CADTH Health Technology Review
Antibiotic Solutions for Surgical Irrigation
Rapid Review
Authors: Nazia Darvesh, Robyn Butcher
Abbreviations
CC
capsular contracture
CDC
Centers for Disease Control and Prevention
CHG
chlorhexidine gluconate
CRP
C-reactive protein
MA
meta-analysis
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
RCT
randomized controlled trial
SR
systematic review
SSI
surgical site infection
TAS
triple antibiotic solution
UTI
urinary tract infection
Key Messages
During surgery, wounds can be washed out, or irrigated, using antibiotic, antiseptic, or saline solutions to prevent infections; the evidence in this report found over 20 different antibiotic solutions used across trials.
Most studies showed that antibiotic irrigation solutions were better or no different compared to using antiseptic, saline, or no irrigation; however, a small number of studies indicated otherwise. One study reported in a systematic review showed fewer infections and complications for antiseptic compared to a triple antibiotic solution, while another study included in the same systematic review found a higher percentage of implant loss when a triple antibiotic solution was compared to antiseptic; data were poorly reported in these studies.
Bacitracin-specific evidence was found in 2 studies; 1 study reported in 1 systematic review showed a higher percentage of infection when bacitracin irrigation was compared to cefazolin and saline irrigation; however, this was not statistically significant. Another study showed no differences in infections requiring surgical intervention or in hospitalization when bacitracin irrigation was compared to no irrigation.
One guideline recommends that wound irrigation and intracavity lavage should not be conducted during surgery, and that applying antibiotics before wound closure should only be done as part of a research trial.
Due to the mixed findings across studies, high-quality research is needed to clarify the role of antibiotic irrigation during surgery. Because guideline recommendations about wound irrigation, specifically, are based on research published before 2008, updated guidelines to include research from more current studies are needed to reflect current practice.
Context and Policy Issues
A surgical site infection (SSI) is an infection localized to the site where a surgery was performed.1 SSIs occur after surgery and can involve skin, tissues, organs, or implanted material below the skin.1 According to the Canadian Patient Safety Institute, 26,000 to 65,000 patients are affected by SSIs per year.2 Several practices may be undertaken to prevent SSIs, and these can take place before (preoperative), during (intraoperative), and after (post-operative) surgery.3 One method to manage wounds from surgeries is intraoperative irrigation with a fluid to remove loose material and decrease bacterial load.4 A similar technique called intracavity lavage also reduces the risk of SSI when body cavities are exposed during surgery.5 Saline, antiseptic, and antibiotic fluid solutions have been used to perform irrigation during surgery.4 However, there are several concerns about using irrigation, including whether fluid can wash away important inflammatory cells needed for healing.6 In addition, there are questions about the potential of antibiotics to prevent normal healing, damage tissue, or contribute to antimicrobial resistance with overuse.6 Further to these concerns, Health Canada conducted a safety review that showed that the antibiotic bacitracin may increase the risk of hypersensitivity, nephrotoxicity, allergic contact dermatitis, or anaphylaxis.7 The guidance from Health Canada is that bacitracin is not indicated as an irrigation solution for prophylaxis during surgical procedures because patients may experience nephrotoxicity and anaphylactic reactions.7
Given the uncertainty around using antibiotic solutions for surgical irrigation, a review to determine the clinical effectiveness of antibiotic solutions for irrigation during surgery is necessary. In 2021, CADTH compiled a reference list of relevant publications identified from a literature search.8 The current report is an upgrade to that CADTH reference list.8 The objectives of this rapid review are to summarize the evidence regarding the clinical effectiveness of antibiotic solutions used for irrigation in any surgery, and to determine evidence-based guidelines regarding the use of antibiotic irrigation solutions to prevent surgical infections.
Research Questions
What is the clinical effectiveness of antibiotic solutions used in surgical irrigation?
What are the evidence-based guidelines regarding the use of antibiotic solutions for surgical irrigation to prevent infection?
Methods
Literature Search Methods
This report makes use of a literature search developed for a previous CADTH report.8 For the previous report, a limited literature search was conducted by an information specialist on key resources, including MEDLINE, Embase, the Cochrane Library, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were antibiotic irrigation and surgery. Search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses (MAs), or network meta-analyses (NMAs), randomized controlled trials (RCTs) or controlled clinical trials, or guidelines. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2011, and September 30, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals (of any age) undergoing any type of surgery |
Intervention | Antibiotic solutions used in surgical irrigation (e.g., bacitracin, vancomycin, cefazolin, gentamicin, metronidazole, clindamycin, ceftriaxone) |
Comparator | Q1: Standard of care, non-antibiotic irrigation solutions (e.g., saline solution, antiseptic solutions [e.g., chlorhexidine, povidone-iodine, acetic acid, sodium hypochlorite]), and/or IV infusion of preoperative antibiotic prophylaxis Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., surgery-related infections, post-operative infections up to 30 days post-surgery, wound healing, length of stay in hospital, and safety). Q2: Recommendations regarding the use of antibiotic solutions in surgical irrigation |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or if they were duplicate publications. Where the intervention included antiseptic, antifungal, steroid, or hormone, the study was excluded. Non-solution versions of the intervention (e.g., oral, powder, drops, ointment, cream, foam) or interventions where items were impregnated with antibiotics were excluded. Only interventions that took place during the intraoperative phase were included or summarized. Comparisons between 2 antibiotics were excluded. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 29 for SRs, the “questionnaire to assess the relevance and credibility of a network meta-analysis”10,11 for NMAs, the Downs and Black checklist12 for RCTs, and the Appraisal of Guidelines for Research and Evaluation II instrument13 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
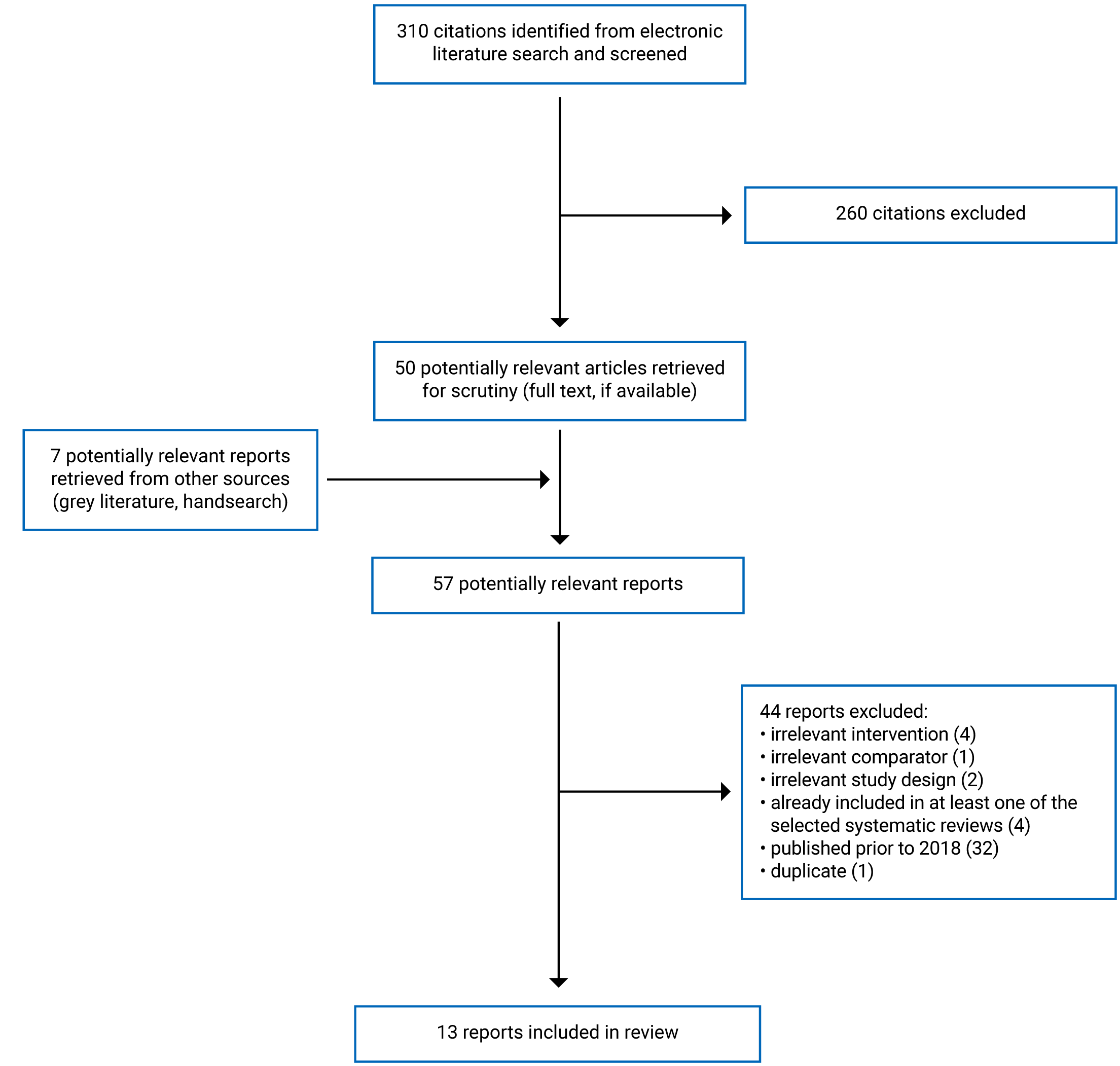
A total of 310 citations were identified in the literature search. Following screening of titles and abstracts, 260 citations were excluded and 50 potentially relevant reports from the electronic search were retrieved for full-text review. Seven potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 44 publications were excluded for various reasons, and 13 publications met the inclusion criteria and were included in this report. These comprised 5 SRs,6,14-17 7 RCTs,18-24 and 1 evidence-based guideline reported in 2 publications.25,26 Appendix 1 presents the PRISMA27 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Study Design
The 5 included SRs6,14-17 were published between 2018 and 2021 and they had broader inclusion criteria than the scope of this review. An SR by Baker et al.14 looked at irrigation during implant-based breast surgery using various irrigation solutions of antibiotics and/or antiseptics. The search dates for the SR14 were unclear, and included 4 retrospective cohort studies that reported interventions and comparators of interest to the current review. An SR by Saeg et al.17 included any study about wound irrigation published from January 2000 to March 2020, which comprised 1 MA, 2 SRs, and 2 retrospective cohort studies with interventions and comparators relevant to the current review. An SR about antimicrobial irrigation by Leas15 included literature published from 2017 to 2021, and had 1 study that was relevant to the current review. It should be noted that the primary study was also included in the SR by Saeg et al.;17 however, the relevant aspects for this report were described in more detail in the Leas publication.15 An SR with NMA by Thom et al.6 included literature published up to February 1, 2017, covering any surgery, and had 20 RCTs relevant to the current review. An SR with MA by López-Cano et al.16 included literature published up to January 31, 2017, covering any surgery, and had 10 RCTs relevant to the current review. There was some overlap in the primary studies that were included in the SRs; therefore, the narrative summaries and pooled estimates from the SRs may contain some data from the same RCTs. This overlap is presented in Appendix 5, Table 17. Across all 5 SRs6,14-17 in the current report, population sizes ranged from 14 patients to 8,892 patients, all studies reported on infections, and follow-up time ranged from 8 days to 1 year.
