CADTH Health Technology Review
Newer Biologics for the Treatment of Plaque Psoriasis
Rapid Review
Authors: Anusree Subramonian, Melissa Walter
Abbreviations
IL
interleukin
PASI
Psoriasis Area Severity Index
NMA
network meta-analysis
RCT
randomized controlled trial
TNF
tumour necrosis factor
Key Messages
Eight systematic reviews with network meta-analysis were identified that compared newer biologics with older biologics in patients with moderate-to-severe plaque psoriasis. There was extensive overlap of primary studies across the systematic reviews and network meta-analyses.
Newer biologics such as secukinumab, ixekizumab, brodalumab and risankizumab were more favourable compared to older biologics (adalimumab, etanercept, and ustekinumab) in reaching 90% or 100% skin clearance, as measured with the Psoriasis Area Severity Index. The risk of side effects was similar between the newer and older biologics.
Context and Policy Issues
Psoriasis is an immune-mediated chronic inflammatory condition affecting the skin, joints, and other systems of the body.1 Plaque psoriasis is the most common type of psoriasis in which inflamed erythematous scaly patches of skin are formed that result in itching, redness and pain. It also often associated with a lower quality of life and can have psychosocial effects. Psoriasis patients are at higher risk of developing other chronic conditions such as cardiovascular disorders, Crohn disease, lymphoma, anxiety, and depression.1 Approximately 1 million Canadians are affected with psoriasis.2 The economic burden of moderate-to-severe plaque psoriasis has been estimated as $1.7 billion annually.3
The diagnosis of psoriasis is made based on clinical findings and the Psoriasis Area Severity Index (PASI) score is used to grade the severity of the disease based on induration, erythema, and scaling.1,4 Management of psoriasis comprises several forms of treatment, often requiring lifelong treatment. The first line of treatment includes topical medications, phototherapy, and oral anti-inflammatory medications. Patients who do not respond to first-line treatment are given systemic therapy with biologic drugs, or conventional therapies. Biologic drugs include monoclonal antibodies and fusion proteins, which are derived from living systems. As they have fewer adverse events compared to conventional therapies, they can be used for long-term treatment.5 The first class of biologic drugs approved for plaque psoriasis were tumour necrosis factor (TNF)–alpha inhibitors such as adalimumab, etanercept, and infliximab; and interleukin (IL)-12 and IL-23 inhibitor such as ustekinumab.1 Since then, several other biologic drugs known as “newer biologics” have been developed. They include anti–IL-17 drugs (e.g., secukinumab, ixekizumab, brodalumab) and anti–IL-23 drugs (e.g., risankizumab, tildrakizumab, guselkumab).5 CADTH has previously reviewed and recommended newer biologic drugs including secukinumab (in 2014),6 ixekizumab (in 2016),7 brodalumab (in 2018),8 and risankizumab (in 2019)9 for the treatment of moderate-to-severe plaque psoriasis.
Many older biologics that are used today have met or are approaching loss of data exclusivity (patent expiry and/or expiry of data protection) after which biosimilar drugs could be used interchangeably. Because of the complex molecular structures, proprietary manufacturing process, and regulatory issues, the development of biosimilars for these drugs is challenging.10 In Canada, an adalimumab biosimilar has only been recently approved11 for psoriasis and those of etanercept and ustekinumab have not been listed. Biologic drugs are also 1 of the highest expenditures in public drug programs. For example, anti-TNF alpha drugs accounted for $ 1,233.9 million in total provincial spending in 2019, making it the drug class with the highest proportion of public drug program spending.12 With the arrival of newer biologics that are reported to be more cost-effective than the older biologics,13,14 a reassessment of place in therapy for biologic drugs plays a key role in formulary management strategies. This could improve patient outcomes, with reduced expenditure. The objective of this report is to summarize the evidence regarding the clinical effectiveness of newer biologic drugs compared to older biologic drugs in patients with moderate-to-severe plaque psoriasis. This report is being produced as part of a larger project at CADTH evaluating the place in therapy for biologics in moderate-to-severe plaque psoriasis and includes a clinical report, utilization study, and environmental scan. This report will summarize and critically appraise the relevant evidence identified from a CADTH refence list.15
Research Question
What is the clinical effectiveness of newer biologics compared to older biologics in patients with plaque psoriasis?
Methods
Literature Search Methods
A limited literature search was conducted for a previous CADTH report15 by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were newer biologics (secukinumab, ixekizumab, brodalumab, or risankizumab) and psoriasis. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, or guidelines. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. The search was also limited to English-language documents published between January 1, 2016 and June 9, 2021. Internet links were provided, where available.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (18 years of age or older) with moderate-to-severe plaque psoriasis |
Intervention | The following newer biologics:
|
Comparator | The following older generation biologics
|
Outcomes | Clinical effectiveness (PASI 100, PASI 90), safety (adverse events, serious adverse events) |
Study designs | Health technology assessments and systematic reviews |
IL = interleukin; PASI = Psoriasis Area Severity Index; TNF = tumour necrosis factor.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2020. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for systematic reviews and “Questionnaire to assess the relevance and credibility of a network meta-analysis”17 for NMAs. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
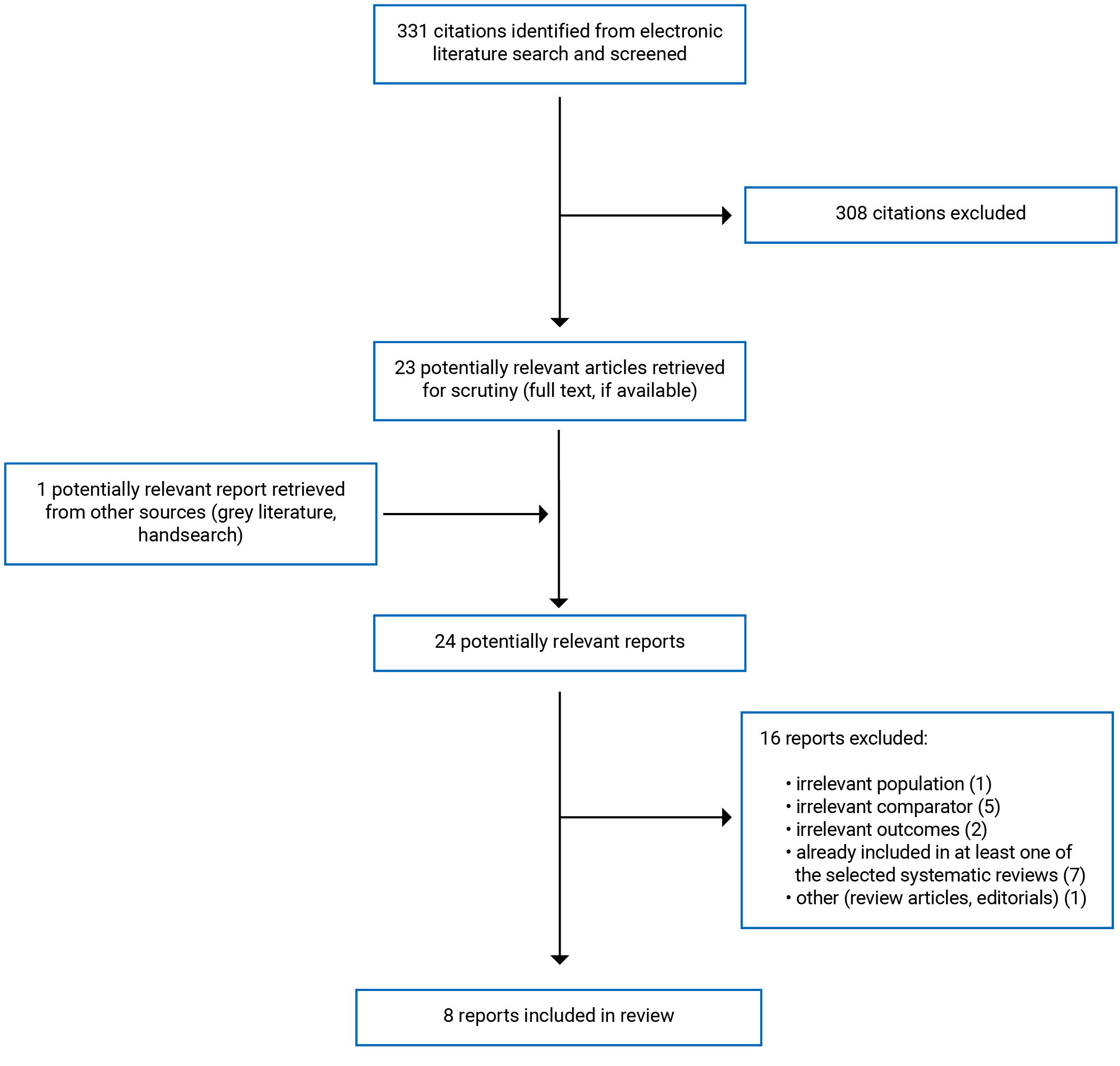
A total of 331 citations were identified in the literature search. Following screening of titles and abstracts, 308 citations were excluded and 23 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 16 publications were excluded for various reasons and 8 publications met the inclusion criteria and were included in this report. These comprised 8 systematic reviews with network meta-analyses.18-25 Appendix 1 presents the PRISMA26 flow chart of the study selection.
Summary of Study Characteristics
Eight systematic reviews with NMA were included in this report.18-25 Four of them were published in 202118-21 and 4 in 2020.22-25 One of the included reviews was a Cochrane living systematic review,20 which means that the authors will continually update the review as new evidence becomes available. The characteristics and results from the version of this living systematic review20 that was most up-to-date at the time this report was produced (i.e., April 2021) are summarized in the current report. Three systematic reviews were updates of previously published reviews.21,22,25
All of the included systematic reviews had broader inclusion criteria than the present review in terms of their interventions and comparators of interest. For example, the Cochrane living systematic review20 considered all systemic treatments for psoriasis, irrespective of dose and duration of treatment, as eligible for inclusion. Therefore, all included NMAs had additional network comparisons beyond those of interest to the present review. They included comparisons between different types of biologic drugs that are relevant to the present report (e.g., anti–TNF-alpha drugs, anti–IL-17 drugs), non-biologic systemic treatments that are non-relevant to this report (e.g., methotrexate, fumaric acid esters, Janus kinase inhibitors), as well as placebo. Only the characteristics and results relevant to the current report, as listed in Table 1, will be summarized in the following sections.
Lastly, 4 systematic reviews19,21-23 were sponsored by pharmaceutical companies and 3 systematic reviews18,20,24 were funded by institutional grants. One review25 was conducted on behalf of the British Association of Dermatologists as an evidence base to produce treatment guidelines.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
All included publications were systematic reviews with NMA. The search strategies were comprehensive, with multiple electronic databases (e.g., Embase, MEDLINE, Cochrane Central Register of Controlled Trials) searched in all systematic reviews.18-25 Other sources such as bibliographies, trial registries, and conference proceedings were searched in 2 reviews.19,20 Two systematic reviews searched for studies published until 202020,21 and 3 systematic reviews searched for studies published until 2019.18,22,24 In 2 systematic reviews, studies published until 201825 and 201723 were captured. The search date was unclear in 1 systematic review.19 In 6 systematic reviews, eligible primary studies were limited to randomized controlled trials (RCTs).18-21,23,24 One systematic review25 included cohort studies in addition to RCTs and another systematic review included long-term extension studies, as well as RCTs.22 The number of primary studies included in the systematic reviews ranged from 1424 to 158.20 There was extensive overlap of included primary studies across the systematic reviews. In 7 systematic reviews,18,19,21-25 more than 85% (range 86% to 98%) of the primary studies were included in 1 or more of the other systematic reviews. In the Cochrane living systematic review,20 which had broader inclusion criteria than the other systematic reviews, 53% of the primary studies overlapped in 1 or more of the other systematic reviews.
Indirect evidence from NMAs was reported in all systematic reviews.18-25 Six systematic reviews18,19,21-24 used a Bayesian approach for the NMA and 2 systematic reviews used frequentist methods for the NMA.20,25 Direct evidence from pairwise meta-analysis was reported in 3 of the included systematic reviews.18,20,24
Country of Origin
The systematic reviews were authored by reviewers from Canada,19,23 China,18,24 France,20 the UK,22,25 and the US.21
Patient Population
The population of interest in 6 systematic reviews were patients with moderate-to-severe plaque psoriasis.18,19,21-25 The Cochrane living systematic review included all patients with moderate-to-severe plaque psoriasis or psoriatic arthritis with moderate-to-severe skin involvement and were at any stage of treatment.20 One review considered all patients (irrespective of age) with moderate-to-severe psoriasis who were treated primarily for their skin disease, although all of the included studies were conducted among adults with moderate-to-severe plaque psoriasis.25
The total number of patients included in the NMAs ranged from 8,40224 to 57, 831.20 The number of participants in the NMA were not reported in 4 reviews.18,19,21,22 Four systematic reviews18,20,24,25 reported an overall mean age of 45 years and 2 systematic reviews reported the mean age by RCT (range from 39.2 to 51).22,23 In 5 systematic reviews, more than half of the patient population were males.20,22-25 Patient characteristics in the included studies were not reported in 2 systematic reviews.19,21 Mean baseline PASI scores of patients in the primary studies were reported in 5 systematic reviews18,20,23-25 and ranged from 8 to 30 across the RCTs in the review by Mahil et al.25 and from 9.5 to 39 in the RCTs in the Cochrane review.20
Interventions and Comparators
All included systematic reviews considered a range of biologic and non-biologic treatments eligible for their review. The interventions and comparators relevant to the current report are subsequently summarized.
