CADTH Reimbursement Review
Elexacaftor-Tezacaftor-Ivacaftor and Ivacaftor (Trikafta)
Sponsor: Vertex Pharmaceuticals (Canada) Incorporated
Therapeutic area: Cystic fibrosis, F508del CFTR mutation
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALT
alanine transaminase
AST
aspartate transaminase
BMI
body mass index
CCFCD
Canadian Cystic Fibrosis Clinic Directors
CCFR
Canadian CF Registry
CDEC
CADTH Canadian Drug Expert Committee
CF
cystic fibrosis
CF CanACT
CF Canada’s Accelerating Clinical Trials Network
CF Canada
Cystic Fibrosis Canada
CFQ-R
Cystic Fibrosis Questionnaire–Revised
CFQ-R (RD)
Cystic Fibrosis Questionnaire–Revised (Respiratory Domain)
CFTR
cystic fibrosis transmembrane conductance regulator
CI
confidence interval
ELX
elexacaftor
ELX-TEZ-IVA
elexacaftor/tezacaftor/ivacaftor + ivacaftor
EMA
European Medicines Agency
FEV1
forced expiratory volume in 1 second
F/F
homozygous for F508del mutation in the CFTR gene
F/G
1 F508del mutation and 1 gating mutation in the CFTR gene
F/MF
1 F508del mutation and 1 minimal function mutation in the CFTR gene
F/R117H
1 F508del mutation and 1 R117H mutation in the CFTR gene
F/RF
1 F508del mutation and 1 residual function mutation in the CFTR gene
F/G
gating mutation in the CFTR gene
HR
hazard ratio
IQR
interquartile range
ITC
indirect treatment comparison
IVA
ivacaftor
IWRS
interactive web response system
LS
least squares
LSMD
least squares mean difference
LUM
lumacaftor
LUM-IVA
lumacaftor-ivacaftor
MID
minimal important difference
MF
minimal function mutation in the CFTR gene
MMRM
mixed-effects model for repeated measures
ppFEV1
percent predicted forced expiratory volume in 1 second
RCT
randomized controlled trial
RF
residual function mutation in the CFTR gene
SAE
serious adverse event
SAP
Special Access Program
SD
standard deviation
SE
standard error
TEZ
tezacaftor
TEZ-IVA
tezacaftor-ivacaftor + ivacaftor
TSQM
Treatment Satisfaction Questionnaire for Medication
ULN
upper limit of normal
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | ELX-TEZ-IVA (Trikafta) ELX 100 mg, TEZ 50 mg, IVA 75 mg (combination tablet), and 150 mg IVA (tablet); oral |
Indication | Treatment of cystic fibrosis in patients aged ≥ 12 years who have at least 1 F508del mutation in the cystic fibrosis transmembrane conductance regulator gene |
Reimbursement request | As per indication |
Health Canada approval status | Approved (NOC); submitted to CADTH pre-NOC |
Health Canada review pathway | Priority review |
NOC date | June 18, 2021 |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
ELX = elexacaftor; IVA = ivacaftor; NOC = Notice of Compliance; TEZ = tezacaftor.
Introduction
Trikafta consists of a fixed-dose combination tablet containing elexacaftor (ELX) 100 mg, tezacaftor (TEZ) 50 mg, and ivacaftor (IVA) 75 mg co-packaged with a tablet containing IVA 150 mg (ELX-TEZ-IVA). ELX-TEZ-IVA is indicated for the treatment of cystic fibrosis (CF) in patients aged 12 years and older who have at least 1 F508del mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. A deletion of phenylalanine 508 in the first nucleotide binding domain (NBD1) (F508del) is the most common mutation in the CFTR gene that results in CF.1 The Canadian Cystic Fibrosis Registry (CCFR) reported that there were 4,344 Canadians living with CF in 2019. Of these, 87.8% of patients carried at least 1 F508del mutation (47.1% were homozygous and 40.7% were heterozygous).1 The sponsor has requested that ELX-TEZ-IVA receive a recommendation to reimburse in accordance with the Health Canada–approved indication. ELX-TEZ-IVA was accepted as a priority review by Health Canada.
The objective of this review was to perform a systematic review of the beneficial and harmful effects of ELX-TEZ-IVA for the treatment of patients aged 12 years and older with CF who have at least 1 F508del mutation in the CFTR gene.
CADTH also reviewed additional studies that did not meet the eligibility criteria of the systematic review but may address important gaps in the evidence from the pivotal and supportive randomized controlled trials (RCTs). These included 1 long-term extension phase study (Study 105),2 1 indirect comparison submitted by the sponsor,3 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease,4,5 and 1 study that modelled the potential impact of ELX-TEZ-IVA on CF-related morbidity and mortality.6
Following the issuance of the draft CADTH Canadian Drug Expert Committee (CDEC) recommendation for ELX-TEZ-IVA in July 2021, the following additional information was provided to CADTH.
Cystic Fibrosis Canada (CF Canada) provided their Health care Advisory Council’s guidelines for the prescribing of CFTR modulators. These guidelines provide recommendations regarding the following aspects of CFTR modulators, including ELX-TEZ-IVA: treatment initiation, assessing the response to treatment, safety monitoring, and discontinuation of therapy. The guidelines have been summarized as an addendum to the CADTH report in Appendix 1.
The sponsor provided additional unpublished data for the use of ELX-TEZ-IVA in patients who initiated treatment with a baseline percent predicted forced expiratory volume in 1 second (ppFEV1) of 90% or greater. These data were not included in the submission to CADTH (the sponsor reported that the data only became available after the CADTH recommendation was issued). As a result of their exclusion from the pivotal trials for ELX-TEZ-IVA, this patient population has been identified as an important gap in the evidence and the information from the sponsor has been summarized as an addendum to the CADTH report in Appendix 2.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Three patient groups, CF Canada, the Canadian Cystic Fibrosis Treatment Society and CF Get Loud, responded to CADTH’s call for patient input. Information for the CF Canada submission was based on a cross-Canada survey of patients and caregivers that was circulated through CF clinics, email, and social media (1,455 respondents). The Canadian Cystic Fibrosis Treatment Society gathered information through 1-on-one and group discussions with individuals with CF, parents, caregivers, and treating physicians. CF Get Loud gathered information from a letter campaign that received 11,364 letters from Canadians, a town hall with CF experts and leaders, and from 20 Canadians who are currently receiving treatment with ELX-TEZ-IVA.
The patient groups emphasized that CF has tremendous impact on those living with the condition, their loved ones, and on society. The most significant clinical impact is in the lungs, where patients experience progressive scarring of their airways and a progressive decline in lung function. Patients may suffer from pulmonary exacerbations requiring weeks of hospitalization and IV antibiotics. Malnutrition is another consequence of CF and those living with the condition are often underweight and may require a feeding tube for supplemental nutrition. Patients may also suffer from CF-related comorbidities, such as CF-related diabetes and CF-related liver disease. In addition to the decline of CF patients’ physical health, many suffer from the unseen effects of CF. These include, but are not limited to, depression, anxiety, and hopelessness. The mental anguish caused by the ever-present awareness of 1’s mortality cannot be expressed in words and are often not quantified. Parents and caregivers have an overwhelming desire to do something to help their loved ones.
Managing CF requires a demanding treatment routine with regular visits to specialized CF clinics. As the disease progresses, even more time and effort are needed to manage the progressive and debilitating symptoms. The condition has a significant impact on patients’ day-to-day quality of life, affecting life decisions that include education, career, travel, relationships, and family planning.
Patients with CF and their loved ones are seeking treatments that can change the trajectory of the disease and improve both life expectancy and quality of life. Improved outcomes include retaining or increasing lung function, improved digestive health, better energy levels, and minimizing symptoms of CF. Patients want to avoid hospital admissions and reduce the need for invasive medical procedures and the treatment burden of daily therapies. They also wish to avoid the adverse effects of therapies, such as osteoporosis, antimicrobial resistance, and CF-related diabetes or liver dysfunction.
Clinician Input
Input From Clinical Experts Consulted By CADTH
Similar to the input from the patient groups, the clinical experts consulted by CADTH indicated that there are significant unmet therapeutic needs for patients living with CF. There are no treatments currently available that can meet the most important goals of therapy, including: prolonging survival, preventing the need for lung transplantation, slowing the decline in lung function over time, or reversing the course of the disease. In addition, the clinical experts noted that the current standard treatments for CF are burdensome for patients and their caregivers.
The clinical experts anticipate that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before the patient develops significant lung disease. The clinical experts noted that ELX-TEZ-IVA could be used in every patient who meets the Health Canada–approved indication, regardless of their current or past treatment regimens. In clinical practice, eligible patients would be identified based on their CFTR genotype; however, there is no practical method that could be used to predict who will be most likely to respond to ELX-TEZ-IVA. The patients who are most in need of treatment with ELX-TEZ-IVA include patients with moderate to severe lung disease (e.g., ppFEV1 ≤ 60%), patients whose body mass index (BMI) is less than or equal to 20 kg/m2, patients with frequent pulmonary exacerbations, and those experiencing a rapid decline in forced expiratory volume (FEV1). However, it could be argued that all patients, including those with mild lung disease or who are pre-symptomatic, could benefit from treatment when considering the long-term outcomes and goal of preventing severe outcomes.
The clinical experts noted that the magnitude of improvement with ELX-TEZ-IVA is far greater than any other currently available treatments for CF (including all other CFTR modulators). ELX-TEZ-IVA would replace earlier CFTR modulators that are significantly less effective (e.g., lumacaftor [LUM]-IVA [Orkambi] and TEZ-IVA + IVA [TEZ-IVA] [Symdeko]) and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA.
The following end points are routinely assessed in Canadian clinical practice: FEV1, nutrition and growth (e.g., BMI or BMI z score), hospital admissions and outpatient treatments for pulmonary exacerbations, and pulmonary exacerbation frequency per year. The magnitude of improvement in CF outcomes that would be considered clinically significant depends on the baseline status of the patient. After initiating treatment with ELX-TEZ-IVA, those with less severe disease or more advanced disease may show smaller changes from baseline in commonly measured end points, but still experience clinically relevant improvements (e.g., stabilization). For ppFEV1 an improvement in ppFEV1 of greater than or equal to 5% would typically be considered clinically meaningful for most patients in Canadian clinical practice. The experts noted that an increase in BMI should only be viewed as a goal of therapy if the patient is malnourished at the time of initiating therapy. Increasing the BMI of a patient who is in the normal range or overweight may pose challenges and should not be viewed as a desirable outcome for evaluating the response to a treatment such as ELX-TEZ-IVA.
Treatment with ELX-TEZ-IVA would most likely be interrupted or discontinued because of adverse events (AEs) or progression to lung transplant. The most likely known AE that would result in discontinuation would be development of persistent liver enzyme abnormalities.
The clinical experts noted that ELX-TEZ-IVA should be prescribed and treatment monitored in an adult or pediatric CF clinic.
Clinician Group Input
Three groups of clinicians responded to CADTH’s call for input: the Canadian Cystic Fibrosis Clinic Directors (CCFCD), CF Canada’s Accelerating Clinical Trials Network, and the Toronto Adult CF Clinic. The input from the clinician groups identified the same unmet medical needs for CF patients and potential place in therapy for ELX-TEZ-IVA as the clinical experts consulted by CADTH. Similar to the clinical experts consulted by CADTH, the clinician groups noted that the impact of ELX-TEZ-IVA has been dramatic and life-altering for the patients who have received the treatment through Health Canada’s Special Access Program (SAP), compassionate access mechanisms, or in clinical trials (including patients who have advanced lung disease).
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review processes. The following were identified as key factors that could impact the implementation of a CADTH recommendation for ELX-TEZ-IVA:
Potential need for objective criteria that can be used to evaluate response to treatment
Potential time points that should be used when evaluating the response to treatment
Advice on the use of ELX-TEZ-IVA in key patient populations that were excluded from the phase III studies
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs (see Drug Program Input).
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
There were 4 double-blind, phase III, RCTs included in the CADTH systematic review: 1 placebo-controlled trial conducted in patients who were heterozygous for the F508del mutation and who had 1 minimal function mutation (F/MF) (Study 102, N = 405); 2 active-controlled trials in patients who were homozygous for the F508del mutation (F/F) (Study 103, N = 107 and Study 109, N = 107); and 1 active-controlled trial in patients who were heterozygous for the F508del mutation and a residual function mutation (F/RF) or a gating mutation (F/G) (Study 104, N = 259).
The double-blind treatment periods were 24 weeks in Study 102 and Study 109, 8 weeks in Study 104, and 4 weeks in Study 103. Studies 103, 104, and 109 all included a 28-day active treatment run-in period where all patients with either an F/F or F/RF genotype received treatment with TEZ-IVA (Studies 103, 109, and the F/RF subgroup of patients in Study 104) and patients with an F/G genotype received treatment with IVA (F/G subgroup of patients in Study 104). Patients were subsequently randomized to receive ELX-TEZ-IVA or to remain on the active treatment administered during the run-in period. All the studies included a screening phase (up to 28 days) and a safety follow-up phase (approximately 4 weeks or entry into an open-label extension phase study).
The inclusion and exclusion criteria for the included RCTs were similar except for the CFTR genotypes (i.e., F/MF, F/F, F/G, or F/RF). Patients were required to have stable CF disease in the opinion of the investigator and a ppFEV1 of 40% or greater and 90% or less at the time of screening. The trials excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 4 weeks before the first dose of study drug. Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.
Efficacy Results
Patients With F/MF Genotype (Study 102)
Treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with placebo at 4 weeks (least squares mean difference [LSMD] = 13.8%; 95% confidence interval [CI], 12.1 to 15.4; P < 0.0001) and 24 weeks (LSMD = 14.3%; 95% CI, 12.7 to 15.8; P < 0.0001). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. Results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses, including those based on age (12 to < 18 years or ≥ 18 years) and ppFEV1 at screening (< 70% or ≥ 70%). The sponsor conducted an additional post hoc subgroup analysis for the subset of patients with a ppFEV1 less than 40% at baseline (16 out of 203 [7.9%] in the placebo group and 18 out of 200 [9.0%] in the ELX-TEZ-IVA group), in which the absolute difference in ppFEV1 with ELX-TEZ-IVA versus placebo was 15.2% (95% CI, 7.3 to 23.1) at 4 weeks and 18.4% (95% CI, 11.5 to 25.3) at 24 weeks.
Treatment with ELX-TEZ-IVA was associated with a lower rate of pulmonary exacerbations compared with placebo (rate ratio = 0.37; 95% CI, 0.25 to 0.55). Similarly, treatment with ELX-TEZ-IVA was associated with lower rates of pulmonary exacerbations requiring hospitalization (rate ratio = 0.29; 95% CI, 0.14 to 0.61) and pulmonary exacerbations requiring IV antibiotic therapy (rate ratio = 0.22; 95% CI, 0.11 to 0.43). Hazard ratios (HR) favoured ELX-TEZ-IVA over placebo for time-to-first pulmonary exacerbation (HR = 0.34; 95% CI, 0.22 to 0.52), time-to-first pulmonary exacerbation requiring hospitalization (HR = 0.25; 95% CI, 0.11 to 0.58), and time-to-first pulmonary exacerbation requiring IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.39).
Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in BMI at 24 weeks compared with placebo (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23 ; P < 0.0001). In patients less than 20 years of age (n = 145), those treated with ELX-TEZ-IVA demonstrated improvements in BMI z score compared with placebo (LSMD = 0.30; 95% CI, 0.17 to 0.43). Similarly, the ELX-TEZ-IVA group demonstrated greater improvement in body weight at 24 weeks compared with the placebo group (LSMD = 2.9 kg; 95% CI, 2.3 to 3.4).
Treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful improvement in Cystic Fibrosis Questionnaire–Revised (Respiratory Domain) (CFQ-R [RD]) score from baseline compared with placebo through 24 weeks (LSMD = 20.2; 95% CI, 17.5 to 23.0).
The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group at 4 weeks (LSMD = –41.2 mmol/L; 95% CI, –44.0 to –38.5) and 24 weeks (LSMD = –41.8; 95% CI, –44.4 to –39.3).
The Treatment Satisfaction Questionnaire for Medication (TSQM) was included as an exploratory end point for patients between the ages of 12 and 17 years. The difference in change from baseline favoured ELX-TEZ-IVA compared with placebo in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4). The TSQM was not included as an end point in Study 109.
Patients With F/F Genotype (Study 103 and Study 109)
In Study 103, treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful increase from baseline in ppFEV1 compared with TEZ-IVA at 4 weeks (LSMD = 10.0%; 95% CI, 7.4 to 12.6; P < 0.0001). Improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. The results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses. A post hoc subgroup analysis from Study 103 suggested that the magnitude of the observed treatment effect (LS mean = 7.8%; 95% CI, 4.8 to 10.8) for CFTR modulator-experienced patients is less than that for CFTR modulator-naive patients (LS mean = 13.2%; 95% CI, 8.5 to 17.9). In Study 109, treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with TEZ-IVA through 24 weeks (LSMD = 10.2%; 95% CI, 8.2 to 12.1; P < 0.0001).
Pulmonary exacerbations were only captured as AEs in Study 103 and Study 109. The percentage of patients with at least 1 pulmonary exacerbation was greater in the TEZ-IVA compared with the ELX-TEZ-IVA group in both studies.
Compared with TEZ-IVA, treatment with ELX-TEZ-IVA was associated with improvements in BMI at 4 weeks in Study 103 (LSMD = 0.60 kg/m2; 95% CI, 0.41 to 0.79) and body weight at 4 weeks (LSMD = 1.6 kg; 95% CI, 1.0 to 2.1). Changes from baseline in BMI and body weight were not investigated in Study 109.
Treatment with ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful improvement in CFQ-R (RD) score from baseline compared with TEZ-IVA at 4 weeks in Study 103 (LSMD = 17.4; 95% CI, 11.8 to 23.0) and through 24 weeks in Study 109 (LSMD = 15.9; 95% CI, 11.7 to 20.1).
The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the TEZ-IVA group at 4 weeks (LSMD = –45.1 mmol/L; 95% CI, –50.1 to –40.1) in Study 103 and through 24 weeks in Study 109 (LSMD = –42.8; 95% CI, –46.2 to –39.3; P < 0.0001).
The TSQM was included as an exploratory end point in Study 103 for patients between the ages of 12 and 17 years. The ELX-TEZ-IVA group demonstrated improvements compared with the TEZ-IVA group in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4). The TSQM was not included as an end point in Study 109.
Patients With F/G and F/RF Genotypes (Study 104)
Treatment with ELX-TEZ-IVA was associated with a statistically significant within-group improvement in ppFEV1 through 8 weeks (LS mean change: 3.7%; 95% CI, 2.8 to 4.6; P < 0.0001). Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 compared to the control group (LSMD = 3.5%; 95% CI, 2.2 to 4.7; P < 0.0001). Subgroup analyses based on the comparator group (i.e., patient genotype) demonstrated absolute improvements in ppFEV1 with ELX-TEZ-IVA versus IVA (LSMD = 5.8; 95% CI, 3.5 to 8.0) and versus TEZ-IVA (LSMD = 2.0; 95% CI, 0.5 to 3.4).
Pulmonary exacerbations were only captured as AEs. Compared with the pooled control group (TEZ-IVA and IVA), fewer ELX-TEZ-IVA-treated patients reported at least 1 pulmonary exacerbation (10.3% versus 2.3%).
Mean BMI increased in both the pooled control group (LS mean = 0.16 kg/m2; standard error [SE] = 0.06) and the ELX-TEZ-IVA group (LS mean = 0.28 kg/m2; SE = 0.06) with no statistically significant difference between the groups (LSMD = 0.13 kg/m2; 95% CI, −0.03 to 0.29).
The ELX-TEZ-IVA group demonstrated a statistically significant increase in CFQ-R (RD) score from baseline (LS mean within-group change = 10.3; 95% CI, 8.0 to 12.7; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in an increase in CFQ-R (RD) score compared to the pooled TEZ-IVA and IVA control group (LSMD = 8.7; 95% CI, 5.3 to 12.1; P < 0.0001). Subgroup analyses demonstrated similar effect sizes for ELX-TEZ-IVA compared with IVA in patients with an F/G genotype (LSMD = 8.9; 95% CI, 3.8 to 14.0; P = 0.0008) and for ELX-TEZ-IVA compared with TEZ-IVA in patients with an F/RF genotype (LSMD = 8.5; 95% CI, 4.0 to 13.1; P = 0.0003). No statistical analyses were performed for changes from baseline in the non-respiratory domains of the CFQ-R.
The ELX-TEZ-IVA group demonstrated a statistically significant decrease in sweat chloride from baseline (LS mean = –22.3 mmol/L; 95% CI, –24.5 to –20.2; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in a decrease in sweat chloride from baseline compared to the pooled control group (LSMD = –23.1 mmol/L; 95% CI, –26.1 to –20.1; P < 0.0001).
Harms Results
Patients With F/MF Genotype (Study 102)
The overall percentage of patients who experienced at least 1 AE was 96.0% in the placebo group and 93.1% in the ELX-TEZ-IVA group. The percentage of patients who experienced at least 1 serious AE (SAE) was 20.9% in the placebo group and 17.3% with ELX-TEZ-IVA. Pulmonary exacerbations were the most reported SAE and were more frequent in the placebo group compared with the ELX-TEZ-IVA group (17.9% versus 6.4%). There were few other SAEs that were reported for more than 1 patient in each treatment group. There were 2 withdrawal due to AEs (WDAEs) reported in the ELX-TEZ-IVA group (1.0%) and none in the placebo group. The reasons for discontinuation from the ELX-TEZ-IVA group included portal hypertension (0.5.%) and rash (0.5%).
Patients With F/F Genotype (Study 103 and 109)
The overall percentage of patients who experienced at least 1 AE in Study 103 and Study 109 was 63.5% and 88.5% in the TEZ-IVA groups, respectively, compared with 58.2% and 92.0% in the ELX-TEZ-IVA groups, respectively. The percentage of patients who experienced at least 1 SAE was 15.9% in the TEZ-IVA group compared with 5.7% in the ELX-TEZ-IVA group of Study 109. The difference between the groups was due to a greater percentage of patients in the TEZ-IVA group who experienced a pulmonary exacerbation compared with the ELX-TEZ-IVA group (11.4% versus 1.1%). SAEs were rare in the 4-week Study 103 and only reported for 1 patient in the TEZ-IVA group (pulmonary exacerbation) and 2 patients in the ELX-TEZ-IVA group (pulmonary exacerbation and rash) (1.9% versus 3.6%). There were no WDAEs reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, WDAEs were reported for 2 patients (2.3%) in the TEZ-IVA group (compulsive disorder and psychotic disorder) and 1 patient (1.1%) in the ELX-TEZ-IVA group (anxiety and depression).
Patients With F/G and F/RF Genotypes (Study 104)
The overall percentage of patients who experienced at least 1 AE was 66.7% in the ELX-TEZ-IVA group and 65.9% in the control group. The percentage of patients who experienced at least 1 SAE was 8.7% in the control group compared with 3.8% in the ELX-TEZ-IVA group. The difference between the groups was due to a greater percentage of patients in the control group who experienced a pulmonary exacerbation that was classified as an SAE compared with the ELX-TEZ-IVA group (5.6% versus 1.5%). There were 2 WDAEs from the control group (1.6%; pulmonary exacerbation and anxiety and depression) and 1 in the ELX-TEZ-IVA group (0.8%; elevated alanine transaminase [ALT] and aspartate transaminase [AST] levels).
Table 2: Summary of Key Results From Selected Pivotal and Protocol Studies
Parameters | Study 102 (F/MF) 24 weeks | Study 103 (F/F) 4 weeks | Study 109 (F/F) 24 weeks | Study 104 (F/G and F/RF) 8 weeks | |||||
|---|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | ||
Absolute change in ppFEV1 (%) | |||||||||
BL; mean (SD) | 61.3 (15.5) | 61.6 (15.0) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) | 68.1 (16.4) | 67.1 (15.7) | |
LSM change (SE) | –0.4 (0.5) | 13.9 (0.6) | 0.4 (0.9) | 10.4 (0.9) | 1.0 (0.7) | 11.2 (0.7) | 0.2 (0.5) | 3.7 (0.5) | |
LSMD (95% CI) | 14.3 (12.7 to 15.8) | 10.0 (7.4 to 12.6) | 10.2 (8.2 to 12.1) | 3.5 (2.2 to 4.7) | |||||
P value | < 0.0001a | < 0.0001a | < 0.0001b | < 0.0001b | |||||
Absolute change in CFQ-R (RD) | |||||||||
BL; mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) | 77.3 (15.8) | 76.5 (16.6) | |
LSM change (SE) | –2.7 (1.0) | 17.5 (1.0) | –1.4 (2.0) | 16.0 (2.0) | 1.2 (1.5) | 17.1 (1.5) | 1.6 (1.2) | 10.3 (1.2) | |
LSMD (95% CI) | 20.2 (17.5 to 23.0) | 17.4 (11.8 to 23.0) | 15.9 (11.7 to 20.1) | 8.7 (5.3 to 12.1) | |||||
P value | < 0.0001b | < 0.0001 | < 0.0001a | < 0.0001 | |||||
Absolute change in BMI (kg/m2) | |||||||||
BL; mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 21.92 (3.89) | 21.17 (3.43) | 24.05 (4.71) | 24.07 (4.72) | |
LSM change (SE) | 0.09 (0.07) | 1.13 (0.07) | –0.07 (0.07) | 0.53 (0.07) | 0.15 (0.13) | 1.59 (0.13) | 0.16 (0.06) | 0.28 (0.06) | |
LSMD (95% CI) | 1.04 (0.85 to 1.23) | 0.60 (0.41 to 0.79) | 1.44 (1.07 to 1.82) | 0.13 (–0.03 to 0.29)c | |||||
P value | < 0.0001b | < 0.0001 | < 0.0001 | NA | |||||
Absolute change in SwCl (mmol/L) | |||||||||
BL; mean (SD) | 102.9 (9.8) | 102.3 (11.9) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) | 56.4 (25.5) | 59.5 (27.0) | |
LSM change (SE) | –0.4 (0.9) | –42.2 (0.9) | 1.7 (1.8) | –43.4 (1.7) | –3.4 (1.2) | –46.2 (1.3) | 0.7 (1.1) | –22.3 (1.1) | |
LSMD (95% CI) | –41.8 (–44.4 to –39.3) | –45.1 (–50.1 to –40.1) | –42.8 (–46.2 to –39.3) | –23.1 (–26.1 to –20.1) | |||||
P value | < 0.0001b | < 0.0001b | < 0.0001 | < 0.0001 | |||||
Pulmonary exacerbations | |||||||||
Patients with evt, n (%) | 76 (37.4) | 31 (15.5) | NA | NA | NA | ||||
Event rate per year | 0.98 | 0.37 | |||||||
Rate ratio (95% CI) | 0.37 (0.25 to 0.55) | ||||||||
P value | < 0.0001 | ||||||||
Pulmonary exacerbations requiring hospitalization | |||||||||
Patients with evt, n (%) | 27 (13.3) | 7 (3.5) | NA | NA | NA | ||||
Event rate per year | 0.24 | 0.07 | |||||||
Rate ratio (95% CI) | 0.29 (0.14 to 0.61) | ||||||||
P value | < 0.0001 | ||||||||
Pulmonary exacerbations requiring IV antibiotics | |||||||||
Patients with evt, n (%) | 42 (20.7) | 9 (4.5) | NA | NA | NA | ||||
Event rate per year | 0.36 | 0.08 | |||||||
Rate ratio (95% CI) | 0.22 (0.11 to 0.43) | ||||||||
P value | < 0.0001 | ||||||||
Time-to-first pulmonary exacerbation | |||||||||
Hazard ratio (95% CI) | 0.34 (0.22 to 0.52) | NA | NA | NA | |||||
P value | < 0.0001 | ||||||||
Time-to-first pulmonary exacerbation requiring hospitalization | |||||||||
Hazard ratio (95% CI) | 0.25 (0.11 to 0.58) | NA | NA | NA | |||||
P value | 0.0011 | ||||||||
Time-to-first pulmonary exacerbation requiring IV antibiotics | |||||||||
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | NA | NA | NA | |||||
P value | < 0.0001 | ||||||||
Summary of AEs, n (%) | |||||||||
At least 1 AE | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) | |
WDAEs | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) | |
Interruption due to AEs | 10 (5.0) | 19 (9.4) | 0 (0) | 0 (0) | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) | |
Grade 3/4 AEs | 15 (7.5) | 19 (9.4) | 1 (1.9) | 0 (0) | 7 (8.0) | 7 (8.0) | 4 (3.2) | 5 (3.8) | |
SAEs | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) | |
Most common AEs, n (%) | |||||||||
Infective PEx of CF | 95 (47.3) | 44 (21.8) | 6 (11.5) | 1 (1.8) | 36 (40.9) | 10 (11.5) | 13 (10.3) | 3 (2.3) | |
Sputum increased | 39 (19.4) | 40 (19.8) | 3 (5.8) | 3 (5.5) | 16 (18.2) | 10 (11.5) | 8 (6.3) | 6 (4.5) | |
Headache | 30 (14.9) | 35 (17.3) | 4 (7.7) | 3 (5.5) | 18 (20.5) | 25 (28.7) | 19 (15.1) | 11 (8.3) | |
Cough | 77 (38.3) | 34 (16.8) | 4 (7.7) | 8 (14.5) | 23 (26.1) | 11 (12.6) | 18 (14.3) | 3 (2.3) | |
AEs of special interest, n (%) | |||||||||
Elevated transaminases | 8 (4.0) | 22 (10.9) | 1 (1.9) | 2 (3.6) | 1 (1.1) | 6 (6.9) | 1 (0.8) | 8 (6.1) | |
Discontinuation | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | |
Interruption | 3 (1.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (0.8) | 0 (0) | |
Serious events | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | |
Any rash events | 13 (6.5) | 22 (10.9) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 11 (12.6) | 5 (4.0) | 4 (3.0) | |
Discontinuation | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
Interruption | 1 (0.5) | 4 (2.0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 1 (0.8) | |
Serious events | 1 (0.5) | 3 (1.5) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
AE = adverse event; BL = baseline; BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; evt = event; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for the F508del mutation with 1 minimal function mutation; F/RF = heterozygous for the F508del mutation with a residual function mutation; IV = IV; IVA = ivacaftor; LSM = least squares mean; LSMD = least squares mean difference; NA = not applicable; PEx = pulmonary exacerbation; RD = respiratory domain; SAE = serious adverse event; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ = tezacaftor; WDAE = withdrawal due to adverse event.
aPre-specified primary end point.
bPre-specified key secondary end point.
cPost hoc analysis only reported for the indirect comparison.
Source: Clinical Study Reports7-10 and additional information provided by sponsor.11
Critical Appraisal
Randomization was stratified based on relevant prognostic factors (i.e., age, sex, baseline ppFEV1, and prior CFTR modulator usage [in Study 104]).7-10 Baseline and demographic characteristics were generally well-balanced across the treatment groups in each of the included studies. Study treatments were administered in a double-blind manner with all groups issued the same number of tablets each day. The AE profile of ELX-TEZ-IVA and the comparators was unlikely to compromise blinding in any of the included trials. There were few patients who discontinued the trials (completion rate ranged from 96.8% to 100%), although the studies were relatively short in duration which may in part explain the high percentage of patients who completed.7-10 Adherence with the study treatments was reported to be greater than 99% across all treatment groups in the included trials.7-10 In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups. The only exception was the lower usage of some antibiotics for pulmonary exacerbations in the ELX-TEZ-IVA group relative to the placebo group in Study 102. This difference was attributable to the efficacy of ELX-TEZ-IVA for reducing pulmonary exacerbations relative to placebo. The primary and key secondary end points were analyzed with statistical testing procedures that controlled the type I error rate and all end points within the statistical testing hierarchies were statistically significant.
The diagnostic criteria used in Study 103 and Study 109 were consistent with Canadian clinical practice for identifying patients with CF who are homozygous for the F508del-CFTR mutation. The gating and residual function (RF) mutations that were used to select patients for inclusion in Study 104 were consistent with the approved indications for TEZ-IVA and IVA in Canada.9,12,13 There were no widely accepted criteria for defining minimal function (MF) mutations in the CFTR gene; therefore, the identification of patients with MF mutations in Study 102 relied on a novel approach designed by the sponsor (i.e., in vitro response to TEZ, IVA, or TEZ-IVA).7 The clinical experts consulted by CADTH noted that terms “residual function” and “minimal function” are not currently used in Canadian clinical practice. Patients with CF with more severe lung disease (e.g., ppFEV1 < 40% at screening) or a normal ppFEV1 at screening (≥ 90%) were excluded from the studies7-10; therefore, the results of the included studies are primarily applicable to patients with moderate (i.e., FEV1 = 40% to 69%) to mild (i.e., FEV1 = 70% to 89%) lung disease. As patients with advanced lung disease are an important subgroup with a high level of unmet medical need, CADTH supplemented this review with additional evidence from observational studies to address this important gap in the RCT evidence.
Study 103, Study 104, and Study 109 included an open-label, 4-week, active treatment period with TEZ-IVA or IVA before randomization. As such, these trials were essentially investigating switching to ELX-TEZ-IVA from either TEZ-IVA or IVA compared with remaining on TEZ-IVA for patients with an F/F or F/RF genotype or remaining on IVA for patients with an F/G genotype. As TEZ-IVA is not widely reimbursed in Canada, the switching design limits the generalizability of the studies directly to the Canadian setting. To address this potential gap in the evidence, the sponsor-submitted indirect comparisons with CADTH to provide an estimate of ELX-TEZ-IVA versus placebo for those with an F/F or F/RF genotype.
Indirect Comparisons
Description of Studies
The sponsor conducted indirect comparisons to derive relative estimates of the clinical efficacy for ELX-TEZ-IVA compared to local standard of care in the F/F, F/RF and F/G populations, given the absence of RCTs. Although head-to-head trials were conducted for ELX-TEZ-IVA versus TEZ-IVA (for patients with F/F or F/RF genotypes) and IVA (for patients with an F/G genotype), the sponsor conducted indirect comparisons to derive estimates of effect for: |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. A literature search conducted by CADTH did not identify any additional published indirect comparisons that included the patients, interventions, and outcomes identified in the protocol for CADTH’s review of ELX-TEZ-IVA.
All the sponsor’s indirect comparisons were conducted using the Bucher method for continuous end points. The sponsor stated that the Bucher method was considered the most appropriate approach for these indirect comparisons because of the 4-week active treatment run-in periods in the ELX-TEZ-IVA trials. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Efficacy Results
For patients with an F/F genotype
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
For patients with an F/G genotype
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
For patients with an F/RF genotype
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Harms Results
The indirect comparison filed by the sponsor did not include any comparisons for AEs.
Critical Appraisal
The primary limitation of the indirect comparisons was the difference in study design across the included studies. The ELX-TEZ-IVA studies (i.e., Study 104 and Study 109) included the open-label, 4-week, active treatment period with TEZ-IVA or IVA before randomization. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Other Relevant Evidence
Long-Term Extension Study
Study 105 is an ongoing, open-label uncontrolled trial that enrolled patients who had completed Study 102 or 103 (i.e., patients with either an F/MF or an F/F genotype). Interim results were reported for 24 weeks of follow-up for Study 102 patients and 36 weeks for Study 103 patients (data cut-off October 2019).2 A total of || patients were enrolled in the extension study (n = || from Study 102 and n = || from Study 103).
Efficacy Results
Among patients previously enrolled in Study 102, the absolute change from baseline to week 24 in ppFEV1 was similar for patients who switched from placebo to ELX-TEZ-IVA (14.9%; 95% CI, 13.5 to 16.3) and for those who remained on ELX-TEZ-IVA (14.3%; 95% CI, 12.9 to 15.7) during the extension study. Patients previously enrolled in Study 103 reported an absolute change from baseline to week 36 in ppFEV1 of 12.8% (95% CI, 10.1 to 15.4) and 11.9% (95% CI, 9.3 to 14.5) during the extension study, for patients previously treated with TEZ-IVA and ELX-TEZ-IVA, respectively.
During treatment with ELX-TEZ-IVA, the annual event rate for pulmonary exacerbations was |||||||||||||||||||||||||||||||| for those previously treated with placebo and |||||||||||||||||||||||||||||||| for those previously treated with ELX-TEZ-IVA in Study 102, and 0.30 (95% CI, 0.20 to 0.45) for those previously enrolled in Study 103.
The least squares (LS) mean change from baseline to week 24 for the CFQ-R (RD) was 19.2 (95% CI, 16.7 to 21.7) for those switched from placebo to ELX-TEZ-IVA (Study 102), and 20.1 (95% CI, 17.6 to 22.6) for those who received ongoing ELX-TEZ-IVA treatment. The LS mean change was 13.8 (95% CI, 8.9 to 18.8) and 14.3 (95% CI, 9.5 to 19.2) for patients from Study 103, respectively, who were switched from TEZ-IVA to ELX-TEZ-IVA, and those treated with ELX-TEZ-IVA in both study periods.
The absolute change in BMI from baseline to week 24 (Study 102) or week 36 (Study 103) ranged from a LS mean of 1.2 kg/m2 to 1.3 kg/m2. The change from baseline in BMI z score was reported for patients who were aged 20 years or younger at the start of the parent studies. The point estimate for the LS mean change from baseline in z scores ranged from 0.30 to 0.43 across the different treatment populations.
Harms Results
Most patients |||||| reported at least 1 AE during the extension study. The most reported AEs were infective pulmonary exacerbation of CF ||||||, cough ||||||, oropharyngeal pain |||||| and nasopharyngitis ||||||. |||| patients |||||| stopped treatment due to AEs and | patients |||||| experienced at least 1 SAE.
Critical Appraisal
Study 105 is an ongoing, uncontrolled, open-label trial that enrolled patients who had completed Study 102 or Study 103. As this was an unblinded study, patient’s expectations of treatment could potentially have biased the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R), or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enrol. For Study 105, the risk of selection bias may be low given that only | patients |||||| out of the || randomized in the parent studies, were not enrolled or treated in the extension study. During the first 24 weeks of follow-up, discontinuation of treatment was also low ( | patients, ||); however, the frequency of missing data was higher for some outcomes relative to others. Issues with the generalizability of these data are the same as for the parent double-blind studies.
Observational Studies in Patients With Advanced Lung Disease
Two observational studies provided short-term data on the efficacy and safety of ELX-TEZ-IVA in patients with CF and with advanced pulmonary disease (ppFEV1 < 40% or under evaluation for lung transplantation). All patients had at least 1 F508del CFTR mutation.
Irish Cohort
The retrospective chart review by O’Shea et al4 reported data for 14 patients who were followed for a mean duration of 4.9 months after starting ELX-TEZ-IVA. Statistically significant improvements were reported for: mean ppFEV1 (increased from 27% [standard deviation {SD} = 7.3] at baseline to 36% [SD = 16.5] after a mean follow-up of 26 days); mean BMI (increased from 20.7 kg/m2 [SD = 3.6] to 22.1 kg/m2 [SD = 3.4]) and mean sweat chloride (reduced from 105 mmol/L [SD = 15] to 54 mmol/L [SD = 23]) after an average of 62 days of follow-up. The rate of infective pulmonary exacerbations requiring hospitalization was 0.28 events per month (SD = 0.17) in the 12 months before ELX-TEZ-IVA, and 0.04 events per month (SD = 0.07) during the 4.9-month follow-up period (P < 0.001).
French Cohort
The prospective cohort study by Burgel et al5 reported data for 245 patients who were followed for a median of 84 days after initiating treatment with ELX-TEZ-IVA. The mean change from baseline in the ppFEV1 was 15.1% (95% CI, 13.8 to 16.4) and the change from baseline in weight was 4.2 kg (95% CI, 3.9 to 4.6), based on pooled data from 1- and 3-month assessments. The authors reported statistically significant reductions in the percentage of patients receiving long-term oxygen (43% at baseline versus 23% at 3 months), non-invasive ventilation (28% at baseline versus 20% at 3 months), and enteral tube feeding (18% at baseline versus 10% at 3 months). Data were missing for 31% of patients at the 3-month visits with no imputation in the analyses. Prior to the initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates in the next 3 months (total of 53 patients; 22%). At the end of follow-up, 5 patients (2%) were on the transplant list or being considered for transplant, 2 patients had received a transplant (0.8%), and 1 patient died while waiting for transplant (0.4%).
Critical Appraisal
The 2 observational studies provided descriptive data on the effects of ELX-TEZ-IVA in CF patients with advanced lung disease. The short-term results showed acute increases in ppFEV1 and weight that were comparable to those observed in the clinical trials; but should be interpreted with caution given the limitations of the open-label, uncontrolled, observational study designs, and the small sample size for the Irish cohort (N = 14). Both studies had a limited follow-up duration, and the monitoring and reporting of patient outcomes were impacted by the COVID-19 pandemic and lockdown measures. The large amount of missing data for some outcomes makes it challenging to interpret and generalize the results of these studies.
Simulation Study for Morbidity and Mortality
Stanojevic et al6 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. The model forecasted an increase in median survival and a reduction in pulmonary exacerbations with the introduction of ELX-TEZ-IVA. The outcomes from these simulations are contingent on the validity of several assumptions that were required to build the model and extrapolate the impacts out to 10 years. There is uncertainty in the extrapolation of short-term effects of ELX-TEZ-IVA in a subset of patients with CF, to the broader population in the longer-term, and in the generalizability of observational data with IVA on the rate of decline in ppFEV1 to patients treated with ELX-TEZ-IVA. Moreover, the model likely overestimates the proportion of CF patients who may receive ELX-TEZ-IVA and impact of treatment on pulmonary exacerbations.
Conclusions
A 24-week, placebo-controlled, RCT (Study 102, N = 403) conducted in patients with an F/MF genotype demonstrated that, compared with placebo, 24-weeks of treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI), health-related quality of life (increase in CFQ-R [RD] scores), CF biomarkers (reduction in sweat chloride), and a reduced rate of pulmonary exacerbations, including events that required IV antibiotics and/or hospitalization to manage. Three additional double-blind, active-controlled RCTs investigated switching to ELX-TEZ-IVA after 4 weeks of treatment with either TEZ-IVA or IVA compared with remaining on those other CFTR modulators. Study 103 (N = 107; 4 weeks) and Study 109 (N = 175; 24 weeks) were conducted in patients with an F/F genotype and demonstrated that treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 and CFQ-R compared with remaining on TEZ-IVA. Study 104 (N = 258; 8 weeks) demonstrated that switching to ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 compared with remaining on IVA in patients with an F/G genotype treatment and a modest improvement compared with remaining on TEZ-IVA for patients with an F/RF genotype. Patients with advanced lung disease were largely excluded from the phase III RCTs; however, post hoc subgroup analyses and data from 2 short-term observational studies suggests that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function in these patients.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., at least 12 years of age with at least 1 F508del mutation). SAEs and WDAEs were rare in the included studies. The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends that ALT and AST be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter. The clinical experts consulted by CADTH noted that the recommendations for monitoring with ELX-TEZ-IVA was not anticipated to result in a substantial increase in the number of the clinic visits for CF patients (particularly after the first year of initiating the treatment).
Introduction
Disease Background
CF, an autosomal recessive condition, is the most common fatal genetic disease affecting children and young adults in Canada. It is caused by mutations in the CFTR gene, which is located on chromosome 7. The CFTR gene encodes a chloride channel that regulates ion and fluid transport across cell membranes. When CFTR is dysfunctional, secretions become tenacious and sticky, resulting in pathology in multiple organs, including the lungs, large and small intestines, pancreatic and bile ducts, and the vas deferens. A deletion of phenylalanine 508 in the first nucleotide binding domain (NBD1) (F508del) is the most common mutation that results in CF.1 The CCFR reported that there were 4,344 Canadians living with CF in 2019. Of these, 87.8% of patients carried at least 1 F508del mutation (47.1% were homozygous and 40.7% were heterozygous).1
More than 2,090 CFTR variants have been identified among patients with CF.1 The CFTR variants have been classified as impaired biosynthesis (class I), defective protein maturation and accelerated degradation (class II), defective regulation of CFTR at the plasma membrane (class III), defective chloride conductance (class IV), diminished CFTR transcription (class V), and accelerated turnover at the cell surface (class VI).14 CFTR variants within classes I to III are associated with severe CF as they are considered non-functional, while CFTR variants in classes IV to VI may retain CFTR function.14,15 The F508del mutation is typically considered a class II CFTR mutation and is a severe mutation resulting in significant loss of function of the CFTR protein. F508del defect causes CFTR to misfold and thus most of the protein is removed before it can reach the cell membrane. In addition, the F508del CFTR presents a defect in channel gating, as well as being unstable and having more rapid turnover at the cell membrane.16,17 Genotyping for mutations in the CFTR gene is routinely performed on almost all patients with CF in Canada and is also part of the newborn screening process.1
CF results in airway obstruction, chronic endobronchial infection, and inflammation, which ultimately lead to destruction of lung tissue through development of bronchiectasis and loss of lung function.18 Although chronic pulmonary therapies instituted early in the disease have reduced the decline in lung function over time, patients who are homozygous for the F508del mutation will develop chronic infection with Pseudomonas and progressive bronchiectasis and airway obstruction. In a cohort of approximately 1,000 healthy young children with CF who did not have Pseudomonas infection at enrolment, there was a greater annual decline in FEV1 over the following 4 years in those who were homozygous for the F508del mutation.19 Chronic endobronchial infection of the airways with bacterial pathogens, such as Pseudomonas aeruginosa (reported in 38% of Canadian CF patients in 2019)1 is associated with a more rapid loss of lung function.20 Acute or chronic endobronchial infections result in further destruction of lung tissue and are associated with respiratory morbidity. Lung disease accounts for the vast majority of death in CF patients (> 80%).1,21
Pulmonary exacerbations are associated with lung function decline, mortality, and may require treatment with IV antibiotics and hospitalization. The Cystic Fibrosis Foundation has reported that approximately 1-third of CF patients will have at least 1 pulmonary exacerbation per year requiring IV antibiotics.21
Maintenance of pulmonary function (higher FEV1) and fewer respiratory exacerbations are associated with increased survival.22 Pulmonary management of CF therefore aims to clear the airways of secretions and treat lung pathogens to minimize inflammation.
Patients who are homozygous or heterozygous for the F508del mutation typically have pancreatic, gastrointestinal, and nutritional disease as well as progressive pulmonary damage. Gastrointestinal and pancreatic involvement results in pancreatic exocrine insufficiency in most individuals with CF, causing malabsorption of fats and fat-soluble vitamins, which leads to malnutrition. Maintaining adequate nutrition is associated with improved clinical outcome and longevity for patients with CF.23 Virtually all of these people will be pancreatic insufficient and will need to take lifelong pancreatic enzyme replacement with every meal as well as fat-soluble vitamin therapy. With increasing age, these patients will develop CF-related diabetes and require therapy with insulin. In 2019, CF-related diabetes was reported in 22.0% of Canadian CF patients (33.5% of adults and 3.3% of children).1
The median age of survival in Canada for a child born with CF in 2019 is estimated to be 53.4 years.1 The CCFR has reported in increase in the median age of death for patients with CF in Canada since the year 2000.1 In 2019 the median age of death was 42.1 years compare with 27.7 years in 2000, 35.1 years in 2013, and 38.9 years in 2016.1,24,25 There is a clear unmet need for better CF therapies (see Patient Group Input and Clinician Input).
Standards of Therapy
The goals of CF therapy include preservation of lung function by minimizing pulmonary infection and inflammation; restoration of baseline pulmonary function, symptoms, and level of inflammation after acute respiratory exacerbations; and maintenance of adequate nutrition. The choice of a therapeutic regimen for CF depends on organ involvement. The severity of lung function impairment and the presence of bacterial pathogens are deterministic factors when selecting chronic pulmonary therapy.
Treatments that are approved and/or available can be broadly classified as therapies used to manage symptoms, complications, and comorbidities of CF, and therapies that aim to correct the underlying defects of the CFTR protein, known as CFTR modulators.
Management of Symptoms, Complications, and Comorbidities
Respiratory treatments consist of physiotherapy and pharmacologic agents such as inhaled antibiotics (e.g., tobramycin, aztreonam, and colistin), anti-inflammatory agents, or mucolytics (e.g., hypertonic saline and/or dornase alfa).26 Nutritional treatments consist of high calorie and high fat diets and pancreatic enzyme replacement for those with pancreatic insufficiency.26,27 Pulmonary exacerbations are treated with oral or IV antibiotics.28 These treatments do not halt, but only slow, the decline in lung function and the progression of disease.
CFTR Modulators
CFTR modulators are a class of medications that aim to correct the underlying defects of the CFTR protein. The CFTR modulators that are currently marketed in Canada or other jurisdictions are classified as follows.
Potentiators, which function by increasing the channel-open probability of the CFTR protein at the cell surface. IVA is a CFTR potentiator.
Correctors, which function by improving the conformational stability of F508del-CFTR protein, resulting in an increased expression of the F508del-CFTR protein at the cell surface. LUM, TEZ, and ELX are CFTR correctors.
Table 4 provides a summary of the CFTR modulators currently marketed or under review in Canada, the CFTR mutations and age ranges for which they been approved by Health Canada, and the reimbursement status within the public drug programs. The currently available CFTR modulators are not approved for use in all patients with at least 1 F508del mutation. The approved indications currently cover those who are homozygous for F508del mutations (Orkambi and Symdeko), heterozygous for the 508del mutation and who also have 1 of the following mutations: RF mutation (Symdeko) or a gating mutation (Kalydeco). Hence, there are subset of individuals who are heterozygous for the F508del mutation who will not be covered by the existing indications. In addition, the clinical benefit of some of the existing treatments (e.g., Orkambi) has been described as modest; therefore, there remains an unmet medical need for treatments with the potential to offer greater treatment effects and benefits.29 In 2019, CF Canada reported that 658 individuals were receiving treatment with CFTR modulators (216 children and 442 adults). The number of patients receiving each treatment were: 146 receiving Kalydeco, 368 receiving Orkambi, and 186 receiving Symdeko.1
Drug
Trikafta consists of a fixed-dose combination tablet containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg co-packaged with a tablet containing IVA 150 mg (ELX-TEZ-IVA). ELX-TEZ-IVA is indicated for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene. The sponsor has requested that ELX-TEZ-IVA receive a recommendation to reimburse in accordance with the Health Canada–approved indication. ELX-TEZ-IVA was accepted as a priority review by Health Canada.
Mechanism of Action
ELX-TEZ-IVA is the third treatment specifically indicated for the treatment of CF patients who have F508del mutation(s) in the CFTR gene. This mutation is believed to be associated with misfolding of the CFTR protein, which results to a lower quantity of CFTR expression at the cell surface. In addition to the reduced quantity of the protein, the mutation results in CFTR that is less stable and has defective channel gating compared with wild-type CFTR. Treatment with ELX-TEZ-IVA results in an increased quantity and improved function of the F508del-CFTR protein at the cell surface, through the following mechanisms29-31:
ELX and TEZ improve the conformational stability of F508del-CFTR protein, resulting in an increased expression of the F508del-CFTR protein at the cell surface
IVA increases the channel-open probability of the CFTR protein at the cell surface
Recommended Dosage
The recommended dose of ELX-TEZ-IVA is 2 combination tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg) in the morning and 1 stand-alone tablet (containing IVA 150 mg) taken in the evening. Both tablets are administered orally (swallowed whole) and should be taken approximately 12 hours apart with fat-containing food. Table 3 provides a summary of the recommended dosage adjustments for patients with hepatic insufficiency or those receiving concomitant treatment with moderate CYP3A inhibitors (e.g., fluconazole or erythromycin) or strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, and clarithromycin).
Table 3: Recommended Dosage Adjustments
Conditions | Dose adjustment | |
|---|---|---|
Hepatic insufficiency | Mild (Child-Pugh Class A) | No dose adjustments |
Moderate (Child-Pugh Class B) | Use not recommendeda | |
Severe (Child-Pugh Class C) | Should not be used | |
CYP3A inhibitors | Moderate CYP3A inhibitors | Morning: 2 ELX-TEZ-IVA tablets (day 1); 1 IVA tablet (day 2) Evening: No dosage |
Strong CYP3A inhibitors | Morning: 2 ELX-TEZ-IVA tablets (twice weekly; 3 to 4 days apart) Evening: No dosage | |
ELX = elexacaftor; IVA = ivacaftor; TEZ = tezacaftor.
aTreatment of patients with moderate hepatic impairment should only be considered when there is a clear medical need and the benefits are expected to outweigh the risks. If used, ELX-TEZ-IVA should be used with caution at a reduced dose, as follows: 2 ELX-TEZ-IVA tablets alternating with 1 ELX-TEZ-IVA tablet taken in the morning, on alternate days. The evening dose of the IVA tablet should not be taken.
Previous CADTH Reviews
This is first submission to CADTH for ELX-TEZ-IVA. CADTH has previously reviewed IVA alone for the following indications: patients 6 years of age and older who have a G551D mutation in the CFTR gene; patients aged 6 years and older who have 1 of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, S549R, or G970R; and patients aged 18 years and older who have an R117H mutation in the CFTR gene.32-34 For each of these indications, CDEC recommended that IVA be reimbursed with conditions. LUM-IVA was previously reviewed for the treatment of CF in patients who are homozygous for the F508del mutation in the CFTR gene and received do not reimburse recommendations in 2016 and 2018.35,36 CADTH was unable to recommend reimbursement for TEZ-IVA as a submission was not filed by the sponsor.37
Table 4: Key Characteristics of CFTR Modulators
Parameters | Trikafta (ELX-TEZ-IVA) | Orkambi (LUM-IVA) | Symdeko (TEZ-IVA) | Kalydeco (IVA) |
|---|---|---|---|---|
Mechanism of action | CFTR potentiator (IVA) and correctors (ELX-TEZ) | CFTR potentiator (IVA) and corrector (LUM) | CFTR potentiator (IVA) and corrector (TEZ) | CFTR potentiator |
Indicationa | Patients aged ≥ 12 years who have at least 1 F508del mutation in the CFTR gene | Patients aged ≥ 2 years of age who are homozygous for the F508del mutation in the CFTR gene | Patients aged ≥ 12 years who are homozygous for the F508del mutation or who are heterozygous for the F508del mutation and have 1 of the following CFTR mutations: P67L, D110H, R117C, L206W, R352Q, A455E, D579G, 711 + 3A→G, S945L, S977F, R1070W, D1152H, 2789 + 5G→A, 3272-26A→G, or 3849 + 10kbC→T | Tablets: Patients ≥ 6 years and weighing ≥ 25 kg with 1 of the following CFTR mutations: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R Tablets: Patients aged ≥ 18 years with an R117H CFTR mutation Granules: Children ≥ 12 months and weighing 7 kg to < 25 kg with 1 of the following CFTR mutations: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R |
Route of administration | Oral tablets | Oral tablets and granules | Oral tablets | Oral tablets and granules |
Recommended dose | Morning: ELX 100 mg, TEZ 50 mg, and IVA 75 mg Evening: IVA 150 mg | Tablets:
Granules
| Morning: TEZ 100 mg and IVA150 mg Evening: IVA 150 mg | Tablets: IVA 150 mg q12h Granules:
|
Serious adverse effects or safety issues | Product monographs of each of the products include a warning about the risk of elevated transaminases (ALT and AST) and monitoring of liver function is recommended before initiating treatment, every 3 months during the first year of treatment, and annually thereafter.12,13,30,38 The product monographs recommends that ELX-TEZ-IVA not be used in patients with severe hepatic impairment; dosage reduction scenarios are provided in the product monographs for IVA, TEZ-IVA, and LUM-IVA.12,13,30,38 | |||
CADTH reviews | Under review | Non-submission37 | ||
ALT = alanine transaminase; AST = aspartate transaminase; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; IVA = ivacaftor; LUM = lumacaftor; q12h = once every 12 hours; TEZ = tezacaftor.
aHealth Canada–approved indications.
Source: Product monographs for Trikafta, Orkambi, Symdeko, and Kalydeco.12,13,30,38
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Three patient groups, CF Canada, the Canadian Cystic Fibrosis Treatment Society and CF Get Loud, responded to CADTH’s call for patient input.
CF Canada is a national not-for-profit corporation committed to improving and lengthening the lives of people living with CF through treatments, research, information, and support. CF Canada funds basic, discovery science, and clinical research, as well as multi-disciplinary CF clinics in Canada, manages the CCFR, and maintains a network of CF advocates. Information for this submission was based on a cross-Canada survey of patients and caregivers that was circulated through CF clinics, email, and social media in January 2021. Of the 1,455 respondents, 31% were adults living with CF, 17% were a spouse or caregiver of an adult living with CF, 12% were parents of 1 or more children with CF between the ages of 12 to 17 years, and 20% were parents of 1 or more children with CF aged 11 years or younger (other respondents were excluded from the data submitted). Of the 422 adults with CF who responded, 12% were currently taking ELX-TEZ-IVA through SAP, 7% received it through a clinical trial, and all but 1 adult was still accessing it. Six percent of respondents had tried to access ELX-TEZ-IVA through SAP but were unsuccessful and 63% have not tried to access ELX-TEZ-IVA but had an indication for it. All respondents were residents of Canada. The patient input submission also includes information from the medical literature and the CCFR.
The Canadian Cystic Fibrosis Treatment Society is a not-for-profit organization whose mandate is to advocate for individuals with CF that require access to medications and medical procedures that save and improve lives. The Canadian Cystic Fibrosis Treatment Society gathered information through 1-on-one and group discussions with individuals with CF, parents, caregivers, and treating physicians.
CF Get Loud is a Canadian grassroots movement that represents a community of greater than 4,000 patients, families, and allies across Canada. Its goal is to bring hope, in the form of new life-saving medicines, to the community. CF Get Loud gathered information for this submission from a letter campaign in July 2020 that received 11,364 letters from Canadians, a town hall with CF experts and leaders in May 2020, and from 20 Canadians who are currently receiving ELX-TEZ-IVA.
Disease Experience
CF is the most common fatal genetic disease affecting children and young adults in Canada. There is no cure.
CF causes various effects on the body, but mainly affects the digestive system and lungs. The clinical progression of CF can vary greatly from person to person, even among those with the same genetic mutations. The most significant clinical impact is in the lungs, where patients have difficulty in clearing secretions, which in combination with aberrant inflammation, leads to persistent infections with cycles of inflammation that are ineffective in clearing infections. This leads to progressive scarring of the airways and a progressive and sometimes rapid decline in lung function. Patients may suffer frequent pulmonary exacerbations requiring weeks of hospitalization and IV antibiotics. Exacerbations cause rapid decline of lung function and more rapid disease progression and are associated with a greater risk of death. Other consequences of having CF include malnutrition and very low BMI, and CF-related comorbidities such as CF-related diabetes and CF-related liver disease. People living with CF are often unable to build enough body mass and may require a feeding tube for supplemental nutrition.
CF has a tremendous impact on the people who live with it, their loved ones, and on society. As the disease advances, even more time and effort are needed to manage the progressive and debilitating symptoms. Children with CF may need to quit school or go part-time and adults with CF may need to leave the work force or undertake part-time work, as may caregivers of children and adults with CF.
In addition to the decline of CF patients’ physical health, many suffer from the unseen effects of CF. These include, but are not limited to depression, anxiety, and hopelessness. The mental anguish caused by the ever-present awareness of 1’s mortality cannot be expressed in words and are often not quantified. Parents and caregivers have an overwhelming desire to do something to help their loved ones. CF Canada reported that significantly more caregivers for adults with CF (44%) said caregiving had a negative impact on their physical health than said it had a positive impact (17%). More than 2-thirds (72%) of reporting caregivers said that caregiving had a negative impact on their mental health while 11% felt that it had a positive effect.
I lost 3 friends in 3 months, while they waited for a lung transplant. It’s not right to bury your friends all under the age of 25. I’ve been to more funerals than weddings in my life. – Adult with CF
I struggled to keep up with work and university and had to spend up to 2 hours a day on exhausting, never ending, treatments. For 20 years I had about 3 hospital admissions a year. This meant I had over 60 hospital admissions, equalling more than 3 years of my life in hospital. – Adult with CF
My 11-year-old daughter spends in excess of 26 hours a week trying to stay healthy. The fight against CF is all encompassing for the family. It requires giving up 2 to 7 hours every day for her therapies. The physical therapies take a toll on my and my wife’s bodies. We both have repetitive strain injuries and arthritis in our hands, wrists, and shoulder. This commitment requires scheduling all meals and everyone’s activities around her therapies. We restrict our social activities to prevent passing on colds and flus. Each day that a control for CF is not available to her is a day that her lungs are deteriorating. All the treatments that she has access to only try to mitigate her existing health problems, none address the root cause. Without the availability of drugs that fix the basic defect in CF, our daughter and others like her will lose their valiant fight as they pass away while gasping for air. – CF parent
Experiences With Currently Available Treatments
Currently available treatments now include 4 CFTR modulator therapies that are indicated for specific CFTR mutations. IVA (Kalydeco) is the only CFTR modulator that is broadly available in Canada and treats approximately 4% of people living with CF. LUM-IVA (Orkambi) and TEZ-IVA (Symdeko) are both second generation CFTR modulators that could benefit as many as 50% of Canadians with CF, but neither is available through public payers in Canada, with the exception of Quebec, which provides access only to those who meet the strict eligibility requirements of the “patient d’exception” program. ELX-TEZ-IVA is the third generation of CFTR modulators.
The patient groups stated that individual responses to currently available CFTR modulators are highly variable and some patients report having benefited greatly from 1 or another of the earlier modulators. The Canadian Cystic Fibrosis Treatment Society reported that its founder has experienced a life-changing benefit from IVA and reported normal weight gain, improved lung function and energy levels, and reduced cough. CF Canada stated that the clinical benefits gained from IVA, LUM-IVA, or TEZ-IVA are more modest than those from ELX-TEZ-IVA. Some patients reported intolerable adverse effects with LUM-IVA in particular.
There are hundreds of therapies that aid in symptom management in the categories of antibiotics, supplemental vitamins, aerosol bronchodilators, mucolytics and pancreatic enzymes, anti-inflammatories, and steroids. Most CF patients take pancreatic enzymes, multi-vitamins, and nutritional supplements to maintain normal growth. Every day, patients with CF perform airway clearance techniques at least twice a day for about 30 to 60 minutes per session to improve the clearance of secretions from their lungs. Inhaled medications are used to open the airways while inhaled antibiotic treatments are used to control infections. The total time spent on maintaining lung health for many patients is 2 to 4 hours each day. People with CF may take more than a hundred different pills a day.
Patients frequently have periods of infection and acute inflammation called exacerbations that require a hospital stay that may be 2 to 4 weeks in duration. Patients may require IV antibiotics administered in the hospital or at home. Eventually the ongoing cycles of infection and inflammation destroy the lungs. Lung transplantation is the last recourse for people with end-stage CF.
Many of the drugs that patients need to take on a regular basis have negative adverse effects. The steroids that are used to reduce the inflammation and help patients recover from the exacerbation ultimately damage organs in the long run, contributing to the development of CF-related diabetes in 35.2% of all Canadian adults with CF. Antibiotics can cause kidney damage and total lifetime dose must be controlled; others permanently stain the teeth. Chronic use of antibiotics leads to resistance and as patients age, a need to try multiple antibiotics to find 1 that works. Because patients are on so many drugs, drug-drug interactions become difficult to manage and can interfere with optimum therapy.
A summary of the day in the life of 1 CF patient with advanced disease, during the evaluation period pre-transplant:
A typical day at home: 6:00 to 7:30 AM: IV (IV) antibiotics (2x40 minutes). They connect with my picc-line. It's rather tedious because of the many steps of the procedure: disinfect, flush with saline, connect the antibiotic, wait 40 minutes, flush with saline again, connect the next antibiotic, wait 40 minutes... etc. Very often, my Mum, Dad or sister will do this for me while I sleep in, so I can catch a bit more sleep. 8:00 to 9:00 AM: wake-up routine; asthma meds, inhaled antibiotics and enzymes, pep-mask physiotherapy, wash all the nebulizers, prep any meds that need to be reconstituted. 9:00 to 10:00 AM: breakfast; meal routine: check blood sugar, take insulin, have breakfast, morning pills (the usuals + check calendar for the ones on a variable schedule), Scandishake, after-breakfast meds, if any (check calendar). 1:00 to 2:00 PM: lunch; repeat meal routine; 2:00 to 4:00 PM: IV antibiotics (3x40 minutes), (concurrent) 3:00 to 3:10 PM: inhaled antibiotics. 4:00 to 5:00 PM: exercise. 6:00 to 7:00 PM: supper; repeat meal routine. 8:00 to 9:00 PM: clapping physiotherapy. 9:00 to 9:30 PM: bedtime routine; asthma meds, inhaled antibiotic, bedtime meds (check calendar). 10:00 to 11:30 PM: IV medications (2x40 minutes) Fairly often, my Mum, Dad or sister will do this 1 for me too so I can go to bed a bit earlier. Juggling the timing of everything is a bit of a headache, mostly because I need to space out eating with physiotherapy (doing physio or exercise tends to give me coughing fits, which makes me throw up if I've eaten too recently). On most days I've also got a limited amount of energy, so I've got to manage my activities to make sure I don't crash before the end of the day. Other regular tasks include: keeping medical appointments (1/week or more); preparing pills in advance (it saves time at meals); speaking with my pharmacist 2 to 3 × a week to order meds, arrange delivery...and…staying on top of insurance reimbursements (3 to 4 hours/month or so).
In addition to the time spent administering daily treatments, the hospitalizations and outpatient CF clinic visits interfere with school and work for both adult patients and the parents of children with CF. Many patients must travel significant distances to specialized CF clinics to receive routine care. CF Canada’s survey findings indicate that the burden for caregivers of individuals with CF to provide standard treatments is significant. Of the caregivers of adults, 40% spend 10 hours or less per week on caregiving activities, but 33% spend between 11 to 20 hours per week, and another 27% spend more than 20 hours per week on caregiving activities. Of the caregivers of children, only 17% spend less than 10 hours per week, 53% spend 11 to 20 hours, 17% spend 21 to 30 hours, and another 12% spend more than 30 hours weekly on disease management. Among caregivers of patients with CF, 60% had to take time off work, 6% to 12% had to leave full-time work for part-time work, 6% to 13% had to quit work altogether, and 2% to 4% had to take time off school or leave school altogether.
Improved Outcomes
Patients with CF are seeking treatments that can change the trajectory of the disease and improve both life expectancy and quality of life. Improved outcomes include retaining or increasing lung function, improved digestive health, better energy levels, and minimizing symptoms of CF. Patients want to avoid hospital admissions and reduce the needs for invasive medical procedures and the treatment burden of daily therapies. They also wish to avoid the adverse effects of therapies, such as osteoporosis, antimicrobial resistance, and CF-related diabetes or liver dysfunction. Patients are seeking a feeling of wellness and well-being that is not provided by the currently available treatments. Patients want treatments that will allow them to attend school and work, be physically and socially active, participate in everyday household activities, have a family, and live a “normal” life.
When asked about what their child or spouse taking ELX-TEZ-IVA could mean for them personally, caregivers said:
She would be totally independent, free to plan her life without all the physical, and medical regime restrictions she has to endure at present, because her health status would improve greatly on the drug. She would finally be able to breathe easy, to be happy and hopeful for a long enriching life. – CF parent
My son would be able to pursue his studies as an Engineer without the health decline that comes with CF. He could work, chase his dreams like anyone else. – CF parent
I wouldn’t have to think about becoming a widow before age 40.– CF spouse
It would have a positive impact all around not only for them, but also on the rest of the family- especially their mental health. – CF parent
Companion Diagnostic
Medical diagnostic laboratories typically conduct panel screens for the most common mutations in Canada. Such tests detect the mutations in approximately 98% of the Canadian CF population. If medically indicated, complete exome sequencing will identify virtually all CF mutations, and in fact, the falling costs of such tests make it even more economical to sequence than to screen panels of mutations. Both the coverage and the availability of genetic testing vary across Canada.
According to the Canadian CF Registry, genetic mutations have been identified in 99% of all patients who were seen in a CF clinic in 2019. Most individuals for whom ELX-TEZ-IVA is indicated are known by their clinic or can be queried by their clinic using the registry.
ELX-TEZ-IVA is the first CFTR modulator therapy available to treat patients with at least 1 copy of the most common CF mutation, F508del.
Experience With Drug Under Review
Two executive team members from CF Get Loud who received ELX-TEZ-IVA through SAP were able to postpone lung transplant, had normal sweat chloride levels, and felt revitalized because of treatment. Another patient with end-stage disease reported an improvement in lung function, weight gain, better sleep, and energy levels after receiving ELX-TEZ-IVA. She experienced such a marked improvement in her physical health that she was able to go running. In addition, her spouse was able to work full time, and her family’s fears for her well-being have been abated. Another adult with severe CF stated that ELX-TEZ-IVA reduced the thick, sticky mucous in her lungs, and made daily airway cleaning treatments easier and more effective. During treatment with ELX-TEZ-IVA, she has had no CF exacerbations, need for IV antibiotics or supplemental oxygen, and has shown a nearly 10% increase in lung function. Plans for a lung transplant have been put on hold. She reported that she is living life like a 38-year-old mother should be.
CF Canada provided input from 53 patients who have experience with the drug under review (28% through clinical trials and 72% through SAP). Forty-six (87%) found their experience with ELX-TEZ-IVA to be very positive, 6 (11%) found it to be positive, and 1 respondent (2%) indicated a neutral experience. There were no negative or very negative experiences reported. In terms of health outcomes, adults reported that ELX-TEZ-IVA has resulted in positive changes to their health. Specifically, it helped them gain weight (87%), increased their lung function (85%), slowed or stopped progression of symptoms (83%), resulted in fewer hospitalizations (83%), improved their energy (83%), improved mucus clearance (81%), and improved mental health (64%) among others. Compared with other treatments, 84% found that ELX-TEZ-IVA is better at improving lung function, 80% noted that it results in fewer pulmonary exacerbations, and 68% found that it is better at improving nutritional status.
My life post Trikafta is not even comparable to before. I haven’t been hospitalized or on antibiotics in over 2 years. I can work and contribute to society like a normal human. – Adult with CF
I have more energy and I am not so fatigued all the time. I barely cough or spit up mucous. I am able to do more activities and not run out of breath so quickly. My appetite has gone up and weight gain has been way easier. – Adult with CF
I did lung transplant work up. I got Trikafta under compassionate care. My lung function increased by 13%. I no longer cough, have gained 25 pounds and have a new quality of life. Put it this way I wasn’t able to walk up a flight of stairs pre-Trikafta I am now bike riding.” – Adult with CF
Seventy-nine percent of parents of children with CF who are 12 years of age or older said that their child’s experience with ELX-TEZ-IVA was very positive, and 21% said it was positive. When compared to other therapies, adult caregivers of children with CF noted that ELX-TEZ-IVA better manages improvements in lung function (93%), improvements in nutritional status (64%), and reductions in rate of pulmonary exacerbations (57%).
My son has never enjoyed better health than he has since accessing this drug. His chronic intestinal issues have cleared up (within days) and he had the longest period in his life without antibiotics. He’s gained weight and height at a rapid rate. He looks healthy.” - Parent of a child with CF
In both the adult and child populations, a number of respondents noted improved sleep and better mental health.
Almost 80% of adults and 92% of caregivers of children with CF reported ELX-TEZ-IVA to be easier to take than other medications, as it was only 3 pills and is taken twice a day. Most respondents noted that the burden of care associated with CF lessens with ELX-TEZ-IVA. After taking ELX-TEZ-IVA, adults with CF spent a median of 10 hours a week on disease management, whereas their caregivers spent a median of 4 hours. Many caregivers of adults with CF reported that treatment with ELX-TEZ-IVA reduced the number of hours spent per week on caregiving activities. The change in burden on caregivers of children was less significant.
The survey also found that 60% of adult respondents who are taking ELX-TEZ-IVA noted the drug has helped them reduce the number of medications they take, including but not limited to inhaled antibiotics (63%), chest therapies (48%), anti-inflammatories (30%), antifungals (26%), and antivirals (22%). Twenty-five percent of respondents said that their child has reduced the number of medications they take since starting ELX-TEZ-IVA (e.g., inhaled antibiotics [67%], chest therapies [33%], and antivirals [33%]).
CF Canada reported that approximately 50% of adults had experienced adverse effects, including but not limited to headache (38%), abdominal pain (29%), rash (21%), diarrhea (17%) nasal congestion (17%), runny nose (17%), and elevated liver enzymes (13%). Almost 30% of children who are taking ELX-TEZ-IVA experienced adverse effects such as headache (25%), elevated liver enzymes (50%), and rash (25%). Adult respondents and adult caregivers of children with CF found all the adverse effects associated with ELX-TEZ-IVA to be acceptable. Cataracts were the least acceptable, with only 2% of adult respondents finding them to be acceptable.
Almost 80% of adult respondents with CF and caregivers of children with CF who were not on ELX-TEZ-IVA said that there is a gap or unmet need in current therapies that ELX-TEZ-IVA could alleviate. In particular, it would give some adult respondents a more efficacious option than other CFTR modulators (61% to 63%), it could be of benefit to those who fail treatment on another CFTR modulator (37%), it would provide a treatment option for patients with specific CFTR mutations that other CFTR modulators are not indicated to treat (35% to 46%), and it would give some choice among the different CFTR modulators (35% to 41%).
Additional Information
The patient groups who provided input for this review feel that Canada has fallen behind other countries in terms of access to CFTR modulators, including the drug under review. Three other CFTR modulators have received Notices of Compliance from Health Canada over the past 8 years, but they remain widely inaccessible for most Canadians with CF, except for 1 drug that most, but not all, who may benefit from it are able to access in several provinces.
One of the biggest complaints from the patient side is requiring us to be “sick enough” to qualify for a drug. Preventive medicine is important. – Adult with CF
Unmet needs include the fact that right now my child cannot access any modulators, and preventive therapies currently are not taking away the progression of her disease. Quality of life is hugely impacted and lessened, having no modulator to improve her overall health and help her body be protected from other illnesses. – CF parent
I worry constantly. Knowing medication may be available that could better her life but she may not be able to access it is very stressful. – CF spouse
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). In addition, as part of the ELX-TEZ-IVA review, a panel of 5 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations where there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion is presented below.
Unmet Needs
There are significant unmet therapeutic needs for patients living with CF. There are no treatments currently available that can effectively achieve the most important goals of therapy: prolong survival, prevent the need for lung transplantation, prevent an accelerated decline in lung function over time, or reverse the course of the disease. In addition, the current standard treatments are burdensome for patients and their caregivers. Patients may not respond or may stop responding over time to the currently available treatments.
Place In Therapy
ELX-TEZ-IVA is a CFTR modulator that functions by increasing the amount of CFTR protein at the cell surface (ELX and TEZ) and by improving the transport of chloride through the CFTR protein (IVA). The mechanism of action for ELX-TEZ-IVA is attractive because it acts directly on the CFTR protein to address the defects that are responsible for the CF phenotype. ELX-TEZ-IVA would be added to existing treatments such as physiotherapy, mucolytics, antiinfectives, and anti-inflammatory treatments (such as azithromycin). The clinical experts noted that the magnitude of improvement with ELX-TEZ-IVA is far greater than any other currently available treatments for CF (including all other CFTR modulators). ELX-TEZ-IVA would replace earlier CFTR modulators that are significantly less effective (e.g., Orkambi and Symdeko) and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA.
It is anticipated that ELX-TEZ-IVA would be used as a preventive therapy with the goal of initiating treatment before the patient develops significant lung disease. The current treatment paradigm would be significantly altered if ELX-TEZ-IVA can successfully prevent or delay progression to end organ disease.
Patient Population
The diagnosis of CF is not challenging in routine clinical practice. All provinces and territories have instituted newborn screening for CF, so most people with CF are now identified via newborn screening and have a confirmed diagnosis by 1 month of age (on average). Sweat chloride testing is available and reliably used to confirm the screening test. The provinces and territories have slightly different testing algorithms and CFTR mutation screening panels; however, all provinces and territories have effective processes. Almost 100% of newly diagnosed infants would have both CFTR mutations identified. Infants who are not identified via newborn screening (i.e., false negatives), are usually diagnosed before 1 year of age after the development of clinical symptoms of CF. There are clear diagnostic guidelines and very little variability in expert opinion. Misdiagnosis and underdiagnosis of CF is exceedingly rare in Canadian clinical practice.
ELX-TEZ-IVA could be used in every patient who meets the Health Canada–approved indication, regardless of their current or past treatment regimens. From a medical perspective, there is no rationale for a patient to demonstrate an inadequate or loss of response to prior therapies. However, from an economic perspective, it might be useful for payers to insist that patients try other treatments (e.g., inhaled antibiotics, mucolytics, anti-inflammatories, and/or chest physiotherapy) before the initiation of ELX-TEZ-IVA. It would be reasonable to require patients to complete important standard CF therapies at the same time as receiving treatment with ELX-TEZ-IVA. In clinical practice, eligible patients would be identified based on their CFTR genotype; however, there is no practical method that could be used to predict who will be most likely to respond to ELX-TEZ-IVA.
The patients with CF who are most likely to respond to treatment with ELX-TEZ-IVA are those who are homozygous or heterozygous for the F508del mutation in the CFTR gene. The patients who are most in need of treatment with ELX-TEZ-IVA include: patients with moderate to severe lung disease (e.g., ppFEV1 ≤ 60%), patients whose BMI is less than or equal to 20 kg/m2, patients with frequent pulmonary exacerbations, and those experiencing a rapid decline in FEV1. However, it could be argued that all patients, including those with mild lung disease, could benefit from treatment when considering the long-term outcomes and goal of prevention of severe outcomes. Given the mechanism of action of the drug under review, pre-symptomatic patients should be considered for treatment.
Assessing Response to Treatment
The following end points are routinely assessed in Canadian clinical practice: FEV1, nutrition and growth (e.g., BMI or BMI z score), hospital admissions and outpatient treatments for pulmonary exacerbations, and pulmonary exacerbation frequency per year. In addition, CF-related quality of life scales can be applied in clinical practice.
The magnitude of improvement in CF outcomes that would be considered clinically significant depends on the baseline status of the patient. For ppFEV1, an improvement in ppFEV1 of greater than or equal to 5% would typically be considered clinically meaningful for most patients in Canadian clinical practice. Those with a high baseline FEV1 (e.g., younger patients) may see much smaller improvements from baseline. Similarly, patients with advanced lung disease may see smaller improvements from baseline, but even stabilization in such patients can be clinically important. FEV1 is routinely assessed in the target population and the experts noted that evaluations could be performed 3 to 4 times per year.
The experts noted that an increase in BMI should only be viewed as a goal of therapy if the patient is malnourished. Increasing the BMI of a patient who is in the normal range or overweight may pose challenges and should not be viewed as a desirable outcome for evaluating the response to a treatment such as ELX-TEZ-IVA. For those who are malnourished, the goal of treatment would be to bring BMI up into the target range and keep it there.
Pulmonary exacerbations are important clinical events for patients with CF and are associated with long-term declines in lung function. The experts noted that the following could be considered clinically relevant with respect to pulmonary exacerbations for typical patients: a decrease in exacerbation frequency by 20% or more; or a reduction of 1 hospital admission for a pulmonary exacerbation. For assessing changes in the frequency of pulmonary exacerbations, a yearly assessment would provide the most relevant data. The clinical experts noted that younger patients typically have fewer pulmonary exacerbations, and it may be possible to demonstrate improvements from baseline in these patients.
The clinical experts noted that sweat chloride testing should be not used to evaluate the response to ELX-TEZ-IVA for the purposes of drug reimbursement.
Discontinuing Treatment
Treatment with ELX-TEZ-IVA would most likely be interrupted or discontinued because of AEs or progression to lung transplant. The most likely known AE that would result in discontinuation would be development of persistent liver enzyme abnormalities. Generally, if liver enzymes are significantly elevated (ALT or AST > 5 × upper limit of normal [ULN]), a reasonable approach would be to stop the treatment and monitor and consider a re-trial of treatment once liver enzymes normalize. If liver enzymes become abnormal again, a decision to discontinue treatment may occur, if the risk of liver enzyme abnormalities outweighs benefit of treatment.
The progression of CF toward end-stage lung disease would not be an indication to discontinue treatment in most cases nor would the need to initiate additional CF therapies because of disease progression. The clinical experts noted that ELX-TEZ-IVA is unlikely to be initiated or continued in patients who have received a lung transplant.
Prescribing Conditions
The only appropriate setting for initiation and monitoring of treatment with ELX-TEZ-IVA is an adult or pediatric CF clinic. This treatment will typically be initiated and monitored in the outpatient clinic setting by a CF physician and the associated multi-disciplinary team (e.g., specialists in respirology, infectious diseases, and gastroenterology). The experts noted that the drug may also be initiated in hospital. It would not be appropriate that ELX-TEZ-IVA would be prescribed and monitored in a non-specialty setting or by a non-specialty physician.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
Three groups of clinicians responded to CADTH’s call for input: CCFCD, CF Canada’s Accelerating Clinical Trials Network, and the Toronto Adult CF Clinic.
The CCFCD noted that there are 42 CF clinics in Canada which deliver a multi-disciplinary specialty care to individuals living with CF. The input from CCFCD notes that each clinic has a physician who serves as the medical director of the clinic. These clinic directors have special training, expertise, and experience in delivering medical care and support to those living with CF. The CCFCD gathered information for their input through personal experience gained by working with and delivering medical services to people with CF, treating people with CF who received ELX-TEZ-IVA through either clinical trials or Health Canada’s SAP. The CCFCD also noted that they conducted a review of the medical and scientific literature and reviewed the CCFR, which is a collection of patient data and other information regarding CF care and outcomes.
CF Canada’s Accelerating Clinical Trials Network (also called CF CanACT) Executive Committee operates under the auspices of CF Canada. Its purposes are to conduct clinical trials in CF and to attract research for new therapies to Canada. The physicians contributing to the input are also clinic directors of 14 clinics serving 60% of the CF population in Canada. They gathered information through the Canadian CF Registry which contains individual patient information on people living with CF, through outcomes of patients who have participated in clinical trials within the network, scientific publications, and personal experience from treating individuals with CF.
The Toronto Adult CF Clinic provides care to adult patients with CF and consists of 5 academic CF respirologists working alongside a multi-disciplinary team including specialized CF pharmacies. Their input reflects a review of published literature on CFTR modulators, clinical guidelines, and their clinical expertise. They also reviewed the outcomes of the 50 patients in their clinic who are receiving ELX-TEZ-IVA through SAP or compassionate access. The group also gathered information from the CF Canada’s CCFR.
Unmet Needs
All 3 clinician groups noted that CF is the most common fatal, genetic disease in the Canadian population and that it affects approximately 4,300 Canadians with an incidence of approximately 1 in 3,600. The clinician groups also noted that CF is a lifelong, chronic, degenerative disease that affects multiple organ systems, most importantly the lungs and digestive system.
All 3 clinician groups noted that mutations in the CF gene cause abnormalities in the CFTR protein which is responsible for the hydration of mucus secretions in the body. As a result, mucus builds up and harbours bacteria leading to chronic infections. Treatments are lifelong and to date the clinicians note that there is no cure for CF. The Toronto Adult CF Clinic noted that the available treatments are either those that treat the consequences of accumulation of the mucus or that aim to address the underlying defects of the CFTR protein. The therapies that treat the downstream consequences of CF in the lungs include chest physiotherapy and exercise to promote clearance of mucus from the airways, inhaled mucolytics, inhaled antibiotics, anti-inflammatory agents (inhaled and oral), inhaled bronchodilators, and in patients with severe lung disease, supplemental oxygen, and non-invasive ventilation. The CCFCD notes that there is a disparity in the availability of CFTR modulators which has Canadian clinicians concerned.
CF CanACT noted that as survival improves, the main cause of morbidity and mortality is lung damage due to a cycle of infection, inflammation, and lung destruction. The daily chest physiotherapy, inhaled mucolytics (e.g., hypertonic saline or dornase alfa) and chronic suppressive inhaled antibiotic therapy (e.g., tobramycin or aztreonam) were noted to improve survival as this strategy aims to slow the evolving lung damage and the resultant decline in lung function that ultimately leads to respiratory failure and death.
The groups noted that CF treatment also focuses on optimizing growth and nutrition and patients require additional pancreatic enzyme supplementation with fat-soluble vitamin supplementation which promote good nutrition and is critically linked to survival. Those living with CF are prescribed treatments which include high calorie, high fat, and high protein diets, medications, and airway clearance treatments. These treatments are initiated at the time of diagnosis and then continued throughout the patient’s life.
In addition, CCFCD noted that there are several classes of medications required for comprehensive treatment, including acute and chronic antibiotic therapies, mucolytics, bronchodilators, pancreatic enzymes, fat-soluble vitamin supplementation, insulin for people with CF-related diabetes, ursodiol for liver disease, and others. CCFCD added that physiotherapy (airway clearance) treatments are prescribed once to several times a day. They noted that most people with CF spend at least 1 or 2 hours a day on treatments and this time increases as the severity of the disease increases. Routine medical visits to the CF clinic every 3 months are recommended and the clinicians note that additional visits may be required due to illness or closer monitoring of progressing symptoms, severe disease, or pre- and post-transplant care. Hospitalizations and home IV treatments may be required for these patients as well. CCFCD added that the indirect costs to patients include lost days of work and school, travel costs, risk of employment insecurity, and decreased lifetime earning potential, non-insured personal medical expenses, and reduced participation in creative and leisure activities.
All 3 clinician inputs noted that lung transplant is required for end-stage respiratory failure and is a treatment for end-stage pulmonary disease. However, CCFCD noted that lung transplant comes with risk factors and additional treatment burden and does not address CF disease in other organ systems. The median length of survival after lung transplant was noted as 10.6 years as reported in the 2019 Registry report, indicating that it is not a cure and comes with considerable medical costs. CCFCD added that lung transplantation is only offered at 4 centres in Canada and relocating to these is required during the transplant process. These are Toronto, Montreal, Edmonton, or Vancouver.
CCFCD added that most of the current CF treatments treat the symptoms, attempt to slow down the progression of the disease, and treat acute exacerbations such as acute pulmonary infections. All 3 clinician inputs noted that CFTR modulators are medications that work on the various defects of the CFTR protein. Although not a cure, CF CanACT adds that these treatments aim to restore the function of the CFTR protein at the cell surface. The first modulator available was IVA and was effective in patients who have “gating” mutations (approximately 4% of the Canadian population). Additionally, CF CanACT noted that IVA is an extremely effective medication, restoring CFTR function with clinical benefits of increasing lung function, reducing hospitalizations, improving nutritional status, decreasing need for lung transplant, and improving survival. The Toronto Adult CF Clinic added that IVA is a potentiator and that correctors such as TEZ and LUM fix the folding defect in the CFTR protein and in combination with IVA are used to correct the protein defect seen in patients with F508del mutation. CF CanACT noted that the F508del mutation is seen in approximately 50% of Canadian patients with CF and for patients with 2 copies of the most common CF mutation, LUM-IVA and TEZ-IVA have been developed; however, these medications are not available provincially and consequently only 12% of Canadian patients with CF receive these through participation in clinical trials or third-party payers. CCFCD agreed with CF CanACT that IVA was recommended for provincial reimbursement and is generally available for qualifying patients, but access to the other mildly effective CFTR modifier medications is limited to participation in clinical trials, private insurance coverage, or very limited special provincial programs.
All 3 clinician groups noted that the most important treatment goals are to cure CF and prevent multisystem, progressive disease manifestations. However, treatments that address the basic defect and restore normal chloride transport are still a decade away. CFTR modulators are noted to provide a therapy that is as close to a cure as the CF realm has seen. The clinicians note that CFTR modulators do not correct the genetic defect but are able to correct defects in the protein structure. The most important goals of therapy are noted by the clinicians groups as follows: increasing life expectancy, preventing development of lung disease, delaying disease progression for people with established disease, improving lung function for people with established disease, reducing frequency of pulmonary exacerbations and avoiding need for admission to hospital, reducing need for lung transplantation, improving quality of life, improving nutrition and growth, reducing psychosocial issues, allowing attendance at school, university, and work, reducing burden of care and number of therapies to maintain care, and altering the disease trajectory.
All 3 clinician inputs agreed that CFTR modulator therapy is the only available treatment that treats the basic defect in CF. These treatments only treat the symptoms and complications of CF and attempt to slow down the progression of the disease. Treatments such as inhaled antibiotics and mucus-thinning agents target downstream consequences of CF lung disease and do not treat the underlying cause of the disease. CF CanACT noted that most patients eventually become refractory to inhaled antibiotics due to the development of antibiotic resistance which leads to more frequent infectious pulmonary exacerbations and eventually lung transplantation.
All 3 clinician groups noted that patients with 2 copies of F508del have a substantial unmet need as only a small minority have been able to access the LUM-IVA or TEZ-IVA combinations. In addition, response is variable and side effects can be considerable. CF CanACT notes that the drug under review will add improvements beyond the effects of LUM-IVA or TEZ-IVA combinations. CF CanACT also notes that patients with very mild or early disease have a great unmet need as current treatments do not reverse the course of disease or prevent end organ damage. The initiation of CFTR modulator therapy before irreversible damage occurs to the lungs, pancreas, and other affected organs should be a primary goal to prevent sequelae and reduce the need of other lifelong treatments such as inhaled antibiotics, inhaled mucolytics, pancreatic enzymes, and insulin which add significant treatment burden and impact quality of life.
CCFCD adds that the development of a highly effective CFTR modifier such as ELX-TEZ-IVA fills a niche in CF care where patients do not have access to another effective treatment. The group also adds that the current review is for patients aged 12 and older. If the clinical trials under way are positive, the group is hopeful that this population will be reviewed. CCFCD added that it is unclear if patients with CF with lung transplant will have non-pulmonary benefits from this medication.
The Toronto Adult CF Clinic added that triple combination therapy with 2 correctors offers a significant response in patients who have at least 1 F508del mutation, thereby providing significant clinical benefit to 90% of Canadians with CF.
All 3 clinician groups noted that patients with a single copy of the F508del paired with another CF mutation (F508del heterozygous) that is not a gating or RF mutation have the greatest unmet need as there are currently no approved CFTR modulator therapies for this population. In patients with single copy F508del and an MF mutation, clinical manifestations are severe and the drug under review is considered a breakthrough as it leads to substantial improvements in lung function and respiratory-related quality of life and markedly reduces exacerbations and hospitalization. The clinicians added that patients with 2 copies of the F508del also have substantial unmet need as only a small minority (< 12%) have been able to access the LUM-IVA or TEZ-IVA treatments; the response to these treatments is variable and often with considerable side effects. Patients with mild or early disease are noted by the clinicians as a group with an unmet need as currently available treatments do not reverse the course of the disease. Initiation of the CFTR modulator therapy before irreversible damage occurs to the organs should be a primary goal.
Place in Therapy
All 3 clinician groups note that ELX-TEZ-IVA addresses the underlying disease process and would be added to the current standard of care for CF as a first-line therapy for those patients with the appropriate CF mutations (i.e., at least 1 F508del mutation in the CFTR gene). ELX-TEZ-IVA should be added to the standard of care regardless of treatment response as it is the only therapy that targets the defect in the CFTR protein. CF CanACT noted that it would be beneficial for eligible patients who are receiving treatment with IVA, TEZ-IVA, or LUM-IVA to switch to ELX-TEZ-IVA. The Toronto Adult CF Clinic noted that there are trials under way to test which downstream therapies may be discontinued in patients on ELX-TEZ-IVA but at this point, all standard of care treatments should be continued.
The clinician groups who provided input to CADTH agreed that ELX-TEZ-IVA is not the first therapy that addresses the underlying defect of CF, rather it is an improvement on the existing CFTR modulators and is indicated for a broader CF population. CF CanACT added that the addition of ELX-TEZ-IVA would hopefully delay disease progression and thus delay the need for other therapies including lung transplant. This improvement in clinical status may lead to other standard or care treatments no longer being required.
Patient Population
All 3 clinician groups agreed that patients with CF who have at least 1 copy of the F508del mutation and are aged 12 years or older would be best suited for treatment with ELX-TEZ-IVA. The groups added that younger patients generally have less severe lung disease but can benefit from a reduction in pulmonary exacerbations which will impact the rate of lung function decline. The Toronto Adult CF Clinic added that clinical trials were conducted in adolescents and adults as well as those with mild and more severe lung disease and all subgroups responded to ELX-TEZ-IVA. The group added that patients with severe lung disease (ppFEV1 < 40%) who received ELX-TEZ-IVA through SAP or compassionate access seem to have a meaningful clinical response. The CCFCD input added that in patients with FEV1 greater than 90%, there are often early signs of CF lung disease present, such as bronchiectasis, mucus plugging, or early mild declines in FEV1% which could benefit from treatment with ELX-TEZ-IVA. CF CanACT noted that all subgroups responded to ELX-TEZ-IVA in the phase III trials.
All 3 clinician groups added that eligible patients would be identified by their CF physician. Newborn screening for CF is now available across Canada and allows for early referral to CF clinics as well as confirmation of the diagnosis of CF and initiation of therapy often before the development of symptoms. The clinicians noted that genetic testing is done at the time of diagnosis and this would determine eligibility for CFTR modulator therapy. CF CanACT also added that there should be no lower limit of lung function to be eligible for treatment with ELX-TEZ-IVA. They cited that many patients with lung function less than 40% who were waiting for lung transplantation improved with ELX-TEZ-IVA to the point where they are no longer required transplantation.
All 3 clinician groups noted that any patient who does not have a CFTR mutation genotype that would respond to the medication or persons with a known allergy or other adverse reaction to this or a similar medication would not be suitable for this medication. The Toronto Adult CF Clinic added that patients with severe liver disease (Child-Pugh Class C) should not be started on ELX-TEZ-IVA. The groups also noted that it is not yet clear if ELX-TEZ-IVA would benefit patients with CF who have had a lung transplant.
The clinician groups also noted that patients who are most likely to exhibit a response to treatment with ELX-TEZ-IVA would be identified by their CF clinic care provider based on having an eligible CFTR genotype and no contraindications to this therapy. The CF CanACT added that the clinical trials have demonstrated that those patients with at least 1 F508del mutation, regardless of the second mutation, respond to this therapy, as noted by improvements in lung function, weight, and reduced pulmonary exacerbations requiring antibiotics. The Toronto Adult CF Clinic added that there is no way to predict which patients would respond to ELX-TEZ-IVA without a trial of therapy.
Assessing Response to Treatment
All 3 clinician groups noted that the outcomes used to determine whether a patient is responding to treatment in clinical practice are the same as those used in clinical trials. The outcomes are measured at every CF clinic visit and documented in the CCFR. The outcomes include FEV1, weight, frequency of pulmonary exacerbations, hospitalizations, and lung transplantation. CF CanACT noted that at each clinic visit, patients have spirometry to measure lung function, have their weight and height measured, and provide a sputum sample for culture. They group added that the assessment by the CF physician would review their respiratory and other CF symptoms and determine the presence of pulmonary exacerbations at or between clinic visits; therefore, additional visits or testing are not required to assess response to therapy with CFTR modulators.
According to all the clinician groups, clinically meaningful response to treatment would be improvements in pulmonary function testing, weight and nutritional status, and quality of life. The groups noted that improvement in lung function, stabilization of lung function over time (i.e., prevention of the usual decline in lung function), reduction in the number of pulmonary exacerbations, reduction or stabilization of respiratory symptoms, improvement in nutritional status, and improvement in quality of life. The Toronto Adult CF Clinic added that in CF, the minimal important difference (MID) for these outcomes has not been determined; however, in this progressive disease, it is more important to demonstrate that therapies can prevent deterioration rather than just showing short-term improvements in lung function.
CCFCD noted that because of the routine clinic visits at 3-month intervals, treatment response is assessed frequently. For TEZ-IVA or LUM-IVA, a visit at 1 month after the start of therapy was also commonly used to assess for early response and potential side effects. The Toronto Adult CF Clinic noted that quarterly clinic visits are standard of care in CF and that is an appropriate frequency to assess response to CFTR modulator therapy. The clinicians from the Toronto Adult CF Clinic added that they would recommend blood work after 1 month on ELX-TEZ-IVA and every 3 months for the first year to ensure no derangements in liver function. CF CanACT added that treatment response time intervals depend on the outcome measure used. As such, they noted that improvement in lung function, stabilization of lung function over time, reduction or stabilization of respiratory symptoms, and improvement in nutritional status should be assessed in the first 3 months of therapy, every 3 to 6 months in the first year of treatment and on a yearly basis subsequently. Changes in quality of life scores should be assessed on a yearly basis.
Discontinuing Treatment
All 3 clinician groups noted that discontinuation of therapy should be considered in patients who have clinically significant adverse effects that persist and recur after stopping and re-initiating therapy. Additionally, the groups added that treatment should be discontinued if there are allergies or the development of signs of worsening liver disease. The treatment should also be discontinued if there are drug-drug interactions with medications such as rifampin or antiseizure medications.
Prescribing Conditions
Treatment of patients with CF with ELX-TEZ-IVA should be limited to CF specialists practising at CF clinics certified by CF Canada.
Additional Considerations
Clinician groups added that the impact of ELX-TEZ-IVA has been dramatic and life-altering for the patients who have received the treatment through SAP, compassionate access, or in clinical trials.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Should prescribing be limited to physicians with expertise in the management of CF? | The only setting appropriate for assessment of patients for appropriateness for this treatment, initiation of treatment, and monitoring of treatment is in an adult or pediatric CF clinic. |
What clinical outcome measures should be used to assess therapeutic response to treatment with ELX-TEZ-IVA? | The following end points have been suggested for adult patients:
|
What magnitude of improvement would be clinically significant for ppFEV1? What would be the appropriate intervals for evaluating response to treatment? | For typical patients in Canadian practice, an improvement in ppFEV1 of ≥ 5% would typically be considered clinically meaningful. However, the magnitude of improvement in ppFEV1 that would be considered clinically significant depends on the baseline status of the patient. Those with a very low ppFEV1 may see smaller improvements from baseline, but even stabilization in such patients can be clinically important. ppFEV1 is routinely assessed in the target population and the experts noted that evaluations could be performed 3 to 4 times per year. |
What magnitude of improvement would be clinically significant for BMI? What would be the appropriate intervals for evaluating response to treatment based on BMI? | The experts noted that increases in BMI should only be viewed as a marker of improvement in patients who are malnourished. For those patients, the goal of therapy is to increase BMI into the normal range. |
Should therapeutic response be assessed using different criteria for patients who are naive to CFTR modulator therapy compared with those who are switching from a different CFTR modulator to ELX-TEZ-IVA? | The magnitude of improvement with ELX-TEZ-IVA is far greater than any other currently available treatments for CF (including all other CFTR modulators). ELX-TEZ-IVA would replace earlier CFTR modulators that are significantly less effective (e.g., Orkambi and Symdeko) and patients currently receiving those drugs would likely be switched to ELX-TEZ-IVA. |
The product monograph indicates that patients with severe hepatic impairment should not be treated with ELX-TEZ-IVA. Would these recommendations be followed in clinical practice? | The clinical experts consulted by CADTH suggested that clinicians may attempt to treat those with severe hepatic impairment using ELX-TEZ-IVA at a reduced dosage, as opposed to using the reduced dosages of the alternative CFTR modulators, which are unlikely to provide the same level of clinical benefit. It was noted that therapeutic trials should be considered for all patients when the potential for benefit exceeds the risk. |
Patients with ppFEV1 < 40% at screening were excluded from the pivotal and supportive phase III trials. Is there evidence to suggest that these patients would benefit from treatment with ELX-TEZ-IVA? | Subgroup data from Study 102 and 2 observational studies included in the CADTH review provided short-term data on the efficacy and safety of ELX-TEZ-IVA in patients with CF and who had advanced pulmonary disease. These studies suggested that treatment with ELX-TEZ-IVA resulted in a clinically meaningful improvement in ppFEV1 for patients who had a baseline ppFEV1 < 40%. The clinical experts consulted by CADTH, the clinician groups who provided input, and the patient groups who provided input have all noted anecdotal evidence, based on clinical experience, that ELX-TEZ-IVA is beneficial for those with advanced lung disease. |
Patients with ppFEV1 > 90% at screening were excluded from the pivotal and supportive phase III trials. Is there evidence to suggest that these patients would benefit from treatment with ELX-TEZ-IVA? | The clinical experts noted that these patients may benefit from treatment with ELX-TEZ-IVA. However, prioritization should be for those patients with more significant disease burden. |
What clinical criteria could be used to identify patients with rapidly progressive disease? | The clinical experts noted that there are no currently accepted definitions for patients with rapidly progressive disease. |
What clinical criteria could be used to determine if patients are non-responders to treatment with ELX-TEZ-IVA (i.e., potential discontinuation criteria)? | Based on the available evidence, non-responders to ELX-TEZ-IVA are likely to be rare. The primary reasons for discontinuing treatment are likely to be related to adverse events (e.g., abnormal liver function tests, rash, or excessive weight gain). |
BMI = body mass index; CF = cystic fibrosis; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; FEV1 = forced expiratory volume in 1 second; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor.
Clinical Evidence
The clinical evidence included in the review of ELX-TEZ-IVA is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of ELX-TEZ -IVA for the treatment of patients aged 12 years and older with CF and who have at least 1 F508del mutation in the CFTR gene.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients aged ≥ 12 years with CF and who have at least 1 F508del mutation in the CFTR gene. Subgroups:
|
Intervention | ELX 100 mg, TEZ 50 mg, IVA 75 mg (morning) + IVA 150 mg (evening) |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and 4 RCTs |
CF = cystic fibrosis; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; FEV1 = forced expiratory volume in 1 second; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for the F508del mutation with 1 minimal function mutation; F/RF = heterozygous for the F508del mutation with a residual function mutation; IVA = ivacaftor; LUM = lumacaftor; RCT = randomized controlled trial; TEZ = tezacaftor.
Note: Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).39 Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was Trikafta (ELX-TEZ-IVA). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on February 22, 2021. Regular alerts updated the search until the meeting of CDEC on June 16, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).40 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 127 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
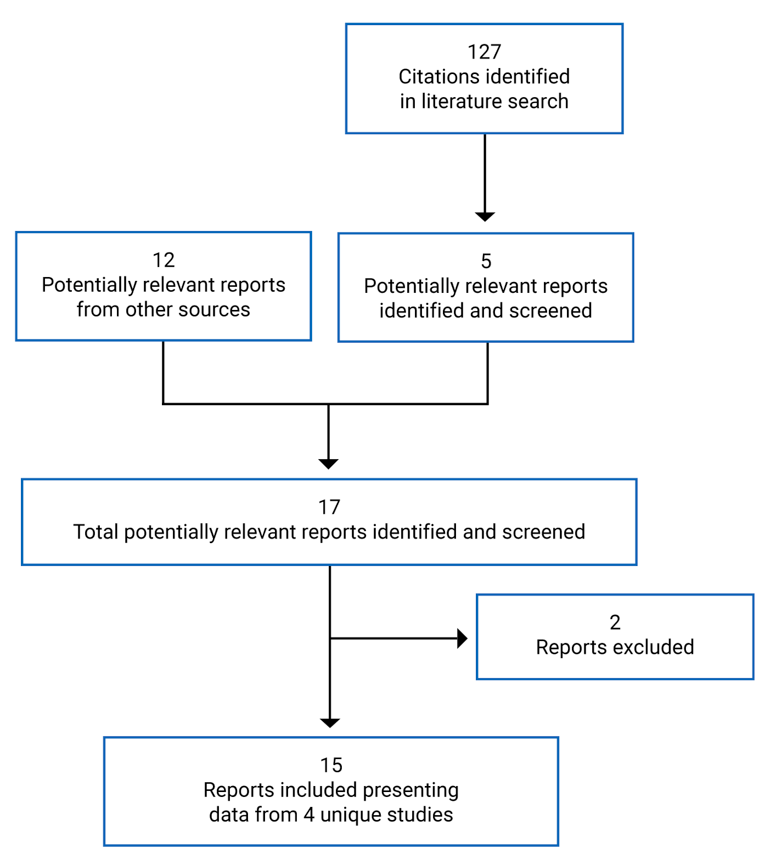
Table 7: Details of Included Studies
Parameters | Study 102 (F/MF) | Study 103 (F/F) | Study 104 (F/RF, F/G) | Study 109 (F/F) |
|---|---|---|---|---|
Designs and populations | ||||
Study design | Phase III, DB, parallel group, placebo-controlled RCT | Phase III, DB, parallel-arm, active-controlled superiority, RCT | Phase III, DB, parallel-arm, active-controlled, superiority, RCT | Phase IIIb, DB, parallel-arm, active-controlled, RCT |
Locations | 110 sites; 13 countries: Australia, Austria, Belgium, Canada, Czech Republic, France, Germany, Greece, Italy, Netherlands, Sweden, UK, US | 44 sites; 4 countries: Belgium, Netherlands, UK, US | 96 sites; 11 countries: Australia, Belgium, Canada, France, Germany, Ireland, Italy, Spain, Netherlands, UK, US | 35 sites; 4 countries: UK, Germany, Belgium, and Australia |
Patient enrolment dates | First patient enrolled: June 15, 2018 Last study visit: April 14, 2019 | First patient enrolled: August 2018 Last study visit: December 28, 2018 | First patient enrolled: August 28, 2019 Last study visit: June 12, 2020 | First patient enrolled: Study initiation: October 3, 2019 Last study visit: July 24, 2020 |
Randomized (N) | 405
| 107
| 259
| 107
|
Inclusion criteria |
|
|
|
|
Exclusion criteria |
| |||
Drugs | ||||
Intervention | ELX 200 mg, TEZ 100 mg, IVA 150 mg (every morning) + IVA 150 (every evening) | |||
Comparator(s) | Placebo | TEZ 100 mg, IVA 150 mg (every morning) + IVA 150 (every evening) | TEZ 100 mg, IVA 150 mg (every morning) + IVA 150 (every evening) IVA 150 mg (every morning) + IVA 150 (every evening) | TEZ 100 mg, IVA 150 mg (every morning) + IVA 150 mg (every evening) |
Duration | ||||
Phase | ||||
Screening | 28 days | 28 days | 28 days | 28 days |
Run-in | Not applicable | 28 days | 28 days | 28 days |
Double blind | 24 weeks | 4 weeks | 8 weeks | 8 weeks |
Follow-up | 28 days (or enter OLE) | 28 days (or enter OLE) | 28 days (or enter OLE) | 28 days (or enter OLE) |
Outcomes | ||||
Primary end point | Absolute change in ppFEV1 from baseline at week 4 | Absolute change in ppFEV1 from baseline at week 4 | Absolute change in ppFEV1 from baseline through week 8 | Absolute change in CFQ-R (RD) from baseline through week 24 |
Secondary and exploratory end points |
|
|
|
|
Notes | ||||
Publications | Middleton et al. (2019)41 Clinicaltrials.gov42 | Clinicaltrials.gov45 | Clinicaltrials.gov46 | Clinicaltrials.gov47 |
ALP = alkaline phosphatase; ALT = alanine transaminase; AST = aspartate transaminase; BMI = body mass index; CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; DB = double blind; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; GFR = glomerular filtration rate; GGT = gamma-glutamyl transferase; IV = IV; IVA = ivacaftor; OLE = open-label extension; PEx = pulmonary exacerbations; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; RD = respiratory domain; SwCl = sweat chloride; TEZ = tezacaftor; TSQM = Treatment Satisfaction Questionnaire for Medication; ULN = upper limit of normal.
Note: Eight additional reports were included: Clinical Study Reports,7-10 FDA Multi-Discipline Review,29 European Public Assessment Report,48 Common Technical Document,49 and the Sponsor’s Clinical Summary.50
Description of Studies
Table 8 provides an overview of the studies that were summarized and appraised by CADTH for the current review of ELX-TEZ-IVA. There were 4 double-blind, phase III, RCTs included in the CADTH systematic review: 1 placebo-controlled trial conducted in patients who were heterozygous for the F508del mutation and who had 1 MF mutation (Study 102); 2 active-controlled trials in patients who were homozygous for the F508del mutation (Study 103 and Study 109); and 1 active-controlled trial in patients who were heterozygous for the F508del mutation and a RF mutation or a gating mutation (Study 104).
CADTH also reviewed additional studies that did not meet the eligibility criteria of the systematic review but may address important gaps in the evidence from the pivotal and supportive RCTs. These included 1 long-term extension phase study (Study 105),2 1 indirect comparison filed by the sponsor,3 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease,4,5 and 1 study that modelled the potential impact of ELX-TEZ-IVA on morbidity and mortality.6
Population | Study name or author | Design | Duration | Status |
|---|---|---|---|---|
Studies Included in systematic review | ||||
F/MF | Study 1027 | Pivotal, phase III, DB, placebo-controlled RCT | 24 weeks | Complete |
F/F | Study 1038 | Pivotal, phase III, DB, active-controlled RCT | 4 weeks | Complete |
Study 10910 | phase III, DB, active-controlled RCT | 24 weeks | Complete | |
F/RF, F/G | Study 1049 | phase III, DB, active-controlled RCT | 8 weeks | Complete |
Long-term extension studies | ||||
F/F, F/MF | Study 1052 | Extension study of Studies 102 and 103 | Up to 96 weeks | Ongoing |
Indirect comparisons | ||||
F/F, F/G, F/RF | Sponsor’s indirect comparison3 | Bucher method indirect comparisons | 8 to 24 weeks | NA |
Studies in patients with advanced lung disease | ||||
F/F, F/MF | O’Shea et al. (2020)4 | Retrospective observational study | Approximately 5 months | Complete |
F/F, F/Othera | Burgel et al. (2020)5 | Prospective observational study | Approximately 3 months | Complete |
Study modelling impact on morbidity and mortality | ||||
F/Otherb | Stanojevic et al. (2020)6 | Microsimulation transition model using Canadian CF Registry data | Up to 2030 | NA |
CF = cystic fibrosis; DB = double blind; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; NA = not applicable; RCT = randomized controlled trial.
aGenotypes for patients who were heterozygous for the F508del mutation were not reported by Burgel et al. (2020).
bThe microsimulation was conducted based on patients with at least 1 F508del mutation with no separate analyses based on the genotype of patients.
Patients With F/MF Genotype
Study 102 was a pivotal, phase III, multi-national, parallel group, placebo-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are heterozygous for the F508del mutation and who have a MF mutation. Study 102 was conducted at 110 sites in 13 countries, including 6 sites in Canada (n = 24). As shown in Figure 2, Study 102 consisted of a 28-day screening period, a 24-week double-blind treatment period, and a 28-day follow-up period. Patients who completed the 24-week treatment period could enrol the open-label extension study (Study 105) or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA or a matching placebo. Randomization was conducted using an interactive web response system (IWRS) and stratified by ppFEV1 at screening (< 70% or ≥ 70%), age at screening (< 18 years or ≥ 18 years of age), and sex (male or female).
An interim efficacy analysis was planned after at least 140 patients completed the week 4 visit and at least 100 patients completed the week 12 visit. The interim analysis was performed by an external independent biostatistician who was not involved in the conduct of Study 102. The results of the interim analysis were reviewed by the independent data monitoring committee. If the independent data monitoring committee declared that Study 102 had crossed the pre-specified efficacy boundary, then the study could be unblinded by a limited team from the sponsor for the purposes of preparing a regulatory submission. Those who were unblinded were not to be involved in or influence the conduct of the remaining part of Study 102. All patients (and their parents, caregivers, and companions), site personnel (including the investigator, the site monitor, and the study team), and members of the sponsor’s study team remained blinded until the final database lock.
Figure 2: Schematic Showing the Design of Study 102
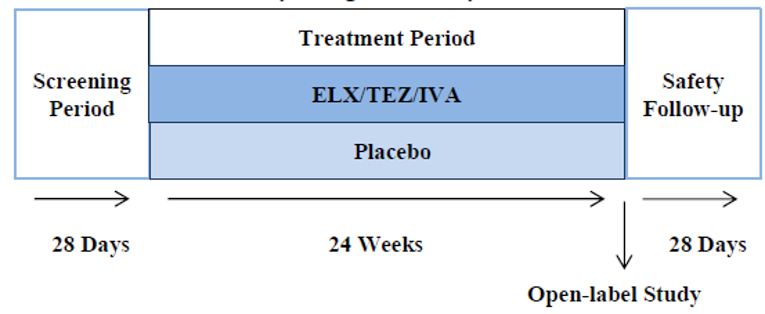
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor + ivacaftor.
Source: Common Technical Document section 2.7.3.49
Patients With F/F Genotype
Study 103 was a pivotal, phase III, multi-national, parallel group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are homozygous for the F508del mutation (F/F). The trial was conducted at 44 sites in 4 countries (Belgium, Netherlands, UK, and the US). As shown in Figure 3, Study 103 consisted of a 28-day screening period, a 28-day open-label run-in period where all patients received TEZ 100 mg and IVA 150 mg once daily in the morning and IVA 150 mg in the evening, a 4-week double-blind treatment period, and a 28-day follow-up period. Patients who completed the 4-week treatment period could enrol the open-label extension study (Study 105) or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA or to continue with TEZ 100 mg once daily and IVA every 12 hours. As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group were also administered a matching placebo tablet for the morning dosage to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening). Randomization was conducted using an IWRS and stratified by ppFEV1 at screening (< 70% or ≥ 70%) and age at screening (< 18 years or ≥ 18 years of age).
Figure 3: Schematic Showing the Design of Study 103
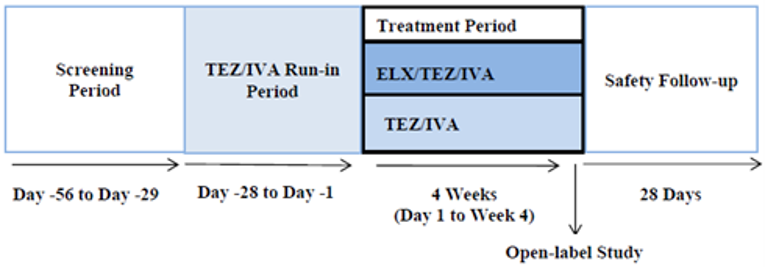
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor + ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Common Technical Document section 2.7.3.49
Study 109 was a phase IIIb, multi-national, parallel group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are homozygous for the F508del mutation (F/F). The trial was conducted at 35 sites in 4 countries (UK, Germany, Belgium, and Australia).10 As shown in Figure 4, Study 109 consisted of a 28-day screening period, a 28-day open-label run-in period where all patients received TEZ 100 mg once daily and IVA 150 mg every 12 hours (TEZ-IVA), a 24-week double-blind treatment period, and a 28-day follow-up period.10 Patients who completed the 24-week treatment period could enrol the open-label extension study (NCT04362761)51 or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA or to continue with TEZ-IVA.10 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group were also administered a matching placebo tablet for the morning dosage to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening).10 Randomization was stratified by ppFEV1 and ppFEV1 category (i.e., < 70% versus ≥ 70%) at day 14 of the TEZ-IVA run-in period; age at screening (< 18 versus ≥ 18 years of age), and whether the patient was receiving CFTR modulator treatment at screening (yes versus no).10
Figure 4: Schematic Showing the Design of Study 109
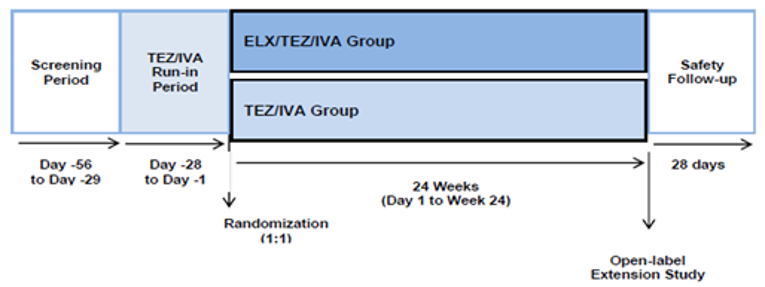
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor + ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Sponsor’s Clinical Summary.50
Patients With F/RF or F/G Genotype
Study 104 was a phase III, multi-national, parallel group, active-controlled, randomized trial conducted to investigate the efficacy and safety of ELX-TEZ-IVA in patients with CF who are heterozygous for the F508del mutation and a gating mutation (F/G) or a residual function mutation (F/RF).9 This study was conducted at 96 sites in 11 countries (Australia, Belgium, Canada, France, Germany, Ireland, Italy, Spain, the Netherlands, UK, and US).9 As shown in Figure 5, Study 104 consisted of a 28-day screening period, a 28-day open-label run-in period where all patients with an F/RF genotype received TEZ 100 mg once daily and IVA 150 mg every 12 hours (TEZ-IVA) and those with an F/G genotype received IVA 150 mg every 12 hours; there was a 4-week double-blind treatment period, and a 28-day follow-up period.9 Patients who completed the 4-week treatment period could enrol the open-label extension study (VX18 to 445 to 110)52 or enter the 28-day safety follow-up period. Eligible patients were randomized (1:1) to receive ELX-TEZ-IVA or to the control group who would continue with TEZ-IVA or IVA as per their genotype.9 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the control group (TEZ-IVA or IVA) also received a matching placebo tablet for the morning dosage to maintain blinding (i.e., both groups administered 2 tablets in the morning and 1 in the evening). Randomization was conducted using an IWRS and stratified by comparator group (IVA versus TEZ-IVA), ppFEV1 at day 14 visit, and sweat chloride at day 14 visit.9
Figure 5: Schematic Showing the Design of Study 104
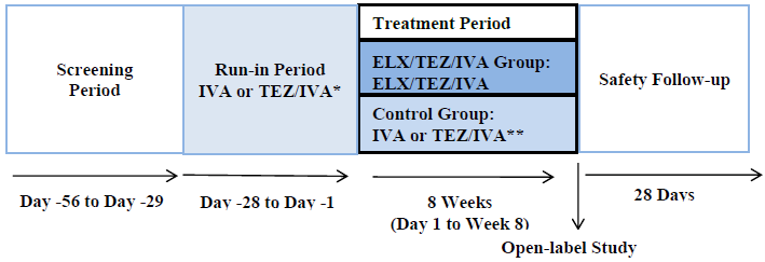
ELX/TEZ/IVA = elexacaftor-tezacaftor-ivacaftor + ivacaftor; IVA = ivacaftor; TEZ/IVA = tezacaftor-ivacaftor.
Source: Common Technical Document section 2.7.3.49
Populations
Inclusion and Exclusion Criteria
Patients With F/MF Genotype
Patients aged 12 years and older were eligible for inclusion in Study 102 if they were heterozygous for F508del and an MF mutation in the CFTR gene and had a confirmed diagnosis of CF (determined by the investigator).34 To be considered “MF” the mutation was required to meet at least 1 of the following criteria:
biologic plausibility of no translated CFTR protein (i.e., the genetic sequence predicts the complete absence of CFTR protein), or
in vitro testing that supports lack of responsiveness to TEZ, IVA, or TEZ-IVA, and evidence of clinical severity on a population basis.7
The mutations that were classified as MF mutations based on in vitro testing met the following criteria in the sponsor’s in vitro experiments: baseline chloride transport that was less than 10% of wild-type CFTR, and an increase in chloride transport of less than 10% over baseline following the addition of TEZ, IVA, or TEZ-IVA in the assay. Clinical severity on a population basis was determining using The Clinical and Functional Translation of CFTR (CFTR2)53 patient registry. Patients with these mutations on 1 allele and F508del on the other allele exhibited evidence of clinical severity as defined as: average sweat chloride greater than 86 mmol/L, and the prevalence of pancreatic insufficiency greater than 50%.7 The complete list of MF mutations are provided in Table 9.
Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of 40% or greater and 90% or less at the time of screening.7 The trials excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 4 weeks before first dose of study drug.34 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.34
Table 9: Minimal Function Mutations in Study 102
Criteria | Mutations | ||||
|---|---|---|---|---|---|
Truncation mutations
| Q2X | L218X | Q525X | R792X | E1104X |
S4X | Q220X | G542X | E822X | W1145X | |
W19X | Y275X | G550X | W882X | R1158X | |
G27X | C276X | Q552X | W846X | R1162X | |
Q39X | Q290X | R553X | Y849X | S1196X | |
W57X | G330X | E585X | R851X | W1204X | |
E60X | W401X | G673X | Q890X | L1254X | |
R75X | Q414X | Q685X | S912X | S1255X | |
L88X | S434X | R709X | Y913X | W1282X | |
E92X | S466X | K710X | Q1042X | Q1313X | |
Q98X | S489X | Q715X | W1089X | Q1330X | |
Y122X | Q493X | L732X | Y1092X | E1371X | |
E193X | W496X | R764X | W1098X | Q1382X | |
W216X | C524X | R785X | R1102X | Q1411X | |
Splice mutations
| 185 + 1G→T | 711 + 1G→T | 1525-1G→A | 1812-1G→A | 3120 + 1G→A |
296 + 1G→A | 711 + 5G→A | 1898 + 1G→C | 1898 + 1G→A | 3121-2A→G | |
296 + 1G→T | 712-1G→T | 1717-8G→A | 2622 + 1G→A | 3121-1G→A | |
405 + 1G→A | 1248 + 1G→A | 1717-1G→A | 2790-1G→C | 3500-2A→G | |
405 + 3A→C | 1249-1G→A | 1811 + 1G→C | 3040G→C (G970R) | 3600 + 2insT | |
406-1G→A | 1341 + 1G→A | 1811 + 1.6kbA→G | 3850-1G→A | 4005 + 1G→A | |
621 + 1G→T | 1525-2A→G | 1811 + 1643G→T | 3120G→A | 4374 + 1G→T | |
Small (≤ 3 nucleotide) insertion/deletion frameshift mutations
| 182delT | 1078delT | 1677delTA | 2711delT | 3737delA |
306insA | 1119delA | 1782delA | 2732insA | 3791delC | |
306delTAGA | 1138insG | 1824delA | 2869insG | 3821delT | |
365-366insT | 1154insTC | 1833delT | 2896insAG | 3876delA | |
394delTT | 1161delC | 2043delG | 2942insT | 3878delG | |
442delA | 1213delT | 2143delT | 2957delT | 3905insT | |
444delA | 1259insA | 2183AA→G | 3007delG | 4016insT | |
457TAT→G | 1288insTA | 2184delA | 3028delA | 4021dupT | |
541delC | 1343delG | 2184insA | 3171delC | 4022insT | |
574delA | 1471delA | 2307insA | 3171insC | 4040delA | |
663delT | 1497delGG | 2347delG | 3271delGG | 4279insA | |
849delG | 1548delG | 2585delT | 3349insT | 4326delTC | |
935delA | 1609delCA | 2594delGT | 3659delC | ||
Non-small (> 3 nucleotide) insertion/deletion frameshift mutations
| CFTRdele1 | CFTR50kbdel | CFTRdele17a-18 | 602del14 | 2372del8 |
CFTRdele2 | CFTRdup6b-10 | CFTRdele19 | 852del22 | 2721del11 | |
CFTRdele2,3 | CFTRdele11 | CFTRdele19-21 | 991del5 | 2991del32 | |
CFTRdele2-4 | CFTRdele13,14a | CFTRdele21 | 1461ins4 | 3121977_3499 + 248del2515 | |
CFTRdele3-10,14b-16 | CFTRdele14b-17b | CFTRdele22-24 | 1924del7 | 3667ins4 | |
CFTRdele4-7 | CFTRdele16-17b | CFTRdele22,23 | 2055del9→A | 4010del4 | |
CFTRdele4-11 | CFTRdele17a,17b | 124del23bp | 2105-2117 del13insAGAAA | 4209TGTT→AA | |
Class II, III, IV mutations not responsive to TEZ, IVA, or TEZ-IVA
| A46Db | I507del | R560T | Y569Db | L1077Pb |
G85E | V520F | R560S | L1065P | M1101K | |
R347P | A559Tb | A561E | R1066C | N1303K | |
L467Pb | |||||
IVA = ivacaftor; %PI = percentage of F508del-CFTR heterozygous patients in the CFTR2 patient registry who are pancreatic insufficient; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Clinical Study Report.7
Patients With F/F Genotype
Patients aged 12 years and older were eligible for inclusion in Study 103 and Study 109 if they were homozygous for the F508del mutation in the CFTR gene and had a confirmed diagnosis of CF (determined by the investigator). Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of 40% or greater and 90% or less at the time of screening.8,10 The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus.8,10 Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before first dose of TEZ-IVA in the run-in period.8,10 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.8,10
Patients With F/G and F/RF Genotypes
Patients aged 12 years and older were eligible for inclusion in Study 104 if they were heterozygous for the F508del mutation and either a gating mutation (F/G) or a residual function mutation (F/RF) and was in a region where their genotype and age group were approved by regulatory authorities for treatment with IVA and/or TEZ-IVA.9 Table 10 provides a summary of the gating mutations and RF mutations.
Patients must have a confirmed diagnosis of CF with have stable disease (both determined based on the opinion of the investigator) and a ppFEV1 of 40% or greater and 90% or less at the time of screening.9 The trial excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus.9 Patients were also considered to be ineligible if they reported an acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 28 days before first dose of TEZ-IVA in the run-in period.9 Patients with a history of solid organ or hematological transplantation were excluded, as were patients with abnormal laboratory values (e.g., hemoglobin < 10 g/dL), abnormal liver function, or abnormal renal function.9
Table 10: Gating and Residual Function Mutations in Study 104
Category | Mutations | ||
|---|---|---|---|
Gating mutations in the CFTR gene | R117H | G551D | G1244E |
G178R | G551S | S1251N | |
S549N | G1069R | S1255P | |
S549R | R1070Q | G1349D | |
Residual function mutations in the CFTR gene | 711 + 3A > G | R117C | S977F |
2789 + 5G > A | E193K | F1052V | |
3272-26A > G | L206W | K1060T | |
3849 + 10kbC > T | R347H | A1067T | |
E56K | R352Q | R1070W | |
P67L | A455E | F1074L | |
R74W | D579G | D1152H | |
D110E | E831X | D1270N | |
D110H | S945L | ||
CFTR = cystic fibrosis transmembrane conductance regulator.
Source: Clinical Study Report.9
Baseline and Demographic Characteristics
Patients With F/MF Genotype
The baseline and demographic characteristics in Study 102 were similar across the ELX-TEZ-IVA and placebo groups, with the exception of a higher percentage of patients in the ELX-TEZ-IVA group reporting prior usage of inhaled hypertonic saline compared with the placebo group (73.5% versus 62.6%) and a higher percentage of those in the ELX-TEZ-IVA group reported to have infection with Pseudomonas aeruginosa within 2 years of screening (75.0% versus 70.0%).7 BMI z score were calculated for patients less than 20 years at screening (mean [SD] = –0.40 [0.98] and –0.37 [0.79] in the placebo and ELX-TEZ-IVA groups, respectively).7
Patients With F/F Genotype
The baseline and demographic characteristics in Study 103 were generally similar across the ELX-TEZ-IVA and TEZ-IVA groups except for the prior usage of CF medications and recent infection with Pseudomonas aeruginosa. A greater percentage of patients in the ELX-TEZ-IVA group of Study 103 reported prior use of azithromycin (60.0% versus 48.1%), inhaled antibiotics (63.6% versus 53.8), bronchodilator (98.2% versus 90.4%), and inhaled corticosteroids (65.5% versus 53.8%).8 Conversely, prior use of inhaled hypertonic saline was greater in the TEZ-IVA group compared with the ELX-TEZ-IVA group (78.8% versus 69.1%).8 A greater percentage of patients in ELX-TEZ-IVA group were reported to have infection with Pseudomonas aeruginosa within 2 years of screening (70.9% versus 59.6%).8
The baseline and demographic characteristics in Study 109 were similar across the ELX-TEZ-IVA and TEZ-IVA groups with the exception that a greater percentage of patients in the TEZ-IVA group reported prior usage of dornase alfa (81.8% versus 71.3%) and inhaled hypertonic saline (64.8% versus 58.6%).
Patients With F/G and F/RF Genotypes
Study 104 enrolled patients with either an F/G or an F/RF genotype. The percentage of patients with an F/RF genotype were 64.3% and 62.1% in the placebo and ELX-TEZ-IVA groups (respectively) and the percentage with an F/G genotype were 35.7% and 37.9% in the placebo and ELX-TEZ-IVA groups (respectively).9 As shown in Table 11, data for TEZ-IVA and IVA groups are pooled into a single “control” group. The ELX-TEZ-IVA and control groups were well-balanced for all baseline and demographic characteristics, with the exception of a greater percentage of patients with prior usage of inhaled antibiotics in the placebo group compared with the ELX-TEZ-IVA group (44.4% versus 37.1%).9
Table 11: Summary of Baseline and Demographic Characteristics
Characteristics | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Sex, n (%) | ||||||||
Male | 105 (51.7) | 104 (52.0) | 24 (46.2) | 24 (43.6) | 43 (48.9) | 44 (50.6) | 65 (51.6) | 65 (49.2) |
Female | 98 (48.3) | 96 (48.0) | 28 (53.8) | 31 (56.4) | 45 (51.1) | 43 (49.4) | 61 (48.4) | 67 (50.8) |
Childbearing potential, n (%) | ||||||||
Yes | 96 (98.0) | 94 (97.9) | 24 (85.7) | 28 (90.3) | 44 (97.8) | 42 (97.7) | 48 (78.7) | 50 (74.6) |
No | 2 (2.0) | 2 (2.1) | 4 (14.3) | 3 (9.7) | 1 (2.2) | 1 (2.3) | 13 (21.3) | 17 (25.4) |
Age at baseline, years | ||||||||
Mean (SD) | 26.8 (11.3) | 25.6 (9.7) | 27.9 (10.8) | 28.8 (11.5) | 27.8 (11.0) | 27.9 (11.8) | 37.6 (14.3) | 37.7 (14.7) |
Median (range) | 25.0 (12.3, 64.0) | 24.4 (12.1, 59.9) | 27.6 (12.4, 60.5) | 27.4 (12.7, 54.1) | 27.8 (12.7, 51.5) | 25.9 (12.2, 58.7) | 37.9 (13.4, 72.7) | 37.2 (12.3, 69.8) |
≥ 12 to < 18 years, n (%) | 60 (29.6) | 56 (28.0) | 14 (26.9) | 16 (29.1) | 27 (30.7) | 25 (28.7) | 9 (7.1) | 15 (11.4) |
≥ 18 years, n (%) | 143 (70.4) | 144 (72.0) | 38 (73.1) | 39 (70.9) | 61 (69.3) | 62 (71.3) | 117 (92.9) | 117 (88.6) |
Hispanic or Latino, n (%) | ||||||||
Yes | 12 (5.9) | 4 (2.0) | 3 (5.8) | 2 (3.6) | 2 (2.3) | 1 (1.1) | 4 (3.2) | 5 (3.8) |
No | 175 (86.2) | 187 (93.5) | 49 (94.2) | 52 (94.5) | 83 (94.3) | 85 (97.7) | 114 (90.5) | 117 (88.6) |
Not collecteda | 16 (7.9) | 9 (4.5) | 0 (0) | 1 (1.8) | 3 (3.4) | 1 (1.1) | 8 (6.3) | 10 (7.6) |
Race, n (%) | ||||||||
White | 184 (90.6) | 186 (93.0) | 52 (100.0) | 54 (98.2) | 88 (100.0) | 85 (97.7) | 111 (88.1) | 122 (92.4) |
African American | 2 (1.0) | 4 (2.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (1.6) | 0 (0) |
Asian | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (3.4) | 0 (0) | 0 (0) |
American Indian | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Other | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 4 (3.2) | 1 (0.8) |
Not collecteda | 16 (7.9) | 9 (4.5) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 9 (7.1) | 9 (6.8) |
Geographic Region, n (%) | ||||||||
North America | 120 (59.1) | 118 (59.0) | 33 (63.5) | 34 (61.8) | 0 (0) | 0 (0) | 48 (38.1) | 49 (37.1) |
Europe/Australia | 83 (40.9) | 82 (41.0) | 19 (36.5) | 21 (38.2) | 88 (100) | 87 (100) | NA | NA |
Europe | NA | NA | NA | NA | NA | NA | 64 (50.8) | 70 (53.0) |
Australia | NA | NA | NA | NA | NA | NA | 14 (11.1) | 13 (9.8) |
Weight (kg) | ||||||||
Mean (SD) | 58.3 (12.7) | 59.8 (12.9) | 59.8 (14.8) | 59.9 (12.7) | 61.6 (14.5) | 58.8 (12.1) | 69.6 (17.4) | 69.5 (16.6) |
Median (range) | 58.0 (31.3, 105.2) | 58.0 (29.0, 108.0) | 55.0 (36.0, 100.0) | 59.0 (36.0, 91.2) | 60.5 (34.0, 111.0) | 58.0 (32.0, 83.0) | 67.0 (41.0, 133.0) | 67.4 (37.0, 125.2) |
BMI (kg/m2) | ||||||||
Mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 21.92 (3.89) | 21.17 (3.43) | 24.05 (4.71) | 24.07 (4.72) |
Median (range) | 20.80 (14.42, 33.80) | 21.36 (15.01, 30.86) | 20.75 (15.61, 34.60) | 21.35 (16.00, 28.44) | 21.28 (15.52, 39.33) | 21.22 (13.84, 35.56) | 23.07 (16.51, 41.62) | 23.15 (15.81, 44.36) |
ppFEV1 category at screening, n (%) | ||||||||
< 70% | 128 (63.1) | 133 (66.5) | 36 (69.2) | 37 (67.3) | 53 (60.2) | 55 (63.2) | 67 (53.2) | 74 (56.1) |
≥ 70% | 74 (36.5) | 67 (33.5) | 16 (30.8) | 18 (32.7) | 35 (39.8) | 32 (36.8) | 59 (46.8) | 58 (43.9) |
Missing | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
ppFEV1 category at baseline, n (%) | ||||||||
< 40 | 16 (7.9) | 18 (9.0) | 4 (7.7) | 6 (10.9) | 2 (2.3) | 6 (6.9) | 2 (1.6) | 2 (1.5) |
≥ 40 to < 70 | 120 (59.1) | 114 (57.0) | 34 (65.4) | 31 (56.4) | 52 (59.1) | 50 (57.5) | 63 (50.0) | 70 (53.0) |
≥ 70 to ≤ 90 | 62 (30.5) | 66 (33.0) | 14 (26.9) | 18 (32.7) | 29 (33.0) | 26 (29.9) | 52 (41.3) | 53 (40.2) |
> 90 | 5 (2.5) | 2 (1.0) | 0 (0) | 0 (0) | 5 (5.7) | 5 (5.7) | 9 (7.1) | 7 (5.3) |
ppFEV1 at baseline (%) | ||||||||
Mean (SD) | 61.3 (15.5) | 61.6 (15.0) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) | 68.1 (16.4) | 67.1 (15.7) |
Median (range) | 60.9 (32.3, 93.7) | 61.6 (33.8, 97.1) | 58.4 (35.0, 89.0) | 61.0 (35.0, 87.4) | 66.1 (35.4, 94.4) | 62.1 (31.9, 102.7) | 68.6 (31.1, 104.1) | 68.3 (29.7, 113.5) |
SwCl (mmol/L) | ||||||||
Mean (SD) | 102.9 (9.8) | 102.3 (11.9) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) | 56.4 (25.5) | 59.5 (27.0) |
Median (range) | 104.0 (68.5, 137.0) | 103.0 (22.5, 156.0) | 90.8 (60.5, 112.0) | 92.8 (67.0, 114.0) | 92.3 (47.5, 113.0) | 89.0 (51.0, 116.0) | 54.0 (10.0, 109.5) | 56.8 (10.0, 116.5) |
CFQ-R (RD) | ||||||||
Mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) | 77.3 (15.8) | 76.5 (16.6) |
Median (range) | 72.2 (16.7, 100.0) | 72.2 (16.7, 100.0) | 72.2 (27.8, 100.0) | 72.2 (22.2, 94.4) | 77.8 (27.8, 100.0) | 72.2 (11.1, 100.0) | 77.8 (11.1, 100.0) | 77.8 (0.0, 100.0) |
CFTR modulator use at screening, n (%) | ||||||||
Yes | 0 (0) | 0 (0) | 34 (65.4) | 32 (58.2) | 39 (44.3) | 39 (44.8) | 59 (46.8) | 64 (48.5) |
No | 203 (100) | 200 (100) | 18 (34.6) | 23 (41.8) | 49 (55.7) | 48 (55.2) | 67 (53.2) | 68 (51.5) |
Prior use of dornase alfa, n (%) | ||||||||
Yes | 164 (80.8) | 162 (81.0) | 48 (92.3) | 51 (92.7) | 72 (81.8) | 62 (71.3) | 66 (52.4) | 69 (52.3) |
No | 39 (19.2) | 38 (19.0) | 4 (7.7) | 4 (7.3) | 16 (18.2) | 25 (28.7) | 60 (47.6) | 63 (47.7) |
Prior use of azithromycin, n (%) | ||||||||
Yes | 114 (56.2) | 110 (55.0) | 25 (48.1) | 33 (60.0) | 44 (50.0) | 49 (56.3) | 57 (45.2) | 57 (43.2) |
No | 89 (43.8) | 90 (45.0) | 27 (51.9) | 22 (40.0) | 44 (50.0) | 38 (43.7) | 69 (54.8) | 75 (56.8) |
Prior use of inhaled antibiotic, n (%) | ||||||||
Yes | 132 (65.0) | 118 (59.0) | 28 (53.8) | 35 (63.6) | 57 (64.8) | 51 (58.6) | 56 (44.4) | 49 (37.1) |
No | 71 (35.0) | 82 (41.0) | 24 (46.2) | 20 (36.4) | 31 (35.2) | 36 (41.4) | 70 (55.6) | 83 (62.9) |
Prior use of any bronchodilator, n (%) | ||||||||
Yes | 191 (94.1) | 187 (93.5) | 47 (90.4) | 54 (98.2) | 80 (90.9) | 75 (86.2) | 111 (88.1) | 113 (85.6) |
No | 12 (5.9) | 13 (6.5) | 5 (9.6) | 1 (1.8) | 8 (9.1) | 12 (13.8) | 15 (11.9) | 19 (14.4) |
Prior use of any inhaled corticosteroids, n (%) | ||||||||
Yes | 119 (58.6) | 120 (60.0) | 28 (53.8) | 36 (65.5) | 58 (65.9) | 56 (64.4) | NR | NR |
No | 84 (41.4) | 80 (40.0) | 24 (46.2) | 19 (34.5) | 30 (34.1) | 31 (35.6) | NR | NR |
Prior use of any inhaled hypertonic saline, n (%) | ||||||||
Yes | 127 (62.6) | 147 (73.5) | 41 (78.8) | 38 (69.1) | 52 (59.1) | 53 (60.9) | 54 (42.9) | 57 (43.2) |
No | 76 (37.4) | 53 (26.5) | 11 (21.2) | 17 (30.9) | 36 (40.9) | 34 (39.1) | 72 (57.1) | 75 (56.8) |
Pseudomonas aeruginosa infection within 2 years of screening, n (%) | ||||||||
Positive | 142 (70.0) | 150 (75.0) | 31 (59.6) | 39 (70.9) | 58 (65.9) | 59 (67.8) | 74 (58.7) | 79 (59.8) |
Negative | 61 (30.0) | 50 (25.0) | 21 (40.4) | 16 (29.1) | 30 (34.1) | 28 (32.2) | 52 (41.3) | 53 (40.2) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; NR = not reported; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
aNot collected in accordance with local regulations.
Source: Clinical Study Reports7-10and additional information provided by the sponsor.11,54
Interventions
Study Drugs
Patients With F/MF Genotype
Study 102 did not include a run-in period and randomized patients received either ELX-TEZ-IVA or matching placebo tablets taken every morning and evening. The placebo tablets were identical in appearance to either the ELX-TEZ-IVA and IVA tablets.
Patients With F/F Genotype
Patients in Study 103 and Study 109 underwent a 28-day open-label run-in period where they received treatment with open-label TEZ 100 mg and IVA 150 once daily in the morning and IVA 150 mg once daily (TEZ-IVA). Randomized patients received either ELX-TEZ-IVA or continued with TEZ-IVA. As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the TEZ-IVA group also administered 2 matching placebo tablets for the morning dosage and those in the ELX-TEZ-IVA group administered 1 matching placebo tablet to maintain blinding (i.e., both groups administered 3 tablets in the morning and 1 in the evening). The placebo and active tablets were identical in appearance.
Patients With F/G and F/RF Genotypes
Patients in Study 104 underwent a 28-day open-label run-in period where all patients with an F/RF genotype received TEZ 100 mg and IVA 150 once daily in the morning and IVA 150 mg once daily in the evening (TEZ-IVA) and those with an F/G genotype received IVA 150 mg every 12 hours. Randomized patients received either ELX-TEZ-IVA or, in the control group, continued with TEZ-IVA or IVA for those with F/RF and F/G genotypes, respectively.9 As the morning dose of ELX-TEZ-IVA is administered as 2 tablets (each containing ELX 100 mg, TEZ 50 mg, and IVA 75 mg), patients randomized to the control groups (TEZ-IVA or IVA) also administered 2 matching placebo tablets for the morning dosage to maintain blinding and those in the ELX-TEZ-IVA group administered 1 matching placebo tablet (i.e., both groups administered 3 tablets in the morning and 1 in the evening). The placebo and active tablets were identical in appearance.
Table 12: Dosage Regimens for the Study Drugs
Study | Intervention | Comparator |
|---|---|---|
Study 102 (F/MF) | Morning: 2 ELX-TEZ-IVA tablets Evening: 1 IVA tablet | Morning: 2 placebo tablets Evening: 1 placebo tablet |
Study 103 (F/F) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
Study 109 (F/F) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
Study 104 (F/G or F/RF) | Morning: 2 ELX-TEZ-IVA tablets + 1 placebo tablet Evening: 1 IVA tablet | F/G Group Morning: 1 IVA tablet + 2 placebo tablets Evening: 1 IVA tablet F/RF Group Morning: 1 TEZ-IVA tablet + 2 placebo tablets Evening: 1 IVA tablet |
ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; TEZ = tezacaftor.
Dose Modifications and Interruptions
The study protocols stated that there were no dose modifications for toxicity permitted in the trials; however, dose interruptions were permitted for patients who met pre-specified criteria related to liver function tests and rash. For the liver function tests, administration of the study treatments was to be interrupted immediately if any of the following criteria were met: ALT or AST greater than 8 times then ULN; ALT or AST greater than 5 times the ULN for more than 2 weeks; and ALT or AST greater than 3 times the ULN, in association with total bilirubin greater than 2 times the ULN and/or clinical jaundice. The potential causes of the elevated liver function tests were to be investigated and treatment was to be discontinued if subsequent ALT or AST values confirmed the initial elevations (i.e., exceeded the thresholds for treatment interruption) and no convincing alternative etiology was identified (e.g., acetaminophen use, viral hepatitis, or alcohol ingestion). If an alternative, reversible cause of elevated transaminases was identified, the study treatment could be resumed once the patient’s transaminase levels returned to baseline or 2 or less times the ULN (whichever was greater). Treatment was also to be interrupted for patients who developed a generalized rash that was a grade 3 or higher AE or an SAE.
Concomitant Medications
Study participants were to remain on a stable CF treatment regimen from 28 days before the start of the run-in period through to completion of the study. Stable CF treatment regimen was defined as the current treatment regimen for CF that the patient had been receiving. Guidelines for stable treatment regimens for CF are as follows.
Those using inhaled tobramycin or other chronically inhaled antibiotics should remain on the regimen throughout the study.
Those who cycle onto and off of an inhaled antibiotic should continue on their prior schedule. The timing of the first dose of study drug on the day 1 visit should be synchronized as closely as possible (e.g., not more than ± 3 days) to the first day in the cycle onto the inhaled antibiotic.
Those who alternate between 2 different inhaled antibiotics should remain on the same cycling schedule during the study. The timing of the first dose of study drug on the day 1 visit should be synchronized as closely as possible (e.g., not more than ± 3 days) to the first day in the cycle onto 1 of the inhaled antibiotics.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 13. These end points are further summarized below. A detailed description and appraisal of the outcome measures is provided in Appendix 4.
Table 13: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
End point | Time point | Study 102 | Study 103 | Study 104 | Study 109 |
|---|---|---|---|---|---|
Spirometry | |||||
Abs change in ppFEV1 | At week 4 | Primary (global) Key secondary (Europe) | Primary | NA | NA |
Through 8 weeks | NA | NA | Primary (within group) Key secondary (vs. control) | NA | |
Through week 24 | Primary (Europe) Key secondary (Europe) | NA | NA | Key secondary | |
Pulmonary exacerbations | |||||
Number of PEx | Through week 24 | Key secondary | NA | NA | NA |
Number of PEx requiring hospitalization | Through week 24 | Other | NA | NA | NA |
Number of PEx requiring IV antibiotics | Through week 24 | Other | NA | NA | NA |
Number of PEx requiring IV antibiotics or hospitalization | Through week 24 | Other | NA | NA | NA |
Time-to-first PEx | Through week 24 | Other | NA | NA | NA |
Time-to-first hospitalization for PEx | Through week 24 | Other | NA | NA | NA |
Time-to-first IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA |
Duration of PEx | Through week 24 | Other | NA | NA | NA |
Duration of hospitalization for PEx | Through week 24 | Other | NA | NA | NA |
Duration of IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA |
Duration of hospitalization or IV antibiotics for PEx | Through week 24 | Other | NA | NA | NA |
Body composition | |||||
Abs change in BMI | At 4 weeks | NA | Other | NA | NA |
At 8 weeks | NA | NA | Other | NA | |
At 24 weeks | Key secondary | NA | NA | NA | |
Abs change in weight | A 4 weeks | NA | Other | NA | NA |
At 24 weeks | Other | NA | NA | NA | |
Abs change in BMI z score | At 24 weeks | Other | NA | NA | NA |
Sweat chloride | |||||
Abs change in sweat chloride | At 4 weeks | Key secondary | Key secondary | NA | NA |
Through 8 weeks | NA | NA | Key secondary (within group and vs. control) | NA | |
Through week 24 | Key secondary | NA | NA | Other | |
Patient reported outcomes | |||||
Abs change in CFQ-R (RD) | At 4 weeks | Key secondary | Key secondary | NA | NA |
Through 8 weeks | NA | NA | Other (within group and vs. control) | NA | |
Through week 24 | Key secondary | NA | NA | Primary | |
Abs change in CFQ-R (non-RD) | At 4 weeks | NA | Other | NA | NA |
Through 8 weeks | NA | NA | Other | NA | |
Through week 24 | Other | NA | NA | NA | |
Abs change in TSQM | At 4 weeks | NA | Other | NA | NA |
At 24 weeks | Other | NA | NA | NA | |
Hospitalizations | |||||
Planned hospitalizations | Through week 24 | Other | NA | NA | NA |
Unplanned hospitalizations | Through week 24 | Other | NA | NA | NA |
Duration of planned hospitalizations | Through week 24 | Other | NA | NA | NA |
Duration of unplanned hospitalizations | Through week 24 | Other | NA | NA | NA |
Abs = absolute; BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; IV = IV; NA = not applicable; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; TSQM = Treatment Satisfaction Questionnaire for Medication.
Percent Predicted FEV1
Percent predicted FEV1 was calculated using the ratio of FEV1 (L) to the predicted FEV1 (L). The predicted FEV1 was calculated using the equations of the Global Lung Function Initiative.7,55 Absolute change from baseline was calculated as post-baseline value minus baseline value. Absolute change from baseline in ppFEV1 was the primary end point of 3 of the included studies:
Study 102 (versus placebo): evaluated at 4 weeks and through 24 weeks in the global European protocols (respectively)
Study 103 (versus TEZ-IVA): evaluated at 4 weeks
Study 104 (within-group change for ELX-TEZ-IVA); evaluated through 8 weeks7-9
Due to the onset of the COVID-19 pandemic, patients in Study 104 could be provided with spirometry devices to perform in-home assessments of lung function (as clinic visits were not occurring). As noted in the Statistical Analysis section, sensitivity analyses were performed to investigate the impact of including and excluding the in-home spirometry measurements.
At the time of this review, a literature search did not identify an accepted MID for absolute change from baseline in ppFEV1 for patients with CF. The clinical experts consulted by CADTH noted that an absolute improvement of 5% is typically considered to be meaningful for acute changes in ppFEV1; however, it was noted that even stabilization of ppFEV1 can be meaningful for patients, especially those who are at risk of rapid decline. Both the clinical experts consulted by CADTH and the clinician groups who provided input into this review noted that slowing the decline in lung function is considered to be more important than short-term increases.
Pulmonary Exacerbations
Pulmonary exacerbations were evaluated as an efficacy end point in Study 102. Pulmonary exacerbations were defined as a change in antibiotic therapy (IV, inhaled, or oral) for any 4 or more of the following signs or symptoms: change in sputum; new or increased hemoptysis; increased cough; increased dyspnea; malaise, fatigue, or lethargy; temperature greater than 38°C; anorexia or weight loss; sinus pain or tenderness; change in sinus discharge; change in physical examination of the chest; decrease in lung function by at least 10% (based on spirometry); or radiographic changes indicative of pulmonary infection. Changes in antibiotic therapy for sinopulmonary signs and/or symptoms were determined and documented by the study investigator at each study visit.7
Several of the criteria for sinopulmonary signs and symptoms were assessed by the investigator alone (including temperature greater than 38°C, anorexia or weight loss, sinus pain or tenderness, change in physical examination of chest, decrease in pulmonary function by 10% [based on spirometry], and radiographic changes indicative of pulmonary infection). Changes in sputum, new or increased hemoptysis, increase cough, increased dyspnea, malaise, fatigue, or lethargy, and change in sinus discharge were independently assessed by the investigator, or together with patient description, evaluated and reported by the investigator. There did not appear to have been an independent adjudication of pulmonary exacerbation events.
The following end points related to exacerbations were evaluated in Study 102:
Rate of pulmonary exacerbations
Rate of pulmonary exacerbations requiring hospitalization
Rate of pulmonary exacerbations requiring IV antibiotics
Rate of pulmonary exacerbations requiring IV antibiotics or hospitalization
Time-to-first pulmonary exacerbation
Time-to-first hospitalization for pulmonary exacerbation
Time-to-first IV antibiotic therapy for pulmonary exacerbation
Time-to-first pulmonary exacerbation requiring IV antibiotics or hospitalization
Duration of pulmonary exacerbations
Duration of hospitalization for pulmonary exacerbation
Duration of IV antibiotic therapy for pulmonary exacerbation
Duration of IV antibiotic therapy or hospitalization for pulmonary exacerbation
BMI and Body Weight
Three of the included studies evaluated changes from baseline in BMI (Studies 102, 103, and 104).7-9 BMI was analyzed as BMI-for-age z score for patients aged 12 to 20 years in Study 102.7 Absolute change from baseline in BMI at 24 weeks was a key secondary end point of Study 102.7 Studies 103 and 104 included absolute change from baseline at 4 and 8 weeks, respectively, as an additional efficacy end point.8,9
Cystic Fibrosis Questionnaire–Revised
The CFQ-R is a disease-specific, health-related quality of life instrument designed for patients with CF, comprised of age-appropriate versions for children aged 6 to 13 (CFQ-C), their parents (who serve as a proxy for their child; CFQ-P), and individuals aged 14 years or older (CFQ-14).56 For children 6 to 11, the CFQ-C is interviewer-administered, and for children aged 12 and 13 year, it is self-administered.57 The number of items and domains vary between versions with the child version including 35 items within 8 domains, parent version including 44 items and 11 domains, and the adolescent and adult version including 50 items within 12 domains (see Figure 18 on page 167).56,57 The domains included in the adolescent and adult version are as follows: a health-related quality of life module including physical functioning, vitality, emotional functioning, social or school functioning, role functioning, body image, eating problems, treatment burden; a symptoms module that includes respiratory symptoms, digestive symptoms, and weight; and a health perception module. A 4-point Likert scale is used to measure frequency (always, often, sometimes, never), intensity (a great deal, somewhat, a little, not at all) and true-false scales (very true, somewhat true, somewhat false, very false). Items within domains are summed and standardized. Individual domain scores range from 0 to 100, with higher scores indicating better health-related quality of life.56 The scales are designed to measure symptoms and functioning during the 2-week period before administration of the questionnaire.58 A difference of at least 4 points in the RD score of the CFQ-R is commonly cited as the MID for patients with CF.59
The absolute change from baseline in the CFQ-R (RD) score was the primary end point of Study 109 and a pre-specified key secondary end point in Study 102 (4 and 24 weeks) and Study 103 (4 weeks).7-10 Absolute change from baseline in the non-respiratory domain scores were included as other efficacy end points in Study 102 (through 24 weeks), Study 103 (at 4 weeks), and Study 104 (through 8 weeks).7-9 Due to the onset of the COVID-19 pandemic, some patients in Study 104 and Study 109 were provided with the CFQ-R to perform in-home assessments. As noted in the Statistical Analysis section, sensitivity analyses were performed to investigate the impact of including and excluding the in-home evaluation of the CFQ-R.
Treatment Satisfaction Questionnaire for Medication
The TSQM is an instrument used to assess a patient’s satisfaction with the study medication and includes 4 domains: effectiveness, side effects, convenience, and global satisfaction.7,8 The TSQM consists of 14 items to form 4 domains: effectiveness (items 1, 2, 3), side effects (items 4, 5, 6, 7, 8), convenience (items 9, 10, 11), and global satisfaction (items 12, 13, 14).7 A 5- or 7-point Likert scale is used to score the domains and each domain score ranges from 0 (least satisfied) to 100 (most satisfied).7,60 The TSQM was included as an additional efficacy end point in Study 102 (evaluated through 24 weeks) and Study 103 (evaluated at 4 weeks).7,8 The sponsor reported that the TSQM was conducted for patients between the ages of 12 and 17 years of age to meet European regulatory commitments.7,8
Sweat Chloride
Sweat chloride samples were obtained from patients using an approved collection device. At each time point, 2 samples were collected, 1 from each of the patient’s arms, and sent to a central laboratory for analysis.7 All of the included studies evaluated absolute change from baseline in sweat chloride. Absolute change from baseline in sweat chloride was a key secondary end point in Study 102 (evaluated at 4 weeks and through 24 weeks), Study 103 (evaluated at 4 weeks), and Study 104 (evaluated as the within-group change for the ELX-TEZ-IVA group through 8 weeks).
Hospitalizations
Study 102 included the frequency and duration of planned CF hospitalizations and unplanned CF hospitalizations as additional end points.
Planned hospitalizations for CF (i.e., antibiotic therapy) were assumed to be for pre-planned IV antibiotic therapy or for pre-planned treatment of CF-related clinical issues or events. Patients who received IV antibiotics for the treatment of an acute pulmonary exacerbation were not to be included in this category of planned hospitalization.
Unplanned hospitalizations for CF were those due to reasons other than protocol-defined acute pulmonary exacerbations, including non-protocol-defined pulmonary exacerbations or other CF-related reasons (e.g., pancreatitis, distal intestinal obstruction syndrome, and so forth).
It is important to note that neither the planned nor the unplanned hospitalization end points included hospitalizations due to protocol-defined pulmonary exacerbations.54 Pulmonary exacerbations requiring hospitalization were evaluated separately (as reported in the section on pulmonary exacerbations).
Adverse Events
AEs were defined as any untoward medical occurrence in a patient during the study, including newly occurring events or worsening of pre-existing conditions (e.g., increased in its severity or frequency). An AE was considered serious if it met any of the following outcomes: fatal; life-threatening; inpatient hospitalization or prolongation of hospitalization; persistent or significant disability/incapacity, congenital anomaly, or birth defect; or an important medical event that jeopardized the patient or required medical or surgical intervention to prevent 1 of the aforementioned outcomes.
Statistical Analysis
Power Calculations
Patients With F/MF Genotype
In Study 102, the power calculation was based on 180 patients and a 10% dropout rate in both the ELX-TEZ-IVA and placebo groups for the final analysis and 70 patients and a 5% dropout rate in both groups for the interim analysis. Assuming a within-group standard deviation of 7%, the trial was estimated to have 98% and 99% power at the interim and final analyses, respectively, to detect a treatment difference of 5% in the primary end point (absolute change from baseline in ppFEV1 at 4 weeks) across the ELX-TEZ-IVA and placebo groups with a 2-sided alpha of 0.044 (interim analysis) and 0.01 (final analysis).
Patients With F/F Genotype
In Study 103, the power calculation was based on 100 patients and a 5% dropout rate at 4 weeks. For the primary end point of absolute change in ppFEV1 from baseline at 4 weeks, assuming a within-group SD of 7%, this trial was estimated to have approximately 93% power to detect a difference of 5.0% for the primary end point, with a 2-sided alpha of 0.05.
In Study 109, the power calculation was based on 158 patients and a 10% dropout rate through 24 weeks. For the primary end point of absolute change in CFQ-R (RD) score from baseline through 24 weeks, assuming a dropout rate of 10% and within-group SD of 18 points, a sample size of 158 patients was estimated to have approximately 90% power to detect a difference of 10 points for the primary end point, with a 2-sided alpha of 0.05. For the key secondary end point of absolute change in ppFEV1 from baseline through 24 weeks, assuming a dropout rate of 10% and within-group SD of 7%, a sample size of 158 patients was estimated to have approximately 98% power to detect a treatment difference of 5%, with a 2-sided alpha of 0.05.
Patients With F/G or F/RF Genotype
In Study 104, the power calculation was based on 125 patients in the ELX-TEZ-IVA group and a 10% dropout rate after 8 weeks. For the primary efficacy end point of absolute change in ppFEV1 from baseline through 8 weeks for the ELX-TEZ-IVA group, assuming a within-group SD of 7.0%, the trial was estimated to have greater than 99% power to detect a within-group difference of 3.0% (1 sample t-test at a 2-sided significance level of 0.05).
Primary Outcomes
In Studies 102, 103, and 104, absolute changes from baseline in ppFEV1 were calculated using a mixed-effects model for repeated measures (MMRM) approach. The models for Study 102 and Study 103 included treatment group, visit, and treatment-by-visit interaction as fixed effects, with continuous baseline ppFEV1, age at screening (< 18 versus ≥ 18 years of age), and sex (male versus female) as covariates. The model for Study 104 included treatment group, visit, and treatment-by-visit interaction as fixed effects, with continuous baseline ppFEV1, continuous baseline sweat chloride, and comparator group (i.e., IVA or TEZ-IVA) as covariates. Missing post-baseline values were not imputed for efficacy analyses conducted using the MMRM approach (assumed data were missing at random). Sensitivity analyses using multiple imputation were performed to assess the robustness of the primary analyses.
There were 2 statistical analysis protocols used in Study 102: the “global” protocol which specified absolute change in ppFEV1 from baseline at 4 weeks as the primary end point; and a European protocol which specified absolute change in ppFEV1 from baseline through week 24 as the primary end point.7 The analysis that was conducted “at 4 weeks” used the 4-week evaluation as the end point and the analysis that was conducted “through 24 weeks” used an average of week 4, week 8, week 12, week 16, and week 24. The sponsor noted that this was due to regulatory requirements in different jurisdictions (i.e., European regulators requested that the primary end point be evaluated through 24 weeks).7 As a result, the statistical testing order of the primary and first key secondary end points was reversed in the 2 protocols (i.e., the primary end point in the global protocol was the first key secondary end point in the European protocol and vice versa).7
Secondary and Other Efficacy End Points
The statistical evaluation of the continuous key and other secondary end points (e.g., ppFEV1, BMI, CFQ-R, weight, and TSQM) were conducted using an MMRM model similar to the 1 used for the primary analysis, but with the additional of the baseline value for the end point of interest as a covariate. For number of pulmonary exacerbations in Study 102 (overall and those requiring IV antibiotics or hospitalization), the comparison between the ELX-TEZ-IVA and the comparator group (i.e., placebo) was conducted using regression analyses for a negative binomial distribution with sex, baseline age group (< 18 versus ≥ 18 years), and baseline ppFEV1 severity at screening (< 70% versus ≥ 70%) as covariates. Time-to-first pulmonary exacerbation (any exacerbation and those requiring IV antibiotics or hospitalization) were analyzed using Cox regression. The sponsor’s model included a main effect for treatment, with covariates for sex, baseline age group (< 18 versus ≥ 18 years), and ppFEV1 severity at screening (< 70% versus ≥ 70%).
Subgroup Analyses
The CADTH review protocol identified 4 subgroups of interest: severity of disease (based on baseline FEV1), CFTR genotype (F/F, F/MF, F/G, and F/RF), prior therapy with CFTR modulator(s), and patient age. The different subgroups that were investigated in the included clinical studies are described in the section below.
Patients With F/MF Genotype
In Study 102, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in ppFEV1): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America or Europe/Australia); prior use of inhaled antibiotic (yes or no); prior use of dornase alfa (yes or no); prior use of inhaled bronchodilator (yes or no); prior use of inhaled hypertonic saline (yes or no); prior use of inhaled corticosteroids (yes or no); prior use of azithromycin (yes or no); and infection with Pseudomonas aeruginosa within 2 years of the screening visit (positive or negative).7 An additional post hoc subgroup analysis was performed for the subset of patients with a ppFEV1 less than 40% at baseline. The subgroup analyses were conducted using an MMRM model similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Patients With F/F Genotype
In Study 103, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in ppFEV1): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America or Europe); prior use of inhaled antibiotic (yes or no); prior use of dornase alfa (yes or no); prior use of inhaled bronchodilator (yes or no); prior use of inhaled hypertonic saline (yes or no); prior use of inhaled corticosteroids (yes or no); prior use of azithromycin (yes or no); and infection with Pseudomonas aeruginosa within 2 years of the screening visit (positive or negative).8 An additional post hoc subgroup analysis was performed based on prior exposure to CFTR modulators (treatment-naive or treatment-experienced). In Study 109, the following pre-planned subgroup analyses were conducted for the primary end point (i.e., absolute change in CFQ-R [RD]): age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); and CFTR modulator use at screening (yes or no).10 For both studies, the subgroup analyses were conducted using an MMRM model similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Patients With F/G or F/RF Genotype
In Study 104, the following pre-planned subgroup analyses were conducted: age at screening (< 18 years or ≥ 18 years); ppFEV1 at baseline (< 70% or ≥ 70%); sex (male or female); geographic region (North America and Europe/Australia); and comparator group (TEZ-IVA comparator or IVA comparator).9 The subgroup analyses were conducted using an MMRM model similar to that used in the primary analysis. There was no adjustment of multiplicity in the subgroup analyses.
Multiplicity Adjustment
Patients With F/MF Genotype
Study 102 included 2 study protocols: a global protocol and a European protocol. The timing and methods for evaluating the primary end point differed between the 2 protocols. In the global protocol, a Lan and DeMets alpha spending function was applied to control the overall type I error rate of 0.05 for the primary end point during the interim analysis and the final analysis such that an alpha of 0.01 would be preserved for the final analysis. The actual alpha at the interim analysis was determined based on the number of patients included in the analysis and since all patients had been on treatment for at least 4 weeks at the time of the analysis, the primary end point of absolute change in ppFEV1 at 4 weeks was tested at an alpha of 0.05 during the interim analysis. Hence, the interim analysis was the primary analysis for Study 102. For the European protocol, the primary end point of absolute change in ppFEV1 through 24 weeks was tested at an alpha of 0.05.
The key secondary end points in Study 102 were tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the type I error rate and for a test to be considered statistically significant all previous tests within the hierarchy must be statistically significant at the 0.05 level. The testing order for the key secondary end points was:
Absolute change in ppFEV1 from baseline through 24 weeks (global protocol) or at 4 weeks (European protocol)
Number of pulmonary exacerbations through 24 weeks
Absolute change in sweat chloride from baseline through 24 weeks
Absolute change in CFQ-R (RD) from baseline through 24 weeks
Absolute change in BMI from baseline at 24 weeks
Absolute change in sweat chloride from baseline at 4 weeks
Absolute change in CFQ-R (RD) from baseline at 4 weeks7
Patients With F/F Genotype
In Study 103, the key secondary end points were formally tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the type I error rate for the multiple key secondary end points tested at an alpha of 0.05. For a test to be considered statistically significant, the previous test within the hierarchy must be statistically significant at the 0.05 level. The testing order of the key secondary end points is as follows:
Absolute change in sweat chloride from baseline at 4 weeks
Absolute change in CFQ-R RD score from baseline at 4 weeks8
In Study 109, a hierarchical fixed-sequence testing procedure was used to first test the primary end point and then the key secondary end point, to control the overall family-wise type I error at a 2-sided alpha of 0.05. The key secondary end point was tested only after the primary end point was determined to be statistically significant.10
Patients With F/G or F/RF Genotype
In Study 104, the key secondary end points were formally tested at an alpha of 0.05 only if the primary end point was statistically significant. A hierarchical testing procedure was used to control the overall type I error rate at an alpha of 0.05 for the primary and key secondary end points tested. For a test to be considered statistically significant within the testing hierarchy, all previous tests within the hierarchy must be statistically significant at the 0.05 level. The testing order of the key secondary end points was as follows:
Absolute change in sweat chloride from baseline through 8 weeks within the ELX-TEZ-IVA group
Absolute change in ppFEV1 from baseline through 8 weeks for the ELX-TEZ-IVA group compared to the control group
Absolute change in sweat chloride from baseline through 8 weeks for the ELX-TEZ-IVA group compared to the control group9
Data Imputation Methods
The MMRM analyses performed in all the included studies assumed that data were missing at random, and no imputation of missing data was performed. As shown in Table 14, sensitivity analyses were performed using multiple imputation to assess the impact of missing data. Missing values were imputed starting from the first visit with missing values, for which all subsequent visits were also missing. Intermediate missing data (i.e., missing values that fell between 2 non-missing values) were assumed to be missing at random and therefore were not imputed.7-10
Table 14: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Study 102 | |||
Absolute change ppFEV1 | MMRM |
| MMRM (multiple imputation) |
Absolute change in: SwCl, BMI, CFQ-R, body weight | MMRM |
| Not applicable |
BMI z score | MMRM |
| – |
Number of PEx, PEx requiring IV antibiotics and/or hospitalization | NBR |
| – |
Time-to-first: PEx, PEx requiring IV antibiotics, and/or hospitalization | Cox regression |
| – |
Study 103 | |||
Absolute change ppFEV1 | MMRM |
| MMRM (multiple imputation) |
Absolute change in: SwCl, BMI, CFQ-R, TSQM, body weight | MMRM |
| Not applicable |
Study 104 | |||
Absolute change ppFEV1 | MMRM |
|
|
Absolute change SwCl | MMRM |
| MMRM any SwCl values < 10 mmol/L were considered missing |
Absolute change in CFQ-R (RD) | MMRM |
| MMRM (only data assessed in clinic)b |
Study 109 | |||
Absolute change in CFQ-R (RD) | MMRM |
|
|
Absolute change in: SwCl and ppFEV1 | MMRM |
| MMRM (multiple imputation) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; IV = IV; IVA = ivacaftor; MMRM = mixed-effects model for repeated measures; NBR = negative binomial regression; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SwCl = sweat chloride; TEZ = tezacaftor; TSQM = Treatment Satisfaction Questionnaire for Medication; vs. = versus.
aPrimary analysis was conducted with clinic spirometry data only. Due to the COVID-19 pandemic, home-assessed spirometry (i.e., spirometry assessed independently by the patients at home) was permitted to be performed. An additional analysis was performed that included pooled clinic and home-assessed spirometry.
bDue to the COVID-19 pandemic, CFQ-R was permitted to be performed at home. The main analysis included pooled CFQ-R data assessed at the clinic and at home and an additional analysis was performed that included only the CFQ-R data that was assessed at the clinic.
Analysis Populations
The analysis sets that were used to evaluate the safety and efficacy end point in the included studies are summarized in Table 15.
Study | Dataset | Description |
|---|---|---|
Study 102 | All subjects set | All randomized patients received at least 1 dose of study drug; used for individual patient data listings and disposition summary |
Full analysis set | All randomized patients who carry the intended CFTR allele mutations and received at least 1 dose of study drug; used for all final efficacy analyses | |
Interim full analysis set | Patients in the full analysis set whose scheduled week 4 visit was on or before the data cut-off (contains the same patients as the full analysis set); used for the interim efficacy analyses | |
Safety set | All patients who received at least 1 dose of study drug; used for safety analyses | |
Study 103 Study 104 Study 109 | All subjects set | All randomized patients or received at least 1 dose of study drug; used for individual patient data listings and disposition summary |
Full analysis set | All randomized patients who carry the intended CFTR allele mutations and received at least 1 dose of study drug; used for all efficacy analyses | |
Safety set (run-in) | All patients who received at least 1 dose of run-in period drug (i.e., TEZ-IVA or IVA); used for safety analyses in the run-in period | |
Safety set (treatment period) | All patients who received at least 1 dose of study drug; used for safety analyses in the treatment period |
CFTR = cystic fibrosis transmembrane conductance regulator; IVA = ivacaftor; TEZ = tezacaftor.
Results
Patient Disposition
Patient disposition is summarized in Table 16 for Study 102 (i.e., the study that did not include a run-in period) and in Table 17 for Study 103, 104, and 109 (i.e., the studies with a run-in period).
Patients With F/MF Genotype
In Study 102, a total of 438 patients were screened for inclusion and 405 patients were randomized (7.5% failed to the meet the eligibility criteria).11 Two hundred and 4 patients were randomized to the placebo group and 201 to the ELX-TEZ-IVA group. One patient in each group was randomized but never received the study drug; therefore, a total of 403 patients were included in the full analysis set for the interim and final analyses. All the patients in the placebo group and 98.5% of those in the ELX-TEZ-IVA group completed the study (overall completion rate of 99.3%). Reasons for discontinuation included AEs (n = 2) and pregnancy (n = 1). All of the patients who completed the study elected to continue in the open-label extension phase.7
Table 16: Patient Disposition in Study Without Run-In Period (Study 102)
Disposition | Placebo | ELX-TEZ-IVA |
|---|---|---|
All subjects set | 204 | 201 |
Interim FAS | 203 | 200 |
FAS | 203 | 200 |
Safety set | 201 | 202 |
Randomized | 204 | 201 |
Randomized but not dosed | 1 | 1 |
Completed treatment, n (%) | 203 (100) | 197 (98.5) |
Prematurely discontinued treatment, n (%) | 0 (0) | 3 (1.5) |
Adverse event | 0 (0) | 2 (1.0) |
Patient refused further dosing | 0 (0) | 0 (0) |
Death | 0 (0) | 0 (0) |
Pregnancy (self or partner) | 0 (0) | 1 (0.5) |
Completed study | 203 (100) | 197 (98.5) |
Prematurely discontinued the study, n (%) | 0 (0) | 3 (1.5) |
Adverse event | 0 (0) | 1 (0.5) |
Withdrawal of consent (not AE) | 0 (0) | 1 (0.5) |
Death | 0 (0) | 0 (0) |
Other | 0 (0) | 1 (0.5) |
Rolled over to open-label study, n (%) | 203 (100) | 197 (98.5) |
ELX = elexacaftor; FAS = full analysis set; IVA = ivacaftor; TEZ = tezacaftor.
Source: Clinical Study Report.7
Patients With F/F Genotype
In Study 103, a total of 118 patients were screened for inclusion and 113 were enrolled in the 28-day TEZ-IVA run-in period (4.2% failed to the meet the eligibility criteria). A total of 108 patients were randomized (56 in the ELX-TEZ-IVA group and 52 in the TEZ-IVA group). One patient in the ELX-TEZ-IVA group was randomized but never received the study drug; therefore, a total of 107 patients were included in the full analysis set. All of the patients in both the ELX-TEZ-IVA and TEZ-IVA groups completed the study (overall completion rate of 100%) and all of the patients elected to continue in the open-label extension phase.8
In Study 109, a total of 180 patients were screened for inclusion and 176 were enrolled in the 28-day TEZ-IVA run-in period (2.2% failed to the meet the eligibility criteria). One patient was excluded from the trial during the run-in period due to a pulmonary exacerbation. This patient was randomized to the ELX-TEZ-IVA group but discontinued before the first dose of the study treatments in the double-blind phase. Therefore, the total number of patients randomized was 176 (88 in the ELX-TEZ-IVA group and 88 in TEZ-IVA group), but only 175 patients were included in the full analysis set. The proportions of patient who completed the study were 98.9% and 97.7% in the ELX-TEZ-IVA and TEZ-IVA groups, respectively. Two patients withdrew due to AEs from TEZ-IVA group and 1 patient withdrew due to AEs from the ELX-TEZ-IVA group. All of the patients who completed the study elected to enroll in the open-label extension study.10
Patients With F/G or F/RF Genotypes
A total of 300 patients were screened for inclusion in Study 104 and 29 (9.7%) failed to the meet the eligibility criteria for the study. A total of 271 patients were enrolled in the 28-day run-in phase where they received treatment with TEZ-IVA or IVA for those with F/RF and F/G mutations, respectively. Ten patients (3.7%) withdrew during the run-in phase. The reasons for discontinuation included AEs (n = 2; 0.7%); refusal to undergo further dosing (n = 1; 0.4%); failure to meet the eligibility criteria for Study 104 (n = 1; 0.4%). The sponsor reported that of the 6 patients who discontinued for “other” reasons (as shown in Table 17), 5 patients withdrew due to the onset of the COVID-19 pandemic and 1 patient for reasons that were related to the eligibility of the study. A total of 259 patients were randomized (133 in the ELX-TEZ-IVA group and 126 in the TEZ-IVA or IVA group—referred to as the control group). One patient in the ELX-TEZ-IVA group discontinued before the first dose of the study treatments in the double-blind phase; therefore, the full analysis set included 258 patients. The proportions of patient who completed the study were 99.2% and 96.8% in the ELX-TEZ-IVA and control groups, respectively. Two patients from the control group withdrew due to AEs and 1 patient from the ELX-TEZ-IVA group withdrew due to AEs (WDAE). With the exception of 1 patient in each of the treatment groups, all the patients who completed the study elected to enroll in the open-label extension study.
Table 17: Patient Disposition in Studies Within Run-In Period (Studies 103, 104, and 109)
Patient Disposition in Studies Within Run-In Period (Studies 103, 104, and 109) | ||||||
|---|---|---|---|---|---|---|
Disposition in run-in period | ||||||
Disposition, n (%) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | |||
TEZ-IVA | TEZ-IVA | TEZ-IVA or IVA | ||||
All subjects set | 113 | 176 | 271 | |||
Safety set (run-in period) | 113 | 176 | 271 | |||
Discontinued treatment | 6 (5.3) | 1 (0.6) | 10 (3.7) | |||
Adverse event | 5 (4.4) | 0 (0) | 2 (0.7) | |||
Refused further dosing | 1 (0.9) | 0 (0) | 1 (0.4) | |||
Eligibility criteria not met | 0 (0) | 1 (0.6) | 1 (0.4) | |||
Other | 0 (0) | 0 (0) | 6 (2.2) | |||
Discontinued study | 6 (5.3) | 1 (0.6) | 12 (4.4) | |||
Adverse event | 4 (3.5) | 1 (0.6) | 3 (1.1) | |||
Consent withdrawn | 2 (1.8) | 0 (0) | 2 (0.7) | |||
Other | 0 (0) | 0 (0) | 7 (2.6) | |||
Disposition in treatment period | ||||||
Disposition | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | |||
TEZ-IVA | ELX-TEZ-IVA | TEZ-IVA | ELX-TEZ-IVA | TEZ-IVA or IVA | ELX-TEZ-IVA | |
Full analysis set | 52 | 55 | 88 | 87 | 126 | 132 |
Safety set (treatment period) | 52 | 55 | 88 | 87 | 126 | 132 |
Randomized | 52 | 56 | 88 | 88 | 126 | 133 |
Randomized but not dosed | 0 (0) | 1 | 0 (0) | 1 | 0 (0) | 1 |
Completed treatment, n (%) | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 122 (96.8) | 131 (99.2) |
Discontinued study, n (%) | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 4 (3.2) | 1 (0.8) |
Adverse event | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) |
Physician decision | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Other | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Completed study, n (%) | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 122 (96.8) | 131 (99.2) |
Entered open-label study, n (%) | 52 (100.0) | 55 (100.0) | 86 (97.7) | 86 (98.9) | 121 (96.0) | 130 (98.5) |
ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; TEZ = tezacaftor.
Exposure to Study Treatments
Study Treatments
Patient exposure to the study drugs is summarized in Table 18.
The median treatment duration was 24 weeks in Study 102 and Study 109, 4 weeks in Study 103, and 8 weeks in Study 104.7-10 Adherence with the study treatments was evaluated by counting the number of study drugs at each visit and was reported to be 99.2% in Study 102, 100% in Study 103, 99.8% in Study 109, and 99.6% in Study 104.7-10
Table 18: Summary of Exposure to the Study Drugs
Exposure | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 201 | ELX-TEZ-IVA N = 202 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Total exposure | ||||||||
Patient weeks | 4,758.7 | 4,761.3 | 204.7 | 221.3 | 2,074.1 | 2,062.7 | 993.4 | 1,050.4 |
Exposure duration (weeks) | ||||||||
Mean (SD) | 23.7 (2.39) | 23.6 (2.62) | 3.9 (0.42) | 4.0 (0.37) | 23.6 (2.2) | 23.7 (1.9) | 7.9 (0.9) | 8.0 (0.7) |
Median (range) | 24.0 (0.3, 25.1) | 24.0 (1.0, 25.1) | 4.0 (3.1, 4.7) | 4.0 (3.3, 4.9) | 24.0 (7.3, 24.9) | 24.0 (6.7, 24.7) | 8.0 (1.3, 9.1) | 8.0 (0.6, 9.0) |
ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; SD = standard deviation; TEZ = tezacaftor.
Concomitant Therapies
Prior and concomitant medications that were used by at least 20% of patients in the included studies are summarized in Table 19. The most commonly used concomitant medications included: mucolytics (inhaled sodium chloride and dornase alfa); bronchodilators (fluticasone propionate, salmeterol xinafoate, salbutamol); antibiotics (ciprofloxacin, sulfamethoxazole/trimethoprim, azithromycin, tobramycin, aztreonam lysine, colistimethate sodium); pancreatic enzymes (pancreatin and pancrelipase); vitamin supplementals (tocopherol and cholecalciferol); proton pump inhibitors (omeprazole); and bile acid (ursodeoxycholic acid).7-10
Patients With F/MF Genotype
A larger percentage of patients in the ELX-TEZ-IVA group were using inhaled sodium chloride compared with the placebo group (81.5% versus 74.9%).7 Three antibiotics were more commonly used in the placebo group compared with the ELX-TEZ-IVA group: tobramycin (55.7% versus 39.0%), ciprofloxacin (35.0% versus 16.0%), and trimethoprim/sulfamethoxazole (26.1% versus 17.0%).7
Patients With F/F Genotype
Study 103 and Study 109 had the smallest sample sizes of the 4 included studies and showed the greatest number of imbalances in the use of concomitant medications across the treatment groups.8,10 In Study 103, a greater percentage of patients in the ELX-TEZ-IVA group received treatment with salbutamol (65.5% versus 59.6%), azithromycin (58.2% versus 46.2%), ursodeoxycholic acid (27.3% versus 19.2%), and fluticasone propionate/salmeterol xinafoate (25.5% versus 17.3%) compared with the TEZ-IVA group.8 Compared with the ELX-TEZ-IVA group, a greater percentage of patients in the TEZ-IVA group received treatment with inhaled sodium chloride (82.7% versus 74.5%), fluticasone propionate (34.6% versus 29.1%), and omeprazole (28.8% versus 18.2%).8 In Study 109, a greater percentage of patients in the ELX-TEZ-IVA group received treatment with aztreonam lysine (25.3% versus 18.2%) and colistimethate sodium (41.4% versus 31.8%) compared with the TEZ-IVA group. Compared with the ELX-TEZ-IVA group, a greater percentage of patients in the TEZ-IVA group received treatment with dornase alfa (81.8% versus 71.3%), tobramycin (40.9% and 29.9%), cholecalciferol (31.8% versus 25.3%), and ciprofloxacin (33.0% versus 17.2%).10
Patients With F/G or F/RF Genotypes
The prior and concomitant medications used in Study 104 were well-balanced across the ELX-TEZ-IVA and the control group.9 As shown in Table 19, the percentage of patients using some concomitant medications was considerably lower in Study 104 compared with the other included trials. These included dornase alfa (52.7% in Study 104 versus 81.6% in Study 102, 92.5% in Study 103, and 76.6% in Study 109); inhaled sodium chloride (51.9% in Study 104 versus 78.2% in Study 102, 78.5% in Study 103, and 75.4% in Study 109); and pancreatin (51.9% in Study 104 versus 63.5% in Study 102, 65.4% in Study 103, and 93.7% in Study 109).7-10
Table 19: Concomitant Medications Used by at Least 20% of Patients
Concomitant medication, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
≥ 1 medication | 203 (100.0) | 200 (100.0) | 52 (100.0) | 55 (100.0) | 88 (100.0) | 87 (100.0) | 126 (100.0) | 132 (100.0) |
Dornase alfa | 165 (81.3) | 164 (82.0) | 48 (92.3) | 51 (92.7) | 72 (81.8) | 62 (71.3) | 66 (52.4) | 70 (53.0) |
Sodium chloride | 152 (74.9) | 163 (81.5) | 43 (82.7) | 41 (74.5) | 67 (76.1) | 65 (74.7) | 66 (52.4) | 68 (51.5) |
Salbutamol | 154 (75.9) | 152 (76.0) | 31 (59.6) | 36 (65.5) | 57 (64.8) | 57 (65.5) | 72 (57.1) | 80 (60.6) |
Pancreatin | 130 (64.0) | 126 (63.0) | 33 (63.5) | 37 (67.3) | 84 (95.5) | 80 (92.0) | 51 (40.5) | 49 (37.1) |
Azithromycin | 118 (58.1) | 111 (55.5) | 24 (46.2) | 32 (58.2) | 47 (53.4) | 48 (55.2) | 58 (46.0) | 57 (43.2) |
Tobramycin | 113 (55.7) | 78 (39.0) | 17 (32.7) | 15 (27.3) | 36 (40.9) | 26 (29.9) | NR | NR |
Cholecalciferol | 87 (42.9) | 89 (44.5) | 19 (36.5) | 20 (36.4) | 28 (31.8) | 22 (25.3) | 38 (30.2) | 44 (33.3) |
Pancrelipase | 62 (30.5) | 62 (31.0) | 16 (30.8) | 15 (27.3) | NR | NR | NR | NR |
Ibuprofen | 58 (28.6) | 62 (31.0) | NR | NR | 16 (18.2) | 22 (25.3) | NR | NR |
Aztreonam lysine | 63 (31.0) | 56 (28.0) | 13 (25.0) | 12 (21.8) | NR | NR | NR | NR |
Acetaminophen | 58 (28.6) | 58 (29.0) | NR | NR | 31 (35.2) | 27 (31.0) | NR | NR |
Ciprofloxacin | 71 (35.0) | 32 (16.0) | NR | NR | 29 (33.0) | 15 (17.2) | NR | NR |
Ursodeoxycholic acid | 43 (21.2) | 56 (28.0) | 10 (19.2) | 15 (27.3) | 27 (30.7) | 28 (32.2) | NR | NR |
Fluticasone propionate and salmeterol xinafoate | 51 (25.1) | 42 (21.0) | 9 (17.3) | 14 (25.5) | 18 (20.5) | 20 (23.0) | NR | NR |
Fluticasone | 45 (22.2) | 46 (23.0) | 18 (34.6) | 16 (29.1) | NR | NR | NR | NR |
Omeprazole | 47 (23.2) | 44 (22.0) | 15 (28.8) | 10 (18.2) | 24 (27.3) | 26 (29.9) | NR | NR |
Sulfamethoxazole/trimethoprim | 53 (26.1) | 34 (17.0) | NR | NR | NR | NR | NR | NR |
Salbutamol | 44 (21.7) | 38 (19.0) | NR | NR | NR | NR | NR | NR |
Tocopherol | NR | NR | NR | NR | 21 (23.9) | 20 (23.0) | NR | NR |
Colistimethate sodium | NR | NR | NR | NR | 28 (31.8) | 36 (41.4) | NR | NR |
ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; TEZ = tezacaftor.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. See Appendix 3 for detailed efficacy data.
Forced Expiratory Volume in 1 Second
Patients With F/MF Genotype
Treatment with ELX-TEZ-IVA was associated with a statistically significant increase from baseline in ppFEV1 compared with placebo at 4 weeks (13.8%; 95% CI, 12.1 to 15.4; P < 0.0001) and 24 weeks (14.3%; 95% CI, 12.7 to 15.8; P < 0.0001). As shown in Figure 6, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study. Results of the sensitivity analyses using MMRM with multiple imputation were consistent with the result of the primary analysis (Table 20).7
Results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses, including those based on age (12 to < 18 years or ≥ 18 years) and ppFEV1 at screening (< 70% or ≥ 70%) (Table 75).7 The sponsor conducted an additional post hoc subgroup analysis for the subset of patients with a ppFEV1 below 40% at baseline (16 out of 203 [7.9%] in the placebo group and 18 out of 200 [9.0%] in the ELX-TEZ-IVA group). Treatment with ELX-TEZ-IVA was associated with an improvement in absolute change in ppFEV1 at 4 weeks (LSMD = 15.2%; 95% CI, 7.3 to 23.1) and through 24 weeks (LSMD = 18.4%; 95% CI, 11.5 to 25.3).7 Complete details regarding these subgroup analyses in patients with advanced lung disease are provided in Table 76.
Figure 6: Absolute Change from Baseline in ppFEV1 in F/MF Genotype
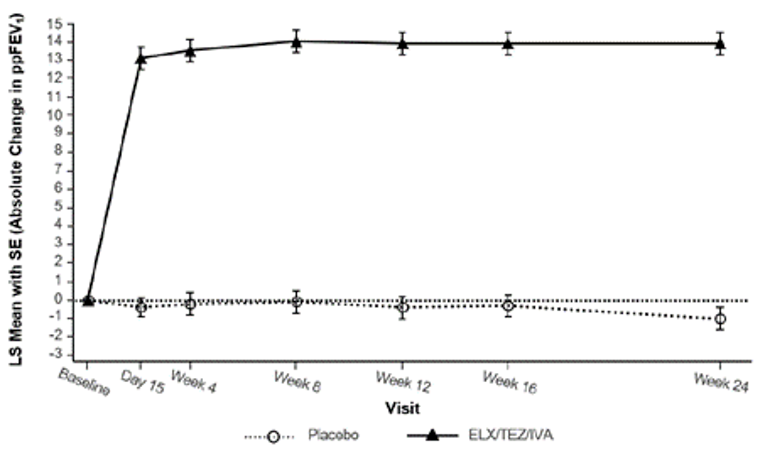
F/MF = heterozygous for F508del mutation with 1 minimal function mutation; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Source: Product Monograph.30
Table 20: Absolute Change From Baseline in ppFEV1 in F/MF Genotype
Parameters | Study 102 (F/MF) | |
|---|---|---|
Placebo (N = 203) | ELX-TEZ-IVA (N = 200) | |
Absolute change from baseline at 4 weeksa | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | –0.2 (0.6) | 13.6 (0.6) |
Patients in analysis, n | 188 | 185 |
LSMD (95% CI) | 13.8 (12.1 to 15.4) | |
P value (vs. placebo) | < 0.0001b | |
Absolute change from baseline at 4 weeks (multiple imputation)a | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | –0.2 (0.6) | 13.6 (0.6) |
Patients in analysis, n | 203 | 200 |
LSMD (95% CI) | 13.8 (12.2 to 15.5) | |
P value (vs placebo) | < 0.0001 | |
Absolute change from baseline through 24 weeksc | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | –0.4 (0.5) | 13.9 (0.6) |
Patients in analysis, n | 203 | 196 |
LSMD (95% CI) | 14.3 (12.7 to 15.8) | |
P value (vs. placebo) | < 0.0001d | |
Absolute change from baseline through 24 weeks (multiple imputation)b | ||
Baseline mean (SD) | 61.3 (15.5) | 61.6 (15.0) |
LS mean change (SE) | –0.4 (0.5) | 13.8 (0.5) |
Patients in analysis | 203 | 200 |
LSMD (95% CI) | 14.3 (12.8 to 15.8) | |
P value (vs. placebo) | < 0.0001 | |
CI = confidence interval; ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor; vs. = versus.
aMMRM included data from the day 15 and week 4 visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age), and sex (male, female) as covariates. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used, including all the data up to week 4. Missing ppFEV1 assessments were imputed only for visits of which all subsequent visits through week 4 were also missing (i.e., missing values that fall between 2 non-missing ones were not imputed).
bPre-specified primary end point.
cMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18, ≥ 18 years of age), and sex (male, female) as covariates. However, the day 15 visit was not included in the estimation of the average treatment effect through week 24. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used. Missing ppFEV1 assessments were imputed only for visits of which all subsequent visits through week 24 were also missing (i.e., missing values that fall between 2 non-missing ones were not imputed).
dPre-specified key secondary end point.
Source: Clinical Study Report.7
Patients With F/F Genotype
Absolute change from baseline in ppFEV1 at 4 weeks was primary end point of Study 103. Treatment with ELX-TEZ-IVA was associated with a statistically significant increase from baseline in ppFEV1 compared with TEZ-IVA at 4 weeks (10.0%; 95% CI, 7.4 to 12.6; P < 0.0001) (Table 21).7 As shown in Figure 7, improvements in ppFEV1 with ELX-TEZ-IVA were observed at the time of the first post-baseline assessment (i.e., day 15) and were higher at all time points throughout the study.7 Results of the sensitivity analyses using MMRM with multiple imputation were consistent with the result of the primary analysis (LSMD = 9.3%; 95% CI, 6.8 to 11.7).7 The results for change from baseline in ppFEV1 were generally consistent across all subgroup analyses; however, there the CIs for the analyses of subgroups with small sample sizes, such as ages 12 to 18 years, were wide (Table 77).7 The European Medical Association (EMA) reported the results of an additional post hoc subgroup analysis from Study 103 (CFTR modulator naive [n = 41] versus treatment-experienced [n = 66]). The observed treatment effect was 7.8% (95% CI, 4.8 to 10.8) for CFTR modulator-experienced patients and 13.2% (95% CI, 8.5 to 17.9) for CFTR modulator-naive patients.48,61
Absolute change from baseline in ppFEV1 through 24 weeks was a pre-specified key secondary end point of Study 109. Treatment with ELX-TEZ-IVA was associated with a statistically significant absolute increase from baseline in ppFEV1 compared with TEZ-IVA through 24 weeks (LSMD = 10.2%; 95% CI, 8.2 to 12.1; P < 0.0001) (Table 21).10 Results of the sensitivity analyses using MMRM with multiple imputation were consistent with the result of the primary analysis (LSMD = 10.1%; 95% CI, 8.2 to 11.9).10 Subgroup analyses were not conducted for change from baseline in ppFEV1 in Study 109.10
Figure 7: Absolute Change From Baseline in ppFEV1 in F/F Genotype
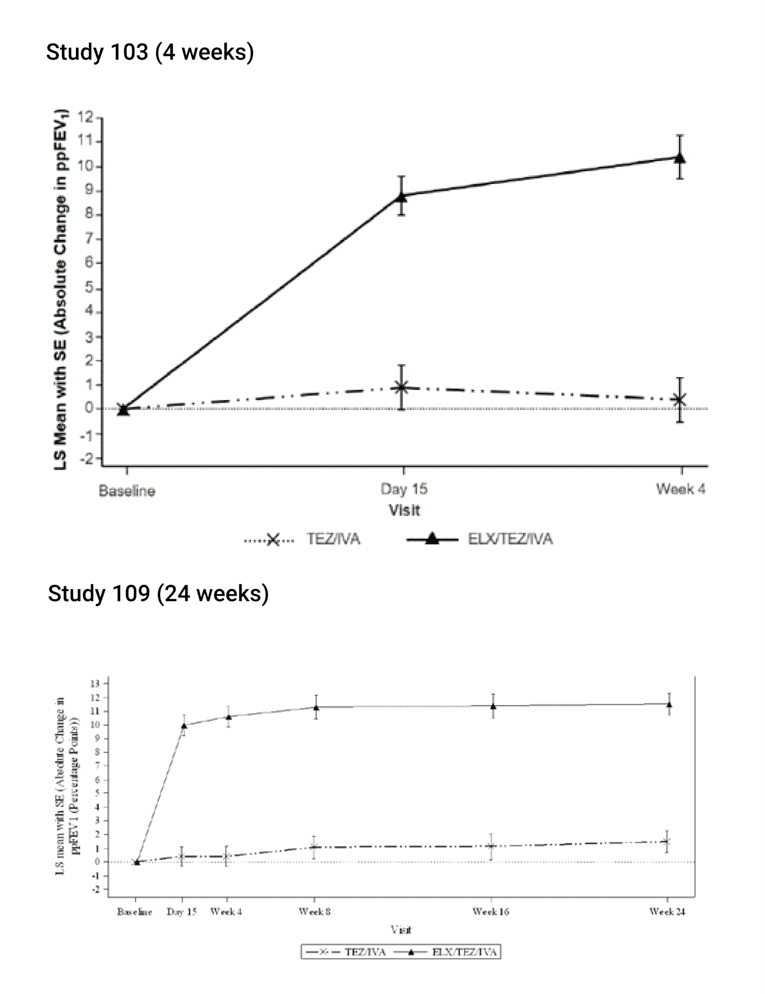
ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/F = homozygous for F508del mutation; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; TEZ/IVA = tezacaftor/ivacaftor + ivacaftor.
Table 21: Absolute Change From Baseline in ppFEV1 in F/F Genotype
Parameters | Study 103 (F/F) at 4 weeks | Study 109 (F/F) through 24 weeks | ||
|---|---|---|---|---|
TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | |
Absolute change from baseline at 4 weeksa or 24 weeksb | ||||
Baseline mean (SD) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) |
LS mean change (SE) | 0.4 (0.9) | 10.4 (0.9) | 1.0 (0.7) | 11.2 (0.7) |
Patients in analysis, n | 49 | 53 | 87 | 86 |
LSMD (95% CI) | 10.0 (7.4 to 12.6) | 10.2 (8.2 to 12.1) | ||
P value (vs. TEZ-IVA) | < 0.0001c | < 0.0001d | ||
Absolute change from baseline at 4 weeksa or 24 weeks (multiple imputation)b | ||||
Baseline mean (SD) | 60.2 (14.4) | 61.6 (15.4) | 64.2 (15.1) | 63.0 (16.7) |
LS mean change (SE) | 0.6 (0.9) | 9.9 (0.9) | 1.3 (0.6) | 11.3 (0.7) |
Patients in analysis, n | 52 | 55 | 88 | 87 |
LSMD (95% CI) | 9.3 (6.8 to 11.7) | 10.1 (8.2 to 11.9) | ||
P value (vs. TEZ-IVA) | < 0.0001 | < 0.0001 | ||
CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor; vs. = versus.
aMMRM included data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1 and age group at the screening visit (< 18, ≥ 18 years of age) as covariates. For the multiple imputation sensitivity analysis, the same MMRM as the primary analysis was used, including all the data up to week 4. Missing ppFEV1 assessments were imputed only for visits of which all subsequent visits through week 4 were also missing (i.e., missing values that fall between 2 non-missing ones were not imputed).
bThe MMRM included data collected in clinic from all available visits up to week 24 with treatment, visit, and treatment-by-visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR modulator use at screening (yes vs. no) were covariates.
cPre-specified primary end point.
dPre-specified key secondary end point.
Patients With F/G and F/RF Genotypes
The primary end point of Study 104 was absolute change in baseline in ppFEV1 through 8 weeks for the ELX-TEZ-IVA group (i.e., within-group change from baseline).9 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 through 8 weeks (LS mean change = 3.7%; 95% CI, 2.8 to 4.6; P < 0.0001) (Table 22).9 Results of the sensitivity analyses using MMRM with multiple imputation were consistent with the result of the primary analysis. An additional pre-specified analysis was performed that included spirometry assessed independently by the patients at home (due to the COVID-19 pandemic) and the results were similar to the primary analysis (LSMD = 3.8; 95% CI, 2.9 to 4.7).9
Absolute change from baseline in ppFEV1 through 8 weeks in the ELX-TEZ-IVA group compared to the control group was a pre-specified key secondary end point of Study 104.9 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in ppFEV1 compared to the control group (LSMD = 3.5%; 95% CI, 2.2 to 4.7; P < 0.0001) (Table 22).9 Similar results were obtained with a sensitivity analyses using MMRM with multiple imputation (LSMD = 3.6%; 95% CI, 2.3 to 4.8; P < 0.0001).9
Subgroup analyses based on the comparator group (i.e., patient genotype) demonstrated improvements in ppFEV1 through 8 weeks with ELX-TEZ-IVA versus IVA (LSMD = 5.8; 95% CI, 3.5 to 8.0) and a smaller effect versus TEZ-IVA (LSMD = 2.0; 95% CI, 0.5 to 3.4).
Table 22: Absolute Change From Baseline in ppFEV1 in F/G or F/RF Genotypes
Parameters | Study 104 (F/G or F/RF) | Study 104 (F/G) | Study 104 (F/RF) | |||
|---|---|---|---|---|---|---|
Control N = 126 | ELX-TEZ-IVA N = 132 | IVA N = 45 | ELX-TEZ-IVA N = 50 | TEZ-IVA N = 81 | ELX-TEZ-IVA N = 82 | |
Absolute change from baseline in ppFEV1 through 8 weeksa | ||||||
Baseline mean (SD) | 68.1 (16.4) | 67.1 (15.7) | 68.1 (16.6) | 66.0 (14.8) | 68.1 (16.4) | 67.8 (16.3) |
Patients in analysis, n | 114 | 115 | 42 | 42 | 72 | 73 |
LS mean change (SE) | 0.2 (0.5) | 3.7 (0.5) | 0.1 (0.9) | 5.8 (0.8) | 0.5 (0.5) | 2.5 (0.5) |
LSMD (95% CI) | 3.5 (2.2 to 4.7) | 5.8 (3.5 to 8.0) | 2.0 (0.5 to 3.4) | |||
P value (vs. control) | < 0.0001b | < 0.0001 | 0.0093 | |||
CI = confidence interval; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
aPre-specified key secondary end point.
bA similar MMRM method as for the primary analysis was applied to each subgroup category, with treatment, visit, and treatment-by-visit as fixed effects and baseline ppFEV1 and baseline SwCl as covariates.
Figure 8: Absolute Change From Baseline in ppFEV1 in F/G or F/RF Genotypes
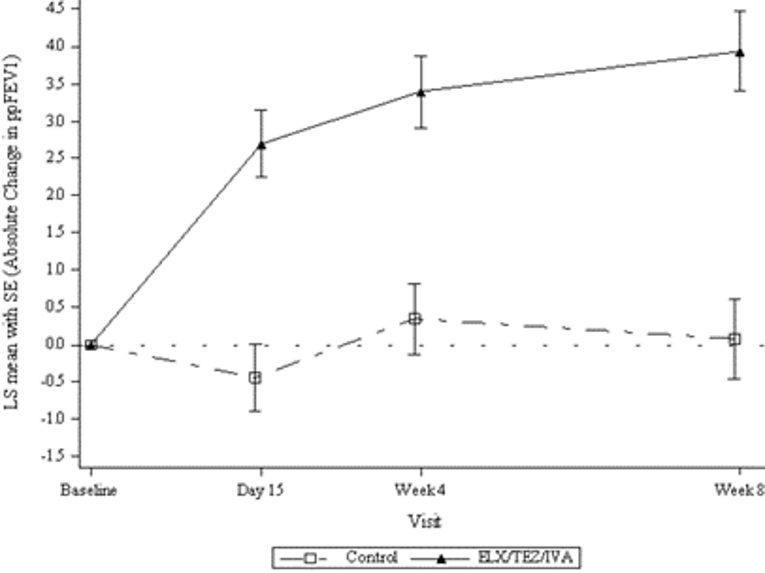
ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error.
Source: Clinical Study Report.9
Pulmonary Exacerbations
Patients With F/MF Genotype
In Study 102, treatment with ELX-TEZ-IVA was associated with a lower rate of the pulmonary exacerbations compared with placebo (rate ratio = 0.37; 95% CI, 0.25 to 0.55).7 Similarly, treatment with ELX-TEZ-IVA was associated with lower rates of pulmonary exacerbations requiring hospitalization (0.29; 95% CI, 0.14 to 0.61) and pulmonary exacerbations requiring IV antibiotic therapy (0.22; 95% CI, 0.11 to 0.43) (Table 23).7
Table 23: Risk of Pulmonary Exacerbations in F/MF Genotype
Pulmonary exacerbations | Study 102 (F/MF) | |
|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | |
Any pulmonary exacerbationa | ||
Patients with events, n (%) | 76 (37.4) | 31 (15.5) |
Number of events, n | 113 | 41 |
Event rate per year | 0.98 | 0.37 |
Rate ratio (95% CI) | 0.37 (0.25 to 0.55) | |
P value | < 0.0001a | |
Pulmonary exacerbation requiring hospitalizationb | ||
Patients with events, n (%) | 27 (13.3) | 7 (3.5) |
Number of events, n | 32 | 9 |
Event rate per year | 0.24 | 0.07 |
Rate ratio (95% CI) | 0.29 (0.14 to 0.61) | |
P value | 0.0010 | |
Pulmonary exacerbation requiring IV antibioticsb | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Number of events, n | 51 | 11 |
Event rate per year | 0.36 | 0.08 |
Rate ratio (95% CI) | 0.22 (0.11 to 0.43) | |
P values | < 0.0001 | |
Pulmonary exacerbation requiring hospitalization or IV antibioticsb | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Number of events | 52 | 11 |
Event rate per year | 0.37 | 0.08 |
Rate ratio (95% CI) | 0.22 (0.11 to 0.42) | |
P value | < 0.0001 | |
CI = confidence interval; ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IV = IV; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor; vs. = versus.
aPre-specified key secondary end point.
bTreatment comparison was carried out using a negative binomial regression model with treatment as a fixed effect; baseline ppFEV1, age at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates; and the logarithm of the patient-specific pulmonary exacerbation analysis period duration in years as the offset. The event rate was calculated based on 336 days (48 weeks) in a year. As the negative binomial regression model did not converge for pulmonary exacerbations requiring hospitalization, a Poisson model with the same structure was used.
Source: Clinical Study Report.7
Data for time-to-first pulmonary exacerbation are summarized in Table 24. HRs favoured ELX-TEZ-IVA compared with placebo for time-to-first pulmonary exacerbation (HR = 0.34; 95% CI, 0.22 to 0.52), time-to-first pulmonary exacerbation requiring hospitalization (HR = 0.25; 95% CI, 0.11 to 0.58), time-to-first pulmonary exacerbation requiring IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.39), and time-to-first pulmonary exacerbation requiring hospitalization or IV antibiotics (HR = 0.19; 95% CI, 0.09 to 0.39).7 For all end points related to pulmonary exacerbations, the results demonstrated statistically significant differences in favour of ELX-TEZ-IVA.
Table 24: Time-to-First PEx in F/MF Genotype
Parameters | Study 102 (F/MF) | |
|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | |
Time-to-first PExa | ||
Patients with events, n (%) | 76 (37.4) | 31 (15.5) |
Hazard ratio, (95% CI) | 0.34 (0.22 to 0.52) | |
P value | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.629 (0.558 to 0.692) | 0.842 (0.783 to 0.886) |
P value from log-rank test | < 0.0001 | |
Time-to-first PEx requiring hospitalizationa | ||
Patients with events, n (%) | 27 (13.3) | 7 (3.5) |
Hazard ratio (95% CI) | 0.25 (0.11 to 0.58) | |
P value vs. placebo | 0.0011 | |
Probability of event-free survival 24 weeks (95% CI) | 0.867 (0.812 to 0.907) | 0.965 (0.927 to 0.983) |
P value from log-rank test | 0.0004 | |
Time-to-first PEx requiring IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | |
P value vs. placebo | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.793 (0.731 to 0.843) | 0.955 (0.915 to 0.976) |
P value vs. placebo | < 0.0001 | |
Time-to-first PEx requiring hospitalization or IV antibioticsa | ||
Patients with events, n (%) | 42 (20.7) | 9 (4.5) |
Hazard ratio (95% CI) | 0.19 (0.09 to 0.39) | |
P value vs. placebo | < 0.0001 | |
Probability of event-free survival 24 weeks (95% CI) | 0.793 (0.731 to 0.843) | 0.955 (0.915 to 0.976) |
P value vs. placebo | < 0.0001 | |
CI = confidence interval; ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IV = IV; IVA = ivacaftor; PEx = pulmonary exacerbation; TEZ = tezacaftor; vs. = versus.
aHazard ratio and P value were calculated using Cox proportional hazard regression, with time-to-first PEx or censoring as the time, treatment as factor, and baseline ppFEV1, age at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates. Probability of event-free survival was estimated using Kaplan–Meier methods.
Source: Clinical Study Report.7
Figure 9: Time-to-First Pulmonary Exacerbation in F/MF Genotype
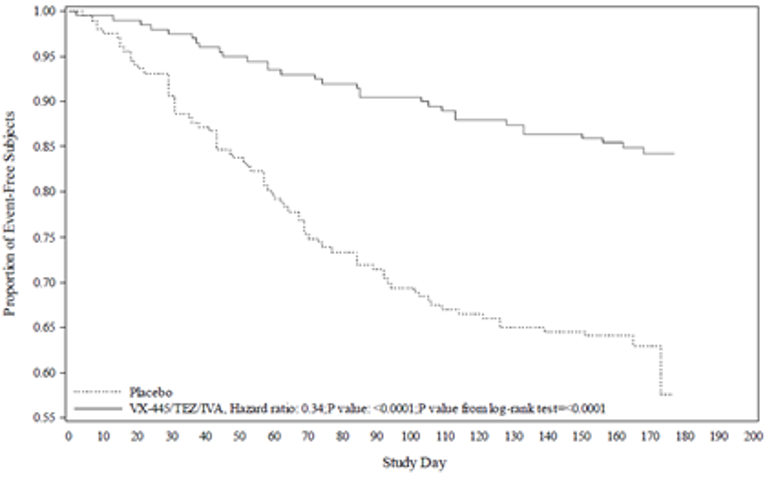
F/MF = heterozygous for F508del mutation with 1 minimal function mutation; VX-445/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Source: Clinical Study Report.7
Table 25 provides a summary of the annualized duration of pulmonary exacerbations in Study 102 for the placebo and ELX-TEZ-IVA groups. Compared with placebo, treatment with ELX-TEZ-IVA was associated with a reduced duration of pulmonary exacerbations (mean [SD] = 24.9 [44.7] versus 6.3 [16.9] days; P < 0.0001), pulmonary exacerbations requiring hospitalization (mean [SD] = 9.9 [30.7] versus 1.6 [9.1]; P = 0.0002), pulmonary exacerbations requiring IV antibiotics (mean [SD]: 14.3 [35.0] versus 1.9 [9.5]; P < 0.0001), and pulmonary exacerbations requiring IV antibiotics or hospitalization (mean [SD]: 14.5 [35.3] versus 1.9 [9.5]; P < 0.0001).
Table 25: Duration of PExs in F/MF Genotype
Parameters | Study 102 (F/MF) | |
|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | |
Annualized duration of PExa | ||
Mean (SD) | 24.9 (44.7) | 6.3 (16.9) |
Median (range) | 0.0 (0.0 to 248.0) | 0.0 (0.0 to 90.9) |
P value vs. placebo | < 0.0001 | |
Annualized duration of PEx requiring hospitalizationa | ||
Mean (SD) | 9.9 (30.7) | 1.6 (9.1) |
Median (range) | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) |
P value vs. placebo | 0.0002 | |
Annualized duration of PEx requiring IV antibioticsa | ||
Mean (SD) | 14.3 (35.0) | 1.9 (9.5) |
Median (range) | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) |
P value vs. placebo | < 0.0001 | |
Annualized duration of PEx requiring IV antibiotics or hospitalizationa | ||
Mean (SD) | 14.5 (35.3) | 1.9 (9.5) |
Median (range) | 0.0 (0.0 to 214.7) | 0.0 (0.0 to 80.0) |
P value vs. placebo | < 0.0001 | |
ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IV = IV; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation TEZ = tezacaftor; vs. = versus.
aAnnualized duration is equal to the total number of days with the corresponding event multiplied by 336 and divided by the total duration of the PEx analysis period in days. For analysis purposes; 1 year is defined as 48 weeks or 336 days. P values were based on a stratified (ppFEV1 group at screening [< 70% vs. ≥ 70%], age group at screening [≥ 12 to < 18 vs. ≥ 18 years], sex [male vs. female]) Wilcoxon rank sum test.
Source: Clinical Study Report.7
Patients With F/F Genotype
Pulmonary exacerbations were only captured as AEs in Study 103 and Study 109.8,10 The percentage of patients with at least 1 pulmonary exacerbation was greater in the TEZ-IVA group compared with the ELX-TEZ-IVA group in both Study 103 (11.5% versus 1.8%) and Study 109 (40.9% versus 11.5%).8,10
Patients With F/G and F/RF Genotypes
Pulmonary exacerbations were only captured as AEs in Study 104.9 Compared with the control group, fewer ELX-TEZ-IVA-treated patients reported at least 1 pulmonary exacerbation (10.3% versus 2.3%).9
BMI and Body Weight
Patients With F/MF Genotype
Study 102 included change from baseline in BMI at 24 weeks as a key secondary end point. Change from baseline in BMI z score (for patients < 20 years of age) and change from baseline in body weight at 24 weeks were pre-specified non-key secondary end points.7 Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in BMI at 24 weeks compared with placebo (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23; P < 0.0001) (Table 26).7 In patients aged 20 years or younger (n = 145), those treated with ELX-TEZ-IVA demonstrated improvements in BMI z score compared with placebo (LSMD = 0.30; 95% CI, 0.17 to 0.43).7 Similarly, the ELX-TEZ-IVA group demonstrated greater improvement in body weight at 24 weeks compared with the placebo group (LSMD = 2.9 kg; 95% CI, 2.3 to 3.4).7
Patients With F/F Genotype
Study 103 included absolute change from baseline in BMI and body weight as exploratory end points (Table 26). Compared with TEZ-IVA, treatment with ELX-TEZ-IVA was associated with improvements in BMI at 4 weeks (LSMD = 0.60 kg/m2; 95% CI, 0.41 to 0.79) and body weight at 4 weeks (LSMD = 1.6 kg; 95% CI, 1.0 to 2.1).8 Change from baseline in BMI and body weight were not pre-specified end points for Study 109 or reported in the clinical study report; however, post hoc analyses for these end points were conducted and included in the sponsor’s indirect treatment comparison (ITC).
Patients With F/G and F/RF Genotypes
Study 104 included absolute change from baseline in BMI at 8 weeks as an additional end point with no statistical analysis performed.9 At 8 weeks, mean BMI had increased in both the control group (LS mean = 0.16 kg/m2; SE = 0.06) and the ELX-TEZ-IVA group (LS mean = 0.28 kg/m2; SE = 0.06; LSMD = 0.13 kg/m2; 95% CI, –0.03 to 0.29).9
Table 26: Absolute Change From Baseline in BMI, BMI z scores, and Body Weight
Parameters | Study 102 (F/MF) At 24 weeks | Study 103 (F/F) At 4 weeks | Study 104 (F/G and F/RF) At 8 weeks | |||
|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Absolute change from baseline in BMI (kg/m2) at 24 weeksa, 4 weeksa, and 8 weeksb | ||||||
N (all patients) | 203 | 200 | 52 | 55 | 126 | 132 |
Baseline mean (SD) | 21.31 (3.14) | 21.49 (3.07) | 21.88 (4.12) | 21.75 (3.19) | 24.05 (4.71) | 24.07 (4.72) |
LS mean change (SE) | 0.09 (0.07) | 1.13 (0.07) | –0.07 (0.07) | 0.53 (0.07) | 0.16 (0.06) | 0.28 (0.06) |
Patients in analysis, n | 202 | 198 | 52 | 55 | 107 | 110 |
LSMD (95% CI) | 1.04 (0.85 to 1.23) | 0.60 (0.41 to 0.79) | 0.13 (–0.03 to 0.29) | |||
P value | < 0.0001c | < 0.0001 | NA | |||
Absolute change from baseline in BMI z score at 24 weeksa | ||||||
N (patients < 20 years) | 74 | 71 | NA | NA | ||
Baseline mean (SD) | –0.40 (0.98) | –0.37 (0.79) | ||||
LS mean change (SE) | 0.04 (0.05) | 0.34 (0.05) | ||||
Patients in analysis | 68 | 64 | ||||
LSMD (95% CI) | 0.30 (0.17 to 0.43) | |||||
P value | < 0.0001d | |||||
Absolute change from baseline in body weight (kg) at 24 weeksa and 4 weeksa | ||||||
N (all patients) | 203 | 200 | 52 | 55 | NA | |
Baseline mean (SD) | 58.3 (12.7) | 59.8 (12.9) | 59.8 (14.8) | 59.9 (12.7) | ||
LS mean change (SE) | 0.5 (0.2) | 3.4 (0.2) | –0.1 (0.2) | 1.5 (0.2) | ||
Patients in analysis | 202 | 198 | 52 | 55 | ||
LSMD (95% CI) | 2.9 (2.3 to 3.4) | 1.6 (1.0 to 2.1) | ||||
P value | < 0.0001 | < 0.0001 | ||||
BMI = body mass index; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor; vs. = versus.
aMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18 vs. ≥ 18 years), and sex (male, female) as covariates.
bMMRM included data from all available visits up to week 8, with treatment, visit, and treatment-by-visit as fixed effects and baseline ppFEV1, baseline sweat chloride and, comparator group (IVA comparator group vs. TEZ-IVA comparator group) as covariates.
cPre-specified key secondary end point.
dPre-specified other secondary end point.
Cystic Fibrosis Questionnaire–Revised (RD)
Patients With F/MF Genotype
Study 102 included 2 key secondary end points related to absolute change from baseline in CFQ-R (RD) scores. Change from baseline through 24 weeks was the fourth key secondary end point and change from baseline at 4 weeks was the seventh and final key secondary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R (RD) score from baseline compared with placebo through 24 weeks (LSMD = 20.2; 95% CI, 17.5 to 23.0) and at week 4 (LSMD = 20.1; 95% CI, 16.9 to 23.2) (Table 27).
Patients With F/F Genotype
Study 103 included absolute change from baseline in CFQ-R (RD) score at 4 weeks as a key secondary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R (RD) score from baseline compared with TEZ-IVA at 4 weeks (LSMD = 17.4; 95% CI, 11.8 to 23.0) (Table 27).
Study 109 included absolute change from baseline in CFQ-R (RD) score through 24 weeks as the primary end point. Treatment with ELX-TEZ-IVA was associated with a statistically significant improvement in CFQ-R (RD) score from baseline compared with TEZ-IVA through 24 weeks (LSMD = 15.9; 95% CI, 11.7 to 20.1) (Table 27).10
Table 27: Absolute Change From Baseline in CFQ-R (Respiratory Domain) Scores for F/MF or F/F Patients
CFQ-R Respiratory Domain | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksa | Study 109 (F/F) through 24 weeksb | |||
|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | |
Absolute change from baseline in CFQ-R (Respiratory Domain) scores at 24 weeks and 4 weeks | ||||||
BL mean (SD) | 70.0 (17.8) | 68.3 (16.9) | 72.6 (17.9) | 70.6 (16.2) | 73.1 (17.6) | 71.2 (19.6) |
LS mean change (SE) | –2.7 (1.0) | 17.5 (1.0) | –1.4 (2.0) | 16.0 (2.0) | 1.2 (1.5) | 17.1 (1.5) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 88 | 87 |
LSMD (95% CI) | 20.2 (17.5 to 23.0) | 17.4 (11.8 to 23.0) | 15.9 (11.7 to 20.1) | |||
P value | < 0.0001c | < 0.0001 | < 0.0001d | |||
BL = baseline; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor.
aMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates.
bMMRM included CFQ-R Respiratory Domain data collected in clinic and at home from all available visits up to week 24 with treatment, visit, and treatment-by-visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR modulator use at screening (yes vs. no) were covariates.
cPre-specified key secondary end point.
dPre-specified primary end point.
Patients With F/G and F/RF Genotypes
In Study 104, the ELX-TEZ-IVA group demonstrated a statistically significant increase in CFQ-R (RD) score from baseline through 8 weeks (LS mean within group = 10.3 points; 95% CI, 8.0 to 12.7; P < 0.0001). Treatment with ELX-TEZ-IVA also resulted in an increase in CFQ-R (RD) score through 8 weeks compared to the control group (LSMD = 8.7; 95% CI, 5.3 to 12.1; P < 0.0001). As shown in Table 28, subgroup analyses demonstrated similar effect sizes for ELX-TEZ-IVA compared with IVA in patients with an F/G genotype (LSMD = 8.9; 95% CI, 3.8 to 14.0; P = 0.0008) and for ELX-TEZ-IVA compared with TEZ-IVA in patients with an F/RF genotype (LSMD = 8.5; 95% CI, 4.0 to 13.1; P = 0.0003).
Table 28: Absolute Change From Baseline in CFQ-R (Respiratory Domain) Scores for F/G or F/RF Patients
CFQ-R (respiratory domain) | Study 104 (F/G or F/RF) | Study 104 (F/RF subgroup) | Study 104 (F/G subgroup) | |||
|---|---|---|---|---|---|---|
Control N = 126 | ELX-TEZ-IVA N = 132 | TEZ-IVA N = 81 | ELX-TEZ-IVA N = 82 | IVA N = 45 | ELX-TEZ-IVA N = 50 | |
Absolute change from baseline in CFQ-R Respiratory Domain scores at 8 weeksa | ||||||
BL mean (SD) | 77.3 (15.8) | 76.5 (16.6) | 78.1 (14.7) | 76.7 (16.9) | 75.8 (17.6) | 76.3 (16.4) |
LS mean change (SE) | 1.6 (1.2) | 10.3 (1.2) | 1.9 (1.6) | 10.4 (1.6) | 1.3 (1.9) | 10.2 (1.8) |
Patients in analysis, n | 126 | 130 | 81 | 81 | 45 | 49 |
LSMD (95% CI) | 8.7 (5.3 to 12.1) | 8.5 (4.0 to 13.1) | 8.9 (3.8 to 14.0) | |||
P value (vs. comparator) | < 0.0001 | 0.0003 | 0.0008 | |||
BL = baseline; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
aMMRM included data from all available visits up to week 8, with treatment, visit, and treatment-by-visit as fixed effects and baseline ppFEV1, baseline SwCl, and comparator group (IVA or TEZ-IVA comparator group) as covariates.
Source: Clinical Study Report.9
Cystic Fibrosis Questionnaire–Revised (Non-Respiratory Domains)
Patients With F/MF Genotype
Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 102. As shown in Table 29, the change from baseline in the ELX-TEZ-IVA treatment group was greater than in the placebo group for the following CFQ-R domains: physical functioning, vitality, emotional state, body image, eating disturbances, treatment burden, health perceptions, weight, role limitations, and social limitations (i.e., all domains with the exception of digestion).
Patients With F/F Genotype
Changes from baseline in the non-respiratory domains of the CFQ-R were assessed as exploratory end points in Study 103.8 The change from baseline in the ELX-TEZ-IVA treatment group was greater than in the placebo group for the following CFQ-R domains: physical functioning, vitality, eating disturbances, health perceptions, weight, role limitations, and social limitations (Table 29).8 Changes from baseline in the non-respiratory domains of the CFQ-R were not assessed in Study 109.
Patients With F/G and F/RF Genotypes
No statistical analyses were performed for changes from baseline in the non-respiratory domains of the CFQ-R in Study 104 (descriptive statistics are summarized in Table 29).
Table 29: Absolute Change From Baseline in CFQ-R Non-Respiratory Domain Scores
Parameters | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksa | Study 104 (F/G or F/RF) through 8 weeksb | |||
|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Physical functioning | ||||||
Baseline mean (SD) | 76.4 (21.6) | 76.5 (21.7) | 76.3 (24.5) | 75.2 (24.0) | 76.5 (21.7) | 77.2 (20.6) |
LS mean change (SE) | –3.3 (0.9) | 9.2 (0.9) | –1.9 (1.9) | 9.9 (1.9) | 0.2 (1.0) | 4.4 (1.0) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 12.5 (9.9 to 15.0) | 11.8 (6.5 to 17.0) | 4.2 (1.4 to 7.0) | |||
P value (vs. comparator) | < 0.0001c | < 0.0001c | NA | |||
Vitality | ||||||
Baseline mean (SD) | 63.8 (18.3) | 62.8 (17.1) | 60.6 (19.9) | 61.4 (17.6) | 65.0 (18.9) | 66.0 (18.8) |
LS mean change (SE) | –5.3 (1.0) | 7.9 (1.0) | –3.6 (2.4) | 8.9 (2.3) | –0.4 (1.3) | 4.6 (1.3) |
Patients in analysis, n | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 13.1 (10.5 to 15.8) | 12.5 (6.0 to 19.0) | 5.0 (1.5 to 8.5) | |||
P value | < 0.0001c | 0.0002c | NA | |||
Emotional state | ||||||
Baseline mean (SD) | 80.2 (16.7) | 82.0 (16.0) | 80.3 (17.8) | 82.1 (14.7) | 78.9 (18.4) | 82.3 (16.3) |
LS mean change (SE) | –0.9 (0.7) | 2.5 (0.7) | 1.1 (1.2) | 2.9 (1.1) | –0.6 (0.9) | 1.0 (0.8) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 3.4 (1.5 to 5.2) | 1.8 (–1.4 to 5.1) | 1.6 (−0.8 to 4.0) | |||
P value | 0.0004c | 0.2727 | NA | |||
Body image | ||||||
Baseline mean (SD) | 77.2 (23.5) | 78.8 (22.1) | 86.1 (21.9) | 80.0 (20.7) | 81.1 (21.0) | 84.0 (20.0) |
LS mean change (SE) | 0.4 (1.0) | 4.2 (1.0) | –0.2 (1.5) | 2.2 (1.5) | 0.6 (1.0) | 0.5 (1.0) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 3.8 (1.2 to 6.5) | 2.4 (–1.7 to 6.6) | –0.1 (–3.0 to 2.7) | |||
P value | 0.0048c | 0.2496 | NA | |||
Eating disturbances | ||||||
Baseline mean (SD) | 89.1 (17.5) | 90.0 (17.9) | 90.0 (16.8) | 89.1 (19.8) | 92.1 (15.8) | 89.8 (19.1) |
LS mean change (SE) | –2.4 (0.8) | 2.5 (0.8) | −0.4 (2.0) | 6.4 (1.9) | –1.2 (1.0) | 1.5 (1.0) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 4.9 (2.6 to 7.1) | 6.8 (1.3 to 12.4) | 2.7 (–0.1 to 5.4) | |||
P value | < 0.0001 | 0.0155 | NA | |||
Treatment burden | ||||||
Baseline mean (SD) | 61.4 (20.2) | 59.2 (19.2) | 58.5 (21.5) | 59.4 (20.4) | 65.8 (21.3) | 69.0 (21.7) |
LS mean change (SE) | –2.0 (0.8) | 4.9 (0.8) | 0.3 (1.9) | 3.7 (1.9) | 2.4 (1.1) | 4.4 (1.1) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 6.8 (4.5 to 9.2) | 3.4 (–2.0 to 8.7) | 1.9 (–1.0 to 4.9) | |||
P value | < 0.0001c | 0.2153 | ||||
Health perceptions | ||||||
Baseline mean (SD) | 64.2 (20.1) | 63.5 (20.5) | 61.6 (23.2) | 63.5 (20.3) | 68.0 (20.6) | 69.3 (19.6) |
LS mean change (SE) | −4.4 (1.1) | 12.6 (1.1) | –0.5 (2.2) | 9.0 (2.0) | –0.9 (1.2) | 5.1 (1.2) |
Patients in analysis, n | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 17.0 (14.1 to 20.0) | 9.5 (3.6 to 15.4) | 6.0 (2.7 to 9.4) | |||
P value | < 0.0001c | 0.0018c | NA | |||
Weight | ||||||
Baseline mean (SD) | 74.1 (31.7) | 74.4 (31.0) | 81.8 (28.3) | 78.2 (33.0) | 89.1 (23.6) | 88.8 (24.3) |
LS mean change (SE) | 0.1 (1.7) | 13.2 (1.7) | −5.0 (3.2) | 7.5 (2.9) | 1.8 (1.5) | 2.0 (1.5) |
Patients in analysis, n | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 13.1 (8.3 to 17.9) | 12.5 (4.1 to 20.9) | 0.2 (−3.9 to 4.3) | |||
P value | < 0.0001c | 0.0041c | NA | |||
Digestion | ||||||
Baseline mean (SD) | 83.4 (16.9) | 83.1 (18.1) | 80.3 (22.7) | 83.0 (18.5) | 85.8 (14.1) | 85.7 (17.8) |
LS mean change (SE) | –0.4 (0.9) | 2.1 (0.9) | 0.2 (2.2) | 1.1 (2.1) | –1.2 (1.2) | –1.4 (1.2) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 2.5 (–0.1 to 5.1) | 0.9 (–5.1 to 6.9) | –0.3 (–3.6 to 3.0) | |||
P value | 0.0594 | 0.7634 | NA | |||
Role limitations | ||||||
Baseline mean (SD) | 83.3 (15.2) | 81.7 (17.5) | 79.0 (17.2) | 80.4 (19.9) | 84.2 (16.7) | 87.3 (17.4) |
LS mean change (SE) | –2.4 (0.8) | 4.4 (0.8) | 0.8 (1.8) | 6.8 (1.7) | 0.4 (1.2) | 0.7 (1.1) |
Patients in analysis, n | 179 | 185 | 44 | 49 | 122 | 123 |
LSMD (95% CI) | 6.8 (4.6 to 9.1) | 6.0 (1.1 to 10.9) | 0.3 (–2.9 to 3.5) | |||
P value | < 0.0001c | 0.0167c | NA | |||
Social limitations | ||||||
Baseline mean (SD) | 68.8 (17.9) | 70.5 (17.0) | 73.5 (16.3) | 67.9 (17.7) | 67.4 (20.3) | 69.7 (19.9) |
LS mean change (SE) | –1.3 (0.8) | 4.6 (0.8) | 1.5 (1.5) | 6.9 (1.5) | –2.0 (1.2) | 0.6 (1.2) |
Patients in analysis, n | 203 | 200 | 52 | 55 | 126 | 130 |
LSMD (95% CI) | 5.9 (3.7 to 8.0) | 5.4 (1.2 to 9.6) | 2.6 (–0.8 to 6.0) | |||
P value | < 0.0001c | 0.0131c | NA | |||
CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor; vs. = versus.
aMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates.
bMMRM included data from all available visits up to week 8, with treatment, visit, and treatment-by-visit as fixed effects and baseline ppFEV1, baseline sweat chloride, and comparator group (IVA comparator group vs. TEZ-IVA comparator group) as covariates.
cNo adjustment for multiplicity was performed; therefore, all P values are considered nominal.
Sweat Chloride
Patients with F/MF Genotype
Absolute change from baseline in sweat chloride at 4 weeks and 24 weeks were key secondary end points of Study 102. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the placebo group at 4 weeks (LSMD = –41.2 mmol/L; 95% CI, −44.0 to –38.5) and 24 weeks (LSMD = –41.8 mmol/L; 95% CI, –44.4 to –39.3) (Table 30).7
Table 30: Absolute Change From Baseline in SwCl in F/MF Patients
Parameters | Placebo N = 203 | ELX-TEZ-IVA N = 200 |
|---|---|---|
Absolute change from baseline in SwCl at 4 weeks (mmol/L)a | ||
Baseline mean (SD) | 102.9 (9.8) | 102.3 (11.9) |
LS mean change (SE) | 0.1 (1.0) | –41.2 (1.0) |
Patients in analysis, n | 196 | 193 |
LSMD (95% CI) | –41.2 (–44.0 to –38.5) | |
P value (vs. placebo) | < 0.0001b | |
Absolute change from baseline in SwCl through 24 weeks (mmol/L)a | ||
Baseline mean (SD) | 102.9 (9.8) | 102.3 (11.9) |
LS mean change (SE) | –0.4 (0.9) | –42.2 (0.9) |
Patients in analysis, n | 201 | 199 |
LSMD (95% CI) | –41.8 (–44.4 to –39.3) | |
P value (vs. placebo) | < 0.0001b | |
CI = confidence interval; ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ = tezacaftor.
aMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates.
bPre-specified key secondary end point.
Source: Clinical Study Report.7
Patients with F/F Genotype
Absolute change from baseline in sweat chloride at 4 weeks and through 24 weeks were key secondary end points of Study 103 and 109, respectively. The ELX-TEZ-IVA group demonstrated statistically significant reductions in sweat chloride compared with the TEZ-IVA group at 4 weeks (LSMD = –45.1 mmol/L; 95% CI, –50.1 to –40.1) in Study 103 and through 24 weeks in Study 109 (LSMD = –42.8; 95% CI, –46.2 to –39.3; P < 0.0001) (Table 31).8,10
Table 31: Absolute Change From Baseline in Sweat Chloride in F/F Genotype
Parameters | Study 103 (F/F) at 4 weeksa | Study 109 (F/F) through 24 weeksb | ||
|---|---|---|---|---|
TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | |
Baseline mean (SD) | 90.0 (12.3) | 91.4 (11.0) | 89.8 (11.7) | 89.0 (12.2) |
LS mean change (SE) | 1.7 (1.8) | –43.4 (1.7) | –3.4 (1.2) | –46.2 (1.3) |
Patients in analysis, n | 48 | 54 | 88 | 87 |
LSMD (95% CI) | –45.1 (–50.1 to –40.1) | –42.8 (–6.2 to –39.3) | ||
P value (vs. TEZ-IVA) | < 0.0001c | < 0.0001 | ||
CFTR = cystic fibrosis transmembrane conductance regulator; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TEZ = tezacaftor.
aMMRM included final data from all available visits, with treatment, visit, and treatment-by-visit interaction as fixed effects and baseline ppFEV1, age group at screening (< 18 vs. ≥ 18 years), and sex (male vs. female) as covariates.
bMMRM included data from all available visits up to week 24 with treatment, visit, and treatment-by-visit as fixed effects; baseline ppFEV1, age group at screening (≥ 12 to < 18 vs. ≥ 18 years), and CFTR modulator use at screening (yes vs. no) were covariates.
cPre-specified key secondary end point.
Patients With F/G and F/RF Genotypes
Absolute change from baseline in sweat chloride through 8 weeks within the ELX-TEZ-IVA group and compared with the control were key secondary end points of Study 104. The ELX-TEZ-IVA group demonstrated a statistically significant decrease in sweat chloride from baseline through 8 weeks (LS mean = –22.3 mmol/L; 95% CI, –24.5 to –20.2; P < 0.0001) (Table 32). Treatment with ELX-TEZ-IVA also resulted in a decrease in sweat chloride from baseline through 8 weeks compared to the control group (LSMD = –23.1 mmol/L; 95% CI, –26.1 to –20.1; P < 0.0001).9
Table 32: Absolute Change From Baseline in SwCl in F/G or F/RF Genotypes
Parameters | Patients with F/G or F/RF | Study 104 (F/RF subgroup) | Study 104 (F/G subgroup) | |||
|---|---|---|---|---|---|---|
Control N = 126 | ELX-TEZ-IVA N = 132 | TEZ-IVA N = 81 | ELX-TEZ-IVA N = 82 | IVA N = 45 | ELX-TEZ-IVA N = 50 | |
Absolute change from baseline in SwCl at 8 weeksa | ||||||
Baseline mean (SD) | 56.4 (25.5) | 59.5 (27.0) | 61.4 (27.3) | 64.7 (27.9) | 47.6 (19.1) | 50.9 (23.3) |
Patients in analysis, n | 119 | 120 | 75 | 77 | 44 | 43 |
LS mean change (SE) | 0.7 (1.1) | –22.3 (1.1) | 1.7 (1.3) | –23.1 (1.3) | –1.8 (2.0) | –21.8 (2.0) |
LSMD (95% CI) | –23.1 (–26.1 to –20.1) | –24.8 (–28.4 to –21.2) | –20.0 (–25.4 to –14.6) | |||
P value vs. control | < 0.0001 | < 0.0001 | < 0.0001 | |||
CI = confidence interval; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
aMMRM included data from all available visits up to week 8, with treatment, visit, and treatment-by-visit as fixed effects and baseline ppFEV1, baseline SwCl, and comparator group (IVA or TEZ-IVA comparator group) as covariates.
Source: Clinical Study Report.9
Treatment Satisfaction
The TSQM was included as an exploratory end point in Study 102 and Study 103 for patients between the ages of 12 and 17 years.
Patients With F/MF Genotype
As shown in Table 33, the ELX-TEZ-IVA group in Study 102 demonstrated improvements compared with the placebo group in the domains for global satisfaction (LSMD = 24.2; 95% CI, 13.6 to 34.9), side effects (LSMD = –4.6; 95% CI, –8.5 to –0.7), and effectiveness (LSMD = 23.2; 95% CI, 13.8 to 32.7).7
Patients With F/F Genotype
In Study 103, the ELX-TEZ-IVA group demonstrated improvements compared with the TEZ-IVA group in the domains for global satisfaction (LSMD = 11.9; 95% CI, 1.8 to 22.0]) and effectiveness (LSMD = 14.4; 95% CI, 3.5 to 25.4) (Table 33).8 The TSQM was not included as an end point in Study 109.10
Patients With F/G and F/RF Genotypes
The TSQM was not included as an end point in Study 104.9
Table 33: Absolute Change From Baseline in TSQM in F/MF and F/F Genotypes
Parameters | Study 102 (F/MF) through 24 weeksa | Study 103 (F/F) at 4 weeksb | ||
|---|---|---|---|---|
Placebo N = 60 | ELX-TEZ-IVA N = 56 | TEZ-IVA N = 14 | ELX-TEZ-IVA N = 16 | |
Global satisfaction | ||||
Baseline mean (SD) | 76.6 (16.4) | 72.1 (21.2) | 87.2 (8.9) | 78.1 (23.4) |
LS mean change (SE) | –8.9 (3.7) | 15.3 (3.9) | –1.0 (3.6) | 11.0 (3.4) |
Patients in analysis, n | 56 | 52 | 14 | 16 |
LSMD (95% CI) | 24.2 (13.6 to 34.9) | 11.9 (1.8 to 22.0) | ||
P value | < 0.0001c | 0.0222c | ||
Convenience | ||||
Baseline mean (SD) | 75.0 (16.4) | 72.9 (21.0) | 85.9 (10.5) | 82.6 (15.3) |
LS mean change (SE) | 6.6 (3.0) | 13.9 (3.1) | 1.7 (3.7) | 6.3 (3.5) |
Patients in analysis, n | 56 | 52 | 14 | 16 |
LSMD (95% CI) | 7.3 (–1.2 to 15.7) | 4.6 (–5.9 to 15.1) | ||
P value | 0.0914 | 0.3794 | ||
Side effects | ||||
Baseline mean (SD) | 98.7 (5.7) | 99.9 (0.9) | 99.1 (3.3) | 96.5 (8.8) |
LS mean change (SE) | –0.1 (1.3) | –4.7 (1.4) | 0.0 (2.5) | –3.5 (2.3) |
Patients in analysis, n | 57 | 52 | 14 | 16 |
LSMD (95% CI) | –4.6 (–8.5 to –0.7) | –3.4 (–10.4 to 3.6) | ||
P value | 0.0198c | 0.3255 | ||
Effectiveness | ||||
Baseline mean (SD) | 67.8 (20.9) | 68.9 (15.9) | 75.0 (12.3) | 71.5 (17.6) |
LS mean change (SE) | –9.5 (3.3) | 13.7 (3.4) | –0.9 (3.9) | 13.6 (3.6) |
Patients in analysis, n | 59 | 53 | 14 | 16 |
LSMD (95% CI) | 23.2 (13.8 to 32.7) | 14.4 (3.5 to 25.4) | ||
P value | < 0.0001c | 0.0116c | ||
ANCOVA = analysis of covariance; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IVA = ivacaftor; LS = least squares; LSMD = least squares mean difference; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; SE = standard error; TSQM = Treatment Satisfaction Questionnaire for Medication; TEZ = tezacaftor.
aANCOVA included data from week 24, with treatment as fixed effect and baseline ppFEV1 and sex (male vs. female) as covariates.
bANCOVA included data from week 4, with treatment as fixed effect and continuous baseline ppFEV1 as covariate.
cNo adjustment for multiplicity was performed; therefore, all P values are considered nominal.
Hospitalizations
Patients With F/MF Genotype
Table 34 provides a summary of the data for planned and unplanned hospitalizations for CF that were reported during Study 102.
Nine events of planned hospitalization for CF were reported for 7 (3.4%) patients in the placebo group compared with 1 event (0.5%) in the ELX-TEZ-IVA group (P = 0.0677). The annualized duration of planned hospitalizations for CF (mean [SD]) was lower in the ELX-TEZ-IVA group compared with the placebo group (0.1 [1.4] days versus 1.0 [7.4] days). There were 21 unplanned hospitalization events in the placebo group (17 patients [8.4%]) and 15 (13 patients [6.5%]) in the ELX-TEZ-IVA group. There was no statistically significant difference in the rate of unplanned hospitalizations for CF between the placebo and ELX-TEZ-IVA groups (rate ratio: 0.80; 95% CI, 0.38 to 1.70; P = 0.5592). There was no statistically significant difference between the ELX-TEZ-IVA and placebo groups for the annualized duration of unplanned hospitalizations for CF (mean [SD]: 1.0 [4.7] days versus 3.0 [12.6] days; P = 0.5724).7
Table 34: CF-Related Hospitalizations in F/MF Patients
Parameters | Placebo N = 203 | ELX-TEZ-IVA N = 200 |
|---|---|---|
Total number of days (years) | 34,187 (101.7) | 33,453 (99.6) |
Planned hospitalizations for CF | ||
Number of patients with events, n (%) | 7 (3.4) | 1 (0.5) |
Number of events | 9 | 1 |
Estimated event rate per yeara | NA | NA |
Rate ratio, 95% CI | NA | |
P value vs. placebo | 0.0677 | |
Unplanned hospitalizations for CF | ||
Number of patients with events, n (%) | 17 (8.4) | 13 (6.5) |
Number of events | 21 | 15 |
Estimated event rate per yearb | 0.19 | 0.15 |
Rate ratio, 95% CI | 0.80 (0.38 to 1.70) | |
P value vs. placebo | 0.5592 | |
Annualized duration of planned hospitalizations for CF | ||
Mean (SD) | 1.0 (7.4) | 0.1 (1.4) |
Median (range) | 0.0 (0.0 to 91.6) | 0.0 (0.0 to 19.9) |
P value vs. placeboc | 0.0218 | |
Annualized duration of unplanned hospitalizations for CF | ||
Mean (SD) | 3.0 (12.6) | 1.0 (4.7) |
Median (range) | 0.0 (0.0 to 81.1) | 0.0 (0.0 to 40.2) |
P value vs. placeboc | 0.5724 | |
CF = cystic fibrosis; CI = confidence interval; ELX = elexacaftor; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; IVA = ivacaftor; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation; TEZ = tezacaftor.
aIf the number of events was less than 5 in either treatment group, no model-based estimates were produced and the P value was be based on a Fisher exact test.
bAnalysis is based on negative binomial regression model: count = treatment + baseline ppFEV1 + age group at screening (≥ 12 to < 18 vs. ≥ 18 years) + sex (male vs. female), with log (duration of the analysis period in years) as offset.
cP values were based on a Wilcoxon rank sum test stratified by ppFEV1 group at screening (< 70% vs. ≥ 70%), age group at screening (≥ 12 to < 18 vs. ≥ 18 years), sex (male vs. female). No adjustment for multiplicity was performed; therefore, all P values are considered nominal.
Source: Clinical Study Report.7
Patients With F/F Genotype
Hospitalizations were only captured in the safety evaluations in Studies 103 and 109.8,10
Patients With F/G and F/RF Genotypes
Hospitalizations were only captured in the safety evaluation of Study 104.9
Harms
Only those harms identified in the review protocol are reported below.
Adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Placebo N = 201 | ELX-TEZ-IVA N = 202 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |||
At least 1 AE | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) | ||
WDAEs | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) | ||
AEs leading to interruption | 10 (5.0) | 19 (9.4) | 0 (0) | 0 (0) | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) | ||
Grade 3/4 AEs | 15 (7.5) | 19 (9.4) | 1 (1.9) | 0 (0) | 7 (8.0) | 7 (8.0) | 4 (3.2) | 5 (3.8) | ||
SAEs | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) | ||
AE = adverse event; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; SAE = serious adverse event; TEZ = tezacaftor; WDAE = withdrawal due to adverse event.
Adverse Events
Table 36 provides a summary of the most frequently reported AEs in the included studies (i.e., those occurring in at least 5% patients in 1 of the treatment groups).
Patients With F/MF Genotype
In Study 102, the overall percentage of patients who experienced at least 1 AE was similar between the placebo group (96.0%) and the ELX-TEZ-IVA group (93.1%). Infective pulmonary exacerbations were the most frequently reported AEs in both the placebo and ELX-TEZ-IVA groups. Consistent with efficacy data, there were fewer patients with pulmonary exacerbations reported as AEs in the ELX-TEZ-IVA group compared with the placebo group (47.3% versus 21.8%). AEs that were reported in at least 5% of patients in the ELX-TEZ-IVA group and which occurred at a frequency of 5% greater compared with the placebo group were: diarrhea (12.9% versus 7.0%), ALT increased (9.9% versus 3.5%), AST increased (9.4% versus 2.0%), rhinorrhea (8.4% versus 3.0%), and influenza (6.9% versus 1.5%).7
Patients With F/F Genotype
In Study 103, the overall percentage of patients who experienced at least 1 AE was 63.5% in the TEZ-IVA group and 58.2% in the ELX-TEZ-IVA group. Infective pulmonary exacerbations of CF were the most frequently reported AE in the TEZ-IVA group and these events occurred at a higher frequency in the ELX-TEZ-IVA group compared to the placebo group (11.5% versus 1.8%). AEs that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency of 5% or greater compared with the TEZ-IVA group were: cough (14.5% versus 7.7%), oropharyngeal pain (7.3% versus 0%), and respiration abnormal (5.5% versus 0%).8
In Study 109, the overall percentage of patients who experienced at least 1 AE was 92.0% in the TEZ-IVA group compared with 88.5% in the ELX-TEZ-IVA group. Infective pulmonary exacerbations of CF were the most frequently reported AE in the TEZ-IVA group and these events occurred at a higher frequency in the ELX-TEZ-IVA group compared to the placebo group (40.9% versus 11.5%). AEs that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency of 5% or greater compared with the TEZ-IVA group were: headache (28.7% versus 20.5%), ALT increased (6.9% versus 1.1%), AST increased (5.7% versus 0%), nasal congestion (6.9% versus 0%), rash (8.0% versus 0%), and productive cough (9.2% versus 3.4%).10
Patients With F/G and F/RF Genotypes
In Study 104, the overall percentage of patients who experienced at least 1 AE was 66.7% in the ELX-TEZ-IVA group and 65.9%in the control group.9 AEs that were reported in at least 5% of patients in the ELX-TEZ-IVA group and occurred at a frequency of 5% or greater compared with the control group were: ALT increased (6.1% versus 0%) and AST increased (6.1% versus 0%).9
Table 36: Adverse Events Occurring in at Least 5% of Patients
Adverse events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 201 | ELX-TEZ-IVA N = 202 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
At least 1 AE | 193 (96.0) | 188 (93.1) | 33 (63.5) | 32 (58.2) | 81 (92.0) | 77 (88.5) | 83 (65.9) | 88 (66.7) |
Infective PEx of CF | 95 (47.3) | 44 (21.8) | 6 (11.5) | 1 (1.8) | 36 (40.9) | 10 (11.5) | 13 (10.3) | 3 (2.3) |
Sputum increased | 39 (19.4) | 40 (19.8) | 3 (5.8) | 3 (5.5) | 16 (18.2) | 10 (11.5) | 8 (6.3) | 6 (4.5) |
Headache | 30 (14.9) | 35 (17.3) | 4 (7.7) | 3 (5.5) | 18 (20.5) | 25 (28.7) | 19 (15.1) | 11 (8.3) |
Cough | 77 (38.3) | 34 (16.8) | 4 (7.7) | 8 (14.5) | 23 (26.1) | 11 (12.6) | 18 (14.3) | 3 (2.3) |
Diarrhea | 14 (7.0) | 26 (12.9) | 3 (5.8) | 2 (3.6) | 7 (8.0) | 8 (9.2) | 8 (6.3) | 5 (3.8) |
URTI | 22 (10.9) | 24 (11.9) | 2 (3.8) | 4 (7.3) | 5 (5.7) | 9 (10.3) | NR | NR |
Nasopharyngitis | 26 (12.9) | 22 (10.9) | 2 (3.8) | 4 (7.3) | 13 (14.8) | 17 (19.5) | NR | NR |
Abdominal pain | 12 (6.0) | 20 (9.9) | 1 (1.9) | 3 (5.5) | 7 (8.0) | 4 (4.6) | 2 (1.6) | 7 (5.3) |
ALT increased | 7 (3.5) | 20 (9.9) | NR | NR | 1 (1.1) | 6 (6.9) | 0 (0) | 8 (6.1) |
Oropharyngeal pain | 25 (12.4) | 20 (9.9) | 0 (0) | 4 (7.3) | 7 (8.0) | 11 (12.6) | NR | NR |
AST increased | 4 (2.0) | 19 (9.4) | NR | NR | 0 (0) | 5 (5.7) | 0 (0) | 8 (6.1) |
Blood CPK increased | 9 (4.5) | 19 (9.4) | NR | NR | NR | NR | NR | NR |
Nasal congestion | 15 (7.5) | 19 (9.4) | 1 (1.9) | 3 (5.5) | 0 (0) | 6 (6.9) | NR | NR |
Rash | 9 (4.5) | 18 (8.9) | NR | NR | 0 (0) | 7 (8.0) | NR | NR |
Pyrexia | 19 (9.5) | 17 (8.4) | NR | NR | NR | NR | NR | NR |
Rhinorrhea | 6 (3.0) | 17 (8.4) | NR | NR | NR | NR | NR | NR |
Nausea | 14 (7.0) | 16 (7.9) | 3 (5.8) | 1 (1.8) | NR | NR | 9 (7.1) | 2 (1.5) |
Rhinitis | 11 (5.5) | 15 (7.4) | NR | NR | NR | NR | NR | NR |
Influenza | 3 (1.5) | 14 (6.9) | NR | NR | NR | NR | NR | NR |
Productive cough | 16 (8.0) | 12 (5.9) | NR | NR | 3 (3.4) | 8 (9.2) | NR | NR |
Vomiting | 10 (5.0) | 12 (5.9) | NR | NR | NR | NR | NR | NR |
Hemoptysis | 28 (13.9) | 11 (5.4) | 5 (9.6) | 2 (3.6) | 6 (6.8) | 3 (3.4) | NR | NR |
Sinusitis | 8 (4.0) | 11 (5.4) | NR | NR | NR | NR | NR | NR |
Blood bilirubin increased | 2 (1.0) | 10 (5.0) | NR | NR | NR | NR | NR | NR |
Fatigue | 20 (10.0) | 9 (4.5) | 2 (3.8) | 3 (5.5) | NR | NR | NR | NR |
Constipation | 12 (6.0) | 6 (3.0) | NR | NR | NR | NR | NR | NR |
Bacterial test positive | 10 (5.0) | 5 (2.5) | NR | NR | 5 (5.7) | 1 (1.1) | NR | NR |
Dyspnea | 13 (6.5) | 5 (2.5) | NR | NR | NR | NR | NR | NR |
Respiration abnormal | NR | NR | 0 (0) | 3 (5.5) | NR | NR | NR | NR |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; CPK = creatine phosphokinase; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; PEx = pulmonary exacerbation; TEZ = tezacaftor; URTI = upper respiratory tract infection.
Serious Adverse Events
Table 37 provides a summary of the SAEs that were reported in the included studies.
Patients With F/MF Genotype
In Study 102, the percentage of patients who experienced at least 1 SAE was 20.9% in the placebo group compared with 17.3% in the ELX-TEZ-IVA group.7 The most commonly reported SAE in either treatment group was infective pulmonary exacerbation of CF. There were more pulmonary exacerbation SAEs in the placebo group compared with the ELX-TEZ-IVA group (17.9% versus 6.4%). There were few other SAEs that were reported for more than 1 patient in each treatment group.7
Patients With F/F Genotype
In Study 103, SAEs were rare and only reported for 1 patient in the TEZ-IVA group (pulmonary exacerbation) and 2 patients in the ELX-TEZ-IVA group (pulmonary exacerbation and rash) (1.9% versus 3.6%).8 In Study 109, the percentage of patients who experienced at least 1 SAE was 15.9% in the TEZ-IVA group and 5.7% in the ELX-TEZ-IVA group. The difference between the groups was due to a greater proportion of patients in the TEZ-IVA group who experienced a pulmonary exacerbation that was classified as an SAE compared with the ELX-TEZ-IVA group (11.4% versus 1.1%). There were no other SAEs that were reported for more than 1 patient in each treatment group.10
Patients With F/G and F/RF Genotypes
In Study 104, the percentage of patients who experienced at least 1 SAE was 8.7% in the control group compared with 3.8% in the ELX-TEZ-IVA group.9 The difference between the groups was due to a greater percentage of patients in the control group who experienced a pulmonary exacerbation that was classified as an SAE compared with the ELX-TEZ-IVA group (5.6% versus 1.5%). There were 4 other SAEs that were reported for more than 1 patient in each treatment group.9
Table 37: Serious Adverse Events
SAEs, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 201 | ELX-TEZ-IVA N = 202 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
At least 1 SAE | 42 (20.9) | 28 (13.9) | 1 (1.9) | 2 (3.6) | 14 (15.9) | 5 (5.7) | 11 (8.7) | 5 (3.8) |
Blood and lymphatic system disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Thrombocytopenia | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Infections and infestations | 36 (17.9) | 13 (6.4) | 1 (1.9) | 1 (1.8) | 10 (11.4) | 1 (1.1) | 8 (6.3) | 2 (1.5) |
Infective PEx of CF | 33 (16.4) | 11 (5.4) | 1 (1.9) | 1 (1.8) | 9 (10.2) | 1 (1.1) | 7 (5.6) | 2 (1.5) |
Influenza | 0 (0) | 3 (1.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Genital herpes simplex | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Oral herpes | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Atypical mycobacterial LRTI | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Coccidioidomycosis | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Lung infection | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Pneumonia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Viral sinusitis | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
LRTI | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Cellulitis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Ear and labyrinth disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Tinnitus | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Respiratory, thoracic, and mediastinal disorders | 6 (3.0) | 4 (2.0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 1 (0.8) | 1 (0.8) |
Hemoptysis | 3 (1.5) | 2 (1.0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 1 (0.8) | 1 (0.8) |
Diaphragmatic paralysis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Nasal polyps | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Painful respiration | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Pleuritic pain | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Pneumothorax spontaneous | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Investigations | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
ALT increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Endocrine disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Hyperparathyroidism primary | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Gastrointestinal disorders | 1 (0.5) | 3 (1.5) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Abdominal pain upper | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Distal intestinal obstruction syndrome | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Small intestinal obstruction | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hepatobiliary disorders | 1 (0.5) | 3 (1.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Cholangitis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Gallbladder enlargement | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Portal hypertension | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hypertransaminasemia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Cholecystitis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Skin and subcutaneous tissue disorders | 2 (1.0) | 3 (1.5) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rash | 1 (0.5) | 2 (1.0) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rash pruritic | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hypersensitivity vasculitis | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Injury, poisoning, and procedural complications | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Post-procedural hemorrhage | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Upper limb fracture | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Musculoskeletal and connective tissue disorders | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Musculoskeletal chest pain | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rhabdomyolysis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Back pain | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Nervous system disorders | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Axonal neuropathy | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Mental impairment | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Neuroglycopenia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
General disorders and admin. site conditions | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Adverse drug reaction | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Medical device site inflammation | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Metabolism and nutrition disorders | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Hypoglycemia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Type 3 diabetes mellitus | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Psychiatric disorders | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 3 (3.4) | 1 (1.1) | 0 (0) | 0 (0) |
Depression | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 0 (0) |
Suicidal ideation | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Anxiety | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (1.1) | 1 (0.8) | 0 (0) |
Insomnia | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
OCD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Psychotic disorder | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Renal and urinary disorders | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Acute kidney injury | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Renal colic | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Nephrolithiasis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Cardiac disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Extrasystoles | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
ALT = alanine transaminase; CF = cystic fibrosis; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LRTI = lower respiratory tract infection; OCD = obsessive-compulsive disorder; PEx = pulmonary exacerbation; SAE = serious adverse event; TEZ = tezacaftor.
Withdrawal Due to Adverse Events
Patients With F/MF Genotype
In Study 102, there were 2 WDAEs reported in the ELX-TEZ-IVA group (1.0%) and none in the placebo group. The reasons for discontinuation from the ELX-TEZ-IVA group included portal hypertension (0.5.%) and rash (0.5%).
Patients With F/F Genotype
There were no WDAEs reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, 2 patients (2.3%) withdrew from the TEZ-IVA group and 1 patient (1.1%) withdrew from the ELX-TEZ-IVA group as a result of AEs. The AEs that resulted in withdrawal from the TEZ-IVA group included obsessive-compulsive disorder (1.1%) and psychotic disorder (1.1%). The AEs that resulted in withdrawal from the ELX-TEZ-IVA group included anxiety and depression (1.1%; 1 patient with both events).
Patients With F/G and F/RF Genotypes
In Study 104, there were 2 WDAEs from the control group (1.6%) and 1 in the ELX-TEZ-IVA group (0.8%). The AEs that resulted in withdrawal from the control group included infective pulmonary exacerbation (0.8%) and anxiety and depression (0.8%; 1 patient with both events). The AEs that resulted in withdrawal from the ELX-TEZ-IVA group included 1 patient with elevated ALT and AST levels.
Table 38: Withdrawal Due to Adverse Events
Events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Any WDAE | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 2 (1.6) | 1 (0.8) |
Infections and infestations | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Infective PEx of CF | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Hepatobiliary disorders | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Portal hypertension | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Skin and subcutaneous tissue disorders | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rash | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Investigations | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
ALT increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
AST increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Psychiatric disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (1.1) | 1 (0.8) | 0 (0) |
Anxiety | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 0 (0) |
Depression | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 0 (0) |
OCD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
Psychotic disorder | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 0 (0) |
ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; OCD = obsessive-compulsive disorder; PEx = pulmonary exacerbation; TEZ = tezacaftor; WDAE = withdrawal due to adverse event.
Interruptions Due to AEs
Patients With F/MF Genotype
In Study 102, AEs leading to treatment interruption were reported for 10 patients (5.0%) in the placebo group and 19 patients (9.4%) in the ELX-TEZ-IVA group.
Patients With F/F Genotype
There were no treatment interruptions due to AEs reported in either the TEZ-IVA or ELX-TEZ-IVA groups in Study 103. In Study 109, treatment interruptions due to AEs were report for 1 patient (1.1%) in the TEZ-IVA group and 2 patients (2.3%) in the ELX-TEZ-IVA group.
Patients With F/G and F/RF Genotypes
In Study 104, AEs leading to treatment interruption were reported for 3 patients (2.4%) in the control group and 5 patients (3.8%) in the ELX-TEZ-IVA group.
Table 39: Treatment Interruptions Due to Adverse Events
Events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Any AEs leading to treatment interruption | 10 (5.0) | 19 (9.4) | 0 (0) | 0 (0) | 1 (1.1) | 2 (2.3) | 3 (2.4) | 5 (3.8) |
Skin and subcutaneous tissue disorders | 2 (1.0) | 4 (2.0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 2 (1.5) |
Rash | 1 (0.5) | 3 (1.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Pruritus | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Rash pruritic | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hypersensitivity vasculitis | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rash macular | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 1 (0.8) |
Urticaria | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Investigations | 3 (1.5) | 4 (2.0) | 0 (0) | 0 (0) | 1 (1.1) | 2 (2.3) | 1 (0.8) | 1 (0.8) |
ALT increased | 2 (1.0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 2 (2.3) | 0 (0) | 0 (0) |
AST increased | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Bilirubin conjugated increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Blood bilirubin increased | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) | 1 (0.8) |
Blood CPK increased | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Blood creatinine increased | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Blood LDH increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
CRP increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Liver function test increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Infections and infestations | 1 (0.5) | 5 (2.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Infective PEx of CF | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Influenza | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Genital herpes simplex | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Oral herpes | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Musculoskeletal and connective tissue disorders | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rhabdomyolysis | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Back pain | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Blood and lymphatic system disorders | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Thrombocytopenia | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Ear and labyrinth disorders | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Tinnitus | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Gastrointestinal disorders | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 1 (0.8) |
DIOS | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Gastritis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Small intestinal obstruction | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Tongue ulceration | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Hepatobiliary disorders | 2 (1.0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Cholangitis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Gallbladder enlargement | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hepatocellular injury | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hypertransaminasemia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Psychiatric disorders | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Emotional distress | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Depression | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Intentional self-injury | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Suicidal ideation | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Respiratory, thoracic, and mediastinal disorders | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Hemoptysis | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; CPK = creatine phosphokinase; CRP = C-reactive protein; DIOS = distal intestinal obstruction syndrome; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LDH = lactate dehydrogenase; PEx = pulmonary exacerbation; TEZ = tezacaftor.
Mortality
There were no deaths reported in any of the included studies.7-10
Notable Harms
The sponsor identified elevated transaminase events and rash events as AEs of special interest in their analysis of safety data from the included studies.7-10 In consultation with clinical experts, CADTH has also included ophthalmological AEs as additional AE of interest for this review.
Elevated Transaminase AEs
Elevated transaminase events included any of the following: ALT abnormal, ALT increased, AST abnormal, AST increased, hepatic enzyme abnormal, hepatic enzyme increased, hypertransaminasemia, liver function test abnormal, liver function test increased, transaminases abnormal, transaminases increased.7
Patients With F/MF Genotype
In Study 102, at least 1 elevated transaminase event was reported for 10.9% of patients in the ELX-TEZ-IVA group compared with 4.0% in the placebo group.7 The majority of events were mild or moderate in severity. None of the events were considered serious in the ELX-TEZ-IVA group (1 serious event was reported in the placebo group). Events leading to treatment interruption were reported for 2 patients (1.0%) in the ELX-TEZ-IVA group and 3 patients in the (1.5%) in the placebo group. No events led to discontinuation of the study drugs during the double-blind treatment period (1 patient in the ELX-TEZ-IVA who had their treatment interrupted eventually discontinued from the open-label extension without resuming treatment).7 The median time to onset of first elevated transaminase event was 57.0 days (range = 1 day to 176 days) in the ELX-TEZ-IVA group and 58.0 days (range = 1 day to 169 days) in the placebo group. The median duration of elevated transaminase events was 17.0 days (range = 4 days to 153 days) in the ELX-TEZ-IVA group and 17.0 days (range = 5 days to 52 days) in the placebo group.7 Additional relevant hepatic AEs were reported for 1.5% of patients in the ELX-TEZ-IVA group (hepatic cirrhosis, hepatocellular injury, and portal hypertension) and 0.5% in the placebo group (hepatocellular injury). None of the events in the ELX-TEZ-IVA group were considered serious.7
Patients With F/F Genotype
In Study 103, at least 1 elevated transaminase event was reported for 3.6% of patients in the ELX-TEZ-IVA group compared with 1.9% in the TEZ-IVA group.8 All of the events were mild in severity and none resulted in the interruption or discontinuation of the study drugs. The median time to onset of first elevated transaminase event was 8.0 days (range = 1 day to 15 days) in the ELX-TEZ-IVA group and the 1 event in the TEZ-IVA group occurred at day 30.8 The median duration of elevated transaminase events was 22.0 days (range = 15 days to 29 days) in the ELX-TEZ-IVA group and the duration was not reported for the single event in the TEZ-IVA group.8
In Study 109, at least 1 elevated transaminase event was reported for 6.9% of patients in the ELX-TEZ-IVA group compared with 1.1% in the TEZ-IVA group. One patient in the ELX-TEZ-IVA group had an event that was considered serious (the single event in the TEZ-IVA was not serious). Events leading to treatment interruption were reported for 2 patients (2.3%) in the ELX-TEZ-IVA group and none in the TEZ-IVA group.10 No events led to discontinuation of the study drugs during the double-blind treatment period. The median time to onset of first elevated transaminase event was 67.0 days (range = 12 days to 169 days) in the ELX-TEZ-IVA group and the patient with events in the TEZ-IVA group was first reported at day 1. The median duration of elevated transaminase events was 16.5 days (range = 3 days to 52 days) in the ELX-TEZ-IVA group and 25.0 (range = 7 days to 43 days) in the TEZ-IVA group.10
Patients With F/G and F/RF Genotypes
In Study 104, at least 1 elevated transaminase event was reported for 6.1% of patients in the ELX-TEZ-IVA group compared with 0.8% in the control group.9 All of the events were mild or moderate in severity. One patient in the ELX-TEZ-IVA group discontinued the study because of elevated transaminases (ALT > 8 × ULN and AST > 5 × ULN). No patients in the control group discontinued the study drug due to transaminase elevations.9 There were no transaminase elevation events that resulted in treatment interruption in the ELX-TEZ-IVA group and 1 event (0.8%) that led to interruption in the control group. The median time to onset of first elevated transaminase event was 19.0 days (range = 4 days to 29 days) in the ELX-TEZ-IVA group and the 1 event in the control group was reported at day 1. The median duration of elevated transaminase events was 19.0 days (range = 4 days to 29 days) in the ELX-TEZ-IVA group and the 1 event in the control group had a duration of 16 days.9
Table 40: Elevated Transaminase Adverse Events
Elevated Transaminase Adverse Events, n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Any events | 8 (4.0) | 22 (10.9) | 1 (1.9) | 2 (3.6) | 1 (1.1) | 6 (6.9) | 1 (0.8) | 8 (6.1) |
ALT increased | 7 (3.5) | 20 (9.9) | 0 (0) | 1 (1.8) | 1 (1.1) | 6 (6.9) | 0 (0) | 8 (6.1) |
AST increased | 4 (2.0) | 19 (9.4) | 1(1.9) | 1 (1.8) | 0 (0) | 5 (5.7) | 0 (0) | 8 (6.1) |
Hypertransaminasemia | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Transaminases increased | 0 (0) | 0 (0) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Liver function test increased | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Events by maximum severity | ||||||||
Mild | 4 (2.0) | 12 (5.9) | (1.9) | 2 (3.6) | 1 (1.1) | 2 (2.3) | 1 (0.8) | 5 (3.8) |
Moderate | 4 (2.0) | 8 (4.0) | 0 (0) | 0 (0) | 0 (0) | 4 (4.6) | 0 (0) | 2 (1.5) |
Severe | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Life-threatening | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Missing | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Events leading to discontinuation | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Events leading to interruption | 3 (1.5) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 2 (2.3) | 1 (0.8) | 0 (0) |
Serious events | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Events leading to death | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
ALT = alanine transaminase; AST = aspartate transaminase; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; TEZ = tezacaftor.
Rash AEs
Rash events were defined as any 1 of 48 different AEs, including rash, urticaria, dermatitis, and erythema.7
Patients With F/MF Genotype
In Study 102, at least 1 rash AE was reported for 10.9% of patients in the ELX-TEZ-IVA group compared with 6.5% in the placebo group.7 The majority of events were mild or moderate in severity, 3 patients (1.5%) in the ELX-TEZ-IVA group had events that were considered serious (rash [n = 2] and rash pruritic [n = 1]), and 1 patient (0.5%) had a serious rash event in the placebo group. Events leading to treatment interruption were reported for 4 patients (2.0%) in the ELX-TEZ-IVA group and 1 patient (0.5%) in the placebo group.7 One patient in the ELX-TEZ-IVA group discontinued the treatment due to a rash AE and no patients in the placebo group discontinued treatment for this reason. The median time to onset of first rash event was 13.5 days (range = 5 days to 157 days) in the ELX-TEZ-IVA group and 27.0 days (range = 1 day to 157 days) in the placebo group. The median duration of rash events was 7.0 days (range = 1 day to 92 days) in the ELX-TEZ-IVA group and 8.0 days (range = 2 days to 61 days) in the placebo group.7
Patients With F/F Genotype
In Study 103, at least 1 rash AE was reported for 3.6% of patients in the ELX-TEZ-IVA group compared with 3.8% in the TEZ-IVA group. One event in the ELX-TEZ-IVA group was considered serious (none in the TEZ-IVA group). No rash events led to study drug interruption or discontinuation.8 The median time to onset of first rash event was 10.5 days (range = 10 days to 11 days) in the ELX-TEZ-IVA group and 20.5 days (range = 14 days to 27 days) in the TEZ-IVA group. The median duration of rash events was 7.0 days (range = 1 day to 13 days) in the ELX-TEZ-IVA group and was reported for the TEZ-IVA group.8
In Study 109, at least 1 rash AE was reported for 12.6% of patients in the ELX-TEZ-IVA group compared with 2.3% in the TEZ-IVA group. All the events were mild or moderate in severity. Events leading to treatment interruption were reported for 1 patient (1.1%) in the ELX-TEZ-IVA group and none in the TEZ-IVA group.10 No events led to discontinuation of the study drugs during the double-blind treatment period. The median time to onset of first rash AE was 42.5 days (range = 2 days to 138 days) in the ELX-TEZ-IVA group and 31.5 (range = 8 days to 55 days) in the TEZ-IVA group. The median duration of elevated transaminase events was 10.0 days (range = 1 days to 135 days) in the ELX-TEZ-IVA group and 2.0 days (range = 1 day to 3 days) in the TEZ-IVA group.10
Patients With F/G and F/RF Genotypes
In Study 104, at least 1 rash AE was reported for 3.0% of patients in the ELX-TEZ-IVA group compared with 4.0% in the control group. All the events were mild or moderate in severity. Events leading to treatment interruption were reported for 1 patient (0.8%) in the ELX-TEZ-IVA group and 1 patient (0.8%) in the TEZ-IVA group. No events led to discontinuation of the study treatments. The median time to onset of the first rash event was 27.5 days (range = 10 days to 38 days) in the ELX-TEZ-IVA group and 13.0 days (range = 5 days to 47 days) in the TEZ-IVA group. The median duration of rash events was 5.5 days (range = 3 days to 10 days) in the ELX-TEZ-IVA group and 10.0 days (range = 3 days to 51 days) in the TEZ-IVA group.7
Rash adverse events n (%) | Study 102 (F/MF) | Study 103 (F/F) | Study 109 (F/F) | Study 104 (F/G and F/RF) | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 203 | ELX-TEZ-IVA N = 200 | TEZ-IVA N = 52 | ELX-TEZ-IVA N = 55 | TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Control N = 126 | ELX-TEZ-IVA N = 132 | |
Any rash events | 13 (6.5) | 22 (10.9) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 11 (12.6) | 5 (4.0) | 4 (3.0) |
Dermatitis allergic | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Drug hypersensitivity | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Rash | 9 (4.5) | 18 (8.9) | 2 (3.8) | 2 (3.6) | 0 (0) | 7 (8.0) | 2 (1.6) | 2 (1.5) |
Rash erythematous | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Rash generalized | 0 (0) | 2 (1.0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Rash macular | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 1 (0.8) |
Rash pruritic | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) |
Urticaria | 3 (1.5) | 1 (0.5) | 0 (0) | 0 (0) | 2 (2.3) | 0 (0) | 1 (0.8) | 0 (0) |
Perioral dermatitis | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
Rash pustular | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) |
Events by maximum severity | ||||||||
Mild | 10 (5.0) | 17 (8.4) | 2 (3.8) | 2 (3.6) | 2 (2.3) | 8 (9.2) | 4 (3.2) | 2 (1.5) |
Moderate | 3 (1.5) | 4 (2.0) | 0 (0) | 0 (0) | 0 (0) | 3 (3.4) | 1 (0.8) | 2 (1.5) |
Severe | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Life-threatening | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Missing | NR | NR | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Events leading to discontinuation | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Events leading to interruption | 1 (0.5) | 4 (2.0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | 1 (0.8) | 1 (0.8) |
Serious events | 1 (0.5) | 3 (1.5) | 0 (0) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Events leading to death | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; TEZ = tezacaftor.
Ophthalmological AEs
Patients With F/MF Genotype
In Study 102, ophthalmologic exams were performed at screening and at the week 24 study visit for patients younger than 18 years of age. Treatment-emergent cataracts were reported for 1 patient in both the ELX-TEZ-IVA and placebo groups (0.5% in both groups). Both events were mild in severity and did not require treatment or lead to interruption or discontinuation of study drug.7
Patients With F/F Genotype
Ophthalmologic exams were performed for patients younger than 18 years of age at screening in both Study 103 and Study 109. Follow-up examinations were not required during the double-blind treatment periods of either study (only during the safety follow-up or enrolment in the open-label extension study).8,10 There were no treatment-emergent cataracts in Study 103.29 In Study 109, 1 patient in both the ELX-TEZ-IVA and TEZ-IVA groups (1.1%) had AEs of cataract. The events were mild in severity and did not require treatment.10
Patients With F/G and F/RF Genotypes
In Study 104, ophthalmologic exams were performed for patients younger than 18 years of age at screening and at the safety follow-up visit (i.e., no examinations during the double-blind treatment period). There were no treatment-emergent cataracts reported in Study 104
Critical Appraisal
Internal Validity
Randomization was performed using an appropriate methodology with adequate allocation concealment (i.e., IWRS) and stratification based on relevant prognostic factors (i.e., age, sex, baseline ppFEV1, and prior CFTR modulator usage [in Study 104]).7-10 Baseline and demographic characteristics were generally well-balanced across the treatments of each of the studies. The only exceptions were differences between some CF therapies at baseline and infection with Pseudomonas aeruginosa within 2 years of screening. In Study 102 and 103, a greater percentage of patients in ELX-TEZ-IVA group were reported to have infection with Pseudomonas aeruginosa within 2 years of screening compared with the comparator groups (75.0% versus 70.0% and 70.9% versus 59.6% in Studies 102 and 103, respectively).7,8 The clinical experts consulted by CADTH noted that this difference is unlikely to be clinically relevant. Similarly, the reviewers for the EMA and FDA concluded that the demographic and baseline characteristics were balanced between the treatment groups of Study 102 and Study 103.29,48
Relative to the comparator groups, the percentage of patients using inhaled hypertonic saline was greater in ELX-TEZ-IVA group in Study 102 (73.5% versus 62.6%) but was lower in the ELX-TEZ-IVA group in Study 103 (78.8% versus 69.1%).7,8 In Study 104, a greater percentage of patients in the TEZ-IVA group reported prior usage of dornase alfa (81.8% versus 71.3%) and inhaled hypertonic saline (64.8% versus 58.6%).9 It is possible that it could favour the treatment groups with greater usage in the respiratory end points, but these patients may have had more severe disease that required additional treatment; hence, any potential impact of these imbalances is uncertain. The clinical experts consulted by CADTH noted that the differences are unlikely to be clinically relevant. There were also differences noted in Study 103 and Study 104 regarding baseline usage of antibiotics used in the treatment of CF. Greater proportions of patients in the ELX-TEZ-IVA group of Study 103 reported usage of azithromycin (60.0% versus 48.1%) and inhaled antibiotics (63.6% versus 53.8) compared with the TEZ-IVA group.8 Conversely, fewer ELX-TEZ-IVA-treated patients reported prior usage of inhaled antibiotics compared with those in the placebo group (44.4% versus 37.1%).8 As has been noted in previous CADTH reviews of CFTR modulators, it is unclear if a greater usage of antibiotics at baseline would be correlated with an increased risk of an exacerbation (e.g., the antibiotics are provided to those who are at the greatest risk) or a decreased risk of an exacerbation (e.g., the concomitant use of antibiotics provides a protective effect that would lower the risk).62 Reviewers for the FDA noted that the handling of concomitant and prohibited medications was reasonable in the pivotal trials.29
Study treatments were administered in a double-blind manner with all groups issued the same number of tablets each day (3 tablets in Study 102 and 4 tablets in Study 103, 104, and 109).7-10 The ELX-TEZ-IVA and IVA tablets were identical in appearance to the comparator tablets (i.e., placebo and TEZ-IVA). The AE profile of ELX-TEZ-IVA and the comparators was unlikely to compromise blinding in the study. The only exceptions could be the increased percentage of patients who experienced a rash in the ELX-TEZ-IVA groups of the 2 24-week trials, although only impacted a minority of patients (8.9% versus 4.5% in Study 103 and 8.0% versus 0% in Study 109).8,9 The clinical experts consulted by CADTH noted that these events were unlikely to lead to unblinding. Reviewers for the FDA noted that the methods for blinding in the pivotal trials was acceptable.29
Patient disposition was thoroughly documented and well-reported by the sponsor in their application to CADTH. There were few patients who discontinued the trials (completion rate ranged from 96.8% to 100%), although the studies were relatively short in duration which may in part explain the high percentage of patients who completed.7-10 The full analysis sets included nearly all randomized patients. Reviewers for the EMA noted that the amount of missing data in the pivotal studies was minimal and not a concern.48
Adherence to the study treatments was evaluated by counting the number of study drugs at each visit and was reported to be greater than 99% across all treatment groups in Studies 102, 103, 104, and 109.7-10 In accordance with the study protocols, the use of concomitant medications remained stable throughout the treatment period for all treatment groups. The only exceptions were the lower usage of some antibiotics for pulmonary exacerbations in the ELX-TEZ-IVA group relative to the placebo group in Study 102.7 Reviewers for the EMA noted that this difference was a consequence of the efficacy of ELX-TEZ-IVA for reducing pulmonary exacerbations relative to placebo.48
There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in the included studies were considered to be appropriate by regulatory authorities and the clinical experts consulted by CADTH.29,48 There was no independent adjudication of pulmonary exacerbation events. As shown in Table 2, when evaluated as an efficacy end point there were fewer patients in Study 102 that met the criteria for a pulmonary exacerbation compared to the number of events reported as AEs (e.g., 37% versus 47% in the placebo group).7 Pulmonary exacerbations were only evaluated as efficacy end points in the 24-week placebo-controlled trial (Study 102).7 In response to an inquiry from CADTH, the sponsor reported that pulmonary exacerbations were not included in the active-controlled trials because the studies would not be powered to detect a difference in pulmonary exacerbations between ELX-TEZ-IVA and the active comparators.54 As both TEZ-IVA and IVA have been shown to reduce the frequency of pulmonary exacerbations in previous placebo-controlled trials with patients who have F/F, F/RF, or F/G genotypes the sponsor noted that a prohibitively large number of patients would be required to sufficiently power the studies to detect a reduction in pulmonary exacerbations.54
Statistical power calculations were reported for all of the included studies and a sufficient number of patients were enrolled and completed the studies.7-10 The number of withdrawal from the trials was well below the 5% or 10% proportion assumed in the sponsor’s statistical power calculations The MMRM analyses for the primary evaluations assumed data were missing at random, which may not be a valid assumption. However, the amount of missing data in the trials was low and sensitivity analyses using multiple imputation were supportive of the primary analyses. Similarly, reviewers for the FDA and EMA noted that the amount of missing data was low in the pivotal trials and did not raise any concerns regarding the statistical approaches used by the sponsor.29,48
In Study 102 the primary end point was the absolute change from baseline in ppFEV1 to 4 weeks in the Global protocol and through 24 weeks in the European protocol.7 The rationale for this difference in protocols was due to guidance from the EMA on the clinical development of drugs for the treatment of CF which states that ppFEV1 should be evaluated after 24 weeks of treatment.63 As the global protocol involved the use of an interim analysis at 4 weeks, the sponsor included a multiplicity adjustment in the statistical analysis plan to control the overall type I error rate at 0.05 for the primary end point (Lan and DeMets alpha spending function).7 The key secondary end points of all of the included studies were tested using a hierarchical approach to control the overall type I error rate at 0.05. All end points within the statistical testing hierarchies were statistically significant. Subgroup analyses and exploratory end points (e.g., TSQM, CFQ-R [non-respiratory domains], hospitalizations) were tested with adjustment for multiple comparisons and all P values are considered nominal.
Studies 103, 104, and 109 all included a 4-week run-in period where patients received open-label treatment with TEZ-IVA (for those with F/F or F/RF genotypes) or IVA (for those with F/G genotypes).8-10 Reviewers for the EMA noted that the duration of the run-in period may have been too short to allow patients who were naive to CFTR modulator therapy to fully realize the benefits of initiating therapy with TEZ-IVA or IVA at the time of the baseline assessment.48 As such, the treatment effects for ELX-TEZ-IVA may be overestimated in the overall study populations As a result, the EMA requested that the results for the post hoc subgroup analysis of CFTR modulator-naive and experienced patients be included in the summary of product characteristics for ELX-TEZ-IVA.48,61
External Validity
The diagnostic criteria used in the screening process for Studies 103 and 109 were consistent with Canadian clinical practice for identifying patients with CF who are homozygous for the F508del-CFTR mutation. The gating and RF mutations that were used to select patients for inclusion in Study 104 were consistent with the approved indications for TEZ-IVA and IVA in Canada.9,12,13 There were no widely accepted criteria for defining MF mutations in the CFTR gene; therefore, the identification of patients with MF mutations in Study 102 relied on a novel approach designed by the sponsor.7 Eligible mutations were identified as having at least 1 of the following characteristics: a genetic sequence that predicts no translated CFTR protein or mutations that lack in vitro responsiveness to TEZ, IVA, or TEZ-IVA and evidence of clinical severity on a population level (average sweat chloride > 86 mmol/L, and a > 50% prevalence of pancreatic insufficiency).7 The majority of patients enrolled in Study 102 (314 out of 403; 78%) had mutations that met the first criterion (i.e., no CFTR protein).48 Overall, the criteria used by the sponsor to identify patients with MF mutations in the CFTR gene were considered acceptable by reviewers for FDA.29 The clinical experts consulted by CADTH noted that terms “residual function” and “minimal function” are not currently used in Canadian clinical practice and that patients are not currently differentiated based on the presence of RF or MF mutations.
Patients with CF with more severe lung disease (e.g., ppFEV1 < 40% at screening) or a normal ppFEV1 at screening (≥ 90%) were excluded from the studies7-10; therefore, the results of the included studies are primarily applicable to patients with moderate (i.e., FEV1 40% to 69%) to mild (i.e., FEV1 70% to 89%) lung disease. This is identical to the phase III trials conducted by the sponsor for other approved combination CFTR modulators (LUM-IVA and TEZ-IVA)64-70 The sponsor reported that this population was selected because they were considered to be the most likely patient group able to show an improvement in lung function in a clinical trial based on their experience with other therapies targeting CF lung disease.49 These screening criteria resulted in trial populations where the proportion of patients with mild lung disease was generally similar to the adult CF population in Canada (approximately 27% of patients had mild lung disease in 2019)1 in Study 102 (31.8%), Study 103 (29.9%), and Study 109 (31.4%); though the proportion of patients with mild disease was greater in Study 104 (40.7%).7-10 The proportion of patients with moderate lung disease in the included studies ranged from 51.6% in Study 104 to 60.7% in Study 103 which is greater than the proportions reported within the overall adult CF population in Canada (approximately 38% in 2019).1 A small minority of patients with a ppFEV1 less than 40% at baseline were enrolled in the included studies (range = 1.6% in Study 104 to 9.3% in Study 103).7-10 These patients with lower lung function would have satisfied the study inclusion criteria in the screening phase, then have demonstrated a ppFEV1 less than 40% at their baseline evaluation. An ad hoc subgroup analysis in Study 102 provided some efficacy data for this small subgroup of patients and suggested that ELX-TEZ-IVA resulted in meaningful improvements relative placebo.7 CADTH considered the results of additional clinical studies conducted to evaluate the use of ELX-TEZ-IVA in patients with CF who have advanced lung disease (see Patients With Advanced Lung Disease).4,5
A majority of the participants were from North America in Study 102 (59%) and Study 103 (63%); however, the majority (51.9%) were from Europe in Study 104 (37.6% from North America) and Study 109 was conducted exclusively in Europe and Australia.7-10 The clinical experts consulted noted that the results from the studies in Europe and Australia would likely be generalizable to the Canadian setting. The included RCTs were conducted at specialized CF clinics.7-10 The clinical experts consulted by CADTH and the clinician groups who provided input indicated that this is consistent with Canadian clinical practice where patients are managed in specialized CF clinics.
The study populations were comprised of almost exclusively White patients (e.g., 99% in Study 103 and Study 109),7-10 which is reflective of the majority of patients with CF in Canada, though the percentage is slightly higher than the proportion reported for the overall CF population in Canada (93.2% in 2019).1 Both Study 102 and Study 104 reported at least 90% of patients were White, but had a large proportion of patients where these data were not collected in accordance with local regulations (6.2% and 7.0%, respectively).7,9
The Cystic Fibrosis Foundation clinical practice guidelines recommend that adult women and men (≥ 20 years of age) maintain a BMI at or above 22 kg/m2 and 23 kg/m2, respectively. Mean baseline BMI was similar in Studies 102, 103, and 109 (range = 21.40 kg/m2 to 21.81 kg/m2)7,8,10; which is slightly below the estimated national median BMI for adult patients with CF (22.7 kg/m2) in Canada.1 In contrast, the mean baseline BMI was greater in Study 104 at 24.06 kg/m2 (23.33 kg/m2 and 24.49 kg/m2 for those with F/G and F/RF genotypes, respectively).9
The included studies excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus.7-10 The CCFR indicated that 3.7% of patients with CF in Canada were infected with Burkholderia cepacia complex species in 2019 (87.7% of whom are adults).1 The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA and that the clinical management of such patients is more complex and variable than those without Burkholderia cepacia infection.
The proportion of patients in the included studies who were positive for Pseudomonas aeruginosa ranged from 59.3% in Study 104 to 72.5% in Study 102 which appears to be greater than what would be expected in the Canadian CF population. Canadian-specific data for Pseudomonas aeruginosa infection rates are not available for a mixed population of adults and adolescents (i.e., those 12 years and older); however, 2019 data are available for the overall Canadian CF population who had not received a lung transplant (38.3%; 1,173 [78.9%] of whom were adults). This suggests that approximately 50% of Canadian adults living with CF who had not undergone a lung transplant were positive for Pseudomonas aeruginosa in 2019 (1,173 of 2,366 [50%]). Subgroup analyses demonstrated similar results with ELX-TEZ-IVA in patients with and without Pseudomonas aeruginosa in the 2 years before screening.
The included studies excluded patients who had a respiratory infection, pulmonary exacerbation, or changes in their therapy for pulmonary disease within 4 weeks before the first dose of study drug. This is identical to the exclusion criteria that were used in the pivotal trials for the other CFTR modulators that are currently approved. The clinical experts consulted by CADTH noted that the exclusion of these patients is unlikely to limit the generalizability of the results to the broader CF patient population.
The use of placebo as the comparator in Study 102 was considered to be appropriate by the FDA and the EMA.29,48 This study was conducted in patients who were heterozygous for the F508del mutation and had a MF mutation in the CFTR gene; this a patient population that is not addressed by any of the indications for the approved CFTR modulators. For patients who were homozygous for the F508del mutation (Study 103 and Study 109), TEZ-IVA (Symdeko) was an appropriate comparator as this drug is currently approved in Canada for the treatment of these patients (although not reviewed by CADTH or currently reimbursed by the participating drug programs).12,37 Study 104 included 2 subpopulations of patients with CF (i.e., F/RF and F/G) and used different active comparators for each population: TEZ-IVA for those who were F/RF and IVA for those who were F/G. These are appropriate comparators for these populations as both products are currently approved in Canada for use in these populations.12,13
All the included studies investigated the use of ELX-TEZ-IVA at the dosage recommended in the product monograph: ELX 200 mg, TEZ 100 mg, and IVA 150 mg in the morning (administered as 2 oral tablets) and 150 mg IVA in the evening (administered in a single oral tablet). In Studies 103, 104, and 109, TEZ-IVA was administered at the dosage recommended in the Canadian product monograph (i.e., TEZ 100 mg and 150 mg IVA in the morning and 150 IVA in the evening).12 Similarly, in Study 104, patients who were F/G in the control group received the dosage of IVA that is recommended in the Canadian product monograph for adults and adolescents (i.e., 1 150 mg tablet every 12 hours).13 Due to the need to ensure that the treatment groups received the same number of tablets, patients in Studies 103, 104, and 109 underwent a more complicated dosage regimen than would be required for typical administration of ELX-TEZ-IVA.8-10 In clinical practice, patients using the typical recommended dosage of ELX-TEZ-IVA, would take 2 tablets in the morning and 1 in the evening (i.e., 3 tablets per day). In contrast, patients in Studies 103, 104, and 109 would take 3 tablets in the morning and 1 tablet in the afternoon (i.e., 4 tablets per day).8-10 Nevertheless, as noted above, adherence with study treatments was very high throughout the run-in and double-blind treatment periods.
Three of the studies for ELX-TEZ-IVA (i.e., Study 103, Study 104, and Study 109) included an open-label, 4-week active treatment period with TEZ-IVA or IVA before randomization. As such, these trials were essentially investigating switching to ELX-TEZ-IVA from either TEZ-IVA or IVA compared with remaining on TEZ-IVA for patients with an F/F or F/RF genotype or remaining on IVA for patients with an F/G genotype. As TEZ-IVA is not widely reimbursed in Canada, the switching design limits the generalizability of the studies directly to the Canadian setting. To address this potential gap in the evidence, the sponsor filed indirect comparisons with CADTH to provide an estimate of ELX-TEZ-IVA versus placebo for those with an F/F or F/RF genotype.
All studies compared the addition of the study treatments to ongoing standard CF-management therapies, which is reflective of how ELX-TEZ-IVA and other CFTR modulators would be administered in clinical practice. In general, the background therapies that were reported at baseline in the included studies were consistent with those used in Canadian clinical practice except for dornase alfa. The proportion of patients using dornase alfa in Canadian clinical practice was reported to be approximately 50% of adults in 2019. This is similar to the percentage using dornase alfa in Study 104 (52.9%),9 but much lower than the percentages in Study 102 (80.9%), Study 103 (92.5%), and Study 109 (76.6%).7,8,10
Similar to the pivotal trials for LUM-IVA64 and TEZ-IVA,67,68 patients in the included studies for ELX-TEZ-IVA were permitted to use inhaled hypertonic saline during the trials. Inhaled hypertonic saline is commonly used in Canadian clinical practice; therefore, this feature improves the generalizability of the studies compared with the pivotal studies for IVA (i.e., STRIVE, ENVISION, and KONNECTION)71-73 where patients were required to discontinue usage of hypertonic saline. CDEC had previously noted that the exclusion of concomitant inhaled hypertonic saline was an important limitation of the IVA clinical trial.32,33
All the included studies evaluated absolute change from baseline in ppFEV1 as a primary and/or secondary end point; however, the timing of evaluation and placement with the statistical testing hierarchy differed across the trials (see Table 13). Spirometry measurements were standardized and performed according to the American Thoracic Society Guidelines (e.g., pre-bronchodilator and before dosing).74,75 Study 102 evaluated the impact of ELX-TEZ-IVA on a range of different outcomes that are important in the management of CF. These included respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., weight and BMI), health-related quality of life (CFQ-R), and clinical events (e.g., pulmonary exacerbations). The other studies included fewer end points (as summarized in Table 13); however, reviewers for the FDA noted that the end points in Study 103 were acceptable end points for a CF development program and acceptable for a 4-week clinical trial.29 As noted in the input from clinician groups, the end points that were in the clinical trials largely align with those that are evaluated in routine clinical practice.
The 4, 8, and 24-week treatment periods used in the included studies were sufficient for observing treatment differences in the primary and secondary end points; however, the duration was insufficient to observe whether treatment with ELX-TEZ-IVA has the potential to modify the course of disease for patients with CF with at least 1 F508del-CFTR mutation. Reviewers for the EMA also noted that important efficacy parameters such as exacerbations and BMI cannot be reliably measured in a study with a duration of 4 weeks (i.e., the duration of Study 103) and considered the extension data from Study 105 as an acceptable source of longer-term efficacy data.48 CADTH has supplemented this review with the data from Study 105 (see Long-Term Extension Studies)2 as well as the sponsor’s simulation study used to estimate the impact of CFTR modulator treatment on morbidity and mortality (see Simulation Study for Morbidity and Mortality).6
As with the pivotal trials conducted for IVA, LUM-IVA, and TEZ-IVA, patients with CF who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA studies.7-10 According to the Canadian CF Registry, 7.8% of the Canadian CF population had received a lung transplant as of 20191; hence, this is a relatively large subpopulation patients who were not studied in the clinical trials. The clinician groups who provided input noted there is a lack of evidence regarding whether ELX-TEZ-IVA would benefit patients with CF who have had a lung transplant. The experts consulted by CADTH noted that ELX-TEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. For those who have undergone a liver transplant, ELX-TEZ-IVA could be initiated as the drug may benefit the patient’s lung function. Post-liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug (due to the potential risk of hepatic AEs with ELX-TEZ-IVA).
As is common in clinical trial settings, patients enrolled in the included RCTs received extensive contact with health professionals over the study periods (e.g., 7 clinic visits and 1 phone contact over a 6-month period in Study 102).7-10 This level of contact is not reflective of routine care for patients with CF with relatively stable disease. The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months (although this has been less frequent in some cases due to the COVID-19 pandemic). The experts consulted by CADTH noted that the level of contact in the clinical trials is typical for CF studies and would not impact the generalizability of the results to the target population in Canada.
Adherence with study treatments was very high throughout the treatment periods of all studies (i.e., > 99%). The clinical experts consulted by CADTH noted that the level of adherence observed in the included studies is not reflective of typical adherence in Canada for adults and adolescents with CF, where adherence with treatments, including orally administered treatments, is considerably lower.66
Table 42 summarizes the generalizability of the evidence.
Table 42: Assessment of Generalizability of Evidence
Domain | Factor | Evidence | CADTH's assessment of generalizability |
|---|---|---|---|
Population | Age | The included trials enrolled patients who were at least 12 years of age at screening. | This is reflective of the indication under review by CADTH. |
Severity of disease | Patients with CF with more severe lung disease (e.g., ppFEV1 < 40% at screening) or a normal ppFEV1 at screening (≥ 90%) were excluded from the RCTs. | The results of the included studies are primarily applicable to patients with moderate (i.e., ppFEV1 40% to 69%) to mild (i.e., ppFEV1 70% to 89%) lung disease. An ad hoc subgroup analysis in Study 102 provided some efficacy data for a small subgroup of patients with ppFEV1 and suggested that ELX-TEZ-IVA resulted in clinically meaningful improvements relative placebo. | |
Post-transplant | Patients with CF who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA studies. | The experts consulted by CADTH noted: • ELX-TEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. • ELX-TEZ-IVA could be initiated in patients who have undergone a liver transplant (as the drug may benefit their lung function). Post-liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug. | |
Burkholderia cepacia complex | The studies excluded patients with a history of colonization with Burkholderia cenocepacia, Burkholderia dolosa, and/or Mycobacterium abscessus. | The clinical experts consulted by CADTH noted that the exclusion of such patients does not significantly lower the generalizability of the study results, given that these patients represent a small minority of those who could be eligible for ELX-TEZ-IVA and that the clinical management of such patients is more complex and variable. | |
Race | The study populations were comprised of almost exclusively White patients. | This reflective of most patients with CF in Canada, although the percentage is slightly higher than the percentage reported for the overall CF population in Canada (93.2% in 2019). | |
Intervention | ELX-TEZ-IVA | All the included studies investigated the use of ELX-TEZ-IVA at the dosage recommended in the product monograph. | In clinical practice, patients using the typical recommended dosage of ELX-TEZ-IVA, would take 2 tablets in the morning and 1 in the evening (i.e., 3 tablets per day). In contrast, patients in Studies 103, 104, and 109 would take 3 tablets in the morning and 1 tablet in the afternoon (i.e., 4 tablets per day). |
Concomitant medications | Concomitant medications for CF are reported in Table 19 for the included studies. | Concomitant medications were generally consistent with those used in Canadian clinical practice except for dornase alfa (estimated to used be approximately 50% of adults). This is similar to the percentage using dornase alfa in Study 104, but lower than the percentages in Study 102, Study 109, and Study 109. | |
Comparator | Placebo | Placebo was the comparator in Study 102. | The use of placebo as the comparator in Study 102 is appropriate as there are no drugs currently approved for use in the treatment of patients with CF who have an F/MF genotype. |
TEZ-IVA | TEZ-IVA was the comparator in Study 103, Study 109, and in Study 104 for the subset of patients with an F/RF genotype. | TEZ-IVA was an appropriate comparator in these studies as this drug is currently approved in Canada for the treatment of patients with CF with an F/F or F/RF genotype (although not reviewed by CADTH or currently reimbursed by the participating drug programs). | |
IVA | IVA was the comparator for the subset of patients in Study 104 with an F/G genotype. | IVA was an appropriate comparator in Study 104 for patients with an F/G genotype as this drug is currently approved in Canada for the treatment of patients with CF with gating mutations (including those who are heterozygous for the f058del mutation). | |
Outcomes | Hospitalizations | Planned and unplanned hospitalizations for CF did not include events that were due to protocol-defined pulmonary exacerbations. | Pulmonary exacerbations are the most common reason for CF-related hospitalizations in Canada; therefore, the exclusion of these events limits the generalizability of the planned and unplanned hospitalization end points. Those end points should be interpreted in conjunction with the data for pulmonary exacerbations that required hospitalization. |
Setting | Clinics | The included RCTs were conducted at specialized CF clinics. | This is consistent with Canadian clinical practice where patients are managed in specialized CF clinics. |
Locations and Canadian sites | Most patients in Study 104 were from Europe and Study 109 was conducted exclusively in Europe and Australia. | The clinical experts consulted noted that the results from the studies in Europe and Australia would likely be generalizable to the Canadian setting. | |
Contact with health care professionals | Patients enrolled in the included RCTs received extensive contact with health professionals over the study periods (e.g., 7 clinic visits and 1 phone contact in Study 102). | This level of contact is not reflective of routine care for patients with CF with relatively stable disease. Patients with stable disease would typically been seen 4 times per year (reduced to 3 times per year during the COVID-19 pandemic). |
CF = cystic fibrosis; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/MF = heterozygous for F508del mutation with 1 minimal function mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; TEZ = tezacaftor.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The sponsor’s objective for the indirect comparisons were to derive relative estimates of clinical efficacy for ELX-TEZ-IVA compared to local standard of care in the F/F, F/RF, and F/G populations, given the absence of RCTs.3 Although head-to-head trials were conducted for ELX-TEZ-IVA versus TEZ-IVA (for patients with F/F or F/RF genotypes) and IVA (for patients with an F/G genotype), the sponsor conducted indirect comparisons to derive estimates of effect for:
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In addition, CADTH conducted a literature search to identify published ITCs that included the patients, interventions, and outcomes as identified in the protocol for CADTH’s review of ELX-TEZ-IVA. A focused literature search for indirect comparisons dealing with CF was run-in MEDLINE All (1946–) and Embase (1974‒) on February 26, 2021. No limits were applied to the search. No published ITCs were identified. Therefore, this section presents the summary of methods and results as well as critical appraisal of the sponsor-submitted ITC.
Description of Indirect Comparison(s)
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 43: Study Selection Criteria and Methods for ITCs
Criteria | ITC for F/F Patients | ITC for F/G Patients | ITC for F/RF Patients |
|---|---|---|---|
Population | |||||||||||||||||||||||||||||||||||||||| |||||||||||||| | |||||||||||||||||||||||||||||||||| |||||||||||||||||||| | |||||||||||||||||||||||||||||||||| |||||||||||||||||||||| |
Intervention | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||
Comparator |
|
|
|
Outcome |
|
|
|
|
|
|
|
Publication characteristics | |||||||||||| | |||||||||||| | |||||||||||| |
Exclusion criteria | |||||||||||| | |||||||||||| | |||||||||||| |
Databases searched | |||||||||||| | |||||||||||| | |||||||||||| |
Selection process | |||||||||||| | |||||||||||| | |||||||||||| |
Data extraction process | |||||||||||| | |||||||||||| | |||||||||||| |
Quality assessment | |||||||||||| | |||||||||||| | |||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/F = homozygous for F508del mutation; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; ITC = indirect treatment comparison; IVA = ivacaftor; LUM-IVA = lumacaftor/ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; RD = respiratory domain; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s ITC.3
ITC for Patients With F/F Genotype
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
ITC Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 44: Indirect Comparisons for F/F Studies
Indirect estimate | Direct estimates (Study) | End points |
|---|---|---|
|||||||||||||| |||||||||||||||| | ELX-TEZ-IVA vs. TEZ-IVA (Study 109) + |||||||||||||||||||||||||||||||||||||||||||| |
|
|||||||||||||| |||||||||||||||||| | ELX-TEZ-IVA vs. TEZ-IVA (Study 109) + |||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; LUM-IVA = lumacaftor/ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison3
Results for ITC Analysis
Included Studies
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 10: Indirect Comparison Network for F/F Genotype

Confidential figure redacted at sponsor’s request.
ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/F = homozygous for F508del mutation; LUM-IVA = lumacaftor/ivacaftor; TEZ/IVA = tezacaftor/ivacaftor + ivacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Study Characteristics
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 45: Study Characteristics for F/F Studies
Characteristics | Study 109 | EVOLVE | TRAFFIC/TRANSPORT |
|---|---|---|---|
Study population | Patients with F/F genotype and ≥ 12 years of age | ||
Run-in period | 4 weeks with TEZ-IVA | None | None |
Treatment period | 24 weeks | 24 weeks | 24 weeks |
Treatment groups |
|
|
|
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% | 40% to 90% |
Schedule of assessments | Day 1, day 15, week 4, every 4 weeks thereafter | Day 1, day 15, week 4, every 4 weeks thereafter | Day 1, day 3, day 15, week 4, every 4 weeks thereafter |
Sample size |
|
|
|
Primary efficacy end point | Absolute change in CFQ-R RD score from baseline through 24 weeks | Absolute change from baseline in ppFEV1 through 24 weeks | Absolute change from baseline in ppFEV1 at 24 weeks (as assessed by the average absolute change at weeks 16 and 24) |
Other efficacy end points | SwCl, ppFEV1, BMI, weight-for-age z score, CFQ-R | SwCl, PEx, BMI, weight-for-age z score, CFQ-R | PEx, BMI, weight-for-age z score, CFQ-R |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; LUM = lumacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Baseline Characteristics
As shown in Table 46, mean ppFEV1 in Study 109 was 64.2% and 63.0% in the TEZ-IVA and ELX-TEZ-IVA groups, respectively, compared with 59.6% and 58.8% in the placebo and TEZ-IVA groups of EVOLVE, respectively, and 59.5% and 59.8% in the placebo and LUM-IVA groups of the pooled TRAFFIC/TRANSPORT studies, respectively. The proportion of male and female patients in each study was similar. The median age of patients was lowest in the TRAFFIC/TRANSPORT studies (23.0 and 24.0 years in the placebo and LUM-IVA groups, respectively) and highest in the TEZ-IVA group of Study 109 (27.7 years). The EVOLVE study had a lower proportion of adolescent patients compared with Study 109 and TRAFFIC/TRANSPORT. Sweat chloride levels were lower in Study 109 (89.8 mmol/L and 89.0 mmol/L in the TEZ-IVA and ELX-TEZ-IVA groups, respectively) compared with those in the EVOLVE trial (100.5 mmol/L and 101.3 mmol/L in the placebo and TEZ-IVA groups, respectively). Mean BMI was similar across the included studies.
Table 46: Baseline and Demographic Characteristics for F/F Studies
Characteristics | Study 109 | EVOLVE | TRAFFIC/TRANSPORT | ||||
|---|---|---|---|---|---|---|---|
TEZ-IVA N = 88 | ELX-TEZ-IVA N = 87 | Placebo N = 256 | TEZ-IVA N = 248 | Placebo N = 371 | LUM-IVA N = 369 | ||
Sex, n (%) | Male | 43 (48.9) | 44 (50.6) | 131 (51.2) | 127 (51.2) | 190 (51.2) | 187 (50.7) |
Female | 45 (51.1) | 43 (49.4) | 125 (48.8) | 121 (48.8) | 181 (48.8) | 182 (49.3) | |
Age at screening (years) | Mean (SD) | 27.6 (11.0) | 27.8 (11.8) | 25.7 (9.5) | 26.9 (11.2) | 25.3 (10.4) | 25.2 (9.6) |
Median | 27.7 | 25.7 | 25.0 | 25.0 | 23.0 | 24.0 | |
Age group at screening, n (%) | ≥ 12 to < 18 | 27 (30.7) | 25 (28.7) | 58 (22.7) | 58 (23.4) | 98 (26.4) | 98 (26.6) |
≥ 18 | 61 (69.3) | 62 (71.3) | 198 (77.3) | 190 (76.6) | 273 (73.6) | 271 (73.4) | |
ppFEV1 | Mean (SD) | 64.2 (15.1) | 63.0 (16.7) | 59.6 (15.0) | 58.8 (14.0) | 59.5 (13.2) | 59.8 (13.6) |
BMI (kg/m2) | Mean (SD) | 21.92 (3.89) | 21.17 (3.43) | 21.12 (2.88) | 20.96 (2.95) | 21.02 (2.92) | 21.50 (3.03) |
SwCl (mmol/L) | Mean (SD) | 89.8 (11.7) | 89.0 (12.2) | 100.5 (10.2) | 101.3 (10.9) | NA | NA |
CFQ-R (RD) score | Mean (SD) | 73.1 (17.6) | 71.2 (19.6) | 69.9 (16.6) | 70.1 (16.8) | 68.8 (17.3) | 68.3 (18.0) |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; NA = not applicable; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Indirect Comparison Results
Table 47 provides a summary of the results for the direct and indirect comparisons for studies conducted in patients with an F/F genotype. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo: |||||||||||||||||| |||||||||||||||||||||||||||||| for absolute change in ppFEV1 from baseline through 24 weeks; |||||||||||||||||||||||||||||||||||||||||||||||||| |||||| for absolute change in sweat chloride from baseline through 24 weeks; |||||||||||||||||||||||||||||||||||||||||||||||||||||||||| for absolute change in BMI from baseline at 24 weeks; and |||||||||||||||||||||||||||||||||||||||||||||||| for absolute change in weight-for-age z-scored from baseline at 24 weeks.
Indirect estimates of effect for ELX-TEZ-IVA compared with placebo are provided for each of the CFQ-R domains. Treatment with ELX-TEZ-IVA was favoured for respiratory symptoms ||||||||||||||||||||||||||||||||||||||||||||||||||||; physical functioning |||||||||||||||| ||||||||||||||||||||||||||||; vitality ||||||||||||||||||||||||||||||||||||||||||||||||; emotional functioning ||||||||||||||||||||||||||||||||||||||||||||||; eating problems (5.5; 95% CI, 1.5 to 9.5; P = 0.0075); treatment burden (9.6; 95% CI, 5.4 to 13.7; P < 0.0001); health perceptions ||||||||||||||||||||||||||||||||||||||||||||||||||; weight ||||||||||||||||||||||||||||||||||||||||||||||||||; role functioning |||||||||||||||||||||||||||||||||| | ||||||; and social functioning ||||||||||||||||||||||||||||||||||||||||||||||||.
Table 47: Results of Direct and Indirect Comparison for F/F Genotype
End point | Direct estimate ELX-TEZ-IVA vs. TEZ-IVA LSMD (95% CI), P value | Indirect estimates Bucher mean between-group difference (95% CI), P value | ||
|---|---|---|---|---|
|||||||||||| | |||||||||||| | |||
Absolute change in ppFEV1 from baseline through 24 weeks | 10.2 (8.2 to 12.1) < 0.0001 | |||||||||||| | ||||||||||||| | |
Absolute change in SwCl from baseline through 24 weeks | –42.9 (–46.3 to –39.5) < 0.0001 | |||||||||||| | ||||||||||||| | |
Absolute change in BMI (kg/m2) from baseline at 24 weeks | 1.44 (1.07 to 1.82) < 0.0001 | |||||||||||| | ||||||||||||| | |
Absolute change in weight-for-age z score from baseline at 24 weeks | 0.40 (0.31 to 0.49) < 0.0001 | |||||||||||| | ||||||||||||| | |
Absolute change from baseline through 24 weeks in CFQ-R domain score | Respiratory symptoms | |||||||||||| | ||||||||||||| | ||||||||||||||| |
Physical functioning | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Vitality | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Emotional functioning | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Body image | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Eating problems | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Treatment burden | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Health perceptions | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Weight | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Digestive symptoms | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
Role functioning | |||||||||||| | ||||||||||||| | |||||||||||||| | |
Social functioning | |||||||||||| | ||||||||||||| | ||||||||||||||| | |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; F/F = homozygous for F508del mutation; IVA = ivacaftor; LSMD = least squares mean difference; LUM = lumacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
Source: Sponsor’s Indirect Treatment Comparison.3
Critical Appraisal
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 48: Assessment of Homogeneity of the ITC for the F/F Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Treatment history | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial eligibility criteria | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Dosing of comparators | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Response in the common comparator (i.e., placebo) |
|
Definitions of end points | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |
Timing of end point evaluation or trial duration | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Clinical trial setting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Study design | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
ELX = elexacaftor; F/F = homozygous for F508del mutation; ITC = indirect treatment comparison; IVA = ivacaftor; LUM = lumacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor.
ITC for Patients With F/G Genotype
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||
It was not reported if a systematic literature search and review was undertaken by the sponsor to identify studies for inclusion; however, CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
ITC Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||
Table 49: Indirect Comparisons for F/G Studies
Indirect estimate | Direct estimates (study) | End points |
|---|---|---|
ELX-TEZ-IVA vs. placebo | ELX-TEZ-IVA vs. TEZ-IVA (subgroup data from Study 104) + IVA vs. placebo (meta-analysis of STRIVE, KONNECTION, and KONDUCT) |
|
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Results for ITC Analysis
Included Studies
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Figure 11: Indirect Comparison Network for F/G Genotype

Confidential figure redacted at sponsor’s request.
ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/G = heterozygous for F508del mutation with a gating mutation; IVA = ivacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Study Characteristics
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||
Table 50: Study Characteristics for F/G Studies
Characteristics | Study 104 (Subset of F/G) | STRIVE (Subset of F/G551D) | KONNECTION (Subset of F/Non-G551D) | KONDUCT (Subset of F/R117H) |
|---|---|---|---|---|
Study population | Patients with F/G (incl. F/R117H) or F/RF genotypes and ≥ 12 years of age | Patients with ≥ 1 G551D gating mutation and ≥ 12 years of age | Patients with ≥ 1 non-G551D gating mutation and ≥ 6 years of age | Patients with ≥ 1 R117H mutation and ≥ 6 years of age |
Design | DB, active-controlled, parallel group RCT | DB, active-controlled, parallel group RCT | DB placebo-controlled, crossover RCT | DB, active-controlled, parallel group RCT |
Active run-in period | 4 weeks with TEZ-IVA or IVA | None | None | None |
Treatment period | 8 weeks | 48 weeks | 8 weeks | 24 weeks |
Treatment groups |
|
|
|
|
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% | ≥ 40% | 40% to 90% for patients aged ≥ 12 years |
Schedule of assessments | Day 1, day 15, week 4, week 8 | Day 1, day 15, week 8, every 4 weeks thereafter | Day 1, week 2, week 4, week 8 of each treatment period | Day 1, week 2, week 4, week 8, week 16, week 24 |
Sample size |
|
|
|
|
|
|
|
|
|
Primary efficacy end point | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through 24 weeks | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through 24 weeks |
Other end points | BMI, CFQ-R, SwCl, weight | BMI, CFQ-R, PEx, SwCl, weight | BMI, CFQ-R, PEx, SwCl, weight | BMI, CFQ-R, PEx SwCl, weight |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; DB = double blind; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/R117H = heterozygous for F508del mutation with 1 R117H mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; ITC = indirect treatment comparison; IVA = ivacaftor; LUM = lumacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s ITC.3
Baseline Characteristics
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||
Table 51: Baseline and Demographic Characteristics for F/G Studies
Characteristics | Study 104 subset of F/G | |||||||||||||||||| | ||||||||||||||| | ||||||||||||||| | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
IVA N = 45 | ELX-TEZ-IVA N = 50 | |||||||||||| |||||| | |||||||||||| |||||| | |||||||||||| |||||| | |||||||||||| |||||| | |||||||||||| |||||| | |||||||||||| |||||| | |||||||
Sex, n (%) | Male | 28 (62.2) | 28 (56.0) | |||||||||||||||| | ||||||||||||||| | ||||||||||||||| | |||||||||||||||| | |||||||||||||||| | ||||||||||||||||| | |||||
Female | 17 (37.8) | 22 (44.0) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | ||||||
Age at screening (years) | Mean (SD) | 30.7 (11.2) | 33.4 (13.8) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
Median | 29.0 | 32.7 | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | ||||||
Age group at screening, n (%) | ≥ 12 to < 18 | 6 (13.3) | 8 (16.0) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
≥ 18 | 39 (86.7) | 42 (84.0) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | ||||||
ppFEV1 | Mean (SD) | 68.1 (16.6) | 66.0 (14.8) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
BMI (kg/m2) | Mean (SD) | 22.91 (3.39) | 23.71 (3.76) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
SwCl (mmol/L) | Mean (SD) | 47.6 (19.1) | 50.9 (23.3) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
CFQ-R RD score | Mean (SD) | 75.8 (17.6) | 76.3 (16.4) | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Indirect Comparison Results
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 52: Results of Direct and Indirect Comparison for F/G Genotype
End point | Direct estimate ELX-TEZ-IVA vs. IVA LSMD (95% CI), P value | Indirect estimates Bucher mean between-group difference (95% CI), P value | ||
|---|---|---|---|---|
||||||||||| | ||||||||||| | |||
Absolute change in ppFEV1 from baseline through 8 weeks | 5.7 (3.5 to 7.9), < 0.0001 | ||||||||||| | ||||||||||| | |
Absolute change in SwCl from baseline through 8 weeks | –20.9 (−27.7 to –14.1), < 0.0001 | ||||||||||| | ||||||||||| | |
Absolute change in BMI (kg/m2) from baseline at 8 weeks | 0.16 (–0.10 to 0.42), 0.2142 | ||||||||||| | ||||||||||| | |
Absolute change in weight-for-age z-scored from baseline at 8 weeks | 0.01 (–0.06 to 0.08), 0.7765 | ||||||||||| | |||||||||| | |
Absolute change from baseline through 8 weeks in CFQ-R domain score | Respiratory symptoms | 8.8 (3.7 to 13.9), 0.0010 | ||||||||||| | ||||||||||| |
Physical functioning | 5.3 (0.8 to 9.7), 0.0205 | ||||||||||| | ||||||||||| | |
Vitality | 1.1 (–4.1 to 6.2), 0.6792 | ||||||||||| | ||||||||||| | |
Emotional functioning | 2.1 (–1.6 to 5.8), 0.2659 | ||||||||||| | ||||||||||| | |
Body image | –3.0 (–7.9 to 2.0), 0.2383 | ||||||||||| | ||||||||||| | |
Eating problems | –1.3 (–5.2 to 2.6), 0.4976 | ||||||||||| | ||||||||||| | |
Treatment burden | 2.3 (–2.1 to 6.6), 0.3075 | ||||||||||| | ||||||||||| | |
Health perceptions | 4.8 (–0.1 to 9.7), 0.0568 | ||||||||||| | ||||||||||| | |
Weight | –3.5 (–10.3 to 3.3), 0.3106 | ||||||||||| | ||||||||||| | |
Digestive symptoms | 3.0 (–1.5 to 7.6), 0.1881 | ||||||||||| | ||||||||||| | |
Role functioning | 0.8 (–5.3 to 6.9), 0.7878 | ||||||||||| | ||||||||||| | |
Social functioning | 2.8 (–2.6 to 8.1), 0.3064 | ||||||||||| | ||||||||||| | |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; IVA = ivacaftor; LSMD = least squares mean difference; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
Source: Sponsor’s Indirect Treatment Comparison.3
Critical Appraisal
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 53: Assessment of Homogeneity of the ITC for the F/G Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Treatment history | Patients in Study 104 underwent open-label treatment with IVA or TEZ-IVA (for those with F/G and F/RF genotypes respectively) for 4 weeks before initiating treatment with the randomized study drugs (i.e., none of the patients were naive to CFTR modulator therapy at the time of baseline measurements). |
Clinical trial eligibility criteria | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Dosing of comparators | The study drugs were used in accordance with recommendations in the Canadian product monographs for ELX-TEZ-IVA and IVA. |
Response in the common comparator (i.e., placebo) | There were differences in the treatment effects in the placebo groups across the 3 placebo-controlled trials:
|
Definitions of end points | The end points included in the ITC were similarly defined and evaluated for each of the included studies. |
Timing of end point evaluation or trial duration | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Withdrawal frequency | There were few withdrawals from each of the trials included in the ITC analysis. |
Clinical trial setting | All 4 of the studies included in the ITC were phase III RCTs conducted at specialized CF clinics. |
Study design | As shown in Table 50, there were differences in the following aspects of the studies:
|
CF = cystic fibrosis; CFTR = cystic fibrosis transmembrane conductance regulator; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/R117H = heterozygous for F508del mutation with 1 R117H mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; ITC = indirect treatment comparison; IVA = ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
ITC for Patients With F/RF Genotype
Study Selection Methods
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||
It was not reported if a systematic literature search and review was undertaken by the sponsor to identify studies for inclusion; however, CADTH did not identify any additional studies that would have met the inclusion criteria but were not included in the ITC.
ITC Analysis Methods
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 54: Indirect Comparisons for F/RF Studies
Indirect estimate | Direct estimates (study) | End points |
|---|---|---|
ELX-TEZ-IVA vs. placebo | ELX-TEZ-IVA vs. TEZ-IVA (subgroup data from Study 104) + TEZ-IVA vs. placebo (EXPAND) |
|
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Results for ITC Analysis
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Figure 12: Indirect Comparison Network for F/RF Genotype

Confidential figure redacted at sponsor’s request.
ELX/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/RF = heterozygous for F508del mutation with a residual function mutation; TEZ/IVA = tezacaftor/ivacaftor + ivacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Study Characteristics
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||.
Table 55: Study Characteristics for F/RF Studies
Characteristics | Study 104 | EXPAND |
|---|---|---|
Study population | Patients with F/G (incl. F/R117H) or F/RF genotypes and ≥ 12 years of age | Patients with F/RF genotypes and ≥ 12 years of age |
Design | DB, active-controlled, parallel group RCT | DB, placebo-controlled, crossover RCT |
Active run-in period | 4 weeks with TEZ-IVA or IVA | None |
Treatment period | 8 weeks | 8 weeks |
Treatment groups |
|
|
ppFEV1 inclusion criteria at screening | 40% to 90% | 40% to 90% |
Schedule of assessments | Day 1, day 15, week 4, week 8 | Day 1, day 15, week 4, week 8, week 12 of each treatment period |
Sample size |
|
|
|
|
|
Primary efficacy end point | Absolute change in ppFEV1 from baseline through 8 weeks | Absolute change in ppFEV1 from baseline through average of week 4 and week 8 measurements |
Other end points | BMI, CFQ-R, SwCl, body weight (Did not include PEx as an efficacy end point) | BMI, CFQ-R, PEx, SwCl, body weight |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; DB = double blind; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; incl. = including; ITC = indirect treatment comparison; IVA = ivacaftor; PEx = pulmonary exacerbation; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s ITC.3
Baseline Characteristics
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| ||||||||||||||||||||||||||||||||||||||||||
Table 56: Baseline and Demographic Characteristics for F/RF Studies
Characteristics | Study 104 | |||| | |||
|---|---|---|---|---|---|
TEZ-IVA N = 81 | ELX-TEZ-IVA N = 82 | |||| |||| | |||| |||| | ||
Sex, n (%) | Male | 37 (45.7) | 37 (45.1) | |||| | |||| |
Female | 44 (54.3) | 45 (54.9) | |||| | |||| | |
Age at screening (years) | Mean (SD) | 41.3 (14.4) | 40.1 (14.7) | |||| | |||| |
Median | 42.0 | 40.3 | |||| | |||| | |
Age group at screening, years, n (%) | 12 to < 18 | 3 (3.7) | 7 (8.5) | |||| | |||| |
≥ 18 | 78 (96.3) | 75 (91.5) | |||| | |||| | |
ppFEV1 | Mean (SD) | 68.1 (16.4) | 67.8 (16.3) | |||| | |||| |
BMI (kg/m2) | Mean (SD) | 24.68 (5.22) | 24.29 (5.23) | |||| | |||| |
SwCl (mmol/L) | Mean (SD) | 61.4 (27.3) | 64.7 (27.9) | |||| | |||| |
CFQ-R (RD) score | Mean (SD) | 78.1 (14.7) | 76.7 (16.9) | |||| | |||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; ELX = elexacaftor; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; RD = respiratory domain; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
Source: Sponsor’s Indirect Treatment Comparison.3
Indirect Comparison Results
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 57: Results of Direct and Indirect Comparison for F/RF Genotype
End point | Direct estimate ELX-TEZ-IVA vs. TEZ-IVA LSMD (95% CI), P value | Indirect estimates Bucher mean between-group difference (95% CI), P value | ||
|---|---|---|---|---|
||||||||| | ||||||||| | |||
Absolute change in ppFEV1 from baseline through 8 weeks | 1.9 (0.5 to 3.4), 0.0104 | ||||||||| | ||||||||| | |
Absolute change in SwCl from baseline through 8 weeks | –24.1 (–27.6 to –20.5), < 0.0001 | ||||||||| | ||||||||| | |
Absolute change in BMI (kg/m2) from baseline at 8 weeks | 0.13 (–0.08 to 0.33), 0.2245 | ||||||||| | ||||||||| | |
Absolute change in weight-for-age z score from baseline at 8 weeks | 0.03 (–0.02 to 0.08), 0.2253 | ||||||||| | ||||||||| | |
Absolute change from baseline through 8 weeks in CFQ-R domain score | Respiratory symptoms | 8.8 (4.3 to 13.4), 0.0002 | ||||||||||||||| | ||||||||||||||| |
Physical functioning | 3.6 (–0.1 to 7.3), 0.0569 | ||||||||||||||| | ||||||||||||||| | |
Vitality | 7.0 (2.3,11.8), 0.0042 | ||||||||||||||| | ||||||||||||||| | |
Emotional functioning | 1.2 (–1.9 to 4.4), 0.4367 | ||||||||||||||| | ||||||||||||||| | |
Body image | 1.2 (–2.2 to 4.7), 0.4813 | ||||||||||||||| | ||||||||||||||| | |
Eating problems | 4.8 (1.0 to 8.5), 0.0128 | ||||||||||||||| | ||||||||||||||| | |
Treatment burden | 1.5 (–2.5 to 5.6), 0.4546 | ||||||||||||||| | ||||||||||||||| | |
Health perceptions | 6.8 (2.3 to 11.2), 0.0031 | ||||||||||||||| | ||||||||||||||| | |
Weight | 2.5 (–2.7 to 7.7), 0.3500 | ||||||||||||||| | ||||||||||||||| | |
Digestive symptoms | –2.3 (–6.9 to 2.2), 0.3090 | ||||||||||||||| | ||||||||||||||| | |
Role functioning | 0.0 (–3.7 to 3.7), 0.9973 | ||||||||||||||| | ||||||||||||||| | |
Social functioning | 2.4 (–2.0 to 6.8), 0.2858 | ||||||||||||||| | ||||||||||||||| | |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; F/RF = heterozygous for F508del mutation with a residual function mutation; IVA = ivacaftor; LSMD = least squares mean difference; ppFEV1 = percent predicted forced expiratory volume in 1 second; SwCl = sweat chloride; TEZ = tezacaftor; vs. = versus.
Source: Sponsor’s Indirect Treatment Comparison.3
Critical Appraisal for ITC Analysis
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
As noted in Table 58, there are important differences in the baseline and end point values across Study 104 and the |||||||| trial, due to the 4 weeks of active treatment that patients in Study 104 received before randomization.
Table 58: Assessment of Homogeneity of the ITC for the F/RF Genotype
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Treatment history | Patients in Study 104 underwent open-label treatment with IVA or TEZ-IVA (for those with F/G and F/RF genotypes respectively) for 4 weeks before initiating treatment with the randomized study drugs (i.e., none of the patients were naive to CFTR modulator therapy at the time of baseline measurements). |
Clinical trial eligibility criteria | The inclusion criteria differed across the 2 studies with respect to CFTR genotypes. Study 104 enrolled patients with F/G (including F/R117H) or an F/RF genotype. |||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||. |
Response in the common comparator (i.e., TEZ-IVA) | Due to the different designs of Study 104 and the ||||||||||||||, there are important differences in the change from baseline within the TEZ-IVA groups that were included in the indirect comparisons:
|
Dosing of comparators | Both ELX-TEZ-IVA and TEZ-IVA were administered in accordance with recommendations in the Canadian product monographs.12,30 However, patients in the TEZ-IVA group of Study 104 would have received this drug for a total of 12 weeks (i.e., 4 weeks in the run-in period and then 8 weeks in the double-blind phase) compared with ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
Definitions of end points | The end points included in the ITC were similarly defined and evaluated for each of the included studies. |
Timing of end point evaluation or trial duration | Both Study 104 and the |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. |
Withdrawal frequency | There were few withdrawals from each of the trials included in the ITC analysis. |
Clinical trial setting | Both Study 104 and |||||||| were phase III RCTs conducted at specialized CF clinics. |
Study design | Study 104 and |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||| in Study 104 where all patients received treatment with TEZ-IVA before randomization. |
CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; F/G = heterozygous for F508del mutation with a gating mutation; F/R117H = heterozygous for F508del mutation with 1 R117H mutation; F/RF = heterozygous for F508del mutation with a residual function mutation; ITC = indirect treatment comparison; IVA = ivacaftor; MMRM = mixed-effects model for repeated measures; ppFEV1 = percent predicted forced expiratory volume in 1 second; RCT = randomized controlled trial; SD = standard deviation; SwCl = sweat chloride; TEZ = tezacaftor.
Summary
The sponsor conducted 3 indirect comparisons using the Bucher method to derive relative estimates of clinical efficacy for: ELX-TEZ-IVA |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||. The sponsor included phase III RCTs that enrolled patients with CF who were at least 12 years of age, had end point measurements at the same time as the ELX-TEZ-IVA studies (i.e., Study 109 and Study 104), included relevant comparators, and enrolled patients with the genotypes of interest (i.e., F/F, F/G, and F/RF).
For patients with an F/F genotype, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 24 weeks: |||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||||||||| for BMI; and |||||||||||||||||||||||||||||||| for the CFQ-R (RD).
For patients with an F/G genotype, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 8 weeks: |||||||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||||||||| for BMI; and |||||||||||||||||||||||||||||| for the CFQ-R (RD).
For patients with an F/RF genotype, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||. The sponsor reported the following indirect estimates of effect for ELX-TEZ-IVA compared with placebo for absolute change from baseline through 8 weeks: |||||||||||||||||||||||||||||||| for ppFEV1; |||||||||||||||||||||||||||||||||||||||||| for BMI; and || |||||||||||||||||||||||||| for the CFQ-R (RD).
The primary limitation of the ITCs was the difference in study design across the included studies. The ELX-TEZ-IVA studies (i.e., Study 104 and Study 109) included the open-label, 4-week active treatment period with TEZ-IVA or IVA before randomization. || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||. As both the ELX-TEZ-IVA and the comparator groups of Study 104 and Study 109 received 4 weeks of treatment with a CFTR modulator, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Other Relevant Evidence
This section includes a summary of the long-term extension study included in the sponsor’s submission to CADTH and 3 additional relevant studies that were considered to address important gaps in the evidence included in the systematic review. Additional information is required on the longer-term efficacy and safety of ELX-TEZ-IVA, and in patients with FEV1 less than 40%, who were excluded from the RCTs, thus data from extension Study 105,2,78 and from 2 observational studies in patients with advanced lung disease have been summarized.4,5 The longer-term impacts of ELX-TEZ-IVA on CF-related morbidity and mortality are unknown, thus the modelling study by Stanojevic et al.6 has been appraised in this section.
Long-Term Extension Studies
This section includes data from Study 105, an ongoing, open-label extension study submitted by the sponsor to CADTH.2,78 This study provides data on longer-term safety and efficacy of ELX-TEZ-IVA in patients with CF (12 years and older) who were either homozygous for the F508del mutation in the CFTR gene (F/F) or who had 1 F508del mutation and 1 MF mutation in the CFTR gene (F/MF). The extension phase studies for patients who were enrolled in Study 104 (i.e., Study 110) and Study 109 (i.e., Study 113) are currently ongoing and no data were available at the time of CADTH’s review.
Methods
Study 105 is an ongoing, open-label uncontrolled trial that enrolled patients with CF aged 12 years and older, who are homozygous or heterozygous for the F508del mutation, and who completed Study 102 or 103 (i.e., patients with either an F/MF or an F/F genotype). A total of || patients were enrolled, with safety and efficacy data reported for || patients who received at least 1 dose of the study drug. The results are summarized for the pre-specified second interim analysis that was conducted after all patients had reached the 24-week visit (data cut-off October 2019).2 The planned treatment duration is 96 weeks, plus a 4-week safety follow-up period.
Populations
All patients who completed Study 102 or Study 103 were eligible for Study 105. This included patients who had their treatment interrupted in the double-blind parent study but completed the last study visit. For the inclusion and exclusion criteria for the Study 102 and 103, please see Table 7 in the Pivotal Studies section of this report.
The demographics of patients included in Study 105 are provided in Table 59, with a breakdown according to parent study and prior treatment received. The baseline data reported reflects the baseline measurement in the parent study. In the overall population of Study 105, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 59: Patient Demographics for Study 105 (FAS)
Baseline characteristica | Parent Study 102 | Parent Study 103 | Study 105 | ||
|---|---|---|---|---|---|
Prior placebo N = 203 | Prior ELX-TEZ-IVA N = 196 | Prior TEZ-IVA N = 52 | Prior ELX-TEZ-IVA N = 55 | |||||||||||| |||||||| | |
Sex, n (%) | |||||
Male | 105 (51.7) | 102 (52.0) | 24 (46.2) | 24 (43.6) | |||| |
Female | 98 (48.3) | 94 (48.0) | 28 (53.8) | 31 (56.4) | |||| |
Age at baseline (years) | |||||
Mean (SD) | 26.8 (11.3) | 25.7 (9.7) | 27.9 (10.8) | 28.8 (11.5) | |||| |
Median (range) | 25.0 (12.3 to 64.0) | 24.4 (12.1 to 59.9) | 27.6 (12.4 to 60.5) | 27.4 (12.7 to 54.1) | |||| |
≥ 12 to < 18 years | 60 (29.6) | 55 (28.1) | 14 (26.9) | 16 (29.1) | |||| |
≥ 18 years | 143 (70.4) | 141 (71.9) | 38 (73.1) | 39 (70.9) | |||| |
Race, n (%) | |||||
White | 184 (90.6) | 183 (93.4) | 52 (100.0) | 54 (98.2) | |||| |
African American | 2 (1.0) | 4 (2.0) | 0 (0) | 0 (0) | |||| |
Asian | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | |||| |
American Indian | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | |||| |
Other | 1 (0.5) | 2 (1.0) | 0 (0) | 0 (0) | |||| |
Not collectedb | 16 (7.9) | 8 (4.1) | 0 (0) | 1 (1.8) | |||| |
Hispanic or Latino, n (%) | |||||
Yes | 12 (5.9) | 4 (2.0) | 3 (5.8) | 2 (3.6) | |||| |
No | 175 (86.2) | 184 (93.9) | 49 (94.2) | 52 (94.5) | |||| |
Not collectedb | 16 (7.9) | 8 (4.1) | 0 (0) | 1 (1.8) | |||| |
Geographic Region, n (%) | |||||
North America | 120 (59.1) | 117 (59.7) | 33 (63.5) | 34 (61.8) | |||| |
Europe/Australia | 83 (40.9) | 79 (40.3) | 19 (36.5) | 21 (38.2) | |||| |
Weight (kg) | |||||
Mean (SD) | 58.3 (12.7) | 60.0 (12.9) | 59.8 (14.8) | 59.9 (12.7) | |||| |
Median (range) | 58.0 (31.3 to 105.2) | 58.0 (29.0 to 108.0) | 55.0 (36.0 to 100.0) | 59.0 (36.0 to 91.2) | |||| |
BMI (kg/m2) | |||||
Mean (SD) | 21.3 (3.14) | 21.5 (3.08) | 21.9 (4.12) | 21.8 (3.19) | |||| |
Median (range) | 20.8 (14.4 to 33.8) | 21.4 (15.0 to 30.9) | 20.8 (15.6 to 34.6) | 21.4 (16.0 to 28.4) | |||| |
ppFEV1 category at baseline, n (%) | |||||
< 40 | 16 (7.9) | 18 (9.2) | 4 (7.7) | 6 (10.9) | |||| |
≥ 40 to < 70 | 120 (59.1) | 112 (57.1) | 34 (65.4) | 31 (56.4) | |||| |
≥ 70 to ≤ 90 | 62 (30.5) | 65 (33.2) | 14 (26.9) | 18 (32.7) | |||| |
> 90 | 5 (2.5) | 1 (0.5) | 0 (0) | 0 (0) | |||| |
ppFEV1 at baseline | |||||
Mean (SD) | 61.3 (15.5) | 61.4 (14.9) | 60.2 (14.4) | 61.6 (15.4) | |||| |
Median (range) | 60.9 (32.3 to 93.7) | 61.4 (33.8 to 97.1) | 58.4 (35.0 to 89.0) | 61.0 (35.0 to 87.4) | |||| |
Sweat Chloride (mmol/L) at baseline | |||||
Mean (SD) | 102.9 (9.8) | 102.4 (11.9) | 90.0 (12.3) | 91.4 (11.0) | |||| |
Median (range) | 104.0 (68.5 to 137.0) | 103.0 (22.5 to 156.0) | 90.8 (60.5 to 112.0) | 92.8 (67.0 to 114.0) | |||| |
CFQ-R (Respiratory Domain) at baseline | |||||
Mean (SD) | 70.0 (17.8) | 68.2 (16.8) | 72.6 (17.9) | 70.6 (16.2) | |||| |
Median (range) | 72.2 (16.7 to 100.0) | 72.2 (16.7 to 100.0) | 72.2 (27.8 to 100.0) | 72.2 (22.2 to 100.0) | |||| |
Medication use at screening, n (%) | |||||
CFTR modulator | NR | NR | NR | NR | |||| |
Dornase alfa | 164 (80.8) | 161 (82.1) | 48 (92.3) | 51 (92.7) | |||| |
Azithromycin | 114 (56.2) | 109 (55.6) | 25 (48.1) | 33 (60.0) | |||| |
Inhaled antibiotic | 132 (65.0) | 116 (59.2) | 28 (53.8) | 35 (63.6) | |||| |
Bronchodilator | 192 (94.6) | 184 (93.9) | 47 (90.4) | 54 (98.2) | |||| |
Inhaled corticosteroids | 122 (60.1) | 120 (61.2) | 28 (53.8) | 36 (65.5) | |||| |
Hypertonic saline | 129 (63.5) | 145 (74.0) | 42 (80.8) | 38 (69.1) | |||| |
Pseudomonas aeruginosa infection within 2 years of screening, n (%) | |||||
Positive | 142 (70.0) | 147 (75.0) | 31 (59.6) | 39 (70.9) | |||| |
Negative | 61 (30.0) | 49 (25.0) | 21 (40.4) | 16 (29.1) | |||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; FAS = full analysis set; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; NR = not reported; SD = standard deviation; TEZ = tezacaftor.
aBaseline of parent study (i.e., Study 102 or Study 103).
bNot collected in accordance with local regulations.
Source: Clinical Study Report.2
Intervention
All patients received open-label ELX 200 mg, TEZ 100 mg, and IVA 150 mg every morning and IVA 150 mg every evening (or the same dose as previously received in Study 102 or 103). |||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Outcomes
The primary objective of Study 105 was to examine the safety and tolerability of ELX-TEZ-IVA, with longer-term efficacy as a secondary objective of the trial. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Statistical Analysis
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Patient Disposition
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 60: Patient Disposition in Study 105
Disposition, n (%) | Prior placebo Study 102 | Prior ELX-TEZ-IVA Study 102 | Prior TEZ-IVA Study 103 | Prior ELX-TEZ-IVA Study 103 | |||||||||||||||||||| |
|---|---|---|---|---|---|
Enrolled, N | 203 | 197 | 52 | 55 | |||| |
Completed 24-week visit, n (%) | 200 (98.5) | 192 (98) | 51 (98.1) | 54 (98.2) | |||| |
Discontinued treatment before 24-week visit, n (%) | 3 (1.5) | 4 (2.0) | 1 (1.9) | 1 (1.8) | |||| |
Adverse events | 2 (1.0) | 2 (1.0) | 1 (1.9) | 1 (1.8) | |||| |
Patient refusal | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | |||| |
Lost to follow-up | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | |||| |
Pregnancy (self or partner) | 0 (0) | 1 (0.5) | 0 (0) | 0 (0) | |||| |
Completed 48-week visit, n (%) | 0 (0) | 0 (0) | 24 (46.2) | 25 (45.5) | |||| |
Discontinued treatment before 48-week visit, n (%) | 4 (2.0) | 4 (2.0) | 3 (5.8) | 2 (3.6) | |||| |
Adverse events | 2 (1.0) | 2 (1.0) | 2 (3.8) | 1 (1.8) | |||| |
Patient refusal | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) | |||| |
Lost to follow-up | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | |||| |
Pregnancy (self or partner) | 0 (0) | 1 (0.5) | 1 (1.9) | 1 (1.8) | |||| |
FAS | 203 | 196 | 52 | 55 | |||| |
Safety set | 201 | 198 | 52 | 55 | |||| |
ELX = elexacaftor; FAS = full analysis set; IVA = ivacaftor; TEZ = tezacaftor.
aOne patient was enrolled in Study 105 but never received a dose of ELX-TEZ-IVA and was excluded from FAS and safety set.
Source: Clinical Study Report.2
Exposure to Study Treatments
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Efficacy
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||
Table 61 provides a summary of the change from baseline in ppFEV1, sweat chloride, CFQ-R (RD), BMI, BMI z score, and weight after 24 weeks of the extension period for those patients who enrolled from Study 102, and up to 36 weeks for those who enrolled from Study 103. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 13: Absolute Change From Baseline in ppFEV1 for Patients From Study 102 Who Entered Study 105 (FAS)

Confidential figure redacted at sponsor’s request.
445 to 102 = Study 102; FAS = full analysis set; LS = least squares; MMRM = mixed-effects model for repeated measures; OL = open-label; PBO = placebo; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; VX-445/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Note: y-axis corresponds to the LS means from the MMRM models at the interim analysis.
Source: Clinical Study Report.2
Figure 14: Absolute Change From Baseline in ppFEV1 for Patients From Study 103 Who Entered Study 105 (FAS)

Confidential figure redacted at sponsor’s request.
445 to 103 = Study 103; FAS = full analysis set; LS = least squares; MMRM = mixed-effects model for repeated measures; OL = open-label; PBO = placebo; ppFEV1 = percent predicted forced expiratory volume in 1 second; SE = standard error; VX-445/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Note: y-axis corresponds to the LS means from the MMRM models at the interim analysis.
Source: Clinical Study Report.2
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Figure 15: Absolute Change From Baseline in BMI for Patients From Study 102 Who Entered Study 105 (FAS)

Confidential figure redacted at sponsor’s request.
445 to 102 = Study 102; BMI = body mass index; FAS = full analysis set; LS = least squares; MMRM = mixed-effects model for repeated measures; OL = open-label; PBO = placebo; SE = standard error; VX-445/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Note: y-axis corresponds to the LS means from the MMRM models at the interim analysis.
Source: Clinical Study Report.2
Figure 16: Absolute Change From Baseline in BMI for Patients From Study 103 Who Entered Study 105 (FAS)

Confidential figure redacted at sponsor’s request.
445 to 103 = Study 103; BMI = body mass index; FAS = full analysis set; LS = least squares; MMRM = mixed-effects model for repeated measures; OL = open-label; PBO = placebo; SE = standard error; VX-445/TEZ/IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Note: y-axis corresponds to the LS means from the MMRM models at the interim analysis.
Source: Clinical Study Report.2
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||
Table 61: Summary of Efficacy Outcomes for Study 105 (FAS)
Analysis | Study 105 (week 24) | Study 105 (week 36) | ||
|---|---|---|---|---|
Placebo in Study 102 N = 203 | ELX-TEZ-IVA in Study 102 N = 196 | TEZ-IVA in Study 103 N = 52 | ELX-TEZ-IVA in Study 103 N = 55 | |
Absolute change from baseline in ppFEV1 (%)a | ||||
Number of patients included in analysis (%) | 189 (93) | 180 (92) | 49 (94) | 51 (93) |
LS mean (95% CI) | 14.9 (13.5 to 16.3) | 14.3 (12.9 to 15.7) | 12.8 (10.1 to 15.4) | 11.9 (9.3 to 14.5) |
Absolute change from baseline in CFQ-R Respiratory Domain (points)a,b | ||||
Number of patients included in analysis (%) | 197 (97) | 192 (98) | 51 (98) | 54 (98) |
LS mean (95% CI) | 19.2 (16.7 to 21.7) | 20.1 (17.6 to 22.6) | 13.8 (8.9 to 18.8) | 14.3 (9.5 to 19.2) |
Absolute change from baseline in sweat chloride (mmol/L)a,b | ||||
Number of patients included in analysis (%) | 187 (92) | 183 (93) | 48 (92) | 50 (91) |
LS mean (95% CI) | –50.3 (–52.9 to –47.8) | –49.0 (–51.6 to –46.4) | –49.4 (–54.3 to –44.5) | –47.2 (–52.0 to –42.5) |
Absolute change from baseline in BMI (kg/m2)a | ||||
Number of patients included in analysis (%) | 196 (97) | 190 (97) | 51 (98) | 53 (96) |
LS mean (95% CI) | 1.2 (1.0 to 1.4) | 1.3 (1.1 to 1.5) | 1.2 (0.8 to 1.5) | 1.3 (1.0 to 1.7) |
Absolute change from baseline in BMI z scorea,c | ||||
Number of patients included in analysis (%) | |||||| | |||||| | |||||| | |||||| |
LS mean (95% CI) | |||||| | |||||| | |||||| | |||||| |
Absolute change from baseline in body weight (kg)a | ||||
Number of patients included in analysis (%) | |||||| | |||||| | |||||| | |||||| |
LS mean (95% CI) | |||||| | |||||| | |||||| | |||||| |
BMI = body mass index; CFQ-R = Cystic Fibrosis Questionnaire–Revised; CI = confidence interval; ELX = elexacaftor; FAS = full analysis set; IVA = ivacaftor; LS = least squares; MMRM = mixed-effects model for repeated measures; NR = not reported; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor.
aData analyzed using the baseline from the parent study. MMRM model with covariates for treatment (as randomized in parent study), visit, treatment*visit interaction, parent study baseline ppFEV1, age group at screening of the parent study (< 18 years vs. ≥ 18 years). Analysis of data from Study 102 also included covariate for sex (male vs. female).
bFor patients previously enrolled in Study 103, the change from baseline in sweat chloride and CFQ-R (Respiratory Domain) were reported for the 24-week visit of the extension study.
cBMI z score was analyzed for patients aged 20 years or younger from the start of the parent study.
Source: Clinical Study Report.2
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, and 0.30 (95% CI, 0.20 to 0.45) for those previously enrolled in Study 103. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Table 62: Summary of Pulmonary Exacerbations Outcomes for Study 105 (FAS)
Analysis | Study 105 (week 24) | Study 105 (week 36) | |
|---|---|---|---|
Placebo in Study 102 |||| | ELX-TEZ-IVA in Study 102 |||| | TEZ-IVA or ELX-TEZ-IVA in Study 103 |||| | |
Cumulative number of pulmonary exacerbationsa | |||
Total number of years of the cumulative treatment period | |||||| | |||||| | |||||| |
Number of patients included in analysis (%) | |||||| | |||||| | |||||| |
Number of patients with events (%) | |||||| | |||||| | |||||| |
Number of events | |||||| | |||||| | |||||| |
Estimated event rate per year (95% CI)b | |||||| | |||||| | |||||| |
Time-to-first pulmonary exacerbation | |||
Number of patients included in analysis (%)a | |||||| | |||||| | |||||| |
Number of patients with events (%) | |||||| | |||||| | |||||| |
Probability of event-free survival at 24 weeks, KM estimate (95% CI) | |||||| | |||||| | |||||| |
Probability of event-free survival at 24 weeks, KM estimate (95% CI) | |||||| | |||||| | |||||| |
CI = confidence interval; ELX = elexacaftor; FAS = full analysis set; IVA = ivacaftor; KM = Kaplan–Meier; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor.
aPulmonary exacerbations event rate was calculated as the total number of events multiplied by 336 days, divided by the total number of days from the first dose of ELX-TEZ-IVA in the parent or extension study (1 year = 336 days). The analysis included 405 patients enrolled in Study 102 and 108 patients enrolled in Study 103.
bNegative binomial model that includes covariates for parent study baseline ppFEV1 and age group at screening of the parent study (≥ 12 to < 18 vs. ≥ 18 years) with log(duration of cumulative ELX-TEZ-IVA efficacy period in years) as offset. Analysis of Study 102 data also included a covariate for sex (male vs. female).
Source: Clinical Study Report.2
Harms
Most patients (93%) reported at least 1 AE during the extension study (740 events out of 100 patient-years). The most reported events were infective pulmonary exacerbation of CF (25%), cough (23%), oropharyngeal pain (15%), and nasopharyngitis (14%). Seven patients (1.4%) stopped treatment due to AEs. The reasons for discontinuation were elevated transaminase levels (3 patients), hepatic encephalopathy (1), depression (1), rash (1), and tinnitus and contusion (1). Eighty patients (16%) experienced a SAE and grade 3 or 4 AEs were reported by 53 patients (11%). No deaths were reported during Study 105.
Thirty-six patients (7%) reported an elevated transaminase event including 11 patients (2%) whose treatment was interrupted as a result. Three patients stopped treatment due to elevated transaminase levels of which 2 patients were classified as experiencing a SAE. Twenty-three patients (5%) had elevated bilirubin events including 19 patients (4%) where the total bilirubin was 2 or more times the ULN. Rash events were reported by 50 patients (10%; 15.8 events out of 100 patient-years). One rash event was classified as a SAE that resolved after treatment was discontinued. No cataracts were reported in the extension period.
Table 63: Summary of Harms in Study 105 (Safety Set)
Adverse events | ELX-TEZ-IVA (|) | |
|---|---|---|
n (%) | Events/100 PY | |
Patients with any adverse event | 471 (93) | 739.9 |
Most common adverse eventsa | ||
Infective pulmonary exacerbation of CF | 127 (25) | 49.6 |
Cough | 118 (23) | 44.3 |
Oropharyngeal pain | 27.0 (15) | 25.7 |
Nasopharyngitis | 69 (14) | 21.6 |
Headache | 66 (13) | 24.9 |
Sputum increased | 63 (13) | 20.6 |
Upper respiratory tract infection | 60 (12) | 18.3 |
Fatigue | 51 (10) | 16.3 |
Nasal congestion | |||||| | |||||| |
Treatment discontinuation due to adverse events | 7 (1) | 3.3 |
Patients with Grade 3 or 4 adverse events | 53 (11) | 19.8 |
Patients with serious adverse events | 80 (16) | 27.5 |
Most common serious adverse eventsb | ||
Infective pulmonary exacerbation of CF | 42 (8) | 12.2 |
Distal intestinal obstruction syndrome | 5 (1) | 1.5 |
Hemoptysis | 5 (1) | 1.5 |
Vascular device infection | 3 (< 1) | 0.8 |
Influenza | 2 (< 1) | 0.5 |
ALT increased | 2 (< 1) | 0.5 |
AST increased | 2 (< 1) | 0.5 |
Deaths | 0 (0) | 0 (0) |
Notable harms | ||
Transaminase elevation events | 36 (7) | 16.5 |
Bilirubin elevation events | 23 (5) | NR |
Rash events | 50 (10) | 15.8 |
Cataracts | 0 (0) | 0 (0) |
ALT = alanine transaminase; AST = aspartate transaminase; CF = cystic fibrosis; ELX = elexacaftor; IVA = ivacaftor; NR = not reported; PY = patient-years; TEZ = tezacaftor.
aReported in 10% of patients.
bReported in at least 2 patients.
Source: Clinical Study Report.2
Critical Appraisal
Internal Validity
Study 105 is an ongoing, uncontrolled, open-label trial that enrolled patients with CF (aged ≥ 12 years) who had at least 1 F508del mutation and who had completed Study 102 or Study 103. As this was an unblinded study, patient’s expectations of treatment could potentially have biased the reporting of subjective outcomes, such as respiratory symptoms (as measured by the CFQ-R), or harms. Extension studies are often limited by selection bias, as only patients who are tolerant to treatment and complete the parent studies are eligible to enroll. For Study 105, the risk of selection bias may be low given that only | patients (||||) out of the || randomized in the parent studies, were not enrolled or treated in the extension study. During the first 24 weeks of follow-up, discontinuation of treatment was also low ( | patients, ||||); however the frequency of missing data was higher for some outcomes relative to others. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || ||||||||||
Data on pulmonary exacerbations were based on a standard definition; |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
External Validity
Issues with the generalizability of these data are the same as for the parent double-blind studies. Please refer to the Systematic Review Critical Appraisal section for a discussion on the external validity of Study 102 and Study 103.
Observational Studies in Patients With Advanced Lung Disease
Two observational studies in patients with advanced pulmonary disease were identified in the literature search conducted by CADTH. The retrospective chart review by O’Shea et al. included 14 patients who received ELX-TEZ-IVA through a managed care program in Ireland.4 The prospective observational cohort study conducted by Burgel et al. reported data for 245 patients who received ELX-TEZ-IVA through an early access program in France.5
Description and Appraisal of Irish Cohort Study
Methods
O’Shea et al.4 reported on a retrospective chart review conducted at the Irish National Referral Centre for Adult CF based in an academic health centre in Dublin, Ireland. Through a managed access program, patients who were homozygous for F508del or heterozygous for F508del with a second MF CFTR mutation were eligible to receive ELX-TEZ-IVA if they had severe lung disease (defined as FEV1 less than 40% predicted) or were on an active lung transplantation list.
Populations
A total of 14 adult patients were initiated on ELX-TEZ-IVA between December 2019 and July 2020. The study included 9 women and 5 men with severe lung disease, 2 of whom were on the transplant list. The mean age of patients was 34.4 years (range = 19 years to 46 years). Eight patients (57%) were homozygous for the F508del mutation and had previously received CFTR modulatory therapy. The other 6 patients were heterozygous for the F508del mutation. All patients were pancreatic insufficient. Other comorbidities included CF-related diabetes (9 patients) and CF-related liver disease (6 patients), including 1 patient who required dose reduction of ELX-TEZ-IVA due to Child-Pugh Score B liver disease. In the year before initiating ELX-TEZ-IVA, the patients had a median of 3 hospitalizations (interquartile range [IQR] = 2.0 to 4.3) and required a median total of 77 days of IV treatment (IQR 43.5 to 137.5 days). Mean ppFEV1, BMI, and sweat chloride levels at baseline are shown in Table 64.
Interventions
All patients received open-label ELX-TEZ-IVA (dose not specified).
Outcomes
Outcomes of interest included the change from baseline in ppFEV1, BMI, and sweat chloride levels, the number of infective pulmonary exacerbations, days spent on IV antibiotics, and the presence of CF comorbidities (i.e., CF-related diabetes or liver disease).
Statistical Analysis
A paired t-test was used to analyze the change in ppFEV1, BMI, and sweat chloride levels, with a 2-sided P value less than 0.05 considered statistically significant. The most recent outcome measurement before the start of ELX-TEZ-IVA was used as the baseline values. The frequency of pulmonary exacerbations was analyzed as the number of events per month, compared with the monthly frequency of events in the year before starting therapy. A chi-square test was used to analyze categorical variables.
Exposure to Study Treatments
Patients were followed for a mean of 4.9 months (SD = 1.9; range 1 months to 8 months) after starting ELX-TEZ-IVA.
Efficacy
The rate of infective pulmonary exacerbations requiring hospitalization was 0.28 events per month (SD = 0.17) in the 12 months before ELX-TEZ-IVA, and 0.04 events per month (SD = 0.07) during the 4.9 month follow-up period (N = 7; P < 0.001).
The mean ppFEV1 improved from 27% (SD = 7.3) at baseline to 36% (SD = 16.5) after a mean follow-up of 26 days (N = 14) (Table 64). The mean BMI increased from 20.7 kg/m2 (SD = 3.6) to 22.1 kg/m2 (SD = 3.4; N = 14), and the mean sweat chloride fell from 105 mmol/L (SD = 15) to 54 mmol/L (SD = 23; N = 11) after an average of 62 days of follow-up.
Table 64: Summary of Efficacy Outcomes–Irish Cohort Study
Outcome | N | Baseline | End point | P valuea | Follow-up time, days, mean (SD) |
|---|---|---|---|---|---|
ppFEV1, %, mean (SD) | 14 | 27.3 (7.3) | 36.3 (16.5) | < 0.0001 | 26.4 (4.2) |
BMI, kg/m2, mean (SD) | 14 | 20.7 (3.6) | 22.1 (3.4) | < 0.0001 | 62 (35) |
Sweat chloride, mmol/L, mean (SD) | 11 | 104.9 (15.0) | 53.6 (23.3) | < 0.0001 | 64 (84) |
BMI = body mass index; ppFEV1 = percent predicted forced expiratory volume in 1 second; SD = standard deviation.
aPaired t-test.
Source: O’Shea et al. (2021).4
Harms
One patient experienced a SAE and required hospitalization for distal intestinal obstruction syndrome. One other patient required treatment interruption due to acute kidney injury that was consider unrelated to the ELX-TEZ-IVA. No other AEs were reported by O’Shea et al.4
Critical Appraisal
O’Shea et al. provides descriptive data for 14 patients with advanced lung disease who were treated with open-label ELX-TEZ-IVA. The mean follow-up time was limited (< 5 months), with the change in ppFEV1 and BMI reported after an average of 1 to 2 months. It appears that exacerbation data were only available for 7 of the 14 patients, and the accuracy and completeness of these data are uncertain. Due to the retrospective design, the study relied on data already collected, which may be missing or inaccurate. Moreover, monitoring and reporting of patient outcomes may have been impacted by the COVID-19 pandemic and lockdown measures. Some of the differences observed in the frequency of exacerbations may be attributable to seasonal variation, and considering the short follow-up time, these data should be interpreted with caution. The generalizability of the findings may be limited given that they were based on a limited sample of patients from a single centre in Ireland and may be subject to selection bias. In addition, the study was published as a letter to the editor and has not undergone peer review.
Description and Appraisal of French Cohort Study
Methods
The objective of the prospective cohort study by Burgel et al. was to evaluate the real-world efficacy and safety of ELX-TEZ-IVA in patients with CF and advanced pulmonary disease.5 The study, conducted by the French CF Reference Center Network, included patients from all 47 CF centres in France who received ELX-TEZ-IVA through an early access program.
Populations
Starting in December 2019, patients with CF were eligible to receive ELX-TEZ-IVA through the early access program if they were aged 12 years or older, had a least 1 F508del mutation, and had advanced respiratory disease (defined as ppFEV1 < 40%), or were under evaluation for lung transplantation. All patients who received ELX-TEZ-IVA in France between December 2020 and August 2021 were included in the study (N = 245).
The median age of patients treated was 31 years (IQR = 24 years to 38 years), of which 17 were adolescents (7%) (Figure 17). Most patients were male (55%) and heterozygous for the F508del mutation (59%). The median baseline ppFEV1 was 29% (IQR = 24% to 34%). Most patients were pancreatic insufficient (96%), 43% had CF-related diabetes, and 6% had cirrhosis or portal hypertension. The patients had received a median 43 days of IV antibiotics (IQR = 24 days to 70 days) and spent 7 days in hospital (IQR = 0 days to 29 days) in the past 12 months.
Most patients were not receiving a CFTR modulator at the start of the study (186 patients, 76%). Of these patients, 41 had previously received LUM-IVA or IVA but had stopped treatment due to AEs (30 patients), lack of effectiveness (10 patients), or other reasons (1 patient). At the start of the study, 59 patients (24%) were switched from another CFTR modulator to ELX-TEZ-IVA (LUM-IVA for 55 patients, TEZ-IVA for 3 patients, and IVA for 1 patient). The patients enrolled were receiving the following other CF therapies at baseline: azithromycin (70%), inhaled antibiotics (76%), dornase alfa (54%), inhaled hypertonic saline (19%), inhaled corticosteroids (50%), oral corticosteroids (11%), long-term oxygen therapy (44%), non-invasive ventilation (29%), and enteral tube feeding (18%).
Figure 17: Baseline Characteristics–French Cohort Study
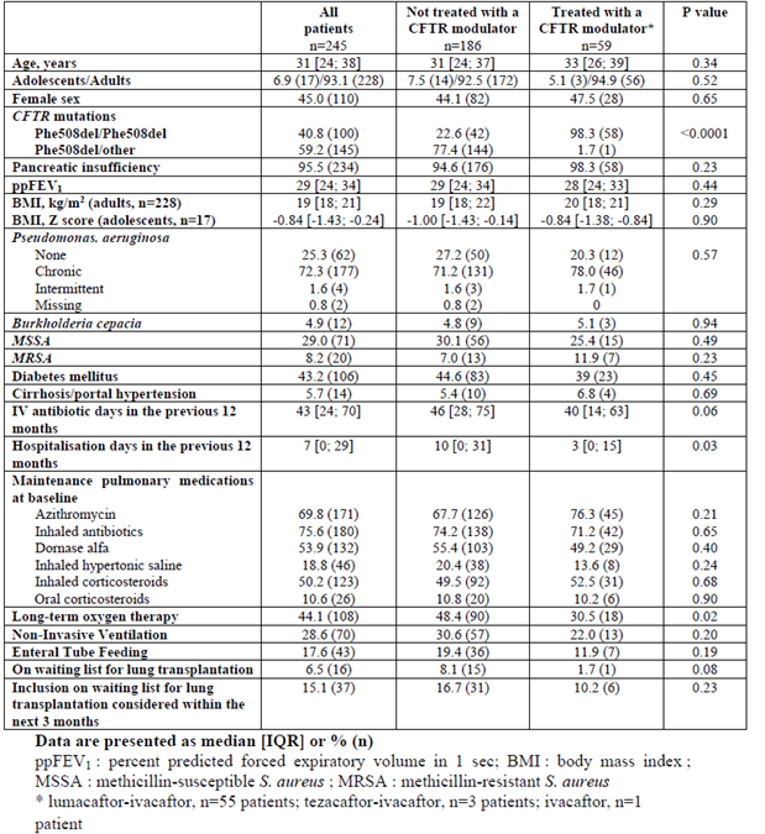
CFTR = cystic fibrosis transmembrane conductance regulator; IQR = interquartile range.
Source: Reproduced from Burgel et al. (2021).5
Interventions
Patients received open-label ELX 200 mg plus TEZ 100 mg once daily, and IVA 150 mg twice daily unless dose modifications were required as per the manufacturer’s recommendations.
Outcomes
Key outcomes were lung transplantation and death, as well as underlying treatment requirements (i.e., oxygen, enteral tube feeding). Change in lung function (ppFEV1) and weight (in kg) were compared between patients who were and were not receiving another CFTR modulator before starting ELX-TEZ-IVA. Comparisons were also completed for patients who were and were not on long-term oxygen or non-invasive ventilation before initiation, and for patients with a ppFEV1 increase above and below the median response for the cohort.
Comparisons were made on the mean number of lung transplantations per year in 2020 versus 2018 to 2019 for all patients with CF in France (approximately 7,500 patients in 2019). Re-transplantations were not included in the counts. The number of deaths without transplantation for 2020 was compared to data from 2015 to 2018. Historical data were obtained from the French CF Registry (deaths) and the Agence de la Biomédecine Registry (transplants), and 2020 data were supplied by the French CF and transplant centres.
Data on patient characteristics were collected at baseline and subsequent visits from the CF centres. Treatment-related AEs documented by the referral physicians were collected from patients’ charts. Scheduled visits were planned at baseline and 1, 3, 6, and 12 months after initiating therapy.
Statistical Analysis
Available data were reported descriptively with between-group comparisons analyzed using a chi-square test or t-test. The change from baseline in ppFEV1 and weight were analyzed using the Wilcoxon paired test. The McNemar paired test was used to analyze the proportion of patients treated with long-term oxygen, non-invasive ventilation, or enteral tube feeding at baseline and at 1 month and 3 months post-initiation. Statistical significance was determined based on a P value of less than 0.05. No a priori hypotheses were defined and there was no imputation for missing data.
Due to the COVID-19 pandemic and the disruption in scheduled clinic visits, some patients were missing the 1- or 3-month follow-up visits. Thus, the authors pooled data for the 2 time points and analyzed the results using the best available data (median observation time 73 days [IQR = 32 days to 88 days]). No details were provided on how the pooled analysis was conducted.
Patient Disposition
A total of 245 patients were included in the study. At the interim analysis cut-off date (September 7, 2020), 7 patients had not had a follow-up visit and 2 patients received a lung transplant shortly after initiation and were therefore excluded from the analysis. Thus, outcome data were reported for 236 patients (96%).
Exposure to Study Treatments
Most patients received the standard dose of ELX-TEZ-IVA (94%), but 15 patients had doses reduced due to drug interactions (10 patients), pre-existing liver disease (3 patients), or other reasons (2 patients). At the interim data analysis cut-off, the median follow-up time was 84 days (range = 16 days to 209 days; IQR = 70 days to 104 days) after the start of ELX-TEZ-IVA.
Efficacy
For the overall cohort, the change from baseline data for ppFEV1 and weight were reported based on pooled 1- and 3-month end point data. The change from baseline in the ppFEV1 was 15.1% (95% CI = 13.8 to 16.4; P < 0.0001; N = 232) and weight was 4.2 kg (95% CI, 3.9 to 4.6; P < 0.0001; N = 236). The change in ppFEV1 and weight for the subgroup of patients who were switched from another CFTR modulator to ELX-TEZ-IVA and those who were not receiving an CFTR modulator at the start of ELX-TEZ-IVA therapy, are summarized in Figure 18.
Prior to the start of ELX-TEZ-IVA therapy, 43% and 28% of patients were receiving long-term oxygen or non-invasive ventilation, respectively (data missing for 4% of patients). At the 1-month visit, 31% and 24% of patients were on oxygen or non-invasive ventilation (missing data for 18% of patients) and at the 3-month visit 23% and 20% remained on oxygen or non-invasive ventilation (missing data for 32% of patients) (P < 0.001 for comparisons versus baseline).
At the start of therapy, 18% of patients were receiving enteral tube feeding, with 12% and 10% on enteral feeding at the 1- and 3-months visits (P < 0.01 versus baseline). Data were missing for 6%, 18%, and 31% of patients at baseline, 1-month, and 3-month visits, respectively.
Prior to initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates in the next 3 months (total of 53 patients; 22%). At the end of follow-up, 5 patients (2%) were on the transplant list or being considered for transplant, 2 patients had received a transplant (0.8%), and 1 patient died while waiting for transplant (0.4%).
Among all patients with CF in France, 33 patients received a lung transplant in 2020 (33 of 265 patients; 12.5%) compared with 72 patients in 2018 and 80 patients in 2019 (overall 152 patients of 735 patients; 21%) (Fisher exact test P = 0.002). In 2020, 16 patients with CF died without transplant, compared to an average of 20 patients per year for 2015 to 2018. Of note 16 of 33 patients who received a transplant and 10 of 16 who died in 2020, were eligible to receive ELX-TEZ-IVA (i.e., had at least 1 F508del mutation); however only 3 patients had received ELX-TEZ-IVA.
No data were reported on the use of IV antibiotics to treat pulmonary exacerbations.
Figure 18: Change in ppFEV1 and Weight–French Cohort Study
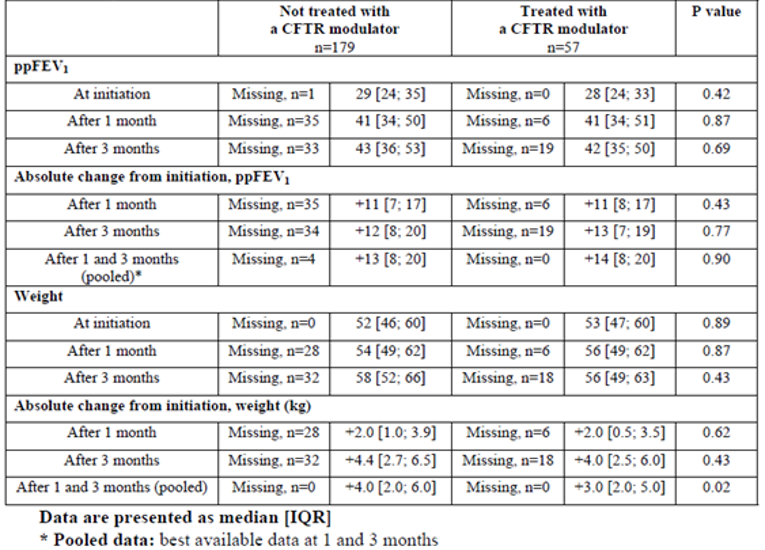
CFTR = cystic fibrosis transmembrane conductance regulator; IQR = interquartile range; ppFEV1 = percent predicted forced expiratory volume in 1 second.
Source: Reproduced from Burgel et al. (2021).5
Harms
The most common treatment-related AEs are summarized in Table 65. These events included gastrointestinal symptoms (10%), localized cutaneous rash (7%), myalgia (5%), and increased bilirubin 3 times or greater the ULN (5%). No patients permanently stopped treatment due to AEs, but 14 patients (6%) had treatment interrupted during the follow-up period reported (median 84 days; IQR = 70 days to 104 days). Rash was the most common reason for temporary discontinuation of ELX-TEZ-IVA. No patients had their therapy interrupted due to increases in liver enzymes, bilirubin, or creatine phosphokinase levels.
Table 65: Adverse Events Potentially Attributable to Treatment–French Cohort Study
Adverse event | n (%) |
|---|---|
Localized cutaneous rash | 17 (7.2) |
Generalized cutaneous rash | 9 (3.8) |
Gastrointestinal symptoms | 24 (10.2) |
Myalgia | 11 (4.7) |
Headache | 10 (4.2) |
Elevated alanine transaminase ≥ 3 x ULN | 6 (2.5) |
Elevated aspartate transaminase ≥ 3 x ULN | 2 (0.8) |
Increase bilirubin ≥ 3 x ULN | 11 (4.7) |
Creatine phosphokinase ≥ 3 x ULN | 8 (3.4) |
ULN = upper limit of normal.
Note: Total N = 236.
Source: Burgel et al. (2021).5
Critical Appraisal
Internal Validity
Burgel et al. (2021)5 provides descriptive data on 245 patients in France with CF and advanced lung disease who were treated with ELX-TEZ-IVA. The prospective, uncontrolled cohort study included all patients who received ELX-TEZ-IVA through an early access program (from all 47 CF centres in France); however, not all patients who were potentially eligible for ELX-TEZ-IVA received treatment. The authors estimated that approximately 78% of eligible patients with advanced lung disease who had at least 1 F508del mutation were included in the study. No information was provided on the patients who did not receive ELX-TEZ-IVA; thus, it is difficult to evaluate the potential for selection bias, and if the patients included in the study are representative of the larger population of patients with advanced pulmonary disease.
Although the study was prospective in design, there were no details on how outcome data were captured, and the planned visit schedule was disrupted due to the COVID-19 pandemic. The 1- and 3-month outcome data were missing for 14% to 32% of patients, with no imputation for missing data. Although the authors attempted to address the missing data for ppFEV1 and weight by pooling the “best available data,” the methods used were not clearly stated. Selecting the “best” result could potentially bias the results if a “better” 1-month result was selected for inclusion in the analysis in patients who were showing a decline in pulmonary function at 3 months. Due to the extent of missing data on the need for oxygen, non-invasive ventilation or enteral tube feeding (18% to 32%), it is difficult to interpret the results of these outcomes.
There were no a priori hypotheses and no adjustments for multiplicity for the outcomes tested. Between-group comparisons were conducted based on a chi-square or t-test, with no adjustment for potential confounders. The observed reduction in lung transplants in patients with CF was potentially confounded by the disruption to the health care system caused by the COVID-19 pandemic and the availability of donor organs. Indeed, Burgel et al. reported that the overall number of lung transplants was 26% lower in 2020. No details were provided on the patient characteristics and other factors that may have impacted the transplant rates, thus the crude estimate of the change in the number of transplants should be interpreted with caution.
The follow-up time was limited (median 84 days) and the authors stated the treatment duration was insufficient to determine the impact on IV antibiotic use. Limited data were reported on AEs during treatment.
External Validity
The clinical experts consulted by CADTH noted the study populations are similar to patients with CF in Canada who have severe illness and that the outcomes assessed were clinically relevant.
Simulation Study for Morbidity and Mortality
The objective of the study by Stanojevic et al.6 was to estimate the potential impact of ELX-TEZ-IVA on morbidity and mortality of patients with CF, including the impact of delayed access to therapy, using a microsimulation model.
Model Structure and Inputs
The model included 4 transition states: mild (ppFEV1 > 70%), moderate (ppFEV1 = 40% to 70%), severe lung function (ppFEV1 < 40%), and transplant. It also included states for lost to follow-up and death. Based on the transition probabilities, patients could randomly move through the states until either lost to follow-up, death, or transplant.
Individual patient history data from the CCFR were used to populate the model. The CCFR includes patients with CF who are followed by 1 of 42 CF clinics in Canada and who have provided consent to participate in the registry (> 99%). All patients who were alive in 2018 were included as the initial population, with their age and pulmonary function state in 2018 used as the baseline.
Transition probabilities were calculated using a logistic regression model based on CCFR data from 2017 to 2018. CCFR data from 2017 was also used to determine the baseline rate of pulmonary exacerbations (i.e., IV antibiotic administered in the hospital or at home) for patients with mild, moderate, and severe lung function status (0.09, 0.09 and 2.2 events per year, respectively).
Based on incidence rates from the CCFR, the model assumed there would be 130 patients newly diagnosed per year, which were distributed across the age spectrum as follows: 0 to 1 years, 69%; 1 to 2 years, 15%; 2 to 18 years, 9%; 18 to 40 years, 6%. The model assumed that children under 6 years of age would have mild pulmonary disease, and that 2.5% of patients aged 20 to 60 years would be lost to follow-up per year (no loss to follow-up for those less than 20 years of age).
All patients 12 years or older who had at least 1 F508del mutation were assumed to receive treatment with ELX-TEZ-IVA. Based on data from Study 102,41 the model assumed patients would show a mean acute increase of 13.8% (SD = 8.6) in the absolute ppFEV1. The model also included a 63% reduction in the rate of pulmonary exacerbations (i.e., 0.055 events per year for patients in the mild state, 0.055 events per year for moderate, and 1.35 events per year for severe). Observational data for IVA was used to predict the rate of lung function decline in patients treated with triple therapy (rate of decline reduced by an average of 50%, SD = 5%).79 The rate of death or transplant was the same for treated and un-treated patients.
The population was simulated from 2019 to 2030 for scenarios that assumed there were no new therapies (baseline analysis) and if ELX-TEZ-IVA was introduced in 2021 or 2025. Ten replications of each scenario were performed, and the results were averaged. The Kaplan–Meier survival curves and median survival were estimated based on individual’s vital status in 5-year blocks (i.e., the median age of survival between 2021 and 2025, or 2026 and 2030). The analysis was run using R software (MicSim package).
Results
The initial population included 4,440 patients who had a reported pulmonary function values in 2017 or 2018 (children aged < 6 years were assumed to be in the healthy state). Of these patients, 62% had mild, 23% had moderate, and 9% had severe lung function values. The baseline model, which assumed no new therapies were introduced, estimated the CF population would increase to 5,415 patients (SD = 15) by 2030 and have a similar distribution of lung function states as the initial population (mild 59%, moderate 22%, and severe 8%). In the simulation where eligible patients received ELX-TEZ-IVA starting in 2021, the total CF population increased to 5,497 patients (SD = 10) in 2030. The distribution of patients with mild, moderate, and severe lung function was 69%, 19%, and 4%, respectively. If ELX-TEZ-IVA was introduced in 2025, the model estimated there would be 5,450 patients (SD = 15) with CF in 2030, and 66%, 20%, and 6% would have mild, moderate, and severe lung function, respectively.
Figure 19 shows a projected survival curve for each scenario in 2030. The estimated median age of survival for the initial population was 57.6 years (95% CI, 52.2 to 62.3) and for the baseline scenario (no new treatments) was 58.4 years (95% CI, 56.9 to 59.8) 2030. If ELX-TEZ-IVA was introduced in 2021, the estimated median age of survival was 67.5 years (95% CI, 66.7 to 68.4), and if ELX-TEZ-IVA was introduced in 2025, the median age of survival was estimated at 63.1 years (95% CI, 62.4 to 63.9) in 2030. The simulated difference in median age of survival was 9.2 years (95% CI, 7.5 to 10.8) and 3.3 years (95% CI, 1.7 to 5.0) if ELX-TEZ-IVA was introduced in 2021 or 2025 respectively, compared with the baseline scenario.
The simulations projected that the total number of pulmonary exacerbations requiring hospitalization or home IV antibiotics would be reduced if all eligible patients received treatment with ELX-TEZ-IVA starting in 2021 (early) or 2025 (delayed) compared with baseline. The early introduction scenario predicted 1,700 (SD = 14) exacerbations in 2030, and the delayed introduction of ELX-TEZ-IVA predicted 1957 (SD = 25) exacerbations. In comparison, the baseline scenario predicted 2,310 (SD = 37) exacerbations in 2030. Cumulatively, the model predicted 25,370 exacerbations (SD = 177) between 2019 and 2030 in the baseline scenario, with 2,141 fewer events (95% CI, 2,043 to 2,239) in the delayed scenario, and 4,135 (95% CI, 4,042 to 4,226) fewer events in the early adoption scenario for ELX-TEZ-IVA.
The model projected there would be 146 fewer transplants by 2030 if ELX-TEZ-IVA was introduced in 2021, and 98 fewer transplants if introduced in 2025.
Figure 19: Microsimulation of Projected Median Survival in 2030
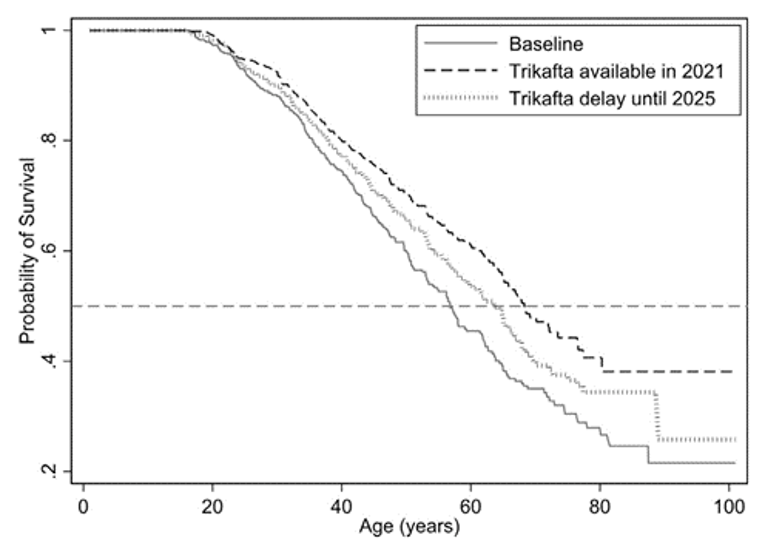
Note: Comparison of the projected median age of survival in 2030 from a single simulation in the baseline scenario (no new therapies or treatments, current transition rates), if elexacaftor/tezacaftor/ivacaftor is introduced in 2021 (“Early”), and if elexacaftor/tezacaftor/ivacaftor is delayed until 2025 (“Delayed”).
Source: Reprinted from Journal of Cystic Fibrosis, 20(2), Stanojevic S, Vukovojac K, Sykes J, Ratjen F, Tullis E, Stephenson AL, Projecting the impact of delayed access to elexacaftor/tezacaftor/ivacaftor for people with Cystic Fibrosis, pg.P243 to 249, 2021, with permission from Elsevier.6
Critical Appraisal
Stanojevic et al.6 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. Individual patient data from the CCFR were used to inform the transition probabilities, exacerbation, and incidence rates and to model the initial population. Use of Canadian data improves the applicability to the current decision problem. In addition, the CCFR has internal checks and validation steps in the electronic data capture system, and quarterly audits to verify and validate the data, which improves the accuracy and completeness of the observational data.
The key issue with the simulation study is the number of assumptions required to build the model and extrapolate the impacts out to 10 years. The major assumptions that impart uncertainty are as follows:
The effects of ELX-TEZ-IVA on ppFEV1 and exacerbations were informed by Study 102, which was 24 weeks in duration. Currently 48 weeks of data are available from an uncontrolled extension study to determine if the observed effects persist in the longer-term.
The model assumes that all patients treated with ELX-TEZ-IVA experience an acute increase in ppFEV1, regardless of their genotype, baseline ppFEV1, or prior exposure to CFTR modulators. The mean 13.8% acute increase in ppFEV1 used to populate the model was based on Study 102, which enrolled a specific subset of patients with CF (i.e., F/MF mutation; CFTR modulator treatment-naive; ppFEV1 ≥ 40 and ≤ 90). It is unclear if the acute effects observed apply to patients who were excluded from this trial. There was variation in the acute treatment effects observed across the other ELX-TEZ-IVA trials which enrolled treatment-experienced patients with different genotypes. These studies reported between-group differences ranging from 3.5% to 10.2% in absolute change ppFEV1. Moreover, none of the trials included patients with normal ppFEV1, thus it is unclear if the acute change in ppFEV1 observed with treatment of ELX-TEZ-IVA is applicable in this population.
The model assumes a 50% reduction in decline in ppFEV1 over time compared with patients not receiving a CFTR modulator, based on US and UK longer-term observational studies with IVA. Currently, there is no information on the impact of ELX-TEZ-IVA on ppFEV1 over time, moreover the background rate of decline in ppFEV1 in the CF population is uncertain. It is unclear if the results of US and UK observational data are representative of the population who receive ELX-TEZ-IVA.
The model assumed a 63% reduction in pulmonary exacerbations for patients treated with ELX-TEZ-IVA based on 24-week data from Study 102. As noted above, there are issues with the extrapolation of short-term data from a subset of patients with CF to the entire modelled population in the longer-term. It also appears that the modelled reduction in pulmonary exacerbations was in addition to the impacts of changes in ppFEV1 on pulmonary exacerbations, thus the effect on exacerbations may be overestimated.
The model assumes all patients 12 years or older with at least 1 F508del mutation will receive treatment for the duration of the simulation. This likely overestimates the number of patients who will be treated, as it does not consider patients with contraindications to treatment, or discontinuation of therapy due to adverse effects or other reasons. The model makes now allowances for nonadherence to treatment and its impact on treatment effects.
No sensitivity analyses were conducted to estimate the impact of various assumptions on the simulation results.
Stanojevic et al.6 also listed other limitations, including that the model defined disease states based on pulmonary function, which is not the only predictor of disease severity or mortality, and that the model assumed the incidence of CF would remain stable, but due to the implementation of pre-natal screening for CF, incidence may decline over time.
Discussion
Summary of Available Evidence
The evidence for this review was derived from a systematic literature review of pivotal and phase III studies that was supplemented with additional studies to address important gaps in the RCT evidence. The systematic review included 4 double-blind, phase III, RCTs: 1 24-week, placebo-controlled trial conducted in patients with the F/MF genotype (Study 102; N = 405); 2 active-controlled trials in patients with the F/F genotypes (one 4-weeks in duration; Study 103; N = 107) and 1 24-weeks in duration (Study 109; N = 107); and 1 active-controlled trial in patients with either the F/RF or F/G genotype (Study 104; N = 259). The evidence from these studies was supplemented with 1 long-term extension phase study (Study 105),2 1 indirect comparison submitted by the sponsor,3 2 observational studies that evaluated the use of ELX-TEZ-IVA in patients with advanced lung disease,4,5 and 1 study that modelled the potential impact of ELX-TEZ-IVA on CF-related morbidity and mortality.6
Study 102 evaluated a range of outcomes that are important in the management of CF, including respiratory function (i.e., ppFEV1), nutritional status and growth (e.g., body weight and BMI), symptoms (CFQ-R [RD]), and clinical events (e.g., pulmonary exacerbations). The other studies included fewer outcomes and no other studies evaluated pulmonary exacerbations as efficacy end points. In general, the end points that were in the clinical trials largely align with those that are evaluated in routine Canadian clinical practice.
The inclusion and exclusion criteria for the included RCTs were similar except for the CFTR genotypes (i.e., F/MF, F/F, F/G, or F/RF). Studies 103, 104, and 109 all included a 28-day active treatment run-in period where all patients with either an F/F or F/RF genotype received TEZ-IVA (Studies 103, 109, and F/RF subset of patients in Study 104) and patients with an F/G genotype received IVA (F/G subset of patients in Study 104). Patients were subsequently randomized to receive ELX-TEZ-IVA or to remain on the active treatment administered during the run-in period.
Patients were also required to have stable CF disease in the opinion of the investigator and a ppFEV1 of 40% or greater and 90% or less at the time of screening for all the included studies. Patients with advanced lung disease (i.e., ppFEV1 < 40%) were an important subgroup for this review, as they may represent those who are in the greatest need of additional intervention. Limited data were available for these patients from ad hoc subgroup analysis in Study 102; however, CADTH conducted additional literature searching to identify other clinical studies conducted to evaluate the use of ELX-TEZ-IVA in patients with CF who have advanced lung disease.
All the studies excluded patients who were infected with some Burkholderia cepacia complex species (i.e., Burkholderia cenocepacia and Burkholderia dolosa). These patients represent 3.7% of overall the CF patient population in Canada1; however, the clinical experts consulted by CADTH noted that the exclusion of such patients does not substantially reduce the generalizability of the study results. This is similar to previous commentary from Cystic Fibrosis Foundation in US in their publication on the considerations for the use of another CFTR modulator (LUM-IVA), where they suggested that there is no basis to conclude that patients with CF with these infections would not benefit from treatment and that such patients may derive the greatest benefit from treatment due to their increased risk for accelerated disease progression and mortality.80
The CCFR reports that 7.8% of the Canadian CF population had received a lung transplant as of 2019 and that the estimated median time of survival for patients with CF who receive a lung transparent is 10.6 years post-transplant.1 Similar to the clinical development programs for the other approved CFTR modulators,64,67,68,72,73 patients who had received a lung transplant (or any organ or hematological transplant) were excluded from the ELX-TEZ-IVA clinical trials. Recommendations from the Institute for Clinical and Economic Review noted that, although excluded from the clinical trials, patients who have had a liver transplant should not be excluded from coverage as clinical expert input indicated that these patients would be likely to benefit from ELX-TEZ-IVA.81 The clinician groups who provided input noted there is a lack of evidence regarding whether or not ELX-TEZ-IVA would benefit patients with CF who have had a lung transplant. The experts consulted by CADTH noted that ELX-TEZ-IVA would not likely be initiated in patients who have undergone a lung transplant. For those who have undergone a liver transplant, ELX-TEZ-IVA could be initiated as the drug may benefit the patient’s lung function. Post-liver transplant patients would likely receive additional monitoring for potential toxicity with a lower threshold for interrupting or discontinuing the drug (due to the potential risk of hepatic AEs with ELX-TEZ-IVA). The sponsor noted in their commentary on the draft CADTH reports that safety and efficacy of ELX-TEZ-IVA was not evaluated in transplanted patients in the clinical trial program. However, the sponsor stated that ELX-TEZ-IVA has been shown to improve multiple clinical outcomes, including nutritional outcomes, and could potentially benefit post-lung or post-liver transplanted patients as CF is multisystemic in nature and continues to progress after organ transplant. The sponsor stated that some clinicians in the US, have been treating post-transplant patients with very strict monitoring protocols to limit possible drug-drug interactions and that outcomes suggest that ELX-TEZ-IVA could be used in these patients. However, the sponsor notes that the only available data at the time of CADTH’s review are case reports with small sample sizes.82-85
Interpretation of Results
Efficacy
Potential improvements in lung function can be evaluated based on short-term changes from baseline (e.g., absolute change from baseline in ppFEV1) or long-term changes evaluating the impact of an intervention on the CF disease course. The data included in this review of ELX-TEZ-IVA includes data for short-term changes, as evaluated in the pivotal and supportive clinical trials, and longer-term changes as assessed in the longer-term extension phase study and modelled in the sponsor’s microsimulation study. When considering lung function measurements in a chronic condition such as CF, the clinical experts consulted by CADTH indicated that the ability of CFTR modulator treatments such as ELX-TEZ-IVA to result in long-term changes is generally considered to be more clinically relevant than acute changes in ppFEV1. Similar statements have been made by regulatory authorities (Health Canada and EMA),86 and health technology assessment agencies (National Institute for Health and Care Excellence and the Australian Pharmaceutical Benefits Advisory Committee) in prior reviews of CFTR modulators.87,88
With respect to the data from the short-term studies (i.e., 4 weeks to 24 weeks), it is important to note the active treatment run-in period in 3 of the 4 RCTs makes it challenging to compare the results across the different genotypes. All patients included in Studies 103, 104, and 109 were receiving treatment with a CFTR modulator at baseline (IVA for those with an F/G genotype or TEZ-IVA for those with an F/F or F/RF genotype). In addition, a subset of patients in Study 104 were receiving treatment with a CFTR modulator at the time of screening. As such, the absolute improvements in ppFEV1 within the ELX-TEZ-IVA groups are likely lower than would be anticipated in patients who are naive to CFTR modulator therapy.
While no published information on the MID in absolute change in ppFEV1 in CF was identified by CADTH, the clinical experts consulted by CADTH noted that CF specialists would generally consider an absolute improvement in ppFEV1 of at least 5% to be clinically relevant. In patients with an F/MF genotype, ELX-TEZ-IVA was associated with a statistically significant and clinically meaningful absolute improvement in ppFEV1 compared with placebo (LSMD = 13.8%; 95% CI, 12.1 to 15.4). Similar results were reported for placebo-treated patients who were crossed over to ELX-TEZ-IVA in Study 105, which demonstrated an absolute increase from baseline in ppFEV1 of 14.9% (95% CI, 13.5 to 16.3) at 24 weeks. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The magnitude of the treatment effect reported for patients with F/MF and F/F genotypes is similar to the 10.6% to 12.5% improvement in ppFEV1 at 24 weeks that was observed with IVA monotherapy compared to placebo in the treatment of patients with CF with gating mutations (STRIVE, ENVISION, and KONNECTION)71-73 and exceeds the improvements in the pivotal trials for LUM-IVA (TRAFFIC [2.6%] and TRANSPORT [3.0%]),64 TEZ-IVA (EVOLVE [4.0%] and EXPAND [6.8%]),69,70 and IVA for patients with the R117H mutation (KONDUCT; 5.0% improvement).76 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| || |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Patients with a ppFEV1 less than 40% at screening were excluded from the RCTs; however, a small number of patients (range = 1.6% in Study 104 to 9.3% in Study 103) satisfied the screening requirements, but had a ppFEV1 that fell below 40% between the run-in period and study baseline.7-10 These patients with lower lung function would have satisfied the study inclusion criteria in the screening phase, then have demonstrated a ppFEV1 of less than 40% at their baseline evaluation. A post hoc subgroup analysis in Study 102 provided some efficacy data for this important subgroup of patients and suggested that ELX-TEZ-IVA improves lung function relative to placebo (mean absolute improvement in ppFEV1 of 18.4%; 95% CI, 11.5 to 25.3 at 24 weeks).7 This increase in ppFEV1 was considered to be clinically meaningful by the experts consulted by CADTH. The input received from clinician groups also noted that patients with a ppFEV1 less than 40% who have received ELX-TEZ-IVA in Canadian CF clinics (through SAP or compassionate access) have demonstrated clinically meaningful improvements to the treatment. Similar results were reported in the prospective cohort study conducted by Burgel et al. who evaluated the real-world efficacy and safety of ELX-TEZ-IVA in patients with CF with a ppFEV1 of less than 40%.5 This study included patients from all 47 CF centres in France who received open-label ELX-TEZ-IVA through an early access program (N = 245). Pooled data following 1 to 3 months of treatment demonstrated a clinically meaningful absolute improvement from baseline in ppFEV1 of 15.1% (95% CI, 13.8 to 16.4). The retrospective chart review by O’Shea et al. included 14 patients with advanced lung disease who received ELX-TEZ-IVA through a managed care program in Ireland.4 Patients were followed for a mean of 4.9 months (SD = 1.9) after starting ELX-TEZ-IVA. The authors reported that mean ppFEV1 improved from 27% (SD = 7.3) at baseline to 36% (SD = 16.5) after approximately 4 weeks of treatment (P < 0.0001).
Burgel et al. reported reductions in the proportion of patients receiving long-term oxygen (43% at baseline versus 23% at 3 months), non-invasive ventilation (28% at baseline versus 20% at 3 months), and enteral tube feeding (18% at baseline versus 10% at 3 months) which were statistically significant; however, the results were limited by a large amount of missing data (due to the onset of the COVID-19 pandemic during the study period). Burgel et al. also reported that, before initiation of ELX-TEZ-IVA, 16 patients were waiting for a lung transplant and 37 were under consideration for inclusion as transplant candidates within the next 3 months (n = 53 patients; 22%). At the end of the follow-up period, there was a reduction in the number of patients on the transplant list or being considered for transplant (5 patients). As only 2 patients had received a transplant (0.8%) and 1 patient had died while awaiting a transplant (0.4%); the reduction appears to be attributable to an improvement in the condition of these patients. The clinical experts consulted by CADTH, the clinician groups who provided input, and the patient group input received by CADTH also noted that ELX-TEZ-IVA has been shown to be beneficial for patients whose lung function has deteriorated to the extent where they have been referred to the lung transplant waiting list, noting that many improved to the point where they no longer required transplantation.
Patients with normal lung function (i.e., ppFEV1 > 90%) were also excluded from the included studies.7-10 As with those who have severe lung disease, these patients were excluded from the pivotal and supportive phase III trials as they were considered less likely to be able to show an improvement in lung function in a short-term clinical trial.49 The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients who have a ppFEV1 of greater than 90% often show early signs of CF lung disease (e.g., bronchiectasis, mucus plugging, or early mild declines in the FEV1) which could potentially benefit from treatment with ELX-TEZ-IVA. The potential for ELX-TEZ-IVA to reduce the frequency of pulmonary exacerbations was noted as an important potential benefit for those with normal lung function. At the time of CADTH’s review, clinical trials have not been conducted to investigate the benefit of ELX-TEZ-IVA in patients with normal lung function.
The ability of an intervention to result in long-term changes in lung function is a more accurate reflection of CF treatment goals and is considered to be a more clinically relevant end point than acute changes in ppFEV1.86-88 The included RCTs were too short to draw conclusions regarding whether or not treatment with ELX-TEZ-IVA would reduce the slope of decline in ppFEV1. Stanojevic et al.6 used a microsimulation model to estimate the impact of treatment with ELX-TEZ-IVA in eligible patients in Canada. The model forecasted an increase in median survival and a reduction in pulmonary exacerbations with the introduction of ELX-TEZ-IVA. The outcomes from these simulations are contingent on the validity of several assumptions that were required to build the model and extrapolate the impacts out to 10 years. There is uncertainty in the extrapolation of short-term effects of ELX-TEZ-IVA in a subset of patients with CF, to the broader population in the longer-term, and in the generalizability of observational data with IVA on the rate of decline in ppFEV1 to patients treated with ELX-TEZ-IVA. Moreover, the model likely overestimates the proportion of patients with CF who may receive ELX-TEZ-IVA and impact of treatment on pulmonary exacerbations.
Pulmonary exacerbations are currently the most common reason for hospitalization of patients with CF24 and, accordingly, these events were identified as an outcome of interest by the patient groups who provided input on this review. Pulmonary exacerbations are clinically significant events for patients with CF and are correlated with increased mortality, greater decline in lung function, reduced quality of life, and increased health costs.89-93 In addition, it has been estimated that many patients with CF experience a permanent reduction in lung function following an exacerbation (i.e., their lung function will not recover to the level it was before the exacerbation). In a large sample of patients with CF (N = 8,479), Sanders et al. estimated that 25% of patients with CF who experienced a pulmonary exacerbation failed to recover to their baseline FEV1.94 A similar observation has been made in an analysis in pediatric patients with CF, where 23% of patients failed to recover to their baseline FEV1 after being treated with IV antibiotics for a pulmonary exacerbation.95
Treatment with ELX-TEZ-IVA was associated with a statistically reduction in the risk of pulmonary exacerbations, including those requiring hospitalization and IV antibiotic therapy, in the 24-week placebo-controlled trial (Study 102). |||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.2,7 The clinical experts consulted by CADTH and regulatory reviewers (FDA and EMA) noted that the reduction in pulmonary exacerbations in Study 102 is clinically meaningful.29,48 In patients with advanced lung disease, the retrospective chart review by O’Shea et al. observed a reduced rate of pulmonary exacerbations requiring hospitalization (0.28 events per month in the 12 months before ELX-TEZ-IVA versus 0.04 events per month during the 4.9 month follow-up period based on data from 7 patients [P < 0.001]). This reduction would be considered clinically important based on the input from the clinical experts consulted by CADTH.
Pulmonary exacerbations were only reported as AEs in Studies 103, 104, and 109.8-10 In response to an inquiry from CADTH regarding why pulmonary exacerbations were not included as efficacy end points in these trials, the sponsor reported that the active-controlled trials would not have sufficient statistical power to detect a difference in pulmonary exacerbations between ELX-TEZ-IVA and the active comparators.54 As both TEZ-IVA and IVA have been shown to reduce the frequency of pulmonary exacerbations in previous placebo-controlled trials with patients who have F/F, F/RF, or F/G genotypes, the sponsor noted that a prohibitively large number of patients would be required to sufficiently power the studies to detect a reduction in pulmonary exacerbations.54 While it is acknowledged that a study designed to evaluate the effects of a treatment on exacerbations would likely require a sizable patient population and at least a 12-month duration, especially if an active treatment comparator was used, it is not clear that such a study with these features is not feasible. In all 3 of the active-controlled studies, the proportions of patients who experienced at least 1 pulmonary exacerbation during the double-blind treatment phases were numerically lower in the ELX-TEZ-IVA group compared with the comparator groups, though no statistical analyses were performed and there were no standard definitions for pulmonary exacerbations that were recorded as AEs.8-10
There are no globally accepted definitions for pulmonary exacerbations in patients with CF. The definitions used in Study 102 were considered to be appropriate by regulatory authorities and the clinical experts consulted by CADTH.29,48 The clinical experts consulted by CADTH noted there would be some variation in routine clinical practice in the threshold for diagnosing and treating pulmonary exacerbations across different CF clinics and/or physicians. This was also evident in Study 102 where there were fewer patients that met the criteria for a pulmonary exacerbation when evaluated as an efficacy end point compared to the number of exacerbations reported as AEs (e.g., 37% versus 47% in the placebo group).7 Although there are no standard definitions currently used in Canadian clinical practice, the clinical experts consulted by CADTH noted that the number of exacerbation events experienced by patients with CF is currently tracked in CF clinics.
Given that CFTR modulators are systemic treatments, the pivotal studies for ELX-TEZ-IVA included end points such as BMI and body weight to evaluate the effect of treatment on the nutritional status of patients with CF. Treatment with ELX-TEZ-IVA was associated with statistically significant improvements in BMI compared with placebo at 24 weeks in those with F/MF genotype and compared with TEZ-IVA at 4 weeks in those with an F/F genotype (LSMD = 1.04 kg/m2; 95% CI, 0.85 to 1.23 and 0.60 kg/m2; 95% CI, 0.41 to 0.79, respectively). The clinical experts consulted by CADTH noted that the improvements in BMI with ELX-TEZ-IVA are clinically meaningful. Similarly, reviewers for the EMA noted that the improvements observed after 24 weeks in Study 102 of treatment with ELX-TEZ-IVA are clinically relevant.48 Reviewers for FDA considered the improvements in BMI that were reported in Study 103 to be clinically relevant; however, the EMA considered the 4-week duration the study to be too short to evaluate the potential benefits of CFTR modulator treatment on an end point such as BMI.48 As such, the extension phase data from Study 105 were considered by the EMA and noted that they are supportive of the clinical benefit for patients with an F/F genotype.48 The 24-week interim analysis from Study 105 suggested that patients with an F/F genotype who received ELX-TEZ-IVA for a minimum of 24-weeks experienced similar within-group improvements from baseline compared with those in Study 102.2 In 14 patients with advanced lung disease, the retrospective chart review by O’Shea et al. reported that the mean BMI increased from 20.7 kg/m2 (SD = 3.6) to 22.1 kg/m2 (SD = 3.4) after approximately 2 months of treatment with ELX-TEZ-IVA.
As stated in the patient group input, CF has a major impact on the quality of life of patients and their caregivers. Treatment with ELX-TEZ-IVA demonstrated statistically significant and clinically meaningful improvements in health-related quality of life (i.e., CFQ-R) in each of the included studies. The magnitude of improvement in the CFQ-R (RD) scores with ELX-TEZ-IVA was 20.2 (95% CI, 17.5 to 23.0) at 24 weeks compared with placebo for patients with an F/MF genotype. In the trials where patients switched to ELX-TEZ-IVA, the improvements in the CFQ-R (RD) scores were 15.9 (95% CI, 11.7 to 20.1) at 24 weeks compared with remaining on TEZ-IVA in patients with an F/F genotype, 8.9 (95% CI, 3.8 to 14.0) at 8 weeks compared with remaining on IVA in patients with an F/G genotype, and 8.5 (95% CI, 4.0 to 13.1) at 8 weeks compared with remaining on TEZ-IVA in patients with an F/RF genotype. The MID for the CFQ-R (RD) is typically cited to be 4.0 points, a threshold which was exceeded in all the included trials. The clinical experts consulted by CADTH and reviewers for the FDA and EMA considered the results to be clinically relevant.29,48
The CADTH review did not identify any RCTs that specifically addressed the use of ELX-TEZ-IVA in patients with prior failure or intolerance to another CFTR modulator. The clinical experts consulted by CADTH noted that prior failure or intolerance to a CFTR modulator should not preclude a patient from receiving a trial with ELX-TEZ-IVA.
The patient input received by CADTH emphasized that the therapeutic regimen for patients with CF requires considerable time each day and is very demanding both physically and mentally for those living with CF and their caregivers. Patients have expressed interest in therapeutic options that could help alleviate their existing treatment burden. ELX-TEZ-IVA was shown to reduce the need for IV antibiotics in Study 102; however, all the included studies investigated the use of ELX-TEZ-IVA added on to the ongoing therapies being used by eligible patients. Concomitant therapies were to remain stable throughout the trial to avoid confounding the study results (except for antibiotics for the treatment of pulmonary of exacerbations). A large RCT is currently being planned to investigate the discontinuation of some concomitant CF therapies (hypertonic saline and dornase alfa) after stabilization with ELX-TEZ-IVA (SIMPLIFY; N = 800 [planned]).96,97 The clinical experts consulted by CADTH and the clinician groups who provided input all noted that ELX/TEX/IVA should be used as an add-on therapy.
Harms
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., at least 12 years of age with at least 1 F508del mutation). SAEs and WDAEs were rare in the included studies. The clinical experts consulted by CADTH noted that patients who experience significant AEs following initial treatment with ELX-TEZ-IVA would not likely be completely discontinued from treatment; rather, treatment with ELX-TEZ-IVA would likely be interrupted and the patient would be re-challenged with the drug following resolution of the event(s). This is consistent with the input received from the 3 clinician groups who noted that discontinuation of therapy should be considered in patients who have clinically significant adverse effects that persist and recur after stopping and re-initiating therapy.
Similar to the development programs for the other CFTR modulators (IVA, LUM-IVA, and TEZ-IVA), patients with abnormal liver function were excluded from the phase III ELX-TEZ-IVA trials. The clinical experts consulted by CADTH noted that most patients who could be eligible for ELX-TEZ-IVA would not have hepatic impairment. The product monograph recommends that the dosage of ELX-TEZ-IVA should be adjusted in patients with moderate hepatic impairment and that the drug should not be used in patients with severe hepatic impairment.30 These recommendations are more restrictive than those in the product monographs for IVA, LUM-IVA, or TEZ-IVA,13,30,38 all of which provide dosage reduction scenarios for patients with CF who have severe hepatic impairment. The clinical experts consulted by CADTH suggested that clinicians may attempt to treat those with severe hepatic impairment using ELX-TEZ-IVA at a reduced dosage, as opposed to using the reduced dosages of the alternative CFTR modulators, which are unlikely to provide the same level of clinical benefit.
The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends that ALT and AST be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter.30 The clinical experts consulted by CADTH noted that the recommendations for monitoring would likely be followed by the clinical community. The clinical experts consulted by CADTH and the clinician groups who provided input noted that patients with CF are typically seen once every 3 months (though this has been less frequent in some cases due to the COVID-19 pandemic). As such, the recommended monitoring regimen for ELX-TEZ-IVA was not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF (particularly after the first year of initiating the treatment).
Similar to IVA, LUM-IVA, and TEZ-IVA, the product monograph for ELX-TEZ-IVA notes that cases of non-congenital cataracts without impact on vision have been reported in pediatric patients who were treated with IVA-containing regimens.12,13,30,38 The product monograph states that the patients who demonstrated these events had other risk factors (e.g., corticosteroid use or exposure to radiation); however, a possible risk attributable to treatment with IVA cannot be excluded. As such, it is recommended that pediatric patients initiating treatment with ELX-TEZ-IVA received baseline and follow-up ophthalmological examinations.30 The clinical experts consulted by CADTH noted that children with CF currently have an ophthalmological examination before starting treatment with a CFTR modulator and are monitored on an ongoing basis thereafter.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The clinical trials included in this review demonstrated that ELX-TEZ-IVA does not appear to be associated with the respiratory AEs (e.g., dyspnea and abnormal respiration) that were reported in the pivotal trials with LUM-IVA.35,36,38,62,98
Other Considerations
The initial approval for ELX-TEZ-IVA by the EMA was for a more restrictive patient population (i.e., patients with CF aged ≥ 12 years who are homozygous for the F508del or heterozygous for F508del with an MF mutation) which reflected the clinical evidence that was submitted at that time (i.e., Studies 102, 103, and 105).48 The sponsor subsequently filed additional data (Study 104) seeking to have the indication expanded to patients with CF who have at least 1 F508del mutation (i.e., the indication currently under review by Health Canada and CADTH).11 The Committee for Medicinal Products for Human Use adopted a positive opinion recommending the indication for ELX-TEZ-IVA be expanded to patients with CF who have at least 1 F508del mutation.99
The sponsor is currently conducting phase III trials investigating the safety and efficacy of ELX-TEZ-IVA in patients aged 6 to 11 years of age100,101 and the safety, tolerability, and pharmacokinetics of ELX-TEZ-IVA in patients aged 2 to 5 years of age. This is similar to the clinical development programs for LUM-IVA and TEZ-IVA. In Canada, the initial Health Canada approval of LUM-IVA was granted in 2016 for patients aged 12 years and older and subsequently expanded to patients aged 6 to 11 in 2017 and then to patients aged 2 to 5 in 2018.102 The FDA recently extended the approval of ELX-TEZ-IVA to include an 177 additional mutations in the CFTR gene that have shown to be responsive to ELX-TEZ-IVA based on data from in vitro assays.31,103
Conclusions
A 24-week, placebo-controlled, RCT (Study 102; N = 403) conducted in patients with an F/MF genotype demonstrated that, compared with placebo, 24-weeks of treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in lung function (increase in ppFEV1), nutritional status (increase in BMI), health-related quality of life (increase in CFQ-R [RD] scores), CF biomarkers (reduction in sweat chloride), and a reduced rate of pulmonary exacerbations, including events that required IV antibiotics and/or hospitalization to manage. Three additional double-blind, active-controlled RCTs investigated switching to ELX-TEZ-IVA after 4 weeks of treatment with either TEZ-IVA or IVA compared with remaining on those other CFTR modulators. Study 103 (N = 107; 4 weeks) and Study 109 (N = 175; 24 weeks) were conducted in patients with an F/F genotype and demonstrated that treatment with ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 and CFQ-R compared with remaining on TEZ-IVA. Study 104 (N = 258; 8 weeks) demonstrated that switching to ELX-TEZ-IVA was associated with statistically significant and clinically meaningful improvements in ppFEV1 compared with remaining on IVA in patients with an F/G genotype treatment and a modest improvement compared with remaining on TEZ-IVA for patients with an F/RF genotype. Patients with advanced lung disease were largely excluded from the phase III RCTs; however, post hoc subgroup analyses and data from 2 short-term observational studies suggests that treatment with ELX-TEZ-IVA resulted in clinically meaningful improvements in lung function in these patients.
ELX-TEZ-IVA was well tolerated in the target patient populations (i.e., at least 12 years of age with at least 1 F508del mutation). SAEs and WDAEs were rare in the included studies. The product monograph notes that elevated transaminases have been observed in patients treated with ELX-TEZ-IVA and recommends that ALT and AST be assessed before initiating treatment with ELX-TEZ-IVA, every 3 months during the first year of treatment, and annually thereafter. The clinical experts consulted by CADTH noted that the recommendations for monitoring with ELX-TEZ-IVA were not anticipated to result in a substantial increase in the number of the clinic visits for patients with CF (particularly after the first year of initiating the treatment).
References
1.The Canadian Cystic Fibrosis registry: 2019 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/registry/2019AnnualDataReport.pdf. Accessed 2020 Dec 17.
2.Clinical Study Report: study 105. A phase 3, open-label study evaluating the long-term safety and efficacy of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous or heterozygous for the F508del mutation) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Mar 20.
3.Drug Reimbursement Review sponsor submission: Trikafta, oral 100 mg/50 mg/75 mg and 150 mg [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jan 22.
4.O'Shea KM, O'Carroll OM, Carroll C, et al. The efficacy of elexacaftor/tezacaftor/ivacaftor in patients with cystic fibrosis and advanced lung disease. Eur Respir J. 2020;05:05.
5.Burgel PR, Durieu I, Chiron R, et al. Rapid improvement after starting elexacaftor-tezacaftor-ivacaftor in patients with cystic fibrosis and advanced pulmonary disease. Am J Respir Crit Care Med. 2021;18:18. PubMed
6.Stanojevic S, Vukovojac K, Sykes J, Ratjen F, Tullis E, Stephenson AL. Projecting the impact of delayed access to elexacaftor/tezacaftor/ivacaftor for people with cystic fibrosis. J Cyst Fibros. 2020;05:05.
7.Clinical Study Report: study 102. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jul 2.
8.Clinical Study Report: study 103. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous for the F508del mutation (F/F) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jun 18.
9.Clinical Study Report: study 104. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a gating or residual function mutation (F/G and F/RF genotypes) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Aug 28.
10.Clinical Study Report: study 109. A phase 3b, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Oct 16.
11.Vertex response to March 10, 2021 request for additional information regarding Trikafta CADTH review [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Mar 22.
12.Symdeko®, tezacaftor/ivacaftor tablets and ivacaftor tablets, tezacaftor 100 mg/ivacaftor 150 mg tablets and ivacaftor 150 mg tablets, oral [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Aug 21: https://pdf.hres.ca/dpd_pm/00058025.PDF. Accessed 2020 Dec 17.
13.Kalydeco®: ivacaftor tablets 150 mg, ivacaftor granules 50 mg per packet, 75 mg per packet [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2019 Jan 25: https://pdf.hres.ca/dpd_pm/00049400.PDF. Accessed 2020 Dec 15.
14.Rowe SM, Miller S, Sorscher EJ. Cystic fibrosis. N Engl J Med. 2005;352(19):1992-2001. PubMed
15.Veit G, Avramescu RG, Chiang AN, et al. From CFTR biology toward combinatorial pharmacotherapy: expanded classification of cystic fibrosis mutations. Mol Biol Cell. 2016;27(3):424-433. PubMed
16.Lukacs GL, Verkman AS. CFTR: folding, misfolding and correcting the DeltaF508 conformational defect. Trends Mol Med. 2012;18(2):81-91. PubMed
17.Okiyoneda T, Barriere H, Bagdany M, et al. Peripheral protein quality control removes unfolded CFTR from the plasma membrane. Science. 2010;329(5993):805-810. PubMed
18.Flume PA, O'Sullivan BP, Robinson KA, et al. Cystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2007;176(10):957-969. PubMed
19.Cogen J, Emerson J, Sanders DB, et al. Risk factors for lung function decline in a large cohort of young cystic fibrosis patients. Pediatr Pulmonol. 2015;50(8):763-770. PubMed
20.Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002;34(2):91-100. PubMed
21.Cystic Fibrosis Foundation patient registry 2019 annual data report. Bethesda (MD): Cystic Fibrosis Foundation; 2020: https://www.cff.org/Research/Researcher-Resources/Patient-Registry/2019-Patient-Registry-Annual-Data-Report/. Accessed 2020 Dec 17.
22.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
23.Corey M, McLaughlin FJ, Williams M, Levison H. A comparison of survival, growth, and pulmonary function in patients with cystic fibrosis in Boston and Toronto. J Clin Epidemiol. 1988;41(6):583-591. PubMed
24.The Canadian Cystic Fibrosis registry: 2013 annual report. Toronto (ON): Cystic Fibrosis Canada; 2015: https://www.cysticfibrosis.ca/uploads/cf%20care/Canadian-CF-Registry-2013-FINAL.pdf. Accessed 2020 Dec 17.
25.The Canadian Cystic Fibrosis registry: 2016 annual data report. Toronto (ON): Cystic Fibrosis Canada; 2017: https://www.cysticfibrosis.ca/uploads/2016%20Registry%20Annual%20Data%20Report.pdf. Accessed 2020 Dec 17.
26.Mogayzel PJ, Jr., Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680-689. PubMed
27.Canadian consensus statement on aerosolized antibiotic use in cystic fibrosis. Toronto (ON): Cystic Fibrosis Canada; 2020: https://www.cysticfibrosis.ca/uploads/About%20Us/CFC005%20AEROSOLIZED%20ANTIBIOTIC%20_englishFinal.pdf. Accessed 2020 Dec 17.
28.Flume PA, Mogayzel PJ, Jr., Robinson KA, et al. Cystic fibrosis pulmonary guidelines: treatment of pulmonary exacerbations. Am J Respir Crit Care Med. 2009;180(9):802-808. PubMed
29.Center for Drug Evaluation and Research. Multi-Disciplinary Review. Trikafta (elexacaftor, tezacaftor and ivacaftor tablets; ivacaftor tablets). Company: Vertex Pharmaceuticals Incorporated. Application No.: 212273. Approval date: 10/21/2019 (FDA approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2019: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/212273Orig1s000MultidisciplineR.pdf. Accessed 2020 Dec 17.
30.Trikafta®: elexacaftor tezacaftor/ivacaftor tablets and ivacaftor tablets, oral 100 mg/50 mg/75 mg and 150 mg [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Nov 11.
31.Center for Drug Evaluation and Research. Label. Trikafta (elexacaftor, tezacaftor and ivacaftor tablets; ivacaftor tablets). Company: Vertex Pharmaceuticals Incorporated. Application No.: 212273. Approval date: 10/21/2019 (FDA approval package). Rockville (MD): U.S. Food and Drug Administration (FDA); 2020: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212273s000lbl.pdf. Accessed 2020 Dec 17.
32.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2013 Mar 22: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_Kalydeco_March-25-13_e.pdf. Accessed 2020 Dec 17.
33.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2014 Dec 19: https://www.cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0379_Kalydeco_Dec-23-14.pdf. Accessed 2020 Dec 17.
34.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor (Kalydeco - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2015 Nov 19: https://www.cadth.ca/sites/default/files/cdr/complete/SR0430_complete_Kalydeco_R117H_Nov-23-15_e.pdf. Accessed 2020 Dec 17.
35.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2016 Oct 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0471_complete_Orkambi-Oct-28-16.pdf. Accessed 2020 Dec 17.
36.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2018 Sep 26: https://www.cadth.ca/sites/default/files/cdr/complete/SR0559%20Orkambi%20-%20CDEC%20Final%20Recommendation%20October%204%2C%202018.pdf. Accessed 2020 Dec 17.
37.CADTH reimbursement review status: tezacaftor/ivacaftor. 2019; https://www.cadth.ca/tezacaftorivacaftor. Accessed 2020 Dec 17.
38.Orkambi®, lumacaftor/ivacaftor tablets 100 mg/125 mg and 200 mg/125 mg, lumacaftor/ivacaftor granules 100 mg/125 mg and 150 mg/188 mg [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2018 Dec 11: https://pdf.hres.ca/dpd_pm/00048664.PDF. Accessed 2020 Dec 17.
39.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
40.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters.
41.Middleton PG, Mall MA, Dřevínek P, et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single Phe508del allele. N Engl J Med. 2019;381(19):1809-1819. PubMed
42.Vertex Pharmaceuticals Incorporated. NCT03525444: A phase 3 study of VX-445 combination therapy in subjects with cystic fibrosis heterozygous for the F508del mutation and a minimal function mutation (F/MF). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03525444. Accessed 2020 Dec 20.
43.Heijerman HGM, McKone EF, Downey DG, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet. 2019;394(10212):1940-1948. PubMed
44.Department of error. Lancet. 2020;395(10238):1694.
45.Vertex Pharmaceuticals Incorporated. NCT03525548: A study of VX-445 combination therapy in CF subjects homozygous for F508del (F/F). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT03525548. Accessed 2020 Dec 20.
46.Vertex Pharmaceuticals Incorporated. NCT04058353: A phase 3 study of VX-445 combination therapy in cystic fibrosis (CF) subjects heterozygous for F508del and a gating or residual function mutation (F/G and F/RF genotypes). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04058353. Accessed 2020 Dec 19.
47.Vertex Pharmaceuticals Incorporated. NCT04105972: A study evaluating the efficacy and safety of VX-445/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04105972. Accessed 2020 Dec 20.
48.Committee for Medicinal Products for Human Use. Assessment report: Kaftrio (ivacaftor/tezacaftor/elexacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2020: https://www.ema.europa.eu/en/documents/assessment-report/kaftrio-epar-public-assessment-report_en.pdf. Accessed 2020 Dec 17.
49.Common technical document 2.7.3 summary of clinical efficacy [internal sponsor's package]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2021 Jan 22.
50.Clinical value of triple combination therapy (elexacaftor/tezacaftor/ivacaftor & ivacaftor) for the treatment of cystic fibrosis in patients 12 years of age and older who have at least 1 F508 deletion mutation in the CFTR gene [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals (Canada); 2021 Jan.
51.Vertex Pharmaceuticals Incorporated. NCT04362761: A study evaluating the long-term safety of elexacaftor combination therapy. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04362761. Accessed 2021 Mar 25.
52.Vertex Pharmaceuticals Incorporated. NCT04058366: Study evaluating the long-term safety and efficacy of VX-445 combination therapy. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/ct2/show/NCT04058366. Accessed 2021 March 25.
53.US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). 2011; http://cftr2.org. Accessed 2021 Mar 2.
54.Vertex response to March 15, 2021 request for additional information regarding Trikafta CADTH review [internal additional sponsor's information]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Mar 23.
55.Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range = the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324-1343. PubMed
56.Quittner AL, Sawicki GS, McMullen A, et al. Erratum to: psychometric evaluation of the Cystic Fibrosis Questionnaire-Revised in a national, US sample. Qual Life Res. 2012;21(7):1279-1290. PubMed
57.Tluczek A, Becker T, Grieve A, et al. Health-related quality of life in children and adolescents with cystic fibrosis: convergent validity with parent-reports and objective measures of pulmonary health. J Dev Behav Pediatr. 2013;34(4):252-261. PubMed
58.Henry B, Aussage P, Grosskopf C, Goehrs JM. Development of the Cystic Fibrosis Questionnaire (CFQ) for assessing quality of life in pediatric and adult patients. Qual Life Res. 2003;12(1):63-76. PubMed
59.Quittner AL, Modi AC, Wainwright C, Otto K, Kirihara J, Montgomery AB. Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. Chest. 2009;135(6):1610-1618. PubMed
60.Regnault A, Balp MM, Kulich K, Viala-Danten M. Validation of the treatment satisfaction questionnaire for medication in patients with cystic fibrosis. J Cyst Fibros. 2012;11(6):494-501. PubMed
61.Summary of product characteristics: Kaftrio 75 mg/50 mg/100 mg film-coated tablets. Amsterdam (NL): European Medicines Agency; 2020: https://www.ema.europa.eu/documents/product-information/kaftrio-epar-product-information_en.pdf. Accessed 2020 Dec 17.
62.CADTH Common Drug Review Clinical Review Report: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2018 Oct: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0559_Orkambi_CL_Report.pdf. Accessed 2020 Dec 17.
63.Committee for Medicinal Products for Human Use. Guideline on the clinical development of medicinal products for the treatment of cystic fibrosis. Amsterdam (NL): European Medicines Agency; 2009: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-medicinal-products-treatment-cystic-fibrosis-first-version_en.pdf. Accessed 2020 Dec 19.
64.Wainwright CE, Elborn JS, Ramsey BW, et al. Lumacaftor–ivacaftor in patients with cystic fibrosis homozygous for Phe508del CFTR. N Engl J Med. 2015;373(3):220-231. PubMed
65.Vertex Pharmaceuticals Incorporated. NCT01807923: A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 years and older who are homozygous for the F508del-CFTR mutation (TRAFFIC). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2015: https://clinicaltrials.gov/ct2/show/NCT01807923. Accessed 2020 Dec 19.
66.Vertex Pharmaceuticals Incorporated. NCT01807949: A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 years and older who are homozygous for the F508del-CFTR mutation (TRANSPORT). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2016: https://clinicaltrials.gov/ct2/show/NCT01807949. Accessed 2020 Dec 19.
67.Vertex Pharmaceuticals Incorporated. NCT02392234: A phase 3 study to evaluate the efficacy and safety of ivacaftor and VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-cystic fibrosis transmembrane conductance regulator (CFTR) mutation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2018: https://clinicaltrials.gov/ct2/show/NCT02392234. Accessed 2020 Dec 19.
68.Vertex Pharmaceuticals Incorporated. NCT02412111: A phase 3 study of tezacaftor (VX-661) in combination with ivacaftor (VX-770) in subjects aged 12 years and older with cystic fibrosis (CF), who have one F508del-CFTR mutation and a second mutation that has been demonstrated to be clinically responsive to ivacaftor. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: https://clinicaltrials.gov/ct2/show/NCT02412111. Accessed 2020 Dec 19.
69.Taylor-Cousar JL, Munck A, McKone EF, et al. Tezacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del. N Engl J Med. 2017;377(21):2013-2023. PubMed
70.Rowe SM, Daines C, Ringshausen FC, et al. Tezacaftor-ivacaftor in residual-function heterozygotes with cystic fibrosis. N Engl J Med. 2017;377(21):2024-2035. PubMed
71.Vertex Pharmaceuticals Incorporated. NCT01614470: Study of ivacaftor in subjects with cystic fibrosis (CF) who have a non-G551D CF transmembrane conductance regulator (CFTR) gating mutation (KONNECTION). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2014: https://clinicaltrials.gov/ct2/show/NCT01614470. Accessed 2020 Dec 20.
72.Ramsey BW, Davies J, McElvaney NG, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med. 2011;365(18):1663-1672. PubMed
73.Davies JC, Wainwright CE, Canny GJ, et al. Efficacy and safety of ivacaftor in patients aged 6 to 11 years with cystic fibrosis with a G551D mutation. Am J Respir Crit Care Med. 2013;187(11):1219-1225. PubMed
74.Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26(1):153-161. PubMed
75.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-338. PubMed
76.Moss RB, Flume PA, Elborn JS, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis who have an Arg117His-CFTR mutation: a double-blind, randomised controlled trial. Lancet Respir Med. 2015;3(7):524-533. PubMed
77.De Boeck K, Munck A, Walker S, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis and a non-G551D gating mutation. J Cyst Fibros. 2014;13(6):674-680. PubMed
78.Griese M, Costa S, Linnemann RW, et al. Safety and efficacy of elexacaftor/tezacaftor/ivacaftor for 24 weeks or longer in people with cystic fibrosis and one or more F508del alleles: interim results of an open-label phase 3 clinical trial. Am J Respir Crit Care Med. 2021;203(3):381-385. PubMed
79.Volkova N, Moy K, Evans J, et al. Disease progression in patients with cystic fibrosis treated with ivacaftor: data from national US and UK registries. J Cyst Fibros. 2020;19(1):68-79. PubMed
80.Considerations for the use of lumacaftor and ivacaftor fixed dose combination oral tablets (Orkambi™) for the management of persons with cystic fibrosis and two F508del CFTR mutations. Bethesda (MD): Cystic Fibrosis Foundation; 2015: https://www.cff.org/PDF-Archive/Orkambi-Whitepaper/. Accessed 2021 Mar 16.
81.Modulator treatments for cystic fibrosis: final policy recommendations. Boston (MA): Institute for Clinical and Economic Review; 2020: http://icerorg.wpengine.com/wp-content/uploads/2020/08/ICER_CF_Policy_Recs_092320.pdf. Accessed 2020 Dec 20.
82.Jakharia K, Doligalski C, Lobo L, Coakley R. Impact of Trikafta on lung function in a cystic fibrosis transplant patient. Chest. 2020;158(4):A2378.
83.Ragan HH, Autry E, Bomersback T. The use of elexacaftor/tezacaftor/ivacaftor in patients with cystic fibrosis post-liver transplantation [abstract 788]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
84.Turowski J, Lehr C, Valapour M, Dasenbrook E. Impact of elexacaftor/tezacaftor/ivacaftor on tacrolimus trough levels in individuals at least 3 years post-lung transplant [abstract 787]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
85.Fitzgerald L, Jia S. Initiating elexacaftor/tezacaftor/ivacaftor in post-lung transplant CF patients [abstract 792]. Paper presented at: 34th Annual North American Cystic Fibrosis Conference. 2020 Oct 7-23; Virtual experience.
86.Committee for Medicinal Products for Human Use. Assessment report: Orkambi (ivacaftor/lumacaftor). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2016: https://www.ema.europa.eu/en/documents/assessment-report/orkambi-epar-public-assessment-report_en.pdf. Accessed 2020 Dec 17.
87.National Institute for Health and Care Excellence. Lumacaftor–ivacaftor for treating cystic fibrosis homozygous for the F508del mutation. (Technology appraisal guidance TA398) 2016; https://www.nice.org.uk/guidance/ta398/resources/lumacaftorivacaftor-for-treating-cystic-fibrosis-homozygous-for-the-f508del-mutation-pdf82602916891333. Accessed 2021 Mar 16.
88.Public summary document: lumacaftor and ivacaftor: tablet containing lumacaftor 200 mg with ivacaftor 125 mg Orkambi®. Canberra (AU): Pharmaceutical Benefit Advisory Committee; 2017: https://www.pbs.gov.au/industry/listing/elements/pbac-meetings/psd/2017-07/files/lumacaftor-ivacaftor-psd-july-2017.pdf. Accessed 2021 Apr 9.
89.Bhatt JM. Treatment of pulmonary exacerbations in cystic fibrosis. Eur. 2013;22(129):205-216. PubMed
90.de Boer K, Vandemheen KL, Tullis E, et al. Exacerbation frequency and clinical outcomes in adult patients with cystic fibrosis. Thorax. 2011;66(8):680-685. PubMed
91.Solem CT, Vera-Llonch M, Liu S, Botteman M, Castiglione B. Impact of pulmonary exacerbations and lung function on generic health-related quality of life in patients with cystic fibrosis. Health Qual Life Outcomes. 2016;14:63. PubMed
92.Waters V, Atenafu EG, Salazar JG, et al. Chronic Stenotrophomonas maltophilia infection and exacerbation outcomes in cystic fibrosis. J Cyst Fibros. 2012;11(1):8-13. PubMed
93.Waters V, Stanojevic S, Atenafu EG, et al. Effect of pulmonary exacerbations on long-term lung function decline in cystic fibrosis. Eur Respir J. 2012;40(1):61-66. PubMed
94.Sanders DB, Bittner RC, Rosenfeld M, Hoffman LR, Redding GJ, Goss CH. Failure to recover to baseline pulmonary function after cystic fibrosis pulmonary exacerbation. Am J Respir Crit Care Med. 2010;182(5):627-632. PubMed
95.Sanders DB, Hoffman LR, Emerson J, et al. Return of FEV1 after pulmonary exacerbation in children with cystic fibrosis. Pediatr Pulmonol. 2010;45(2):127-134. PubMed
96.Mayer-Hamblett N, Nichols DP, Odem-Davis K, et al. Evaluating the impact of stopping chronic therapies after modulator drug therapy in cystic fibrosis: the SIMPLIFY study design. Ann Am Thorac Soc. 2021. PubMed
97.Nichols D. NCT04378153: Impact of discontinuing chronic therapies in people with cystic fibrosis on highly effective CFTR modulator therapy (SIMPLIFY). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04378153. Accessed 2021 Feb 23.
98.CADTH Common Drug Review Clinical Review Report: lumacaftor/ivacaftor (Orkambi - Vertex Pharmaceuticals [Canada] Incorporated). Ottawa (ON): CADTH; 2016 Jan 26: https://www.cadth.ca/sites/default/files/cdr/clinical/SR0471_Orkambi_CL_Report.pdf. Accessed 2020 Dec 17.
99.Committee for Medicinal Products for Human Use. Summary of opinion (post authorisation): Kaftrio (ivacaftor / tezacaftor / elexacaftor). Amsterdam (NL): European Medicines Agency; 2021: https://www.ema.europa.eu/en/documents/smop/chmp-post-authorisation-summary-positive-opinion-kaftrio-ii-01_en.pdf. Accessed 2021 Mar 30.
100.Vertex Pharmaceuticals Incorporated. NCT04545515: A study evaluating the long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis (CF) subjects 6 years and older and F/MF genotypes. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04545515. Accessed 2020 Dec 17.
101.Vertex Pharmaceuticals Incorporated. NCT04353817: A study evaluating efficacy and safety of elexacaftor/tezacaftor/ivacaftor in subjects 6 through 11 years of age with cystic fibrosis and F/MF genotypes. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/NCT04353817. Accessed 2020 Dec 17.
102.Health Canada. Notice of Compliance (NOC) for Orkambi. 2020; https://health-products.canada.ca/noc-ac/index-eng.jsp. Accessed December 17, 2020.
103.Vertex Pharmaceuticals Incorporated. Vertex announces FDA approvals of TRIKAFTA® (elexacaftor/tezacaftor/ivacaftor and ivacaftor), SYMDEKO® (tezacaftor/ivacaftor and ivacaftor) and KALYDECO® (ivacaftor) for use in people with CF with certain rare mutations. 2020; https://news.vrtx.com/press-release/vertex-announces-fda-approvals-trikaftar-elexacaftortezacaftorivacaftor-and-ivacaftor. Accessed 2020 Dec 19.
104.Davies JC, Moskowitz SM, Brown C, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1599-1611. PubMed
105.Keating D, Marigowda G, Burr L, et al. VX-445-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1612-1620. PubMed
106.Bhatia R, Kaye M, Roberti-Miller A. Longitudinal assessment of exercise capacity and quality of life outcome measures in cystic fibrosis: a year-long prospective pilot study. J Eval Clin Pract. 2020;26(1):236-241. PubMed
107.Issues in the design of clinical trials of aerosolized antimicrobials for the treatment of cystic fibrosis. Day 2: efficacy endpoints for clinical trials of aerolised antimicrobials. Silver Spring (MD): U.S. Food and Drug Administration; 2010: https://www.fda.gov/downloads/Drugs/NewsEvents/UCM231055.pdf. Accessed 2021 Mar 24.
108.Report of the workshop on endpoints for cystic fibrosis clinical trials. Amsterdam (NL): European Medicines Agency; 2012: https://www.ema.europa.eu/docs/en_GB/document_library/Report/2012/12/WC500136159.pdf. Accessed 2021 Mar 24.
109.Quittner AL, Buu A, Messer MA, Modi AC, Watrous M. Development and validation of The Cystic Fibrosis Questionnaire in the United States: a health-related quality-of-life measure for cystic fibrosis. Chest. 2005;128(4):2347-2354. PubMed
110.Modi AC, Lim CS, Driscoll KA, Piazza-Waggoner C, Quittner AL, Wooldridge J. Changes in pediatric health-related quality of life in cystic fibrosis after IV antibiotic treatment for pulmonary exacerbations. J Clin Psychol Med Settings. 2010;17(1):49-55. PubMed
Appendix 1: Summary of CF Canada Guidelines
Note that this appendix has not been copy-edited.
Indications for Starting CFTR Modulator Therapy
All Canadians with a confirmed diagnosis of CF should have access to Health Canada-approved CFTR modulators based on their variants in CFTR.
The diagnosis of CF requires:
Clinical symptoms/features or a positive newborn screen and either
Two disease-causing CFTR variants; Or
Sweat chloride concentration >60 mmol/L (On 2 occasions if only one CFTR variant known).
To be eligible for CFTR modulator therapy, the following will apply:
Mutation: F508del/Any CFTR variant or Gating variant/Any CFTR variant or R117H/Any CFTR variant
These genotype recommendations are based on phase III clinical trials showing substantial clinical improvement with CFTR modulators and Health Canada approval.
Age: as approved by Health Canada
CFTR modulators should be initiated at the YOUNGEST age possible with the goal of attenuating disease progression and improving clinical status. Data suggest that early introduction can reverse disease progression, such as restoring pancreatic function. There is NO data to support withholding CFTR modulators until significant clinical symptoms have developed or a drop in lung function occurs.
Lung function: No minimum or maximum FEV1
In Canada, due to improvements in care, early-stage lung disease is increasingly being seen in adolescents and adults with CF as defined by conventional spirometry measurement. This will become common with the availability of highly effective modulator therapy. However, FEV1 is not a useful marker in mild lung disease, in part, due to its relatively insensitivity to detection of early small airways destruction. This is illustrated, when CF patients with no abnormality in lung function underwent chest CT imaging. Despite a normal FEV1 there was evidence of significant structural lung disease. Additionally, several trials have shown that in patients with normal lung function (ppFEV1>90%) the addition of a CFTR modulator caused further significant gains in ppFEV1, illustrating improvement to be made in mild CF lung disease. The most recent data showed in children aged 6-11 years with an average ppFEV1:89% of whom 45% had ppFEV1>90%, the addition of ELX-TEZ-IVA produced an increase in ppFEV1 of 10%. Consequently, no upper limit of lung function should be required for eligibility as further significant gains in respiratory health can be made in CF patients with mild lung disease.
Patients with lung function that is low (ppFEV1<40%) or are awaiting lung transplantation also improve on treatment to the point where many no longer need transplantation. Consequently, no lower limit of lung function should be required for eligibility.
Pancreatic status: Pancreatic sufficient and insufficient
Pancreatic status does not affect eligibility. The majority of patients with CF are pancreatic insufficient but some patients are not. Early introduction of CFTR modulator therapy has the potential to restore pancreatic function or delay onset of pancreatic insufficiency. In patients with pancreatic sufficiency, CFTR modulators will likely preserve pancreatic function.
Healthcare Advisory Council guidelines for prescribing a CFTR Modulator
Figure 20 summarizes the various different Health Canada-approved CFTR modulators. The recommended CFTR variant, age of initiation, and duration for each modulator is provided.
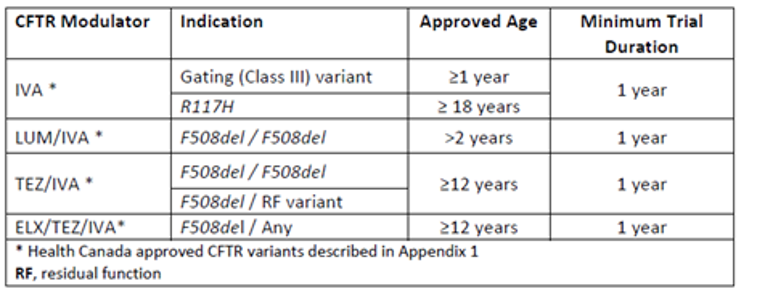
Pre-modulator assessment
If a patient has not had a confirmatory sweat test and/or CF genotyping this should be undertaken. Baseline clinical assessments required are illustrated in Figure 21 and Figure 22. These should be obtained when the patient is clinically stable.
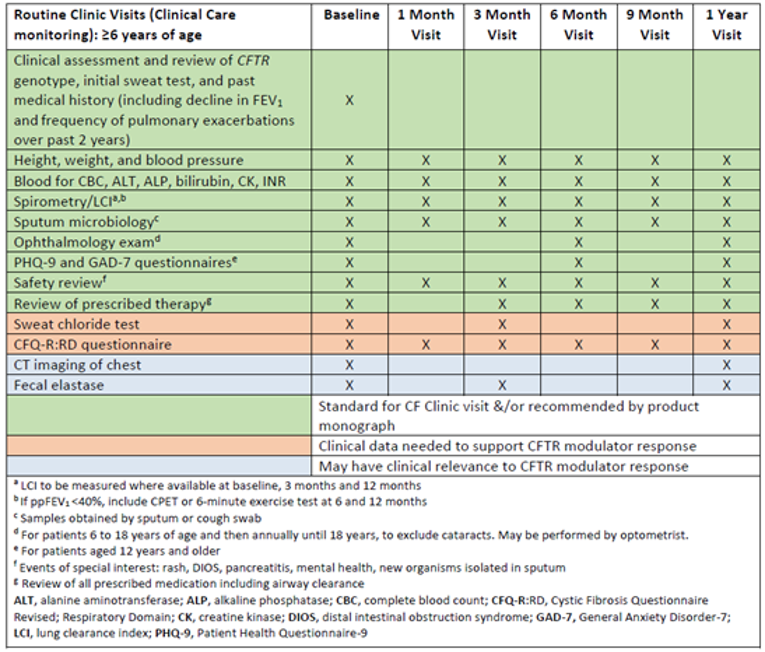
Figure 22: Schedule for baseline evaluation and monitoring of patients under 6 years of age who commence on CFTR modulators
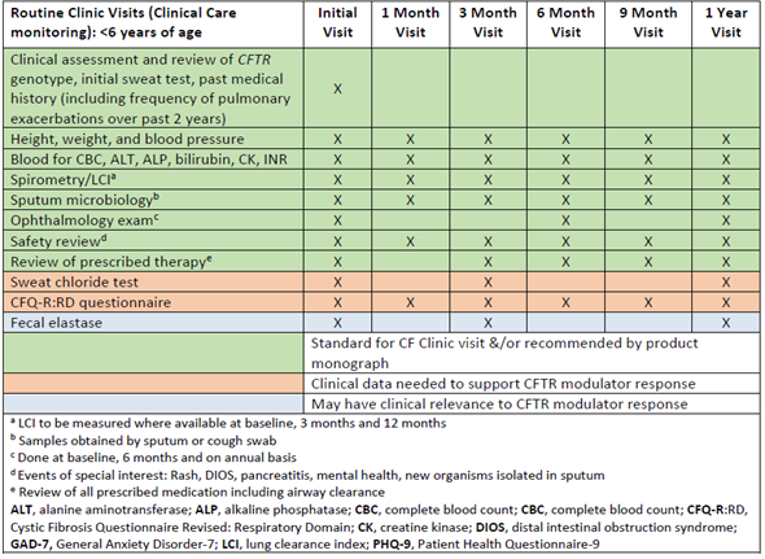
Response to therapy
Clinical trials for CFTR modulators have reported improvements in lung function and weight, and reduced pulmonary exacerbations requiring antibiotics. As CFTR modulators are systemic medications, they impact CFTR function in the sweat glands as measured by the concentration of chloride in sweat. Although this does not have direct clinical significance at an individual level other than reducing risk of dehydration or heat stroke, it is a biomarker of the effect of CFTR modulator and trials have shown modulator use is associated with a reduction in sweat chloride.
Longer-term follow-up studies have evaluated the impact of CFTR modulators on FEV1 rate of decline. These studies have shown an improvement in lung function trajectory with a slowing in the rate of FEV1 decline compared to patients not on CFTR modulators. However, patients STILL have a decline in FEV1 over time DESPITE the impact of CFTR modulators. Patients with CF have bronchiectasis with chronic infection and irreversible structural lung damage which will impact FEV1 recovery and trajectory. As life expectancy improves for patients with CF it is expected that FEV1 will still decline year to year due to the natural aging of the patient even in the presence of CFTR modulators.
Modelling and real-life experience with CFTR modulator introduction have shown significant reduction in disease severity and improvement in clinical parameters in patients with significant disease burden. In addition, patients report an impact on respiratory symptoms, sleep quality, general well-being and physical self-esteem, and a reduced treatment burden. Patients reported renewed and unexpected physical strength, leading to greater self-confidence, autonomy, and long-term planning, after treatment initiation.
Consideration should be given to CF-related comorbidities. Although not reported in clinical studies, patients may experience improvement in CF issues such as sinus disease, pancreatitis, and CF-related diabetes with the introduction of CFTR modulators.
Data has suggested that there may be responders and non-responders to CFTR modulator therapy. In order to identify responders, the recommendation is to evaluate CFTR modulator therapy for a MINIMUM duration of 1 year. This duration is needed to accurately assess reductions in pulmonary exacerbations, provide adequate lung function data to determine improvement and stabilization of FEV1 over time and monitor improvement in nutrition.
Meaningful clinical responses to be monitored include:
Improvement in lung function as measured by FEV1 or Lung Clearance Index (where available) obtained at a time of clinical stability
Reduction in the number of pulmonary exacerbations
Stabilization of lung function over time (i.e., attenuation of the usual decline in lung function)
Reduction or stabilization of respiratory symptoms
Improvement in nutritional status
Improvement in quality of life scores
Reduction in sweat chloride
Concurrent Treatment
At the present time, all patients commenced on a CFTR modulator should continue with current treatments as directed by their CF clinic (e.g., pancreatic enzymes, mucolytics, inhaled antibiotics, bronchodilators, anti-inflammatory agents). They should continue to be monitored quarterly as per CF standards of care. Ongoing clinical studies will determine if any CF treatments can be discontinued once patients are on CFTR modulator therapy. The schedule of clinical assessment and monitoring is outlined in Figure 21 and Figure 22.
Treatment Response
It is expected that responders will have at:
3 months
Absolute improvement in ppFEV1 of >5%, measured at time of clinical stability; OR
A decrease in sweat chloride by 20% or 20mmol/L from baseline; OR
Improvement in respiratory symptoms (as measured by CFQ-R: Respiratory Domain) > 4 points.
12 months
No adverse events or medication safety issues, and one or more of:
Reduction in pulmonary exacerbations (IV or oral antibiotic treatment) by 20%; OR
Stabilization of lung function rate of decline above baseline; OR
Improvement in nutritional status with normalization of growth and nutrition; OR
Radiological improvement or stability in Chest CT scan.
Figure 23 is a summary of changes in expected outcomes for responders to different CFTR modulators
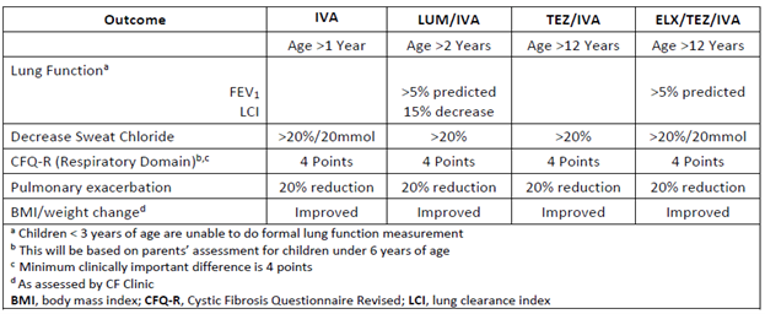
Monitoring
Comprehensive monitoring of patients who are commenced on CFTR modulators is detailed in Figure 21 and Figure 22. Clinics should aim to follow this schedule in order to demonstrate response to therapy.
Side Effects
After initiation of CFTR modulators, it is important to focus on safety outcomes and monitor for potential adverse effects. A systematic review of safety outcomes reported in real-world studies of the 4 market-available CFTR modulators has recently been published and is an excellent source of reference, but there are limited reports of longer-term real-world experience, especially with ELX-TEZ-IVA. Therefore, vigilant post-market monitoring for both expected and unexpected adverse effects is warranted.
Safety issues of note are:
a) Liver enzymes and/or bilirubin
Elevated transaminases have been observed in patients on CFTR modulators. Isolated elevation in bilirubin can also be seen in some cases. This can occur at any time during treatment even if the modulator has been previously well tolerated. Rarely does this result in the need to interrupt therapy, reduce the dose, or discontinue the modulator. Elevated transaminases and bilirubin will need to be reviewed to further determine the need to interrupt therapy, reduce the dose, or discontinue the modulator. It is recommended that liver enzymes should be monitored every 3 months in the first year and then annually. For individuals with moderate or severe CF-related liver disease, recommendations for dosage adjustments are available. Worsening of liver function has been observed in patients with pre-existing cirrhosis and portal hypertension who have started CFTR modulators.
b) Rash or hypersensitivity reactions
Rash is relatively common following initiation of CFTR modulators and has been reported in real-world studies for each of IVA, LUM/IVA, and TEZ/IVA. Rare cases of delayed hypersensitivity reactions have also been reported. Few individuals required interruption or discontinuation of therapy for rash or hypersensitivity reactions. Similar occurrence was seen in clinical trials, with cases of rash being reported for all 4 CFTR modulators, and serious rash or discontinuation due to rash being reported for ELX-TEZ-IVA and LUM/IVA. The incidence of rash events appears to be higher in female CF patients, particularly those on hormonal contraceptives, and more frequent on ELX-TEZ-IVA, but the mechanism behind this is unclear.
c) Drop in FEV1 and respiratory symptoms
Of the available CFTR modulators, LUM/IVA has had the highest reported respiratory-related side effects. Chest tightness, dyspnea, increased sputum, and declines in ppFEV1 were among the most common respiratory symptoms and tended to occur within the first few days after initiation. Bronchodilators were beneficial in mitigating symptoms of chest tightness, wheeze, and increased work of breathing in some individuals. Improvement in or resolution of symptoms occurred within 1–4 weeks following initiation, but symptoms and/or ppFEV1 below baseline could persist beyond this and some patients may require a dose reduction or discontinuation altogether to achieve resolution.
d) GI-related adverse effects
Symptoms of abdominal pain, nausea, and vomiting have been reported in the real-world studies, but rarely prompted discontinuation of therapy. Concerns have been raised about the potential for distal intestinal obstruction syndrome (DIOS) following initiation of highly effective CFTR modulators. Therefore, patients with chronic constipation and/or other risk factors for DIOS should be closely monitored following initiation.
e) Blood pressure elevation
Elevations in blood pressure were reported in the phase III clinical trials for LUM/IVA and ELX-TEZ-IVA. For ELX-TEZ-IVA, 4% of treated subjects had systolic blood pressure >140 mm Hg and 10 mm Hg increase from baseline on at least 2 occasions. Similarly, 1% had diastolic blood pressure >90 mm Hg and 5 mm Hg increase from baseline on at least 2 occasions. The mechanism by which CFTR modulators may cause blood pressure elevations remains unclear.
f) Creatine kinase
Creatine kinase elevations have been reported in clinical trials for all 4 CFTR modulators. Clinical context of elevations is important, as CK levels fluctuate significantly with exercise and physical activity, especially if intensive, and may take a few days to normalize thereafter. Although the clinical relevance of CK elevations is unclear, some cases may be serious enough to warrant interruption or discontinuation of therapy.
g) Mental health
Cases of negative impacts on mental health (e.g., depression, anxiety) have been reported for all 4 market-available CFTR modulators, even in individuals without a prior history of mental health concerns, raising a signal for a potential association with CFTR modulators. Although a causal relationship has not been established and a mechanism is not clear, it is an important potential outcome to be mindful of. In addition, there are significant drug-drug interactions with LUM/IVA and antidepressant medications.
h) Cataracts
Cases of non-congenital lens opacities have been reported in pediatric patients treated with IVA-containing regimens. Although other risk factors were present in some cases (such as corticosteroid use, exposure to radiation), a possible risk attributable to treatment with IVA cannot be excluded. Baseline and follow-up ophthalmological examinations are recommended in pediatric patients initiating treatment with CFTR modulators to be done at baseline, 6 months, and on annual basis until age 18.
Drug-Drug Interactions
It is important to assess for drug-drug interactions when starting or stopping medications in an individual on a CFTR modulator or when transitioning from different CFTR modulators. IVA, TEZ, and ELX are substrates of cytochrome P450 (CYP) enzyme CYP3A. Therefore, strong and moderate inhibitors (e.g., azole antifungals) of CYP3A can increase exposure to IVA, TEZ, and ELX, while inducers (e.g., rifampin) can decrease serum levels. Recommendations are available for how to dose-adjust modulators when taken concomitantly with moderate or strong CYP3A inhibitors, but concomitant use with inducers should be avoided. It is important to note that foods and herbal products can also affect CYP3A (food or drinks containing grapefruit can inhibit CYP3A in the gastrointestinal tract, while the herbal product St. John’s wort induces CYP3A).
CFTR modulators have also been associated with inhibition or induction of enzymes. IVA and one of its metabolites weakly inhibit CYP3A and P-glycoprotein (P-gp), and potentially CYP2C9. Because of the potential impact on CYP3A and CYP2C9, the international normalized ratio should be closely monitored in individuals on warfarin who are starting or stopping a CFTR modulator. Alternatively, LUM is an inducer of CYP3A and UDP-glucuronosyltransferase (UGT) enzymes, and may increase metabolism of concomitant medications that are substrates of these enzymes (e.g., hormonal contraceptives, azole antifungals, select immunosuppressants, and psychotropic medications).
Special considerations for patients receiving IVA, LUM/IVA, TEZ/IVA CFTR Modulators
Health Canada approved ELX-TEZ-IVA in June 2021 for CFTR variants F508del/Any in patients 12 years and older. In the near future this age limit will likely be reduced to >6 years of age. A small number of children will remain on either LUM/IVA or IVA. Data has shown that ELX-TEZ-IVA has superiority over TEZ/IVA in patients with 2 copies of F508del. In a study comparing patients F508del/MF or gating variant who were randomized to either continue taking TEZ/IVA or IVA or switched to ELX-TEZ-IVA a modest incremental improvement in FEV1 was observed, with significant gains in CFQ-R-Resp domain and further reduction in sweat chloride levels. All patients on IVA, LUM/IVA or TEZ/IVA, should have the opportunity to transition to the triple therapy combination, ELX-TEZ-IVA.
Pregnancy and CFTR Modulators
CFTR modulators may increase fertility in women with CF due to improvement in clinical status and to their impact on the mucus in the cervix and uterus and so it is important for women on CFTR modulators to use birth control to prevent unplanned pregnancies. The clinical trials of CFTR modulators excluded women who were not using effective contraception, so the effect of these drugs on a developing human fetus is unknown. Animal studies of the individual drugs IVA, LUM, TEZ, and ELX CFTR indicate no impact on organogenesis at normal human doses. Real-world experience is limited but case reports and an international survey have demonstrated that CFTR modulators appear to be well tolerated during pregnancy. As discontinuation of CFTR modulators has been associated with significant decline in clinical status, the risks/benefits of CFTR therapy during pregnancy must be discussed, ideally before pregnancy. CFTR modulators are expressed in breast milk. As CFTR modulators have been associated with cataracts in children, it would be advisable that infants born to mothers taking CFTR modulators have ophthalmologic examination.
CF Patients Who Have Received a Lung Transplantation
Lung transplant is a treatment option for people with CF with end-stage lung disease. While CFTR modulators would not be expected to directly improve lung graft function, they have potential to alleviate extrapulmonary manifestations of CF such as chronic rhinosinusitis and gastrointestinal disease. Of note, paranasal sinuses may act as a reservoir for pathogens following transplantation, therefore treatment of chronic rhinosinusitis with CFTR modulators may reduce respiratory infectious complications after lung transplantation.
With the introduction of TEZ/IVA/ELX, evidence is emerging of its use after lung transplant. Drug-drug interaction between CFTR modulators and immunosuppressants, such as calcineurin inhibitors, should be expected. In addition, liver injury secondary to use of CFTR modulators may complicate management of a lung transplant recipient prescribed antimicrobials and immune suppressing medications associated with hepatoxicity. The general recommendations on response to CFTR modulator therapy following initiation would not be applicable to the lung transplant population. It is recommended that a CF specialist be involved in the initiation of CFTR modulators and subsequent monitoring of a CF patient who has undergone lung transplant and commenced on a CFTR modulator.
Discontinuation
Discontinuation (or dose reduction) of CFTR modulator therapy should be considered in patients who have clinically significant adverse effects that persist or recur despite a decrease in dose (if appropriate) and/or stopping and re-challenge. Examples of these reactions may include:
Elevation of transaminases beyond the higher range of fluctuations observed in patients with CF (>8X ULN) or 3XULN of transaminases and bilirubin (>2 x ULN)
Allergic reactions to treatment and failed desensitization challenges
However, the risk-benefit of discontinuing treatment should be considered on a case-by-case basis depending on the severity of the adverse event and risk of stopping treatment. Therapy should be discontinued in patients who, as assessed by the CF team, do not meet criteria for response to the CFTR modulator or are non-adherent to the CFTR modulator. This decision to discontinue therapy should be done after clinical stability, any confounding comorbidities have been assessed and nonadherence issues have been addressed.
How to Start CFTR Modulators
Given the large number of patients who will qualify for CFTR modulators, initiation will at first impose challenges on individual CF clinics. How this will be undertaken will be determined by individual CF centres based on the number of eligible patients, clinic resources, and provincial availability. For patients who have had a significant adverse reaction to a CFTR modulator and a re-challenge is deemed appropriate, or if initiation at a reduced dose and titrating to full-dose is preferred, potential protocols are summarized in the systematic review performed by Dagenais et al.
Summary
The approval of CFTR modulators by Health Canada is a milestone in CF care and is the first time that a CF treatment has targeted the basic defect and not the consequences of the disease. Real-world evidence suggests that CFTR modulators will slow the progression of disease and reduce mortality. All patients who are eligible should be started on therapy as soon as possible to prevent lung disease progression and comorbidities.
Patients should be started on an age-appropriate, CFTR variant-specific modulator with a recommended duration of at least 1 year. Response to therapy and safety should be monitored. If response to therapy is seen, then patients will continue indefinitely on the CFTR modulator therapy and standard of care treatment. Follow-up will be determined by their CF clinic. Discontinuation of modulator therapy should be performed in patients with significant side effects or those who are deemed non-responders after 1 year of therapy. Efficacy data should be collected as part of the CCFR or as part of a prospective study.
Appendix 2: Synopsis of Real-world Analyses Conducted on the Effectiveness of ELX-TEZ-IVA in Patients with Pre-treatment ppFEV1 > 90
Note that this appendix has not been copy-edited.
Background
The efficacy and safety of ELX-TEZ-IVA among patients with CF aged 12 years and older have been studied in pivotal phase III VX-445-102 and 103 clinical trials. One of the key inclusion criteria in the phase III clinical trials is patients with a ppFEV1 value that is ≥ 40% and ≤ 90%. Clinical efficacy of ELX-TEZ-IVA among patients with a pre-treatment ppFEV1 > 90% is unknown. Vertex conducted 2 separate descriptive analyses of the effectiveness of ELX-TEZ-IVA among patients with ppFEV1 > 90% in the real-world setting. The analysis and the corresponding results are described below.
Interim Analysis of a Subgroup of Patients With PpFEV1 > 90% in the HELIO Real-world Study
HELIO is an ongoing US multi-centre, prospective, observational study of clinical effectiveness of ELX-TEZ-IVA in the real-world setting. The study is sponsored by Vertex Pharmaceuticals and no drug was supplied for the study. All study data including clinical characteristics (age, genotype) and ppFEV1 values based on in-clinic spirometry were extracted from patient EMRs.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 66: Age and Spirometry Outcomes for all Patients and a Subgroup of Patients With ppFEV1 more than 90 in the HELIO Interim Dataset
||||||VVVVV | ||||||VVVVV |
|---|---|
||||||VVVVVVVVVVVVVVVVVVVVVVVVV | |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
||||||VVVVVVVVVVVVVVVVVVVVVVVVV | |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
Analysis of Patients With ppFEV1 Greater Than 90 in the US CF Foundation Patient Registry (CFFPR) Real-World Data
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 67: Age and ppFEV1 for F/MF and F/F Patients With ppFEV1 > 90 in US CFFPR Dataset
||||||VVVVV | ||||||VVVVV |
|---|---|
||||||VVVVVVVVVVVVVVVVVVVVVVVVV | |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
||||||VVVVVVVVVVVVVVVVVVVVVVVVV | |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
|||||| | |||||| |
Sponsor’s Conclusions
Results from 2 separate analyses of real-world data show that ELX-TEZ-IVA treatment is associated with clinically meaningful improvements in ppFEV1 in a subset of patients with pre-treatment ppFEV1 > 90. The magnitude of treatment effects in the F/MF group were similar in both studies.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Limitations Identified By the Sponsor
These findings are based on observational studies using data that were not collected for research purposes. The lack of a comparator group in these studies make causal interpretation of these results impossible. Some of the data in these real-world studies were collected during the COVID-19 period. The impact of the COVID-19 pandemic on the measurements or missing data were not evaluated.
Appendix 3: Literature Search Strategy
Note that this appendix has not been copy-edited.
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: February 22, 2021
Alerts: Bi-weekly search updates until project completion
Study Types: No search filters were applied
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search Strategy
(trikafta* or kaftrio* or (ELX adj2 TEZ adj2 IVA) or (elexacaftor adj2 tezacaftor adj2 ivacaftor)).ti,ab,kf,ot,hw,rn,nm.
(ivacaftor* or kalydeco* or symdeko* or symkevi* or VX770 or VX-770 or Y740ILL1Z).ti,ab,kf,ot,hw,rn,nm.
(elexacaftor* or VX-445* or VX445 or WHO 11180 or WHO11180 or RN67GMB0V).ti,ab,kf,ot,hw,rn,nm.
(tezacaftor* or symdeko* or symkevi* or VX661 or VX-661 or RW88Y506K).ti,ab,kf,ot,hw,rn,nm.
2 and 3 and 4
1 or 5
(((triple or tri) adj3 (combination* or combo or therap*)) or ETI).ti,ab,kf.
Cystic Fibrosis/ or ((cystic adj2 fibrosis) or mucoviscidos* or fibrocystic or F508del).ti,ab,kf.
7 and 8
6 or 9
10 use medall
*elexacaftor plus ivacaftor plus tezacaftor/
(trikafta* or kaftrio* or (ELX adj2 TEZ adj2 IVA) or (elexacaftor adj2 tezacaftor adj2 ivacaftor)).ti,ab,kw,dq.
12 or 13
*ivacaftor/ or *ivacaftor plus tezacaftor/
(ivacaftor* or kalydeco* or symdeko* or symkevi* or VX770 or VX-770).ti,ab,kw,dq.
15 or 16
*elexacaftor/
(elexacaftor* or VX-445* or VX445 or WHO 11180 or WHO11180 or RRN67GMB0V0).ti,ab,kw,dq.
18 or 19
*tezacaftor/ or *ivacaftor plus tezacaftor/
(tezacaftor* or symdeko* or symkevi* or VX661 or VX-661 or 8RW88Y506K).ti,ab,kw,dq.
21 or 22
17 and 20 and 23
14 or 24
(((triple or tri) adj3 (combination* or combo or therap*)) or ETI).ti,ab,kf,dq.
Cystic Fibrosis/ or ((cystic adj2 fibrosis) or mucoviscidos* or fibrocystic or F508del).ti,ab,kw,dq.
26 and 27
25 or 28
(conference review or conference abstract).pt.
29 not 30
31 use oemezd
11 or 32
remove duplicates from 33
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results trikafta or kaftrio or vx-445 or elexacaftor]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- trikafta or kaftrio or vx-445 or elexacaftor]
Grey Literature
Search dates: February 8-16, 2021
Keywords: trikafta, kaftrio, vx-445, elexacaftor, ELX/TEZ/IVA, cystic fibrosis
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search.
Appendix 4: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Davies JC, Moskowitz SM, Brown C, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1599-1611.104 | Intervention (not ELX-TEZ-IVA) |
Keating D, Marigowda G, Burr L, et al. VX-445-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. N Engl J Med. 2018;379(17):1612-1620.105 | Study design (phase II) |
ELX-TEZ-IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor.
Appendix 5: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 70: Subgroup Analyses for Absolute Change From Baseline to Week 4 in ppFEV1 in Study 102
Subgroups | Placebo | ELX-TEZ-IVA | ELX-TEZ-IVA vs. Placebo LSMD (95% CI) | |||
|---|---|---|---|---|---|---|
n | LS mean (SE) | n | LS mean (SE) | |||
Age at screening | ≥12 to <18 years | 53 | 3.5 (1.3) | 46 | 17.3 (1.4) | 13.8 (10.0 to 17.5) |
≥18 years | 135 | -1.1 (0.6) | 139 | 12.6 (0.6) | 13.6 (11.9 to 15.4) | |
ppFEV1 at baseline | <70% | 128 | 0.4 (0.8) | 124 | 14.5 (0.8) | 14.2 (12.0 to 16.3) |
≥70% | 60 | -1.2 (0.9) | 61 | 11.8 (0.9) | 13.0 (10.6 to 15.5) | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; LS = least squares; LSMD = least squares mean difference; n = number of patients in subgroup analysis; ppFEV1 = percent predicted forced expiratory volume in one second; SE = standard error.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.7
Table 71: Subgroup Analyses for Absolute Change from Baseline in ppFEV1 for Patients with Baseline ppFEV1 < 40% (Study 102)
Time Point | Study 102 (M/F) | ||
|---|---|---|---|
Placebo (N = 16) | ELX-TEZ-IVA (N = 18) | ||
At 4 weeks | Baseline mean (SD) | 37.5 (2.1) | 37.0 (1.7) |
LS mean (SE) | 0.8 (2.8) | 16.0 (2.6) | |
Patients in analysis | 16 | 17 | |
LSMD (95% CI) | 15.2 (7.3 to 23.1) | ||
P value | <0.0001 | ||
Through 24 weeks | Baseline mean (SD) | 37.5 (2.1) | 37.0 (1.7) |
LS mean (SE) | 0.3 (2.4) | 18.7 (2.3) | |
Patients in analysis | 16 | 17 | |
LSMD (95% CI) | 18.4 (11.5 to 25.3) | ||
P value | <0.0001 | ||
CI = confidence interval; ELX-TEZ-IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; F/MF = one F508del mutation and one minimal function mutation in the CFTR gene; LSMD = least squares mean difference; LS = least squares; ppFEV1 = percent predicted forced expiratory volume in one second; SD = standard deviation; SE = standard error.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.7
Table 72: Subgroup Analyses for Absolute Change from Baseline to week 4 in ppFEV1 in Study 103
Subgroups | TEZ/IVA | ELX-TEZ-IVA | ELX-TEZ-IVA vs. TEZ/IVA LSMD (95% CI) | |||
|---|---|---|---|---|---|---|
n | LS mean (SE) | n | LS mean (SE) | |||
Age at screening | ≥12 to <18 years | 11 | 0.2 (2.1) | 15 | 14.8 (2.0) | 14.7 (9.0 to 20.4) |
≥18 years | 38 | 0.6 (1.0) | 38 | 9.0 (1.0) | 8.4 (5.6 to 11.2) | |
ppFEV1 at baseline | <70% | 37 | 0.6 (1.1) | 35 | 11.7 (1.2) | 11.2 (8.0 to 14.4) |
≥70% | 12 | 0.9 (1.5) | 18 | 7.3 (1.3) | 6.3 (2.3 to 10.4) | |
CI = confidence interval; ELX-TEZ-IVA = elexacaftor/tezacaftor/ivacaftor + ivacaftor; LS = least squares; LSMD = least squares mean difference; n = number of patients in subgroup analysis; ppFEV1 = percent predicted forced expiratory volume in one second; SE = standard error; TEZ/IVA = tezacaftor/ivacaftor + ivacaftor.
MMRM analyses for the subgroups were similar to those performed for the primary analyses.
Source: Clinical Study Report.8
Appendix 6: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
FEV1 (primary outcome in Study 102, 103, and 104; key secondary outcome in Study 109)
CFQ-R respiratory symptom domain (primary outcome in Study 109, key secondary outcome in Study 102 and 103, other outcome in Study 104)
Findings
Table 73: Summary of Outcome Measures and The Respective Measurement Properties
Outcome measure | Type | Conclusions about Measurement Properties | MID |
|---|---|---|---|
FEV1 | Pulmonary function test (maximal amount of air forcefully exhaled in one second) | FEV1 has been shown to relate to morbidity, disease progression, and mortality in CF, and thus is a meaningful surrogate marker for survival. FEV1 is highly dependent on patient cooperation and effort to perform test and can only be used on children old enough to comprehend and follow the instructions given. It has a ceiling effect for patients with mild lung impairment. | Not defined |
CFQ-R Respiratory Symptom Domain | Respiratory symptom scale of a disease-specific HRQoL instrument | Validity:
Reliability: Internal consistency reliability and test-retest reliability was acceptable. Responsiveness: Limited assessment of responsiveness reported in the literature. | Anchor based: Stable CF: 4.0 points59; Exacerbation of CF: 8.5 points59 Distribution based: |
CF = cystic fibrosis; CFQ-R = Cystic Fibrosis Questionnaire – Revised; FEV1 = forced expiratory volume in one second; HRQoL = health-related quality of life; MID = minimal important difference.
Forced Expiratory Volume in One Second
FEV1 is the maximal amount of air forcefully exhaled in one second, expressed in litres.75 The measured volume is converted to a percentage of predicted normal value, which is adjusted based on age, sex, and body composition.75 FEV1 is used to establish the severity of lung disease (normal or mild pulmonary dysfunction, > 70% predicted; moderate dysfunction, 40% to 69% predicted; and severe dysfunction, < 40% predicted), tracking changes in lung function over time, and in evaluating the effectiveness of therapeutic interventions in CF.63,75
FEV1 is a commonly used end point for clinical trials of obstructive lung diseases including CF107 and is the preferred end point in the European Medicines Agency guidance document on the development of therapeutic drugs for CF, based on the fact that the main pulmonary defect in CF is obstructive.63 FEV1 has been shown to relate to morbidity, disease progression, and mortality in CF, making it a meaningful surrogate marker for survival.63,107,108
However, there are limitations with the use of FEV1 for patients with CF:
The maneuver required to assess FEV1 is highly dependent on patient cooperation and effort:
The test (spirometry) should be repeated at least 3 times to ensure reproducibility75
Spirometry can only be used on children old enough to comprehend and follow the instructions given (6 years old or more), and only on patients who are able to understand and follow instructions63,107
FEV1 can generally only be underestimated. The only exception in which FEV1 can be overestimated is in individuals with some diseases where a softer exhalation can reduce the spasm or collapse of lung tissue, thereby artificially elevating the measure.
FEV1 is unable to detect early lung damage or early bronchiectasis in patients with CF.108
There are limited data on the magnitude of change in FEV1 that is clinically meaningful. The short-term variability in FEV1 is unclear for patients with CF.108
There are no established MIDs for FEV1 in patients with CF.108 Bhatia, Kaye and Roberti-Miller106 estimated the MID for the ppFEV1 based on data from 12 patients with moderate to severe CF who were followed for 1 year. They reported an MID of 7.1%, that was calculated using distribution-based methods (i.e., half the SD at baseline). However, the authors of this study stated this estimate was preliminary and required validation.106
FEV1 improvement has a ceiling effect for patients with mild lung impairment.107
FEV1 decline is only meaningful over time and is subject to seasonal and environmental effects.107
The European Medicines Agency suggests a study duration of 6 months for the demonstration of efficacy on respiratory function (based on repeated measurements of FEV1) with a 12-month follow-up for safety.63
CF is a multi-organ disease and FEV1 only measures lung health.107
Cystic Fibrosis Questionnaire – Revised
The CFQ-R is a disease-specific HRQoL instrument designed for patients with CF, comprised of age-appropriate versions for children aged six to 3 (CFQ-C), their parents (who serve as a proxy for their child; CFQ-P), and individuals ≥ 14 years of age (CFQ-14).56 For children 6 to 11, the CFQ-C is interviewer-administered, and for 12 and 13 year-olds, it is self-administered.57 The number of items and domains vary between versions with the child version including 35 items within 8 domains, the parent version has 44 items and 11 domains, and the adolescent and adult version has 50 items within 12 domain (Figure 24).56,57 The domains included in the adolescent and adult version are as follows: HRQoL module including physical functioning, vitality, emotional functioning, social or school functioning, role functioning, body image, eating problems, treatment burden; symptoms module that includes respiratory symptoms, digestive symptoms, and weight; and a health perception module. A 4-point Likert scale is used to measure frequency (always, often, sometimes, never), intensity (a great deal, somewhat, a little, not at all) and true-false scales (very true, somewhat true, somewhat false, very false). Items within domains are summed and standardized. Individual domain scores range from 0 to 100, with higher scores indicating better HRQoL.56 The scales are designed to measure symptoms and functioning during the 2-week period prior to administration of the questionnaire.58
In Study 102, 103, 104, and 109, patients aged 12 and 13 years completed the CFQ-C and their parents completed the CFQ-P questionnaire. All patients who were 14 years and older completed the CFQ-14 version. The survey was provided in the patient’s native language, if a validated translation was available, otherwise the patient did not complete the questionnaire.
Figure 24: CFQ-R Scales and Exemplar Items
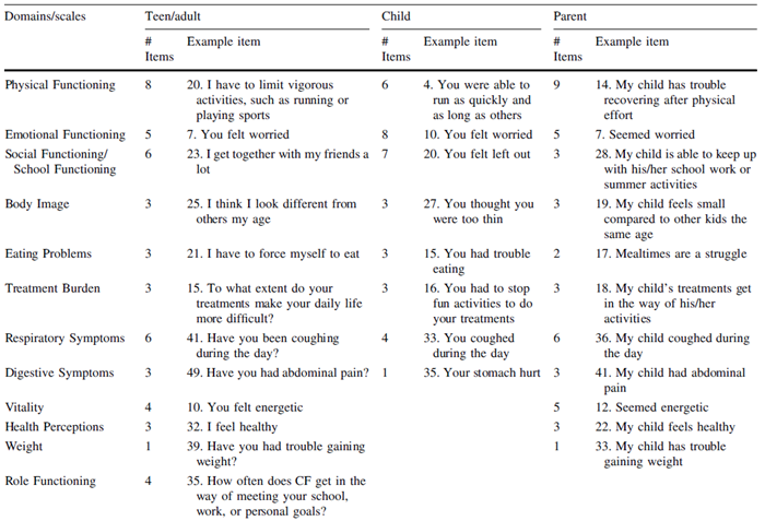
Source: Reprinted by permission from Springer Nature: Springer Nature Quality of Life Research. Erratum to: Psychometric evaluation of the Cystic Fibrosis Questionnaire–Revised in a national, US sample. Quittner AL, Sawicki GS, McMullen A, et al., 2021.56
Several studies have evaluated the validity and reliability of the CFQ-R questionnaire.56 and its original version.57,58,109,110 Quittner et al. (2012)56 examined the psychometric properties of the CFQ-R using data from the Epidemiologic Study of Cystic Fibrosis, a national US multi-centre longitudinal cohort study containing CFQ-R and health outcomes data from 7,330 patients aged 6 years to 70 years, plus data from 2,728 parents for the CFQ-P. Quittner et al. (2012)56 reported adequate internal consistency (Cronbach alpha ≥ 0.70) for most domains and scales on each of the 3 versions, with lower reliability (< 0.6) found for treatment burden, social functioning, or school functioning. For the respiratory symptom domain, the Cronbach alpha reported was 0.87, 0.69, 0.82 for the CRQ-14, CFQ-C, and CFQ-P, respectively.56
Discriminant validity was demonstrated as CFQ-R scores were consistently lower for patients who were sick, compared with those who were well for all 3 versions of the instrument.56 If a patient’s clinical encounter form included any documentation of “sickness” within 21 days of the CFQ-R completion date, the patient was considered sick. For the respiratory domain specifically, the effect size for the difference in mean scores for sick versus well patients with CF ranged from –0.59 to –0.95 across the 3 versions.56
Discriminant validity was also assessed by testing the ability of the CFQ-R scales to differentiate between groups of patients with increasing severity of disease based on ppFEV1. It was hypothesized that most CFQ-R scales (except for digestion) would vary by lung function. For all 3 versions of the questionnaire, statistically significant differences in scores were detected between disease severity stages for most CFQ-R domains. Scores for the digestion domain showed no difference across the pulmonary function disease stages.56 For children, however, this analysis had limitations, because this population had less variability in disease severity as few school-age children had a FEV1 < 70% predicted.56
Construct validity: There was fair-to-moderate correlations between CFQ-R scales and health outcomes, including ppFEV1 (correlation range, 0.25 to 0.51), number of pulmonary exacerbations treated with IV antibiotics (range = −0.23 to −0.35), and BMI (range = 0.22 to 0.44).56 The strongest correlations were demonstrated for the physical functioning and respiratory domains with ppFEV1 (range = 0.33 to 0.51 and 0.32 to 0.42, respectively) and for the weight scale and BMI (range = 0.42 and 0.44 on the CFQ-P and CFQ-14, respectively). The respiratory domain showed weak correlation with the number of exacerbations (range = --0.24 to -0.29).56 Overall, the correlations were lower for the CFQ-C and CFQ-P than the CFQ-14.
Quittner et al. (2012)56 also reported fair-to-moderate agreement between the child and parent versions on all scales of the CFQ-R (intraclass correlation coefficient range = 0.26 to 0.56); however, stronger agreement was found on domains that measured more observable signs and symptoms, such as physical functioning (r = 0.46), eating problems (r = 0.56), and respiratory symptoms (r = 0.55).56 Tluczek et al. (2013)57 examined parent-child concordance in CFQ (original version) domains for children aged 8 years to 13 years and adolescents aged 14 years to 18 years (total N = 92 pairs). Five of the domains of the CFQ-C instrument were similar to the parent-reported CFQ-14, with children reporting better HRQoL than parents for the digestive symptoms and body image domains.57 Male children reported worse HRQoL on emotional functioning that their parents. Adolescents rated HRQoL higher than their parents on weight, body image, digestive symptoms, eating disturbance, physical and emotional functioning, treatment burden, and respiratory symptoms.57 Many of the differences were driven by male adolescents.57
Quittner et al. (2005)109 showed the CFQ-14 (original 44 item version) correlated well with the SF-36 based on data from 212 adolescents and adults with CF with mild to severe pulmonary disease. Correlations were strong (range = 0.57 to 0.84) between similar dimensions of the CFQ-14 and SF-36 (physical, health perceptions and general health, vitality, role/role physical, emotional functioning, and mental health, and social) and weak to moderate (range = 0.19 to 0.42) between scales not expected to be related (digestion and role scales of the CFQ and general health and mental health scales of the SF-36). Test-retest reliability was also assessed on a subset of 21 patients with stable disease. With repeat administration over 14 days the intraclass correlation coefficients ranged from 0.45 (social domain) to 0.90 (respiratory symptoms), with 7 of 12 domains showing intraclass correlations that exceeded the generally accepted threshold of 0.7 for reliability.109 In the initial development of the CFQ instrument, Henry et al. (2003)58 reported test-retest reliability was acceptable for the CFQ-14 respiratory domain (ICC 0.88) but not for the CFQ-C respiratory domain (ICC 0.48) when tests were repeated approximately 8 days apart in 22 adolescents or adults, and 22 children with stable CF.
Limited data were identified that evaluated the responsiveness of the CFQ (original version) domains. Henry et al. (2003)58 reported large effect size (0.63 to 1.17) for the respiratory symptom and physical functioning domains of the CFQ-14 and CFQ-C in 24 adolescents or adults, and 17 children who showed clinical improvement after antibiotic treatment for an exacerbation. The effect size for other domains were moderate to weak.58
The MID was estimated for the CFQ-R respiratory symptom scale in 2 study populations: one with patients with stable CF and chronic P. aeruginosa airway infection (N = 140); the other with patients with exacerbation of CF and chronic P. aeruginosa airway infection (N = 84).59 Both anchor-based and distribution-based methods were used. The anchor-based methods used a Global Rating of Change Questionnaire that assessed patients’ perceptions of the change in their respiratory symptoms. The MID for patients with stable disease was estimated to be 4.0 points, and for patients with exacerbation, 8.5 points.59 The MID values based on distribution methods (0.5 standard deviation of mean change in scores or 1 standard error of the mean for baseline scores) showed similar results for the stable patients (MID 6.2 and 6.1) and those with an exacerbation (9.6 and 10.1).59 Another study estimated the MID for the CFQ-R respiratory scale based on longitudinal data from 12 CF patients with moderate to severe pulmonary disease who were followed for 1 year. Using distribution-based methods, the MID estimates ranged from 6.0 to 8.4 points (mean 7.3) in this pilot study.106
The main limitations of the CFQ-R are ceiling effects for certain scales (notably the eating and weight scale for the CFQ-14, eating, digestion, and body image for CFQ-C; and eating, weight, body image, and school functioning for CFQ-P), potential difficulty for patients to understand some of the items (e.g., CFQ-R respiratory, item “trouble breathing”), and concerns that a patient may not be able to distinguish between some of the response items on the scale (e.g., response choices such as “somewhat” versus “a little”).56,107
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
BSC
best supportive care
CF
cystic fibrosis
CFTR
cystic fibrosis transmembrane conductance regulator
ELX
elexacaftor
F/F
genotype homozygous for F508del mutation
F/G
genotype heterozygous for F508del mutation with a gating mutation
F/MF
genotype heterozygous for F508del mutation with 1 minimal function mutation
F/RF
genotype heterozygous for F508del mutation with a residual function mutation
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
IVA
ivacaftor
LUM
lumacaftor
MF
minimal function
ppFEV1
percent predicted forced expiratory volume in 1 second
QALY
quality-adjusted life-year
RF
residual function
TEZ
tezacaftor
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | ELX-TEZ-IVA (Trikafta); ELX 100 mg, TEZ 50 mg, IVA 75 mg (combination tablet), and IVA 150 mg (tablet) |
Submitted price | ELX-TEZ-IVA (Trikafta),100 mg/50 mg/75 mg and 150 mg tablets: $840 per daily dose |
Indication | For the treatment of CF in patients aged ≥ 12 years who have at least 1 F508del mutation in the CFTR gene |
Health Canada approval status | Approved (NOC); submitted to CADTH pre-NOC |
Health Canada review pathway | Priority review |
NOC date | June 18, 2021 |
Reimbursement request | As per indication |
Sponsor | Vertex Pharmaceuticals (Canada) Incorporated |
Submission history | Previously reviewed: Yes (IVA monotherapy) Indication: CF, R117H CFTR gating mutation Recommendation date: November 19, 2015 Recommendation: List with criteria/condition, including a substantial reduction in price |
CF = cystic fibrosis; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; IVA = ivacaftor; NOC = Notice of Compliance; TEZ = tezacaftor.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Microsimulation |
Target population | Patients with CF aged ≥ 12 years who have at least 1 F508del mutation in the CFTR gene, represented by the following 4 genotypes considered in separate analyses:
|
Treatment | ELX-TEZ-IVA, with BSC |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (approximately 65 years) |
Key data sources |
|
Submitted results | 1. Homozygous for F508del-CFTR (F/F): ICER vs. BSC = $358,763 per QALY (incremental costs: $4,638,324; incremental QALYs: 12.93) 2. Heterozygous for F508del-CFTR with an MF mutation (F/MF): ICER vs. BSC = $358,597 per QALY (incremental costs: $4,526,116; incremental QALYs: 12.59) 3. Heterozygous for F508del-CFTR with an RF mutation (F/RF): ICER vs. BSC = $531,195 per QALY (incremental costs: $3,782,240; incremental QALYs: 7.12) 4. Heterozygous for F508del-CFTR with a gating mutation (F/G), inclusive of R117H
|
Key limitations |
|
CADTH reanalysis results | CADTH conducted reanalyses which included the removal of an additional benefit of ELX-TEZ-IVA on the long-term rate of decline in ppFEV1 and pulmonary exacerbations; the removal of dynamic pricing of ELX-TEZ-IVA; the inclusion of costs for ELX-TEZ-IVA in the period for which it achieved a survival benefit in comparison with BSC; the removal of an adjustment to drug acquisition costs by patient compliance; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. 1. Homozygous for F508del-CFTR (F/F): ICER vs. BSC = $1,140,840 per QALY 2. Heterozygous for F508del-CFTR with an MF mutation (F/MF): ICER vs. BSC = $1,150,105 per QALY 3. Heterozygous for F508del-CFTR with an RF mutation (F/RF): ICER vs. BSC = $1,911,977 per QALY 4. Heterozygous for F508del-CFTR with a gating mutation (F/G), inclusive of R117H
ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH. A price reduction in excess of 90% for ELX-TEZ-IVA is required for all 4 genotypes in order for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC. |
BSC = best supportive care; CF = cystic fibrosis; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; IVA = ivacaftor; LY = life-year; MF = minimal function; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Conclusions
The clinical evidence submitted by the sponsor demonstrated that elexacaftor 100 mg, tezacaftor 50 mg, ivacaftor 75 mg, and ivacaftor 150 mg (ELX-TEZ-IVA) led to statistically and clinically significant improvements in acute percent predicted forced expiratory volume in 1 second (ppFEV1), weight-for-age z score, and pulmonary exacerbation rates. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| are associated with uncertainty due to key differences in the designs of included trials. There was no evidence on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1, or pulmonary exacerbation rates beyond the trial period for any genotype.
CADTH identified several major limitations with the submitted economic evaluation, the following were addressed in reanalyses: the removal of an additional benefit of ELX-TEZ-IVA on the long-term rate of decline in ppFEV1 and pulmonary exacerbations; the removal of dynamic pricing of ELX-TEZ-IVA; the inclusion of costs for ELX-TEZ-IVA in the period for which it achieved a survival benefit in comparison with best supportive care (BSC); the removal of an adjustment to drug acquisition costs by patient compliance; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. In the CADTH base case, in comparison with BSC, the incremental cost-effectiveness ratio (ICER) for ELX-TEZ-IVA is: $1,140,840 per quality-adjusted life-year (QALY) in the genotype homozygous for the F508del mutation (F/F); $1,150,105 per QALY in the genotype heterozygous for the F508del mutation with 1 minimal function mutation (F/MF); and $1,911,977 per QALY in the genotype heterozygous for the F508del mutation with a residual function mutation (F/RF). For the genotype heterozygous for the F508del mutation with a gating mutation (F/G), ELX-TEZ-IVA is associated with an ICER of $1,067,215 when compared with BSC, while a pairwise ICER of $181,718 per QALY was estimated in comparison with IVA monotherapy.
The key drivers in the analyses are drug acquisition costs and assumptions on the long-term benefits with ELX-TEZ-IVA which were uncertain. ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH. A price reduction in excess of 90% for ELX-TEZ-IVA is required for all 4 genotypes in order for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process and, specifically, information that pertains to the economic submission.
Three separate patient input submissions were received from Cystic Fibrosis Canada, CF Get Loud, and the Canadian Cystic Fibrosis Treatment Society. Information was gathered via a cystic fibrosis (CF) community townhall and letter campaign, survey, and one-on-one and group discussions, respectively, from Canadian patients, caregivers, and treating physicians. Patient input noted how burdensome CF is, on both patients living with the disease, as well as their caregivers. Many patients currently only receive treatment for the management of symptoms. The first priority of treatment was noted to be a reduction or stop in lung function decline, as well as an increase in lung function and reduction in pulmonary exacerbations. These all would serve to increase patient quality of life, reduce disease burden, and increase life expectancy. Patients with experience with ELX-TEZ-IVA have noted that their condition has significantly improved, targeting the cause of their symptoms, rather than the symptoms themselves, with limited side effects.
Clinician group input was received from Cystic Fibrosis Canada’s Accelerating Clinical Trials Network Executive Committee, the Toronto Adult CF Clinic, and the Canadian Cystic Fibrosis Clinic Directors. The clinicians noted that since 2010, cystic fibrosis transmembrane conductance regulator (CFTR) modulators have been developed to treat the underlying defect of CF, but that currently only 4% of Canadians have the “gating” mutation which IVA monotherapy is effective on, and that the other CFTR modulator therapies are not funded publicly; thus many patients remain untreated and currently receive supportive care that does not treat the root cause of CF. The clinicians indicated that ELX-TEZ-IVA would be a highly impactful treatment, and that given its indication includes patients who have only 1 copy of the F508del mutation in addition to 2 copies, it could impact nearly 90% of patients with CF in Canada, and it would become the standard of care in the indicated population in place of existing CFTR modulators and supportive therapy. Experts noted that the greater unmet need was in patients with the minimal function mutation or homozygous for the F508del mutation due to a lack of available CFTR options. There was uncertainty about whether the use of ELX-TEZ-IVA would result in lower BSC use. Clinician input also noted that patients on CFTR modulator therapies may still have benefits from therapy even after lung transplantation.
Drug plan input noted concerns over the likely high budgetary impact of ELX-TEZ-IVA and the need for a sense of the price reduction required for ELX-TEZ-IVA to be considered cost-effective.
Several of these concerns were addressed in the sponsor’s model.
IVA was included as a comparator for patients with a gating or R117H mutation, whereas BSC was included as a comparator for all other treatment options.
The sponsor’s model considered the impact of treatment on acute lung function, the long-term rate of decline in lung function, and pulmonary exacerbations.
BSC was included in addition to CFTR modulator therapy, up until the point at which patients on BSC alone died. After this point, no disease management costs were incurred.
In addition, CADTH addressed some of these concerns as follows.
CADTH included disease management costs while on CFTR modulators for the entire time horizon.
CADTH tested the impact of CFTR modulators on inpatient hospitalization and pharmacotherapy costs.
CADTH was unable to address the following concerns raised from stakeholder input.
CADTH could not consider the costs of CFTR modulator therapy after lung transplantation.
Economic Review
The current review is for ELX-TEZ-IVA for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing ELX-TEZ-IVA in combination with BSC for the treatment of CF in patients aged 12 years and older who have at least 1 F508del mutation in the CFTR gene, represented by the following 4 genotypes:
homozygous for F508del-CFTR (F/F)
heterozygous for F508del-CFTR with a minimal function (MF) mutation (F/MF)
heterozygous for F508del-CFTR with a residual function (RF) mutation (F/RF)
heterozygous for F508del-CFTR with a gating mutation (F/G), inclusive of R117H
The sponsor compared the submitted drug regimen with BSC alone in all 4 subgroups, as well as IVA monotherapy in the subgroup of patients with an F/G genotype.1 The modelled population is aligned with the approved Health Canada indication and funding request.
The recommended dose of ELX-TEZ-IVA is 2 tablets of ELX 100 mg, TEZ 50 mg, and IVA 75 mg taken in the morning and 1 tablet of IVA 150 mg taken in the evening, approximately 12 hours apart, with fat containing food.2 Both ELX 100 mg, TEZ 50 mg, and IVA 75 mg and IVA 150 mg cost $280.00 per tablet, for a daily cost of treatment of $840.00 and an annual cost of $306,600 per patient. BSC alone consisted of recommended medications (such as mucolytics, inhaled and oral antibiotics, inhaled hypertonic saline, nutritional supplements, enteral tube feeding, pancreatic enzymes, antifungal agents, and corticosteroids) and physiotherapy. The daily per patient cost associated with IVA monotherapy was $840.00, or an annual cost of $306,600, based on its list price. All patients on CFTR modulator therapies also received BSC. The costs associated with ELX-TEZ-IVA and IVA monotherapy were adjusted for compliance in the sponsor’s submission.1
The clinical outcomes predicted by the model were QALYs and life-years. The economic analysis was undertaken over a lifetime time horizon (approximately 65 years) from the perspective of the public health care payer. Discounting (1.5% per annum) was applied to both costs and outcomes.1
Model Structure
The sponsor conducted a patient-level simulation model (i.e., microsimulation), with a typical patient profile for each genotype informed by various CFTR modulator trials.1 The patient profile was run through the model to project a patient’s CF disease progression and associated life expectancy, costs, and utilities (Figure 1). In the sponsor’s base case, the average patient profile was run 250 times, and the expected costs and clinical effects of ELX-TEZ-IVA, BSC, and IVA (for the F/G, inclusive of R117H genotype only) were calculated. This process was repeated 200 times, for each genotype. During each cycle for a given patient profile, the hypothetical average patient was at risk of various clinical events associated with costs, mortality, and utility values. At the beginning of each cycle, the model would calculate a patient’s mortality risk based on a Cox proportional hazards model which linked survival in CF to several risk factors.3 The following characteristics were included in the calculation of mortality risk: age, sex, ppFEV1, annual number of pulmonary exacerbations, prior respiratory infection status, CF-related diabetes, weight-for-age z score, and pancreatic sufficiency status. Age, ppFEV1, pulmonary exacerbation rate, and weight-for-age z score were updated with each cycle a patient remained alive, while the remaining characteristics remained static. If a patient remained alive, the model also tracked treatment discontinuation and lung transplant eligibility and occurrence. Treatment with a CFTR modulator was assumed to impact disease progression and mortality through effects relating to ppFEV1, weight-for-age score, and pulmonary exacerbation rates. During each cycle, patients would accrue life-years and QALYs, whereas costs were applied at the end of each run of 250 patients for efficiency gains.
Model Inputs
The baseline age-specific risk of death in the model was derived from a cohort study of the Canadian CF Registry by Stephen et al.4 The Kaplan–Meier data from this study was digitized and extrapolated using parametric survival analysis to generate mortality risk for the lifetime time horizon, with the Gompertz curve selected as the best fitting option. This baseline hazard was then adjusted using a Cox proportional hazard model developed by Liou et al.,3 which accounted for the patient characteristics noted in the model structure section above. The hazard of mortality in the model was assumed to be no lower than that of the general population of Canada.
The characteristics informing the mortality risk in the model were based on an average patient profile primarily generated from pooled mean baseline characteristics of CFTR modulator trials, and specific to each genotype. The trials informing the baseline characteristics of age, sex, ppFEV1 and weight-for-age z score included the trials for lumacaftor-ivacaftor (LUM-IVA), tezacaftor-ivacaftor (TEZ-IVA), and IVA monotherapy, in addition to the trials for ELX-TEZ-IVA, to have a larger sample size (Table 3). For the homozygous F/F genotype, data from the TRAFFIC, TRANSPORT (both using LUM-IVAand EVOLVE (TEZ-IVA trials were used.5,6 Data from Studies 103 and 109,7,8 ELX-TEZ-IVA trials, were excluded from informing baseline patient characteristics for the F/F genotype, as the patients in these trials were not treatment naive and thus were thought to not accurately reflect baseline patient profiles in the absence of treatment. Data from Study 102, an ELX-TEZ-IVA trial, was used to inform baseline characteristics for the heterozygous F/MF population.9 The heterozygous F/RF population’s baseline characteristics were informed by the EXPAND trial (TEZ-IVA),10 while the STRIVE and KONNECTION trials, both IVA monotherapy trials, informed the heterozygous F/G population.11,12 Study 104, an ELX-TEZ-IVA trial, was not used to inform the F/G and F/RF population’s baseline characteristics as this trial included patients with prior exposure to CFTR modulators at baseline.13 The baseline rate of pulmonary exacerbations requiring IV antibiotics and/or hospitalization was derived from Whiting et al.14 The rate of CF-related diabetes at baseline was based on a study of the Canadian CF Registry,1 and a patient’s status was assumed to not change over the entire time horizon.
Table 3: Baseline Characteristics Key Data Sources
Genotype | Source |
|---|---|
Homozygous for F508del-CFTR | TRAFFIC, TRANSPORT, and EVOLVE trials.5,6 Note: Studies 103 and 109 were excluded due to patients having prior CFTR modulator treatment exposure at baseline. |
Heterozygous for F508del-CFTR and 1 MF mutation | Study 102 |
Heterozygous for F508del-CFTR with an RF mutation | EXPAND10 Note: Study 104 was excluded due to patients having prior CFTR modulator treatment exposure at baseline. |
Heterozygous for F508del-CFTR with a gating mutation, inclusive of R117H | Note: Study 104 was excluded due to patients having prior CFTR modulator treatment exposure at baseline. |
CFTR = cystic fibrosis transmembrane conductance regulator; MF = minimal function; RF = residual function.
As noted above, ppFEV1, the annual number of pulmonary exacerbations, and weight-for-age z score could be affected by treatment, and were updated every cycle, along with age. All other characteristics remained constant from baseline. The treatment effects of CFTR modulators considered in the model were derived from the relevant phase III studies and open-label extensions. This included Study 102 for the heterozygous F/MF subgroup9; Study 103 and 109 for homozygous F/F genotype7,8; and Study 104 for both the heterozygous F/G and F/RF genotypes.13 As these trials predominantly compared ELX-TEZ-IVA to other CFTR modulators, except for Study 102 in the F/MF genotype. Multiple indirect treatment comparisons (ITCs) were necessary for the comparison to BSC for the other genotypes, as BSC is the current standard of care in 3 of the genotypes evaluated. The sponsor’s ITC employed the Bucher method, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |
Patients on BSC alone were expected to not have any acute increases in ppFEV1 and were assumed to have a long-term decline in ppFEV1 in line with a study by Leung et al.15 The same rate of decline was applied to all genotypes, except the heterozygous F/RF genotype, as they are typically thought to have a milder form of disease and thus a slower rate of decline. The reduction in rate of decline for patients receiving CFTR modulators was not available from the ITC or the sponsor’s trials assessing ELX-TEZ-IVA. The results of observational studies of the long-term impact of TEZ-IVA on long-term ppFEV1 were assumed to be applicable to ELX-TEZ-IVA. Patients receiving BSC alone were assumed to have no change in weight-for-age z score, whereas patients receiving CFTR modulators had a placebo-adjusted mean change from baseline weight-for-age z score derived from the ITC as noted above.1
The baseline rate of occurrence of pulmonary exacerbations for each cycle was based on the patient’s ppFEV1 and age, according to a formula derived by Goss et al.16 and was not genotype specific. This rate was applied as derived by Goss et al. to patients receiving BSC alone, while the rate for patients on CFTR modulators, including ELX-TEZ-IVA, was adjusted by a rate ratio derived by the sponsor. This was based on an assumed additional treatment impact on pulmonary exacerbations beyond those explained by the improvements in ppFEV1 in CFTR modulator-treated patients captured in the Goss et al. formula. The sponsor attempted to calibrate the pulmonary exacerbation rate ratio for patients on a CFTR modulator observed in the trials compared with that of a patient receiving BSC alone to account for the potential double counting of the benefit due to the better ppFEV1 observed with CFTR modulators. This was done for rates over a 2-year period and assumed to apply to the entirety of the time horizon, with the option to apply different rates for the period for which there was observed data and for the period for which there was no observed data.
The sponsor’s model also accounted for treatment discontinuation and compliance. Discontinuation rates for the model period corresponding to the trial duration period were obtained from the phase III trials for ELX-TEZ-IVA and IVA monotherapy, whereas open-label extension studies were used to inform a “post-acute” phase of the model up to an additional 96 weeks in length, after which no patients discontinued treatment in the model.7-9,13 If a patient discontinued a CFTR, they no longer received the impact of treatment on lung function decline or pulmonary exacerbation rate, but did maintain their acute increase in ppFEV1. The sponsor also used compliance rates from the trials to inform treatment costs in the acute period (first 24 weeks), which were genotype specific, and a study by Suthoff et al.,17 which was not genotype specific, to inform treatment compliance beyond the period for which there was trial data. Compliance was assumed to have no impact on treatment efficacy, and only affected the costs associated with CFTR modulators. The rate of lung transplantation was derived by the sponsor, and a separate mortality risk for patients following a lung transplant was applied based on a study in the literature.18 Neither were genotype specific. Adverse events in the model were based on the relevant phase III trials for the respective genotypes.
In the absence of utilities based on a generic instrument (e.g., the EuroQol 5-Dimensions questionnaire), the sponsor used an equation developed by Solem et al. that included ppFEV1 and pulmonary exacerbations as predictors of an EuroQol 5-Dimensions questionnaire index utility score. For this calculation, each pulmonary exacerbation was assumed to last 21.7 days, based on the TRAFFIC and TRANSPORT trials.19 The sponsor also included a treatment-specific utility increment for patients receiving ELX-TEZ-IVA, as it was felt that the equation by Solem et al. did not capture the impact of treatment on non-respiratory outcomes. This was not applied to patients receiving IVA monotherapy. The utility for a patient post-lung transplant was obtained from a study by Whiting et al.14 No disutilities related to adverse events were included in the model, as they were assumed to have minimal impact on patient quality of life.
Costs considered in the model included drug acquisition, monitoring, disease management, lung transplantation, and adverse event costs. The cost of ELX-TEZ-IVA was submitted by the sponsor, whereas the price of IVA monotherapy was based on the available list price from the Ontario exceptional access program formulary.20 For these medications, the sponsor employed a dynamic pricing approach, whereby the introduction of a first generic into the market after loss of patent exclusivity would lead to a 25% reduction in the prices of ELX-TEZ-IVA and IVA, followed by a second generic entry further reducing their prices by 50%. These assumptions were based on a pan-Canadian Pharmaceutical Alliance office framework for pricing expectations upon generic entry.21 Additional costs associated with CFTR modulator use included monitoring costs consisting of liver function tests and ophthalmologist visits, as per their product monographs, with the costs obtained from the Ontario Schedule of Benefits.22,23
Routine medical care associated with CF was also included in the model, consisting of clinician visits, hospitalizations, infection prevention, and management of comorbidities. Such costs were applied in the model by disease severity, which were defined based on ppFEV1 thresholds, and further divided into pulmonary exacerbation and non-pulmonary exacerbation-related costs. A sponsor-commissioned burden of illness study, consisting of a chart review, was used to inform the health care resource use associated with the routine disease management costs,1 and further supplemented by data from the 2014 Canadian CF Registry.1 Costs related to physician and laboratory services were obtained from the Ontario Schedule of Benefits, while hospitalization costs were derived from a study by Skolnik et al.24 The sponsor further adjusted the disease management costs specific to inpatient visits and pharmacotherapy for patients on CFTR modulators, based on studies in the literature which indicated a reduction in CF-related inpatient admissions and outpatient IV and antibiotic use.25,26 As a result, differential annual inpatient costs and annual pharmacotherapy costs were estimated for patients on BSC alone and CFTR modulators. The sponsor also excluded disease management costs for patients on CFTR modulators after the similar patient on BSC had died in a given simulation, while only incurring CFTR modulator therapy costs for the remainder of the time horizon.
The sponsor assumed 13.2% of patients with a ppFEV1 less than 40% would receive a lung transplant. Lung transplantation costs were obtained from Alberta Health Services, with follow-up costs obtained from the literature.27,28 The cost of each adverse event was assumed to be equal to the cost of a single general practitioner assessment.22
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically with 250 average patients individually simulated for 200 iterations for the base case and scenario analyses. The deterministic and probabilistic results were similar. The probabilistic findings are presented below. The sponsor’s base case is based on publicly available list prices for comparators (i.e., IVA).
Base-Case Results
The sponsor presented their results by genotype. For the F/F genotype, ELX-TEZ-IVA was associated with incremental costs of $4,638,324 and QALYs of 12.93 when compared with BSC, for an ICER of $358,763 per QALY. Similar results were observed in the F/MF genotype. In the F/RF genotype, fewer incremental costs ($3,782,240) and fewer incremental QALYs (7.12) were observed with ELX-TEZ-IVA, for an ICER of $531,195 per QALY compared with BSC. For the F/G genotype, ELX-TEZ-IVA was associated with an ICER of $353,239 per QALY when compared with BSC. A pairwise ICER of $256,956 per QALY was estimated in comparison with IVA monotherapy, though when considered sequentially, IVA monotherapy was extendedly dominated. The full results of the sponsor’s base case are presented in Table 4.
The sponsor also presented an ICER versus BSC for all genotypes combined, weighted by their prevalence. The overall weighted ICER was $366,677 per QALY.
Table 4: Summary of the Sponsor’s Economic Evaluation Results by Genotype
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|---|---|
Homozygous for F508del-CFTR (F/F) | |||||||
BSC | 1,335,292 | Ref | 20.50 | Ref | 18.18 | Ref | Ref |
ELX-TEZ-IVA | 5,973,616 | 4,638,324 | 32.39 | 11.89 | 31.11 | 12.93 | 358,763 |
Heterozygous for F508del-CFTR with 1 minimal function mutation (F/MF) | |||||||
BSC | 1,311,789 | Ref | 20.48 | Ref | 18.20 | Ref | Ref |
ELX-TEZ-IVA | 5,837,906 | 4,526,116 | 30.79 | 11.61 | 30.79 | 12.59 | 359,597 |
Heterozygous for F508del-CFTR with a residual function mutation (F/RF) | |||||||
BSC | 1,166,549 | Ref | 20.35 | Ref | 18.35 | Ref | Ref |
ELX-TEZ-IVA | 4,948,789 | 3,782,240 | 26.58 | 6.22 | 25.47 | 7.12 | 531,195 |
Heterozygous for F508del-CFTR with a gating mutation (F/G) | |||||||
BSC | 1,254,845 | Ref | 21.09 | Ref | 18.90 | Ref | Ref |
ELX-TEZ-IVA | 5,439,607 | 4,184,761 | 32.14 | 11.05 | 30.75 | 11.85 | 353,239 |
IVA | 4,357,458 | Ref | 29.11 | Ref | 26.53 | Ref | Ref |
ELX-TEZ-IVA | 5,439,607 | 1,082,149 | 32.14 | 3.02 | 30.75 | 4.21 | 256,956 |
BSC = best supportive care; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; QALY = quality-adjusted life-year; Ref = reference; TEZ = tezacaftor.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted 2 scenario analyses probabilistically. The scenario of note was the use of static pricing for ELX-TEZ-IVA and IVA monotherapy, instead of the sponsor’s base-case assumption of dynamic pricing resulting in price reductions for CFTR modulator therapies at the end of patent exclusivity. This scenario led to increases in the ICERs for ELX-TEZ-IVA when compared with BSC above $500,000 per QALY gained in all genotypes, and a weighted ICER of $513,088 per QALY. The ICER in comparison to IVA monotherapy in the F/G genotype decreased to $74,416 per QALY.
The sponsor also conducted several deterministic sensitivity analyses, assessing alternative assumptions and inputs on model results. The parameters with the greatest impact on model results were post-trial compliance with ELX-TEZ-IVA, as well as altering the impact of ELX-TEZ-IVA on ppFEV1 decline and pulmonary exacerbations.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
The long-term impact of treatment with ELX-TEZ-IVA on ppFEV1 is uncertain. In addition to an acute increase in ppFEV1 from treatment with ELX-TEZ-IVA or IVA, the sponsor also assumed that treatment with a CFTR modulator would slow the rate of decline of ppFEV1 when compared with the rate of decline with patients not receiving disease modifying treatment. In the absence of available data with ELX-TEZ-IVA in support of this assumption, the sponsor assumed that evidence from TEZ-IVA would be applicable, given its 2 components are part of the ELX-TEZ-IVA formulation. Due to the absence of data specific to ELX-TEZ-IVA in support of a slowing of the rate of lung function decline, this assumption is highly uncertain. Additionally, the relative reduction in the rate of decline in ppFEV1 with TEZ-IVA used to inform the value for ELX-TEZ-IVA was based on a retrospective analysis and may not have accounted for all confounders, as the analysis could only adjust for variables captured in the registry used to conduct the analysis. Additionally, the analysis was based on only 96 weeks of data, yet the reduction in rate of decline was applied for the entire model time horizon, meaning there is no long-term evidence in support of this assumption for TEZ-IVA, let alone ELX-TEZ-IVA. The sponsor’s model was not flexible enough to change this relative rate reduction over time. Overall, these issues lead to uncertainty with the benefit of ELX-TEZ-IVA on long-term ppFEV1, leading to a potential overestimation of the total QALYs and potential underestimation of the costs associated with ELX-TEZ-IVA in the sponsor’s base case.
CADTH removed the long-term relative reduction in the rate of ppFEV1 decline for both ELX-TEZ-IVA and IVA in the CADTH base case.
The assumption of an impact of CFTR modulator therapy on the pulmonary exacerbation rate beyond its impact mediated by improvements in ppFEV1 is highly uncertain. The sponsor used a relationship identified in the literature to determine the baseline pulmonary exacerbation rate according to ppFEV1 and age. The sponsor determined that their model initially produced an overestimation of the rate of pulmonary exacerbations with ELX-TEZ-IVA using this relationship alone when compared with BSC in comparison with the relative risk of pulmonary exacerbations from the pivotal trial, Study 102. The sponsor calibrated the first 2 years of pulmonary exacerbation rates in the model with the values from the trial to determine an additional relative reduction in pulmonary exacerbations with ELX-TEZ-IVA beyond its impact mediated by changes in ppFEV1. While there is some plausibility to this assumption according to the clinical experts consulted by CADTH, there is uncertainty as to how long this additional benefit would be observed. The sponsor assumed this additional impact on pulmonary exacerbations would be applicable for the entire modelled time horizon, despite only having data for up to 48 weeks. This potentially underestimates the number of pulmonary exacerbations and overestimates total QALYs and underestimates costs in favour of ELX-TEZ-IVA in comparison with BSC.
CADTH removed the additional reduction in pulmonary exacerbations beyond the impact mediated by ppFEV1 in its reanalysis for both ELX-TEZ-IVA and IVA in the period for which there was no observed data.
The magnitude of benefit with ELX-TEZ-IVA on acute increases in ppFEV1 and weight-for-age z score is uncertain. BSC was a comparator of interest in all 4 subgroups, but the pivotal studies assessing the clinical efficacy of ELX-TEZ-IVA for 3 of the 4 genotypes included an active comparator and not BSC alone, meaning there was no direct head-to-head evidence in comparison with BSC for these genotypes. The sponsor derived placebo-adjusted estimates of acute increases in ppFEV1 and weight-for-age z score via 3 ITCs for the F/RF, F/G, and F/F genotypes. The CADTH clinical review noted that patients received a 4-week run-in period with an active agent in the ELX-TEZ-IVA studies, whereas none of the other trials included in the indirect comparisons had a similar run-in period. This led to key differences among the included trials, as the study designs, baseline values, and the end point values for the common comparator were different. There is the potential that these differences may introduce bias into the ITC analysis. The direction and magnitude of bias is uncertain, and applies not only to the comparison with BSC for all 3 of the relevant genotypes (i.e., F/F, F/RF, and F/G), but the comparison with IVA in the F/G genotypes as well.
CADTH could not address this limitation in reanalyses.
The dynamic pricing for CFTR modulator therapies is uncertain and underestimates drug acquisition costs with ELX-TEZ-IVA. In their submitted base case, the sponsor employed a dynamic pricing approach for ELX-TEZ-IVA. Following the loss of patent exclusivity, generics were assumed to be introduced, leading to a 25% reduction in the price of ELX-TEZ-IVA with the first generic, followed by a 50% reduction in price with the introduction of a second generic after 19 and 20 years in the model time horizon, respectively. Similar assumptions were included for IVA. While price reductions arising from the availability of generic entrants is possible, there is tremendous uncertainty as to if and when price reductions for ELX-TEZ-IVA would occur. Patents are frequently extended (i.e., evergreened), leading to uncertainty with the exact timing of entry of a generic, and there is no guarantee on the number of generic entries in the market. CADTH guidance states that full costs for ELX-TEZ-IVA at its submitted price for the entire time horizon should be accounted for. In the sponsor’s base case, dynamic pricing reduces the total drug acquisition costs associated with ELX-TEZ-IVA, as well as with IVA monotherapy, biasing results in their favour.
CADTH disabled the dynamic pricing function in the CADTH reanalysis.
The compliance-adjusted drug costs underestimate the total costs associated with ELX-TEZ-IVA. The sponsor adjusted the price of ELX-TEZ-IVA by the assumed compliance rate (80%) in the “post-acute” period of the model (i.e., the period for which there was no observed data), with the assumption that savings would be incurred by the health care system based on a lack of compliance. There is limited evidence to support the real-world compliance rate with ELX-TEZ-IVA, and the sponsor did not adjust treatment efficacy in the model to align accordingly. Additionally, ELX-TEZ-IVA would be dispensed, regardless of whether the patients were compliant, thus resulting in the full drug acquisition costs to the public health care payer. This adjustment resulted in an underestimation of the drug acquisition costs associated with ELX-TEZ-IVA, biasing results in its favour in comparison with BSC.
CADTH assumed patients were 100% compliant in reanalyses to ensure all drug acquisition costs were accounted for.
The exclusion of health care costs in the period over which there is a gain in survival leads to an underestimation of the costs associated with ELX-TEZ-IVA. The sponsor failed to consider costs associated with CF care for patients on CFTR modulators after the similar patient on BSC had died, that is, only considering CFTR modulator therapy costs for the remainder of the time horizon. This assumption was made based on the sponsor asserting that accounting for the costs borne by the health care system for the additional period of survival associated with ELX-TEZ-IVA does not align with how society values treatment. This exclusion of costs incurred by the health care system does not reflect the public health care payer perspective. This assumption led to an underestimation of the total costs associated with ELX-TEZ-IVA.
CADTH included all costs relevant to the public health care payer in the additional survival period for patients on ELX-TEZ-IVA or IVA in the CADTH base case.
The impact of ELX-TEZ-IVA on health care resource use beyond its impact mediated through improving lung function is uncertain. Health state costs in the sponsor’s submitted model were primarily based on ppFEV1, with greater costs for patients with a worse ppFEV1. The sponsor included costs associated with inpatient and outpatient hospitalizations, routine antibiotics, and diagnostics. The sponsor further adjusted the disease management costs specific to inpatient hospital visits and pharmacotherapy for patients on CFTR modulators, based on studies in the literature which indicated a reduction in CF-related inpatient admissions and outpatient IV and antibiotic use.25,26 As a result, differential annual inpatient costs and annual pharmacotherapy costs were estimated for patients on BSC alone and CFTR modulators. The clinical experts consulted by CADTH indicated there was some plausibility for this assumption, potentially mediated through other factors such as nutritional status, but the magnitude of the impact of factors outside of ppFEV1 not accounted for by ppFEV1 remained uncertain. Upon review of the sponsor’s sources for the reductions in costs associated with inpatient hospital visits and pharmacotherapy, CADTH noted that the studies cited by the sponsor were observational before and after studies, assessing the impact of CFTR modulator use on relevant costs. These studies did not indicate whether they controlled for patient ppFEV1, or any other factors for that matter. As a result, it is difficult to determine whether the magnitude of difference in costs before and after CFTR modulator use observed in these studies was due to ppFEV1, which is already factored into the sponsor’s submitted model via treatment efficacy, or another factor as asserted by the sponsor. The sponsor’s approach likely underestimates the inpatient hospital visit and outpatient antibiotic use costs associated with CFTR modulator use, biasing results in favour of ELX-TEZ-IVA.
CADTH assumed inpatient hospital costs and annual pharmacotherapy costs were the same for all patients in the model with a similar ppFEV1, regardless of whether they were receiving a CFTR modulator.
Treatment-specific utility increment for patients on ELX-TEZ-IVA leads to potential overestimation of total benefit. The sponsor based utility values in the submitted model on an equation by Solem et al.,19 which determines a utility based on the EuroQol 5-Dimensions questionnaire according to a patient’s ppFEV1 and whether they experienced a pulmonary exacerbation. The sponsor included an additional utility increment for patients on ELX-TEZ-IVA based on an analysis comparing the utility scores, according to the Cystic Fibrosis Questionnaire–Revised (8 Dimensions), of patients on ELX-TEZ-IVA versus those on placebo in the relevant ELX-TEZ-IVA trials, adjusting for ppFEV1. Based on this analysis, there was a difference in utility score for patients on ELX-TEZ-IVA in comparison with BSC not explained by ppFEV1. The sponsor’s analysis comparing Cystic Fibrosis Questionnaire–Revised (8 Dimensions) scores from the trials did not account for pulmonary exacerbation rates, which are already included in the sponsor’s utility estimate, meaning the difference observed in the sponsor’s analysis may be explained by pulmonary exacerbations. It is difficult to know what proportion of the difference in utility score from the trial is attributable to pulmonary exacerbations, though pulmonary exacerbations were accounted for in the equation by Solem et al. The sponsor should have explicitly modelled the other events they felt contribute to quality of life not captured by Solem et al. to allow for greater transparency in understanding what contributes to the quality of life estimates and to what extent. The inclusion of a treatment-specific utility increment for patients on ELX-TEZ-IVA potentially leads to double counting of utility gains with ELX-TEZ-IVA, likely biasing results in favour of ELX-TEZ-IVA.
CADTH removed the treatment-specific utility increment with ELX-TEZ-IVA in the CADTH base-case analysis.
The sponsor’s model lacked transparency and its programming prevented CADTH from fully exploring the uncertainty with the submitted model. The submitted model was programmed with limited transparency. CADTH was unable to fully explore the uncertainty with parameters in the model. Additionally, key changes to the sponsor’s inputs produced results that lacked face validity, indicating issues with the model’s mechanics.
CADTH could not address this limitation in reanalyses. CADTH conducted a stepwise analysis of the base case which produced results that lacked face validity, yet this change did not appear to lead to issues when incorporated in the CADTH base case.
The ppFEV1 threshold for lung transplantation referral overestimates the proportion of patients receiving lung transplants. The sponsor assumed 13.2% of people with a ppFEV1 less than 40% receive a lung transplant. The proportion of patients receiving a transplant is likely appropriate, but the cut-off chosen does not align with clinical practice. Clinical experts consulted by CADTH for this review indicated a ppFEV1 of 30% as the threshold to initiate a lung transplant referral. Given a larger number of patients on BSC and IVA monotherapy were likely to have a ppFEV1 close to the lung transplant threshold, the use of a higher cut-off likely led to a greater number of patients on BSC and IVA incurring the costs associated with a lung transplantation, biasing results in favour of ELX-TEZ-IVA.
CADTH set the lung transplant threshold to a ppFEV1 of 30% in the CADTH base case.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation (not noted as limitations to the submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Mortality with CF is assumed to be no lower than that of the general population | Appropriate |
Pancreatic insufficiency, prior respiratory infection, and CF-related diabetes status were assumed to remain unchanged from baseline over time | Appropriate |
Long-term rate of decline in ppFEV1 for patients with the homozygous F/F genotype is applicable to the heterozygous minimal function (F/MF) and gating (F/G) genotypes | This is likely to be appropriate, though there is some uncertainty associated with this assumption |
Rates of long-term decline in ppFEV1 for the heterozygous with residual function (F/RF) genotype were assumed to be similar to that of the mild disease group in Leung et al. (2020)15 | Appropriate |
Patients would not discontinue therapy after the initial 120 weeks on therapy | Appropriate |
All adverse events observed in the model would only incur a physician visit and would not require any additional treatment or affect patient quality of life. | Appropriate; the only adverse event observed with ELX-TEZ-IVA which may incur additional costs is liver function test abnormalities, which may require additional laboratory work, which is likely already captured in routine management costs |
CF = cystic fibrosis; ELX = elexacaftor; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CADTH undertook a stepped analysis, incorporating each change detailed in Table 6 into the sponsor’s model to highlight the impact of each change. Each genotype is presented separately. The summary results of the CADTH reanalyses for the F/F genotype are presented in Table 7. The results for the F/MF, F/RF, and F/G genotypes are presented in Appendix 4.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Reduction in rate of ppFEV1 decline compared with BSC | 61.5% with ELX-TEZ-IVA, 47.1% with IVA | No reduction in rate of decline of ppFEV1 |
2. Pulmonary exacerbation rate ratio with ELX-TEZ-IVA vs. BSC after acute period | ELX-TEZ-IVA: 0.31 IVA: 0.72 | ELX-TEZ-IVA: 1.0 IVA: 1.0 |
3. Dynamic pricing of ELX-TEZ-IVA and IVA | 25% price reduction after 19 years for ELX-TEZ-IVA and 5 years for IVA 50% price reduction after 20 years for ELX-TEZ-IVA and 6 years for IVA | No price reduction over entire time horizon |
4. Disease management costs in period of survival benefit while on ELX-TEZ-IVA | Not included | Included |
5. Patient compliance rate | 80% after acute period | 100% after acute period |
6. Impact of ELX-TEZ-IVA on hospital and inpatient visit costs beyond impact on lung function | Annual inpatient costs:
Annual pharmacotherapy costs:
| Annual inpatient costs:
Annual pharmacotherapy costs:
|
7. Treatment-specific utility associated with ELX-TEZ-IVA | Included additional utility increment of 0.0785 while on ELX-TEZ-IVA | No utility increment for ELX-TEZ-IVA use |
8. Lung transplant referral cut-off | ppFEV1 of ≤ 40% | ppFEV1 of ≤ 30% |
CADTH base case | 1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 | |
BSC = best supportive care; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; TEZ = tezacaftor; vs. = versus.
For the F/F genotype, ELX-TEZ-IVA was associated with incremental costs of $8,171,598 and QALYs of 7.13 when compared with BSC, for an ICER of $1,140,840 per QALY. Similar results were observed in the F/MF genotype. In the heterozygous F/RF genotype, incremental costs ($6,412,761) and incremental QALYs (3.35) were observed with ELX-TEZ-IVA, for an ICER of $1,911,977 per QALY compared with BSC. For the F/G genotype, ELX-TEZ-IVA was associated with an ICER of $1,067,215 when compared with BSC. A pairwise ICER of $181,718 per QALY was estimated in comparison with IVA monotherapy, although when considered sequentially, IVA monotherapy was extendedly dominated. The comparison with IVA is based on the publicly available price of IVA. The full results of the CADTH base case are presented in Table 8 and example disaggregate results all genotypes are available in Appendix 4.
The sponsor’s model also produced an ICER versus BSC for all genotypes combined, weighted by their prevalence. The weighted ICER was $1,158,851 per QALY. The changes to the sponsor’s base case with the greatest impact were the removal of dynamic pricing from the introduction of generic options and removing the assumption that drug costs should be adjusted by patient compliance. This further emphasizes the impact of drug acquisition costs as a key driver in the model.
Table 7: Summary of the Stepped Analysis of the CADTH Reanalysis Results—F/F Genotype
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 1,335,292 | 18.18 | Ref |
ELX-TEZ-IVA | 5,973,616 | 31.11 | 358,763 | |
CADTH reanalysis 1 | BSCa | 1,527,886 | 21.92b | Ref |
ELX-TEZ-IVA | 5,503,973 | 28.68 | 588,343 | |
CADTH reanalysis 2 | BSCa | 1,345,172 | 18.25 | Ref |
ELX-TEZ-IVA | 6,026,427 | 30.23 | 390,692 | |
CADTH reanalysis 3 | BSCa | 1,343,452 | 18.26 | Ref |
ELX-TEZ-IVA | 7,923,922 | 31.06 | 514,071 | |
CADTH reanalysis 4 | BSCa | 1,335,292 | 18.18 | Ref |
ELX-TEZ-IVA | 6,218,915 | 31.11 | 377,736 | |
CADTH reanalysis 5 | BSCa | 1,323,954 | 18.32 | Ref |
ELX-TEZ-IVA | 7,337,600 | 31.24 | 465,431 | |
CADTH reanalysis 6 | BSCa | 1,314,630 | 18.41 | Ref |
ELX-TEZ-IVA | 6,085,921 | 31.36 | 368,269 | |
CADTH reanalysis 7 | BSCa | 1,343,212 | 18.15 | Ref |
ELX-TEZ-IVA | 5,973,364 | 29.60 | 404,275 | |
CADTH reanalysis 8 | BSCa | 1,344,761 | 18.25 | Ref |
ELX-TEZ-IVA | 5,983,972 | 31.11 | 360,792 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) | BSCa | 1,353,297 | 18.36 | Ref |
ELX-TEZ-IVA | 9,524,895 | 25.52 | 1,140,840 |
BSC = best supportive care; ELX = elexacaftor; F/F = homozygous for F508del mutation; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aReference product is least costly alternative.
bSponsor’s model produced results which do not meet face validity.
Table 8: Summary of the CADTH Base-Case Results by Genotype
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY)a |
|---|---|---|---|---|---|
Homozygous for F508del-CFTR (F/F) | |||||
BSC | 1,353,297 | Ref | 18.36 | Ref | Ref |
ELX-TEZ-IVA | 9,524,895 | 8,171,598 | 25.52 | 7.16 | 1,140,840 |
Heterozygous for F508del-CFTR with 1 minimal function mutation (F/MF) | |||||
BSC | 1,327,598 | Ref | 18.33 | Ref | Ref |
ELX-TEZ-IVA | 9,244,232 | 7,916,634 | 25.22 | 6.88 | 1,150,105 |
Heterozygous for F508del-CFTR with a residual function mutation (F/RF) | |||||
BSC | 1,172,463 | Ref | 18.37 | Ref | Ref |
ELX-TEZ-IVA | 7,585,224 | 6,412,761 | 21.73 | 3.35 | 1,911,977 |
Heterozygous for F508del-CFTR with a gating mutation (F/G) | |||||
BSC | 1,265,862 | Ref | 18.99 | Ref | Ref |
ELX-TEZ-IVA | 8,544,374 | 7,728,512 | 25.81 | 6.82 | 1,067,215 |
IVA | 8,053,502 | Ref | 23.11 | Ref | Ref |
ELX-TEZ-IVA | 8,544,374 | 490,872 | 25.81 | 2.70 | 181,718 |
BSC = best supportive care; CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; Ref = reference; TEZ = tezacaftor.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
Price reduction analyses were conducted using both the sponsor and CADTH base case assuming proportional price reductions for ELX-TEZ-IVA. Table 9 includes the summary of price reductions and Appendix 4 for full price reduction analyses for all genotypes, including price reductions for the entire population combined weighted by prevalence, and in comparison with IVA for the F/G genotype. A price reduction in excess of 90% is required for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in comparison with BSC for all genotypes. The exact price reduction required varies by genotype but is smallest for the F/G genotype and greatest for the F/RF genotype.
Table 9: CADTH Price Reduction Analyses
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
Homozygous for F508del-CFTR (F/F) | ||
No price reduction | 358,763 | 1,140,840 |
90% | Dominant | 122,809 |
95% | Dominant | 63,617 |
99% | Dominant | 26,127 |
Heterozygous for F508del-CFTR with 1 minimal function mutation (F/MF) | ||
No price reduction | 359,597 | 1,150,105 |
90% | Dominant | 116,347 |
95% | Dominant | 59,734 |
99% | Dominant | 11,864 |
Heterozygous for F508del-CFTR with a residual function mutation (F/RF) | ||
No price reduction | 531,195 | 1,911,977 |
90% | Dominant | 163,565 |
95% | Dominant | 65,822 |
99% | Dominant | Dominant |
Heterozygous for F508del-CFTR with a gating mutation (F/G) | ||
No price reduction | 353,239 | 1,067,215 |
90% | Dominant | 85,764 |
95% | Dominant | 32,146 |
99% | Dominant | Dominant |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
CADTH also undertook a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of ELX-TEZ-IVA. This included:
A reduction in pulmonary exacerbations observed with ELX-TEZ-IVA or IVA based on observed trial data is assumed to apply in the period for which there is no available data for the entire time horizon, as per the sponsor’s base-case assumption.
The rates of ppFEV1 decline with ELX-TEZ-IVA or IVA are 61.5% and 41.7% slower, respectively, in comparison with BSC, as per the sponsor’s base-case assumption.
Treatment-specific utility increment from benefits beyond improvements in lung function and pulmonary exacerbations for patients on ELX-TEZ-IVA included, as per sponsor’s base-case assumption.
The results of the CADTH scenario analyses are available in Table 10 for the F/F genotype and Appendix 4 for the F/MF, F/RF, and F/G genotypes. Each of the scenarios highlight the impact of assuming additional benefit with ELX-TEZ-IVA, despite a lack of supporting evidence, and none produced an ICER less than $799,000 per QALY when compared with BSC. These scenario analyses are again driven by the high drug acquisition costs with ELX-TEZ-IVA, which offset the QALY gains.
Table 10: Summary of the CADTH Scenario Analyses—F/F Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Long-term reduction in pulmonary exacerbations included for ELX-TEZ-IVA | BSC | 1,342,715 | 18.42 | Ref |
ELX-TEZ-IVA | 9,508,335 | 27.17 | 932,866 | |
Slower rate of decline in ppFEV1 | BSC | 1,345,424 | 18.35 | Ref |
ELX-TEZ-IVA | 10,363,468 | 28.90 | 855,150 | |
Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSC | 1,369,429 | 18.48 | Ref |
ELX-TEZ-IVA | 9,538,670 | 27.02 | 956,907 |
BSC = best supportive care; ELX = elexacaftor; F/F = homozygous for F508del mutation; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; ppFEV1 = percent predicted forced expiratory volume in 1 second; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
CADTH also conducted 2 additional scenario analyses for the F/G genotype where 50% and 98% price reductions with IVA were assumed, respectively. Fifty percent was arbitrarily chosen to provide information on the potential magnitude of a price reduction for IVA on the ICER, while 98% was based on the suggested price reduction included as part of the CADTH Canadian Drug Expert Committee reimbursement recommendation conditions for IVA for the F/G genotype.29 Based on a 50% price reduction for IVA, in the CADTH base case, the ICER increased to more than $1.5M per QALY, while at a 98% price reduction for IVA, in the CADTH base-case ICER increased to more than $2.6M per QALY.
Issues for Consideration
TEZ-IVA (Symdeko) is indicated in Canada for the treatment of patients 12 years of age or older who are homozygous for the F508del mutation or who are heterozygous for the F508del mutation and have 1 of the following mutations in the CFTR gene: P67L, D110H, R117C, L206W, R352Q, A455E, D579G, 711 + 3A→G, S945L, S977F, R1070W, D1152H, 2789 + 5G→A, 3272 to 26A→G, and 3849 + 10kbC→T. It was not submitted to CADTH for appraisal. LUM-IVA (Orkambi) is indicated for a subset of the population in Canada who are aged 2 years or older and homozygous for the F508del mutation, but it did not receive a positive listing recommendation from CADTH. The cost-effectiveness of ELX-TEZ-IVA in comparison to either drug is unknown.
IVA was previously reviewed by CADTH in 2015. IVA received a recommendation to list, with 1 of the conditions being a substantial reduction in price of approximately 98%.29 The publicly available list price of IVA is the same as the price that was submitted to CADTH in 2015, and it was the value used in the sponsor’s submission. ELX-TEZ-IVA was not considered cost-effective in comparison with IVA in the CADTH base case for the F/G genotypes, and this does not account for any confidential price reductions for IVA. This was explored in part in scenario analyses.
Data informing treatment efficacy with ELX-TEZ-IVA for 3 of the 4 genotypes were from trials that included a run-in period, and as a result, these trial populations consisted of treatment exposed or experienced patients. The majority of patients indicated for treatment with ELX-TEZ-IVA in Canadian clinical practice will be treatment naive. It is unclear what the direction of bias may be.
Overall Conclusions
The clinical evidence submitted by the sponsor demonstrated that ELX-TEZ-IVA led to statistically and clinically significant improvements in acute ppFEV1, weight-for-age z score, and pulmonary exacerbation rates. The sponsor conducted an ITC to inform |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| in the absence of direct evidence of ELX-TEZ-IVA with IVA and BSC. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| are associated with uncertainty due to key differences in the designs of included trials. There was no evidence on the long-term impact of ELX-TEZ-IVA on the rate of decline of ppFEV1, or pulmonary exacerbation rates beyond the trial period.
Beyond a lack of evidence on the long-term benefits of ELX-TEZ-IVA and the issues with the sponsor’s submitted ITC, CADTH identified several additional major limitations with the submitted economic evaluation. The sponsor included several assumptions around drug costs and health care resource use, including dynamic drug pricing due to generic entry, adjusting drug costs for patient compliance, and the exclusion of disease management costs for the period for which ELX-TEZ-IVA was associated with a survival benefit. These assumptions led to an underestimation of the total drug acquisition and health care costs associated with ELX-TEZ-IVA. The sponsor also included a treatment-specific utility increment to account for the impact of treatment with ELX-TEZ-IVA beyond its impact mediated via ppFEV1 and pulmonary exacerbations, but the estimate by the sponsor likely leads to double counting of benefits already incorporated in the model.
Several of these limitations were addressed in the CADTH base-case reanalysis. Changes to the model included: the removal of an additional benefit of ELX-TEZ-IVA or IVA on the long-term rate of decline in ppFEV1 and pulmonary exacerbations beyond those mediated by ppFEV1; the removal of dynamic pricing of ELX-TEZ-IVA or IVA; the inclusion of costs for ELX-TEZ-IVA in the period for which it achieved a survival benefit in comparison with BSC; the removal of an adjustment to drug acquisition costs by patient compliance; and the removal of a treatment-specific utility increment for patients on ELX-TEZ-IVA. In comparison with BSC, the CADTH base-case analysis resulted in an ICER of $1,140,840 per QALY in the F/F genotype, $1,150,105 per QALY in the F/MF genotype, and $1,911,977 per QALY in the F/RF genotype. For the F/G genotype, ELX-TEZ-IVA was associated with an ICER of $1,067,215 when compared with BSC. A pairwise ICER of $181,718 per QALY was estimated in comparison with IVA monotherapy. This analysis only considered the publicly available list price of IVA, and the ICER would likely be substantially higher should the confidential price paid by public drug plans be significantly lower.
The key drivers in the analysis were the acquisition costs of ELX-TEZ-IVA, as well assumptions related to the long-term benefits associated with ELX-TEZ-IVA, which were uncertain. ELX-TEZ-IVA was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY in any scenario conducted by CADTH, including scenarios where CADTH reincorporated the additional long-term benefits on reducing the rate of decline of ppFEV1, additional benefit on rates of pulmonary exacerbations, or the on-treatment utility increment with ELX-TEZ-IVA. Uncertainty remains, as CADTH was unable to address limitations with the ITC which informed the acute increases in ppFEV1 and weight-for-age z score for 3 of the 4 genotypes. A price reduction in excess of 90% for ELX-TEZ-IVA is required for all 4 genotypes in order for ELX-TEZ-IVA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trikafta (triple combination therapy [elexacaftor/tezacaftor/ivacaftor & ivacaftor]) tablets, oral 100 mg/50 mg/75 mg and 150 mg. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2021 Jan 22.
2.Trikafta®, 100 mg elexacaftor, 50 mg tezacaftor, 75 mg ivacaftor (combination tablet) and 150 mg ivacaftor [product monograph]. Toronto (ON): Vertex Pharmaceuticals (Canada) Incorporated; 2020 Nov 11.
3.Liou TG, Adler FR, Fitzsimmons SC, Cahill BC, Hibbs JR, Marshall BC. Predictive 5-year survivorship model of cystic fibrosis. Am J Epidemiol. 2001;153(4):345-352. PubMed
4.Stephenson AL, Tom M, Berthiaume Y, et al. A contemporary survival analysis of individuals with cystic fibrosis: a cohort study. Eur Respir J. 2015;45(3):670-679. PubMed
5.Wainwright CE, Elborn JS, Ramsey BW, et al. Lumacaftor–ivacaftor in patients with cystic fibrosis homozygous for Phe508del CFTR. N Engl J Med. 2015;373(3):220-231. PubMed
6.Taylor-Cousar JL, Munck A, McKone EF, et al. Tezacaftor–ivacaftor in patients with cystic fibrosis homozygous for Phe508del. N Engl J Med. 2017;377(21):2013-2023. PubMed
7.Clinical Study Report: study 103. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are homozygous for the F508del mutation (F/F) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jun 18.
8.Clinical Study Report: study 109. A phase 3b, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Oct 16.
9.Clinical Study Report: study 102. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2019 Jul 2.
10.Rowe SM, Daines C, Ringshausen FC, et al. Tezacaftor-ivacaftor in residual-function heterozygotes with cystic fibrosis. N Engl J Med. 2017;377(21):2024-2035. PubMed
11.Ramsey BW, Davies J, McElvaney NG, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med. 2011;365(18):1663-1672. PubMed
12.De Boeck K, Munck A, Walker S, et al. Efficacy and safety of ivacaftor in patients with cystic fibrosis and a non-G551D gating mutation. J Cyst Fibros. 2014;13(6):674-680. PubMed
13.Clinical Study Report: study 104. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of elexacaftor combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a gating or residual function mutation (F/G and F/RF Genotypes) [internal sponsor's report]. Toronto (ON): Vertex Pharmaceuticals Incorporated; 2020 Aug 21.
14.Whiting P, Al M, Burgers L, et al. Ivacaftor for the treatment of patients with cystic fibrosis and the G551D mutation: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2014;18(18):1-106. PubMed
15.Leung GJ, Cho TJ, Kovesi T, Hamid JS, Radhakrishnan D. Variation in lung function and nutritional decline in cystic fibrosis by genotype: an analysis of the Canadian cystic fibrosis registry. J Cyst Fibros. 2020;19(2):255-261. PubMed
16.Goss CH, Burns JL. Exacerbations in cystic fibrosis. 1: Epidemiology and pathogenesis. Thorax. 2007;62(4):360-367. PubMed
17.Suthoff ED, Bonafede M, Limone B, O'Callaghan L, Sawicki GS, Wagener JS. Healthcare resource utilization associated with ivacaftor use in patients with cystic fibrosis. J Med Econ. 2016;19(9):845-851. PubMed
18.Stephenson AL, Sykes J, Berthiaume Y, et al. Clinical and demographic factors associated with post-lung transplantation survival in individuals with cystic fibrosis. J Heart Lung Transplant. 2015;34(9):1139-1145. PubMed
19.Solem CT, Vera-Llonch M, Tai M, O’Callaghan L. Pulmonary exacerbations, lung dysfunction, and Eq-5d measures in adolescents and adults with cystic fibrosis and homozygous for the F508del-Cftr mutation. Value Health. 2016;19(3):A116-A117.
20.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health, Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Apr 22.
21.Government of Saskatchewan Drug Plan and Extended Benefits Branch. Pan-Canadian generics. Pan-Canadian tiered pricing framework. 2014: http://formulary.drugplan.health.gov.sk.ca/PanCanadianGenerics. Accessed 2021 Apr 22.
22.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 Apr 22.
23.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2021 Apr 22.
24.Skolnik K, Ronksley P, Pendharkar S, Wick J, Quon B. Hospitalization-related costs for canadian cystic fibrosis patients. Pedatr Pulmonol. 2018;53(S2):S148-S456.
25.Feng LB, Grosse SD, Green RF, Fink AK, Sawicki GS. Precision medicine in action: the impact of ivacaftor on cystic fibrosis-related hospitalizations. Health Aff (Millwood). 2018;37(5):773-779. PubMed
26.Hassan M, Bonafede M, Limone B, Hodgkins P, Suthoff E, Sawicki G. 28 Reduction in pulmonary exacerbations (PEx) after initiation of ivacaftor: a retrospective cohort study among patients with cystic fibrosis (CF) treated in real-world settings. J Cyst Fibros. 2016;15.
27.Government of Alberta. Alberta Interactive Health Data Application. Average cost of lung transplant procedure in 2017/2018. 2019; http://www.ahw.gov.ab.ca/IHDA_Retrieval/. Accessed 2021 Apr 22.
28.Vasiliadis H-M, Collet J-P, Penrod JR, Ferraro P, Poirier C. A cost-effectiveness and cost-utility study of lung transplantation. J Heart Lung Transplant. 2005;24(9):1275-1283. PubMed
29.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: ivacaftor. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/ivacaftor-13. Accessed 2021 Apr 21.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 11: CADTH Cost Comparison Table of CFTR modulator therapies for Cystic Fibrosis
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Elexacaftor/ Tezacaftor/ Ivacaftor (Trikafta) | 100 mg/ 50 mg/ 75 mg | Tablet | 280.0000a | Two tablets in the morning | 560.00 | 204,400 |
Ivacaftor | 150 mg | Tablet | 280.0000a | 150 mg in evening at least 12 hours apart from Elexacaftor/ Tezacaftor/ Ivacaftor dose | 280.00 | 102,200 |
Regimen cost | 840.00 | 306,600 | ||||
CFTR modulator therapies | ||||||
Ivacaftor (Kalydeco) | 150 mg | Tablet | 420.0000 | 150 mg twice daily | 840.00 | 306,600 |
Lumacaftor/ Ivacaftor (Orkambi) | 200 mg/ 125 mg | Tablet | 170.5357b | 400/250 mg every 12 hours | 682.14 | 248,982 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed February 2021), unless otherwise indicated, and do not include dispensing fees.
aSponsor-submitted price.
bPrice obtained from IQVIA Delta PA database for the Association québécoise des pharmaciens propriétaires. It is identical to the price in the 2018 submission of Orkambi to CADTH.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | No | Model lacks transparency with regards to programming, and changes to certain parameters lead to results that do not meet face validity. See key limitations section. |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
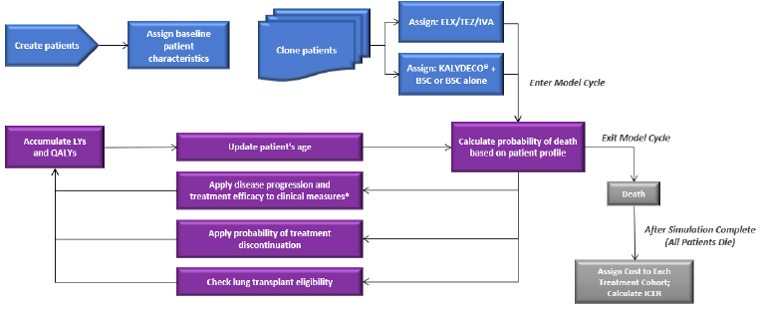
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results – F/F Genotype
Parameter | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 28.17 | 20.66 | 7.51 |
Discounted QALYs | |||
Total | 25.52 | 18.36 | 7.16 |
Discounted costs | |||
Total | $9,524,895 | $1,353,297 | $8,171,598 |
Drug Acquisition | $8,112,593 | $0 | $8,112,593 |
Non-PEx-Related Disease Management Costs | $518,110 | $409,314 | $108,796 |
PEx-Related Costs | $886,012 | $933,740 | -$47,728 |
Lung Transplant Costs | $5,488 | $8,438 | -$2,949 |
Adverse Event Cost | $2,477 | $1,805 | $672 |
Monitoring Cost | $214 | $0 | $214 |
ICER ($/QALY) | 1,140,840 | ||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results – F/MF Genotype
Parameter | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 27.78 | 20.59 | 7.20 |
Discounted QALYs | |||
Total | 25.22 | 18.33 | 6.88 |
Discounted costs | |||
Total | $9,244,232 | $1,327,598 | $7,916,634 |
Drug Acquisition | $7,880,106 | $0 | $7,880,106 |
Non-PEx-Related Disease Management Costs | $503,128 | $406,935 | $96,193 |
PEx-Related Costs | $852,829 | $911,056 | -$58,226 |
Lung Transplant Costs | $4,596 | $7,809 | -$3,212 |
Adverse Event Cost | $3,361 | $1,799 | $1,563 |
Monitoring Cost | $211 | $0 | $211 |
ICER ($/QALY) | 1,150,105 | ||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 15: Disaggregated Summary of CADTH’s Economic Evaluation Results – F/RF Genotype
Parameter | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 23.77 | 20.36 | 3.41 |
Discounted QALYs | |||
Total | 21.73 | 18.37 | 3.35 |
Discounted costs | |||
Total | $7,585,224 | $1,172,463 | $6,412,761 |
Drug Acquisition | $6,465,606 | $0 | $6,465,606 |
Non-PEx-Related Disease Management Costs | $436,389 | $397,331 | $39,058 |
PEx-Related Costs | $680,237 | $772,516 | -$92,279 |
Lung Transplant Costs | $249 | $790 | -$541 |
Adverse Event Cost | $2,556 | $1,827 | $730 |
Monitoring Cost | $186 | $0 | $186 |
ICER ($/QALY) | 1,911,977 | ||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; PEx = pulmonary exacerbations; QALY = quality-adjusted life-year; TEZ = tezacaftor.
Table 16: Disaggregated Summary of CADTH’s Economic Evaluation Results – F/Gating Genotype
Parameter | ELX-TEZ-IVA | IVA | Incremental | ELX-TEZ-IVA | BSC | Incremental |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 28.27 | 25.51 | 2.76 | 28.27 | 21.14 | 7.12 |
Discounted QALYs | ||||||
Total | 25.81 | 23.11 | 2.70 | 25.81 | 18.99 | 6.82 |
Discounted costs | ||||||
Total | $8,544,374 | $8,053,502 | $490,872 | $8,544,374 | $1,265,862 | $7,278,512 |
Drug Acquisition | $7,431,590 | $6,879,992 | $551,597 | $7,431,590 | $0 | $7,431,590 |
Non-PEx-Related Disease Management Costs | $479,679 | $455,988 | $23,691 | $479,679 | $415,471 | $64,208 |
PEx-Related Costs | $627,687 | $712,727 | -$85,040 | $627,687 | $843,954 | -$216,266 |
Lung Transplant Costs | $2,212 | $2,926 | -$733 | $2,212 | $4,569 | -$2,357 |
Adverse Event Cost | $3,001 | $1,670 | $1,331 | $3,001 | $1,869 | $1,133 |
Monitoring Cost | $205 | $198 | $7 | $205 | $0 | $205 |
ICER ($/QALY) | 181,718 | 1,067,215 | ||||
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; LY = life-year; QALY = quality-adjusted life-year; PEx = pulmonary exacerbations; TEZ = tezacaftor.
Table 17: Summary of the Stepped Analysis of the CADTH Reanalysis Results – F/MF Genotype
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 1,311,789 | 18.20 | Ref |
ELX-TEZ-IVA | 5,837,906 | 30.79 | 359,597 | |
CADTH reanalysis 1 | BSCa | 1,498,933 | 21.91b | Ref |
ELX-TEZ-IVA | 5,464,167 | 28.62 | 591,045 | |
CADTH reanalysis 2 | BSCa | 1,320,056 | 18.20 | Ref |
ELX-TEZ-IVA | 5,874,309 | 30.08 | 383,526 | |
CADTH reanalysis 3 | BSCa | 1,317,038 | 18.23 | Ref |
ELX-TEZ-IVA | 7,740,588 | 30.72 | 514,277 | |
CADTH reanalysis 4 | BSCa | 1,311,789 | 18.20 | Ref |
ELX-TEZ-IVA | 6,070,997 | 30.79 | 378,116 | |
CADTH reanalysis 5 | BSCa | 1,305,465 | 18.40 | Ref |
ELX-TEZ-IVA | 7,177,922 | 31.11 | 461,789 | |
CADTH reanalysis 6 | BSCa | 1,291,696 | 18.41 | Ref |
ELX-TEZ-IVA | 5,939,935 | 30.96 | 370,303 | |
CADTH reanalysis 7 | BSCa | 1,321,835 | 18.22 | Ref |
ELX-TEZ-IVA | 5,840,781 | 29.30 | 407,940 | |
CADTH reanalysis 8 | BSCa | 1,320,181 | 18.324 | Ref |
ELX-TEZ-IVA | 5,840,613 | 30.84 | 358,608 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) | BSCa | 1,327,598 | 18.33 | Ref |
ELX-TEZ-IVA | 9,244,232 | 25.22 | 1,150,105 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aReference product is least costly alternative.
bSponsor’s model produced results which do not meet face validity.
Table 18: Summary of the Stepped Analysis of the CADTH Reanalysis Results – F/RF Genotype
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 1,166,549 | 18.35 | Ref |
ELX-TEZ-IVA | 4,948,789 | 25.47 | 531,195 | |
CADTH reanalysis 1 | BSCa | 1,202,778 | 18.25 | Ref |
ELX-TEZ-IVA | 4,880,389 | 24.33 | 604,469 | |
CADTH reanalysis 2 | BSCa | 1,166,549 | 18.48 | Ref |
ELX-TEZ-IVA | 4,988,492 | 24.46 | 637,370 | |
CADTH reanalysis 3 | BSCa | 1,171,595 | 18.23 | Ref |
ELX-TEZ-IVA | 6,260,521 | 25.40 | 709,672 | |
CADTH reanalysis 4 | BSCa | 1,171,838 | 18.30 | Ref |
ELX-TEZ-IVA | 5,079,849 | 25.51 | 541,803 | |
CADTH reanalysis 5 | BSCa | 1,164,440 | 18.50 | Ref |
ELX-TEZ-IVA | 6,074,822 | 25.74 | 677,980 | |
CADTH reanalysis 6 | BSCa | 1,153,131 | 18.71 | Ref |
ELX-TEZ-IVA | 5,070,063 | 25.81 | 551,905 | |
CADTH reanalysis 7 | BSCa | 1,179,227 | 18.32 | Ref |
ELX-TEZ-IVA | 4,955,493 | 24.38 | 623,279 | |
CADTH reanalysis 8 | BSCa | 1,163,093 | 18.33 | Ref |
ELX-TEZ-IVA | 4,956,263 | 25.42 | 535,262 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) | BSCa | 1,172,463 | 18.37 | Ref |
ELX-TEZ-IVA | 7,585,224 | 21.73 | 1,911,977 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aReference product is least costly alternative.
Table 19: Summary of the Stepped Analysis of the CADTH Reanalysis Results – F/Gating Genotype
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | BSCa | 1,254,845 | 18.90 | Ref |
ELX-TEZ-IVA | 5,439,607 | 30.75 | 353,239 | |
IVA | 4,357,458 | 26.53 | Ref | |
ELX-TEZ-IVA | 5,439,607 | 30.75 | 256,956 | |
CADTH reanalysis 1 | BSCa | 1,417,560 | 22.65b | Ref |
ELX-TEZ-IVA | 5,341,212 | 29.04 | 614,513 | |
IVA | 4,352,171 | 27.68 | Ref | |
ELX-TEZ-IVA | 5,341,212 | 29.05 | 727,929 | |
CADTH reanalysis 2 | BSCa | 1,265,797 | 18.96 | Ref |
ELX-TEZ-IVA | 5,424,868 | 30.26 | 367,840 | |
IVA | 4,386,440 | 26.29 | Ref | |
ELX-TEZ-IVA | 5,424,868 | 30.26 | 261,530 | |
CADTH reanalysis 3 | BSCa | 1,256,288 | 18.84 | Ref |
ELX-TEZ-IVA | 7,222,595 | 30.63 | 506,256 | |
IVA | 6,929,905 | 26.42 | Ref | |
ELX-TEZ-IVA | 7,222,595 | 30.63 | 69,644 | |
CADTH reanalysis 4 | BSCa | 1,254,845 | 18.90 | Ref |
ELX-TEZ-IVA | 5,634,895 | 30.75 | 369,723 | |
IVA | 4,641,254 | 26.53 | Ref | |
ELX-TEZ-IVA | 5,634,895 | 30.75 | 235,940 | |
CADTH reanalysis 5 | BSCa | 1,249,417 | 19.07 | Ref |
ELX-TEZ-IVA | 6,715,024 | 31.07 | 455,536 | |
IVA | 5,299,034 | 26.84 | Ref | |
ELX-TEZ-IVA | 6,715,024 | 31.07 | 335,068 | |
CADTH reanalysis 6 | BSCa | 1,233,789 | 19.10 | Ref |
ELX-TEZ-IVA | 5,535,858 | 31.03 | 360,371 | |
IVA | 4,474,804 | 26.88 | Ref | |
ELX-TEZ-IVA | 5,535,858 | 31.03 | 255,502 | |
CADTH reanalysis 7 | BSCa | 1,264,522 | 18.84 | Ref |
ELX-TEZ-IVA | 5,445,807 | 29.48 | 393,180 | |
IVA | 4,356,746 | 26.40 | Ref | |
ELX-TEZ-IVA | 5,445,807 | 29.48 | 353,663 | |
CADTH reanalysis 8 | BSCa | 1,256,493 | 18.89 | Ref |
ELX-TEZ-IVA | 5,442,667 | 30.71 | 354,160 | |
IVA | 4,369,365 | 26.54 | Ref | |
ELX-TEZ-IVA | 5,442,667 | 30.71 | 257,488 | |
CADTH base case (1 + 2 + 3 + 4 + 5 + 6 + 7 + 8) | BSCa | 1,265,862 | 18.99 | Ref |
ELX-TEZ-IVA | 8,544,374 | 25.81 | 1,067,215 | |
IVA | 8,053,502 | 23.11 | Ref | |
ELX-TEZ-IVA | 8,544,374 | 25.81 | 181,718 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
aReference product is least costly alternative.
bSponsor’s model produced results which do not meet face validity.
Scenario Analyses
Table 20: CADTH Price Reduction Analyses – F/F Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 358,763 | 1,140,840 |
20% | 271,979 | 911,065 |
40% | 185,306 | 688,647 |
60% | 97,295 | 462,872 |
80% | 11,359 | 234,391 |
90% | Dominant | 122,809 |
95% | Dominant | 63,617 |
99% | Dominant | 26,127 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 21: CADTH Price Reduction Analyses – F/MF Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 359,597 | 1,150,105 |
20% | 271,340 | 890,600 |
40% | 181,556 | 691,087 |
60% | 97,436 | 454,045 |
80% | 19,244 | 228,823 |
90% | Dominant | 116,347 |
95% | Dominant | 59,734 |
99% | Dominant | 11,864 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 22: CADTH Price Reduction Analyses – F/RF Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 531,195 | 1,911,977 |
20% | 404,089 | 1,450,082 |
40% | 267,487 | 1,092,575 |
60% | 147,419 | 725,112 |
80% | 19,564 | 228,823 |
90% | Dominant | 163,565 |
95% | Dominant | 65,822 |
99% | Dominant | Dominant |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 23: CADTH Price Reduction Analyses – F/Gating Genotype
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | ICERs for ELX-TEZ-IVA vs. IVA ($/QALY) | ||
|---|---|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis | Sponsor base case | CADTH reanalysis |
No price reduction | 353,239 | 1,067,215 | 256,956 | 181,718 |
20% | 267,111 | 867,470 | 12,391 | Dominant |
40% | 178,019 | 646,511 | Dominant | Dominant |
60% | 94,534 | 416,675 | Dominant | Dominant |
80% | 9,081 | 197,655 | Dominant | Dominant |
90% | Dominant | 85,764 | Dominant | Dominant |
95% | Dominant | 32,146 | Dominant | Dominant |
99% | Dominant | Dominant | Dominant | Dominant |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 24: CADTH Price Reduction Analyses – Weighted Analysis, All Genotypes Combined
Analysis | ICERs for ELX-TEZ-IVA vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 366,677 | 1,158,851 |
20% | 274,342 | 905,132 |
40% | 181,030 | 675,441 |
60% | 89,643 | 431,471 |
80% | Dominant | 189,848 |
90% | Dominant | 71,348 |
95% | Dominant | 9,409 |
99% | Dominant | Dominant |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; vs. = versus.
Table 25: Summary of the CADTH Scenario Analyses – F/MF Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Long-term reduction in pulmonary exacerbations included for ELX-TEZ-IVA and IVA | BSCa | 1,315,201 | 18.39 | Ref |
ELX-TEZ-IVA | 9,235,037 | 26.74 | 948,352 | |
Slower rate of decline in ppFEV1 | BSCa | 1,317,115 | 18.28 | Ref |
ELX-TEZ-IVA | 10,087,862 | 28.66 | 844,774 | |
Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSCa | 1,344,233 | 18.50 | Ref |
ELX-TEZ-IVA | 9,299,255 | 26.99 | 937,242 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Table 26: Summary of the CADTH Scenario Analyses – F/RF Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Long-term reduction in pulmonary exacerbations included for ELX-TEZ-IVA and IVA | BSCa | 1,163,814 | 18.66 | Ref |
ELX-TEZ-IVA | 7,748,631 | 23.50 | 1,361,540 | |
Slower rate of decline in ppFEV1 | BSCa | 1,170,642 | 18.45 | Ref |
ELX-TEZ-IVA | 7,917,417 | 23.26 | 1,401,649 | |
Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSCa | 1,190,025 | 18.70 | Ref |
ELX-TEZ-IVA | 7,655,183 | 23.29 | 1,407,131 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Table 27: Summary of the CADTH Scenario Analyses – F/Gating Genotype
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Long-term reduction in pulmonary exacerbations included for ELX-TEZ-IVA and IVA | BSCa | 1,250,925 | 19.01 | Ref |
ELX-TEZ-IVA | 8,601,483 | 27.06 | 913,444 | |
IVA | 8,094,188 | 23.83 | Ref | |
ELX-TEZ-IVA | 8,601,483 | 27.06 | 156,872 | |
Slower rate of decline in ppFEV1 | BSCa | 1,258,673 | 18.94 | Ref |
ELX-TEZ-IVA | 9,269,970 | 28.96 | 799,838 | |
IVA | 9,002,579 | 26.19 | Ref | |
ELX-TEZ-IVA | 9,269,970 | 28.96 | 96,607 | |
Inclusion of treatment-specific utility increment for patients on ELX-TEZ-IVA | BSCa | 1,280,460 | 19.13 | Ref |
ELX-TEZ-IVA | 8,538,176 | 27.09 | 912,456 | |
IVA | 8,087,692 | 23.49 | Ref | |
ELX-TEZ-IVA | 8,538,176 | 27.09 | 125,123 | |
50% price reduction with IVA | IVA | 4,611,030 | 22.90 | Ref |
ELX-TEZ-IVA | 8,509,406 | 24.49 | 1,504,018 | |
98% price reduction with IVA | IVA | 1,324,151 | 23.07 | Ref |
ELX-TEZ-IVA | 8,556,441 | 25.76 | 2,682,202 |
BSC = best supportive care; ELX = elexacaftor; ICER = incremental cost-effectiveness ratio; IVA = ivacaftor; QALY = quality-adjusted life-year; TEZ = tezacaftor; Ref = reference.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 28: CADTH Summary Findings From the Sponsor’s Budget Impact Analysis
Key take-aways of the BIA |
|---|
|
ELX = elexacaftor; IVA = ivacaftor; TEZ = tezacaftor
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted an epidemiology-based budget impact analysis (BIA), assessing the expected budgetary impact of the reimbursement of ELX-TEZ-IVA and IVA for the treatment of CF in patients who are 12 years of age or older with at least 1 F508del-CFTR mutation. The analysis was conducted over a 3-year time horizon, from the perspective of Canadian public drug payers. The sponsor’s BIA considered a reference scenario which primarily consisted of BSC, with IVA monotherapy included as a comparator for patients heterozygous for a F508del-CFTR with a gating or R117H mutation on the second allele. The sponsor’s submission did not consider other CFTR modulators given they are not listed in Canadian jurisdictions. Key inputs to the BIA are documented in Table 29. The sponsor’s estimate of market size is primarily based on data generated from the Canadian CF Registry, and further reduced based on the proportion of patients covered by provincial formularies, Figure 2.
The sponsor also made the following key assumptions:
All patients with CF are captured in the Canadian CF patient registry.
70% of indicated patients would be covered by provincial drug programs, and the other 30% would have private insurance coverage.
The market uptake of ELX/ TEZ/ IVA and IVA would |||||||||||||||||||||||||||||| in Year 1, 2, and 3, respectively, for patients without a F508del/R117H or Gating genotype.
For patients with the F508del/Gating genotype 12 years of age or older or an F508del/R117H genotype 18 years of age or older|||||||||||||||||||||||||||| were assumed to switch from IVA to ELX/ TEZ/ IVA and IVA in Years1, 2, and 3, respectively. Additionally, the utilization rate of IVA was assumed to be |||| in each year.
Patients are 80% compliant with ELX/ TEZ/ IVA and IVA.
The diagnosis rate of CF with at least 1 an F508del-CFTR mutation is 100%.
Genotype-specific subpopulations grow at the same rate as the general CF population.
No drug mark-up or dispensing fees were considered in the base-case analyses.
All patients are assumed to receive background BSC at the same rate. These costs were assumed to cancel each other out and were not included in the sponsor’s analysis.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population

Source: Sponsor’s pharmacoeconomic submission1
Table 29: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review Patients naive to CFTR modulators Patients eligible for IVA | 2,046 / 2,080 / 2,115 77 / 78 / 80 |
Market Uptake (3 years) | |
Uptake (reference scenario) Patients naive to CFTR modulators Best supportive care Patients eligible for IVA Best supportive care IVA | |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |
Uptake (reference scenario) Patients naive to CFTR modulators ELX/ TEZ/ IVA and IVA Best supportive care Patients eligible for IVA ELX/ TEZ/ IVA and IVA Best supportive care IVA | |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||| |
Cost of treatment (per patient) | |
Cost of treatment per year, adjusted for 80% compliance ELX/ TEZ/ IVA and IVA Best supportive care IVA | $245,448 $0 $245,448 |
CFTR = cystic fibrosis transmembrane conductance regulator; ELX = elexacaftor; IVA = ivacaftor; TEZ = tezacaftor.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base-case estimates that the incremental budget impact associated with the reimbursement of ELX-TEZ-IVA and IVA for the treatment of CF in patients who are 12 years of age or older with at least 1 F508del-CFTR mutation would be $18,946,936 in Year 1, $97,434,723 in Year 2, and $270,432,262 in Year 3, for a cumulative 3-year budget impact of $386,812,921. The entire budget impact was estimated to be from patients naive to CFTR modulators, as the costs associated with ELX-TEZ-IVA and IVA and IVA were identical, thus leading to identical reference and new drug scenario costs in the population switching from IVA monotherapy.
The sponsor conducted several sensitivity analyses assessing the impact of alternative assumptions related to compliance rates, predicted utilization rates of ELX-TEZ-IVA and IVA, as well as increasing the size of the eligible patient population. All had a significant impact on results, with the greatest impact observed for the scenario assuming a 100% compliance rate, where the 3-year budget impact rose to $483,516,151. Additionally, the sponsor conducted a scenario analysis including mark-ups and dispensing fees. This scenario resulted in a 3-year budget impact of $407,484,178.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Anticipated uptake of ELX-TEZ-IVA in treatment-naive patients is underestimated. The sponsor assumed that the uptake of ELX-TEZ-IVA in the new drug scenario for patients for whom there are no publicly listed CFTR modulators (i.e., all genotypes included in the indication, except for patients with a gating or R117H mutation) would be |||| in the first year, |||||| in second year and 75% in the third. The clinical experts consulted by CADTH for this review considered these estimates to be vastly underestimated, and that between 90% and 100% of patients eligible for ELX-TEZ-IVA would be prescribed ELX-TEZ-IVA. The sponsor’s assumed market uptake vastly underestimated the total costs associated with the uptake of ELX-TEZ-IVA in the sponsor’s base case, leading to an underestimate of the total budget impact associated with ELX-TEZ-IVA.
CADTH assumed 95% of treatment-naive patients would receive ELX-TEZ-IVA in all 3 years of the BIA.
Compliance-adjusted drug costs underestimate the total costs associated with the uptake of ELX-TEZ-IVA to public drug plans. In their base case, the sponsor adjusted the price of ELX-TEZ-IVA by the assumed compliance rate (80%), with the assumption that savings would be incurred by public drug plans due to patients not being 100% compliant. There is limited evidence to support the real-world compliance rate with ELX-TEZ-IVA. Additionally, the full complement of ELX-TEZ-IVA would be dispensed, regardless of whether the patient was compliant, thus resulting in the full costs of treatment being incurred by the public drug payer. This underestimated the total costs associated with ELX-TEZ-IVA and its total budget impact.
CADTH assumed patients were 100% compliant in reanalyses, in alignment with the CADTH pharmacoeconomic base case.
Proportion of patients estimated to receive IVA in the reference scenario is not aligned with the sponsor’s submitted pharmacoeconomic model. According to the sponsor, |||||| of patients eligible to receive IVA monotherapy receive IVA. This is not aligned with the sponsor’s pharmacoeconomic model, which noted that an estimated |||||| of patients eligible to receive IVA monotherapy currently receive it. While this does not impact the sponsor’s base case, as patients eligible for IVA only switch to ELX-TEZ-IVA if they are receiving IVA monotherapy, and the costs thus cancel each other out, it does have an impact in analyses where patients eligible for IVA and not receiving IVA would switch to ELX-TEZ-IVA. In such a scenario, having more patients not on therapy with IVA who would then go on to receive ELX-TEZ-IVA would lead to additional incremental costs associated with ELX-TEZ-IVA.
CADTH addressed this in reanalyses by assuming 75% of patients eligible for IVA received IVA.
Assumption that patients eligible for IVA but not receiving it would elect not to receive ELX-TEZ-IVA is inappropriate. The sponsor assumed patients eligible for IVA but not receiving it would continue to not receive disease modifying drugs. Clinical expert feedback indicated that approximately half of patients eligible for IVA but not receiving IVA would be prescribed ELX-TEZ-IVA. This had limited impact on the sponsor’s base case, as they assumed a very small proportion of patients were not receiving IVA, but nonetheless underestimated the potential budget impact associated with ELX-TEZ-IVA.
CADTH assumed 95% of patients eligible for IVA but not receiving it would switch from BSC to ELX-TEZ-IVA.
Estimated proportion of patients with public coverage for CFTR modulator therapy is uncertain. The sponsor assumed 70% of the population indicated for ELX-TEZ-IVA would have public coverage, thus reducing the total eligible population size by 30%. The evidence cited by the sponsor for this assumption was internal data not available to CADTH, and uncertainty remains as to the proportion of the indicated population who would be covered by public drug plans. There is uncertainty in the proportion of patients with public versus private insurance. If more than 70% of the population would be covered, the anticipated budget impact associated with ELX-TEZ-IVA would be higher. If fewer are covered, the anticipated budget impact would be lower.
CADTH assumed 70% coverage in the base-case analysis, and tested scenarios of 50% coverage and 100% coverage.
CADTH Reanalyses of the Budget Impact Analysis
Based on the identified limitations, CADTH’s base-case analysis included changes to the anticipated market share of ELX-TEZ-IVA in all 3 years, the patient compliance rate, the proportion of patients eligible for IVA who are assumed to receive IVA, and the proportion of patients eligible for IVA not receiving IVA who would be prescribed ELX-TEZ-IVA. CADTH also corrected the sponsor’s base case to address an issue with the calculation of the number of treatment-naive patients eligible for ELX-TEZ-IVA. The calculations in the submitted model did not align with the expected population size based on the included parameters.
Table 30: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correction to sponsor’s base case | ||
1. Correction to formulas calculating number of patients expected to be treated with ELX-TEZ-IVA | Patient population size overestimated by a small amount and not aligned with expectations based on included parameters | Accurate population size estimates based on included parameters |
Changes to derive the CADTH base case | ||
1. Market share of ELX-TEZ-IVA | |||| Y1/ |||| Y2/ |||| Y3 | 95% Y1/ 95% Y2/ 95% Y3 |
2. Patient compliance on ELX-TEZ-IVA or IVA | 80% | 100% |
3. Proportion eligible for IVA receiving IVA in reference scenario | |||| | 75% |
4. Proportion of patients eligible for IVA but not receiving it who would receive ELX-TEZ-IVA | |||| | 50% |
CADTH base case | 1 + 2 + 3 + 4 | |
ELX = elexacaftor; IVZ = ivacaftor; TEZ = tezacaftor.
Applying these changes increased the total 3-year budget impact associated with the introduction of ELX-TEZ-IVA to $1,279,931,452. The results of the CADTH stepwise reanalysis are presented in summary format in Table 31 and a more detailed breakdown is presented in Table 32. Removing the adjustment of drug acquisition costs by patient compliance rate and the increasing the anticipated market share had the greatest impact.
Table 31: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $386,812,921 |
Submitted base case - corrected | $383,022,602 |
CADTH reanalysis 1 | $429,025,123 |
CADTH reanalysis 2 | $1,018,762,544 |
CADTH reanalysis 3 | $383,022,602 |
CADTH reanalysis 4 | $383,851,820 |
CADTH base case | $1,279,931,452 |
BIA = budget impact analysis.
CADTH also conducted scenario analyses considering:
The 99% price reduction needed to for ELX-TEZ-IVA to be as close as possible to a $50,000 per QALY willingness-to-pay threshold in the CADTH base-case economic evaluation
Drug acquisition costs being adjusted by a compliance rate of 80%
Public drug plan coverage of 50%
Public drug plan coverage of 100%
Market uptake of ELX-TEZ-IVA of 50% in all 3 years
Each of the scenarios produced results that differed from the CADTH base case. The scenario with the greatest impact was increasing public coverage to 100%, which lead to a 3-year total budget impact of $1,828,473,503. Reducing the market uptake to 50% nearly halved the anticipated budget impact to $676,716,788 over 3 years.
Table 32: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $12,831,385 | $13,047,017 | $13,266,273 | $13,489,213 | $39,802,503 |
New drug | $12,831,385 | $31,993,953 | $110,700,996 | $283,920,475 | $426,615,424 | |
Budget impact | $0 | $18,946,936 | $97,434,723 | $270,431,262 | $386,812,921 | |
CADTH base case | Reference | $12,530,650 | $12,741,228 | $12,955,345 | $13,173,059 | $38,869,632 |
New drug | $12,530,650 | $432,294,937 | $439,559,667 | $446,946,481 | $1,318,801,084 | |
Budget impact | $0 | $419,553,709 | $426,604,322 | $433,773,421 | $1,279,931,452 | |
CADTH scenario analysis: 99% price reduction | Reference | $12,530,650 | $12,741,228 | $12,955,345 | $13,173,059 | $38,869,632 |
New drug | $12,530,650 | $19,039,067 | $17,948,183 | $6,903,846 | $43,891,096 | |
Budget impact | $0 | $6,297,840 | $4,992,838 | $6,269,213 | $5,021,464 | |
CADTH sensitivity analysis – 80% Compliance | Reference | $10,024,520 | $10,192,982 | $10,364,276 | $10,538,448 | $31,095,705 |
New drug | $10,024,520 | 345,835,949 | $351,647,733 | $357,557,185 | $1,055,040,867 | |
Budget impact | $0 | $335,642,967 | $341,283,458 | $347,018,737 | $1,023,945,162 | |
CADTH sensitivity analysis – 50% public drug coverage | Reference | 8,950,464 | $9,100,877 | $9,253,818 | $9,409,328 | $27,764,023 |
New drug | $8,950,464 | $308,782,098 | $313,971,190 | $319,247,486 | $942,000,774 | |
Budget impact | $0 | $299,681,221 | $304,717,373 | $309,838,158 | $914,236,752 | |
CADTH sensitivity analysis – 100% public drug coverage | Reference | $17,900,928 | $18,201,754 | $18,507,635 | $18,818,656 | $55,528,045 |
New drug | $17,900,928 | $617,564,195 | $627,942,381 | $638,494,972 | $1,884,001,549 | |
Budget impact | $0 | $599,362,441 | $609,434,746 | $619,676,316 | $1,828,473,503 | |
CADTH sensitivity analysis – 50% market share | Reference | $12,530,650 | $12,741,228 | $12,955,345 | $13,173,059 | $38,869,632 |
New drug | $12,530,650 | $234,564,856 | $238,506,725 | $242,514,838 | $715,586,420 | |
Budget impact | $0 | $221,823,628 | $225,551,381 | $229,341,779 | $676,716,788 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.