Seven RCTs18-24 published between 2018 and 2021 were included. One study by Krahn et al.19 was a cluster randomized crossover trial. All studies included some form of blinding. Six studies were conducted at 1 centre18,20-24 and 1 study was conducted across 28 centres in Canada and the Netherlands.19 In 6 RCTs, patients were randomized,18-21,23,24 and in 1 RCT, mastectomy pockets were randomized.22 Across the 7 RCTs,18-24 population sizes ranged from 40 to 19,603 and follow-up time ranged from 1 week to 606 days.
One guideline published in 201926 by the National Institute for Health and Care Excellence (NICE) on prevention and treatment of SSIs is included in the current review. This guideline was an update to a 2008 guideline.25 In this report, both the 201926 and 200825 publications are referenced for completeness of reporting. The recommendations for wound irrigation and intracavity lavage were based on the 2008 guideline,25 and the recommendations for antiseptics and antibiotics before wound closure were based on the 2019 guideline.26 Although the NICE guidelines do not provide recommendations specifically for antibiotics, they provide recommendations for wound irrigation, intracavity lavage, and general antiseptic and antibiotic application before wound closure.
Both the 2008 and 2019 versions of the guideline were developed by searching in 6 or more databases and scanning reference lists. The 2008 guideline assessed quality using 8 hierarchical levels with informal and formal consensus steps, while the 2019 guideline used Risk of Bias in Systematic Reviews, the Cochrane risk of bias tool, Risk Of Bias In Non-randomised Studies – of Interventions, and Grading of Recommendations Assessment, Development and Evaluation, depending on study design with a committee discussion of the evidence.
Country of Origin
Three SRs14,15,17 were from the US, 1 SR6 was from England, and 1 SR was from Spain.16 Among the included RCTs, 3 were from the US,20,22,24 1 from Egypt,18 1 from Iran,21 1 from Nigeria,23 and 1 was a study conducted across multiple centres in Canada and the Netherlands.19 The included guideline is for those working in the UK or using services of the National Health Service in England, Wales, and Northern Ireland.25
Patient Population
Three SRs included relevant studies of patients undergoing breast surgery,14,15,17 1 SR included relevant studies of patients undergoing surgeries with primary site closures,6 and 1 SR included relevant studies of patients undergoing various procedures such as abdominal, trauma, biliary tract, colorectal, hernia, breast, soft tissue, or cardiovascular surgeries.16 One SR6 reported that studies had patients of varying age groups, mostly adults, and that some studies such as those with Caesarean sections enrolled only women. Other SRs did not specify age, gender, or sex of included populations.
Across RCTs, included populations were patients undergoing breast reconstruction,22 open appendectomy,18 laparoscopic colectomy,21 neurosurgical procedures,23 benign gynecologic surgery,24 nonemergent open pancreatoduodenectomy,20 or cardiac implantable electronic device procedures.19 The mean age ranged from 27.9 to 72.0 years across the RCTs. Two RCTs included only female patients,22,24 2 RCTs did not specify gender,20,21 1 RCT had a greater proportion of patients who were female,18 1 RCT had a greater proportion of patients who were male.23 One RCT19 reported 33.9% patients who were female and did not specify gender for the remaining population. Recognizing that gender and sex are different, gendered terms used in this report reflect the reporting in the included studies, and it is unclear how these terms were defined and measured.
For the included guideline,25,26 the target population is children, young people, and adults undergoing surgery involving a skin cut. The intended users of the guideline are people having surgeries and their carers, health care professionals, and commissioners and providers.
Interventions and Comparators
Relevant interventions across studies varied and included irrigation and lavage with single or multiple antibiotics solutions such as ampicillin, bacitracin, cefamandole, cefazolin, cefotaxime, cefotetan, cefoxin, cefoxitin, cefuroxime, cephaloridine, cephalothin, cephapirin, cephradine, chloramphenicol, gentamicin with clindamycin, gentamicin, kanamycin with cephalothin, kanamycin, moxalactam, neosporin, polymyxin B, triple antibiotic solution (TAS), taurolin, or tetracycline. All studies that reported TAS as an intervention were included in this report because TAS used in Canada commonly includes a mixture of bacitracin, cefazolin, and gentamicin, which are applicable to the current review. Relevant comparators across studies included saline irrigation and lavage, chlorhexidine gluconate irrigation, or no irrigation. One SR with MA16 included studies that compared antibiotic irrigation to placebo, where the placebo arm comprised patients who did not have prophylactic topical antibiotic agents, other antibiotics, or antiseptic. In this report, the results for this study are reported in the results for antibiotic irrigation compared to no irrigation.
The specific procedures for surgeries varied across studies. Only antibiotic-related surgical processes are described in this report. In the Nguyen et al. study,22 all patients were given cefazolin intravenously at least 30 minutes before the surgery. The TAS intervention consisted of 50,000 U of bacitracin, 1 g of cefazolin, and 80 mg of gentamicin in 500 mL of normal saline.22 The chlorhexidine gluconate control contained 0.05% chlorhexidine gluconate in sterile water.22 After surgery, all patients were given cefazolin intravenously for 24 hours or until discharge followed by a 14-day treatment of oral sulfamethoxazole and trimethoprim DS 800 mg/160 mg 2 times per day (100 mg doxycycline 2 times per day for patients who had sulfa allergies).22
In the Emile et al. study,18 all patients were given 2 g of cefotaxime and 500 mg of metronidazole at anesthesia induction as part of antibiotic prophylaxis. The interventions were either 160 mg of gentamicin in 400 mL of normal saline (0.9% sodium chloride) or normal saline alone applied using a 20 cm syringe to irrigate each layer of the wound before closure.18 In the control group, layer-by-layer wound closure was performed with polyglactin 2/0 sutures and no irrigation.18 All patients received 1 g of cefotaxime intravenously within 12 hours of their incisions being closed.18
In the Negahi et al. study,21 the intervention group received lavage with a suction-irrigation machine containing 240 mg of gentamicin and 600 mg of clindamycin dissolved in 500 mL of sterile saline, and the control group received lavage with 500 mL of sterile saline only.
In the Okunlola et al. study,23 both study groups were given 2 g of parenteral ceftriaxone intravenously when anesthesia commenced and 1 g of ceftriaxone intravenously every 12 hours for 24 hours after surgery. In addition, the intervention group received irrigation with 250 mg/mL of ceftriaxone in normal saline and the control group received plain normal saline irrigation using jet and droplets from a 50 mL syringe.
In the Slopnick et al. study,24 the intervention group received irrigation of a solution containing 200,000 U polymyxin B sulphate and 40 mg neomycin sulphate, while the control group had irrigation with normal saline only. All patients received cefazolin for antibiotic prophylaxis and metronidazole for hysterectomy in patients who were premenopausal unless patients were allergic.24
In the Maatman et al. study,20 the intervention group received irrigation with polymyxin B, 500,000 U in 1 L of normal saline, and the control group received irrigation with 1 L of 0.9% sodium chloride. In both cases, 2 L of each solution was used for irrigation.20 All patients were given 2 g of IV ceftriaxone and 1 g of IV metronidazole within 60 minutes of skin incision.20
In the randomized crossover trial,19 there were 4 randomly assigned 6-month periods where participating centres used different sequences of incremental or conventional procedures. In the conventional period, a single dose of cefazolin (1 g to 2 g) was given intravenously 60 minutes before skin incision. If patients were allergic to penicillin, vancomycin (1 g to 1.5 g) was given intravenously 120 minutes before skin incision. In addition to the aforementioned procedure with cefazolin or vancomycin, the incremental period applied an intraoperative wound pocket wash using bacitracin 50,000 U diluted in 50 mL of saline before skin closure, and patents were given oral cephalexin (500 mg 4 times per day) or cephadroxil (1,000 mg 2 times per day for 2 days) after the operation. For patients who were allergic to penicillin, clindamycin 150 mg to 300 mg was prescribed 3 times per day. Thus, regarding this report, the relevant comparison in the study19 was between antibiotic irrigation with bacitracin pocket wash and no irrigation. Authors of the study19 reported that bacitracin was not available at 1 Canadian site and at all Netherlands sites, so cefazolin or saline pocket wash was administered. Limitations of this procedural change are discussed in the Summary of Critical Appraisal section.
The NICE guideline25,26 considered all methods before, during, and after surgery to minimize surgery risk. However, the current review focuses only on aspects relating to intraoperative methods for wound irrigation, intracavity lavage, and antibiotic application before wound closure.
Outcomes
Several outcomes were reported across the SRs and RCTs: infection-related outcomes (including SSI, infection requiring surgical intervention, white blood cell count, C-reactive protein [CRP]), capsular contracture (CC), hospital-related outcomes (hospital stay, hospitalization for infection), pain-related outcomes (pain, painkiller needed), patient satisfaction, wound-related outcomes (necrosis, hematoma, seroma, wound dehiscence, wound infection), adverse events and complications (including surgical site occurrence, urine retention or ileus, intra-abdominal abscess, bowel obstruction, intestinal fistula, urinary tract infection (UTI), implant loss, allergic reaction, pancreatic fistula, organ failure, sepsis, delayed gastric emptying, bile leak, venous thromboembolism, cholangitis, myocardial infarction), and death.
Several studies did not provide definitions or had unclear definitions for outcomes. For studies that defined outcomes, 1 SR6 and 2 RCTs18,22 referenced the Centers for Disease Control and Prevention (CDC) definition for SSIs. The CDC definition of an SSI is an infection that happens after surgery in the area of the body (incision, organ, or space) where the surgery occurred.28,29 In the Nguyen et al. study,22 SSIs were further classified as minor if patients required oral antibiotics; major if patients required IV antibiotics, hospitalization, or incision and washout; or referred to as explantation if patients needed a bilateral explant after developing a persistent non-infectious rash. In the Krahn et al. study,19 hospitalization for pocket or cardiac implantable electronic device infections was categorized as pocket infection, endocarditis, or bloodstream infection. In the Maatman et al. study, SSIs were defined using another study30 that monitored and reported on SSIs over a 2-year period.
Pain was measured in the Emile et al. study18 at the 1-week follow-up using the Visual Analogue Scale, which ranged from 0 to 10, with 0 indicating absence of pain at incision site and 10 implying worse severe pain at incision site.
Patient satisfaction with the outcome of the surgery was measured in the Emile et al. study18 at the 6-week follow-up as unsatisfied, partly satisfied, or completely satisfied indicating causes of dissatisfaction, if applicable.
Surgical site occurrence was measured in the Emile et al. study18 and included SSI, necrosis, cellulitis, serous or purulent drainage, chronic and/or non-healing wound, seroma, hematoma, wound dehiscence, or fistula at the surgical site.
UTI was measured in the Slopnick et al. study24 at 6 weeks post-surgery. This study adapted the CDC’s definition of a symptomatic UTI: “(1) at least one sign or symptom accompanied by positive urine culture with ≥105 colony‐forming units/mL, (2) symptomatic UTI with clinician decision to treat as reported by the patient, or (3) at least one sign or symptom with positive urine dipstick.”24
Post-operative pancreatic fistula was defined using the definition from the International Study Group on Pancreatic Fistula with a fluid drain output at 3 or more days after surgery and amylase greater than 3 times the upper limit of laboratory normal. Clinically relevant post-operative pancreatic fistula were those graded as B or C as defined by the International Study Group on Pancreatic Fistula.
The 2008 version25 of the NICE guideline considered wound infection rates and SSI, and the 2019 version26 of the guideline considered SSI, mortality, hospital stay, post-operative antibiotic use, adverse events, and complications.
Additional details regarding the characteristics of the included publications are provided in Appendix 2, Table 2, Table 3, and Table 4.
Summary of Critical Appraisal
Systematic Reviews
All 5 SRs6,14-17 described the interventions and outcomes of interest clearly, 4 SRs6,14-16 described the specific study populations of interest, and 3 SRs6,15,16 stated comparator groups of interest. All SRs6,14-17 included literature from at least 2 databases, which is a strength; however, only 3 SRs6,16,17 supplemented searches with reference list scanning, and 1 SR with NMA6 consulted clinical trial registries and reference lists of other relevant SRs. No SRs reported searching grey literature, which limits the breadth of literature found in these SRs. Only 2 SRs15,16 established protocols before review conduct; it is unclear, for the remaining SRs,6,14,17 whether outcomes of interest were established before review conduct.
In 3 SRs,14,16,17 screening and data extraction were conducted by at least 2 reviewers. In 1 SR,6 2 reviewers screened articles and appraised risk of bias; however, it is unclear whether data extraction was also conducted in duplicate. In 1 SR,15 it is unclear whether study selection and extraction was conducted in duplicate. In SRs where screening and data extraction were not completed in duplicate, is unclear if there was any bias in the study selected or potential errors in the data extracted and reported from these publications.
The level of detail provided about each included study varied across SRs and no SRs provided sufficient detail on all study characteristics. In 4 SRs,6,15-17 authors described interventions, comparators, outcomes, and study designs in detail, which is a strength, but patient populations were not described in sufficient detail. One SR14 did not provide further details on populations, interventions, comparators, and outcomes. Insufficient detail on any study characteristics may limit how the results from these SRs can be applied to other contexts. Three SRs6,15,16 used an appropriate method to assess risk of bias. One SR14 did not report assessing risk of bias. Another SR17 used a method to assess bias but it did not consider study design, confounding, unconcealed allocation, outcome measurement, or reporting bias, and bias was not accounted for when reporting results. For these latter 2 SRs,14,17 since the risk of bias assessment was not sufficiently completed, the interpretation of results may be limited because the quality of the evidence is unknown. In addition, for 3 SRs,6,14,17 it is unclear how the reported conflicts of interest or funding may have affected the reporting of the results.
Heterogeneity across studies was considered and described in 4 SRs,6,14,16,17 which is a strength. In the 1 SR15 that did not discuss heterogeneity, the impact of potential heterogeneity on the results is unknown. Strengths of the 2 SRs6,16 that conducted quantitative analyses include that both studies applied appropriate methods for combination of results while taking heterogeneity and risk of bias of individual studies into account. Further, the strengths of the SR with NMA6 are that both direct and indirect comparisons were included, inconsistency was assessed, results from individual studies were provided, treatment effect estimates with measures of uncertainty and a rank probability plot with uncertainty were provided, heterogeneity was explored through additional analyses by important patient or publication characteristics. The limitations of the SR with NMA6 are that the results are likely biased due to unexplained high heterogeneity and the low quality of individual studies. This limits the conclusions that can be drawn from this SR with NMA.6
Randomized Controlled Trials
All 7 RCTs18-24 sufficiently described their objectives, interventions, and main outcomes, and 4 RCTs18,20,22,24 clearly described patient characteristics, which is a strength. Further, randomization occurred in all 7 RCTs18-24 to balance intervention and control groups as much as possible so that effects could be attributed to the intervention; however, in the Nguyen et al. study,22 it remains unclear whether the investigators used appropriate allocation techniques to prevent selection bias. In the randomized crossover trial,19 since bacitracin was unavailable at 1 Canadian site and all Netherlands sites, a cefazolin or saline pocket wash was administered instead; the results may have been biased because the intervention and comparator groups did not match across study groups. All SRs18-24 included blinding of study personnel. Three RCTs19,21,22 had no blinding or unclear blinding of patients; however, because the intervention took place during surgery, it is unlikely that patients would discover what infection prevention protocol they received.
Five RCTs18,21-24 occurred at single centres and patients were likely from the same population; however, these patients may not be generalizable to other populations beyond these clinical settings. One RCT20 did not clarify if it took place at a single centre or multiple centres.
Five RCTs18-20,22,23 described main findings and 5 SRs18-20,22,24 described covariates in sufficient detail. Two RCTs21,24 did not report complete details, which may limit understanding of the results. Further, 4 RCTs20-23 did not report clearly on controlling for potential confounders so it is unclear if the results may be biased. It is unclear if statistical tests could adequately answer the research question in 6 RCTs.18,20-24 In 2 RCTs,22,23 authors noted that their studies had small sample sizes; these studies may not have been sufficiently powered to detect any effects. In 1 RCT,21 a power calculation was not provided so the power is unclear, and in another RCT,24 the study sample was smaller than what the power calculation required. In 1 RCT,18 the study had sufficient power, but the data were analyzed using a per-protocol approach that did not reflect the randomization assignment and may have biased results. In 1 RCT,24 some covariates were not adjusted for, and in another RCT,20 the low infection rate could not be explained.
Four RCTs18-20,24 had minimal to no loss to follow-up. In 1 RCT,19 there was higher noncompliance in the intervention group, which was mainly attributed to administration of oral antibiotics before surgery. In addition, 2 RCTs21,23 had unclear follow-up and 1 RCT22 had early termination. Within each study, these differences between groups may have biased the results. Loss to follow-up may have affected results if reasons for dropout were related to the intervention.
Guideline
This section considers research included in both the 200825 and 201926 versions of the NICE guideline. The overall objectives, health questions, and populations were described in sufficient detail. The guideline described the target population and included important stakeholders in guideline development. Sufficient methods were used to search for evidence, describe evidence selection, appraise the quality of the evidence, considered benefits and harms in formulating recommendations, ensure the guideline was reviewed, and implement a process for updating the guideline. For the 2019 version26 of the guideline, the methods for formulating the recommendations were not described in sufficient detail, and the link between recommendations and supporting evidence was unclear. Key recommendations were clearly visible and auditing criteria were posted. However, the recommendations are to not conduct wound irrigation in general; there are no detailed recommendations about specific antibiotics or preparations to avoid, clear advice on alternative options, or barriers and facilitators to implementing the guidance. Although competing interests of the guideline development group members were recorded, it is unclear how any funding affected formation of the guideline as funding was not reported in the publication.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3, Table 5, Table 6, and Table 7.
Summary of Findings
Appendix 4 presents the main study findings by outcome in Table 8, Table 9, Table 10, Table 11, Table 12, Table 13, Table 14, Table 15, and Table 16.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Infection
Two SRs6,14 and 1 RCT22 reported results comparing antibiotic solution to antiseptic solution. In 1 SR with NMA,6 results showed that antibiotic irrigation was not statistically superior to antiseptic irrigation. The other SR14 had relevant data from 2 retrospective cohort studies; 1 demonstrated a statistically significant reduction in risk of infection in the chlorhexidine gluconate (CHG) group compared to the TAS group, while the other study did not report analyses comparing TAS and CHG. One RCT22 included in the current review found that SSI did not differ statistically between TAS and CHG groups, even when results were broken down by infection type (minor, major, explantation).
Four SRs6,14,15,17 and 4 RCTs18,20,21,23 reported results comparing antibiotic solution to saline with mixed findings. Two SRs showed that infections were reduced in a cefuroxime and gentamicin group compared to a saline group,15 a cephalothin group compared to a saline group,15 and an antibiotic group compared to a normal saline group,17 based on MA and NMA results. However, 1 SR with MA16 showed that based on 3 RCTs and 753 patients, beta-lactam antibiotic irrigation solutions were not effective in reducing SSIs compared to no antibiotic solution irrigation. In addition, 1 SR and 3 RCTs showed no statistically significant differences in infection for bacitracin compared to saline,14 cefazolin compared to saline,14 gentamicin-saline compared to saline,18 ceftriaxone compared to saline,23 and polymyxin B compared to saline.20 One RCT21 reported that CRP levels after 12 hours were better in a gentamicin-clindamycin lavage group compared to normal saline lavage group; no further details were provided.
Two RCTs18,19 compared antibiotic irrigation to no irrigation. One RCT18 demonstrated a statistically significant lower value of SSIs for a gentamicin-saline group compared to a no irrigation group; however, post hoc analyses showed no statistically significant difference. In a randomized crossover trial,19 there was no statistically significant difference in infections requiring surgical intervention between bacitracin and no irrigation.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Capsular Contracture
One SR14 reported results from a retrospective cohort study that found no difference in CC between the TAS and CHG groups.
Three SRs14,15,17 had mixed results on the effect of antibiotic solution irrigation on CC when compared to saline solution. Two SRs found no differences in CC between a TAS group compared to a saline group in a retrospective cohort study,14 between a cefuroxime and gentamicin group compared to a saline group,15 or a cephalothin group compared to a saline group. In 1 SR17 that included 2 SRs and 2 RCTs, there were mixed findings; 1 retrospective cohort study found a statistically significant reduction in CC in a TAS groups compared to a normal saline group, 1 included MA reported reduced CC with antibiotic irrigation compared to normal saline irrigation, no differences in CC between TAS and normal saline from another retrospective cohort study, and no differences in CC between antibiotic irrigation and normal saline from another included SR.
No studies examined the effectiveness of antibiotic irrigation compared to no irrigation on CC.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Hospital-Related Outcomes
No studies examined the effectiveness of antibiotic irrigation compared to antiseptic irrigation on hospital-related outcomes (e.g., hospital stay, hospitalization). Three RCTs18,20,21 reported results for the effect of antibiotic irrigation compared to saline irrigation on hospital stay. One RCT21 showed that hospital stay in days was lower for the gentamicin-clindamycin lavage group compared to the normal saline lavage group and this was statistically significant. The other 2 RCTs showed no statistically significant differences in hospital stay for a gentamicin-saline group compared to a saline group,18 and a polymyxin B group compared to saline group.20
Two RCTs comparing gentamicin-saline to no irrigation18,19 found no statistically significant differences between the 2 regarding hospital stay or hospitalization for infection after surgical procedures.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Pain-Related Outcomes
One RCT18 showed no difference in pain visual analogue scores between a gentamicin-saline group and a saline group. Another RCT21 showed statistically significant differences in mean pain score between gentamicin-clindamycin lavage and normal saline lavage groups at both 3 hours and 24 hours after surgery, and the amount of acetaminophen needed after 24 hours was significantly lower in the gentamicin-clindamycin lavage group. However, no statistically significant differences were seen for the amount of acetaminophen needed after 3 hours of surgery or pethidine needed after 24 hours of surgery.
One RCT18 showed that pain visual analogue scores were similar between a gentamicin-saline group and a no irrigation group.
No studies examined the effectiveness of antibiotic irrigation compared to antiseptic irrigation on pain-related outcomes.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Patient Satisfaction
One RCT18 found that a significantly higher percentage of patients in gentamicin-saline and saline groups were completely or partly satisfied with the outcome of their procedures compared to no irrigation; this was statistically significant.
No studies examined the effectiveness of antibiotic irrigation compared to antiseptic irrigation on patient satisfaction.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Wound-Related Outcomes
Results from 3 SRTs18,21,22 showed no differences in necrosis, hematoma, seroma, and wound infection across study groups.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Adverse Events and Complications
One SR14 reported that in 1 retrospective cohort study, patients who received irrigation with CHG showed a greater reduction in complications compared to those who had TAS irrigation; this was statistically significant. Another retrospective cohort study in the same SR14 showed a lower percentage of implant loss in the CHG group compared to the TAS group; however, the level of statistical significance in the difference was not reported. One RCT22 showed that no patients in TAS or CHG groups had any allergic reactions.
Three RCTs18,20,24 that compared antibiotic to saline irrigation found no statistically significant differences in adverse events or complications between the groups. One RCT18 showed no differences in surgical site occurrences, or urine retention or ileus between gentamicin-saline and saline groups. Another RCT24 showed no difference in treatment required for UTI between neosporin compared to saline groups, even when limiting results by UTI timing or those needing vaginal prolapse repair. This study24 also reported finding no association between antibiotic irrigation and new urinary frequency or urgency after surgery, and there were no adverse events related to antibiotic irrigation. Another RCT20 found no difference in post-operative pancreatic fistula or clinically relevant post-operative pancreatic fistula between polymyxin B and saline groups. Other complications that showed no statistically significant differences between groups were organ failure, sepsis, delayed gastric emptying, bile leaks, UTIs, venous thromboembolism, cholangitis, or myocardial infarction.
In the RCT18 that compared gentamicin-saline to no irrigation, surgical site occurrences were significantly lower for gentamicin-saline compared to no irrigation and there were no differences in urine retention or ileus between groups.
A randomized crossover trial19 showed that adverse events were rare in both bacitracin and no irrigation groups.
Clinical Effectiveness of Antibiotic Irrigation Solutions on Mortality
One RCT22 comparing TAS to CHG indicated that overall, there were 2 patient deaths out of a study population of 88 patients. One RCT23 comparing ceftriaxone to saline showed that 30-day mortality was 10.6% overall and was not associated with SSI; a breakdown by study groups was not provided. Another RCT20 showed that both 30-day and 90-day mortality were not significantly different for polymyxin groups compared to saline groups.
No studies examined the effectiveness of antibiotic irrigation compared to no irrigation on mortality.
Guidelines Regarding the Use of Antibiotic Solutions for Surgical Irrigation to Prevent Infection
The NICE guideline25,26 does not recommend wound irrigation to reduce the risk of SSI based on evidence from well-conducted MAs, SRs of RCTs, or RCTs with a low risk of bias. The NICE guideline25,26 does not recommend intracavity lavage to reduce the risk of SSI based on mixed evidence from well-conducted MAs, SRs of RCTs, or RCTs with a low risk of bias; and 3 trials with high risk of bias. The NICE guideline26 recommends application of antibiotic to the would before closure only when conducting clinical trials, based on 1 low-quality RCT and moderate quality RCT.
Limitations
Limitations to the body of evidence include high heterogeneity, low generalizability, and a lack of guidelines with more recent evidence. Included SRs6,14-17 noted the high heterogeneity across studies, which varied by surgery type, specific antibiotics used for irrigation, comparator groups, and outcomes measured. Patients undergoing surgery varied greatly and procedures included breast implant surgeries, neurologic procedures, cardiac device operations, gynecological surgeries, and appendectomies, among others. Two SRs6,16 were conducted on any surgery. The antibiotics studied also varied across studies and comprised over 20 different agents that were used alone or in combinations of 2 or 3 antibiotics in a solution. Comparator groups included antiseptic, saline solution, or no irrigation. Outcomes across studies also varied and were grouped into 8 categories in the current report.
The evidence is also limited by low generalizability. Of the 7 RCTs18-24 included in this report, 119 enrolled patients within Canada and from the Netherlands, whereas the others did not include patients from Canada. Six RCTs18,20-24 were conducted at single centres; it is unclear whether their results are applicable to populations beyond surgical patients presenting to specific departments in these institutions. Therefore, overall, the generalizability of the findings in the Canadian context is unclear. In addition, it is unclear whether findings in the current report may be replicated for surgeries other than those mentioned in the included evidence.
The current report found 1 evidence-based guideline,25,26 which included recommendations about wound irrigation and intracavity lavage based on a 2008 version25 of the guideline, and recommendations about antibiotic use before wound closure based on a 2019 version26 of the guideline. For the wound irrigation guideline based on evidence up to 2008, it is unclear whether there are newer studies published in 2008 and later that may change the conclusions. Given that Health Canada recommendations for bacitracin changed in December 2020,7 new guidelines may be required to reflect current practice.
Conclusions and Implications for Decision- or Policy-Making
A rapid review was conducted to examine the effectiveness of antibiotic solutions for surgical irrigation, and to summarize recommendations for using antibiotic irrigation to prevent surgical infection. The review is an upgrade of a 2021 CADTH report8 that provided a reference list of relevant studies on the topic identified from the literature. The rapid review identified 5 SRs6,14-17 (1 with MA and 1 with NMA), 7 RCTs,18-24 and 1 guideline reported in 2 publications,25,26 published between 2018 and 2021. The current report includes more studies than the CADTH 2021 reference list report8 because it evaluated full-text articles to determine relevancy of studies that may have had unclear information from only titles and abstracts. Over 20 different solutions of antibiotics were reported in included studies as interventions, and comparators included antiseptic, saline, or no irrigation.
For studies comparing antibiotic solution to antiseptic solution, no significant effects were found in higher-level evidence (SR6 or RCT22) on infection, while 1 retrospective study included in 1 SR14 found a significant effect of antibiotic compared to antiseptic solution on infection. One retrospective study included in an SR14 showed a significant effect of antibiotic irrigation on complications. Across all the included studies, there were no significant effects of antibiotic solution over antiseptic solution on CC or wound-related outcomes, and mixed effects for hospital-related outcomes, pain, and painkiller use.
For studies comparing antibiotic solution to saline, 36,15,17 out of 4 SRs showed significant effects on infection, while 318,20,23 out of 4 RCTs showed no effects on infection. One RCT21 showed that CRP levels were better in the gentamicin-clindamycin lavage group compared to the normal saline lavage group. One RCT18 found that patients in the antibiotic group were more satisfied with the outcome of their surgery. Across all studies, there were no significant effects or mixed effects of antibiotic solution over saline on CC, hospital stay, pain, and wound-related outcomes. Findings on mortality were unclear due to poor reporting.
For studies comparing antibiotic solution to no irrigation, 1 RCT18 found higher patient satisfaction when comparing antibiotic to no irrigation. There were mixed effects for antibiotic irrigation on infection, adverse events, and complications, and no effects found for hospital stay, pain, and wound-related outcomes.
The included guideline25,26 recommended that wound irrigation and intracavity lavage should not be used to reduce SSIs, and that antibiotics should only be applied before closure as part of clinical research trials.
Most studies included in the current review indicated that antibiotic solutions for irrigation were better or no different compared to antiseptic, saline, or no irrigation on various outcomes; however, 1 retrospective study included in 1 poorly reported SR14 found a significant reduction in infections and complications in a CHG group compared to a TAS group while another retrospective study included in the same SR14 found a higher percentage of implant loss in the TAS group compared to the CHG group, although no data on statistical significance was reported.
Regarding bacitracin-specific evidence, 1 retrospective cohort study included in 1 poorly reported SR14 showed a higher percentage of infection in a bacitracin irrigation group when comparing it to cefazolin and saline irrigation groups; however, this was not statistically significant. One randomized crossover trial19 showed no statistically significant differences between bacitracin irrigation and no irrigation on infections requiring surgical intervention or hospitalization for infections from cardiac rhythm device implants.
The findings of the current review suggest that the literature is mixed regarding any potential benefits or harms of antibiotic solutions for surgical wound irrigation. There was high heterogeneity across studies and most RCTs were either not powered sufficiently to detect any effects or had potential selection bias. No high-quality SRs were found, and several had methodological weaknesses such as search strategies that were not comprehensive, lack of reporting on duplicate screening and extraction, and insufficient reporting of the details of each included study. Future high-quality SRs and RCTs can be conducted to target some of the limitations of the current review, and new primary research where evidence gaps currently exist can be added to the literature (e.g., the effectiveness of antibiotic irrigation compared to no irrigation on CC in breast surgery, antibiotic irrigation compared to antiseptic irrigation on hospital-related outcomes). Because the 1 included guideline25,26 includes recommendations from 2008 for wound irrigation specifically, an updated guideline with more recent literature that reflects current practice for this type of intervention may be helpful for practitioners.
Because of the mixed findings from the literature, contraindication of bacitracin in recent Health Canada guidance,7 and NICE guidelines25,26 that do not recommend wound irrigation, decision-makers may also consider the resources needed to perform wound irrigation or stop using this process altogether. For example, clinicians may consider whether current non-irrigation infection prevention protocols that take place before, during, and after surgery (e.g., preoperative hand decontamination, post-operative wound cleansing with saline) may be sufficient until updated guidelines with more recent research becomes available.
References
1.Global guidelines for the prevention of surgical site infection. 2nd ed. Geneva (CH): World Health Organization; 2018: https://apps.who.int/iris/bitstream/handle/10665/277399/9789241550475-eng.pdf?sequence=1&isAllowed=y. Accessed 2022 Jan 5.
2.Canadian surgical site infection prevention audit month. Recap report. Ottawa (ON): Canadian Patient Safety Institute; 2016: https://www.patientsafetyinstitute.ca/en/toolsResources/Documents/SSI%20Audit%202016_Recap%20Report%20EN.pdf. Accessed 2022 Jan 12.
3.Anderson DJ, Sexton DJ. Overview of control measures for prevention of surgicalsite infection in adults. In: Post PW, ed. UpToDate. Waltham (MA): UpToDate; 2021: https://www.uptodate.com. Accessed 2022 Jan 12.
4.Armstrong DG, Meyr AJ. Basic principles of wound management. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: https://www.uptodate.com. Accessed 2022 Jan 12.
5.Norman G, Atkinson RA, Smith TA, et al. Intracavity lavage and wound irrigation for prevention of surgical site infection. Cochrane Database Syst Rev. 2017;10(10):CD012234. PubMed
6.Thom H, Norman G, Welton NJ, Crosbie EJ, Blazeby J, Dumville JC. Intra-cavity lavage and wound irrigation for prevention of surgical site infection: systematic review and network meta-analysis. Surg Infect (Larchmt). 2021;22(2):144-167. PubMed
7.Bacitracin for injection (50,000 IU per vial) and the risk of nephrotoxicity and anaphylactic reactions. Ottawa (ON): Government of Canada; 2020: https://recalls-rappels.canada.ca/en/alert-recall/bacitracin-injection-50000-iu-vial-and-risk-nephrotoxicity-and-anaphylactic-reactions. Accessed 2022 Jan 12.
8.Antibiotic solutions for surgical irrigation. CADTH rapid response report: reference list. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/htis/2021/RB1594%20Antibiotic%20solutions%20for%20surgical%20irrigation%20Final.pdf. Accessed 2021 Dec 8.
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
11.Jansen JP, Trikalinos T, Cappelleri JC, et al. Supplementary material to: Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Dec 8.
14.Baker NF, Hart AM, Carlson GW, Losken A. A systematic review of breast irrigation in implant-based breast surgery. Ann Plast Surg. 2021;86(3):359-364. PubMed
15.Leas B, Talati N. Effectiveness of intra-operative antimicrobial irrigation to prevent surgical site infection in clean surgeries. An evidence review from Penn Medicine’s Center for Evidence-based Practice. Philadelphia (PA): University of Pennsylvania; 2021.
16.López-Cano M, Kraft M, Curell A, et al. Use of topical antibiotics before primary incision closure to prevent surgical site infection: a meta-analysis. Surg Infect (Larchmt). 2019;20(4):261-270. PubMed
17.Saeg F, Schoenbrunner AR, Janis JE. Evidence-based wound irrigation: separating fact from fiction. Plast Reconstr Surg. 2021;148(4):601e-614e. PubMed
18.Emile SH, Elfallal AH, Abdel-Razik MA, El-Said M, Elshobaky A. A randomized controlled trial on irrigation of open appendectomy wound with gentamicin- saline solution versus saline solution for prevention of surgical site infection. Int J Surg. 2020;81:140-146. PubMed
19.Krahn AD, Longtin Y, Philippon F, et al. Prevention of arrhythmia device infection trial: the PADIT trial. J Am Coll Cardiol. 2018;72(24):3098-3109. PubMed
20.Maatman TK, Weber DJ, Timsina LR, et al. Antibiotic irrigation during pancreatoduodenectomy to prevent infection and pancreatic fistula: a randomized controlled clinical trial. Surgery. 2019;166(4):469-475. PubMed
21.Negahi A, Arminfar A, Vaseghi H, Moradi M, Alemrajabi M. Evaluating the effect of gentamicin-clindamycin lavage on post-operational pain and infection through laparoscopic colectomy surgery. J Coloproctol. 2020 Jan-Mar;40(1):008-011.
22.Nguyen L, Afshari A, Green J, et al. Post-mastectomy surgical pocket irrigation with triple antibiotic solution vs chlorhexidine gluconate: a randomized controlled trial assessing surgical site infections in immediate tissue expander breast reconstruction. Aesthet Surg J. 2021;41(11):NP1521-NP1528. PubMed
23.Okunlola AI, Adeolu AA, Malomo AO, Okunlola CK, Shokunbi MT. Intra-operative wound irrigation with ceftriaxone does not reduce surgical site infection in clean neurosurgical procedures. Br J Neurosurg. 2020:1-4. Online ahead of print. PubMed
24.Slopnick EA, Welles Henderson J, Chapman G, et al. Cystoscopy with antibiotic irrigation during pelvic reconstruction and minimally invasive gynecologic surgery: a double-blind randomized controlled trial. Neurourol Urodyn. 2020;39(8):2386-2393. PubMed
25.Surgical site infection: prevention and treatment of surgical site infection. NICE clinical guidelines, no. 74. London (UK): National Collaborating Centre for Women's and Children's Health; 2008: https://www.ncbi.nlm.nih.gov/books/NBK53731/. Accessed 2022 Jan 10.
26.Surgical site infections: prevention and treatment. NICE guideline NG125. London (UK): National Institute for Health and Care Excellence; 2019: https://www.nice.org.uk/guidance/ng125/resources/surgical-site-infections-prevention-and-treatment-pdf-66141660564421. Accessed 2021 Oct 04.
27.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
28.Berríos-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for Disease Control and Prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017;152(8):784-791. PubMed
29.Surgical Site Infection (SSI). Washington (DC): Centers for Disease Control and Prevention; 2010: https://www.cdc.gov/hai/ssi/ssi.html. Accessed 2022 Jan 11.
30.Ceppa EP, Pitt HA, House MG, et al. Reducing surgical site infections in hepatopancreatobiliary surgery. HPB. 2013;15(5):384-391. PubMed
Appendix 1: Selection of Included Studies
Note that this appendix has not been copy-edited.
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Baker 202114 US Funding source: consultancy to RTI Surgical | Unclear search dates 8 retrospective cohort studies, 1 prospective cohort study; 4 retrospective cohort studies relevant to the present review with sufficient detail | Patients undergoing implant-based breast surgery | Intervention: breast pocket irrigation using TAS, bacitracin, or cefazolin Comparator: saline or CHG irrigation | Outcomes: infection, complications, CC Follow-up: NR |
Leas 202115 US Funding source: University of Pennsylvania Health System | Literature published 2017 to 2021 1 SR, 4 RCTs, 8 NRS, 1 narrative review; 1 narrative review relevant to the present review | Patients undergoing plastic surgery for breast augmentation 5,556 patients | Intervention: irrigation using cephalothin, or cefuroxime and gentamicin Comparator: saline irrigation | Outcomes: infection, CC Follow-up: up to 1 year |
Saeg 202117 US Funding source: royalties from Thieme and Springer Publishing | Literature published January 2000 to March 2020 5 MAs, 6 SRs, 8 RCTs, 3 prospective cohort studies, 9 retrospective cohort studies; 1 MA, 2 SRs, and 2 retrospective cohort studies relevant to the present review | Patients undergoing breast implant surgery 55 to 8,892 patients across studies | Intervention: TAS or antibiotic irrigation Comparator: normal saline irrigation | Outcomes: infection, CC Follow-up: NR |
Thom 20216 England Funding sources: UK NIHR Manchester BRC, NIHR Biomedical Research Centre University Hospitals Bristol NHS Foundation Trust, University of Bristol, NIHR via Cochrane Infrastructure, Cochrane Programme Grant | Literature published up to February 1, 2017 59 RCTs in SR, 42 RCTs in NMA; 20 RCTs relevant to the present review | Patients undergoing surgeries with primary site closure 14 to 360 patients across studies | Intervention: irrigation with ampicillin, cefazolin, tetracycline, cephapirin, cefamandole, moxalactam, cefoxitin, cefotetan, kanamycin, taurolin, cefoxin, kanamycin and cephalothin, cephalothin, gentamicin, gentamicin and clindamycin, or chloramphenicol Comparator: saline or no irrigation | Outcome: SSI Follow-up: 8 days to 8 weeks |
López-Cano 201916 Spain Funding source: no financial support received | Literature published up to January 31, 2017 40 RCTs in SR, 35 RCTs in NMA; 10 RCTs relevant to the present review | Inclusion criteria: patients undergoing colorectal, hernia, soft tissue, breast, cardiovascular, biliary tract, abdominal, trauma surgeries Exclusion criteria: eye surgery, antibiotic dressings, antibiotic-impregnated beds, cements 62 to 401 patients across studies | Intervention: topical antibiotic irrigation solution (cephaloridine, cephradine, cefamandole, cefotaxime, ampicillin, gentamicin) at incision site before primary closure Comparator: patients with surgical incisions where prophylactic topical antibiotic agents were not used | Outcome: SSI Follow-up: NR |
BRC = Biomedical Research Centre; CC = capsular contracture; CHG = chlorhexidine gluconate; MA = meta-analysis; NHS = National Health Service; NIHR = National Institute for Health Research; NMA = network meta-analysis; NRS = nonrandomized study; NR = not reported; RCT = randomized controlled trial; SR = systematic review; SSI = surgical site infection; TAS = triple antibiotic solution
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Nguyen 202122 US Funding source: no financial support received | RCT (1:1; each patient served as own control, mastectomy pockets were randomized), blinded, single centre | Inclusion criteria: females 18 to 81 years old undergoing bilateral mastectomy and eligible for immediate TE breast reconstruction Exclusion criteria: allergy to antibiotic intervention or CHG; undergoing bilateral reconstruction using other techniques, or unilateral mastectomy and reconstruction 88 female patients, mean age 47 years | Intervention: TAS breast pocket irrigation (cefazolin, bacitracin, gentamicin in saline) Comparator: CHG breast pocket irrigation | Outcomes: SSI, necrosis, hematoma, seroma, allergic reaction, allergic reaction, death Follow-up: 28 to 606 days |
Emile 202018 Egypt Funding source: no sources of funding | RCT, double-blind, single centre | Inclusion criteria: 16- to 65-year-olds with acute appendicitis Exclusion criteria: appendicular abscess/ mass, appendicitis associated with generalized peritonitis, acute abdomen, normal appendix, steroid or immunosuppressive medication 113 female, 92 male, mean age 27.9 (SD 8.7) | Interventions:
Comparator: no irrigation (n = 69) | Outcomes: SSI, complications, hospital stay, pain, patient satisfaction, seroma, hematoma, wound dehiscence Follow-up: 1, 2, 4, and 6 weeks after surgery |
Negahi 202021 Iran Funding source: NR | RCT, double-blind, single centre | 40 patients undergoing laparoscopic colectomy | Intervention (n = 20): gentamicin-clindamycin lavage Comparator (n = 20): normal saline lavage | Outcomes: pain, painkiller need, white blood cell count, hospital stay, C-reactive protein level, wound infection Follow-up: up to 30 days |
Okunlola 202023 Nigeria Funding source: NR | RCT, blinded, single centre | Adults undergoing neurosurgical procedures 50 female, 82 male, mean age 48.5 | Intervention (n = 66): intravenous ceftriaxone at induction of anesthesia followed by 12 hourly for 24 hours post-operatively and intraoperative wound irrigation with ceftriaxone in saline Comparator (n = 66): intravenous ceftriaxone at induction of anesthesia followed by 12 hourly for 24 hours post-operatively and intraoperative wound irrigation with plain normal saline | Outcomes: SSI, wound edge necrosis, mortality Follow-up: up to 30 days |
Slopnick 202024 US Funding source: no extra-institutional funding | RCT (1:1), double-blind, single centre | Inclusion criteria: female adults undergoing gynecological surgery requiring intraoperative cystoscopy Exclusion criteria: history of UTIs, neurogenic bladder, neomycin or polymyxin allergy, nephrolithiasis, congenital urogenital anomaly, pregnancy, or surgery with intradetrusor onabotulinumtoxin A injection, mesh excision, or fistula repair; positive urine culture Mean age 51.6 (range 29 to 86) | Intervention (n = 111): Neosporin irrigation (200,000 U polymyxin B sulfate and 40 mg neomycin sulfate) Comparator (n = 116): normal saline irrigation | Outcomes: treatment of UTI, adverse events Follow-up: 6 weeks |
Maatman 201920 US Funding source: Department of Surgery, Indiana University School of Medicine | RCT, double-blind, single centre | Inclusion criteria: adults undergoing nonemergent open pancreato-duodenectomy Exclusion criteria: imprisoned, pregnant, undergoing concomitant colectomy/hepatectomy; allergic to study medications; preoperative serum creatinine >2.0 mg/dL Intervention group: mean age 63.7 (SEM 1.3) Comparator group: mean age 64.4 (SEM 1.5) | Intervention (n = 95): intraperitoneal irrigation with polymyxin B in saline Comparator (n = 95): saline irrigation | Outcomes: SSI, hospital stay, POPF, complications, mortality Follow-up: up to 90 days |
Krahn 201819 Canada and Netherlands Funding source: CANNeCTIN network and clinical trial grant from CIHR | Cluster randomized crossover trial, blinded, multi-centre (24 centres Canada, 4 centres Netherlands) | 19,603 patients undergoing cardiac implantable electronic device procedures Mean age 72.0 (SD 13.1) 33.9% female | Incremental therapy: IV cefazolin and preoperative vancomycin (vancomycin only for penicillin-allergic patients); intraoperative wound pocket wash of bacitracin in saline; post-operative oral cephalexin 4 times/day, or cephadroxil 2 times/day for 2 days (clindamycin 3 times/day for penicillin-allergic patients; sites where bacitracin was not available used cefazolin or saline instead Conventional therapy: single dose of preoperative IV cefazolin 60 minutes before skin incision (vancomycin within 120 minutes before skin incision in penicillin-allergic patients) | Outcome: hospitalization for device infection, infection requiring surgical intervention, adverse events Follow-up: within 1 year |
CANNeCTIN = The Canadian Network and Centre for Trials Internationally; CHG = chlorhexidine gluconate; CIHR = Canadian Institutes of Health Research; IV = intravenous; NR = not reported; POPF = post-operative pancreatic fistula; RCT = randomized controlled trial; SD = standard deviation; SEM = standard error of the mean; SSI = surgical site infection; TAS = triple antibiotic solution; TE = tissue expander; UTI = urinary tract infection
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: health care professionals; commissioners and providers; people having surgery (their families and carers) Target population: adults, young people, children undergoing surgery involving a cut through the skin | Methods for before, during, and after surgery to minimize infection risk; only guidelines for intraoperative wound irrigation, intracavity lavage, and antibiotic application before wound closure are relevant to the present review | SSIs | 2008 guideline Searches in 6 databases for English publications; scoping searches to identify other guidelines with reference lists checked; additional evidence submitted by stakeholders 2019 guideline New evidence found; searches in 10 databases for English publications; additional searches from reference lists and other SRs’ reference lists | 2008 guideline 8 levels of hierarchical evidence across study designs 2019 guideline SRs: ROBIS, RCTs: Cochrane ROB or ROBINS-I tool, GRADE for quality of evidence | 2008 guideline Informal consensus methods seeking evidence where needed, followed by formal consensus methods 2019 guideline Committee discussion of evidence | Experts were involved in the guideline development; regular surveillance for 2008 guideline after 3, 6, and 8 years prompted an update; external stakeholders asked to review guideline draft |
GRADE = Grading of Recommendations Assessment, Development and Evaluation; RCT = randomized controlled trial; ROB = risk of bias; ROBINS-I = Risk Of Bias In Non-randomised Studies - of Interventions; ROBIS = Risk of Bias in Systematic Reviews; SR = systematic review; SSI = surgical site infection
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 29 and the ISPOR Questionnaire10,11
Strengths | Limitations |
|---|---|
Baker 202114 | |
|
|
Leas 202115 | |
|
|
Saeg 202117 | |
|
|
Thom 20216 | |
|
|
López-Cano 201916 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; MA = meta-analysis; NMA = network meta-analysis; NRS = nonrandomized study; RCT = randomized controlled trial
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist12
Strengths | Limitations |
|---|---|
Nguyen 202122 | |
|
|
Emile 202018 | |
|
|
Negahi 202021 | |
|
|
Okunlola 202023 | |
|
|
Slopnick 202024 | |
|
|
Maatman 201920 | |
|
|
Krahn 201819 | |
|
|
Table 7: Strengths and Limitations of Guideline Using AGREE II13
Item | |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Unclear |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Unclear |
16. The different options for management of the condition or health issue are clearly presented. | Unclear |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings for Infection-related Outcomes
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to antiseptic solution irrigation | |
Baker 202114 SR | Retrospective cohort studies Merceron et al. (2019)
Haynes (2018)
|
Nguyen 202122 RCT |
|
Thom 20216 SR | Based on NMA results of 42 RCTs and 11, 726 patients, antibiotic is not statistically superior to antiseptic: SSI OR 0.77 (95% CrI, 0.4 to 1.54) |
Antibiotic solution irrigation compared to saline irrigation | |
Baker 202114 SR | Boustany et al. (2018)
|
Leas 202115 SR | Campbell (2018)
|
Saeg 202117 SR | Lynch et al. (2018)
|
Thom 20216 SR | Based on NMA results, antibiotic agents have statistically lower odds of SSI compared to saline.
“Antibiotic irrigation most likely to have lowest SSI rates relative to non-antibacterial irrigation (p. 150).”6 |
Emile 202018 RCT | No statistically significant differences in SSI between gentamicin-saline compared to saline irrigation (P = 0.99)
Based on post hoc analyses, the gentamicin-saline group had similar SSI rate compared to saline irrigation group (not statistically significant, P = 0.67). Overall, there was superficial incisional SSI in 15 patients and deep incisional SSI in 2 patients who were given antibiotics based on sensitivity and culture tests. (Values not broken down by study group) Five patients (29.4%) needed infected surgical wound drainage. (Values not broken down by study group) |
Negahi 202021 RCT | Specific measure for random variability (e.g., standard deviation, standard error of the mean) not defined in study
|
Okunlola 202023 RCT | No statistically significant difference in SSI between ceftriaxone and normal saline groups (P = 1.00)
|
Maatman 201920 RCT | No statistically difference between groups for SSI (P > 0.61)
“The overall incidence of superficial SSI and organ-space SSI was 4.7% (n = 9) and 7.9% (n = 15), respectively. The diagnosis of superficial SSI was made by (n = 4) purulent discharge (criteria 1), (n = 4) symptoms of infection with surgical opening of the wound (criteria 3), and (n = 1) culture positivity (criteria 2). The diagnosis of organ-space SSI was made by culture positivity (criteria 2) in all cases. The rate of superficial SSI was 3% vs 6%, and the rate of organ space infection was 7% vs 8% (P > .31 each) (p. 471).”20 |
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | SSI significantly lower for gentamicin-saline and saline groups compared to no irrigation (statistically significant, P = 0.005). SSI significantly lower for gentamicin-saline compared to no irrigation (statistically significant, P = 0.02).
Posthoc analysis: Gentamicin-saline group lower SSI rate compared to no irrigation group which was not statistically significant (Authors report P = 0.02; unclear whether there is statistical significance or not). |
Krahn 201819 RCT | Infection requiring surgical intervention was not statistically significant between groups
|
Antibiotic solution irrigation compared to no antibiotic solution irrigation | |
López-Cano 201916 SR | Surgical site infections Evans et al. (1974)
Pitt et al. (1980)
Freischlag et al. (1984)
Moesgaard et al. (1989)
Seco et al. (1990)
Lazorthes et al. (1992)
|
López-Cano 201916 SR (continued) | Al-Shehri et al. (1994)
Moesgaard et al. (1988)
Praveen et al. (2009)
Ruiz-Tovar et al. (2012)
Evans et al. (1974), Pitt et al. (1980) and Moesgaard et al. (1989) (2 RCTs, 753 patients)
|
CHG = chlorhexidine gluconate; CI = confidence interval; CrI = credible interval; CRP = C-reactive protein; MA = meta-analysis; OR = odds ratio; RCT = randomized controlled trial; RR = relative risk; SR = systematic review; SSI = surgical site infection; TAS = triple antibiotic solution; WBC = white blood cells
Table 9: Summary of Findings for Capsular Contracture
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to antiseptic solution irrigation | |
Baker 202114 SR | Merceron et al. (2019)
|
Antibiotic solution irrigation compared to saline irrigation | |
Baker 202114 SR | Drinane et al. (2014)
|
Leas 202115 SR | Campbell et al. (2018)
|
Saeg 202117 SR | Retrospective cohort studies Blount et al. 2013
Drinane et al. (2016)
SRs/MAs Samargandi et al. (2018)
Lynch et al. (2018)
|
CC = capsular contracture; CHG = chlorhexidine gluconate; CI = confidence interval; MA = meta-analysis; RR = relative risk; SR = systematic review; TAS = triple antibiotic solution
Table 10: Summary of Findings for Hospital-Related Outcomes
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to saline irrigation | |
Emile 202018 RCT | Mean hospital stay in days similar across groups (not statistically significant, P = 0.18)
|
Negahi 202021 RCT | Hospital stay in days significantly lower in antibiotic group (statistically significant, P = 0.014)
|
Maatman 201920 RCT | Post-operative duration of hospital stay in median number of days (not statistically significant, P = 0.69)
|
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | Mean hospital stay in days similar across groups (not statistically significant, P = 0.18)
|
Krahn 201819 RCT | No statistically significant differences in hospitalization across groups
|
CI = confidence interval; OR = odds ratio; RCT = randomized controlled trial; SD = standard deviation
Table 11: Summary of Findings for Pain-Related Outcomes
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to saline irrigation | |
Emile 202018 RCT | Pain visual analogue score was similar across groups (not statistically significant, P = 0.83)
|
Negahi 202021 RCT | Specific measure for random variability (e.g., standard deviation, standard error of the mean) not defined Mean pain score after 3 hours of operation (statistically significant, P = 0.0011)
Mean pain score after 24 hours of operation (statistically significant, P < 0.0001)
Acetaminophen needed after 3 hours (not statistically significant, P = 0.06)
Acetaminophen amount needed after 24 hours (statistically significant, P = 0.004)
Pethidine amount needed after 24 hours (not statistically significant, P = 0.12)
|
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | Pain visual analogue score was similar across groups (not statistically significant, P = 0.83)
|
RCT = randomized controlled trial; SD = standard deviation
Table 12: Summary of Findings for Patient Satisfaction
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to saline irrigation | |
Emile 202018 RCT | Patient satisfaction, rated as completely or partly satisfied, was higher in the gentamicin-saline and saline groups compared tothe no irrigation group (statistically significant, P <0.001)
|
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | Patient satisfaction, rated as completely or partly satisfied, was higher in the gentamicin-saline and saline groups compared to the no irrigation group (statistically significant, P <0.001)
|
RCT = randomized controlled trial
Table 13: Summary of Findings for Wound-Related Outcomes
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to antiseptic irrigation | |
Nguyen 202122 RCT | Necrosis did not differ between TAS and CHG groups (not statistically significant, P = 0.45)
Hemotoma did not differ between TAS and CHG groups (not statistically significant, P = 0.56)
Seroma did not differ between TAS and CHG groups (not statistically significant, P = 0.65)
|
Antibiotic solution irrigation compared to saline irrigation | |
Emile 202018 RCT | Seroma was similar across study groups (not statistically significant, P = 0.11)
Overall, 4 patients with wound hematoma and 33 patients with wound seroma had one stich removed and collected fluid under antibiotic coverage was evacuation. Results were not broken down by study groups. Hematoma was similar across study groups (not statistically significant, P = 0.84)
Wound dehiscence was similar across study groups (not statistically significant, P = 0.22)
Two patients had superficial wound dehiscence secondary to SSI and were given daily dressing until complete healing by secondary intention. |
Negahi 202021 RCT | Specific measure for random variability (e.g., standard deviation, standard error of the mean) not defined
|
Okunlola 202023 RCT | “The six patients with superficial epidermolysis of the wound edge had satisfactory wound healing but three out of the four patients with full thickness wound edge necrosis developed SSI (p. 2).”23 |
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | Seroma was similar across study groups (not statistically significant, P = 0.11)
Overall, 4 patients with wound hematoma and 33 patients with wound seroma had one stich removed and collected fluid under antibiotic coverage was evacuation. Hematoma was similar across study groups (not statistically significant, P = 0.84)
Wound dehiscence was similar across study groups (not statistically significant, P = 0.22)
Two patients had superficial wound dehiscence secondary to SSI and were given daily dressing until complete healing by secondary intention. |
CHG = chlorhexidine gluconate; RCT = randomized controlled trial; SSI = surgical site infection; TAS = triple antibiotic solution
Table 14: Summary of Findings for Adverse Events and Complications
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to antiseptic irrigation | |
Baker 202114 SR | Retrospective cohort studies Merceron et al. (2019)
Haynes (2018)
|
Nguyen 202122 RCT | No patients in either TAS or CHG groups had any allergic reactions. |
Antibiotic solution irrigation compared to saline irrigation | |
Emile 202018 RCT | “Surgical site occurrence (includes SSI, necrosis, cellulitis, chronic and/or non-healing wound, wound dehiscence, serous or purulent drainage, seroma (pocket of sterile clear serous fluid at the site of the incision), hematoma (collection of blood or clots in the surgical wound), or fistula at surgical site (p.142).”18
Results for urine retention or ileus (not statistically significant, P = 0.45)
Intra-abdominal abscess: no events Bowel obstruction: no events Intestinal fistula: no events Adverse effects due to gentamicin use: no events |
Slopnick 202024 RCT | No difference between groups for treatment of UTI (not statistically significant, P = 0.718)
No difference between groups remained after limiting UTI timing to 2 weeks after surgery (not statistically significant, P = 509)
No difference between groups remained after limiting to those needed vaginal prolapse repair (not statistically significant, P = 0.768)
No association between antibiotic irrigation and new urinary frequency or urgency after surgery (not statistically significant, P = 0.07)
“There were no adverse events related to the use of antibiotic irrigation (p. 2389).”24 |
Maatman 201920 RCT | Overall POPF 28.4% (n = 54). No statistically significant difference between study groups (P = 0.63)
Overall, clinically relevant POPF 11.1% (n = 21). No statistically significant difference between groups (not statistically significant, P = 1.0)
“All patients in this study underwent a duct to mucosa anastomotic technique for the pancreaticojejunostomy. No difference was observed in estimated blood loss, pancreatic duct size, gland texture, operative time, blood transfusion rates, or fistula risk score between the treatment and control groups (p. 471).”20 Organ failure (not statistically significant, P = 1.0)
Sepsis (not statistically significant, P = 0.50)
Delayed gastric emptying (not statistically significant, P = 0.75)
|
Maatman 201920 RCT (continued) | Bile leak (not statistically significant, P = 1.0)
UTI (not statistically significant, P = 0.62)
Venous thromboembolism (not statistically significant, P = 0.25)
Cholangitis (not statistically significant, P = 1.0)
Myocardial infarction (not statistically significant, P = 1.0)
|
Antibiotic solution irrigation compared to no irrigation | |
Emile 202018 RCT | “Surgical site occurrence (includes SSI, necrosis, cellulitis, chronic and/or non-healing wound, wound dehiscence, serous or purulent drainage, seroma (pocket of sterile clear serous fluid at the site of the incision), hematoma (collection of blood or clots in the surgical wound), or fistula at surgical site (p.142).”18
Results for urine retention or ileus (not statistically significant, P = 0.45)
Intra-abdominal abscess: no events Bowel obstruction: no events Intestinal fistula: no events Adverse effects due to gentamicin use: no events |
Krahn 201819 RCT | Overall, adverse events were rare (0.26%) and similar in both study groups. |
CHG = chlorhexidine gluconate; CI = confidence interval; OR = odds ratio; POPF = post-operative pancreatic fistula; RCT = randomized controlled trial; SR = systematic review; SSI = surgical site infection; TAS = triple antibiotic solution; UTI = urinary tract infection
Table 15: Summary of Findings for Mortality
Study citation and study design | Detailed findings |
|---|---|
Antibiotic solution irrigation compared to antiseptic irrigation | |
Nguyen 202122 RCT | 2 patients died, with a mean follow-up time to death of 446.5 days |
Antibiotic solution irrigation compared to saline irrigation | |
Okunlola 202023 RCT | Overall, 30-day mortality was 10.6% and was not associated with SSI. |
Maatman 201920 RCT | 30-day mortality (not statistically significant, P = 1.0)
90-day mortality (not statistically significant, P = 1.0)
|
RCT = randomized controlled trial; SSI = surgical site infection
Table 16: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
2008 guideline Wound irrigation and intracavity lavage: | 2008 guideline “There is evidence of no difference in SSI incidence after intraoperative subcutaneous wound irrigation using antibiotics or saline. [EL = 1+]. There is evidence from one study of decreased SSI incidence following intraoperative subcutaneous wound irrigation using povidone-iodine compared with saline. [EL = 1+]. There is evidence from one study of no difference in SSI incidence following use of subcutaneous wound irrigation compared with the use of a drain but with no irrigation. [EL = 1+]. There is evidence from one study that wound irrigation of the muscles and subcutaneous fat tissue (using saline under pressure with a syringe) compared with no irrigation decreases the incidence of SSI. [EL = 1+] (p. 71-72)”25 “There is evidence of no difference in SSI incidence after antibiotic compared with saline lavage. [EL = 1+]. There is evidence from one study that the incidence of SSI is decreased when tetracycline lavage is compared with saline lavage. [EL = 1+]. There is evidence of no difference in SSIs incidence between antiseptic and saline intraoperative intracavity lavage. [EL = 1+]. There is evidence from one small study of fewer wound infections when povidone-iodine is used for post-operative lavage of the perineal space compared with saline. [EL = 1+]. There is evidence from one small study that there is no difference in wound infection rates between use of AOPW compared with saline for lavage. [EL = 1−]. There is evidence from one trial that the incidence of SSI is lower following treatment with intravenous latamoxef compared with lavage with tetracycline. [EL = 1+]. There is evidence of no difference in SSI incidence following the use of drains alone compared with saline lavage. [EL = 1+] There is evidence from one study of fewer SSIs occurring following pulsed saline lavage compared with saline lavage with a jug or syringe during hemiarthroplasty for displaced intracapsular fractured neck of femur. [EL = 1− ] There is evidence from one small study that there is a significant increase in wound infection rates using saline CPPL compared with no CPPL. [EL = 1−]. Evidence from one small trial suggests that there is no difference in SSI rates between use of IV cefamandole or lavage and irrigation with cefamandole or lavage and irrigation and IV cefamandole. [EL = 1+]. Evidence from one small trial suggests that there is no difference in wound infection rate following lavage and wound irrigation with either saline or cefazolin. [EL = 1+] (p. 71-72)”25 |
2019 guideline Antibiotics before wound closure: • “Only apply an antiseptic or antibiotic to the wound before closure as part of a clinical research trial (p. 12).”26 | 2019 guideline Topical cefotaxime Outcomes at 1 month after surgery
These results were also consistent in the following subgroups:
Topical cephaloridine Outcomes at 1 month after surgery
This result was also consistent in the following subgroups:
|
AOPW = acidic oxidative potential water; CPPL = closed saline post-operative peritoneal lavage; EL = evidence level; IV = intravenous; RCT = randomized controlled trial; SSI = surgical site infection.
Appendix 5: Overlap Between Included Systematic Reviews
Table 17: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Baker 202114 | Leas 202115 | Saeg 202117 | Thom 20216 | López-Cano 201916 |
|---|---|---|---|---|---|
Merceron TK, et al. Mod Plast Surg. 2019;9(4):74-85. | Yes | No | No | No | No |
Boustany AN, et al. Indian J Plast Surg. 2018;51(1):7-14. | Yes | No | No | No | No |
Campbell CA. Ann Plast Surg. 2018;80(6S Suppl 6):S398-S402 | No | Yes | Yes | No | No |
Haynes DA. Conference abstract presented at SESPRS 61st Annual Meeting; June 2018. | Yes | No | No | No | No |
Lynch JM et al. Aesthetic Plast Surg. 2018;42:1179–1186 | No | No | Yes | No | No |
Samargandi OA et al. Plast Surg (Oakv.) 2018;26:110-119. | No | No | Yes | No | No |
Drinane JJ et al. Ann Plast Surg. 2016;77:32-36. | No | No | Yes | No | No |
Ruiz-Tovar J et al. Surg Infect (Larchmt). 2016;17(1):65-70. | No | No | No | Yes | No |
Blount AL et al. Aesthet Surg J. 2013;33:516-521. | No | No | Yes | No | No |
Drinane JJ et al. Plast Reconstr Surg Glob Open. 2013;1:e55. | Yes | No | No | No | No |
Ruiz-Tovar J et al. J Am Coll Surg. 2012;214:202-207. | No | No | No | Yes | Yes |
Ruiz-Tovar J et al. Conference abstract presented at 24th European Congress on Surgical Infections. May 2011 | No | No | No | Yes | No |
Praveen S and Rohaizak M. Asian J Surg. 2009;32:59-63 | No | No | No | No | Yes |
Mirsharifi SR et al. Tehran Univ Med J. 2008;65(11):71-5. | No | No | No | Yes | No |
Carl SH and Hampton RS. Am J Obstet Gynecol. 2000;182(1):S96-S. | No | No | No | Yes | No |
Al-Shehri MY et al. Ann Saudi Med. 1994;14:233–236. | No | No | No | Yes | Yes |
Magann EF et al. Obstet Gynecol. 1993;81(6):922-5. | No | No | No | Yes | No |
Lazorthes F et al. Surg Gynecol Obstet. 1992;175:569–570. | No | No | No | No | Yes |
Schein M et al. Arch Surg. 1990;125(9):1132-5. | No | No | No | Yes | No |
Seco JL et al. Am J Surg. 1990;159:226–230. | No | No | No | No | Yes |
Moesgaard F et al. Dis Col Rectum. 1989;32:36–38. | No | No | No | No | Yes |
Moesgaard F et al. Acta Chir Scand. 1988;154:589–592. | No | No | No | No | Yes |
Case WG et al. Surg Res Commun. 1987;2:103–105. | No | No | No | Yes | No |
Greig J et al. Chemioterapia. 1987;6(2 Suppl):595–6. | No | No | No | Yes | No |
Dashow EE et al. Obstet Gynecol. 1986;68:473–8. | No | No | No | Yes | No |
Elliott JP and Flaherty JF. Obstet Gynecol. 1986;67(1):29–32. | No | No | No | Yes | No |
Silverman SH et al. Dis Colon Rectum. 1986;29(3):165–9. | No | No | No | Yes | No |
Freischlag J et al. Surgery. 1984;96:686–693. | No | No | No | No | Yes |
Levin DK et al. Am J Obstet Gynecol. 1983;147(3):273–7. | No | No | No | Yes | No |
Lord JW et al. Am J Surg. 1983;145(2):209–12. | No | No | No | Yes | No |
Halsall AK et al. Pharmatherapeutica. 1981;2(10):673–7. | No | No | No | Yes | No |
Oleson A et al. Ugeskrift for Laeger. 1980;142(22):1415–8. | No | No | No | Yes | No |
Pitt HA et al. Ann Surg. 1980;192:356–363. | No | No | No | No | Yes |
Evans C et al. Br J Surg. 1974;61:133–135. | No | No | No | No | Yes |
Rambo WM. Am J Surg. 1972;123(2):192–5. | No | No | No | Yes | No |
Moylan JA et al. Surg Forum. 1968;19(d):66–7. | No | No | No | Yes | No |
Note: This table has not been copy-edited.
Appendix 6: References of Potential Interest
Previous CADTH Reports
CADTH. 2021; https://www.cadth.ca/antibiotic-solutions-surgical-irrigation.
Review Articles
31.Awad AN, Heiman AJ, Patel A. Implants and breast pocket irrigation: outcomes of antibiotic, antiseptic, and saline irrigation. Aesthet. 2021;09:09.
32.Mann M, Wright CH, Jella T, et al. Cranial surgical site infection interventions and prevention bundles: a systematic review of the literature. World Neurosurg. 2021;148:206-219.e4. PubMed
33.Pop-Vicas AE, Abad C, Baubie K, Osman F, Heise C, Safdar N. Colorectal bundles for surgical site infection prevention: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2020;41(7):805-812. PubMed
34.Lynch JM, Sebai ME, Rodriguez-Unda NA, Seal S, Rosson GD, Manahan MA. Breast pocket irrigation with antibiotic solution at implant insertion: a systematic review and meta-analysis. Aesthetic Plast Surg. 2018;42(5):1179-1186. PubMed
35.Nelson RL, Iqbal NM, Kravets A, et al. Topical antimicrobial prophylaxis in colorectal surgery for the prevention of surgical wound infection: a systematic review and meta-analysis. Tech Coloproctol. 2018;22(8):573-587. PubMed
36.Yao R, Tan T, Tee JW, Street J. Prophylaxis of surgical site infection in adult spine surgery: a systematic review. J Clin Neurosci. 2018;52:5-25. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.