The anti–IL-17 drugs, secukinumab, ixekizumab, and brodalumab were considered as interventions of interest in 7 systematic reviews.18-23,25 The anti–IL-23 drug risankizumab was considered in 7 reviews.18-22,24,25
As for the comparators, the anti-TNF alpha drugs adalimumab and etanercept were considered in 7 systematic reviews.18-23,25 The anti–IL-12 and anti–IL-23 drug ustekinumab was considered in all systematic reviews.18-25
Four19,21-23 systematic reviews included only approved or licensed doses of these drugs, whereas 3 reviews included the drugs irrespective of dosage.18,20,25 In 3 systematic reviews,19-21 multiple doses of ustekinumab (45 mg, 90 mg, or weight-based dose [45 mg if weight is 100 kg or less, 90 mg if weight is more than 100 kg]) were grouped together in the analysis, whereas in 1 review,24 they were compared separately. In 3 systematic reviews,22,23,25 only the weight-based dosage, which is the licensed dosage of ustekinumab in Canada, was considered. The dose of ustekinumab was unclear in 1 systematic review.18 Similarly, in the systematic review by Shi et al.,24 18 mg, 75 mg, 90 mg, 150 mg, and 180 mg doses of risankizumab were compared separately in the NMA. In Canada, the approved dose of risankizumab is 150 mg.27
Outcomes
PASI is a tool used to assess and grade the severity of psoriatic lesions. It is determined by grading the severity of erythema, induration, scale, and area of involvement.28 PASI is reported as a score from 0 to 72. The percentage change in PASI from baseline (PASI response) is used in clinical trials to indicate the magnitude of improvement after treatment.4,29 PASI 100, a 100% improvement from baseline, is also called complete clearance.29 Higher PASI responses are found to be associated with improvements in health-related quality of life.30 PASI 90 and PASI 100 response rates refer to the proportions of patients who achieved a 90% and a 100% reduction in PASI score compared to baseline, respectively.
Among the included systematic reviews, a PASI 90 response rate was reported in 7 reviews18,20-25 and a PASI 100 response rate was reported in 3 reviews.21-23
Safety outcomes relevant to the current report were the occurrence of any adverse events or any serious adverse events. The former was reported in 3 systematic reviews18,19,24 and the latter in 2 systematic reviews19,20
Treatment outcomes were measured after short-term (end of induction phase) and long-term (end of maintenance phase) treatment. The induction phase is the treatment period up to 16 weeks after start, although the induction phase can last up to 24 weeks depending on the type of drug.31 Long-term or maintenance phase outcomes are measured after 48 to 52 weeks of treatment. Among the included systematic reviews, 7 reviews18-21,23-25 reported short-term outcomes (10 to 16 weeks18,19,21,23-25 or 8 to 24 weeks20) and 4 reviews19-22 reported long-term or maintenance phase outcomes.
Summary of Critical Appraisal
The included systematic reviews with NMAs were critically appraised using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for systematic reviews and “Questionnaire to assess the relevance and credibility of a network meta-analysis”17 for network meta-analyses as a guide. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Relevance
The included systematic reviews18-25 had clearly defined objectives and inclusion criteria that included components of population, interventions, comparators, and outcomes, all of which were relevant to the current report. As the included reviews had broader inclusion criteria than the current report in the interventions and comparators, all included NMAs had additional network comparisons beyond those of interest to the current review. In the Cochrane living systematic review,20 studies of patients with moderate-to-severe plaque psoriasis (relevant to this report), as well as those with psoriatic arthritis with moderate to-severe skin involvement (not relevant to the current report), were considered eligible. It was unclear whether the inclusion of a broader population could have affected the overall results with respect to the current report.
Credibility
The review methods were registered and established a priori in 3 reviews.19,20,25 The Cochrane systematic review20 was conducted as a living review, with a pre-established protocol. Any changes or deviations from the protocol and the rationale for these changes were clearly reported and justified in 2 reviews.20,25 However, in 5 reviews it was unclear whether a protocol was published before the conduct of the review.18,21-24 In the absence of a published protocol, it could not be independently assessed whether there were any important deviations from the protocol that could have introduced risks of bias. Considering the review design and objectives, most of the reviews appropriately included only RCTs.18-21,23,24 A comprehensive search to identify eligible studies was conducted in the reviews.18-25 Multiple electronic databases were searched in all reviews18-25 and additional sources such as trial registries and bibliographies were searched in 2 reviews.19,20 In 7 reviews, the literature search was conducted within 24 months before the publication of the review and the key search words and strategies were reported.19-25 In 1 review published in 2020, the search was conducted in 201723; therefore, relevant trials published after 2017 would not be included in this systematic review. In the same review, keywords and search strategies were not reportedl.18 A list of excluded studies, together with reasons for exclusion, was reported in 3 reviews.20,22,25 There was a low risk of publication bias reported by 4 reviews18,20,24,25 using funnel plots18,20,24,25 or Egger’s test.18 In 4 reviews, it was unclear whether publication bias was examined.19,21-23
Study selection and data extraction from the included studies were done by 2 reviewers, independently, in 4 reviews.18,20,24,25 Any discrepancies were resolved through discussion with a third reviewer. This approach lowers the risk of errors and ensures eligible studies are not missed. In 1 review, the second reviewer did a data check on 50% of the studies selected by the first reviewer.22 In 3 reviews, it was unclear whether study selection and data extraction were done in duplicate.19,21,23 Sources of funding for the individual studies were reported in 2 reviews.20,25 Most of the primary studies were funded by pharmaceutical companies, as reported in the Cochrane review.20
Risk of bias assessment of the included studies were conducted using acceptable instruments in 5 reviews.18,20,22,24,25 Risk of bias assessment of the primary studies were conducted using the Cochrane risk of bias tool in 3 reviews,20,22,24 the modified Jadad scale in 1 review,18 and the NICE checklist in 1 review.25 They found that the RCTs were, in general, of low to medium risk of bias. In 3 reviews, it was unclear whether a quality assessment of the individual studies was done.19,21,23 A high risk of bias in the individual studies could lower the internal validity of the overall result.
The internal validity of an NMA is affected by potential effect modifiers and their distribution across the primary studies. Patient factors such as age, weight, duration of disease, disease severity (measured as baseline PASI score), and prior treatment are some of the potential effect modifiers relevant to this report. The details of included primary studies such as clinical characteristics and demographics of patients, dose and treatment duration of interventions, and outcomes were reported in 5 reviews.18,20,22,24,25 In the 3 reviews in which they were not reported,19,21,23 an assessment of between-study heterogeneity and the distribution of the potential effect modifiers was not possible.
Analysis
All included systematic reviews combined the findings from the primary studies using NMA. Six systematic reviews18,19,21-24 reported indirect evidence using a Bayesian approach for the NMA and 2 used frequentist methods for the NMA.20,25 Network diagrams of the included studies were reported for each NMA. Individual interventions and comparators, including placebo, were considered in separate nodes that formed an interconnected network.18-25 Networks for the short-term treatments were full, whereas the networks for some of the effects of long-term treatment (e.g., PASI 100 after long-term treatment) were relatively sparse because of the low number of trials identified.19,21,22
In the Bayesian NMAs, most of the NMAs were conducted using both fixed and random effects models.18,19,21-24 For the networks for the short-term treatment, random effects models were used.18,19,21-24 In the networks for long-term treatment in 2 reviews, a fixed-effects model was used because of a sparse network.19,21 Residual deviance and deviance information criterion were used to determine which model to choose.18,22,23 Vague or noninformative priors were used in 3 reviews,19,21,23 which, together with a random-effects model, could result in more conservative estimates.32 Informative priors, drawn from PASI responses in individual trials, were used in 1 review.22 In 2 reviews, it was unclear whether informative or noninformative priors were used.18,24
In 3 reviews, pairwise meta-analyses were conducted and direct comparative evidence between interventions and comparators was reported.18,20,24 The results from direct and indirect evidence were generally consistent in these reviews. The number of RCTs contributing to each of the pairwise analyses, effect sizes, and heterogeneity (I2), were reported. Consistency between direct and indirect results were evaluated in the reviews using various methods such as loop-specific approach (the Bucher method),20,22,25 node segmentation,24 back calculations,23 or by visual inspection of the forest plots.25 Inconsistencies between direct and indirect evidence were not investigated in 2 reviews.19,21
Heterogeneity in NMAs result from factors such as differences in population characteristics or treatment duration between the primary studies included in the network. High heterogeneity between trials could lower the internal validity of results of the NMA. Heterogeneity was assessed using qualitative methods,22,23 Cochran’s Q test,24 visual inspection,25 or using the heterogeneity variance parameter (Tau squared).20 In the review by Armstrong et al., a reference arm adjustment was used to account for possible between-trial heterogeneity.21 Meta-regression analyses or sensitivity analyses were conducted using prespecified covariates to minimize the effects of heterogeneity in 6 reviews.18,20,22-25 In 2 reviews, it was unclear whether heterogeneity was assessed or if meta-regression analyses were conducted.19,21 It is possible that 1 or more of potential sources of heterogeneity were not adjusted for in the analysis. For example, in the review by Mahil et al.,25 a subgroup analysis including licensed doses of drugs was conducted; however, other possible factors were not adjusted for. “Equal heterogeneity” between the comparators was assumed.25
In all included NMAs, trials with up to 1618,19,21,23-25 or 2420 weeks of treatments were grouped in the short-term networks and those with 48 to 52 weeks19-22 of treatment were grouped in long-term networks. It is possible that these within-network differences in follow-up time introduced some heterogeneity. In the Cochrane living review,20 all doses of eligible interventions were pooled together, whereas in other reviews,19,21-23,25 either only licensed doses were considered or different doses were allocated separate nodes in the network.21,24,25 In the NMA by Xue et al.,23 a multinomial likelihood NMA model was used in which all outcomes (PASI 75, PASI 90, PASI 100) were grouped in the same network rather than analyzing them in separate NMAs. The relative treatment effects of 1 PASI end point could be affected by response level at other PASI end points. In the NMA by Yasmeen et al.,22 a separate NMA was conducted including long-term extension studies. In studies in which the placebo arm was switched to active therapy in the extension study, it was assumed that placebo response in the induction phase will continue to the maintenance phase. The validity of this assumption is unclear.
Reporting Quality
The reporting quality of the included reviews were generally good. PRISMA flow diagrams were reported to show the study selection process.18-25 Results of individual studies were not reported in 7 reviews.18-21,23-25 Forest plots for direct comparisons and network diagrams for NMAs were reported.18-25 All results of direct and indirect comparisons were reported, together with appropriate measures of uncertainty (95% confidence intervals of frequentist NMAs20,25 and 95% credible intervals for Bayesian NMAs).18,19,21-24 Overall conclusions were balanced and discussed in light of limitations.
Conflicts of Interest
Half of the included reviews were sponsored by pharmaceutical companies that manufactures biologic therapy drugs.19,21-23 Review authors indicated conflicts of interests such as receiving funding from the pharmaceutical companies.
Summary of Findings
The clinical effectiveness of the relevant anti–IL-17 drugs (secukinumab, ixekizumab, and brodalumab) and the anti–IL-23 drug (risankizumab) compared with anti-TNF drugs (adalimumab and etanercept) and the anti–IL-12 and anti–IL-23 drug (ustekinumab) are subsequently summarized. Short-term results refer to those obtained after the induction phase (up to 16 or 24 weeks) of treatment. Long-term results refer to those obtained after the maintenance phase (48 to 52 weeks) of treatment.
The direct and indirect comparison results are summarized for each of the interventions separately. Direct comparison results are from pairwise meta-analysis of head-to-head trials reported in the systematic reviews. The evidence for direct comparisons may have been reported in more than 1 systematic review but are only summarized once in this report.
Indirect results are from NMAs. There was extensive overlap in the primary studies that were included in the NMAs (53% to 98% overlap); the pooled estimates from separate NMAs thus contain some of the same data.
Appendix 4 presents the main study findings from the included reviews
Clinical Effectiveness of Secukinumab
PASI 90 Response Rate (Short-Term)
No relevant direct comparative evidence regarding secukinumab and adalimumab was identified for the outcome PASI 90. Indirect evidence from 4 NMAs found that secukinumab was favourable to adalimumab in reaching a PASI 90 response with short-term treatment.18,20,21,25
Direct evidence from 1 RCT found that the likelihood of achieving a PASI 90 response was statistically significantly higher in the secukinumab group compared to the etanercept group.20 Indirect evidence from 4 NMAs suggested that secukinumab was favourable to etanercept in reaching PASI 90 with short-term treatment.18,20,21,25
Direct evidence from 2 RCTs found that the likelihood of achieving a PASI 90 response was statistically significantly higher in the secukinumab group compared to the ustekinumab group.20 Four systematic reviews with NMA reported indirect comparative results of secukinumab versus ustekinumab. Secukinumab was favourable to ustekinumab (all doses) in reaching PASI 90 with short-term treatment.18,20,21,25
PASI 90 Response Rate (Long-Term)
No relevant direct evidence regarding secukinumab versus adalimumab or etanercept was identified for the outcome PASI 90 response after long-term treatment. Direct evidence for secukinumab versus ustekinumab from 2 RCTs was reported in 1 systematic review, which found that secukinumab was associated with a better likelihood of reaching PASI 90 than ustekinumab after long-term treatment.20 Two systematic reviews with NMA reported indirect comparative results of secukinumab versus these 3 drugs. Secukinumab was favourable to adalimumab, to etanercept, and to ustekinumab in reaching PASI 90 after long-term treatment.21,22
PASI 100 Response Rate (Short-Term)
No relevant direct evidence regarding secukinumab versus adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response after short-term treatment. Indirect evidence from 2 NMAs21,23 showed that secukinumab was favourable to adalimumab, to etanercept, and to ustekinumab (all doses) in reaching PASI 100 after short-term treatment.
PASI 100 Response Rate (Long-Term)
No relevant direct evidence regarding secukinumab versus adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response rate after long-term treatment. Indirect evidence from 2 NMAs showed that secukinumab was favourable compared to adalimumab, etanercept, and ustekinumab (all doses) in achieving PASI 100 after long-term treatment.21,22
Adverse Events (Short-Term)
No relevant direct comparative evidence regarding secukinumab and adalimumab was identified. Indirect evidence from 3 systematic reviews with NMAs suggested that no therapy was favoured regarding the risk of adverse events when secukinumab was compared to adalimumab after short-term treatment.18-20
Direct evidence from 1 RCT reported in a systematic review found that there was no difference in the risk of adverse events when the secukinumab group was compared to the etanercept group.20 Indirect evidence from 3 systematic reviews with NMAs suggested that the risk of adverse events after short-term treatment with secukinumab therapy was not different compared to that with etanercept.18-20
Direct comparison results for secukinumab versus ustekinumab from 2 RCTs was reported in a systematic review.20 There was no difference in the risk of adverse events when the secukinumab group was compared to the ustekinumab group. Indirect evidence from 3 NMAs suggested that no therapy was favoured when comparing the risk of adverse events of secukinumab to that of ustekinumab after short-term treatment.18-20
Adverse Events (Long-Term)
No relevant direct comparative evidence regarding secukinumab and adalimumab, etanercept, or ustekinumab were identified. Indirect evidence from a systematic review with NMA suggested that the risk of adverse events of secukinumab was not different compared to that of adalimumab or ustekinumab after long-term treatment.19 No relevant direct or indirect comparative evidence regarding secukinumab and etanercept was identified; therefore, no summary can be provided.
Serious Adverse Events (Short-Term)
No relevant direct comparative evidence regarding secukinumab and adalimumab was identified. Indirect evidence from 2 systematic reviews with NMAs suggested that the risk of serious adverse events with secukinumab was not different compared to that of adalimumab after long-term treatment.19,20
Direct comparison results for secukinumab versus etanercept from 1 RCT was reported in a systematic review.20 There was no difference in the risk of experiencing a serious adverse event between the secukinumab group and the etanercept group. Indirect evidence from 2 systematic reviews with NMAs suggested that the risk of serious adverse events with secukinumab was not different compared to etanercept after long-term treatment.18-20
Direct comparison results for secukinumab versus ustekinumab from 2 RCTs was reported in a systematic review.20 The risk of serious adverse events was not different between the secukinumab group and the ustekinumab group. Indirect evidence from 2 systematic reviews with NMAs suggested that the risk of serious adverse events with secukinumab was not different compared to ustekinumab after long-term treatment.19,20
Serious Adverse Events (Long-Term)
No relevant direct comparative evidence regarding secukinumab and adalimumab, etanercept, or ustekinumab were identified. A systematic review with NMA reported indirect comparative results of secukinumab versus adalimumab and ustekinumab.19 The risk of serious adverse events with secukinumab was not different than that of adalimumab or of ustekinumab after long-term treatment. No relevant direct or indirect comparative evidence regarding secukinumab and etanercept was identified; therefore, no summary can be provided.
Clinical Effectiveness of Ixekizumab
PASI 90 Response Rate (Short-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab was identified for the outcome PASI 90. Four systematic reviews with NMA reported indirect comparative results of ixekizumab versus adalimumab.18,20,21,25 Ixekizumab was favourable to adalimumab at reaching PASI 90 after short-term treatment.
Direct evidence from 2 RCTs showed that ixekizumab was associated with a statistically significantly higher likelihood of achieving PASI 90 compared to etanercept.20 Indirect evidence from 4 systematic reviews with NMA suggested that ixekizumab was favourable to etanercept in reaching PASI 90 with short-term treatment.18,20,21,25
Direct evidence from 1 RCT showed that the likelihood of achieving PASI 90 was statistically significantly higher in the ixekizumab group compared to the ustekinumab group.20 Indirect evidence from 4 NMAs18,20,21,25 suggested that ixekizumab was favourable to ustekinumab (all doses) in reaching PASI 90 response with short-term treatment.
PASI 90 Response Rate (Long-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab or etanercept was identified for the outcome PASI 90 after long-term treatment. Indirect evidence from 2 systematic reviews with NMA suggested that ixekizumab was favourable compared to adalimumab, as well as to etanercept, in reaching PASI 90 after long-term treatment.21,22
Direct evidence from 1 RCT as reported in 1 systematic review20 showed that ixekizumab was associated with a statistically significantly higher likelihood of achieving PASI 90 compared to ustekinumab. Indirect evidence from 2 NMAs suggested that ixekizumab was favourable to ustekinumab in reaching PASI 90 with long-term treatment.21,22
PASI 100 Response Rate (Short-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response after short-term treatment. Two systematic reviews with NMA reported indirect comparative results of ixekizumab versus these 3 drugs.21,23 Ixekizumab was found to be favourable to adalimumab, to etanercept, and to ustekinumab (all doses) in reaching PASI 100 after short-term treatment.21,23
PASI 100 Response Rate (Long-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab, etanercept, or ustekinumab was identified for this outcome. Indirect evidence from 2 NMAs21,22 suggested that ixekizumab was favourable to adalimumab, etanercept, and ustekinumab in reaching PASI 100 after long-term treatment.
Adverse Events (Short-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab was identified. Indirect evidence from 3 NMAs suggested that the risk of adverse events with ixekizumab was not different from that of adalimumab after short-term treatment.18-20
Direct evidence from 2 RCTs as reported in a systematic review20 showed that the risk of adverse events in the ixekizumab group and the etanercept group were not significantly different. Indirect evidence from 3 systematic reviews with NMAs suggested that the risk of adverse events with ixekizumab was not different than that of etanercept after short-term treatment.18-20
Direct evidence from 1 RCT as reported in a systematic review20 showed that the risk of adverse events in the ixekizumab group and the ustekinumab group were not significantly different. Indirect evidence from 3 systematic reviews with NMAs suggested that the risk of adverse events with ixekizumab was not different than that of ustekinumab after short-term treatment.18-20
Adverse Events (Long-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab, etanercept, or ustekinumab were identified. A systematic review with NMA reported indirect comparative results of ixekizumab versus adalimumab and ustekinumab.19 The risk of adverse events with ixekizumab was not different than that of adalimumab or ustekinumab after long-term treatment. No relevant direct or indirect comparative evidence regarding ixekizumab and etanercept was identified; therefore, no summary can be provided.
Serious Adverse Events (Short-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab was identified. Indirect evidence from 2 systematic reviews with NMAs suggested that the risk of serious adverse events with ixekizumab was not different than that of adalimumab after long-term treatment.19,20
Direct evidence from 2 RCTs (reported in a systematic review20) showed that the risk of adverse events in the ixekizumab group and the etanercept group were not significantly different. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with ixekizumab was not different compared to etanercept after long-term treatment.18-20
Direct evidence from 1 RCT as reported in a systematic review20 showed that the risk of adverse events in the ixekizumab group and the ustekinumab group were not significantly different. Indirect evidence from 2 systematic reviews with NMAs suggested that the risk of serious adverse events with ixekizumab was not different compared to ustekinumab after long-term treatment.19,20
Serious Adverse Events (Long-Term)
No relevant direct comparative evidence regarding ixekizumab and adalimumab, etanercept, or ustekinumab were identified. A systematic review with NMA reported indirect comparative results of ixekizumab versus adalimumab and ustekinumab.19 No therapy was favoured when comparing the risk of serious adverse events of ixekizumab with adalimumab or ustekinumab after long-term treatment. No relevant direct or indirect comparative evidence regarding ixekizumab and etanercept was identified; therefore, no summary can be provided.
Clinical Effectiveness of Brodalumab
PASI 90 Response Rate (Short-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab or etanercept was identified for the outcome PASI 90. Five systematic reviews with NMA reported indirect comparative results of brodalumab compared to adalimumab and to etanercept.18,20,21,23,25 Brodalumab was favourable to adalimumab and to etanercept in achieving PASI 90 after short-term treatment.
Direct evidence from 2 RCTs showed that brodalumab was associated with a statistically significantly higher likelihood of reaching PASI 90 compared to ustekinumab.20 Indirect evidence from 5 NMAs18,20,21,23,25 showed that brodalumab was favourable to ustekinumab (all doses) in reaching PASI 90 with short-term treatment.
PASI 90 Response Rate (Long-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 90 response rate after long-term treatment. Two systematic reviews with NMA reported indirect comparative results of brodalumab versus these drugs.21,22 Brodalumab was favourable to adalimumab, to etanercept, and to ustekinumab in reaching PASI 90 after long-term treatment.
PASI 100 Response Rate (Short-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response rate after short-term treatment. Indirect evidence from 2 NMAs21,23 suggested that brodalumab was favourable compared to adalimumab, to etanercept, and to ustekinumab (all doses) in reaching PASI 100 after short-term treatment.
PASI 100 Response Rate (Long-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response rate after long-term treatment. Two NMAs reported indirect comparative results of brodalumab versus these drugs.21,22 Brodalumab was favourable to adalimumab, to etanercept, and to ustekinumab in reaching PASI 100 after long-term treatment.
Adverse Events (Short-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab or etanercept was identified. Indirect evidence from 3 NMAs suggested that the risk of adverse events with brodalumab was not different compared to adalimumab or etanercept after short-term treatment.18-20
Direct comparison results for brodalumab versus ustekinumab from 2 RCTs was reported in a systematic review.20 Adverse events in the brodalumab group and the ustekinumab group were not significantly different. Indirect evidence from 3 NMAs suggested that the risk of adverse events with brodalumab was not different compared to ustekinumab after short-term treatment.18-20
Adverse Events (Long-Term)
No relevant direct or indirect comparative evidence regarding brodalumab and adalimumab, etanercept, or ustekinumab was identified; therefore, no summary can be provided.
Serious Adverse Events (Short-Term)
No relevant direct comparative evidence regarding brodalumab and adalimumab or etanercept was identified. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with brodalumab was not different compared to adalimumab or etanercept after long-term treatment.19,20
Direct evidence from 2 RCTs as reported in a systematic review20 showed that the risk of adverse events in the brodalumab group and the ustekinumab group were not significantly different. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with brodalumab was not different compared to ustekinumab after long-term treatment.19,20
Serious Adverse Events (Long-Term)
No relevant direct or indirect comparative evidence regarding brodalumab and adalimumab, etanercept, or ustekinumab was identified; therefore, no summary can be provided.
Clinical Effectiveness of Risankizumab
PASI 90 Response Rate (Short-Term)
Direct evidence from 1 RCT showed that risankizumab was associated with a statistically significantly higher likelihood of reaching PASI 90 compared to adalimumab.20 Indirect evidence from 4 NMAs suggested that risankizumab was favourable to adalimumab in reaching PASI 90 with short-term treatment.18,20,21,25
No relevant direct comparative evidence regarding risankizumab and etanercept was identified for the outcome PASI 90 response rate. Indirect evidence from 4 NMAs suggested that risankizumab was favourable to etanercept in reaching PASI 90 with short-term treatment.18,20,21,25
Direct comparison results for risankizumab versus ustekinumab was reported in 2 systematic reviews.20,24 Direct evidence from 3 RCTs showed that the likelihood of reaching PASI 90 response was statistically significantly higher in the risankizumab group compared to the ustekinumab group.20 In the other review,24 in which various doses of risankizumab (18 mg to 180 mg) were compared to weight-based dosing of ustekinumab, the likelihood of reaching PASI 90 response was statistically significantly higher with 150 mg (2 RCTs) and 180 mg (1 RCT) of risankizumab. There were no differences between lower doses of risankizumab (18 mg, 90 mg) and ustekinumab (1 RCT each).24 Five systematic reviews with NMA reported indirect comparative results of risankizumab versus ustekinumab.18,20,21,24,25 Indirect evidence from 4 NMAs found that risankizumab was favourable to ustekinumab in reaching PASI 90 with short-term treatment. In the fifth review,24 risankizumab 150 mg and 180 mg were favourable to a weight-based dose of ustekinumab. All doses of risankizumab (18 mg to 180 mg) were comparable to ustekinumab 45 mg and 90 mg doses in eliciting PASI 90 responses after short-term treatment.
PASI 90 Response Rate (Long-Term)
No relevant direct comparative evidence regarding risankizumab and adalimumab or etanercept was identified for the outcome PASI 90 response rate after long-term treatment. Indirect evidence from 2 NMAs21,22 showed that risankizumab was favourable to adalimumab and to etanercept in reaching PASI 90 after long-term treatment.
Direct evidence from 2 RCTs (reported in 1 systematic review20) showed that PASI 90 response rates were statistically significantly higher in the risankizumab group compared to the ustekinumab group. Indirect evidence from 2 NMAs suggested that risankizumab was favourable to ustekinumab in reaching PASI 90 after long-term treatment.21,22
PASI 100 Response Rate (Short-Term)
No relevant direct comparative evidence regarding risankizumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response rate after short-term treatment. Indirect evidence from an NMA21 found that risankizumab was superior to adalimumab, to etanercept, and to ustekinumab (all doses) in reaching PASI 100 after short-term treatment.
PASI 100 Response Rate (Long-Term)
No relevant direct comparative evidence regarding risankizumab and adalimumab, etanercept, or ustekinumab was identified for the outcome PASI 100 response rate after long-term treatment. Two systematic reviews with indirect evidence from 2 NMAs suggested that risankizumab was favourable to all 3 comparators (adalimumab, etanercept, and ustekinumab) in improving PASI 100 after long-term treatment.21,22
Adverse Events (Short-Term)
Direct evidence from 1 RCT (reported in 1 systematic review) showed that the risk of adverse events in the risankizumab group and the adalimumab group were not significantly different.20 Indirect evidence from 3 NMAs suggested that the risk of adverse events with risankizumab was not different compared to adalimumab after short-term treatment.18-20
No relevant direct comparative evidence regarding risankizumab versus etanercept was identified. Indirect evidence from 3 NMAs suggested that the risk of adverse events with risankizumab was not different compared to etanercept after short-term treatment.18-20
Direct comparison results for risankizumab versus ustekinumab was reported in 2 systematic reviews.20,24 Results of the pairwise meta-analyses between various doses of risankizumab and a weight-based dose of ustekinumab showed that the risk of adverse events between risankizumab and ustekinumab was not different. Indirect evidence from 4 NMAs18-20,24 suggested that the risk of adverse events with risankizumab (all dose ranges) was not different compared to ustekinumab (45 mg, 90 mg, and weight-based dose) after short-term treatment.
Adverse Events (Long-Term)
No relevant direct comparative evidence regarding risankizumab and adalimumab was identified. Indirect evidence from 1 NMA19 showed that the risk of adverse events with risankizumab was not different compared to adalimumab after long-term treatment.
No relevant direct or indirect comparative evidence regarding risankizumab and etanercept was identified; therefore, no summary can be provided.
No relevant direct comparative evidence regarding risankizumab and ustekinumab was identified. Indirect evidence from 1 NMA NMA19 showed that risankizumab was favourable to ustekinumab in terms of the risk of experiencing adverse events after 48 to 52 weeks of treatment.
Serious Adverse Events (Short-Term)
Direct evidence from 1 RCT (reported in 1 systematic review20) showed that the risk of serious adverse events in the risankizumab group and the adalimumab group were not significantly different. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with risankizumab was not different when compared to adalimumab after short-term treatment.18-20
No relevant direct comparative evidence regarding risankizumab versus etanercept was identified. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with risankizumab was not different when compared to etanercept after short-term treatment.18-20
Direct evidence from 3 RCTs (reported in a systematic review20) showed that risk of serious adverse events between risankizumab and ustekinumab was not significantly different. Indirect evidence from 2 NMAs19,20 suggested that the risk of serious adverse events with risankizumab were not different when compared to ustekinumab after short-term treatment.
Serious Adverse Events (Long-Term)
No relevant direct comparative evidence regarding risankizumab versus adalimumab or ustekinumab was identified. Indirect evidence from 2 NMAs suggested that the risk of serious adverse events with risankizumab was not different when compared to adalimumab or to ustekinumab after long-term treatment.18-20
No relevant direct or indirect comparative evidence regarding risankizumab and etanercept was identified; therefore, no summary can be provided.
Limitations
The overall evidence identified in this report was drawn primarily from indirect evidence because of the lack of adequate head-to head trials. There was extensive (up to 98%) overlap of primary trials included across the NMAs and, because of this extensive overlap, it was not possible to present the data only once, so that the overall results from the NMAs contain some of the same data. The validity of indirect evidence depends on the accuracy of the assumptions used such as that of transitivity, homogeneity, and consistency. Although the primary studies were assessed by the authors of the systematic reviews as low to moderate risk of bias, it is possible that the quality of individual studies and the heterogeneity of the included studies could affect the overall results. Key methodological limitations of the included reviews were described in an earlier section. It was unclear how many primary trials were conducted in Canada; therefore, a generalizability to Canadian settings remains unknown.
Conclusions and Implications for Decision- or Policy-Making
The purpose of this report was to compare the clinical effectiveness of newer biologics with older biologics in patients with moderate-to-severe plaque psoriasis. Eight systematic reviews with NMAs18-25 were identified for this report. Overall, the included systematic reviews were of moderate to high quality. There was extensive overlap (53% to 98%) of primary studies identified across the systematic reviews and NMAs, and the findings from this report should be interpreted in the context of this overlapping evidence.
In patients with moderate-to-severe plaque psoriasis, newer biologic drugs such as secukinumab, ixekizumab, brodalumab, and risankizumab were favourable to older biologics such as adalimumab, etanercept, and ustekinumab in achieving PASI 90 or PASI 100 responses.18-25 The results of the NMAs for the outcomes of PASI 90 and PASI 100 response showed that these newer biologics are more effective than the older biologic drugs after short-term (induction phase) and long-term (maintenance phase) treatments. When compared to the older biologics, the risk of adverse events and serious adverse events during treatment with newer biologics was not different. All included systematic reviews reported indirect results from the NMAs.18-25 Three reviews also included direct comparative evidence from pairwise meta-analysis18,20,24 (this evidence was summarized once per comparison in this report). The findings of the direct and indirect results were consistent. The results were also consistent across the NMAs.
The Cochrane living systematic review20 provided the most up-to-date and comprehensive evidence regarding the clinical effectiveness of newer biologics. The comparative effect sizes reported in the Cochrane living systematic review were lower than the other reviews; however, the review included psoriatic arthritis patients with skin involvement, which may limit the generalizability of the results from that systematic review to the patients with moderate-to-severe plaque psoriasis. Half of the systematic reviews were sponsored by pharmaceutical companies with authors declaring conflicts of interests;19,21-23 however, the findings across the NMAs were consistent irrespective of funding sources. Similar to the findings from this report, an overview of NMAs of biologics for plaque psoriasis from 2021 that compared the quality of the methods and the findings across NMAs also highlighted consistent findings across NMAs despite differences in methodology used in the NMAs and the potential bias from the sources of funding.33 Cost-effectiveness studies of targeted treatment for moderate-to-severe plaque psoriasis have reported that brodalumab, ixekizumab and secukinumab were cost-effective at various willingness-to-pay thresholds.34
CADTH has previously issued recommendations for secukinumab,6 ixekizumab,7 brodalumab,8 and risankizumab9 for the management of moderate-to-severe plaque psoriasis. With improved effectiveness and a comparable safety profile, these drugs could improve patient outcomes and help patients tolerate treatment better. To better understand the landscape of plaque psoriasis management across Canada and to support formulary management strategies, an environmental scan has been initiated by CADTH,35 as well as a utilization study warranted to understand the patterns of use of biologic drugs across the public drug plans.36
References
1.Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983-994.PubMed
2.Canadian Psoriasis Network. Psoriaisis Journey to stability National Report – Canadians’ Journey Living with Psoriasis – Winter 2018. 2018; https://www.canadianpsoriasisnetwork.com/wp-content/uploads/2018/09/JTSFinal-r.pdf. Accessed 2021 Aug 17.
3.Levy AR, Davie AM, Brazier NC, et al. Economic burden of moderate to severe plaque psoriasis in Canada. Int J Dermatol. 2012;51(12):1432-1440.PubMed
4.Clinical Review Report: Guselkumab (Tremfya): (Janssen Inc.): Indication: For the treatment of adult patients with moderate-to-severe plaque psoriasis who are candidates for systemic therapy or phototherapy. Appendix 5, Validity of Outcome Measures.. Ottawa (ON): CADTH; 2018: https://www.ncbi.nlm.nih.gov/books/NBK534046/. Accessed 2021 Aug 31.
5.Tseng J-C, Chang Y-C, Huang C-M, Hsu L-C, Chuang T-H. Therapeutic Development Based on the Immunopathogenic Mechanisms of Psoriasis. Pharmaceutics. 2021;13(7):1064.PubMed
6.Reimbursement Reviews: Secukinumab. Ottawa: CADTH; 2014: https://cadth.ca/secukinumab. Accessed 2021 Aug 30.
7.Reimbursement Reviews: Ixekizumab. Ottawa: CADTH; 2016: https://cadth.ca/ixekizumab Accessed 2021 Aug 30.
8.Reimbursement Reviews: Brodalumab. Ottawa: CADTH; 2018: https://cadth.ca/brodalumab. Accessed 2021 Aug 30.
9.Reimbursement Reviews: Risankizumab. Ottawa: CADTH; 2019: https://cadth.ca/risankizumab Accessed 2021 Aug 30.
10.Yu N, Bach P, Trusheim M. Biosimilars: Market Changes do not equal policy success. 2021; https://www.drugpricinglab.org/research/biosimilars-market-growth-give-a-false-sense-of-security/. Accessed 2021 Aug 30.
11.Drug Programs Policy and Strategy Branch: Drugs and Devices Division. Ontario Drug Benefit Formulary/Comparative Drug Index Edition 43. Toronto: Ministry of Health; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/formulary43/summary_edition43_20210319.pdf. Accessed 2021 Aug 30.
12.Prescribed Drug Spending in Canada, 2020. Ottawa: CIHI; 2020: https://www.cihi.ca/en/prescribed-drug-spending-in-canada-2020. Accessed 2021 Aug 31.
13.Igarashi A, Igarashi A, Graham CN, Gilloteau I, Tani Y. Evaluating the cost-effectiveness of secukinumab in moderate-to-severe psoriasis: a Japanese perspective. J Med Econ. 2019;22(1):7-15.PubMed
14.Bagel J LT, Green LJ. What Does Efficacy Cost? Evidence for Relative Cost-Effectiveness of Biologic Therapies for Psoriasis. Practical Dermatology 2019 Oct. https://practicaldermatology.com/articles/2019-oct/what-does-efficacy-cost-evidence-for-relative-cost-effectiveness-of-biologic-therapies-for-psoriasis. Accessed 2021 Aug 30.
15.Hill S, Walter M. Newer Biologics for the Treatment of Plaque Psoriasis (CADTH reference list). Ottawa CADTH; 2021: https://cadth.ca/newer-biologics-treatment-plaque-psoriasis. Accessed 2021 Aug 31.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Jansen JP, Trikalinos T, Cappelleri JC, et al. Appendix A: Questionnaire to assess the relevance and credibility of a network meta-analysis. Value Health. 2014;17(2):Supplementary Material.
18.Xu S, Gao X, Deng J, Yang J, Pan F. Comparative efficacy and safety of biologics in moderate to severe plaque psoriasis: a multiple-treatments meta-analysis. J. 2021;19(1):47-56.
19.Shear NH, Betts KA, Soliman AM, et al. Comparative safety and benefit-risk profile of biologics and oral treatment for moderate-to-severe plaque psoriasis: A network meta-analysis of clinical trial data. J Am Acad Dermatol. 2021;22:22.PubMed
20.Sbidian E, Chaimani A, Garcia-Doval I, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta‐analysis. Cochrane Database Syst Rev. 2021(4).
21.Armstrong AW, Soliman AM, Betts KA, et al. Comparative Efficacy and Relative Ranking of Biologics and Oral Therapies for Moderate-to-Severe Plaque Psoriasis: A Network Meta-analysis. Dermatol Ther (Heidelb). 2021;11(3):885-905.PubMed
22.Yasmeen N, Sawyer LM, Malottki K, Levin LA, Didriksen Apol E, Jemec GB. Targeted therapies for patients with moderate-to-severe psoriasis: a systematic review and network meta-analysis of PASI response at 1 year. Journal of Dermatological Treatment. 2020:1-15.PubMed
23.Xue W, Saharia P, Gray E, et al. Efficacy of Brodalumab for Moderate to Severe Plaque Psoriasis: A Canadian Network Meta-Analysis. J Cutan Med Surg. 2020;24(6):561-572.PubMed
24.Shi J, Xu J, Chen Y. A network meta-analysis for the comparison of efficacy and safety of interleukin (IL)-23 targeted drugs in the treatment of moderate to severe psoriasis. Dermatol Ther. 2020;33(4):e13802.PubMed
25.Mahil SK, Ezejimofor MC, Exton LS, et al. Comparing the efficacy and tolerability of biologic therapies in psoriasis: an updated network meta-analysis. Br J Dermatol. 2020;183(4):638-649.PubMed
26.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34.PubMed
27.CADTH Common Drug Review. Clinical Review Report Risankizumab (Skyrizi). Ottawa: CADTH; 2019: https://cadth.ca/sites/default/files/cdr/clinical/sr0583-skyrizi-clinical-review-report.pdf. Accessed 2021 Aug 17.
28.Armstrong AW, Parsi K, Schupp CW, Mease PJ, Duffin KC. Standardizing Training for Psoriasis Measures: Effectiveness of an Online Training Video on Psoriasis Area and Severity Index Assessment by Physician and Patient Raters. JAMA Dermatol. 2013;149(5):577-582.PubMed
29.Wu AG, Conway J, Barazani L, Roy B, Cline A, Pereira F. Is Clear Always Clear? Comparison of Psoriasis Area and Severity Index (PASI) and the Physician’s Global Assessment (PGA) in Psoriasis Clearance. Dermatol Ther (Heidelb). 2020;10(5):1155-1163.PubMed
30.Revicki DA, Willian MK, Menter A, Saurat JH, Harnam N, Kaul M. Relationship between Clinical Response to Therapy and Health-Related Quality of Life Outcomes in Patients with Moderate to Severe Plaque Psoriasis. Dermatology. 2008;216(3):260-270.PubMed
31.Mrowietz U, Kragballe K, Reich K, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Archives of Dermatological Research. 2011;303(1):1-10.PubMed
32.Ren S, Oakley JE, Stevens JW. Incorporating Genuine Prior Information about Between-Study Heterogeneity in Random Effects Pairwise and Network Meta-analyses. Med Decis Making. 2018;38(4):531-542.PubMed
33.Wright E, Yasmeen N, Malottki K, et al. Assessing the Quality and Coherence of Network Meta-Analyses of Biologics in Plaque Psoriasis: What Does All This Evidence Synthesis Tell Us? Dermatol Ther (Heidelb). 2021;11(1):181-220.PubMed
34.Hendrix N, Ollendorf DA, Chapman RH, et al. Cost-Effectiveness of Targeted Pharmacotherapy for Moderate to Severe Plaque Psoriasis. J Manag Care Spec Pharm. 2018;24(12):1210-1217.PubMed
35.Formulary Management of Biologics in Plaque Psoriasis-Environment Scan. Ottawa: CADTH; 2021 Jun 30: https://cadth.ca/index.php/formulary-management-biologics-plaque-psoriasis. Accessed 2021 Aug 30.
36.Utilization of Biologic Disease-Modifying Antirheumatic Drugs for Plaque Psoriasis. Ottawa: CADTH; 2021 Aug 17: https://cadth.ca/utilization-biologic-disease-modifying-antirheumatic-drugs-plaque-psoriasis. Accessed 2021 Aug 30.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Armstrong et al.(2021)21 US Funding sources: AbbVie Inc. | Study design: Systematic review and NMA of (phase II/III/IV) RCTs. NMA design: Bayesian NMA with fixed and random-effects model Number of primary studies included in the NMA: 71 Number of head-to-head RCTs relevant to this report: 9 | Patients (18 years or older) with moderate to severe plaque psoriasis, and are eligible for systemic therapies or phototherapy Total number of patients included in the NMA: NR Mean age: NR Sex: NR Baseline PASI score: NR | Eligible interventions: Anti–IL-23; anti–IL-17 drugs, anti-TNF alpha drugs, anti-phosphodiesterase type-4 inhibitor, anti–IL-12/23 drug, dimethyl fumarate Relevant interventions:
Relevant comparators:
| Outcomes: PASI 90, PASI 100 Follow-up: Short-term (10 to 16 weeks from baseline) and long-term (48 to 52 weeks from baseline) |
Sbidian et al., (2021)20 France Funding sources: National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Skin; Complex Reviews Support Unit, funded by the National Institute for Health Research (project number 14/178/29) | Study design: Living systematic review and NMA of (phase II/III/IV) RCTs. NMA design: Frequentist NMA Number of RCTs included in the NMA: 130 Number of head-to-head RCTs relevant to this report: 14 | Patients (18 years or older) with moderate to severe plaque psoriasis, or psoriatic arthritis (with moderate to severe psoriasis) at any stage of treatment. Total number of patients included in the NMA: 57,831 Overall mean age: 45 years Range of mean age across RCTs: 27 to 56.5 years Sex: 67.2% males Mean baseline PASI score: 20 (range 9.5 to 39) | Eligible interventions: All systemic treatments for psoriasis irrespective of the dose and duration of treatments Relevant interventions:
Comparators:
| Primary outcome: PASI 90 at induction phase, serious adverse events at induction phase Secondary outcomes: PASI 90 at 52 weeks, adverse events at induction phase Follow-up: Induction phase and up to 52 weeks. |
Shear et al.,(2021)19 Canada Funding sources: AbbVie Inc. | Study design: systematic review and NMA of (phase II/III/IV) RCTs. NMA design: Bayesian NMA with fixed and random effects models. Number of primary studies included in the NMA: 52 Number of head-to-head RCTs relevant to this report: 8 | Patients (18 years or older) with moderate to severe psoriasis, and are eligible for systemic therapies or phototherapy Total number of patients included in the NMA: NR Mean age: NR Sex: NR Baseline PASI score: NR | Eligible interventions: Anti–IL-23 drugs; anti–IL-17 drugs, anti–TNF alpha drugs, anti-phosphodiesterase type-4 inhibitor, anti–IL-12/23 drugs, dimethyl fumarate Relevant interventions:
Relevant comparators:
| Outcomes: Any adverse events, any serious adverse events Follow-up: Short-term (12 to 16 weeks from baseline) and long-term (48 to 56 weeks from baseline) |
Xu et al., (2021)18 China Funding sources: National Natural Science Foundation of China (81273169, 81573218 and 81773514, 82073655) | Study design: systematic review and NMA of RCTs. NMA design: Bayesian NMA with random-effects model. Number of primary studies included: 66 Number of head-to-head RCTs relevant to this report: NR | Patients with moderate to severe plaque psoriasis Total number of patients included in the NMA: 26,334 Mean age: ranged from 39.2 to 51 years across RCTs Sex: NR Mean baseline PASI score: 20.43 (SD 4.85) | Eligible interventions: biologic drugs Relevant interventions:
Comparators:
| Outcomes: PASI 90, Adverse events Follow-up: 16 weeks |
Mahil et al., (2020)25 UK Funding sources: British Association of Dermatologists. | Study design: systematic review and NMA of RCTs and cohort studies (for long-term efficacy/safety) NMA design:
| All patients with moderate to severe psoriasis treated mainly for skin disease. Total number of patients included in the NMA: NR Mean age:44.7 years Sex: 68.7% male Baseline PASI score ranged from 8 to 30 across the RCTs | Eligible interventions: All doses and durations of biologics, methotrexate or placebo Relevant interventions: Brodalumab, Ixekizumab, Risankizumab, secukinumab Relevant comparators: Adalimumab, Etanercept, Ustekinumab (weight-based dosing) | Outcomes: PASI 90 (clear/nearly clear) Follow-up: 3 to4 months, 1 year, 3 years |
Shi et al., (2020)24 China Funding sources: Nantong Science and Technology Project, Grant/Award Number: JC2019054 | Study design: systematic review and NMA of RCTs. NMA design:
| Patients with moderate to severe psoriasis Total number of patients included in the NMA: 8,402 Mean age: 45.7 years Sex:70.2% males Mean baseline PASI score: Ranged from 18 to 25.7 across RCTs | Eligible interventions: various dose ranges of IL-23 targeted drugs (Ustekinumab [IL-12/23], guselkumab, tildrakizumab, risankizumab) Relevant intervention: Risankizumab (18 mg, 75mg, 90mg, 150mg, 180mg) Relevant comparator: ustekinumab (45mg, 90mg, weight-based dosing) | Outcomes: PASI 90, Adverse events Follow-up: 12 to 16 weeks (acute/induction phase) |
Xue et al., (2020)23 Canada, UK Funding sources: Bausch Health, Canada Inc. | Study design: systematic review and NMA of (phase II/III) RCTs. NMA design:
| Adult patients with moderate to severe plaque psoriasis Total number of patients included in the NMA: NR Mean age 44.6 Sex: 69% males Mean baseline PASI score: 21 | Eligible interventions: Brodalumab, secukinumab, ixekizumab, guselkumab, adalimumab, etanercept, ustekinumab, infliximab, placebo Relevant interventions: Anti–IL-17 drugs: Brodalumab, secukinumab, ixekizumab Relevant comparators:
| Outcomes: PASI 90, PASI 100 Follow-up: At the end of induction period (10 to 16 weeks) |
Yasmeen et al., (2020)22 UK Funding sources: Leo Pharma A/S | Study design: systematic review and NMA of RCTs and long-term extension studies. Number of primary studies included: 28 Number of head-to-head RCTs relevant to this report: 7 | Adult patients with moderate to severe plaque psoriasis Total number of patients included in the NMA: NR Mean age: ranged from 42 to 51 years across RCTs Sex: 41% to 91% males Mean baseline PASI score: NR | Eligible interventions: Licensed doses of adalimumab, apremilast, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, ustekinumab, dimethyl fumarate compared with placebo, other biologic therapies or non-biologic systemic therapy. Relevant interventions: Brodalumab, secukinumab, ixekizumab, risankizumab Relevant comparators: Adalimumab, etanercept, ustekinumab. | Outcomes: PASI 90, PASI 100 Follow-up: 1 year |
IL = interleukin; NMA = network meta-analysis; NR = not reported; PASI = Psoriasis Area Severity Index; RCT = randomized controlled trial; SD = standard deviation; TNF = tumour necrosis factor.
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 216 and the ISPOR Questionnaire17
Strengths | Limitations |
|---|---|
Armstrong et al. (2021)21 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. No major interventions or comparators were excluded from eligibility. Phase II/III/IV clinical trials were considered eligible for the review. Multiple databases were searched to identify eligible studies. Keywords and search strategy were reported and were relevant to the objective of the review. Search was conducted within 24 months of the publication of the review. Some characteristics of the included studies such as the population and outcomes in each treatment arm were reported. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. For the short-term effects NMA, a random-effects model was used to account for possible heterogeneity. For the long-term effects NMA fixed-effects model was used due to a sparse network. In the short-term network a reference arm adjustment was used to address possible heterogeneity. Since this was a Bayesian NMA, results were reported appropriately as odds ratio and 95% credible intervals to account for uncertainty. Vague (non-informative) prior distributions were used to ensure the distributions was based on observed data. | It was unclear whether the review methods were established a priori. It was unclear whether the study selection and data extraction was done in duplicate. A list of excluded studies was not provided. A risk of bias assessments for the included studies were not conducted. Potential effect modifiers were not considered in the analysis. As baseline characteristics of individual study participants such as duration of disease, age and comorbidities were not reported, an assessment of these possible effect modifiers on the overall results could not be done. Heterogeneity between the trials was not measured. Source of funding of the individual trials were not reported. Results of direct comparison from head-to-head trials were not reported. Inconsistency between direct and indirect comparison were not tested or reported in the review. All individual studies that reported outcomes between 10 to 16 weeks of treatment were grouped together in the short-tern network. All individual studies that reported outcomes between 48 to 52 weeks were grouped in the long-term outcome. It is possible that these within-network differences in follow-up time introduced some heterogeneity. Safety outcomes were not considered in the analysis. Publication bias was not investigated. The NMA was sponsored by pharmaceutical company which manufactures biologic therapy drugs. Review authors indicated conflicts of interests related to pharmaceutical companies. |
Sbidian et al. (2021)20 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. No major interventions or comparators were excluded from eligibility. The review was conducted as a living systematic review, with regular updates to the evidence base, analysis, and conclusion. Methodology and protocol of the review were established prior to the review as an adapted living systematic review protocol. Differences from protocol and review were listed and justified. The rationale for including phase II/III/IV trials were explained. A comprehensive literature search across multiple databases was used to identify eligible studies. Keywords and search strategy were reported and were relevant to the objective of the review. Search was conducted within 24 months of the publication of the review. Study selection, data extraction and risk of bias assessment were done in duplicate by 2 independent reviewers. A list of excluded studies along with reason for exclusion were provided. Quality assessment of the included studies were conducted using Cochrane’s Risk of Bias tool. Detailed characteristics and risk of bias assessment for each of the included studies were reported in the review. Source of funding of the included studies was reported when available. A network meta-analysis was conducted using frequentist methods. Evidence in the quality of evidence from the NMA was assessed using CINeMA approach. Domains such as consider within-study bias, publication bias, transitivity, imprecision, heterogeneity and inconsistency were assessed in this approach. Pairwise meta-analysis of head-to-head trials were conducted using random-effects model. This provided direct comparative evidence which was relevant to the current report. | The review had a broader scope than the current report. Therefore, the included networks in the NMA consisted of several nodes which were not relevant to the review. It is unclear whether the additional interventions and comparators would have affected the overall results. Effect of long-term treatment (up to 52 weeks) was not assessed in the review. All individual studies that reported outcomes between 8 to 24 weeks of treatment were grouped together in the network. It is unclear whether grouping of studies with different treatment duration could have affected the results. Results of the individual studies were not reported. |
The network diagram of studies included in the NMA was provided. The studies formed an interconnected network. The network was not sparse. A list of possible effect modifiers (e.g., age, sex, duration of illness) were provided. Potential sources of heterogeneity between the studies were also identified prior to the review. Meta-analysis was conducted if studies were relatively similar. Steps were taken to ensure the assumption of transitivity. Heterogeneity in in the NMA was assessed using heterogeneity variance parameter and observation of the network. Subgroup analyses and meta-regression were planned to minimize heterogeneity; however, no heterogeneity was found. Inconsistency between direct and indirect comparisons were assessed using “loop-specific approach” and “side-splitting method.” Overall reporting quality was good with graphical presentation of evidence network and pairwise meta-analysis, tabular reporting of direct and indirect results and appropriate measures of uncertainty (95% CI). Publication bias was examined using comparison adjusted funnel plot, and no risk of any publication bias was identified. | |
Shear et al. (2021)19 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. No major interventions or comparators were excluded from eligibility. The systematic review was registered in PROSPERO Phase II/III/IV clinical trials were considered eligible for the review. A comprehensive literature search across multiple databases were searched to identify eligible studies. Search was conducted within 24 months of the publication of the review. NMA was conducted using Bayesian method. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. For the short-term effects NMA, a random-effects model was used to account for possible heterogeneity. For the long-term effects NMA fixed-effects model was used due to a sparse network. Since this was a Bayesian NMA, results were reported appropriately as odds ratio and 95% credible intervals to account for uncertainty. Vague (non-informative) prior distributions were used to ensure the distributions was based on observed data. The review conclusions were fair and balanced. | It was unclear whether the review methods deviated from the planned protocol. It was unclear whether the study selection and data extraction was done in duplicate. A list of excluded studies was not provided. Risk of bias assessments for the included studies were not conducted. The results of the NMA were not discussed in light of possible bias in the trials. Potential effect modifiers were not considered in the analysis. As baseline characteristics of individual study participants such as duration of disease, age and comorbidities were not reported, an assessment of these possible effect modifiers on the overall results could not be done. Heterogeneity between the trials was not measured. Sensitivity analyses were not conducted Source of funding of the individual trials were not reported. Results of direct comparison from head-to-head trials were not reported. Inconsistency between direct and indirect comparison were not tested and reported in the review. All individual studies that reported outcomes between 12 to 16 weeks of treatment were grouped together in the short-term network. All individual studies that reported outcomes between 48 to 56 weeks were grouped in the long-term outcome. It is possible that these within-network differences in follow-up time introduced some heterogeneity. The risk of publication bias was not investigated. The NMA was sponsored by pharmaceutical company which manufactures biologic therapy drugs. Review authors indicated conflicts of interests related to pharmaceutical companies. |
Xu et al. (2021)18 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. Only double blind RCTs were considered eligible for the review. A comprehensive literature search across multiple databases were searched to identify eligible studies. Keywords and search strategy were reported. Search was conducted within 24 months of the publication of the review. Study selection, data extraction and risk of bias assessment of the included studies were conducted independently by 2 reviewers. Discrepancies were resolved through discussion with a third reviewer. Risk of bias of the included studies were assessed using modified Jadad scale. Overall quality of the studies was rated as “good.” Characteristics of included studies such as number of patients, their mean age and sex, duration of illness and weight were reported. A Bayesian NMA was conducted. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. Direct comparative evidence was reported as the results of pairwise meta-analysis. Meta-regression analyses were conducted by adjusting for possible effect modifiers (age, sex ratio, duration of disease, PASI scale and Jadad score) to investigate the sources of heterogeneity. Sensitivity analyses were conducted Deviance information criterion of both fixed and random-effects model were assessed. They were found to be close, although data were not reported, Publication bias assessed using funnel plots and Eggers test did not find any significant bias for the relevant outcomes. The review authors had not conflict of interests. | It was unclear whether the review methods were established a priori. A list of excluded studies was not provided. Source of funding of the included studies was not reported. Individual study results were not reported. All individual studies that reported outcomes between 12 to 16 weeks of treatment were grouped together in the network. It is possible that these within-network differences in follow-up time introduced some heterogeneity. Duration of treatment was not considered as a covariant in the meta-regression Effect of long-term treatment (up to 52 weeks) was not assessed in the review. |
Mahil et al. (2020)25 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. The review was an update to a previously published NMA. The systematic review was registered in PROSPERO. Review methods were previously established and deviations to the original protocol and the review were reported. The review included RCTs and cohort studies (for long-term efficacy and safety outcomes). A comprehensive literature search across multiple databases were searched to identify eligible studies. Keywords and search strategy were reported. Search was conducted within 24 months of the publication of the review. Study selection, data extraction and risk of bias assessment were done in duplicate by 2 independent reviewers. A list of excluded studies along with reason for exclusion was provided. Quality assessments of the included studies were conducted using Cochrane’s Risk of Bias tool. The overall risk of bias of the included studies were reported as “low.” Quality of evidence was assessed using GRADE Detailed characteristics and risk of bias assessment for each of the included studies was reported in the review. Sources of funding of the included studies were reported. A network meta-analysis was conducted using frequentist methods. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. The network was not sparse. | Direct comparative evidence in the form of pairwise meta-analysis was not reported. Possible effect modifiers (e.g., duration of disease, comorbidities) were not considered. For the outcomes relevant to current report, 1 of the 15 loops showed inconsistency. It was unclear if an attempt to minimize the inconsistency with analysis. A rationale for the use of random-effects model was not provided. It was assumed that there was ‘equal heterogeneity’ across all comparators. No subgroup analysis or meta-regression was conducted to adjust for other possible sources of heterogeneity. Individual study results were not reported. All individual studies that reported outcomes between 12 to 16 weeks of treatment were grouped together in the network. It is possible that these within-network differences in follow-up time introduced some heterogeneity. Effect of long-term treatment (up to 52 weeks) was not assessed in the review. |
It was reported that the patient characteristics were similar across the studies. Inconsistency between direct and indirect comparisons was assessed using visual inspection of forest plots, loop-specific inconsistency plots and inconsistency factors. Heterogeneity in the analysis were assessed using visual inspection of forest plots. Subgroup analysis using only licensed doses of interventions and comparators were conducted. Overall reporting quality was good with graphical presentation of evidence network and pairwise mete-analysis, tabular reporting indirect results and appropriate measures of uncertainty (95% CI). Publication bias was examined using funnel plots for different outcomes, and low risk of any publication bias was identified. The review authors had no conflict of interests. | |
Shi et al. (2020)24 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome The study included RCTs. A comprehensive literature search across multiple databases was used to identify eligible studies. Keywords and search strategy were reported. Search was conducted within 24 months of the publication of the review. Study selection, data extraction and risk of bias assessment of the included studies were conducted independently by 2 reviewers. Discrepancies were resolved through discussion with a third reviewer. Detailed characteristics and a risk of bias assessment for each of the included studies were reported in the review. Risk of bias assessment were conducted using Cochrane’s risk of bias tool. Most of the included studies were at low risk of bias. Quality of evidence was assessed using GRADE system. A network meta-analysis was conducted using Bayesian methods. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. The network was not sparse. Results of both direct and indirect comparisons were reported. Direct comparisons were from pairwise meta-analysis. Consistency between direct and indirect comparisons were assessed using node segmentation. No inconsistencies were observed. Heterogeneity was assessed using Cochran’s Q test and I2 statistics. Sensitivity analysis was conducted in situations with high heterogeneity. Overall reporting quality was good with graphical presentation of evidence network and pairwise mete-analysis, tabular reporting indirect results and appropriate measures of uncertainty (95% CrI). Publication bias was assessed using funnel plots, there was low risk of publication bias. There were no conflicts of interests for the review authors. | The review was not registered. It was unclear wither a protocol was established before the conduct of the review. A list of excluded studies was not reported in the review. Sources of funding of the individual studies were not reported. Potential effect modifiers (e.g., duration of disease) were not listed and were not adjusted for in the analysis. The rationale for using random-effects model was unclear. Individual study results were not reported. The priors (informative or non-informative) used in the analysis was unclear. All individual studies that reported outcomes between 12 to 16 weeks of treatment were grouped together in the network. It is possible that these within-network differences in follow-up time introduced some heterogeneity |
Xue et al. (2020)23 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. The study included phase II/III RCTs. Observational studies were excluded from the review. A comprehensive literature search across multiple databases was used to identify eligible studies. A clinical expert was consulted during the conduct of the NMA. A network meta-analysis was conducted using Bayesian methods. The network diagram of studies included in the NMA were provided. The studies formed an interconnected network. The network was not sparse. A feasibility assessment was conducted prior to the NMA to mitigate between-study differences. Studies with irrelevant dosing regimen were excluded from the NMA. A list of possible effect modifiers was provided. The list was fairly comprehensive. Heterogeneity and inconsistency of trials were assessed qualitatively for the listed effect modifiers. Consistency between direct and indirect evidence was assessed using back calculations. Meta-regression analyses were performed to minimize heterogeneity in the feasibility analysis. Sensitivity analyses were conducted to assess the impact of effect modifiers on the results of the NMA. Results were consistent with that of the base-case analysis. The Bayesian NMA was conducted using non-informative priors. The choice of fixed or random effects were determined using residual deviance and deviance information criterion. Appropriate measures of uncertainty (95% CrI) were included while reporting the results of the NMA. | It was unclear whether review methods (protocol) were established before the conduct of the review. Keywords and search strategies were not reported. The search was conducted in 2017, which was more than 24 months before the publication of the review. Relevant trials published after 2017 would not be included in this SR. It was unclear whether study selection and data extraction and was performed independently by 2 reviewers. A list of excluded studies and reasons for exclusion were not provided. Characteristics of the included studies (e.g., study population, demographics, duration of treatment) were not reported. Individual study results were not reported. Although it was reported that the quality of included studies were high, it was unclear if a risk of bias assessment was conducted. Risk of bias assessment of each if the included studies were not reported. Source of funding of the included studies were not reported. Direct comparisons in the form of pairwise meta-analysis were not conducted. All individual studies that reported outcomes between 12 to 16 weeks of treatment were grouped together in the network. However, it was reported that the clinical expert consulted for the review confirmed this grouping as appropriate. Long-term efficacy outcomes or safety outcomes were not considered. Weight-based dosing of ustekinumab was grouped with ustekinumab 45 mg. It is possible that this introduced some heterogeneity in the analysis lowering the internal validity. The reviewers used a multinomial likelihood NMA model in which all outcomes (PASI 75, PASI 90, PASI 100) were grouped in the same network, compared to analyzing them in separate NMAs. The relative treatment effects of 1 PASI end point could be affected by response level at other PASI end points. The risk of publication bias was not assessed. The review was sponsored by a pharmaceutical company. The review authors also declared conflicts of interests related to pharmaceutical companies. |
Yasmeen et al. (2020)22 | |
The research questions and inclusion criteria for the review included components of population, interventions, comparators, and outcome. They were relevant to the current report. The review methods were established prior to the conduct of the review. The review included RCTs and long-term extension studies. A comprehensive literature search across multiple databases was used to identify eligible studies. Keywords and search strategy were reported. Search was conducted within 24 months of the publication of the review. Studies that were excluded from the NMA (but included in the SR) were described along with reasons for exclusion. Characteristics of included studies (e.g., number of patients, demographics, previous treatments, disease duration) were described in detail. Quality assessment of the included studies were conducted using Cochrane Risk of Bias tool. The risk of bias for each included study were reported. A network meta-analysis was conducted using Bayesian methods. Both fixed and random effects were used. Preferred model (random effects) was decided using deviance information criterion and residual deviance. PASI 75 responses from the included studies were used in setting up informative priors. Prior exposure to biologic therapy was considered as an effect modifier. Sensitivity analysis was conducted to adjust for this factor. Results were consistent with that of the base-case analysis. The network diagram of studies included in the NMA was provided. Inconsistency between direct and indirect results were assessed using 2-stage Bucher method. Between-study heterogeneity was assessed qualitatively | It was unclear whether the protocol was registered and published. Any potential deviations from the protocol were not reported. A list of studies excluded from the systematic review were not provided. Source of funding for the individual studies was not reported. Study selection and data extraction were conducted by 1 reviewer. A second reviewer independently performed a data check on 50% of the studies. Discrepancies were resolved by discussion or with a third reviewer. It is possible that other possible effect modifiers were not considered in the analysis (e.g., demographical, duration of disease) Direct comparisons using pairwise meta-analysis was not conducted. Meta-regression analysis with prespecified covariates were not conducted to minimize heterogeneity. Primary analysis in the NMA (analysis 1) included all studies that reported 52-week outcome. The network for this outcome was sparse on visual inspection. A secondary analysis (analysis 2) was conducted including long-term extension studies. In studies in which placebo arm was switched to active therapy in the extension study, it was assumed that placebo response in induction phase will continue to maintenance phase. The validity of this assumption is unclear. Using this assumption, more studies could be included in the analysis creating a full network for analysis 2. Discontinuation of treatments or dose adjustments after induction phase were not considered in the NMA. It is possible that many patients would receive adjusted doses after the initial period in case of low response. The risk of publication bias was not assessed. The review was sponsored by a pharmaceutical company. The review authors also declared conflicts of interests related to pharmaceutical companies. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; CINeMA = confidence in network meta-analysis; CrI = credible interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; ISPOR = International Society for Pharmacoeconomics and Outcomes Research.
Note that this appendix has not been copy-edited.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — PASI 90
Comparison | Study citation | Treatment responsea |
|---|---|---|
Short -term treatment (up to 16 or 24 weeks) | ||
Secukinumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.46 (95% CrI, 1.91 to 3.13) |
Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.45 (95% CI,1.27 to 1.65) | |
Xu et al., ((2021))18 | Indirect evidence from NMA: RR = 2.7 (95% CrI,1.51 to 4.5) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 2.29 (95% CrI, 1.37 to 3.84) Licensed doses: OR = 2.99 (95% CrI = 1.78 to 5.00) | |
Secukinumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 8.42 (95% CrI, 6.22 to 11.46) |
Sbidian et al., (2021)20 | Direct evidence: RR = 2.32 (95% CI, 1.85 to 2.92) [1 RCT] Indirect evidence from NMA: RR = 2.40 (95% CI, 2.12 to 2.72) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 4.5 (95% CrI, 3.03 to 6.25) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 4.51 (95% CI, 3.24 to 6.27) Licensed doses: OR = 5.27 (95% CI, 3.84 to 7.24) | |
Secukinumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: secukinumab vs. ustekinumab 90mg, OR = 2.01 (95% CrI, 1.50 to 2.74) secukinumab vs. ustekinumab 45mg, OR = 2.31 (95% CrI, 1.77 to 3.02) secukinumab vs. ustekinumab (weight-based dosing), OR = 2.21 (95% CrI, 1.77 to 2.72) |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.40 (95% CI, 1.30 to 1.50) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.40 (95% CI, 1.31 to 1.49) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 2.23 (95% CrI, 1.54 to 2.98) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 2.03 (95% CI, 1.46 to 2.81) Licensed doses: OR = 2.44 (95% CI, 1.80 to 3.32) | |
Ixekizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.58 (95% CrI, 2.67 to 4.74) |
Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.82 (95% CI, 1.63 to 2.04) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 4.35 (95% CrI, 2.5 to 7.69) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 3.70 (95% CI, 2.23 to 6.12) Licensed doses: OR = 4.59 (95% CI, 2.77 to 7.60) | |
Ixekizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 12.23 (95% CrI, 8.74 to 17.19) |
Sbidian et al., (2021)20 | Direct evidence: RR = 2.98 (95% CI, 2.24 to 3.98) [2 RCTs]; I2 = 76% Indirect evidence from NMA: RR = 3.02 (95% CI = 2.69 to 3.38) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 7.14 (95% CrI, 5.2 to 10) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 7.26 (95% CI, 5.50 to 9.59) Licensed doses: OR = 8.10 (95% CI, 6.21 to 10.55) | |
Ixekizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: ixekizumab vs. ustekinumab 90mg, OR = 2.93 (95% CrI, 2.11 to 4.11) ixekizumab b vs. ustekinumab 45mg, OR = 3.35 (95% CrI, 2.49 to 4.56) ixekizumab vs. ustekinumab (weight-based dosing), OR = 3.21 (95% CrI, 2.44 to 4.18) |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.73 (95% CI, 1.41 to 2.12) [1 RCT] Indirect evidence from NMA: RR = 1.76 (95% CI, 1.56 to 1.98) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 3.60 (95% CrI, 2.47 to 5.21) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 3.26 (95% CI, 2.36 to 4.51) Licensed doses: OR = 3.75 (95% CI, 2.74 to 5.14) | |
Brodalumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.41 (95% CrI, 2.61 to 4.57) |
Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.32 (95% CI, 1.13 to 1.54) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 2.12 (95% CrI, 1.19 to 3.84) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 1.95 (95% CI, 1.18 to 3.23) Licensed doses: OR = 3.25 (95% CI, 1.93 to 5.49) | |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 2.11 (95% CrI, 1.72 to 2.67) | |
Brodalumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 11.69 (95% CrI, 8.35 to 16.77) |
Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 2.19 (95% CI, 1.89 to 2.54) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 3.47 (95% CrI, 2.33 to 5.54) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 3.84 (95% CI, 2.64 to 5.57) Licensed doses: OR = 5.74 (95% CI, 3.92 to 8.39) | |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 2.84 (95% CrI, 2.35 to 3.52) | |
Brodalumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: brodalumab vs. ustekinumab 90mg, OR = 2.80 (95% CrI, 2.00 to 4.06) brodalumab vs. ustekinumab 45mg, OR = 3.20 (95% CrI, 2.36 to 4.49) brodalumab vs. ustekinumab (weight-based dosing), OR = 3.06 (95% CrI, 2.39 to 3.99) |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.27 (95% CI, 1.16 to 1.39) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.28 (95% CI, 1.17 to 1.39) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.73 (95% CrI, 1.24 to 2.48) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 1.73 (95% CI, 1.31 to 2.27) Licensed doses: OR = 2.66 (95% CI, 2.06 to 3.44) | |
Xue et al., (2020)23 | Indirect evidence from NMA: brodalumab vs. ustekinumab 90mg, RR = 1.43 (95% CrI, 1.23 to 1.69) brodalumab vs. ustekinumab 45mg, RR = 1.62 (95% CrI, 1.43 to 1.86) | |
Risankizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.49 (95% CrI, 2.75 to 4.46) |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.53 (95% CI, 1.33 to 1.75) [1 RCT] Indirect evidence from NMA: RR = 1.62 (95% CI, 1.44 to 1.81) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 3.84 (95% CrI, 2.0 to 7.14) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 3.66 (95% CI, 2.10 to 6.37) Licensed doses: OR = 4.23 (95% CI, 2.39 to 7.48) | |
Risankizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 11.96 (95% CrI, 8.60 to 16.86) |
Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 2.67 (95% CI, 2.33 to 3.07) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 6.25 (95% CrI, 3.70 to 10) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 7.18 (95% CI, 4.69 to 11.01) Licensed doses: OR = 7.47 (95% CI, 4.83 to 11.54) | |
Risankizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: risankizumab vs. ustekinumab 90mg, OR = 2.86 (95% CrI, 2.05 to 4.08) risankizumab vs. ustekinumab 45mg, OR = 3.27 (95% CrI, 2.43 to 4.50) risankizumab vs. ustekinumab (weight-based dosing), OR = 3.13 (95% CrI, 2.44 to 4.04) |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.67 (95% CI, 1.43 to 1.93) [3 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.56 (95% CI, 1.41 to 1.72) | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 3.14 (95% CI, 2.05 to 4.68) | |
Mahil et al., (2020)25 | Indirect evidence from NMA: All doses: OR = 3.23(95% CI, 2.27 to 4.59) Licensed doses: OR = 3.46 (95% CI, 2.41 to 4.96) | |
Shi et al., (2020)24 | Direct evidence: Ustekinumab (weight-based dosing) vs risankizumab 150 mg, OR = 0.27 (95% CI, 0.16 to 0.45) [2 RCTs]; I2 = 0% Ustekinumab (weight-based dosing) vs risankizumab 180 mg, OR = 0.15 (95% CI, 0.033 to 0.70) [1 RCT] Ustekinumab (weight-based dosing) vs risankizumab 18 mg, OR = 1.4 (95% CI, 0.37 to 0.5.1) [1 RCT] Ustekinumab (weight-based dosing) vs risankizumab 90 mg, OR = 0.24 (95% CI, 0.058 to 1.0) [1 RCT] Indirect evidence from NMA: Risankizumab 18 mg: vs. ustekinumab 45 mg, OR = 0.41 (95%CrI, 0.0039 to 4.3) vs. ustekinumab 90 mg, OR = 0.28 (95%CrI, 0.025 to 2.9) vs. ustekinumab weight-based dosing, OR = 0.63 (95%CrI, 0.11 to 3.6) Risankizumab 75 mg: vs. ustekinumab 45 mg, OR = 1.4 (95% CrI, 0.20 to 9.9) vs. ustekinumab 90 mg, OR = 0.96 (95% CrI, 0.13 to 6.8) vs. ustekinumab weight-based dosing, OR = 2.2 (95% CrI, 0.29 to 16) Risankizumab 90 mg: vs. ustekinumab 45 mg, OR = 15 (95% CrI, 0.81 to 6.8e + 02) vs. ustekinumab 90 mg, OR = 10 (95% CrI, 0.52 to 4.8e + 02) vs. ustekinumab weight-based dosing, OR = 2.2 (95% CrI, 2.0 to 8.1e + 02) Risankizumab 150 mg: vs. ustekinumab 45 mg, OR = 2.2 (95% CrI, 0.58 to 8.4) vs. ustekinumab 90 mg, OR = 1.5 (95% CrI, 0.37 to 5.9) vs. ustekinumab weight-based dosing, OR = 3.4 (95% CrI, 1.2 to 10) Risankizumab 180mg: vs. ustekinumab 45 mg, OR = 1.9 (95% CrI, 0.17 to 23) vs. ustekinumab 90 mg, OR = 1.3 (95% CrI, 0.11 to 16) vs. ustekinumab weight-based dosing, OR = 2.9(95% CrI, 0.46 to 20) | |
Long-term treatment (48 to 52 weeks) | ||
Secukinumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 1.91 (95% CrI, 1.35 to 2.71) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.29 (95% CrI, 1.09 to 1.76) Analysis 2: RR = 1.32 (95% CrI, 1.11 to 1.79) | |
Secukinumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.34 (95% CrI, 2.54 to 4.41) |
Yasmeen et al., (2020)22a | Indirect evidence from NMA: Analysis 1: RR = 1.76 (95% CrI, 1.31 to 2.71) Analysis 2: RR = 1.74 (95% CrI, 1.31 to 2.61) | |
Secukinumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: secukinumab vs. ustekinumab (weight-based dosing), OR = 1.66 (95% CrI, 1.42 to 1.95) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.22 (95% CrI, 1.08 to 1.49) Analysis 2: RR = 1.25 (95% CrI, 1.1to 1.53) | |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.23 (95% CI, 1.15 to 1.31) [2 RCTs]; I2 = 0% Indirect evidence from NMA: NR | |
Ixekizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.43 (95% CrI, 1.37 to 4.33) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.37 (95% CrI, 1.08 to 2.09) Analysis 2: RR = 1.4 (95% CrI, 1.12 to 2.06) | |
Ixekizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 4.24 (95% CrI, 2.51 to 7.26) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.87 (95% CrI, 1.32 to 3.24) Analysis 2: RR = 1.85 (95% CrI, 1.33 to 3.02) | |
Ixekizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: ixekizumab vs. ustekinumab (weight-based dosing), OR = 2.11 (95% CrI, 1.39 to 3.26) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.3 (95% CrI, 1.11 to 1.7) Analysis 2: RR = 1.33 (95% CrI, 1.13 to 1.73) | |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.30 (95% CI, 1.11 to 1.52) [1 RCT] Indirect evidence: NR | |
Brodalumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.49 (95% CrI, 2.21 to 5.52) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.51 (95% CrI, 1.17 to 2.37) Analysis 2: RR = 1.53 (95% CrI, 1.18 to 2.38) | |
Brodalumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 6.09 (95% CrI, 4.07 to 9.16) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 2.05 (95% CrI, 1.39 to 3.72) Analysis 2: RR = 2.02 (95% CrI, 1.39 to 3.52) | |
Brodalumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: brodalumab vs. ustekinumab (weight-based dosing), OR = 3.03 (95% CrI, 2.37 to 3.92) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.43 (95% CrI, 1.18 to 1.92) Analysis 2: RR = 1.46 (95% CrI, 1.19 to 1.97) | |
Risankizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 5.48 (95% CrI, 3.49 to 8.61) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.6 (95% CrI, 1.2 to 2.63) Analysis 2: RR = 1.62 (95% CrI, 1.21 to 2.61) | |
Risankizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 9.56 (95% CrI, 6.46 to 14.28) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 2.18 (95% CrI, 1.43 to 4.14) Analysis 2: RR = 2.13 (95% CrI, 1.42 to 3.86) | |
Risankizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: risankizumab vs. ustekinumab (weight-based dosing), OR = 4.76 (95% CrI, 3.64 to 6.29) |
Yasmeen et al., (2020)22 b | Indirect evidence from NMA: Analysis 1: RR = 1.52 (95% CrI, 1.2 to 2.15) Analysis 2: RR = 1.54 (95% CrI, 1.22 to 2.17) | |
Sbidian et al., (2021)20 | Direct evidence: RR = 1.73 (95% CrI, 1.46 to 2.05) [2 RCTs]; I2 = 20% Indirect evidence from NMA: NR | |
CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; PASI = Psoriasis Area Severity Index; RCT = randomized controlled trial; RR = risk ratio; vs. = versus.
Note: Direct evidence for pairwise comparisons may have been reported by more than 1 systematic review but are only presented once in the table to avoid reporting results in duplicate (where possible).
aFor all effect estimates (e.g., RR or OR), a value > 1 favours the first drug. .
b For studies from Yasmeen et al., 2020,22 Analysis 1 indicates an analysis of studies with comparative evidence at 52 weeks and Analysis 2 indicates an analysis of long-term extension studies and induction phase results for placebo patients who switched to active therapy in the long-term extension phase.
Table 5: Summary of Findings by Outcome — PASI 100
Comparison | Study citation and study design | Treatment responsea |
|---|---|---|
Short -term treatment (up to 16 or 24 weeks) | ||
Secukinumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.62 (95% CrI, 2.00 to 3.40) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 2.47 (95% CrI, 1.75 to 3.51) | |
Secukinumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 11.52 (95% CrI, 8.03 to 16.66) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 3.86 (95% CrI, 2.93 to 5.12) | |
Secukinumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: secukinumab vs. ustekinumab 90 mg, OR = 2.09 (95% CrI,1.53 to 2.92) secukinumab vs. ustekinumab 45 mg, OR = 2.43 (95% CrI, 1.83 to 3.27) secukinumab vs. ustekinumab (weight-based dosing), OR = 2.32 (95% CrI, 1.84 to 2.90) |
Xue et al., (2020)23 | Indirect evidence from NMA: secukinumab vs. ustekinumab 90 mg, RR = 1.32 (95% CrI, 0.99 to 1.76) secukinumab vs. ustekinumab 45 mg, RR = 1.63 (95% CrI, 1.28 to 2.05) | |
Ixekizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.78 (95% CrI, 2.80 to 5.05) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 3.56 (95% CrI, 2.61 to 4.98) | |
Ixekizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 16.60 (95% CrI, 11.31 to 24.53) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 5.57 (95% CrI, 4.42 to 7.18) | |
Ixekizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: ixekizumab vs. ustekinumab 90mg, OR = 3.02 (95% CrI, 2.15 to 4.32) ixekizumab vs. ustekinumab 45mg, OR = 3.51 (95% CrI, 2.58 to 4.85) ixekizumab vs. ustekinumab (weight-based dosing), OR = 3.35 (95% CrI, 2.52 to 4.39) |
Xue et al., (2020)23 | Indirect evidence from NMA: ixekizumab vs. ustekinumab 90mg, RR = 1.91 (95% CrI, 1.48 to 2.48) ixekizumab vs. ustekinumab 45mg, RR = 2.35 (95% CrI, 1.91 to 2.9) | |
Brodalumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.62 (95% CrI, 2.74 to 4.86) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 3.48 (95% CrI, 2.52 to 5.0) | |
Brodalumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 15.90 (95% CrI, 10.83 to 23.92) |
Xue et al., (2020)23 | Indirect evidence from NMA: RR = 5.43 (95% CrI, 4.09 to 7.51) | |
Brodalumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: brodalumab vs. ustekinumab 90mg, OR = 2.89 (95% CrI, 2.04 to 4.26) brodalumab vs. ustekinumab 45mg, OR = 3.36 (95% CrI, 2.45 to 4.78) brodalumab vs. ustekinumab (weight-based dosing), OR = 3.20 (95% CrI, 2.48 to 4.19) |
Xue et al., (2020)23 | Indirect evidence from NMA: brodalumab vs. ustekinumab 90mg, OR = 1.85 (95% CrI, 1.45 to 2.48) brodalumab vs. ustekinumab 45mg, OR = 2.29 (95% CrI, 1.86 to 2.88) | |
Risankizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.69 (95% CrI, 2.89 to 4.76) |
Risankizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 16.26 (95% CrI, 11.13 to 24.11) |
Risankizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: risankizumab vs. ustekinumab 90mg, OR = 2.95 (95% CrI, 2.09 to 4.29) risankizumab vs. ustekinumab 45mg, OR = 3.43 (95% CrI, 2.52 to 4.80) risankizumab vs. ustekinumab (weight-based dosing), OR = 3.27 (95% CrI, 2.53 to 4.25) |
Long-term treatment (48 to 52 weeks) | ||
secukinumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 1.93 (95% CrI, 1.34 to 2.81) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.53 (95% CrI, 1.17 to 2.33) Analysis 2: RR = 1.57 (95% CrI, 1.21 to 2.36) | |
Secukinumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.53 (95% CrI, 2.62 to 4.84) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 2.46 (95% CrI, 1.66 to 4.2) Analysis 2: RR = 2.4 (95% CrI, 1.65 to 3.9) | |
Secukinumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 1.67 (95% CrI, 1.43 to 1.95) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.4 (95% CrI, 1.16 to 1.88) Analysis 2: RR = 1.45 (95% CrI, 1.2 to 1.83) | |
Ixekizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.43 (95% CrI, 1.37 to 4.34) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.72 (95% CrI, 1.16 to 3.08) Analysis 2: RR = 1.76 (95% CrI, 1.25 to 2.94) | |
Ixekizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 4.45 (95% CrI, 2.60 to 7.66) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 2.75 (95% CrI,1.66 to 5.62) Analysis 2: RR = 2.67 (95% CrI, 1.71 to 4.93) | |
Ixekizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.10 (95% CrI, 1.40 to 3.16) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.57 (95% CrI, 1.21 to 2.27) Analysis 2: RR = 1.62 (95% CrI, 1.27 to 2.29) | |
Brodalumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 3.42 (95% CrI, 2.16 to 5.49) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 2.04 (95% CrI,1.37 to 3.76) Analysis 2: RR = 2.06 (95% CrI, 1.39 to 3.7) | |
Brodalumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 6.26 (95% CrI, 4.12 to 9.60) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 3.27 (95% CrI, 1.9 to 6.92) Analysis 2: RR = 3.13 (95% CrI, 1.87 to 6.27) | |
Brodalumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 2.96 (95% CrI, 2.35 to 3.73) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 1.87 (95% CrI, 1.42 to 2.71) Analysis 2: RR = 1.91 (95% CrI, 1.43 to 2.78) | |
Risankizumab vs. adalimumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 5.14 (95% CrI, 3.29 to 8.13) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 2.28 (95% CrI, 1.47 to 4.44) Analysis 2: RR = 2.28 (95% CrI, 1.49 to 4.27) | |
Risankizumab vs. etanercept | Armstrong et al., (2021)21 | Indirect evidence from NMA: risankizumab vs. etanercept, OR = 9.40 (95% CrI, 6.30 to 14.23) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 3.66 (95% CrI, 2.03 to 8.26) Analysis 2: RR = 3.47 (95% CrI, 1.98 to 7.29) | |
Risankizumab vs. ustekinumab | Armstrong et al., (2021)21 | Indirect evidence from NMA: OR = 4.44 (95% CrI, 3.49 to 5.68) |
Yasmeen et al., (2020)22b | Indirect evidence from NMA: Analysis 1: RR = 2.1 (95% CrI,1.5 to 3.28) Analysis 2: RR = 2.11 (95% CrI, 1.51 to 3.26) | |
CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; PASI = Psoriasis Area Severity Index; RCT = randomized controlled trial; RR = risk ratio.
Note: Direct evidence for pairwise comparisons may have been reported by more than 1 systematic review but are only presented once in the table to avoid reporting results in duplicate (where possible).
aFor all effect estimates (e.g., RR or OR), a value > 1 favours the first drug. .
b For studies from Yasmeen et al., 2020,22 Analysis 1 indicates an analysis of studies with comparative evidence at 52 weeks and Analysis 2 indicates an analysis of long-term extension studies and induction phase results for placebo patients who switched to active therapy in the long-term extension phase.
Table 6: Summary of Findings by Outcome — Adverse Events (Any)
Comparison | Study citation and study design | Treatment response |
|---|---|---|
Short -term treatment (up to 16 or 24 weeks) | ||
Secukinumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.10 (95% CI, 0.99 to 1.22) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.23 (95% CrI, 0.99 to 1.55) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.83 (95% CrI, 0.61 to 1.14) A value < 1 favours the first drug | |
Secukinumab vs. etanercept | Sbidian et al., (2021)20 | Direct evidence: RR = 1.00 (95% CI, 0.89 to 1.12) [1 RCT] Indirect evidence from NMA: RR = 1.05 (95% CI, 0.96 to 1.14) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.62 (95% CrI, 0.90 to 2.89) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.08 (95% CrI, 0.84 to 1.42) A value < 1 favours the first drug | |
Secukinumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.06 (95% CI, 0.98 to 1.16) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.07 (95% CI, 0.99 to 1.15) value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.14 (95% CrI, 0.96 to 1.35) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.88 (95% CrI, 0.69 to 1.13) A value < 1 favours the first drug | |
Ixekizumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.10 (95% CI, 0.99 to 1.23) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.24 (95% CrI,0.99 to 1.56) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.75 (95% CrI, 0.54 to 1.06) A value < 1 favours the first drug | |
Ixekizumab vs. etanercept | Sbidian et al., (2021)20 | Direct evidence: RR = 1.06 (95% CI, 0.97 to 1.15) [2 RCTs]; I2 = 11% Indirect evidence from NMA: RR = 1.05 (95% CI, 0.97 to 1.15) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.63 (95% CrI, 0.90 to 2.94) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.98 (95% CrI, 0.76 to 1.29) A value < 1 favours the first drug | |
Ixekizumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.03 (95% CI, 0.93 to 1.13) [1 RCT] Indirect evidence from NMA: RR = 1.07 (95% CI, 0.98 to 1.17) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.15 (95% CrI, 0.89 to 1.46) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.81 (95% CrI, 0.61 to 1.07) A value < 1 favours the first drug | |
Brodalumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.07 (95% CI, 0.95 to 1.21) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.18 (95% CrI, 0.94 to 1.50) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.84 (95% CrI, 0.60 to 1.19) A value < 1 favours the first drug | |
Brodalumab vs. etanercept | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.02 (95% CI, 0.92 to 1.14) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.54 (95% CrI, 0.86 to 2.77) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.09 (95% CrI, 0.81 to 1.49) A value < 1 favours the first drug | |
Brodalumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.00 (95% CI, 0.93 to 1.09) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.04 (95% CI, 0.95 to 1.15) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.09 (95% CrI, 0.90 to 1.32) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 0.90 (95% CrI, 0.68 to 1.19) A value < 1 favours the first drug | |
Risankizumab vs. adalimumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.08 (95% CI, 0.82 to 1.43) [1 RCT] Indirect evidence from NMA: RR = 0.99 (95% CI, 0.87 to 1.12) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.87 (95% CrI, 0.70 to 1.09) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.12 (95% CrI, 0.73 to 1.72) A value < 1 favours the first drug | |
Risankizumab vs. etanercept | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 0.95 (95% CI, 0.84 to 1.06) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.14(95% CrI, 0.63 to 2.07) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.46 (95% CrI, 0.99 to 2.18) A value < 1 favours the first drug | |
Risankizumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 0.97 (95% CI, 0.85 to 1.11) [3 RCTs]; I2 = 9% Indirect evidence from NMA: RR = 0.96 (95% CI, 0.87 to 1.07) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.80 (95% CrI, 0.64 to 1.01) A value > 1 favours the first drug | |
Xu et al., (2021)18 | Indirect evidence from NMA: RR = 1.19 (95% CrI, 0.84 to 1.72) A value < 1 favours the first drug | |
Shi et al., (2020)24 | Direct evidence: Ustekinumab (weight-based dosing) vs risankizumab 150 mg, OR = 1.5 (95% CI, 0.88 to 2.6) [2 RCTs]; I2 = 0% Ustekinumab (weight-based dosing) vs risankizumab 180 mg, OR = 1.2 (95% CI, 0.30 to 0.44) [1 RCT] Ustekinumab (weight-based dosing) vs risankizumab 18 mg, OR = 0.60 (95% CI, 0.11 to 0.27) [1 RCT] Ustekinumab (weight-based dosing) vs risankizumab 90 mg, OR = 0.82 (95% CI, 0.15 to 2.7) [1 RCT] Indirect evidence from NMA: Risankizumab 18 mg: vs. ustekinumab 45 mg, OR = 2.1 (95% CrI, 0.56 to 9.2) vs. ustekinumab 90 mg, OR = 2.1 (95% CrI, 0.54 to 8.7) vs. ustekinumab weight-based dosing, OR = 1.7 (95% CrI, 0.51 to 5.6) Risankizumab 75 mg: vs. ustekinumab 45 mg, OR = 0.68 (95% CrI, 0.28 to 1.8) vs. ustekinumab 90 mg, OR = 0.70 (95% CrI, 0.26 to 1.7) vs. ustekinumab weight-based dosing, OR = 0.54 (95% CrI, 0.20 to 1.4) Risankizumab 90 mg: vs. ustekinumab 45 mg, OR = 2 (95% CrI, 0.47 to 8.7) vs. ustekinumab 90 mg, OR = 2.0 (95% CrI, 0.45 to 8.3) vs. ustekinumab weight-based dosing, OR = 1.6 (95% CrI, 0.45 to 5.4) | |
Risankizumab 150 mg: vs. ustekinumab 45 mg, OR = 0.76 (95% CrI, 0.44 to 1.5) vs. ustekinumab 90 mg, OR = 0.78 (95% CrI, 0.42 to 1.4) vs. ustekinumab weight-based dosing, OR = 0.61 (95% CrI, 0.34 to 1.1) Risankizumab 180mg: vs. ustekinumab 45 mg, OR = 1.0 (95% CrI, 0.29 to 4.3) vs. ustekinumab 90 mg, OR = 1.1 (95% CrI, 0.28 to 4.0) vs. ustekinumab weight-based dosing, OR = 0.83 (95% CrI, 0.28 to 2.6) | ||
Long-term treatment (48 to 52 weeks) | ||
Secukinumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.22 (95% CrI, 0.77 to 1.93) A value > 1 favours the first drug |
Secukinumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.98 (95% CrI, 0.79 to 1.22) A value > 1 favours the first drug |
Ixekizumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.58 (95% CrI, 0.69 to 3.64) A value > 1 favours the first drug |
Ixekizumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.27 (95% CrI, 0.67 to 2.47) A value > 1 favours the first drug |
Risankizumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.77 (95% CrI, 0.41 to 1.46) A value > 1 favours the first drug |
Risankizumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.62 (95% CrI, 0.42 to 0.91) A value > 1 favours the first drug |
CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio.
Note: Direct evidence for pairwise comparisons may have been reported by more than 1 systematic review but are only presented once in the table to avoid reporting results in duplicate (where possible).
Table 7: Summary of Findings by Outcome — Serious Adverse Events
Comparison | Study citation and study design | Treatment response |
|---|---|---|
Secukinumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.02 (95% CI, 0.58 to 1.79) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.35 (95% CrI, 0.57 to 3.14) A value > 1 favours the first drug | |
Secukinumab vs. etanercept | Sbidian et al., (2021)20 | Direct evidence: RR = 1.08 (95% CI, 0.41 to 2.82) [1 RCT] Indirect evidence from NMA: RR = 1.21 (95% CI, 0.72 to 2.03) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.68 (95% CrI, 0.31 to 9.45) A value > 1 favours the first drug | |
Secukinumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.26 (95% CI, 0.70 to 2.30) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.12 (95% CI, 0.73 to 1.72) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.30 (95% CrI, 0.70 to 2.51) A value > 1 favours the first drug | |
Ixekizumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.08 (95% CI, 0.60 to 1.96) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.36 (95% CrI, 0.56 to 3.45) A value > 1 favours the first drug | |
Ixekizumab vs. etanercept | Sbidian et al., (2021)20 | Direct evidence: RR = 1.07 (95% CI, 0.55 to 2.06) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.28 (95% CI, 0.77 to 2.13) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.70 (95% CrI, 0.30 to 10.26) A value > 1 favours the first drug | |
Ixekizumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 6.09 (95% CI, 0.30 to 125.89) [1 RCT] Indirect evidence from NMA: RR = 1.19 (95% CI, 0.67 to 2.12) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.31 (95% CrI, 0.51 to 3.63) A value > 1 favours the first drug | |
Brodalumab vs. adalimumab | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.04 (95% CI, 0.53 to 2.04) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.98 (95% CrI, 0.38 to 2.42) A value > 1 favours the first drug | |
Brodalumab vs. etanercept | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 1.23 (95% CI, 0.64 to 2.37) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.20 (95% CrI, 0.21 to 7.04) A value > 1 favours the first drug | |
Brodalumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.51 (95% CI, 0.64 to 3.56) [2 RCTs]; I2 = 0% Indirect evidence from NMA: RR = 1.15 (95% CI, 0.64 to 2.06) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.94 (95% CrI, 0.42 to 2.15) A value > 1 favours the first drug | |
Risankizumab vs. adalimumab | Sbidian et al., (2021)20 | Direct evidence: RR = 1.12 (95% CI, 0.46 to 2.72) [1 RCT] Indirect evidence from NMA: RR = 0.70 (95% CI, 0.4 to 1.22) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.61 (95% CrI, 0.28 to 1.27) A value > 1 favours the first drug | |
Risankizumab vs. etanercept | Sbidian et al., (2021)20 | Indirect evidence from NMA: RR = 0.83 (95% CI, 0.46 to 1.50) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.76 (95% CrI, 0.14 to 4.30) A value > 1 favours the first drug | |
Risankizumab vs. ustekinumab | Sbidian et al., (2021)20 | Direct evidence: RR = 0.57 (95% CI, 0.24 to 1.32) [3 RCTs]; I2 = 35% Indirect evidence from NMA: RR = 0.77 (95% CI, 0.48 to 1.26) A value < 1 favours the first drug |
Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.59 (95% CrI, 0.28 to 1.29) A value > 1 favours the first drug | |
LONG-TERM (48 to 52 weeks) | ||
Secukinumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.29 (95% CrI, 0.54 to 3.14) A value > 1 favours the first drug |
Secukinumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.23 (95% CrI, 0.83 to 1.85) A value > 1 favours the first drug |
Ixekizumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 2.04 (95% CrI,0.48 to 9.05) A value > 1 favours the first drug |
Ixekizumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 1.94 (95% CrI, 0.67 to 6.05) A value > 1 favours the first drug |
Risankizumab vs. adalimumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.80 (95% CrI, 0.26 to 2.51) A value > 1 favours the first drug |
Risankizumab vs. ustekinumab | Shear et al., (2021)19 | Indirect evidence from NMA: OR = 0.76 (95% CrI, 0.43 to 1.40) A value > 1 favours the first drug |
CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio.
Note: Direct evidence for pairwise comparisons may have been reported by more than 1 systematic review but are only presented once in the table to avoid reporting results in duplicate (where possible).
Appendix 5: References of Potential Interest
Previous CADTH Reports
37.Adalimumab for adult patients with plaque psoriasis: a review of clinical effectiveness. Ottawa: CADTH; 2020 Jun. (CADTH rapid response report: summary with critical appraisal). https://cadth.ca/adalimumab-adult-patients-plaque-psoriasis-review-clinical-effectiveness
Review Articles
38.Wright E, Yasmeen N, Malottki K, et al. Assessing the Quality and Coherence of Network Meta-Analyses of Biologics in Plaque Psoriasis: What Does All This Evidence Synthesis Tell Us? Dermatol Ther (Heidelb). 2021 Feb;11(1):181-220. PubMed
39.Karpińska-Mirecka A, Bartosińska J, Krasowska D. The effects of selected biologics and a small molecule on Health-Related Quality of Life in adult plaque psoriasis patients: A systematic review and meta-analysis. PLoS ONE [Electronic Resource]. 2020;15(12):e0241604. PubMed
40.Sandhu VK, Ighani A, Fleming P, Lynde CW. Biologic Treatment in Elderly Patients With Psoriasis: A Systematic Review. J Cutan Med Surg. 2020 Mar/Apr;24(2):174-186. PubMed
41.Egeberg A, Andersen YMF, Halling-Overgaard AS, et al. Systematic review on rapidity of onset of action for interleukin-17 and interleukin-23 inhibitors for psoriasis. J Eur Acad Dermatol Venereol. 2020 Jan;34(1):39-46. PubMed
42.van Winden MEC, van der Schoot LS, van de L'Isle Arias M, et al. Effectiveness and Safety of Systemic Therapy for Psoriasis in Older Adults: A Systematic Review. JAMA Dermatol. 2020 11 01;156(11):1229-1239. PubMed
43.Witjes H, Khatri A, Diderichsen PM, Mandema J, Othman AA. Meta-Analyses of Clinical Efficacy of Risankizumab and Adalimumab in Chronic Plaque Psoriasis: Supporting Evidence of Risankizumab Superiority. Clin Pharmacol Ther. 2020 02;107(2):435-442. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca