The UW Health guideline14 favours enteral NAC regimen over IV regimen, as the enteral regimen is equally efficacious and less expensive. The recommendations of 1 guideline13 were based on evidence the authors assessed as low quality, while those in the other guideline14 were based on a mix of evidence the authors assessed to be low to high quality.
CADTH previously published 2 Rapid Response reports: 116 on the clinical effectiveness and cost-effectiveness of point-of-care devices to measure acetaminophen toxicity, and the other17 on the evidence-based guidelines regarding the administration of IV NAC for patients with acute acetaminophen overdose in the pre-hospital setting. The first report16 identified 3 clinical studies on point-of-care tests, and no economic evaluations. The second report17 identified 1 guideline, which recommends NAC treatment for all patients experiencing acetaminophen overdose who were at risk of hepatotoxicity; however, this report did not include the strength of the recommendation, and it did not assess the strengths and limitations of the guideline. None of the previous CADTH reports examined the clinical utility of point-of-care devices that measure acetaminophen toxicity for patients with suspected overdose. Thus, there is a need for future research on the clinical utility and cost-effectiveness of point-of care devices for management of acetaminophen toxicity.
References
1.Acetaminophen. Drugs and Medical Devices 2016; https://www.canada.ca/en/health-canada/services/drugs-medical-devices/acetaminophen.html. Accessed 19 Jul 2021.
2.Agrawal S, Khazaeni B. Acetaminophen Toxicity. Treasure Island (FL): StatPearls Publishing; 2021: https://www.ncbi.nlm.nih.gov/books/NBK441917/. Accessed 19 Jul 2021.
3.Burns MJ, Friedman SL, Larson AM. Acetaminophen (paracetamol) poisoning in adults: Pathophysiology, presentation, and evaluation. 2021; https://www.uptodate.com/contents/acetaminophen-paracetamol-poisoning-in-adults-pathophysiology-presentation-and-evaluation.
4.ACETYLCYSTEINE SOLUTION: 200 mg/mL solution for injection or inhalation [product monograph]. Boucherville (QC): Sandoz; 7 Dec 2011: https://pdf.hres.ca/dpd_pm/00015046.PDF.
5.Taylor RR, Hoffman KL, Schniedewind B, Clavijo C, Galinkin JL, Christians U. Comparison of the quantification of acetaminophen in plasma, cerebrospinal fluid and dried blood spots using high-performance liquid chromatography-tandem mass spectrometry. J Pharm Biomed Anal. 2013;83:1-9. PubMed
6.Nagaraja P, Murthy KC, Rangappa KS. Spectrophotometric method for the determination of paracetamol and phenacetin. J Pharm Biomed Anal. 1998;17(3):501-506. PubMed
7.Vilchez JL, Blanc R, Avidad R, Navalón A. Spectrofluorimetric determination of paracetamol in pharmaceuticals and biological fluids. J Pharm Biomed Anal. 1995;13(9):1119-1125. PubMed
8.Speed DJ, Dickson SJ, Cairns ER, Kim ND. Analysis of paracetamol using solid-phase extraction, deuterated internal standards, and gas chromatography-mass spectrometry. J Anal Toxicol. 2001;25(3):198-202. PubMed
9.Dale C, Aulaqi AA, Baker J, et al. Assessment of a point-of-care test for paracetamol and salicylate in blood. Qjm. 2005;98(2):113-118. PubMed
10.Zhang Y, Huang Z, Wang L, et al. Point-of-Care Determination of Acetaminophen Levels with Multi-Hydrogen Bond Manipulated Single-Molecule Recognition (eMuHSiR). Anal Chem. 2018;90(7):4733-4740. PubMed
11.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 19 Jul 2021.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Chiew AL, Reith D, Pomerleau A, et al. Updated guidelines for the management of paracetamol poisoning in Australia and New Zealand. Med J Aust. 2020;212(4):175-183. PubMed
14.Acetylcysteine (N-acetylcysteine) - Adult/Pediatric - Inpatient/Emergency Department Clinical Practice Guideline. Madison (WI): UW Health; 2019: https://www.uwhealth.org/cckm/cpg/medications/Acetylcysteine-(N-acetylcysteine)---Adult-Pediatric---Inpatient-Emergency-Department-190729.pdf. Accessed 19 Jul 2021.
15.Heard KJ. Acetylcysteine for acetaminophen poisoning. N Engl J Med. 2008;359(3):285-292. PubMed
16.Point of Care Devices for Assessing Acetaminophen Toxicity. Ottawa (ON): CADTH; 2007: https://www.cadth.ca/media/pdf/htis/Point%20of%20Care%20Devices%20for%20Acetaminophen%20Toxicity.pdf. Accessed 19 Jul 2021.
17.N-Acetylcysteine for Acute Acetaminophen Overdose in the Pre-Hospital Setting: Guidelines. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/june-2015/RB0876%20Acetycysteine%20Infusion%20Final.pdf.
18.NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. Canberra (AU): National Health and Medical Research Council 2009: https://www.mja.com.au/sites/default/files/NHMRC.levels.of.evidence.2008-09.pdf. Accessed 19 Jul 2021.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
Chiew et al. (2020)13 | ||||||
Intended users: All health care providers involved in the management of acute acetaminophen overdose. Target population: Adult and pediatric patients with acetaminophen overdose. | NAC regimens for the management of acetaminophen poisoning. | Health benefits and side effects of NAC in protecting against acetaminophen toxicity. | The evidence from literature was systematically identified. | The level of evidence and the strength of recommendations were graded using GRADE methodology. The rating scheme for the strength of evidence and recommendations were not reported. | Members of the Treatment of Paracetamol Poisoning Writing group completed a detailed literature review and critically appraised the existing evidence. Drafts of the evidence-based recommendations were developed. The summary recommendations follow the NHMRC guidance18 | Externally peered reviewed. Published in a peer-reviewed journal. |
UW Health (2019)14 | ||||||
Intended Users: Physicians, advanced practice providers, pharmacists, and nurses Target Population: Adult and pediatric patients with acetaminophen overdose, with non-acetaminophen-induced acute liver failure, alcohol-induced liver failure, and at risk for contrast induced nephropathy. | NAC for appropriate indication and dosing. Different indications considered in this guideline include acetaminophen overdose, non-acetaminophen-induced acute liver failure, alcohol-induced liver failure, and at risk for contrast induced nephropathy. | Health benefits and side effects of NAC in protecting against acetaminophen toxicity. | The evidence from the literature was systematically identified, including RCT (high quality), observational study (low quality), and expert consensus (very low quality). Quality of evidence was assigned, and external factors were considered such as balance of benefits and harms, patient preferences, and cost-effectiveness. | The level of evidencea and the strength of recommendationsb are graded using GRADE methodology. | The guideline is managed by the centre for Clinical Knowledge Management, which regularly review the content to ensure up-to-date evidence. Clinicians and non-clinicians are involved in the development of the guideline. The recommendations were created via a consensus process. | The guideline was reviewed by external reviewers. Published in UW Health website. |
GRADE = Grades of Recommendation Assessment, Development and Evaluation; NAC = N-acetylcysteine; NHMRC = National Health and Medical Research Council; RCT = randomized controlled trial; UW = university of Wisconsin.
Note: this table has been formatted for accessibility but has not been copy-edited.
aLevel of evidence.
High = We are confident that the effect in the study reflects the actual effect.
Moderate = We are quite confident that the effect in the study is close to the true effect, but it is also possible it is substantially different.
Low = The true effect may differ significantly from the estimate.
Very low = The true effect is likely to be substantially different from the estimated effect.”14 (p. 11)
bStrength of recommendations.
Strong = The net benefit of the treatment is clear; patient values and circumstances are unlikely to affect the decision.
Conditional = Recommendation may be conditional upon patient values and preferences, the resources available, or the setting in which the intervention will be implemented.”14 (p. 11)
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II11
Item | Chiew et al. (2020)13 | UW Health (2019)14 |
Domain 1: Scope and Purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder Involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of Development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes |
Domain 4: Clarity of Presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No |
Domain 6: Editorial Independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; UW = university of Wisconsin.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has been formatted for accessibility but has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
Chiew et al. (2020)13 | |
“A two-bag acetylcysteine regimen slows the initial loading dose and simplifies the protocol (i.e., 200 mg/kg over 4 h followed by 100 mg/kg over 16 h). This is widely used in toxicology units around Australia and has been shown to significantly reduce the rates of adverse reactions.”13 (p. 176) Evidence supporting this recommendation came from 4 observational studies and 1 conference abstract on the efficacy of 2-bag NAC regimen to treat acetaminophen overdose. | Level of evidence: Low Strength of recommendation: Strong |
“Those with an initial paracetamol concentration greater than double the nomogram line may benefit from an increased dose of acetylcysteine. The second bag in the two-bag acetylcysteine regimen should be doubled to 200 mg/kg intravenous acetylcysteine over 16 hours (instead of 100 mg/kg over 16 h). Patients with even higher concentrations (e.g., ≥ triple the nomogram line) may benefit from even higher acetylcysteine doses. These patients should be discussed with a clinical toxicologist or a Poisons Information Centre.”13 (p. 176) This recommendation was developed based on evidence from a narrative review of acetaminophen and NAC dose and duration and an observational study assessing the effect of increased NAC dose for treatment of massive acetaminophen overdose. | Level of evidence: Low Strength of recommendation: Strong |
“Acetylcysteine should be continued if the paracetamol concentration is greater than 10 mg/L (66 µmol/L) or ALT is elevated (> 50 U/L) and increasing (if baseline ALT > 50 U/L).”13 (p. 176) Three narrative reviews and 1 observational study provided evidence for this recommendation. The observational study assessed a dose-dependent relationship between plasma acetaminophen concentration and liver injury despite prompt treatment with NAC. | Level of evidence: Low Strength of recommendation: Strong |
UW Health (2019)14 | |
“N-acetylcysteine should be used in the management of acetaminophen overdose for adults and pediatrics.”14 (p. 5) This recommendation was developed based on evidence from 2 narrative reviews, including an UptoDate review. | Level of evidence: High Strength of recommendation: Strong |
“It is reasonable to use enteral N-acetylcysteine regimens preferentially over intravenous regimens, unless a patient is unable to tolerate an enteral regimen, as the enteral regimen is equally efficacious and less expensive.”14 (p. 5) Three narrative reviews and 1 observational study on the efficacy of oral NAC vs. IV NAC provided evidence for this recommendation. | Level of evidence: Moderate Strength of recommendation: Conditional |
“For the management of acetaminophen overdose, N-acetylcysteine should be dosed on actual weight up to a maximum of 100 kg for IV administration”14 (p. 5) This recommendation was developed based on evidence from 1 UptoDate review. | Level of evidence: High Strength of recommendation: Strong |
“Administration (of N-acetylcysteine) should be initiated within 8 hours of ingestion or as soon as after ingestion (of acetaminophen).”14 (p. 5) Two narrative reviews and 1 clinical policy in the management of patients with acetaminophen overdose presenting to the emergency department provided evidence for this recommendation. | Level of evidence: High Strength of recommendation: Strong |
“If ingestion time is unknown or there have been multiple acetaminophen ingestions, N-acetylcysteine should be administered if there is any evidence to suggest significant acetaminophen overdose and detectable acetaminophen levels or any degree of transaminitis.”14 (p. 5) This recommendation was developed based information from 2 narrative reviews and 1 clinical policy in the management of patients with acetaminophen overdose presenting to the emergency department. | Level of evidence: Low Strength of recommendation: Strong |
“IV N-acetylcysteine dosing is 150 mg/kg load over one hour, followed by a continuous infusion at 12.5 mg/kg/hr for 20 hours or more.”14 (p. 6) This recommendation was developed based on evidence from 1 narrative review on NAC dosing recommendations in acetaminophen toxicity and 1 observational study on the effect of increased NAC dose for massive acetaminophen overdose. | Level of evidence: Low Strength of recommendation: Conditional |
“N-acetylcysteine treatment discontinuation may be considered when a single acetaminophen concentration is below 10 mcg/mL and AST has decreased to fewer than 1,000 units/L.”14 (p. 6) Evidence from 1 narrative review and 1 observational study on the duration of NAC therapy for acute acetaminophen overdose provided evidence for the development of this recommendation. | Level of evidence: Moderate Strength of recommendation: Conditional |
APAP = N-acetyl-p-aminophenol; ALT = alanine aminotransferase; AST = aspartate aminotransferase; GRADE = Grades of Recommendation Assessment, Development and Evaluation; NAC = N-acetylcysteine; UW = university of Wisconsin.
Appendix 5: References of Potential Interest
Previous CADTH Reports
1.Point of Care Devices for Assessing Acetaminophen Toxicity. Ottawa (ON): CADTH; 2007: https://www.cadth.ca/media/pdf/htis/Point%20of%20Care%20Devices%20for%20Acetaminophen%20Toxicity.pdf. Accessed 19 Jul 2021.
2.N-Acetylcysteine for Acute Acetaminophen Overdose in the Pre-Hospital Setting: Guidelines. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/june2015/RB0876%20Acetycysteine%20Infusion%20Final.pdf. Accessed 19 Jul 2021.
Additional References
3.BC Emergency Medicine Network. Acetaminophen Overdoses. Point-of-care emergency clinical summary. 2020; https://www.bcemergencynetwork.ca/clinical_resource/acetaminophen-overdoses/. Accessed 19 Jul 2021.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca